Embed Size (px)
Citation preview
Psychotropics in pregnancy & the peripartum period:
impacts on fetus & neonate
Facundo Garcia-Bournissen, MD PhD Assistant Professor, Clinician Researcher
Division of Pediatric Clinical Pharmacology, Dept of Pediatrics, Children’s Hospital, LHSC
I have been a consultant at some time or another in the past 5 years, directly or indirectly, for several companies and organizations involved in pediatric drug development including DNDi, ELEA, Chemo, Savant, Kalobios, Eisai, Bayer, Inmunova, Novartis & GSK
I hold no commercial (or other) interests in any of these companies
My opinions are my own and do not necessarily agree with those of my employer(s), or those of my family, friends, coworkers, acquaintances, or anybody else

• To describe the role of the FRAME Clinic (Fetal Risk Assessment from Maternal Exposure)
• To understand the nature and extent of the potential risks and benefits associated to women exposure to psychotropics during pregnancy
• To review principles of risk evaluation for psychotropic exposure during pregnancy
• To describe neonatal manifestations of psychotropic use during pregnancy and lactation

Questions, or patients to refer… Give us a call! 519-685-8500 ext 58293
Fax: 519-685-8156
• Scarcity of data on risk of medications to the developing fetus
• Unfortunately, collecting data requires “accidents” (e.g. pregnant women taking medications before they know they are pregnant, or because they cannot stop them)
• “Accidents” take time to happen…

• Very few clinical trials enroll pregnant women (or women in general…)
• However, many women have conditions that require medications, and many of these women get pregnant, or desire to get pregnant
• Many diseases, if untreated, may represent a risk for the developing fetus (e.g. asthma, epilepsy, depression, psychosis, infections, etc)
• Appropriate pharmacological management of certain conditions is in fact beneficial for the pregnancy
• >80% of agents known to produce defects in humans also cause defects in at least one test animal
• However, many drugs (>1,200!) that cause malformations in some animal models are known NOT to cause malformations in humans
• Animal data can’t always be extrapolated to humans: • Considerable variability between species (and even strains)
• Lab animals are generally inbred, and have their own set of common malformations (e.g. kidney in rats)
• Behavioral and intellectual effects of medications are difficult to recognize in animals
• Nobody should take medications they don’t need…
• But patients should receive (and deserve) the most effective and safer treatments available
• In many (most, actually) cases, there are no good reasons to deny effective treatments to pregnant women
• In some cases, people just don’t care, or may not think that there may not be risks for them or their pregnancy…
• As average age of pregnancy increases, more and more women get pregnant while also needing treatment for chronic conditions
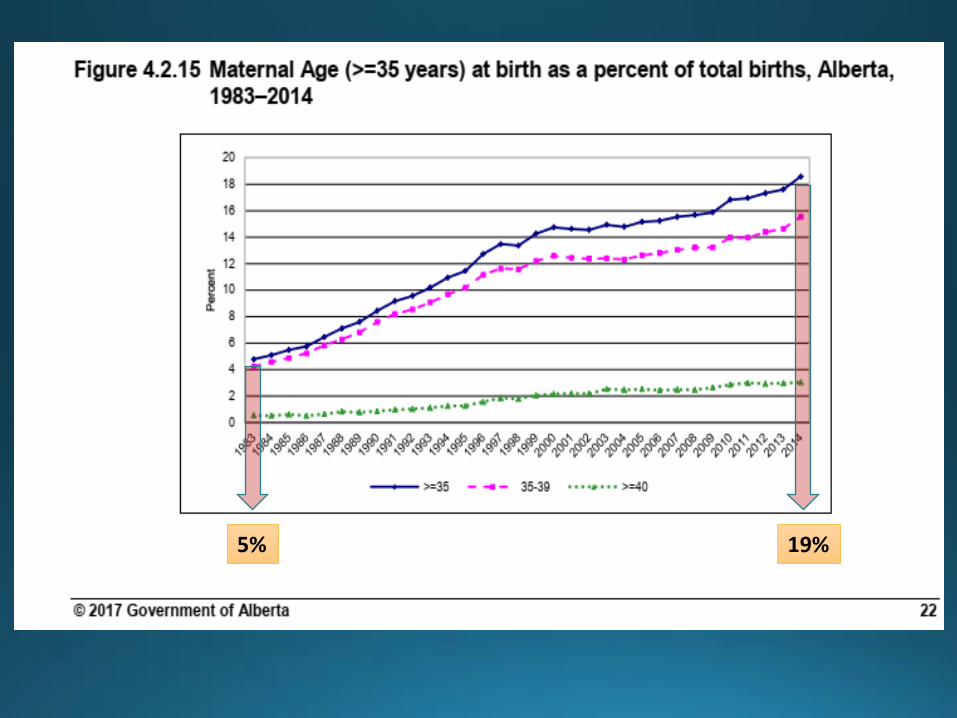
5% 19%
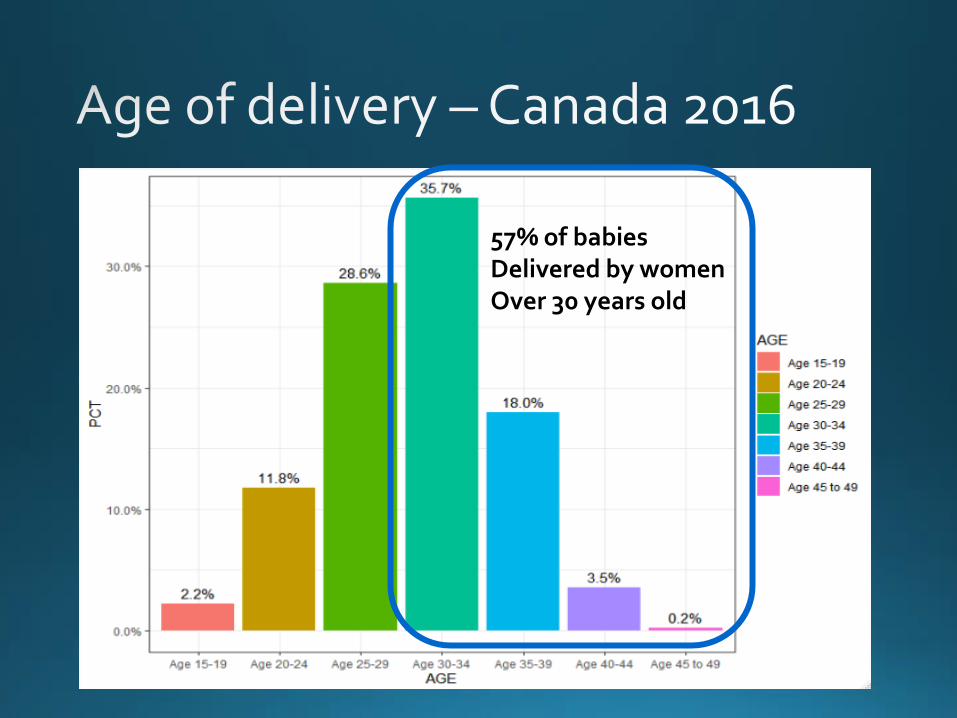
57% of babies Delivered by women Over 30 years old
• Right to health (WHO): right of everyone to enjoy the highest attainable standard of physical and mental health
• This is a human right.
•Women are humans.
• therefore they have a right to safe and effective medications to support their health, irrespective of life stage (e.g. pregnancy, lactation, etc)
The question should be:
“if a pregnant woman needs a medication, why doesn’t she receive it?”
• >90% of pregnant women take some medication (average of 2.9 prescriptions)
• <10% of medications approved from 1980 to 2010 have sufficient data to determine fetal risks
• Most drugs are not labeled for use in pregnancy
• Risks (real or perceived) of medications to the fetus a significant source of anxiety for pregnant women and their families
• <50% pregnancies are planned
Mitchell et al. Am J Obstet Gynecol. 2011 Jul; 205(1):51.e1-8. Adam et al. Am J Med Genet C Semin Med Genet. 2011 Aug 15; 157C(3):175-82.
• There’s over 3000 FDA-approved drugs
• Only small fraction (<2%) has been associated with substantial teratogenic risk
• It takes >6 years since approval to determine risk
• (if it exists… it takes decades to show that there is no risk!)
Lo et al. Obstet Gynecol 2002;100:465-73

• The placenta goes through many different developmental stages during the pregnancy, becoming increasingly complex
• Although it might prevent some drugs from crossing into the fetus, as a general rule, it does NOT
• Most drugs can be assumed to make its way into fetal circulation to some extent, with few exceptions
• Teratogen: a substance (e.g. drug) that can affect fetal growth or development, leading to a structural or functional defect, or fetal death
• Major malformations: life-threatening or requiring surgical correction (prevalence ~1-3% of live births)
• Minor malformations: not life threatening or requiring surgical correction. Many go unnoticed. (Actual prevalence???)
• Functional defects: Growth delays, learning / intellectual deficits, neurobehavioral and metabolic / biochemical anomalies
• Teratogen: a substance (e.g. drug) that can affect fetal growth or development, leading to a structural or functional defect, or fetal death
• Major malformations: life-threatening or requiring surgical correction (prevalence ~1-3% of live births)
• Minor malformations: not life threatening or requiring surgical correction. Many go unnoticed. (Actual prevalence???)
• Functional defects: Growth delays, learning / intellectual deficits, neurobehavioral and metabolic / biochemical anomalies
Most are NOT drug related (we think…)
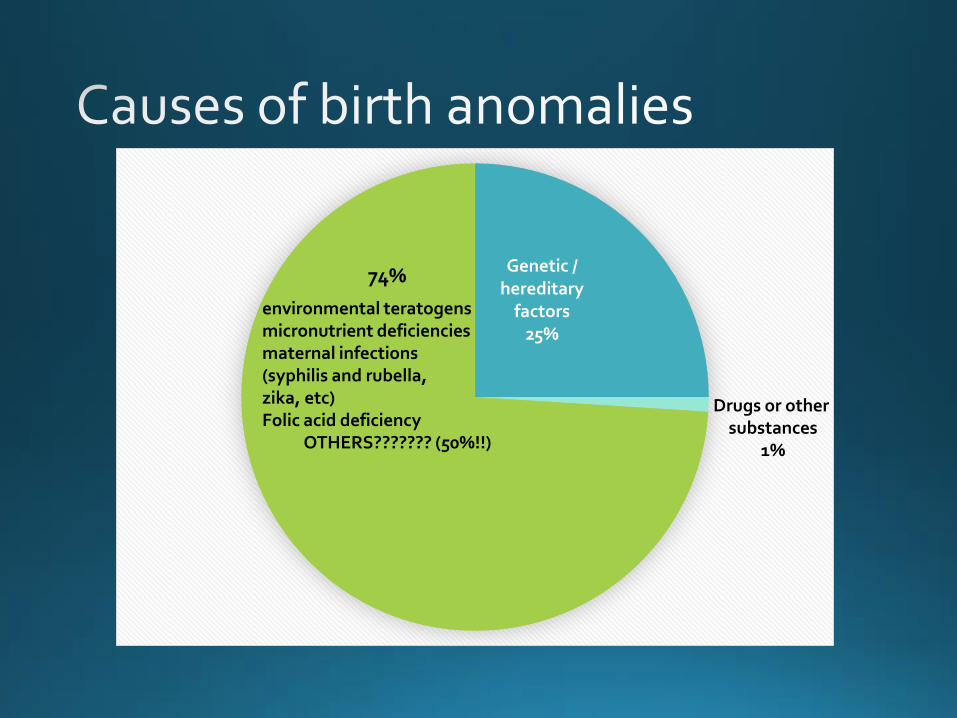
Genetic / hereditary
factors 25%
74%
environmental teratogens micronutrient deficiencies maternal infections (syphilis and rubella, zika, etc) Folic acid deficiency OTHERS??????? (50%!!)
Drugs or other substances
1%
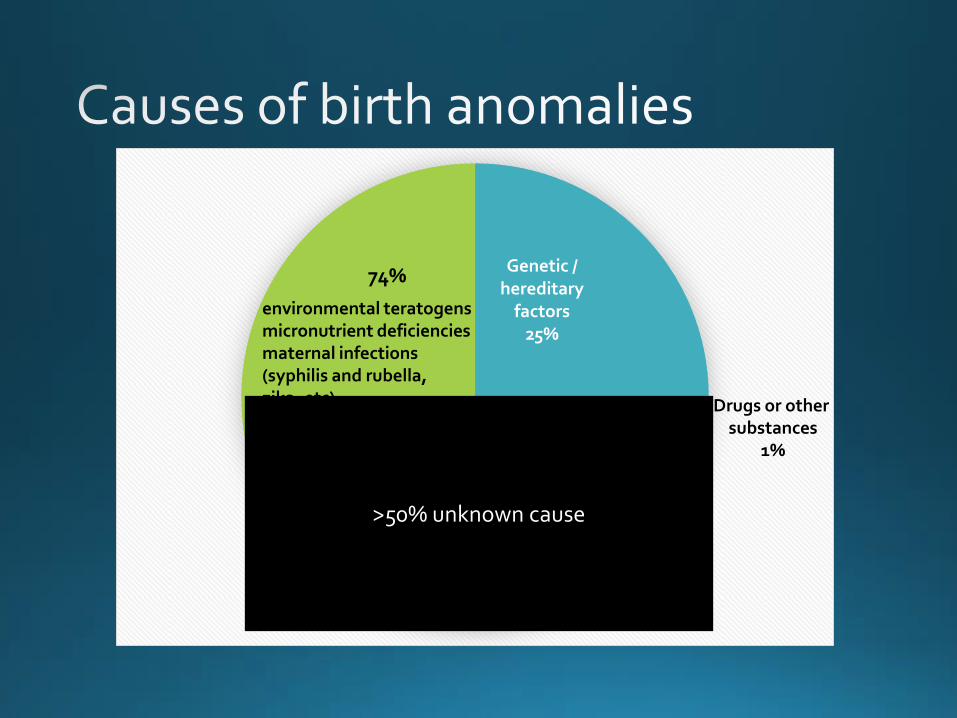
Genetic / hereditary
factors 25%
74%
environmental teratogens micronutrient deficiencies maternal infections (syphilis and rubella, zika, etc) Folic acid deficiency OTHERS??????? (50%!!)
Drugs or other substances
1%
>50% unknown cause
20
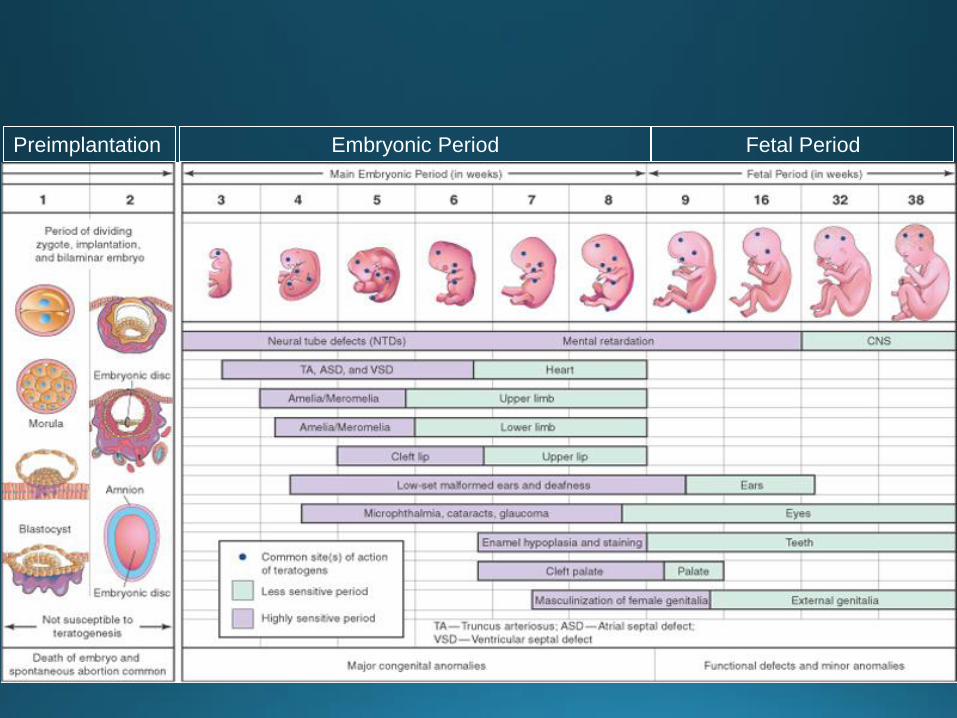
Preimplantation Embryonic Period Fetal Period
21
Preimplantation Embryonic Period Fetal Period
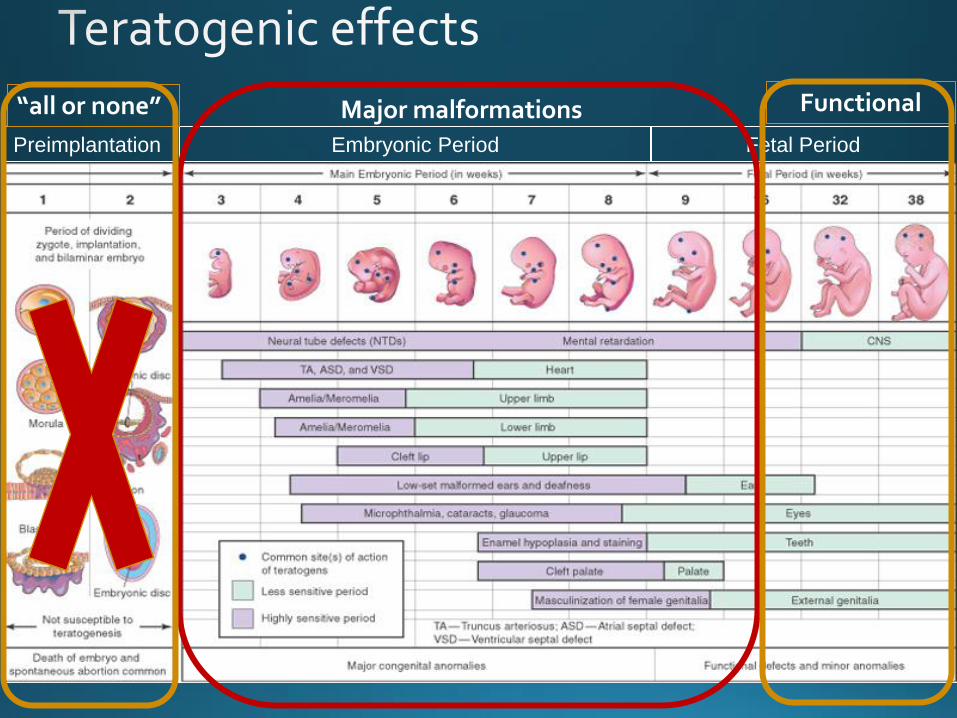
Major malformations Functional “all or none”
• Timing of exposure (sensitive period) • Early exposures (“all or none” period) -> increase in spontaneous
abortions
• Organogenesis period -> Major malformations -> depend on timing and drug effect
• Functional effects -> Could, in theory, take place at any time, but timing and drug effect play a role (e.g. ACEI, immunosuppressors)
• Brain development is a continuum (about which we know little about!)
• Dose of drug (threshold, dose-response)
• Genetic susceptibility
• If a baby is born with a malformation -> 99/100 times is NOT due to a drug or toxin
• When counseling pregnant women taking medications: • risks depend on medication & maternal disease
• Consider maternal risks of untreated disease
• When counseling women planning to get pregnant, risks depends on: • medication
• maternal disease
• Availability and risks of alternative treatments (e.g. mycophenolate vs azathioprine)

• Risk of major malformation = 2 – 4% at birth
• Assessment of magnitude of increase in risk above baseline is important
• Need to put risk in perspective: • Every pregnancy has, in average, a 97% chance (or risk…) of a
healthy baby
• These 97% chances are decreased to some extent by age, genetics and sometimes drugs and environmental factors
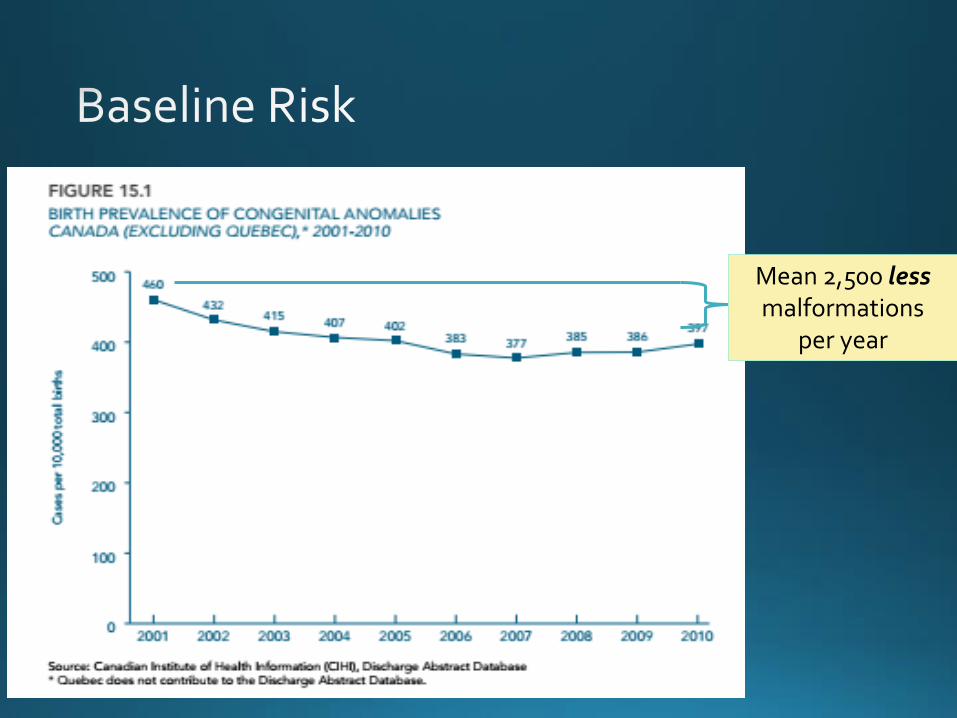
Mean 2,500 less malformations
per year
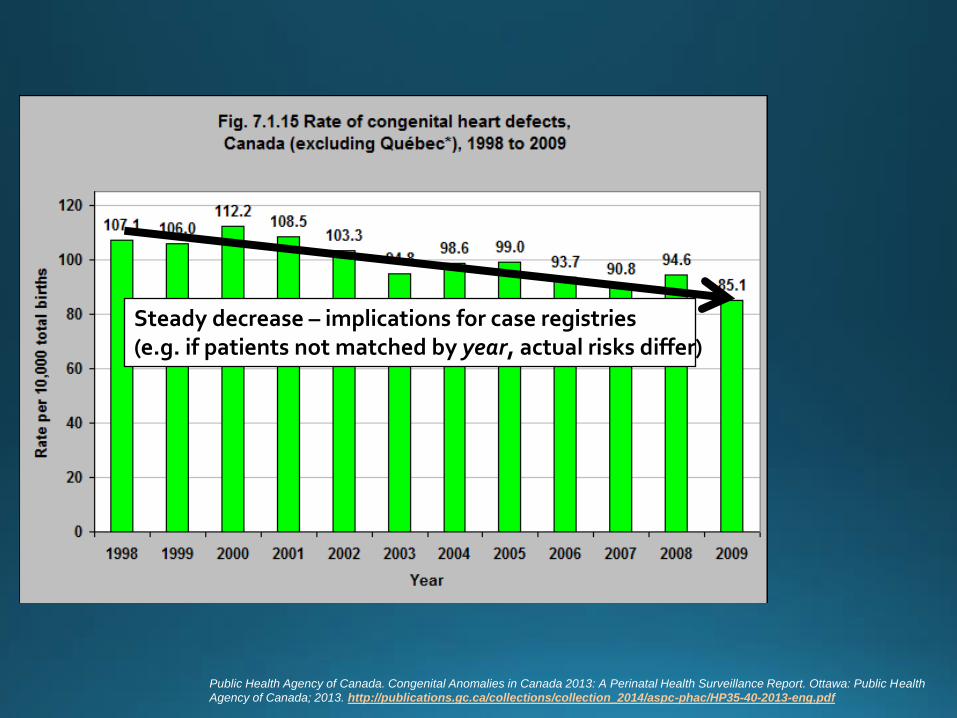
Public Health Agency of Canada. Congenital Anomalies in Canada 2013: A Perinatal Health Surveillance Report. Ottawa: Public Health
Agency of Canada; 2013. http://publications.gc.ca/collections/collection_2014/aspc-phac/HP35-40-2013-eng.pdf
Steady decrease – implications for case registries (e.g. if patients not matched by year, actual risks differ)

Br Med J (Clin Res Ed). 1987 Oct 31;295(6606):1100.
Expected births
Actual
Approximately 2,500 pregnancies were terminated
Throughout Europe, an estimated 10,000 – 15,000
pregnancies were terminated out of fear (unwarranted)
Misinformation and fear can also be “teratogens”
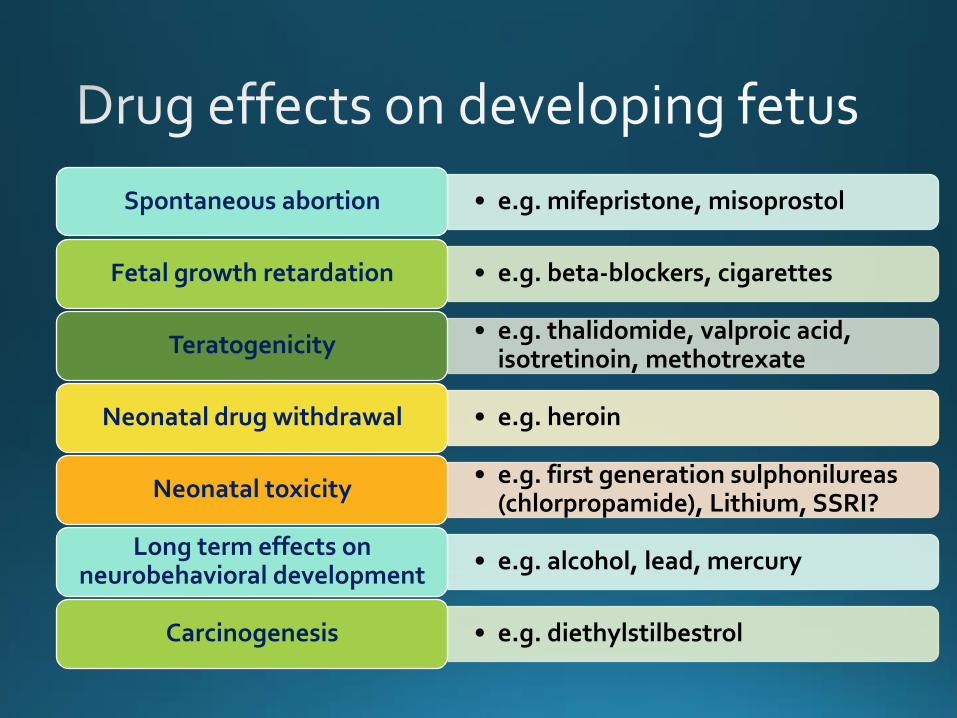
• e.g. mifepristone, misoprostol Spontaneous abortion
• e.g. beta-blockers, cigarettes Fetal growth retardation
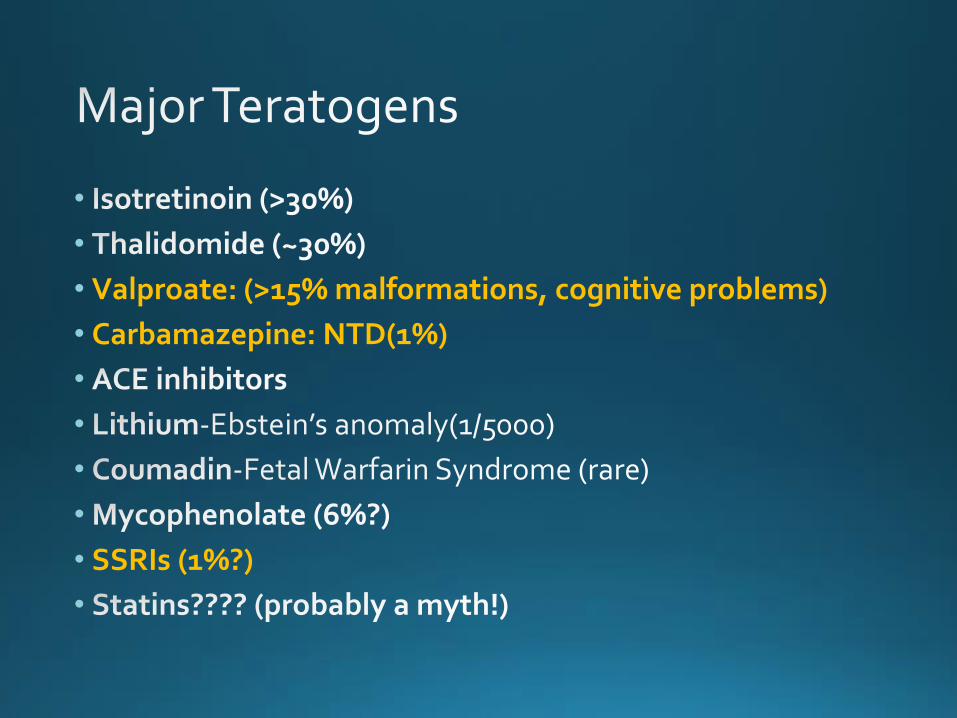
• e.g. thalidomide, valproic acid, isotretinoin, methotrexate
Teratogenicity
• e.g. heroin Neonatal drug withdrawal
• e.g. first generation sulphonilureas (chlorpropamide), Lithium, SSRI?
Neonatal toxicity
• e.g. alcohol, lead, mercury Long term effects on
neurobehavioral development
• e.g. diethylstilbestrol Carcinogenesis
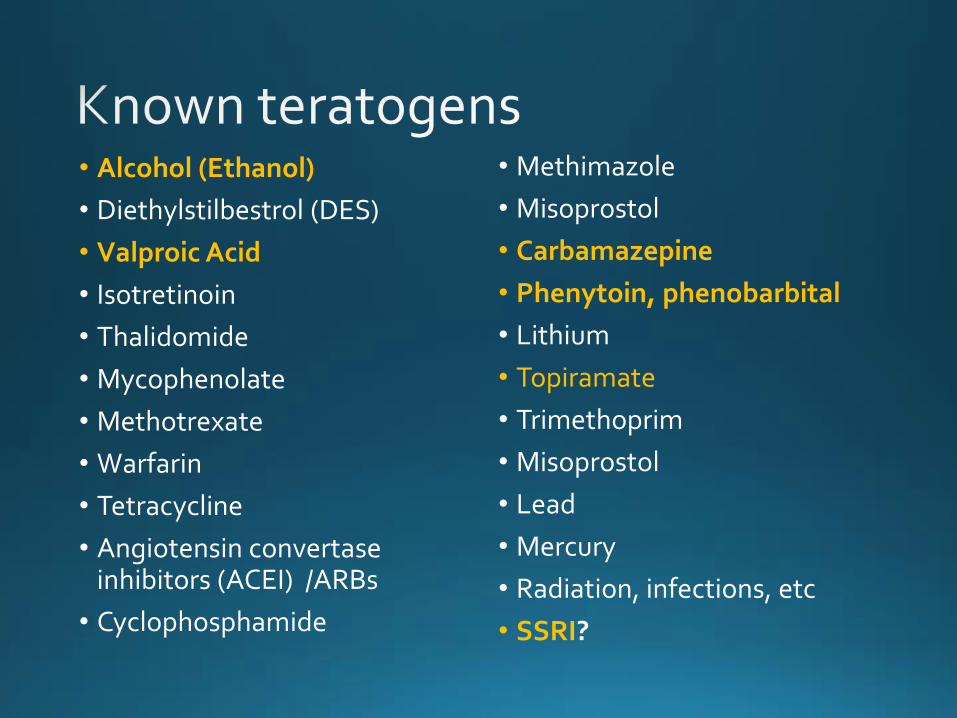
• Alcohol (Ethanol)
• Diethylstilbestrol (DES)
• Valproic Acid
• Isotretinoin
• Thalidomide
• Mycophenolate
• Methotrexate
• Warfarin
• Tetracycline
• Angiotensin convertase inhibitors (ACEI) /ARBs
• Cyclophosphamide
• Methimazole
• Misoprostol
• Carbamazepine
• Phenytoin, phenobarbital
• Lithium
• Topiramate
• Trimethoprim
• Misoprostol
• Lead
• Mercury
• Radiation, infections, etc
• SSRI?
•
•
• Valproate: (>15% malformations, cognitive problems)
• Carbamazepine: NTD(1%)
•
•
•
•
• SSRIs (1%?)
•
Examples of problem drugs
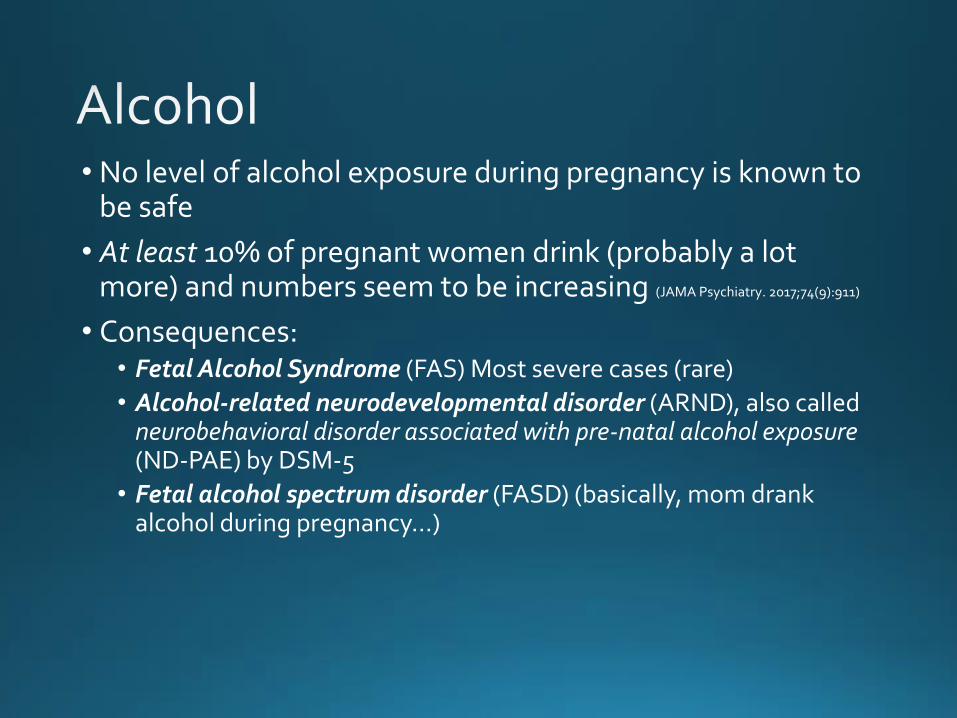
• No level of alcohol exposure during pregnancy is known to be safe
• At least 10% of pregnant women drink (probably a lot more) and numbers seem to be increasing (JAMA Psychiatry. 2017;74(9):911)
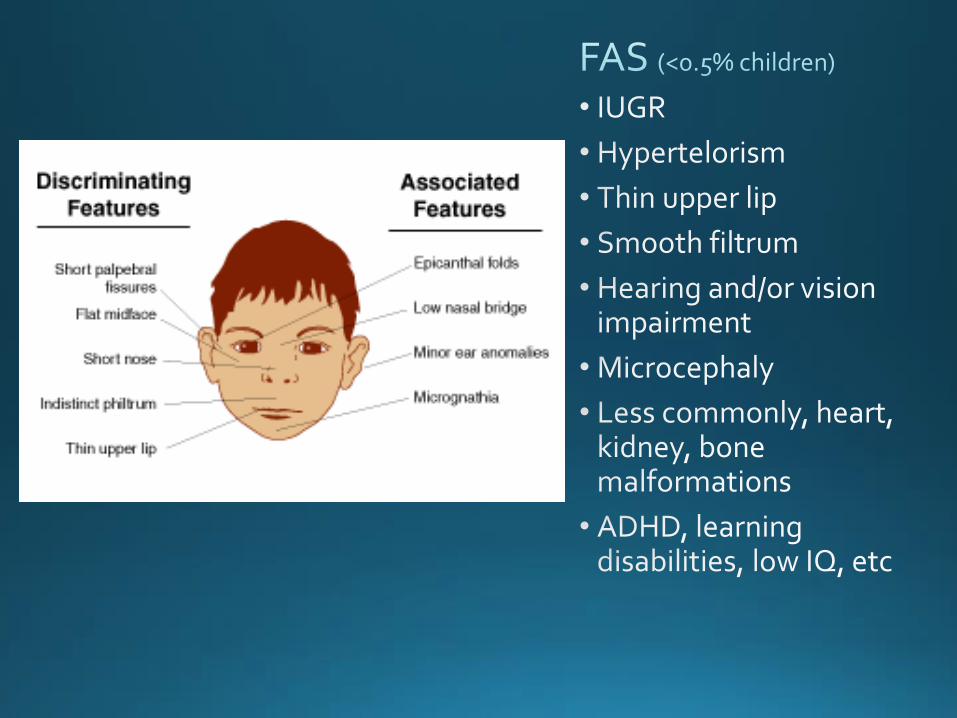
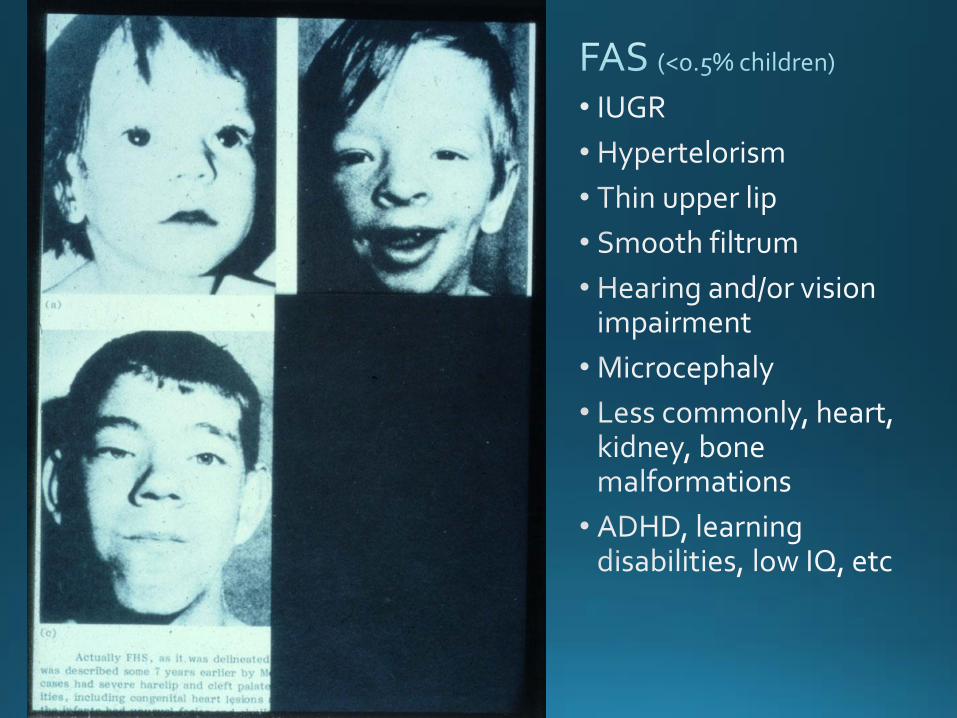
• Consequences: • Fetal Alcohol Syndrome (FAS) Most severe cases (rare)
• Alcohol-related neurodevelopmental disorder (ARND), also called neurobehavioral disorder associated with pre-natal alcohol exposure (ND-PAE) by DSM-5
• Fetal alcohol spectrum disorder (FASD) (basically, mom drank alcohol during pregnancy…)
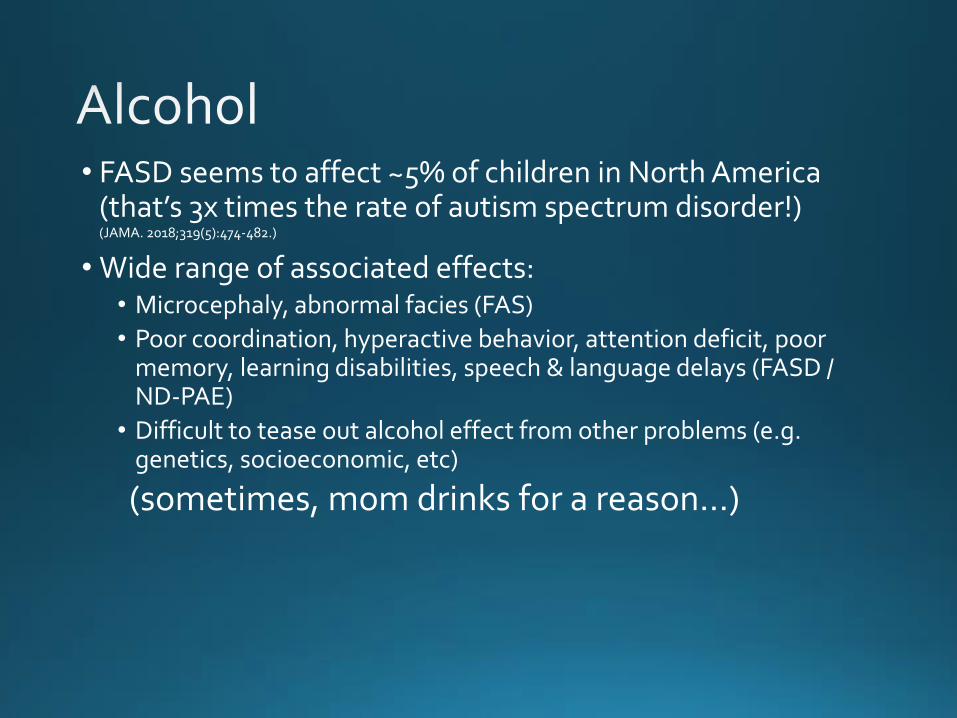
• FASD seems to affect ~5% of children in North America (that’s 3x times the rate of autism spectrum disorder!) (JAMA. 2018;319(5):474-482.)
• Wide range of associated effects: • Microcephaly, abnormal facies (FAS)
• Poor coordination, hyperactive behavior, attention deficit, poor memory, learning disabilities, speech & language delays (FASD / ND-PAE)
• Difficult to tease out alcohol effect from other problems (e.g. genetics, socioeconomic, etc)
(sometimes, mom drinks for a reason…)
• Anticonvulsant, regularly used for other conditions too (e.g. mood stabilizer)
• Fetal valproate syndrome: • Congenital heart defects
• Neural tube defects
• Orofacial clefts
• Genital abnormalities, skeletal abnormalities
• Developmental delay (IQ reduction of 8–10 points)
• Autism spectrum disorder
• Incidence (dose dependent) ~10 - 24%



• Affects up to 20% of pregnant women
• Women who discontinue therapy (very common) have a high rate of relapse of depressive symptoms
• Untreated depression increases significantly the risk for post-partum depression
• In most cases, to maintain the same effect, women need significantly higher doses (due to pharmacokinetics changes in 2nd and 3rd trimester)
• Sudden discontinuation of antidepressants is not recommended and can (will) be a very displeasing event
• SSRI (fluoxetine, paroxetine, citalopram, etc) have been cause of concern for a long time
• Potential problems in pregnancy: • Cardiovascular malformations
• Neonatal pulmonary hypertension
• Neonatal “withdrawal” syndrome
• Bleeding complications in the mother
• But little solid evidence available to support most of the adverse effects proposed
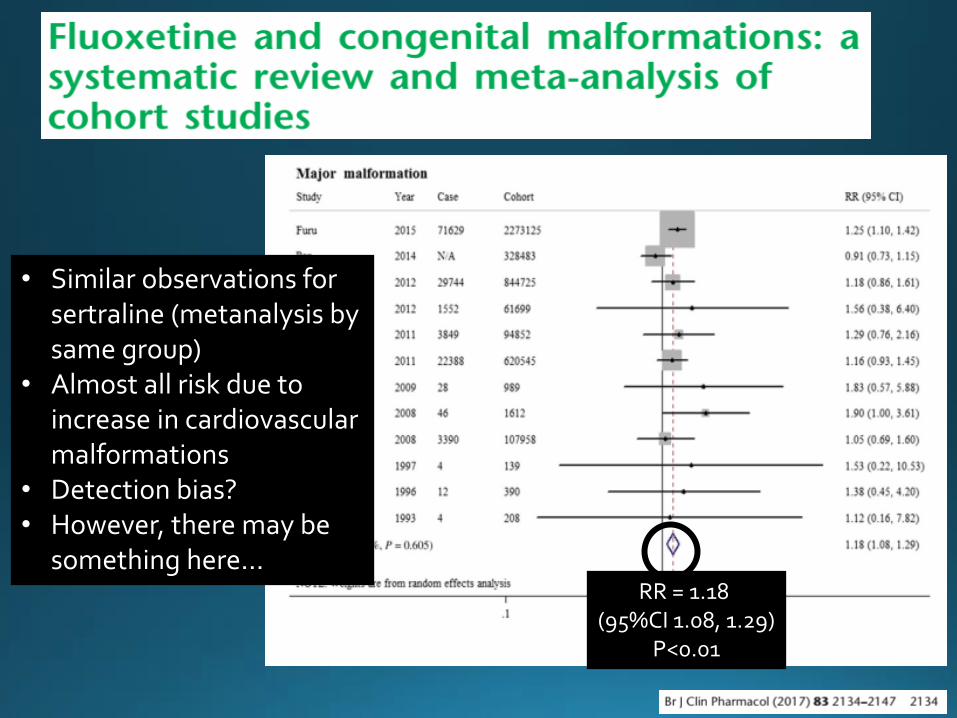
RR = 1.18 (95%CI 1.08, 1.29)
P<0.01
• Similar observations for sertraline (metanalysis by same group)
• Almost all risk due to increase in cardiovascular malformations
• Detection bias? • However, there may be
something here…
• Poor neonatal adaptation syndrome (NAS): • loosely-defined syndrome
• ~ 10-30% neonates of women treated with SSRI / SNRI during pregnancy
• May include a combination of: • Jitteriness, Irritability, Tremors, Shivering, Restlessness
• feeding difficulty
• Temperature instability
• respiratory difficulty
• Sleep problems
• jaundice, rigidity, hypoglycaemia and high pitch crying
• Differential diagnosis is wide including metabolic, infectious, cardiologic and congenital disorders
• The diagnosis of PNAS should only be made after other possible causes ruled out
• Some, or all, of these observations can be part of the normal adaptation of the newborn to extrauterine life (e.g. PNAS was described in neonates of women with depression NOT on antidepressants)
• PNAS disappears within the first days of life, rarely lasts >2 weeks
• Role of endocannabinoid system in pregnancy implantation, placentation and fetal neurologic development
• Components of endocannabinoid system present early in pregnancy
• Studies using animals show that in utero exogenous cannabinoid may disrupt normal brain development and function
• Possible effects of cannabis use on endocannabinoid-mediated neuronal maturation and disruption of developing neurotransmitter systems

cdc.gov
4% of pregnant women used marijuana in the USA in 2014
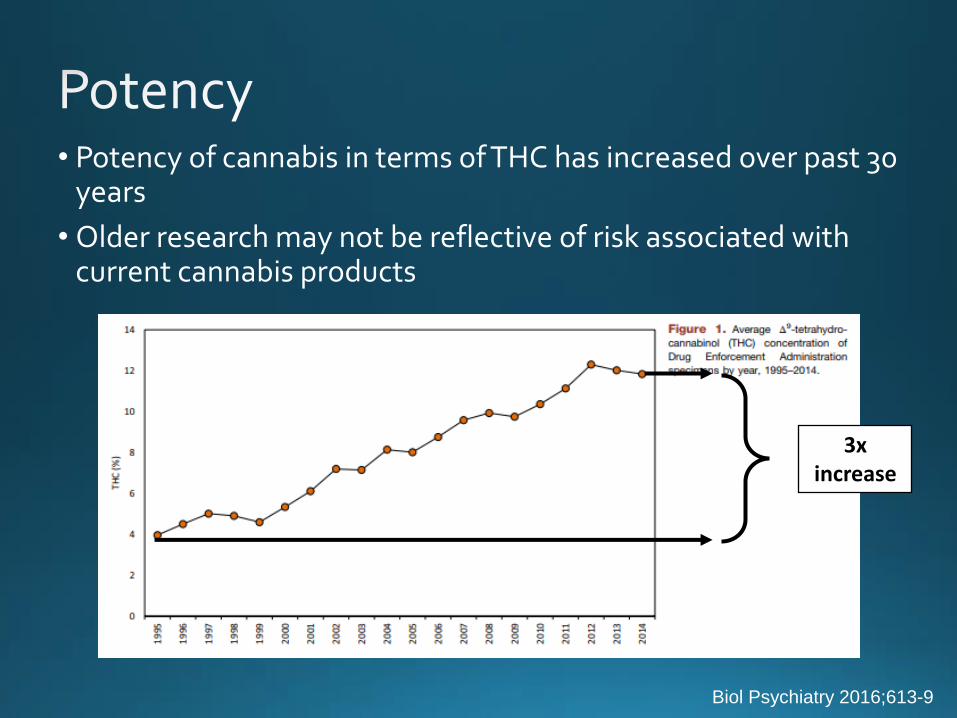
• Potency of cannabis in terms of THC has increased over past 30 years
• Older research may not be reflective of risk associated with current cannabis products
Biol Psychiatry 2016;613-9
3x increase

• Evidence on outcomes mixed and inconsistent
• No characteristic pattern of malformations
• Significantly lower birthweight for infants exposed to cannabis in utero compared with those not exposed (~110g) in some studies (but nothing in others!)
• No association between in utero exposure to cannabis and preterm birth
• Exposed infants more likely to be admitted to NICU (OR 2.02)
• Tobacco use is a major confounder!
BMJ Open 2016;6:e009986 Obstet Gynecol 2016;128:713-23
• Neurobehavioural effects have been shown in some studies during the newborn period
• Possible neurodevelopmental deficits in older children, adolescents and young adults prenatally exposed to marijuana (Am J Obstet Gynecol 2017;216:27-30)
• Possible effects on executive functioning (e.g. attention, inhibitory control, planning), and poorer school achievement
• Possible behavioural problems
• Association to depression and anxiety during adolescence
• However… data is really scarce and contradictory
• “Larger studies found no statistically significant associations between prenatal marijuana exposure and children’s outcomes” (Sharapova et al. Paediatr Perinat Epidemiol. 2018;1–21. -> from the CDC)
(Pharmacol Ther 2018;182:133-51)
Women who are pregnant, or contemplating pregnancy, should be encouraged to
discontinue marijuana use
(and alcohol, and tobacco, and vaping, and eating high-sodium high-fat foods, …)
Maybe
OK
OK
OK
• The range of uses of anti-psychotic medications continues to expand
• The number of available agents also continues to expand
• Older (“typical”) agents commonly interfered with fertility (so little data are available during pregnancy)
• Newer (“Atypical”) drugs do not interfere as much with fertility, which has led to a lot more pregnancy exposures
• Withholding anti-psychotic medication from a pregnant woman with a severe psychiatric condition is certainly risky
• (e.g. bipolar disorder has >70% recurrence rate during pregnancy if medication is discontinued)
• To date, no increase in the risk for major malformations has been identified with typical or atypical antipsychotics (at least with the better studied agents: e.g. trifluoperazine, or olanzapine, risperidone, aripiprazole, quetiapine, etc)
• Use of some of these drugs (e.g. risperidone, quetiapine, olanzapine, clozapine) has been linked to higher risks for gestational diabetes
• Breastfeeding is the best food and stimulant for growth and cognitive development of the baby
• Babies have a right to be breastfed (any decision to deprive a baby of breastmilk should be clearly thought out and explained)
• Deciding not to breastfeed is NOT without risk (e.g. increase in the risk for infections, possibly poorer cognitive outcomes, etc)
• Little data is available for risks for most psychiatric medications during lactation
• In most cases, drug transfer into breastmilk is limited
• A great source of information: Lactmed (https://www.ncbi.nlm.nih.gov/books/NBK501922/?report=classic)
• For some drugs, there is good evidence of safety: • Fluoxetine, Paroxetine
• Olanzapine, Quetiapine
• Lorazepam, Carbamazepine, Levetiracetam
• Few drugs with evidence of risk: • Lamotrigine?, Atenolol, Barbiturates, Ethosuximide, Codeine, THC?

• Most drugs are probably safe in pregnancy, but some can cause malformations
• Even those that do cause malformations, only do so in a fraction of exposed babies
• Be particularly cautious about newer agents - many fetal toxicities have been identified years after release
• Counseling depends on exposure, but also on context: • After the fact (e.g. a baby with a malformation • During the fact (e.g. a pregnant woman taking a medication) • Before the fact (e.g. a woman planning a pregnacy and taking
medications)
• Minimize use as much as possible, but don’t deny effective medications to patients that need them!
• When in doubt… FRAME!
Questions, or patients to refer… Give us a call! 519-685-8500 ext 58293
Fax: 519-685-8156 [email protected]

• Case Reports, Registries: • Suffer from a substantial recall bias (women who have a difficult
pregnancy outcome more likely to recall medication use)
• Clinicians more likely to report bad or unexpected outcomes
• Few clinicians or patients would report a positive outcome (e.g. no malformation), especially if medication use was off-label, or accidental
• Cohorts: • Studies are usually done by retrospectively comparing the infants
of mothers exposed to the medication to those who were not
• Do not examine WHY the medication was given
• Many times don’t take into account variation in other factors (e.g. decrease in incidence of malformations due to folic acid food supplementation, better medical care, early terminations, etc)