Embed Size (px)
DESCRIPTION
Psychosocial Interventions in Psychosis (PSI). James Kelly Senior Clinical Psychologist Lancashire Early Intervention Services. Question. What do you understand by the term Psychosocial Interventions (PSI)? What has your experience been of working in a PSI model?. - PowerPoint PPT Presentation
Citation preview

Psychosocial Interventions in Psychosis
(PSI)
James KellySenior Clinical Psychologist
Lancashire Early Intervention Services

EIS Shared Learning Conference
Question
• What do you understand by the term Psychosocial Interventions (PSI)?
• What has your experience been of working in a PSI model?

A brief look at evidence for PSI approaches
• Cognitive Behaviour Therapy: Recommended– 31 RCT’s reviewed, quality checks on methodology (N=3052)– Small but clear effect on symptoms, including depression, but not on
relapse rates.• Family Interventions (FI): Recommended
– 38 RCT’s met quality checks (5 were follow ups) (N=3134)– 32 studies (N=2429) included in meta analysis– FI reduces relapses consistently, improve social impairment and reduce
Expressed Emotion.• Art Therapy: Considered for Negative Symptoms
– 7 RCT’s of art therapy• Defeat focussed Cognitive Therapy (Grant et al, 2011)
– 1 RCT

Predictors of responsiveness to CBT
• Belief Flexibility: Garety, 1997• Dorsolateral Prefrontal Cortex activity and its connectivity to
the cerebellum (Kumari et al., 2009).• Psychological view of problem and potential to gain control
over them (Freeman et al., 2013).• Neural Changes as a result of CBT: decreased activation of
inferior frontal, insula, thalamus, putamen and occipital areas to fearful and angry expressions.
• Reduction of fMRI response in inferior frontal-insular and occipital clusters during angry expressions correlated directly with symptoms improvement.

Summary of Effectiveness of CBTp• Some evidence that CBTp can improve positive symptoms and
depression.– Some patients more likely to respond than others (Garety et al.,
2008; Dunn et al., 2012).• Negative symptoms improve with behavioural activation and
targeting of defeat beliefs (Grant et al, 2011)• CBTp can be helpful in EIS (Bird et al., 2012)• CBT may be more useful than medication in prodromal period
(Morrison et al., 2012; Stafford et al., 2013)• May be useful in those who refuse meds (Morrison et al.,
2014)• Controversial area, claims disputed (Lynch et al., 2010)

EIS Shared Learning Conference
NICE (2014) Guidelines
• Offer CBT to all people with a diagnosis of schizophrenia. This can be started either during the acute phase or later, including in inpatient settings.
• Offer Family intervention to all families of people with a diagnosis of schizophrenia who live with or are in close contact with the service user.
• Also suggests offering these to people at risk of developing psychosis.

Service users want equal access to psychological therapies Rethink survey (2010)
Research suggests that only 1 in 10 access CBT, and less than 3% of families access structured FI, despite NICE guidance (Schizophrenia Commission, 2012)

THE ABANDONED ILLNESS
A report by the S ch izophren ia C om m ission
N ovem ber 2012
“Research has led to a range of evidence-based psychological treatments. We know much more about ‘what works’ than we used to... The committed individuals who went into the mental health profession to improve lives should be helped to do exactly that.”
Prof Sir Robin Murray
This is where IAPT-SMI comes in

Question…
• What challenges do you think we face in implementing PSI in Early Intervention Services?

EIS Shared Learning Conference
Why doesn’t it happen?
• Competing demands and priorities in tight financial climate.
• Lack of up to date knowledge (at all levels of the NHS)
• Insufficient therapists & supervisors with adequate training/competences.
• Lack of appropriate, available training & supervision.
• Organisational/team philosophy and priorities.
• Workforce without specific training
• Culture hard to sustain

69% of Trusts claim funding challenges for providing access to psychological therapies for people with a diagnosis of schizophrenia
94% have encountered obstacles in making psychological therapies available, including insufficient skilled staff

EIS Shared Learning Conference
Why increase access?• Cognitive-behavioural therapy and Family Interventions for
psychosis (CBTp & FIp) are clinically and cost effective• Improve outcomes, reduce relapse and reduce service use,
especially time in hospital • Cost savings up to 2-4K per course of therapy• Service users and carers like them – high satisfaction ratings• NICE recommend CBTp (16+ weekly/fortnightly sessions)
offered to everybody with psychosis • FIp (10+ sessions over 3-12 months) to everybody with a
caregiver• Current provision unable to meet demand

EIS Shared Learning Conference
Lancashire Care: 3 tier model • Whole Service Ethos of Psychosocial Care :
– Matched care or tiered approached to delivering psychological care across whole workforce
• Education & Training :– PSI Training: All of our staff are trained in CBT-informed
interventions (manualised, effective and accredited)– Behavioural Family Therapy: We have 20+ staff trained and
have our own BFT trainers – CBT & CBFI: Cohort of staff trained to Masters & Diploma level – REaCh: Routine Enquiry about Childhood Adversity
• Research and Contribution to Evidence-Base -– E.g., LEAD Clinic, IMPACT Trial & REACT Trial

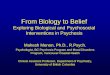
A Matched-Care / Tiered Approach to Psychological Care
Psycho-social
interventions
Case managers/
ST&R
Tier 2
Tier 3
Formal CBT or FI,
Discrete Problems
Staff with:
Formal CBT training or COPE Msc
(under supervision)
Complex / multiple
problems longer term CBT
or FI
Tier 1Specific PSI
Training
Supervision/ Consultation
Cognitive Therapists
Clinical Psychologists

North Lancashire
East Lancashire
Central & West Lancashire
Aligned Therapist Aligned Therapist Aligned Therapist
Case Discussion and Formulation
(Therapist and Case Manager)
Core PSI Tier 1
Formal CBT / FI
(Tiers 2 and 3)
Supervision, consultation & ongoing support from Therapist
and Team Leader
Review Outcome and Effectiveness
Psychological Assessment including Case Manager
Review Outcome

3 days of PSI training for all EIS workers & a manual/ written resource
• To support EIS staff in the delivery of a CBT-informed approach.
• To evaluate impact on knowledge, confidence and application of PSI in routine clinical practice.
• To build on existing knowledge & skills. • To include on-going supervision and support.• Should be easily integrated into practice and
supports EI service model.

Core Competecies for Psychosis


PSI Manual
• Engagement (MI skills)• Normalising Approaches• Maintenance Formulation• Problem lists and Prioritisation• SMART Goals & Agenda Setting• Activity Scheduling• Relapse Prevention (+ Manual)• Recovery Approach• Measuring Change

Supporting Practice Change
• Monthly Formulation groups• PSI focus in clinical supervision• Ongoing weekly support from liaison sessions• Solid foundation of CBT informed knowledge
and skills within EIS• Springboard for further CBT training



Low intensity interventions: a pilot• Low intensity interventions: staff are trained to deliver brief,
manualised interventions.• Helped people with psychosis to achieve personal goals whilst
targeting depression related inactivity or anxious avoidance.• 11 out of 12 people achieved their personal goals• Significant improvements in depression, clinical distress,
activity levels, negative symptoms and delusions across 3 time points, no change in hallucinations or anxious avoidance
• High staff and participant satisfaction.• Feasible therapy, needs controlled study, higher n.• Suggests skilling a workforce with CBT skills may be feasible.

Discussion
• Reflections on this approach to delivering CBT and FI informed Case Management.

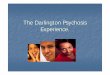
Measuring outcome
• IAPT SMI: PROMS– Sessional
• Choice short form– Start, Middle, End
• Work Social Adjustment Scale (WSAS)• Euroqual 5d (EQ-5D)• Psychosis Symptoms Rating Scale (PSYRATS)• Warwick Edinburgh Mental Wellbeing Scale (WEMWEBS)
– Middle & End• Friends and Family, Patient Experience Questionnaire.

66 - 10 9 30
60 - - - -
66 70 - - -
70 - 12 - -
70 - - - -
- - - - -
60 - 10 - -
- - - - -
Session one
Session Two
Session Three
Session Four
Session Five
Session Six
Session Seven
Session Eight
Choice WEMWBS
WSAS EQ5D
PSYRATS
PROMS
Paired Outcomes
% Improved
% Deteriorated

CHOICE (Greenwood et al.)

Lancashire Care Trust




Final Comments & Questions