Embed Size (px)
Citation preview

Soc Psychiatry Psychiatr Epidemiol (1997) 32:379-386 �9 Springer-Verlag 1997
A.C. Kouzis �9 W . W . Eaton
Psychopathology and the development of disability
Accepted: 5 November 1996
Abstract The objective was to determine the effect of preexisting psychopathology on days missed from work or usual activities ("disability days") in a large community sample (N = 3481). Logistic regression analyses were performed with the presence or absence of disability days (wave 2) as the dependent variable. The effects of sociodemographic variables, six psychi- atric disorders, a high distress score, and chronic physical conditions (wave 1) were studied. Separate analyses were conducted for the total sample and four subgroups (labor force participants, homemakers, men, and women). The adjusted odds ratios and 95% confi- dence intervals (95% CI) for subjects with onset of panic disorder were 7.3 (95% CI = 1.8,28.7); for those with chronic major depressive disorder, 7.2 (95% CI = 0.3,160.6); and for those with chronic high dis- tress, 5.0 (95% CI = 2.6,9.9). The relative odds for developing a disability were greater for those with either type of psychiatric disorder or high distress than for those with any prior physical illness or those with a prior disability day. Disability days experienced by persons with psychopathology result in diminished quality of life, economic losses, and increased need for health services. Improved health services and educa- tional and work adjustments for emotionally disabled persons are recommended.
Introduction
Restricted activity days, or disability days, experienced by persons is an important measure of functioning
A.C. Kouzis ( ~ ) . W.W. Eaton The Johns Hopkins University, School of Hygiene and Public Health, Department of Mental Hygiene, 624 North Broadway, Baltimore, MD 21205, USA
status and well-being (Golden 1986; Patrick et al. 1988; Scholes et al. t991; Stanfield et al. 1995). Persons with depression, schizophrenia, alcohol and other drug abuse or dependence experience functional disabilities that limit their lives and ability to relate to others both socially and occupationally. The association between depressive disorders and disability has been recently recognized as detrimental to work productivity and efficiency (Broadhead et al. 1990; Craig and Van Natha 1983; Mintz et al. 1992; Turner and Noh 1988; Von Korffet al. 1992). Days lost from work, a reduced sense of well-being, and a need for health services are often an outcome of psychopathology. Disabilities are signifi- cant for policy makers who make decisions regarding economic losses and for the provision of services in the society.
The 1978 US Social Security Survey of Disability and Work estimated that 1.1 million adults in house- holds, or about 1% of the adult population, were seriously disabled mentally ill. These figures represent- ed only those in households and those between the ages of 20 and 64 years, they focused only on those receiving payments for work disability and considered only cases of at least 1 years duration (Ashbaugh et al. 1983). The National Health Interview Survey (NHIS) of 1989 found 2.8 million adults 18 years or older living in households, or about 1.6% of the adult population, who were either unable to work or limited in their work because of their severe mental illness (Barker et al. 1989). These were based on reports of household mem- bers' specific diagnoses reported by a single respondent in the household. Other surveys of psychiatric dis- orders have found more than 15% of the population have a mental disorder (Kessler et al. 1994; Robins et al. 1991). Thus, it is expected that many more people experience either a less severe, or a temporary, dis- ability ("disability day") than those recognized as mentally disabled by the Social Security Administra- tion or those included in the Health Interview Surveys (Okpaku et al. 1994).

380
Previous studies estimated associations of various measures of functioning with specific chronic medical conditions; few comparisons were made with patients experiencing distress or psychopathology (Mintz et al. 1992). Studies on physical functioning that included mental illness were restricted to psychological distress or depressed mood (Bruce et al. 1994; Frerichs et al. 1982; Neff et al. 1980; Satin and Morrett 1985; Selzer et al. 1968) and failed to adjust statistically for physical condition. Others have examined the relationship be- tween depression and functional disability among pa- tient samples (Gardiner 1980; Rutter 1977; Shaffer et al. 1972; Wells et al. 1989). Wells et al. (1989) focused on depression, citing its "association with large decre- ments in patient well-being and functioning." Ormel et al. (1993) found depression and anxiety were asso- ciated with mild to moderate disability, and that sever- ity of psychiatric illness and disability show synchrony of change.
There are few studies on psychopathology and dis- ability days. Von Korff et al. (1992), in a 1-year follow- up study of 185 medical patients who were high utiliz- ers of ambulatory health care, found a relation between disability measures that included disability days and depression. Broadhead et al. (1990) investigated the relationship between psychopathology and disability days, but examined only depression and depressive symptoms. Persons with major depression experienced almost five times greater risk of disability days in their community study. A significant association between physical functioning, including bed days in the last 2 weeks and affective and anxiety disorders, was dem- onstrated by Wells et al. (1988) in Los Angeles. How- ever, their analysis was restricted to cross-sectional data and to interviews with non-Hispanic whites and Mexican Americans. In the United Kingdom, Jenkins (1985) found one-third of executive civil servants re- ported minor psychiatric morbidity.
Depression may be related to disability because it is associated with non-psychiatric medical conditions. A positive relationship has been found between phy- sical illness and depression or psychological distress (Aneshensel et al. 1984; Craig and Van Natta 1983; Kathol and Petty 1981; Langer and Michael 1963; Neff et al. 1980). Significant differences in mental health were found to exist between patients with- out chronic physical conditions and those with any of five chronic physical conditions studied by Stewart et al. (1989). This differs from a few previous studies showing no such effect (Cassileth et al. 1984; Mason et al. 1983). A number of studies (Berkman et al. 1986; Craig and Van Natta 1983; Earle et al. 1979; Kasl and Cobb 1969; Rosenbaum and Raz 1977; Turner and Noh 1988) show the physically disabled to be signifi- cantly more depressed, or more psychologically dis- tressed generally, although others disagree (Crown and Crown 1973; Nelson and Gruver 1978; Stern et al. 1976).
Psychiatric disorders have also been linked with disabilities resulting from injuries. Paranoid ideation, clinical depression, and social stress have been sus- pected as possible causes of injuries (Holt 1981; Selzer et al. 1968). An association between affective distur- bances and disabling injuries among 18- to 64-year- olds and phobic symptoms and disabling injuries for 65- to 74-year-olds has been suggested by Aboraya (1991).
In sum, research on disability days to date has focused on general mental health of the physically challenged, on injuries, or on the depressed versus the non-depressed. There is little research tracing the evolution of psychopathology and disability in the general population. Recent longitudinal evidence has utilized patient samples in primary care (OrmeI et al. 1993; Von Korff et al. 1992) or been limited to depression (Aneshensel et al. 1984; Broadhead et al. 1990; Mintz et al. 1992; Von Korff et al. 1992; Wells et al. 1992), from which generalization to other psychopathology or the general population remains difficult.
Our prior analyses at baseline produced significant odds ratios of the effects of sociodemographic char- acteristics and psychopathology on disability days for emotional reasons only, for those employed full time in the labor force (Kouzis and Eaton 1994). Sub- jects with major depressive disorders had the strongest association with disability, with a 27 times greater likelihood of being absent from work for emotional reasons. Those with a panic disorder followed closely, with an odds 20 times that of others of missing work. Comparing the odds of absenteeism for physical health reasons, only respondents with cardiovascular disease or cancer were more likely to experience a dis- ability day.
This paper, in contrast, has focused on 9eneral dis- ability days, because it is felt that psychiatric problems may be an important cause of disability days, not necessarily labeled as emotional by respondents. For example, psychopathology may lead to physical condi- tions through a direct biological action ("psychoso- matic disorder") or through its effects on prevalence or curative health behaviors. Alternatively, respondents may label days not at work as deriving from physical illness, when in fact they are due to psychopathology ("mental health days").
The research reported here considers days missed from work or usual activities ("disability days") associated with a range of specific psychiatric dis- orders and psychosocial distress. Longitudinal data from a community survey permit an examination of the relevance of changes in psychiatric disorders to the development of disability. We assess and adjust for the influence of sociodemographic characteristics on these relationships. Further, the analysis statist- ically controlled for the effects of chronic medical conditions.

38t
Methods
Study sample
The sample was drawn from the Eastern Baltimore Mental Health Survey conducted during 1981 as part of the National Institute of Mental Health (NIMH) Epidemiologic Catchment Area (ECA) Pro- gram (Eaton and Kessler 1985; Eaton et al. 1981; 1984). It has recently been reported (Public Health Newsletter 1992) that East Baltimore has "the highest rates of premature disability and death in the state." The ECA program is a series of epidemiologic surveys conducted by university-based researchers in five metropolitan com- munities in the United States. This paper reports analyses from The Johns Hopkins University site of the ECA program.
The Baltimore site included three contiguous mental health catch- ment areas with an adult population of approximately 175,000. The data include information on 2768 individuals originally identified through a probability sample of adult household residents who were interviewed regarding their health, mental health, and health servi- ces use, and who were located and successfully reinterviewed 1 year later. The response rate in the first wave of the East Baltimore sample was 78%, and there was about 20% attrition between waves (Eaton et al. 1992; Von Korff 1985). Details concerning the charac- teristics of this population have been presented elsewhere (Eaton et al. 1984; Eaton and Kessler 1985).
Measurement
Each participant in the survey underwent a 90-min interview that included the National Institute of Mental Health Diagnostic Inter- view Schedule (DIS), which was scored to reflect DSM-III diagnoses (hence the label "DIS/DSM-III disorder") (American Psychiatric Association 1987; Robins et al. 1981). At follow-up symptoms ex- perienced within the previous year were counted only if they met the severity criteria of the DIS and were not explained by physical illness, medications, alcohol, or other drug use.
Incidence, remission, and chronicity were determined for each of the psychiatric disorders. Cases where subjects were negative at baseline and positive at follow-up were deemed "onset" cases, those where subjects were positive at baseline and negative at follow-up we called "remission," and those where the subjects were positive at both baseline and follow up became "chronic" cases. Thus, for each of the six disorders and distress there were four categories: no diagnoses (reference category), incidence, remission, and chronicity.
Several sets of variables included in the Eastern Baltimore site of the NIMH's ECA program were not included in other ECA sites. The Baltimore site included the General Health Questionnaire (GHQ) to measure distress that might not be connected to a specific mental disorder. The GHQ was designed for study of the relation- ship of psychiatric problems to general heaRh care utilization, and has good psychometric properties (Goldberg 1972). The standard threshold of 4 points or more was used to define those in the sample considered to be at "high distress."
In the follow-up interview respondents were asked questions pertaining to disability over the previous 3 months. Specifically, they were asked, "During the last 3 months, were there any times when you were kept from your work, school, or usual activities for at least 1 whole day because of an injury or because you weren't feeling well?" Prior disability status as determined at baseline refers to having 1 or more disability days for emotional problems, physical conditions, or injuries. As in the Health Interview Surveys, 3 months was selected as our recall period, a compromise offering an adequate number of responses and necessary recency. The questions on dis- ability days are used in many health surveys in the US and their reliability and validity is well known and adequate (Brown and Adams 1992; Revicki et al. 1994).
The sociodemographic variables included: age in years, sex, race, education, income level in dollars, insurance, marital status, and employment status. Information regarding employment status was attained by asking respondents what they were doing during most of the previous week (as in the labor force surveys). Insurance refers to private or publicly assisted forms of payment for health care services. Private forms of insurance include health insurance plans paying part or all doctor bills, health maintenance organizations (HMOs), and prepaid group practice plans. Publicly assisted medical assist- ance or other public programs such as welfare or public assistance forms of health care as well as Medicare from Social Security were also considered.
Questions on chronic health conditions were drawn from the Health Interview Survey. Respondents were queried as to whether they were currently experiencing specific physical health conditions. These included asthma, high sugar or diabetes, heart trouble, high blood pressure, arthritis or rheumatism, trouble breathing, a stroke and/or cancer.
Data analysis
Unlike simple random sampling, in which respondents have equal probabilities of selection, the multistage sampling procedures of the East Baltimore Epidemiologic Catchment Area survey lead to un- equal probabilities of selection. Therefore, a weight was assigned to each respondent based on his or her selection probability and weighted data are used in our analyses and reported in the text and tables. Results based on weighted data can thus be generalized to the East Baltimore community. The weighting procedure adopted here- in also adjusts variance estimates for the clustered aspect of the sampling so that tests of significance are conservative (Kessler et aI. 1985; Leaf et al. 1991).
As the number of disability days was highly skew, analyses were performed using logistic regression, with the presence or absence of disability days as the dependent variable (Cleary and Angel 1984; Fleiss et al. 1986). In the first stage of the logistic regression a multi- variate sociodemographic model was created for disability days. Variables were retained if the estimates were significant or if their inclusion substantially changed the magnitude of coefficients for other terms. In the second stage of modeling, psychiatric variables were added to the best fitting sociodemographic model. There was one regression equation for each psychiatric disorder. Dis- ability days associated with six psychiatric disorders and the pres- ence of high distress were each compared to the values for respon- dents without that specific DIS/DSM-III diagnosis (Boyd et al. 1984).
Results
T h e s a m p l e in E a s t B a l t i m o r e is a b o u t 6 3 % female ( T a b l e 1). W h i l e the l a rges t age g r o u p c o m p r i s e s y o u n g a d u l t s u n d e r 30 yea r s of age ( 2 8 % , n = 777), t he differ- ence b e t w e e n th is a n d the s m a l l e s t g r o u p s , t hose be- t w e e n 30 a n d 64 yea r s old, is o n l y 4 % , O n e - t h i r d a re A f r i c a n - A m e r i c a n ( 3 5 % , n = 958) a n d 4 0 % (n = 1124) a re m a r r i e d . O n l y o n e - t h i r d e a r n $20 ,000 or m o r e a year , w i t h 4 5 % (n = 1165) l i v ing in p o v e r t y o r !ow- i n c o m e levels. F u l l - t i m e e m p l o y e d w o r k e r s c o m p r i s e less t h a n o n e - h a l f ( 44%, n = 1205) of the s amp le . E i g h t y - t h r e e p e r c e n t (n = 2288) h a v e p r i v a t e o r p u b l i c h e a l t h i n s u r a n c e . T h i r t y - e i g h t p e r c e n t (n = 1048) ex- p e r i e n c e d at l eas t 1 d i s a b i l i t y d a y a t b a s e l i n e a n d 4 5 % (n = 1259) h a v e o n e o r m o r e c h r o n i c diseases .

382
Table 1 Description of Baltimore Epidemiologic Catchment Area Sample ~
n %
Sex Male 1,027 37 Female L741 63
Age (years) 18-29 777 28 30-44 655 24 45-64 659 24 65 + 713 26
Education Eighth grade or less 737 27 Ninth to eleventh grade 694 25 High school 799 29 Beyond high school 538 19
Race African American 958 65 White and other 1,810 35
Marital status Married 1,644 60 Not married 1,124 40
Health insurance Insurance 2,288 83 No insurance 480 17
Income Under $4,999 444 16 $5,000 12,499 721 29 $12,500-19,999 475 19 $20,000 + 825 34
Employment Full-time 1,205 44 Not full-time 1,557 56
Chronic diseases One or more 1,259 45 None 1,509 54
Disability None 1,712 62 One or more 1,048 38
"The total sample consists of 2768 individuals. Data were required to be complete for age, sex, and race. For other variables the total does not always equal 2768 because of missing data
There is no striking variation in the percentage of respondents with disability days in the population ac- cording to sociodemographic variables (Table 2). Per- sons with disabilities at baseline were most likely (52%) to have a disability day at follow-up. Those with more than a high school education reported the second high- est rate of absences (43%). The aging and persons with no prior disability days had the lowest absences at 31%. The crude odds differed trivially from the ad- justed relative odds. The odds of having a disability day, adjusting for all the personal characteristics and chronic physical conditions, are presented in the far right column. Persons with 1 or more disability day at baseline had the greatest odds of having a disability
day, with odds 2.2 (95% CI = 1.69, 2.90) times greater than those with no prior disability. African-Americans and those with less than a high school education ex- perienced the lowest odds of missing work or other activities.
The percentage of those with at aleast 1 disability day at wave 2 by type of psychopathology, the number of persons with each disorder according to our tem- poral classification, and the adjusted odds of having a disability day for each psychiatric disorder are con- sidered in Table 3. Each of eight main rows contains a separate model controlling for sociodemographic fac- tors, chronic medical condition, and temporal charac- teristics of that particular disorder (onset, remission, and chronicity). The psychiatric disorders include ma- jor depressive disorder, alcohol abuse and dependence, other drug abuse/dependence, panic disorder, obsessive-compulsive disorder, and phobic disorder. Categories of high distress scores, and those with any DIS/DSM-III disorder, were also included. Per- sons with no DIS/DSM-III disorder were the compari- son group for those in any DIS/DSM-III disorder group.
The 19 subjects with chronic DIS/DSM-III panic disorders had the largest percentage reporting a dis- ability day (100%), closely followed by the 14 subjects with chronic major depression, with 90% disability days and those with chronic high distress at 77%. Only 28% of those experiencing incidence of alcohol abuse or dependence reported at least one disability day.
The adjusted association of type of psychopathology on disability days appears in the far right column of Table 9. Subjects experiencing new occurrence or onset of a panic disorder had the greatest adjusted odds of missing work (OR = 7.3, 95%CI = 1.84, 28.69). This was followed by subjects experiencing a chronic major depressive disorder, with an odds ratio of 7.2 (95%CI = 0.33, 160.62), although this did not reach conventional levels of significance. Large confidence intervals caution us regarding the possible stability of these findings. The chronic distress group had relative odds of 5.0 (95%CI = 2.83, 6.30). The lowest odds of having a disability day were for subjects with onset of alcohol abuse or dependence (0.6 OR, 95%CI = 0.24, 1.31), although this was not significant.
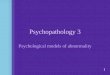
The results of temporal changes in psychopathology for the three strongest categories (panic, depression, and high distress) reflect levels of disability that might be expected, for the most part (Fig. 1). For example, the percentage with disability days rises for those with incident panic and high distress and falls for those with remission of panic and distress. Levels are high and remain high for both chronic panic and high distress, and are lowest for those who do not have panic or high distress on either wave. This pattern for absence of disorder at both waves, and for chronic disorder, is what is displayed for depression; but there appears to be no difference in disability for those having a new

Table 2 Significant predictors of disability days at wave 2 (n = 2619)
Percentage in sample with Crude odds of Adjusted odds of having disability days having disability days disability days
383
Sex Male 34 1.00 1.00 Female 43 1.43 1.39 (1.07, 1.82)
Age (years) 18-29 41 1.14 1.87 (1.15, 3.05) 30-44 42 1.17 1.81 (1.12, 2.93) 45 64 39 1.00 1.55 (1.01, 2.38) 65 + 31 1.00 1.00
Education Eighth grade or less 34 0.79 0.63 (0.41, 0.98) Ninth to eleventh grade 38 0.93 0.69 (0.47, 1.02) High school 38 0.97 0.67 (0.47, 0.96) Beyond high school 46 1.00 1.00
Race African American 32 0.68 0.60 (0.43, 0.85) White and other 41 1.00 1.00
Chronic physical condition One or more 43 1.34 1.59 (1.t7, 2.16) None 36 1.00 1.00
Disability days at wave 1 One or more 52 2.38 2.23 (1.69,2.90) None 31 1.00 1.00
Table 3 Disability days at follow-up and temporal patterns of psychopathology for 2619 subjects (DIS/DSM-III National Institute of Mental Health Diagnostic Interview Schedule scored to reflect DSM-III diagnoses, GHO General Health Questionnaire)
Type of Psychopathology a Percentage with 1 + No. with Adjusted 95% confidence disability days ~ psychopathology odds ratio a interval
DIS/DSM-III Major depressive disorder
DIS/DSM-III Alcohol abuse/dependence
DIS/DSM-III Drug abuse/dependence
DIS/DSM-III Panic disorder
DIS/DSM-III Obsessive-compulsive disorder
DIS/DSM-III Phobic disorder
Any DIS/DSM-III disorder
High GHQ score b
Onset Remission Chronic
Onset Remission Chronic
Onset Remission Chronic
Onset Remission Chronic
Onset Remission Chronic
Onset Remission Chronic
Onset Remission Chronic
Onset Remission Chronic
66 27 2.4 (0.55, 10.50) 63 68 2.4 (0.96, 6.21) 90 14 7.2 (0.33,160.62)
28 57 0.6 (0.24, 1.31) 48 73 1.5 (0.70, 3.05) 48 71 1.5 (0.72, 3.14)
48 29 1.4 (0.48, 4.24) 46 52 1.4 (0.54, 3.85) 50 14 1.4 (0.25, 7.83)
71 32 7.3 (1.84, 28.69) 61 67 0.8 (0.31, 2.03) 100 19 1.0 (0.23, 4.45)
60 39 2.0 (0.68, 6.16) 45 44 1.1 (0.40, 2.88) 64 16 2.1 (0.32, 13.8)
49 112 1.6 (0.81, 3.04) 49 345 1.4 (0.95, 2.16) 48 111 1.3 (0.66, 2.51)
46 218 1.1 (0.66,1.80) 38 446 1.4 (0.98, 2.06) 38 313 2.0 (1.28, 2.96)
59 196 2.6 (1.58, 4.46) 45 274 1.3 (0.83, 2.04) 77 144 5.0 (2.56, 9.90)
a In prior 6 months b In prior several weeks ~ In prior 3 months d Adjusted for sex, age, education, race, chronic physical condition, and disability days at wave t

384
Fig. 1 Mean disability days and temporal patterns of psychopathology. �9 Absence; + onset; �9 remission; �9 chronic
DIS/DSM-III Major Depresive Disorder
MEAN DISABILITY DAYS 12
O.B l
0.6
0 4
0 2 I
L BASELINE 1 YEAR FOLLOW UR
DISIDSM-III Panic Disorder MEAN DISABILITY DAYS
1
0.8
0.6
0,4
0.2
12
1
0.8
06
0.2
O
High GHQ Distress
MEAN DISABILITY DAYS
BASELINE 1 YEAR FOLLOW UF~ BASELINE 1 YEAR FOLLOW DR
onset versus a remission, these being in between the chronic and absent groups. It may be that depressive symptomatology undulates too slowly for onset and remission to have a strong effect within the passage of 1 year's time.
Depression had a stronger effect than chronic phy- sical condition on disability days. For example, the odds ratio for chronic physical condition was 1.59, smaller than the odds ratios in Table 3 (2.4, 2.4, 7.2).
In order to examine robustness of findings, addi- tional models were examined. To test whether the in- clusion of any specific physical condition changed the pattern of results, each individual physical condition was entered into the regression equations. The largest associations were found for subjects suffering from stroke (OR = 2.6, 95%CI = 0.92, 2.81) or diabetes (OR = 2.3, 95%CI = 0.26, 1.57). These did not exceed the odds for psychiatric disorders in the respective models. Also, separate analyses were conducted without chronic physical condition in the regression equation, and the effects of depression on disability remained unchanged. Separate analyses of Tables 2 and 3 were also repeated for four subgroups (those employed full time in the labor force, full time homemakers, women, and men). The overall strength and direction of findings of the relationships were similar to those of the total sample.
Discussion
In both cross-sectional and longitudinal analyses, and for emotional and general disability days, mental dis- orders had the strongest association with missing days from work, school, or one's usual activities. This was
true after statistical adjustment for known sociodemo- graphic variables, prior disability, and physical condi- tion.
We categorized temporal change in psychiatric dis- orders as onset, remission, or chronic. Our findings indicate a pervasive link between chronic disorders and disabilities, except in the case of panic disorders, where onset proved a greater predictor for absence from work or usual activities. Persons experiencing onset of panic attacks for the first time may be prompted by the fear of myocardial infarction to seek medical care and/or avoid strenuous activities, thus experiencing disability. Panic disorder has been found to be the most common DIS diagnosis for which people seek treatment (Boyd 1986). Respondents with a chronic panic disorder may feel less danger and thus be less prone to call a phy- sician. Ours is essentially a 2-wave longitudinal design, by which causality may be inferred rather than perfect- ly established; thus, our analysis shows how disability and psychopathology evolve together over time. None- theless, the longitudinal data allow a more cogent anal- ysis of causal relationship than has been possible in prior research.
Alcohol, drug; and mental (ADM) disorders are ma- jor causes of morbidity, disability, and mortality. Ac- cording to one report, the costs of depression approx- imate those for heart disease (Greenberg et al. 1993; Stoudemire et al. 1986). The economic burden of ADM disorders in the United States, whether measured in direct costs (diagnoses and treatment of patients) or indirect costs (reduced earnings due to lost productiv- ity, premature death, and other related costs) (Bartel and Taubman 1986; Barth 1990; Frank and Gertler 1987; Mullaky and Sindelar 1994; Rice et al. 1990), is staggering: estimates for 1985 were $273.3 bil- lion (Richardson 1994). For depression, the annual

385
e c o n o m i c b u r d e n for 1990 has been e s t i m a t e d at $44 b i l l i on ( G r e e n b e r g et al. 1993). Yet h u m a n suffer ing a n d the d i m i n i s h e d qua l i t y of life a s s o c i a t e d wi th i l lness defy such " h u m a n cap i t a l cos t s " m o d e s of m e a s u r e - ment . P r e v e n t i o n a n d t r e a t m e n t efforts s h o u l d e m b r a c e c lose r sc reen ing a n d su rve i l l ance in p r i m a r y ca re a n d e d u c a t i o n a l a n d w o r k a d j u s t m e n t s for the e m o t i o n a l l y d i sab led as are p l anned for o ther g roups with disabilities.
Acknowledgements This analysis was supported by National Insti- tute of Mental Health (NIMH) grant MH 47447 and MH 14592.
Thomas Grein, MD, MPH, provided technical assistance with the data. We thank the editor and two anonymous reviewers for their criticisms.
The ECA Program is a series of five epidemiologic research studies performed by independent research teams in collaboration with staff of the division of Biometry and Epidemiology (DBE) of the NIMH. During the period of data collection, the ECA program was supported by cooperative agreements. The NIMH Principal Collaborators were Darrel A. Regier, MD, Ben Z. Locke, MSPH, William W. Eaton, PhD (October 1 1978, through October 1 1983), and Jack Burke, MD (October 1 1983, through March 1 1987). The NIMH Project Officers were Carl A. Taube, PhD, and William Huber. The Principal Investigators and Co-investigators from the five sites were: Jerome K. Myers, PhD, Myrna M. Weissman, PhD, and Gary L. Tischler, MD, Yale University, New Haven, CT (U01 MH 33870); Morton Kramer, ScD, Ernesl Gruenberg, MD, DPH and Sam Shapiro, MS, Johns Hopkins University, Baltimore, MD (U01 MH 33870); Lee N. Robins, PhD, and John Helzer, MD, Washington University, St. Louis, M. (U01 MH 33883); Dan Blazer, MD, and Linda George, PhD, Duke University, Durham, N.C. (U01 MH 35386); and Marvin Karno, MD, Richard L. Hough, PhD, Javier I. Escobar, MD, M. Audrey Burnam, PhD, and Diane Timbers, PhD, University of California at Los Angeles (U01 MH 35865).
References
Aboraya AS (t991) Determinants of disabling injuries. Dissertation, Johns Hopkins University School of Hygiene and Public Health, Baitimore
Aneshensel CS, Frerichs RR, Huba GJ (1984) Depression and phys- ical illness: A multiwave, nonrecursive causal model. J Health Soc Behav 25:350
American Psychiatric Association (1987) Diagnostic and Statistical manual of mental disorders (DSM-III), 3rd edn (revised). APA, Washington, D.C.
Ashbaugh J, Leaf PJ, Manderscheid R, Eaton WW (1983) Estimates of the size and selected characteristics of the adult chronically mentally ill population living in US household. Res Community Merit Health J 3:3
Barker PR, Manderscheid RW, Hendershot GE, Jack SS, Schoen- born CA, Goldstrom I (1992) Serious mental illness and disabil- ity in the adult household population: United States, 1989. Ad- vance data fiom vital and health statistics no.218 National Center for Health Statistics, Hyattsville
Bartel A, Taubman P (1986) Some economic and demographic consequences of mental illness. J Labor Econ 4:243
Barth PS (1990) Workers' compensation for mental stress cases. Behav Sci Law 8:349
Berkman LF, Berkman CS, Kasl S, Freeman DF, Leo L, Ostfeld AM, et al. (1986) Depressive symptoms in relation to phys- ical health and functioning in the elderly. Am J Epidemiol 124:372
Boyd JH (1986) Use of mental health services for the treatment of panic disorder. Am J Psychiatry 43:1569
Boyd JH, Burke JD, Gruenberg E, et al (1984) Exclusion criteria of DSM-III: A study of co-occurrence of hierarchy-free syndromes. Arch Gen Psychiatry. 41:983
Broadhead WE, Blazer DG, George LK, Tse CK (1990) Depression, disability days, and days lost from work in a prospective epi- demiologic survey. J Am Med Assoc 264:2524
Brown JB, Adams ME (1992) Patients as reliable reporters of medi- cal care process: Recall of ambulatory encounter events. Med Care 30:400
Bruce ML, Seeman TE, Merril SS, Blazer DG (1994) The impact of depressive symptomatology on physical disability: MacArthur studies of successful aging. Am J Pubic Health 84:1796
Cassileth BR, Lusk EJ, Strouse TB et al (1984) Psychosocial status in chronic illness: A comparative analysis of six diagnostic groups. N Engl J Med 311:506
Cleary PD, Angel R (1984) The analysis of relationship involving dichotomous dependent variables. J Health Soc Behav 25:334
Craig TJ, Van Natta P (1983) Disability and depressive symptoms in two communities. Am J Psychiatry 140:598
Crown S, Crown JM (1973) Personality in early rheumatoid disease. J Psychosom Res 189
Earle JR, Perricone P J, Maultsby DM, Perricone N, Turner RA, Davis J (1979) Psychosocial adjustment of rheumatoid arthritis patients from two alternative treatment settings. J Rheum 6:80
Eaton WW, Kessler LG (1985) Epidemiologic field methods in psychiatry: The NIMH epidemiologic catchment area program. Academic Press, Orlando
Eaton WW, Regier DA, Locke BZ, Taube CA (1981) The Epi- demiologic Catchment Area program in the National Institute of Mental Health. Public Health Rep 96:319
Eaton WW, Holzer CE, Von Korff M, Anthony JA, Helzer JE, George LK, et al (1984) The design of the Epidemiologic Catch- ment Area surveys. Arch Gen Psychiatry 41:942
Eaton WW, Anthony JC, Tepper S, Dryman A (1992) Psychopatho- logy and attrition in the Epidemiologic Catchment Area surveys. Am J Epidemiol 135:1951
Fleiss JL, Williams JB, Dubro AF (1986) The logistic regression analysis of psychiatric data. J Psychiatr Res 20:145
Frank R, Gertler P (1987) The effect of mental distress on income: results from a community survey. Working paper no. 2433. National Bureau of Economic Research, Cambridge, Mass.
Frerichs RR, Aneshensel CS, Yokopenic PA, Clark VA (1982) Physical health and depression: An epidemiologic survey. Prey Med I 1:639
Gardiner BM (1980) Psychological aspects of rheumatoid arthritis. Psychol Med 10:159
Goldberg D (1972) The detection of psychiatric illness by question- naire. Oxford University Press, London
Golden PM (1986) Health, United States, 1986 (prevention profile). DHHS publication PHS 87-1232. US Government Printing Office, Washington, D.C.
Greenberg PE, Stiglin LE, Finkelstein SN, Berndt ER (t993) The economic burden of depression in 1990. J Clin Psychiatry 54:405
Holt PL (1981) Stressful life events preceding road traffic accidents. Injury 13: t l l
Jenkins R (1985) Minor psychiatric morbidity in employed men and women and its contribution to sickness absence. Br J Ind Med 42:147-154
Kasl SV, Cobb S (1969) The intrafamilial transmission of rheuma~ toid arthritis. V. Differences between rheumatoid arthritis and controls on selected personality variables. J Chron Dis 22:239
Kathol RG, Petty F (1981) Relationship of depression of medical illness: A critical review. J Affect Disord 3:111
Kessler LG, Felson R, Royall R, et al (1985) Parameter and variance estimation. In: Eaton WW., Kessler LG (eds) Epidemiologic field methods in psychiatry: the NIMH Epidemiologic Catchment Area program. Academic Press, Orlando
Kessler RC, McGonagle KA, Zhao S, Nelson CB, Hughes M, Eshleman S, Wittchen H-U, Kendler KS (1994) Lifetime and 12-month prevalence of DSM-III-R psychiatric disorders in the United States. Arch Gen Psychiatry 51:8

386
Kouzis AC, Eaton WW (1994) Emotional disability days: prevalence and predictors. Am J Public Health 84:1304
Langer TS, Michael ST (1963) Life stress and mental health, vol 2. Free Press of Glencoe, London
Leaf PJ, Myers JK, McEvoy LT (1991) Procedures used in the Epidemiologic Catchment Area study. In: Robins LN, Regier DA (eds) Psychiatric disorders in America: the Epidemiologic Catch- ment Area studies. Free Press, New York
Mason JH, Weener J, Gertman PM, Meenan RF (1983) Health status in chronic disease: a comparative study of rheumatoid arthritis. J Rheum 10:763
Mintz J, Mintz LI, Arruda M J, Hwang SS (1992) Treatment of depression and the functional capacity to work. Arch Gen Psy- chiatry 49:761
Mullahy J, Sindelar JL (1994) Alcoholism and income: the role of indirect effects. Milbank O 92:359
Neff JA, Husaini BA, McCorkeI J (1980) Psychiatric and medical problems in rural communities. Soc Sci Med 14A:331
Nelson M, Gruver NN (1978) Self-esteem and body-image concept in paraplegics. Rehab Couns Bull 21:108
Okpaku SO, Sibulkin AE, Schenzler C (1994) Disability determina- tion for adults with mental disorders: Social Security Administra- tion vs. Independent Judgments. Am J Public Health 84:1791
Ormel J, Von Korff M, Van Den Bink W, Katon W, Brilman E, Oldehinkel T (1993) Depression, anxiety, and social disability show synchrony of change in primary care patients. Am J Public Health 83:385
Patrick DL, Stein J, Porta M, Porter CQ, Ricketts TC (1988) Poverty, health services, and health status in rural America. Milbank O 66:105
Public Health Newsletter (1992) Baltimore receives $2 million grant for community-based public health program. Public Health Newsletter 6:1
Revicki DA, Irwin D, Reblando J, Simon GE (1994) The accuracy of self-reported disability days. Med Care 32:401
Rice DP, Kelman S, Miller LS, Dunmeyer S (1990) The economic costs of alcohol and drug abuse and mental illness: 1985. Report submitted to the Office of Financing and Coverage Policy of the Alcohol, Drug Abuse, and Mental Health Administration, US Department of Health and Human Services. Institute for Health and Aging, University of California, San Francisco
Richardson M (1994) The impact of the Americans with Disabilities Act on employment opportunity for people with disabilities. Ann Rev Public Health 15:91
Robins LN, Regier DA (eds) (1991) Psychiatric disorders in America: The Epidemiologic Catchment Area Study. Free Press, New York
Robins LN, Helzer JE, Croughan J, Ratcliff KS (1981) The National Institute of Mental Health Diagnostic Interview Schedule: Its history, characteristics, and validity. Arch Gen Psychiatry 38:381
Rosenbaum M, Raz D (1977) Denial locus of control and depression among physically disabled and nondisabled men. J Clin Psychia- try 33:672
Rutter BM (1977) Some psychological concomitants of chronic bronchitis. Psychol Med 129:403
Satin MS, Morrett CH (1985) Census tract predictors of physical, psychological and social functioning for needs assessment. Health Serv Res 20:342
Scholes D, LaCroix AZ, Wagner EH, Grothaus LC, Hecht JA (1991) Tracking progress toward national health objectives in the elder- ly: What do restricted activity days signify? Am J Public Health 81:485
Selzer ML, Rogers JE, Kern S (1968) Fatal accidents: The role of psychopathology, social stress, and acute disturbance. Am J Psy- chiatry 124:1028
Shaffer JW, Nussbaum K, Little JM (1972) MMPI profiles of dis- ability insurance claimants. Am J Psychiatry 129:403
Stanfield S, Feeney A, Head J, Canner R, North F (1995) Sickness absence for psychiatric illness: the Whitehall II Study. Soc Sci Med 40:189-197
Stern M J, Pascale L, McLoone JR (1976) Psychosocial adaptation following an acute myocardial infarction. J Chron Dis 513
Stewart AL, Greenfield S, Hays RD, Rogers WH, Berry SD, et al (1989) Functional status and well-being of patients with chronic conditions: results from the Medical Outcomes Study. J Am Med Assoc 262:907
Stoudemire A, Frank R, Hedemark N, Kamlet M, Blazer D (1986) The economic burden of depression. Gen Hosp Psychiatry 8:387
Turner R J, Noh S (1988) Physical disability and depression: a longi- tudinal analysis. J Health Soc Behav 29:23
Von Korff M, Cottler L, George LK, Eaton WW, Leaf PJ, Burnam A (1985) Nonresponse and nonresponse bias in the ECA surveys. In: Eaton WW, Kessler LG Epidemiologic field methods in psychiatry: the NIMH Epidemiologic Catchment Area program. Academic Press, Orlando, p 85
Von Korff M, Ormel J, Katon W, Lin EHB (1992) Disability and depression among high utilizers of health care: A longitudinal analysis. Arch Gen Psychiatry 49:91
Wells KB, Golding JM, Burnam MA (1988) Psychiatric disorder and limitations in physical functioning in a sample of the Los Angeles general population. Am J Psychiatry 145:712
Wells KB, Stewart A, Hays RD, Burnam A, Rogers W, Daniels M, Berry S, et al (1989) The functioning and well-being of depressed patients: Results from the Medical Outcomes Study. J Am Med Assoc 262:914
Wells KB, Burnam MA, Rogers W, Hays R, Camp P (1992) The course of depression in adult outpatients: Results from the medi- cal outcomes study. Arch Gen Psychiatry 49:788