Embed Size (px)
Citation preview

Psychological Training for Health- Care Professionals in Oncology A Way to Improve Communication Skills
NICOLE DELVAUX“ AND DARIUS RAZAVIb
“Unite de Psycho-Oncologie lnstitut JuIes Bordet 1 rue Hkger Bordet
B-1000 Brussels, Belgium
bService Mkdico-Psychologique Hzpital Universitaire Saint-Pierre
Rue Haute 322 B-1000 Brussels, Belgium
INTRODUCTION
A 47% prevalence of psychiatric disorders has been reported in cancer patients populations.’ Among these, adjustment disorders are the most frequent. They are often related to the risk of therapeutic failure, type and length of therapy, treatment impact on quality of life, coping problems, and availability of social support. It is obvious that cancer patients who do not meet DSM-I11 criteria for psychiatric disorders also experience dis- tress.
Several studies provide evidence that psychosocial interventions reduce patients’ psychological distress.2 Sanson-Fisher and Maguire3 also argue that the way doctors communicate with their patients affects not only the adequacy of the clinical interview and the detection of psycho- logical disturbance, but also patients’ compliance and satisfaction with care. Unfortunately, a substantial proportion of the problems developed by cancer patients remain ~ntreated.~” This failure to identify many of the patients’ problems seems related mostly to insufficient psychosocial knowledge and deficient communication skills among health profession- als who care for these patients and their families.
Nowadays, medicine in general and oncology in particular are con- fronted not only with an exponential growth of scientific knowledge, but also with numerous questions regarding their clinical applications. Medical progress has created many new difficulties in the process of deci- sion making and communicating with patients and their relatives. Some new clinical situations, such as organ transplantation, which implies approaching the donor’s family, or patients’ requests to hasten death,
336

DELVAUX &I RAZAVI: PSYCHOLOGICAL TRAINING FOR PROFESSIONALS 337
need to be resolved with high-quality comm~nication.~,~ Moreover, it is often recognized that cancer care is highly stressful.yJo
Stressors are usually cumulative in oncology: critical decisions, errors yielding important consequences, communication of bad news, numer- ous therapeutic failures, administration of treatments with serious side effects, contacts with mutilated/disfigured patients, emotionally loaded relationships, death of patients. A lot of these stressors imply communi- cation with patients, relatives, and colleagues. They may lead to the development of burnout, which may influence quality of care, occupa- tional life, and/or institutional functioning.
Interventions and strategies have been proposed to help staff deal with cancer care: staff selection, financial and organizational facilities, and also training and research opportunities. Training is probably one of the most cost-effective ways of reducing stress in cancer care and of improving satisfaction with care and enhancing quality of care."
The term "psychological training program" (PTP) will be used here to describe all teaching strategies developed in order to help health care pro- fessionals deal with communication problems in oncology. The impor- tance of PTP is often acknowledged. It is being implemented more and more frequently in general hospitals and other health care settings. However, elaboration of content, form, and techniques vary with the experience and personal options of the trainer.12-15 There have been sev- eral studies regarding their effectiveness. This paper will discuss the potential benefit of PTP and its impact on psychosocial care.
OBJECTIVES
Health professionals are confronted with numerous clinical situations in which communication cannot be avoided: diagnostic disclosure, uncontrolled chronic pain, compliance problems during curative treat- ments, aggressive patients, informed consent, euthanasia request, suicidal risk, and breaking bad news (like poor prognosis or death). The main objective of PTP remains to make health care professionals sensitive to communication problems with patients and relatives. These problems are influenced by personal difficulties in coping with fear of death, fear of the unknown, fear of being unable to respond to patients' questions, and fear of reactivating patients' distress. PTP should help health professionals develop their communication skills and cope with these complex clinical problems.
Basic communications skills can also be useful in other daily profes- sional situations such as obtaining a case history, conveying information about treatment, reassuring patients, achieving patients' satisfaction, and monitoring patients and relatives' adaptation to illness and treatment. In clinical practice, some health care professionals still find it hard to elicit

338 ANNALS NEW YORK ACADEMY OF SCIENCES
psychosocial as well as physical problems, or to do it without taking too much time. They frequently express a need for communication strategies and guidelines.
In medical communication, two types of behaviors are considered important: instrumental and socioemotional behaviors.16 They corre- spond to the main purposes of the medical consultation: on one hand exchanging information-including taking and giving information- which is necessary for solving clinical problems, and on the other hand creating a therapeutic relationship, which is necessary for obtaining the patient’s trust. More specifically, communication with cancer patients and their families has support as a third purpose.
In clinical practice and during training sessions, information and emo- tional support are often used without any previous information taking and assessment of patients’ needs. A major objective of PTP in oncology is thus to develop an understanding of the needs of patients and families. It should enable one to identify patients’ objectives and requests, to detect emotional distress, and to evaluate patients’ understanding of transmit- ted information. Each communication function is achieved by using eval- uative, informative, and supportive strategies. For assessing patients’ problems, evaluative strategies may use open questions, clarification, and checking. Training may help health care professionals improve their abil- ity to clarify the exact nature and extent of the problems encountered by patients, and feel and recognize their emotional reactions. Information has a well-known function in clinical practice but is used most often with- out elaboration of what has been understood. PTP allows participants to experiment with the advantages of progressive information. It also high- lights the need for basic but often neglected strategies such as introducing oneself and ending the interview. Support includes many verbal and nonverbal strategies such as setting up the interview and the relationship, and the use of silence and empathy. It has been experienced in training sessions that all these supportive strategies often facilitate the evaluative function.
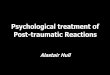
If the potential effect of PTP is the enhancement of communication skills (FIG. l), there are still many questions related to other potential effects such as: the impact of training on health care professionals-their attitudes, quality of care, coping with stress, professional growth; and the impact on patients-their satisfaction with care, detection of their needs, compliance with treatment, quality of life. The effects of training on com- munication skills and attitudes could be linked with a better quality of care (with higher diagnostic and therapeutic competencies) and with more effective coping with occupational stressors met in oncology; how- ever, there is not enough empirical evidence of these relationship^.'^ FIGURE 1 schematizes the expected impact of psychological training on patients and carers through an improvement of communication skills.

DELVAUX & RAZAVI: PSYCHOLOGICAL TRAINING FOR PROFESSIONALS 339
HEALTH PROFESSIONALS
I I PSYCHOLOGICAL TRAINING
ATTITUDE CHANGE - IMPROVEMENT
OF BASIC
COMMUNICATION QUALITY OF CARE -
SKILLS AND -I KNOWLEDGES
STRESS CONTROL
-L PROFESSIONAL GROWTH
PATIENTS AND FAMILIES
- RECOGNITION OF NEEDS
- SATISFACTION WITH CARE
____) QUALITY OF LIFE
- COMPLIANCE
FIGURE 1. Psychological training.
TECHNIQUES
To be effective, PTP in oncology needs to be connected with clinical practice, and training techniques should be active. Available techniques are cognitive, behavioral, experiential, supportive. Cognitive techniques include theoretical information, courses, seminars, and lectures. Cognitive approaches in PTP should give health care professionals an understanding of psychosocial aspects of cancer and help them develop a method of communicating with patients. During training sessions, train- ers often give theoretical input. But there is a risk of reducing active par- ticipation and transmitting too simplistic information about complex facts or concepts. Homework and journal clubs are therefore useful. Reading materials on the most important concepts in the field are now available. International scientific journals are complemented by several books: the Handbook of Psychooncology,‘ the Oxford Textbook of Palliative Medicine,’sand, in French, the Abrkgk de Psycho-oncol~gie.’~
Experiential techniques include case history discussions, staff obser- vations, and supervisions. During a training session, case history obser- vation gives the opportunity to present, discuss, and analyze practical situations in their complexity. It outlines the personal strategies in com- munication and heightens the self-awareness of health care professionals. It clarifies which areas are important to explore in order to determine the nature and extent of the patients’ problems. It also offers opportunities for exchanges with colleagues about psychosocial matters-opportunities

340 ANNALS NEW YORK ACADEMY OF SCIENCES
that are often lacking in clinical practice. To be effective, this technique has to be used in small group sessions in order to stimulate discussion. Helping the participants present the clinical situations seems useful: the methodology for presentation should include information on the purpose of the interview, the history of the patient, the history of the present ill- ness, specific physical and psychosocial problems, attitude towards ill- ness, available support, The clinical presentation should end with a question from the participant in order to induce discussion.
Behavioral techniques include role playing exercises, patients' inter- views under observation, and walking rounds. Role playing exercises have been widely used for teaching communication skills.2n This consists of asking participants during a training session to play different roles (patient, family, nurse, physician, etc.) and to discuss the simulated inter- view. The identification with played roles enables participants to observe and analyze feelings, attitudes, perceptions, and behaviors induced by clinical practice. It helps to experiment with communication strategies, such as setting up the interview, getting the patient to talk, controlling an interview, using assessment questions before informing and counseling. Role playing exercises are perhaps one of the most formative techniques. But trainers have to use them very carefully, with clear instructions, in the secure context of small group sessions. When scripts are proposed, they should be as close as possible to clinical practice and usual situations. The use of audiovisual techniques such as videotaped role playing exercises and video- or audiotaped patient interviews should be encouraged.
Staff support and stress management programs include stressor iden- tification, symptom recognition and monitoring, occupational and per- sonal objective clarification, discussion of communication problems, and sometimes behavioral techniques (relaxation). Staff support programs benefit from a small number of participants (no more than 8 to 12). The good atmosphere of group support is also related to participants' motiva- tion, positive inputs from the authorities, experienced leadership, and regular and convenient meeting times and places.2I
PROGRAMS
General professional training remains essentially targeted to technical care, with limited concern for the psychological problems generated by cancer diagnosis and treatment. Few doctors and nurses involved in can- cer care receive any formal training in basic interviewing, assessment, and counseling skills. Even if they had received some such training, it is usu- ally limited to nondirective methods such as listening and reflecting. While such methods are of value in some situations, they can be counter- productive with cancer patients.22
In order to help some specialists (such as those involved with breast

DELVAUX & RAZAVI: PSYCHOLOGICAL TRAINING FOR PROFESSIONALS 341
cancer care, stoma care, pain and symptom control, care of children with cancer, etc.), the training programs should also focus on the psychological dimensions of supportive care and rehabilitation. Various training pro- grams are now being proposed. The need for specific training in pallia- tive care is now also a c k n o ~ l e d g e d ? ~ ~ ~ Efforts have been made to train future professionals during their undergraduate p e r i ~ d . ' ~ , ~ ~ ~ This is often not enough, because basic education is focused mostly on technical care and, because of time limitations, does not allow extensive focus on psy- chosocial
PTPs are being developed for several groups of professionals involved in cancer care (physicians, nurses, mental health professionals) working in institutions (cancer centers, general hospitals, hospices, etc.) or in-home care programs.
PTPs range from one-day courses to longer specific curricula that require mild to intensive involvement of participants. Most of them are residential workshops and take place during the weekend and are less often organized in the working environment. All these PTPs vary in form, content, and duration. They include basic and postbasic trainings.
In Great Britain, for example, three- to five-day residential workshops in small groups are proposed for physicians, nurses, social workers, and chaplains.22 Videotaped interviews and structured role playing exercises are used. Sharing experiences and discussing them give insight into how a patient or a relative may feel, outline the positive aspects of coping with stress, help the participants identify the risk of projective attitudes, and also offer alternative communication strategies. As participants progress through the workshops, they start wondering about how they can apply their new skills within their own work and still survive emotionally.
Another PTP using cognitive, experiential, and behavioral techniques was proposed in Belgium to health care professionals working with ter- minal patients.41 These modules were flexible in their schedule in order to allow attendance by busy doctors and nurses. They lasted 12 hours spread over 4, 6, 8, or 10 sessions. Their aims were to develop a better understanding of death and dying issues related to cancer and to foster more positive attitudes toward care of the dying.
For those who offer workshops or short training programs, a key challenge is to help participants apply in their clinical practice what they have learned. Attempts to organize consolidation modules have been made. Peripatetic teachers may organize regular short workshops for already trained participants working together.19 Remote learning approachesmay be used for individual feedback of audiotaped material; new miniature two-way radios enabling health care professionals to be supervisedduring their live interviews with patients or relatives are also being
Longer PTPs are increasingly being recommended. Several groups are working on this topic in the United States and Europe. Full-time curric-

342 ANNALS NEW YORK ACADEMY OF SCIENCES
ula are now a ~ a i l a b l e . ~ ~ , ~ ~ The European School of Oncology organizes fel- lowships of several weeks in supportive and palliative care. The Memorial Sloan-Kettering Cancer Center in New York and the Jules Bordet Institute in Brussels propose a two-year curriculum in psychoon- cology. These two years are dedicated to training in clinical practice and research. This curriculum may benefit from a third year for consolidating the skills acquired and for training teachers.
EFFECTIVENESS
Up to now, little has be done to evaluate existing training for health care professionals dealing with cancer patient.43 Training effectiveness can be evaluated by attitudinal, behavioral, or cognitive changes. Psychological stress-related symptoms are supposed to be another vari- able because of their potential influence on quality of occupational life and on quality of care.
Several authors have considered changes in attitudes towards cancer or death as a result of participation in training groups. Results reported are usually positive, but evaluation is often i n f o ~ m a l . ' ~ ~ ~ , ~ ~ More formal assessment of training effectiveness does not always support the per- ceived success of the training program.4749
Several other methodological and theoretical problems are still unre- solved-e.g., what are the short- and long-term emotional, cognitive, and behavioral changes induced by training? Are attitude changes linked with behavior changes? What are the optimal content and duration for effective PTP?
In a controlled study, the effectiveness of a 12-hour PTP was assessed with a semantic differential attitude questionnaire. The assessment was made just after the end of the training and one year 1ater.41,43*50 The results showed that post-training changes were particularly significant for sub- jects reporting negative attitudes before training. However, one year after training, post-training changes were no longer noticed.
In order to improve effectiveness, longer modules were tested. In one of these studies, 72 oncology nurses were randomly assigned to a 24-hour PTP or to a waiting list.51 Attitudes assessed by a semantic differential q~estionnaire,4~ occupational stress assessed by the Nursing Stress and communication skills assessed by standardized videotaped role play- ing exercises were used to compare trained and control subjects. The results show a significant training effect on attitudes, especially on those related to self-concept, and on the level of occupational stress related to inadequate preparation. Limited changes were found regarding post- training communication skills. Trained subjects were significantly more in control of the interview compared to control subjects. The results show that a 24-hour PTP is effective. Results show that post-training changes in

DELVAUX & RAZAVI: PSYCHOLOGICAL TRAINING FOR PROFESSIONALS 343
attitude score + monodisciplinary group (35h) n=18
I 1 I 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 I I I I I I I I I I I I I 1 I I 1 1 t4weeks t l t2 t3
t l : before training t2 : after training t3 : before first consolidation training week t4 : after third consolidation training week
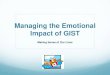
FIGURE 2. Training effectiveness and consolidation of attitudes.

attitude score
ANNALS NEW YORK ACADEMY OF SCIENCES
. \ pco.01
I pco.01 ns/
-o- multidisciplinary group (24h) n=55
--C- monodisciplinary group (24h) n=32
-*- control group n=42
I I I I I , I I
t l t2 t3 t4 months
tl : before training t2 : after training t3 : two months after training t4 : twelve months after training
FIGURE 3. Training effectiveness on attitudes: comparison of multidisciplinary versus monodisciplinary groups.

DELVAUX & RAZAVI: PSYCHOLOGICAL TRAINING FOR PROFESSIONALS 345
attitudes were no longer noticed two months after training. The same trend was observed for post-training Nursing Stress Scale scores.51
The lack of consolidation observed two months after training may be explained by the loss of the ”peer support group effect.” It can also be hypothesized that the trained participants do not find support and/or time in their institutions to give them the opportunity to practice their skills.
Therefore, the question of whether or not PTP should be longer and /or consolidated by several follow-up sessions should be investi- gated. Different questions related to the optimal number of sessions and the duration and content of the training remain unanswered. In an unpublished pilot study, consolidation modules (three monthly full-time weeks of 35 hours) were assessed after an initial 35-hour training week. Consolidation modules enabled more behavioral training techniques to be used (such as case discussions and role playing exercises) and imple- mentation of skills in everyday work to be discussed. The results show a significant consolidation effect of post-training attitude changes. FIGURE 2 illustrates immediate (just after the end of the training) post-training atti- tude changes and shows significant consolidation (8 and 17 weeks after training) of these attitude changes. A statistically significant decrease of a mean attitude score means a ”positive” attitude change.
Other possible predictors such as the benefit of multidisciplinary ver- sus monodisciplinary groups should also be investigated. A pilot study assessing post-training changes of multidisciplinary training groups shows that attitude changes were still noticeable not only just after train- ing, but also two months later. FIGURE 3 illustrates 2 and 12 months post- training attitude changes in a trained group compared with a control group of health care professionals. An increase of mean attitude score two months after the end of the training is found in monodisciplinary training groups. A statistically significant increase of a mean attitude score means a ”negative” attitude change. An advantage of multidisciplinary versus monodisciplinary groups may thus be also hypothesized.
CONCLUSION
To improve the psychological and social care of cancer patients, health care professionals must be trained in basic interviewing, assessment, and counseling skills. PTP should therefore give the ability to detect, clarify, and organize key verbal and nonverbal cues that patients and relatives give about their problems, to control the interview and maintain its focus, to acquire precision in assessment strategies and open directive questions (e.g., dates, names, symptom intensity), and to explore emotionally loaded areas (e.g., the wish to die, prognosis, death) in a helpful and not- too-painful way.

346 ANNALS NEW YORK ACADEMY OF SCIENCES
PTP should be available in all health care settings devoted to cancer care. Consolidation training programs should also be available to stimu- late the implementation of learned skills. A special effort should also be devoted to broader competence and skills in order to respond more ade- quately to complex problems encountered in oncology. Ethical issues, for example, are numerous in oncology. They are often related to psycholog- ical, social, legal, and spiritual matters. Ethics education may focus specifically on problems that are not targeted by PTP. Ethics education should aim at improving clinicians’-mostly physicians’-ability to iden- tify and discuss ethical problems with patients, relatives, and c011eagues.~~ This specific training should prepare health care professionals to analyze and cope with the complexities of difficult clinical situations such as truth-telling, informed consent, active and passive euthanasia, do-not resuscitate orders, deciding curative and palliative treatments, etc.
Developing full-time curricula in psychooncology is another way to improve standards in quality of care. It should also help deal with the sig- nificant lack of experts in this area. Moreover, there are not enough well- trained professionals who can provide PTP at the present time. For this reason, training key persons in teaching methods is a priority. Finally there are also obstacles to implementing PTP, such as the skepticism of health care professionals (especially physicians) about its usefulness. Research on training effectiveness should also be developed. These stud- ies should aim at assessing effectiveness of PTP by measuring the impact of communication skills improvement on quality of care and patients’ quality of life. This will convince not only skeptical health care profes- sionals but also hospital managers to invest time and money in this type of training.
REFERENCES
1. HOLLAND, J. C. & J. H. ROWLAND, Eds. 1989. Handbook of Psychooncology. Oxford University Press. Oxford.
2. HILL, D. R., K. KELLEHER & S. SHUMAKER. 1992. Psychosocial interventions in adult patients with coronary heart disease and ‘cancer. Gen. Hosp. Psychiatry 14 (Suppl.): 28-42.
3. SANSON-FISHER, R. & P. MAGUIRE. 1980. Should skills in communicating with patients be taught in medical schools? Lancet ii: 523-526.
4. MAGUIRE, P. 1984. Communication skills and patient care. In Health Care and Human Behaviour. A. Steptoe & A. Matheews, Eds.: 153-173. Academic Press. London.
5. DAWN CAMP, L. 1988. A comparison of nurses’ recorded assessments of pain with perceptions of pain as described by cancer patients. Cancer Nurs.
6. FORD, S., L. FALLOWFIELD & S. LEWIS. 1994. Can oncologists detect distress in their out-patients and how satisfied are they with their performance during bad news consultations? Br. J. Cancer 70: 767-770.
7. STEIN, A., T. HOPE & J. D. BAUM. 1995. Organ transplantation: Approaching
ll(4): 237-243.

DELVAUX & RAZAVI: PSYCHOLOGICAL TRAINING FOR PROFESSIONALS 347
the donor's family. Br. Med. J. 310: 1149-1150. 8. BLOCK, S. D. & J. A. BILLINGS. 1994. Patient requests to hasten death. Arch.
Intern. Med. 154: 2039-2047. 9. DELVAUX, N., D. RAZAVI & C. FARVACQUES. 1988. Cancer care, a stress for health
professionals. SOC. Sci. Med. 27(2): 159-166. 10. RAMIREZ, A. J., J. GRAHAM, M. A. RICHARDS, A. CULL, W. M. GREGORY, M. S.
LEANING, D. C. SNASHALL & A. R. TIMOTHY. 1995. Burnout and psychiatric disorder among cancer clinicians. Br. J. Cancer. 71: 1263-1269.
11. FALLOWFIELD, L. 1995. Can we improve the professional and personal fulfil- ment of doctors in cancer medicine? Br. J. Cancer. 71: 1132-1133.
12. ANDERSON, J. A. 1979. Practical approach to teaching about communication with terminal cancer patients. J. Med. Educ. 5 4 823-824.
13. BERTMAN, S. L., H. GREENE & C. A. WYATT. 1982. Humanistic health care edu- cation in a hospice/palliative care setting. Death Educ. 5: 391408.
14. SHI", M., M. ROSARIO, H. MORCH & D. E. CHESTNUT. 1984. Coping with job stress and burnout in human services. J. Pers. SOC. Psychol. 4 6 864-876.
15. ZIEGLER, J. L., N. KANAS, W. M. STRULL & N. A. BENNET. 1984. Stress discus- sion group for medical interns. J. Med. Educ. 59: 205-207.
16. HALL, J. A., D. L. ROTER & N. R. KATZ. 1987. Task versus socioemotional behaviors in physicians. Med. Care. 25(5): 399-412.
17. STEWART, M. & D. ROTER. 1990. Communicating with Medical Patients. Sage Publications. Newbury Park, CA.
18. DOYLE, D., G. W. HANKS & N. MCDONALD, Eds. 1993. Oxford Textbook of Palliative Medicine. Oxford University Press. Oxford.
19. RAZAVI, D. & N. DELVAUX, Eds. 1994. Psycho-oncologie, Masson. Paris. 20. MCMANUS, I. C., C.A. VINCENT, S. THOM & J. KIDD. 1993. Teaching communi-
cation skills to clinical students. Br. Med. J. 306: 1322-1327. 21. LEDERBERG, M. 1989. Psychological problems of staff and their management.
In Handbook of Psychooncology. J. C. Holland & J. H. Rowland, Eds: 631-646. Oxford University Press. Oxford.
22. MAGUIRE, P., D. RAZAVI & R. ZIITOUN. 1990. Training in psychosocial oncol- ogy. In Psychosocial Aspects of Oncology. J. C. Holland & R. Zittoun, Eds.: 137-142. Springler-Verlag. New York, NY.
23. SAINSBURY, M. J. & G. W. MILTON. 1975. The nurse in a cancer ward. Med. J.
24. VACHON, M. L., A. L. LYALL & S. J. J. FREEMAN. 1978. Measurement and man- agement of stress in health professionals working with advanced cancer patients. Death Educ. 1: 365-375.
25. DICKINSON, G. E. & A. A. PEARSON. 1980. Death education and physicians' attitudes toward dying patients. Omega 1I: 167-183.
26. DOYLE, D. 1982. An education center for professionals. Death Educ. 6 213-226.
27. JELLINEK, M. S., M. DIE TRILL, S. PASSIK, E I. FAWZY, M. BARD & A. WEISMAN. 1992. The need for multidisciplinary training in counseling the medically ill: Report of the training committee of the Linda Pollin Foundation. Gen. Hosp. Psychiatry 14(Suppl.): 3-10.
28. DIMAGGIO, J. R. 1993. Educating psychiatry residents about death and dying: A national survey. Gen. Hosp. Psychiatry. 1 5 166-170.
29. WEBER, J. 1994. New directions in palliative care education. Support. Care Cancer 2 16-20.
30. BLCCH, S. 1975. Teaching medical students how to care for the dying. Med.
Aust. 2 911-913.

348 ANNALS NEW YORK ACADEMY OF SCIENCES
J. Aust. 2 902-903.
Educ. 10 269-273. 31. BLOCH, S. 1976. Instruction on death and dying for the medical student. Med.
32. BARTON, D., M. K. CROWDER & J. M. FLEXNER. 1979. Teaching about dying and death in a multidisciplinary student group. Omega 10: 265-270.
33. MARKS, S. C. & S. L. BERTMAN. 1980. Experiences with learning about death in the undergraduate anatomy curriculum. J. Med. Educ. 5 5 48-52.
34. BENOLIEL, J. Q., Eds. 1982. Death Education for the Health Professional. McGraw-Hill. New York, NY.
35. GOODELL, B. W., J. I. DONOHUE & J. Q. BENOLIEL. 1982. Death education in medical school A seminar in terminal illness. Death Educ. 5 363-389.
36. ZELINSKY, L. F. & J. A. THORSON. 1983. Educational approaches to preparing social work student for practice related to death and dying. Death Educ. 6:
37. Channon, L. D. 1984. Death and the preclical medical student: I.
38. LIEFF, J. D. 1982. Eight reasons why doctors fear the elderly, chronic illness
39. MCLEAN, U. 1979. Learning about death. J. Med. Ethics. 5: 68-70. 40. POPE, S. 1992. Fundamentals for a new concept of oncology nursing in the
professional nursing education program. Cancer Nurs. 15(2): 137-147. 41. RAZAVI, D., N. DELVAUX, C. FARVACQUES & E. ROBAYE. 1988. Immediate effec-
tiveness of brief psychological training for health professionals dealing with terminally ill cancer patients: A controlled study. SOC. Sci. Med. 27(4):
42. FORBES, F. J. 1994. Towards an optimal teaching programme for supportive care. Support. Care Cancer 2 7-15.
43. DELVAUX, N., D. RAZAVI, C. FARVACQUES & E. ROBAYE. 1988. The effectiveness of a psychological training designed for health care professionals dealing with terminal cancer patients. In A Safer Death. Multidisciplinary Aspects of Terminal Care: 171-184. Plenum Press. New York, NY.
44. SHANFIELD, S. B. 1981. The mourning of health care professionals: An impor- tant element in education about death and loss. Death Educ. 4 385-395.
45. WISE, T. N. 1987. Training oncology fellows in psychological aspects of their speciality. Cancer 39(6): 2584-2587.
46. SCOTT, J. F. & N. MACDONALD. 1993. Education in palliative medecine. In Oxford Textbook in Palliative Medicine. D. Doyle , G. W. Hanks & N. Macdonald, Eds.: 761-780. Oxford University Press. Oxford.
47. SILBERFARB, P. M. & P. M. LEVINE. 1980. Psychosocial aspects of neoplastic dis- ease. 11. Group support for the oncology nurse. Gen. Hosp. Psychiatry. 33:
48. MILES, M. S. 1980. The effects of a course on death and grief on nurses’ atti- tudes toward dying patients and death. Death Educ. 4 245-260.
49. AMARAL, P., A. M. NEHEMKIS & L. FOX. 1981. Staff support on a cancer ward: A pilot project. Death Educ. 5: 267-274.
50. RAZAVI, D., N. DELVAUX, C. FARVACQUES & E. ROBAYE. 1991. Brief psychologi- cal training for health professionals dealing cancer patients: A one-year assessment. Gen. Hosp. Psychiatry 13: 253-260.
51. RAZAVI, D., N. DELVAUX, S. MARCHAL, A. BREDART, C. FARVACQUES & M. PAESMANS. 1993. The effects of a 24-hour psychological training program on attitudes, communication skills and occupational stress in oncology: A ran-
313-322.
Experiences with death. Death Educ. 8: 231-235.
and death. J. Transpers. Psychol. 1 4 47-60.
369-375.
192-1 97.

DELVAUX & RAZAVI: PSYCHOLOGICAL TRAINING FOR PROFESSIONALS 349
domized study. Eur. J. Cancer 29A(13): 1858-1863.
of an instrument. J. Behav. Assess. 3: 11-23.
Wiley & Sons. Chichester, U.K.
52. GRAY-TOFT, P. & J. G . ANDERSON. 1980. The nursing stress scale: Development
53. BYRNE, P., Eds. 1990. Medicine, medical ethics and the value of life. John