Embed Size (px)
Citation preview

Journal of Plastic, Reconstructive & Aesthetic Surgery (2012) 65, 439e447
Psychological morbidity and facial volume in HIVlipodystrophy: Quantification of treatmentoutcome*
Lisa Nelson*, Kenneth J. Stewart
Edinburgh Plastic Surgery Unit, St Johns Hospital, Livingston, Howden Road, West Lothian EH56 6PP, Scotland
Received 18 August 2011; accepted 8 November 2011
KEYWORDSHIV Lipodystrophy;Fillers;3-D imaging;Psychologicaloutcomes
* Presentations: EURAPS Annual MeeMarch 2011.* Corresponding author. Tel.: þ0150E-mail address: drlisanelson@hotm
1748-6815/$-seefrontmatterª2011Bridoi:10.1016/j.bjps.2011.11.024
Summary HIV lipoatrophy is a stigmatizing condition associated with significant psycholog-ical morbidity. The aim of this study was to evaluate change in facial volume and psychologicalmorbidity following treatment with autologous fat, Sculptra� and Bio-alcamid�.Methods: HIV LD patients were treated based on a clinical assessment in a prospective, obser-vational study. 3-D images were obtained pre-operatively then at 2, 6 and 12 months post-operatively using the DI3D system. Volume changes were measured using DI3D software. TheDAS-24 and HADS were used to assess psychological morbidity at similar time intervals.Results: Forty-eight patients with HIV LD were treated: 16 patients had Bio-alcamid�, 20patients received Sculptra� and 12 patients underwent fat transfer. The mean injected volumeof Bio-alcamid� was 25.5 cc which was comparable to the measured volume change at follow-up. The mean injected volume of fat was 20.1 cc, which did not differ from the measuredvolumes at 2 months. There was a mean reduction in measured volume change to11.2 cc at6 months and 10 cc at 12 months.
For Sculptra�, the mean volume change compared to baseline was 8.7 cc at 2 months,increasing to 12.6 cc at 6 months and 12.3 cc at 12 months.
ANOVA tests demonstrated no difference in psychological outcomes between groups. Therewas a significant improvement in DAS-24 scores compared to baseline for all 3 groups. No corre-lation between change in facial volume and psychological measures was demonstrated.Conclusions: Change in 3-D measured facial volume for all 3 groups was seen. Treatment wasassociated with improved body image perception.ª 2011 British Association of Plastic, Reconstructive and Aesthetic Surgeons. Published byElsevier Ltd. All rights reserved.
ting, Manchester, May 2010, Royal Society of Medicine Facial Reconstruction Meeting, Edinburgh,
6 532000/þ447759537478 (mob).ail.com (L. Nelson).
tishAssociationofPlastic,ReconstructiveandAestheticSurgeons.PublishedbyElsevierLtd.All rightsreserved.

440 L. Nelson, K.J. Stewart
HIV lipodystrophy is a syndrome characterized by changes1
inclusion criteria included concurrent anti-retroviral
in body fat distribution associated with the use of anti-retroviral therapy.2e4 Three clinical patterns are recog-nized: lipoatrophy alone, lipohypertrophy alone anda mixed type.The stigmatizing effect of body changes may influencehealth-related quality of life and anxiety and depression.5
Facial lipoatrophy, in particular appears to be associatedwith the most detrimental psychological effects due to theunique importance of facial appearance in terms of‘identity’.6
Plastic surgery is now the mainstay of treatment forestablished lipodystrophy as medical intervention isgenerally ineffective. Soft tissue augmentation withautologous fat transfer (AFT) is reported in the treatmentof HIV lipodystrophy7,8 although studies are limited by smallnumbers, subjective assessment and lack of long-termdata.
Bio-alcamid� is an alkylic resin containing 96% pyrogen-free water and 4% alkylimide-amide groups which becomesenclosed within a thin collagen capsule following injec-tion.9 A number of early studies demonstrated the safety ofBio-alcamid10,11 and excellent cosmetic results withminimal complications in patients with HIV-associatedfacial lipoatrophy.9,12,13
Polylactic acid (PLA) (SculptraTM) is a biocompatible,bioabsorbable synthetic polymer which induces a foreignbody giant cell reaction, followed by a progressive increasein collagen deposition as the bioactive material is degradedand undergoes resorption. This neocollagenesis is thoughtto account for the gradual volume enhancement of PLA.There is a growing body of literature on the use of PLA inthe correction of facial lipoatrophy.14e16 However, clinicalstudies which utilize 3-D imaging to evaluate facial volumechange following treatment with fillers are lacking.
The aim of this study was to evaluate change in 3-Dfacial volume and psychological morbidity following treat-ment for HIV lipodystrophy with AFT, PLA and Bio-alcamid.
Method
Study design
A prospective, multi-centre study was designed to assesschanges in psychological morbidity and facial volumefollowing treatment with AFT, PLA and Bio-alcamid for HIVlipodystrophy.
Ethical considerations
Ethical approval was granted from the Multi-CentreResearch Ethics Committee for Scotland.
Sample
Fifty consecutive patients with HIV facial lipoatrophy wererecruited from plastic surgery clinics in Edinburgh andGlasgow utilizing criteria for body changes attributable tolipodystrophy developed by Carr et al.4 Patient assessmentwas performed by the lead researcher in both sites. Other
therapy and optimal HIV management (undetectable viralload and CD4þ greater than 200) for the safety of thepatient and the operating team. Two patients developedHIV-related medical co-morbidities precluding surgery andtherefore only 48 patients underwent treatment. Informedconsent was obtained for all patients.
Treatment procedures
Choice of treatment was largely determined by clinicalassessment. Patients with sufficient donor site fat weretreated with AFT. Patients with generalized lipoatrophyreceived treatment with either PLA or Bio-alcamid.Although the study was initially designed to randomizepatients to PLA or Bio-alcamid, the majority of patients hada strong preference for choice of filler (due to the differ-ence in properties and injection method), which thereforedetermined treatment type. Bio-alcamid and fat injectionswere administered under general anaesthesia due to theanticipated discomfort of injecting large volumes ofmaterial to widespread areas of the face, and the potentialrisk for needlestick injury if the patient were to flinch.
Autologous fat transfer
A solution containing 1 l saline, 40 mg bupivacaine and 1 mgadrenaline, was infiltrated to the subcutaneous fat of theperiumbilical region.
Fat was harvested and centrifuged using the Colemantechnique. Purified fat was re-injected in multiple planesto lipoatrophic areas using a blunt 2 mm cannula and 1 mlsyringe.
Polylactic acid
One vial of PLA per cheek was reconstituted with 3 mlsterile water and 2 ml 1% lignocaine. Injection was carriedout using a tunneling technique for the cheeks and multiplesmall boluses to the temporal fascia. Massage to dispersethe product was performed after each session and ona daily basis thereafter. Treatments were carried out atintervals of one month. The number of treatment sessionsand volume of suspension injected was adjusted accordingto the severity of lipoatrophy.
Bio-alcamid
Antibiotic prophylaxis with co-amoxiclav was administeredintra-operatively. Pre-filled 3 ml syringes and an 18G needlewere used for injection. A blunt needle was used to createa pocket by fanning in the hypodermis of affected areas.The product was then injected until satisfactory augmen-tation was obtained. Histoacryl glue was used to seal theinjection sites.
Outcome measures
3-D imagingThe cameras, configured as a stereo- The DI3D Facialcamera is a precision 3D system which accuratelycaptures surface texture using high-resolution digital

Psychological morbidity and facial volume in HIV lipodystrophy 441
cameras, pair, recover the 3-D distance to features on thesurface of the face by triangulation. Pre-operative andpost-operative images were aligned using anatomicallandmark localization. Volumetric analysis was per-formed on the aligned model using a three-dimensionalback plane and the DI3D software volume tool. Baselineimages were captured prior to treatment, and thenrepeated at 2, 6 and 12 months post-treatment.
Psychological measuresThe Derriford Appearance Scale (DSA-24) is a validated,condition-specific quality-of-life measure developed forassessing concern about physical appearance. Theresponse category indicating more distress scores thehighest. The minimum score is 11 and the maximum is 96.The Hospital Anxiety and Depression Scale (HADS) isdivided into anxiety (HADS-A) and depression (HADS-D)
Table 1 Demographics of autologous fat, PLA and Bio-alcamid
AFT (nZ 12) PL
GenderN (%) Male 8 (67) 16N (%) Female 4 (33) 4
UnitN Edinburgh 11 11N Glasgow 1 9
Age (years)Mean� SD 43.4� 8.1 45
Risk factorsN (%) MSM 6 (50) 14N (%) IVDA 2 (17) 2N (%) Heterosexual 3 (25) 1N (%) Other 0 1N (%) Unknown 1 (8) 2
HIV infection (years)Mean� SD 11.4� 5.2 10
HAART duration (years)Mean� SD 9� 3.8 7.
CD4 count (cell/mm3)Mean� SD 595� 287 55
HIV RHA <50 copies/mLN (%) 12 (100) 19
BMI (kg/m2)Mean� SD 23.5� 2.2 20
Skin fold thickness(mean of 5 areas, mm)Mean� SD 8.3� 3.3 5.
Clinical gradeMean, patient 2.1 2.Mean, surgeon 1.7 1.
Clinical patternN (%) Lipoatrophy only 1 (8) 13N (%) Lipohyertrophy only 0 0N (%) Mixed morphology 11 (92) 7
subscales, each containing seven items. Scores of 0e7 inrespective subscales are considered normal, with 8e10borderline and 11 or over indicating clinical ‘caseness’.17
All patients completed the DAS-24 and HADS question-naires prior to treatment then at 2, 6 and 12 monthsfollowing treatment.
Patient satisfactionA visual analogue scale graded 1 to 10 (1Z very unsat-isfied, 10Z very satisfied) was devised to assess patientsatisfaction with surgery.
Statistical analysis
Patient demographics, HIV-related factors and clinicalfeatures were summarized by treatment group, and
treatment groups.
A (nZ 20) Bio-alcamid (nZ 16) p Value
(80) 15 (94)(20) 1 (6) 0.177
151 0.012
.5� 11.4 45.3� 4.9 0.78
(70) 12 (75)(10) 1 (6)(5) 2 (13)(5) 0(10) 1 (6) 0.758
.7� 6.4 12.2� 3.9 0.72
1� 4.6 9.2� 3.5 0.28
1� 239 548� 287 0.91
(95) 16 (100) 1.000
.6� 2.9 1.4� 3.2 0.08
3þ 2.3 5.1� 2.7 0.008
1 2.7 0.0166 2.1 0.06
(65) 8 (50) 0.0050
(35) 8 (50)

442 L. Nelson, K.J. Stewart
compared using analysis of variance (ANOVA) for continuousmeasures and Fishers exact test for categorical variables.
To assess the potential for bias due to loss to follow-up,the baseline characteristics of those with or without follow-up measurements were compared with two sample t-tests.
Differences between volume measurements at eachfollow-up visit were summarized by treatment, andwithin-treatment changes were tested using one-sample t-tests. Differences between groups were analyzed usingANOVA.
Association between the number of PLA treatmentsreceived and facial volumes was tested using Pearsoncorrelation coefficient.
For psychological measures, changes over baseline weretested with paired t-tests, within-treatment groups.
Correlations between changes in psychological measuresover baseline and facial volumes at follow-up were testedusing Pearson correlation coefficient.
Results
Baseline characteristics of study group
Table 1 summarizes demographic and clinical characteris-tics of each treatment group at baseline.
Thirty patients completed 12-month follow-up. Amissing-value analysis comparing baseline volume andpsychological measurements between those patients withcomplete data and those patients with incomplete datademonstrated no significant differences between the twogroups.
3-D facial volume measurements
The change in facial volume and psychological measurescompared to baseline for each treatment group is summa-rized in Table 2.
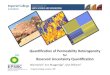
Examples of pre- and post-operative images for eachtreatment method are shown in Figures 1e3.
The greatest mean injected volume was seen with Bio-alcamid (25.5 cc). In six patients who underwent a minorrevision procedure (removal or re-injection of 1 cc or lessper cheek), there was difficulty in accurately measuringsmall volumes of Bio-alcamid removed. Thus, the residual
Table 2 Mean, SD and number of observations of volume injectMean, SD and number of observations of changes over baseline,
Visit Bio-alcamid Fat
Raw data Changeoverbaseline
p-Valuefor change
Raw data Cob
Injected 25.5 (13.4),NZ 18
20.1 (9.3),NZ 10
2 Month 28.3 (13.9),NZ 15
1.1(6.7),NZ 15
pZ 0.083 17.1 (7.8),NZ 7
�N
6 Month 26.7 (15.5),NZ 8
0.7 (3.1),NZ 8
pZ 0.742 11.2 (5.2),NZ 7
�N
12Month 27.7 (13.4),NZ 7
3.4 (2.6),NZ 7
pZ 0.031 10.0 (7.9),NZ 5
�N
injected volume of Bio-alcamid was uncertain and 12-month 3-D images were not completed in these patients.For three patients who underwent revision with largerinjected volumes, the total injected volumes were re-calculated and further follow-up 3-D volume measure-ments were compared with the revised volumes.
In the AFT group, no difference in mean volume changerelative to baseline was demonstrated at 2 months.However, a reduction in mean volume to 11.2 cc at 6months (pZ 0.03) and 10 cc at 12 months following treat-ment was seen (pZ 0.1). This represents 66% of injectedvolume relative to baseline remaining at 6 months and 54%at 12 months.
The mean number of treatment sessions for PLA was 5(range 2e9). The one sample t-test demonstrated a signifi-cant change in measured 3-D volume compared to baselinefor PLA at all follow-up intervals. No correlation betweennumber of PLA treatment sessions and volume change overtime was demonstrated.
Psychological measures
Mean DAS, HADS-A and HADS-D scores are summarized bytreatment group and follow-up interval in Table 3.
Comparison of psychological measures between treat-ment groups using ANOVA demonstrated no significantdifference in DAS-24, HADS-A or HADS-D scores at baselineor throughout follow-up.
Derriford appearance scale
For Bio-alcamid, a significant difference in DAS scorescompared to baseline was found at all time intervals. In thefat group, improvements in DAS scores were also demon-strated at all follow-up visits, although the values did notreach significance as a consequence of small sample size.Significant improvements in DAS scores were found at alltime intervals in the PLA group, although there was anincrease in scores at 12 months.
Hospital anxiety and depression scale
In the Bio-alcamid group, post-treatment scores reachedsignificance for HADS-D at 2 months only. Some
ed or volume relative to baselineby visit and treatment type.with paired t-test p-values for test of zero change.
New fill
hangeveraseline
p-Valuefor change
Raw data Changeoverbaseline
p-Valuefor change
� (�),NZ 0
4.9 (5.9),Z 6
pZ 0.156 8.7 (7.2),NZ 14
e (e),NZ 0
p< 0.001
7.3 (7.1),Z 7
pZ 0.047 12.6 (10.7),NZ 7
� (�),NZ 0
0.016
9.0 (9.5),Z 5
pZ 0.312 12.3 (13.5),NZ 5
� (�),NZ 0
0.019

Figure 1 Pre-treatment and 12 months post-treatment with Bio-alcamid.
Psychological morbidity and facial volume in HIV lipodystrophy 443
improvement in HADS-A and HADS-D scores was found in thefat group, although values only reached significance forHADS-D at 6 months. No significant improvement in HADS-Aor HADS-D scores was demonstrated for the PLA group.
No correlation between change in psychologicalmeasures and change in facial volume compared to baselinewas seen at any time point.
Mean patient satisfaction scores were 8.7/10 for Bio-alcamid, 8.7/10 for PLA and 9/10 for AFT. Two patients withsevere lipoatrophy required nine PLA treatment sessions
Figure 2 Pre-treatment and 12 month
and still considered the final volume augmentationinsufficient.
Discussion
This study was designed to evaluate change in facial volumeand psychological measures in a cohort of patients under-going treatment for HIV facial lipoatrophy. Randomizationof patients to treatment type was prevented by insufficient
s post-treatment with fat transfer.

Figure 3 Pre and post 9 PLA treatments.
444 L. Nelson, K.J. Stewart
autologous donor fat in some patients. The weaknesses ofthe study relating to incomplete follow-up, small samplesize, and lack of randomization limit the extent ofcomparison that can be made between treatment groups.However, some observations based on the results of thisstudy can be made.
3-D volume results
Patients in the Bio-alcamid group had the most severeclinical grade of lipoatrophy and required the greatestinjection volumes to achieve correction. Therefore, oneadvantage of Bio-alcamid in reconstructive surgery is that itcan be injected in large quantities to achieve an immediatecorrection. The product is also considered to be a perma-nent filler due to the stability of its chemical properties andresistance to hydrolysis.18 Indeed, the results of this study,utilizing 3-D imaging as a sensitive measure of facial softtissue volume change, demonstrated no significant differ-ence in measured volume post-operatively compared toinjected volumes. Although the mean 2-month volumemeasurements were slightly higher than mean injectedvolumes, this may represent residual post-operativeoedema, which subsequently decreased by 6 months. Thedistribution of volume change in the treated areas was notanalyzed in this study but would be an extremely usefulinvestigation of product migration in future.
This study provides new, objective data on 3-D facialvolume change following fat transfer. The results showedno difference in mean volume of transferred fat comparedto baseline at 2 months. However, the percentage volumeremaining at follow-up compared to injected volume was66% at 6 months and 56% at 12 months. However, thecomposition of the volume change is unknown and mayrepresent survival of the transferred fat or simply fibrosis.
Some researchers have proposed that survival of adipose-derived stem cells in the stromal cell fraction of trans-planted fat is a major factor and may account for thevariability in survival of fat grafts between individuals.19
Studies of PLA therapy for HIV-associated facial lipoa-trophy have demonstrated increased ultrasound measure-ments of dermal thickness and improved quality of life upto 96 weeks.14 Only one other study provides 3-D volumedata on PLA therapy for HIV lipodystrophy.20 From thevolume data available and clinical impression of patientsand practitioners, PLA appears to be an effective treatmentfor patients with mild to moderate facial lipoatrophy butmay not provide sufficient volume augmentation forpatients with severe lipoatrophy. No correlation betweenvolume change over time and number of treatment sessionswas found in this study. Whether the maximum volumeaugmentation achieved with PLA is related to number oftreatment sessions or individual response to neocolla-genesis is would useful area of further investigation.
Psychological measures
Neither this study nor any published comparativestudies21,22 have been able to demonstrate a psycholog-ical advantage of one type of treatment for faciallipoatrophy.
In the AFT group, 92% of patients had mixed lipodys-trophy. Therefore, patients may have ongoing concernsrelating to body fat distribution. One drawback of the DAS-24 is that the scale is not specific to facial lipoatrophy. Thedata also demonstrates a small increase in DAS scores forPLA at 12 months which was also found by Ong et al. Thismay relate to anticipatory anxiety about the recurrence oflipoatrophy despite evidence of ongoing 3-D volumeaugmentation.

Table 3 Mean, SD and number of observations of DAS, HADS-A and HADS-D, by visit and treatment type. Mean, SD and number of observations of changes over baseline, withpaired t-test p-values for test of zero change.
Outcome Visit Bio-alcamid Fat NewFill
Raw data Change overbaseline
p-Value forchange
Raw data Change overbaseline
p-Valuefor change
Raw data Change overbaseline
p-Valuefor change
DAS Baseline 55.5 (18.4),NZ 16
48.4 (19.3),NZ 12
2 Month 40.9 (13.6),NZ 15
�13.5 (15.2),NZ 15
pZ 0.008 40.8 (20.9),NZ 9
�8.9 (16.3),NZ 9
pZ 0.285 56.2 (19.8),NZ 2037.6 (15.3),NZ 16
�14.4 (14.5),NZ 16
pZ 0.002
6 Month 45.1 (15.6),NZ 12
�12.8 (13.1),NZ 12
pZ 0.012 43.1 (21.2),NZ 10
�10.0 (16.2),NZ 9
pZ 0.138 38.1 (18.4),NZ 8
�15.0 (17.7),NZ 8
pZ 0.050
12 Month 41.3 (17.2),NZ 13
�12.4 (15.6),NZ 13
pZ 0.017 43.3 (22.6),NZ 9
�6.4 (16.5),NZ 9
pZ 0.172 46.1 (25.7),NZ 8
�13.2 (10.8),NZ 8
pZ 0.016
HADS-A Baseline 9.4 (5.3),NZ 16
9.2 (4.8),NZ 12
2 Month 6.5 (4.1),NZ 15
�2.4 (4.4),NZ 15
pZ 0.068 8.7 (4.5),NZ 9
�1.3 (3.2),NZ 9
pZ 0.549 9.8 (5.4),NZ 209.0 (4.7),NZ 16
�0.1 (4.1),NZ 16
pZ 0.938
6 Month 9.2 (4.7),NZ 12
�0.6 (2.2),NZ 12
pZ 0.406 7.6 (6.6),NZ 10
�3.2 (4.4),NZ 9
pZ 0.084 9.0 (5.4),NZ 8
0.1 (3.8),NZ 8
pZ 1.000
12 Month 7.5 (5.0),NZ 13
�1.0 (2.9),NZ 13
pZ 0.360 8.3 (6.1),NZ 9
�0.9 (3.4),NZ 9
pZ 0.438 9.6 (6.5),NZ 8
�0.5 (4.4),NZ 8
pZ 0.778
HADS-D Baseline 7.6 (6.5),NZ 16
5.3 (4.5),NZ 12
2 Month 4.1 (4.7),NZ 15
�2.9 (4.0),NZ 15
pZ 0.003 4.1 (3.7),NZ 9
�1.2 (3.6),NZ 9
pZ 0.405 7.2 (5.0),NZ 20
�1.1 (3.6),N Z 16
pZ 0.144
6 Month 7.0 (5.1),NZ 12
�1.2 (3.5),NZ 12
pZ 0.220 3.9 (4.3),NZ 10
�3.2 (3.0),NZ 9
pZ 0.014 5.7 (4.9),NZ 166.0 (3.0),NZ 8
�1.8 (3.2),NZ 8
pZ 0.159
12 Month 5.5 (4.8),NZ 13
�0.8 (2.5),NZ 13
pZ 0.176 4.4 (3.9),NZ 9
�1.0 (2.9),NZ 9
pZ 0.222 7.1 (5.4),NZ 8
�1.6 (2.7),NZ 8
pZ 0.122
Psych
ologica
lmorbidity
andfacia
lvo
lumein
HIV
lipodystro
phy
445

446 L. Nelson, K.J. Stewart
The results for HADS-A and HADS-D demonstratea similar pattern for each treatment group, with early post-operative improvement in scores, followed by an increasein scores at 12 months. This may relate to complications oftreatment or the return of psychological symptoms.
In this study, no correlation between facial volume withDAS or HADS was found. This lack of correlation is consis-tent with previous studies of patients with HIV lipodys-trophy23 and other facial deformities24 which havedemonstrated a dissociation between physical deformityand psychosocial distress.
Complications relating to the use of Bio-alcamid haveemerged during the study period25,26 and results from thisstudy have been published previously.27
In our unit, Bio-alcamid is no longer offered as a treat-ment option. Treatment with alternative fillers such ashyaluronic acid,28,29 and calcium hydroxlyapatite30 has alsobeen reported. However, for patients with severe lipoa-trophy, the cost of these treatments would be high giventhe large injection volumes and repeated re-injectionsrequired.
No evidence of lipohypertrophy of transferred fat wasseen in this patient group, despite harvesting fat from thedorso-cervical fat pad in one patient. The pattern ofvolume change observed was highly variable betweenpatients and this may reflect the underlying lipodystrophicprocess. Guallar et al. have demonstrated a high expressionof proliferating cell nuclear antigen (PCNA), a marker geneof cell proliferation, in adipocytes harvested from thebuffalo hump region.31 Further investigation of thesebiochemical markers may explain the differences in fatlongevity in patients with HIV lipodystrophy. Compared tothe risks of complications associated with injectable fillers,and other surgical options, the simplicity and safety ofautologous fat transfer makes it an attractive treatmentoption.
Conclusions
In summary, this study has provided objective, measured3-D volume data for patients undergoing treatment for HIVfacial lipoatrophy. Changes in facial volume compared tobaseline were observed in all three treatment groups.Overall, treatment was associated with improved bodyimage quality of life, although no correlation betweenchange in facial volume and psychological measures wasdemonstrated.
Autologous fat transfer continues to remain thepreferred treatment option in those patients with sufficientdonor fat due to the safety of this technique and lowcomplication rate.
Conflict of interest statement
None of the authors have any financial or conflict of interestin the research or products reported in this article.
Funding
This research was funded by the following charities:
1. The Henry Smith Charity, 6th Floor, 65 LeadenhallStreet, London EC3A 2AD, UK.
2. The Sick Kids Foundation, Edinburgh, UK.3. The William Rooney Plastic and Reconstructive Surgery
Fund, Edinburgh, UK.4. NHS Lothian Endowments Fund, Edinburgh, UK.
Ethical board review
This research has received full ethical approval from theMulti-Centre Research Ethics Committee for Scotland.(Study ID number: REC06/MRE00/39)
Clinical trial registration
Trial database: ClinicalTrials.gov.Date: 23/05/11.ClinicalTrials.gov Identifier: NCT01359917.
Acknowledgements
Medical Illustration department, St John’s Hospital.
References
1. Carr A, Samaras K, Chisholm DJ, Cooper DA. Pathogenesis ofHIV-1-protease inhibitor-associated peripheral lipodystrophy,hyperlipidaemia, and insulin resistance. Lancet 1998;351(9119):1881e3.
2. Miller A, Carr A. S E. HIV lipodystrophy: prevalence, severityand correlates of risk in Australia. HIV Med 2003;4(3):293e301.
3. Sattler F. Body habitus changes relating to lipodystrophy. ClinInfect Diseases 2003;36:84e90.
4. Carr A, Law M, Group HLCDS. An objective lipodystrophyseverity grading scale derived from the lipodystrophy casedefinition score. J Acquire Immun Def Syndrom 2003;33(5):571e6.
5. Colins E, Wagner C, Walmsley S. Psychological impact of lip-odystrophy syndrome in HIV infection. AIDS Reader 2000;10:546e51.
6. Tebble N, Thomas D, Price P. Anxiety and self-conciousness inpatients with minor facial lacerations. J Adv Nursing 2004;47(4):417e26.
7. Serra-Renom J, Fontdevila J. Treatment of facial fat atrophyrelated to treatment with proteast inhibitors by autologous fatinjection in patients with Human Immunodeficiency Virusinfection. Plas Recon Surg 2004;114(2):551e5.
8. Coleman S. Treatment of facial fat atrophy related to treat-ment with protease inhibitors by autologous fat injection inpatients with Human Immunodeficiency Virus infection. PlasRecon Surg 2004;114(2):556e8.
9. Protopapa C, Sito G. Caporale. Bio-alcamid in drug-inducedlipodystrophy. J Cosmetic Laser Ther 2003;5:226e30.
10. Formigli L, Zecchi S, Protopapa C. Bio-alcamid: an electronmicroscopic study after skin implantation. Plas Recon Surg2004;113(3):1104e6.
11. Pacini S, Ruggiero M, Cammarota N. Bio-alcamid, a novelprosthetic polymer, does not interfere with morphological andfunctional characteristics of human skin fibroblasts. Plas ReconSurg 2003;111(1):489e91.
12. Lahiri A, Waters R. Experience with Bio-alcamid, a new softtissue endoprosthesis. JPRAS 2007;60:663e7.

Psychological morbidity and facial volume in HIV lipodystrophy 447
13. Ramon Y, Lucian F, Ullman Y. Preliminary experiences with Bio-alcamid in HIV facial lipoatrophy. Dermatology 2007;214:151e4.
14. Valantin M, Aubron-Olivier C, Ghosn J. Polylactic acid implants(Newfill) to correct facial lipoatrophy in HIV-infected patients:results of the open-label study VEGA. AIDS 2003;17:2471e7.
15. Moyle G, Lysakova L, Brown S. A randomized open-label studyof immediate versus delayed polylactic acid injections for thecosmetic management of facial lipoatrophy in persons with HIVinfection. HIV Med 2004;5(2):82e7.
16. Mest DR, Humble G. Safety and efficacy of poly-L-lactic acidinjections in persons with HIV-associated lipoatrophy: the USexperience. Dermatol Surg 2006;32(11):1336e45.
17. Zigmond A, Snaith R. The hospital anxiety and depressionscale. Acta Psych Scand 1983;67:361e70.
18. Ramires P, Miccoli M, Panzarini L. In vitro and in vivo biocom-patibility of a polyalkylimide hydrogel for soft tissue augmen-tation. J Biomed Mater Res 2005;72(2):230e8.
19. Billings Jr E, May Jr JW. Historical review and present status offree fat graft autotransplantation in plastic and reconstructivesurgery. Plastic Reconstruct Surg 1989;83(2):368e81.
20. Ong J, Clarke A, White P, Johnson MA, Withey S, Butler PEM.Objective evidence for the use of polylactic acid implants inHIV-associated facial lipoatrophy using three dimensionalsurface laser scanning and psychological assessment. J PlastReconstruct Aesthetic Surg 2009;62(12):1627e35.
21. Negredo E, Higueras C, Adell X, et al. Reconstructive treatmentfor antiretroviral-associated facial lipoatrophy: a prospectivestudy comparing autologous fat and synthetic substances. AIDSPatient Care Stds 2006;20(12):829e37.
22. Guaraldi G, Orlando G, De Fazio D, et al. Comparison of threedifferent interventions for the correction of HIV-associated
facial lipoatrophy: a prospective study. Antiviral Ther 2005;10(6):753e9.
23. Ong J, Clarke A, White P, Johnson M, Withey S, Butler PEM. Doesseverity predict distress? The relationship between subjectiveand objective measures of appearance and psychologicaladjustment, during treatment for facial lipoatrophy. BodyImage 2007;4(3):239e48.
24. Bryant R, Harvey A. Initial post-traumatic stress responsesfollowing motor-vehicle accidents. J Trauma Stress 1996;9:223e34.
25. Jones D, Carruthers A, Fitzgerald R. Late-appearing abscessesafter injections of nonabsorbable hydrogel polymer for HIV-associated facial lipoatrophy. Dermatol Surg 2007;33:193e8.
26. Karim R, Hage J, van Rozelaar L. Complications of poly-alkylimide 4% injections (Bio-alcamid): a report of 18 cases.J Plast Recontruct Aesthetic Surg 2006;59:1409e14.
27. Nelson L, Stewart KJ. Early and late complications of poly-alkylimide gel (Bio-Alcamid). J Plast Reconstuct Aesthetic Surg2011;64(3):401e4.
28. Gooderham M, Solish N. Use of hyaluronic acid for soft tissueaugmentation of HIV associated facial lipodystrophy. DermatolSurg 2005;31(1):104e8.
29. Ritt M, Hillebrand-Haverkort M, ten Veen J. Local treatment offacial lipodystrophy in patients receiving HIV protease inhibitortherapy. Acta Chirurgiae Plasticae 2001;43(2):54e6.
30. Eviatar J, Silvers S, Echavez M. Restorative treatment of HIV-associated facial lipoatrophy. Plast Reconstruct Surg 2005;116(3):29e30.
31. Guallar JP, Gallego-Escuredo JM, Domingo JC, et al. Differen-tial gene expression indicates that ‘buffalo hump’ is a distinctadipose tissue disturbance in HIV-1-associated lipodystrophy.AIDS 2008;22(5):575e84.