Embed Size (px)
Citation preview
14 RICHARD BLANTON
5. Universities must use their training funds to attract and keep able clinicians who combine the attributes of scientist and artist in a way which most approximates the image which we wish the profession to develop. We should realize that such per- sons will not always have the academic goal of research and publication to the same degree as our pure scientists, but we should expect that a person who typifies our tentative image will create new knowledge and skills and transmit them in appro- priate ways.
6. The field of clinical psychology must have freedom to grow without artificial restraints in the form of overregulation from universities, professional organizations, or coordinate professional groups. In the early stages of our growth, fear of failure may be a more potent force in determining our ways of doing than hope of success. Our response to threats is usually to formalize our knowledge, our practices, our goals. I think that this is premature and that it handicaps us greatly in transmitting to the student the image of the person we wish him to become. For this reason, I look upon licensing laws and board examinations with mixed feelings. To the extent that these prematurely specify the meaning of the term “psychologist”, the emergence of an adequate image will be delayed. The formation of this image for all of our students out of all of the materials of our art and our science is the principal goal of training.
Last, but most important, we must resolve our conflicts about the applica- tion of psychological science and the training of those who are to do it. If action without knowledge is blind, and knowledge without action is empty, it would seem that we should be neither blind artists, nor empty scientists, but responsible and enlightened human beings.
REFERENCES
7.
1. ASTIN, A. The functional autonomy of paychotherapy. Amer. Psychologist, 1961, 75-78.
PSYCHODIAGNOSTIC PREFERENCE BY PROFESSIONAL AFFILIATION AND LENGTH OF EXPERIENCE’
ALVIN R. MAHRER
Denver V A Hospital
PROBLEM This research investigated the extent to which psychodiagnosticians’ pro-
fessional affiliation (i.e. , psychologist or psychiatrist) and length of experience are related to psychodiagnostic preferences. The empirical questions put to this project were the following: (1) To what extent do psychologists and psychiatrists differ in drawing psychodiagnostic inferences from given clinical information? (2) To what extent is length of professional experience a factor in the kinds of psychodiagnostic inferences drawn from given clinical information?
Previous studies have indicated that psychologists and psychiatrists seem to operate similarly in their analyses of case history data @), whereas differences were reported in their definitions of psychological concepts@). Length of experience in a given field seems to be somewhat less than a significant factor in judging protocols of drawings“, 1 6 ) and in prediction of military effectiveness (8 ) . Plag(17) further has
‘The author would like to express his appreciation to Dr. Nelson Jones and Fred H. Herring for their extremely helpful critical readings of the manuscript, and to Dr. Donald Stilson for his statistical consultation.

PSYCHODIAGNOSTIC PREFERENCE BY AFFILIATION AND EXPERIENCE 15
suggested that nonpsychological personnel may prove more effective than trained psychologists in predicting Naval recruits’ future service performance. Arnhoff ( 2 )
found that inter-judge agreement on judging amount and kind of psychopathology decreased with amount of professional experience, although a repetition of Arnhoff’s study(12), using revised instructions, reversed the results. Jones (13) and Hunt and Jones(’O), working in the same general area, found that amount of professional ex- perience per se was not a significant differentiating factor. On the other hand, amount of experience is offered as a significant variable in classical psychophysical judgments (4, 19), in making finer clinical assessments (11), in life predictions from inter- view data(3), and in the description and judged nature of ( 6 ) the ideal thera- peu tic relationship.
As another aspect of this general field, the present study focuses on a comparison of psychologists and psychiatrists at three levels of professional experience, with the task being that of making psychodiagnostic judgments from meager clinical in- formation.
METHOD The subjects included 300 VA psychodiagnosticians selected randomly from a
population of 1271 VA psychologists, psychiatrists, psychologist trainees, and psychiatric residents. These were divided into two groups on the basis of discipline, i.e., staff psychologists and psychologist trainees comprising one group of 150 psycho- logists, and staff psychiatrists and psychiatric residents comprising a second group of 150 psychiatrists.
The subjects were also divided on the basis of length of experience. The ap- proximate modal year in which our subjects either received the doctorate in psy- chology or completed psychiatric residency training was 1952. With this as the point of demarcation, the subjects were divided into three groups of 100 each. The “low experience” group included 50 VA psychiatric residents and 50 psychologist trainees. The “moderate experience” group included 50 VA staff psychologists who received the doctoral degree in 1952 or thereafter, and 50 staff psychiatrists who completed psychiatric residencies in 1952 or thereafter. Finally, the “high exper- ience” group was composed of 50 staff psychologists who had received the doctorate prior to 1952, and 50 staff psychiatrists who had completed psychiatric residency training prior to 1952.
The present study used seven psychodiagnostic cues selected on the basis of a previous study (16) investigating the psychodiagnostic properties of 120 cues which were taken randomly from the psychological, social work, and psychiatric reports of 500 consecutively admitted neuropsychiatric patients at Fitzsimons Army Hospital. The seven cues selected represented (a) three kinds of professional reports (four sentences from psychiatric reports, three from psychological reports, and three from social histories); (b) a variety of psychiatric diagnoses; and (c) offered a variety of diagnostic responses to each sentence; no single sentence led uniformly to a single diagnostic inference (l6).
These seven cues were given to 300 diagnosticians who were instructed to assign a single diagnosis to each cue. A-list of 36 standard psychiatric diagnoses taken in toto from the American Medical Association’s standard nomenclature of mental disorders (14) accompanied the instructions. The seven cues descriptive of seven neuropsychiatric patients were as follows :
1. There are symptoms of crying and depression which may be reactions to perceived failure and lack of acceptance.
2. In November, 1948, the patient re-enlisted in the Army because he was looking for a secure job.
3. He partici ated in no extra-curricular activities but worked extensively on cars and called this his only fobby . . . . He states that he is aware of no strange mood which might come before his seizures.
He says he has recent periods of depression, although he has had frequent periods of de- pression even prior to his service.
4.
16 ALVIN R. MAHRER
5 . During this time the patient revealed he was unable to adjust to the military and do his duties because of constant worries and thinking about the problems of his family and his brother’s family, so the patient stated, “I got fed up and took off AWOL in February, 1943.” . . . He denies any previous suicide attempts.
6. Several times the patient reminded the technician that he loves his wife but there is just so much a man can take.
7. On December 7, 1955, following hospitalization, the patient returned to a semblance of reality a t . . . . . . Hospital . . . . He said they would be whispering to him and would say things to him which disturbed the patient.
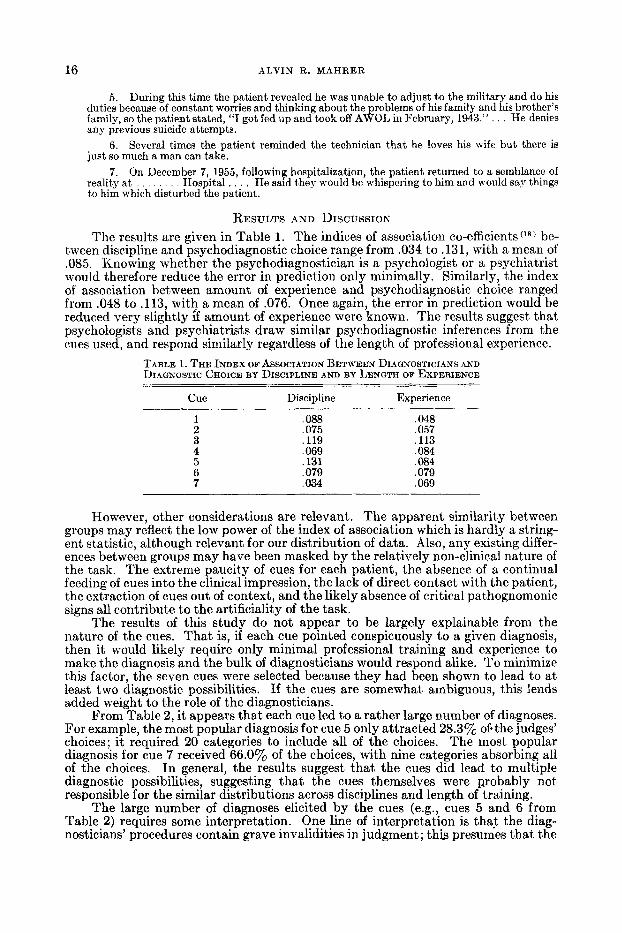
RESULTS AND DISCUSSION The results are given in Table 1. The indices of association co-efficients(’*) be-
tween discipline and psychodiagnostic choice range from .034 to .131, with a mean of .085. Knowing whether the psychodiagnostician is a psychologist or a psychiatrist would therefore reduce the error in prediction only minimally. Similarly, the index of association between amount of experience and psychodiagnostic choice ranged from .048 to .113, wit? a mean of .076. Once again, the error in prediction would be reduced very slightly if amount of experience were known. The results suggest that psychologists and psychiatrists draw similar psychodiagnostic inferences from the cues used, and respond similarly regardless of the length of professional experience.
TABLE 1. THE INDEX OF ASSOCIATION BETWEEN DIAGNOSTICIANS AND DIAGNOSTIC CHOICE BY DISCIPLINE AND BY LENGTH OF EXPERIENCE
- Cue Discipline Experience
,088 ,075 ,119 .069 ,131 .079 ,034
,048 .057 ,113 . O s i ,084 ,079 ,069
However, other considerations are relevant. The apparent similarity between groups may reflect the low power of the index of association which is hardly a string- ent statistic, although relevant for our distribution of data. Also, any existing differ- ences between groups may have been masked by the relatively non-clinical nature of the task. The extreme paucity of cues for each patient, the absence of a continual feeding of cues into the clinical impression, the lack of direct contact with the patient, the extraction of cues out of context, and the likely absence of critical pathognomonic signs all contribute to the artificiality of the task.
The results of this study do not appear to be largely explainable from the nature of the cues. That is, if each cue pointed conspicuously to a given diagnosis, then it would likely require only minimal professional training and experience to make the diagnosis and the bulk of diagnosticians would respond alike. To minimize this factor, the seven cues were selected because they had been shown to lead to at least two diagnostic possibilities. If the cues are somewhat ambiguous, this lends added weight to the role of the diagnosticians.
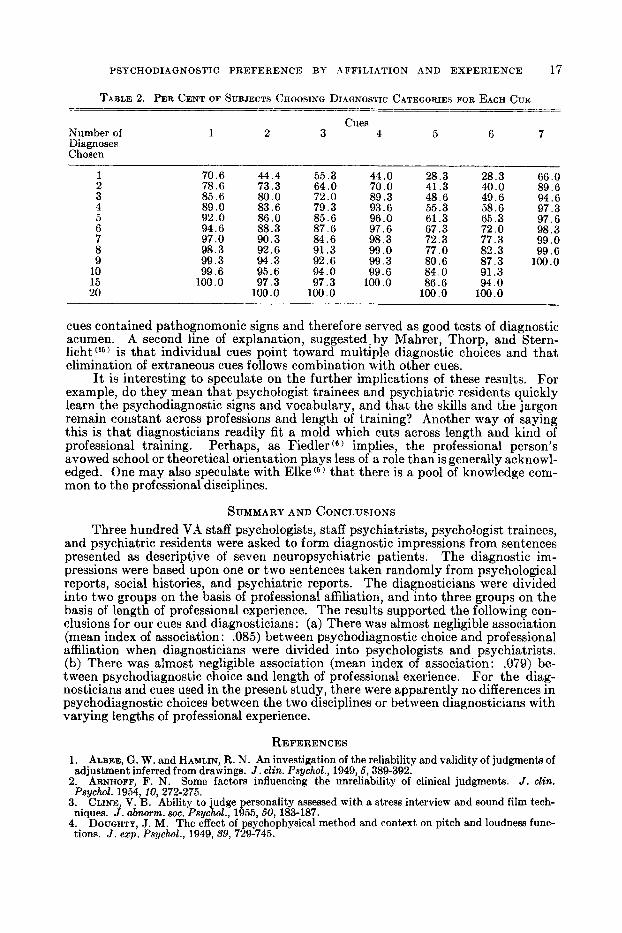
From Table 2, it appears that each cue led to a rather large number of diagnoses. For example, the most popular diagnosis for cue 5 only attracted 28.3% of.the judges’ choices; it required 20 categories to include all of the choices. The most popular diagnosis for cue 7 received 66.0% of the choices, with nine categories absorbing all of the choices. In general, the results suggest that the cues did lead to multiple diagnostic possibilities, suggesting that the cues themselves were probably not responsible for the similar distributions across disciplines and length of training.
The large number of diagnoses elicited by the cues (e.g., cues 5 and 6 from Table 2) requires some interpretation. One line of interpretation is that the diag- nosticians’ procedures contain grave invalidities in judgment; this presumes that the
PSYCHODIAGNOSTIC PREFERENCE BY AFFILIATION AND EXPERIENCE 17
TABLE 2. PER CENT OF SUBJECTS CHOOSING DIAGNOSTIC CATEGORIES FOR EACH CUE -- _ _ ~ -_
Cues Number of 1 2 3 4 5 6 7 Diagnoses Chosen
1 70.6 44.4 55.3 44.0 28.3 28.3 66 . O 2 78.6 73.3 64 .O 70.0 41.3 40.0 89.6 3 85.6 80.0 72.0 89.3 48.6 49.6 94.6 4 89.0 83.6 79.3 93.6 55.3 58.6 97.3 5 92.0 86.0 85.6 96.0 61.3 65.3 97.6 6 94.6 88.3 87.6 97.6 67.3 72.0 98.3 7 97.0 90.3 84.6 98.3 72.3 77.3 99.0 8 98.3 92.6 91.3 99.0 77.0 82.3 99.6
99.3 80.6 87.3 100.0 9 99.3 94.3 92.6 10 99.6 95.6 94.0 99.6 84.0 91.3 15 100.0 97.3 97.3 100.0 86.6 94 .O 20 100.0 100.0 100.0 100.0
cues contained pathognomonic signs and therefore served as good tests of diagnostic acumen. A second line of explanation, suggested. by Mahrer, Thorp, and Stern- licht (16) is that individual cues point toward multiple diagnostic choices and that elimination of extraneous cues follows combination with other cues.
It is interesting to speculate on the further implications of these results. For example, do they mean that psychologist trainees and psychiatric residents quickly learn the psychodiagnostic signs and vocabulary, and that the skills and the jargon remain constant across professions and length of training? Another way of saying this is that diagnosticians readily fit a mold which cuts across length and kind of professional training. Perhaps, as Fiedler ( 6 ) implies, the professional person’s avowed school or theoretical orientation plays less of a role than is generally acknowl- edged. One may also speculate with Elke(5) that there is a pool of knowledge com- mon to the professional disciplines.
SUMMARY AND CONCLUSIONS Three hundred VA staff psychologists, staff psychiatrists, psychologist trainees,
and psychiatric residents were asked to form diagnostic impressions from sentences presented as descriptive of seven neuropsychiatric patients. The diagnostic im- pressions were based upon one or two sentences taken randomly from psychological reports, social histories, and psychiatric reports. The diagnosticians were divided into two groups on the basis of professional affiliation, and into three groups on the basis of length of professional experience. The results supported the following con- clusions for our cues and diagnosticians: (a) There was almost negligible association (mean index of association : .085) between psychodiagnostic choice and professional affiliation when diagnosticians were divided into psychologists and psychiatrists. (b) There was almost negligible association (mean index of association: .079) be- tween psychodiagnostic choice and length of professional exerience. For the diag- nosticians and cues used in the present study, there were apparently no differences in psychodiagnostic choices between the two disciplines or between diagnosticians with varying lengths of professional experience.
REFERENCES 1. ALBEE, G. W. and HAMLIN, R. N. An investigation of the reliability and validity of judgments of
2. ARNHOFF, F. N. Some factors influencing the unreliability of clinical judgments. J . d in .
3. CLINE, V. B. Ability to judge personality assessed with a stress interview and sound fiIm tech-
4. DOUGHTY, J. M. The effect of psychophysical method and context on pitch and loudness func-
adjustment inferred from drawings. J . d in . PsychZ., 1949,6, 389-392.
P s @ ~ 1954,10,272-275.
niques. J . abnorm. SOC. Psychol., 1955,60, 183-187.
tions. J . exp. Psychnl., 1949, 39, 729-745.
18 ALVIN R. MAHRER
5.
6.
7.
8.
9.
10.
11.
12.
13.
ELKE, F. Specialists interpret the case of Harold Holzer. J . abnorm. SOC. Psychol., 1947, 42, 99-1 1 I .
FIEDLER, F. A comparison of therapeutic relationships in psychoanalytic, nondirective, and Adlerian therapy. J . consult. Psychol., 1950, 14, 436-445.
FIEDLER, F. Qualitative studies on the role of therapists’ feeling toward their patients. In 0. H. Mowrer (Ed.), Psychotherapy theory and research. New York: Ronald Press, 1953. Pp. 296-315.
GLASS, A. J., RYAN, F. J., LUBIN, A., RAMANA, C. V. and TUCKER, A. C. Psychiatric prediction and military effectiveness. Part I. U . S. arm. formed. J., 1956,12, 1427-1443.
GRAYSON, H. M. and TOLMAN, RUTH. A semantic study of concepts of clinical psychologists and psychiatrists. J . abnorm. sac. Psychol., 1950, 45, 216-231.
HUNT, W. A. and .JONES, N. F. The reliability of clinical judgments of asocial tendency. J . clin. Psychol., 1958, 14, 232-235.
HUNT, W. A. and JONES, N. F. Clinical judgment of some aspects of schizophrenic thinking. J . elin. Psychol., 1958, 1 4 , 235-239.
HUNT, W. A., JONES, N. F. and HUNT, EDNA. Reliability of clinical judgment as a function of clinical experience. J . clin. Psychol., 1957, IS, 377-378.
JONES, N. E. Context effects in judgment as a function of experience. J . clin. Psychol., 1957, IS, 379-382. - . - -_-
14. JORDAN, E. P. (Ed.) Standard nomenclature of disease and standard nomenclature of operations.
1,5. MAHRER, A. R., THORP, T. and STERNLICHT, I. The role of cues in psychodiagnosis. J . gen.
16. NADLER, E. B., FINK, S. L., SHONTZ, F. C. and BRINK, R. W. .J. clin. Psychol., 1959,l4, 39-41. 17. PLAG, J. A. Some considerations of the value of the psychatric screening interview. J . clin.
18. WALLIS, W. A. and ROBERTS, H. V. Statistics: a new approach. Glencoe, Ill.: The Free Press,
Phila.: Blakiston, 1947.
Psychol., 1960, 62, 247-256.
Psychol., 1961, 17, 3-8.
1956.
A SEMANTIC APPROACH TO PSYCHOLOGICAL NOSOLOGY* LAWRENCE N. SOLOMON
Western Behavioral Sciences Institute L a Jolla, California
PROBLEM Classification systems in science serve the purpose of organizing the subject
matter into meaningfully related groups and of facilitating the scientist’s prediction and control of his variables. It was undoubtedly such considerations that prompted Kraepelin to formulate his original classification of mental disorders. The denotative significance of kraepelin’s original categories have been carefully transmitted from generation to generation of clinical practitioners, in this way enhancing communica- tion between workers in the field of mental health. But recent in~estigationc~) of the communication process has revealed that the “meaning” of any concept is multivariate in nature, and that concepts carry connotative as well as denotative significances. The diagnostic categories in psychology and psychiatry are rich in implication (connotative meaning) and there is every reason to believe that these connotations vary greatly among clinicians and thereby reduce the fidelity of their communication.
Indeed, Korman(2) has recently demonstrated significant inter-group differ- ences in semantic structures and in degree of connotative similarity assigned to diagnostic and therapeutic concepts between psychologists and social workers. He also demonstrated that for psychologists, certain therapeutic concepts tended to cluster semantically into three groups of connotatively equivalent or interchange- able terms. These three groups of terms were: (a) EST, directive psychotherapy,
‘This research was supported in part by a grant from the Sigma Xi-RESA Research Fuqd.





























