-
PSYCHOANALYTICTHEORIES OF PERSONALITY
Instructor: Michael J. Gerson, PhD
Copyright 1993, 1994 by the Institute of Advanced Psychological
Studies. All rights reserved.Except as permitted under the United
States Copyright Act of 1976, no part of this publication may
be reproduced or distributed in any form or by any means, or
stored in a data base or retrieval system,without the prior written
permission of the publisher.
-
Introduction
The following course is an examination of the psychoanalytic
theories ofpersonality. In an effort to synthesize nearly 100 years
of theoretical formulations,there are some inevitable conflicts,
contradictions and confusions that arise relative toterminology.
Freud, for example wrote about "character types" while today, the
DSM-IV (see American Psychiatric Association, 1952, 1968, 1980,
1987, 1994) refers to"personality disorders;" Kohut reconstructed
some of the psychoanalyticmetapsychology into a study of "self' and
"disorders of self," while Kernbergelaborated upon "borderline
personality organization." While each of the above termsdemarcates
justifiably different territories, it is imperative that we also
recognize anecessary unity among these terms as a goal toward an
improved understanding of thehuman experience. The fact that so
many different terms become justified to illustratedifferent areas
of interest only attests to the complexity of the mind, emotions
andbehavior. F or the purposes of this course I will utilize the
terms "character" and"personality" somewhat interchangeably only
making differentiations where necessaryand significant. Other terms
such as "ego," "self," and "identity" have
well-establisheddifferentiations in the literature that require
careful consideration regarding underlyingtheoretical models. Also,
in an effort to make this course comprehensive, a variety
oftheoretical models or paradigms will be referred to with some
occasional digressionsfor clarification purposes. It is our hope
that this multi-modal approach will allow youto consider the
information both critically and in a manner that can best be
integratedinto your clinical experience.
Along the lines of the goal of clinical integration, the DSM-IV
categories ofPersonality Disorders will also be incorporated into
the discussion. While werecognize that the DSM-IV is an
atheoretical compendium of nosological conditions,the rich
psychoanalytic history on personality formation and pathology can
offerinformative and challenging insights into an understanding of
these conditions.
1
-
What Constitutes Personality Formation?
Personality formation refers to the process whereby an
individual becomes anindividual; that is, the process whereby one
develops stable and enduring patterns ofthinking, feeling, and
behaving. These patterns are, to a large degree, adaptations bothto
the internal demands of instinctual drives and tensions as well as
to the externaldemands for conformity and socialization. Character
formation represents a resolutionto these conflicts and can
therefore be seen as a person's best effort at "staying sane."In a
more technical sense, personality results from autoplastic
(self-modifying)adaptations that are ego-syntonic (subjectively
congruent). Classic psychoanalytictheories on personality formation
are in many ways remarkably consistent with thesocial
interactionist's position in contemporary child development theory,
to the extentthat psychoanalytic models have anticipated a
necessary integration of innatepredispositions with environmental
factors. Their major points of departure are thatthe innate
predispositions that psychoanalytic theories consider consist of
instincts anddrives rather than temperament features. The earliest
environmental factors ofpsychoanalytic theories are limited almost
exclusively to the qualities of and theimaginative constructions of
the parent-child interactions as experienced by the child,rather
than a more broadly based inclusion of learning theory,
sociological, andcultural factors.
With parents as the personification of external reality, the
psychoanalytictheories examine the processes by which parents serve
as models for ego, ego-ideal,and superego formations. The
psychodynamics of introjection and identification serveas the
fundamental processes for this aspect of character shaping in
concert with thespecific events of psychosexual and psychosocial
developmental stages. This meansthat when and how the parent-child
conflicts arise, and when and how they areresolved, will determine
whose attitudes the child imitates and incorporates; whetherfor
example, the nurturing characteristics of the parents or their
prohibitive attitudesbecome part of the child's legacy.
Constitutional factors may also play a part in the
psychoanalytic theories aboutcharacter formation to the extent that
some persons may be better able or more ill-equipped at managing
the tensions caused by aggressive and sexual drives. Somepeople may
be better able at identifying and adjusting to the needs of the
child thanothers and be capable, in varying degrees, to tolerate
the projections of the infant'sfantasies. This consideration leaves
the door open for biological and genetictransmission theories about
personality and is consistent with findings
regardingtemperament.
2
-
The phenomena of fixation and regression are particularly
illuminating to ourunderstanding of personality development because
they suggest the importance ofdifferent developmental stage
experiences and their possibly intrusive impact upon
thepersonality, or the resolution of these experiences by adjusting
the personality intonormalizing them. That is to say, developmental
crises can be dealt with dynamicallythrough repression and other
defensive measures possibly leading to some form ofneurotic
compromise formation that may emerge episodically in the form
ofpsychoneurotic symptoms, or developmental crises can be resolved
by adjusting ordistorting the character in a manner such that the
crises are assimilated and integratedinto behavior that appears
relatively normal. Thus, whether one is induced by periodicstresses
or cues to regress to previous developmental events, or whether one
carrieswith him or her the artifacts of these events in the form of
fixations, the significanceof a person's developmental history can
serve to shape the various personality traits.The extent to which
these traits are normal or pathological is usually considered
amatter of flexibility. This distinction, based on degree of
flexibility is largely thecriterion used in DSM-IV to differentiate
personality traits from personalitydisorders.
What Constitutes a Personality or Character Disorder?
As I alluded to above, there is an important distinction between
neuroticsymptoms and character traits. Freud noted in 1913 that the
neurotic symptoms arisefrom a failure of repression, i.e., a return
of the repressed that disrupts the normal andexpectable functioning
of the individual. By contrast, classical theory suggests
thatcharacter traits owe their existence to the success of
repression and the defensivesystem that is able to achieve a
pattern of relative stability through reaction formationand
sublimation. In subsequent writings that elaborated on the
processes of the egoand the id, Freud (1923) expanded upon the
process of identification as a form ofadaptation. In the context of
a lost object (or relationship) the process of identificationcan
function such that an internalized representation is constructed
and the conflict(loss/ mourning) can be minimized or resolved by a
special form of internalizationcalled introjection. The
introjection of the parental or societal attitudes in the form
ofthe superego likewise allows for an enduring referential base of
right and wrongagainst which a resolution of conflict or the
restitution for misdeeds can be made. Theprocess of introjection
accounts for the relatively enduring characteristics of thesuperego
structure. Thus, identification, internalization and introjection
arefundamental processes that establish the adaptive capacity of
the ego system such thatconflict can be prophylactically avoided.
The net result is a psychic system shaped tothe demands of the
instinctual drives and the constraints of external reality.
3
-
In the case of character disorders we are examining a
heterogeneous group ofpersonality styles that share the common
features of being habitually inflexible inpatterns of thought,
affect and behavior and who also experience their being
inflexiblewithout any apparent subjective distress. Thus, other
people experience the conflictsand contradictions of the
personality styles, but not the persons who exhibit them.Clearly
these are disorders of relationship in that the pathology is
recognizable only inthe context of an other and that these
disorders are paradoxically inconspicuous totheir owners. As one
might expect, the absence of subjective distress eliminates
anymotivation for change and can severely diminish the prospects
for a favorableprognosis in treatment. While persons may be
unlikely to seek treatment directly for apersonality disorder, they
are likely to seek treatment for an associated condition suchas
marital dissatisfaction or job-related stress. Certainly, it is
also possible for personssuch as these to seek treatment for an
unrelated issue such as the death of a familymember and then face
the impact of this stressor upon a given rigid, inflexible
over-adapted personality organization. In either case a
psychoanalytically oriented cliniciancan generally expect that what
distresses a patient is the initial focus of treatment,while their
character style dictates how treatment needs to be conducted. For
thisreason an assessment of character style and / or character
disorder is essential for acomplete understanding of the patient
and treatment planning.
Otto Fenichel in his classic treatise on The Psychoanalytic
Theory of Neurosis(1945) provided one of the most thorough
examinations of character disorders andoffered a basis for the
classification of character traits. He noted that some
character"attitudes" (i.e., stereotyped ego reactions) demonstrate
a reciprocal relationshipbetween character traits and neurotic
symptoms. That is, a character attitude is anattempt to "make the
best of established neurotic conditions." These patients
sacrificetheir developmental potential through the wasteful
expenditure of energy in the formof definitive patterns of constant
counter-cathexis. The resulting limited patterns ofdefense lead to
a permanent deforming of the ego. For Fenichel, the character of
anindividual is constituted by the ego's habitual modes of
adjustment to and from theexternal world and toward the superego
and id. The characteristic types-of-combiningthese modes with one
another constitute character and what he termed
"characterattitudes." These attitudes are changes that are brought
about through the adaptationalre-shaping of the instinctual
demands. Therefore, Fenichel was describing character asa
sub-process of the ego that essentially stylizes the operation of
the various egofunctions. Character sets the distinctive stamp upon
how the ego system achieves itsvarious purposes. In the case of
pathological character, the stamp is routinized andstereotypical -
certainly not geared toward being generative and creative.
Thecharacter can be
4
-
highly functional, but only in a limited sense given that life
is reliably unpredictable.
As a basis for the classification of character traits, Fenichel
chose thedistinction between whether a character trait aims at
discharging an instinctualimpulse or suppressing it. The former
group he referred to as Sublimation Types andthe latter group
Reactive Types. F or the most part he believed that the
SublimationType was non-pathological since it succeeds in replacing
an existing instinctualimpulse with an impulse that is compatible
with the ego and one that is organized andinhibited as to aim-- "a
channel and not a dam for the instinctual stream" (Fenichel,1945,
p. 471). These character trait types are of greatest importance for
the treatmentof character disorders as they represent the goal of
transforming the reactive type intothe sublimation type and thereby
achieving "successful repressions."
Reactive character types which are the subject of study for
psychopathologyare further sub-divided into phobic attitudes and
reaction formations. Phobic attitudesreflect attitudes of avoidance
and an escape from the awareness of instinctualdemands. Reaction
formation attitudes reflect attitudes of opposition in the hopes
ofcamouflaging the instinctual demands in a sea of exaggeration and
counter-cathexis.So, for example, a phobic-type character might
devote his or her life to combatpornography as an avoidance of his
or her own lustful desires; while the reaction-formation type might
pursue a career as a comedic actor to oppose feared emotions
ofdepression and sadness. Both of these character types reveal a
fundamental conflictbetween the instinctual drives and the ego
system's ability to manage them. Characterserves a defensive
function in protecting the integrity of the ego through its
persistentreactive style.
By examining the function of character or personality traits
vis-a-vis theinstinctual drives we are also essentially examining
the relationship between characterand the emotions. Fenichel noted
that the defensive function of character types is notonly directed
against impulses but rather against the emotions related to the
impulses.Narcissistic characters, for example, who seek out
confirmation from others abouttheir power and prestige may do so to
defend against the primitive dependency needsand associated
feelings of helplessness and powerlessness. These same
individualsmay sometimes tolerate some emotions because they can be
justified as reasonableand rational thus utilizing rationalization
as a defense which serves to support a senseof narcissistic
omnipotence.
5
-
Fenichel proposed an organization of character types that
afforded a distinctionbetween the enduring, ego-syntonic features
of the character disorder and theepisodic, ego-dystonic features of
the psychoneuroses. His typology addressed thedifferent
manifestations of character types relative to the management of
instinctualdrives. A more contemporary attempt at organizing our
understanding of characterdisorders has been put forth by Otto
Kernberg (1967, 1976, 1980). While much ofKernberg's work examines
the dynamics and characteristics of the borderlinepersonality
organization, his scholarly critiques of theory have resulted in
anunderstanding of personality disorders based upon the development
of ego andsuperego structures and their related processes. Kernberg
distinguishes betweenhigher-level character pathology and
lower-level character pathology. Higher-levelpatients possess a
well integrated superego structure that is relatively punitive
andsevere. The ego is also well integrated to the extent that there
is a stable ego-identity,self-concept and representational world.
While the defensive operations may beextensive, they utilize
repression to resolve conflict and retain ego integrity. In
short,the higher level character pathologies are quite similar to
Fenichel's reactive types.Examples of these disorders would include
the hysterical (histrionic), obsessive-compulsive and the
depressive-masochistic (a depressive character capable
ofexperiencing guilt about anger at a lost object and able to
tolerate mourning, i.e. adysthymic disorder). The lower-level
character pathologies exhibit severe structuraldeficits in the ego
and superego and related developmental consequences. Thesepersons
have minimal superego integration and a tendency toward the use of
primitivedefenses such as splitting, projection, denial,
projective-identification and idealization.The resulting internal
world of these patients is unintegrated and split into
dissociatedego states.
Dissociated ego states refer to an immature fixation of ego
developmentresulting from the predominant use of the splitting
defense. In this defense, mentalrepresentations of self and object
developed through aggressive strivings are split offfrom the mental
representations of self and object developed through
libidinalstrivings. The net effect is an unintegrated set of bad
and good representations thatretain primitive, crude and simplistic
distinctions between self and object and betweenbad and good
emotional experiences. The perception of reality is severely
limited andthe tendency toward idealization and devaluation is
predetermined. The developmentof emotions is likewise restrained by
the bad-good dichotomy such that ambivalenceis not experienced and
therefore neither are the subtleties of emotional experiences.The
entire spectrum of human emotions is reduced to a simple bad-good
dimension.Examples of the lower-level character pathologies include
the narcissistic, borderlineand anti-social personalities.
6
-
What Kernberg is offering is a typology based around the
development of egoand superego. Those disorders which exhibit
primitive or infantile ego and superegodevelopment are at the lower
end of the continuum, while those with more mature egoand superego
development would be at the higher end. To proceed with
thiscomparison we will need to identify the various structural
features of the mind andtheir corresponding operations.
A structural analysis of the mind corresponds to an analysis of
the mentalprocesses from the point of view of the id, ego, and
superego structures. Thepredominant focus is upon the development
and operation of the ego system withregard to the management of
instinctual drive derivatives; the autonomous egofunctions such as
language, intelligence, motility, perception and thought;
primaryand secondary thinking processes; defensive operations; and
the structural derivativesof object relationships. Another
dimension of structural analysis addresses the relativestrength or
weakness of the ego with regard to the capacity to tolerate
frustration oranxiety this includes the control imposed over
instinctual impulses and the channelsavailable for the sublimation
of drives. Ego weakness which would predictablyrepresent the
lower-level character disorders would evidence a lack of
anxietytolerance such that the ego reacts to anxiety with
regression or additional symptomformation. Impulse pressures
likewise are discharged unpredictably and erratically bythe
lower-level disorders while they can be specifically expressed in
an ego-syntonicepisode by higher level disorders. Sublimatory
channels reflect assessments ofpotential versus actual performance.
The lower-level disorders being inhibited withregard to their
potential performance are unable to utilize their creativity. Thus
thisaspect of ego functioning is limited both in terms of the
patient's capacity for creativeenjoyment and creative achievement.
A similar distinction is suggested by Winnicott(1960) in his
comparison of the true and false-self. In that example, the
true-self,which represents a constitutional potential, is
facilitated developmentally by thestimulation of creative
expression. The false-self represents the adaptation allymotivated
compromises to reality and a protective process for the true-selfs
integrity.
What Kernberg presents in his classification of personality
disorders is a meansfor comparing the different types of characters
relative to each other on the dimensionof structural integration.
In doing so he postulates both quantitative and
qualitativedistinctions that are etiologically based (i.e., he
presumes the causes of the disorder,why it appears the way it does)
rather than being merely descriptively based (i.e.,describing the
manifest presentation of the symptoms in terms of how
thepsychodynamics account for the appearance of the disorder).
Kernberg's use of theterm "borderline personality organization"
further allows for an examination of
7
-
a spectrum of conditions along the continuum of structural
development from pre-psychotic to neurotic levels of
functioning.
We will now explore some of the personalities of the DSM-IV as a
referentialbase of character types and discuss them in term of
descriptive, structural, defensive,and object-relational
conditions. As you are probably aware, the DSM-IV isatheoretical
and descriptive such that it divides the personality disorders into
threeclusters (A, B, C) based upon manifest symptoms. Cluster A
represents thosedisorders whose symptoms are odd and eccentric.
These include the Paranoid,Schizoid, and Schizotypal Personalities.
Cluster B is characterized as being dramatic,emotional, and
erratic. This cluster includes the Borderline, Narcissistic,
Histrionic,and Anti-Social Personalities. Cluster C is described as
anxious and fearful and isconstituted by the Dependent, Avoidant,
and Obsessive-Compulsive. The DSM-III-Rincluded the Passive
Aggressive Personality Disorder in Cluster C as well; thedisorder
would be diagnosed as "NOS" using the DSM-IV.
Cluster A
The Paranoid Personality Disorder describes individuals
characterized bysuspiciousness, mistrust, irritability, and
emotional coldness. They appear hyper-vigilant to anticipated
dangers and are likely to put others on the defensive by
beingaccusatory and judgmental. Like all character types, these
persons perceive and actupon the environment in this manner all the
time. This is in contrast to a DelusionalDisorder where a patient
is likely to have evolved a delusional explanation orjustification
for their views or behavior. This latter condition is also not
reflective of alifetime pattern or a pervasive orientation to the
world, but rather, is a symptomaticcondition that arose from the
breakdown of repression. In paranoia the impulse and itsderivative
ideational content is projected onto the environment where it can
bedefended against externally. Freud (1911) in the Schreber case
elucidated the processwhereby paranoia evolved from the repressed
homosexual urges of the patient. In aseries of defensive
transformations the thought derivative "I love him" was denied
andtransformed by reaction formation into "I don't love him, I hate
him." This moreconsciously acceptable idea was projected in the
further transform "It is not that I hatehim, he hates me!" With
this version of the thought near consciousness, the patientcould
modify the idea slightly with rationalization to become "I hate him
because ofhis hatred for me." Thus Freud accounted for the range of
persecutory, erotic, andjealous delusions as the transforms of
unacceptable libidinal drive derivatives.
8
-
For the Paranoid Personality we see a slightly different picture
from that ofdelusional paranoia in that there is a constant flow of
aggressively determinedprojections from the patient to the
environment that establishes a world that isdangerous. This world
becomes the reification of the patient's intolerable feelings
andthoughts. The relationship to the world and its occupants is
understandably dangerousgiven that it is constantly being populated
by these aggressively determinedprojections. The internal world of
the patient is prevented from maturing beyond theinfantile level
given that the negative part-objects are being projected and are
thusunavailable for integration with the positive part-objects that
are retained. A viciouscycle ensues such that the projections are
reintrojected as perceptions of hostility anddanger. An
intensification of the splitting process keeps the patient's
libidinallydetermined part-objects (positive part-objects) from
being contaminated by theseperceptions of danger and affords a
false sense of objectivity and perspective. Thepatient has effected
an internal polarization of aggressive and libidinal
part-objectswith the former being attributed to the perception of
external events and the latter tothe patient's rational, objective
mind. Emotional restrictiveness would be a by-productof a process
that maintains the basic simplicity of good-bad, me-not me
distinctionscaused by the splitting defense. This restriction of
affect is typical for this character.
With all of the above description of the psychodynamic
machinations it must beremembered that these processes are not
operating independent of reality. Cameron(1963) notes that the
origin of the Paranoid Personality is likely an environment thatwas
. hostile, unloving, possibly abusive, but certainly not conducive
for thedevelopment of basic trust.
The Schizoid Personality can also be presumed to have originated
from anenvironment that was lacking in basic trust (Cameron, 1963).
They differ to the extentthat the expression of rage and aggression
was so stifled as to leave the individualpassive, compliant,
obedient, and detached. Fairbairn (1940) stressed the role
ofdepersonalization, de-realization, and disturbances of the
reality-sense such that thesepersons sense themselves as
artificial. He describes how these patients refer to a"plate-glass"
between them and others with a strange sense of unfamiliarity with
thefamiliar and familiarity with the unfamiliar. One gets the
impression that thesepatients exist in a perennial dream-like
detachment. Winnicott's concept of the "falseself" personality
would help to describe how the "true self" (core creative
self)remains protected and insulated by a false adaptive self. This
"false self," even ifsufficiently competent to negotiate the events
of life, could only, at best, achieve a"false" ego-strength and
"false" self-esteem. The "true self" always remains
hidden,impoverished, suffering and lacking in
9
-
experience. The life and accomplishments of the individual seem,
to them, inauthenticand devoid of pride.
The interpersonal relations of the Schizoid are, as Guntrip
(1952) described: "emptiedby a massive withdrawal of real libidinal
self ... The attitude to the outer world is thesame:
non-involvement and observation at a distance without any feeling
... "(p. 86).Thus, we see a patient who remains in their own
asocial existence whose pain,rejection, anger, and longing, all
expectable emotional scars from a childhood ofcoldness and
betrayal, are masked behind a shroud of apparent apathy. Whereas
thesepatients appear bland and deadened, they may engage in active
primary processreveries which are rarely revealed to any of the few
relations they may have.Therapists sometimes underestimate these
patient's true emotional commitment andunwittingly victimize them
with premature terminations or other countertransferencerejections
like falling asleep or changing their appointment times.
From an object relations perspective we could expect that the
self-objectimages of these patients are not clearly differentiated.
Rather than projecting theaggressively determined object
representations into the environment and thendefending against them
externally, as the Paranoid Personality does, these patientsregress
to a pre-psychotic state of self-object undifferentiation. Their
ability to remainstable at this level prevents them from
degenerating into a more classic schizophrenicautism. The
withdrawal of object libido is not reinvested in the self, as we
would seein a Narcissistic Personality, but rather is dissipated
into primary process imaginingsand "protective" distractions. This
latter process gives the Schizoid their detached,dream-like
appearance.
An interesting and somewhat unique description of the Schizoid
patient ispresented by Bollas (1989) in what he calls the
"ghostline personality." These patientsexperience a failure of the
"potential space" between the self and the other such thatthe child
cannot "live" in this intermediate or transitional area. The
consequence ofthis failure is a psychic death of the part of the
"true self' or the potential "true self' orthe transitional object.
The essence of that which dies is transferred to an inner
worldBollas refers to as the "alternative world." This "alternative
world" functions as aninternal world populated by the foreclosed
self states and object representations.Unlike the conventional use
of the internal world to contain representations of objectsin
external reality, this "alternative world" contains ghosts of
object and selfrepresentations that could not be sustained. This
realm of the mind becomes thepsychic afterlife. The patient
conserves these ghosts in the "alternative world" wherethey can
potentially be re-incarnated through the transference. It is
through thealiveness of the analyst, who serves as
10
-
the transitional object, that the "alternative world" can be
transformed. Thesealternative objects can be transformed into "true
self' states and objectified objects bythe use of the transitional
object (therapist) who provides life and an arena wherein toshare
the experience of the "alternative world." What Bollas so
poetically capturesabout the Schizoid Personality is the macabre
romanticizing of a death-like being statethat could easily remain
unseen by a superficial symptomatic description of thepatient.
In contrast to the Schizoid Personality who withdraws passively
from socialcontact, is the Schizotypal Personality who withdraws
erratically and is active only onthe fringes of social contact.
These personalities have historically been viewed as"stabilized
schizophrenics" by Bleuler (1911), "autistic personalities" by
Kraepelin(1919), "ambulatory schizophrenics" by Zilboorg (1941), or
the "schizophrenicphenotype" (the full term from which
"schizotypal" is a shortened form) by Rado(1950). What is striking
about these patients is their peculiarities of speech, behavior,and
beliefs which can give them the appearance of a psychosis. They
remain,however, connected to reality if only in the form of
bizarre, eccentric, or out-of-the-ordinary beliefs. Like the
Schizoid Personality, their emotional life is deadened, butthe
Schizotypal is clearly capable of explosive and aggressive
outbursts (Millon,1981).
So, if we were to extend the above discussion about the
psychodynamics and objectrelatedness of the Schizoid to that of the
Schizotypal, we could propose that ratherthan a massive withdrawal
of libidinal cathexis, here we find an occasional intenseinfusion
of aggressive energy in some part-object representation. Given that
thesepatients present with the "primary symptoms" of schizophrenia
(disturbed associationsof thought; splits between affect and
intellect; ambivalence toward objects; and anautistic detachment
from reality (Bleuler, 1911)), their self and object
representationswould be fragments of external reality. Should their
detachment from society beintruded upon in some way their internal
state becomes agitated and they perceive thisas a violent
aggressive act. The primitive quality of their mind is limited in
itscapacity to accommodate to the intrusion and they regress to a
pre-psychotic fusedself-object experience with the intrusion. Their
aggressive explosions are essentiallyan externalization of this
internal chaos. Some stabilizing ego functions allow for asemblance
of a synthesizing of these fragmented elements by adhering to
fringebeliefs such as UFO's; clairvoyance; reincarnation; etc. The
interface between theirprimary process thinking and society's
"twilight zone" of belief systems, gives thesepatients a meeting
ground that supports their ability to connect. Their odd speech
andneologisms can likewise serve as a consolidation of autistic
thinking with a sociallanguage system. They can thus retain their
detachment by employing unusual oridiosyncratic words
11
-
while weaving them into a conventional fabric of social
discourse. They are, at once,connected, and detached hence their
erratic style.
The erratic quality of the Schizotypal together with their
aggressive capabilitiessometimes confuses this character with the
Borderline Personality (Millon, 1981).This similarity exists only
at the level of some manifest symptoms. A more basicdifference is
postulated by the various psychodynamic descriptions to follow.
Cluster B
The Cluster B disorders of DSM-IV include the Borderline,
Narcissistic, Anti-Social,and Histrionic Personality Disorders.
While Kernberg describes these as varyingalong a continuum of
"borderline personality organization, " other
psychoanalyticdescriptions can view them as relatively discrete and
autonomous disorders (Knight,1957; Schmideberg, 1947; Stem,
1938).
The Borderline Personality Disorder as presented in DSM-IV has
the manifestsymptoms of: unstable interpersonal relationships;
impulsive behavior; affectiveinstability; inappropriate intense
anger or rage; recurrent suicidal threats, gestures orbehavior;
marked and persistent identity disorder; chronic feelings of
emptiness orboredom; and frantic efforts to avoid real or imagined
abandonment.
Historically, the Borderline Personality Disorder has referred
to a condition midwaybetween neurotic disorders and psychotic
disorders (Stem, 1938) or as a complex oftraits and symptom
features of both neurotic and psychotic type that constellates in
arather stabilized instability (Schmideberg, 1947, 1959). Knight
(1957) added to thepsychodynamic understanding by highlighting
ego-weakness as a critical feature ofthe disorder. Kernberg's
formulations (1967, 1975) about the borderline
personalityorganization has incorporated all the above into an
object-relations model.
Kernberg (1967, 1975) attributes the symptoms to the
"dissociation of ego-states"under the impact of primitive defenses
such as splitting, projection, projectiveidentification, and
denial. The psychic stress experienced by the Borderline patient
inan effort to organize internal and external experience leads to
an intensification of thesplitting process leaving the patient
ultimately unable to integrate good and bad self-object images.
Aggressive instincts are not neutralized so the intensity of these
drivesremains powerful and infantile. Idealization and
12
-
devaluation are typical derivatives of the un-neutralized
aggressive drive.
Unlike the Paranoid patient who actively defends against the
projections ofaggressively determined object images, the Borderline
patient is fixated at a level ofambi-tendency with the world (i.e.,
an approach-avoidance type oscillation).
The Borderline alternately projects the aggressive images to get
distance fromthem, then reintrojects the object in response to
feelings of estrangement andabandonment.
Masterson (1981) offers another variation of the Borderline
Personalitypsychodynamics through the incorporation of
developmental theory and the conceptof a "split object-relations
unit." Briefly, this model focuses on the adaptivecharacteristics
of the mother and child during the rapprochement sub-phase of
theseparation-individuation process in Mahler's theory. Significant
for this sub-phasetoward the development of Self, is the child's
ability to retain the newly evolved,tenuously held experiences of
separateness under the impact of individuationautonomy and the need
for periodic re-attachment to the mother. Masterson contendsthat
parental inconsistency during this period can result in an
abandonment depressionthat is fundamental to borderline
psychopathology. The child can experience thematernal part-object
representation as withdrawing, angry and critical of the
child'sefforts to separate. The affective link to this experience
(a form of emotional memory)is a profound abandonment panic,
depression, helplessness, emptiness, or rage. Thechild's part-self
representation is internalized as inadequate, bad, ugly or
insignificant.The resulting personality disturbance centers around
the projections and defensesagainst abandonment as it emerges in
interpersonal relationships. Clearly, bothMasterson and Kernberg
describe personalities that meet the DSM symptoms; theydiffer in
terms of how and why the symptoms appear.
In turning to an examination of the Narcissistic Personality
Disorder we shouldbegin with Freud's rather straight forward model
of libidinal maturity. Freud originallydescribed narcissism as the
mid-point between auto-erotic and object love (Freud,1910).
Therefore, the body becomes a love object as a transition from
auto-eroticsensations to the appreciation for the other. In 1914
this concept was linked to libidotheory wherein a developmental
progression for libido was presented. In theautoerotic phase,
"primary narcissism" was the investment of libido into
theexperience of the body. This investment is eventually made into
an other who canthen be loved as the self once was. Object-love
comes to replace self-love as anelaboration and extension of
loving. Complications to this sequence can occur whenthe object of
the person's love fails to be sufficiently gratifying or
13
-
is abandoning and rejecting. Under these conditions, libido is
withdrawn from objectsand re-invested in the self. This defensive
re-cathexis of the ego (ego and self wereused interchangeably)
leads to an exaggeration of self importance and power.
Themegalomania, omnipotence and grandiosity of this form of
narcissism was viewed aspathological and a "secondary narcissism"
(as opposed to normal "primarynarcissism"). For Freud, then, a
pathological narcissist was the result of a libidinallydetermined
regression to a pre-object-love state. Wilhelm Reich (1926) coined
theterm "phallic-narcissist" to refer to a fixation at the phallic
stage of developmentwhere arrogance and self-assurance serve as
defenses against castration anxiety.
As was noted earlier, Kernberg views narcissistic pathology as a
variant of theborderline personality organization. He interprets
the arrogance and grandiosity as adefense against the projection of
oral rage. This rage stems from a incapacity todepend upon
"internalized good objects" that keep the narcissist in a perpetual
state ofinner emptiness and abandonment. Their anger is a
revengeful resentment for theirincapacitating internal world.
Kernberg notes that these patients often reveal historiesof parents
who were cold, aggressive, and spiteful towards their children. He
alsonotes that the children were often once viewed by the parents
as having special talentsor genius making them exceptional targets
for the parent's idealization and eventualdevaluation.
Masterson (1981) describes the Narcissistic Personality also as
a variant ofborderline pathology, but with regard to an
object-relations unit of the parent andchild that is rewarding for
clinging, dependent, and regressive behavior. The child
isessentially fixated by the parent-child dyad at a level of
self-object fusion thatundermines the child's ability to
differentiate and further guarantees the child'sinevitable
disappointment with others who could never supplant the
parent-childspecialness. In contrast to Kernberg who would tend to
view the NarcissisticPersonality as a slightly more developed
Borderline disorder, Masterson sees theNarcissistic Personality as
pre-dating the development of the Borderline Personalitygiven the
more symbiotic character to the part-object relations fused
unit.
Heinz Kohut (1971, 1977) has offered an explanation of
narcissism that isfundamentally different from any of the above. He
posits that at birth two fonns oflibido exist and follow different
lines of development. Object libido follows the pathelucidated by
Freud and is responsible for the transformation of auto-eroticism
intoobject-love. This process is essential to the maturation of the
ego system indifferentiating self from object representations.
Another form of libido, narcissisticlibido, is responsible for the
development of Self as a separate psychic structure.
14
-
The development of Self requires the integration of two major
"spheres;" the"grandiose self' and the "idealized parental imago."
The former represents the residueof infantile grandiosity while the
latter represents the residue of dependency andprotective
symbiosis. Collectively, these spheres represent the "bi-polar
Self. "
The development of narcissism is facilitated by the maintenance
and creation ofselfobjects which are representations of the
person's Self organization. That is, theyare what the compound word
itself represents, a merged self and object experience(pure
subjectivity). Selfobjects serve to maintain the child's
equilibrium by adjustingto shifts in internal emotional
vulnerability. Parents function as the first selfobjectsthrough the
provision of an empathic relationship to the child that mirrors the
child'sself state. Serving as a selfobject they provide a
transforming or transmuting functionfor the child's painful
emotional experiences (not unlike the auxiliary ego functions
orstimulus barrier functions discussed by object-relations
theorists). Pathology resultsfrom empathic failures that impede the
integration of the two spheres of the Selfleaving one or the other
to serve in a compensatory fashion. For instance, a failure
ofgrandiosity can be compensated by a symbiotic re-fusion with an
idealized parentalimago selfobject, or, a disappointment by a
fallen ideal can be compensated by agrandiose inflation, seeking
validation from the world.
As pathological conditions persist, the dynamic tension arc
between these twopoles of Self oscillates to extreme degrees of
compensation that prevent essentialintegration and keep the Self
fixed at an infantile level. This process may soundsimilar to the
reinforced splitting mechanism described by Kernberg, but is used
in anentirely different context. Kernberg was describing ego
integration with self assubsumed within those processes. Kohut is
referring to the development of Self asseparate from ego such that
the development of Self and ego are independent.Interestingly,
these differences prove to be quite profound when we compare
howthese different theories interpret the severity of the
narcissistic pathology. TheKernberg narcissists
(narcissistic-borderlines) are illustrative of more
severeborderline conditions than the Kohut narcissists. This latter
group could theoreticallyhave higher developed ego functions than
the narcissistic-borderlines would suggestand owe their
narcissistic pathology solely to a failure of Self development. In
anyevent, Kohut's model proposes forms of narcissistic
transferences that correspond tothe selfobject representations of
the grandiose and idealized parental imago spheresthat are
immensely helpful in understanding the unique requirements of
thetherapeutic alliance; namely the mirroring, merger, alter-ego
and idealizing functions.
15
-
The Anti-Social Personality is an individual with a life history
of aggressive,destructive, oppositional, and defiant acts. They are
often regarded as lacking aconscience and operating without guilt
or empathy. They manifest a diffuse lack ofimpulse control that
results in frequent irresponsible and thoughtless behaviors
which,at the time of performance (and possibly afterward as well),
are ego-syntonic. TheDSM behavioral criteria for this disorder
attempts to account for the long history ofanti-social conduct by
requiring evidence of symptomatology before age 15 as well
asafterward. What the symptom description lacks, however, are the
essential, but lessobvious, characterological features of the
sociopath. DSM-III-R replaced the olderDSM-II categories of
Sociopathic Personalities (Dissociative and Anti-Social Types)with
the Anti-Social Personality Disorder. The psychodynamic literature
howeverdescribes a character disorder of the sociopath whose charm,
intelligence, callousnessand ability to manipulate others is lost
by the contemporary description that appearsmore indicative of a
common criminal type. The sociopath that Fenichel (1945),Cleckley
(1959), Cameron (1963), and Kernberg (1967) describe is a person
whosebasically borderline personality structure uses others and
society as exploited part-objects to compensate for structural
deficiencies. The absence of conscience, forexample, which is often
cited as indicative of the sociopath is compensated for
byexploiting the conscience of others. These persons project their
anger, hatred, and rageon others who are then made to feel guilty
for feeling revengeful.
Prior to a recent California state execution, a condemned
prisoner chastised.society for its inhumane treatment of him and
its barbaric punishments. The convictedmurderer, who shot two
teenagers after stealing their car, praised the protesters of
theexecution and condemned the state for failing to be empathic
about his abusivechildhood. After once winning a stay of execution
some years earlier, the convictcommented "oh, well" when asked
about his gratitude toward the protesters. This useof projective
identification puts into the Other what the sociopath never has
toconsciously feel. They are spared from developing a superego by
essentiallymanipulating society into serving that function. The
sociopath's behavior can berationalized as a failure of society or
the "system" in creating their personality.Without an internal
capacity for guilt there can be no empathy or compassion.
Thesupervising responsibility for the ego is externalized giving
free reign to instinctualdrives and wishes, hence the high
incidence of impulse disorders, addictions, andsexual perversions.
Collectively, these individuals come to personify the dark side
ofhumanity and, as such, are of an ironic necessity for civilized
social values. Theyprovide the necessary dialectic for the
good-evil dichotomy. Perhaps it is for thisreason that these
patients create such powerful countertransference reactions. They
tapinto the anti-social or sociopathic potential that each of us
has attempted to mature outof. Winnicott
16
-
(1956) notes that the "anti-social tendency" retains a sense of
hope in a world that canbe nurturing. Once hope is lost, the
anti-social tendency gives rise to delinquency andcriminality. I
was once taught that a child would rather be a bad child in a good
worldthan a good child in a bad world. The sociopath, having lost
all hope, depicts a badchild in a bad world where guilt and remorse
are non-existent.
To complete our discussion of Cluster B, we will now turn our
attention to theHistrionic Personality Disorder. These individuals
typically present as sociallymotivated, dramatic, exhibitionistic,
and yet, dependent persons. Compared to theother disorders of this
Cluster, the Histrionic is clearly higher functioning in terms
ofego structure, types of defenses used, emotional development,
insight into themselves,and apparent developmental level (Kernberg,
1975). While these patients can exhibitthe impulse conflicts, fears
of abandonment, hyper-emotionality, and interpersonalmanipulations
which would suggest a similarity with the above disorders,
theHistrionic demonstrates these symptoms from a more reality based
and matureperspective. For example, the Histrionic Personality may
be impulsive in regard totheir behavior, but this impulsivity would
be more in line with spontaneity rather thanthe destructive or
dangerous acting-out by the Borderline or Anti-Social
Personalities.The Histrionic fears abandonment and loss out of
strong dependency needs but tendsto protect from these experiences
by maintaining a backlog of friendships andacquaintances. Once
faced with a loss or abandonment they can recover by utilizingmore
mature ego functions like reality testing or sublimating their
dependency needsinto altruistic endeavors. As the long history of
the term hysterical-histrionic suggests,these persons are highly
emotional and seem to be consumed by affect over intellect.
While once thought to be a female disorder related to a
"wandering womb"(Millon, 1981), their emotional lability coupled
with cultural stereotyping still tends tosuggest patients with a
distinct "feminine character" (Cameron, 1963). The emotionalquality
of these patients is quite different from the other Cluster B
conditions as well.While the Narcissistic Personality is likely to
experience intense envy with acorresponding wish to destroy and
spoil, the Histrionic tends toward jealousy and awish to win over
or possess. The Borderline intrudes into the
psychologicalboundaries of others while the Histrionic seduces and
entices the crossing ofboundaries. If the Borderline needs to be
contained emotionally; the Narcissistentertained; the Anti-Social
restrained; the Histrionic needs to do the entertaining.They
require recognition and are active in the pursuit of being noticed.
The Narcissistwould never be content with just being noticed, they
must be admired!Developmentally, Histrionic patients are fixated at
the phallic level
17
-
of sexual development (Cameron, 1963). They have not resolved
the oedipal conflictand seem to be in a continual re-creation of
oedipal triangles. The ability to fosterrivalries serves to
reinforce the patient's need for external validation as a
desired"prize" to the victor and also protects the patient from the
fear of the intimacy thatmight evolve should they settle into a
long-term dyad. In this case, the dyad oftentakes on parent-child
characteristics which represent repressed incestuous
conflictsnecessitating an outside relationship or extra-marital
affair to displace the sexualdrives. The ensuing triangle keeps all
of the relationships manageably superficial.
Under stress, these patients are prone toward regressions which
resemble thelower-level character disorders of the borderline
spectrum. While they also present apredominantly "false" self as
evidenced by their being easily influenced by fads andtrends
(Millon, 1981) and their tendency to market themselves as if a
commodity, theyare sufficiently developed structurally (Kernberg,
1967) as to be able to capitalize oncreative talents and skills
indicative of a fair degree of "true" self development(Winnicott,
1960). Their subsequent inability to retain the narcissistic
suppliesachieved by their accomplishments suggests the
insufficiency of the "true" self, hencetheir dependency upon others
for acceptance and approval.
Cluster C
The final cluster of personality disorders is distinguished by
the manifestation ofanxiety and fearfulness in their symptom
pictures. This cluster is comprised of theDependent, Avoidant,
Passive-Aggressive, and Obsessive-Compulsive PersonalityDisorders.
While these conditions all express varying examples of anxiety and
fearthey do not appear to have other pronounced mood or thought
disturbances. Thesecharacters are more typical of neurotic
conditions and seem to best be accounted for interms of
developmental fixations and ego defense configurations.
The Dependent Personality Disorder has been alternatively called
the Passive-Dependent (Cameron, 1963), the Compliant-Type (Horney,
1945), and theSubmissive Character (Millon, 1981). Utilizing
Freud's psychosexual stages as areferent for character fixations or
regressions, Abraham (1924) presented the "Oral-Character." These
individuals presumably bring with them an expectation forcontinued
nurturing and gratification from the world. They remain helpless
child-likepersons expecting to be rescued, protected, fed, and
supported. Fenichel (1945) addedthat these characters become
fixated to the world of oral wishes and disinclined tocare for
themselves. They can identify with persons by whom they
18
-
wish to be cared for and therefore act as generous indulgent
parents. In doing so, theyact toward others as they wish others
would act toward them. Their lack of self-protectiveness borders on
masochism and self sacrifice in an obstinate, and yet naive,refusal
to move from this passive-dependent position.
The Dependent Personality uses their weakness and inadequacy to
circumventresponsibilities and can also employ self-depreciation as
a manipulation of others togain their attention and receive their
absolution. This process has to be carefullybalanced to avoid guilt
which would only reinforce the vicious cycle of guilt
andforgiveness. They tend to rationalize their dependency by
attributing theirhelplessness to circumstances, luck or some other
external source of control. TheDependent, like the idealizing
Narcissist, will ally with powerful others to cover-uptheir own
inadequacy. The Narcissist attempts to "psychically steal" those
attributesthrough their supplication to the other, while the
Dependent merely desires a life ofsecure passivity in the shadows
of the ideal one. The Dependent willingly submergestheir
independence in return for acceptance and support, they do not
desire a vicariousself-aggrandizement through this association.
Predictably, these persons alsosubmerge or repress all expressions
of anger or aggressiveness as this could be lethalto their
dependency needs. The hostile impulses, feelings or thoughts are
turnedagainst the self in an effort to protect the relationship at
all costs. Their anxiety andfear is largely of their own
individuality emerging such that it would threaten anorientation
dedicated to compliance and submission.
The Avoidant Personality Disorder is also dependent upon others
foracceptance but is consumed by fears of criticism, embarrassment,
humiliation, andshame. They represent what Fenichel (1945) called a
"phobic character" as theyreactively avoid situations they
originally wished for. Out of the anxiety generated bythe "what if.
.. " predictions of doom, these persons built a character dedicated
toallaying chronic insecurity and fear. Their defenses against the
anticipated rejectionfoster defenses against defenses and a
spreading of anxiety to limitless proportions.Since this is
characteristic of the person's relationship to life, the
over-reactions arenot noticeable subjectively. These are worrisome
individuals who always findinsecurities and ambiguities to support
their concerns. Avoidant Personalities areactively detached
(Millon, 1981) and actively dependent. They withdraw in fear
butwith desire, unlike the Schizoid who is apathetic. Rather than
responding to theanxiety over dependency needs with passive
compliance and a repression ofaggressive impulses, the Avoidant
represses libidinal as well as aggressive impulses.The motivation
for the repression of the aggressive impulses would be similar to
theDependent while the repression or suppression of libidinal
impulses protects themfrom the pain of desire. Diminished sexual
needs and
19
-
expression avoids the potential for rejection and humiliation. A
retreat into fantasycan serve as an outlet for these impulses.
Given a lack of real experience, the fantasiestend to be both
aggressive and sexual which, when coupled with a punitive
superego,can justify the need for self-exile. Avoidant
Personalities help perpetuate theirloneliness and isolation largely
from an identification with those who weredepreciating and
rejecting. They maintain a relationship with their abusers by
playingboth roles in their mind, that of the belittled and
condemned child, as well as therejecting parent. They are not
beaten down into apathy like the Schizoid nor angeredinto battle
like the Paranoid; the Avoidant, instead, tries to hide from the
persecutorwho resides within them and from whom they also hope to
gain acceptance.
The Passive-Aggressive Personality Disorder has been described
both as an "oralsadistic melancholiac" by Abraham (1924) and
Menninger (1940) and as the"masochistic character" by Reich (1933)
and Homey (1939). The term "passive-aggressive personality" was
also credited to the U.S. Joint Armed Services nosologyof medical
classifications (cited in Millon, 1981) to describe those persons
with aunique propensity for undermining morale and proving to be
corrosive to authoritativestructure.
Abraham (1924) differentiated the oral stage into a receptive,
passive, suckingstage and an aggressive, destructive, biting stage.
In the late oral stage, biting becomesas aggressively determined
process of incorporation where the object is destroyed inthe
process of internalization (i.e., it is cannibalized). The ego
develops an attitude ofambivalence toward the object which is now
experienced under the influence of theaggressive instinct. The
formerly all-gratifying object is now at times
frustrating,depleted, or injured. Menninger (1940) notes that
sadism replaces passive dependencyand gives rise to a
characterological type that is the direct opposite,
namelypessimistic, blaming, contemptuous and petulant. The person
becomes over-demanding and perpetually discontented. The
Passive-Aggressive character representsa back and forth movement
from oral dependency to oral sadism that keeps theemotional and
interpersonal functioning at an infantile level.
Reich (1933) describes a passive form of aggression in persons
who usesuffering and a tendency to complain to inflict pain upon
and debase both themselvesand others who care for them. He proposed
that a deep disappointment in love liesbehind their provocation of
love objects. Their "infantile spite reaction" is an attemptto get
back at those who they feel rejected them by courting love through
provocationand defiance. Homey (1939) added that the masochistic
type despises their owndependency. Their inordinate need for
20
-
others leads to inevitable disappointment and regressive
retaliation. Given stronginhibitions about the destructiveness of
their aggressive fantasies and the guilt theyevoke, the individual
regresses to a passive-dependent position where a pseudo-aggression
such as forgetfulness, procrastination, or self-demeaning behaviors
canemerge in a disguised form of unintentional hostility. The fear
and anxiety overdependency leaves these patients to view almost
everyone as a potential tyrant to bemistrusted and disobeyed.
The final character type to be discussed is the
Obsessive-Compulsive PersonalityDisorder. These are persons who are
caught in a powerful ambivalence overconformity and rebellion. They
utilize thoughts and actions to bind the anxietygenerated by
conflicting impulses under the scrutiny of a powerfully
repressivesuperego. Freud (1908) specified three distinct traits of
the "anal character" thatprovide a clear description of the
Obsessive-Compulsive Personality: orderly,parsimonious, and
obstinate. The orderliness comprises bodily cleanliness,
reliability,and conscientiousness. Parsimony can be exaggerated to
the point of avarice, andobstinacy may amount to outright defiance.
He clearly identified an array ofambivalent characteristics that
were subsequently elaborated upon by Abraham (1921)to include
exaggerated criticism of others, avoidance of initiative, and a
preoccupationwith the control over money and time (there is never
enough of either).
While the above addresses mostly the obsessive or thinking
components of thecharacter, Reich (1933) discussed the compulsive
or behavioral characteristics. Theseinclude a pedantic sense of
order typified by cataloging, indexing and organizing andan
unswerving adherence to pattern and routine. Rado (1959) described
how thesepersons are most critically affected by the experience of
toilet training during the analphase of development. The mother and
child engage in a "battle of the chamber pot"wherein the child is
enraged by mother's interference with the bowel clock andresponds
with a defiant resistance and a fearful obedience to her
punishments. Thedisobedient child is made to feel guilty, undergo
deserved punishment and ask forforgiveness. The guilt comes to
repress the defiant rage, and obedience overcomesdefiance. We see,
here, the precursors to reaction-formation in the form of a pride
inobedience that hides the desire for rebellion, and the beginning
of undoing patternsthat expiate sins with ritualized acts to "undo"
evils and wrongs.
These persons become extraordinarily consistent to the point of
being rigid andunyielding. They have learned to repress all urges
toward autonomy or individualitythat might challenge real or
imagined authority. Secretly, they wish to subvertauthority, but
instead, use these wishes to further strengthen a restrictive
21
-
superego structure. They vigorously defend rules and convention
lest they exposesome excuse for disobedience. Since emotions are
expressions of subjective truth theymay betray the cognitive
conforming pattern. Thus, emotions are mistrusted and to bedefended
against. Defenses such as rationalization, intellectualization, and
isolation allserve the organizing and controlling need to conform
emotions to some pre-set socialstandard .. These are classic
bureaucrats who adhere to "the book" for protocol andpropriety.
When faced with unanticipated events these persons can become
paralyzedor search frantically for the "correct" course of action.
They are likely to spend anhour looking for a lost shopping list
that would take 10 minutes to re-create. While
theObsessive-Compulsive Personality is also a procrastinator like
the Passive-Aggressive, the former is constricted by anxiety over
deciding on an action while thelatter is withholding the action in
order to control.
The Obsessive-Compulsive is also credited with higher
functioning sublimatorychannels (Kernberg, 1967) allowing them
socially acceptable channels foraggressivity such as police work or
surgery, and outlets for conformity such as forjudges and
administrators. To the extreme, these tendencies can be
debilitating andrestricting leaving the patient frustrated and
bitter. Such conditions can lead to personswho are fiercely
moralistic or over controlling of themselves or others. It may
beinteresting to contrast this character with the Histrionic who is
almost the directopposite in many ways. The Histrionic is so
emotional they can hardly think, whilethe Obsessive-Compulsive is
so into thinking they avoid feeling. The Histrionic isspontaneous
while the Obsessive-Compulsive rarely varies their routine.
TheHistrionic is hyper-sexual while the Obsessive-Compulsive is
sexually constrainedand conservative. The Histrionic sees a world
of impressions and sensations while theObsessive-Compulsive sees a
world that is precise and geometrically balanced. Inshort, they are
a marriage made in heaven. Each can provide a vicarious expression
ofthe other's repressed wishes.
Conclusion
This brings to an end this review of the psychoanalytic theory
of personality.While I have tried to be somewhat comprehensive of a
broad base of availableliterature, a great deal of material had to
be omitted with respect to time andpracticality. Should you wish to
pursue this subject more fully, I would direct you tothe reference
section and other IAPS courses on psychoanalytic theory and
technique.
22
-
References
Abraham, K. (1921). Contributions to the theory of the anal
character. In Selected Paperson Psychoanalysis. London:
Hogarth.
Abraham, K. (1924). The influence of oral eroticism on character
formation. In SelectedPapers on Psychoanalysis. London:
Hogarth.
Abraham, K. (1925). Character formation on the genital level of
the libido. In SelectedPapers on Psychoanalysis. London:
Hogarth.
American Psychiatric Association. (1952). Diagnostic and
statistical manual of mentaldisorders (DSM-I) (1st ed.).
Washington, DC: American Psychiatric Association.
American Psychiatric Association. (1968). Diagnostic and
statistical manual of mentaldisorders (DSM-II) (2nd ed.).
Washington, DC: American Psychiatric Association.
American Psychiatric Association. (1980). Diagnostic and
statistical manual of mentaldisorders (DSM-III) (3rd ed.).
Washington, DC: American PsychiatricAssociation.
American Psychiatric Association. (1987). Diagnostic and
statistical manual of mentaldisorders (DSM-III-R) (3rd ed.
revised). Washington, DC: American PsychiatricAssociation.
American Psychiatric Association. (1987). Diagnostic and
statistical manual of mentaldisorders (DSM-IV) (4th ed.).
Washington, DC: American PsychiatricAssociation.
Bollas, C. (1989). Forces of Destiny. London: Free Association
Books.
Cameron, N. (1963). Personality Development and Psychopathology:
A DynamicApproach. Boston: Houghton, Mifflin Co.
Cleckley, H. (1941). The Mask of Sanity. St. Louis: Mosby.
Cleckley, H. (1959). Psychopathic states. In S. Arieti (Ed.),
American Handbook of
Psychiatry. New York: Basic Books.
23
-
Federn, P. (1947). Principles of psychotherapy in latent
schizophrenia. AmericanJournal of Psychotherapy, 1, 129-139.
Fenichel, O. (1945). The Psychoanalytic Theory of Neurosis. New
York: Norton.
Freud, S. (1908) Character and anal eroticism. In Collected
Papers. London:Hogarth.
Freud, S. (1911). Psychoanalytic notes upon an autobiographical
account of a caseof paranoia. In Collected Papers. London:
Hogarth.
Freud, S. (1914). On narcissism: an introduction. In Collected
Papers. London:Hogarth.
Freud, S. (1915). Some character types met with in
psycho-analytic work. In CollectedPapers. London: Hogarth.
Freud, S. (1925). Libidinal types. In Collected Papers. London:
Hogarth.
Horney, K. (1939). New Ways in Psychoanalysis. New York:
Norton.
Kernberg, O. (1967). Borderline personality organization.
Journal of AmericanPsychoanalytic Association, 15, 641-685.
Kernberg, O. (1975). Borderline Conditions and Pathological
Narcissism. New York:Jason Aronson.
Kernberg, O. (1980). Internal World and External Reality. New
York: Jason Aronson.
Kohut, H. (1971). The Analysis of the Self. New York:
International Universities Press.
Kohut, H. (1977) The Restoration of the Self. New York:
International UniversitiesPress.
Masterson, J. (1981). The Narcissistic and Borderline Disorders:
An IntegratedApproach. New York: Brunner/Mazel.
24
-
Menninger, K. (1940). Character disorders. In J.F. Brown (Ed.),
The Psychodynamics ofAbnormal Behavior, pp. 384-403. New York:
McGraw-Hill.
Millon, T. (1981). Disorders of Personality. New York: John
Wiley and Sons.
Rado, S. (1959). Obsessive behavior. In S. Arieti (Ed.),
American Handbook ofPsychiatry, Vol. 1. New York: Basic Books.
Reich, W. (1933). Charakteranalyse. Leipsig: Sexpol Verlag.
Reich, W. (1949). Character Analysis (3rd Ed.). New York:
Farrar, Straus, and Giroux.
Schmideberg, M. (1947). The treatment of psychopaths and
borderline patients. AmericanJournal of Psychotherapy, 1,
45-55.
Winnicott, D.W. (1956). The antisocial tendency. In Through
Pediatrics to Psycho-Analysis. New York: Basic Books.
Winnicott, D.W. (1960). Ego distortion in terms of the true and
false self. In TheMaturation Processes and the Facilitating
Environment. London: Hogarth.
25
-
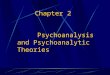
Appendix
CLASSIC PSYCHO-SEXUAL DEVELOPMENT
Borderline
ORAL DEPENDENCY Narcissistic
Paranoid/Schizoid
ANAL CONTROL Obsessive-Compulsive
URETHRA
PHALLIC
GENITAL
KERNBER
STRUCTUAInfantile (Borderline)
WINNICOL C
POW
MAT
G : BORDE
L DIFFERE Narc
TT : TRUE/F
False Self
TrueSelf OMPETITION Anti-Social
Grandiose Narcissist
ER
Hysterical
URITY
RLINE PERSONALITY ORGANIZATION
NTIATION : SUPEREGO DEVELOPMENT
issistic Histrionic
ALSE SELF
26
Social Conformity
Creative Potential
-
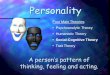
FENICHEL : CHARACTER TYPES
SUBLIMATION REACTIVE
PHOBIC REACTION-FORMATION
AVOIDANT OBSESSIVE-COMPULISIVE
KOHUT : DEVELOPMENT OF SELF
POLES OF SELF
GRANDIOSE IDEALIZED PARENTAL IMAGE
MERGER TWINSHIP ALTER-EGO IDEALIZATION
27
-
MASTERSON : DEVELOPMENTAL OBJECT RELATIONS
RORU WORU
Rewarding Object -Relations Unit Withdrawing Object -Relations
Unit
Reinforced for Clinging (Narcissistic) Abandoned for
Independence (Borderline)
Pre-Ambivalent Ambitendant/Ambivalent
BOLLAS : GHOSTLINE PERSONALITY
28
ExternalObject
GHOSTLINE
TransitionalSpaceInternalWorldAlternativeWorld