Embed Size (px)
Citation preview

Psychiatric Comorbidity of Smoking and Nicotine Dependence: An Epidemiologic
Perspective
Naomi Breslau, Ph.D.
Department of Epidemiology
Michigan State University
College of Human Medicine
email: [email protected]
A recent report in the JAMA called
attention to the observation that smokers
are disproportionately persons with mental
illness.

The connection between smoking and
substance abuse has a long history. However,
the association between smoking and mental
disorders has been recognized since
approximately 1990.
“Persons with a current mental disorder
consumed approximately 44.3% of
cigarettes smoked by the U.S. population.”
(Lasser et al., 2000, JAMA)
National Comorbidity Survey (NCS)
A representative sample of 8,098 persons 15-54 years of age in the U.S. surveyed in 1990 - 1992.
Information on smoking was gathered in a representative subset of 4,414.
Lifetime History of Daily Smoking
“Did you ever smoke daily for one
month or more?”

Lifetime Comorbidity of Smoking and Disorders
The odds ratio estimates smokers’ risk
for a specific DSM-IIIR disorder relative
to persons who never smoked daily.
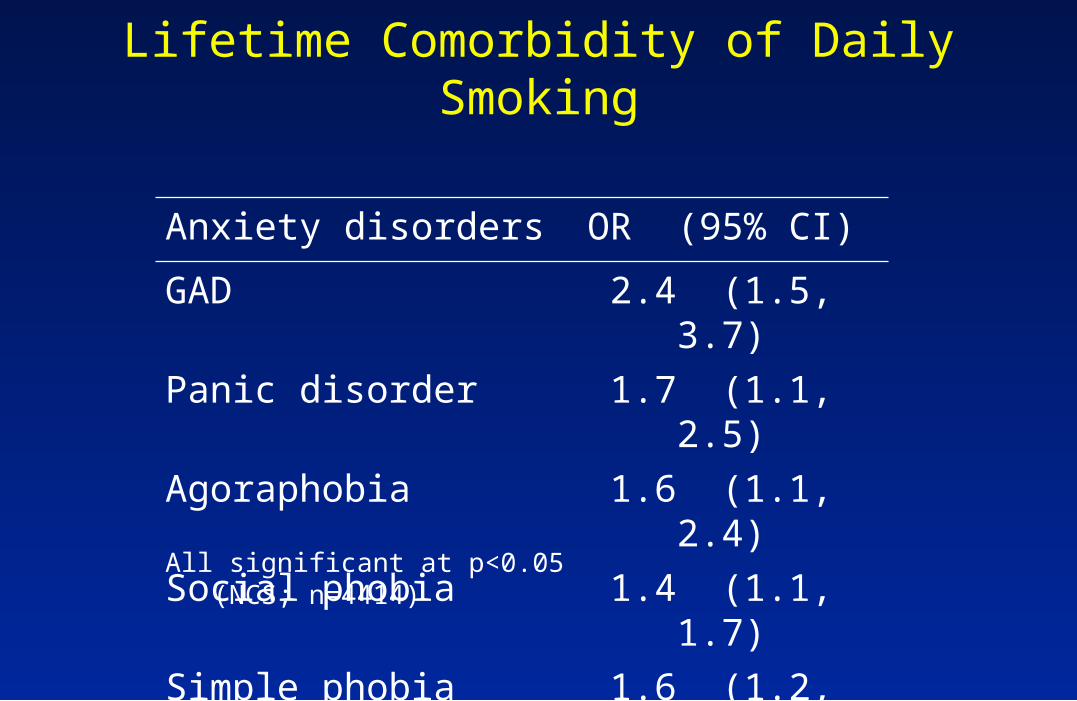
Lifetime Comorbidity of Daily Smoking
Anxiety disorders OR (95% CI)
GAD 2.4 (1.5, 3.7)
Panic disorder 1.7 (1.1, 2.5)
Agoraphobia 1.6 (1.1, 2.4)
Social phobia 1.4 (1.1, 1.7)
Simple phobia 1.6 (1.2, 2.0)
All significant at p<0.05 (NCS; n=4414)

Lifetime Comorbidity of Daily Smoking
Affective disorders OR (95% CI)
Depression 1.7 (1.3, 2.2)
Dysthymia 1.7 (1.2, 2.4)
All significant at p<0.05 (NCS; n=4414)
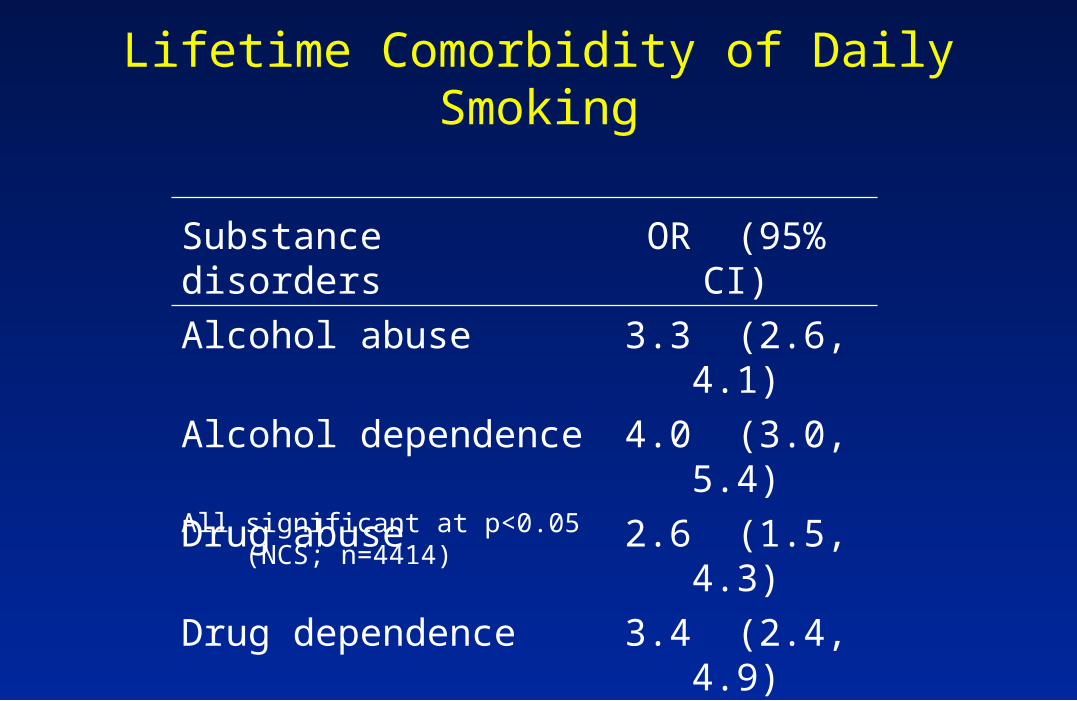
Lifetime Comorbidity of Daily Smoking
All significant at p<0.05 (NCS; n=4414)
Substance disorders OR (95% CI)
Alcohol abuse 3.3 (2.6, 4.1)
Alcohol dependence 4.0 (3.0, 5.4)
Drug abuse 2.6 (1.5, 4.3)
Drug dependence 3.4 (2.4, 4.9)
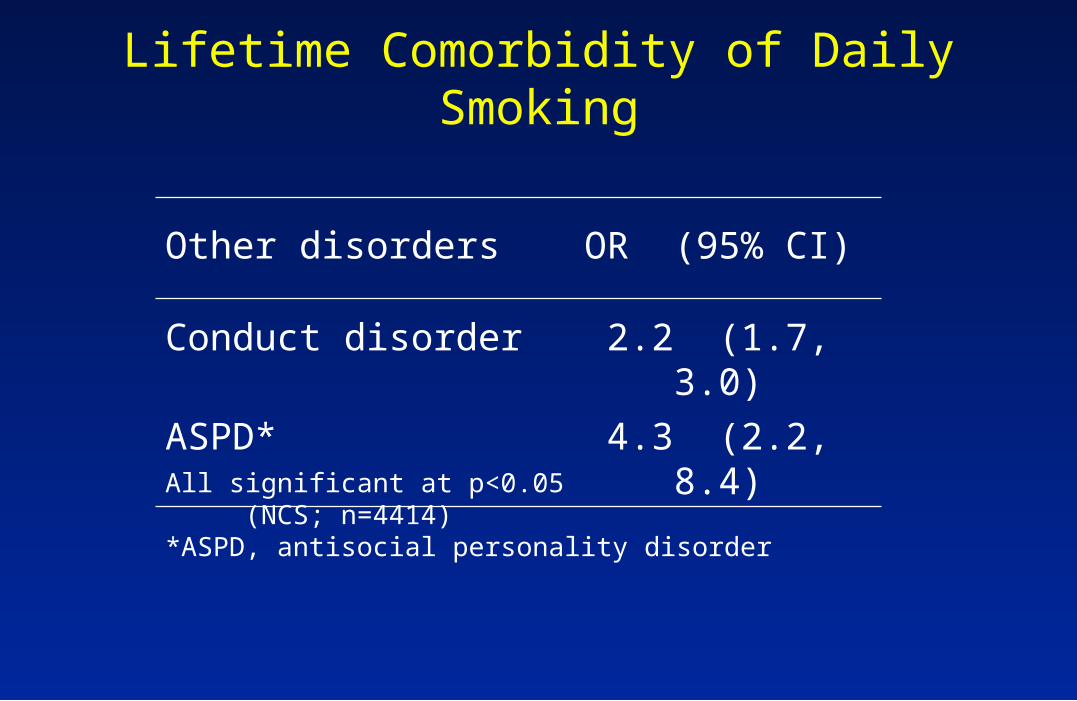
Lifetime Comorbidity of Daily Smoking
Other disorders OR (95% CI)
Conduct disorder 2.2 (1.7, 3.0)
ASPD* 4.3 (2.2, 8.4)
All significant at p<0.05 (NCS; n=4414)*ASPD, antisocial personality disorder
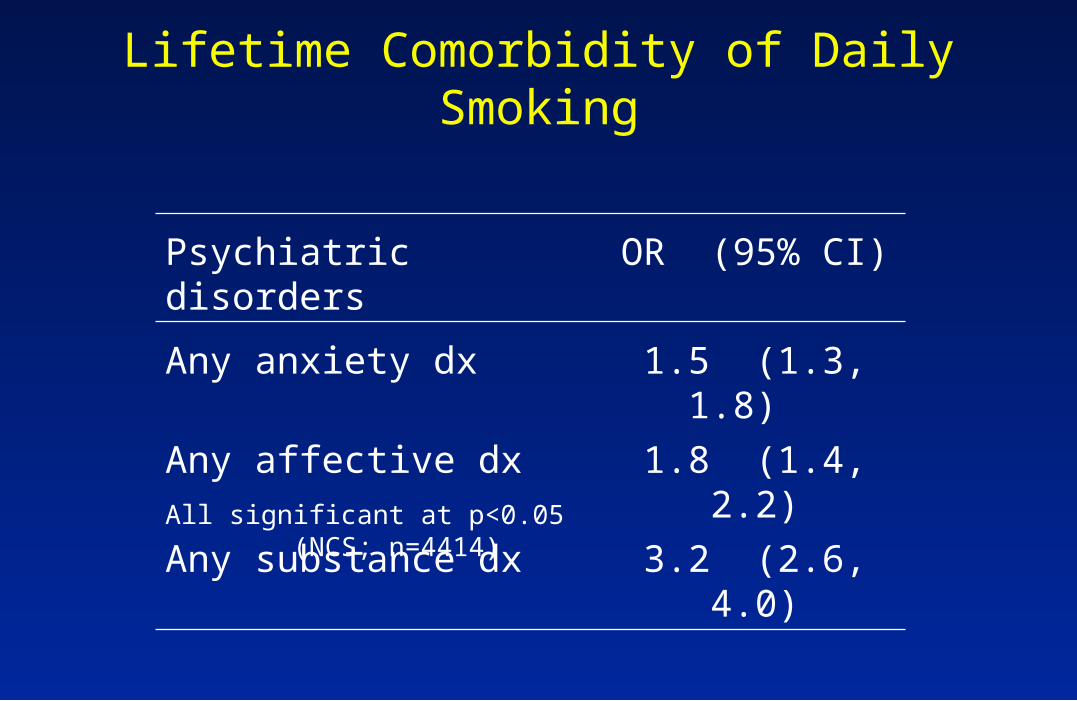
Lifetime Comorbidity of Daily Smoking
Psychiatric disorders OR (95% CI)
Any anxiety dx 1.5 (1.3, 1.8)
Any affective dx 1.8 (1.4, 2.2)
Any substance dx 3.2 (2.6, 4.0)
All significant at p<0.05 (NCS; n=4414)
Although depression and anxiety
predominate in females, the strength of
the associations with smoking is similar in
both sexes.
Conversely, although substance use disorders
are more prevalent in males than females, the
strength of the associations with smoking varies
little between the sexes.
The associations of psychiatric disorders
with tobacco dependence are stronger than
with non-dependent smoking.
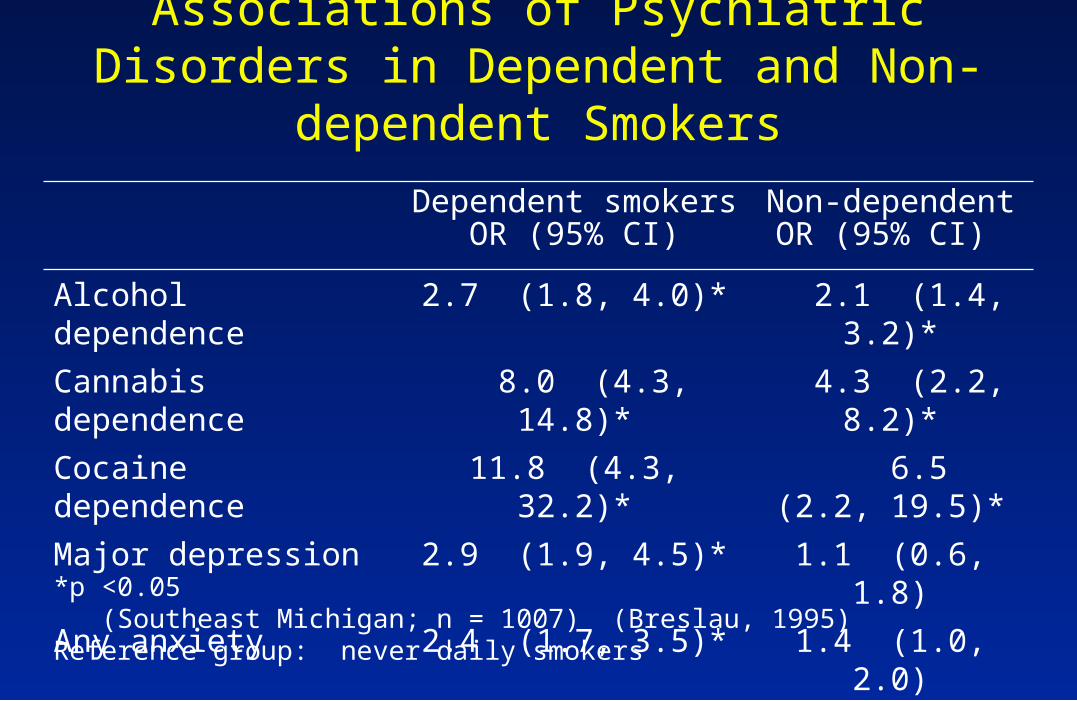
Dependent smokersOR (95% CI)
Non-dependent OR (95% CI)
Alcohol dependence 2.7 (1.8, 4.0)* 2.1 (1.4, 3.2)*
Cannabis dependence 8.0 (4.3, 14.8)* 4.3 (2.2, 8.2)*
Cocaine dependence 11.8 (4.3, 32.2)* 6.5 (2.2, 19.5)*
Major depression 2.9 (1.9, 4.5)* 1.1 (0.6, 1.8)
Any anxiety 2.4 (1.7, 3.5)* 1.4 (1.0, 2.0)
Associations of Psychiatric Disorders in Dependent and Non-dependent Smokers
*p <0.05 (Southeast Michigan; n = 1007) (Breslau, 1995)Reference group: never daily smokers

Potential Explanations for Smoking-Mental Illness Association
1. Mental illness as ‘cause’ of smoking.
2. Smoking as ‘cause’ of mental illness.
3. Common predispositions to both smoking and mental illness.
1. Mental illness as ‘cause’ of smoking
a. Mental illness smoking initiation
b. Mental illness progression to regular
smoking and dependence
c. Mental illness reduced capacity to quit
These three hypotheses are subsumed under the notion of “self medication.”
Accordingly, smoking begins as a successful attempt to relieve painful feelings.

Vulnerable persons find the effects of nicotine
powerfully reinforcing; this occurs before they
develop physiologic dependence;dependent
smokers smoke to avoid withdrawal.
2. Smoking as cause of mental illness
a. Nicotine & other pharmacologic smoking substances effect on brain
b. Smoking lung function (panic dx)

3. Correlated liabilities for both smoking & disorder
a. Low self esteem
b. Associating with peers who smoke and have behavior problems
c. Shared genetic predisposition (e.g. for impulsivity)

Causality in observational studies?
Temporal order between a
postulated cause and an outcome.
(A necessary condition)
Evidence that a postulated “cause”
(e.g. smoking) does not predict subsequent
“outcome” (e.g. depression) can be used to
rule out a causal explanation.

However, evidence that the postulated
“cause” predicts increased risk for
subsequent onset of outcome is often
equivocal.
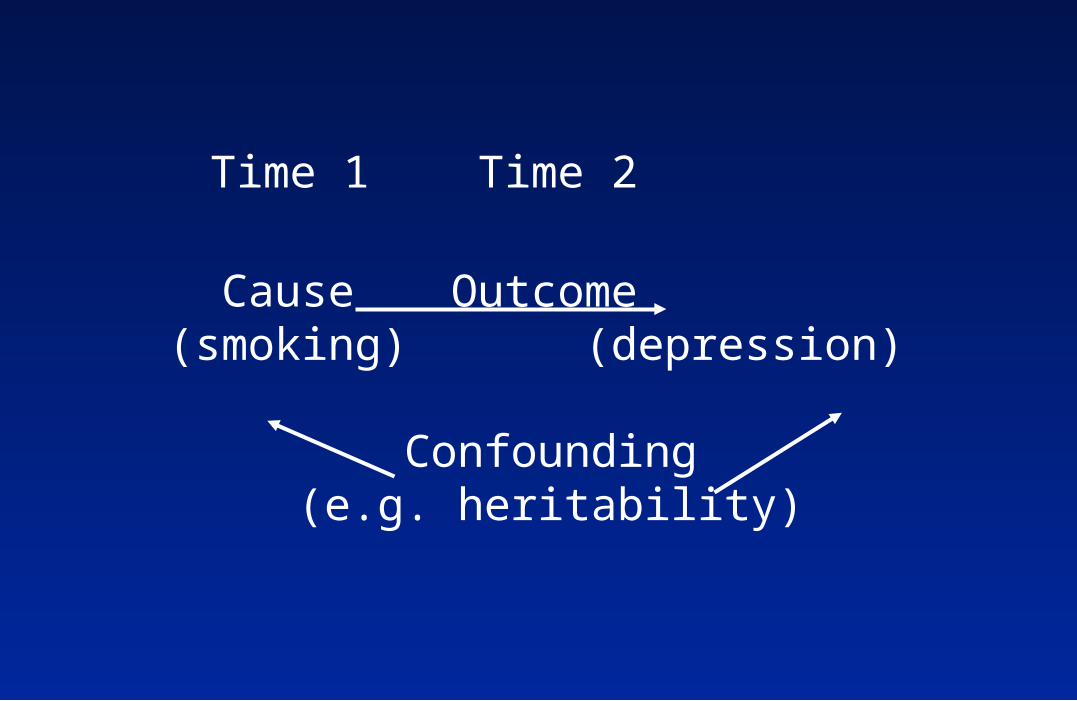
Time 1 Time 2
Cause Outcome (smoking) (depression)
Confounding(e.g. heritability)

Preexisting Disorders & Risk for Daily Smoking, Nicotine Dependence, & Persistence (vs. quitting):
Odds Ratios
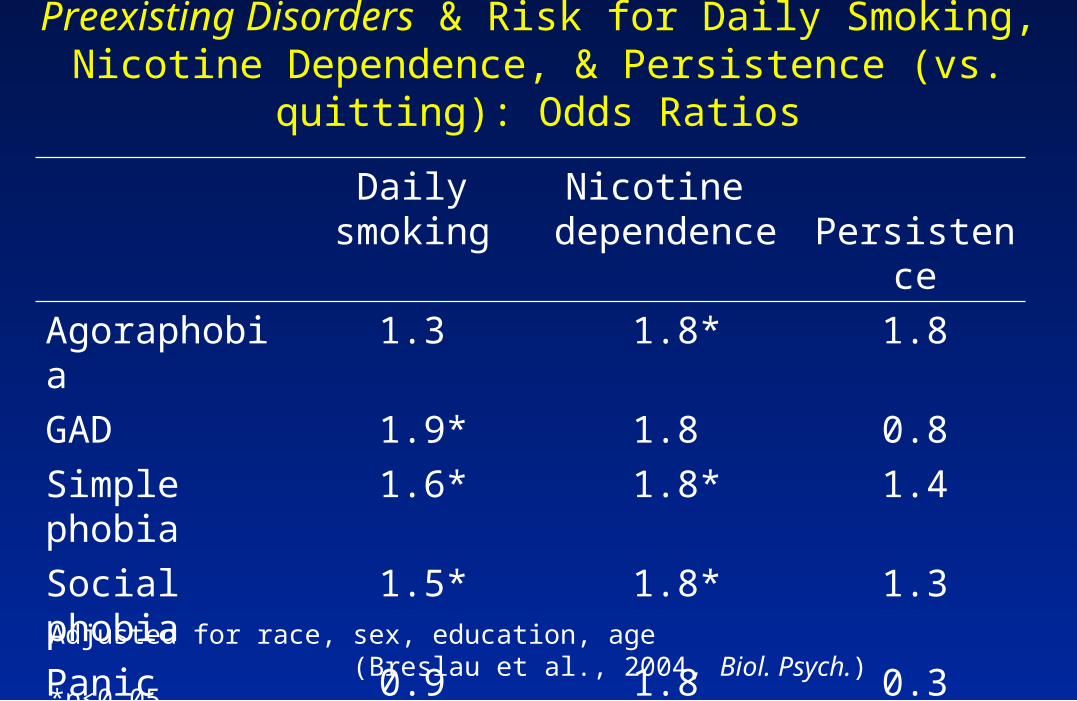
Adjusted for race, sex, education, age (Breslau et al., 2004, Biol. Psych.)*p<0.05 (NCS; n = 4414)
Daily smoking
Nicotinedependence Persistence
Major depression 1.5* 2.0* 0.8
Dysthymia 1.6* 0.9 0.5
Adjusted for race, sex, education, age (Breslau et al., 2004, Biol. Psych.)*p<0.05 (NCS; n = 4414)
Preexisting Disorders & Risk for Daily Smoking, Nicotine Dependence, & Persistence (vs. quitting):
Odds Ratios
Daily smoking
Nicotine dependence Persistence
Agoraphobia 1.3 1.8* 1.8
GAD 1.9* 1.8 0.8
Simple phobia 1.6* 1.8* 1.4
Social phobia 1.5* 1.8* 1.3
Panic disorder 0.9 1.8 0.3
PTSD 2.1* 1.7* 0.9

Preexisting Disorders & Risk for Daily Smoking, Nicotine Dependence, & Persistence (vs. quitting):
Odds Ratios
Adjusted for race, sex, education, age (Breslau et al., 2004, Biol. Psych.)*p<0.05 (NCS; n = 4414)
Daily smoking
Nicotinedependence Persistence
Alcohol A/D 1.4* 1.8* 0.7
Drug A/D 1.6* 1.7* 0.9

The role of psychiatric disorders varied
across stages of smoking; it played a role
in onset of daily smoking and progression
to dependence, but not in quitting.
Active vs. Past (remitted) Disorders
The majority of preexisting disorders, when active, predicted the subsequent onset of daily smoking and smokers’ progression to dependence.
In contrast, remitted disorders did not predict subsequent smoking.

Does smoking increase the risk for
subsequent onset of specific psychiatric
disorders?
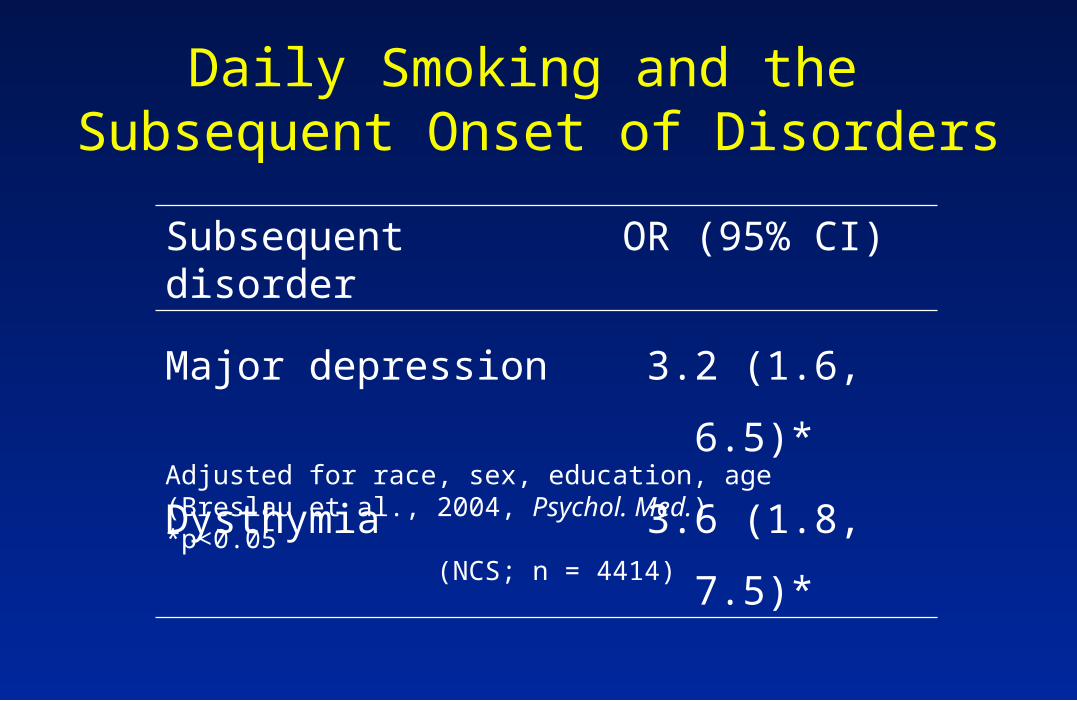
Daily Smoking and the Subsequent Onset of Disorders
Subsequent disorder OR (95% CI)
Major depression 3.2 (1.6, 6.5)*
Dysthymia 3.6 (1.8, 7.5)*
Adjusted for race, sex, education, age (Breslau et al., 2004, Psychol. Med.)*p<0.05 (NCS; n = 4414)
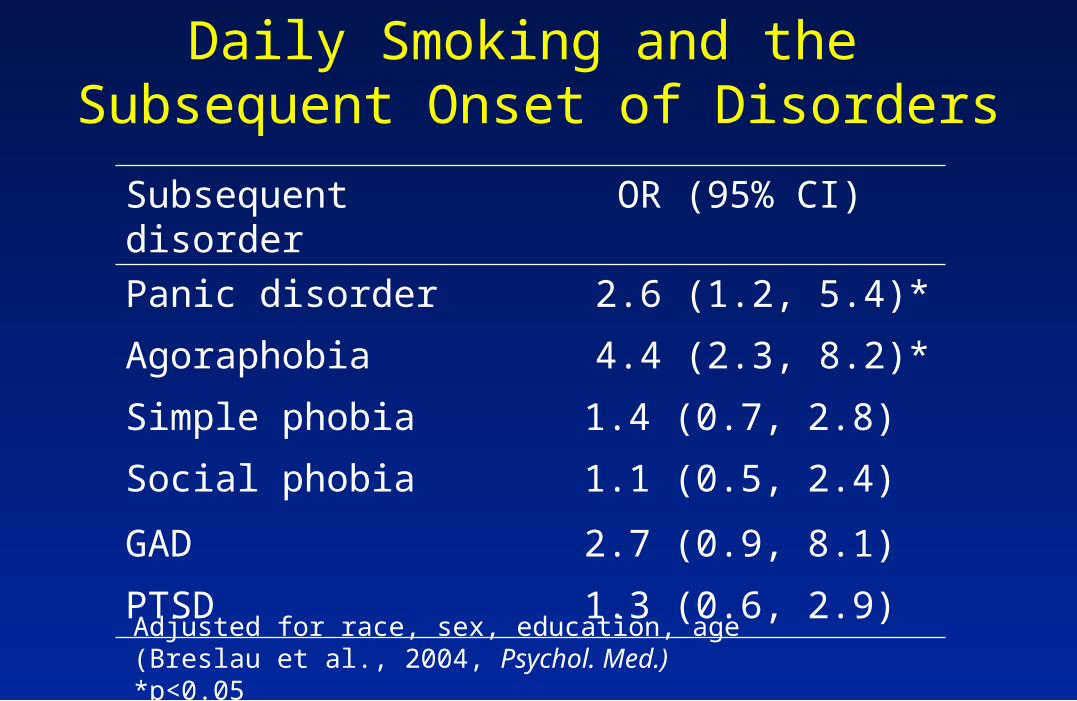
Daily Smoking and the Subsequent Onset of Disorders
Subsequent disorder OR (95% CI)
Panic disorder 2.6 (1.2, 5.4)*
Agoraphobia 4.4 (2.3, 8.2)*
Simple phobia 1.4 (0.7, 2.8)
Social phobia 1.1 (0.5, 2.4)
GAD 2.7 (0.9, 8.1)
PTSD 1.3 (0.6, 2.9)
Adjusted for race, sex, education, age (Breslau et al., 2004, Psychol. Med.)*p<0.05 (NCS; n = 4414)
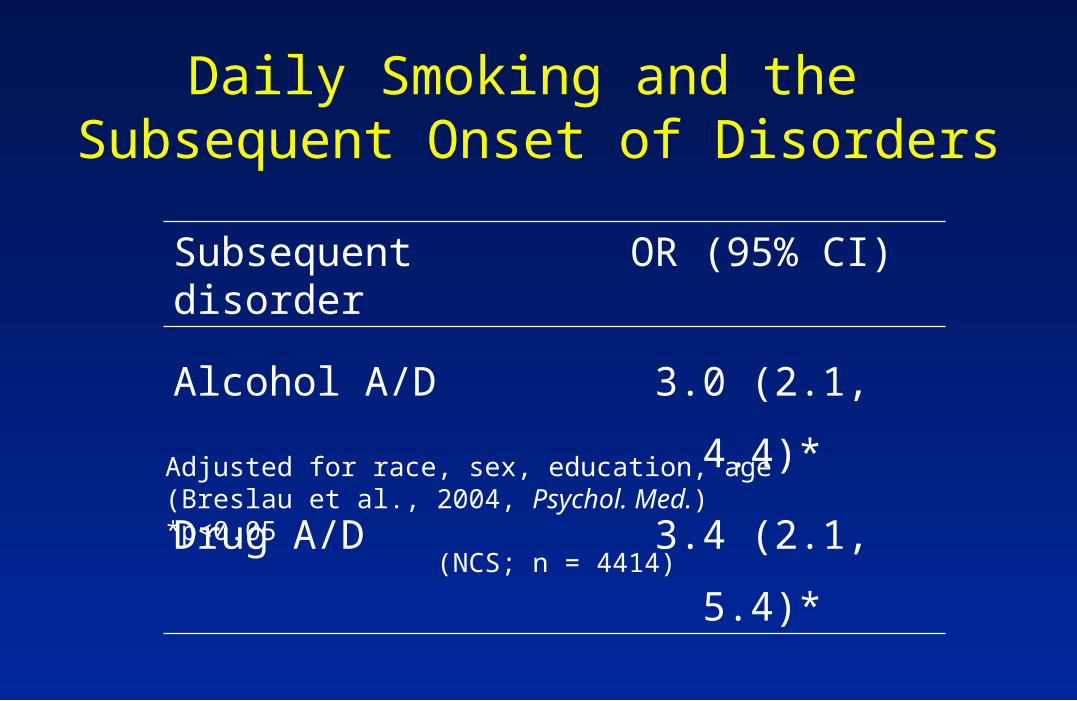
Daily Smoking and the Subsequent Onset of Disorders
Subsequent disorder OR (95% CI)
Alcohol A/D 3.0 (2.1, 4.4)*
Drug A/D 3.4 (2.1, 5.4)*Adjusted for race, sex, education, age (Breslau et al., 2004, Psychol. Med.)*p<0.05 (NCS; n = 4414)
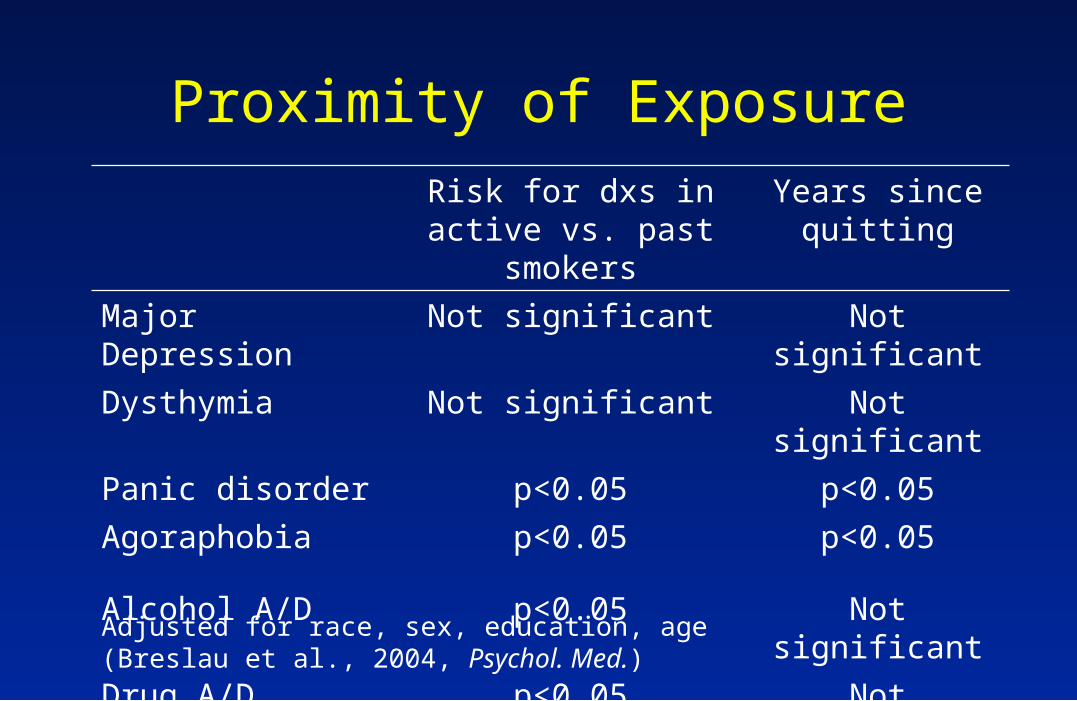
Risk for dxs in active vs. past smokers
Years sincequitting
Major Depression Not significant Not significant
Dysthymia Not significant Not significant
Panic disorder p<0.05 p<0.05
Agoraphobia p<0.05 p<0.05
Alcohol A/D p<0.05 Not significant
Drug A/D p<0.05 Not significant
Adjusted for race, sex, education, age (Breslau et al., 2004, Psychol. Med.) (NCS; n = 4414)
Proximity of Exposure

Treatment of smoking is unlikely to reduce onset of depression: past smokers
do not differ from active smokers.
Smoking is unlikely to cause depression.
Depression and smoking are likely to be linked by common predisposition (genetic
evidence).
Smoking and Depression
Smoking and Panic Disorder
Evidence of risk only in one direction (smoking panic disorder)
Active smoking, but not past smoking, increases risk.
In past smokers, there is a decreased risk for panic onset with passage of time since quitting.
Active smoking may be a marker
for other substance use disorders.
These results are based on retrospective
data, using statistical methods that take into
account information on age of onset of
disorders and age of onset of smoking.
Evidence from prospective studies
of smaller samples (not national)
support these findings.
Summary
1. Little evidence for influence of depression on smoking initiation.
2. Support for progression to daily smoking/nicotine dependence.
3. No support for reduced quitting.
1. Increased risk in smokers.
2. Potential role for respiratory problems.
Depressionas cause
Panic dxas outcome
Summary
1. Smoking and/or alcohol precede(s) use of illicit drugs.
2. The smoking-illicit drug sequence is more common in females.
Smoking, alcohol & illicit drugs




![PTSD in the Elderly2013 [Read-Only] - LeadingAge …...Services, 1995) November 14, 2013 Irit Felsen, PhD 17 PTSD Comorbidity • PTSD strongly comorbid with other disorders (Breslau,](https://img.pdfslide.us/doc/110x75/5e926181caad0a580f71cda0/ptsd-in-the-elderly2013-read-only-leadingage-services-1995-november-14.jpg)








![Introduction to Comorbidity Auto Saved]](https://img.pdfslide.us/doc/110x75/577d33b31a28ab3a6b8b7d51/introduction-to-comorbidity-auto-saved.jpg)













