Embed Size (px)
Citation preview
83
* PSP Discussion Paper Series
19705November 1995
Poverty Assessment in GhanaUsing Qualitative and Participatory Research
Methods
Andy Norton
Ellen Bortei-Doku Aryeetey
David Korboe
D.K. Tony Dogbe
November 1995
Poverty and Social Policy DepartmentHuman Capital Development and Operations Policy
The World Bank
Pub
lic D
iscl
osur
e A
utho
rized
Pub
lic D
iscl
osur
e A
utho
rized
Pub
lic D
iscl
osur
e A
utho
rized
Pub
lic D
iscl
osur
e A
utho
rized

Abstracts
This Booklet of Abstracts contains short summaries of recent PSP Discussion Papers; copies of specific papersmay be requested from Patricia G. Sanchez via All-in-One. The views expressed in the papers are those of theauthors and do not necessarily represent the official policy of the Bank. Rather, the papers reflect work inprogress. They are intended to make lessons emerging from the current work program available to operationalstaff quickly and easily, as well as to stimulate discussion and comment. They also serve as the building blocksfor subsequent policy and best practice papers.
Preface
This paper is one of a series undertaken as part of the Extended Poverty Study in Ghana. Asynthesis of this work is available in Ghana: Poverty Past, Present and Future (Report No.140504-GH. Population and Human Resources Division, West Central Africa Department, WorldBank, Washington D.C., June 29, 1995). Four of the background papers are appearing in thePoverty and Social Policy Discussion Paper Series:
Harold Coulombe and Andrew McKay, 'An Assessment of Trends in Poverty inGhana, 1988-92.' Poverty and Social Policy Discussion Paper No. 81, WorldBank, Washington D.C. (November 1995)
Lionel Demery, Shiyan Chao, Rene Bernier and Kalpana Mehra, 'The Incidence ofSocial Spending in Ghana.' Poverty and Social Policy Discussion Paper No. 82,World Bank, Washington D.C. (November 1995)
Andy Norton, David Korboe, Ellen Bortei-Dorku and D.K. Tony Dogbe, 'PovertyAssessment in Ghana using Qualitative and Participatory Research Methods.'Poverty and Social Policy Discussion Paper No. 83, World Bank, WashingtonD.C. (November 1995)
Christine Jones and Ye Xiao, 'Accounting for the Reduction in Rural Poverty inGhana, 1988-1992.' Poverty and Social Policy Discussion Paper No. 84, WorldBank, Washington D.C. (November 1995)
The papers draw upon the work of many. The contributions of the Ghana Statistical Service,Ministry of Health, and Ministry of Education in the Government of Ghana, and of UNICEF andthe Canadian Intemational Development Agency (CIDA), are gratefully acknowledged. The viewsexpressed are those of the authors. They should not be attributed to the World Bank, its Board ofDirectors, its management or any of its member countries.

Acknowledgments
This overview report has been compiled by Andrew Norton, drawing heavily on inputsfrom the other authors. Fieldwork for this study has been carried out over three phases, withinputs of support from ODA (field costs phase I & 2) GTZ (support to costs of training, phase1) and UNICEF (support to phase 3).
Acknowledgments are due to: the field teams (members listed below) for theirenthusiasm and commitment; the two Task Managers who have been involved in the ExtendedPoverty Study for the World Bank, Lionel Demery and Tom Stephens, for their firm support;the administrative and logistical staff of CEDEP (the NGO who coordinated the study) for theirefficiency and hard work; and above all the members of poor rural and urban communities whogave their time to share their analyses of poverty with us.
Team members:
Phase 1.
Research Supervisor - Dr. Andrew NortonLead Researcher- Dr. Ellen Bortei-Doku AryeeteyTeam Leaders - Dr. Felix Fiadjoe
- Mr. Dan Inkoom- M. Wim Alberts
Members - Mrs.Margaret Doku- Ms. Margaret Assan- Ms. Judith Thompson- Mr. Samuel Dodoo- Mr. Martin Dery- Mr. Dominic B. Kanyoke- Mr. Thomas Kuby- Mr. D.K. (Tony) Dogbe- Mr. Ben Arthur
Administrative Officer Mrs. Salome AhenkoraResearch Manager - Mr. D.K. (Tony) Dogbe
Phase 2Research Supervisor - Dr. Andrew NortonLead Researcher - Dr. Ellen Bortei-Doku AryeeteyTeam Leaders - Mr. Wim Alberts
- Mr. D.K. (Tony) DogbeMembers - Dr. Felix Fiadjoe
- Rev. Fr. Anyomi- Mr. Robert Kuwornu- Mr. Robert Agarku- Mrs. Salome Ahenkora- Mr. Charles Owusu- Mr. Dan Amuah- Mr. Martin Dery- Mr. Samuel Dodoo- Mr. Dominic B. Kanyoke- Mr. Paa Kwesi Afari
Administrative Officer Ms. Celia MarshallResearch Manager - Mr. D.K. (Tony) Dogbe
Travelling Secretariat - - Mr. Kwaku Ahenkora- Mr. Kwame Apiagyei
Phase 3Research Supervisors - Mr D.K. Tony Dogbe
- Dr Andrew NortonLead Researcher - Dr David KorboeTeam Leaders - Mr. Kweku Ahenkora
- Mr. D.K. Tony Dogbe- Dr. David Korboe
Members - Mr. Dela Afenyadu- Ms. Vida Affum- Mrs.Doris Amoyaw- Ms. Mercy Anim- Ms. Theresa Baffoe- Mr. Robert de Graft Agyarko- Mr. Samuel Duodu- Mr. Dominic Kanyoke- Mr. Kwaine Manhyia- Mr. Kojo Mbir- Mr. Kojo Mensah-Abrampa- Mr. Kwame Opoku- Ms. Dora Owusu- Ms. Petrina Owusu Yeboah
Administrative Officer - Mrs Salome Ahenkora
* Abstract
The Ghana Participatory Poverty Assessment was conducted over three phases in fifteencommunities by mixed teams of academic researchers, government staff and personnel of NGOs.Key findings on the local experience of poverty included the following: the main elements indefining the poorest members of communities were disability, age combined with the lack of adultchildren, widowhood and childlessness; the incidence and depth of poverty is greatest in the ruralnorth; assets at the community level (such as access to water for domestic and productive use,access to services and natural resources) are seen as more important to rural communities thanurban; gender dimensions are critical to understanding poverty - this emerged primarily through thefinding that there are substantial elements of separation to men's and women's livelihood in muchof urban and rural Ghana.
The concept of vulnerability captures many dimension of the experience of deprivation inrural Ghana. Seasonal vulnerability is particularly strong in the rural north (especially the UpperRegions), manifested in chronic food insecurity often affecting whole communities. Views oflong-term trends in rural communities focused on environmental issues such as declining accessand quality of water, declining soil fertility and declining common property resources for thevulnerable to fall back on in times of crisis. Key long-term trends identified by the urban poorrelated to the evolution of policy frameworks in the era of adjustment. While a considerableimprovement is seen as having occurred in the early phase of economic reform (1983 to 1988)there is a general perception that opportunities for the urban poor have been becoming moreconstrained in the last six to seven years.
The investigation of the conmunities' own assessment of their priority needs was aconsistent theme in the research. The strongest elements emerging from the priority rankings in therural north were food security, water (both for domestic and productive use), access to health care,and education. The picture that emerged from priority rankings in the rural south was morediverse. Again, access to curative healthcare emerged as a strong and consistent priority, whileimprovements in transport infrastructure (roads and bridges) was also a strong theme - reflectingproblems in accessing both markets and services. Other common themes included access to credit,off-farm employment and water for domestic use. The most consistent concerns in priorityrankings in urban communities were with inadequate employment opportunities and the supply ofsmall-enterprise credit. The condition of the urban infrastructure was also a major issue - withsupply of water again a strong theme.
Investigation of the barriers the poor face in accessing healthcare services highlighted thefollowing issues: cost barriers are a major issue in accessing formal healthcare, both in terms ofoverall cost and the lack of flexibility in rescheduling treatments. Furthermore, provisions forexempting the poor from user charges are not working. In education, the major concern of mostcommunity members and teachers canvassed was with issues of quality rather than of basic access.Major concerns included: poor quality of teaching and facilities; lack of supervision of teachers;lack of clear feedback to parents on childrens' performance; the policy of retrenchment ofuntrained teachers leading to shortages of teachers in isolated rural communities.

CONTENTS
Executive Summary and Key Policy Findings
1. Introduction
1.1 Background of the Study1.2 Methodology1.3 Field Sites
2. Main Findings
2.1 Local Conceptions of Poverty2.2 Priorities of the Poor in Poverty Reduction2.2.1 Strategies for Moving out of Poverty2.3 Vulnerability: Dynamic Dimensions of Poverty2.3.1 Seasonal Dimensions of Poverty2.3.2 Long-Term Trends in Poverty2.4 Survival Strategies and 'Safety Nets'2.4.1 Survival and Coping Strategies2.4.2 Formal and Informal Safety Nets2.5 Perceptions of Service Quality and Access in the Health Sector2.6 Perceptions of Service Quality and Access in the Education Sector2.6.1 Access and Utilization2.6.2 Local Views of Education Quality2.6.3 Perceived Relevance of Education2.7 Domestic Water and Sanitation

Executive Summary and Key Policy Messages
The Ghana Participatory Poverty Assessment was conducted over three phases, and atotal of fifteen communities were involved, selected to give a representative picture ofthe living conditions of the poor in Ghana. In particular, care was taken to representadequately the rural and urban dimensions of poverty, as well as the different regions,major livelihood groups and agro-ecological zones in the country. The overallobjective of the study was to contribute to social policy formulation in Ghana throughexpanding understanding of the processes that produce and reproduce poverty indifferent environments and among different social groups. Special emphasis was givenin the third phase of the study to understanding the poor's experience andunderstanding of the constraints they face in terms of access and quality of delivery ofkey social services. The main conclusions of the study are as follows.
T'he experience and understanding of poven'y
The nature of poverty in Ghana. In all communities the local experience andunderstanding of poverty and vulnerability was examined. In broad terms ourconclusions support those of the quantitative analysis of the GLSS within the ExtendedPoverty Study by emphasizing that the incidence and depth of poverty is greatest in therural north. This emerged through both the extent to which poverty was judged to beprevalent throughout the whole of communities (even in local terms) and the criteriawhich were used to define that poverty. In the rural north the predominant feature ofpoverty was a general crisis of livelihoods in terms of the lack of remotely adequatebasic foodstuffs to feed the household for all or part of the year. A summary of thelocal conceptions of poverty and vulnerability leads to the following key messages:
In all sites there were consistent elements in defining 'the poorest of the poor',which focused on the intersection of a variety of conditions which lead tohouseholds which have no labor resources, and individuals who have no controlover labor resources of any kind. The key elements were disability, age combinedwith the lack of adult children, widowhood and childlessness. Female householdheadship was more likely to appear as an indicator of poverty in the rural north thanthe rural south or urban contexts. While female headship as such is not related in asimple sense to poverty the combination for women of age, widowhood and lack ofadult children was frequently seen as associated with chronic vulnerability.
* Assets at the community level were seen as more important to rural communitiesthan urban - these included access to water for domestic and productive use, accessto public services, access to an abundant natural resource base in terms of fertilefarmland and common property resources, and access to transport infrastructure,markets and extension services.
i
* The view of poverty as being a dynamic condition impacting on entire communitieswas particularly strong in the northern rural areas, vulnerable to drought and to the'hungry season' prior to the single main annual harvest of bulk foodstuffs. Thematerial collected supports the view that the experience of depth of poverty andvulnerability in the rural north is greater than in other areas through the fact thataccess to food predominates in local views of poverty, and that in somecommunities serious food insecurity prevails for at least part of the year forvirtually every community member. Nonetheless the material is suggestive of somevariation - with highly populated areas in the Upper East (Bawku and BongoDistricts) suffering the worst conditions.
* In urban areas poverty tends to be seen more as an individual condition - with keyelements in defining well-being including access to stable employment, the abilityto acquire marketable skills and access to seed capital (as well as the fundamentalasset of physical health and strength).
* As well as physical assets (livestock, capital etc.) and human assets (health, skills)an individual's social network, and membership of social institutions forms a keydimension of well-being and livelihood security. Access to land often comesthrough community membership rather than the market, and the accessibility of asupportive kin network is critical at times of personal crisis (urgent need for moneyto pay hospital bills, etc.).
* Gender dimensions emerged primarily through stressing the fact that there aresubstantial elements of separation to men's and women's livelihoods in manysections of the rural and urban poor in Ghana. In ranking exercises in rural areasthere was a tendency for men to rank men and women to rank women, rather thanseeing households as unified entities. Men and women thus also stressed differentelements to the experience of poverty in some communities.
The results of the priority rankings. The issue of the communities' own assessment oftheir priority needs was a consistent theme in our research. Where possible these viewswere solicited through focus groups which reflected the diversity of the communitiesunder study in terms, at least, of gender and generational issues. The major findingscan be grouped into three broad regional 'blocks': the rural north (the Upper Regionsand the Northern Region), the rural south (including the transition zone, forest zoneand the coastal savannah - for our purposes communities in Brong Ahafo, Volta,Western and Central Regions) and urban communities (including intermediate ruraltowns in the Volta and Central Regions, and communities within the major urbancenters of Accra, Tamale and Techiman).
Priority rankings in the rural north. The strongest themes emerging from the priorityranking exercises in the rural north are food security, water (both for productive anddomestic use), access to health care, and education. A particular nexus of conditions
ii
affects extremely resource-poor communities in the Upper Regions (especially verydensely populated areas such as Bongo and Bawku) which finds expression in theconstant emphasis on the provision of dry-season water for productive as well asdomestic purposes. In essence rainfed agriculture of a traditional kind has become sounproductive that the provision of a dry-season income is now essential to anythingapproaching a viable level of livelihoods. Dry season water supply, through wells anddams, provides for vegetable gardening which can be a highly significant support toincomes, and for pasturing animals in the vicinity of the village so that manureresources - invaluable for farming land depleted by decades of continual farmingwithout fallow - can be utilized to a far greater extent than is possible if animals haveto move to a distant dry-season transhumance site. Emphasis on domestic water supplyis also strong in communities that have not benefited from external programs such asthe CIDA and NORRIP community water projects. The other consistent emphasis is onhealthcare provision - reflecting both poor conditions in terms of access, and the valueof physical health and strength which is a consistent theme in the local views of povertyreflected from all areas.
Priority rankings in the rural south. The picture emerging from priority rankings inthe rural south is more diverse - reflecting the greater diversity in terms of livelihoodsystems and environment in this zone, as well as the tendency towards greater socialstratification, and therefore intra-community diversity. In some communities, such asButre in Western Region, food security was not a major concern even for the poor -although this was not true of all the sites (food supply was very insecure for the poorercommunity members in Afrangua, in Central Region). Again access to curativehealthcare emerged as a strong and consistent theme - in only one community was thisnot listed as a priority need. Improvements in transport infrastructure (roads andbridges) emerged as a major priority in three of the five southern rural communities.This reflects to some extent the ecological conditions of much of southern Ghana,where heavier and more persistent rainfall can in extreme cases lead to communitiesbecoming totally isolated for periods of the year. In addition to denying access toservices, poor quality access roads are frequently seen as impacting negatively on theeconomic opportunities available. Difficulties of road access are a major disadvantagein relation to highly perishable products such as tomatoes. Access to water for domesticuse again emerged as a major theme, especially in the village of Butre in WesternRegion. In communities where water did not feature as a priority in ranking exercisesthis could often be traced to an intervention by an outside agency.
Other common themes included access to off-farm employment and credit for farming(predominantly men) and trading activities (predominantly women). Better sanitationand drainage emerged as themes in three of the five communities. In general theemphasis on education was lower than in the north - though in large measure this isprobably because the situation in terms of provision was better (all of thesecommunities had at least one primary school, and two - Derma and Dekpor Horme,also had Junior Secondary Schools). For those communities which did not have Junior
iii
Secondary Schools, the distances to travel to such facilities were usually less than in thenorth.
Priority rankings in the urban communities. In the six urban communitiesdifferentiation in perceived needs was marked - even in some cases between differentsections of the town which experienced different kinds of problems in relation to urbanservices. The most consistent concerns, reflecting the nature of urban livelihoods werewith inadequate employment opportunities and the supply of small-enterprise credit.Although these elements were very consistently scored they were rarely the firstpriority. An exception was Sekondi - which has seen the almost total disappearance ofa once-active labor-market associated with the port and associated services. Priorityrankings seemed to reflect to a large degree the condition of the local urbaninfrastructure. In particular it was interesting to note that three of our five communitieshad major problems of supply of potable water. Other issues of urban infrastructurethat received emphasis in some communities were sanitation (especially in theTechiman Zongo where facilities were almost non-existent) and urban roads. The latterwas only mentioned once, but in an interesting context. East Maamobi has had accessroads since 1987 (provided under the World Bank Urban 1 Project). The Maamobifield team stressed that this is usually one of the first things that the participantsmentioned in terms of new senrices that have come into the area. The roads are said tohave brought much improvement to the area for diverse reasons. These included greatlyimproved physical security making journeys at night (a particularly important benefitfor women) and ease of access to health facilities.
Strategies for moving out of poverty. There was no uniform perception of howindividuals might move out of a condition of poverty. In urban areas there waswidespread despondency about the future. Informants noted that recruitment tounskilled wage-labor in government service had virtually dried up with structuraladjustment policies - and unskilled wage-labor was disliked for the reasons outlinedabove. Therefore increasingly well-being is seen as tied to the capacity to acquire skillswhich can be used in a self-employed context (predominantly within the informalsector). This is said to be leading to increased competition for apprenticeship positions,and thereby increasing costs to individuals of gaining access to such training. In ruralareas where there are substantial opportunities in terms of cash crop production (muchof southern Ghana) access to capital for farming enterprises is continually raised as themost significant 'blockage' to individual progress. In the poorer communities ofnorthern Ghana, the constraints at the level of the Region or community are continuallyraised as more significant than those at the level of the household or individual. Theindividual strategy most commonly used to cope with, or move out of, poverty is labormigration. The paradox here is that in migrating substantial numbers of residents ofpoor communities end up by severing their ties with the sender community, thuseventually ending transfers to ltheir kin group. In northern Ghana the accumulation oflivestock was often seen as an important strategy for moving out of poverty. Apartfrom the inherent productive value of livestock rearing, the manure provided for the
iv
farm is critical to households' farm production (especially under conditions of landscarcity).
Rural communities saw far more opportunities for action at the level of the communityto increase livelihood security than their counterparts in the urban sector. In urbancommunities only the occupational associations to which many in the informal sectorbelong were mentioned in this context. Although local leaderships exist in urban areasthey seem to be commonly viewed as distant from the concerns of the poor. Ruralcommunities showed considerable enthusiasm for mobilization to support the provisionof social and economic infrastructure, taking the form of assistance with constructionand maintenance of facilities such as schools and clinics, as well as more unusualinitiatives such as a desire to establish a grain bank in a food-insecure community in theUpper East Region. It is notable that, although northern communities had much thesame analysis of the importance of social infrastructure their ability to provide cash tosupport such construction projects was very highly constrained - while contributions interms of labor could be mobilized at the same level as the south. Service provisionsystems that rely to a substantial extent on the capacity of local communities to generatecash will thus lead to equity problems in terms of access.
The views of appropriate action to support poverty reduction initiatives which could betaken by government and NGOs reflected to a large degree the priorities listed above.In the rural south and in urban areas provision of improved employment opportunitieswas seen as a major priority for government action - although the sense of specificdetails of what actions this might involve were not clear. Similarly credit emerged as amajor concern both for farming and small-scale trading activities (the latter particularlyfor women). This is seen as an area for both government and NGO intervention.Improved access to water and quality of water supply were major issues in some of theurban communities, as was improved sanitation. To a greater degree than in ruralcommunities, urban communities tend to see domestic water and sanitation asappropriate areas for government intervention. In rural areas of the south there was astrong concern in some communities with the condition of the road infrastructure . Theimprovement of road infrastructure was generally seen as an area suitable forcollaboration between community level institutions (mobilizing labor and maintenancefunds) and outside agencies, particularly local government (provision of capital,equipment and possibly food-for-work incentives). Partnerships with governmentministries were seen as the appropriate means for increasing access to basic health andeducation services. There is still a tendency to see the community's role in terms ofcontributing labour (and sometimes materials) to the construction and maintenance ofphysical infrastructure. In the rural north the view of appropriate support from outsideagencies reflected the issues of water supply, food security and service deliveryoutlined above. In some cases there was a distinction between the kinds of assistancethat government and NGOs should best provide (with NGOs seen as having anadvantage generally where extensive capacity building support to local institutions isrequired, e.g. managing a cereal bank).
v
Vulnerability. Poor peoples' conceptions of poverty often correspond closely to thenotion of vulnerability - a dynamic notion which captures the sense of threat posed bythe negative effects of various forms of change over time, whether in the form ofseasonal variation, long-term trends, or various kinds of shock.
Seasonality and poverty. Seasonal fluctuations were a major aspect of well-being in allresearch sites. In addition to the well-documented phenomena of stress points in theagricultural cycle, which takes its most severe form in the 'hungry season' problems ofmany savannah communities, there are significant seasonal cycles in urban occupationsrelated to factors such as weather (impact on building), the cycle of social activity andkey festivals, and market flows related to the agricultural year. As has been notedabove the major seasonal foodi security issue in Ghana is the extreme 'hunger season'experienced by many communities in the north - especially those where intensepopulation pressure has led to declining soil fertility (for example, Komaka, Beo Tankoand Sombo in our sample). These communities experience major problems of basicfood supply even in a normal year - and the impact of drought years can be extreme.As a general rule, the more diverse the farming system, in terms of the mix of basicstaples and crops grown to generate income, the less was the degree of vulnerability toseasonal food scarcity. On top of that cassava, as a crop which can be available forharvesting all year round, often plays a special role in mitigating vulnerability.
Where there are marked seasonal changes such as in the north, seasonal patterns ofillness have been observed. Ill-health is said to be most prevalent at the peak of the dryseason in February and March, by which time the food situation has started to worsen.Fevers, stomach disorders and respiratory diseases were described as the most commonat this time. By experience the most dangerous time to fall sick is during the rainyseason when there is very limited food supply, and no money to go to the hospital. Itis also the time when people need their energy most to work on their farms. Worsestill, increased poverty during the lean season makes it difficult for the family torespond adequately when someone falls sick at this time. In the middle and coastal beltdouble maxima rainfall areas of communities such as Butre, Kpando Gabi, Derma andDekpor Horme, there is apparently little differentiation in the seasonal occurrence ofsickness. Cholera and diarrhoea seem to peak during the 'time of mangoes' in theminor rainy season, but other diseases occur all-year round.
Long-term trends. Views of trends in rural communities tend to focus onenvironmental issues such as declining access and quality of water, declining soilfertility and declining common property resources for the vulnerable to fall back on intimes of crisis. The view of the urban poor relates in more detail to the evolution ofpolicy frameworks in the era of adjustment. While a considerable improvement isappreciated to have occurred in the early phase of economic reform (from 1983 to1988) there is a general perception that opportunities for the urban poor have beenbecoming more constrained in the period since the last six to seven years. In part thisis attributed to increased 'crowding' of the informal sector due to both low levels ofdemand and increasing numbers of people trying to survive in this sector. The increase
vi
is variously attributed to retrenchees searching for new livelihoods and Ghanaiansreturning to the country from other parts of West Africa as a result, in part, ofimprovements in the general climate in Ghana, and varying kinds of problems affectingother countries (recession, conflict). In all communities there is some concern overwhat is perceived to be a very poor situation in relation to assistance with credit fortrading and productive activities. In the urban areas this is perceived as a decliningtrend whereas in some rural areas this seems to be perceived more as a continuation ofan unsatisfactory situation.
The list of aspects of decline in environmental conditions in rural areas included: wateraccess (declining levels of the water table, decreasing quantity, quality and duration ofstream flow); availability and quality (fertility) of farm land and pasture for animals;access to a range of products from common property areas, for both own consumptionand sale for income (including fuelwood, medicines, foraged foodstuffs such as snails,fruits, mushrooms, bushmeat, and other non-timber forest produce). In the northernsavannah communities the key elements of environmental change were perceived to bedeclining soil fertility due to decreasing fallow periods, declining water resources asoutlined above and a shortening of the rainy season, combined with less predictability.In the relatively more agriculturally abundant communities of the middle and coastal belt,important changes have taken place in crop mixes in response to environmental degradation,as well as market demands. The drought and accompanying bush-fires of 1983 were notedin many communities as a 'watershed' point following which there were long-term changesin the local ecology.
Another long-term trend which was highlighted in some areas was a tendency toweakening of the bonds of local social institutions of kinship and community. InNyingare in the Northern Region, for example, focus groups among women revealed aperception that ten years ago there was strong social cohesion in the village. Communallabor institutions were still strong (and acting as a safety net for householdsexperiencing problems in terms of labor due to sickness or disability), respect andauthority was still given to the chief and his elders, community solidarity was still expressedthrough mutual support and assistance for one another. Decline in the traditionalinstitutional framework for such reciprocal arrangements was a fear expressed in other sitesin the north associated with increasing levels of temporary and long-term labour migration.Such changes clearly create increased vulnerability for the poorer sections of suchcommunities, by weakening their 'social assets' in terms of networks of kinship andcommunity through which they could mobilise claims on food and labour from theirneighbours. In one urban site - which had been affected by the recent ethnic conflict in thenorth - fear was expressed that Ghana's evolving democratic system could also fomentsocial disintegration.
Survival and Coping Strategies. The coping strategies we recorded in the course of thethree phases were very diverse. Some of the more common elements included:
vii
* For the rural north: Out-migration in search of employment; sending children tostay with kin in times of stress; using 'famine foods' gathered from the bush.
* For the rural south: Reducing expenditures (taking children out of school); changesin conjugal patterns (contracting informal unions due to inability of young men tomake bridewealth payments).
* For the urban south: Reducing expenditures, including relying increasingly oncooked food sellers, withdrawing children from school; diversifying income sources
An important point to note on coping strategies, is that different coping strategies at theindividual level are not available equally to all categories of the population. Forexample, market-based fallback mechanisms such as migration from the rural north aremore readily available to young men than to many women, children or the elderly(although there is evidence of increasing female migration). The removal of the youngman may even have negative effects for the livelihoods of those left behind (dependingon the level of transfers received). Where a common 'fallback' mechanism appears tohave negative consequences for more vulnerable sections of the populationconsideration needs to be given to possible alternatives. For example, over the lastfifteen years some areas of the Upper East Region have diversified with considerablesuccess into vegetable farming as a dry-season activity, providing an alternative sourceof income which may firstly, reduce male out-migration, and secondly, provide incomeon a broader basis within the community. Provision of dry-season water sources tosupport this kind of activity was the main priority need emerging from the ruralcommunities in the Upper Regions. Assistance of this kind may strengthen community-based fallback mechanisms (local 'safety-nets') through encouraging communitysolidarity and cohesion.
By all accounts many of the long-standing coping strategies that are known in resource-poor communities are becoming less accessible for combating stress periods. This isexplained by the fact that most of these strategies are themselves under threat becauseof worsening ecological conditions and the escalating cost of living. The situationappears to be more grave in northern Ghana, where in communities such as Beo Tankothe consumption of wild foods forms a regular part of strategies of dry-season survival,though one should not under-estimate the looming deprivation in other parts of thecountry.
Fonnal and infonnal 'safety nets". The capacity to help disadvantaged kin or communitymembers was frequently listed as an attribute of the non-poor in our study. At the sametime there was a general sense in many communities that community or kin-based systemsof mutual aid were becoming weaker (as descnbed under trends in social cohesion above).One area where assistance from kdn was consistently cited as critical was in accessing socialservices - particularly emergency healthcare. External sources provided valuable butrelatively rare assistance in many of the field sites. Best placed were those communities
Vi.
with an ongoing NGO program. Governmental safety nets were not mentioned by anyinformants as being in any way relevant for the poorest members of these communities.
Perceptions of access and qualit in healthcare
Many small rural communities in Ghana have very low levels of access to modernhealth facilities. Despite the already low level of coverage, there are situations in whichhealth services have been closed down or withdrawn in the case of mobile services.Where mobile services exist their effectiveness is frequently undermined by problemsof lack of punctuality, and the charging of informal, extra-legal fees. As a result peoplein the rural communities rely extensively on traditional health providers such astraditional birth attendants (TBAs), herbalist/bone-setters, fetish priests drug peddlersand spiritualists. Close proximity to modern health facilities in the urban centres hasconsiderably reduced dependence on these informal sources, though there are certaincategories of illness that people prefer to take to a traditional healer. Examples weregiven of situations in which relatives had withdrawn their patients from hospital to betaken to traditional healers.
Everywhere the selection of a health care provider is contingent upon many factors, andas a result visits to a health facility tend to follow a sequence. A visit normally startswith the most accessible and the least expensive of the facilities available, though otherconsiderations such as type of illness rather than cost and convenience may influencethe sequence. Sequencing of visits to the health care facility commonly takes thefollowing form. Many people depend on home remedies or visits to the herbalist as thefirst step in the treatment of illness. When it becomes critical they will proceed to thedoctor or the spiritualist / fetish priest, depending on the local classification of theillness.
Under current conditions of hunger, the willingness and ability of poor people to spendon amenities such as orthodox healthcare is low. In all three regions studied, high usercosts are resulting in the exclusion of the poor from utilization of hospital services.The public medical system -- laden with accessibility constraints, extralegal charges andoften requiring high financial outlays for transport -- is widely perceived as expensive.Predictably, hospital consultations fall significantly in the "lean season", even thoughdisease tends to be more endemic then, especially among children. In some of thegovernment hospitals (one in particular) there appeared to be a situation of completechaos in relation to charges for healthcare. Official staff appeared unable to giveconsistent figures for charges for the most basic services. Furthermore, unofficial rentswere charged for a wide range of small services.
There were generally positive perceptions of all healthcare providers who lived in thecommunity. Services provided from healthcare personnel outside of their official roles(as friends, neighbors, kin or community members) were in cases more appreciatedthan the official facilities they worked in. In the sites where community health workershad been trained the services was perceived positively. The diagnostic services of drug
ix
store chemists were highly valued. Chemists were generally perceived as "doctors"and therefore, implicitly, as giving higher status and more reliable advice and treatmentthan nurses - perceptions which contribute to the dangers of self medication.
Provisions for cost exemption for the poor generally do not work. Exemptionprovisions were found to be much more effective when executed by ailment rather thanby direct means testing (i.e. for the poor). Indeed, the latter is proving costly inadministrative resources -- money as well as staff time. Only in the mission andcharity hospitals is exemption by means found to be working reasonably well; but eventhen, with high hidden costs. Sometimes, the assistance of the Department of SocialWelfare has to be solicited, and transport facilities provided to enable applicants'circumstances to be investigated. This system is slow and bureaucratic - furthermore,once someone has been identified as poor they generally still do not get treated as thereis no provision for resources to assist them.
In terms of barriers to access to formal healthcare it was noted in all our northerncommunities that even the wealthy do not generally store their resources in the form ofcash. Therefore finding funding for an emergency treatment is not just a problem forthe poor - it applies to everyone in such communities. Generally speaking it takessome days to arrange for the sale of an animal (generally the means by which cash israised). Under these conditions, it is not surprising thatflexibility in accepting deferredpayment was often more valued as an attribute of a service provider than the simplelevel of cost.
The main groups affected by retrenchment in the health sector have been the less skilledpersonnel -- drivers, cleaners, orderlies and similar categories. The most obviousconsequence of their retrenchment has been the adverse impact on hospital cleaningservices. It must be said, though, that while the situation may have been worsened bythe recent retrenchment of lower status personnel, public hospitals in Ghana have had along history of problems with efficient cleaning. Apart from its inimical effect oncleaning operations, another outcome of the policy of retrenching auxiliary nurses hasbeen to entrench pre-existing staff shortages. Throughout the country, relatives of in-patients are having to stay on the wards to help look after their sick kin. Previously,auxiliaries would have been available to perform this function. At one site, wheremajor losses have been incurred through the retrenchment of auxiliary nurses,necessary cuts are having to be made to the size of outreach teams.
Access to outreach services. The mobile health services introduced under the PHCportfolio have' had modest success in reaching remote areas. However, according toour research the achievements in respect of coverage are somewhat offset by the factthat public outreach teams have tended to be rather unreliable with keeping dates andtimes. Not uncommonly, they arrive a day or more late, when villagers are notexpecting them and have leit for their farms. The principal factor constrainingoutreach visits to peripheral sites was reported to be financial, in particular budgetarycutbacks resulting in reduced transport allocations and fuel rations. The reduction in
x
auxiliary nurse numbers has also imposed strains on the capacity of some healthadministrations to release professionally qualified nurses for outreach work.
On occasion, we found outreach teams levying unofficial charges ostensibly to offsettheir transport expenses and to purchase necessary consumables for treatment andnutritional demonstrations. These kinds of informal charges are, of course, not subjectto any form of exemption for the poor - and consequently essential public healthservices (such as vaccinations) are being priced in some instances beyond the reach ofthe poor.
Perceptions of access and quality in education
Factors impeding access to basic education services:
* At the community level very poor condition of school buildings (rural communities);disincentives to continuing education due to lack of Senior Secondary Schoolfacilities in rural areas (the cost of boarding fees puts secondary education waybeyond the reach of the children of the poor). In urban communities parents havea greater range of options and are not constrained to the same degree by theavailability of schools within the community area.
* At the household level lack of resources to purchase equipment and school fees.Costs of schooling are perceived as having risen rapidly in comparison to capacityto pay. Heavy costs are borne in the first year of JSS due to requirements ofhouseholds to purchase equipment for students (uniform, table and chair, math sets,technical drawing board), and in the last year due to costs of registration for exams.These costs outweigh that of the official school fees. Rising real costs combine withpoverty to keep significant numbers of children out of school, often as drop-outs.Cost barriers also remain significant in relation to education for access to primaryschooling. A major component of this is rising PTA fees in line with increasingcommunity responsibility for maintenance of structures etc. The rising costs aremore dramatic in relation to the north - as the ending of the policy of free schoolingin the early 80s has meant that the rise in costs is steeper there. The bulk of thecosts are not composed of formal school fees, however, as with JSS. At all levelsin certain households the main perceived cost of education was the opportunity costof losing the child's labor for domestic and productive purposes.
* No evidence was found of any provision for cost exemption for the poor ineducation. Sympathetic headmasters frequently allow children to attend for sometime without paying fees, but headteachers are accountable in the end for collectingfees for all pupils and are not empowered to make exemptions. This runs counterto an assertion the Minister of Education made in a widely broadcast speech thatchildren should not be expelled from school for non-payment of fees. Some NGOs
xi
fund the costs of school fees for the poor (the largest to do this for its project sitesis World Vision International).
* Evidence was found (especially in secondary schools) of schools being forced totolerate increased levels of absenteeism as many children have to earn the moneyfor their school fees.
* The classic pattern of a drop in the ratio of girls to boys between primary and JSSwas observed. Some informants felt that the high costs of JSS were a factor indiscouraging female attendance. Some informants also drew the classic conclusionof low female school attendance contributing to higher incidence of teenagepregnancy, the contracting of socially inappropriate unions and therefore initiatingcycles of poverty.
Local perceptions of the quality of education services. The major concern of mostcommunity members and teachers canvassed in our study (especially the third phase)was with issues of quality rather than of basic access. The mushrooming of ruralschools (through community initiative, particularly under the ongoing reforms) hasmeant that educational resources have had to be spread quite thin. Thus, while schoolsmay be more accessible (in terms of proximity; not costs), rural communities tend tohave so few teachers per school as to render the quality and value of education in suchschools questionable. In terms of the quality of education the following main messagesemerged from the research:
* Consistent with the findings of the second round of the Ghana Living StandardsSurvey, the quality of education was found to be perceived as low across the sitesstudied - in the views of both community members and service providers. Sharingof furniture built for individual pupils is common. Many children are doingpiecework or helping on their parents farms and pastures after school, leaving themexhausted and with no time for their homework.
* In some sites supervision of teachers was a major concem - especially with respectto children being made to work on teachers' farms during class hours. Anotherconcem (particularly in urban areas) was that teachers put all their efforts into'private' lessons for children who stay behind after the formal class is over. Thesingle greatest factor that seemed to determine the efficiency of the system ofteacher supervision was the availability of transportation allowances for schools'inspectors.
* Parents complained that under the new (post reforms) system feedback on theperformance of children in class was confusing (this appears to be related to the factthat the overall class position of the child is no longer reported - which is the easiestthing for an illiterate parent to understand). Thus the poor performance of their
xii
children at examinations frequently comes as a shock - and the parents' help is notenlisted in encouraging the child to perform better.
The policy of retrenchment of untrained teachers is leading to a shortage of teachersin isolated rural communities. Our research suggests that trained teachers are oftenunwilling to take up rural postings, especially in isolated areas. There may also beunfortunate results in terms of the gender balance of the teacher force - the majorityof untrained teachers are women.
In terms of the perceived relevance of education the following main messages emergedfrom the research:
* The criteria by which local communities defined the 'relevance' of the educationservice were based on two factors: the ability of children to get jobs, the ability ofchildren to read and write in English (so that illiterate parents no longer have to goelsewhere to get letters read and written, compromising the privacy of the family,and children can perform basic tasks like identifying the correct hospital card forfamily members etc.). In only one community was literacy mentioned in relation tolearning improved techniques in traditional occupations - in relation to farming inthe Mamprusi village in the Northern Region. In relation to these criteria education(at the level to which it is pursued by the poor - generally no higher than JSS) isperceived to be failing. People consistently said that their children could not readand write at the end of school. In relation to this parents and teachers in some sitesargued that the new educational curriculum was too broad - with insufficient timeand attention paid to basic literacy.
- Regarding the match between user aspirations and the revised curriculum for first-cycle (ISS) schools, our findings indicate that the reforms are not fulfilling thepurpose for which they were designed. In both rural and urban areas, theimplementation of the technical training component, king-pin in the educationalreform program, is largely perceived as unsatisfactory. In case after case -- inschools, communities and in GES offices -- informants alluded to the lack of tools,working materials, workshop buildings and trained teachers. This situation, aserious impediment to effective skills training in the JSSs, has arisen mainlybecause, in the current cost-sharing framework, communities are not onlyresponsible for financing capital requirements and school furniture, but also forproviding tools and other inputs needed for the program. Consistently, therefore,the skills training objective is being undermined by the high incidence of poverty.There is also a clear regional dimension to this, with our research suggesting thatcommunities in the poorer areas of the country (in this case specifically the sites inour sample in northern Ghana) are less able to meet these extra responsibilities thanthose elsewhere. Lack of skilled craft teachers is also a major constraint in all therural areas in our study. The technical training component was consistentlydescribed as the weakest link in the JSS agenda.
xiii
In terms of the functional literacy program the research teams found that the level ofavailability of materials was very good. The main constraint in most communities(especially rural ones) was the lack of availability of volunteer facilitators. This wasgenerally seen as resulting from the low level of material incentive for people to dothis. The majority of participants in all sites were adult women (there was no evidenceof the program picking up school-leavers who had had to abandon their education).
Local perceptions of water and sanitation services
Within the towns and villages studied, the availability of safe water and sanitation isoften a function of NGO, or other donor presence. Many poor households rely onstreams and uncovered wells of dubious purity. Except where interventions have beenimplemented, therefore, water quality tends to be particularly poor during the dryseason when natural water sources tend to dry up. In the Northern Region in particularhuge amounts of women's labor time during the dry season are expended on fetchingwater - affecting their potential access to employment and income-generatingopportunities. Evidence from all three rounds of the PPA indicate that for communitieswhere water supply is problematic this remains the over-riding priority - especially forwomen. In all low-income urban sites, we found a high level of indiscriminatedefecation, largely resulting from extremely low levels of provision. Understandably,women are more concerned about the deficiencies of water and sanitation: it is they andthe children who are responsible for replenishing household water supplies; and culturalnorms prevent them from evacuating their bowels in open spaces.
Obtaining land is a major issue in relation to some kinds of urban services. There is aparticular problem with obtaining land for latrines as it lowers the value of surroundingproperty. It was found that while VIP latrines functioned excellently in ruralcommunities where population density is low they were virtually impossible to maintainin densely settled urban areas at the concentrations they existed in the areas studied. Itis therefore recommended that a review should be made of means by which DistrictAssemblies can find ways of making more land available for latrines in poor urbanareas - in order to decrease pressure on existing facilities, and thereby set up a virtuouswhere the presence of a latrine in a neighborhood is no longer regarded as a health andenvironmental hazard.
Summaiy: key policy messages
The following are the key policy issues and recommendations emerging from our work:
1. Policy implications of priorities in poor rural and urban communities. As aresult of using a variety of different methods, including needs ranking exercises, andcomparing results from a variety of sites the following general messages emerge fromlocal communities:
xiv
* improved livelihood security for the rural north: People perceive a general crisis oflivelihoods, exacerbated by deteriorating environmental conditions. In much of thenorth the problems of the 'hungry season' dominate local views of poverty.Raising the productivity and improving the robustness of farming systems in fragileenvironments is not an easy task, but it is nonetheless one that needs revisitingthrough all means possible, including: provision of dry season water resources toassist livestock rearing and dry-season gardening initiatives (these are particularlyvaluable because income can be generated in the lean season); agricultural researchand extension services which are attuned to the needs of poor farmers; improved'safety net' provision for the poorest. Our research suggests that the endemicproblems of food security in northern Ghana in particular have never received theserious attention they merit. While all communities surveyed prefer the prospect ofassistance to develop the productivity and security of their livelihoods to 'safety net'kinds of assistance, the severity of problems experienced by the poor in the northsuggests a need for a more robust response in terms of an ongoing institutionalframework for addressing the worst affected social groups and areas. Northerncommunities also showed a relatively higher level of emphasis on education as apriority - which may reflect the greater importance of accessing the migrant labormarket for these communities.
* improved access and quality in healthcare is a priority: This was the mostconsistent message from all of the sites, rural and urban. Accessibility was seen interms of both cost and non-cost barriers. The key to improved access and qualitylies in a vigorous promotion of a community-based approach to both basic curativeand preventive services. Detailed recommendations of healthcare are providedbelow.
* improved transport infrastructure is a priority in rural areas: In many ruralcommunities improving access to markets and to services such as hospital care wasseen to a large extent in terms of the unreliability of physical access. This wasparticularly true of some of the southern communities, where access during therains was highly restricted.
* access to water for domestic consumption: Was invariably the top priority incommunities experiencing particular difficulties with this. These includedcommunities in the rural north, south, and some urban communities. This was aparticularly strong priority for women, and for children - the groups which haveprimary responsibility for domestic water provision. Schoolchildren in Tamalelisted the time spent fetching water as the single greatest problem they faced inpursuing an education.
xv
access to employment opportunities, credit and skills training: Emerged as the mostconsistent priorities in our urban sites - along with specific concerns related to thecondition of the local urban infrastructure.
It should be noted that apart from the themes outlined above, which emerged with someconsistency, many other priority needs reflected closely specific social and economicenvironments. We would recommend, firstly, that donor agencies and governmentconsider the priorities expressed above as an input in developing poverty-focused sectorprograms and projects, and; secondly, that bearing in mind the locally specific natureof many of the constraints which communities perceive in seeking to improve thesecurity and quality of their livelihoods, that the process of strengthening the local levelcapacity to plan and implement programs in a participatory fashion with communitiesthrough a District level planning approach should be strongly supported.
2. Regional dimensions of poverty. Our research strongly supports the findings ofthe quantitative Poverty Profile that the depth and extent of poverty is greatest in therural north. This emerged principally through the consistent stress on food security asthe defining feature of poverty and vulnerability in poor northern communities. Wealso found considerable varialion in the depth of poverty by community - with thepoorest being those communities where the natural resource base has become extremelydepleted as a result of high population densities. Particular dimensions of povertywhich are worth noting include: the strong identification of poverty with community-level factors (access to natural resources, services etc.); the strong seasonal dimensionsof poverty related to water supply and food security.
3. Gender, and the intra-household allocation of responsibilities and distribution ofresources. Findings of the PPA confirm conclusions from many other studies of Ghanathat men and women have substantially different bases for their livelihoods, and thatthere is a high separation of income streams within the household. They also confirmthe common conclusion that the labor burden of women is generally much greater thanthat of men, restricting their access to market-based income generating opportunities.The high labor burden of women, of course has a range of other implications for theirwell-being, including health implications. Two main conclusions can be drawn fromthis:
* if monitoring systems are to provide a comprehensive picture of the impact ofeconomic reform on the poor they need to disaggregate income and consumptiontrends at a level below the household - trends in terms of gender cannot be 'readoff' by looking at the difference between female and male-headed households.
* a very wide range of priorities are suggested for sector policy, and projectinterventions, including: specific attention across a wide variety of fields to makingavailable to women technologies which can lessen their labor burden (includingimproved year-round access to domestic water, grinding mills to lessen burdens of
xvi
food preparation, improved access to travel and transportation, and technologieswhich lessen the labor burden of fuel collection); paying specific attention to theaccess of women to health and education services; paying specific attention toincreasing the productivity of economic activities in which women are alreadyinvolved; paying specific attention to the low level of access to women to credit andproductive services (e.g. agricultural extension).
4. Access to services: implications of community roles in the provision of socialinfrastructure. The research found evidence to support the hypothesis that thedifferential capacity of communities to contribute to cost-recovery in health andeducation may lead to regional inequities in the provision of social infrastructure, andhence access to services. At a fundamental level, it can be assumed that, given equalpopulation size, the capacity of communities in different areas to provide labor for'community projects' (typically oriented towards the construction of physicalstructures, e.g.. clinic, schools) will be fairly similar, but the capacity to raise cash isclearly dependent on a range of other considerations, including wealth and the level ofmonetization of the local economy. Patterns of settlement also influence the level ofrelative effort that is being demanded of communities - with economies of scale forlarger settlements in the provision of some social infrastructure. As has been notedabove, there is a strong regional dimension to the capacity that different communitieshave to contribute cash to community projects such as the construction of infrastructurefor education and health - broadly following the major 'fault lines' of poverty whichare confirmed in Ghana by both quantitative and qualitative analysis.
5. Environmental decline and rural livelihoods. Processes of environmentaldegradation emerge as a major concern in all rural areas of Ghana. These have anumber of different dimensions: declining water access and quality in terms of bothunderground and surface water resources; deteriorating soil fertility in some areas dueto reduced fallow periods, increased intensity of land-use; changes in the crop mix dueto environmental as well as economic factors (e.g.. the spread of swollen shoot diseasefor cocoa, St. Paul's wilt disease for coconut). This emphasizes the fact that the issueof accelerated growth is not necessarily the same as that of sustainable growth, inenvironmental or social terms. Given the importance which the predominant areas ofagricultural development in recent years have for the economic future of Ghana(predominantly Western and Brong-Ahafo Regions) there must be a concern that theagricultural productivity of these regions will suffer in the long run as have the centralareas of the forest zone over recent years. This will harm incomes for the poor both inthe short run (in those areas) and in the long run through declining migrationopportunities.
6. Access to education. The research suggests a combination of constraints inaccess to education which apply at both the level of the household and the level of thecommunity (although provision at the level of the community was seen as lessimportant in poor urban areas). These are summarized above. In terms of specificareas where action could be implemented to improve the situation we recommend:
xvii
* a review of the possibility of instituting cost-exemption provisions to those areas ofschool expenses under the control of schools (regular and special fees, uniformrequirements)
* the contributions that communities are making in education through provision andmaintenance of infrastructure should be recognized - as should the fact thatcontributions in labor are easier for poor communities to make than contributions ofcash (whether at the level of the community or the individual household throughschool fees)
* strengthening of systems of school supervision through provision of transport andtraveling allowances
* there is a need to develop local institutions to manage scholarship schemes - currentlyeducation beyond the JSS level is totally inaccessible to children from poor rural areas- which affects the perceived incentive to send children to school at all levels
* the fact that under the new system (since the education reforms) feedback on pupilperformance is complex for illiterate parents to understand should be addressed -parents need information about the progress of their children if their help is to beenlisted in encouraging their children, and not over-burdening them with productive ordomestic tasks to the point where they perform ineffectively at school
* guidelines should be developed to ensure that the policy of retrenchment of unqualifiedteachers does not remove teaching staff from poor and isolated rural communities.
7. Access, utilization and quality of healthcare. Until the real costs of consultationare reduced substantially (through improvements in fee exemption facilities andprocedures, the elimination of graft and by meaningful improvements to outreach as wellas regular out-patient services), poor people will continue to avoid the public medicalsystem or postpone consulting it when ill. Especially necessary in this respect are:
* awareness creation regarding legitimate costs and exemptions
• introduction of clear and transparent systems for levying charges in large healthfacilities (preferably with a single point for payment within the hospital so it is clearthat other charges are unofficial and illicit - a system which has been adopted at somemission hospitals)
* awareness creation regarding the detrimental impact of drug abuse (dangers of shortcourses of drugs etc.);
xv.
* an expansion of (and improvement in) outreach services; including community-basedschemes (CHWs etc.)
* the implementation of practicable exemption provisions for the poor, particularly atcommunity level.
* a renewed investigation of the possibility of instituting systems of either deferredpayment, or community-based credit, for medical treatment - people in poorcommunities, especially in the north, often hold wealth in forms other than cash (e.g..cattle) which means that money for emergency treatment cannot be raised rapidly evenif the household has the resources to pay.
In relation to extending the effectiveness of cost-exemption provisions the followingactions are recommended for consideration:
* extension of cost exemption provisions applied by ailment to a wider range of diseaseswhich disproportionately affect the poor (or for which the poor are more likely to usepublic services) as this type of exemption provision is far easier to implement thansystems which require the service provider to make a means-based assessment of anindividual
* piloting of community-based and managed exemption systems (involving communitylevel institutions)
* and/or an extension of cost-exemption provision by age-group (elderly, children) -again as this is easier to implement than means-tested measures
* and/or the introduction of provisions to waive user fees on a District-wide basis inareas suffering from particular crises (e.g.. civil conflict, drought)
* a comprehensive review of this issue involving both the Ministry of Health and theDepartment of Social Welfare so that clear instructions can be developed for staff oncost exemption for poor and vulnerable groups
* improved flow of information to communities about their entitlements in relation tocost-exemption
XIX

LINRODUCTION
1.1 Background to the Study
The Ghana Participatory Poverty Assessment forms part of the Extended PovertyStudy. The following report covers material from three phases of the research. Thefirst was in May/June 1993, the second in April/May 1994, and the third in November1994. This exercise forms part of the World Bank's Extended Poverty Study, and hasbeen supported primarily by the UK Overseas Development Administration (phases I &2), and UNICEF (phase 3) with additional funding for the first phase provided byGTZ. In total fifteen communities participated in the research, six urban and nine rural,and nine of Ghana's ten regions were represented in the sample chosen.
The teams which carried out the research consisted of broadly four categories ofparticipant: academic researchers; personnel of the Ministry of Local Government andRural Development; personnel from local non-governmental organizations; andpersonnel from international development agencies. Before each of the three fieldworkexercises a training workshop was held. The training workshops covered a set ofresearch methods commonly known under the title PRA (Participatory RuralAppraisal). In the first phase two experienced international PRA trainers participated -after that training was predominantly handled by research participants. Practical andlogistic arrangements for the fieldwork were coordinated by a Ghanaian NGO(CEDEP).
The following report consists of material derived from that fieldwork. The materialpresented here has gone through a process of synthesis involving the preparation offield site reports for each of the fifteen communities covered by the research as well astwo extensive synthesis documents. These reports are: Ghana Participatory PovertyAssessment, Synthesis Report (Rounds 1 & 2), and Extended Poverty Study (PPA Phase3): Access and Utilization of Basic Social Services by the Poor in Ghana. Preparationof these documents was predominantly carried out by the lead researchers for eachphase of the PPA - for the first two exercises, Dr. Ellen Bortei-Doku Aryeetey (ISSER,University of Ghana, Legon) and for the third phase Dr. David Korboe (UST,Kumasi).
A participatory approach to carrying out country poverty assessments has been found tohave considerable benefits for both the content and impact of the study.' The reasonsfor involving and consulting with a range of stakeholders, including the poor are: tounderstand better the social, economic and political dynamics which perpetuate povertyin a given country; to ensure that strategies identified for poverty reduction reflect the
1 See Andrew Norton and Tom Stephens, Participation in Poverty Assessments, Technical Paper, ENVSPfor a fuller discussion of this (forthcoming, 1995)
1
real concerns voiced by the poor; to promote ownership of the proposed solutions by avariety of stakeholders; and to build in-country institutional capacity for ongoinganalysis of poverty and formulation of policies to reduce it. The specific objectives ofthe first two phases of the research were the following:
a) to explore local conceptions of poverty, vulnerability and relative well-being inpoor urban and rural communities in Ghana.
b) to explore what the poor themselves see as the most effective actions for povertyreduction which can be taken by i) individuals or families, ii) communities, iii)government agencies, iv) other institutions
c) to investigate what people in poor urban and rural communities see as the mainconcerns and problems in their lives at present and how these have changed over thelast 5-10 years
In effect phases one and two were designed as a discrete research project. In the courseof the evolution of the Extencled Poverty Study, however, it was decided to focus inmore detail on a specific issue - namely the question of the access and utilization of keypublic services by the rural and urban poor. A third phase of research was thereforeinitiated which focused on this specific issue. The objectives for the third phase wereas follows:
a) to illustrate the ways in which the rural and urban poor perceive service delivery(both governmental and non-governmental) in the fields of health, education andwater/sanitation, in terms of:- their level of access to services provided- the relevance of the services provided in terms of the capacity to meet their perceivedneeds- their level of utilization of services, and the significance of various constraints whichimpede access and utilization.
b) to illustrate the perceptions of service providers within the governmental serviceprovision structures, primarily at the District and sub-District levels concerning:- the specific needs of the poor in relation to service delivery- factors which impede access to services by the poor- ways in which service delivery to the poor might be improved.
The principle change in methodology from the first two phases of research was the factthat participation in the research was extended from the community level to includeservice providers in the field of health and education (including those in the informalsector, such as traditional healers).
2
1.2 Methodology
The research methods selected for the Ghana PPA were predominantly drawn from aset of techniques commonly known under the rubric of Participatory Rural Appraisal.These include both forms of investigation familiar from other forms of qualitativeresearch, such as focus groups, conversational and semi-structured interviewing, andsome other techniques specific to PRA. These involve structured analytical exercisescarried out by local people through which they elaborate their own analysis of themajor issues they face in their lives. Examples of such exercises include wealthranking; matrix ranking and scoring to assess priority needs and the performance ofservice providers; institutional diagramming; seasonality diagramming to assesspatterns in livelihoods and; participatory mapping of communities to assess socialgroups, service provision and natural resource endowments.
1.3 Field Sites
The following comprises a preliminary overview of the findings of the qualitative andparticipatory research carried out within the Extended Poverty Study in Ghana. Theresearch was carried out in fifteen communities, with some additional material drawnfrom two sites which were included in the training program for the first phase of theresearch. The fifteen sites were:
Phases 1 & 2
i. Sombo (Nadowli District) Upper West Regionii. Komaka (Bawku West District) Upper East Regioniii. Beo Tankou (Bongo District) Upper East Regioniv. Derna (Tano District) Brong Ahafo Regionv. Butre (Ahanta West District) Western Regionvi. Sekondi (Shama Ahanta East District) Western Regionvii. East Maamobi (Ayawaso East District) Greater Accra Regionviii. Dekpor Horme (Ketu District) Volta Regionix. Kpando Gabi (Kpando District) Volta Region
Phase 3
x. Chagni (Tamale District) Northern Regionxi. Nyingare (Mamprusi District) Northern Regionxii Techiman (Techiman District) Brong Ahafo Regionxiii Koforidua (Sunyani District) Brong Ahafo Regionxiv Afrangua (Mfantsiman District) Central Regionxv Breman-Asikuma (Breman-Asikuma District ) Central Region
3
Site selection was designed, on the basis of available quantitative and secondarymaterial as well as the extensive experience of the research teams, to create a purposivesample which would be illustrative of the living conditions of the poor in Ghana, interms of the following major criteria:
* rural/urban balance* modes of livelihood (farming, fishing, pastoralism etc.)* agro-ecological zones* major ethnic/cultural groupings (matrilineal vs. patrilineal, etc.)* level of access to services and infrastructure* level of integration with markets.
Another factor which influenced site selection was a desire on the part of the teams towork in communities where institutional mechanisms were present which could take upissues raised in the research with the communities concerned. To some extent this mayhave created a bias in the sample towards communities with access to a developmentprogram (whether NGO or government supported). Where this appears to be an issuesome allowance is made in the analytical treatment of the material.
2MAIN FINDINGS
The aim of this section is to summarize the principal conclusions from the three phasesof research of the Ghana PPA. Principal policy implications will be outlined in thefinal section of the paper.
2.1 Local Conceptions of Poverty
Local conceptions of poverty were investigated in all sites, to elicit local experiencesand understandings of the nature of poverty in Ghana. Poverty at the level of a livedexperience refers to prevailing cultural values concerning 'needs' - the poor are thosewho fall below an acceptable standard of livelihood. This has social dimensions - theyare people who cannot participate as full members in the daily life of theircommunities. Sometimes the social status of a person may determine their economicstatus - migrant groups may lack access to high quality farmland not only because theylack money, but also because they lack entitlements in respect of the local social
2institutions which determine land access. The values which define poverty vary fromone community to another, ancl defining the poor at the national level, for the purposesof public policy, is not the same issue as defining the poor in a local community. Thereis much to be learned, however, from seeing how poverty is viewed and experienced
2In our study this was illustrated particularly strongly in the immigrant farmers from the Upper WestRegion who were a substantial sub-section of the population of the rural town of Derma in Brong-AhafoRegion.
4
by local communities and households, and our findings suggest that there are significantgeneral messages that can be drawn from these perspectives.
In looking at local understandings it is important to recognize that poverty hasdimensions that apply at different levels of social organization. The constraints whichact on a household's access to income or services are different at the level of theindividual, the household and the community. A child's access to education, forexample, may have the following dimensions: at the level of the household, lack ofmoney for fees and other costs and concern about missing the child's productive anddomestic labor; at the level of the community lack of facilities such as schools andbasic transport infrastructure.
The theme of local views of poverty and well-being was explored through two principalmethods: wealth ranking exercises for households, individuals and communities, andsemi-structured interviews. The major conclusions emerging from the material gatheredin our research on local views of poverty are as follows:
Criteria for assessing poverty and vulnerability at the level of the household andindividual. These varied by region, and according to the gender and generation ofinformants, as is outlined below. To the extent that generalization is possible thefollowing elements can be outlined as consistent elements in local views of thecharacteristics of poverty and well-being:
* Physical assets: These can be divided into physical assets for production(extremely diverse - including animals, grinding mills, access to land, fishingequipment etc. in rural areas and diverse assets to support productive, andespecially trading activities in urban areas, such as vehicles) and non-productiveassets which facilitate a higher standard of livelihood and social status - particularlythe type and condition of housing. Both forms of assets also function as stores ofwealth which can assist households to survive lean times and therefore reducevulnerability to temporary crises.
Hunan assets: The key importance of labor as an asset in poor urban and ruralcommunities received constant emphasis in terms of the emphasis on disability, age,health, childlessness and widowhood in defining the bottom strata of the poor. Inthis category was placed mentally ill people who could not fend for themselves,handicapped people, old people who could no longer work (and lacked networks ofkin for support), and generally weak (sick, not healthy) people. In urban areas thepossession of marketable skills (more than formal education) was frequently cited asa key asset that distinguished the poor from the non-poor.
* Social assets: An individual's social status and network is a critical resource. Asnoted above, in rural areas community membership generally confers access toproductive resources such as land, and access to and control over labor is critically
5
affected by an individuals social status (including gender) and position within thekin group. The social network is also critical for support in times of need - somuch so that in some urban areas people refused to carry out wealth rankingexercises as they argued that it is only when a person is in crisis (e.g. a sickness inthe family) that you can assess their level of access to support from kin - which is akey factor in assessing their security of livelihood. Social marginality throughisolation from kin networks is a key element of poverty for many migrant groups.
* Activities: In some rural communities the necessity to engage in casual 'by-day'labor was seen as indicative of the poor; the capacity to assist with communityprojects, and to help disadvantaged kin was seen as an indicator of wealth in mostrural communities.
* Level of conswnption: In respect of consumption secure access to income and foodpredominated in most sites. In urban areas emphasis on the diversity of the diet aswell as absolute access to food was frequently an indicator of wealth. The otherkey element defining poverty at this level (applying mostly in the rural and urbansouth) was the quality of clothing of an individual and his or her children.
* Access to services: At the household level this was predominantly seen in terms ofhealth and education. The capacity to educate children beyond primary level was afrequent indicator of wealth for the urban and rural south. In terms of health accesswas generally perceived in terms of capacity to pay - in relation to education otherfactors were also involved (especially the opportunity cost of the child's labor foreither agricultural production, income generation or domestic labor).
Criteria for assessing poverty at the level of the community. Rurl poverty, especially inthe north, is often seen as community poverty, where everybody in the communityexperiences low incomes, and lacks basic necessities such as water, roads, clinic andschools. For this reason whole communities are often described as poor - and it is possibleto carry out 'ranking' exercises which rank communities according to the level of well-being of their members, in the same way as is usually done with households or individuals.The criteria which emerge generally fall into three main groups:
* Command over natural resources of the comnunity as a whole: Including in particularaccess to abundant fertile farmiing land, access to common property resources fromwhich essential material for livelihoods such as fuelwood and foraged foodstuffs can begathered, and most importantly of all in the north, access to water for both domestic andproductive needs.
* Access to public services: (education, health - level of provision within the community);
* Access to transport infrastructure., markets, and ease of mobility: Concern over roadtransport infrastructure, for example was particularly strong in many communities in
6
the forest zone, where, during the heavy rains, a poor quality access road can lead towhole areas being without any form of access to vital services such as curativehealthcare, as well as markets for local produce.
As a general rule community poverty is a more comfortable topic for general discussionthan individual or household level poverty, as it avoids the uncomfortable sense ofjudgement of individual worth and demeaning connotations of dependency which frequentlyunderlie such discussions.
Views of Community Poverty in two Northern Communities
Beo Tanko. Bongo District, Upper East RegionMost of the issues of dramatic concern to residents of Beo Tanko (even the poor) were issues thataffected everyone in the community, whatever the level of individual resources they controlled.Of overwhelming concern were issues such as the really dramatic problems associated with accessto water, and the lack of a school or health post in the community. In seeking to probe the issue of'community-poverty' and assets held at the community level the team asked a focus group ofwomen to cite examples of 'better-off' communities and what the characteristics of these are.They mentioned Adaboya, Akayonga and Dua because they have the following:water -for dry season gardening, human consumption, saving timefor womena market-place -provides income from petty tradingfor womengood farmlands - abundance of good quality landforfarming, goodfieldsnatural resources (common property resources) - abundance of economic trees for income-generation for women - sheahnut trees, dawadawa. Abundant forage and pasture for livestock,goats, sheep etc. - which in turn means abundant manurefor 'compoundfarms'.
Komaka, Bawku West District, Upper East RegionThere are rich and poor villages in the area. According to the young men the rich areas have dawadawaand sheanut trees from which these communities make money. Some rich communities have waterwhich enables them to make dry season gardens and with the proceeds they are able to buy "zinc' toroof their houses. Some places have muddy areas and are therefore able to plant rice and after the rice,they plant onions in the dry season. In richer communities, because there are schools, there are moreeducated people who bring 'zinc' to roof their parent's houses. They also have bigger markets fromw'oich they are able to trade. The poorer ones lack these and others like medical facilities. Examples ofricher communities are Gogo and Zebilla and it's surrounding areas. This is because they have water tomake dry season gardening. Examples of poorer communities are Agatuse, Komeka and Sapeliga.
The old men also identified the following as the attributes of a rich community:.- The community has a dam for dry season gardening.- The community has a school, maiket and a health facility .-The community has a large number of houses-The community has a grinding mill .
source: site reports, field teams
The understanding of stratification in poor urban and rural communities. Investigatingthe experience and understanding of poverty, vulnerability and well-being in poor ruraland urban communities involves not only looking at how people define thoseconditions, but also how they see the distribution of those categories. There wasconsiderable variation in this - with poorer communities tending towards morehomogeneity in the level of livelihood. In general, informants divided society (and in
7
particular, their own communities) into four broad wealth cohorts. At one end of thewealth spectrum are those who are perceived as being definitely well off, those whohave stable assets to bequeath to their dependents. To paraphrase from the descriptionspresented by our informants, "they feed their children properly; they live in goodhouses ... which they will pass on to their dependents; and they are able to assistothers". These members are simply referred to as the "rich" (very few could be namedin the rural communities studied; relatively more in the urban). At the other extremeare the chronically hungry, variously referred to as the "extremely poor", the"perennially needy" and the "pathetic". These were said to comprise two broadgroups: firstly "God's poor" - a group in which a variety of factors combine to producea level of destitution which has no apparent remedies - key factors here includedisability, age, widowhood and childlessness (female-headship of households appearedas an indicator of poverty in the rural north, but less so in urban areas and the ruralsouth); secondly a group vvho were seen as chronically poor without obviousdisadvantages related to health, disability and age - but who were generally resourceless- without significant other assets or skills. Significant among the resourceless sub-group in the rural south are some immigrant widowers and other landless sojourners,many of whom lack not just economic means, but social assets (e.g., supportive kinnetworks) as well. In between the two extremes (rich and perennially poor) are themajority -- the cohort of so-called "deprived, but hard-working" members of society --the "not-so-poor" or "hand-to-mouth" category. In poor rural communities, especiallyin the north, they may be particularly vulnerable to seasonal fluctuations in well-being,and their living conditions can be almost as difficult as those of the perennially poor.
Regional dimensions of the undlerstanding of poveny. Criteria for defining wealth in thenorthern rural communities were based to a significantly greater degree on foodavailability than in southern rural communities - reflecting the greater vulnerability anddepth of poverty in the rural north. In one of the southern field sites (one of thecommunities where the workihop research was carried out, Darko) village womenactually had difficulty identifying the 'poorest' strata of the village as they felt thatshould mean people who do not get enough to eat - and they were clear that there wasno one in the village who went hungry. By contrast the classification by women intocategories of 'rich', 'medium' and 'poor' in the village of Sombo was predominantlybased on criteria of food security. A poor woman was described as follows:
"A woman who cannot afford to buy a bowl of grain. One who hasto work for others in order to get a share of the crop and after eatingit, has nothing left, and has to fall on wild leaves or berries tosurvive.n
In the community of Beo Tankou in Bongo District in the Upper East Region villagersdistinguished between two categories of the poor: the 'beggar with one bag' who hasfood which lasts for a few months but has to beg for food in the lean season and forseed to plant, and; the 'beggar with two bags' who has to beg in both seasons(predominantly disabled people, orphans, and the aged without adult children to
8
support them). In a wealth ranking exercise 63 % of the community were estimated tobe 'beggars with one bag' and 30% to be 'beggars with two bags'. Only 7% were seenas having no problem with security of food stocks. A key factor in the greatervulnerability of the northern communities in terms of food security is the fact that thesingle, short, rainy season means that there is only one substantial food harvest peryear. The far more diverse food farming patterns of the rural south mean that thelivelihood systems are more robust and seasonal dimensions of poverty much lesssevere.
9
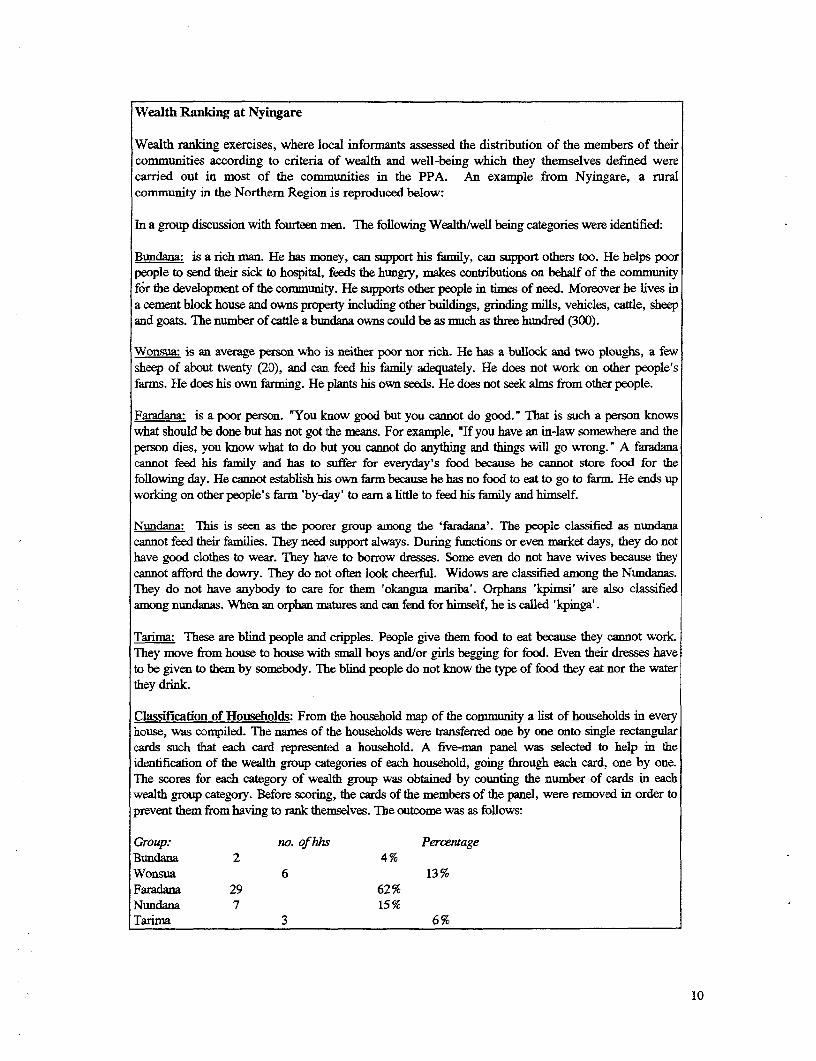
Wealth Ranking at Nyingare
Wealth ranking exercises, where local informants assessed the distribution of the members of theircommunities according to criteria of wealth and well-being which they themselves defined werecarried out in most of the communities in the PPA. An example from Nyingare, a ruralcommunity in the Northem Region is reproduced below:
In a group discussion with fourteen nen. The following Wealth/well being categories were identified:
Bundana: is a rich man. He has money, can support his family, can support others too. He helps poorpeople to send their sick to hospital, feeds the hungry, makes contributions on behalf of the communityfor the development of the community. He supports other people in times of need. Moreover he lives ina cement block house and owns property including other buildings, grinding mills, vehicles, cattle, sheepand goats. The number of cattle a bunidana owns could be as much as three hundred (300).
Wonsua: is an average person who is neither poor nor rich. He has a bullock and two ploughs, a fewsheep of about twenty (20), and can feed his fanily adequately. He does not work on other people'sfarms. He does his own farming. He plants his own seeds. He does not seek alms from other people.
Faradana: is a poor person. 'You know good but you cannot do good." That is such a person knowswhat should be done but has not got the means. For example, "If you have an in-law somewhere and theperson dies, you know what to do but you cannot do anything and things will go wrong." A faradanacannot feed his family and has to suffer for everyday's food because he cannot store food for thefollowing day. He cannot establish his own farm because he has no food to eat to go to farm. He ends upworking on other people's farm 'by-day' to earn a little to feed his family and himself.
Nundana: This is seen as the poorer group among the 'faradana'. The people classified as nundanacannot feed their families. They need support always. During functions or even market days, they do nothave good clothes to wear. They have to borrow dresses. Some even do not have wives because theycannot afford the dowry. They do not often look cheerful. Widows are classified among the Nundanas.They do not have anybody to care for them 'okangua mariba'. Orphans 'kpimsi' are also classifiedamong nundanas. When an orphan matures and can fend for himself, he is called 'kpinga'.
Tarima: These are blind people and cripples. People give them food to eat because they cannot work.They move from house to house with small boys and/or girls begging for food. Even their dresses haveto be given to them by somebody. The blind people do not know the type of food they eat nor the waterthey drink.
Classification of Households: From the household map of the community a list of households in everyhouse, was compiled. The names of the households were transferred one by one onto single rectangularcards such that each card represented a household. A five-man panel was selected to help in theidentification of the wealth group categories of each household, going through each card, one by one.The scores for each category of wealth group was obtained by counting the number of cards in eachwealth group category. Before scoring, the cards of the members of the panel, were removed in order toprevent them from having to rank themselves. The outcome was as follows:
Group: no. of hhs PercentageBundana 2 4%Wonsua 6 13%Faradana 29 62%Nundana 7 15%Tarima 3 6%
10
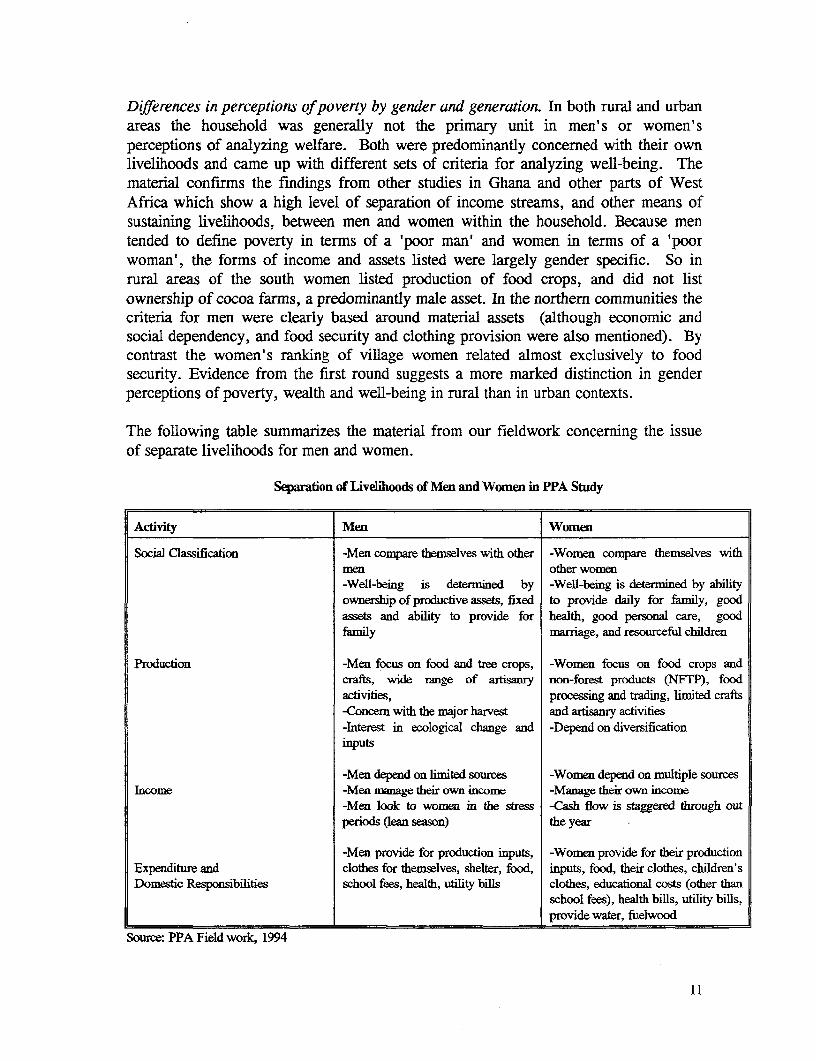
Differences in perceptions of poverty by gender and generation. In both rural and urbanareas the household was generally not the primary unit in men' s or women'sperceptions of analyzing welfare. Both were predominantly concerned with their ownlivelihoods and came up with different sets of criteria for analyzing well-being. Thematerial confirms the findings from other studies in Ghana and other parts of WestAfrica which show a high level of separation of income streams, and other means ofsustaining livelihoods, between men and women within the household. Because mentended to define poverty in terms of a 'poor man' and women in terms of a 'poorwoman', the forms of income and assets listed were largely gender specific. So inrural areas of the south women listed production of food crops, and did not listownership of cocoa farms, a predominantly male asset. In the northern communities thecriteria for men were clearly based around material assets (although economic andsocial dependency, and food security and clothing provision were also mentioned). Bycontrast the women's ranking of village women related almost exclusively to foodsecurity. Evidence from the first round suggests a more marked distinction in genderperceptions of poverty, wealth and well-being in rural than in urban contexts.
The following table summarizes the material from our fieldwork concerning the issueof separate livelihoods for men and women.
Separation of Livelihoods of Men and Women in PPA Study
Activity Men Women
Social Classification -Men compare themselves with other -Women compare themselves withmen other women-Well-being is determined by -Well-being is determined by abilityownership of productive assets, fixed to provide daily for family, goodassets and ability to provide for health, good personal care, goodfamily marriage, and resourceful children
Production -Men focus on food and tree crops, -Women focus on food crops andcrafts, wide range of artisanry non-forest products (NFIP), foodactivities, processing and trading, limited crafts-Concern with the major harvest and artisanry activities-Interest in ecological change and -Depend on diversificationiniputs
-Men depend on limited sources -Women depend on multiple sourcesIncome -Men manage their own income -Manage their own income
-Men look to women in the stress -Cash flow is staggered through outperiods (lean season) the year -
-Men provide for production inputs, -Women provide for their productionExpenditure and clothes for themselves, shelter, food, inputs, food, their clothes, children'sDomestic Responsibilities school fees, health, utility bills clothes, educational costs (other than
school fees), health bills, utility bills,provide water, fuelwood
Source: PPA Field work, 1994
11
Urban households at East Maamnobi and Sekondi operate along the same pattems of separatelivelihoods between men and vomen. Here husbands not engaged in primary productionare expected to give 'chop morney' to add to their wives' efforts. The issue of inadequate'chop money' remains a serious bone of contention in many urban households. Wives oftencomplain that the chop money is less than half what is required, in which case they areforced to contribute a greater share than the men.
By contrast women in northern Ghana work more directly under the supervision of theirhusbands or male relatives, though increasingly there are areas in which they maintainindependent resources. All over the country the trend is for women to establish their ownfarms in addition to the family or men's farms. In fieldwork in the two communities in theUpper East Region in 1994 we found that female labour migration is starting to becomemore acceptable socially. It was also noted that the phenomenon of female headship ofhouseholds was more common in the south (urban and rural) than the north. Thecorrelation between poverty ancl female headship appeared to apply only to the north to anyreliable extent - where the rare female-headed households tend to be genuinely sociallymarginal under the patrilineal kinship systems which prevail in the north.
By and large, generational differences in the view of poverty appeared to be a featureof rural rather than urban pe:rspectives of poverty, and of men rather than women -with older men stressing a traditional view of wealth relating to assets that definedstatus under a purely agrarian system of livelihoods, while younger men express agreater concern with cash income and the acquisition of skills which can produce suchan income. In the northern community of Sombo, a stark generational differenceemerged in the perception of family size. Older people (both male and female)considered the number of household members as a measure of wealth ("they will growup and support you in old age") young men and women saw this as a cause of poverty,because of the inability of parents to cater for and educate children sufficiently. Tosome extent these perceptions reflect social change (with an increased emphasis onindividual income as opposed to the large family farming unit among the young), andto some extent they reflect the developmental, cycle of the household, as a large numberof young children represents a burden to younger parents, while they become an assetin terms of transfers of income and labor as they grow up and the parents age.
12
Gender and Livelihoods in Butre, Western Region
Butre is a small fishing village, with a population of Ahanta and Fanti peoples. The kinshipsystems of both groups are mnatrilineal. There are strong gender dhmeions in fishing and farmingactivities. The majority of the canoe owners are older men plus a few young men. A handful ofwomen have acquired their own canoes which are operated by their male relatives. Normally the personwho owns the canoe also owns the fihing net and outboard motor where there is one. Invariably inevery house where there is a fisherman there is a woman who smokes and markets fish. We did findhowever that some fish smokers have no male relatives in fishing. Fishsmoking is very important forthe women. They tend to combine it with farming, though a few are engaged solely in farming or fishsmoking. Farming is far more significant for women than for the men. Land for farming can beobtained from the chief or the family heads, by both men and women. Wives who are not natives ofButre depend more on their husbands for farm land. The women cultivate both the main subsistencecrop, cassava, and small quantities of maize, as well as commercial crops like tomatoes and onions.Gender segregation in work is very distinct at Butre. Whereas the men rely on their sons and malerelatives to support them in fishing, the women depend on their daughters and female relatives forlabour assistance. It appears that men devote all of their labour to their occupational pursuits, whilewomen commit themselves to both their occupations and their domestic responsibilities such ascooking, cleaning, child care. Very often these multiple tasks are performed simultaneously during theday. Child labour is invaluable for women to meet their labour requirements for domestic chores; bothyoung boys and girls fetch water, clean and baby-sit alongside their mothers.
The Concept of Household at Butre: A wide variety of demographic composition and managementpatterns can be found in the compounds in Butre. Whereas many compounds constitute one householdby virtue of their common family origins and 'head' and shared feeding arrangements, It is common tofind multiple household heads in one compound. In a few instances migrant fishermen and localresidents occupy rented rooms. Compounds are not only known by their heads but also by theoccupants of the rooms. This was vividly illustrated in the social map prepared by a women's group,in which an attempt was made to represent every room in every compound in Butre! Separatelivelihoods based on separately owned and managed resources between men and women, is common ofhousehold arrangements at Butre. Spouses and relatives sharing a household / compound do not pooltheir resources into a common fund for the home, but rather contribute to domestic expenses. Thoughchildren are seen as dependents, they are expected to earn their keep as soon as they are able, in theform of unpaid labour service.source: field site report
Differences in the understanding of poverty in rural and urban areas. A comparison ofthe experiences and understanding of poverty in rural and urban areas reveals a numberof points of differentiation at a general level. The view of poverty as communitypoverty, where everybody in the community experiences low incomes, and lacks basicnecessities such as water, roads, clinic and schools, is considerably stronger in rural thanurban areas. This is also the case for the view of poverty as a transient conditionaffecting whole communities in periods of crisis or seasonal stress. In poor urbancommunities there is greater differentiation between individuals in terms of their personalwealth and their access to community resources. Here it is the middle group that is seen tobe in the majority, though the third group considered to be the poor appears to be quitelarge. The idea of community poverty does not feature as prominently here as one finds inthe runal areas, as social amenities are generally available. The determining factor here isnot availability but affordability.
13
In urban areas the degree of long-ternn vulnerability of individuals was often seen asbeing tied to their level of acquisition of marketable skills within the informal sector.Unskilled wage work within the private sector was disliked due to a perceivedpowerlessness of workers in the face of abuses and breaches of (verbal) contracts bytheir employer. Unskilled self-employed laboring (market truck-pushers, 'loading-boys' etc.) was seen as leaving the individual extremely vulnerable to sickness,disability (temporary or permanent), and infirmity due to aging. While self-employedartisans might not earn more than such laborers, they are envied for having highersocial status and much greater long-term security. All groups in the informal sector,however, envied those in formnal sector waged employment (i.e. where the employeehas a contract of employment). For those with informal sector skills, access to seedcapital was an important dimension in defining the non-poor.
Summary: key assets of the rural and urban poor. A summary of the local conceptionsof poverty and vulnerability leads to the following key messages:
a In all sites there were consistent elements in defining 'the poorest of the poor',which focused on the intersection of a variety of conditions which lead tohouseholds which have no labor resources, and individuals who have no controlover labor resources of any kind. The key elements were disability, age combinedwith the lack of adult children, widowhood and childlessness. Female householdheadship was more likely to appear as an indicator of poverty in the rural north thanthe rural south or urban contexts. While female headship as such is not related in asimple sense to poverty the combination for women of age, widowhood and lack ofadult children was frequently seen as associated with chronic vulnerability.
• Assets at the community level were seen as more important to rural communitiesthan urban - these included access to water for domestic and productive use, accessto public services, access to an abundant natural resource base in terms of fertilefarmland and common property resources, and access to transport infrastructure andmarkets.
* The view of poverty as being a dynamic condition impacting on entire communitieswas particularly strong in the northern rural areas, vulnerable to drought and to the'hungry season' prior to the single main annual harvest of bulk foodstuffs. Thematerial collected supports the view that the experience of depth of poverty andvulnerability in the rural north is greater than in other areas through the fact thataccess to food predominates in local views of poverty, and that in somecommunities serious food insecurity prevails for at least part of the year forvirtually every community member. Nonetheless the material is suggestive of somevariation - with highly populated areas in the Upper East (Bawku and BongoDistricts) suffering the worst conditions.
14
* In urban areas poverty tends to be seen more as an individual condition - with keyelements in defining well-being including access to stable employment, the abilityto acquire marketable skills and access to seed capital (as well as the fundamentalasset of physical health and strength).
* As well as physical assets (livestock, capital etc.) and human assets (health, skills)an individual's social network, and membership of social institutions forms a keydimension of well-being and livelihood security. Access to land often comesthrough community membership rather than the market, and the accessibility of asupportive kin network is critical at times of personal crisis (urgent need for moneyto pay hospital bills, etc.).
* Gender dimensions emerged primarily through stressing the fact that there aresubstantial elements of separation to men's and women's livelihoods in manysections of the rural and urban poor in Ghana. In ranking exercises in rural areasthere was a tendency for men to rank men and women to rank women, rather thanseeing households as unified entities. Men and women thus also stressed differentelements to the experience of poverty in some communities.
2.2 Priorities of the Poor in Poverty Reduction
In all communities covered in our study the issue of the priorities of the poor in relationto appropriate action for poverty reduction was examined. While perhaps the mostimportant element to examine in relation to public policy is what the urban and ruralpoor see as the most important actions for government and other outside agencies totake, it was also considered important to explore local views of the roles thatindividuals, households and communities could take in order to contribute toovercoming the key constraints that they faced. This confirmed that in no instance didthe members of poor urban and rural communities regard the key issues they faced asones over which they were completely powerless and for which outside 'charity' wouldbe the only solution. There was a complete recognition that action by the state andNGOs should be matched by an equivalent effort from poor communities andhouseholds.
The results of the priority rankings. The issue of the communities' own assessment oftheir priority needs was a consistent theme in our research. Where possible these viewswere solicited through focus groups which reflected the diversity of the communitiesunder study in terms, at least, of gender and generational issues. The major findingscan be grouped into three broad regional 'blocks': the rural north (the Upper Regionsand the Northern Region), the rural south (including the transition zone, forest zoneand the coastal savannah - for our purposes communities in Brong Ahafo, Volta,Western and Central Regions) and urban communities (including one intermediaterural town in Volta Region, and communities within the major urban centers of Accra,Tamale and Techiman). In examining the issue of community priorities we have taken
15
care in the interpretation: the fact that a service does not appear as a priority need maybe because the community is satisfied with the existing service - rather than that they donot regard it as important. It should be noted that material on health and education isalso examined under separate headings in sections 2.6 and 2.7 below.
Priority rankings in the rural north. The strongest themes emerging from the priorityranking exercises in the rural north are food security, water (both for productive anddomestic use), access to health care, and education.
In the semi-arid north only one community failed to rank water as a priority need -Nyinagare in the Northern Region - which can be attributed fairly clearly to the factthat the community has been provided with a borehole by the NORRIP water program.It is also partly due to the fact that agriculture in the area of Nyingare is suffering lessfrom over-use of limited land resources by a dense population that in the communitiesof the Upper Regions, where, particularly in Bongo and Bawku, rainfed farming is nowso unproductive that resources which can provide dry season income (such as a dam fordry-season gardening) are becoming increasingly critical for basic survival.
In Beo Tanko, in Bongo District, Water was consistently evaluated the most pressingneed of the community. Among the linkages that were expressed in different contextswere the following: deterioration in the level of water supply has decreased animalholdings in the village, thereby reducing soil fertility by decreasing manure resourcesavailable (poor water supply also encourages villagers to pasture cattle elsewhere whichhas the effect of reducing farn production - a far more serious problem for villageswhich face land scarcity); poor water supply creates a huge extra burden for villagewomen; lack of dry-season water supply means that the village lacks effective meansfor dry season income-generation through vegetable gardening, shea nut extraction,processing of dawadawa for sale etc.; the poor quality of the village water supply leadsto severe health problems which in turn impact on the productive capacity of thevillage. The major articulated demand in relation to water in Beo Tanko is theprovision of a dam. The villagers say that a hard layer of rock has defeated all effortsto sink boreholes and hand-dug wells. They also want a dam, however, because it isthe most convenient source of water for dry-season gardening and livestock.
16
Water in Tanko
The community informed the team that the only source of water in the dry season was a small pond"which resembles a traditional grave". One had to squeeze tight in order to get access to the waterwhich comes in tiny driblets. This information was confirmed by the team leader who took time offto visit the pond. He found out that only one woman could enter the 'hole' at a time and only half acalabash of water could be scooped out at a time. For this reason, women have to wait several hoursto fetch water in turns. It was reported that women usually went in two batches. The first batchleaves around 7.00 p.m. (after supper) and returns around mid-night. The second batch leavesaround mid-night and returns at dawn or day-break depending on the n umber of women who mightbe waiting at any one particular time. The same pond provides water for the community in the rainyseason. A focus group of village men linked the lack of water with the high illness of disease in thevillage, citing guinea worm, bilharzia, diarrhea, stomach pains and skin rashes as ailments linked tothe bad water that community members drink
source: field team site report
In Komaka, in Bawku, food security was seen as the principle problem facing thecommunity, while, again, a dam was seen as the most practical solution to this problemas it would allow the villagers to increase the fertility of their farms through pasturinganimals locally, and would provide dry season income through vegetable farming(currently those of the villagers who are able walk six miles to another site to do this).People in Komaka made an explicit link between provision of a dam and the capacity toretain young men in the village and prevent temporary and permanent out-migration ofthe youth. In Sombo, in the Upper West Region, people also saw provision of a dam asone of the top two priorities for the community. In Nyingare the emphasis onstrengthening the productive system was still on rainfed farming - with the village menexpressing a hope for renovation of the local farmers' service center which used toprovide help in promoting animal traction for farming.
The other consistent messages emerging from the priority rankings carried out in therural north was that improved access to education and curative healthcare werepriorities among most communities and social groups. Improved access to curativehealthcare emerged as one of the top four priorities listed in all ranking exercisescarried out in the rural north. The need was usually expressed through a desire to havea clinic facility within the community, as physical distance and cost of transport wereseen as major barriers to access. The emphasis placed on education as a priority needwas variable - with a strong emphasis emerging from Nyinagare in the NorthernRegion, where improved access to education was the first priority, and lower emphasisin other sites, even those like Beo Tanko and Komaka where there is no primaryschool in the village and children have to walk three miles or more to the nearestfacility. In Nyingare there was a primary school but it did not cater for classes four tosix - so to complete their schooling the children had to walk a distance of over twomiles to and from Gambaga.
17
Access to grinding-mills for processing millet also emerged as a priority for women intwo of the sites. Essentially this reduces dramatically the time spent of food processingby women, and thus, along with domestic water supply, is a major issue for them.
In summary, priorities from the rural north focused on basic livelihoods, reflecting theendemic problems of food security experienced in this area, as well as the chronicproblems of domestic water supply that affect communities which have not benefitedfrom external aid such as the NORRIP and CIDA programs of village water supply.The emphasis on provision of dry season water for productive purposes is worthhighlighting as it reflects two key problems that afflict the communities which are inthe most difficult situation in terms of high population densities, land scarcity anddeclining soil fertility (conditions which are characteristic of the Bongo and Bawkuareas). A dry season water source (such as a dam) can provide two key elements whichstrengthen the local livelihood systems: enabling livestock owned by villagers topasture in the area for longer periods of the year thus providing manure for chronicallyunder-nourished farming land and; providing for vastly increased dry season incomethrough vegetable gardening to compensate for the decline of productivity in thetraditional grain-farming system. The other consistent emphasis is on healthcareprovision - reflecting both poor conditions in terms of access, and the value of physicalhealth and strength which is a consistent theme in the local views of poverty reflectedfrom all areas.
Priority Rankings in the Rural South. The picture emerging from priority rankings inthe rural south is more diverse - reflecting the greater diversity in terms of livelihoodsystems and environment in this zone, as well as the tendency towards greater socialstratification, and therefore inira-community diversity. In some communities, such asButre in Western Region, food security was not a major concern even for the poor -although this was not true of all the sites (food supply was very insecure for the poorercommunity members in Afrangua, in Central Region). Again access to curativehealthcare emerged as a strong and consistent theme - in only one community was thisnot listed as a priority need, which was Derma in Brong-Ahafo Region where areasonably well-stocked clinic functions, and improved access to healthcare was seenmainly in terms of the condition of the access road, which is impassable for periods inthe rains, denying access to hospital care. Improvements in transport infrastructure(roads and bridges) emerged as a major priority in three of the five southern ruralcommunities. This reflects ito some extent the ecological conditions of much ofsouthern Ghana, where heavier and more persistent rainfall tends to lead tocommunities becoming totally isolated for periods of the year.3 In addition to denyingaccess to services, poor quality access roads are frequently seen as impacting negativelyon the economic opportunities available. Derma, for example, has come to specialize
3 Though it is important to note that some areas of northem Ghana also suffer from rainy-season isolationfrom services and markets. This is especially true of some of the Mamprusi settled areas in the northerpart of the Northern Region which are known, with a touch of grim humor, as 'overseas'.
18
in tomato production in recent years. Difficulties of road access are a majordisadvantage in relation to highly perishable crops such as this.
Access to water for domestic use again emerged as a major theme, especially in thevillage of Butre in Western Region. In a pattern repeated in some other sites, threewells had been dug with local assistance at points over the last twenty years, but notone of them was now functioning reliably. A local spring had become the major watersource, but it is muddy, the water has a salty taste, and it is seen by villagers as thesource of guinea worm infection. During the dry season women spend long periods inthe day and night queuing for water. In communities where water did not feature as apriority in ranking exercises, such as Afrangua in the Central Region, this could oftenbe traced to an intervention by an outside agency (in this case the NGO, World VisionInternational who sunk a borehole in 1986).
Other common themes included access to off-farm employment and credit for farming(predominantly men) and trading activities (predominantly women). Better sanitationand drainage emerged as themes in three of the five communities. In general theemphasis on education was lower than in the north - though in large measure this isprobably because the situation in terms of provision was better (all of thesecommunities had at least one primary school, and two - Derma and Dekpor Horme,also had Junior Secondary Schools). For those communities which did not have JuniorSecondary Schools, the distances to travel to such facilities were usually less than in thenorth.
Priority Rankings in the Urban Communities. Six urban communities were covered bythe study, including intermediate towns in Volta and Central Regions (populations of10-15,000) where many aspects of livelihoods remained rural in character, and poorcommunities within four other urban centers: Accra (East Maamobi), Sekondi, Tamale(Chagni) and Techiman (Zongo and Dwemoh). Again, differentiation was marked -even in some cases between different sections of the town which experienced differentkinds of problems in reaction to urban services. The most consistent concerns,reflecting the nature of urban livelihoods were with inadequate employmentopportunities and the supply of small-enterprise credit. Although these elements wereconsistently scored they were rarely the first priority. An exception was Sekondi -which has seen the almost total disappearance of a once-active labor-market associatedwith the port and associated services. As the business steadily disappeared due to thelong-term impact of the construction of ports at Tema and Takoradi the economy ofthis community became increasingly dependent on fishing, for men, and fish-smokingand trading for women. The stagnant economy means that the youth at Sekondi have anover-riding concern with the issue of un- and under-employment.
Priority rankings seemed to reflect to a large degree the condition of the local urbaninfrastructure. In particular it was interesting to note that three of our five communitieshad major problems of supply of potable water.
19
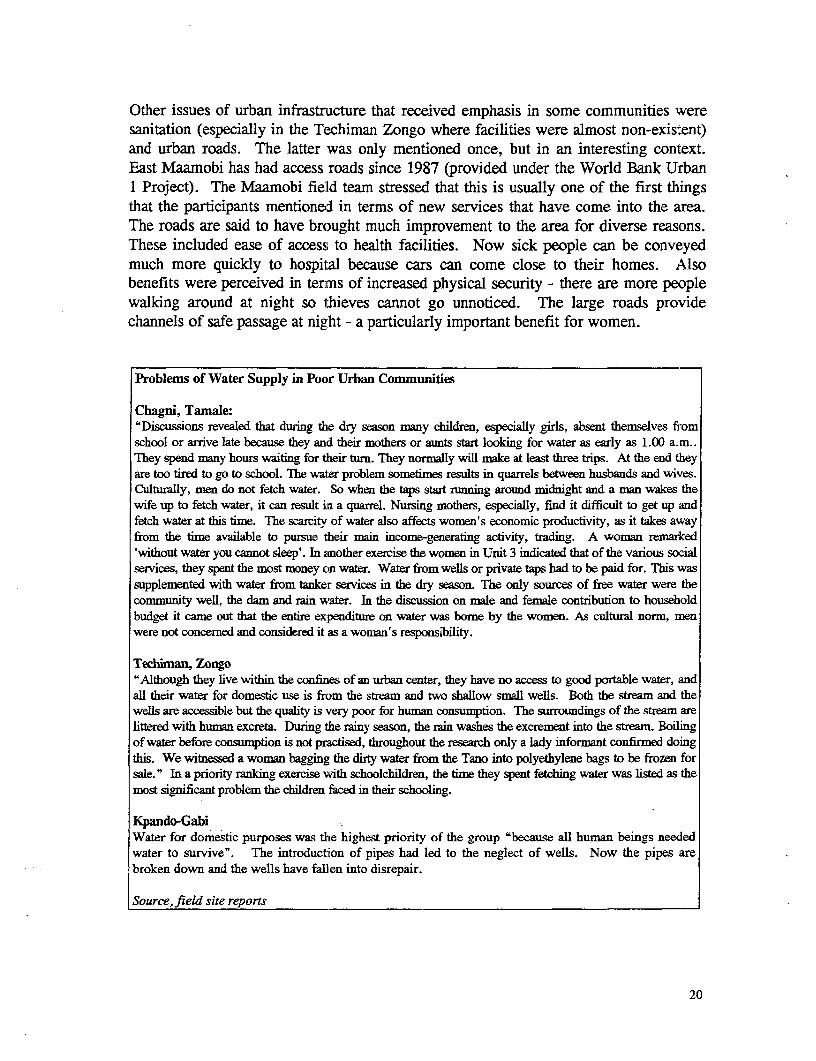
Other issues of urban infrastructure that received emphasis in some communities weresanitation (especially in the Techiman Zongo where facilities were almost non-existent)and urban roads. The latter was only mentioned once, but in an interesting context.East Maamobi has had access roads since 1987 (provided under the World Bank Urban1 Project). The Maamobi fieLd team stressed that this is usually one of the first thingsthat the participants mentioned in terms of new services that have come into the area.The roads are said to have brought much improvement to the area for diverse reasons.These included ease of access to health facilities. Now sick people can be conveyedmuch more quickly to hospilaL because cars can come close to their homes. Alsobenefits were perceived in terms of increased physical security - there are more peoplewalking around at night so thieves cannot go unnoticed. The large roads providechannels of safe passage at nig;ht - a particularly important benefit for women.
Problems of Water Supply in Poor Urban Conmunities
Chagni, Tamale:"Discussions revealed that dunng the dry season many children, especially girls, absent themselves fromschool or arrive late because they and their mothers or aunts start looking for water as early as 1.00 a.m..They spend many hours waiting for their turn. They normaUy wilU make at least three trips. At the end theyare too tired to go to school. The water problem sometimes results in quarrels between husbands and wives.Culturally, men do not fetch water. So when the taps start running around midnight and a man wakes thewife up to fetch water, it can result in a quarrel. Nursing mothers, especially, find it difficult to get up andfetch water at this time. The scarcity of water also affects women's economic productivity, as it takes awayfrom the time available to pursue their main income-generating activity, trading. A woman remarked'without water you cannot sleep'. In Enother exercise the women in Unit 3 indicated that of the various socialservices, they spent the most money on water. Water from wells or private taps bad to be paid for. This wassupplemented with water from tanker services in the dry season. The only sources of free water were thecommunity well, the dam and rain water. In the discussion on male and female contribution to householdbudget it came out that the entire expenditure on water was bome by the women. As cultwral norm, menwere not concerned and considered it as a woman's responsibility.
Techisnan, Zongo"Although they live within the confines of an urban center, they have no access to good portable water, andall their water for domestic use is from the stream and two shallow smal wells. Both the stream and thewells are accessible but the quality is very poor for human consumption. The surroundings of the stream arelittered with human excreta. During the rainy season, the rain washes the excrement into the stream. Boilingof water before consumption is not practised, throughout the research only a lady informant confinned doingthis. We witnessed a woman bagging the dirty water from the Tano into polyethylene bags to be frozen forsale." In a priority ranking exercise with schoolchildren, the time they spent fetching water was listed as themost significant problem the children faced in their schooling.
Kpando-GabiWater for domestic purposes was the highest priority of the group "because all human beings neededwater to survive". The introduction of pipes had led to the neglect of wells. Now the pipes arebroken down and the wells have fallen into disrepair.
Source, field site reports
20
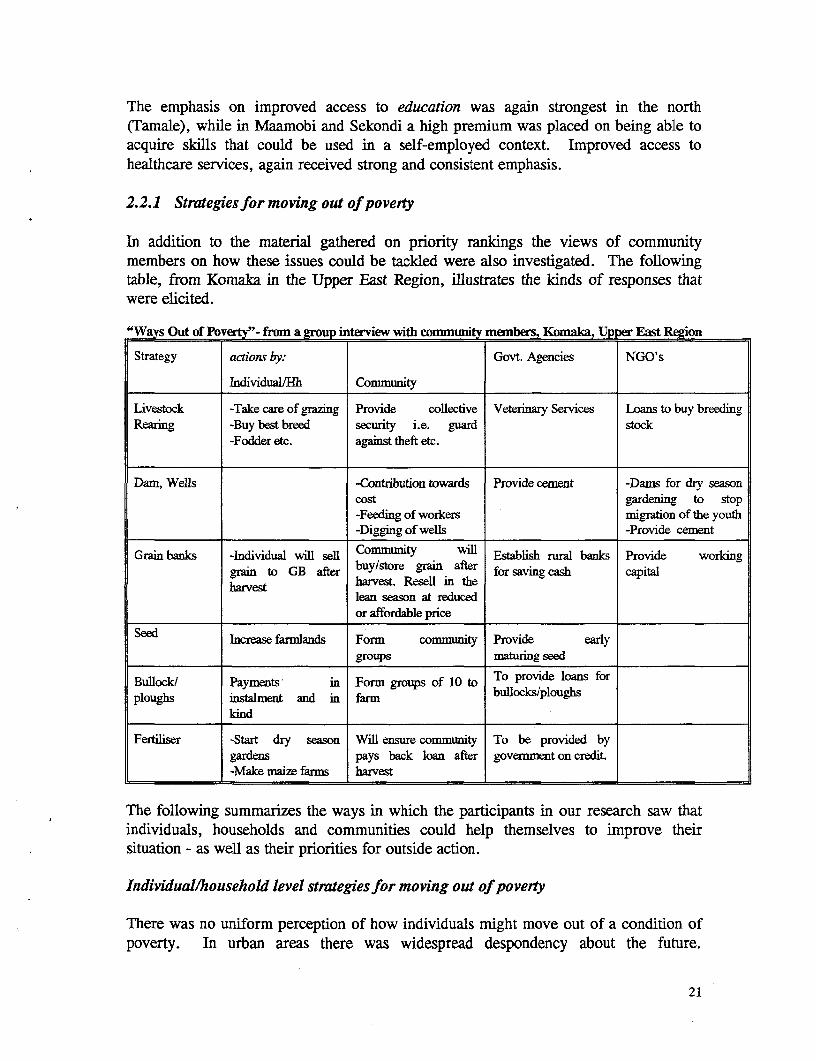
The emphasis on improved access to education was again strongest in the north(Tamale), while in Maamobi and Sekondi a high premium was placed on being able toacquire skills that could be used in a self-employed context. Improved access tohealthcare services, again received strong and consistent emphasis.
2.2.1 Strategiesfor moving out of poverty
In addition to the material gathered on priority rankings the views of communitymembers on how these issues could be tackded were also investigated. The followingtable, from Komaka in the Upper East Region, illustrates the kinds of responses thatwere elicited.
"Ways Out of Poverty"- from a group interview with community members, Komaka, Upper East Region
Strategy actions by: Govt. Agencies NGO's
IndividualMlh Community
Livestock -Take care of grazing Provide collective Veterinary Services Loans to buy breedingRearing -Buy best breed security i.e. guard stock
-Fodder etc. against theft etc.
Dam, Wells -Contribution towards Provide cement -Dams for dry seasoncost gardening to stop-Feeding of workers migration of the youth
l__________ -Digging of wells -Provide cement
Grain banks -Individual will sell Community will Establish rural banks Provide workinggrain to GB after buy/store grain after for saving cash capitalharvest harvest. Resell in the
lean season at reducedor affordable price
Seed Increase farmlands Form community Provide earlyl____________ groups maturing seed
Bullock/ Payments in Form groups of 10 to To provide loans forploughs insalment and in farm bullockslploughs
kind
Fertiliser -Start dry season Will ensure community To be provided bygardens pays back loan after govemment on credit.-Make maie farms harvest
The following summarizes the ways in which the participants in our research saw thatindividuals, households and communities could help themselves to improve theirsituation - as well as their priorities for outside action.
Individuallhousehold level strategies for moving out of poverly
There was no uniform perception of how individuals might move out of a condition ofpoverty. In urban areas there was widespread despondency about the future.
21
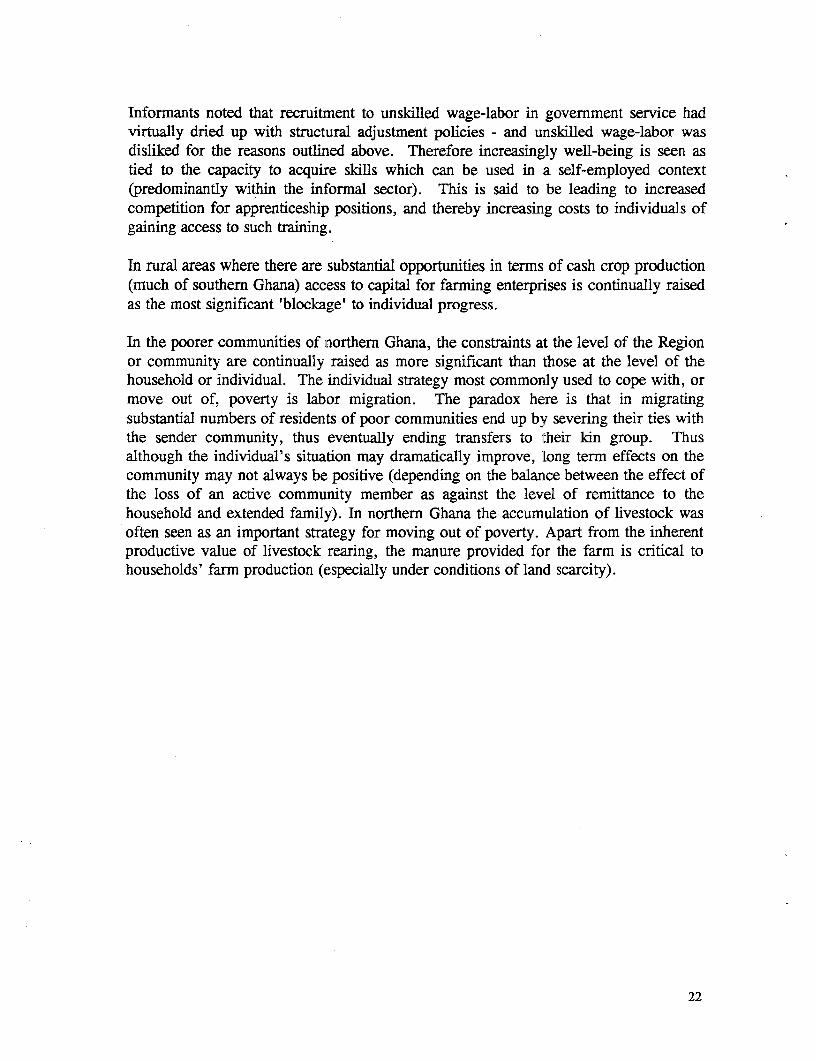
Informants noted that recruitment to unskilled wage-labor in government service hadvirtually dried up with structural adjustment policies - and unskilled wage-labor wasdisliked for the reasons outlined above. Therefore increasingly well-being is seen astied to the capacity to acquire skills which can be used in a self-employed context(predominantly within the informal sector). This is said to be leading to increasedcompetition for apprenticeship positions, and thereby increasing costs to individuals ofgaining access to such training.
In rural areas where there are substantial opportunities in terms of cash crop production(much of southern Ghana) access to capital for farming enterprises is continually raisedas the most significant 'blockage' to individual progress.
In the poorer communities of northern Ghana, the constraints at the level of the Regionor community are continually raised as more significant than those at the level of thehousehold or individual. The individual strategy most commonly used to cope with, ormove out of, poverty is labor migration. The paradox here is that in migratingsubstantial numbers of residents of poor communities end up by severing their ties withthe sender community, thus eventually ending transfers to their kin group. Thusalthough the individual's situation may dramatically improve, long term effects on thecommunity may not always be positive (depending on the balance between the effect ofthe loss of an active community member as against the level of remittance to thehousehold and extended family). In northern Ghana the accumulation of livestock wasoften seen as an important strategy for moving out of poverty. Apart from the inherentproductive value of livestock rearing, the manure provided for the farm is critical tohouseholds' farm production (especially under conditions of land scarcity).
22
Costs of Apprenticeship
The cost and period of study under apprenticeships vary according to the vocation, and sometimes theaptitude of the student. On the average it takes about three years to go through an artisanal course. Overthe past ten years the training fees involved in apprenticeships have risen considerably, making it difficultfor the youth from poorer homes to gain access to this previously accessible institution. The types ofcharges that are involved include: an initial charge, usually 50-100,000 cedis; cost of tools andequipment (varies from around 15-100,000; the costs of the graduation party (drinks, gifts, sheep,money).
Anane Bokor Fitters Workshop at East Maamobi..There are 2 masters and 17 apprentices here. The apprentices have to pay the following initial costs:¢50,000, unspecified drinks, tools worth about ¢50,0004150,000. The training takes 4 years, they are given adaily allowance of C100-¢200.
Prince of Peace Hairdressing Salon, East Maainobi...Mad. Ama has 2 apprentices, they have to pay the following initial costs:¢30,000-¢40,000, 4 towels, 2pkts rollers, set of combs.
Somnelimes apprentices cannot pay the fees...Peter at Sekondi could not continue school after middle 4,because his parents could not afford it. He went into tailoring apprenticeship at the cost of C20,000 (now¢50,000), a pkt of matches, cigarettes, beer, schnapps. His father could not pay the entire costs so half of it waswaived. His graduation fee was one sheep and one bottle of schnapps.
Some of the Fees are More Reasonable...At the coffin maker's workshop in Sekondi apprentices are required to pay -3,000, a bottle of schnapps, 5 pktscigarettes, 12 boxes of matches
Although securing access to education for children is clearly a very high priority forhouseholds it did not emerge as a particularly strong element in peoples' presentation ofstrategies for moving out of poverty at the household level in rural areas of southernGhana (although it did feature in the rural north). It is of course possible that althougheducation for children is highly valued, local experience suggests that it is not aparticularly important strategy for moving out of poverty for the household as a whole.
Community-level strategies for povery reduction
The mobilization, at the community level, of resources for the provision of transport,social and economic infrastructure has long been a feature of Ghanaian life. Whileprovision of labor appears to be fairly universal, the capacity of communities tocontribute cash varies greatly. One community (Derma, in Brong-Ahafo Region) hadput a great deal of effort into the provision of community-level assets (including anunfinished tomato-processing plant, a clinic, two Junior Secondary Schools, a RuralBank, and a still unfinished program of rural electrification). While communityinvolvement in the provision of social infrastructure is also widespread, communityinvolvement (as in Derma) in the provision of productive infrastructure tends to be
23
dependent on the identification of specific income-enhancing strategies which can becarried out at the community level.
It is notable that, although northern communities had much the same analysis of theimportance of social infrastructure their ability to provide cash to support suchconstruction projects was very highly constrained - while contributions in terms oflabor could be mobilized at the same level as the south. As has been noted above, thekey resource at the community level in much of northern Ghana is the provision of adry season water source - both for domestic use and productive activities. Over recentyears (since the mid-1970s) dry season farming of a range of crops for market sale (inparticular onions) has become a vital survival strategy for many communities andindividuals, especially in the Upper East Region. While communities are prepared tomake extensive labor inputs to small dam facilities, the cash costs of establishing themtend to be outside their reach.
It was striking that while rural communities had established practices for the support ofcommunity-level initiatives, and also innovative ideas for extending these - in urbancommunities there was little that people felt they could accomplish through collectiveaction at this level4 . In terms of moving out of poverty only the occupationalassociations to which many in the informal sector belong were mentioned in thiscontext. Although local leaderships exist in urban areas they seem to be commonlyviewed as distant from the concerns of the poor.
Local views of priorites for public action for poverty reduction
The local priorities for public action for poverty reduction varied between our sites inline with the differences outlined above. For the rural north the major concerns werewith strengthening livelihoods through provision of water for dry season productiveactivities and domestic use, and with improved service delivery in health and education.A role for outside agencies was perceived in terms of providing assistance withconstruction of dams and provision of wells. In relation to service provision the poorlevel of access to both health and education facilities was a major concern. Whilecommunities could help in provision of physical infrastructure effective sustainablemanagement of schools and clinics was seen as being a matter for public action. Inrelation to NGOs, a high level of appreciation was voiced for NGO efforts in healthand education provision, and a, recognition of certain areas where NGOs had specialistexpertise which could assist in strengthening local livelihoods. In Komaka, forexample, the community members were keen to establish a grain bank to createemergency food stocks in the village and thus reduce vulnerability to both drought andthe ravages of the 'lean season'. This was seen as an area where NGO assistance waslikely to be more appropriate and effective than government assistance.
4. See page 108, Aryeetey, et al. (Synthesis Report, Phase 1 & 2)
24
In the rural south and in urban areas provision of improved employment opportunitieswas seen as a major priority for government action - although the sense of specificdetails of what actions this might involve were not clear. Similarly credit emerged as amajor concern both for farming and small-scale trading activities (the latter particularlyfor women). This is seen as an area for both government and NGO intervention.Improved access to water and quality of water supply were major issues in some of theurban communities, as was improved sanitation. To a greater degree than in ruralcommunities, urban communities tend to see domestic water and sanitation asappropriate areas for government intervention. In rural areas of the south there was astrong concern in some communities with the condition of the road infrastructure . Theimprovement of road infrastructure was generally seen as an area suitable forcollaboration between community level institutions (mobilizing labor and maintenancefunds) and outside agencies, particularly local government (provision of capital,equipment and possibly food-for work incentives). As in the north partnerships withgovernment ministries were seen as the appropriate means for increasing access to basichealth and education services. There is still a tendency to see the community's role interms of contributing to the construction and maintenance of physical infrastructure.
2.3 Vulnerability: Dynamic Dimensions of Poverty
Frequently local understandings of people in poor rural and urban communities of thekey elements in sustaining their livelihoods concur more with the concept of'vulnerability' than that of poverty. The idea of a secure livelihood is frequently moreimportant than the incentive to maximize income.5 To ensure this security people needmore than just access to opportunities for employment or increasing the productivity oftheir self-employed or household based activities and access to social services. Theyalso need a structure of stable institutions at the local level which provide a frameworkfor local cooperation in a variety of critical areas - which may include managing thenatural resource base of the community; community based systems for assistingvulnerable groups; systems of cooperation in farming or other productive activities.
Vulnerability is a 'dynamic' concept which refers to the way people experience changeover time. Such change may have a number of different dimensions:
* seasonal change: Including periods of stress in terms of food supply, the incidenceof disease and workloads (especially of women) in relation to farming, access tofuel and access to water
* long-term trends: For example declining soil fertility, unfavorable movements interms of trade, changes in the labor market etc.
* 'shocks': Experienced either at the level of the region or community (e.g. drought)or at the level of the individual/household (e.g. illness).
5 See, for example, Robert Chambers, Introduction IDS Bulletin on Vulnerability 1989
25
Some of these issues have been covered under local conceptions of poverty above, but abrief summary of some further issues can provide useful further insights into the natureof poverty and change in Ghana.
2.3.1 Seasonal dimensions of poverty
Seasonal fluctuations were a major aspect of well-being in all research sites. Inaddition to the well-documented phenomena of stress points in the agricultural cycle,which takes its most severe form in the 'hungry season' problems of many savannahcommunities, there are significant seasonal cycles in urban occupations related tofactors such as weather (impact on building), the cycle of social activity and keyfestivals, and market flows related to the agricultural year. The cycle of festivals has acomplex effect on urban trades: major festivals, especially Christmas, bring largenumbers of out-migrants back from overseas where they may be very high eamersindeed in local terms, causing a reported peak in building activity in one community asthey provided major infusions of cash for house-building projects which are effectedover a period of severai years. Festivals also lead to high spending on personalappearance, and peak activity for hairdressers and tailors - while the period of a majorfestival constitutes a slump in business for cooked food sellers, as people are moreinclined to prepare food at home.
As has been noted above the major seasonal food security issue in Ghana is the extreme'hunger season' experienced by many communities in the north - especially those whereintense population pressure has led to declining soil fertility (for example, Komaka,Beo Tanko and Sombo in our sample). These communities experience major problemsof basic food supply even in a normal year - and the impact of drought years can beextreme. As a general rule, the more diverse the farming system, in terms of the mixof basic staples and crops grown to generate income, the less was the degree ofvulnerability to seasonal food scarcity. On top of that cassava, as a crop which can beavailable for harvesting all year round, often plays a special role in mitigatingvulnerability.
26
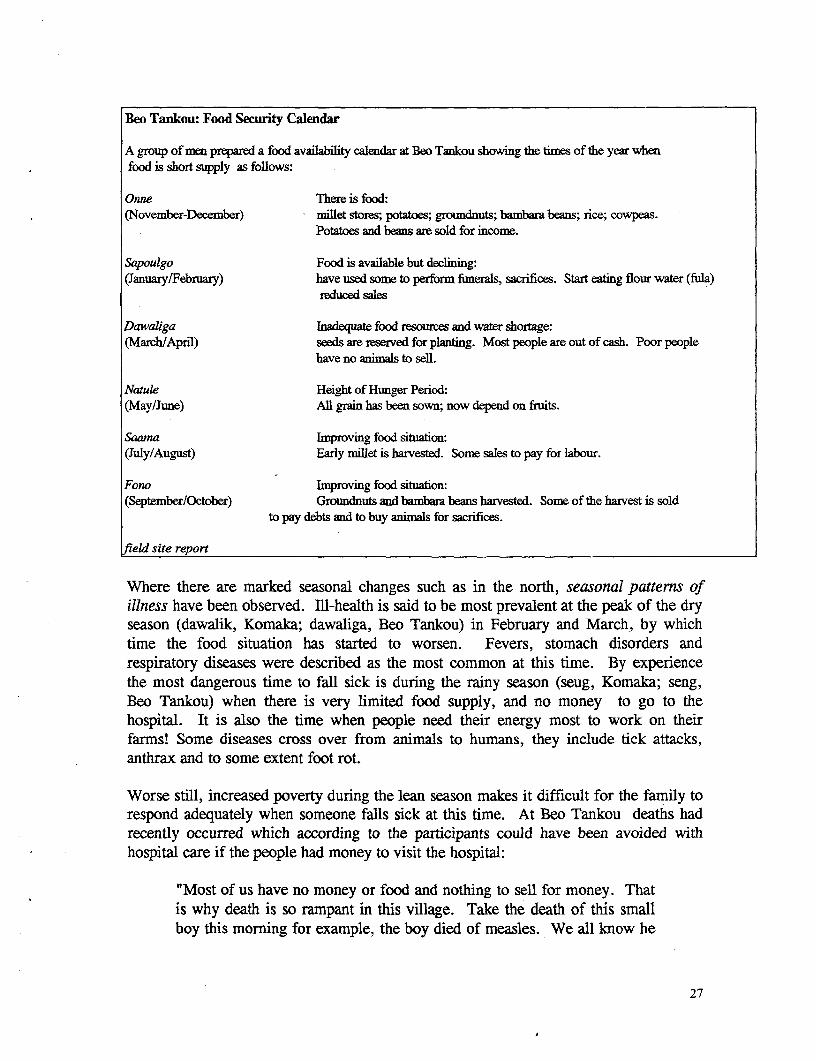
Beo Tankou: Food Security Calendar
A group of men prepared a food availability calendar at Beo Tankou showmig the times of the year whenfood is short supply as follows:
Onne There is food:(November-December) millet stores; potatoes; groundnuts; bambara beans; rice; cowpeas.
Potatoes and beans are sold for income.
Sapoulgo Food is available but declining:(January/February) have used some to perform funerals, sacrifices. Start eating flour water (fula)
reduced sales
Dawaiga Inadequate food resources and water shortage:(March/April) seeds are reserved for planting. Most people are out of cash. Poor people
have no animals to sell.
Natule Height of Hunger Period:(May/June) All grain has been sown; now depend on frtits.
Saama Improving food situation:(July/August) Early millet is harvested. Some sales to pay for labour.
Fono Improving food situation:(September/October) Groundnuts and bambara beans harvested. Some of the harvest is sold
to pay debts and to buy animals for sacrifices.
field site report
Where there are marked seasonal changes such as in the north, seasonal patterns ofillness have been observed. Ill-health is said to be most prevalent at the peak of the dryseason (dawalik, Komaka; dawaliga, Beo Tankou) in February and March, by whichtime the food situation has started to worsen. Fevers, stomach disorders andrespiratory diseases were described as the most common at this time. By experiencethe most dangerous time to fall sick is during the rainy season (seug, Komaka; seng,Beo Tankou) when there is very limited food supply, and no money to go to thehospital. It is also the time when people need their energy most to work on theirfarms! Some diseases cross over from animals to humans, they include tick attacks,anthrax and to some extent foot rot.
Worse still, increased poverty during the lean season makes it difficult for the family torespond adequately when someone falls sick at this time. At Beo Tankou deaths hadrecently occurred which according to the participants could have been avoided withhospital care if the people had money to visit the hospital:
"Most of us have no money or food and nothing to sell for money. Thatis why death is so rampant in this village. Take the death of this smallboy this morning for example, the boy died of measles. We all know he
27
could have been cured at the hospital. But the parents had no money andso the boy died a slow and painful death not out of measles but out ofpovertyl".(A group of men at Beo Tankou, 1994).
In the middle and coastal belt double maxima rainfall areas of communities such asButre, Kpando Gabi, Derma and Dekpor Horme, there is apparently littledifferentiation in the seasonal occurrence of sickness. Cholera and diarrhoea seem topeak during the 'time of mangoes' in the minor rainy season, but other diseases occurall-year round.
2.3.2 Long-Term Trends in Poveny
Long-term trends in the rural sites
The predominant factors in the perceptions of long-term trends of rural populations areenvironmental. For poor urban populations they relate to the labor market and theperceived availability of work and demand for informal sector products and services.
The list of aspects of decline in environmental conditions in rural areas included: wateraccess (declining levels of the water table, decreasing quantity, quality and duration ofstream flow); availability and quality (fertility) of farm land and pasture for animals;access to a range of products from common property areas, for both own consumptionand sale for income (including fuelwood, medicines, foraged foodstuffs such as snails,fruits, mushrooms, bushmeat, and other non-timber forest produce). In the northernsavannah communities the key elements of environmental change were perceived to bedeclining soil fertility due to decreasing fallow periods, declining water resources asoutlined above and a shortening of the rainy season, combined with less predictability.
In the relatively more agriculturally abundant communities of the middle and coastal belt,important changes have taken place in crop mixes in response to environmental degradation,as well as market demands. Some of the changes have however been introduced viagovernment policy, as in the case of rice production following the Afife dam at DekporHorme, and tomatoes at Derma. At Dekpor Horme sugarcane, oil palm, agor trees andbamboo have been replaced in significance by cassava as the main reserve or stress periodcrop, especially for women, after the construction of the dam led to large scale alienation ofvillage lands. It is important to note that before the dam the number of significant cashcrops was greater for both men and women. Though the middle belt communities have arelatively better situation with regards to food production than we find in northern Ghana,increasing problems with soil fertility pose a threat to food secunty. At Butre a time linediscussion with a Mad. Sefua oII natural resources revealed that soil fertility had droppedfrom a perceived high level to a low point, since the 1940s. She indicated the loss of cropvariety that has accompanied this process as follows:
28
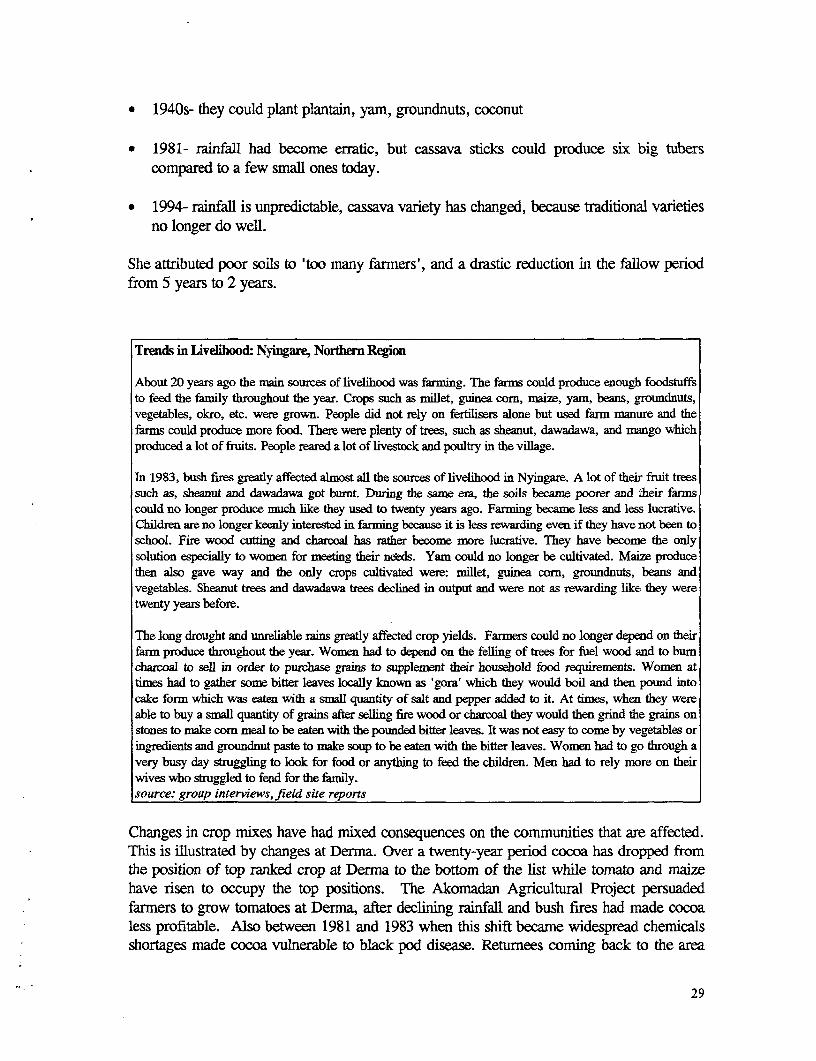
* 1940s- they could plant plantain, yam, groundnuts, coconut
* 1981- rainfaU had become erratic, but cassava sticks could produce six big tuberscompared to a few small ones today.
* 1994- rainfall is unpredictable, cassava variety has changed, because traditional varietiesno longer do well.
She attributed poor soils to 'too many farmers', and a drastic reduction in the fallow periodfrom 5 years to 2 years.
Trends in Liveihood: Nyingare, Norhern Region
About 20 years ago the man sources of livelihood was farming. The farms could produce enough foodstuffsto feed the family throughout the year. Crops such as millet, guinea corn, maize, yam, beans, groundnuts,vegetables, okro, etc. were grown. People did not rely on fertilisers alone but used farm manure and thefarms could produce more food. There were plenty of trees, such as sheanut, dawadawa, and mango whichproduced a lot of fruits. People reared a lot of livestock and poultry in the village.
In 1983, bush fires greatly affected almost all the sources of livelihood in Nyingare. A lot of their fiuit treessuch as, sheanut and dawadawa got bumt. During the same era, the soils became poorer and their farmscould no longer produce much like they used to twenty years ago. Farming became less and less lucrative.Children are no longer keenly interested in farming because it is less rewarding even if they have not been toschool. Fire wood cutting and charcoal has rather become more lucrative. They have become the onlysolution especially to women for meeting their needs. Yam could no longer be cultivated. Maize producethen also gave way and the only crops cultivated were: millet, guinea corn, groundnuts, beans andvegetables. Sheanut trees and dawadawa trees declined in output and were not as rewarding like they weretwenty years before.
The long drought and unreliable rains greatly affected crop yields. Farmers could no longer depend on theirfarm produce throughout the year. Women had to depend on the felling of trees for fuel wood and to bumcharcoal to sell in order to purchase grains to supplement their household food requirements. Women attimes had to gather some bitter leaves locally known as 'gora' which they would boil and then pound intocake form which was eaten with a small quantity of salt and pepper added to it. At times, when they wereable to buy a small quantity of grains after selling fire wood or charcoal they would then grind the grains onstones to make com meal to be eaten with the pounded bitter leaves. It was not easy to come by vegetables oringredients and groundnut paste to make soup to be eaten with the bitter leaves. Women had to go through avery busy day struggling to look for food or anything to feed the children. Men had to rely more on theirwives who struggled to fend for the family.source: group interviews,field site reports
Changes in crop mixes have had mixed consequences on the communities that are affected.This is illustrated by changes at Derma. Over a twenty-year period cocoa has dropped fromthe position of top ranked crop at Derma to the bottom of the list while tomato and maizehave risen to occupy the top positions. The Akomadan Agricultural Project persuadedfarners to grow tomatoes at Derma, after declining rainfall and bush fires had made cocoaless profitable. Also between 1981 and 1983 when this shift became widespread chemicalsshortages made cocoa vulnerable to black pod disease. Returnees coming back to the area
29
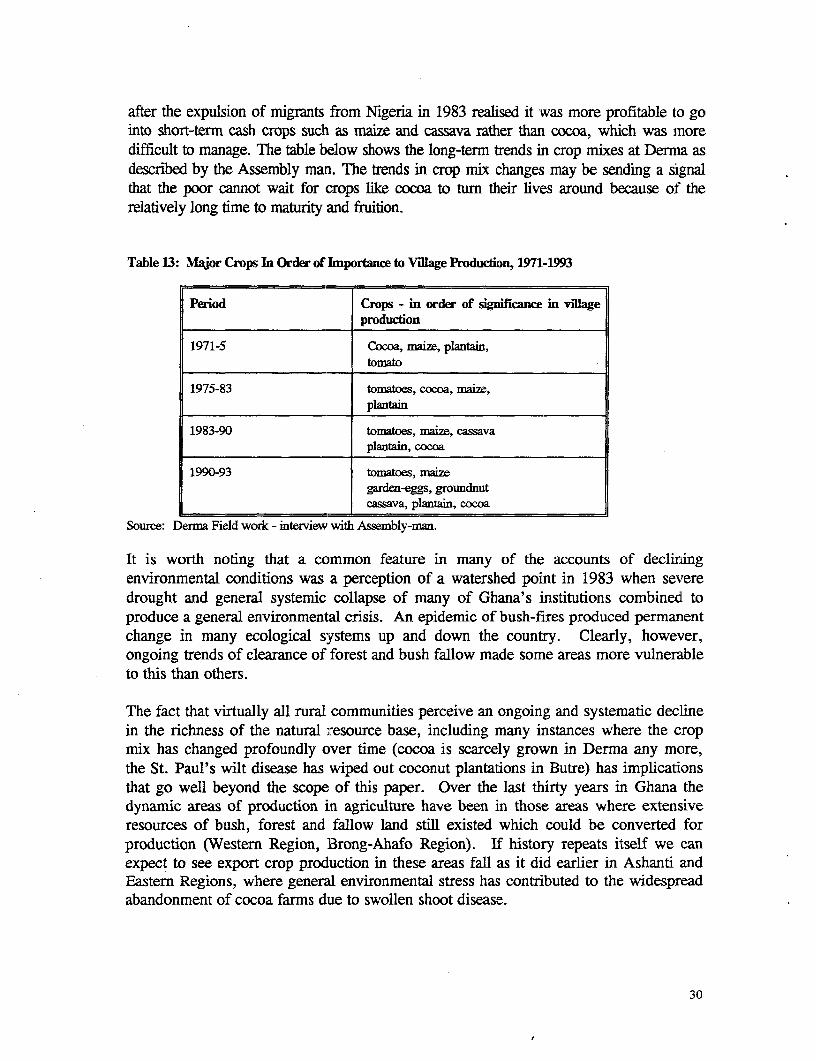
after the expulsion of migrants from Nigeria in 1983 realised it was more profitable to gointo short-term cash crops such as maize and cassava rather than cocoa, which was moredifficult to manage. The table below shows the long-term trends in crop mixes at Derma asdescribed by the Assembly man. The trends in crop mix changes may be sending a signalthat the poor cannot wait for crops like cocoa to turn their lives around because of therelatively long time to maturity and friition.
Table 13: Major Crops In Order of Inportance to Village Production, L971-L993
Period Crops - in order of significance in villageproduction
1971-5 Cocoa, maize, plantain,tomato
1975-83 tomatoes, cocoa, maie,plantain
1983-90 tomatoes, mnaiz, cassavaplantain, cocoa
1990-93 tomatoes, maizegarden-eggs, groundnutcassava, plantain, cocoa
Source: Derma Field work - interview with Assembly-man.
It is worth noting that a ccommon feature in many of the accounts of decliningenvironmental conditions was a perception of a watershed point in 1983 when severedrought and general systemic collapse of many of Ghana's institutions combined toproduce a general environmental crisis. An epidemic of bush-fires produced permanentchange in many ecological systems up and down the country. Clearly, however,ongoing trends of clearance of forest and bush fallow made some areas more vulnerableto this than others.
The fact that virtually all rural communities perceive an ongoing and systematic declinein the richness of the natural resource base, including many instances where the cropmix has changed profoundly over time (cocoa is scarcely grown in Derma any more,the St. Paul's wilt disease has wiped out coconut plantations in Butre) has implicationsthat go well beyond the scope of this paper. Over the last thirty years in Ghana thedynamic areas of production in agriculture have been in those areas where extensiveresources of bush, forest and fallow land still existed which could be converted forproduction (Western Region, Brong-Ahafo Region). If history repeats itself we canexpect to see export crop production in these areas fall as it did earlier in Ashanti andEastern Regions, where general environmental stress has contributed to the widespreadabandonment of cocoa farms due to swollen shoot disease.
30
Another long-term trend which was highlighted in some areas was a tendency toweakening of the bonds of local social institutions of kinship and community. InNyingare in the Northern Region, for example, focus groups among women revealed aperception that ten years ago there was strong social cohesion in the village. Menorganized themselves in groups through communal labor to assist each other to buildand roof houses. Women supported each other to do farm work such as sowing,weeding and harvesting. A woman who had recently given birth to a baby was alwayssupported by older women with firewood and young girls to care for their babies andeven to give treatment to the babies whenever they fell sick. The individual families triedto support each other. Women would move in groups in search of food to feed theirchildren. They went to the bush in groups to cut fire wood and to burn charcoal to sell.Respect and authority was still given to the chief and his elders. Community solidarity wasstill expressed through mutual support and assistance for one another. Decline in thetraditional institutional framework for such reciprocal anrangements was a fear expressed inother sites in the north associated with increasing levels of temporary and long-term labourmigration. Such changes clearly create increased vulnerability for the poorer sections ofsuch communities, by weakening their 'social assets' in terms of networks of kinship andcommunity through which they could mobilise claims on food and labour from theirneighbours.
Long-term trends in urban sites
In urban areas, local analysis of long-term trends in livelihoods indicate that people feelthat there has been a continuing downward slide in many types of business, whichstarted around 1988, and their standards of living are falling. This followed on aperiod of generally perceived improvement and recovery from around 1983 to 1988.The following reasons were offered for this change: low levels of demand for manyinformal sector products and services; an increase in the numbers of people seeking tosustain livelihoods through urban self-employment due to factors such as retrenchmentfrom govemment service, parastatals and the private sector, or large numbers ofGhanaians returning from abroad due to the poor condition of many economies in theregion, such as Ivory Coast, Liberia, Togo and Nigeria. Paradoxically someinformants perceived very substantial increases in both the amount of activity in manyurban trades, and the level of unemployment. This was partly explained by the factthat many categories of urban worker were seen as severely under-employed, and thatsome categories were not perceived as in employment at all (for example apprentices)because they were working without salary in order to develop skills.
To illustrate these trends, in East Maamobi, Almost all the participants indicated thatthere has been a decline in their business since 1988, with a sharp drop in 1993. Somewomen traders explained that their business improved after 1983 when the situation was theworst they could remember. Subsequently conditions improved steadily till about 1988, butby 1990 the decline in their business started again. They were unable to give anyquantitative indicators of this pattern, as many of them do not keep written records on theirbusiness. However statements such as 'at first I could sell this basketful of palmfruit before
31
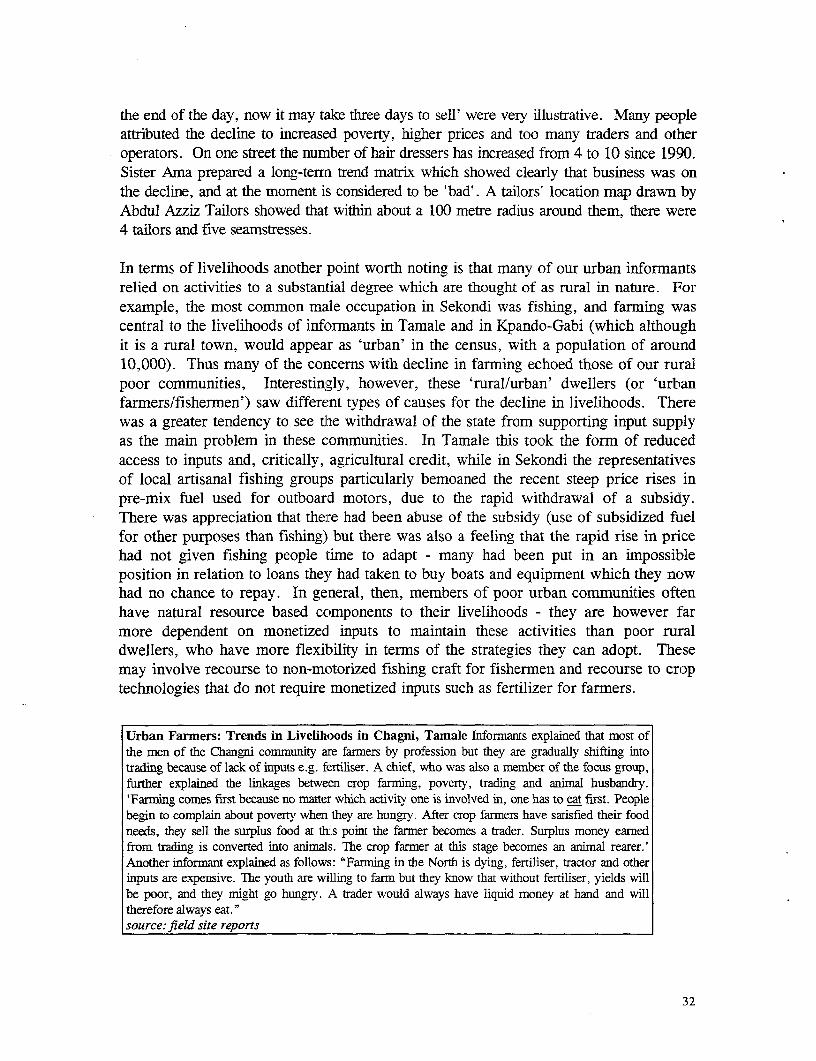
the end of the day, now it may take three days to sell' were very illustrative. Many peopleattributed the decline to increased poverty, higher prices and too many traders and otheroperators. On one street the number of hair dressers has increased from 4 to 10 since 1990.Sister Ama prepared a long-terrn trend matrix which showed clearly that business was onthe decline, and at the moment is considered to be 'bad'. A tailors' location map drawn byAbdul Azziz Tailors showed that within about a 100 metre radius around them, there were4 tailors and five seamstresses.
In terms of livelihoods another point worth noting is that many of our urban informantsrelied on activities to a substantial degree which are thought of as rural in nature. Forexample, the most common male occupation in Sekondi was fishing, and farming wascentral to the livelihoods of informants in Tamale and in Kpando-Gabi (which althoughit is a rural town, would appear as 'urban' in the census, with a population of around10,000). Thus many of the concerns with decline in farming echoed those of our ruralpoor communities, Interestin!gly, however, these 'rural/urban' dwellers (or 'urbanfarmers/fishermen') saw different types of causes for the decline in livelihoods. Therewas a greater tendency to see the withdrawal of the state from supporting input supplyas the main problem in these communities. In Tamale this took the form of reducedaccess to inputs and, critically, agricultural credit, while in Sekondi the representativesof local artisanal fishing groups particularly bemoaned the recent steep price rises inpre-mix fuel used for outboard motors, due to the rapid withdrawal of a subsidy.There was appreciation that there had been abuse of the subsidy (use of subsidized fuelfor other purposes than fishing) but there was also a feeling that the rapid rise in pricehad not given fishing people time to adapt - many had been put in an impossibleposition in relation to loans they had taken to buy boats and equipment which they nowhad no chance to repay. In general, then, members of poor urban communities oftenhave natural resource based components to their livelihoods - they are however farmore dependent on monetized inputs to maintain these activities than poor ruraldwellers, who have more flexibility in terms of the strategies they can adopt. Thesemay involve recourse to non-motorized fishing craft for fishermen and recourse to croptechnologies that do not require monetized inputs such as fertilizer for farmers.
Urban Farmers: Trends in Livelihoods in Chagni, Tamale Informants explained that most ofthe men of the Changni comnmunity are fanners by profession but they are gradually shifting intotrading because of lack of inputs e.g. fertiliser. A chief, who was also a member of the focus group,further explained the linkages between crop farming, poverty, trading and animal husbandry.'Farming comes first because no matter which activity one is involved in, one has to eat first. Peoplebegin to complain about poverty when they are hungry. After crop farmers have satisfied their foodneeds, they sell the surplus food at this point the farmer becomes a trader. Surplus money earnedfrom trading is converted into animals. The crop farmer at this stage becomes an animal rearer.'Another informant explained as follows: "Farming in the North is dying, fertiliser, tractor and otherinputs are expensive. The youth are willing to farm but they know that without fertiliser, yields willbe poor, and they might go hungry. A trader would always have liquid money at hand and willtherefore always eat."source: field site reports
32
In some of the communities evidence was found of retrenchees who had suffered rapiddeclines in living standards, moving from the local 'rich' category to the mainstreampoor. One retrenchee interviewed in Breman-Asikuman in the Central Region indicatedthat since she lost her job with the Cocoa Board she had become totally dependent onbrewing the local gin (akpeteshie) for income. She was no longer able to afford to buyclothing for herself or her children (rated as her top expenditure item beforeretrenchment) or pay school fees, and was having difficulty meeting essential medicalexpenses. She said her colleagues who have been redeployed have either resorted topetty trading or farming, or have traveled outside the area to look for employment.Retrenchment was seen as having negative effects at the community level in terms ofreduced market opportunities, job avenues for the youth and an increase in the rate ofcrime such as theft.
Social cohesion again emerged as a concern in the urban north as it had in the ruralnorth. The urban community in Chagni was the only community in the study whichwas heavily affected by the ethnic conflict between members of the Konkomba andDagomba ethnic groups which erupted in northern Ghana in 1993 6. The box belowsummarizes the views from that community. Two points should be noted - this is aviewpoint from one side of the conflict, the Dagombas - it was not possible (in partbecause of the conflict) for any work to be done involving either side in the easternparts of the Northern Region where the conflict was severe. The second point thatshould be noted is that the community elders' concern with issues of social cohesion isunderstandable given the recent experience of this conflict. People are aware thatGhana is moving into a new phase with the reintroduction of democratic forms ofgovernance which is perceived in poor communities as creating dangers as well asopportunities.
In conclusion, views of trends in rural communities tend to focus on environmentalissues such as declining access and quality of water, declining soil fertility anddeclining common property resources for the vulnerable to fall back on in times ofcrisis. The view of the urban poor relates in more detail to the evolution of policyframeworks in the era of adjustment. While a considerable improvement is appreciatedto have occurred in the early phase (from 1983 to 1988) there is a general perceptionthat opportunities for the urban poor have been becoming more constrained in theperiod since the last six to seven years. In all communities there is some concern overwhat is perceived to be a very poor situation in relation to assistance with credit fortrading and productive activities. In the urban areas this is perceived as a decliningtrend whereas in some rural areas this seems to be perceived more as a continuation ofan unsatisfactory situation.
6 For those not familiar - this was an extremely serious conflict set against the comparatively peacefulhistory which Ghana has enjoyed. Estimates of the casualties vary widely but generally cite figures of wellover a thousand dead.
33
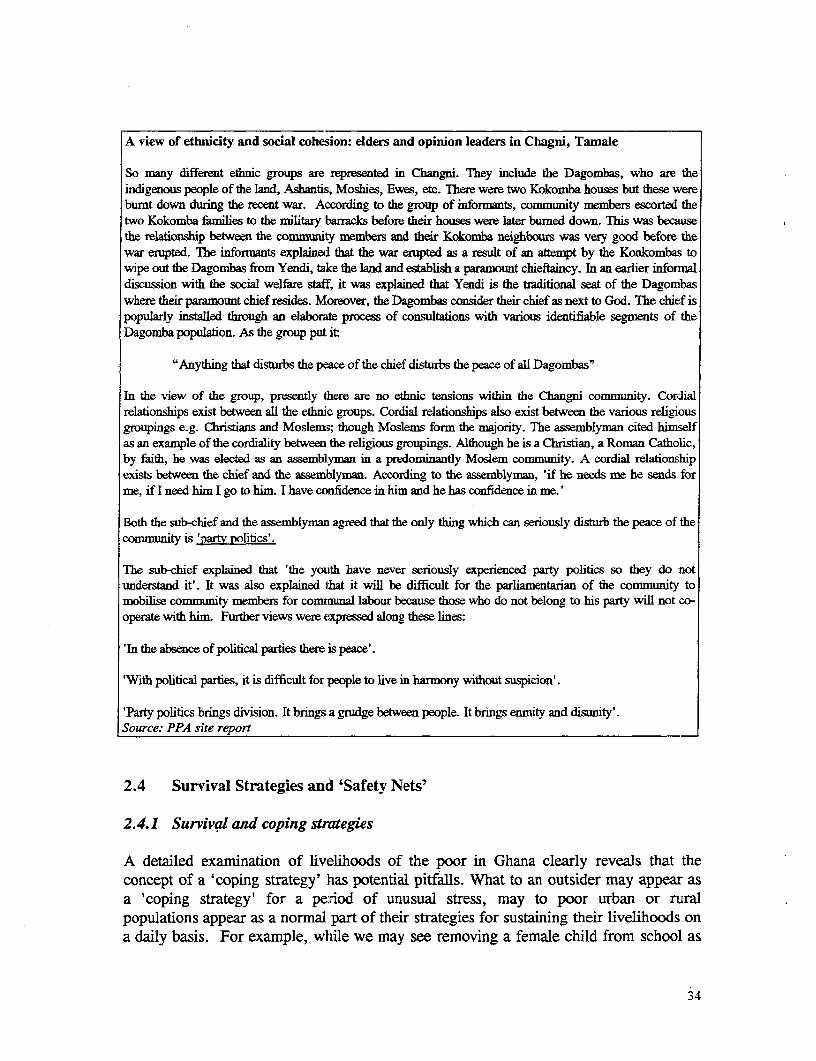
A view of ethnicity and social cohesion: elders and opinion leaders in Chagni, Tamale
So many different ethnic groups are represented in Changni. They include the Dagombas, who are theindigenous people of the land, Ashantis, Moshies, Ewes, etc. There were two Kokomba houses but these wereburnt down during the recent war. According to the group of informants, commumnty members escorted thetwo Kokomba failies to the nilitary barracks before their houses were later burned down. This was becausethe relationship between the community members and their Kokomba neighbours was very good before thewar erupted. The informants explained that the war erupted as a result of an attempt by the Konkombas towipe out the Dagombas from Yendi, take the land and establish a paramount chieftaincy. In an earlier informaldiscussion with the social welfare staff, it was explained that Yendi is the traditional seat of the Dagombaswhere their paramount chief resides. Moreover, the Dagombas consider their chief as next to God. The chief ispopularly installed through an elaborate process of consultations with various identifiable segments of theDagomba population. As the group put it:
"Anything that disturbs the peace of the chief disturbs the peace of all Dagombas"
In the view of the group, presently there are no ethnic tensions within the Changni community. Cordialrelationships exist between aU the ethnic groups. Cordial relationships also exist between the various religiousgroupings e.g. Christians and Moslems; though Moslems form the majority. The assemblyman cited himselfas an example of the cordiality between the religious groupings. Although he is a Christian, a Roman Catholic,by faith, he was elected as an assemblyman in a predominantly Moslem community. A cordial relationshipexists between the chief and the assemblynan. According to the assemblyman, 'if he needs me he sends forme, if I need him I go to him. I have confidence in him and he has confidence in me.'
Both the sub-chief and the assemblymarn agreed that the only tbing which can seriously disturb the peace of thecommunity is 'partv politics'.
The sub-chief explained that 'the youth have never seriously experienced party politics so they do notunderstand it'. It was also explained that it will be difficult for the parliamentarian of the community tomobilise community members for comraunal labour because those who do not belong to his party will not co-operate with him. Further views were expressed along these lines:
'In the absence of political parties there is peace'.
'With political parties, it is difficult for people to live in harmony without suspicion'.
'Party politics brings division. It brings a grudge between people. It brings enmity and disunity'.Source: PPA site report
2.4 Survival Strategies and 'Safety Nets'
2.4.1 Survival and coping strategies
A detailed examination of livelihoods of the poor in Ghana clearly reveals that theconcept of a 'coping strategy' has potential pitfalls. What to an outsider may appear asa 'coping strategy' for a period of unusual stress, may to poor urban or ruralpopulations appear as a normal part of their strategies for sustaining their livelihoods ona daily basis. For example, while we may see removing a female child from school as
34
a 'coping strategy', to the family concerned it may appear as a fairly routinewithdrawal of what was in any case a 'luxury' item of expenditure. Nonetheless,certain defined strategies can be identified which apply to people's attempts to copewith the consequences of negative changes over times (seasonal stress, temporary'shocks', long-term negative trends). Both the negative impacts, and the strategies thatevolve to cope with them may occur at various levels: household, individual orcommunity. For example, the loss of a member of the household labor force duringthe farming season to illness, with accompanying medical expenses, constitutes a'shock' at the level of the household's livelihood, with no necessary broader impact. Adrought year impacts on a whole community, though the responses it provokes may beorganized at various levels, including the household, the wider kin group and thecommunity.
The coping strategies we recorded in the course of the three phases were very diverse.Some of the more common elements included:
- For the rural north: Out-migration in search of employment; sending children tostay with kin in times of stress; using 'famine foods' gathered from the bush.
- For the rural south: Reducing expenditures (taking children out of school); changesin conjugal patterns (contracting informal unions due to inability of young men tomake bridewealth payments).
* For the urban south: Reducing expenditures, including relying increasingly oncooked food sellers, withdrawing children from school; diversifying income sources
An important point to note on coping strategies, is that different coping strategies at theindividual level are not available equally to all categories of the population. Forexample, market-based fallback mechanisms such as migration from the rural north aremore available to young men than to many women, children or the elderly.7 Theremoval of the young man may even have negative effects for the livelihoods of thoseleft behind (depending on the level of transfers received).8
Where a common 'fallback' mechanism appears to have negative consequences formore vulnerable sections of the population consideration needs to be given to possiblealternatives. For example, over the last fifteen years some areas of the Upper East
7 Although there was a perception in many communities that femnale migration was increasing. This isbacked up by studies carried out of girls, predominantly from the Northern Region, who migrate to Accrato work as market porters, frequently living on the streets. See Bearing the Weight: The Kayayoo,Ghana's Working Girl Child Agarwal, Attah, Apt, Grieco, Kwakye and Turner, paper presented to theUnicef Conference on the Girl Child January, 1994.s For discussions of the effects of differential market access by gender on fallback mechanisms for menand women see Ann Whitehead, "I'm Hungry, Mum: the Politics of Domestic Budgeting"in OfMarriageand the Market ed. Young, Wolkowitz and McCullagh, 1981. Also Whitehead, 1987, DistributionalEffects of Cash Crop Innovation: The Peripherally Commercialised Farmers of North East Ghana.
35
Region have diversified with considerable success into vegetable farming as a dry-season activity, providing an alternative source of income which may firstly, reducemale out-migration, and secondly, provide income on a broader basis within thecommunity. Provision of dry-season water sources to support this kind of activity wasthe main priority need emerging from the rural communities in the Upper Regions.Assistance of this kind may strengthen community-based fallback mechanisms (local'safety-nets') through encouraging community solidarity and cohesion.
The adaptations which the urban poor reported included an increasing recourse tocooked food sellers, which prove cheaper than attempting to cook at home. It was alsoreported that it was easier to limit expenditure on quantity by using cooked food sellers,perhaps an indication that the hospitality norms of traditional Ghanaian cultures makethe consumption of regular meals in densely crowded residential spaces sociallyuncomfortable. An increasing tendency to pay for both goods and services 'byinstallments' was also reported..
By all accounts many of the long-standing coping strategies that are known in resourcepoor communities are becoming less accessible for combating stress periods. This isexplained by the fact that most of these strategies are themselves under threat becauseof worsening ecological conditions and the escalating cost of living. The situationappears to be more grave in northern Ghana, where in communities such as Beo Tankothe consumption of wild foods forms a regular part of strategies of dry-season survival,though one should not under--estimate the looming deprivation in other parts of thecountry.
Coping strategies in the middle belt and the coastal zones have suffered as a result ofenvironmental degradation. T:ree crops at Butre have lost their significance as 'fallback' resources, with the destruction of coconut trees from Cape St. Paul Coconut Wiltdisease. Oil palm trees that have been planted in replacement mostly by men, have notstarted fruiting in the majority of cases. With this disaster women have also lost theopportunity to earn income from coconut oil processing, and all the economic by-products that come with coconut processing; the coconut technology is likely to be lostto the subsequent generations of men and women. In forest zone communities such asDerma the income-generation and nutrition benefits of some gathered items of minorforest produce have become increasingly less available (for example, snails which werecommonly gathered for sale in parts of the year in Derma). This follows a generalpattern where degradation of common property or open access resources tends to have aheavy impact on the poor who are disproportionately dependent on these resources dueto lower levels of access to land and labour for farming.
2.4.2 Formal and informal safety nets
In several instances a criteria for identifying those who were not poor, wealthy or highstatus was their capacity to help kdn or 'help the community'. By contrast poverty insome instances (especially one of the workshop sites, Darko) was associated with
36
'dependency' on others for survival. In larger, more ethnically diverse, and complexsituations the network of support individuals can mobilize is not in any simple senselinked to 'the community' (viewed as a homogenous social group bound by commonnorms and carrying out some activities in common). One area where assistance fromkin was consistently cited as critical was in accessing social services - especiallyemergency healthcare.
External sources provided valued, but relatively rare assistance in many of the fieldsites. Best placed were those communities with an ongoing NGO program, such asAfrangua, and Koforidua (World Vision), or Komaka (Action Aid). On a lesssystematic basis the Baptist and Catholic churches had provided assistance in two crisisyears (1983 and 1992) in the community of Sombo (Upper West Region).Governmental safety nets were not mentioned by any informants as being in any wayrelevant for the poorest members of these communities. Our research suggests that theendemic problems of food security in northern Ghana in particular have never receivedthe serious attention they merit. While all communities surveyed prefer the prospect ofassistance to develop the productivity and security of their livelihoods to 'safety net'kinds of assistance, the severity of problems experienced by the poor in the northsuggests a need for a more robust response in terms of an ongoing institutionalframework for addressing the worst affected social groups and areas.
2.5 Local Perceptions of Service Quality and Access in the Health Sector
Many small rural communities in Ghana have very low levels of access to modernhealth facilities. Despite the already low level of coverage, there are situations in whichhealth services have been closed down or withdrawn in the case of mobile services.9
As a result people in the rural communities rely extensively on traditional healthproviders such as traditional birth attendants (TBAs), herbalist/bone-setters, fetishpriests drug peddlers and spiritualists. Close proximity to modern health facilities in theurban centres has considerably reduced dependence on these informal sources, thoughthere are certain categories of illness that people prefer to take to a traditional healer.'0Examples were given of situations in which relatives had withdrawn their patients fromhospital to be taken to traditional healers.
Everywhere the selection of a health care provider is contingent upon many factors, andas a result visits to a health facility tend to follow a sequence. A visit normally startswith the most accessible or least expensive of the facilities available, though otherconsiderations such as type of illness rather than cost and convenience may influencethe sequence. Sequencing of visits to the health care facility commonly takes the
9 An ante-natal clinic at Beo Tankou has been terminated
'° . In northern Ghana, for example, fractures are always taken to traditional practitioners - 'bone-setters'.In Central Region epileptics were taken to local spiritualist churches in search of a cure.
37
following form. Many people depend on home remedies or visits to the herbalist as thefirst step in the treatment of illness. When it becomes critical they will proceed to thedoctor or the spiritualist / fetish priest, depending on the local classification of theillness.
The following section summarises local views on different types of healthcare services:
* Home remedies: For the average person cut off from a clinic or chemist, homeremedies are affordable and available. Both men and women learn about medicinalplants from their close relatives; the women are particularly familiar with herbs thatcure childhood diseases, and female reproductive disorders. Home remedies includethe use of herbs, peddled drugs, and good nutritious food. But the knowledge islimited and not effective for very sick people. Home remedies are thus seen moreas for first aid and minor ailments.
* Herbalist: The herbalist is always available. Though knowledge of medicinal treesand other plants is quite extensive in the community, the herbalist is recognised forhis/her special skills in maldng them work. Their speciality in the north is bone-setting. But times have changed and some people have become sceptical aboutherbs, commenting that "traditional medicines have lost their potency, people haveforgotten how to make them work" (Group of men, Beo Tankou, 1994). Threats tothe availability of herbs were also raised as an issue. Evidence of genetic erosion isgrowing due to difficulties that have been observed in finding certain varieties ofherb plant species. It is widely feared in the rural communities one day that theseplants would disappear altogether. Apart from the problems with the naturalresource base, there is concern that the herbalist is no longer honest, and reliable.For the sake of profit, he is now prepared to dupe his patients. The excessivecommercialisation of the vocation is believed to have reduced the potency of herbs.In the words of an old man at Komaka, Bawku, "At first they used to charge only afowl. Now they take at least a fowl, guinea fowl, and C2,000."
* Fetish priest/soothsayer: 'They are available in the community or neighbouringcommunities. They advise on what sacrifices to make in order to get well, orovercome other kinds of misfortune (apart from ill-health).
* Spiritualist: The place of a spiritualist rivals that of the herbalist or fetish priest inmany ways. They are more commonly found in the south than in the north ofGhana. Many derive their strength from Christian teaching, though in practice thereare overlaps between their spiritualism, occultism and fetish practices. Sicknesscaused by witchcraft is said to be the speciality of the spiritualist. At Butre theNakaba Gardens where Maame Osofo casts out demons is highly rated in thesequencing of health care visits. Like the herbalist and fetish, spiritualists are easilyaccessible and also very flexible in their charges. The women at Butre doacknowledge however that there are diseases that the Nakaba Gardens cannot cure.
38
* Clinic: It is widely appreciated that modem health care facilities such as clinicshave powerful treatment for very sick people. All over, women and menacknowledge that child mortality for certain diseases such as measles has reduced.Similarly death in pregnancy and child birth has gone down compared to the past.Illnesses such as hernia can now be cured by surgery. In spite of the high regard forhospital treatment, patients obviously do not always take this route. Some of thereasons that are given are cited below. People are discouraged from going to theclinic because of the high costs involved. In addition one has to pay beforetreatment. Whether they get well or not, subsequent charges are not reduced. Fromthe north there were complaints that non-literate and poor patients are shown nosympathy at the clinics: ".. nurses at each point want to take money from you... .Itis not first come first served or treated but those who have money get treatment,and those who do not have money die ..... The pharmacists at the clinics givepatients less quantity of the drug than the doctor has prescribed and sell what theyshould have given to you." (A group of 13 women at Komaka, 1994). But theseexperiences are not necessarily universal in the Ghanaian context. Elsewhere in thesouth the health staff are described as pleasant and hardworking, though patientshave to wait too long to see a doctor.
3 Drug seller/chemists: In the case of minor ailments the drug seller can givemedicine for quick relief (e.g. headache). The drug seller is usually a peddler, hehas a mobile service and often has no formal knowledge of drugs or doses, exceptinformation he has picked up on the job. He is seen to be good because he sellsmedicine on credit. But the drug seller can be dishonest about his medicalknowledge and treatment: "There is danger of overdose because they do not explainor inform mothers of the correct dosage ... If you say you have stomach-ache andhe has not got the medicine, he will give you one for headache because it is themoney he is after." (13 women at Komaka, 1994).
In the urban centres, chemists or pharmacists gain a very good reputation if they arekind and understanding about their patients' problems. Their kindness is expressed interms of selling prescriptions to people in small batches, or sometimes allowing peopleto pay for the full prescription by instalment. This raises very serious problems withregards to drug abuse and the complications that arise as a result. When people cannotafford the prescription they may simply abandon it.
With the introduction of the health sector reforms -- comprising the Primary HealthCare (PHC) program and the Expanded Program on Immunization (EPI), patients arenow expected to share in the costs of health delivery. Drug costs are now beingrecovered in full (through the cash-and-carry system), 1 and patients are required tocontribute towards the cost of consultations as well.
"Indeed, drug prices are frequently marked up in cash-and-carry pharmacies to cover inflation and pettylosses.
39
In general, the most accessible health options in the communities studied are thoseunder private control. In urban areas, where they are more widely available,drugstores tend to be the first choice of the sick. In spite of assurances given prior tothe introduction of the cash-and-carry system, the research teams were consistently toldthat private drugstores tend to be better stocked than hospital pharmacies are.Sometimes referred to as "'doctors" 12 by community members, drugstore-keeperstypically dispense orthodox rnedication without prescription, parceling out drugs inwhatever combinations and quantities the self-prescribing customer requests and is ableto afford.13 In the view of local populations the male drug-store keeper is oftenincorrectly perceived as having a higher level of diagnostic skill than the female clinicnurse. At home, nurses are consulted by local residents for advice and treatment (insome cases their informal assistance in the capacity of community members appearedmuch more highly appreciated than the services of the formal institutions for whichthey worked).
In rural communities, particularly in the northern savannah (where poverty is moreintense and orthodox/ quasi-conventional healthcare is less readily available), herbstend to be the first option in sickness. Northern communities also rely on remarkablycompetent "bone-setters" to restore fractured limbs -- we would hasten to add,however, that this is done without the benefit of anesthesia! Common in most ruralareas are traditional birth attendants -- or TBAs -- who deliver babies, using indigenousskills. It is also common for the sick to combine treatments from a variety of sources(e.g., exorcism with herbal preparations; or herbs with conventional medicines boughtfrom drugstores). Even hospital patients will sometimes combine their doctor'streatment with herbal applications.
The least orthodox categories (such as the "spiritual churches" and herbalists) are mostpatronized by the ultra-poor and the oldest members of society -- who also tend to havethe most traditional lifestyles. The study also revealed that while these groups are themost dominant users, many other rural households use the services of such infornalhealth delivery agencies during periods of financial hardship. There are several reasonsfor the higher utilization of informal healthcare options, including:
the generally superior accessibility of such healthcare providers (not only do theytend to be locally resident whereas orthodox facilities are only available in thelarger towns; bureaucracy and waiting times are negligible compared with public
' 2This may explain why the latest round of the Ghana Living Standards Survey is reporting incrediblyhigh levels of professional consultations.
13The Techiman team reports, from interviews with drugstore managers, that drug abuse is increasing inthe area. Common names for popular stimulants include "Mike Tyson" and "Carl Lewis". It is alsowidely recognized that antibiotics (especially ampicillin), typically purchased from local drugstores inshort doses, are used by the public to deal with all manner of health problems, from small cuts toheadaches!
40
hospitals, where one often has to queue for three to five hours before being attendedto);
* the lower costs involved (in response to a question about comparative costs, wewere told by a focus group of men: "spiritual churches charge no fees; one simplygives what one can when one can");
* the flexibility of payment (herbalists, TBAs, "bone-setters" and "spiritual healers"are more likely to accept deferred payments or payments in kind; this is particularlyappreciated during periods of extreme hardship, when cash is not easily available);and
* the additional services included in the packages of some alternative healthcareproviders; in the north, for example, TBAs are reported to be providing postnatalcare -- including bathing the baby and shaping its head! Also in the north, thehostile attitude of public sector nurses and paramedical personnel was mentioned asa barrier to access.
But for a few exceptions (of some state-trained TBAs and certain northern hospitalswhich have incorporated the services of bone-setters into the mainstream healthcaredelivery system), informal healthcare providers operate in complete isolation of theMinistry of Health. Hospital authorities have frequently reported serious complicationsarising from erroneous diagnoses, wrong doses and superstitious treatmentsadministered by informal healthcare providers.
At the drugstore level, access to credit is normally dependent on one's perceived creditrating. Formal sector workers and people with reasonably comfortable residentrelatives have least difficulty accessing such credits. A drugstore manager at Asikumaindicated that as many as three in ten of his customers purchase their drugs on credit.For seriously ill patients, intra-lineage transfers are the principal medium by whichmedical treatment is financed. The desperately poor and those whose families are notperceived as credit-worthy must either fall on the most expensive moneylenders,14
delay seeking orthodox medical help, depend on the largesse of kith and kin, or mustutilize the informal healthcare options. The Brong Ahafo and Central Region teamsfound, from separate reviews of relevant hospital records, that in-patient attendancerates fall significantly in the "hungry season" (February/March - July), when farmlabor demands and the incidence of disease are both high. Sadly, antenatalconsultations are not excepted.
'4Monthly interest rates can be as high as 50 per cent (as in Asikuma). Across the hinterland, poor peopleare sometimes compelled to sell economic assets (cattle, planting seed, etc.) on the buyers' terms or topawn their farms to extortionist moneylenders. It appears ironical that richer households in the publicservice are often able to obtain loans at sub-inflation interest rates from workplace sources and frominstitutions such as the Home Finance Company.
41
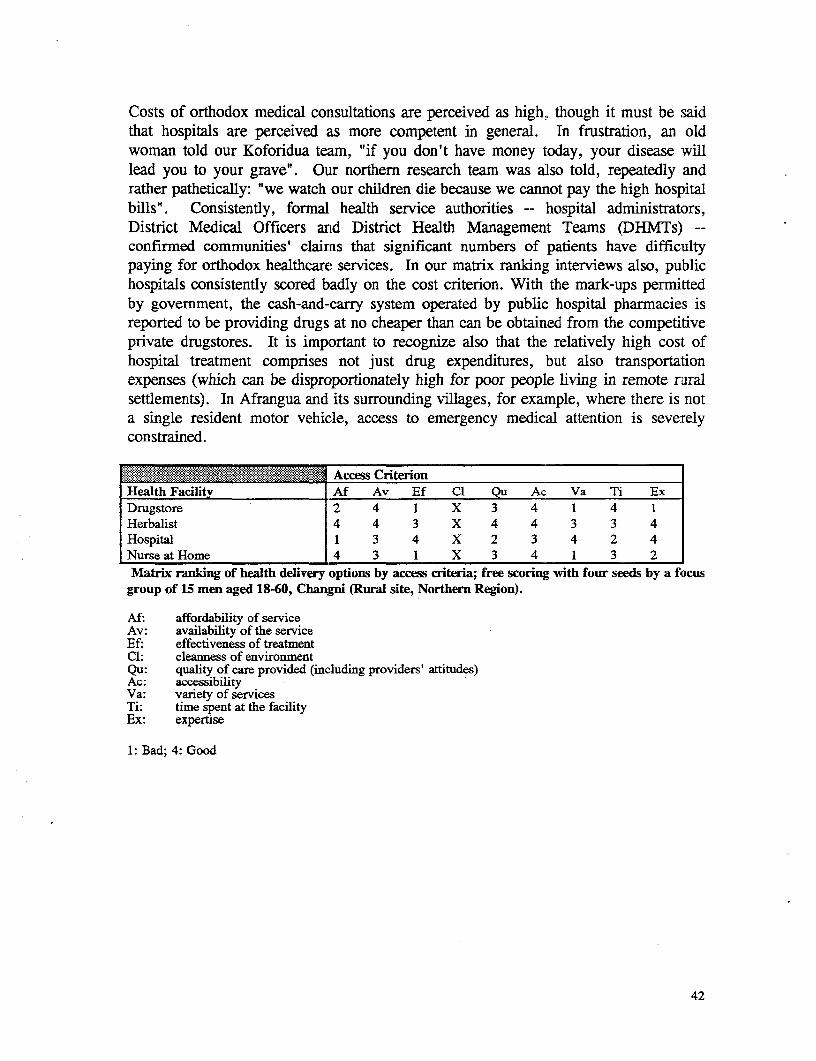
Costs of orthodox medical consultations are perceived as high, though it must be saidthat hospitals are perceived as more competent in general. In frustration, an oldwoman told our Koforidua team, "if you don't have money today, your disease willlead you to your grave". Our northern research team was also told, repeatedly andrather pathetically: "we watch our children die because we cannot pay the high hospitalbills". Consistently, formal health service authorities -- hospital administrators,District Medical Officers and District Health Management Teams (DHMTs) --confirmed communities' claims that significant numbers of patients have difficultypaying for orthodox healthcare services. In our matrix ranking interviews also, publichospitals consistently scored badly on the cost criterion. With the mark-ups permittedby government, the cash-and-carry system operated by public hospital pharmacies isreported to be providing drugs at no cheaper than can be obtained from the competitiveprivate drugstores. It is important to recognize also that the relatively high cost ofhospital treatment comprises not just drug expenditures, but also transportationexpenses (which can be disproportionately high for poor people living in remote ruralsettlements). In Afrangua and its surrounding villages, for example, where there is nota single resident motor vehicle, access to emergency medical attention is severelyconstrained.
.****..*......... Access Cr_rin Health Facility Af Av Ef Cl Qu Ac Va Ti ExDrugstore 2 4 1 X 3 4 1 4 1Herbalist 4 4 3 X 4 4 3 3 4Hospital 1 3 4 X 2 3 4 2 4Nurse atHome 4 3 1 X 3 4 1 3 2Matrix ranking of health delivery options by access criteria; free scoring with four seeds by a focus
group of 15 men aged 18-60, Changni (Rural site, Northern Region).
Af: affordability of serviceAv: availability of the serviceEf: effectiveness of treatmentCl: cleanness of environmentQu: quality of care provided (including providers' attitudes)Ac: accessibilityVa: variety of servicesTi: time spent at the facilityEx: expertise
1: Bad; 4: Good
42
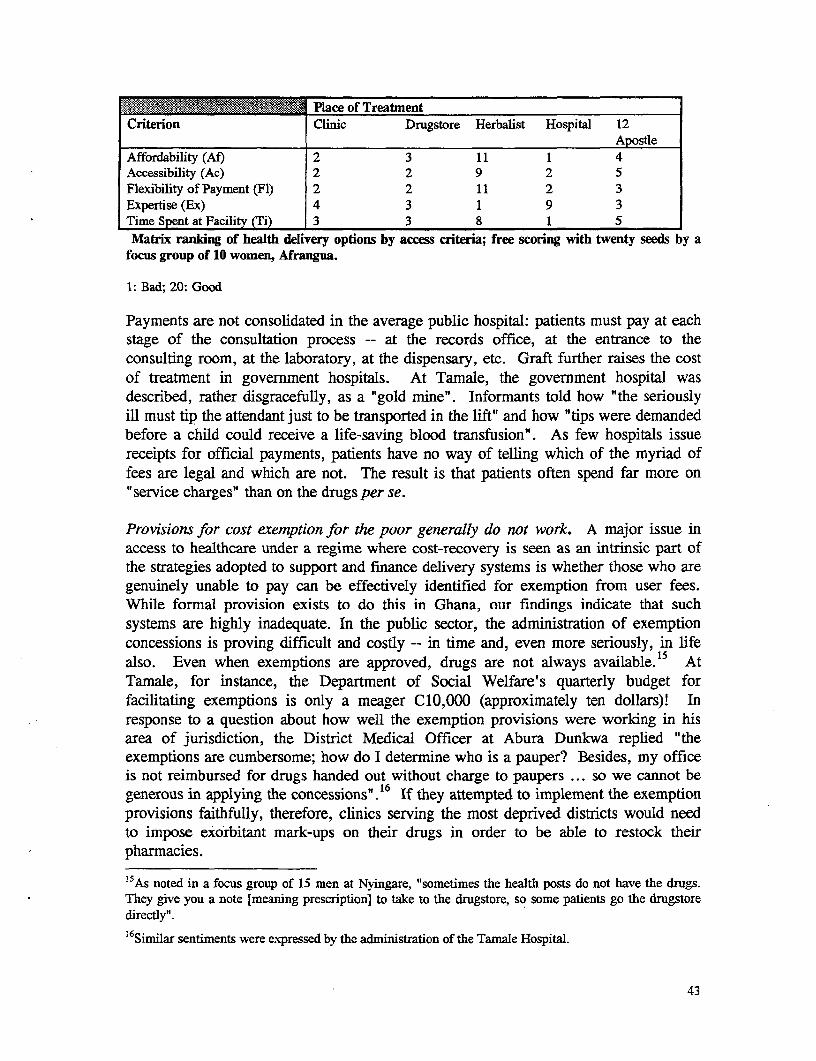
lace of TreatmentCriterion Clinic Drugstore Herbalist Hospital 12
ApostleAffordability (Af) 2 3 11 1 4Accessibility (Ac) 2 2 9 2 5Flexibility of Payment (Fl) 2 2 11 2 3Expertise (Ex) 4 3 1 9 3Time Spent at Facility (Ti) 3 3 8 1 5Matrix ranking of health delivery options by access criteria; free scoring with twenty seeds by a
focus group of 10 women, Afrangua.
1: Bad; 20: Good
Payments are not consolidated in the average public hospital: patients must pay at each
stage of the consultation process -- at the records office, at the entrance to the
consulting room, at the laboratory, at the dispensary, etc. Graft further raises the cost
of treatment in government hospitals. At Tamale, the government hospital was
described, rather disgracefully, as a "gold mine". Informants told how "the seriously
ill must tip the attendant just to be transported in the lift" and how "tips were demanded
before a child could receive a life-saving blood transfusion". As few hospitals issue
receipts for official payments, patients have no way of telling which of the imyriad of
fees are legal and which are not. The result is that patients often spend far more on
"service charges" than on the drugs per se.
Provisions for cost exemption for the poor generally do not work. A major issue in
access to healthcare under a regime where cost-recovery is seen as an intrinsic part of
the strategies adopted to support and finance delivery systems is whether those who are
genuinely unable to pay can be effectively identified for exemption from user fees.While formal provision exists to do this in Ghana, our findings indicate that such
systems are highly inadequate. In the public sector, the administration of exemption
concessions is proving difficult and costly -- in time and, even more seriously, in life
also. Even when exemptions are approved, drugs are not always available. 1 5 At
Tamale, for instance, the Department of Social Welfare's quarterly budget for
facilitating exemptions is only a meager C10,000 (approximately ten dollars)! In
response to a question about how well the exemption provisions were working in his
area of jurisdiction, the District Medical Officer at Abura Dunkwa replied "the
exemptions are cumbersome; how do I determine who is a pauper? Besides, my office
is not reimbursed for drugs handed out without charge to paupers ... so we cannot be
generous in applying the concessions"." If they attempted to implement the exemption
provisions faithfully, therefore, clinics serving the most deprived districts would need
to impose exorbitant mark-ups on their drugs in order to be able to restock their
pharmacies.
15As noted in a focus group of 15 men at Nyingare, "sometimes the health posts do not have the drugs.They give you a note [meaning prescription] to take to the drugstore, so some patients go the drugstoredirectly".
'6 Similar sentiments were expressed by the administration of the Tamale Hospital.
43
The discretionary nature of curTent exemption guidelines is also reported to be leavingthe system susceptible to abuse by staff. In any case, few poor people are meaningfullyaware of the existence of the fee exemption provisions. Exceptions to the generallypoor effectiveness of existing exemptions are limited to cases of tuberculosis, leprosy,AIDS, cholera and other diseases with serious public health implications; in otherwords, targeting is only proving successful where it is implemented by ailment ratherthan through administratively cumbersome means-testing procedures.
NGO and mission hospitals17 tend to operate special needs units and are reportingremarkably greater levels of success in determining patients' financial means and inidentifying the poor, but that is mainly on account of significantly higher levels ofmotivation and commitment, which cannot be taken for granted in the state system.Even then, high costs are sometimes incurred soliciting assistance from the Departmentof Social Welfare for recovering debts or for investigating patients' backgrounds andthe financial circumstances of their kinsfolk. 18 Treatment at NGO and missionhospitals is routinely subsidizeid; the subsidy on drugs can be as high as 90 per cent.Sometimes they offer follow-up services to out-patients who lack social networks; theymay also provide home counseling to AIDS sufferers and free rations to malnourishedpatients.
An important criterion for determining a patient's eligibility for fee-free treatment inmission hospitals such as the Catholic Hospital at Asikuma and the Baptist MedicalCenter at Nalerigu is the financial standing of the patient's extended family. Thus, apatient's social networks are investigated before a recommendation for free treatment ismade. That being so, commLunity clinics have an innate advantage that ought to beexplored in the fee exemption debate. The fact that the Nyingare community hassuccessfully implemented a levy-free policy for destitute households using thecommunity standpipe shows that community-based approaches are worthy of someattention.
Where adequate staffing is unavailable (the norm across Ghana), state hospitalauthorities and social workers who must be jointly consulted in determining a patient'seligibility for exemption often have their offices in different parts of the town. Theirdifferent responsibilities to varied clienteles and authorities also means that their workschedules are typically divergent. Even when they coexist in the same hospital, theyare not always properly integrated into the hospital system. At the Tamale Hospital,for example, the social workers complained of being ignored in the fonnulation of thehospital's social policy framework.
17Such as the Catholic Hospital at Asikuma, the Holy Family Hospital at Techiman, and the BaptistMedical Center at Nalerigu. In general, mission hospitals receive government support in the form of basicstaff salaries at levels of finding similar to what state hospitals receive, but are permnitted a higher level ofautonomy in their operations.
"'Source: Catholic Hospital, Breman Asikuina.
44
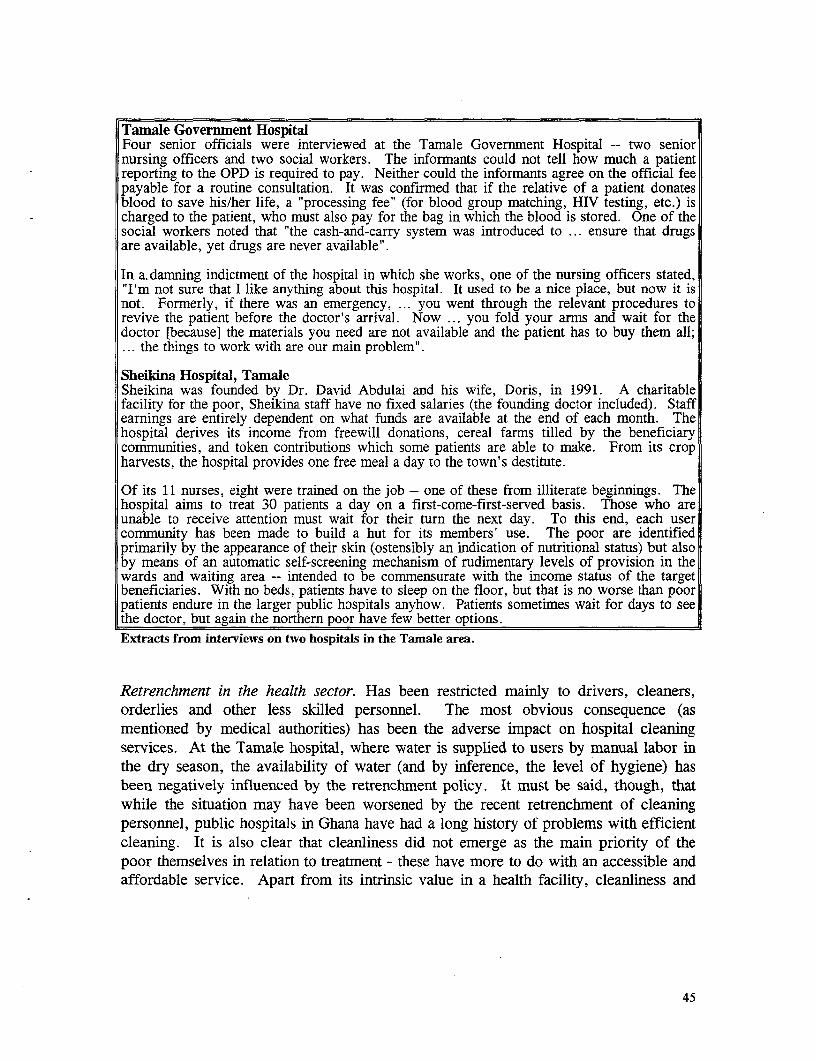
Tamale Government HospitalFour senior officials were interviewed at the Tamale Govermnent Hospital -- two seniornursing officers and two social workers. The informants could not tell how much a patientreporting to the OPD is required to pay. Neither could the informants agree on the official feepayable for a routine consultation. It was confirmed that if the relative of a patient donatesblood to save his/her life, a "processing fee" (for blood group matching, HIV testing, etc.) ischarged to the patient, who must also pay for the bag in which the blood is stored. One of thesocial workers noted that "the cash-and-carry system was introduced to ... ensure that drugsare available, yet drugs are never available".
In a.damning indictment of the hospital in which she works, one of the nursing officers stated,"I'm not sure that I like anything about this hospital. It used to be a nice place, but now it isnot. Formerly, if there was an emergency, ... you went through the relevant procedures torevive the patient before the doctor's arrival. Now ... you fold your arms and wait for thedoctor [because] the materials you need are not available and the patient has to buy them all;... the things to work with are our main problem".
Sheikina Hospital, TamaleSheikina was founded by Dr. David Abdulai and his wife, Doris, in 1991. A charitablefacility for the poor, Sheikina staff have no fixed salaries (the founding doctor included). Staffearnings are entirely dependent on what funds are available at the end of each month. Thehospital derives its income from freewill donations, cereal farms tilled by the beneficiarycommunities, and token contributions which some patients are able to make. From its cropharvests, the hospital provides one free meal a day to the town's destitute.
Of its 11 nurses, eight were trained on the job -- one of these from illiterate beginnings. Thehospital aims to treat 30 patients a day on a first-come-first-served basis. Those who areunable to receive attention must wait for their turn the next day. To this end, each usercommunity has been made to build a hut for its members' use. The poor are identifiedprimarily by the appearance of their skin (ostensibly an indication of nutritional status) but alsoby means of an automatic self-screening mechanism of rudimentary levels of provision in thewards and waiting area -- intended to be commensurate with the income status of the targetbeneficiaries. With no beds, patients have to sleep on the floor, but that is no worse than poorpatients endure in the larger public hospitals anyhow. Patients sometimes wait for days to seethe doctor, but again the northern poor have few better options.Extracts from interviews on two hospitals in the Tamale area.
Retrenchment in the health sector. Has been restricted mainly to drivers, cleaners,orderlies and other less skilled personnel. The most obvious consequence (asmentioned by medical authorities) has been the adverse impact on hospital cleaningservices. At the Tamale hospital, where water is supplied to users by manual labor inthe dry season, the availability of water (and by inference, the level of hygiene) hasbeen negatively influenced by the retrenchment policy. It must be said, though, thatwhile the situation may have been worsened by the recent retrenchment of cleaningpersonnel, public hospitals in Ghana have had a long history of problems with efficientcleaning. It is also clear that cleanliness did not emerge as the main priority of thepoor themselves in relation to treatment - these have more to do with an accessible andaffordable service. Apart from its intrinsic value in a health facility, cleanliness and
45
improved maintenance would also obviously have a beneficial impact on staff morale -so this is an area worth considering for improvement19.
Apart from its inimical effect on cleaning operations, the social outcome of the policyof retrenching auxiliary nurses has been to entrench pre-existing staff shortages.Throughout the country, relatives of in-patients are having to stay on the wards to helplook after their sick kin. Previously, auxiliaries would have been available to performthis function. Trained on the job, their services augmented those of the professionallyqualified nurses, freeing the latter to undertake outreach assignments. According to theDistrict Medical Officer at Abura Dunkwa, the size of his outreach team has had to becut in order to maintain an adequate number of nurses at the health centers. Otherresearch teams did not report similar findings, however.
In those hospitals which have access to non-state funds (e.g., the Techiman HolyFamily Hospital, the Asikurna Catholic Hospital and the Saltpond GovernmentHospital), the problems created by retrenchment (specifically, the reduction incleanliness and the decline in ward care) are being redressed by recruiting new handsoff the state payroll. In order to maintain a decent level of competent staffing all yearround, the Holy Family Hospital at Techiman is buying back leave days (holiday time)from serving personnel. At the Saltpond Hospital, evidently one of the cleanergovernment hospitals, funds are being raised from a variety of sources -- appealing forsupport from the town's expatriate citizenry, renting out space and levying extra-statutory charges on services offered (thereby raising further the cost of access for thepoor). Across the country, it is common knowledge that government hospitals arefacing very real problems tending their grounds and keeping their premises clean.
Based on the limited evidence available (from the Gambaga District and Mpeseduadze),it would appear that community-based clinics are a popular option. Certainly, theconcept is much cherished by the villages with whom we spoke (see illustration 6, forexample). Even though the Mpeseduadze clinic has now collapsed, the CommunityHealth Assistant (CHA) who had ran the facility during its existence is very wellspoken of and is still consulted by large numbers of villagers for diagnoses andprescriptions.20 Any gifts which patients are able to present in appreciation for servicesrendered are graciously receilved by the CHA, himself a member of the largercommunity. Owing to misconduct on the part of some CHAs, however, the entireconcept of community-based clinics manned by state-trained CHAs has been abandoneddefacto -- an action akin to throwing the baby out with the bath water. The extension
19 Given the low level of technology associated with cleaning functions outside of specialized areas(sterilization etc.) this would appear to be an area where contracting out this function to people who wouldhave difficulty getting formal sector jobs (local women's' groups etc.) could be investigated as a low-costsolution.20According to the Mpeseduadze chief and the local Assemblyman, the limited assistance which the CHAis able to provide is preferred to the services available at the government hospital located some sixkilometers away. An important reason given for the CHA's extreme popularity is his welcomingdemeanor. In contrast, nursing staff at government hospitals were routinely described as rude.
46
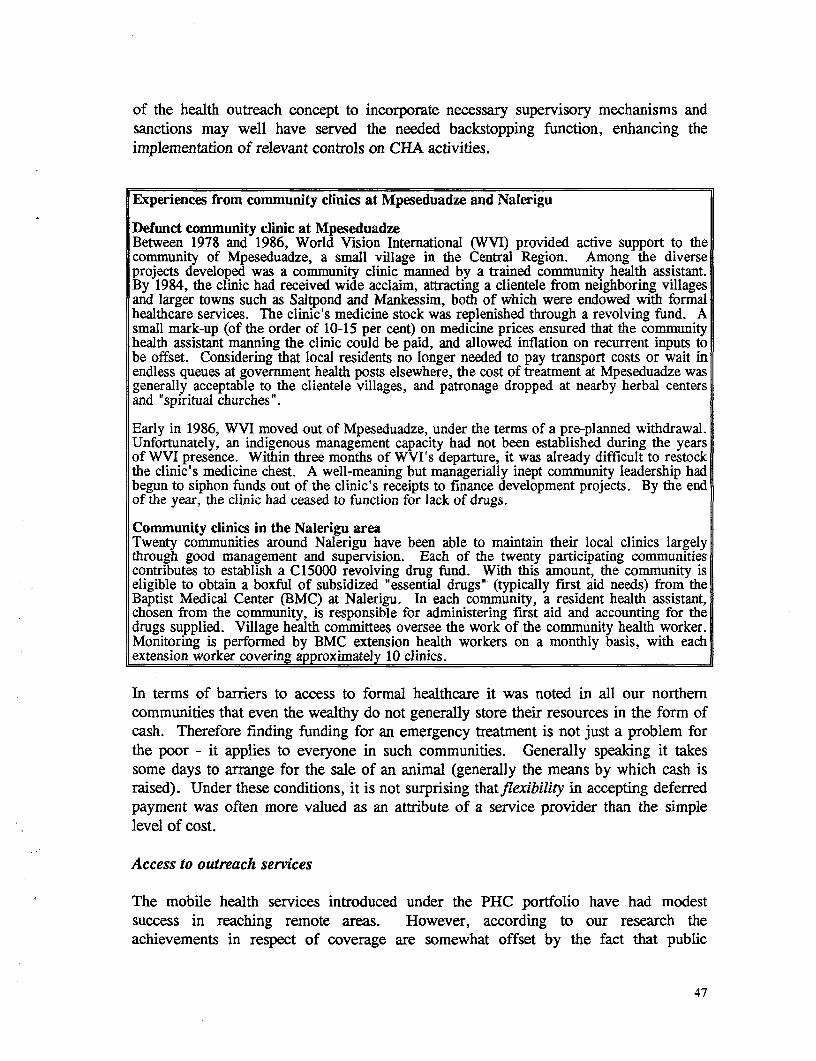
of the health outreach concept to incorporate necessary supervisory mechanisms andsanctions may well have served the needed backstopping function, enhancing theimplementation of relevant controls on CHA activities.
Experiences from community clinics at Mpeseduadze and Nalerigu
Defunct community clinic at MpeseduadzeBetween 1978 and 1986, World Vision International (WVI) provided active support to thecommunity of Mpeseduadze, a small village in the Central Region. Among the diverseprojects developed was a community clinic manned by a trained community health assistant.By 1984, the clinic had received wide acclaim, attracting a clientele from neighboring villagesand larger towns such as Saltpond and Mankessim, both of which were endowed with formalhealthcare services. The clinic's medicine stock was replenished through a revolving fund. Asmall mark-up (of the order of 10-15 per cent) on medicine prices ensured that the communityhealth assistant manning the clinic could be paid, and allowed inflation on recurrent inputs tobe offset. Considering that local residents no longer needed to pay transport costs or wait inendless queues at government health posts elsewhere, the cost of treatment at Mpeseduadze wasgenerally acceptable to the clientele villages, and patronage dropped at nearby herbal centersand "spiritual churches".
Early in 1986, WVI moved out of Mpeseduadze, under the terms of a pre-planned withdrawal.Unfortunately, an indigenous management capacity had not been established during the yearsof WVI presence. Within three months of WVI's departure, it was already difficult to restockthe clinic's medicine chest. A well-meaning but managerially inept community leadership hadbegun to siphon funds out of the clinic's receipts to finance development projects. By the endof the year, the clinic had ceased to function for lack of drugs.
Community clinics in the Nalerigu areaTwenty communities around Nalerigu have been able to maintain their local clinics largelythrough good management and supervision. Each of the twenty participating communitiescontributes to establish a C15000 revolving drug fund. With this amount, the community iseligible to obtain a boxful of subsidized "essential drugs" (typically first aid needs) from theBaptist Medical Center (BMC) at Nalerigu. In each community, a resident health assistant,chosen from the community, is responsible for administering first aid and accounting for thedrugs supplied. Village health committees oversee the work of the community health worker.Monitoring is performed by BMC extension health workers on a monthly basis, with eachextension worker covering approximately 10 clinics.
In terms of barriers to access to formal healthcare it was noted in all our northemcommunities that even the wealthy do not generally store their resources in the form ofcash. Therefore finding funding for an emergency treatment is not just a problem forthe poor - it applies to everyone in such communities. Generally speaking it takessome days to arrange for the sale of an animal (generally the means by which cash israised). Under these conditions, it is not surprising thatflexibility in accepting deferredpayment was often more valued as an attribute of a service provider than the simplelevel of cost.
Access to outreach services
The mobile health services introduced under the PHC portfolio have had modestsuccess in reaching remote areas. However, according to our research theachievements in respect of coverage are somewhat offset by the fact that public
47
outreach teams have tended to be rather unreliable with keeping dates and times. Notuncommonly, they arrive a day or more late, when villagers are not expecting them andhave left for their farms. The principal factor constraining outreach visits to peripheralsites was reported to be financial, in particular budgetary cutbacks resulting in reducedtransport allocations and fuel rations. The reduction in auxiliary nurse numbers has alsoimposed strains on the capacity of some health administrations to release professionallyqualified nurses for outreach work. These losses may well be a contributing factor tothe inability of outreach teams to be punctual in their village rounds.
Discussions with the Acting Medical Officer for the Abura Dunkwa-Kwamankesedistrict, and confirmed through community interviews at Afrangua, revealed that themost reliable outreach teams are succeeding mainly by levying unofficial charges tooffset their transport expenses21 and to purchase necessary consumables for treatmentand nutritional demonstrations. Supplementary interviews conducted in Kumasi and atAbura Dunkwa revealed that it is common for Maternal and Child Health (MCH) teamsto run out of growth monitoring and antenatal record cards as well as other medicalsupplies (syringes, needles, cotton wool, etc.). Sometimes, DHMTs are compelled toseek financial assistance from their District Assemblies. Under the straitened fundingconditions, however, District Assemblies are unable to provide much financial supportto needy outreach teams.
While the amounts charged at the MCH consultations (for immunizations, weighingand other basic services) may appear small -- of the order of C200 per monthlyconsultation -- the evidence from this study shows that rural women sometimes havedifficulty meeting this cost. The poorest mothers are, thus, sometimes compelled toskip immunizations.22 The reason may be partially explained by the fact that theresponsibility for meeting the non-food needs of infants tends to be left to thewomenfolk. Of the few women specifically interviewed on the subject, none seemedaware that the bulk of the fees being charged are unofficial.23 This is to be expectedsince receipts are not being issued for payments made by the public.
Mobile health services run by the state are generally restricted to the immediate needsof children and expectant/nursing mothers. In practice, this means immunizations,weighing, advice on child spacing and the administration of oral rehydration salts tochildren suffering from diarrheal dehydration. In communities such as Afrangua,general consultations and the community health education component of the PHC
21Evidence from the education sector (particularly interviews with FLP coordinators, teachers and GESpersonnel) suggests that the timely reirnbursement of legitimate transport and travel (T&T) claims may bea major incentive in ensuring successful extension work. In each region, the depressing impact of theslow response in reimbursing such claims was cited as a supervision problem.22The unreliability of outreach visits (in terms of keeping dates and times) is another factor that affects theefficiency of the immunization program.23The only approved charge, apart from drug costs, is a nominal C50 fee for weight checks.Immunization and ante-natal services are meant to be fully exempt from charge.
48
program are largely being sidelined owing to inadequate staff numbers. The educationcomponent is intended to address issues such as water purification and storage, personalhygiene and environmental sanitation. Of particular concern is the fact that relevantanti-malaria information is not reaching the poor, even though malaria remains themain cause of morbidity in all three ecological zones (GSS 1993: 23).
In rural areas, where birth rates remain high, family planning advice is bypassing theadolescent female population. Despite the planned parenthood campaign being directedat mothers (in its practical implementation), our Brong Ahafo and Central Region teamsfound several women who would not practice family planning, convinced instead thatlarge numbers of children are an effective cultural strategy for securing their partners'affection. The two teams also report that women who have had multiple marriages tendto have significantly more children. In the face of persisting poverty, and with menroutinely defaulting in their traditional obligation of fending for their partners, divorcesrates are high and the search for new conjugal unions is common. Not only is the roleof an efficient family planning program -- sensitively designed to respond to thedynamics of culture and poverty -- particularly important. It is also plausible that thesuccess of the family planning program may depend, to a significant degree, on theincorporation of fundamental poverty-reduction measures.
2.6 Local Perceptions of Service Quality and Access in the Education Sector
2.6.1 Access and utilization
Owing to public funding constraints and the general shift to what is described as ademand-oriented, community-based approach to provision, communities are nowrequired to contribute substantially towards the cost of educating their children. This,in the government's view, is meant to "ensure financial sustainability" of the educationpolicy (ISSER 1993: 15). The costs are not only monetary: communities must alsoprovide relevant labor inputs for structural works. Statistical data from the last tworounds of the Ghana Living Standards Survey (GLSS) confirm a substantial rise inhousehold expenditure on education. Interviews with parents and school authoritiesindicate that the statutory fees payable to the government are only a small fraction ofthe myriad of hidden costs which parents have to bear under the present educationalprogram (see below).
Primary schools and junior secondary schools (JSSs) are available in most establishedurban centers, but less so in rural areas. Senior Secondary School (SSSs) aremoderately available in urban areas, but an absolute rarity in rural areas. As a result,rural dwellers tend to regard the JSS as the terminal stage in de facto educationopportunities. While the non-availability problem is worst in rural communities of thenorthern savannah (confirmed by data from all three rounds of the GLSS), it is typicalfor rural pupils (particularly those at JSS level) to walk several kilometers to school --sometimes crossing rivers in boats or wading through streams en route. Problems of
49
accessibility, and in particular the high transport expenditures necessitated by longcommuting distances, were often cited by villagers as a key factor contributing to thesignificant drop-out rate at the transitional stages (viz. primary to JSS; and JSS to SSS).Formal fees payable for SSS education are perceived to be very high. In the words ofan informant at Changni, "some fathers have never counted twenty thousand cedis atany one time in their lives, yet parents are being asked to pay [annual fees of up to]forty-five thousand cedis [at SSS level]".24 During the rainy season, access can beseriously impeded in rural areas by the lack of roads and transport facilities. Yet,according to the government's education blueprint, a central objective of the reformpackage is to increase the rate of school enrollment (ISSER 1993: 15).
Creches are less well provided but, where provided, the patronage demonstrates ademand for the service. Female members of the Asikuma Youth Association (generallyaged between 25 and 40) also identified a crehe as their principal concern. Parents atAsikuma report that, under new government regulations, children under five years willno longer be accepted in state--run nurseries. This is likely to lead to a decline in theability to pay for formal child-minding services, which will be available in the privatesector only. If this were to happen it is likely that larger numbers of mothers wouldeither be compelled to stay at home or would have to carry their toddlers to work.
Access to Education: a Child at Gambaga JSS
Kwame Lambor comes from a family of nineteen children. Each morning, he walks the one-and-a-half-mile stretch to his school, the Gambaga JSS. His father, a "faralana" (poor man),has no money to buy fertilizers to improve the output of his leached farmland. His annualharvest averages two 50-kilogram sackfuls of maize. In order to feed his household, he seekswork on other people's farms, receiving about C300 (30 US cents) for a full day's hire.Kwame sometimes leaves home for school without eating. During the rainy season, he issometimes unable to go to school if the river which he has to cross floods its banks. In the dryseason also, he has to spend much of his mornings searching for water, which makes schoolingdifficult.
De facto GES policy, in respect of basic education, is that communities should beresponsible for erecting their own schools. In the more established urban areas, pre-existing state-built schools are likely to be available. In any case, GES's liability iscurrently limited to providing teachers, textbooks and some consumables such as chalkand registers. Even then, our research teams found that in the schools visited in thethird phase of the research these conditions were generally not fulfilled.
Some District Assemblies are levying supplementary annual charges on parents (C1500per child for the Cape Coast District) in order to finance necessary structuralrehabilitation works. According to GES officials at Asikuma, some of the moredeprived rural schools in that district are using children's labor to generate income tosupplement meager school budgets. As with the sanctioned costs of MCH services,official school fees do not seem particularly high (reported to be around C1050 per
24Comment made in a focus group interview with 15 men aged 18-60, Changni.
50
annum), but poor parents sometimes find these difficult to pay. This situation isaggravated by the proliferation of other (hidden but quite legal) expenditures: ad hoclevies for structural works, annual parent-teacher association levies (C5000 in parts ofthe north), supplementary sports fees, examination fees, initial registration fees (C4000at Changni) and sometimes costs of providing classroom furniture for individual pupils.School uniforms (at approximately C6000 each), travel costs (where pupils have totravel to school by motorized transport), lunch money and expenses on stationery andconsumable inputs for practical crafts lessons are further additions that raise the realcost of education. Also significant in raising household education expenditures is thehigh birth rate in rural areas
Though the Ministry of Education has issued clear instructions forbidding the expulsionof pupils on grounds of non-payment of fees, headteachers often feel compelled to actto the contrary since they are held directly accountable for the collection of fees.Tuming indebted children away is particularly common in the last months of theacademic year, before the main harvest.25
In some cases, this strategy proves successful in forcing parents to pay up onoutstanding fees, but there are also many instances where pupils never return to theclassroom once they have been sent away for their fees. At Changni, in the north,drop-out rates are reported to be a high 45 per cent -- typically on account of parents'inability to pay their wards' fees. At the Mpeseduadze Primary School, 15 out of 23pupils from a neighboring village, Asafonna, dropped out in the last academic year onsimilar grounds. On numerous occasions, and in all three regions, we came acrosschildren from poor homes who were compelled to find piecework in order to settletheir fees, or to purchase other basic needs such as pencils and school uniforms. Giventhat the bottom line in the reformed education program is to eradicate illiteracy, thedistressing situation described above must beg the critical question of the sustainabilityof the cost recovery formula being administered. In the rural hinterland especially,cuts in government expenditure have worsened an already inferior position.
In the severely deprived northern savannah, where education had been free of chargeuntil recently, the financial impact of the new cost recovery approach seems to beparticularly harsh. Given the severity of poverty across the savannah belt (and the highincidence of poverty-induced mortality), the northern communities studied areespecially anxious about the future of education under the current cost-sharing regime.Informant after informant decried the real cost of education as high, and the financialreturns low.
Functional literacy. In respect of the community-based Functional Literacy Program(FLP), access is largely dependent on the availability of a volunteer instructor
25Source: focus group discussion with nine teachers at Mpeseduadze, near Afrangua. The group includedtwo headteachers.
51
(facilitator). FLP officials report serious difficulties in recruiting suitable facilitators.2 6
This is not surprising, as such volunteers are expected to teach classes several timeseach week without remuneration. Expectedly, motivation and commitment are lowamong the program's facilitators; they may arrive late or absent themselves withoutgiving notice. It must be said, however, that the situation is somewhat better in ruralareas-perhaps, because teaching is a prestigious career in the perception of poorGhanaians.
Among learners too, enrollment is low and drop-out rates high. Interviews withinformants suggest that this situation may be indirectly attributed to poverty. Olderadults, the main targets of the program, are often exhausted after working long hoursduring the day, thereby affecting their ability to participate productively in the eveningclasses. Attendance rates also tend to drop substantially in the farming season (whenlabor demands are highest) and during festive periods (when non-natives travel out tocelebrate the season in their own home villages). The most common request made by
27learners was for better lighting. Many complained that the aging process had affectedtheir eyesight, and that they found night reading difficult.
2.6.2 Local views of education quality
The major concern of most community members and teachers canvassed in our study(especially the third phase) was with issues of quality rather than of basic access. Themushrooming of rural schools (through community initiative, particularly under theongoing reforms) has meant that educational resources have had to be spread quite thin.Thus, while schools may be rnore accessible (in terms of proximity; not costs), ruralcommunities tend to have so few teachers per school as to render the quality and valueof education in such schools questionable.
Teachers, officials of the Ghana Education Service (GES), literate parents and oldersiblings were consistently emphatic that the quality of education has declinedsubstantially over the last decade. The results of the 1994 SSS examinations are arevealing testimony to this oft-repeated assertion. Of some 42000 registeredcandidates, just over 1000 passed the examination! The sentiments of many parentsand teachers are aptly encapsulated in the words of a GES official at Cape Coast whoopined that "to reduce the duration of basic education so suddenly and drastically [from17 years to 12] without adequate preparation is criminal." In the larger cities of Accraand Kumasi, irate parents continue to criticize the reforms, describing them as "anexpensive experiment with a whole nation's education" and "an ill-planned programwhose implementation is prodcucing nothing but illiterate (sic) school leavers".
26IThe Central Region research team was fortunate to be accommodated on a common campus with FLPorganizers participating in a review session at the time of our fieldwork. It was, thus, possible to holdsome quite useful discussions in our Free time.27Many poor homes across the country only own one lantern. This can be a serious problem when onemember of the household has to participate in night classes.
52
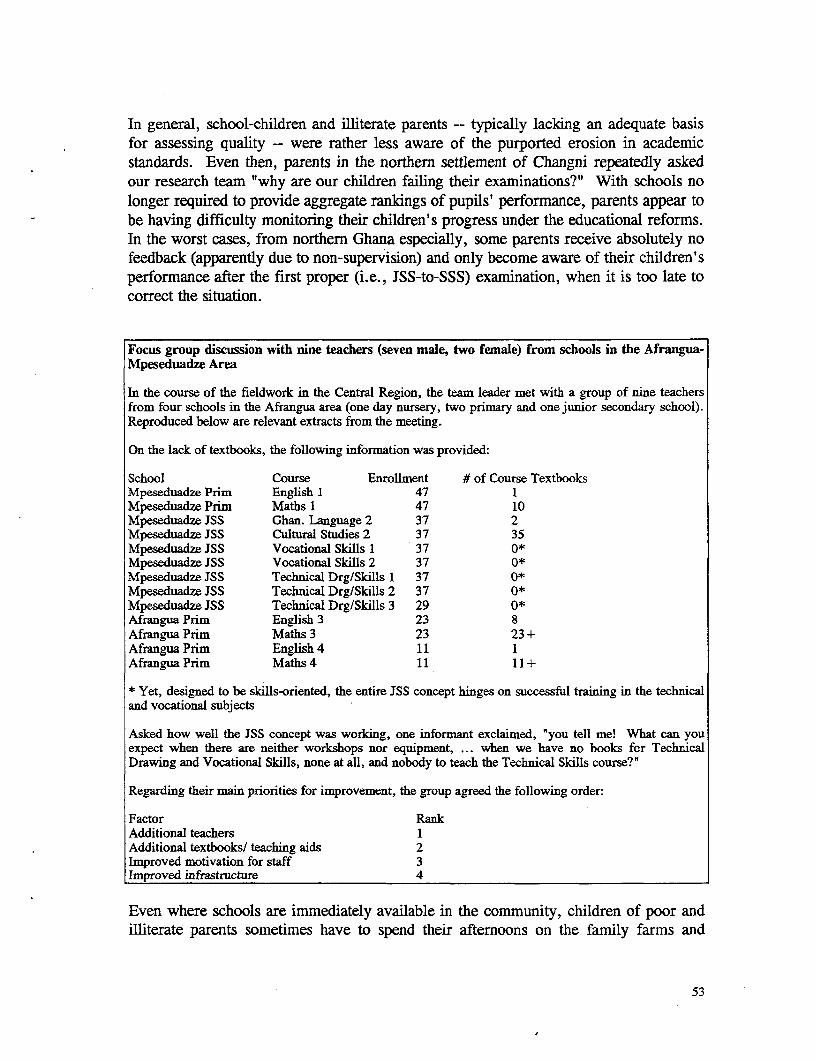
In general, school-children and illiterate parents -- typically lacking an adequate basisfor assessing quality -- were rather less aware of the purported erosion in academicstandards. Even then, parents in the northern settlement of Changni repeatedly askedour research team "why are our children failing their examinations?" With schools nolonger required to provide aggregate rankings of pupils' performance, parents appear tobe having difficulty monitoring their children's progress under the educational reforms.In the worst cases, from northern Ghana especially, some parents receive absolutely nofeedback (apparently due to non-supervision) and only become aware of their children'sperformance after the first proper (i.e., JSS-to-SSS) examination, when it is too late tocorrect the situation.
Focus group discussion with nine teachers (seven male, two female) from schools in the Afrangua-Mpeseduadze Area
In the course of the fieldwork in the Central Region, the team leader met with a group of nine teachersfrom four schools in the Afrangua area (one day nursery, two primary and one junior secondary school).Reproduced below are relevant extracts from the meeting.
On the lack of textbooks, the following information was provided:
School Course Enrollment # of Course TextbooksMpeseduadze Prim English 1 47 1Mpeseduadze Prim Maths 1 47 10Mpeseduadze JSS Ghan. Language 2 37 2Mpeseduadze JSS Cultural Studies 2 37 35Mpeseduadze JSS Vocational Skills 1 37 0*Mpeseduadze JSS Vocational Skills 2 37 0*Mpeseduadze JSS Technical Drg/Skills 1 37 0*Mpeseduadze JSS Technical Drg/Skills 2 37 0*Mpeseduadze JSS Technical Drg/Skills 3 29 0*Afrangua Prim English 3 23 8Afrangua Prim Maths 3 23 23 +Afrangua Prim English 4 11 1Afrangua Prim Maths 4 11 11+
* Yet, designed to be skills-oriented, the entire JSS concept hinges on successful training in the technicaland vocational subjects
Asked how well the JSS concept was working, one informant exclaimed, 'you tell me! What can youexpect when there are neither workshops nor equipment, ... when we have no books for TechnicalDrawing and Vocational Skills, none at all, and nobody to teach the Technical Skills course?"
Regarding their main priorities for improvement, the group agreed the following order:
Factor RankAdditional teachers 1Additional textbooks/ teaching aids 2Improved motivation for staff 3Improved infrastructure 4
Even where schools are immediately available in the community, children of poor andilliterate parents sometimes have to spend their afternoons on the family farms and
53
pastures or helping with other household economic undertakings (such as petty trading)and domestic chores. Ultimately they either cannot find the time, or are too exhausted,to do their school homework properly. During festivals and funerals also, parentstraveling to their native villages sometimes take their children along, causing losses ofup to two weeks in schooling time. The obvious result is a decline in their ability tounderstand future lessons and to benefit effectively from tuition received. A similarfate befalls those other children who must work in order to finance their education.
In the basic education program, defacto policy of the GES is to provide one teacher for35-40 pupils. The enforcement by GES officials of this so-called "enrollment factor"prescription has been particularly inimical to the provision of quality education in ruralschools. Classes in such schools are often compelled to share teachers. The result is areduction in the attention that can be devoted to each class, with a corresponding loss inoverall efficiency and quality of instruction in rural areas. Ultimately, government'sintention of developing the country's human capital through decent education is boundto be undermined by such dismal conditions.
In contrast to rural schools which tend to be underutilized, urban schoolrooms tend tobe overpopulated. At Techiman Zongo, 93 students share a standard JSS 1 classroom.Under such conditions of overcrowding, we can expect, ceteris paribus, a high risk ofcross-infection. Given the twin problems of (non-)affordability of healthcare and theroutine misuse of antibiotics, overcrowding in classrooms may indeed represent agreater problem than is generally recognized. In the Techiman school underdiscussion, controlling the students is only achieved with difficulty, and teachers arereported to be having trouble rnoving through non-existent aisles to provide one-to-onetutoring.
It is also common, in deprivecd areas -- both rural and urban -- to find pupils sharingstandard classroom furniture built for individual use. Teachers interviewed were of theview that approximately one-third of pupils share chairs and desks in the Afranguaarea. At the Mpeseduadze Primary School, two children share a chair only 300centimeters wide, and at Tamale, a standard bench (approximately 1.5 meters wide) isshared by five pupils. Equally appalling is the situation at Nyingare, where someteachers lack chairs and some schoolchildren are compelled to squat or kneel on thescreed floor while using their benches as desk space. Evidently, the quality ofeducation cannot be satisfactory under such conditions of learning. Symptomatically,we found numerous examples of JSS children (mainly rural, less so of urban) whocould not spell their own surnames correctly. In a focus group discussion with sixmales (of mixed ages) at Afrangua, it was also affirmed -- and unanimously so -- thatmany of the village's Class Six pupils cannot read Class Two books satisfactorily.These findings are consistent with those of Oti-Boateng et al (1990: 26) who report that"the appallingly low literacy and numeracy rates ... are only in part accounted for by
2"Respiratory tract infections were often listed among the commonest diseases afflicting poorcommunities.
54
individuals who have never attended school.... For the majority [of the very poor andrural residents in general], school attendance fails to equip them with the most basicskills. "
It is ironical that the most deprived schools also tend to be the ones with the higheststaff turnover rates. Such schools, often located in the rural areas, are dependent onnational service personnel to fill teaching shortfalls. It is common knowledge,however, that national service postings are typically made in November, a full twomonths after the academic year has commenced. Problems with finding suitableaccommodation further delay their reporting for duty.
The new policy of phasing out non-professional teachers. Has contributed further tostaff shortages in deprived rural districts. GES officials in the Central Region reportthat women are disproportionately represented in the non-professional group (perhaps,because their multiple roles -- especially their childbearing responsibilities -- leave themwith little time for pursuing further studies). That non-professional teachers have beenmuch more willing to accept postings to deprived areas than have professionally trainedteachers is widely acknowledged in Ghana, and is especially important to theunderstanding of the impact of retrenchment on the quality of education. The generalembargo on new recruitment into the public sector also means that national servicepersonnel, after acquiring relevant teaching skills in their one year of service, cannoteasily be retained in the system. In any event, there can be little logic in a policy thatseeks to retrench one group of non-professional teachers while relying on another groupof untrained, inexperienced teachers with high turnover characteristics.
With the low rate of teacher production nationwide, teaching shortfalls have becomeparticularly difficult to fill. For the 1994/95 academic year, for example, the entiredistrict of Asikuma-Odoben-Brakwa (one of 110 in Ghana) received only 13 teacherswhereas there were 146 full-time vacancies to be filled. It is altogethercounterproductive that these new recruits were not sent to fill any of the existingvacancies but were rather made to replace non-professional teachers in the district'sprimary schools.29 The current shortfall for the Northern Region stands at some 2300.Across the country, it is no longer possible to compensate for temporary shortfallsarising from maternity and illness -- which, in earlier decades, were addressed bycalling on so-called "supply (reserve) teachers". Interviews with officials of the GESindicate that the shortage of teachers has been caused by two main factors: theconversion, since the late 1970s, of large numbers of teacher training colleges intosecondary schools; and the increased demand for teachers arising from the rise inpopulation and school enrollment, and the enlargement of the teaching curricula atprimary and JSS levels. Also believed to be significant is the fact that the functional
29This in spite of the fact that some were specially trained in key technical subjects for which JSSs arecomplaining of teacher shortages. In this respect, retrenchment in the education sector is also causing anunderutilization of prime manpower resources.
55
literacy program is relying for its administrative functions on teaching staff siphonedfrom the classrooms.
In separate interviews with teachers and officials of the GES, informants emphasizedthe lack of textbooks. At Dwemoh in Brong-Ahafo, a class of sixty-odd pupils sharethree French textbooks between them. At Asikuma, the headteacher of the CatholicBoys School lamented, "there are some subjects for which we have no textbooks at all
not even one for the teacher's reference" .30 English readers for Class Four pupilshave not been printed since 1]990; and according to the Textbooks Officer at CapeCoast, a parent of a Class One pupil would need to spend C18000 if he wished tofurnish his child with the necessary textbooks.3 ' In the face of such logisticalinadequacies, a bleak manpower situation and real difficulties in household financing ofeducational needs, it is not surprising that educational workers are generaLLy cynicalabout the anticipated rewards of the educational reform program.
In respect of the factors that make for quality education, teachers interviewed are of theunanimous view that the availability of teachers is the most critical. Even the JSS ofthe Catholic Boys' School at Asikuma, adjudged the best in the district for the 1991/92academic year, now has no Mathematics or Technical Skills teacher! Given the generalstate of inadequate school staffing in the communities studied, there can be little doubtthat the problem of quality education is very real, and that the implications are indeedominous.
If assessed from observations3 of actual classroom tuition, the quality of instruction isnot always satisfactory. Particularly in the hinterland, it is not uncommon to findpoorly paid teachers treating their teaching assignments as a part-time undertaking.Such teachers may devote prime schooling time to other work (e.g., selling in themarket, at Techiman; farming in most of the other sites) as a means of supplementingtheir incomes. The field teaims received several reports of teacher absenteeism andcomplaints of pupils being compelled to spend school hours on teachers' private farms.Sometimes, children are simpLy left to play throughout the school day -- a complaintrepeatedly made by schoolchildren at Nyingare in the Northern Region. On occasion,the lack of textbooks was attributed partly to headteachers' defaulting in collectingsupplies from their district capitals.
Both the GES and teachers interviewed in focus groups admit to the inadequacy ofschool supervision. A diversity of transport-related problems -- inadequate motorbikes,insufficient fuel supplies and the lack of financial resources for reimbursing transportcosts -- were cited as the main reasons for this condition. It was reported in three GES
30A focus group of nine teachers (seven mnale; two female) from Mpeseduadze and its surrounding villagesmade similar observations.3 1This cost rises significantly at higher levels of the educational ladder.32We surreptitiously observed classes in session at Afrangua, Mpeseduadze and Asikunia.
56
offices (at Abura Dunkwa, Asikuma and Cape Coast) that this situation has improved invery recent months following the receipt of special funds provided by GES forreimbursing headteachers and supervisors for approved travel expenses.
In areas where school buildings are old, it is common to find walls that are crumbling,roofs that are either ripped or lealdng,33 classrooms that are damp and murky, andscreed floors that are seriously pitted. Structural problems were frequently cited byschool authorities and GES officials as posing a risk to school populations.
Funding difficulties cause the collapse of a school roof at Gambaga
In an example from the state-run Presbyterian JSS at Gambaga (in northern Ghana), seriousfunding constraints had prevented a sagging roof from being repaired. Under thegovernment's educational sector reforms, communities are entirely responsible for all structuralmaintenance expenditures. Owing to the dire state of poverty, manifest in a high rate ofmalnutrition, this community was unable to raise the necessary finance. Eventually, inOctober 1994, the roof collapsed on a roomful of schoolchildren while their class was insession. Twelve children were injured, with one suffering fractures in both legs.
Another important factor commonly cited by GES officials, teachers and some literateparents for the noticeable decline in educational quality is the increase in the number ofsubjects taught in basic schools. Whereas the Middle School system which has beenreplaced by the JSS taught only four core subjects (English, Mathematics, Geographyand History), JSS pupils are now required to study 12 or so subjects. Necessarily, thisexpansion of the teaching curriculum has resulted in a reduction in the hours allocatedto English as a course. Logically, the decline in the ability of pupils to understand theEnglish language has adverse implications for understanding other courses taught inthat language.34 Further impairing the appreciation of the English language is thepractice of teaching junior classes (up to the Primary 3 level) in native languages.
2.6.3 Perceived relevance of education
In terms of the perceived relevance of education the following main messages emergedfrom the research.
The criteria by which local communities defined the 'relevance' of the educationservice were based on two factors: the ability of children to get jobs, the ability ofchildren to read and write in English (so that illiterate parents no longer have to goelsewhere to get letters read and written, compromising the privacy of the family, andchildren can perform basic tasks like identifying the correct hospital card for familymembers etc.). In only one community was literacy mentioned in relation to learningimproved techniques in traditional occupations - in relation to farming in the Mamprusi
33In the rainy season, such problems can cause serious disruptions of classes.34Even "Arabic" (qur'anic) schools, common in Islamic communities in the north and in the migrantzongos, are shifting voluntarily to the secular system in order to benefit more from English tuition.
57
village in the Northern Region. In relation to these criteria education (at the level towhich it is pursued by the poor - generally no higher than JSS) is perceived to befailing. People consistently said that their children could not read and write at the endof school. In relation to this parents in some sites argued that the first-cycle (primaryand JSS) curriculum was too broad - with insufficient time and attention paid to basicliteracy.
Regarding the match between user aspirations and the revised curriculum for first-cycleschools, our findings indicate that the reforms are not fulfilling the purpose for whichthey were designed. In both rural and urban areas, the implementation of the technicaltraining component, king-pin in the educational reform program, is largely perceived asunsatisfactory. In case after case -- in schools, communities and in GES offices --informants alluded to the lack of tools, working materials, workshop buildings andtrained teachers. This situation, a serious impediment to effective skills training in theJSSs, has arisen mainly because, in the current cost-sharing framework, communitiesare not only responsible for financing capital requirements and school furniture, butalso for providing tools and other inputs needed for the program. Consistently,therefore, the skills training objective is being undermined by the high incidence ofpoverty. There is also a clear regional dimension to this, with our research suggestingthat communities in the poorer areas of the country (in this case specifically the sites inour sample in northern Ghana) are less able to meet these extra responsibilities thanthose elsewhere. Lack of skilled craft teachers is also a major constraint in all the ruralareas in our study. The technical training component was consistently described as theweakest link in the JSS agenda.
2.7 Domestic Water and Sanitation
Within the towns and villages studied, the availability of safe water and sanitation isoften a function of NGO presence. Many poor households rely on streams anduncovered wells of dubious purity. Except where interventions have beenimplemented, therefore, water quality tends to be particularly poor during the dryseason when natural water sou;rces tend to dry up. In the Northern Region in particularhuge amounts of women's labor time during the dry season are expended on fetchingwater - affecting their potential access to employment and income-generatingopportunities. Evidence from all three rounds of the PPA indicate that for communitieswhere water supply is problematic this remains the over-riding priority - especially forwomen. In those communities where water problems had been successfully addressedit was generally the result of either NGO or donor-funded interventions.
In all low-income urban sites, we found a high level of indiscriminate defecation,largely resulting from extremely low levels of provision. Understandably, women aremore concerned about the deficiencies of water and sanitation: it is they and thechildren who are responsible for replenishing household water supplies; and culturalnorms prevent them from evacuating their bowels in open spaces.
58
Obtaining land is a major issue in relation to some kinds of urban services. There is aparticular problem with obtaining land for latrines as it lowers the value of surroundingproperty. It was found that while VIP latrines functioned excellently in ruralcommunities where population density is low they were virtually impossible to maintainin densely settled urban areas at the concentrations they existed in the areas studied. Itis therefore recommended that a review should be made of means by which DistrictAssemblies can find ways of making more land available for latrines in poor urbanareas - in order to decrease pressure on existing facilities, and thereby set up a virtuouswhere the presence of a latrine in a neighborhood is no longer regarded as a health andenvironmental hazard.
59
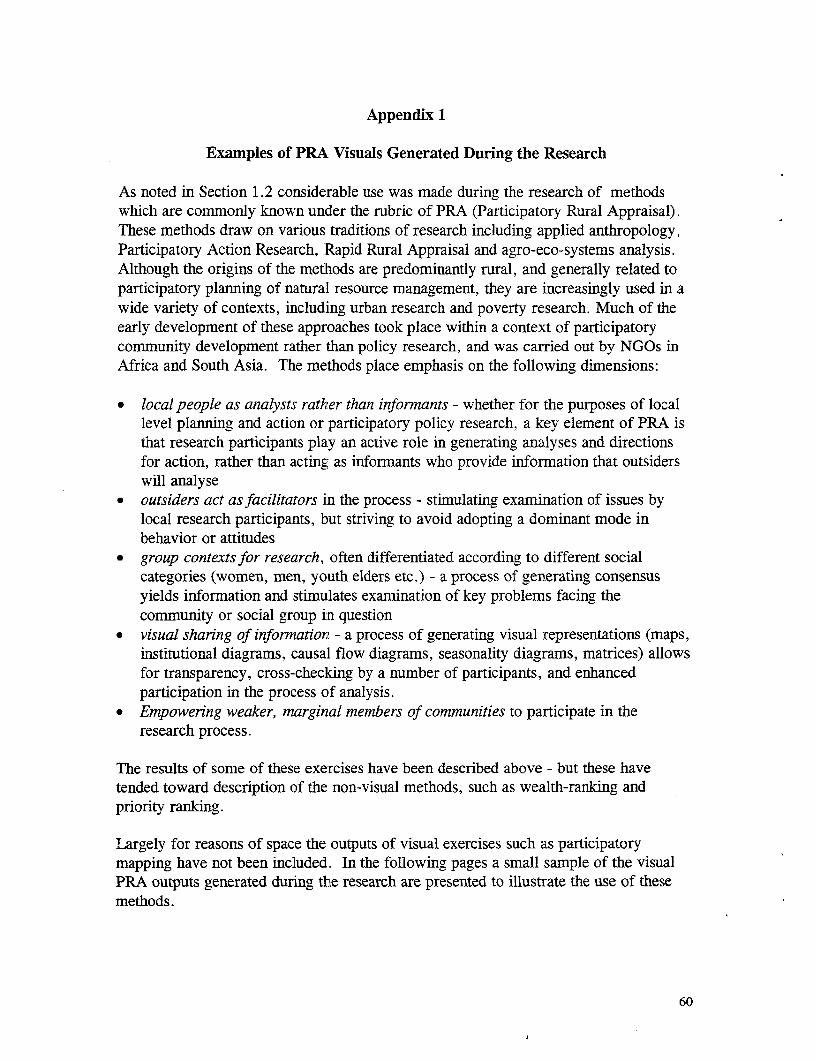
Appendix 1
Examples of PRA Visuals Generated During the Research
As noted in Section 1.2 considerable use was made during the research of methodswhich are commorly known under the rubric of PRA (Participatory Rural Appraisal).These methods draw on various traditions of research including applied anthropology,Participatory Action Research, Rapid Rural Appraisal and agro-eco-systems analysis.Although the origins of the methods are predominantly rural, and generally related toparticipatory planning of natural resource management, they are increasingly used in awide variety of contexts, including urban research and poverty research. Much of theearly development of these approaches took place within a context of participatorycommunity development rather than policy research, and was carried out by NGOs inAfrica and South Asia. The methods place emphasis on the following dimensions:
* local people as analysts rather than informants - whether for the purposes of locallevel planning and action or participatory policy research, a key element of PRA isthat research participants play an active role in generating analyses and directionsfor action, rather than acting as informants who provide information that outsiderswill analyse
- outsiders act as facilitators in the process - stimulating examination of issues bylocal research participants, but striving to avoid adopting a dominant mode inbehavior or attitudes
• group contexts for research, often differentiated according to different socialcategories (women, men, youth elders etc.) - a process of generating consensusyields information and stimulates examination of key problems facing thecommunity or social group in question
* visual sharing of information - a process of generating visual representations (maps,institutional diagrams, causal flow diagrams, seasonality diagrams, matrices) allowsfor transparency, cross-checking by a number of participants, and enhancedparticipation in the process of analysis.
* Empowering weaker, marginal members of communities to participate in theresearch process.
The results of some of these exercises have been described above - but these havetended toward description of the non-visual methods, such as wealth-ranking andpriority ranking.
Largely for reasons of space the outputs of visual exercises such as participatorymapping have not been included. In the following pages a small sample of the visualPRA outputs generated during the research are presented to illustrate the use of thesemethods.
60
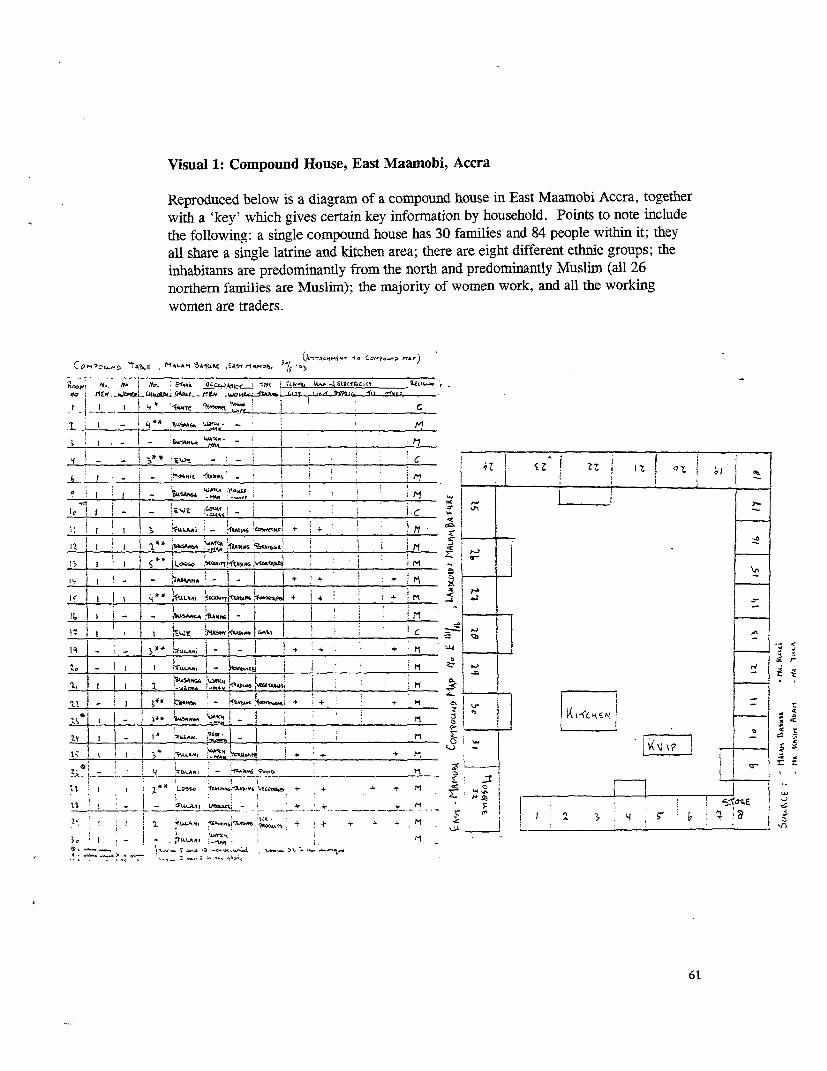
Visual 1: Compound House, East Maamnobi, Accra
Reproduced below is a diagram of a compound house in East Maamobi Accra, togetherwith a 'key' which gives certain key information by household. Points to note includethe following: a single compound house has 30 families and 84 people within it; theyall share a single latrine and kitchen area; there are eight different ethnic groups; theinhabitants are predominantly from the north and predominantly Muslim (all 26northern families are Muslim); the majority of women work, and all the workingwomen are traders.
- J.A44O4;~< 3*t CCZ8)O I z 7e i_ _ _ _ _ _ ____ _ _ _ _ _ _ _ _ _ _ _ Kw, l a i ~ s
_ _I _ _ _ _ _ _ _ _ _ _ _ _ _ _ __Y I I C__ _ _ _ _
I .I _ 2IL* * WaS, A** k - _ I ; '
j~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~
; ~ ~ _ _ _ '__!_,____K=-
3*4 ' *Rw I- __ _ _ _ _ _ 2 , r + : ' a o z i Z z1 4
i.~ . 2. _ | _ iiLfu* t . S .i'_ II I 1_ ________________-___!_____- i c e
_ l . I -tA'F' Z + ri _
1t ~ ~ ~ _ _ _ _ _ _ _ _ _ _ _ _ C, 'l C al6. *e
;_ _ _ I , ; ;, .-
i, I f - 4 *bwsA^ 5^,j ___ ____________ _ _
____ 4 ,, AE i i1o~ 4 ' N I+ u -s
_ _ _ _ -. .. *,,I C^ t44s-1 3fA & .. j
tt~~~ L- ~ F ! N W" .> ; _ -
li 3A > 1.W ". C | _ it j . ' ' 9 Z .: l A < V Al Z ' | j C
_ j^,(_ l w Z_ t I , , o E U:ctr l z iu^^e !1 § § l w . i < ,Z r <s~~O
1;~~~~~~S$% m +jF,,^ ^ ,,# '
2j, Si___ laL4_s - u*>b 7) ni_ 3 lM
1: tI I 1*4Loss tgA.'1.6XAhE~;fEi | + + [tI I -*~~ ~ ~~~~~~~~~~ ~ ~ ~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~ Z i H+II i E
6 1
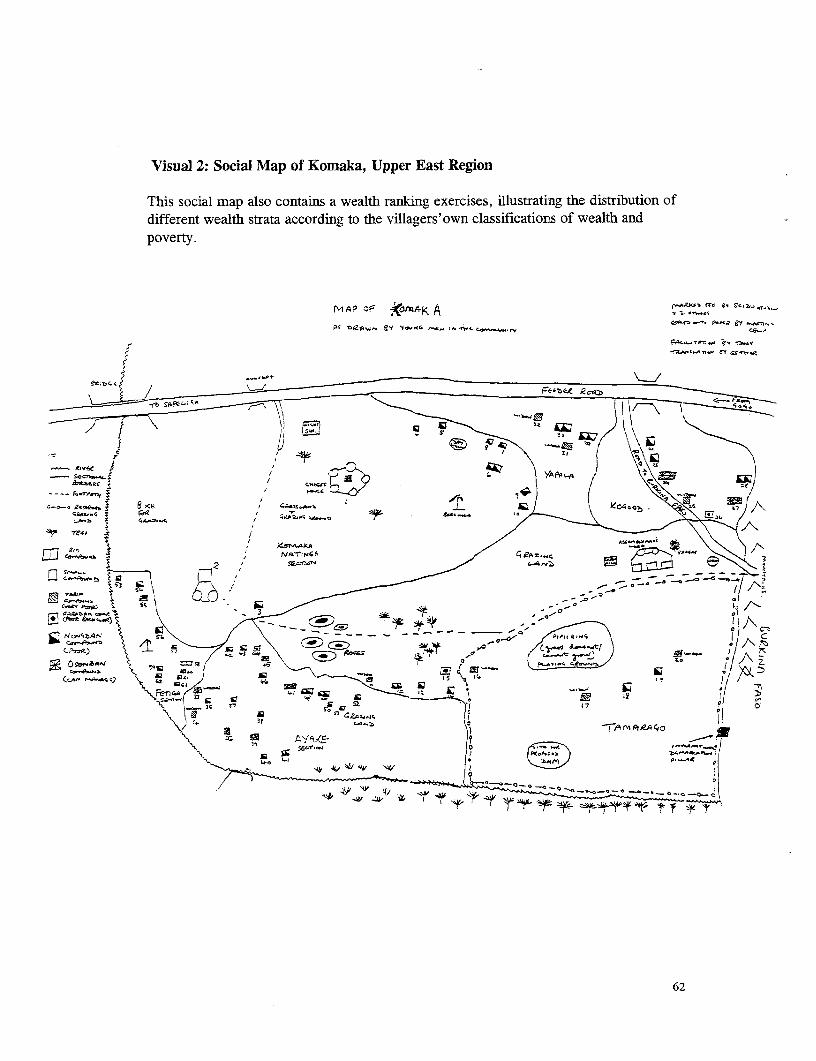
Visual 2: Social Map of Komaka, Upper East Region
This social map also contains a wealth ranking exercises, illustrating the distribution ofdifferent wealth strata according to the villagers'own classifications of wealth andpoverty.
f~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~ ._ f P.,,_s - y ,os -
'
) k }{ fiS A'A CW
fowst74~~~~~~~N AP O; bm-` A-
4 2 ,' :uca _/ ¢;> m2 72orr5tel e\ - 7 -° --
EI V4aAtA.w C a!l * Ct) * - a I
g Oa^< 'e Gs?g *5 _ S {° _ ° ~~~~~~~~~~~~~~0 p*
'7~~~~~~~~~~~~~~~~Z
X Cma X,\14q- 1? f-o-.47~~~~~~~i~4o
"IQ~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~,
AM
0-s<S 04 ;1 4 1 @ 6
62
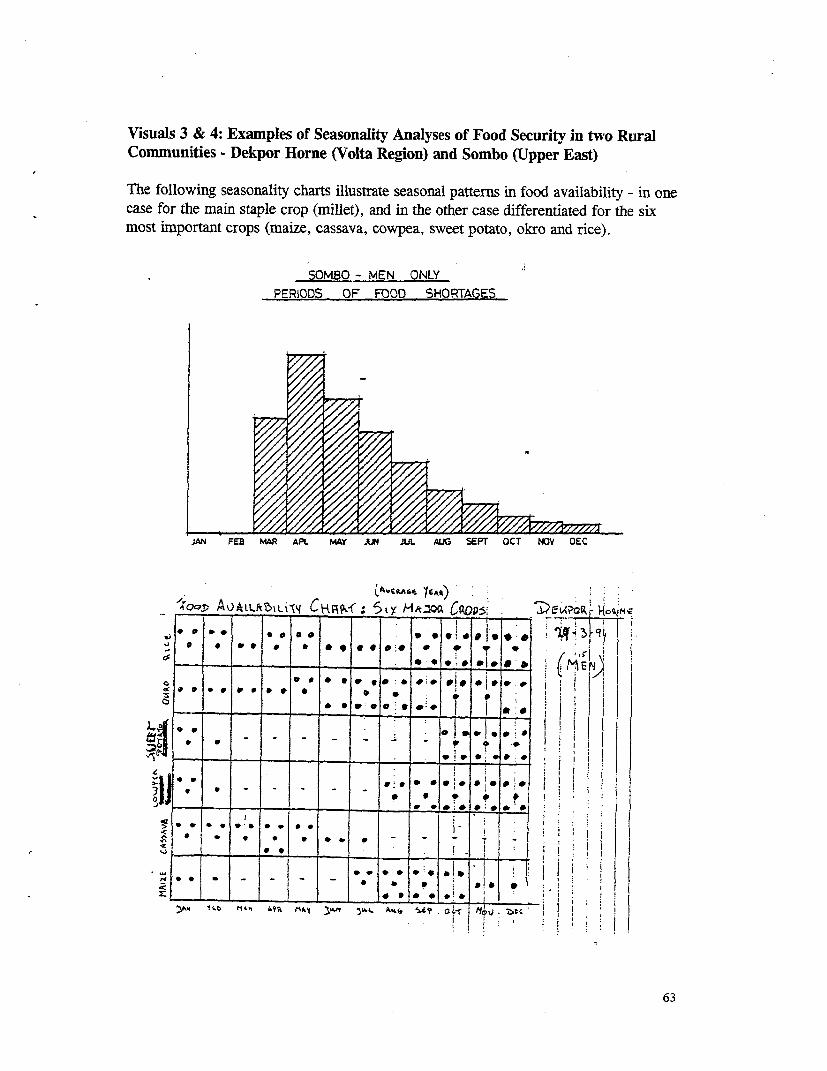
Visuals 3 & 4: Examples of Seasonality Analyses of Food Security in two RuralCommunities - Dekpor Horne (Volta Region) and Sombo (Upper East)
The following seasonality charts illustrate seasonal patterns in food availability - in onecase for the main staple crop (millet), and in the other case differentiated for the sixmost important crops (maize, cassava, cowpea, sweet potato, okro and rice).
SOMBO - MEN ONLYPERIODS OF FOOD SHORTAGES
uw FEB MAR APt MAY JN JUL AuG SEPT OCT NOV OEC
-o, A A L 51 V j c 9 i lAVCBAsS YEAR) :
__O___ AVA5L3L15 M CKRP,: M d*.°0 CpopS5 _ E_ ___,
:T..
*.e . we1 *# e ,eF|**
4 jj. w . - -¢ 3 e A - ' Z-tc
-£E SiL' 9 I 5 ~* 6-0 -s r -s arm -t 9 9W * i 1f . .1.{ * i f
63
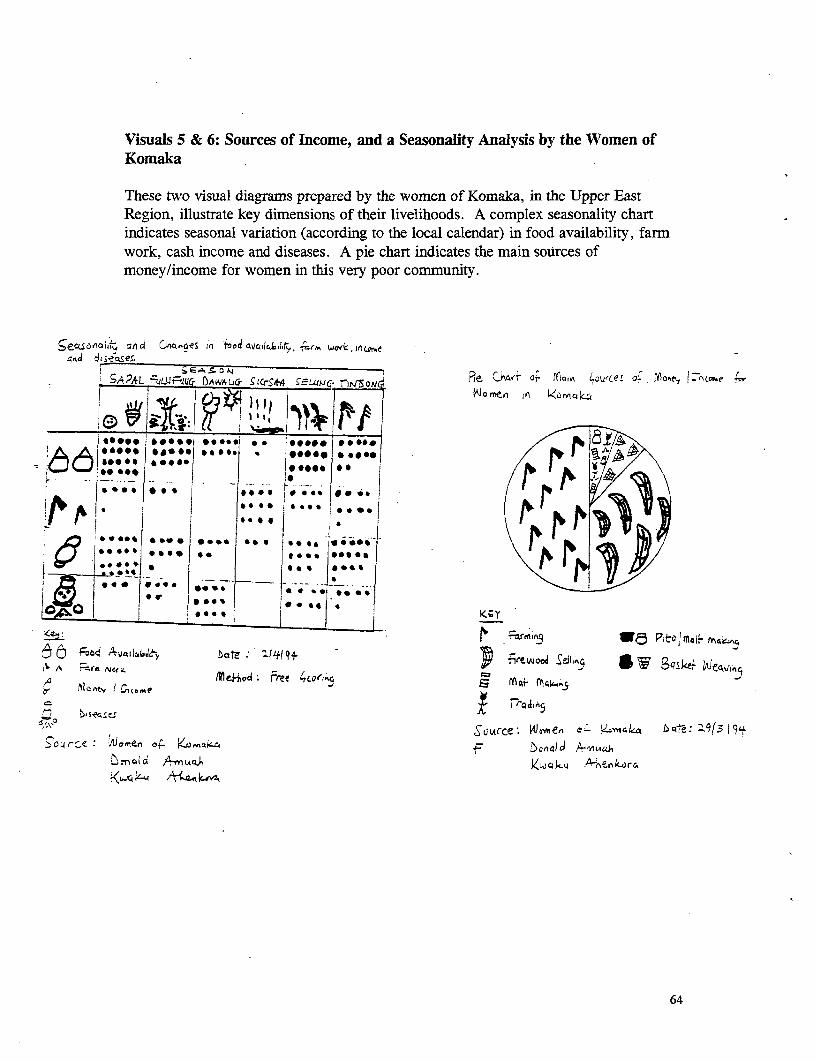
Visuals 5 & 6: Sources of Income, and a Seasonality Analysis by the Women ofKomaka
These two visual diagrams prepared by the women of Komaka, in the Upper EastRegion, illustrate key dimensions of their livelihoods. A complex seasonality chartindicates seasonal variation (according to the local calendar) in food availability, farmwork, cash income and diseases. A pie chart indicates the main sources ofmoney/income for women in this very poor community.
5e4enal;j 5, dCA Ag In f0do 40141o.hIF ro c,, nG>cs.iffi . aiaO',, , -sech;t, ~wrkj~o
SAPAL ut2QFquG IWAUL(-r .Q*4 SEWIJci. r0or Re. Ci- S Tln L CeZ ok fo tZr.e f
.... * 0**O*O.04 so 0 9 on^ z
*** *ae* Is *.e *} i... **.
11 . -* ** -vi§§* *. ****- **0
! A * .*X* *,*~ * .............. * *. . *** -I- tA/4 IiSSOCS***, * *** * ,,...'**. .\ *db
8*0*B : :* **:* C.r..j
t Ao _ .... .. _ _ ... ;
*.~~~~~~~~~~~~ @440g8 PtdtaF 4^
A fF drIn Mei+O4 Free 4co's.V mqt f4;4^. 5
5Cource; 4œn¢ cQ bt:'|1s
an A -' )4"1 utq.~ Vwqk~A *ive r% k-~o r c 4
64
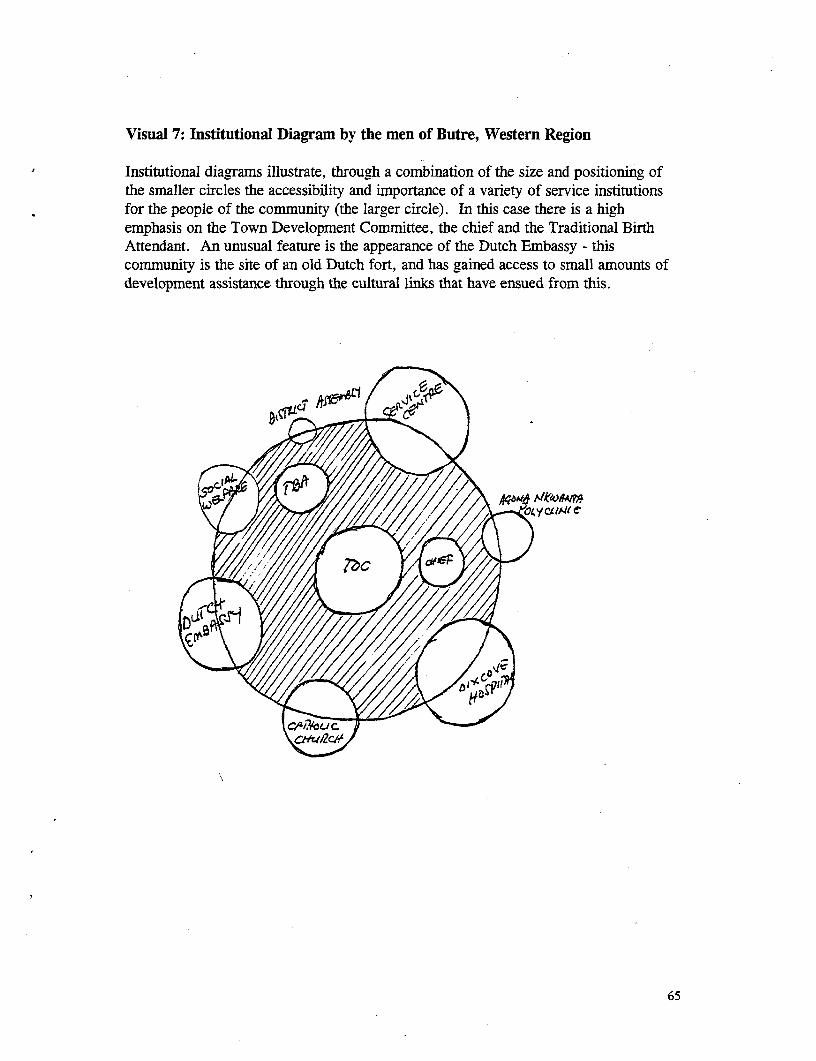
Visual 7: Institutional Diagram by the men of Butre, Western Region
Institutional diagrams illustrate, through a combination of the size and positioning ofthe smaller circles the accessibility and importance of a variety of service institutionsfor the people of the community (the larger circle). In this case there is a highemphasis on the Town Development Committee, the chief and the Traditional BirthAttendant. An unusual feature is the appearance of the Dutch Embassy - thiscommunity is the site of an old Dutch fort, and has gained access to small amounts ofdevelopment assistance through the cultural links that have ensued from this.
65





























