Embed Size (px)
Citation preview
Introduction
Accidental trauma involving the extremities is becom-ing more common due to its connection with increasingsocial violence [1]. The resultant arterial injuries cancause life-threatening bleeding, hematoma, distal ische-mia due to thrombosis, laceration or disruption of thelumen, pseudoaneurysm formation or an arteriovenousfistula in involved segments [1±4]. The detection anddefinition of vascular injury by angiography is essentialfor its optimal management [2±4].
Exsanguinating hemorrhage and pseudoaneurysmare potentially life-threatening complications of limbtrauma. At present, prompt surgical exploration is therecommended treatment. Recently, stent-grafts havebecome available and their percutaneous placementmay be an attractive management alternative in select-ed patients [5±7]. We report an unusual case of an exsan-guinating hemorrhage with a large post-traumatic pseu-doaneurysm involving the femoral artery and complica-ted by wound infection, which was treated by stent-graftplacement.
Case report
A 19-year-old man was hit by a fast-moving truck. Hewas admitted to another hospital with a compound su-pracondylar fracture of right femur, which was treatedby external fixation, debridement and bone grafting.Three weeks later he developed massive hemorrhagefrom the site of fixation and went into shock. He wasstabilized with supportive treatment, including multipleblood transfusions, and one fixator pin was removed,following which his bleeding subsided. The bleeding re-curred 5 days later. At this stage he was referred to ourhospital.
At admission, the limb was edematous, numb, andthe popliteal, posterior tibial and dorsalis pedis pulseswere not palpable. The capillary circulation was pre-served. There was evidence of wound infection at thesite of fracture with cellulitis and pus discharge. Therewas active bleeding from the site of fixation.
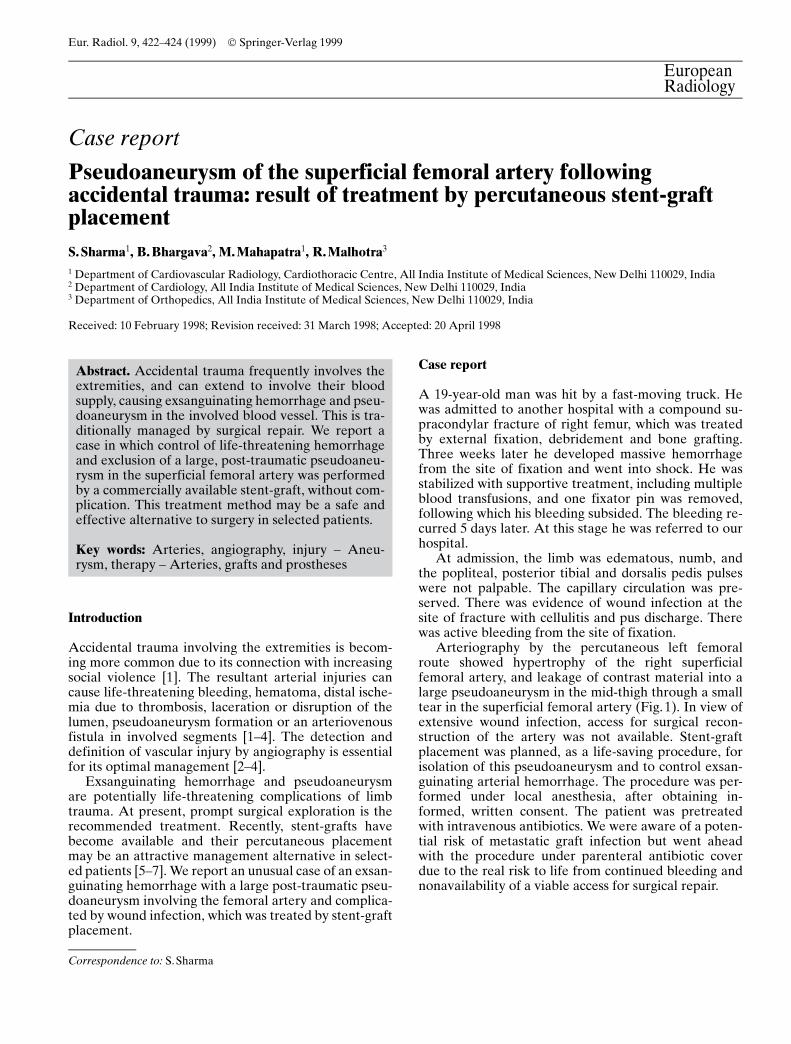
Arteriography by the percutaneous left femoralroute showed hypertrophy of the right superficialfemoral artery, and leakage of contrast material into alarge pseudoaneurysm in the mid-thigh through a smalltear in the superficial femoral artery (Fig.1). In view ofextensive wound infection, access for surgical recon-struction of the artery was not available. Stent-graftplacement was planned, as a life-saving procedure, forisolation of this pseudoaneurysm and to control exsan-guinating arterial hemorrhage. The procedure was per-formed under local anesthesia, after obtaining in-formed, written consent. The patient was pretreatedwith intravenous antibiotics. We were aware of a poten-tial risk of metastatic graft infection but went aheadwith the procedure under parenteral antibiotic coverdue to the real risk to life from continued bleeding andnonavailability of a viable access for surgical repair.
Eur. Radiol. 9, 422±424 (1999) Ó Springer-Verlag 1999
EuropeanRadiology
Case report
Pseudoaneurysm of the superficial femoral artery followingaccidental trauma: result of treatment by percutaneous stent-graftplacementS. Sharma1, B. Bhargava2, M. Mahapatra1, R. Malhotra3
1 Department of Cardiovascular Radiology, Cardiothoracic Centre, All India Institute of Medical Sciences, New Delhi 110029, India2 Department of Cardiology, All India Institute of Medical Sciences, New Delhi 110029, India3 Department of Orthopedics, All India Institute of Medical Sciences, New Delhi 110029, India
Received: 10 February 1998; Revision received: 31 March 1998; Accepted: 20 April 1998
Abstract. Accidental trauma frequently involves theextremities, and can extend to involve their bloodsupply, causing exsanguinating hemorrhage and pseu-doaneurysm in the involved blood vessel. This is tra-ditionally managed by surgical repair. We report acase in which control of life-threatening hemorrhageand exclusion of a large, post-traumatic pseudoaneu-rysm in the superficial femoral artery was performedby a commercially available stent-graft, without com-plication. This treatment method may be a safe andeffective alternative to surgery in selected patients.
Key words: Arteries, angiography, injury ± Aneu-rysm, therapy ± Arteries, grafts and prostheses
Correspondence to: S.Sharma

Technique
At the beginning of the procedure, a 7 Fr, 45 cm long ar-terial sheath with an indwelling valve (Boston Scientific,Watertown, Mass.) was placed in the right groin by anantegrade, percutaneous route. Heparin (5000 IU) wasgiven at this stage. An exchange-length J-shaped guide-wire was placed across the aneurysm. The right superfi-cial femoral artery measured 5.2 mm in diameter. Thelocation of the site of the leak and the pseudoaneurysmwas surface-marked by placing clamps at the proximaland distal ends of the lesion. A 6 mm diameter, 6 cmlong-self-expanding stent-graft (Passager, Boston Scien-tific, Watertown, Mass.) was used. Its cartridge wasthreaded over the guidewire and 50 cm3 of ice-cold ster-ile saline was flushed from the side-vent of the cartridgeto shrink the stent to its smallest size. It was locked withthe 7 Fr sheath by tightening the leur lock. The stent-graft was positioned across the aneurysm with the helpof a pusher catheter and was released by withdrawingthe sheath over it.
The stent-graft was expanded further by a 6 mm di-ameter balloon catheter that was inflated with contrastmaterial diluted 1 :3 with saline at 40 �C. A check arte-riogram showed isolation of the aneurysm, no leakageof contrast material and brisk antegrade flow into thedistal arteries (Fig. 2). The guidewire was withdrawn,the sheath removed, and hemostasis achieved by man-ual compression. No complication was observed.
The patient was started on antiplatelet therapy withoral aspirin 100 mg/day for 3 months. He also receivedantibiotics for 5 days after treatment. The bleeding stop-ped completely after the procedure and the distal pulseswere well felt. Follow-up evaluation was performed byclinical examination and duplex sonography. At3 months there was no recurrence of bleeding, distalpulses were well felt and showed normal flow velocities.There was no evidence of graft infection during follow-up, as evidenced by total and differential leucocyticcounts, C-reactive protein and blood culture.
Discussion
Stent-graft isolation of aortic or arterial aneurysms hasemerged as an attractive alternative to surgery in se-lected patients. The technical feasibility and initial re-sults in patients with aortic and iliac artery aneurysms,and with arteriovenous fistula, have been reported[5±11]. Their use in treating vascular injuries has rarelybeen reported [5, 6].
Christensen and colleagues [5] reported one case ofan asymptomatic common iliac artery pseudoaneurysmtreated by a covered stent. Althaus et al. [6] reportedtwo patients with traumatic injury to the external iliacartery who were treated by self-expanding, uncoatedstents. The injury was caused by a road accident inboth cases and Wallstents (Schneider, Minneapolis,Minn.) were used to isolate the injured segment. Onepatient died 1 h later and the second patient was doingwell 12 months later.
The use of stent-grafts in the emergency treatment oftraumatic arterial injuries has rarely been reported[5±13]. Our case confirms the viability of this treatmentmethod in the emergency room. The procedure is sim-ple and does not require additional expertise. We useda commercially available covered stent (Passager, Bos-ton Scientific) to isolate the pseudoaneurysm and con-trol exsanguinating hemorrhage. Surgical access to thebleeding site and the pseudoaneurysm was not availabledue to the presence of extensive wound infection. Theother surgical alternative was to ligate the superficialfemoral artery in its proximal part and interpose a longjump graft between the proximal femoral and distalpopliteal arteries. However, the presence of extensiveedema and widespread superficial infection precludedthis approach. The only other option was to amputatethe limb. Percutaneous endoprosthesis placement toisolate the diseased arterial segment is an attractivemanagement alternative. However, the presence of in-fection is generally considered as an absolute contrain-dication for stent-graft placement. If the infection ex-
S.Sharma et al.: Stent-graft isolation of femoral artery pseudoaneurysm 423
Fig.1. Selective right superficial femoral arteriogram in the an-teroposterior view showing leakage of contrast material through ahole in the artery and an adjacent large pseudoaneurysm
Fig.2. Selective right su-perficial femoral arterio-gram in the anteroposteriorview after stent-graftplacement showing recon-structed right superficialfemoral artery with isola-tion of the aneurysm andno leakage of contrast ma-terial

tends to involve the stent-graft, it can have serious con-sequences. There is also a possibility of metastatic graftinfection. We were aware of these risks but employedthis treatment method as a life-saving measure in viewof the deteriorating general condition of the patientand lack of a viable surgical alternative. The follow-upresponse has confirmed its utility in extreme situations.
Percutaneous stent-graft insertion in the manage-ment of arterial trauma offers many advantages, includ-ing short procedure time, less invasive technique, im-mediate isolation of the aneurysm and bleeding sitefrom the circulation without the need for general anes-thesia, minimal blood loss, and reduced hospital stay,morbidity and mortality. These advantages are especial-ly relevant in patients at high risk to surgery because ofadvanced cerebrovascular, cardiovascular or other sys-temic disease.
The overall complication rate is low [5±11]. The re-ported complications include distal migration of thestent, residual leak, late growth of the aneurysmal cav-ity, distal embolization, infection and contralateral ve-nous thrombosis in patients with an iliac artery aneu-rysm [6±10]. It is also important to remember that endo-vascular treatment with a stent-graft may not relieve thecompressive symptoms caused by the aneurysm. Thefate of the thrombosed aneurysms is not clearly under-stood. Therefore, in patients with symptoms caused bycompression from the aneurysmal sac, this treatmentmethod may not be indicated unless associated medicaldisease precludes surgery.
We conclude that endovascular treatment of trau-matic arterial tear, resultant pseudoaneurysm and ex-sanguinating hemorrhage is technically feasible in emer-gency situations. Its use in the presence of infection isunusual but may be warranted by overriding factors,such as an immediate threat to life. There is a paucityof data to show the long-term viability of this treatmentmethod. Further experience is needed before its placerelative to surgery can be established.
References
1. Ulflaker R, Elliott BM (1996) Percutaneous endoluminal stent-graft repair of an old traumatic femoral arteriovenous fistula.Cardiovasc Intervent Radiol 19: 120±122
2. Jebara VA, Haddad SN, Ghossain MA (1991) Emergency ar-teriography in the assessment of penetrating trauma to the low-er limbs. Angiology 42: 527±532
3. Rose SC, Moore EE (1988) Trauma angiography: the use ofclinical findings to improve patient selection and case prepara-tion. J Trauma 28: 240±245
4. Frykberg ER, Crump JM, Vines FS, et al (1989) A reassess-ment of the role of arteriography in penetrating proximity ex-tremity trauma: a prospective study. J Trauma 29: 1041±1052
5. Christensen L, Justensen P, Larsen KE (1996) Percutaneoustreatment of an iliac pseudoaneurysm with endoprosthesis im-plantation. Acta Radiol 37: 542±544
6. Althaus SJ, Keskey TS, Harker CP, Coldwell DM (1996) Percu-taneous placement of self-expanding stent for acute traumaticarterial injury. J Trauma 41: 145±148
7. Parodi J (1996) Endovascular repair of aortic aneurysms, arte-riovenous fistulas and false aneurysms. World J Surg 20:655±663
8. Blum U, Voshage G, Lammer J, et al (1997) Endoluminalstent-grafts for infrarenal abdominal aortic aneurysms. N EnglJ Med 336: 13±20
9. Murphy K, Richter G, Henry M, Encarnacion C, Le V, PalmazJ (1996) Aortoiliac aneurysms: management with endovascularstent-graft placement. Radiology 198: 473±480
10. Razavi M, Dake M, Semba C, Nyman U, Liddell R (1995) Per-cutaneous endoluminal placement of stent-grafts for the treat-ment of isolated iliac artery aneurysms. Radiology 197: 801±804
11. Krajcer Z, Khoshnevic R, Leachman D, Herman H (1997) En-doluminal exclusion of an iliac artery aneurysm by wallstentendoprosthesis and PTFE vascular graft. Texas Heart Inst J24: 11±14
12. Blais C, Bonneau D (1994) Postangioplasty pseudoaneurysmtreated with a vascular stent. AJR 162: 238±239
13. O'Brien CJM, Rankin RN (1994) Percutaneous managementof large neck aneurysms with arterial stent placement and coilembolization. J Vasc Interr Radiol 5: 443±448
S.Sharma et al.: Stent-graft isolation of femoral artery pseudoaneurysm424
Book review EuropeanRadiology
Prescher A., Bohndorf K.: Radiologische Anatomie und Topogra-phie des Halses. Stuttgart: Georg Thieme, 1996, 214 pages, 107 il-lustrations, DM 198.00, ISBN 3-13-106721-7
The authors of this book state in their preface that they intend tointroduce physicians, medical students and neck surgeons to the in-terpretation of imaging procedures of the neck. Accordingly thelayout of the content conforms to the needs of daily radiologicalpractice. It starts with typical conventional tomograms of the cervi-cal spine in two planes, including useful measurements. The largestpart of the book deals with computed tomography (CT) and mag-netic resonance tomography (MRT) of the neck in the typical threeplanes. The axial plane is illustrated only for CT images, the au-thors stating that direct comparison of axial CT and MRT showsthat information is redundant. Some readers might disagree withthis opinion since nerves, vessels and neck compartments are vi-sualized somewhat differently by MRT. However, the presentedaxial CT series and the attached sketches are of very good quality
and high educational standard. The MR tomograms, presented inthe coronal and sagittal planes, confirm on the other hand the greatvalue of MRT in the evaluation of soft tissue structures of the neck.
Additional chapters deal with the anatomy of vessels, nerves,lymph nodes, ligaments and salivary glands of the neck area usingimages or sketches. A special chapter covers functional radiologyof the pharynx and larynx. These topics are still important in spiteof their limited use today. Some sketches of the anatomical com-partments of the neck and a large index of anatomical expressionswith reference to their presentation in the CT and MR sectioncomplete this little atlas.
The book is handy and comprehensive and can be recommend-ed for daily work in CT and MRT departments. Since it is based onthe Nomina Anatomica (6th edn, Churchill Livingstone 1989) itcan be used by non-German readers also. The price of DM 198.00seems reasonable for all persons who work especially in the fieldof head and neck. K. Reisner, Karlsruhe





























