Embed Size (px)
Citation preview
1
PRP, BMAC, Stem cells The Basics
Jim Bradley M.D.Clinical Professor Orthopedics UPMC
Head Team Physician – Pittsburgh Steelers Consultant – Miami Marlins
Justin Arner MD Resident UPMC
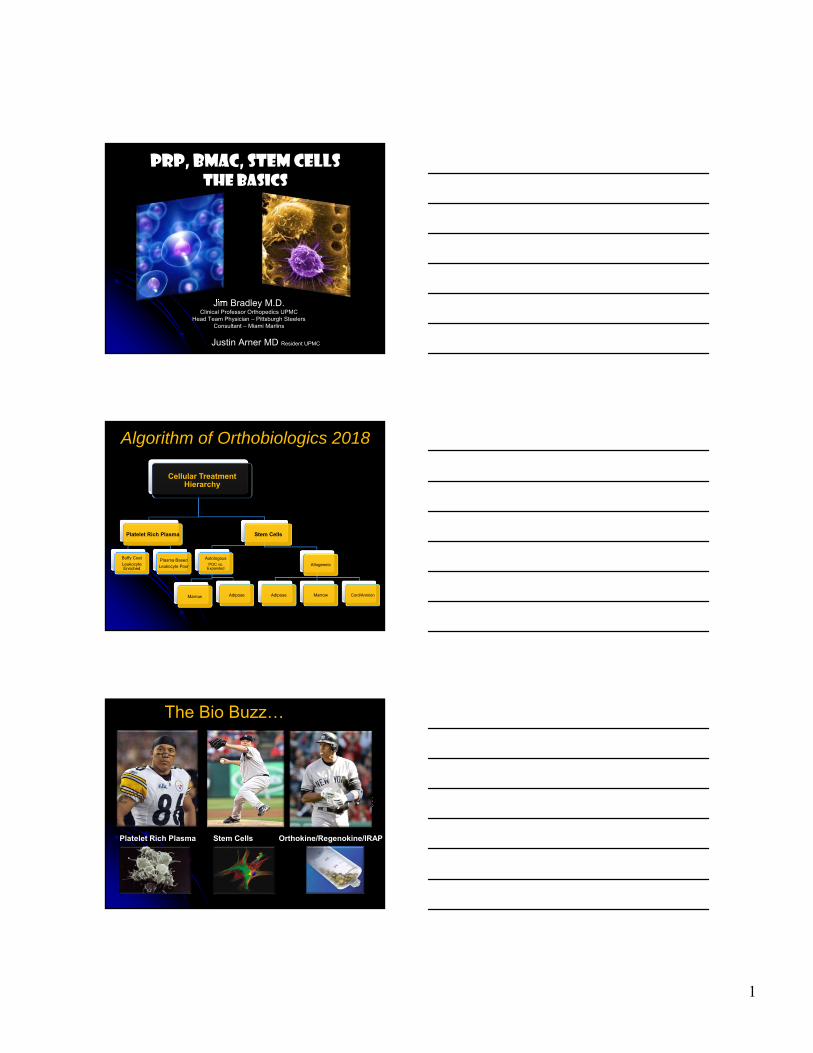
Cellular Treatment Hierarchy
Platelet Rich Plasma
Buffy Coat
Leukocyte Enriched
Plasma Based
Leukocyte Poor
Stem Cells
AutologousPOC vs.
Expanded
Marrow Adipose
Allogeneic
Adipose Marrow Cord/Amnion
Algorithm of Orthobiologics 2018
The Bio Buzz…
Platelet Rich Plasma Stem Cells Orthokine/Regenokine/IRAP
Growth factors from platelets & factors in the plasma that modulate the healing process.
• Large amount of literature (Level 1&2)• Better understanding of best PRP form
Multipotent cells, able to differentiate into several cell lineages.
Clinical use in orthopedics is increasing specifically for cartilage issues
Anabolic and inhibitory cytokines taken from incubated monocytes
• Very little clinical data• High cost/hype• Not cleared in the US• Requires blood banking • Any benefits over PRP?

2
The Top 10 Things you need to know about PRP & Stem cells
#1 There are Critical Obstacles to Widespread
Biologic TxRegulatory Pathway
Point of care cellular Tx Minimal manipulation Autologous Efficacy not related to the metabolic activity of the cells
Research High level comparative studies (millions $$$) Used in many applications, need data on all indications
Reimbursement Coding for some products in not available Deemed “Experimental” by Ins. Co. Individual approvals
FDAIndications to date: “an orthopedic surgical site”

3
Legality
NFLMLBNHLNCAAWADA
GOOGLE Sites 2018 PRP - 19,100,000
Stem cells - 93,500,000PRP - 20,100,000Stem Cells - 103,000,000
#2 Definition of PRP
Platelet-Rich
Plasma
Autologous plasma fraction that has a concentration of platelets above
baseline (200,000 platelets/uL)1
Autologous concentration of
platelets in a small volume of plasma.2
Plasma fraction with a concentration of at
least 1,000,000 platelets/uL.3
1. L. Mazzucco, V. B., E. Cattana, R. Guaschino, P. Borzini,: Not every PRP-gel is born equal Evaluation of growth factor availability for tissues through four PRP-gel preparations: Fibrinet, RegenPRP-Kit, Plateltex and one manual procedure. , 2009.
2. Marx, R. E.: Platelet-rich plasma: evidence to support its use. Journal of Oral and Maxillofacial Surgery, 62(4): 489-496, 2004.3. Marx, R.E. Platelet-Rich Plasma (PRP): What is PRP and what is not PRP? Implant Dentistry, 10(4): 225-228, 2001.
There is None

4
Robert Marx, D.D.S. “definition” of PRP platelet concentration
“incorrectly quoted as dogma” 2001 White Paper in Implant Dentistry1
Minimum 1,000,000 platelets/µL = 5x PRP Whole blood baseline – 1.5 -2 x 105 platelets µL
NO supporting citations or references
1. Marx RE. Platelet-rich plasma (PRP): what is PRP and what is not PRP? Implant Dent. 2001;10(4):225-8.
2. Marx RE, Carlson ER, Eichstaedt RM, Schimmele SR, Strauss JE, Georgeff KR. Platelet-rich plasma: Growth factor enhancement for bone grafts. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 1998 Jun;85(6):638-46.
Definition of PRP
High concentrations (6-11x) may have a paradoxically inhibitory effect
1. Weibrich G et al. Effect of platelet concentration in platelet-rich plasma on peri-implant bone regeneration. Bone 2004; 34(4): 665-671.2. Choi et al. Effect of PRP concentration on the viability and proliferation of aveolar bone cellsInter J Maxillofac Surg. 20053. Graziani F et al. The in vitro effect of different PRP concentrations on osteoblasts and fibroblasts. Clin Oral Impl Res 2006; 17: 212-219.
Optimal Concentration of Platelets is Unknown !!!
Viability & proliferation of cells was suppressed by high concentrations but increased by moderate concentrations. 2
It may be different for different pathologies
1. Concentration of platelets to bind the available GF receptors without oversaturation
2. Triggering a positive proliferative response3. Without inducing a negative feedback inhibition4. Receptor levels may vary between tissues
therefore ideal PRP concentrations may as well
What is the Optimal Concentration of Platelets?

5
#3 All Current Systems are NOT the same
ACP, Biomet GPS, PReP, MTF cascade, Harvest & Magellan
Differences in blood volume, centrifuge rate/time, delivery method, activating agent, WBC count, PRP volume, Platelet & GF concentration
What do we have today ?
Buffy coat based PRP systems GPS Harvest Magellan
Plasma based PRP systems ACP Cascade BTI (Anitua/Sanchez)
All use platelet GF release What differs is WBC’s, RBC’s & plasma
concentrations
#4 PRP is EXTREMELY Complex
Delivery methods Activate +/-
Plasma-based vs. Buffy coat White cells +/-
Dozens of commercially available systems (40) Variable spin protocols & cellular milieu product
Significant variability in cellular concentrations Vs. systems Vs. individuals Vs. SAME individual
Frequency of dosing Acute vs. Chronic? Anatomic site specific?

6
Alpha granules
Platelet activators
Meta‐analysis
WBC content
Exogenous activation
Clotting factors
Spray
Neutrophil rich
Buffy coat systems
Plasma based systems
Neutrophil poor
Delivery technique
Hydrogel
Endogenous activation
Thrombin
Ultrasound guided injections
Clot/Scaffold
Ca2Cl + Thrombin
Tissue specific
Baseline Levels
Activation Method
Varied [platelets/μL]
Erythrocytes
Ca2Cl
Type I Collagen
> 1,250,000 platelets/μL
> 750,000 to 1,250,000 platelets/μL
> Baseline to 750,000 platelets/μL
Platelet‐poor plasma
Dense granules
Fibrinogen levelsGrowth factor levels
Spin Protocol
Varied individual platelet count
Preparation method
Platelet aggregation
pH
Local anesthetics
Anticoagulants
Anti‐oxidant response
Dosing Frequency
Delivery platform
Antimicrobial effect
Inflammation
Cytokines
Ideal anatomic location
Closed procedure
Open procedure
ChronicAcute
Growth factor kinetics
Platelet‐rich plasma
Multitude of Variables Contribute to Mixed Results
#5 PRP: A Previous Decade of Flawed Research Methodology??
#6 The Fundamentals Have Been Missed!!
Back to the Fundamentals : the beginning of the PAW system
7
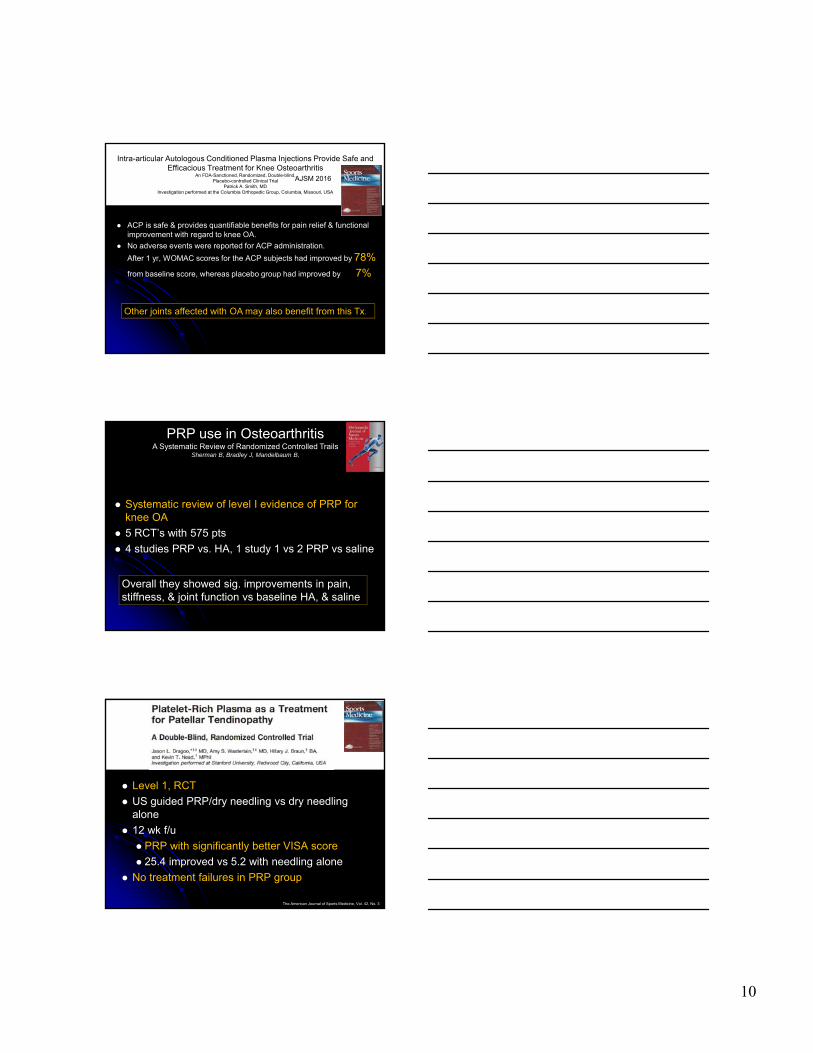
… and It can get VERY complicated
Platelet Rich Plasma: The PAW Classification System: Arthroscopy Vol 28 No. 7 July 2012
P2 n I B beta
#7 Where ?
OVERALL Office Experience
Total > 450 patients 90% Athletes - > 900 injections 250 lower extremities injuries 200 upper extremities injuriesNFL, MLB, NHL (30%)
Only injection code used Recently had to charge $200/injection

8
Clinical ApplicationsMy Experience
Knee Disorders
• DJD
• MCL/LCL sprains
• Patellar Tendonitis
• Symptomatic Bipartite Patella
Ankle/LE Disorders
• Achilles Tendonitis
• Ankle Sprain (ATFL)
• Peroneal tendons
• Soleus Muscle Strain
• High Ankle Sprains
Soft Tissue LE Disorders
• Rectus Strain
• Proximal Hamstring Strain ( Ct guided )
• Mid/Distal Hamstring Strain
Clinical Applications
Shoulder Disorders
• Shoulder DJD
• Rot (prct) Cuff Tears
• Rotator Cuff Tendinopathy
• SLAP Lesions
• AC Separation
Elbow Disorders
• UCL (partial) tear
• Med/Lat Epicondylitis
• OCD lesions
My Clinical Protocol
ACP - 1 injection a wk for 3wks if better after 2 no more
Start 24-48 hrs after acute injuryNo changes rehab protocol

9
Office Overall Outcomes
Successful outcome = Resolution of symptoms, asymptomatic return to play, no surgery
Poor outcome = Recurrence of symptoms, inability to return to play, surgery
Outcomes/Success RateKnee
Good
Not GoodGood
Not Good
Good
Not Good
MCL 100% DJD 74%
Patellar Tendon 43%
Formulation Specific ResultsAuthor Diagnosis Formulation Outcome
Patel, AJSM 2013 Knee OA Leukocyte poor Significant difference
Filardo, Musk.Disord 2012
Knee OA Leukocyte rich No difference
Cerza, AJSM 2012 Knee OA Leukocyte poor Significant difference
Sanchez, Arthro2012
Knee OA Leukocyte poor Significant difference
Spakova, Am J Phys Med Rehab 2012
Knee OA Leukocyte poor Significant difference
Filardo, KSSTA 2012
Knee OA Leukocyte rich No difference
2014 TOBI, PRP Symposium Jason Dragoo, MD
10
Intra-articular Autologous Conditioned Plasma Injections Provide Safe and Efficacious Treatment for Knee Osteoarthritis
An FDA-Sanctioned, Randomized, Double-blind,Placebo-controlled Clinical Trial
Patrick A. Smith, MDInvestigation performed at the Columbia Orthopedic Group, Columbia, Missouri, USA
ACP is safe & provides quantifiable benefits for pain relief & functional improvement with regard to knee OA.
No adverse events were reported for ACP administration.
After 1 yr, WOMAC scores for the ACP subjects had improved by 78%
from baseline score, whereas placebo group had improved by 7%
AJSM 2016
Other joints affected with OA may also benefit from this Tx.
Systematic review of level I evidence of PRP for knee OA
5 RCT’s with 575 pts
4 studies PRP vs. HA, 1 study 1 vs 2 PRP vs saline
PRP use in OsteoarthritisA Systematic Review of Randomized Controlled Trails
Sherman B, Bradley J, Mandelbaum B,
Overall they showed sig. improvements in pain, stiffness, & joint function vs baseline HA, & saline
Level 1, RCT
US guided PRP/dry needling vs dry needling alone
12 wk f/u
PRP with significantly better VISA score
25.4 improved vs 5.2 with needling alone
No treatment failures in PRP group
The American Journal of Sports Medicine, Vol. 42, No. 3

11
Level 4, Case series 28 athletes
17 professional 11 semiprofessional
*Chronic, failed conservative tx PRP injection x 3 2 yr f/u Significantly improved VISA, VAS, and lysholm scores 16 pts (57%) returned to completely normal Only 3 needed surgery
The American Journal of Sports Medicine, Vol. 42, No. 4
My top 4 LE office favorites
1. Early OA
2. MCL/LCL sprains
3. Early splits in the post/med menisco-capsular junction
4. Elbow partial UCL
What does the Literature say about shoulder & PRP?

12
Positive effectAuthor Yea
rJournal
Level of evidence
Investigation Effect N Avg f/u (mo.)
Limitations
Ebert 2017 AJSM 1 PRP effect on double row SS repairs ≤ 20mm(2 injections @ 7 & 14 days)
PRP:-Significant postop clinical improvements.-High level pt satisfaction.-Greater max abd strength @ midterm f/u.
6 42 -PRP components not measured.-The reported [Platelet] was obtained from the general commercial system info.-All [Platelet], [WBC], & [GF] from individual pts were assumed to be the same.-Tendon quality was evaluated via subjective measures.-Results not correlated with larger or multiple tears, or single-row repair.-Pts were not blinded to their randomization (+/- post-op injection).-Study did not evaluate or report on return to sport involving higher demand upper limb movements.
Sengodan 2017 J Clin Imaging Sci
2 U/S guided L-PRP effect on Partial RCTs (52% Traumatic 48% Degenerative)
L-PRP: -Markedly improved clinical, radiological, and functional shoulder outcomes.
20 2 -PRP components not measured or reported.-Various tear etiologies, types, and locations.-No control group.-Small sample size.-Short f/u.
Kim 2017 Cell Transplant
2 BMAC-PRP effect on TDSCs &Partial RCTs non-responsive to conservative tx
BMAC-PRP: -Enhancedproliferation/migration of TDSCs & prevents aberrant chondrogenic
12 3 -PRP components not measured.-TDSCs from a single donor.-No control group.-Small sample size.-Short f/u.
Positive effectAuthor Yea
rJournal
Level of evidence
Investigation Effect N Avg f/u (mo.)
Limitations
Ebert 2017 AJSM 1 PRP effect on double row SS repairs ≤ 20mm(2 injections @ 7 & 14 days)
PRP:-Significant postop clinical improvements.-High level pt satisfaction.-Greater max abd strength @ midterm f/u.
6 42 -PRP components not measured.-The reported [Platelet] was obtained from the general commercial system info.-All [Platelet], [WBC], & [GF] from individual pts were assumed to be the same.-Tendon quality was evaluated via subjective measures.-Results not correlated with larger or multiple tears, or single-row repair.-Pts were not blinded to their randomization (+/- post-op injection).-Study did not evaluate or report on return to sport involving higher demand upper limb movements.
Sengodan 2017 J Clin Imaging Sci
2 U/S guided L-PRP effect on Partial RCTs (52% Traumatic 48% Degenerative)
L-PRP: -Markedly improved clinical, radiological, and functional shoulder outcomes.
20 2 -PRP components not measured or reported.-Various tear etiologies, types, and locations.-No control group.-Small sample size.-Short f/u.
Kim 2017 Cell Transplant
2 BMAC-PRP effect on TDSCs &Partial RCTs non-responsive to conservative tx
BMAC-PRP: -Enhancedproliferation/migration of TDSCs & prevents aberrant chondrogenic
12 3 -PRP components not measured.-TDSCs from a single donor.-No control group.-Small sample size.-Short f/u.
Positive effectAuthor Yea
rJournal
Level of evidence
Investigation Effect N Avg f/u (mo.)
Limitations
Tahririan 2016 Adv Biomed Res
2 U/S guided PRP effect on Pts with <1cm partial RCTs (bursal side) non-responsive to conservative tx
Single PRP injection:-Reduced pain & improved ROM in pts w/ bursal side partial RCT who failed to respond to conservative tx.-Data showed the effectiveness of PRP injection reduces by age.
17 3 -Platelets were measured but WBC count was not.-No control group.-Non-randomized.-Small sample size.-Short f/u.
D’Ambrosi 2016 Musculoskel Surg
1 PRP effect on Degenerative full-thickness SS tears (grade C2-C3)
PRP: -Reduces pain @ short-term f/u, allowing more rapid recovery of mobilization & improved function.-No significant difference in DASH score or U/S after 6 mo.
40 6 -Measured pts baseline [Platelet] but did not measure PRP components.-No placebo group.-Short f/u.
Lädermann 2016 Orthop Traumatol Surg Res
2 L-PRP clinical & radiologic effects on SS interstitial RCTs
L-PRP: -Showed significant and clinically relevant effect on RCT size and clinical parameters.
25 6 -PRP components not measured.-The reported [Platelet] was obtained from the general commercial system info.-All [Platelet], [WBC], & [GF] from individual pts were assumed to be the same
13
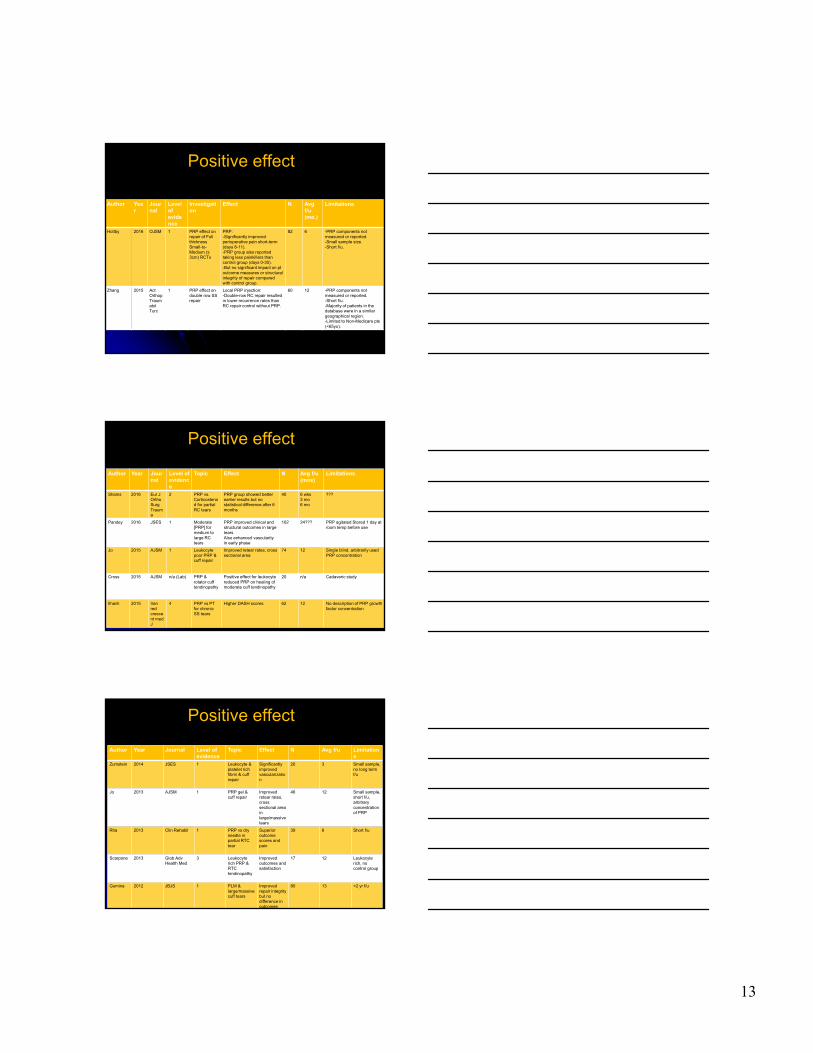
Positive effect
Author Year
Journal
Level of evidence
Investigation
Effect N Avg f/u (mo.)
Limitations
Holtby 2016 OJSM 1 PRP effect on repair of Full thickness Small-to-Medium (≤ 3cm) RCTs
PRP: -Significantly improvedperioperative pain short-term (days 8-11). -PRP group also reported taking less painkillers than control group (days 0-30).-But no significant impact on ptoutcome measures or structural integrity of repair compared with control group.
82 6 -PRP components not measured or reported.-Small sample size.-Short f/u.
Zhang 2015 Act Orthop Traumatol Turc
1 PRP effect on double row SS repair
Local PRP injection:-Double-row RC repair resulted in lower recurrence rates than RC repair control without PRP.
60 12 -PRP components not measured or reported.-Short f/u.-Majority of patients in the database were in a similar geographical region.-Limited to Non-Medicare pts (<65yo).
Positive effect
Author Year Journal
Level of evidence
Topic Effect N Avg f/u (mos)
Limitations
Shams 2016 Eur J Ortho SurgTrauma
2 PRP vs. Corticosteroid for partial RC tears
PRP group showed better earlier results but no statistical difference after 6 months
40 6 wks3 mo6 mo
???
Pandey 2016 JSES 1 Moderate [PRP] for medium to large RC tears
PRP improved clinical and structural outcomes in large tearsAlso enhanced vascularity in early phase
102 24??? PRP agitated Stored 1 day at room temp before use
Jo 2015 AJSM 1 Leukocyte poor PRP & cuff repair
Improved retear rates, cross sectional area
74 12 Single blind, arbitrarily used PRP concentration
Cross 2015 AJSM n/a (Lab) PRP & rotator cuff tendinopathy
Positive effect for leukocyte reduced PRP on healing of moderate cuff tendinopathy
20 n/a Cadaveric study
Ilhanli 2015 Iran red crescent med J
4 PRP vs PT for chronic SS tears
Higher DASH scores 62 12 No description of PRP growth factor concentration
Positive effect
Author Year Journal Level of evidence
Topic Effect N Avg f/u Limitations
Zumstein 2014 JSES 1 Leukocyte & platelet rich fibrin & cuff repair
Significantly improved vascularization
20 3 Small sample, no long term f/u
Jo 2013 AJSM 1 PRP gel & cuff repair
Improved retear rates, cross sectional area in large/massive tears
46 12 Small sample, short f/u, arbitrary concentration of PRP
Rha 2013 Clin Rehabil 1 PRP vs dry needle in partial RTC tear
Superior outcome scores and pain
39 6 Short f/u
Scarpone 2013 Glob Adv Health Med
3 Leukocyte rich PRP & RTC tendinopathy
Improved outcomes and satisfaction
17 12 Leukocyte rich, no control group
Gumina 2012 JBJS 1 PLM & large/massive cuff tears
Improved repair integrity but no difference in outcomes
80 13 <2 yr f/u

14
Positive effect
Author Year Journal Level of evidence
Topic Effect N Avg f/u Limitations
Barber 2011 Arthroscopy 3 PRFM & Cuff repair
Improved retear rates and Rowe scores w/PRFM
40 31 Sample size, lack of randomization
Randelli 2011 JSES 1 PRP & Rotator cuff repair
Reduced pain in first few postoperative months
53 24 Unknown quantity of platelets & growth factors
Neutral/Negative effectAuthor Year Journ
alLevel of evidence
Topic Effect N Avg f/u (mos)
Limitations
Gwinner 2016 Arch Ortho Trauma Surg
3 Two-staged PRP application to RC repair
No significantimprovement but trend for lower retear rates
36 24 ???
Flury 2016 AJSM 1 PRP vs. Ropivacaine (local anesthetic)
PRP group showed no significant functional improvement
120 24 No description of growth factor concentration only 1 injection platelet concentration unknown dilution with NaCl
Say 2016 J Ortho Surg
3 Single dose of PRP vs. steroid for subacromialimpingement sydrome
Steroid injection was more effective than PRP in Constant score and VAS pain
60 6 wks6 mo
PRP was prepared manually using single spin rotation.Reported 4 fold increase but did not report actual [platelets/μL]
Verhaegen 2016 JSES 2 Arthroscopic needling for RC augmented with PRP
PRP group showed no beneficial effect on RC healing
40 3 mo6 mo1 yr
No description of growth factor concentration, leukocyte-rich prp, short F/U
Wehren 2015 KSSTA 3 ACP vs cortisone subacromial injections for partial RTC tears
Early improvement in outcomes w/ACP but no difference at 6 months
50 6 No description of growth factor concentration
Hak 2015 Sports Health
2 PRP & Rotator cuff repair
No diff in outcomes 23 6 wks No description of growth factor concentration, short f/u
Wang 2015 AJSM 1 PRP & Rotator cuff repair
No improvement in outcomes/tendon healing
60 16 wks No exact determination of growth factor concentration, short f/u
Author Year Journal Level of evidence
Topic Effect N Avg f/u (Mos)
Limitations
Carr 2015 AJSM 1 Leukocyte rich PRP & acromioplasty
No diff in outcomes, reduced cellularity & vascularity
60 24 Leukocyte rich PRP, one injection, biopsy 12 weeks post injection
Malavolta 2014 AJSM 1 PRP liquid w/thrombin
No improvement in retear rates or clinical outcomes
54 24 Platelet poor plasma used, injected before portals were closed
Werthel 2014 Int J Shoulder Surg
2 Leukocyte poor ACP & cuff repair
No improvement in retear rates or outcomes
65 19 No description of growth factor concentration, differing amts of ACP injected
Charousset 2014 Arthroscopy 3 PRP & Rotator cuff repair
No diff in outcomes, recurrent tear rate or healing rate
61 28.6 No description of growth factor concentration, underpowered, single injection
Antuna 2013 Acta Orthop Belg
1 PRF and larg/massive cuff repairs
No diff in clinical outcomes/retear rates
28 >24 Small sample size
Weber 2013 AJSM 1 PRFM & cuff repair
No improvement in structural integrity, perioperative morbidity or outcomes
60 16 wks No description of growth factor concentration, short f/u
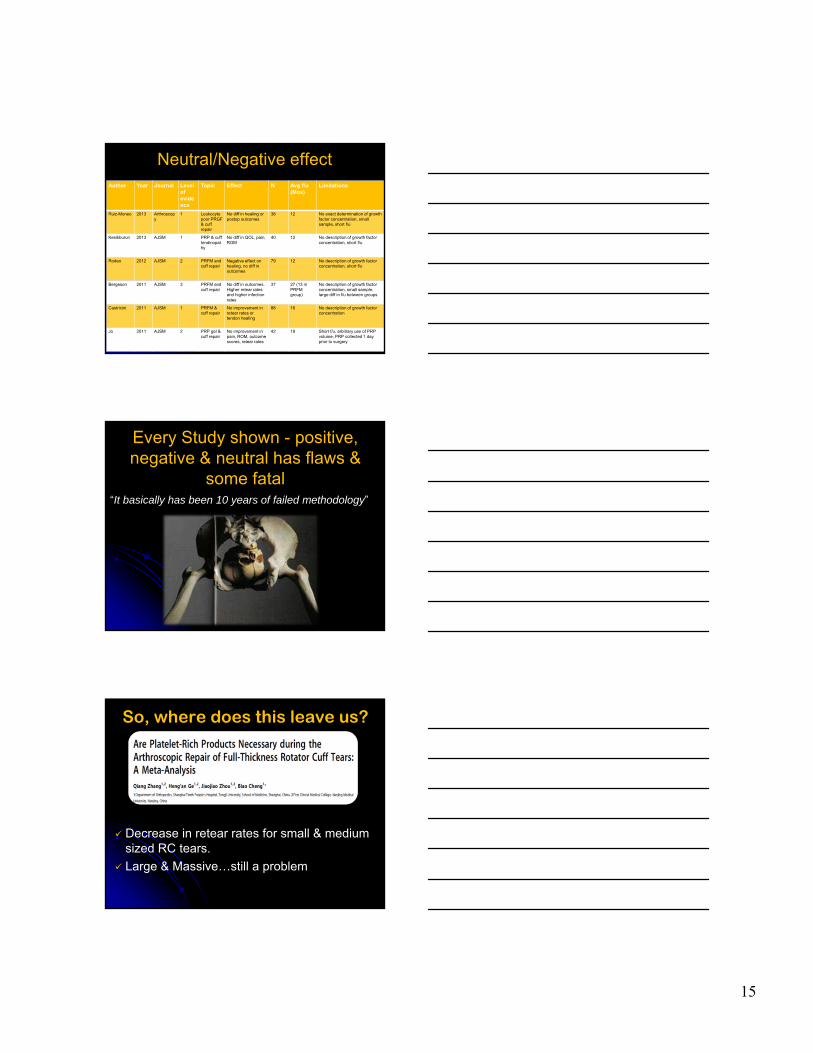
Neutral/Negative effect
15
Author Year Journal Level of evidence
Topic Effect N Avg f/u (Mos)
Limitations
Ruiz-Moneo 2013 Arthroscopy
1 Leukocyte poor PRGF & cuff repair
No diff in healing or postop outcomes
38 12 No exact determination of growth factor concentration, small sample, short f/u
Kesikburun 2013 AJSM 1 PRP & cuff tendinopathy
No diff in QOL, pain, ROM
40 12 No description of growth factor concentration, short f/u
Rodeo 2012 AJSM 2 PRFM and cuff repair
Negative effect on healing, no diff in outcomes
79 12 No description of growth factor concentration, short f/u
Bergeson 2011 AJSM 3 PRFM and cuff repair
No diff in outcomes. Higher retear rates and higher infection rates
37 27 (13 in PRFM group)
No description of growth factor concentration, small sample, large diff in f/u between groups
Castricini 2011 AJSM 1 PRFM & cuff repair
No improvement in retear rates or tendon healing
88 16 No description of growth factor concentration
Jo 2011 AJSM 2 PRP gel & cuff repair
No improvement in pain, ROM, outcome scores, retear rates
42 19 Short f/u, arbitrary use of PRP volume, PRP collected 1 day prior to surgery
Neutral/Negative effect
Every Study shown - positive, negative & neutral has flaws &
some fatal“It basically has been 10 years of failed methodology”
So, where does this leave us?
Decrease in retear rates for small & medium sized RC tears.
Large & Massive…still a problem

16
#8 Practical Basic Science studies over the last 6 years
Basic Science University of Connecticut Human Soft Tissue Research Lab
Mazzocca G, McCarthy B, Romeo A, Bradley J, Arciero R 2009 -17
PRP the basicsUse plasma based (low WBC’s)
Platelet # does not make a difference (3X)
GF’s vary everyday
Platelet to WBC ratio is key (2000:1)
Steroids deactivate AG
Caines kill everything
NSAIDs don’t make a difference Antibiotic & Anti-inflammatory
Modifies post op pain
Multiple injections better one /wk x 3
ACP HA Toradol work synergistically in OA

17
O.R. Experience
Have used all the major PRP systems in the OR
Top 3 UE ACP OR favorites
1. RCR
2. RC revision
3. Revision Labral repairs
Post-op Pain relief is the major indication
Significant reduction in narcotic use
#9 Stem Cells are here to stay!

18
My Clinical Protocol
BMAC - 1 injection with or without scope usually mild to mod OA knee2% Hct 7ccs + PRP 3cc
Adult
Hematopoietic
Peripheral blood
Mesenchymal
Mesoderm
SynoviumAdipose PeriosteumBone
marrow
Germ
Sperm/Egg
Embryonic
Fetus
Not approved for use in
orthopaedics
Classification of Stem Cells
Cell Source
Cell Type
Tissue Source
Tissue Type
MSC’s What the heck are they?
Unspecialized cells with a self renewal potential which can differentiate into different adult cell types (mesenchymal tissue)
Can exert regulatory effect on local & distant cells
Can be isolated from almost every tissue
Found as perivascular cells
Secrete massive levels of immunomodulatory & trophic substances
Modulate T-cell response

19
Improve healing by a synergistic Triple Action Mechanism
1. Direct participation in repair (diff into damaged or lost cells)
2. Stimulation of local cells via paracrine mechanism (indirectly promote vascularization, proliferation & differentiation via soluble factors)
3. Anti-inflammatory or immunomodulatory activity (modulate inflammatory cascade)
It May not be their ability to differentiate
• MSC’s are the body’s “Drug Store” Trophic properties
• Anti-inflammatory, Anti-apoptotic, Anti-microbial
• Induce cell proliferation & angiogenesis, reduce scar formation
• Locally derived SC maybe more effective than other sources
MSC’s most relevant contribution maybe is to provide a suitable microenvironment for tissue repair not direct repair
Recent In vivo MSC studiesStudy N F/U
Mean Age
Cells Result Conclusion
Koh et al.2014
37 26.5 months
57.4 Buttock Fat pad Mean 3.8x106
• IKDC & Tegner significantly improved (P < .001)
• 94% good to excellent results• 76% of repairs abnormal or severely
abnormal by ICRS
Despite lack of lesion healing, improvement in pain & function. Poorer outcomes with large lesions & high BMI
Koh et al.2013
18 24.3 months
54.6 Infrapatellarfat padMean 1.18x106 with PRP
• WOMAC improved from 50 to 30 (P < .001)
• Lysholm improved from 40 to 73 (P < .001)
• VAS improved from 4.8 to 2.0 (P < .005)
Intra-articular injection of AD MSC is effective inimproving pain & function
Jo et al.2014
18 6 months
18-75 Abdominal FatLow 1.0x107
Med 5.0x107
High 1.0x108
High dose group only• WOMAC improved @ 6 months• Size of cartilage defect decreased
(arthroscopy)• Volume of cartilage increased (histology)
Intra-articular injection of 1.0x108 AD MSC intoknee with OA improved function & pain
Xie et al.2014
42 12 weeks
Rabbit 1. BMSC + PRP
2. ADSC + PRP
BMSC + PRP showed:• Higher proliferation rate & higher
expression of cartilage-specific genes/proteins than ADSC
• Improved gross appearance, subchondralbone regeneration, and histological & immunohistochemical characteristics
PRP as a scaffold for stem cells is synergistic for chondrocyte proliferation & viability

20
Why Concentrate Bone Marrow?
Angel BMC at 96 hrs.BMA at 96 hrs.
Healing trinity: Cell, Signal, Scaffold
“Biologics are here to stay & will be a mainstay of many operative & non-operative
treatment protocols.”- JPB, 2011
#10
Thank youPittsburgh Pa























![[ITA]Buffy.8x01. .the.long.Way.home](https://img.pdfslide.us/doc/110x75/54e725824a7959397d8b478a/itabuffy8x01-thelongwayhome.jpg)