Embed Size (px)
Citation preview

ENTRAPMENT AND OTHER FOCAL NEUROPATHIES 0733-8619/99 $8.00 + .OO
PROXIMAL NEUROPATHIES OF THE UPPER EXTREMITY
Kimberly L. Goslin, MD, PhD, and Lisa S. Krivickas, MD
LONG THORACIC NERVE
Anatomy
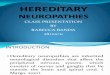
The long thoracic nerve is a pure motor nerve, providing innervation exclusively to the serratus anterior muscle (Fig. 1). It arises before for- mation of the brachial plexus from the ventral rami of the C5-C7 spinal nerves, with the largest component coming from C6. Immediately on ex- iting the intervertebral foramen, branches from the C5 and the C6 roots combine to form a common nerve trunk proximal to the middle scalene muscle and are usually joined by a branch from C7 after traversing this muscle. The nerve passes behind the clavicle and is angulated as it enters the axilla and runs posterior to the brachial plexus. It then passes over the first and the second ribs before descending superficially along the thoracic wall on the surface of the serratus anterior.
Clinical Presentation
The serratus anterior muscle primarily functions to anchor and sta- bilize the scapula and thus the shoulder girdle during movement. With assistance from the pectoralis major and minor muscles, it also protracts the scapula (pulls the scapula anteriorly). Injury to the long thoracic nerve
From the Department of Neurology, Oregon Health Sciences University, Portland, Oregon (KLG); and the Department of Physical Medicine and Rehabilitation, Harvard Medical School, and Electrodiagnostic Services, Spaulding Rehabilitation Hospital, Boston, Mas- sachussetts (LSK)
NEUROLOGIC CLINICS
VOLUME 17 - NUMBER 3 * AUGUST 1999 525

526 GOSLIN & KRIVICKAS
-acic n.
Figure 1. Long thoracic nerve originates from the C5-C7 nerve roots, proximal to the brachial plexus. It runs inferiorly behind the clavicle, and descends along the thoracic wall to innervate the serratus anterior muscle. (From Fisher M: Other rnononeuropathies of the upperextrernity. ln Brown WF, Bolton CF (eds): Clinical Electrornyography, 2nd ed. Boston, Butteworth, 1993, 271 ; with permission.)
produces scapular winging. Because of the central role played by the ser- ratus anterior in anchoring the scapula, active abduction of the affected arm is often limited to 90". With the arm at rest by the side of the body, the scapula as a whole translates medially with the inferior angle also rotating medially. The involved shoulder appears somewhat lower be- cause of the scapular rotation. These abnormalities are accentuated by having the patient flex the arm anteriorly (by pushing against a wall or performing push ups).
Long thoracic neuropathy is often painless, and patients may not be aware of its presence until they note scapular winging in a mirror or experience shoulder dysfunction. Because of muscle imbalance around the shoulder girdle, many patients develop a dull ache around the shoulder; they may even develop rotator cuff pathology because of altered bio-

PROXIMAL NEUROPATHIES OF THE UPPER EXTREMITY 527
mechanics. A more severe, burning pain occurs when serratus anterior weakness is caused by neuralgic amyotrophy. With injuries caused by excessive nerve stretching during physical activity, a sharp pain in the shoulder may radiate to the neck and the upper arm.52
Differential Diagnosis
With long thoracic mononeuropathy, shoulder muscles other than the serratus anterior may appear weak (deltoid, supraspinatus, infraspina- tus), suggesting the possibility of injury to the axillary or suprascapular nerves. However, if these muscles are tested with the examiner’s hand stabilizing the scapula, much of the apparent weakness disappears. Weak- ness of trapezius or rhomboid muscles also produces scapular winging. In contrast to serratus anterior weakness, which produces medial trans- lation of the scapula and medial rotation of the inferior angle, trapezius dysfunction produces lateral translation of the scapula accompanied by medial rotation of the inferior angle, producing a true shoulder droop. Damage to the dorsal scapular nerve with rhomboid weakness produces scapular winging with prominence of the inferior angle and lateral trans- lation of the scapula, accentuated by arm abduction. C6 or C7 radiculop- athies may also produce weakness of the serratus but involve- ment of other muscles is also expected. Several muscular dystrophies may be associated with scapular winging relatively early in their course. How- ever, bilateral involvement, slow progression and a specific pattern of in- volvement of other muscles distinguish these disorders from long thoracic neuropathy. Avulsion of the serratus anterior from the scapula also may produce winging and simulate a nerve injury.
Electrodiagnostic Evaluation
Electrodiagnosis of long thoracic nerve palsy relies primarily on the needle electrode examination (NEE) portion of the electrodiagnostic eval- uation (EDX). There is no reliable way to study this nerve with nerve- conduction (NCS), although several techniques have been de- ~ ~ r i b e d . ~ , ~ ~ , ~ ~ , ~ ~ Most of the techniques use a needle electrode to record the compound motor action potential (CMAP) from the serratus anterior, so no useful information is obtained from the amplitude of the response. When recording with needle electrodes, minimal movement of the needle drastically alters the amplitude. Latency information is of questionable significance because lesions of this nerve are unlikely to be demyelinating in pathophysiology. To exclude the possibility of a more widespread bra- chial plexus lesion, sensory nerve conductions should be performed, studying especially those nerve fibers that travel through the upper and the middle trunks of the brachial plexus (the lateral antebrachial cutane- ous, median, and radial sensory nerves) and thus have the same root innervation as the long thoracic nerve.

528 GOSLIN & KRIVICKAS
In long thoracic neuropathy, NEE abnormalities are restricted to the serratus anterior muscle. This is a difficult muscle to study. It can be ap- proached below the inferior angle of the scapula or along the midaxillary line. Caution must be taken to insert the needle directly over a rib. If the needle is inserted too deeply between ribs, a pneumothorax may result. Intercostal muscle activity may be mistaken for residual serratus anterior activity. This can be assessed by comparison of the level of electromyo- graphic activity when the patient takes a deep breath with that obtained during attempted contraction of the serratus muscle. Other C5-C6-C7- innervated muscles and cervical paraspinal muscles should be sampled to exclude a radiculopathy or brachial ple~opathy.~~
General Diagnostic Tests
Electrodiagnosis is the main tool for evaluating long thoracic neurop- athy. Cervical spine and brachial plexus MRI studies may be also indicated when a radiculopathy or plexopathy is being considered in the differential diagnosis.
Origin
The three major causes of isolated long thoracic nerve injuries are neuralgic amyotrophy, trauma, and repetitive activities producing exces- sive stretch or traction of the nerve.4l Neuralgic amyotrophy typically presents with the acute onset of severe, burning shoulder pain without a known history of trauma. Within a few days, the pain begins to dissipate, and weakness develops. Multiple portions of the brachial plexus may be involved in a patchy pattern. Parsonage and Turner73 found that 30 of 136 patients who have neuralgic amyotrophy had abnormalities limited to the long thoracic nerve. other^^^^^^^^^^^^,^^^ have also reported a high frequency of isolated long thoracic neuropathy with neuralgic amyotrophy. The su- praspinatus, infraspinatus, deltoid, serratus anterior, or muscles inner- vated by the anterior interosseous nerve are also commonly involved. There have been several reports of postoperative long thoracic neuropa- thy65 that may be a form of neuralgic amyotrophy or a stretch injury caused by positioning during surgery.
The long thoracic nerve lies superficially in the supraclavicular re- gion, where it is subject to trauma.50 Kauppila and K e ~ n a h a n ~ ~ reviewed 197 cases of long thoracic neuropathy and found that 32 were iatrogenic related to local invasive procedures along the course of the nerve: first rib resection^,^^ mastectomies with axillary node scalenectomies, chest tube insertion, and infraclavicular plexus anesthesia. The incidence of long thoracic nerve palsy after radical mastectomy is approximately 10% and is 1.1% after simple mastectomy.22,26 No cases have been reported after lumpectomy with axillary node dissection, but a long thoracic mono- neuropathy has been reported as a result of radiation therapy given in conjunction with l~rnpectomy.~~

PROXIMAL NEUROPATHIES OF THE UPPER EXTREMITY 529
It is thought that the straight course of the long thoracic nerve from origin to insertion, its fixation at the scalenus medius and serratus anterior muscles, as well as the angulation of the nerve as it enters the axilla make it vulnerable to stretch injuries. Such injuries may occur from trauma or repetitive stressful movement of the s h o ~ l d e r . ~ ~ , ~ ~ The stretch theory of long thoracic nerve injury is supported by a cadaver study in which a proximal segment of the long thoracic nerve was stretched to twice its normal resting length by raising the ipsilateral arm overhead and turning the head to the opposite side.41 Elongation of any nerve by greater than 10% of its resting length may result in neurapraxia.12 Sports- or work- related injuries of the long thoracic nerve occur when the ipsilateral arm is in an outstretched, overhead position7I as in weight training, ballet warm-up stretches,Io3 chopping wood, playing golf and tennis, gymnas- tics, wrestling, batting a baseball,4l operating industrial machinery, and using a Long thoracic nerve injury has also occurred from chi- ropractic manipulation of the cervical spine.72 Overhead arm positioning may be a factor in some of the isolated long thoracic neuropathies occur- ring during surgery with general a n e s t h e ~ i a . ~ ~ , ~ ~ Traction or compression of the neurovascular structures may occur during anesthesia when the upper arm is passively moved while the serratus anterior is paralyzed and thus not fixing the scapula to the chest wall.
In addition to the stretch theory of long thoracic neuropathy, Horo- witz and to cant in^^^ proposed several potential mechanisms of entrap- ment based on nerve dissections in 100 cadavers: (1) scalenus spasm or injury compressing intramuscular fibers of the nerve, (2) angulation of the nerve trunk as it crosses the second rib and its overlying heavy muscu- lature, (3) trapping of the nerve between the coracoid process and the second rib when the scapula is forced medially, and (4) inflammation of the bursae with which the nerve is associated, causing nerve compression. These mechanisms have not been ~onf i rmed.~~
If one receives a direct blow to the shoulder or the lateral thoracic wall while playing football or during a fall, the nerve may be compressed, producing injury.91 Another form of compressive neuropathy has been reported in soldiers and hikers who carry heavy backpacks and has been termed rucksack p a l ~ y . ~ ~ , ~ ~
Practical Management
Treatment depends on the mechanism of nerve injury. If caused by overuse, initial management consists of rest and avoidance of the offend- ing precipitating movement. Physical therapy is essential to maintain shoulder range of motion and to increase strength of the trapezius and rhomboids to maximize scapular stability. Active exercises should be per- formed in the supine position during the early phases of recovery, allow- ing the weight of the body to fix the scapula against the thorax, hereby preventing further winging and overstretching of the nerve. Special at- tention should also be given to stretching the latissimus dorsi, levator

530 GOSLIN & KRIVICKAS
scapulae, pectoralis minor, and rhomboid muscles, which have a tendency to become contracted and painful.
Numerous orthotic devices have been advocated for maintaining the scapula against the thorax9* and in an attempt to correct scapular dys- function, but most are ineffective86 or poorly tolerated. A variety of sur- gical procedures have been proposed to replace serratus anterior muscle function. Because of the long course of the nerve, these procedures should only be performed after 2 years have passed without apparent recov- e r ~ . ~ ~ , ~ ~ The most commonly performed procedures are transposition of the pectoralis major, pectoralis minor, rhomboids, or teres major mus- c l e ~ . ~ ~ ~ ~ ~ , ~ ~ ~ Another surgical approach is scapulothoracic fusion, which eliminates the scapular winging but at the expense of reduced scapulo- thoracic motion.
Prognosis
Most injuries caused by carrying, lifting, or stretch are incomplete, and good functional recovery occurs. Fardin30 studied electromyography (EMG) abnormalities in 10 patients up to 45 months after such injuries to the long thoracic nerve, with good functional outcome in 9 of the 10 pa- tients. Gregg et a14' described 10 cases of isolated complete paralysis of the serratus anterior muscle in young athletes. Full recovery occurred in an average of 9 months, with a maximum of 2 years. Recovery of long thoracic neuropathy from neuralgic amyotrophy has a similar prognosis and time c o ~ r s e . ~ ~ , ~ ~ Even in patients who regain full functional use of the arm, mild scapular winging may persist. Patients who have long thoracic nerve palsy caused by trauma have a poorer prognosis with only partial or no recovery because they usually have a more severe lesion.40 Needle EMG can be used to help evaluate recovery. Because the reinnervation distance is a long one, it may take as long as 6 months before nascent motor unit potentials appear after axonotmetisis of the long thoracic nerve. If there is no electromyographic evidence of nerve function at 2 years, the prognosis for spontaneous recovery is poor and consideration should be given to one of the surgical procedures described above.
SUPRASCAPULARNERVE
Anatomy
The suprascapular nerve is the only peripheral nerve originating from the upper trunk of the brachial plexus (Fig. 2). Fibers are primarily from C5 with some contributions from C6 and C4. The suprascapular nerve crosses the posterior cervical triangle and runs under the trapezius and the omohyoid muscles and then through the suprascapular notch to innervate the supraspinatus muscle. The suprascapular notch is a fibros- seous foramen bridged by the transverse scapular ligament. Within the

PROXIMAL NEUROPATHIES OF THE UPPER EXTREMITY 531
Figure 2. Suprascapular nerve originates directly from the upper trunk of the brachial plexus. It runs through the suprascapular notch (A) to innervate the supraspinatus muscle, then wraps around the spinoglenoid notch (B) to supply the infraspinatus muscle. (From Haymaker W, Woodhall B: Peripheral Nerve Injuries. Philadelphia, WB Saunders, 1953; with permission.)
supraspinatus fossa, the nerve provides sensory branches to the gleno- humeral and acromioclavicular joints. The nerve then traverses the spi- noglenoid notch at the lateral end of the scapular spine to innervate the infraspinatus muscle. The spinoglenoid notch is frequently covered by the spinoglenoid (or inferior transverse scapular) ligament. Although the su- prascapular nerve is generally considered a pure motor nerve, it also pro- vides joint sensation and occasionally a cutaneous sensory branch over- lapping in distribution with the axillary nerve.4a
Clinical Presentation
The suprascapular nerve can be entrapped at the level of the supra- scapular notch or spinoglenoid notch. With entrapment at the suprascap- ular notch, the primary symptoms are shoulder pain and weakness. The pain is deep and throbbing, located along the superior border of the scap-

532 GOSLIN & KRIVICKAS
ula with extension toward the shoulder joint, occasionally radiates down the arm.20,77 Maneuvers that adduct the scapula or rotate the head away from the involved shoulder, such as flexing the shoulder while reaching across the chest, exacerbate the pain. Tenderness over the scapular notch is sometimes present. Weakness of the supraspinatus, a shoulder abductor, and of the infraspinatus, a shoulder external rotator, can usually be dem- onstrated. Occasionally, deltoid muscle atrophy accompanies suprascap- ular nerve injury because of disuse. In contrast, isolated suprascapular nerve injury at the spinoglenoid notch most often presents with painless atrophy of the infraspinatus and weakness of shoulder external rotation.32
Differential Diagnosis
Because shoulder pain is one of the chief complaints of patients who have suprascapular neuropathy, various musculoskeletal conditions must be considered in the differential diagnosis. These include subacromial bursitis, bicipital tendonitis, rotator cuff tendonitis, rotator cuff tears, impingement syndrome, acromioclavicular joint arthritis, and adhesive capsulitis (frozen shoulder syndrome). Both rotator cuff tears and supra- scapular nerve lesions cause weakness of shoulder abduction despite a strong deltoid muscle. Mild atrophy of the supraspinatus or infraspinatus may occur with a rotator cuff tear as a result of disuse rather than nerve injury.
A second consideration in the differential diagnosis is a cervical ra- diculopathy affecting the C5 and the C6 roots in which there is pain felt along the medial border of the scapula, frequently radiating into the arm. Atrophy and weakness of the deltoid and biceps muscles may occur but are usually mild in radiculopathies produced by degenerative joint or disk disease of the cervical spine. Atrophy and weakness are much more pro- nounced in traumatic injuries to the nerve roots, such as in root avulsion.
Neuralgic amyotrophy must also be considered in the differential di- agnosis of a suprascapular neuropathy. The supraspinatus and infraspi- natus are two of the most commonly involved muscles, and occasionally are the only muscles affected.28,73,88,99,100 Some previously reported pa- t i e n t ~ ~ " , ~ ~ , ~ ~ , ~ ~ , ~ ~ who had spontaneous suprascapular entrapment neurop- athy may actually have had neuralgic amyotrophy.
Finally, an axillary neuropathy may present with weakness of arm abduction (deltoid) and lateral rotation (teres minor) similar to that seen with a suprascapular neuropathy. Atrophy of the deltoid muscle and sen- sory loss over the lateral aspect of the shoulder, however, typically accom- pany an axillary neuropathy.
Electrodiagnostic Evaluation
Demonstration of denervation, by needle EMG, confined to the su- praspinatus or i n f r a s p i n a t u ~ ~ ~ , ~ ~ , ~ ~ is the best objective evidence of supra-

PROXIMAL NEUROPATHIES OF THE UPPER EXTREMITY 533
scapular neuropathy." If either of these muscles is denervated, it is essen- tial to sample other C5- and C6-innervated muscles as well as the cervical paraspinal muscles, to exclude a cervical radiculopathy or more wide- spread brachial plexus lesion.78 A motor latency may be measured from Erb's point, recording from the supraspinatus or the infraspinatus muscle with a monopolar needle. For the supraspinatus muscle, the upper limit of normal is 3.7 ms for distances of 7 to 12 For the infraspinatus muscle, the upper limit of normal is 4.3 ms for distances of 10 to 15 Prolonged latencies to affected muscles have been reported in suprascap- ular n e ~ r o p a t h y . ' , ~ ~ , ~ ~ In one case' the significant prolongation of latency was confined to the infraspinatus muscle, pinpointing a distal entrapment site. On the other hand, a normal NCS does not rule out suprascapular nerve entrapment.82,83 Patients who have muscle atrophy because of ro- tator cuff injuries have normal EDXs.
General Diagnostic Tests
The suprascapular notch is seen on anterior-posterior radiographs if the radiograph beam is tilted caudally 15" to 30". Visualization of the notch allows one to look for osteophytes or other bony abnormalities that may entrap the suprascapular nerve. MRI of the shoulder is the imaging study of choice when looking for a ganglion cyst causing suprascapular nerve compression at the spinoglenoid notch. In addition, the MRI allows as- sessment of rotator cuff integrity and exclusion of a rotator cuff tear from the differential diagnosis. Ganglion cysts are often associated with tears of the superior glenoid labrum (the SLAP lesion), which are sometimes visualized on MRI but may also be associated with false-negative MRI studies. An uncommon diagnostic test is to inject a local anesthetic into the scapular notch, blocking the suprascapular nerve. Pain alleviation af- ter the injection suggests suprascapular nerve entrapment.I7 Since the dif- ferential diagnosis of suprascapular neuropathies also includes C5-C6 ra- diculopathies and brachial plexopathies, cervical or brachial plexus MRIs may also assist in making the correct diagnosis.
Origin
Of the two potential sites of suprascapular nerve entrapment, the suprascapular and the spinoglenoid notches, the most common is com- pression or stretching of the nerve in its passage through the suprascap- ular notch, where it is tethered by its branch to the supraspinatus. Trauma to the shoulder region is a common cause of suprascapular neuropa- thy.43,55,82,s3,104 Any acute forcible depression of the shoulder, such as that produced by a football tackle or that which occurs with a fall on the point of the shoulder, or repetitive minor depressions may injure the nerve. Fractures at the suprascapular notch, which are unc0mmon,2~ or excessive callus formation after a scapular fracture may also compress the

534 GOSLIN & KRIVICKAS
nerve. Various review^"^^^^^^^ report an incidence of 2% to 35% for supra- scapular nerve injury with acute dislocation of the shoulder. But with dislocations, almost all suprascapular neuropathies are associated with additional axillary, radial, or musculocutaneous neuropathies. A 10% in- cidence of suprascapular nerve injury has been reported after primary repair of massive rotator cuff tears.Io6
In patients who lack a history of direct trauma, the suprascapular nerve may be injured by repetitive motions involving the scapulothoracic and shoulder joints. Persistent or repetitive forced cross-body adduction of the arm may eventually produce suprascapular nerve injury.y2 Ana- tomic observations have confirmed this sling e f f e ~ t , s ~ , ~ ~ because move- ments of the shoulder joint apply traction to the nerve and cause com- pression against the rigid inferior border of the superior transverse ligament. This mechanism of injury has been reported in a woman vig- orously polishing her car for two hourss1 and in a postoperative patient reaching across his body to grab an overhead trapeze.y3 This mechanism may also be responsible for suprascapular neuropathies in gymnasts, foot- ball swimmers, weight lifters, pitchers, and tennis player^.^^,'^^
There have been at least 70 reports of suprascapular nerve entrap- ment at the spinoglenoid notch by ganglionic c ~ s ~ s . ~ ~ , ~ ~ , ~ ~ , ~ ~ Ganglion cysts typically form after tears of the glenoid labrum, much as Baker's cysts in the popliteal fossa form after meniscal tears. Injury at the spinoglenoid notch may also be caused by repetitive movements that stretch the nerve across the lateral edge of the spine of the scapula. An implicated position is maximum external rotation of the arm with approximately 90" of ab- duction and 20" of hyperextension. Activities requiring this arm position are the volleyball s e r ~ e ? ~ , ~ ~ weight lifting, and baseball pitchings4 Elite level volleyball players have developed asymptomatic atrophy of the in- fraspinatus, and it is believed that the eccentric contraction of the infras- pinatus during the volleyball serve contributes to compression of the nerve near the spinoglenoid
Practical Management
In the repetitive microtrauma often seen in athletes, avoiding the of- fending movement or altering technique generally corrects the problem. Nonoperative therapy consists of range-of-motion exercises for the shoul- der, strengthening of the muscles that stabilize the scapula (serratus an- terior, rhomboids, trapezius, and levator scapulae), and strengthening of the rotator cuff muscles themselves. Rehabilitation of virtually any shoul- der problem should begin with strengthening of the scapular stabilizers so that the rotator cuff muscles have a strong base of support against which they may function. In the setting of a severe suprascapular nerve injury, the shoulder may be unstable because of muscle paralysis; if this is the case, movements such as shoulder depression while lifting weight (as in carrying a heavy suitcase), throwing with the affected arm, and

PROXIMAL NEUROPATHIES OF THE UPPER EXTREMITY 535
reaching far across the body should be avoided as they place the shoulder at risk for subluxation or dislocation.
For persistent symptoms unresponsive to nonoperative treatment, surgical exploration may be indicated, with release of the transverse scap- ular ligament.17,83 In cases of blunt trauma with or without scapular frac- ture, a period of observation is recommended prior to any surgical inter- vention, generally 6 months; however, a severe comminuted fracture of the scapula with obvious involvement of the scapular notch may be an indication for earlier surgical exploration with resection of the transverse scapular ligament and neurolysis. When there is clear underlying pathol- ogy such as a tumor, early surgical management is important.
When a ganglion cyst is present at the spinoglenoid notch, surgical excision has produced excellent results in many cases.40,69,94,10' If rotator cuff pathology is also suspected and shoulder arthroscopy is performed, arthroscopic debridement of the cyst is p ~ s s i b l e . ~ ~ , ~ ~ A less invasive, yet successful, approach is CT-guided needle aspiration.'O
Prognosis
The prognosis for recovery of suprascapular neuropathies caused by blunt trauma, repetitive movements, and neuralgic amyotrophy is excel- lent with conservative treatment. Martin et aF6 reviewed the results of nonoperative management of 15 cases. Good outcome was observed in 12 of the 15, and the remaining three responded to surgery. This suggests that surgery should only be undertaken when there is a clear pathologic lesion or when conservative therapy fails. Antoniadis et a16 summarized long-term follow-up in 25 cases from various causes treated with surgery after failure of conservative methods: 84% of patients were pain free after surgery, and motor function improved significantly in 86.7% of patients. Similar results are cited by 0 t h e r ~ . ~ ~ , ~ ~ , ~ ~ , ~ 0 ~
AXILLARY NEUROPATHY
Anatomy
The axillary nerve is a mixed motor and sensory nerve providing innervation to the deltoid and teres minor muscles and cutaneous sensory fibers to a small area over the lateral aspect of the shoulder (Fig. 3). It is a terminal branch of the posterior cord of the brachial plexus formed from C5 and C6 fibers, running through the upper trunk and posterior cord. At its origin, the nerve travels along the anterior surface of the subsca- pularis muscle to its lower border where it joins the posterior circumflex humeral artery. Together the nerve and artery turn posteriorly to leave the axilla through the quadrilateral space, which is bounded superiorly by the inferior edge of the teres minor muscle, laterally by the surgical

536 GOSLIN & KRIVICKAS
Sensory branch'-'
Radial
I Figure 3. Axillary nerve originates from the posterior cord of the brachial plexus. The nerve innervates the teres minor and deltoid muscles and supplies sensation to the lateral shoulder. (From Haymaker W, Woodhall B: Peripheral Nerve Injuries. Philadelphia, WB Saunders, 1953; with permission.)
neck of the humerus, medially by the long head of the triceps, and infe- riorly by the teres major. Distal to the quadrilateral space, a branch is supplied to the teres minor. The axillary nerve then separates into three branches: an anterior branch to the middle and anterior aspects of the deltoid, a posterior branch to the posterior deltoid, and the upper lateral brachial cutaneous nerve, which supplies the skin over the deltoid.
Clinical Presentation
Axillary neuropathies result in a well-defined patch of sensory loss over the lateral shoulder. Weakness and atrophy of the deltoid limit shoul- der abduction. Involvement of the teres minor causes mild weakness of shoulder external rotation. The weakness is only partial, because the in- fraspinatus is a stronger external rotator.

PROXIMAL NEUROPATHIES OF THE UPPER EXTREMITY 537
Differential Diagnosis
The differential diagnosis of a suspected axillary neuropathy includes a lesion of the posterior cord of the brachial plexus, suprascapular neu- ropathy, a C5 or C6 radiculopathy, and neuralgic amyotrophy. Testing muscles innervated by other branches of the posterior cord, such as the radial nerve, allows a distinction to be made between a posterior cord lesion and an axillary neuropathy. A suprascapular neuropathy may pro- duce a similar pattern of weak arm abduction and external rotation but without any sensory loss. Deltoid weakness may be detected in a C5 or C6 radiculopathy, but involvement of other muscles, radicular pain, or sensory symptoms in the forearm or hand should also be present. Axillary neuralgic amyotrophy and musculoskeletal causes of shoulder pain, in- cluding rotator cuff tears, also should be considered in the differential diagnosis.
Electrodiagnostic Evaluation
Axillary motor NCSs can be performed by stimulating at Erb’s point and recording with a monopolar needle or surface electrode over the del- toid. For stimulation at Erbs point with a distance of 15 to 21 cm, the upper limit of normal for distal latency is 4.9 Since axillary neurop- athies are usually axon-loss lesions, motor conduction studies do not gen- erally provide more information than may be obtained from EMG. In the setting of an acute nerve injury, however, the amplitude of the CMAP recorded with a surface electrode may give an estimation of the degree of axon loss. Needle EMG is used to demonstrate denervation or reinner- vation in the deltoid and the teres minor muscles. If abnormalities are found in these muscles, the electromyographer should test other muscles innervated by the upper trunk and the posterior cord to ensure that the abnormalities found in the axillary-innervated muscles are not part of a more widespread brachial plexus lesion. C5 and C6 muscles not inner- vated by the axillary nerve and the cervical paraspinal muscles should also be tested to exclude the possibility of a cervical radiculopathy. The sensory branch of the axillary nerve is not routinely studied in the elec- trophysiology laboratory.
General Diagnostic Tests
When symptoms are caused by trauma, radiographs of the shoulder and humerus should be obtained to exclude the possibility of a fracture or shoulder dislocation. When a cervical radiculopathy is being consid- ered in the differential diagnosis, a cervical spine MRI may be indicated. Vascular quadrilateral space syndrome is diagnosed by arteriography re-

538 GOSLIN & KRIVICKAS
vealing occlusion of the posterior circumflex humeral artery when the arm is abducted and externally rotated.
Origin
The most common cause of axillary neuropathy is trauma, especially dislocation of the s h o ~ l d e r ~ ~ r ~ l , ~ ~ or humeral fracture. Axillary nerve injury is a well-known complication of anterior shoulder dislocation because the short course of the nerve around the humeral neck puts the nerve at risk for a traction injury with forward humeral displacement. Toolanen et a196 examined early complications after anterior dislocation of the shoulder and found 35 of the 55 patients had deltoid muscle denervation. The ax- illary nerve is thought to be the nerve most vulnerable to traction injury of the brachial plexus because it is closely tethered to the deltoid muscle.34 Other traumatic causes of axillary neuropathy include crutch palsy (which also often involves radial nerve injury), intramuscular injection in the pos- terior shoulder,S1 and direct blows to the shoulder girdle or quadrilateral space in athletes who wrestle or play football, rugby, and Axil- lary neuropathy occasionally follows general anesthesia or sleeping in a prone position with the arms raised above the head.2
Rare cases of entrapment in the quadrilateral space have been re- ported.'6,21 Quadrilateral space syndrome is caused by compression of the posterior humeral circumflex artery or the axillary nerve by associated vessels or hypertrophied muscles and is most common in young athletic individual^.^^ Symptoms develop gradually with intermittent paresthesias in the upper extremity during forward flexion, abduction, or both. Exter- nal rotation of the arm aggravates the symptoms. The pain is poorly local- ized to the anterior aspect of the shoulder, and usually there is no weakness.
Axillary nerve involvement is common in neuralgic amyotrophy. Del- toid weakness can be demonstrated in 50% of cases. Usually the supra- scapular nerve is also affected, but in approximately 10% of patients who have neuralgic amyotrophy, only the deltoid is involved.99
Practical Management
The importance of physical therapy in the management of patients who have nerve injury about the shoulder cannot be overemphasized. Range of motion must be maintained to avoid joint contractures. Conser- vative treatment is recommended when an incomplete nerve injury is present. If the lesion seems to be complete, the patient should be reex- amined with needle EMG in approximately 3 months. The distance from the site of injury to the deltoid muscle is relatively short, so some recovery should be expected within 3 to 4 months. Reinnervation usually occurs first in the posterior portion of the deltoid, so this area should always be

PROXIMAL NEUROPATHIES OF THE UPPER EXTREMITY 539
tested. If there is no evidence of reinnervation, surgical exploration and nerve grafting should be considered. As in other cases of peripheral nerve injury, it is preferable to perform nerve grafting less than 6 months after the onset of the
Prognosis
A partial nerve injury sustained in association with fracture or dis- location of the head of the humerus usually recovers f ~ l l y . " , ~ ~ , ~ ~ Axillary nerve injury associated with traction to the brachial plexus, has a less favorable p r o g n ~ s i s . ~ , ~ ~ Leffert and S e d d ~ n ~ ~ noted that six of the nine patients with isolated axillary nerve injury failed to regain full deltoid muscle strength. Berry and Bri19 reported that only two of their eight pa- tients who presented with complete deltoid paralysis regained useful del- toid muscle function. Injury to the nerve by blunt trauma to the shoulder has a variable prognosis. Perlmutter et a174 performed long-term follow- up in athletes who had isolated axillary nerve injury caused by a direct blow to the anterior lateral deltoid. Of seven athletes, three had significant recovery of function with conservative treatment, three had good recovery after surgery, and one had no recovery. Because the axillary nerve is com- posed primarily of motor fibers and travels only a short distance from its origin to its muscle insertion, it has a good prognosis for functional re- covery after surgical Petrucci et a176 reported that in 21 pa- tients who underwent nerve grafting, recovery of deltoid strength was extremely rapid and complete in all.
MUSCULOCUTANEOUS NERVE
Anatomy
The musculocutaneous nerve is a mixed motor and sensory nerve. It innervates three of the elbow flexor muscles (the biceps, brachialis, and coracobrachialis) and provides cutaneous sensory branches to the lateral forearm (Fig. 4). It arises directly from the lateral cord of the brachial plexus, in the upper arm near the inferior border of the pectoralis major muscle. It receives contributions from C5-C7 cervical roots via the upper and middle trunks of the brachial plexus. Contribution from C7 is mini- mal. The nerve innervates the coracobrachialis at the level of the axilla and pierces this muscle to run in the fascia1 plane between the biceps and brachialis muscles. In the region of the elbow, this nerve runs deep to the brachial fascia, over the brachialis muscle. Distal to the elbow, the terminal extension of the musculocutaneous nerve continues as the lateral antebra- chial cutaneous sensory nerve. In the forearm, this nerve becomes sub- cutaneous and separates into two terminal divisions, anterior and poste- rior, to supply sensation to the lateral half of the forearm to the level of

540 GOSLIN & KRIVICKAS
Musculocutaneous n.
Coracobrachialis
.::- Biceps brachii I M.
Figure 4. Musculocutaneous nerve originates from the lateral cord of the brachial plexus. The nerve innervates the biceps, brachialis, and coracobrachialis muscles. It continues distal to the elbow as a pure sensory nerve, providing sensation to the lateral forearm. (From Hay- maker W, Woodhall B: Peripheral Nerve Injuries. Philadelphia, WB Saunders, 1953; with permission.)
the wrist. The musculocutaneous nerve is relatively fixed where it pierces the coracobrachialis muscle and at the point where it exits through the deep fascia at the elbow. It is vulnerable to traction at these sites.
Clinical Presentation
The signs and symptoms of a musculocutaneous neuropathy depend on the location of the nerve injury. The coracobrachialis muscle flexes and adducts the shoulder and stabilizes the head of the humerus in the glenoid fossa. The brachialis and biceps are flexors of the elbow. The biceps brachii also supinates the forearm and flexes the arm at the shoulder. Proximal

PROXIMAL NEUROPATHIES OF THE UPPER EXTREMITY 541
involvement of the nerve causes weakness of elbow flexion, an absent biceps reflex, and sensory loss in the lateral forearm. But some supination and elbow flexion may still be possible because the supinator and bra- chioradialis muscles contribute to supination; the brachioradialis, exten- sor carpi radialis longus, and pronator teres muscles contribute to elbow flexion. Because of extensive overlap in cutaneous sensory nerve territo- ries, lesions of musculocutaneous nerve may only result in a narrow band of sensory loss along the lateral aspect of the volar forearm.
The lateral antebrachial cutaneous nerve may become entrapped at the elbow, between the biceps tendon or fascia and the brachialis muscle. Pain in the cubital fossa is the presenting complaint and is exacerbated by arm pronation and elbow extension. The nerve may be tender to pal- pation at the elbow. Acutely, the patient may note a burning dysesthesia along the radial aspect of the volar forearmx and mild limitation of elbow extension when the elbow is in complete pronation. The fully pronated position places maximal tension on the nerve, thus exacerbating pain.
Differential Diagnosis
A ruptured biceps tendonI3 presents with weakness of forearm flex- ion, but the biceps muscle can be seen contracted into a small hard ball. C5 or C6 radiculopathies may produce biceps weakness, but denervation or weakness of other muscles (infraspinatus, brachioradialis, deltoid, paraspinal muscles) should be present as well as radicular pain and sen- sory symptoms in the hand. With a musculocutaneous nerve injury, sen- sory deficits are not present distal to the wrist. Brachial plexus injuries involving the lateral cord have involvement of median sensory fibers in the hand in addition to a musculocutaneous neuropathy. Occasionally, patients who have compression of the lateral antebrachial cutaneous nerve are misdiagnosed as having refractory lateral epicondylitis (tennis elbow) or median-nerve compression.x Muscles innervated by the musculocuta- neous nerve are frequently involved in neuralgic amyotrophy, but weak- ness is rarely limited solely to the distribution of the musculocutaneous nerve.
Electrodiagnostic Evaluation
The goal of the EDX study is to demonstrate isolated involvement of the musculocutaneous nerve and to exclude a brachial plexopathy or cer- vical radiculopathy. The most important NCS is the lateral antebrachial cutaneous sensory study. This sensory potential can be elicited by stim- ulating just lateral to the biceps tendon at the elbow and recording over the nerve approximately 12 cm distally along a line connecting the stimu- lation point to the radial pulse.x9 With this technique, the onset latency was 1.8 ? 0.1 ms (range 1.6 to 2.1 ms) and the conduction velocity was 57 to 75 m/s. The mean amplitude was 24 +- 7.2 pV with a range of 12

542 GOSLIN & KRIVICKAS
to 50 pV. This sensory response may be technically difficult to obtain in older or obese individuals. Therefore, if the response is absent or has a low amplitude, it should be compared with that from the uninvolved arm. Both distal and proximal nerve involvement result in an abnormal lateral antebrachial cutaneous NCS. When abnormalities are present, it is im- portant to perform other sensory NCS, especially those in which fibers that pass through the lateral cord or upper trunk (median to the thumb, radial) are tested. Abnormalities in these sensory potentials suggest more widespread brachial plexus involvement or neuropathy.
Proximal motor NCSs can be performed by one's stimulating at the axilla and Erb's point and recording with either a monopolar needle or surface electrodes over the biceps m u s ~ l e . ~ ~ , ~ ~ When surface electrodes are used to record the CMAP, the amplitude may be compared side to side to assess the degree of axon loss, and between Erbs point and the axilla, to look for conduction block.
Needle EMG is normal in musculocutaneous neuropathies at the el- bow. In proximal lesions, there is denervation, reinnervation, or both in the biceps. The brachialis and coracobrachialis can also be examined but are more difficult to localize and offer little additional information, except in suspected entrapment of the nerve in the coracobrachialis muscle, in which case, denervation would be expected in the brachialis and biceps muscles but not in the coracobrachialis. If abnormalities are found in the biceps, other upper-trunk-innervated muscles should be examined to en- sure that the abnormalities are not part of a more widespread lesion. Ex- amination of the cervical paraspinal muscles helps exclude the possibility of a C5-C6 radiculopathy.
General Diagnostic Tests
Radiographs of the elbow may be indicated to look for other causes of antecubital fossa pain such as bone spurs or degenerative joint disease. MR imaging of the cervical spine may also occasionally be helpful.
Origin
Proximal isolated musculocutaneous neuropathies are r a ~ e . ' ~ , ~ ~ More commonly, they occur with widespread traumatic lesions of the shoulder or upper arm, especially fractures of the proximal humerus. Livesodl described five cases of isolated musculocutaneous nerve injury from shoulder dislocation. One case was reported after midclavicular f r ac t~ re .~ Postoperative musculocutaneous nerve injury was observed in 3 of 54 cases of fracture of the lateral clavicle that were treated by transposition of the coracoid process onto the cla~icle.'~ The transposition of the cora- coid process with its attached muscles probably caused a stretch injury of the musculocutaneous nerve at the site of its passage through the cora- cobrachialis muscle.

PROXIMAL NEUROPATHIES OF THE UPPER EXTREMITY 543
It has been suggested that musculocutaneous nerve injuries occur where the nerve pierces the coracobrachialis muscle. It is relatively fixedIo7 at this site and can be injured, either from nerve stretch distal to where it is tightly anchored or as a result of pressure produced by vigorous, inter- mittent coracobrachialis muscle contractions or chronic muscle hypertro- phy. This mechanism is suspected in musculocutaneous neuropathies oc- curring after heavy weight liftingI3 or after violent extension of the forearm such as occurs when falling on an outstretched hand with elbow h y p e r e ~ t e n d e d . ~ , ~ ~ , ~ ~ Entrapment of the nerve at the coracobrachialis mus- cle may also be the mechanism of musculocutaneous nerve injury after surgical procedures requiring abduction and external rotation of the arm.29 Alternatively, EwingZ9 proposed that, based on cadaver studies, the actual mechanism of injury during surgery was stretching of the brachial plexus, with the musculocutaneous nerve particularly susceptible to injury.
Injury to the musculocutaneous nerve more commonly occurs with entrapment of the distal sensory branch at the elbow between the biceps tendon or fascia and the brachialis muscle. The lateral free margin of the biceps aponeurosis compresses the musculocutaneous nerve. The com- pression force is accentuated when the forearm is fully pronated. Injury to the lateral antebrachial cutaneous nerve has been reported with a num- ber of repetitive activities, including inserting 3000 screws in a single weekends and playing tennis. Compression of the lateral antebrachial cu- taneous nerve may also occur where the nerve assumes its subcutaneous superficial position. Injury has been reported as being caused by the strap of a heavy a waitress's tray,Io5 and during v e n i p u n c t ~ r e . ~ ~ ~ ~ ~ ~
Practical Management
Initial conservative therapy includes restriction of precipitating activ- ities and oral anti-inflammatory agents. If conservative therapy fails, fur- ther treatment recommendations depend on the site of musculocutaneous nerve injury. If nonoperative therapy fails to alleviate symptoms of en- trapment at the elbow, surgical decompression is suggested with excision of a triangular wedge of biceps tendon directly over the nerve. This pro- cedure has produced excellent results.8
When there is a more proximal injury to the nerve with severe axon loss and failure of recovery within 6 months, surgery is recommended to reinnervate the paralyzed biceps muscle and provide some elbow flex- i ~ n . ~ ~ ~ ~ ~ A variety of nerves have been used as grafts for the musculocu- taneous nerve (pectoral, thoracodorsal, intercostal, spinal accessory, ul- nar). The outcome of nerve-grafting procedures becomes progressively worse when delayed more than 6 months pos t in j~ ry .~ , '~ ,~~ In cases for which surgery is delayed for more than 6 months, a free muscle transfer innervated by an intercostal nerve may be the best ~ p t i o n . ~ Surgical pro- cedures should only be performed after needle EMG demonstrates com- plete absence of axonal continuity to the biceps muscle, thereby excluding the possibility of spontaneous recovery.

544 GOSLIN & KRIVICKAS
Prognosis
Most isolated musculocutaneous neuropathies, particularly those caused by stretch injuries or neuralgic amyotrophy, are incomplete and respond to conservative therapy with good recovery. Severe proximal in- juries of the musculocutaneous nerve, treated with nerve-grafting or neu- rotization techniques, have a more variable outcome, with an estimated 64% of patients regaining functional elbow flexion 2 years after sur- gery.h4,ss Residual sensory loss in all types of musculocutaneous neurop- athies is common.
SUMMARY
Isolated lesions of the proximal nerves of the shoulder and arm, in- cluding the long thoracic, suprascapular, axillary, and musculocutaneous nerves, are uncommon. These nerves are more commonly injured in com- bination by trauma or in idiopathic brachial neuritis (neuralgic amyotro- phy). The evaluation of these mononeuropathies relies heavily on electro- diagnostic testing, particularly needle EMG, because most are axon-loss lesions. The differential diagnosis of each of these mononeuropathies in- cludes cervical radiculopathy, brachial neuritis, and soft-tissue injury to the shoulder girdle. As with all nerve injuries, prognosis for recovery of function depends on the extent of axon loss.
References
1. Aiello I, Serra G, Triana CC, et al: Entrapment of the suprascapular nerve at the spi-
2. Aita J F An unusual compressive neuropathy. Arch Neurol47:742-744,1984 3. Alasaka Y, Hara T, Takahashi M: Restoration of elbow flexion and wrist extension in
brachial plexus paralysis by means of free muscle transplantation by innervated nerve. Ann Hand Surg 9:341-350,1990
4. Alfonsi E, Moglia A, Sandrini G, et al: Electrophysiological study of long thoracic nerve conduction in normal subjects. EMG Clin Neurophysiol26:63-67, 1986
5. Alnot J Y Infraclavicular lesions. In Terzis JD (ed): Microreconstruction of Nerve Inju- ries. Philadelphia, WB Saunders, 1987, pp 393-402
6. Antoniadis G, Richter H, Rath S, et al: Suprascapular nerve entrapment: experience with 28 cases. J Neurosurg 85:1020-1025,1996
7. Bartosh RA, Dugdale TW, Nielson R Isolated musculocutaneous nerve injury compli- cating closed fracture of the clavicle: A case report. Am J Sports Med 20:356-359, 1992
8. Bassett FH, Nunley JA: Compression of the musculocutaneous nerve at the elbow. J Bone and Joint Surg 64A(7):1050-1052, 1982
9. Berry H, Bril V Axillary nerve palsy following blunt trauma to the shoulder region: A clinical and electrophysiological review. J Neurol Neurosurg Psychiatry 45:1027-1032, 1982
10. Biedert RM: Atrophy of the infraspinatus muscle caused by a suprascapular ganglion. Clin J Sports Med 6:262-264,1996
11. Blom S, Dahback LO: Nerve injuries in dislocations of shoulder joint and fracture of the neck of the humerus. Chir Scand. 136:461-466, 1970
noglenoid notch. Ann Neurol 12:314-316, 1982

PROXIMAL NEUROPATHIES OF THE UPPER EXTREMITY 545
12. Bora FW, Pleasure DE, Didizian NA: A study of nerve regeneration and neuroma for- mation after nerve suture by various techniques. Am J Hand Surg 1:138-143, 1976
13. Braddom RL, Wolfe C: Musculocutaneous nerve injury after heavy exercise. Arch Phys Med Rehabil59:290-293, 1978
14. Brown JT Nerve injuries complicating dislocation of the shoulder. J Bone Joint Surg 34B:526, 1972
15. Brown WF, Bolton C F Other mononeuropathies of the upper extremities. Irz Clinical Electromyography. Stoneham, MA, Butterworth, pp 271 -305
16. Cahill BR Quadrilateral space syndrome. In Omer GE, Spinner M (eds): Management of Peripheral Nerve Problems. Philadelphia, Saunders, 1980, pp 602-606
17. Callahan JD, Scully TB, Shapiro SA, et al: Suprascapular nerve entrapment. J Neuro- surgery 74:893-896,1991
18. Caspi I, Ezra E, Nerubay J, et al: Musculocutaneous nerve injury after coracoid process transfer for clavicle instability. Acta Orthop Scand 58:294-295, 1987
19. Chuang DCC, Yeh MC, Wei FC: Intercostal nerve transfer of the musculocutaneous nerve in avulsed brachial plexus injuries: Evaluation of 66 patients. J Hand Surg 17A: 822428,1992
20. Clein LJ: Suprascapular entrapment neuropathy. J Neurosurg 3:337-342,1975 21. Cormier PJ, Matalon TA, Preston MW: Quadrilateral space syndrome: A rare cause of
shoulder pain. Radiology 167797-798,1988 22. Delmar AR, Minton JP: Complications associated with mastectomy. Surg Clin North
Am 63:1331-1352, 1983 23. del Sasso L, Mondini A, Brambilla S: A case of isolated paralysis of serratus anterior.
Ital J Orthop Traumatol 14:533-537, 1988 24. Drez D: Suprascapular neuropathy in the differential diagnosis of rotator cuff injuries.
Am J Sports Med 4:43-45,1976 25. Dumitru D: Brachial plexopathies and mononeuropathies. In Electrodiagnostic Medi-
cine. Philadelphia, Hanley & Belfus, 1995, pp 585-642 26. Duncan M, Lotze M, Gerber L, et al: Incidence, recovery, and management of serratus
anterior muscle palsy after axillary node dissection. Surg Clin North Am 63:1243-1247, 1983
27. Edeland HG, Zachrissen BE: Fracture of the scapular notch associated with lesion of the suprascapular nerve. Acta Orthop Scand 46:758-763, 1975
28. England JD, Sumner AJ: Neuralgic amyotrophy: An increasingly diverse entity. Muscle Nerve 10:60-68,1987
29. Ewing MR Postoperative paralysis in the upper extremity: Report of five cases. Lancet 1:99-103,1950
30. Fardin P, Negrin P, Dainese R: The isolated paralysis of the serratus anterior muscle: Clinical and electromyographical follow-up of 10 cases. Electromyogr Clin Neurophy- siol 18:379-386, 1978
31. Fehrman DA, Orwin JF, Jennings RM: Suprascapular nerve entrapment by ganglion cysts: A report of six cases with arthroscopic findings and review of the literature. Arthroscopy 11:727-734, 1995
32. Ferreti A, Cerullo G, Russo G: Suprascapular neuropathy in volleyball players. J Bone Joint Surg 69A:260-263, 1987
33. Foo CL, Swann M: Isolated paralysis of the serratus anterior: A report of 20 cases. J Bone Joint Surg 65B:552-556, 1983
34. Friedman AH, Nunley JA, Urbaniak JR, et al: Repair of isolated axillary nerve lesions after infraclavicular brachial plexus injuries: Case reports. Neurosurgery 27403-407, 1990
35. Fritz RC, Helms CA, Steinbach LS, et al: Suprascapular nerve entrapment: Evaluation with MRI imaging. Radiology 182:437-444,1992
36. Ganzhorn RW, Hocker JT, Horowitz M, et al: Suprascapular nerve entrapment. A case report. J Bone Joint Surg 63A:492-498,1981
37. Gariepy R, Derome A, Laurin CA: Brachial plexus paralysis following shoulder dislo- cation. Can J Surg 5:418-421, 1962
38. Gelmers H, Buys D: Suprascapular entrapment neuropathy. Acta Neurochir 38:121- 127,1977

546 GOSLIN & KRIVICKAS
39. Goodman CE, Kenrick MM, Blum MV Long thoracic nerve palsy: A follow-up study.
40. Goss TP, Aronow MS, Coumas JM: The use of MRI to diagnose suprascapular nerve
41. Gregg JR, Labosky D, Harty M: Serratus anterior paralysis in the young athlete. J Bone
42. Hale B R Handbag paresthesia [letter]. Lancet 2:470, 1976 43. Hadley MN, Sonntag VKH, Pittman HW: Suprascapular nerve entrapment. A summary
of seven cases. J Neurosurg 64:843-848,1986 44. Hayes JM, Zehr DJ. Traumatic muscle avulsion causing winging of the scapula. J Bone
Joint Surg 63A:495-497,1981 45. Herzmark MH: Traumatic paralysis of the serratus anterior relieved by transplantation
of the rhomboidei. J Bone Joint Surg. 33A:235-238, 1951 46. Hirasawa Y, Sakakida K Sports and peripheral nerve injury. Am J Sports Med 11:420-
426, 1983 47. Holzgraefe M, Kuwowski B, Eggert S: Prevalence of latent and manifest suprascapular
neuropathy in high-performance volleyball players. Br J Sports Med 28:177-179,1994 48. Horiguchi M: The cutaneous branch of some human suprascapular nervs. J Anat
49. Horwitz MT, Tocantins LJ: Isolated paralysis of the serratus anterior muscle. J Bone
50. Ilfeld FW, Holder HG: Winged scapula: Case occurring in soldier from knapsack. JAMA
51. Johnson EW: Axillary nerve injury. Arch Neurol41:1022-1028, 1984 52. Johnson JTH, Kendall MO: Isolated paralysis of the serratus anterior muscle. J Bone
53. Kaplan PE: Electrodiagnostic confirmation of long thoracic nerve palsy. J Neurol Neu-
54. Kauppila LI, Vastamaki M: Iatrogenic serratus anterior palsy: long-term outcome in 26
55. Kaplan PE, Kernahan WT Rotator cuff rupture: Management with suprascapular neu-
56. Khalili AA: Neuromuscular electrodiagnostic studies in entrapment neuropathy of the
57. Kim SM, Goodrich A: Isolated proximal musculocutaneous nerve palsy: Case report.
58. Kraft GH: Axillary, musculocutaneous, and suprascapular nerve latency studies. Arch
59. Leffert RD, Seddon HJ: Infraclavicular brachial plexus injuries. J Bone Joint Surg 47B:9-
60. Leffert RD: Brachial plexus injuries. N Engl J Med 291:1059-1067, 1974 61. Liveson JA: Nerve lesions associated with shoulder dislocation: An electrodiagnostic
study of 11 cases. J Neurol Neurosurg Psychiatry 47742-744,1984 62. Lorhan PH: Isolated paralysis of the serratus magnus following surgical procedures.
Arch Surg 54:656-659, 1954 63. Makin G, Brown WF, Ebers GC: C7 radiculopathy: Importance of scapular winging in
clinical diagnosis. J Neurol Neurosurg Psychiatry 49:640-644, 1986 64. Malessy MJA, Thomeer RTWM: Evaluation of intercostal to musculocutaneous nerve
transfer in reconstructive brachial plexus surgery. J Neurosurg 88:266-271, 1998 65. Martin JT Postoperative isolated dysfunction of the long thoracic nerve: A rare entity
of uncertain etiology. Anesth Analg 69:614-619, 1989 66. Martin SD, Warren RF, Martin T, et al: Suprascapular neuropathy: Results of non-
operative therapy. J Bone Joint Surg 79A:1159-1165,1997 67. Moore TI', Fritts HM, Quick DC, et al: Suprascapular nerve entrapment caused by
supraglenoid cyst compression. J Shoulder Elbow Surg 6:455-462, 1997 68. Nagano A, Ochiai N, Okinaga S: Restoration of elbow flexion in root lesions of brachial
plexus injuries. J Hand Surg 17A:815-821, 1992
Arch Phys Med Rehabil. 56:352-355,1976
entrapment caused by a ganglion. Orthopedics 17359-362, 1994
Joint Surg 61A:825-832,1979
130:191-195,1980
Joint Surg 37A:567-574, 1955
120:448-449,1942
Joint Surg 37A:567-574,1955
rosurg Psychiatry 43:50-52, 1980
patients. Chest 109:31-34, 1996
ropathy. Arch Phys Med Rehabil65:273-275,1984
suprascapular nerve. Orthop Rev 13:27-28,1974
Arch Phys Med Rehabil65:735-736,1984
Phys Med Rehabil53:383-387,1972
23, 1965

PROXIMAL NEUROPATHIES OF THE UPPER EXTREMITY 547
69. Ogino T, Minami A, Kato H, et al: Entrapment neuropathy of the suprascapular nerve
70. Oh SJ: Nerve conduction in focal neuropathies. In Clinical Electromyography: Nerve
71. Overpeck DO, Ghormley RK: Paralysis of the serratus magnus muscle. JAMA 114:1194-
72. Oware A, Herskovitz S, Berger AR: Long thoracic nerve palsy following cervical chi-
73. Parsonage MJ, Turner JWA: The shoulder girdle syndrome. Lancet I:973-978,1948 74. Perlmutter GS, Leffert RD, Zarins B: Direct injury to the axillary nerve in athlete playing
75. Petrera JE, Trojaborg W Conduction studies of the long thoracic nerve in serratus an-
76. Petrucci FS, Morelli A, Raimondi PL: Axillary nerve injuries-21 cases treated by nerve
77. Post M, Mayer J: Suprascapular nerve entrapment. Clin Orthop 223:126-136,1987 78. Preston DC, Shapiro BE: Proximal neuropathies of the shoulder and arm. In Electro-
myography and Neuromuscular Disorders: Clinical-Electrophysiologic Correlations. Wouburn, MA, Butterworth-Heinemann, 1998, pp 455-469
79. Pugliese GN, Green RF, Antonacci A: Radiation induced long thoracic nerve palsy. Cancer 60:1247-1248,1987
80. Rapp IH: Serratus anterior paralysis treated by transplantation of the pectoralis minor. J Bone Joint Surg 36A:852-854,1954
81. Reid AC, Hazelton RA: Suprascapular nerve entrapment in the differential diagnosis of shoulder pain. Lancet 2:477,1979
82. Rengachary SS, Neff JP, Singer PA, et al: Suprascapular entrapment neuropathy: A clinical, anatomical, and comparative study. Part 1: Clinical study. Neurosurgery 5:441- 446,1979
83. Rengachary SS, Burr D, Lucas S, et al: Suprascapular entrapment neuropathy: A clinical, anatomical, and comparative study. Part 2: anatomical study. Neurosurgery 5:447-451, 1979
84. Ringel SP, Treihaft M, Carry M, et al: Suprascapular neuropathy in pitchers. Am J Sports Med 18:80-86,1990
85. Samil M, Carvalho GA, Nikkhah G, et al: Surgical reconstruction of the musculocuta- neous nerve in traumatic brachial plexus injuries. J Neurosurg 87881-886, 1997
86. Schultz JS, Leonard JA: Long thoracic neuropathy from athletic activity. Arch Phys Med Rehabil73:87-90,1992.
87. Shah K, Stefaniwsky L: Long thoracic nerve palsy: Case report. Arch Phys Med Rehabil
88. Spillane JD: Localized neuritis of the shoulder girdle. Lancet II:532-535, 1943 89. Spindler HA, Felsenthal G: Sensory conduction in musculocutaneous nerve. Arch Phys
90. Steiman I: Painless infraspinatus atrophy due to suprascapular nerve entrapment. Arch
91. Stewart JD: The nerves arising from the brachial plexus. In Focal Peripheral Neuropa-
92. Sunderland S: Nerves and Nerve Injuries ed 2. Edinburgh, Churchill Livingstone, 1978,
93. Swafford, AR, Lichtman DH: Suprascapular nerve entrapment-Case report. J Hand Surg 757-60,1982
94. Takagishi K, Maeda K, Ikeda T, et a1 Ganglion causing paralysis of the suprascapular nerve. Acta Orthop Scand 62:391-393,1991
95. Tirman PFJ, Feller JF, Janzen DL, et al: Association of glenoid labral cysts with labral tears and glenohumeral instability: Radiologic findings and clinical significance. Ra- diology 190:653-658, 1994
96. Toolanen G, Hildingsson C, Hedlund T, et al: Early complications after anterior dislo- cation of the shoulder in patients over 40 years. Acta Orthop Scand 64:549-555 1993
by a ganglion. J Bone Joint Surg 73A:141-147,1991
Conduction Studies ed 2. Baltimore, Williams and Wilkins, 1993, pp 496-574
1196,1940
ropractic manipulation. Muscle Nerve 18:1351, 1995
contact sports. Am J Sports Med 25:65-68, 1997
terior palsy of different etiology. Neurology 34:1033-1037,1984
graft and neurolysis. J Hand Surg 7A:271-278,1982
63~585-586,1982
Med Rehabil59:20-22 1978
Phys Med Rehabil69:641-643,1988
thies ed 2. New York, Raven Press Ltd, 1993, pp 141-156
pp 796-801,843-848

548 COSLIN & KRIVICKAS
97. Trojaborg W: Motor and sensory conduction in the musculocutaneous nerve. J Neurol
98. Truong XT, Rippel DV Orthotic devices for serratus anterior palsy: Some biomechanical
99. Tsairis P, Dyck PJ, Multder DW: Natural history of brachial plexus neuropathy: Report
100. Turner JWA, Parsonage MJ: Neuralgic amyotrophy (paralytic brachial neuritis). Lancet
101. Uppal GS, Uppal JA, Dwyer AP: Glenoid cysts mimicking cervical radiculopathy. Spine
102. Vastamaki M, Kauppila LI: Etiologic factors in isolated paralysis of the serratus anterior muscle: A report of 197 cases. J Shoulder Elbow Surg 2:240-243,1993
103. White SM, Witten CM: Long thoracic nerve palsy in a professional ballet dancer. Am J Sports Med 21:626-627, 1993
104. Yoon TN, Grabois M, Guillen M: Suprascapular nerve injury following trauma to the shoulder. J Trauma 21:652-655, 1981
105. Young AW, Redmond D, Belandres P: Isolated lesion of the lateral cutaneous nerve of the forearm. Arch Phys Med Rehabil71251-252, 1990
106. Zanotti RM, Carpenter JE, Blasier RB, et al: The low incidence of suprascapular nerve injury after primary repair of massive rotator cuff tears. J Shoulder Elbow Surg. 6258- 264,1997
107. Zeuke VW, Heidrich R: Pathogenese der isolierten, postoperative Lahmung des Nerves musculocutaneous. Schweitz Arch Neurol Psychiatr 114289-294, 1974
108. Zoltan JD: Injury to the suprascapular nerve associated with anterior dislocation of the shoulder: Case report and review of the literature. J Trauma 19203-206, 1979
Neurosurg Psychiatry 39:890-899,1976
considerations. Arch Phys Med Rehabil60:66-69, 1979
on 99 patients. Arch Neurol27109-117,1972
11209-212, 1957
20:2257-2260,1995
Address reprint requests to Kimberly L. Goslin, MD, PhD
Department of Neurology L226 Oregon Health Sciences University
3181 SW Sam Jackson Park Road Portland, OR 97201
e-mail: [email protected]