Embed Size (px)
Citation preview
Providing palliative care to patients with advanced COPD:current challenges and strategies
Tara Lohmann MD FRCPC
Internal Medicine, Respirology
University of Calgary
Faculty/Presenter Disclosure
• Faculty: Tara Lohmann
• Relationships with financial sponsors:–None
Disclosure of Financial Support
• This program has NOT received financial support
• This program has NOT received in-kind support
• Potential for conflict(s) of interest:– N/A
Mitigating Potential Bias
• N/A
Objectives
• Appreciate the unique aspects of COPD
• Identify challenges in the palliative management of patients with advanced COPD
• Be aware of some recent interventions and models of care for palliative care in advanced COPD
Palliative care consult
• 69 M, severe COPD (FEV1 = 38% predicted) on home O2
• Baseline MMRC dyspnea score 3/4
• Admitted to hospital 2 days ago with AECOPD causing acute hypercapnic respiratory failure requiring BPAP
• You are consulted to help manage his symptoms (dyspnea, cough/sputum, anxiety) and help with decision-making

What are the challenges you face in managing patients with advanced COPD in your practice?
PC in COPD: Challenges
• Timing of palliative interventions
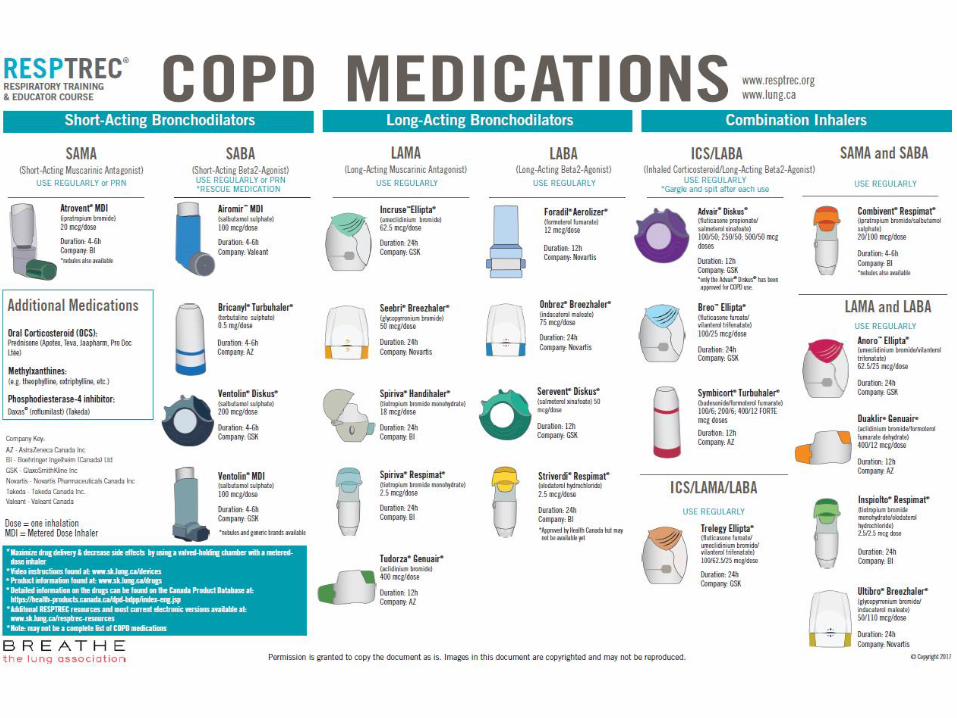
• Inhaler devices
• Opioids –dosing and safety
• Non-invasive ventilation (NIV)
• Oxygen
• Dyspnea crises
• Rx of Cough and Sputum
• Management of anxiety
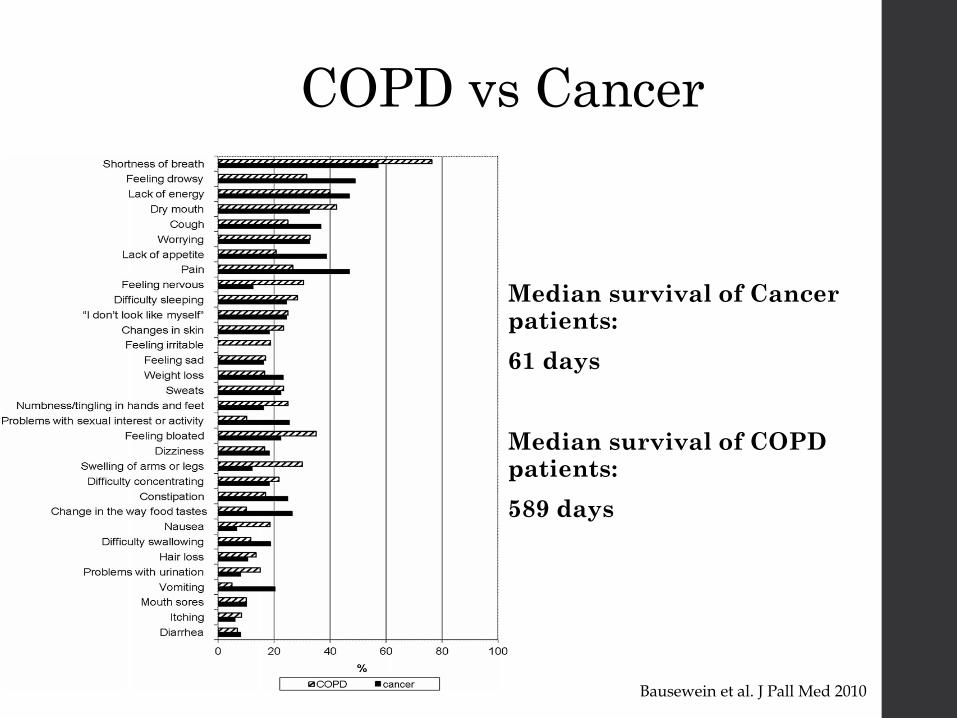
COPD vs Cancer
Median survival of Cancer patients:
61 days
Median survival of COPD patients:
589 days
Bausewein et al. J Pall Med 2010
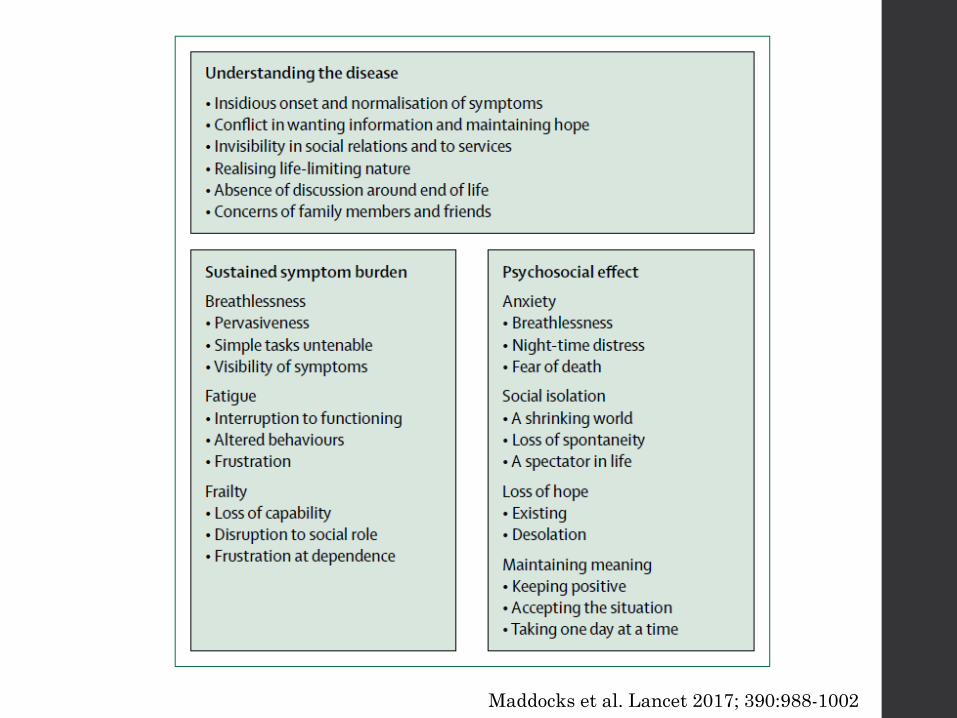
Maddocks et al. Lancet 2017; 390:988-1002
Palliative Care in COPD: Too little, too late?
• 16% of deceased patients with COPD had PC service before their death (vs. 56% with COPD and cancer)
- 1/3 received PC within 1 month before death
• Patients with COPD more likely to die in hospital
Bloom et al. ERJ 2018; 51
Dyspnea in COPD
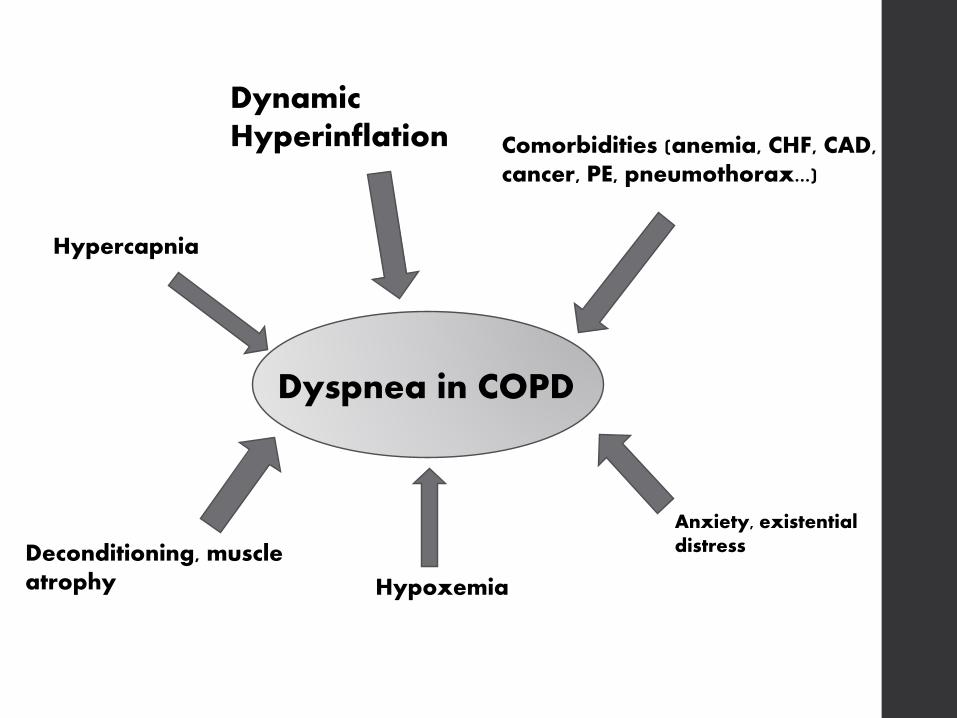
Dyspnea in COPD
Dynamic Hyperinflation
Deconditioning, muscle atrophy Hypoxemia
Anxiety, existential distress
Hypercapnia
Comorbidities (anemia, CHF, CAD, cancer, PE, pneumothorax...)
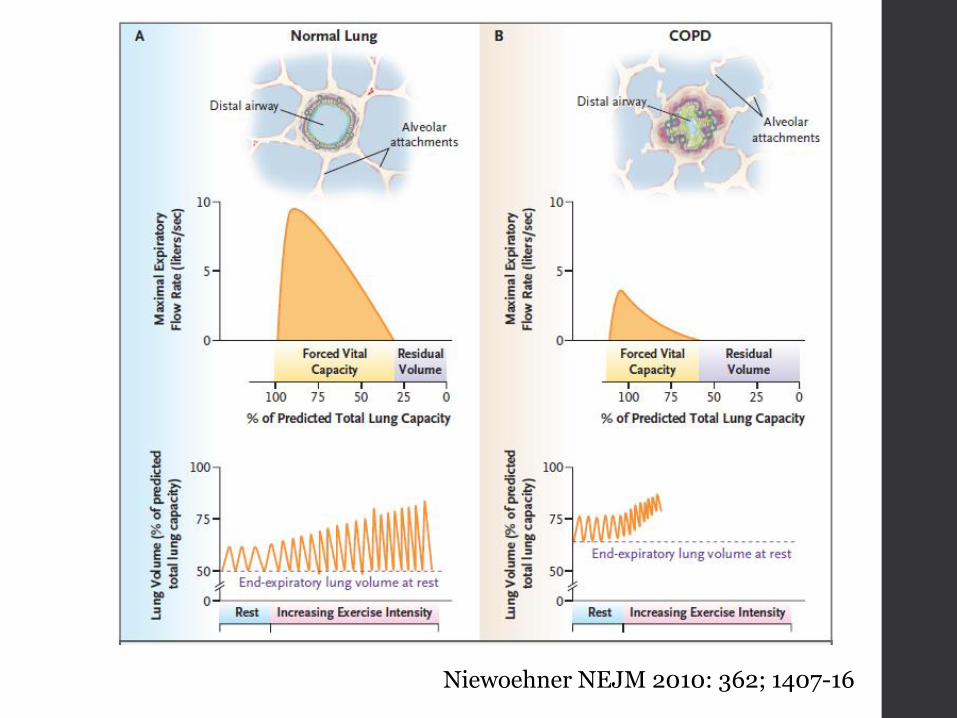
Niewoehner NEJM 2010: 362; 1407-16
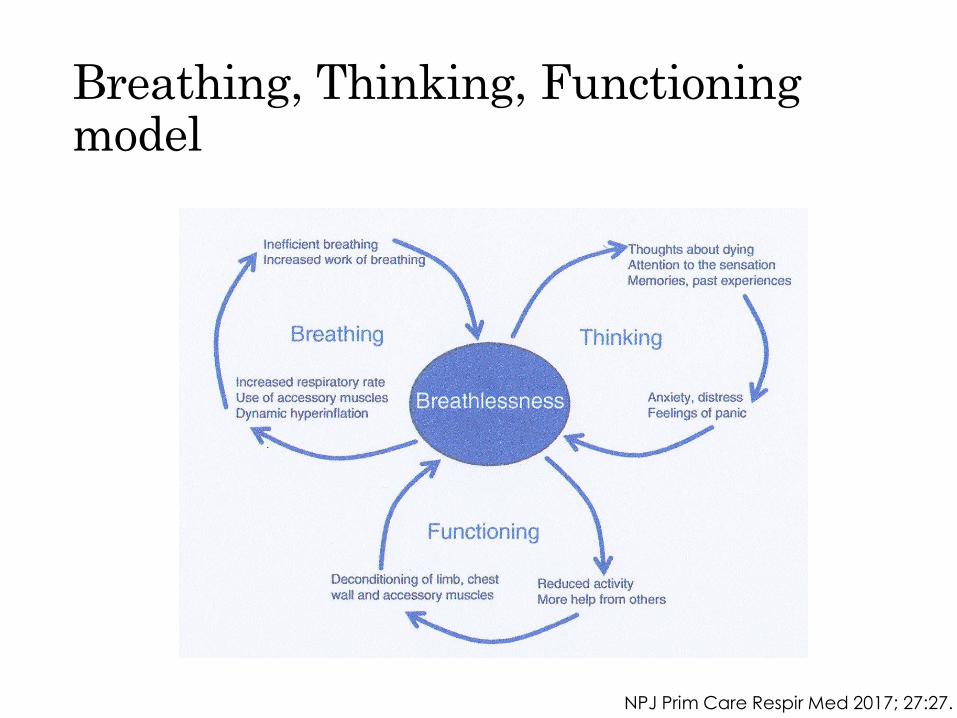
Breathing, Thinking, Functioning model
NPJ Prim Care Respir Med 2017; 27:27.
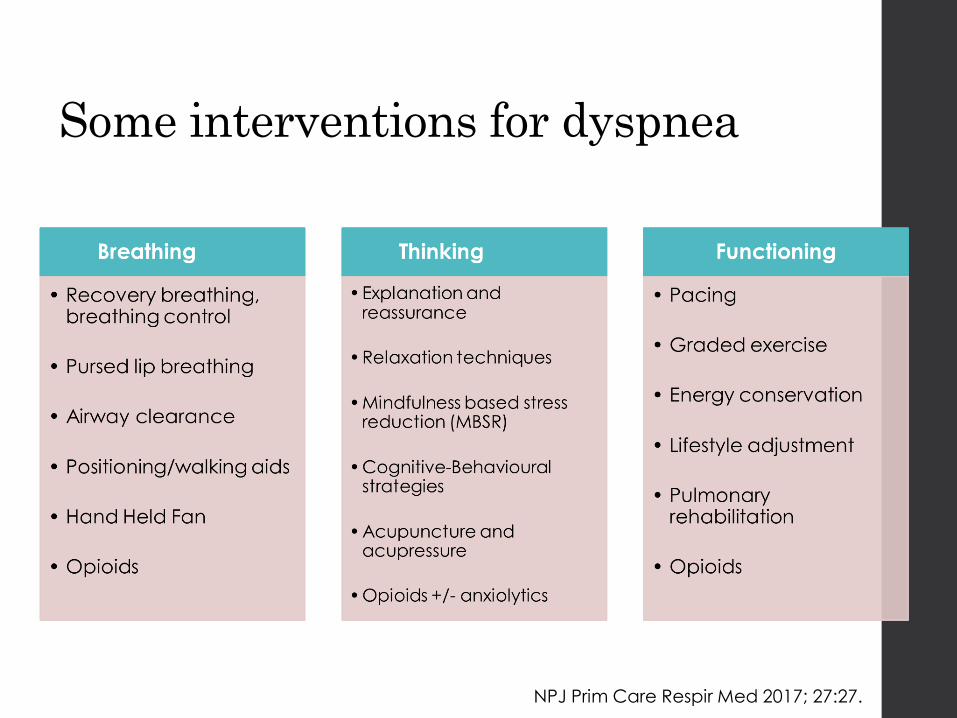
Some interventions for dyspnea
NPJ Prim Care Respir Med 2017; 27:27.
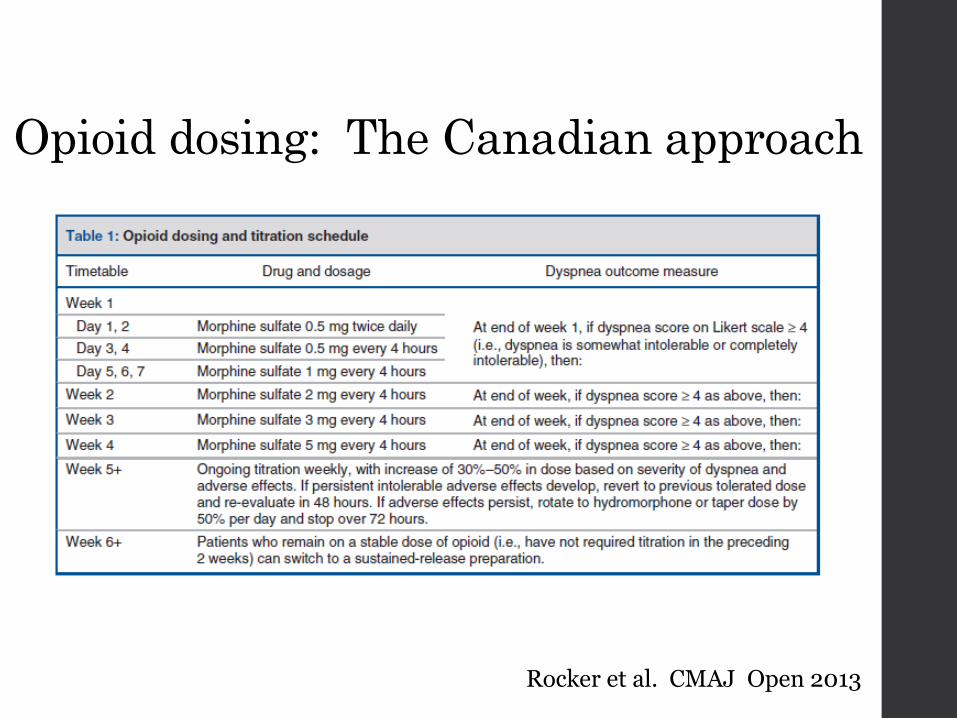
Rocker et al. CMAJ Open 2013
Opioid dosing: The Canadian approach
Opioid dosing: The Australian Approach
• Morphine SR 20 mg po daily (Abernethy A et. al BMJ 2003)
• Morphine SR 10 mg daily, increasing by 10 mg each week to a max of 30 mg daily (Currow DC et al. J Pain Symptom Manage 2011)

Opioids - Safety
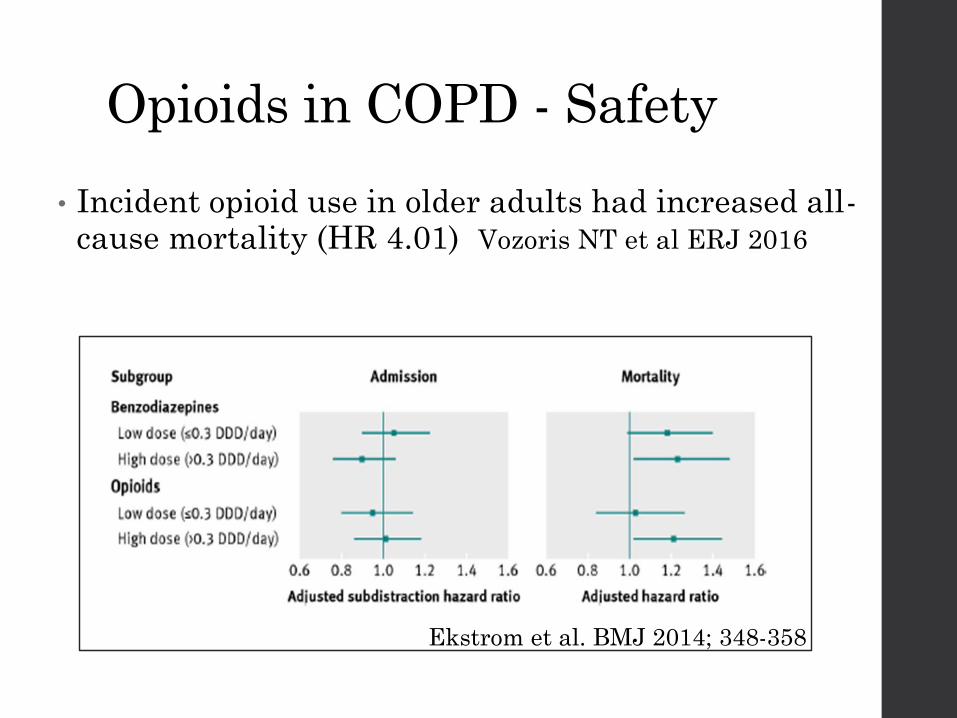
Opioids in COPD - Safety
• Incident opioid use in older adults had increased all-cause mortality (HR 4.01) Vozoris NT et al ERJ 2016
Ekstrom et al. BMJ 2014; 348-358
How do you manage this patient’s distressing mucous hypersecretion?
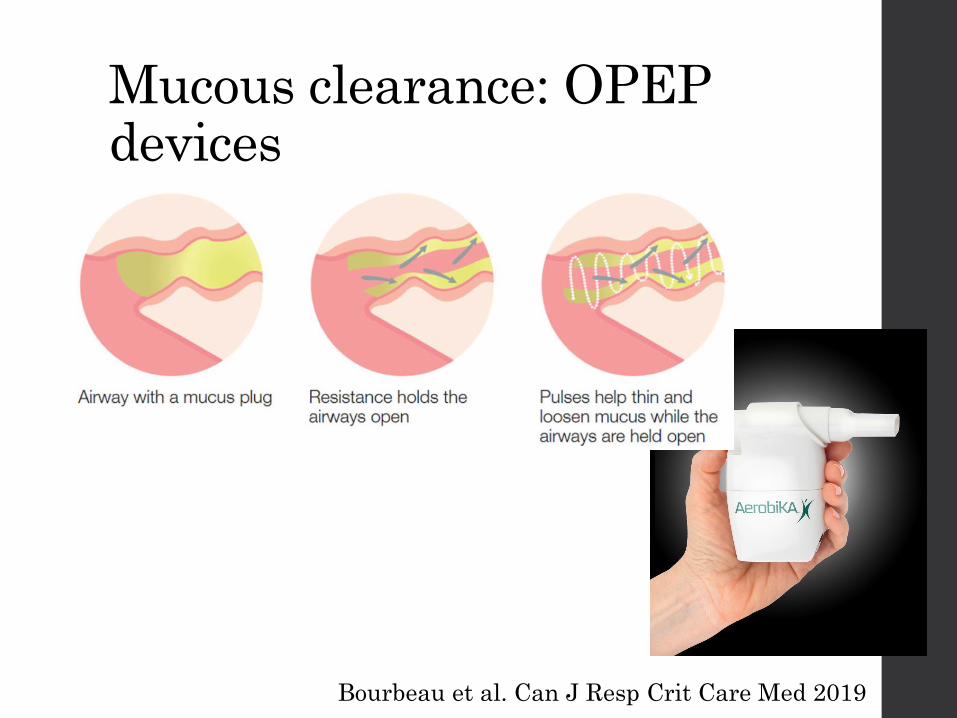
Mucous clearance: OPEP devices
Bourbeau et al. Can J Resp Crit Care Med 2019
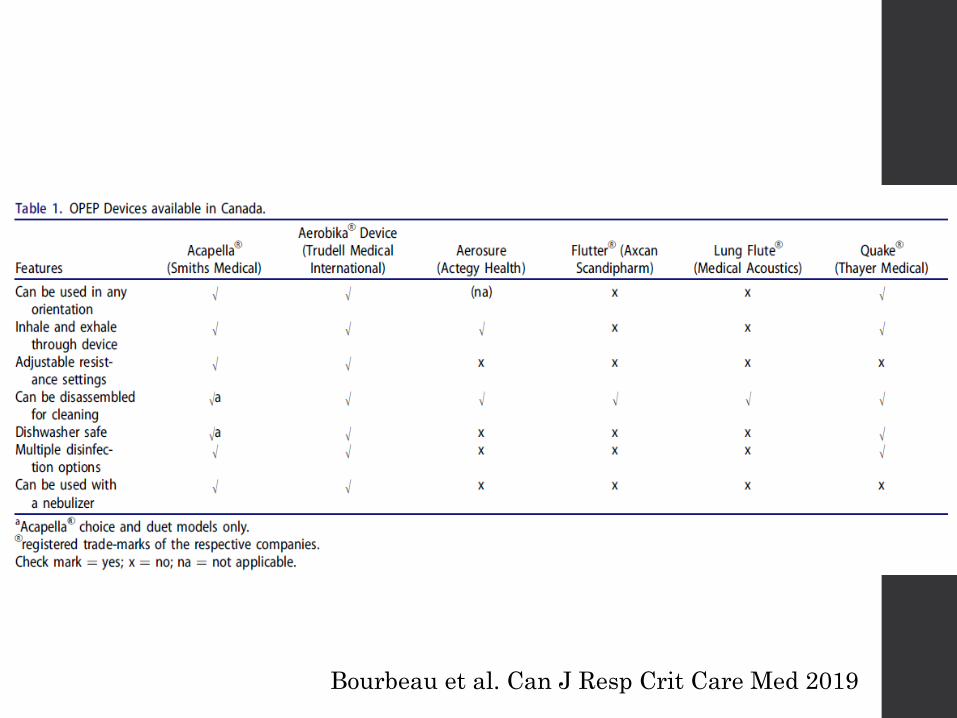
Bourbeau et al. Can J Resp Crit Care Med 2019

Pearls (What’s new?)
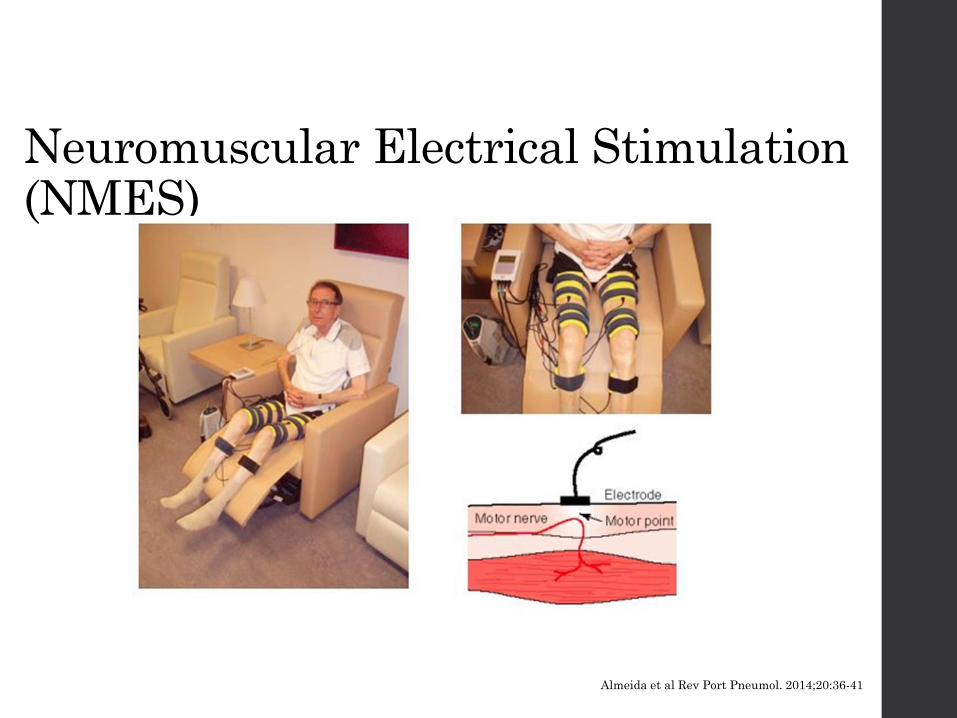
Almeida et al Rev Port Pneumol. 2014;20:36-41
Neuromuscular Electrical Stimulation (NMES)
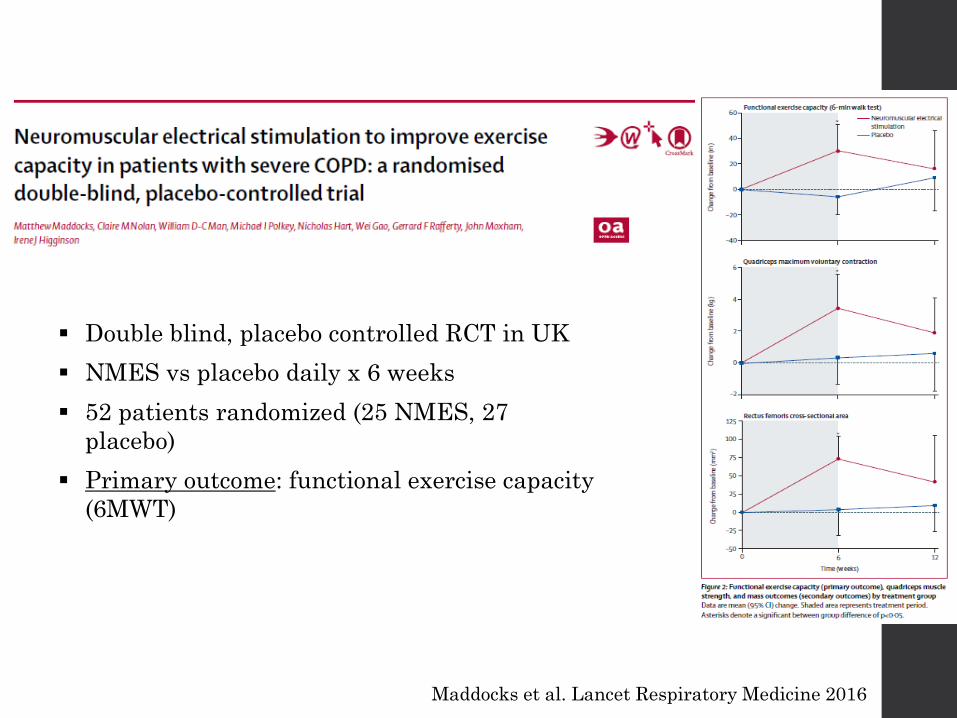
▪ Double blind, placebo controlled RCT in UK
▪ NMES vs placebo daily x 6 weeks
▪ 52 patients randomized (25 NMES, 27
placebo)
▪ Primary outcome: functional exercise capacity
(6MWT)
Maddocks et al. Lancet Respiratory Medicine 2016
Update on non-opioid pharmacologic Rx of dyspnea
• Benzodiazepines: Still no good evidence for use in dyspnea management
• Aerosol furosemide: Does not uniformly reduce dyspnea in healthy subjects Respir Physiol Neurobiol 2018; 247: 24-30
• Cannabinoids: No change in VAS but reported ‘air hunger’ descriptors less frequently Chronic Respir Dis 2011; 8(2): 109
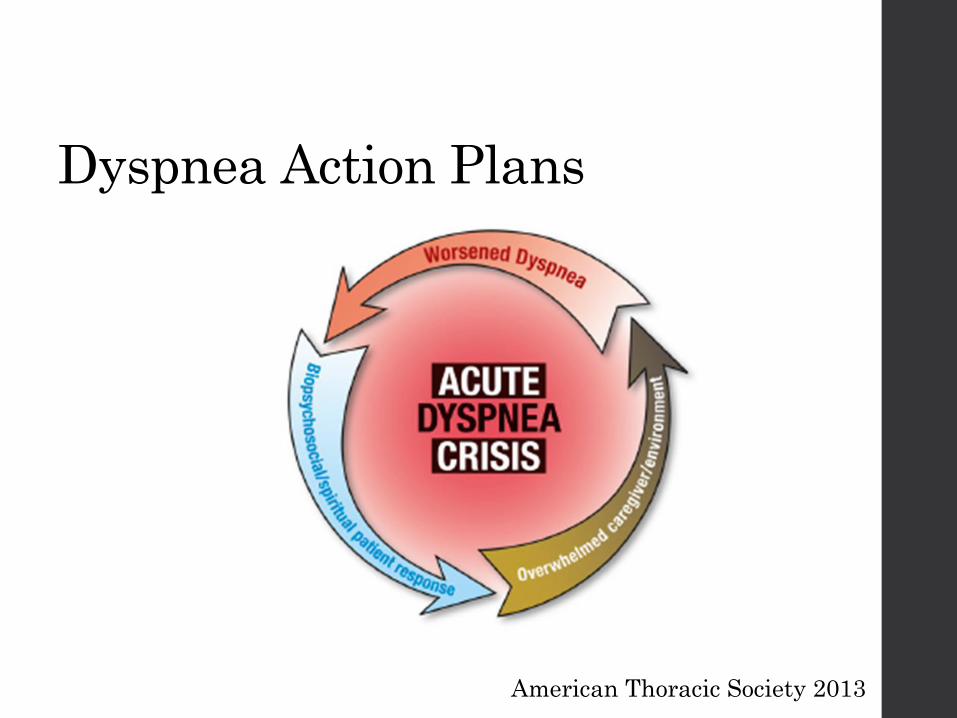
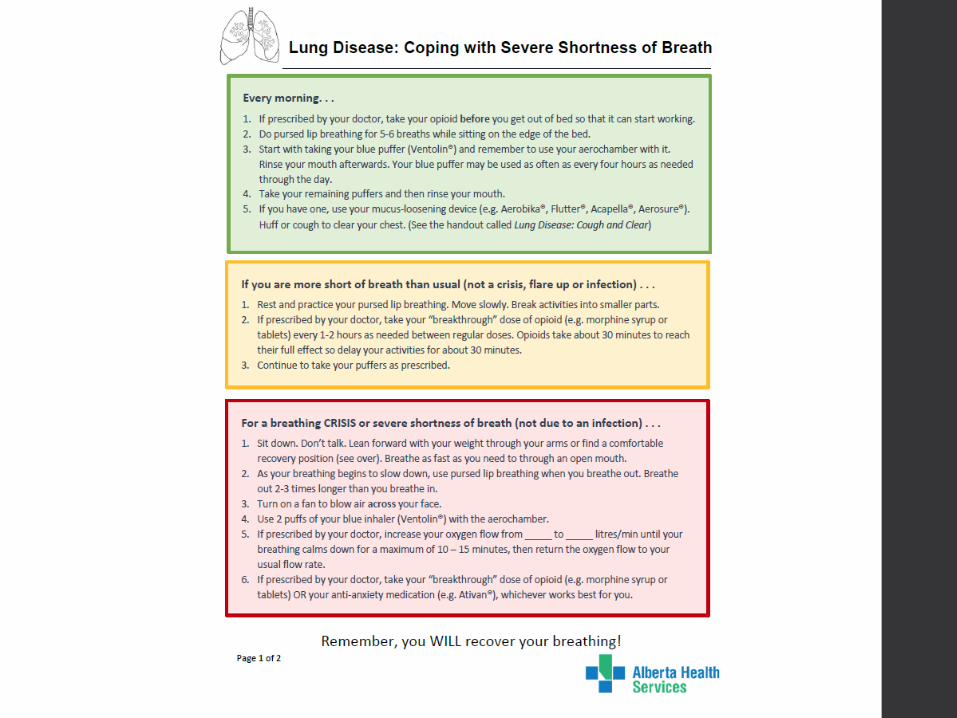
Dyspnea Action Plans
American Thoracic Society 2013
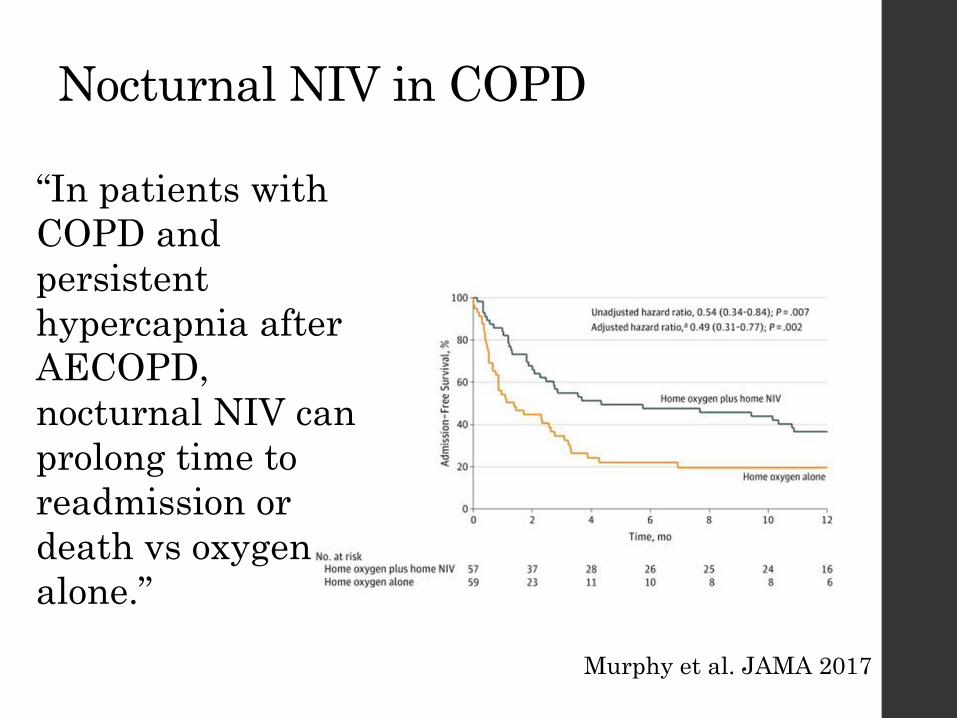
Nocturnal NIV in COPD
Murphy et al. JAMA 2017
“In patients with
COPD and
persistent
hypercapnia after
AECOPD,
nocturnal NIV can
prolong time to
readmission or
death vs oxygen
alone.”
NIV in COPD
• What will be the challenges of NIV use in your patients who are nearing the end of life?
Photo from Fisher & Paykel Healthcare
Models of Integrated Palliative Care in COPD
•Integrated palliative and respiratory care (UK)
•INSPIRED (Halifax, NS)
•CARE clinic (Calgary, AB)

• Improved breathlessness mastery (CRQ) in the intervention group vs. control
• Pre-post analysis: intervention group had improved quality of life, dyspnea, mastery, POS at 6 weeks.
• Survival benefit in the intervention group
Higginson et al. Lancet Respir Med 2014 (2): 979-987.
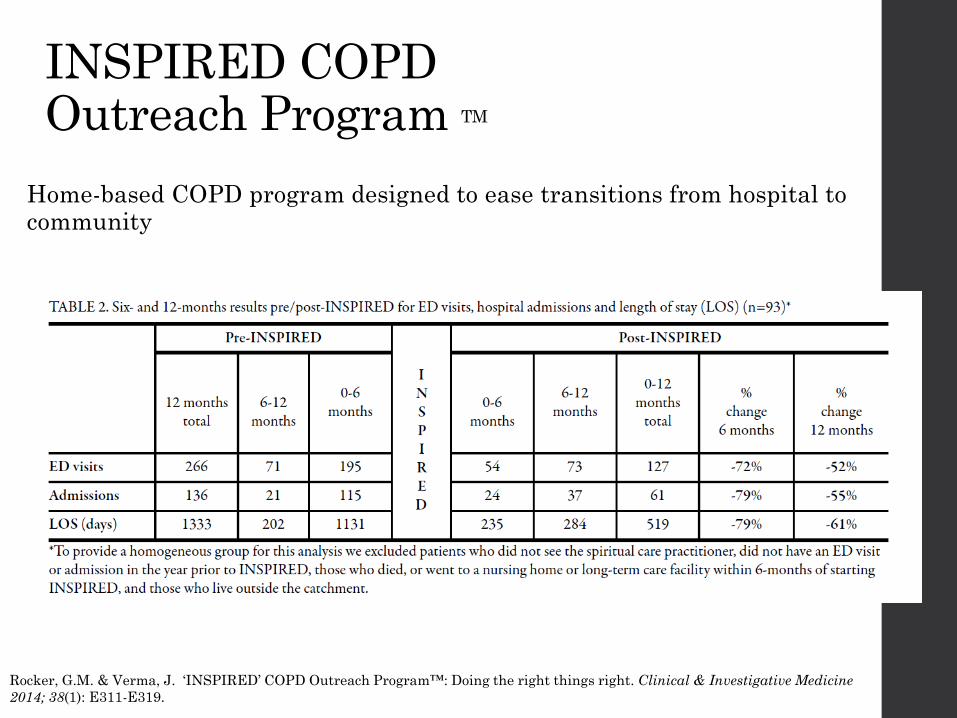
INSPIRED COPD Outreach Program TM
Home-based COPD program designed to ease transitions from hospital to community
Rocker, G.M. & Verma, J. ‘INSPIRED’ COPD Outreach Program™: Doing the right things right. Clinical & Investigative Medicine
2014; 38(1): E311-E319.
• Outpatient Respirology/Palliative care clinic for pts with severe disease
• Multidisciplinary team
• Person-centred care
• Comprehensive symptom assessment & management
ESAS
Dyspnea action plans
Opioid titration
• Longer appointment times
• Advance Care Planning and Goals of Care discussions
• Home visits
• Support for referring physician
• Education for trainees
• Close involvement with homecare teams
Calgary Advanced Respiratory diseasE clinic (CARE)
Summary
• People with COPD face unique challenges as the disease progresses
• Inhalers can reduce dyspnea in COPD (provided they are used properly)
• Opioids likely carry some risk
• New symptom control measures are available