Embed Size (px)
Citation preview

PROVIDER REFORM REQUIRES A ‘POPULATION VALUE-BASED’ PURCHASING SYSTEM
Dr Brian RuffPPO ServeSouth African ProfessionalProvider Organisation Services
Current….
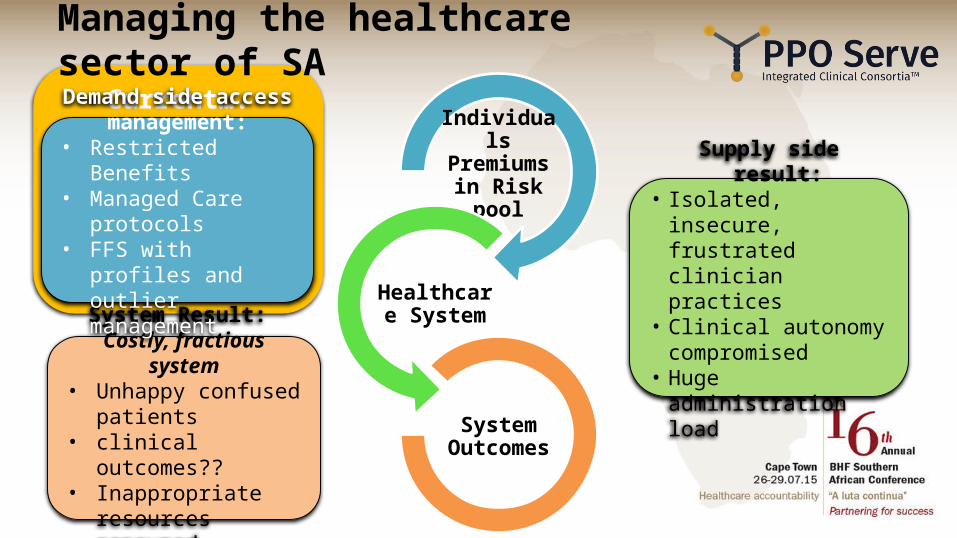
Managing the healthcare sector of SA
System Result: Costly, fractious system• Unhappy confused
patients• clinical outcomes??• Inappropriate
resources consumed
Supply side result:• Isolated, insecure,
frustrated clinician practices
• Clinical autonomy compromised
• Huge administration load
Demand side access management:
• Restricted Benefits• Managed Care
protocols• FFS with profiles and
outlier management
Individuals Premiums in
Risk pool
Healthcare System
System Outcomes
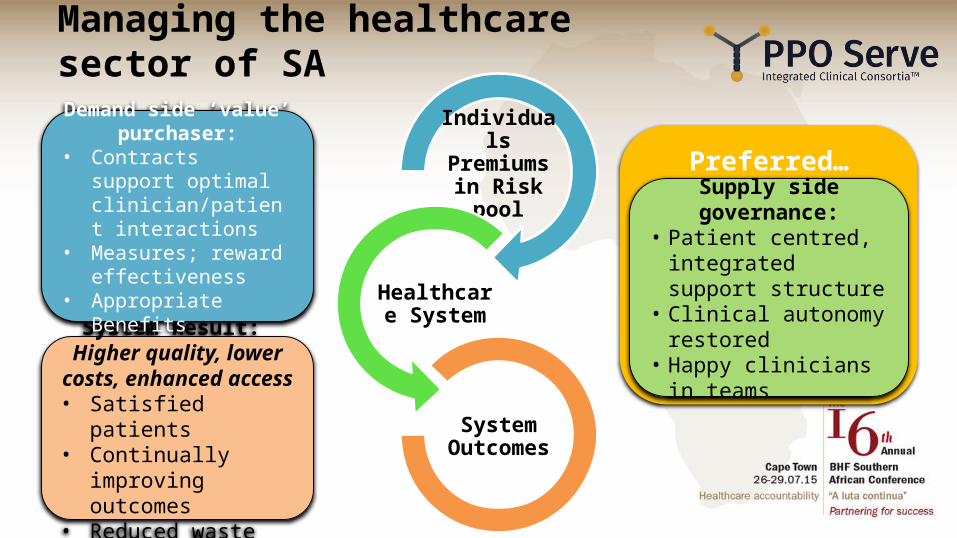
Preferred…
Managing the healthcare sector of SA
Individuals Premiums in
Risk pool
Healthcare System
System Outcomes
System Result: Higher quality, lower
costs, enhanced access• Satisfied patients • Continually improving
outcomes• Reduced waste
Supply side governance:• Patient centred,
integrated support structure
• Clinical autonomy restored
• Happy clinicians in teams
Demand side ‘value’ purchaser:
• Contracts support optimal clinician/patient interactions
• Measures; reward effectiveness
• Appropriate Benefits
Imagine a healthcare system…• That is organised around you and your family's medical and social problems
with a tailored care plan which reflects your preferences and leads to routine monitoring and reach out
• Where all healthcare professionals, including doctors, work together in local teams organised around you, focused on coordination and the quality of your medical care, with no gaps or waste. The team has a shared understanding of your complete care plan so interactions with you & family are straightforward
• Your Medical Scheme backs the clinical team to make the right decisions in a contract that measures and rewards quality care. Your benefits are comprehensive and affordable
Building blocks of Healthcare system reformPopulation medicine and the healthcare system: • Planned: capacity = local population needs • Patient & Community centered • Accountable for production / outcomes
Integrated local healthcare systems:• Collaborative Teams • Multidisciplinary, proactive patient centered approach
• Autonomous – owned & managed by working clinicians • Well supported – management, support staff; Health IT
Value contract – funds from ‘shared value’ with Medical Schemes:• Individual/FFS replaced by monthly Population Risk team fees +
Upside ‘Value’ rewards – quality/prudence measures• Competition is between coherent systems ~ via Schemes
How to achieve Population Medicine / Integrated Care / Value Contract?
6
Integrated Clinical ConsortiaTM
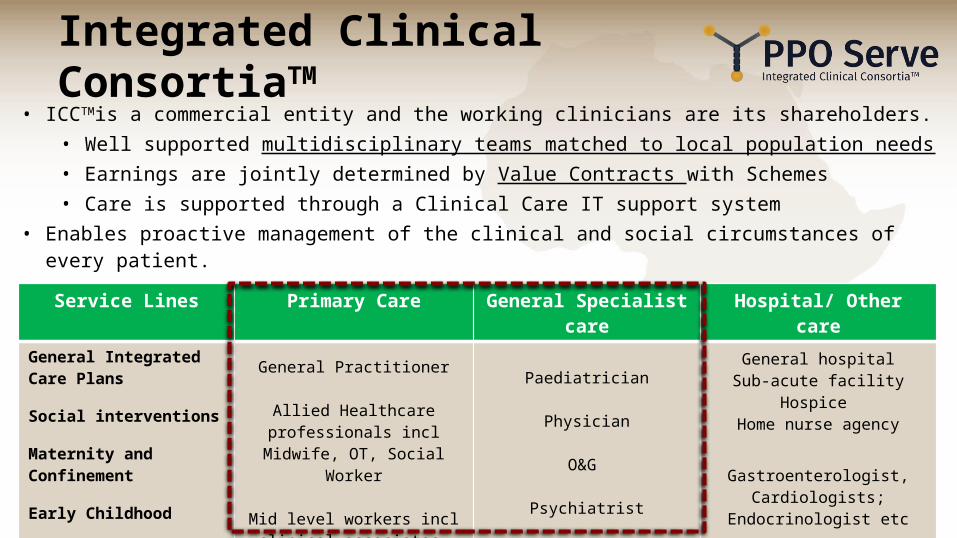
Service Lines Primary Care General Specialist care Hospital/ Other care
General Integrated Care Plans
Social interventions
Maternity and Confinement
Early Childhood
ENT & Respiratory Care
General Practitioner
Allied Healthcare professionals incl Midwife, OT, Social Worker
Mid level workers incl clinical associates, nurse coordinators
Paediatrician
Physician
O&G
Psychiatrist
General & ENT Surgeon
General hospitalSub-acute facility
Hospice Home nurse agency
Gastroenterologist, Cardiologists; Endocrinologist etc
Community organisations
Integrated Clinical Consortium Sub-contract
• ICCTMis a commercial entity and the working clinicians are its shareholders. • Well supported multidisciplinary teams matched to local population needs• Earnings are jointly determined by Value Contracts with Schemes • Care is supported through a Clinical Care IT support system
• Enables proactive management of the clinical and social circumstances of every patient.

Local; integrated care delivery to stable, defined populations
Hospital and other specialists
Home Nurse agency; Step down hospital
Rad/ Path
General Practitioner; Allied Healthcare Professionals; Mid level workers
Paediaticians; Physicians; Geriatricians; Psychiatrists; Gynaecologists; ENT, Urologists
Integrated Clinical ConsortiumSupported by PPO Serve
6 GPs; Allieds; mid level workers
0.5 Physici
an
0.3 Paeds
0.2 Psych
0.1 ENT, Uro
0.2 Gynae
6 GPs; Allieds; mid level workers
0.5 Physici
an
0.3 Paeds
0.2 Psych
0.1 ENT, Uro
0.2 Gynae
6 GPs; Allieds; mid level workers
0.5 Physici
an
0.3 Paeds
0.2 Psych
0.1 ENT, Uro
0.2 Gynae
6 GPs; Allieds; mid level workers
0.5 Physici
an
0.3 Paeds
0.2 Psych
0.1 ENT, Uro
0.2 Gynae
6 GPs; Allieds; mid level workers
0.5 Physici
an
0.3 Paeds
0.2 Psych
0.1 ENT, Uro
0.2 Gynae
6 GPs; Allieds; mid level workers
0.5 Physici
an
0.3 Paeds
0.2 Psych
0.1 ENT, Uro
0.2 Gynae
6 GPs; Allieds; mid level workers
0.5 Physici
an
0.3 Paeds
0.2 Psych
0.1 ENT, Uro
0.2 Gynae
6 GPs; Allieds; mid level workers
0.5 Physici
an
0.3 Paeds
0.2 Psych
0.1 ENT, Uro
0.2 Gynae
6 GPs; Allieds; mid level workers
0.5 Physici
an
0.3 Paeds
0.2 Psych
0.1 ENT, Uro
0.2 Gynae
6 GPs; Allieds; mid level workers
0.5 Physici
an
0.3 Paeds
0.2 Psych
0.1 ENT, Uro
0.2 Gynae
Complex; multi morbidity 2%
Chronic illness
8%
At risk25%
Healthy 65%
DiabetesPVD
IHD isolation
MyelomaEarly dementia
obesity
Hyper-tension
Care plans by need segments
15
60
203 2
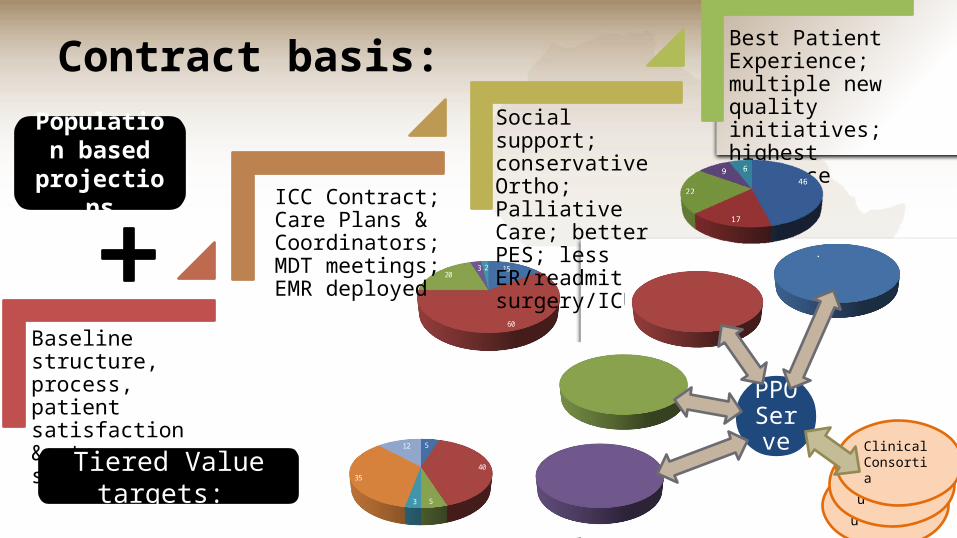
Contract basis:
Baseline structure, process, patient satisfaction &outcome scores
ICC Contract; Care Plans & Coordinators; MDT meetings; EMR deployed
Social support; conservative Ortho; Palliative Care; better PES; less ER/readmit, surgery/ICU
Best Patient Experience; multiple new quality initiatives; highest prudencePopulation
based projections
Tiered Value targets:
PPO Serve
Clinical Consortiu
Clinical Consortiu
Clinical Consortia
5
40
5
0
3
35
12
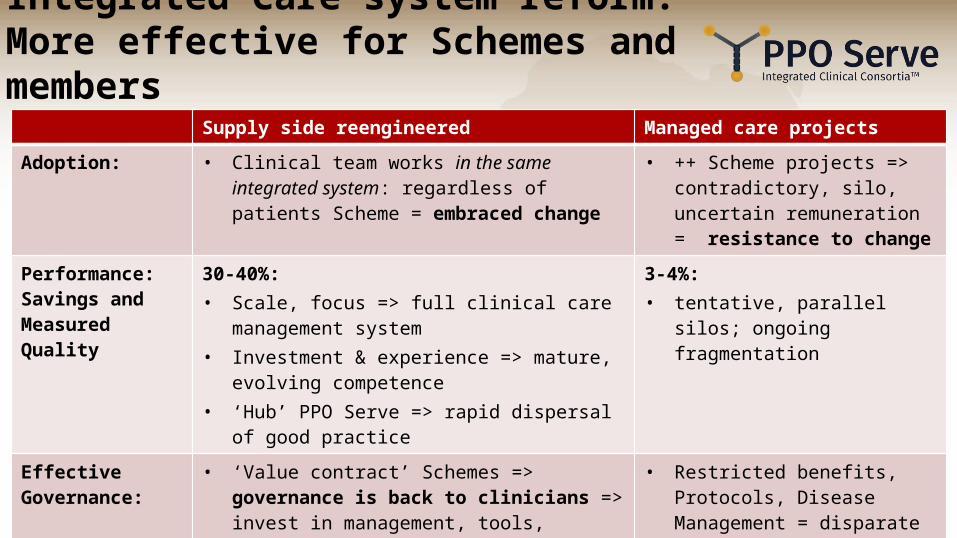
Supply side reengineered Managed care projects
Adoption: • Clinical team works in the same integrated system: regardless of patients Scheme = embraced change
• ++ Scheme projects => contradictory, silo, uncertain remuneration = resistance to change
Performance: Savings and Measured Quality
30-40%:• Scale, focus => full clinical care management system• Investment & experience => mature, evolving
competence • ‘Hub’ PPO Serve => rapid dispersal of good practice
3-4%:• tentative, parallel silos; ongoing
fragmentation
Effective Governance:
• ‘Value contract’ Schemes => governance is back to clinicians => invest in management, tools, infrastructure => autonomy, efficacy, clinical excellence => Better outcomes
• Restricted benefits, Protocols, Disease Management = disparate efforts, low effect => poor system performance
Integrated Care system reform: More effective for Schemes and members
Integrated Clinical Consortia: Patients Value PropositionPatients:• personalised care (plan) from an complete local
system• healthcare services are patient centered,
coordinated, accountable • Rare interactions with Schemes Consumers:• local health systems are branded, known entities
with sound reputations for the quality of their integrated care
Peninsula ICCTM - Effective Care • Schemes that contract with them share their
reputation and sell their story
Integrated Clinical Consortia: Individual Clinicians Value Proposition• Income is generous links to patient complexity, clinical practice experience &
merit• Gratifying work - proactive population care; top of scope practice & team
work matching each individual patient needs
• Clinical autonomy regained in a collaborative, commercial entity which they own & govern. Elected clinical leaders promote healthcare quality and prudence:• Peer mentoring • Strategic performance and planning• Promotes consortiums brand /
reputation for integrated quality careConsortium as a local empowering nexus: balancing the strength of Schemes & network hospitals

THANK YOU





























