Embed Size (px)
Citation preview

Provider Perceptions of Mental Health Literacy AmongYouth
Amy N. Mendenhall • Susan Frauenholtz •
Aislinn Conrad-Hiebner
� Springer Science+Business Media New York 2013
Abstract Approximately one in five children will have a mental health disorder at
some point in their lifetime (Merikangas et al. Pediatrics 125:75–81, 2010). Despite
this prevalence, many children are uninformed and unaware of how to recognize
and manage mental health disorders. Previous efforts to increase mental health
literacy focused on adults, not children. The purpose of this article is to begin filling
this gap by utilizing a survey to describe children’s mental health providers’ per-
ceptions of the amount, accuracy, and origin of mental health literacy in the children
and adolescents they treat and how mental health literacy impacts their work.
Eighty-seven mental health providers completed an online survey to explore per-
ceptions of children’s mental health literacy. Per providers’ reports, results dem-
onstrate that children’s mental health literacy is low, inaccurate, and inconsistent.
Consistent with previous research, providers reported that children primarily rely on
friends and peers for information about mental health disorders, with family as a
close second. Implications of these findings for social work practitioners,
researchers, and children are discussed.
Keywords Children � Youth � Adolescents � Mental health � Mental
health literacy � Mental health providers
Provider Perceptions of Mental Health Literacy Among Youth
Recent statistics indicate that mental health disorders remain prevalent among
children in the United States, creating enormous difficulties for both the children
themselves and their families (NIMH 2005). Approximately 20 % of children (or 1
A. N. Mendenhall (&) � S. Frauenholtz � A. Conrad-Hiebner
School of Social Welfare, University of Kansas, 1545 Lilac Avenue,
Lawrence, KS 66044-3184, USA
e-mail: [email protected]
123
Child Adolesc Soc Work J
DOI 10.1007/s10560-013-0321-5
in 5) currently or at some point in their lifetime will have a mental health disorder
(Merikangas et al. 2010). Yet in spite of the frequency with which children
experience mental health disorders, many remain uninformed and unaware of how
to recognize and manage them. In other words, they lack mental health literacy. The
term ‘‘mental health literacy’’, was first coined by the Australian researcher Anthony
Jorm and his colleagues in the late 1990s as an extension of the term ‘‘health
literacy,’’ and is defined as ‘‘knowledge and beliefs about mental health disorders
which aid their recognition, management or prevention’’ (Jorm et al. 1997, p. 182).
The initial mental health literacy survey conducted by Jorm et al. (1997) revealed
low levels of mental health literacy among Australian adults in the general public.
These striking results triggered a call by Jorm and his colleagues for efforts to raise
public levels of mental health literacy to increase mental health disorder recognition
and improve treatment utilization. The U. S. National Institute of Health (2000) has
also made research efforts to make mental health literacy a top priority.
In response, the topic of mental health literacy has garnered enthusiasm from
mental health researchers across the globe, spurring a substantial area of research
and the development of interventions to improve mental health literacy.
However, these efforts have predominately focused on adult populations and
have not given adequate consideration to the specialized concerns surrounding
the mental health literacy of children and adolescents. This is troubling, as the
initial onset of mental health disorders often occurs in childhood or adolescence
and early intervention might be helpful in reducing the severity and persistence
of early incipient mental health disorders (Kessler et al. 2007). Symptoms of
mental health disorders in children do not always present or manifest themselves
as they do in adults and certain disorders are diagnosed primarily in children
(American Psychiatric Association [DSM-IV-TR] 2000); hence the need for
mental health literacy research addressing the unique considerations of children
and youth.
A lack of accurate information and stereotypes about mental health disorders
held by both adults and youth can act as obstacles preventing children with mental
health disorders from getting the care they need (Rickwood et al. 2005). Therefore,
increasing mental health literacy among children and adolescents could result in the
reduction of stigma among peers and greater utilization of quality mental health
care. In addition, increased mental health literacy can provide children and
adolescents with the knowledge and skills they need to manage their own mental
health and act as helpful social supports to peers experiencing mental health
disorders. This is critical because research has shown that children are more likely
to rely on informal supports such as friends and family for information and
assistance relating to mental health. So by improving mental health literacy among
children and adolescents, we may be able to close the gap between those with
mental illness and those who actually receive treatment and increase the likelihood
of early identification and treatment. In order for efforts to increase mental health
literacy to be most effective, researchers and practitioners must first be aware of the
current level of mental health literacy among children and adolescents and how that
literacy was acquired.
A. N. Mendenhall et al.
123

Mental Health Literacy of Children and Youth
This section presents an overview of children’s mental health literacy related to the
prevention, identification, and treatment of mental health disorders and the
predictors of mental health literacy in children and adolescents. Because the field
of children’s mental health literacy is still developing, the literature remains
inconclusive but identifiable trends are emerging.
Children and Adolescents’ Mental Health Literacy Related to the Prevention,
Identification, and Treatment of Mental Health Disorders
Research indicates adolescents believe mental health disorders can be prevented by
having contact with friends and family and using self-help techniques such as
exercise, relaxation, and the avoidance of alcohol and drugs. Counter to clinical
wisdom, adolescents tend to believe that avoiding stressful situations is a helpful
prevention strategy (Jorm et al. 2010). Recent research suggests that mental health
disorder recognition among children and adolescents remains low, inconsistent, and
may vary by disorder (Wahl et al. 2012) although children and adolescents do
appear to be able to distinguish between peers with and without symptoms of
clinical disorders (Swords et al. 2011). In one study, Olsson and Kennedy (2010)
discovered that less than half of adolescents could correctly identify depression
(42.4 %) or anxiety (27.5 %), and Wright et al. (2005) observed poor recognition of
psychosis and depression among adolescents as well. However, it appears
adolescents may be more likely to recognize depression than other psychiatric
disorders (Leighton 2010; Olsson and Kennedy 2010), particularly if suicidal
ideation is present (Burns and Rapee 2006).
When considering treatment, the research indicates that children and adolescents
prefer informal sources of support such as friends, family and the internet over
specialized mental health services, and professionals with a general title such as
‘‘counselor’’ are viewed as more helpful than specialists such as psychologists or
psychiatrists (Jorm and Wright 2007; Wisdom and Agnor 2007; Wright et al. 2005).
Similarly, when responding to a peer with a mental health disorder, adolescents
identify informal interventions such as talking to and supporting a peer as their first
response before considering professional help (Jorm et al. 2007) and express
reluctance to engage the help of an adult (Kelly et al. 2006). Wahl et al.’s (2012)
recent study revealed that less than half of the middle school students they surveyed
believed medication could be helpful in treating a mental health disorder, and nearly
one-third thought that individuals with severe mental health disorders cannot get
better even with treatment.
Predictors of Mental Health Literacy in Children and Adolescents
Studies of mental health literacy among children and adolescents have identified
demographic characteristics that seem to impact mental health literacy. The findings
are not entirely consistent, but females generally demonstrate higher levels of
recognition of mental disorders (Cotton et al. 2006). Although further exploration is
Provider Perceptions of Mental Health Literacy Among Youth
123

required, a child’s age appears to predict mental health literacy as well. Hennessy
et al. (2008) discovered children begin identifying mental health problems in their
peers as young as preschool, but demonstrate increased ability to identify a wider
range of disorders as they get older, with attribution to internal causes becoming
more common in adolescence (Boxer and Tisak 2003). A school-based study of
adolescents conducted by Leighton (2010) indicated that socioeconomic status and
low educational attainment may not be associated with mental health literacy.
Continued study is needed to clarify the predictors of mental health literacy in
children and adolescents.
These initial studies suggest that although children and adolescents have some
knowledge of mental health disorders, many appear to lack the ability to recognize
mental health disorders and seek out effective treatment. While continued mental
health literacy research employing samples of children, adolescents, and their
caregivers is needed, little attention has been paid to the observations of
professionals who work with children with mental health disorders on a daily
basis, creating a significant gap in the emerging mental health literacy literature.
Providers’ first-hand observations of child and adolescent mental health literacy can
inform interventions designed to increase mental health literacy among children and
adolescents. Providers’ experiences can also enhance mental health treatment by
ensuring services are designed to appropriately address children and adolescents’
knowledge of and attitudes toward mental health disorders. The purpose of this
article is to begin filling the gap by utilizing a survey to describe children’s mental
health providers’ perceptions of the amount, accuracy and origin of mental health
literacy in the children and adolescents they treat and how mental health literacy
impact their work.
Method
Design and Procedures
This study is based on data collected from an online survey that was available from
July 2011 through September 2011. The target population was social workers in
Kansas or surrounding areas who work with children facing mental health
difficulties and their families. Participants were recruited by advertisements with a
direct link to the survey in e-newsletters or emails sent by the local NASW chapter,
the local school social workers association, and a children’s mental health
stakeholder’s group. The linked webpage included (1) additional details about the
purpose and methods of the study, (2) a link to start the survey, (3) and a place to
register for a $100 gift card drawing. Individuals who clicked the direct link from
the advertisement to find out more information about the study were eligible to
register for a $100 gift card drawing regardless of whether they actually completed
the survey. The anonymous survey did not collect personal identifying information
or link the participants’ email to their responses; the personal information for the
drawing was collected completely separate from the survey responses.
A. N. Mendenhall et al.
123

Survey
The survey included 29 items, all of which were multiple choice or short answer,
and took approximately 10 min to complete. The survey items were derived from a
review of the literature and discussions with mental health professionals, and the
final survey was reviewed for content and readability by a panel of mental health
researchers and clinicians. Qualtrics Survey Software was utilized to create and
administer the survey.
The survey items were grouped into four categories: (1) demographic charac-
teristics (age, gender, race, educational background, practice setting, number of
years working with youth); (2) providers’ perceptions of the parent’s mental health
literacy (how much knowledge do they have, where do they get their knowledge,
how accurate is their knowledge); (3) providers’ perceptions of youth’s mental
health literacy (how much knowledge do they have, where do they get their
knowledge, how accurate is their knowledge); and (4) the impact of youth and
parent mental health literacy on the providers’ work with families (does parent
knowledge impact how you approach your work, does child knowledge impact how
you approach your work, do you provide education to improve mental health
literacy). This paper focuses on the data collected in the third section about provider
perceptions about the youth’s mental health literacy.
Participants
A total of 104 individuals accessed the initial website explaining the study. Of those
individuals, 87 completed or almost fully completed the survey (at least half of the
questions were answered), 5 completed the demographic questions but did complete
any additional questions, 12 read the introductory website but never started the
actual survey. It is estimated that up to 1,000 individuals may have received
information about the study through advertisements in e-newsletters and emails.
However, exact distribution numbers are not known and not all of the individuals
receiving the study information through these means were eligible as the study was
specifically geared towards professionals who work or have worked with children
and adolescents who have mental illness. As such, a response rate cannot be
calculated, and results should not be generalized to all social workers working with
youth. Analyses were run using responses from the 87 participants who fully
completed or completed at least half of the questions. 78 % of participants were
(n = 68) female and the average age was 46 years (SD = 13.18). Respondents
were predominantly white (92 %, n = 80). The majority of the respondents had a
master’s degree in social work (80.5 %, n = 70), and even though this survey was
developed for social workers, there was a small portion of non-social workers who
completed it (15 %, n = 13). Table 1 lists basic demographics, the populations the
respondents worked with, and the average number of years working with that
population.
Provider Perceptions of Mental Health Literacy Among Youth
123

Analyses
SPSS Version 20 was used for all data analysis. Descriptive statistics were used to
summarize how providers characterized the mental health literacy of youth with
whom they worked. Spearman’s q and v2 analyses were conducted to test for the
relation between practitioner characteristics and their perceptions of the amount and
accuracy of child mental health literacy.
Results
The providers who completed the survey were asked how much knowledge children
typically have about mental illness the first time that they interact with the youth. Of
the providers, 85 % (n = 74) reported that the youth have ‘‘none’’ or ‘‘very little’’
knowledge about mental illness. When asked how they would characterize the
knowledge that the children did have, 62 % (n = 54) of the providers reported that
the knowledge that the youth do have is ‘‘inaccurate’’ or ‘‘very inaccurate,’’ whereas
the remaining providers (38 %, n = 32) reported the knowledge was a ‘‘mixture of
inaccuracy and accuracy.’’ None of the providers characterized the mental illness
knowledge level of the children they work with as ‘‘accurate’’ or ‘‘very accurate.’’
Table 1 Selected
demographics of mental health
providers (N = 86)
Variables Values
Age, M (SD) 46.8 (13.2)
Male, N, % 18, 21
White, N, % 80, 92
Educational background N, %
Bachelor’s social work 4, 4.6
Master’s social work 70, 80.5
Master’s psychology 2, 2.3
Master’s counseling 6, 6.9
Other 5, 5.7
Practice setting N, %
Schools 31, 35.6
Private practice 13, 15
Community mental health center 12,13.8
Social services agency 7, 8
Psychiatric hospital/residential treatment 6, 6.9
Other mental health setting 5, 5.7
Hospital/healthcare 4, 4.6
Other 9, 10.3
Number of years working with children with mental
illness, M (SD)
14.41
(11.9)
A. N. Mendenhall et al.
123
Providers’ perception of the amount of knowledge children have was positively
correlated with the accuracy of the knowledge (spearman’s q = .504, p \ .000).
When asked whether the amount or accuracy of child knowledge about mental
illness affects the work (or treatment plan) with the family, 11 % (n = 9) of
respondents said ‘‘not at all’’, 49 % (n = 42) said ‘‘to some extent’’, 26 % (n = 22)
said ‘‘to a moderate extent’’, and 14 % (n = 12) said ‘‘to a great extent’’.
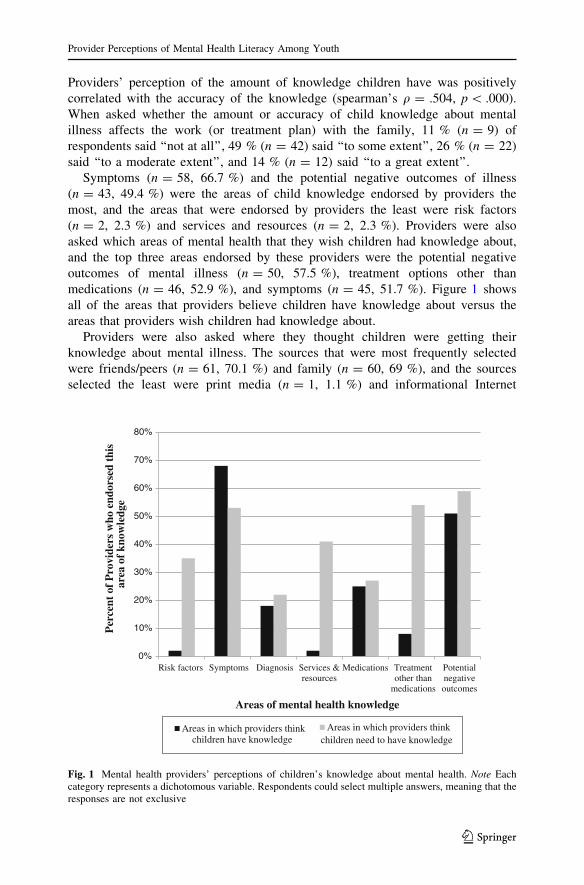
Symptoms (n = 58, 66.7 %) and the potential negative outcomes of illness
(n = 43, 49.4 %) were the areas of child knowledge endorsed by providers the
most, and the areas that were endorsed by providers the least were risk factors
(n = 2, 2.3 %) and services and resources (n = 2, 2.3 %). Providers were also
asked which areas of mental health that they wish children had knowledge about,
and the top three areas endorsed by these providers were the potential negative
outcomes of mental illness (n = 50, 57.5 %), treatment options other than
medications (n = 46, 52.9 %), and symptoms (n = 45, 51.7 %). Figure 1 shows
all of the areas that providers believe children have knowledge about versus the
areas that providers wish children had knowledge about.
Providers were also asked where they thought children were getting their
knowledge about mental illness. The sources that were most frequently selected
were friends/peers (n = 61, 70.1 %) and family (n = 60, 69 %), and the sources
selected the least were print media (n = 1, 1.1 %) and informational Internet
0%
10%
20%
30%
40%
50%
60%
70%
80%
Risk factors Symptoms Diagnosis Services &resources
Medications Treatmentother than
medications
Potentialnegativeoutcomes
Per
cent
of
Pro
vide
rs w
ho e
ndor
sed
this
Areas of mental health knowledge
Areas in which providers thinkchildren have knowledge
Areas in which providers thinkchildren need to have knowledge
are
a of
kno
wle
dge
Fig. 1 Mental health providers’ perceptions of children’s knowledge about mental health. Note Eachcategory represents a dichotomous variable. Respondents could select multiple answers, meaning that theresponses are not exclusive
Provider Perceptions of Mental Health Literacy Among Youth
123
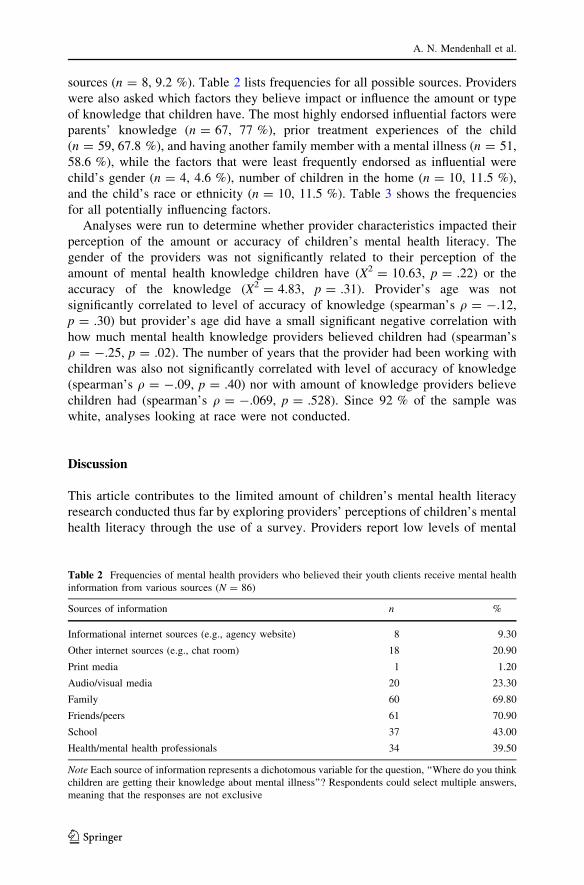
sources (n = 8, 9.2 %). Table 2 lists frequencies for all possible sources. Providers
were also asked which factors they believe impact or influence the amount or type
of knowledge that children have. The most highly endorsed influential factors were
parents’ knowledge (n = 67, 77 %), prior treatment experiences of the child
(n = 59, 67.8 %), and having another family member with a mental illness (n = 51,
58.6 %), while the factors that were least frequently endorsed as influential were
child’s gender (n = 4, 4.6 %), number of children in the home (n = 10, 11.5 %),
and the child’s race or ethnicity (n = 10, 11.5 %). Table 3 shows the frequencies
for all potentially influencing factors.
Analyses were run to determine whether provider characteristics impacted their
perception of the amount or accuracy of children’s mental health literacy. The
gender of the providers was not significantly related to their perception of the
amount of mental health knowledge children have (X2 = 10.63, p = .22) or the
accuracy of the knowledge (X2 = 4.83, p = .31). Provider’s age was not
significantly correlated to level of accuracy of knowledge (spearman’s q = -.12,
p = .30) but provider’s age did have a small significant negative correlation with
how much mental health knowledge providers believed children had (spearman’s
q = -.25, p = .02). The number of years that the provider had been working with
children was also not significantly correlated with level of accuracy of knowledge
(spearman’s q = -.09, p = .40) nor with amount of knowledge providers believe
children had (spearman’s q = -.069, p = .528). Since 92 % of the sample was
white, analyses looking at race were not conducted.
Discussion
This article contributes to the limited amount of children’s mental health literacy
research conducted thus far by exploring providers’ perceptions of children’s mental
health literacy through the use of a survey. Providers report low levels of mental
Table 2 Frequencies of mental health providers who believed their youth clients receive mental health
information from various sources (N = 86)
Sources of information n %
Informational internet sources (e.g., agency website) 8 9.30
Other internet sources (e.g., chat room) 18 20.90
Print media 1 1.20
Audio/visual media 20 23.30
Family 60 69.80
Friends/peers 61 70.90
School 37 43.00
Health/mental health professionals 34 39.50
Note Each source of information represents a dichotomous variable for the question, ‘‘Where do you think
children are getting their knowledge about mental illness’’? Respondents could select multiple answers,
meaning that the responses are not exclusive
A. N. Mendenhall et al.
123

health literacy in the children they treat, with a substantial number of providers
indicating children have very limited knowledge or none at all. In addition,
providers describe much of the mental health knowledge children have as inaccurate
and inconsistent. These results support previous findings (e.g. Olsson and Kennedy
2010; Wahl et al. 2012) and highlight even further the need for targeted efforts to
improve mental health literacy among children. Overall, results of the survey are
congruent with the limited research available regarding children’s mental health
literacy, indicating providers’ perceptions are likely reflective of the level of mental
health literacy of the children they serve.
When asked about where children receive information about mental health
disorders, providers reported friends and peers as the most significant source of
information, with family following as a very close second. These results reinforce
the findings of Jorm and Wright (2007) and others (Wisdom and Agnor 2007;
Wright et al. 2005) that children appear most likely to rely on informal sources of
support, such as friends and family, for information about and assistance with
managing mental health disorders. Providers identified schools as the third most
likely location where their child clients learn about mental health. Results from this
survey illustrate the importance of raising mental health literacy among not only
children, but also their key supports such as parents and caregivers, teachers,
coaches, and others who children frequently encounter and may turn to for help with
a mental health disorder. Additionally, because children are likely to turn to
informal social supports, such as friends, for information about and assistance with
mental health disorders, it is crucial that efforts to raise mental health literacy
target all children and not only those previously diagnosed with a mental health
disorder; thereby better preparing age-related peers to identify signs of a disorder in
others and intervene if a friend turns to them for assistance. An increased focus and
further development of school-based mental health literacy interventions hold
promise as a potentially effective way to universally increase the mental health
literacy of all children and adolescents (Pinto-Foltz et al. 2011; Schacter et al.
2008).
Table 3 Frequencies of mental
health providers who believed
their youth clients’ mental
health literacy was influenced or
impacted by various factors
(N = 86)
Note Each source of information
represents a dichotomous
variable for the question, ‘‘What
factors do you think impact or
influence the amount or
accuracy of children’s
knowledge of mental illness’’?
Respondents could select
multiple answers, meaning that
the responses are not exclusive
Factors n %
Child’s age 59 67.8
Child’s race/ethnicity 10 11.5
Child’s level of education 37 42.5
Child’s symptom severity 38 43.7
Child’s diagnosis 27 31
Child’s gender 4 4.7
Parents’ knowledge 67 77
Prior treatment experiences of the child 59 67.8
Area where they live 20 23
Number of children in the home 10 11.5
Having another family member with mental illness 51 58.6
The media 22 25.3
Provider Perceptions of Mental Health Literacy Among Youth
123

Providers identified parent knowledge of mental health disorders as the most
influential factor impacting the amount or accuracy of children’s mental health
knowledge. This result seems logically consistent, given that the providers in this
survey and children themselves both report family as one of the top resources for
mental health support and information. This finding also supports the work of Jorm
et al. (2008), which discovered that parents and children are more likely to share
mental health attitudes with each other than with professional clinicians. Providers’
perceptions that children with previous treatment experiences or another family
member with a mental health disorder increase mental health literacy are similar to
previous findings in the literature (Leighton 2010). It seems plausible that children
will acquire more accurate information about mental health disorders while in
treatment or, similarly, will obtain second-hand information by observation of a
parent or sibling’s experience with a mental health disorder and related treatment.
These findings support the need for and potential benefits of further integrating a
psychoeducational component into mental health disorder interventions with all
children and families.
Startlingly, 60 % of providers stated that the children’s level of mental health
knowledge impacted their work with the child ‘‘not at all’’ or only ‘‘to some extent’’.
It appears that some providers may not be adequately assessing the mental health
knowledge and attitudes of the children they treat and using that information to
inform their practice. Given that treatment experiences appear to increase children’s
knowledge of mental health disorders, providers themselves must be further
educated about the importance of addressing mental health literacy in their work
with children. By incorporating interventions and activities to increase child mental
health literacy, and adapting those interventions to the child’s current level of
mental health knowledge, providers could hone their treatment approach to meet the
unique needs of the individual child being served and potentially improve the
quality of treatment outcomes.
Surprisingly, given the popularity of the internet and other forms of social media
among children and adolescents, providers identified them as less likely sources of
mental health information in the children and adolescents they treat than
interpersonal resources. When children utilize web-based resources, according to
the providers surveyed, it appears they are more likely to access informal sources,
such as chat rooms, instead of informational resources such as the National Institute
of Mental Health’s website or other agency-based resources. This result is
concerning, as the quality of the mental health information provided on informal
sites is not reliable and could be inaccurate. Although it is impossible to know if
providers’ perceptions are representative of children’s online actions, this finding
demonstrates the need to further develop and refine readily available, legitimate
internet resources that are visually appealing and designed specifically for children
and adolescents. Such initiatives could prove fruitful in improving mental health
literacy in children and initial research indicates online interventions hold promise
(Oh et al. 2009).
Although directionality could not be assessed from the survey, providers did
report a child’s age substantially influences the amount or accuracy of a child’s
mental health knowledge, echoing the results of Boxer and Tisak (2003) and
A. N. Mendenhall et al.
123
Hennessy et al. (2008). Although previous research has indicated that girls may have
higher levels of mental health literacy than their male counterparts (Cotton et al.
2006), the providers in this survey did not report similar observations in their practice.
In addition, race and ethnicity were not identified by providers as significantly
influencing children’s mental health literacy. A variety of factors could account for
these results. Providers’ perceptions could be accurate, revealing that factors such as
race and sex are not key predictors of mental health literacy. Conversely, it is also
possible that providers themselves are not fully aware of the role that socio-
demographic factors play in influencing mental health literacy in children or that these
providers’ client populations lack diversity. Finally, perhaps additional factors, such
as personal and family experience with mental health disorders, are more salient
regardless of a child’s socio-demographic status. Much work remains to be done in
parceling out the role of socio-demographics as predictors of mental health literacy.
The responses of providers also revealed valuable information that can be used to
refine and focus current efforts underway to increase children’s mental health
literacy. Providers expressed the desire for more children to know about the
potentially negative outcomes of mental health disorders if left untreated, as well as
increased child knowledge about available treatments, an area where children
consistently demonstrate a lack of knowledge and inaccurate understanding in the
literature (Jorm et al. 2010; Wahl et al. 2012). Given the significant discrepancy
between those diagnosed with mental health disorders and those who access the
growing number of evidence-based treatments now available, increased focus on
information about treatment options should be a top priority of mental health
literacy interventions. In addition, although providers indicated children are most
likely to have knowledge regarding the symptoms of mental health disorders, they
also expressed the need for further education regarding symptom identification.
These results parallel the literature, which indicates children have some ability to
identify the symptoms of mental health disorders but lack full and consistent
knowledge (Olsson and Kennedy 2010; Wahl et al. 2012). Increased symptom
identification can also play a critical role in ensuring more children diagnosed with a
mental health disorder are referred for treatment.
The primary limitation of this survey study is its reliance upon a relatively small
convenience sample of providers who responded to an advertisement. Therefore, it
is not possible to assess the response rate, and the viewpoints of those providers
choosing to respond may differ and not be representative of the larger pool of
potential respondents who did not complete the survey. Further, survey respondents
were generally quite homogeneous with regards to sex, race, age and educational
background. In addition, social workers in school settings accounted for more than
one-third of respondents and were overrepresented. This lack of diversity among
respondents could also have contributed to bias in the survey results. Because this
survey investigated the self-reported perceptions of providers and not the first-hand
responses of children themselves, it is possible that the providers’ perceptions
contained inaccuracies and additional unknown bias. Finally, the perceptions of
children’s mental health literacy identified by providers were informed by their
observations of children whom they see in clinical practice. While these perceptions
provide valuable information, it is important to consider that the mental health
Provider Perceptions of Mental Health Literacy Among Youth
123

literacy of those children may not be generalizable and could differ from that of
their peers who have mental health disorders but have not accessed treatment, as
well as children without mental health disorders.
However, in spite of the limitations noted above, this article provides a
significant contribution to the mental health literacy literature because of its focus
on children’s literacy, an area frequently overlooked in current mental health
literacy research. In particular, this paper’s focus on providers’ perceptions, even
with the unavoidable limitations, provides another perspective regarding how
providers view and use the mental health knowledge of the children they serve. The
inclusion of this viewpoint is essential to discern how provider perceptions may be
consistent or differ from other findings related to children’s mental health literacy.
Indeed, although providers’ perceptions may be biased, they also bring a unique
strength not found in surveys which rely on child and adolescent self-report, given
that children are likely unable to accurately report and describe knowledge they do
not have. Areas of congruence and potential discrepancy between provider and child
self-report surveys can be used to deepen our understanding of children’s mental
health literacy and develop more effective mental health literacy interventions.
While significant progress has been made in the growing area of children’s mental
health literacy research to inform practice and improve outcomes for children with
mental health disorders, much more remains to be discovered.
Acknowledgments This research was supported by a Grant from the University of Kansas New Faculty
General Research Fund.
References
American Psychiatric Association. (2000). Diagnostic and statistical manual of mental disorders (4th
ed.). Washington, DC: American Psychiatric Association.
Boxer, P., & Tisak, M. (2003). Adolescents’ attributions about aggression: An initial investigation.
Journal of Adolescence, 26, 559–573.
Burns, J. R., & Rapee, R. M. (2006). Adolescent mental health literacy: Young people’s knowledge of
depression and help seeking. Journal of Adolescence, 29(2), 225–239.
Cotton, S. M., Wright, A., Harris, M. G., Jorm, A. F., & McGorry, P. D. (2006). Influence of gender on
mental health literacy in young Australians. Australian and New Zealand Journal of Psychiatry,
40(9), 790–796.
Hennessy, E., Swords, L., & Heary, C. (2008). Children’s understanding of psychological problems
displayed by their peers: A review of the literature. Child: Care, Health and Development, 34, 4–9.
Jorm, A. F., Korten, A. E., Jacomb, P. A., Christensen, H., Rodgers, B., & Pollitt, P. (1997). ‘‘Mental
health literacy’’: A survey of the public’s ability to recognize mental disorders and their beliefs
about the effectiveness of treatment. Medical Journal of Australia, 166, 182.
Jorm, A. F., Morgan, A. J., & Wright, A. (2008). Interventions that are helpful for depression and anxiety
in young people: A comparison of clinicians’ beliefs with those of youth and their parents. Journal
of Affective Disorders, 111(2/3), 227–234.
Jorm, A. F., Morgan, A. J., & Wright, A. (2010). Actions that young people can take to prevent
depression, anxiety and psychosis: Beliefs of health professionals and young people. Journal of
Affective Disorders, 126, 278–281.
Jorm, A. F., & Wright, A. (2007). Beliefs of young people and their parents about the effectiveness of
interventions for mental disorders. Australian and New Zealand Journal of Psychiatry, 41, 656–666.
Jorm, A. F., Wright, A., & Morgan, A. J. (2007). Beliefs about appropriate first aid for young people with
mental disorders: Findings from an Australian national survey of youth and parents. Early
Intervention Psychiatry, 1, 61–70.
A. N. Mendenhall et al.
123

Kelly, C. M., Jorm, A. F., & Rodgers, B. (2006). Adolescents’ responses to peers with depression or
conduct disorder. Australian and New Zealand Journal of Psychiatry, 40(63), 63–66.
Kessler, R. C., Amminger, G. P., Aguilar-Gaxiola, S., Alonso, J., Lee, S., & Ustun, T. B. (2007). Age of
onset of mental disorders: A review of recent literature. Current Opinion Psychiatry, 20(4), 359–364.
Leighton, S. (2010). Using a vignette-based questionnaire to explore adolescents’ understanding of
mental health issues. Clinical Child Psychology and Psychiatry, 15(2), 231–250.
Merikangas, K. R., He, J. P., Brody, D., Fisher, P. W., Bourdon, K., & Koretz, D. S. (2010). Prevalence
and treatment of mental disorders among US children in the 2001–2004 NHANES. Pediatrics,
125(1), 75–81.
National Institute of Mental Health. (2005). Mental illness exacts heavy toll, beginning in youth. Retrieved from
http://www.nimh.nih.gov/science-news/2005/mental-illness-exacts-heavy-toll-beginning-in-youth.shtml.
Oh, W., Jorm, A. F., & Wright, A. (2009). Perceived helpfulness of websites for mental health
information: A national survey of young Australians. Social Psychiatry and Psychiatric
Epidemiology, 44(4), 293–299.
Olsson, D. P., & Kennedy, M. G. (2010). Mental health literacy among young people in a small US town:
Recognition of disorders and hypothetical helping responses. Early Intervention in Psychiatry, 4(4),
291–298.
Pinto-Foltz, M. D., Logsdon, M. C., & Myers, J. A. (2011). Feasibility, acceptability, and initial efficacy
of a knowledge-contact program to reduce mental illness stigma and improve mental health literacy
in adolescents. Social Science and Medicine, 72, 2011–2019.
Rickwood, D., Deane, F. P., Wilson, C. J., & Ciarrochi, J. (2005). Young people’s help-seeking for
mental health problems. Advances in Mental Health, 4(3), 218–251.
Schacter, H. M., Giradi, A., Ly, M., Lacroix, D., Lumb, A. B., van Berkom, J., et al. (2008). Effects of
school-based interventions on mental health stigmatization: A systematic review. Child and
Adolescent Psychiatry and Mental Health, 2, 18.
Swords, L., Hennessy, E., & Heary, C. (2011). Adolescents’ beliefs about sources of help for ADHD and
depression. Journal of Adolescence, 34(3), 485–492.
Wahl, O., Susin, J., Lax, A., Kaplan, L., & Zatina, D. (2012). Knowledge and attitudes about mental
illness: A survey of middle school students. Psychiatric Services, 63(7), 649–654.
Wisdom, J. P., & Agnor, C. (2007). Family heritage and depression guides: Family and peer views
influence adolescent attitudes about depression. Journal of Adolescence, 30(2), 333–346.
Wright, A., Harris, M. G., Wiggers, J. H., Jorm, A. F., Cotton, S. M., & McGorry, P. D. (2005).
Recognition of depression and psychosis by young Australians and their beliefs about treatment.
Medical Journal of Australia, 183, 18–23.
Provider Perceptions of Mental Health Literacy Among Youth
123





























