Embed Size (px)
Citation preview

Proton Beam Therapy at Mayo Clinic
Jon J. Kruse, Ph.D.Mayo Clinic Dept. of Radiation Oncology
Rochester, MN

History of Proton Therapy at Mayo
• 2002: Decided to consider particle therapy – analysis and education
• 2006: Initial meetings with manufacturers
• 2007: Initial RFP• Protons + Carbon• Scattered + Scanned beams
• 2008: Decision that the future was scanning particle beams
• 2/2010: Permission to Plan• RST + AZ

History of Proton Therapy at Mayo
• 3/2010: Final RFP, protons only
• 11/2010: Board of Trustees approval
• 12/2010: Selected Hitachi as vendor
• 5/2011: Mayo/Hitachi contract signed
• 9/2011: RST groundbreaking
• 6/2013: Equipment installation began
• 3/2015: First RST Tx rooms accepted
• 6/2015: First Tx in RST

Mayo Clinic Proton Beam Therapy Centers
• Two identical treatment facilities• Rochester, MN 2015• Phoenix, AZ 2016
• Synchrotron-based
• Four gantries (180 degrees)
• One fixed beam room
• All five nozzles in each facility are identical – optimized for scanning beam only

Mayo Clinic Proton Beam Therapy Centers
• Design goals• Highest quality treatment available• High efficiency
• ~1200 patients per year, per facility
• Infrastructure for efficient treatment of complex disease sites• Radiographic imaging suites outside
treatment room• Remote anesthesia• Scanning beam nozzles

Both Centers Adjacent to Photon Clinics

Facility Layout

Facility Layout

Half Gantry Treatment Room


10/15/2011

03/09/20125/8/2012
Richard O. Jacobson Building

05/03/20125/8/2012
Richard O. Jacobson Building

5/8/2012
Richard O. Jacobson Building05/22/2012

08/30/201210/08/2012

11/12/2012


Rochester Install 9-24-13

Rochester G3 9-24-13


Treating Cancer with Scattered Protons
Patient
Tumor
250 MeV Proton Beam

Patient
Tumor
250 MeV Proton Beam
Treating Cancer with Scattered Protons

Treating Cancer with Scattered Protons
Patient
Tumor
Reduced Energy Proton Beam

Treating Cancer with Scattered Protons
Patient
Tumor
Add Double Scatterer
Tradeoff between field size and range

Treating Cancer with Scattered Protons
Patient
Tumor
Add Field Aperture

Treating Cancer with Scattered Protons
Patient
Tumor
Custom machined brass part must be changed
between fields
Nozzle must be very close to patient
And brass is expensive, and a potential source
of neutrons

Treating Cancer with Scattered Protons
Patient
Tumor
Spread out peak with modulator wheel
Must accept maximum modulation width over
entire tumor

Treating Cancer with Scattered Protons
Patient
Tumor
Match Distal Proton Range with Compensator
Compensator must be machined for each field,
and changed by hand

250 MeV Proton Beam
Raster-scanned Proton BeamPatient
Tumor

Treating Cancer with Scanned ProtonsPatient
Tumor
Variable EnergyProton Beam
Y-Scanning Magnets
X-Scanning Magnets

Active Scanning Proton Beams
Passive Scattering Active Scanning

Proton Developments at Mayo
• Hitachi has installed a scanning proton treatment room at M.D. Anderson
•Mayo’s facility is scanning beam only
• Redesign of many components• Synchrotron• Gantry • Nozzle• Console/HMI• IGRT
• Efficient treatment of complex cases

MDA -> Mayo Synchrotron
Smaller Footprint24ft 18.5ft dia.
Fewer ComponentsLower CostLess PowerSimpler Maintenance
Fast Room SwitchSmaller Beam Spot

Gantry~5M smaller
~60 tons lighterBetter patient
access
Gantry~5M smaller
~60 tons lighterBetter patient
access
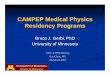
MDA
Mayo

Old Spot
New Spot
New Nozzle: Smaller Spot
10/08/2012 Richard O. Jacobson Building
TumorNormal Organ

Scanning Nozzle RedesignMD Anderson Nozzle Mayo Nozzle
Gillin et al., Med Phys 37 (2010) p. 154

New Console

New HMI

New HMI

HMI Design w/ RTT in Omika

~Monthly Design Meetings in Hitachi

Mayo-Hitachi Design Teams at Hitachi Works
Mayo-Hitachi Omika Teams at Omika Works

Facility Infrastructure for Complex Cases
Anesthesia SuiteImaging Rooms
Beam Matched Tx Rooms

Why Do Active Scanning?
• Dosimetric advantages• No tradeoff between field size/depth• Variable modulation width• Higher resolution distal range
compensation• No hardware in the beam
• Easier planning• IMPT• Adaptive planning without new hardware
• Efficiency• Cycle through Tx fields from control room

Why Not Do Active Scanning?
• Lateral penumbra• Scattered beams can achieve a very sharp
lateral penumbra, via brass aperture very close to the patient• With scanning beams, in some cases the
lateral penumbra is dominated by spot size in air – not as sharp as a collimated scattered beam
• Interplay• Time dependent dose delivery of a scanning
beam is problematic for moving tumors

Interplay• Scattered beams irradiate entire target
volume with almost no time dependence• Traditional photon ‘ITV’ approach to
moving targets works fairly well
• Scanning beams scan through the target volume• ~mSec time scale for a single spot• ~100s to 1000s spots per layer• ~Several to dozens of layers per field• ~Seconds to change energy• 1 field may take tens of seconds to ~ 1 min• Some portions of target may be double
painted, others missed

Interplay Effects
Bert et al., PMB 53 (2008) p. 2253

Solutions for Moving Targets
• Optimized Planning Parameters
• Gating
• Breath hold
• Repainting
• Tracking

Optimized Planning: Spot Spacing
Bert et al., IJROBP 73 (2009) p. 1270

Optimized Planning: Scanning Direction
Static 1 cm parallel 1 cm orthogonal
Johnson et al., in preparation

Delivery Options: Breath Hold
• Careful patient selection a must
• Feedback tools, coaching
• Reduced treatment time• Faster energy changes• Reduced number of energy levels

Reducing Number of Energy Levels
Gillin et al., Med Phys 37 (2010) p. 154

Reducing Number of Energy Levels
• Mini ridge filter introduces modest spatial dependence of beam energy
• Spatial component disappears quickly with phantom scatter
• Shallower dose falloff allows for fewer energy levels
• Decreased treatment time
• Higher dose/spotCournyea et al., AAPM 2013 Tues AM

Treatment Times with Ridge Filter
• Standard plans: • 67 s (no MRF)• <30 s (w/ MRF)
• Stereotactic plans:• 95.4 s (no MRF)• 47.7 s (min)
• Diminishing gains as MRF thickness increased. MRF Thickness (cm)
0 0.5 1 1.5 2 2.5
Ave
rage
Tim
e/F
ield
(s)
0
20
40
60
80
100 SRσ2
SRσ3 SRσ4
σ2
σ3 σ4
SRσ2
SRσ3 SRσ4
σ2
σ3 σ4
Cournyea et al., AAPM 2013 Tues AM

Delivery Options: Repainting
• Only a portion of the prescribed dose delivered in a single pass
• Repeat the delivery multiple times per fraction
• Individual hot/cold spots averaged out as number of repaints increases

Delivery Options: Repainting
1 Scan 10 Scans
Furukawa et al., Med Phys 37 (2010) p. 4874

IGRT in Mayo Clinic Half Gantry
• Fast Intra-Tx imaging at any gantry/couch position
• Fluoroscopy capable
• Large FOV
• No moving parts –stable imaging isocenter
• 6 DOF matching software

IGRT in Mayo Clinic Half Gantry
• Limited to two imaging angles
• FOV is 30 cm x 30 cm at isocenter –may not see center of tumor volume for non-isocentric plans
• Not CBCT capable

Utility of CBCT for Protons
• Bony anatomy is often a poor surrogate for target/critical anatomy
• Fiducials or CT localization required in cases where we expect movement of soft tissues relative to radiographically evident bony anatomy
• Photons: Place target tissue at isocenter, don’t worry about ‘upstream’ bony anatomy
• Protons: ??

CT Localization for Protons: Pelvis
• Change in position of bony anatomy alters dose distribution
• CT localization may be of limited use

• Change in position of rib causes minimal disturbance of dose distribution
• CT localization of lung tumors desirable for proton therapy
CT Localization for Protons: Lung

CBCT for Lung?
•Mayo proton facilities will be scanning beam only
• Treatments of mobile tumors will probably require gating/breath hold
• Free-Breathing CBCT imaging a poor reference for gated/breath held treatment
• Gated/breath held CBCT not impossible, but not easy

CBCT for Adaptive Protocols
• Proton dose calculation is extremely sensitive to CT number accuracy
• CT number accuracy / consistency not generally a priority in CBCT
• Increased scatter relative to helical CT degrades imaging performance

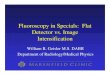
Helical/CBCT Phantom Images
Helical CT
CBCT
Images Courtesy of T.J. Whitaker

CT on Rails

CT on Rails
• Robot moves patient to imaging isocenter
• CT translates over patient for imaging
• Robot moves patient back to treatment isocenter while CT registration is performed
• Helical CT image quality• Images for adaptive imaging
• Fast image acquisition
• 4D imaging capability