Embed Size (px)
Citation preview

Outpatient and Ambulatory Surgery CAHPS
® Survey
Protocols and Guidelines Manual
Version 1.2
December 2015


This page intentionally left blank.


Centers for Medicare & Medicaid Services i Outpatient and Ambulatory Surgery CAHPS Survey Protocols and Guidelines Manual
COMMUNICATIONS AND TECHNICAL SUPPORT FOR THE OUTPATIENT AND
AMBULATORY SURGERY CAHPS SURVEY
Hospital outpatient departments, ambulatory surgery centers and survey vendors may use
the following resources to obtain information or technical support with any aspect of the
Outpatient and Ambulatory Surgery CAHPS Survey.
For general information, important news, updates, and all materials to support implementation of
the Outpatient and Ambulatory Surgery CAHPS Survey:
https://oascahps.org/
For technical assistance, contact the Outpatient and Ambulatory Surgery CAHPS Survey
Coordination Team as noted below.
By e-mail: [email protected]
By telephone: (866) 590-7468
Hospital outpatient departments, ambulatory surgery centers and Outpatient and Ambulatory
Surgery CAHPS (OAS CAHPS) Survey vendors must provide the facility’s name and CMS
Certification Number (CCN) when contacting the OAS CAHPS Survey Coordination Team by
e-mail or telephone for technical assistance.

ii Centers for Medicare & Medicaid Services Outpatient and Ambulatory Surgery CAHPS Survey Protocols and Guidelines Manual
This page intentionally left blank.

Centers for Medicare & Medicaid Services iii Outpatient and Ambulatory Surgery CAHPS Survey Protocols and Guidelines Manual
LIST OF ABBREVIATIONS AND ACRONYMS
OUTPATIENT AND AMBULATORY SURGERY CAHPS SURVEY PROTOCOLS AND
GUIDELINES MANUAL
Abbreviation/ Acronym Term/Phrase
AAPOR American Association for Public Opinion Research
AHRQ Agency for Healthcare Research and Quality
ASC Ambulatory surgery center
CAH Critical access hospital
CAHPS Consumer Assessment of Healthcare Providers and Systems
CATI Computer-assisted telephone interview
CCN CMS Certification Number (formerly known as the Medicare Provider
Number)
CMS Centers for Medicare & Medicaid Services
CPT Current Procedural Terminology
DHHS Department of Health and Human Services
DSRS Disproportionate stratified random sampling
FAQ Frequently Asked Questions (a list of frequently asked questions and
suggested responses)
HIPAA Health Insurance Portability and Accountability Act
HOPD Hospital outpatient department
ICD-9-CM International Classification of Diseases, 9th Revision, Clinical Modification
ICD-10 International Classification of Diseases, 10th Revision
IRB Institutional Review Board
MRN Medical Record Number
NCOA National Change of Address
NQF National Quality Forum
OAS CAHPS Outpatient and Ambulatory Surgery CAHPS Survey
OMB Office of Management and Budget
OPPS Outpatient Prospective Payment System
PHI Private health information
PII Personally identifiable information
PSRS Proportionate stratified random sampling
QAP Quality Assurance Plan
RAT-STATS Regional Advanced Techniques Staff Statistics Program
SAS Statistical Analysis System

iv Centers for Medicare & Medicaid Services Outpatient and Ambulatory Surgery CAHPS Survey Protocols and Guidelines Manual
Abbreviation/ Acronym Term/Phrase
SID Sample identification (number)
SRS Simple random sampling
SSS Stratified systematic sampling
XML Extensible Markup Language

Centers for Medicare & Medicaid Services v Outpatient and Ambulatory Surgery CAHPS Survey Protocols and Guidelines Manual
OUTPATIENT AND AMBULATORY SURGERY CAHPS SURVEY PROTOCOLS AND GUIDELINES MANUAL
TABLE OF CONTENTS
Communications and Technical Support for the Outpatient and Ambulatory
Surgery CAHPS Survey i
List of Abbreviations and Acronyms Outpatient and Ambulatory Surgery
CAHPS Survey Protocols and Guidelines Manual iii
I. Overview of the Contents of the Protocol and Guidelines Manual 1 Overview 1
Section-by-Section Contents of the Outpatient and Ambulatory Surgery CAHPS
Survey Protocols and Guidelines Manual 1
II. Introduction and Background 5 Overview of CAHPS Survey 5
Development of the OAS CAHPS Survey 6 Office of Management and Budget and Public Comment Process 7 OAS CAHPS Survey Instrument 7
OAS CAHPS Survey Data Collection and Public Reporting 7 Sources of Information About the OAS CAHPS Survey 8
III. Survey Participation Requirements 11
Overview 11 Roles and Responsibilities 11 Responsibilities of Both HOPDs/ASCs and Survey Vendors 17
Vendor Business Requirements 19
IV. Sampling Procedures 27
Overview 27 Step 1: Obtain a Monthly Patient Information File from Each Client HOPD or ASC
Under the Same CCN 28 Step 2: Examine the Monthly Patient Information File for Completeness and
Possible Duplication 35
Step 3: Identify Eligible Patients and Construct a Sampling Frame 36 Step 4: Determine the Sampling Method Most Appropriate for the OAS CAHPS
Survey for This CCN 37
Step 5: Determine the Sample Size and Sampling Rate, and Select the Sample 39 Step 6: Verify or Update Contact Information For Sampled Patients 49 Step 7: Assign Unique Sample Identification Numbers 50 Step 8: Finalize the Monthly Sample File and Initiate Data Collection Activities 50
Sampling Issues and Errors 51
V. Mail-Only Administration Procedures 55

OUTPATIENT AND AMBULATORY SURGERY CAHPS SURVEY PROTOCOLS AND GUIDELINES MANUAL
TABLE OF CONTENTS
vi Centers for Medicare & Medicaid Services Outpatient and Ambulatory Surgery CAHPS Survey Protocols and Guidelines Manual
Overview 55 Data Collection Schedule 55 Questionnaires, Letters, and Envelopes 56
Mailing Requirements and Recommendations 61 Data Receipt, Data Entry, and Optical Scanning Requirements 62 Staff Training 65 Quality Control Guidelines for Mail-only Survey 65
VI. Telephone-Only Administration Procedures 67
Overview 67
Data Collection Schedule 67 Telephone Interview Development Process 68
Telephone Interviewing Requirements 70 Telephone Interviewer Training 74
Telephone Data Processing Procedures 74 Telephone-Only Quality Control Guidelines 75
VII. Mail with Telephone Follow-Up (Mixed-Mode) Survey Administration
Procedures 77 Overview 77
Data Collection Schedule 77 Questionnaires, Letters, and Envelopes 79
Data Receipt, Data Entry, and Optical Scanning Requirements 84 Staff Training 86
Telephone Interview Development Process 87 Telephone Interviewing Requirements and Recommendations 89 Interviewer Training 93
Telephone Data Processing Procedures 94 Mixed-Mode Quality Control Guidelines 94
VIII. Confidentiality and Data Security 97 Overview 97 Safeguarding Patient Data 97 Confidentiality Agreements 100
Physical and Electronic Data Security 100
Communicating With Sample Members About Confidentiality and Security 101
IX. Data Processing and Coding 103 Overview 103
Sample Identification Numbers 103 Data Processing Decision Rules and Coding Guidelines 104 Survey Disposition Codes 108
Definition of a Completed Survey or Survey Completion Criteria 108

OUTPATIENT AND AMBULATORY SURGERY CAHPS SURVEY PROTOCOLS AND GUIDELINES MANUAL
TABLE OF CONTENTS
Centers for Medicare & Medicaid Services vii Outpatient and Ambulatory Surgery CAHPS Survey Protocols and Guidelines Manual
Handling Blank Questionnaires 113 Quality Control Measures 113 Computing the Response Rate 116
X. The OAS CAHPS Survey Web Portal 118
Overview 118
The OAS CAHPS Web Portal 118 System and Security Requirements for the OAS CAHPS Web Portal 133
XI. File Preparation and Data Submission 138
Overview 138
Data File Preparation 138 Step 1: Format and Clean Survey Data Following the XML File Specifications 138
XML Data File Specifications 139 Step 2: Data File Submission 143
Step 3: Review and Follow -Up on Data Upload Reports 145 Quarterly Data Submission Deadlines 145 Potential Situations When Vendors Will Not Submit Data 146
Data Submission Quality Control 147
XII. Web Portal Reports 150
Overview 150
Reports for Survey Vendors 150
Reports for Ambulatory Surgery Centers and Hospital Outpatient Departments 153
XIII. Oversight Activities 156
Overview 156 Quality Assurance Plan 156 Data Review 157 Communication Between Survey Vendors and the Coordination Team 158
Requirement for Clients 158 Site Visits to Survey Vendors 158 Corrective Action Plans 160
XIV. Public Reporting 162
Overview 162 Measures That Are Reported 162 Adjustment and Reporting of Results 163 Facility Preview Reports 164 Public Reporting Periods 164
XV. Exceptions Request Process and Discrepancy Notification Report 166
Overview 166

OUTPATIENT AND AMBULATORY SURGERY CAHPS SURVEY PROTOCOLS AND GUIDELINES MANUAL
TABLE OF CONTENTS
viii Centers for Medicare & Medicaid Services Outpatient and Ambulatory Surgery CAHPS Survey Protocols and Guidelines Manual
Exceptions Request Process 166 Review Process 166 Discrepancy Notification Report 167
Discrepancy Report Review Process 168

OUTPATIENT AND AMBULATORY SURGERY CAHPS SURVEY PROTOCOLS AND GUIDELINES MANUAL
TABLE OF CONTENTS
Centers for Medicare & Medicaid Services ix Outpatient and Ambulatory Surgery CAHPS Survey Protocols and Guidelines Manual
Appendix A: Vendor Application Form
Appendix B: English: Mail Survey Cover Letters, Mail Questionnaires,
Instructions for Scannable Mail Questionnaire, Telephone
Interview Script
Appendix C: Spanish: Mail Survey Cover Letters, Mail Questionnaires,
Instructions for Scannable Mail Questionnaire, Telephone
Interview Script
Appendix D: Chinese: Mail Survey Cover Letters, Mail Questionnaires,
Instructions for Scannable Mail Questionnaire
Appendix E: Additional Language Cover Letters and Questionnaire
(forthcoming)
Appendix F: Consent to Share Identifying Information Question
Appendix G: OMB Paperwork Reduction Act Language
Appendix H: Frequently Asked Questions for Telephone Interviewers
(English)
Appendix I: General Guidelines for Telephone Interviewers
Appendix J: Frequently Asked Questions for Telephone Interviews
(Spanish)
Appendix K: XML Data File Layout for Standard Header Record
Appendix L: XML Data File Layout for Disproportionate Stratified
Random Sampling (DSRS) Header Record
Appendix M: XML Data File Layout for Zero Sampled File
Appendix N: Instructions for Preparing a Survey Vendor Quality
Assurance Plan
Appendix O: Exceptions Request Form
Appendix P: Discrepancy Notification Report
OUTPATIENT AND AMBULATORY SURGERY CAHPS SURVEY PROTOCOLS AND GUIDELINES MANUAL
TABLE OF CONTENTS
x Centers for Medicare & Medicaid Services Outpatient and Ambulatory Surgery CAHPS Survey Protocols and Guidelines Manual
Exhibits
9.1 Steps for Determining Whether a Questionnaire Meets Completeness Criteria 109
9.2 How Response Rates Are Calculated 117
10.1 OAS CAHPS Web Portal 119
10.2 OAS CAHPS Home Page (Public Web portal) 120
10.3 Announcements Page on the OAS CAHPS Web Portal 122
10.4 Recent Announcements on the OAS CAHPS Web Portal Home Page 122
10.5 Facility User Registration Form 124
10.6 CCN Registration Form 125
10.7 Manage User Console 126
10.8 Vendor Registration Form Link 129
10.9 Facility Dashboard 132
10.10 Vendor Dashboard 132
11.1 Link to Data Submission Tool 144
11.2 Uploading Multiple Files 145

OUTPATIENT AND AMBULATORY SURGERY CAHPS SURVEY PROTOCOLS AND GUIDELINES MANUAL
TABLE OF CONTENTS
Centers for Medicare & Medicaid Services xi Outpatient and Ambulatory Surgery CAHPS Survey Protocols and Guidelines Manual
Tables
4.1 Information Needed From ASCs/HOPDs for Patient Served During Sample Month 31
4.2 Response Rates Obtained by Mode Anticipated for OAS CAHPS 40
5.1 Mail-Only Administration Schedule and Protocol 55
6.1 Prescribed Order of Activities and Timing for an All-Telephone OAS CAHPS
Survey 67
7.1 Tasks and Schedule of Activities for Mail with Telephone Follow-Up 77
9.1 OAS CAHPS Survey Disposition Codes 109
14.1 Crosswalk of Composite Measures and Global Ratings 163
14.2 Data Submission Deadlines linked to the (Anticipated) Public Reporting Period 164


Centers for Medicare & Medicaid Services 1 Outpatient and Ambulatory Surgery CAHPS Survey Protocols and Guidelines Manual
I. OVERVIEW OF THE CONTENTS OF THE PROTOCOL AND GUIDELINES MANUAL
Overview
The Outpatient and Ambulatory Surgery CAHPS Survey Protocols and Guidelines Manual has
been developed by the Centers for Medicare & Medicaid Services (CMS) to provide guidance
and standard protocols for conducting the Outpatient and Ambulatory Surgery Consumer
Assessment of Healthcare Providers and Systems (CAHPS®) Survey, hereafter referred to as the
“OAS CAHPS Survey”. The OAS CAHPS Survey measures the experiences of patients who
receive outpatient or ambulatory services from hospital outpatient departments (HOPDs) and
ambulatory surgery centers (ASCs). This section provides survey vendors, HOPDs, and ASCs
with a top-level view of the contents of this manual. Each section is briefly described below,
along with an explanation of the contents of the appendices.
Section-by-Section Contents of the Outpatient and Ambulatory Surgery CAHPS Survey Protocols and Guidelines Manual
II. Introduction and Background
The Introduction and Background chapter provides information about the purpose of the OAS
CAHPS Survey and history of the OAS CAHPS Survey initiative, including a discussion of the
instrument development and pilot test activities. It also includes information about the public
reporting timeline and sources for more information about the OAS CAHPS Survey.
III. OAS CAHPS Survey Participation Requirements
This chapter describes the roles and responsibilities of CMS, the OAS CAHPS Survey
Coordination Team, HOPDs and ASCs, and approved survey vendors during the OAS CAHPS
Survey mode experiment. It also includes information on the vendor rules of participation and
business requirements for becoming an approved survey vendor. Information about how to
communicate with and obtain technical assistance from the OAS CAHPS Survey Coordination
Team is also provided in the OAS CAHPS Survey Participation Requirements chapter.
IV. Sampling Procedures
This chapter describes the sampling process for the OAS CAHPS Survey. It includes
requirements for developing the sample frame of eligible patients from HOPDs and ASCs, and
the method to be followed in selecting the sample of patients.

I. Overview of the Contents of the Protocol and Guidelines Manual December 2015
2 Centers for Medicare & Medicaid Services Outpatient and Ambulatory Surgery CAHPS Survey Protocols and Guidelines Manual
V. Mail-Only Administration Procedures
The Mail-Only Administration Procedures chapter contains the protocols and guidelines for
administering the OAS CAHPS Survey as a mail-only survey. The data collection schedule,
production and mailing requirements, data receipt and processing requirements, and quality
control guidelines associated with conducting a mail-only mode survey are covered in detail.
VI. Telephone-Only Administration Procedures
Procedures and guidelines for administering the OAS CAHPS Survey as a telephone-only survey
are provided in the Telephone-Only Administration Procedures chapter. The data collection
schedule, the electronic data collection and tracking system, telephone interviewing
requirements, and quality control guidelines associated with conducting a telephone-only mode
survey are covered in detail.
VII. Mixed-Mode Administration Procedures
The Mixed-Mode Administration Procedures chapter contains the protocols and guidelines for
administering the OAS CAHPS Survey as a mixed-mode survey—that is, mail survey with
telephone follow-up of nonrespondents. The data collection schedule, production and mailing
requirements, electronic data collection and tracking system, telephone interviewing
requirements, data receipt and processing requirements, and quality control for conducting a
mixed-mode survey are covered in detail.
VIII. Confidentiality and Data Security
The requirements and guidelines for protecting the identity of sample members, confidentiality
of respondent data, ensuring data security, instructions for handling confidential data, and the
importance of confidentiality agreements are covered in this chapter. The importance of
establishing and maintaining physical and electronic data security, and explaining these measures
to sample members, is also covered.
IX. Data Processing and Coding
Data processing procedures, including the assignment of a unique sample identification number
to each sampled case, decision rules for assigning survey disposition codes, quality control
measures, and the definition of a completed survey are described in the Data Processing and
Coding chapter.
X. OAS CAHPS Survey Website
The OAS CAHPS Survey website chapter provides detailed information about the OAS CAHPS
Survey website and the data submission process, including screen shots of the data submission
tool and instructions for data submission.

December 2015 I. Overview of the Contents of the Protocol and Guidelines Manual
Centers for Medicare & Medicaid Services 3 Outpatient and Ambulatory Surgery CAHPS Survey Protocols and Guidelines Manual
XI. File Preparation and Submission
The File Preparation and Submission chapter provides an overview of the purpose and functions
of the OAS CAHPS Survey website and a summary description of how to prepare and submit
data files following OAS CAHPS Survey data file preparation and submission guidelines.
XII. OAS CAHPS Survey Website Reports
The OAS CAHPS Survey Website Reports chapter provides an overview of the reports available
to vendors and HOPDs and ASCs through the OAS CAHPS Survey website. The reports are
described briefly, with an emphasis on the intended audience for each report and how the reports
should be used.
XIII. Oversight Activities
The Oversight Activities chapter provides information about the quality assurance activities that
the OAS CAHPS Survey Coordination Team and CMS will undertake to ensure the successful
administration of the OAS CAHPS Survey by survey vendors. The chapter begins with a
discussion of the vendor Quality Assurance Plan and reviews the various activities that the
Coordination Team will conduct to ensure compliance with OAS CAHPS Survey protocols and
guidelines.
XIV. Public Reporting
The Public Reporting chapter presents an overview of the public reporting of OAS CAHPS
Survey results, including the composite measures and global items that are publicly reported,
adjustments by mode (if applicable), preview reports, and public reporting periods.
XV. Exceptions Request Process and Discrepancy Notification Report
The Exceptions Request Process and Discrepancy Notification Report chapter describes the
process to be used to request an exception to the OAS CAHPS Survey protocols, including
guidelines for submitting an Exceptions Request Form. This section also covers the process for
alerting the OAS CAHPS Survey Coordination Team of an unplanned discrepancy in data
collection procedures.
Appendices
The appendices contain copies of the Vendor Application Form, questionnaires, cover letters and
telephone interview script (in English and other languages), the optional Consent to Share
Identifying Information Question, Office of Management and Budget approval statement,
frequently asked questions for telephone interviewers, general guidelines for telephone
interviewers, XML data file layout for standard header record, XML data file layout for
disproportionate stratified random sampling, XML data file layout for zero sampled patient file,

I. Overview of the Contents of the Protocol and Guidelines Manual December 2015
4 Centers for Medicare & Medicaid Services Outpatient and Ambulatory Surgery CAHPS Survey Protocols and Guidelines Manual
Quality Assurance Plan instructions, Exception Request Form, and Discrepancy Notification
Report.
The Outpatient and Ambulatory Surgery CAHPS Survey Protocols and
Guidelines Manual
An electronic file of the Outpatient and Ambulatory Surgery CAHPS Survey Protocols and
Guidelines Manual and its appendices are available on the project website at
https://oascahps.org/ in both MS Word and .pdf formats. To conserve paper, the OAS CAHPS
Survey Coordination Team is printing a limited number of hardcopy versions of this manual.
Organizations can request a hardcopy manual by sending an e-mail to the OAS CAHPS Survey
Coordination Team at [email protected].

Centers for Medicare & Medicaid Services 5 Outpatient and Ambulatory Surgery CAHPS Survey Protocols and Guidelines Manual
II. INTRODUCTION AND BACKGROUND
Overview of CAHPS Survey
The Centers for Medicare & Medicaid Services (CMS) has partnered with the Agency for
Healthcare Research and Quality (AHRQ), an agency within the United States Department of
Health and Human Services, to develop surveys measuring patient perspectives of care.
Beginning in 1995 as part of the Consumer Assessment of Healthcare Providers and Systems
(CAHPS) initiative, AHRQ and its CAHPS grantees began to develop surveys focusing on
patient experiences with their healthcare. Since 1995, the initiative has expanded to cover a
range of surveys of health care services at multiple levels of the delivery system, including
patients receiving care from both ambulatory and institutional settings. The intent of the CAHPS
initiative is to provide a standardized survey instrument and data collection methodology for
measuring patients’ perspectives on patient care. CAHPS is meant to complement the data that
providers collect to support improvements in internal customer services and quality-related
activities.
The Outpatient and Ambulatory Surgery CAHPS (OAS CAHPS) Quality
Initiative
In November 2002, the Quality Initiative was launched to ensure quality health care for all
Americans through accountability and public disclosure. The initiative aims to (a) empower
consumers with quality of care information to help them make more informed decisions about
their health care, and (b) stimulate and support providers and clinicians to improve the quality of
health care.1 The Quality Initiative was launched nationally in November 2002 for nursing
homes (the Nursing Home Quality Initiative), and expanded in 2003 to the nation’s home health
care facilities (the Home Health Quality Initiative) and hospitals (the Hospital Quality Initiative).
This Quality Initiative is continuing for ambulatory surgery centers (ASCs) and hospital
outpatient departments (HOPDs), through the national implementation of OAS CAHPS.2
1 Centers for Medicare & Medicaid Services. http://www.cms.gov/Medicare/Quality-Initiatives-Patient-
Assessment-Instruments/QualityInitiativesGenInfo/index.html. Also http://www.cms.gov/Research-Statistics-Data-
and-Systems/Research/CAHPS/index.html 2 http://cms.hhs.gov/Research-Statistics-Data-and-Systems/Research/CAHPS/OAS-CAHPS.html

II. Introduction and Background December 2015
6 Centers for Medicare & Medicaid Services Outpatient and Ambulatory Surgery CAHPS Survey Protocols and Guidelines Manual
Definition of HOPD and ASC
An HOPD is a unit of a hospital whose primary focus is to perform outpatient surgeries and
outpatient procedures. CMS specifically defines eligible HOPDs as units within the hospital
which bill under the OPPS (Outpatient Prospective Payment System). Additionally, outpatient-
focused units that are within critical access hospitals (CAHs) are also eligible as HOPDs even
though CAHs do not bill under OPPS. There can be more than one HOPD in a hospital. Not
every hospital has an HOPD.
An ASC is a freestanding medical facility that performs outpatient surgeries and procedures.
CMS specifically defines eligible ASCs as distinct entities that operate exclusively for the
purposes of furnishing outpatient surgical services to patients. The ASC must have an agreement
with CMS and meet the general conditions and requirements in accordance with 42 CFR 416
subpart B. The ASC may also have physician offices on site, but it does not have any overnight
patients. Some ASCs have more than one location, typically in a geographic region.
Development of the OAS CAHPS Survey
The OAS CAHPS Survey seeks to provide information about patients’ perception of the care
they receive from Medicare-certified HOPDs and ASCs. The OAS CAHPS development began
in 2012. The survey development process followed the principles and guidelines outlined by
AHRQ and its CAHPS® Consortium in developing a patient experience of care survey.
Development included reviewing surveys submitted as a result of a public call for measures,
reviewing existing literature, conducting focus groups with patients who had recent outpatient
surgery, conducting cognitive interviews with patients to test their understanding and ability to
answer the questions, obtaining stakeholder input on the draft survey and other issues that may
affect implementation, and conducting a field test. The goal of the survey development contract
was to identify and include dimensions of care that patients and other consumers want or need to
inform their choice of an outpatient surgery department/center.
A field test was conducted in the summer of 2014 with 36 facilities (18 HOPDs and 18 ASCs) to
test the reliability and validity of the survey items and implementation procedures. Based on the
field test findings, the survey instrument was revised and finalized.
After the survey instrument was finalized, a mode experiment was conducted in 2015. The
objective of the mode experiment was to test the effect on survey responses of using three data
collection modes: mail-only, telephone-only, and mixed mode (mail with telephone follow-up of
nonrespondents). CMS also used data from the mode experiment to determine whether and to
what extent characteristics of patients participating statistically influence OAS CAHPS survey
results. Statistical models were developed to adjust or control for these patient characteristics
before the survey results were publicly reported. Data from the mode experiment were also

December 2015 II. Introduction and Background
Centers for Medicare & Medicaid Services 7 Outpatient and Ambulatory Surgery CAHPS Survey Protocols and Guidelines Manual
analyzed to detect potential nonresponse bias; the results of these analyses determined whether
applicable nonresponse statistical adjustments must be made on the OAS CAHPS Survey data.
Office of Management and Budget and Public Comment Process
CMS received approval of the OAS CAHPS Survey from the United States Office of
Management and Budget with control number 0938-1240.
OAS CAHPS Survey Instrument
The OAS CAHPS Survey instrument contains 37 items that cover topics such as access to care,
communications, and experience of the facility and interactions with facility staff. There are two
global items: one asks the patient to rate the care provided by the HOPD or ASC, and the second
asks the patient about his or her willingness to recommend the HOPD or ASC to family and
friends. The survey also contains items that ask for self-reported health status and basic
demographic information (race/ethnicity, education attainment level, language spoken in the
home, etc.).
The OAS CAHPS Survey is currently available in English, Spanish, and Chinese. A version is
provided for both mail and telephone survey administration modes. HOPDs and ASCs and their
survey vendors will not be permitted to translate the OAS CAHPS Survey into any other
languages. CMS will provide additional translations over time based on the language needs of
patients. Please check the OAS CAHPS Survey website, https://oascahps.org/, for
announcements about additional translations.
OAS CAHPS Survey Data Collection and Public Reporting
Starting in 2016, Medicare-certified HOPDs and ASCs will be invited to submit data on a
voluntary basis for national implementation of the OAS CAHPS Survey. Interested facilities
contract with survey vendors to conduct the Survey on their behalf. Survey vendors interested in
administering the OAS CAHPS Survey must complete and submit an application, attend OAS
CAHPS Survey training sessions, complete a Training Certification Form, and participate in
periodic update trainings sponsored by CMS. Survey vendors cannot collect and submit data to
CMS until they receive approval to conduct the survey.
Following each quarter of survey data collection, vendors submit the survey data they collected
using the data submission tool function on the OAS CAHPS Survey website
(https://oascahps.org/). The data submitted are reviewed, cleaned, scored, and adjusted by the
OAS CAHPS Survey Coordination Team. Survey results are compiled for each HOPD and
ASC. Public reporting includes four rolling quarters of data; the publicly available results are
published on CMS' website. Before the data are publicly reported a “preview” report containing
the individual results is made available to each facility for review through the OAS CAHPS
Survey website.

II. Introduction and Background December 2015
8 Centers for Medicare & Medicaid Services Outpatient and Ambulatory Surgery CAHPS Survey Protocols and Guidelines Manual
Sources of Information About the OAS CAHPS Survey
More information about the OAS CAHPS Survey and ambulatory and outpatient surgical care is
available at the two websites described below.
The OAS CAHPS Survey Website (https://oascahps.org/)
The OAS CAHPS Survey Coordination Team maintains a website, which is available at
https://oascahps.org/ and hereafter in this chapter referred to as the OAS CAHPS website or
simply as the “website.” This website provides general information about the OAS CAHPS
Survey, contains the protocols and materials needed for survey implementation, and is one of the
main vehicles for communicating information about the survey to HOPDs, ASCs, and survey
vendors. The website has both public and secure pages.
The public access pages contain the following:
• general information about the OAS CAHPS Survey;
• announcements about updates or changes in the survey protocols or materials and
participation requirements;
• requirements for becoming an OAS CAHPS Survey vendor;
• data collection materials, protocols, and guidelines for administration of the OAS CAHPS
Survey;
• a list of approved OAS CAHPS Survey vendors;
• quality assurance plan requirements;
• oversight activities;
• data submission requirements; and
• information about how to obtain technical assistance.
The Outpatient and Ambulatory Surgery CAHPS Survey Protocols and Guidelines Manual is
updated annually to reflect changes to participation requirements and changes in survey
protocols, materials, and procedures. However, CMS and the Coordination Team use the OAS
CAHPS website to disseminate important interim updates and news about the OAS CAHPS
Survey, including information related to participation requirements, updates and changes to
survey protocols or survey materials, information about upcoming events (e.g., data submission
deadlines, vendor training sessions), and public reporting. Announcements posted on the OAS
CAHPS Survey website may clarify or supersede existing protocols.

December 2015 II. Introduction and Background
Centers for Medicare & Medicaid Services 9 Outpatient and Ambulatory Surgery CAHPS Survey Protocols and Guidelines Manual
Therefore, it is critically important that survey vendors, HOPDs, and ASCs check the OAS
CAHPS Survey website frequently for updates. To view announcements, go to the website at
https://oascahps.org/ and click on the “Announcement” link. The announcements are listed in
chronological order with the most recent announcement listed first.
The secure or restricted-access sections of the OAS CAHPS Survey website are accessible only
to OAS CAHPS Survey vendors and HOPDs and ASCs that have registered for and been
provided credentials to access the links on the private sections of the website. The links
provided within this section of the website will enable HOPDs and ASCs to:
• authorize a survey vendor to submit OAS CAHPS Survey data on their behalf, switch
vendors, or view the facility’s authorization history;
• view data submission reports for data submitted by their respective survey vendors; and
• “preview” their OAS CAHPS Survey results before the results are publicly reported.
Additional secured links on the OAS CAHPS Survey website are accessible to survey vendors
who have been given access credentials. These private secured links allow survey vendors to:
• view the current list of HOPDs and ASCs that have authorized the vendor to submit data on
their behalf; and
• access the OAS CAHPS Survey data submission tool and reports containing information
about submitted data.
More detailed information about the OAS CAHPS Survey website is included in Chapter X of
this manual.
The Medicare Website (http://www.medicare.gov)
This website is maintained by CMS and contains information on the services Medicare provides.
The Medicare website provides information to the public on various quality measures. Viewers
can obtain comparative information about HOPDs and ASCs by state, ZIP code, and county.
OAS CAHPS Survey results are based on survey response data from the four quarters for which
OAS CAHPS Survey data are available, and are “refreshed” each calendar year quarter.

II. Introduction and Background December 2015
10 Centers for Medicare & Medicaid Services Outpatient and Ambulatory Surgery CAHPS Survey Protocols and Guidelines Manual
This page intentionally left blank.

Centers for Medicare & Medicaid Services 11 Outpatient and Ambulatory Surgery CAHPS Survey Protocols and Guidelines Manual
III. SURVEY PARTICIPATION REQUIREMENTS
Overview
This chapter describes participation requirements for the Outpatient and Ambulatory Surgery
Patient Experience of Care Survey (OAS CAHPS), including the roles and responsibilities of the
Centers for Medicare & Medicaid Services (CMS) and its OAS CAHPS Survey Coordination
Team, hospital outpatient departments (HOPDs) and ambulatory surgery centers (ASCs), and
survey vendors that administer the OAS CAHPS Survey for HOPDs and ASCs. This chapter
also discusses the rules of participation and outlines the business requirements that survey
vendors must meet to be approved to administer the OAS CAHPS Survey. Information about
obtaining technical assistance from the Coordination Team is also provided in this chapter.
Roles and Responsibilities
CMS is responsible for ensuring that the OAS CAHPS Survey is administered using
standardized survey protocols and data collection and processing methods. CMS works very
closely with its OAS CAHPS Survey Coordination Team to provide training, technical
assistance, and oversight to approved survey vendors. Technical assistance is also provided to
HOPDs and ASCs because they are responsible for contracting with an approved survey vendor
to conduct the OAS CAHPS Survey on their behalf and for providing a patient information file
containing data about patients served during the sample month to their survey vendor each
month. Survey vendors are responsible for conducting the OAS CAHPS Survey on behalf of
their client HOPDs and ASCs following the standard protocols and guidelines described in this
manual.
The roles and responsibilities of each of these participating organizations are described below.
CMS and the OAS CAHPS Survey Coordination Team Responsibilities
CMS and the OAS CAHPS Survey Coordination Team are responsible for the following
activities on the OAS CAHPS Survey:
• disseminate information about OAS CAHPS Survey administration;
• train survey vendors on OAS CAHPS Survey protocols and requirements;
• monitor data integrity of OAS CAHPS Survey administration to ensure the quality and
comparability of the data;

III. Survey Participation Requirements December 2015
12 Centers for Medicare & Medicaid Services Outpatient and Ambulatory Surgery CAHPS Survey Protocols and Guidelines Manual
• provide technical assistance to HOPDs and ASCs and approved OAS CAHPS Survey
vendors via a toll-free telephone number, e-mails, and the OAS CAHPS website at
https://oascahps.org/;
• conduct oversight and quality assurance of survey vendors;
• receive and conduct final processing of OAS CAHPS Survey data submitted by all approved
survey vendors;
• calculate and adjust OAS CAHPS Survey data for mode and patient-mix effects prior to
publicly reporting survey results; and
• generate preview reports containing OAS CAHPS Survey results for participating HOPDs
and ASCs to review prior to public reporting.
Hospital Outpatient Departments’ and Ambulatory Surgery Centers’
Responsibilities
Participating HOPDs or ASCs must:
• Contract with an approved OAS CAHPS survey vendor to conduct their survey on a monthly
basis.
• Authorize the contracted survey vendor to collect and submit OAS CAHPS Survey data to
the OAS CAHPS Survey Data Center on the facility’s behalf.
• Work with their approved vendor to determine a date each month by which the vendor will
need the monthly patient information file allowing adequate time for vendor sampling and
fielding the survey by the 21st of the month.
• By the agreed-upon date, compile and deliver to the survey vendor a complete and accurate
list of patients (i.e., the monthly patient information file) and information that will enable the
vendor to administer the survey.
• Use a secure method to transmit monthly patient information files to the survey vendor,
ensuring that data are encrypted prior to sending to the vendor.
• Work with their approved vendor to determine a date each month or quarter by which the
vendor will submit data to the OAS Data Center.
• Review data submission reports to ensure that their survey vendor has submitted data to the
OAS CAHPS Data Center on time and without data problems (allow ample time for this
prior to the quarterly data submission deadlines because data cannot be corrected after the
deadline has passed).

December 2015 III. Survey Participation Requirements
Centers for Medicare & Medicaid Services 13 Outpatient and Ambulatory Surgery CAHPS Survey Protocols and Guidelines Manual
• Review OAS CAHPS Survey results prior to public reporting.
• Avoid influencing patients in any way about how to answer the OAS CAHPS Survey. For
example, HOPDs and ASCs may not hand out any information to patients about how to
answer the survey. (Please refer to the section below titled Communications With Patients
About the OAS CAHPS Survey.)
Communications With Patients About the OAS CAHPS Survey
It is important to avoid influencing patient responses to the OAS CAHPS Survey. Any
information or communication about the survey from HOPDs and ASCs may introduce bias to
the survey. It is acceptable for HOPDs and ASCs to inform patients that they may be asked to
respond to a patient experience survey. It is not acceptable, however, for HOPDs or ASCs to do
any of the following:
• Send or provide information to patients in advance alerting them about the survey.
• Provide a copy of the OAS CAHPS Survey questionnaire or cover letters to the patients.
• Include words or phrases verbatim from the OAS CAHPS Survey in marketing or
promotional materials.
• Attempt to influence their patients’ answers to the OAS CAHPS Survey questions.
• Tell the patients the facility hopes or expects their patients will give them the best or highest
rating or to respond in a certain way to the survey questions.
• Offer incentives of any kind to the patients for participating (or not) in the survey.
• Help the patient answer the survey questions, even if the patient asks for the provider’s help.
• Ask patients why they gave a certain response or rating to any of the OAS CAHPS Survey
question.
• Include any messages or materials promoting the HOPD or ASC or the services it provides in
survey materials, including mail survey cover letters, questionnaires, and telephone interview
scripts.
HOPDs and ASCs should never ask their patients if they would like to be included in the survey.
All patients selected to participate in the OAS CAHPS Survey must be able to decide on their
own whether they wish to participate and will be provided an opportunity to do so as part of the
survey process.

III. Survey Participation Requirements December 2015
14 Centers for Medicare & Medicaid Services Outpatient and Ambulatory Surgery CAHPS Survey Protocols and Guidelines Manual
Survey Vendor Responsibilities
The list below provides a synopsis of the responsibilities of survey vendors on the OAS CAHPS
Survey.
• Complete the Vendor Application, which will be available on the OAS CAHPS Survey
website approximately 3 months prior to the next scheduled Introduction to the OAS CAHPS
Survey Webinar training session.
• Participate in and successfully complete the Introduction to the OAS CAHPS Survey
Webinar training session and in all update training sessions.
• The survey vendor’s designated CAHPS project manager must also complete a Training
Certification Form after participating in the Introduction to the OAS CAHPS Survey
Webinar training session.
• Ensure that all survey vendor staff who work on the OAS CAHPS Survey are trained and
follow the standard OAS CAHPS Survey protocols and guidelines.
• Report any deviations from the protocols and guidelines to the OAS CAHPS Survey
Coordination Team within 24 hours after the discrepancy has been discovered, either through
a Discrepancy Notification Report (see Chapter XV) or other e-mail or telephone contact
with the Coordination Team.
• Follow the participation requirements listed in Section VI of the Vendor Application and also
repeated in the following chapters in this manual.
• Work with appropriate HOPD/ASC staff to create monthly patient information files,
including data elements needed and file format specifications, and decide on a date each
month by which the HOPD or ASC must provide each monthly patient information file.
• Receive and perform checks of the monthly patient information files provided by HOPDs
and ASCs to ensure that they include the entire eligible population and all required data
elements.
• Sample patients, following the sampling protocols described in this manual (see Chapter IV).
• Administer the OAS CAHPS Survey in accordance with the protocols specified in
Chapters V–VII of this manual and oversee the quality of work performed by staff and any
subcontractors, if applicable.
• Verify that each client HOPD or ASC has authorized the vendor to submit data on the
facility’s behalf.
December 2015 III. Survey Participation Requirements
Centers for Medicare & Medicaid Services 15 Outpatient and Ambulatory Surgery CAHPS Survey Protocols and Guidelines Manual
• Prepare and submit data files to the OAS CAHPS Survey Data Center following the
guidelines specified in Chapters IX and X of this manual.
• Review all data submission reports for client facilities to ensure that data have been
successfully uploaded and received.
Survey Vendor Participation Requirements
Survey organizations interested in becoming an approved survey vendor for the OAS CAHPS
Survey must agree to the following requirements of participation, as specified in Section VI of
the Vendor Application Form (Appendix A) and noted below.
• Participate in both the Introduction to the OAS CAHPS Survey Training Session and in any
subsequent update trainings. The vendor’s staff member designated as the Project Director
for the OAS CAHPS Survey must attend these trainings; we strongly advise that the vendor’s
sampling and data managers also attend. All training sessions will be conducted via Webinar
and require that the survey vendor register in advance for the session and attend the session.
The survey vendor’s designated OAS CAHPS Project Manager must complete a post-
training certification exercise, also referred to as a Training Certification Form, after
attending the Introduction to the OAS CAHPS Survey training session. The Introduction to
the OAS CAHPS Survey training session will be provided in two 4-hour sessions. Each
Update training session, when offered, will usually consist of one 2- to 3-hour session.
• Review the Outpatient and Ambulatory Surgery CAHPS Protocols and Guidelines Manual
and follow the protocols and procedures described in this manual during survey
administration. This manual is the main resource for survey vendors to use in implementing
all stages of the OAS CAHPS Survey—from sampling and data collection to file
development and submission. It is expected that vendors will refer to this manual frequently
and adhere to all protocols contained within it. Protocol and policy updates will be posted on
the OAS CAHPS Survey website, so vendors are expected to check the website frequently
for such notifications.
• Communicate in a timely manner (within 24 hours when possible) with the OAS CAHPS
Survey Coordination Team any instances when the survey is not following the protocols and
guidelines in this manual. As explained in Chapter XV, there are two forms which are used
in this regard: the Exception Request (regarding a planned deviation) and the Discrepancy
Notification (regarding a discrepancy that has already occurred). When these two forms are
not appropriate for the instance, contact the OAS CAHPS Survey Coordination team through
the Contact Us link on the OAS CAHPS Web Portal (Chapter X).
III. Survey Participation Requirements December 2015
16 Centers for Medicare & Medicaid Services Outpatient and Ambulatory Surgery CAHPS Survey Protocols and Guidelines Manual
• Check the OAS CAHPS website frequently to review announcements and protocol updates,
and review and respond as appropriate to e-mails from the OAS CAHPS Survey
Coordination Team (e-mails will be from [email protected]).
• Develop and submit a Quality Assurance Plan (QAP), following guidelines described in
Chapter XIII of this manual and the QAP instructions provided in Appendix N. Survey
vendors must complete and submit a QAP within 6 weeks after the vendor’s first quarterly
OAS CAHPS Survey data submission. The QAP must be updated annually or as needed
whenever changes are made to key personnel, survey modes being administered, or
protocols. The QAP must include the following elements:
• organizational background and staff experience;
◦ identifying and recruiting HOPDs and ASCs
◦ work plan;
◦ sampling protocols and quality assurance procedures;
◦ survey administration protocols and quality assurance procedures;
◦ data security, confidentiality, and privacy protocols; and
◦ copies of the survey instrument (questionnaire or computer-assisted telephone interview
[CATI] script) and cover letters.
• Participate and cooperate in all oversight activities conducted by the OAS CAHPS Survey
Coordination Team, including but not limited to conference calls and site visits, as deemed
necessary. Additionally, the Coordination Team may request teleconference calls with
vendors to review sampling protocols, file submissions, or any other aspect of the data
collection process. Documentation and requirements that vendors are expected to follow in
light of these oversight activities are described in the Vendor Application Form
(Appendix A) and in Chapter XIII of this manual.
• Acknowledgement that review of, and agreement with, these participation requirements is
necessary for participation and public reporting of results through the CMS website. As
noted on the Vendor Application, all survey vendors seeking approval to conduct the OAS
CAHPS Survey must review and agree to the participation requirements listed in Section VI
of the Vendor Application and described in the bullets above. Vendors that fail to adhere to
or comply with the participation requirements risk losing their status as an approved OAS
CAHPS Survey vendor.

December 2015 III. Survey Participation Requirements
Centers for Medicare & Medicaid Services 17 Outpatient and Ambulatory Surgery CAHPS Survey Protocols and Guidelines Manual
• To maintain their standing as an approved OAS CAHPS vendor, all vendors must update (as
needed) and resubmit their QAP annually. All vendors must also correct any issues
identified by the OAS CAHPS Survey Coordination Team, whether they are identified at a
site visit or during the course of data collection.
Responsibilities of Both HOPDs/ASCs and Survey Vendors
Administering the OAS CAHPS Survey in Conjunction With Other Surveys
Some HOPDs and ASCs may wish to conduct other patient surveys to support internal quality
improvement activities. A “survey,” for purposes of this project, is defined as a formal, patient
experience/satisfaction survey. A formal survey, regardless of the data collection mode
employed, is one in which the primary goal is to ask standardized questions of a sample of the
patient population. Contacting patients to assess their care at any time or calling a patient to
check on services received are both considered to be routine patient contacts, not surveys.
HOPDs and ASCs that are administering other outpatient care patient surveys must follow the
following guidelines.
With regard to sampling and ensuring that patients are not overburdened by multiple surveys:
• For each sample month, HOPDs and ASCs (working in conjunction with their survey
vendor) must select the OAS CAHPS Survey sample prior to selecting the samples for any
other HOPD or ASC survey.
• In the event that another CMS-sponsored effort is also conducting a survey of patients in the
ASC/HOPD that month, the facility must contact the OAS CAHPS Survey Coordination
Team to make arrangements for both surveys.
With regard to questionnaire content:
• In other surveys that an HOPD or ASC conducts, the facility can include questions that ask
for more in-depth information about OAS CAHPS issues, but should not repeat the OAS
CAHPS questions or include questions that are very similar.
• The following are some examples of the types of questions that should not be included in any
other surveys the facility conducts:
◦ “On a scale of 0 to 10, how would you rate the outpatient surgery care you received?”
(This question is the same as Q23 in the OAS CAHPS Survey Questionnaire.)
◦ “Would you recommend this facility to your family or friends?” and “Would you
recommend our services or call us in the future?” (These questions are similar to Q24 in
the OAS CAHPS Survey Questionnaire.)

III. Survey Participation Requirements December 2015
18 Centers for Medicare & Medicaid Services Outpatient and Ambulatory Surgery CAHPS Survey Protocols and Guidelines Manual
◦ “Was our staff friendly, professional, and courteous?” (This question is similar to Q7 in
the OAS CAHPS Survey Questionnaire.)
Adding Supplemental Questions to the OAS CAHPS Questionnaire
Survey vendors and their client HOPDs and ASCs may elect to add up to 15 questions to the
OAS CAHPS survey. These could be questions they develop themselves or use from an existing
survey.
• All supplemental questions must be placed after the core OAS CAHPS Survey questions
(Q1-Q24). Supplemental questions may be placed either before or after the OAS CAHPS
Survey “About You” questions. (Refer to the Questionnaire in Appendix B.)
• We strongly recommend that facilities/vendors avoid sensitive questions or lengthy
additions, because these will likely reduce expected response.
• Supplemental questions cannot ask patients why they gave a certain response or rating to any
of the OAS CAHPS survey questions.
• Supplemental questions do not need to be approved by or reported to CMS. However,
survey vendors should review the appropriateness of supplemental questions added to the
OAS CAHPS Survey and share any concerns they have directly with the HOPD or ASC or
the OAS CAHPS Survey Coordination Team.
• Survey vendors must not include responses to the supplemental questions on the data files
that will be submitted to the OAS CAHPS Survey Data Center.
• HOPDs and ASCs cannot add questions that repeat any of the survey items in the core OAS
CAHPS Survey verbatim, even if the response scale is different.
• Supplemental questions cannot be used with the intention of marketing or promoting services
provided by the HOPD or ASC or any other organization. An example of question for
marketing or promotion is: “Can you provide the names and contact information of any
friends or family members who are interested in learning about the services we provide?”
• Supplemental questions cannot ask sample patients to identify other individuals who may
need outpatient surgical services because of privacy and confidentiality issues they raise if
personally identifiable information (PII) were shared with the HOPD or ASC without that
person’s knowledge and permission.
• The Consent to Share Identifying Information question (Appendix F), if vendors elect to
include it, is considered one of the 15 allowable Supplemental Questions. The Consent to
Share Identifying information asks sample members if they will permit the survey vendor to

December 2015 III. Survey Participation Requirements
Centers for Medicare & Medicaid Services 19 Outpatient and Ambulatory Surgery CAHPS Survey Protocols and Guidelines Manual
link their name and identifying information to their survey responses. If an HOPD or ASC
would like this identifying data, their survey vendor must include the Consent to Share
Identifying Information question. This question is typically placed at the end of the
questionnaire, as the last question. The Consent to Share Identifying Information question is
available in English, Spanish, and Chinese at this time. Additional languages may be added
in the future.
If a survey vendor, HOPD, or ASC wishes to add more than 15 supplemental questions, the
vendor should submit an Exceptions Request Form (ERF) (see Chapter XV Exceptions Request
Process and Discrepancy Notification Report). The ERF should explain the questions and
provide an estimate of the additional time required for sample members to respond to them.
Vendor Business Requirements
Survey vendors must have proven experience in conducting mail-only, telephone-only, and
mixed-mode surveys. Any organization that owns, operates, or provides staffing for an HOPD
or ASC is not permitted to administer its own OAS CAHPS Survey or administer the survey on
behalf of any other HOPDs and ASCs. CMS believes an independent third party (survey vendor)
will be better able to solicit unbiased responses to the OAS CAHPS Survey; therefore, CMS
requires that HOPDs and ASCs contract with an independent, approved OAS CAHPS Survey
vendor to administer the OAS CAHPS Survey on their behalf.
The following types of organizations will not be eligible to administer the OAS CAHPS Survey
(as an approved OAS CAHPS Survey vendor):
• organizations or divisions within organizations that own or operate an HOPD or ASC or
provide outpatient or ambulatory surgical services, even if the division is run as a separate
entity to the HOPD or ASC;
• organizations that provide telehealth, monitoring of outpatient or ambulatory surgery
patients, or teleprompting services for HOPDs and ASCs; and
• organizations that provide staffing to HOPDs and ASCs for providing care to outpatient or
ambulatory surgery patients.
Survey vendors seeking approval as an OAS CAHPS Survey vendor must have the capability
and capacity to collect and process all survey-related data for the survey administration mode
they intend to use on the OAS CAHPS Survey following standardized procedures and guidelines.
The business requirements that survey vendors must meet are described in the following
sections.

III. Survey Participation Requirements December 2015
20 Centers for Medicare & Medicaid Services Outpatient and Ambulatory Surgery CAHPS Survey Protocols and Guidelines Manual
Relevant Business Experience
The following section describes the business experience a vendor must possess. Vendors should
submit the Vendor Application Form (Appendix A) only if they meet these requirements.
Vendors will also need to document details of this experience in their QAP. The OAS CAHPS
Survey Coordination Team will—through its review of Vendor Applications, through its review
of QAPs, and through site visits—confirm that vendors meet these requirements. These
requirements are the following.
A vendor must have relevant business experience, including a minimum of 3 years in business, a
minimum of 2 years conducting surveys with individuals, and a minimum of 2 years conducting
surveys in the selected data collection mode. A “survey of individuals” is defined as the
collection of data from individuals selected by statistical sampling methods and the data
collected are used for statistical purposes. An applicant organization must:
• Have conducted surveys of individuals responding about their own experiences.
• Be able to demonstrate that a statistical sampling process (e.g., simple random sampling,
proportionate stratified random sampling, or disproportionate stratified random sampling was
used in the conduct of previously conducted survey(s). This means that the organization has
to have conducted surveys where a sample of individuals was selected.
• Be able to demonstrate that it has conducted surveys of individuals as an organization for at
least 2 years. If someone within the applicant organization has relevant experience obtained
while in the employment of a different organization, that experience will not count toward
the 2-year minimum of survey experience.
• Currently possess all required facilities and systems to implement the OAS CAHPS Survey.
CMS and its OAS CAHPS Survey Coordination Team reserve the right to request
photographs of the applicant organization’s telephone call center for organizations applying
for the telephone-only and mixed modes, scanning and data processing systems if applying
for the mail-only or mixed modes, and other relevant equipment and facilities.
The following are examples of data collection activities that do not satisfy the requirement of
experience conducting surveys of individuals, as defined for the OAS CAHPS Survey, and will
not be considered as part of the experience that OAS CAHPS requires:
• polling questions administered to trainees or participants of training sessions or educational
courses, seminars, or workshops;
• focus groups, cognitive interviews, or any other qualitative data collection activities;
• surveys of fewer than 600 individuals;

December 2015 III. Survey Participation Requirements
Centers for Medicare & Medicaid Services 21 Outpatient and Ambulatory Surgery CAHPS Survey Protocols and Guidelines Manual
• surveys conducted that did not involve using statistical sampling methods;
• Internet or Web-based surveys; and
• interactive Voice Recognition Surveys.
Survey Capabilities and Capacity
The following section describes the capabilities and capacity which vendors must possess to be
approved for OAS CAHPS. There are specific requirements pursuant to Personnel, Facilities
and Systems, Security Policies, mail administration, telephone administration, mixed-mode
administration, data processing, and file submission. The OAS CAHPS Survey Coordination
Team will—through its review of Vendor Applications, through its review of QAPs, and through
site visits—confirm that vendors meet these requirements. These requirements are the following.
Personnel
Vendors must designate a Project Director with relevant survey experience, designate a
Sampling Manager with sample frame development and sample selection experience, and
designate a programmer capable of processing data and preparing data files for electronic
submission.
Facilities and Systems
Vendors must currently have the following facilities and systems:
• a secure commercial work environment,
• meet all local commercial code requirements, and
• physical facilities, electronic equipment, and software to receive sample files from
participating facilities and upload OAS CAHPS data to the Data Center.
Vendors must conduct all of their OAS CAHPS business operations within the United States.
This requirement applies to all staff and subcontractors. Home-based or virtual interviewers or
mail survey staff may not be used to administer the OAS CAHPS survey nor may they conduct
any survey administration process.
Security Policies
Vendor and all subcontractors must have and implement systems and security policies which
protect the security of PII as defined by the Health Insurance Portability and Accountability Act.
This includes sample data and survey data. Vendors will be required to submit policies.
Submissions must describe in sufficient detail policies and procedures for:
III. Survey Participation Requirements December 2015
22 Centers for Medicare & Medicaid Services Outpatient and Ambulatory Surgery CAHPS Survey Protocols and Guidelines Manual
• authorizing and de-authorizing individuals to access PII and survey data (including
background checks, training, signed agreements);
• preventing unauthorized individuals from accessing PII and survey data in physical format
(including key card/locked access, locked file cabinets);
• preventing unauthorized individuals from accessing data in electronic format (including
password protections, firewalls, data encryption software, personnel access limitation
procedures, and virus and spyware protection);
• safeguarding PII and survey data in physical format against loss or destruction (including fire
and building safety codes);
• safeguarding PII and survey data in electronic format against loss or destruction (e.g., offsite
daily backups); and
• destroying PII and survey data when specified.
Further information on security policies is presented in Chapter VIII.
Mail-Only Survey Administration
Vendors who are using mail-only survey administration must have the capability to:
• assign a random, unique, de-identified identification number to each sampled patient;
• obtain and verify addresses of sampled patients;
• print according to formatting guidelines professional-quality survey questionnaires
(containing single-coded questions, code-all-that-apply questions) and materials;
• merge and print sample patient name and address, and the name of the outpatient facility on
personalized mail survey cover letters and print unique sample identification on the survey
questionnaire;
• track fielded surveys throughout the protocol, avoiding respondent burden and losing
respondents;
• receive and process (key entry or scanning) completed questionnaires received;
• track and identify nonrespondents for follow-up mailing;
• provide a toll-free customer support line and respond to calls from sample members within
48 hours; and

December 2015 III. Survey Participation Requirements
Centers for Medicare & Medicaid Services 23 Outpatient and Ambulatory Surgery CAHPS Survey Protocols and Guidelines Manual
• assign final status codes in accordance with OAS CAHPS coding requirements to describe
the final result of work on each sampled case (see Chapter IX).
Telephone-Only Survey Administration
Vendors who are using telephone-only survey administration must have the capability to:
• assign a random, unique, de-identified identification number to each sampled patient;
• verify telephone numbers;
• develop computer programs for electronically administering the survey (for CATI);
• collect data using CATI which allows seamless administration of single-coded questions,
code-all-that-apply questions;
• track fielded surveys throughout the protocol, avoiding respondent burden and losing
respondents;
• schedule callbacks to nonrespondents at varying times of the day and week;
• provide a toll-free customer support line and respond to calls within 48 hours;
• assign final status codes in accordance with OAS CAHPS coding guidelines to reflect the
results of attempts to obtain completed interview with sampled cases; and
• conduct monitoring of interviewers.
Mixed-Mode Survey Administration
Vendors that apply for administering the OAS CAHPS Survey as a mixed-mode survey (mail
with telephone follow-up of non-respondents) must have the capability to adhere to all mail-only
and telephone-only survey administration requirements described above. In addition, they must
have an electronic tracking system that can track cases from the mail survey through telephone
follow-up activities.
Data Processing and File Submission
Vendors must have the capability to:
• Scan or key responses to single coded questions, code-all-that-apply questions from
completed surveys.
• Develop data files and edit and clean data according to standard protocols.
• Follow all data cleaning and data submission rules, including verifying that data files are de-
identified and contain no duplicate cases.

III. Survey Participation Requirements December 2015
24 Centers for Medicare & Medicaid Services Outpatient and Ambulatory Surgery CAHPS Survey Protocols and Guidelines Manual
• Export data from the electronic data collection system to an XML template, confirm that the
data were exported correctly and that the XML files are formatted correctly and contain the
correct data headers and data records.
• Submit data electronically in the specified format (XML) to the OAS CAHPS secured
website.
◦ Vendors must work with the OAS CAHPS Survey Coordination Team to quickly resolve
data problems and data submission problems. As stated above with regard to the
Discrepancy Notification Report, vendors must inform the OAS CAHPS Survey
Coordination Team promptly (within 24 hours after the discrepancy has been identified,
when possible) of any deviation from the protocol. Vendors are encouraged to submit
their test data files early so as to reveal any potential problems, and afford time to address
them prior to submission.
Adherence to Quality Assurance Guidelines
Vendors must have prior experience, facilities, equipment and software to enable them to:
• Incorporate well-documented quality control procedures (as applicable) for:
◦ in-house training of staff involved in survey operations
◦ printing, mailing, and recording of receipt of survey questionnaires
◦ telephone administration of survey
◦ coding and editing of survey data and survey-related materials
◦ scanning or keying in survey data
◦ preparation of final person-level data files for submission
◦ all other functions and processes that affect the administration of the OAS CAHPS
Survey
• Participate in any conference calls and site visits requested by the Coordination Team as part
of overall quality monitoring activities. Site visits will be conducted with all approved
vendors.
• Provide documentation as requested for site visits and conference calls, including but not
limited to staff training records, telephone interviewer monitoring records, and file
construction documentation.
December 2015 III. Survey Participation Requirements
Centers for Medicare & Medicaid Services 25 Outpatient and Ambulatory Surgery CAHPS Survey Protocols and Guidelines Manual
Participation in Training and Quality Assurance Activities
Survey vendors must participate in all required training and quality assurance activities necessary
to ensure the successful implementation of the OAS CAHPS Survey. This includes the
following requirements:
• Review and follow all procedures described in the OAS CAHPS Protocols and Guidelines
Manual that are applicable to the selected survey data collection mode.
• Attend all CMS Introduction and Vendor Update training sessions. (Failure to complete all
required vendor training will result in withdrawal of approved vendor status.)
• Participate in any conference calls and site visits requested by the OAS CAHPS Survey
Coordination Team as part of overall quality monitoring activities. Site visits will be
conducted with all approved vendors. Vendors must provide documentation as requested for
site visits and conference calls, including but not limited to staff training records, telephone
interviewer monitoring records, sample frame development documentation, and file
construction documentation.
Subcontractor Requirements
Any survey vendor using a subcontractor in any capacity on the OAS CAHPS Survey is required
to complete the relevant sections of the Vendor Application Form (Appendix A) about each of its
subcontractors. Information requested on the Vendor Application about subcontractor
capabilities is similar to that requested for vendors. Details must be provided about the
capabilities and capacity of the subcontractor to handle mail, telephone, and mixed-mode survey
activities. Further, specific information must also be provided about the subcontractor’s quality
assurance practices, data security policies, and facilities and systems.
If a vendor applicant organization’s subcontractor will conduct substantive work to support the
implementation of the OAS CAHPS Survey, that subcontractor is strongly encouraged to attend
relevant portions of the Introduction to OAS CAHPS Webinar Training Session and all OAS
CAHPS Update Training Sessions. For purposes of this survey, “substantive work” is defined as
follows:
• ANY statistical function, including sample selection,
• telephone survey data collection (i.e., if an approved vendor is subcontracting telephone data
collection activities),
• mail or questionnaire receipt and processing, and
• construction or submission of XML data files.

III. Survey Participation Requirements December 2015
26 Centers for Medicare & Medicaid Services Outpatient and Ambulatory Surgery CAHPS Survey Protocols and Guidelines Manual
If an applicant vendor will be using a subcontractor to conduct any substantive work as defined
above, the subcontractor organization will be subject to the same or similar requirements as the
applicant vendor.
Additional Requirements
CMS and its OAS CAHPS Survey Coordination Team reserve the right to request additional
information from applicant organizations to help determine whether approval status should be
granted. Information requested may include the following:
• Taxpayer Identification Number;
• website address;
• detailed description of surveys conducted that demonstrate statistical sampling and data
collection capabilities;
• photographs of applicant organization’s facilities and systems;
• resumes of key staff, demonstrating experience with data collection, sampling, and computer
programming; and
• additional descriptions of processes, including treatment of confidential data, control or
tracking systems, quality assurance practices, and XML file construction.

Centers for Medicare & Medicaid Services 27 Outpatient and Ambulatory Surgery CAHPS Survey Protocols and Guidelines Manual
IV. SAMPLING PROCEDURES
Overview
This chapter describes the procedures survey vendors should use for sample selection. The
process includes requesting a file of patients for the hospital outpatient departments or
ambulatory surgery centers (HOPDs or ASCs), identifying patients and procedures eligible for
the survey, constructing a sampling frame, and selecting a patient sample each month. The
sampling procedures described in this chapter were developed to ensure standardized
administration of the OAS CAHPS Survey by all survey vendors and to ensure comparability of
the data and survey results that are publicly reported.
Before explaining patient sampling steps, it is
necessary to explain facility eligibility and how the
OAS CAHPS is constructed for analysis and
reporting. See the text box for a review of the
definition of a facility that is eligible for OAS
CAHPS. When this chapter refers to “facilities” or
“HOPDs or ASCs” it is referring to HOPDs and
ASCs that meet this definition. The unit of
analysis in OAS CAHPS is the CCN, not the
individual ACS and HOPD. Implications are as
follows:
• For HOPDs: Every HOPD that is under this
hospital’s CCN needs to participate in OAS
CAHPS for the sample to be valid. Vendors should work with their client hospital to learn
what HOPDs it contains and include all HOPDs in OAS CAHPS.
• For ASCs: Every department or location within the ASC that is under their CCN needs to
participate in OAS CAHPS for the sample to be valid. Vendors should work with their client
ASCs to learn what locations or departments their CCN comprises and include all of them in
OAS CAHPS.
The remaining sections in this chapter on sampling are organized in the general chronological
order in which the corresponding tasks will take place.
• Step 1: Obtain a monthly patient information file from each client HOPD or ASC under the
same CCN.
Definition of OAS CAHPS-eligible facility
(For further detail see Chapter II)
HOPD: A unit of a hospital whose primary
focus is to perform outpatient surgeries and
procedures, is Medicare-certified, has a CMS
Certification Number (CCN), and bills CMS
under the Outpatient Prospective Payment
System (OPPS).
ASC: A freestanding medical facility that
performs outpatient surgeries and
procedures, is Medicare-certified, has a
CCN, and meets the general conditions and
requirements in accordance with 42 CFR
416 subpart B.

IV. Sampling Procedures December 2015
28 Centers for Medicare & Medicaid Services Outpatient and Ambulatory Surgery CAHPS Survey Protocols and Guidelines Manual
• Step 2: Examine the monthly patient information file for completeness and work with the
HOPD or ASC to obtain missing data elements. Process and check the file for duplicate
information.
• Step 3: Identify eligible patients and surgeries/procedures and construct a sampling frame.
• Step 4: Determine the sampling method most appropriate for the OAS CAHPS survey for
this CCN.
• Step 5: Determine the sample size and sampling rate and select the sample.
• Step 6: Verify or update contact information for sampled patients.
• Step 7: Assign a unique sample identification number to each selected sampled patient.
• Step 8: Finalize the monthly sample file and initiate data collection activities.
Step 1: Obtain a Monthly Patient Information File from Each Client HOPD or ASC Under the Same CCN
Schedule for Receiving the Monthly Patient Information File
HOPDs or ASCs administering the OAS CAHPS Survey must submit a monthly patient
information file to their contracted OAS CAHPS Survey vendor each time they conduct the
survey.
Survey vendors select samples each month from the frame of patients who meet survey eligibility
criteria. Survey vendors also initiate the survey on a monthly basis. It is critical that client
HOPDs and ASCs provide monthly patient information in a timely manner, leaving vendors
enough time to conduct sampling and quality control checks before the monthly survey is
initiated. For each monthly set of sampled patients, the survey must be initiated within 21 days
after the sample month ends. CMS recognizes that on rare occasions an HOPD or ASC may
have a situation that may prevent it from providing the monthly patient information in time for
the vendor to initiate the survey within 21 days after the sample month ends. Therefore, the
vendor can initiate the survey within 26 days after the sample month ends. These exceptions are
described in Chapters V, VI, and VII pursuant to each mode of data collection.
Sampling More Frequently Than Monthly
Some HOPDs and ASCs may prefer to deliver patient records to their survey vendors more
frequently than monthly (e.g., weekly, biweekly) per their convenience. This is acceptable,
provided that sampling is done using a monthly patient information file.

December 2015 IV. Sampling Procedures
Centers for Medicare & Medicaid Services 29 Outpatient and Ambulatory Surgery CAHPS Survey Protocols and Guidelines Manual
However, if the survey vendor wishes to perform sampling on a continuous basis it must
complete and submit an Exceptions Request Form that explains its reasons and proposed
procedures. It may receive approval from CMS for more frequent sampling. Information about
the Exceptions Request Form and process is provided in Chapter XV of this manual.
Patient Eligibility Requirements—12 Criteria
1. Patients who had at least one outpatient surgery/procedure during the sample month
(including outpatient surgeries and procedures when the patient had an overnight stay for
observation but was not admitted to the hospital);
2. Patients who were at least 18 years of age when they received their outpatient surgery or
procedure;
3. Patients regardless of insurance or method of payment;
4. Patients whose outpatient surgery or procedure was given in an HOPD or ASC as defined by
the project;
5. Patient’s surgery or procedure meets project eligibility definitions, which are as follows:
5a. A procedure is OAS CAHPS-eligible if it has a G-Code3 of G0104, G0105, G0121 or
G0260, or
5b. A surgery, diagnostic procedure, or other type of procedure is OAS CAHPS-eligible if it
has a CPT-44 code in the 10021– 69990 range, was performed in an outpatient surgery
department or ambulatory surgery center, was not billed as Laboratory, Radiology,
Physical Therapy, Respiratory Therapy, or Diagnostic studies and if it has no
accompanying modifier of 73 or 74 (discontinued procedure)5,6
5c. Also note that a facility may assign more than one code to a surgery or procedure. The
presence of one eligible G-code or CPT code is all that is needed to make it OAS
CAHPS-eligible.
6. Patients who have a domestic U.S. mailing address;
7. Patients who are not deceased;
3 G Codes (HCPCS Level II) are alphanumeric medical procedure codes for temporary procedures and professional
services. HCPCS Level II codes are maintained by CMS. 4 Current Procedural Terminology (CPT).
5 Modifiers 73 and 74 (discontinued procedure) indicate that a procedure or surgery did not take place. CPT-4 codes
with Modifier 73 or 74 should be excluded. 6 Vendors with HOPD clients should note that hospitals perform procedures within these codes across a variety of
departments in a hospital. OAS CAHPS is only surveying patients who received these procedures in a HOPD which
focuses on outpatient procedures and bills under OPPS (as defined in Chapter II.)

IV. Sampling Procedures December 2015
30 Centers for Medicare & Medicaid Services Outpatient and Ambulatory Surgery CAHPS Survey Protocols and Guidelines Manual
8. Patients who do not reside in a nursing home;
9. Patients who were not discharged to hospice care following their surgery;
10. Patients who are not identified as prisoners;
11. Patients who did not request that the HOPDs or ASCs not release their name and contact
information to anyone other than facility personnel, hereafter referred to in this manual as “no
publicity” patients; and
12. Some states have regulations and laws governing the release of patient information for
patients with specific illnesses or conditions, and for other special patient populations,
including patients with HIV/AIDS. It is the ASC’s or HOPD’s responsibility to identify any
applicable state laws and regulations and exclude state-regulated patients from the survey as
required by law or regulation.
Construction of Monthly Patient Information Files
When the HOPD or ASC provides the files, it must include the following:
• all patients whose outpatient surgery or procedure was given in an HOPD or ASC as defined
by the project (eligibility criterion #4)
• all patients who had at least one outpatient surgery/procedure during the sample month
(including outpatient surgeries and procedures when the patient had an overnight stay for
observation but was not admitted to the hospital) (eligibility criterion #1)
• all patients regardless of insurance or method of payment (eligibility criterion #3)
and they must exclude the following
• patients who cannot be surveyed because of state regulations (eligibility criterion #12)
• no-publicity patients (eligibility criterion #11)
• prisoners if known (eligibility criterion #10)
• nursing home residents if known (eligibility criterion #8)
• patients discharged to hospice if known (eligibility criterion #9), and
• deceased patients if known (eligibility criterion #7).
The HOPD/ASC and their vendor should reach a mutually acceptable arrangement as to whether
the facility, or the vendor, should be responsible for excluding patients who fail eligibility
criteria 2 [age], 5 [surgical code], and 6 [domestic address].

December 2015 IV. Sampling Procedures
Centers for Medicare & Medicaid Services 31 Outpatient and Ambulatory Surgery CAHPS Survey Protocols and Guidelines Manual
With the exception of these categories of patients to exclude, facilities must supply all patients
served monthly. No patients may be held back for any other reason.
It is the survey vendor’s responsibility to ensure that
• the facility understands which patients to include and exclude from the files, and
• the facility provides the vendor with sufficient information to identify and exclude patients
who do not meet eligibility requirements.
Survey vendors must retain the monthly patient information files supplied by their clients for a
minimum of 18 months. This information is subject to review during site visits.
Monthly HOPD and ASC files must contain information at both the patient and the facility level,
as described below.
Information Needed From HOPDs and ASCs for Each Patient on the
Monthly Patient Information File
HOPDs and ASCs are required to provide all of the information shown in Table 4.1 for each
patient in the monthly patient information file. The information the HOPD or ASC provides will
be used by the survey vendor to survey sampled patients and will be used by the OAS CAHPS
Survey Coordination Team for data analysis.
Table 4.1 Information Needed From ASCs/HOPDs for Patient Served During Sample Month
Data Element Required Reason Needed
Patient’s full name (First Name, Middle Initial, and Last Name as separate fields)
Survey administration
Gender Survey administration and analysis
Patient’s date of birth (MMDDYYYY) Survey eligibility
Mailing address (Patient Mailing Address 1, Patient Mailing Address 2, Address City, Address State, and Address Zip Code as separate data fields)
Survey administration
Patient’s telephone number including area code Survey administration
Indication whether telephone number is a cell phone Telephone survey administration (ensuring compliance with FCC Regulations)
Medical Record Number (Patient’s HOPD or ASC medical record number)
Deduplication of patients before sampling
Procedure code(s) (CPT or G code) Survey eligibility
Date of procedure (MMDDYYYY) Survey administration
Name of location where surgery occurred Survey administration (to use facility name that will be familiar to the sampled patient)

IV. Sampling Procedures December 2015
32 Centers for Medicare & Medicaid Services Outpatient and Ambulatory Surgery CAHPS Survey Protocols and Guidelines Manual
Information Needed From Each HOPD or ASC at the Facility Level
HOPDs and ASCs are required to submit several facility-level data elements along with their
monthly patient information file. These elements are the CCN, the name associated with the
CCN, the Sample Month, Sample Year, Mode of Survey, Type of Sampling Method, Number of
Patients Served, and Number of Patients on the File Submitted to the Vendor. The “Number of
Patients Served” is the total number of patients the HOPD or ASC served during the sample
month. This total should include patients who had at least one outpatient surgery or procedure at
any point during the sample month, regardless of whether the patient is OAS CAHPS-eligible.
Further explanation of these required numbers is found in Chapter XI and in Appendix K (XML
File Layout for Standard Header Record).
Definition and Explanation of Some of the Data Elements Required From
HOPDs and ASCs
This section provides more explanation on some of the variables on the monthly patient
information file.
• Patient’s date of birth. Patients must be 18 years of age on the day of their outpatient
surgery/ procedure to be eligible for participation in the OAS CAHPS Survey.
• Vendors should ensure that their client HOPDs and ASCs include each patient’s mailing
address, even if a telephone survey is planned for that HOPD or ASC. For facilities planning
telephone surveys, the mailing address for each patient is needed so that the vendor can
obtain or verify the sample patient’s telephone number. The facilities provide the initial
contact information; however, survey vendors are strongly encouraged to use address
verification or telephone number look-up services to obtain updated contact information.
• Patient telephone phone number is needed for mixed-mode and phone-only surveys. It is
strongly recommended for mail-only modes because the telephone can be used to validate or
update the patient’s address information.
• Indication of cell phone is needed for mixed-mode and phone-only surveys. FCC regulations
prohibit auto-dialing of cell phone numbers. Therefore, cell phone numbers need to be
identified in advance to allow the vendor to treat cell phone numbers in a way that complies
with FCC regulations. Vendors are advised to familiarize themselves with all applicable state
and federal laws. If the facility is unable to advise the survey vendor as to which telephone
numbers provided are cell phone numbers, it is the vendor’s responsibility to obtain from an
external source an up-to-date list of cell phone numbers and land line numbers which have
been ported to cell phone from an external source. The external source must be compared to
the phone numbers of the sampled patients to identify any phone numbers which are cell
phones.

December 2015 IV. Sampling Procedures
Centers for Medicare & Medicaid Services 33 Outpatient and Ambulatory Surgery CAHPS Survey Protocols and Guidelines Manual
• The patient’s medical record number is the unique identifier that the HOPD or ASC assigns
to the patient that allows the HOPD or ASC to track and document the care provided to the
patient. This number, along with other data elements, will allow the vendor to keep track of
whether each patient has been recently sampled.
• CPT-4 codes are a standardized set of five-digit codes developed by the American Medical
Association. The CPT codes relevant to OAS CAHPS are divided into the following
categories:
◦ 10021–10022 general
◦ 10030–19499 integumentary system
◦ 20000–29999 musculoskeletal system
◦ 30000–32999 respiratory system
◦ 33010–37799 cardiovascular system
◦ 38100–38999 hemic and lymphatic systems
◦ 39000–39599 mediastinum and diaphragm
◦ 40490–49999 digestive system
◦ 50010–53899 urinary system
◦ 54000–55899 male genital system
◦ 55920–55980 reproductive system and intersex
◦ 56405–58999 female genital system
◦ 59000–59899 maternity care and delivery
◦ 60000–60699 endocrine system
◦ 61000–64999 nervous system
◦ 65091–68899 eye and ocular adnexa
◦ 69000–69979 auditory system
◦ 69990 microsurgery
Vendors should work closely with facilities to ensure that only eligible surgeries and procedures
are included in the sample. Some HOPDs and ASCs perform additional procedures that would
not be inappropriate for the OAS CAHPS Survey because of the limited involvement of the
doctors and nurses or the fact that the CPT code represents preadmission testing, postsurgery
follow-up testing, physical therapy, respiratory therapy, laboratory, or radiology testing only.

IV. Sampling Procedures December 2015
34 Centers for Medicare & Medicaid Services Outpatient and Ambulatory Surgery CAHPS Survey Protocols and Guidelines Manual
For example, the following CPT codes fall within the range for Codes for Surgery but are not
considered to be eligible for OAS CAHPS:
• 16020, 16025, 16030: Dressings or debridement of partial-thickness burns, initial or
subsequent
• 29581: Application of multilayer compression system; leg (below knee), including ankle and
foot
• 36600: Arterial puncture, withdrawal of blood for diagnosis
• 36416: Collection of capillary blood specimen
• 36415: Collection of venous blood by venipuncture
Additional CPT codes within the eligible range may also be excluded; however, the vendor must
submit an Exception Request form to document the codes to be excluded.
• G Codes or HCPCS Level II codes are alphanumeric medical procedure codes for temporary
procedures and professional services. HCPCS Level II codes are maintained by CMS. At
this time, only four G-codes are OAS CAHPS-eligible: G0104, G0105, G0121, and G0260.
Name of location where surgery occurred. Some HOPDs or ASCs are part of larger, multisite
institutions. The monthly patient information file should state the name of the location where
each patient received his or her surgery. This name is included on the cover letter so that the
patient recognizes the name of this location. It may not be the official name of the facility. If
there is only one location for all patients, then this value will be identical for all patients.
Although location where surgery occurred is part of the monthly patient information file, OAS
CAHPS does not report survey results for individual locations or units within the CCN. OAS
CAHPS reports only at the CCN level.
Protocol for No Eligible Patients Served in the Sample Month
If the HOPD or ASC did not perform any outpatient surgeries/procedures or did not serve any
patients who met survey eligibility criteria during the sample month, the HOPD or ASC must
still submit a monthly patient information file or an e-mail notification to its survey vendor
stating that no survey-eligible patients were served during that sample month.
Vendors are still required to submit data to the OAS CAHPS Data Center for a month when there
are no eligible cases. The vendor submits a Zero Eligible File in this situation. The vendor must
indicate on the file that there were zero eligible cases in data element for “Eligible Patients” and
enter all other information required in the Header Record Section of the XML file (refer to
Chapter XI in this manual for more information about data file preparation and submission). If

December 2015 IV. Sampling Procedures
Centers for Medicare & Medicaid Services 35 Outpatient and Ambulatory Surgery CAHPS Survey Protocols and Guidelines Manual
the vendor does not submit a zeroeligible file in this case, CMS and the OAS CAHPS Survey
Coordination Team will view the HOPD or ASC as having “missed” a sample month. HOPDs or
ASCs for which an OAS CAHPS Survey data file is not submitted for a month in the reporting
period may be considered as being noncompliant with OAS CAHPS Survey participation
requirements.
Protocol for Administering Other Surveys in Conjunction With the OAS
CAHPS Survey
Some HOPDs and ASCs may wish to administer other surveys of their patients. The following
guidelines should be used if the HOPD or ASC is planning to administer other surveys in
addition to the OAS CAHPS Survey.
If an HOPD or ASC will be fielding another survey of its patients, it must provide a file of all
OAS CAHPS-eligible patients to its survey vendor for the OAS CAHPS Survey first, prior to
selecting patients for any other survey. Patients who were not randomly selected into the OAS
CAHPS Survey sample for the sample month may be included in a sample for a separate survey
that the vendor conducts on the HOPD’s or ASC’s behalf that month. This secondary survey
sample must be selected after the OAS CAHPS Survey sample has been drawn. This means the
secondary survey must use the unused OAS CAHPS sample. The vendor cannot provide the list
of sampled patients for OAS CAHPS to the HOPD or ASC because this would be a violation of
the patient’s confidentiality. Because of the coordination required between surveys, both surveys
must be administered by the same vendor.
Facilities that are conducting patient surveys in parallel with OAS CAHPS are reminded that they
are allowed to add up to 10 questions of their own to the OAS CAHPS questionnaire.
Subsuming the questions from their other survey into OAS CAHPS and discontinuing the other
survey may be more efficient than administering both surveys simultaneously.
Approved OAS CAHPS Survey vendors are expected to work closely with their client HOPDs
and ASCs to identify patients who are eligible for inclusion in other surveys the facilities
conduct. It is very important to avoid burdening patients with both OAS CAHPS and other
surveys. If the other survey is CMS-sponsored, vendors should contact the OAS CAHPS Survey
Coordination Team to make arrangements for both surveys.
Step 2: Examine the Monthly Patient Information File for Completeness and Possible Duplication
Survey vendors should examine each monthly patient information file provided by their client
facilities to ensure that information they need for determining survey eligibility for all patients
and surgeries on the file has been provided. These include CPT or G code(s) classifying the
surgery, patient date of birth, and date of surgery/procedure. If patient information needed for

IV. Sampling Procedures December 2015
36 Centers for Medicare & Medicaid Services Outpatient and Ambulatory Surgery CAHPS Survey Protocols and Guidelines Manual
sample selection is missing, the vendor should work with the HOPD or ASC to obtain all missing
data before selecting the sample.
Survey vendors should check the monthly patient information file to ensure that it does not
include duplicate information—that is, to ensure that a patient does not appear more than once on
this month’s file. If duplicate information is included on the file received, the vendor should
make a copy of the monthly patient information file and remove the duplicate information on the
new file. Note that vendors are required to retain the original monthly patient information files
submitted by their client HOPDs and ASCs, and any new copies made, for possible audits by
CMS and the OAS CAHPS Survey Coordination Team.
When checking the monthly patient information files to identify “duplicate” patients or patients
who may have been listed on the file more than once, vendors should use the patient’s Medical
Record Number (MRN) and at least one other patient data element to check for duplicate cases.
Data elements that will be useful for identifying duplicates include the surgery code(s), patient’s
name, date of birth, telephone number, etc. Using the MRN in conjunction with other patient
data elements will help ensure that patients identified as duplicate patients on the file are indeed
“duplicate” records. If a patient had more than one surgery/procedure in the sample month, it is
to be expected that he or she will have more than one record in the monthly patient information
file. Vendors should remove the patient’s record associated with a surgery code that is not OAS
CAHPS-eligible. If the patient received procedures on different dates in the month and the
procedures on all dates are OAS CAHPS-eligible, the vendor should remove the records for the
earlier procedures and keep only the latest procedure on the sample frame.
The vendor should have a different staff member conduct a QC check on these two processes
(completeness check, removal of duplicates) before proceeding to Step 3.
Step 3: Identify Eligible Patients and Construct a Sampling Frame
After the completeness check and the duplicate patient removal, the survey vendor should verify
the eligibility of the patients. As stated above, HOPDs and ASCs may elect to remove ineligible
patients and surgeries before supplying the monthly patient information file, or may elect to have
their vendor do it on their behalf. Either way, the vendor should do the following:
1. Compute patient age at the time of surgery by use of the date of birth and surgery date.
Verify that the patient was 18 years of age or older at the time of his or her surgery.
2. Verify that the surgery or procedure for each patient is OAS CAHPS-eligible according to its
CPT code(s) or G code(s) and that the procedure was performed in an ASC/HOPD and not
billed as Laboratory, Radiology, Physical Therapy, Respiratory Therapy, or Diagnostic
Studies.

December 2015 IV. Sampling Procedures
Centers for Medicare & Medicaid Services 37 Outpatient and Ambulatory Surgery CAHPS Survey Protocols and Guidelines Manual
3. Verify that patients have a U.S. domestic address.
4. Verify that the date of the surgery/procedure is within the sample month.
These four checks align with the Patient Eligibility Requirements listed in Step 1. Patients who
fail any of these verifications are not OAS CAHPS-eligible and should be removed from the
sample frame.
After the completeness and duplication review in Step 2 and the removal of ineligible patients in
Step 3, there is another step that must be performed before creating a definitive sample frame for
the month. That step is to remove all patients who were sampled for OAS CAHPS in the
previous 5 months.
To reduce respondent burden, outpatient surgical patients can only be sampled by OAS CAHPS
once in a 6-month period. Therefore, the survey vendor must also exclude from the sample
frame patients who were included in the OAS CAHPS Survey sample during the 5 months
preceding the sample month. Vendors must compare all eligible patients on the new month’s
file to all patients selected for the survey in the past 5 months and identify any repeats.
Such repeating patients are ineligible and must be removed from the sample frame. This
determination must be made before sampling from the sample frame begins.
For purposes of audit and quality assurance, survey vendors must keep the monthly patient
information files submitted by all HOPDs and ASCs and the sampling frame created for each
sample month for 18 months. Vendors must record and retain documentation showing the
reasons patients were excluded from the sample frame created for each HOPD and ASC for each
sample month, and provide documentation of all staff quality control checks that were completed
during the sampling process. This documentation will be subject to review by the OAS CAHPS
Survey Coordination Team during site visits.
Step 4: Determine the Sampling Method Most Appropriate for the OAS CAHPS Survey for This CCN
As a reminder, OAS CAHPS
participation within the CCN must be
comprehensive. As stated in Step 1, all
components within the CCN which are
OAS CAHPS-eligible are to be included
in OAS CAHPS. When this chapter
mentions the term “components” it refers
to the definition in the text box.
The components present in the CCN, the
Definition of “Component” Used in This Chapter
Components of an HOPD: Any departments,
locations, or other divisions which meet the definition
of an OAS CAHPS-eligible HOPD and which bill
under the hospital’s CCN.
Components of an ASC: Any departments, locations,
or centers which are within or associated with the
eligible ASC and which bill under the ASC’s CCN.
For sampling purposes, components are considered
sampling strata.

IV. Sampling Procedures December 2015
38 Centers for Medicare & Medicaid Services Outpatient and Ambulatory Surgery CAHPS Survey Protocols and Guidelines Manual
volume of eligible patients in each, and analytic goals of the client CCN dictate which sampling
method is most appropriate. There are four acceptable sampling methods for OAS CAHPS:
• Simple random sampling method
• Stratified systematic sampling method
• Proportionate stratified random sampling method
• Disproportionate stratified random sampling method
Simple Random Sampling (SRS) Method
Appropriate use: When there is a single component within the CCN.
Example: Northshore Ambulatory Surgery Center sees about 400 patients per month. It does
not share the CCN with any other surgery centers and has only one location.
Stratified Systematic Sampling (SSS) Method
Appropriate use: There are two or more components (strata) within the CCN and patients from
all components need to be included in the OAS CAHPS sample proportionally to their volume in
the CCN to make a valid sample. However, the strata are small or the facility does not wish to
track results at the strata level.
Example: ABC Surgery Center comprises three locations (strata). They all bill under the same
CCN. Location A served 100 eligible patients in the sample month, Location B, 140, and
Location C, 80 eligible patients in the sample month, for a total of 320 eligible patients.
Proportionate Stratified Random Sampling (PSRS) Method
Appropriate use: There are two or more components (strata) within the CCN and patients from
all components need to be included in the OAS CAHPS sample proportionally to their volume in
the CCN to make a valid sample. Additionally:
• the HOPD or ASC would like to keep track of samples and results for each stratum, or
• the HOPD or ASC would like to designate other aggregates of operating units for tracking
while using the same sampling rate for each.
Example: Any-City Best Care Surgical Center comprises three locations (strata) but they all bill
under the same CCN. These patients were located in Facility A, which serves 200
patients/month, Facility B, which serves 150 patients/month, and Facility C, which serves 180
patients/month. Facility A has been in operation for 10 years, but Facilities B and C were opened

December 2015 IV. Sampling Procedures
Centers for Medicare & Medicaid Services 39 Outpatient and Ambulatory Surgery CAHPS Survey Protocols and Guidelines Manual
in the last 2 years. Any-City Best Surgical Center wants the survey estimates from each location
to have statistical precision and would like to track them separately over time.
Additional requirements and limitations: A minimum of 10 eligible patients must be in each
stratum for PSRS sampling to be used. The statistical precision of survey results at the stratum
level will not be very good unless the stratum sample size is about the size of the overall sample
requirements (25 completed surveys per month).
Disproportionate Stratified Random Sampling (DSRS) Method
Appropriate use: There are two or more components (strata) within the CCN and the CCN
wishes to achieve statistically precise survey estimates for the component facilities.
Example: Memorial Hospital includes three eligible outpatient departments (strata): Same Day
Surgery (120/month), Outpatient (100/month), and Endoscopy (40/month). Memorial wants each
department’s survey estimate to have statistical precision.
Additional requirements and limitations: A minimum of 10 eligible patients must be in each
stratum for DSRS sampling to be used. The goal of the DSRS is to obtain sufficient statistical
power to detect differences at the stratum level. Vendors wishing to use DSRS must submit an
Exceptions Request Form to the OAS CAHPS Survey Coordination Team.
Deciding Which Method to Use
The facility, in conjunction with the vendor, should determine which of the four OAS CAHPS-
approved sampling methods described above is most appropriate for their CCN and meets the
analytic needs of the facility. Unless disproportionate stratified random sampling has been
approved for use, if there are two or more components with the CCN either stratified systematic
sampling or proportionate stratified random sampling must be used. Simple random sampling
may not be used if there are two or more components.
The same sampling method must be used for all sample months in the quarter. Vendors may
switch to a different sampling method only at the beginning of a new quarter.
Step 5: Determine the Sample Size and Sampling Rate, and Select the Sample
Select an Appropriate Sample Size Each Month
The target for the statistical precision of OAS CAHPS Survey results that will be publicly
reported is based on a reliability criterion. The reliability target for the OAS CAHPS Survey
ratings and most of the composites is 0.8 or higher. For reasons of statistical precision, a target
minimum of 300 completed OAS CAHPS Surveys has been set for each HOPD or ASC over
each 12-month reporting period. This is an average of 25 completed surveys per month.

IV. Sampling Procedures December 2015
40 Centers for Medicare & Medicaid Services Outpatient and Ambulatory Surgery CAHPS Survey Protocols and Guidelines Manual
The mode of administration of the survey will be an important factor in determining sample size
and response rates. Table 4.2 shows response rates by mode which are anticipated for OAS
CAHPS and the sample sizes needed based on these rates.
Table 4.2 Response Rates Obtained by Mode Anticipated for OAS CAHPS
Mode Expected Response Rate Sample Size for 25 Responses/Month
Mail only 32% 77
Phone only 32% 77
Mixed 40% 62
The sample size estimates above were derived using the following formula:
Sample size = (number of responses needed) (response rate) = 25 (response rate)
where the value used for the number of responses needed is 25. These sample size estimates
have been rounded up to the nearest integer. Each vendor should work with its client HOPD or
ASC and use experience on other surveys with similar populations to determine the appropriate
data collection mode and expected response rate to use as a guide for calculating monthly sample
sizes.
Determine the Sampling Rate
Survey vendors must determine a sampling rate and use that rate to ensure that an even
distribution of patients is sampled over a 12-month period. To determine the sampling rate,
vendors will need to have a good estimate of the size of the sample frame. The typical frame size
will depend on the number of patients served by the HOPD or ASC and the percentage of these
patients and surgeries/procedures that are OAS CAHPS-eligible.
Vendors should expect that there will be variability in the number of patients the HOPD or ASC
serves and the number eligible for the survey because these characteristics vary over time. In
some cases there could be seasonality to surgeries, depending on the mix of patients served by
different HOPDs or ASCs. The number of patients to be selected each month to yield a
minimum of 300 annual completed surveys will ultimately be determined by trial and error.
The sampling rate must be approximately the same for each month in a quarter. The first month
that an HOPD or ASC participates in the OAS CAHPS Survey the facility might have an
atypically high number of patients eligible for the survey because none of the patients will have
been sampled in the preceding sample months. Therefore, the vendor should adjust the sampling
rate for the first sample month to make the sample for that month about equal to subsequent
sample months. The rate may be increased in subsequent months to achieve the target of 300

December 2015 IV. Sampling Procedures
Centers for Medicare & Medicaid Services 41 Outpatient and Ambulatory Surgery CAHPS Survey Protocols and Guidelines Manual
annual completed surveys, but should not be decreased simply to avoid exceeding 300 completed
surveys.
The survey vendor should estimate a sampling rate by working with their client HOPDs and
ASCs to understand the number of patients served and how many of them will typically be
eligible. This is described below.
Using Prior Months From the HOPD or ASC in the Determination of the
Sampling Rate
The vendor should work with the HOPD or ASC prior to the first sample month that the HOPD
or ASC begins its participation in the OAS CAHPS Survey to estimate the sample frame size.
This sample frame size should be estimated from the number of patients served monthly and the
percentage of those patients and surgeries/procedures which are OAS CAHPS-eligible. The
HOPD or ASC should supply to the vendor monthly patient information files with all the
required data elements (see Table 4.1) for each of the preceding 3 to 6 months. The more months
the facility provides, the better the vendor will be able to estimate sample frame size and its
variability. A single month can be nonrepresentative of an ASC’s or HOPD’s patient size or
surgeries/procedures performed, so consider a range of months to guard against estimating
sampling rates that will yield a sampling frame that is either too large or too small.
In looking at the sample frame information for the 3 to 6 months that precede the first sample
month of participation, the vendor should apply the same sample frame construction criteria for
each month that it would apply for the first sample month. Note that in the first month’s sample
file, the rule that a patient cannot be sampled more than once in the 6-month period will not be a
constraint. In the second month of the 3- to 6-month test period, all patients sampled in the first
month will be excluded from the frame. Only patients not sampled the previous sample month
can be included on the sample frame for the second (and subsequent) month(s).
Once the vendor has a good understanding of the average monthly frame size, the vendor should
calculate the sampling rate using the formula
Sampling rate = (Required sample size) (frame size)
The required sample size, as explained above, is
Required sample size = (number of responses needed) (response rate)
Adjustments to the sampling rate may be needed over time to reach the annual target of 300
completes over each of the rolling four quarter periods. However, sampling rate should not
fluctuate wildly between months. All patients sampled in a sample month must be surveyed.
The target of 300 completed surveys is not a quota after which surveying or processing can stop.

IV. Sampling Procedures December 2015
42 Centers for Medicare & Medicaid Services Outpatient and Ambulatory Surgery CAHPS Survey Protocols and Guidelines Manual
Sampling Rates That Yield Above and Below the Minimum Number of
Patients
The targeted number of completed surveys for OAS CAHPS is 300 over a 12-month period.
Some HOPDs and ASCs may want to survey more of their patients. Reasons for doing so
include having more patients represented in the survey results or achieving a reliability target for
a component within the CCN, a type of patient or a surgical procedure. There is no upper limit to
the number of patients who may be surveyed for OAS CAHPS. However, the vendor should still
use a sampling rate and select a sample (rather than surveying all eligible patients each month) so
that the sample is evenly distributed across a 12-month period. As a reminder, samples that are
selected disproportionately―that is, with a different sampling rate for different strata―require
approval from the OAS CAHPS Survey Coordination team via an Exceptions Request Form.
As stated previously, the survey vendor should determine a sampling rate and select the sample
so that there is an even distribution of patients over a 12-month period. For some facilities with
low patient volumes, in some sample months the number of survey-eligible patients served may
be less than the number required by the sampling rate. In this case, it is acceptable to sample,
and then survey, all survey-eligible patients served during that sample month.
Generation of Random Numbers Needed for Sample Selection
All four methods of sampling approved for OAS CAHPS described in Step 4 require the use of
random numbers. Survey vendors should use a random number generator that is generally
accepted as having satisfied criteria of randomness. The random numbers should be generated
from the uniform distribution―each number having an equal probability of selection. Most
random number generators are pseudo-random number generators that repeat numbers after some
specified period. An acceptable random number generator will repeat only after many billions of
numbers are produced. An important feature of the random number generator is the “seed”
number used to start the cycle. The seed number must be known and retained as part of the
documentation vendors keep so that the sampling process can be reproduced for OAS CAHPS
Survey Coordination Team site visits. The selection of the seed number should be such that it
cannot be manipulated.
Survey vendors should use a reputable statistical program like SAS v9 either to select a sample
from a frame using its procedures for survey sample selection or to generate random numbers
that can be applied as described above. An appropriate seed often used is the clock time as
measured by the computer. This seed varies each fraction of a second but the value used is
documented by the program and is part of the output that can be retained.
Another reliable program, which runs under Windows, is RAT-STATS, developed by the
Department of Health and Human Service (DHHS) Inspector General’s Office. Survey vendors
can download this program at no cost from https://oig.hhs.gov/compliance/rat-stats/index.asp.

December 2015 IV. Sampling Procedures
Centers for Medicare & Medicaid Services 43 Outpatient and Ambulatory Surgery CAHPS Survey Protocols and Guidelines Manual
In addition to the RAT-STATS program, survey vendors may download a detailed user’s guide
and comprehensive manual describing how this program operates. There are many sampling
tools in the program. One module can simply produce a sample size, n, random integers between
1 and the frame size, using the computer clock to generate the seed, which is retained and
reported.
Both SAS and RAT-STATS are examples of readily available, high-quality, rigorously tested
tools for selecting samples randomly. Commonly available spreadsheet programs also have
random number generators; however, do not use these random number generators when selecting
monthly samples for the OAS CAHPS Survey because they do not generate a report of the seed
used. Note, however, that a spreadsheet is an acceptable way to present and manipulate the
sample frame.
It is also especially critical to document how the random start number was generated and how the
sample frame was sorted for survey oversight purposes. During oversight telephone calls or site
visits the OAS CAHPS Survey Coordination Team will check each vendor’s sampling
procedures and documentation, including documentation of all quality control checks conducted
by vendor staff.
The following are two acceptable ways to choose a random sample of patients from the sample
frame for the OAS CAHPS Survey.
Method 1—Generate N Random Numbers
Sort the sample frame of N eligible patients by any replicable method.
• Generate the N random numbers.
• Assign the random numbers in the order generated to each element in the frame.
• Re-sort the elements as ordered by the random numbers.
• Select the first n, the sample size required for the mode used.
In this way, the initial sort of the data does not affect the result, although a standard sort order
should always be used so that it does not appear that a frame has been altered. This method
requires generating as many random numbers as there are patients on the frame.
Method 2—Generate n random numbers
If the random number generator is able to produce integers from a range of values, given that N is
the size of the sample frame of eligible patients, we can use the following steps to select our
sample.

IV. Sampling Procedures December 2015
44 Centers for Medicare & Medicaid Services Outpatient and Ambulatory Surgery CAHPS Survey Protocols and Guidelines Manual
• Generate n distinct random integers whose values range from 1 to N, where n is the sample
size required for the mode used.
• Select the element of the frame that corresponds to the random number generated. For
example, if the random number 10 is generated then select the 10th element on the frame for
the sample.
• Continue selection of elements according to the random numbers generated until all n distinct
elements have been selected.
For Method 2, the initial sort of the data does affect the result and the vendor should clearly
document any sorting or file manipulation that occurred prior to random number generation.
Either Method 1 or Method 2 may be used for Simple Random Sampling (SRS), Proportionate
Stratified Random Sampling (PSRS) or Disproportionate Stratified Random Sampling (DSRS).
Method of Simple Random Sampling (SRS)
Appropriate Use: Simple random sampling can be used when there is a single component
within the CCN. For example, if there is only one eligible HOPD in the hospital’s CCN or only
one location in the ASC’s CCN, simple random sampling can be used.
Example: Northshore Ambulatory Surgery Center sees about 400 patients per month. It does
not share the CCN with any other surgery centers. From looking over the past 3-6 months it is
revealed that on average 350 patients per month are OAS CAHPS-eligible. Northshore is
required to obtain 25 completed surveys per month (300 completed surveys / 12 months = 25
completed surveys per month). Because the surgery center will be doing mixed-mode data
collection to which a 40% response rate is expected, it will need to sample 62.5 patients per
month (25 completes / .40 response rate = 62.5 selected patients), which is rounded up to 63.
Northshore’s sampling rate is 62.5/350, or 17.8%.
Use either Method 1 or Method 2 for selecting the patients from the sample frame.
If Method 1 is used, sort the month’s eligible patient list by the random number and select the
first 63 patients. If Method 2 is used, generate 63 random numbers between 1 and 350. Select
the elements from the frame that correspond to the random numbers generated.
Method of Stratified Systematic Sampling (SSS)
Appropriate Use: Vendors may use Stratified Systematic Sampling when a CCN is comprised
of two or more strata and patients from all strata need to be included in the OAS CAHPS sample
proportionally to their volume in the CCN, to make a valid sample. SSS is appropriate when the
strata are small and/or the facility does not wish to track results at the strata level.

December 2015 IV. Sampling Procedures
Centers for Medicare & Medicaid Services 45 Outpatient and Ambulatory Surgery CAHPS Survey Protocols and Guidelines Manual
Example ABC Surgery Center comprises three locations but they all bill under the same CCN.
Location A served 100 eligible patients in the sample month. Location B served 140 eligible
patients in the sample month. Location C served 80 eligible patients in the sample month. There
are 320 eligible patients in this sample month. Assume the vendor expects a 40% response rate.
The vendor will want to sample 63 patients each month to ensure about 25 completed surveys
each month to total approximately 300 completed surveys in a 12-month period.
63 patients * 40% response rate = 25 completed surveys
25 completed surveys *12 months = 300 completes in a year
The vendor needs to sample 63 patients in total from ABC Regional Medical Center, but the
locations A, B, and C should be representative (proportionate) in this total. The vendor should
calculate the proportion of patients from each location, as shown in Column B. The vendor
should then allocate the 63 patients proportionally to each location, as shown in Column C.
A.
Patient Count
B. Proportion of Patients on
Frame (Column A/320)
C. Number of Patients to be
Sampled (63 x Column B/100)
(numbers rounded up)
Location A 100 31.25 19.69 (round to 20)
Location B 140 43.75 27.56 (round to 28)
Location C 80 25 15.75 (round to 16)
Total 320 100 64
Although the vendor’s goal was to get 63 patients, it is important to round up to the next highest
integer. In this example, the sum in column C shows the total sample size ends up being 64
patients. Rounding down could result in not achieving the target of 300 completed interviews in
a 12-month period.
Once the vendor knows how many patients to sample from each location, the vendor will apply
the Systematic Sampling Process to the sample frame for each location. First, the vendor will
need to select a starting observation. To do this the vendor should use a random number
generator to apply random numbers to all frame members. Then the vendor should find the
lowest random number and the corresponding frame member will be the first sample member and
be the starting point of the systemic sample. Next, the vendor needs to calculate the size of the
interval. For Location A, the frame has 100 patients and 20 need to be sampled. The interval
will be 100 / 20 = 5. The vendor will take Sample Member #1 based on the random number
generation. Let’s say Patient #19 had the lowest random number and was the first patient
selected. Using the interval of 5, the vendor will go down the list and select Patient #24, then
Patient #29, Patient #34, and so on until 20 patients are selected. If the starting number is toward

IV. Sampling Procedures December 2015
46 Centers for Medicare & Medicaid Services Outpatient and Ambulatory Surgery CAHPS Survey Protocols and Guidelines Manual
the bottom of the list (e.g., Patient #90), the vendor would go to the top of the list and continue
down again, considering the list to be circular.
Vendors should not allow a patient to be selected multiple times. No sorting should occur. After
selecting the 20 patients from Location A, the vendor should repeat this process on the list of
eligible patients from Location B, and on the list of eligible patients from Location C. The
interval will always be 5.
Method of Proportionate Stratified Random Sampling (PSRS)
Appropriate use: There are two or more components (strata) within the CCN and patients from
all components need to be included in the OAS CAHPS sample proportionally to their volume in
the CCN to be a valid sample. Additionally,
• the HOPD or ASC would like to keep track of samples and results for each stratum, or
• the HOPD or ASC would like to designate other aggregates of operating units for tracking
while using the same sampling rate for each.
In PSRS, the same sampling rate must be applied to each stratum included in the sample. The
strata created must be large enough to support the same sampling rate in each stratum.
Example: Any-City Best Care Surgical Center comprises three locations (strata) but they all bill
under the same CCN. The surgical center serves 530 patients per month, across Facility A,
which serves 200 patients/month, Facility B, which serves 150 patients/month, and Facility C,
which serves 180 patients/month. Facility A has been in operation for 10 years, but Facilities B
and C were opened in the last 2 years. Any-City Best Surgical Center wants the survey estimates
from each location to have statistical precision and would like to track them separately over time.
These facilities each serves as a stratum for sampling. The vendor for this ASC selected a
sampling rate of approximately 45%, based on its prior experience with this client facility.
The sampling rate for the CCN as a whole is 45%, to get 239 sampled patients in the sample
month. Then the vendor will apply that same sampling rate to each stratum, as demonstrated
below:
• Location A: 200 eligible patients * 45% sampling rate = 90 patients sampled
• Location B: 150 eligible patients * 45% sampling rate = 68 patients sampled
• Location C: 180 eligible patients * 45% sampling rate = 81 patients sampled
The vendor would round any fractions of a patient up to the next largest whole number. For
example, a sample of 67.5 patients should become 68 sampled patients. The vendor should use

December 2015 IV. Sampling Procedures
Centers for Medicare & Medicaid Services 47 Outpatient and Ambulatory Surgery CAHPS Survey Protocols and Guidelines Manual
Method 1 or 2 to select the sample of 90 patients in Location A, 68 patients in Location B, and 81
patients in Location C.
This vendor uses mixed-mode administration and expects a response of rate of 40% (see
Table 4.2). If the vendor achieves a response rate of 40% the number of completed surveys will
be as follows:
• Location A: 62 patients sampled * 40% Response Rate = 36 completed surveys
• Location B: 68 patients sampled * 40% Response Rate = 28 completed surveys
• Location C: 81 patients sampled * 40% Response Rate = 33 completed surveys
The total number of completed surveys from this CCN in the sample month is 97, which greatly
exceeds the number of responses needed to get 300 completed interviews in a 12-month period.
Additionally, each stratum (location) has 25 or more completed surveys and is on target to
achieve 300 completed surveys in the 12-month period. There will be adequate statistical
precision to track estimates for each location.
Even if a facility does not have a large number of eligible patients in each stratum, it may still
use PSRS. It may not achieve enough completed surveys in a stratum to have good statistical
precision, but may still proceed so long as each stratum has a minimum of 10 sampled patients
each month.
Method of Disproportionate Stratified Random Sampling (DSRS)
Appropriate use: DSRS is another appropriate sampling option if a hospital, for example, with
multiple HOPDs wishes to achieve statistically precise numbers for each HOPD. To achieve as
good a level of precision for the separate units (in this example, the HOPDs) as required for the
CCN as a whole, each unit would have to have the same number of completed surveys as the
CCN as a whole. In this case, the sampling rate may be different for each stratum. To allow the
separate strata to be recombined to represent the HOPD or ASC as a whole the sampling rate for
each stratum must be reported in the data submitted to the OAS CAHPS Survey Coordination
Team. This will permit appropriate weighting of the respondents in computing results. Different
sampling rates in strata with particularly high or low ratings could otherwise distort the ratings.
If an HOPD or ASC chooses to use DSRS, its survey vendor must do the following:
• Complete and submit an Exceptions Request Form;
• Use the same name for each stratum in each month in the quarter;

IV. Sampling Procedures December 2015
48 Centers for Medicare & Medicaid Services Outpatient and Ambulatory Surgery CAHPS Survey Protocols and Guidelines Manual
• Make sure that each stratum has a minimum of 10 patients eligible to be included in the
survey during the sample month; and
• Provide to the OAS CAHPS Survey Data Center additional information about each stratum,
including the following:
◦ The name of the stratum;
◦ The total number of patients sampled in each stratum during the sample month;
◦ The total number of patients on the file submitted by the HOPD or ASC for that stratum;
◦ The number of patients in the stratum who were eligible for the survey during the sample
month; and
◦ The total number of patients sampled during each sample month.
Example: Memorial Hospital includes three eligible outpatient departments (strata): Same Day
Surgery (120/month), Outpatient (100/month), and Endoscopy (40/month). Memorial wants
statistically precise survey estimates for each department. Assume that the target for each
stratum is the same as for the CCN as a whole, that 25 is the target number of responses, and that
the expected response rate is 40 percent. Therefore, to get the same precision for each stratum
the sample size would be 62 for each of the three strata in this example. Because of the differing
patient volumes for these departments, the vendor’s sampling rate to achieve a sample size of 62
varies, as shown below:
• Same Day Surgery: 120 eligible patients * 51% sampling rate = 62 sampled patients of
whom 40% respond to get 25 completed interviews.
• Outpatient: 100 eligible patients * 62% sampling rate = 62 sampled patients of whom 40%
respond to get 25 completed interviews.
• Endoscopy : 40 eligible patients * 100% sampling rate = 40 sampled patients of whom 40%
respond to get 16 completed interviews.
Note that the survey vendor will report the number of patients eligible for the survey and the
number sampled to the OAS CAHPS Survey Data Center for use in computing weights for the
HOPD or ASC when the data are combined (this information is provided in the vendor’s data
submission, see Appendix L, XML File Layout for DSRS Header Record). Patients in Location
A had a lower probability of selection than those in Location B and C, and that will be accounted
for when the data from sample members in the strata are combined. Survey vendors should keep
in mind that a minimum of 10 eligible patients must be in each stratum for DSRS sampling to be
used.

December 2015 IV. Sampling Procedures
Centers for Medicare & Medicaid Services 49 Outpatient and Ambulatory Surgery CAHPS Survey Protocols and Guidelines Manual
The goal of the DSRS process is to obtain about 300 completed interviews for each stratum (e.g.,
location) in the 12-month period. This will provide sufficient statistical power to detect
differences at the stratum level. In this example, Location C will have lower statistical power
because the number of completes (only 16 are expected) will probably not reach 300 in the 12-
month period because of the lower number of eligible patients.
Step 6: Verify or Update Contact Information For Sampled Patients
We strongly recommend that survey vendors send patient mailing addresses of sampled patients
through an outside address service, such as the National Change of Address (NCOA) or a similar
provider, to confirm or update patient contact information. In addition, vendors conducting
either a telephone-only or mixed-mode data collection are urged to send the most updated
mailing addresses through a telephone number–provider service to attempt to obtain an updated
telephone number. Performing these quality control activities prior to the start of data collection
will result in fewer surveys returned as undeliverable and fewer unproductive telephone call
attempts.
Vendors are also reminded that in Step 2 they were to request contact information for all patients.
If an HOPD or ASC does not provide an address or telephone number for a patient on the
monthly patient information file and this omission was not rectified in Step 2, the vendor should
recontact the HOPD or ASC for the missing information for all patients contained on the ASC’s
or HOPD’s original data file. Asking for the information for all patients is important because the
vendor may not reveal to the facility which patients were selected for OAS CAHPS.
The vendor should also attempt to find an address and phone number for the sampled patients
who lack it. In most cases an HOPD or ASC will have the patient’s telephone number which was
obtained for the purpose of calling them to follow up on their recovery.
Vendors should also note that even if an address or telephone number cannot be obtained for a
patient, the patient is still eligible for inclusion on the sample frame (and in the survey if
sampled) if he or she meets all other survey eligibility criteria. That is, patients with missing
mailing addresses are considered eligible for the survey and can be sampled. If a patient sampled
for a Mail Only survey lacks an address the patient should be assigned the survey disposition
code of 330—Bad Address/Undeliverable Mail or No Address. If a patient sampled for a
telephone-only survey lacks a telephone number the patient should be assigned the survey
disposition code of 340—Wrong, Disconnected, or No Telephone Number. If a patient sampled
for a mixed-mode survey has a telephone phone number or an address he or she should proceed
with the survey; if the patient has neither he or she should be assigned the survey disposition
code of 340—Wrong, Disconnected, or No Telephone Number.

IV. Sampling Procedures December 2015
50 Centers for Medicare & Medicaid Services Outpatient and Ambulatory Surgery CAHPS Survey Protocols and Guidelines Manual
Step 7: Assign Unique Sample Identification Numbers
Survey vendors are responsible for assigning a unique alphanumeric sample identification (SID)
number to every sample member selected into each monthly sample. Procedures for assigning
unique SID numbers are described in Chapter IX and are repeated here in summary form only.
Vendors will track the status of a sampled patient/case throughout the data collection process
using the SID. Note that this number is different from the medical record number that HOPDs
and ASCs will provide to the survey vendor with other information needed to construct the
sample frame. The SID number cannot contain any combination of letters, numbers, or any
information that could link it with a particular sampled patient. For example, no part of the
patient’s name, address, date of birth, telephone number, Social Security number, visit dates, or
Medicare Number can be used or included in the SID number under any circumstances. The SID
number also cannot include any information that would identify the HOPD or ASC that served
the patient (i.e., ASC’s or HOPD’s name, address, CCN). Each month, vendors must use a new
set of unique SID numbers for the new set of patients sampled that month. Vendors must not
reuse the same SID numbers—that is, once a SID number is assigned, it should never be assigned
again to any sampled patient, either in the current quarter or in subsequent quarters.
Step 8: Finalize the Monthly Sample File and Initiate Data Collection Activities
As soon as the sampling activities described above have been completed, data collection for the
sample month should begin. Survey vendors must initiate the survey for each monthly sample
within 3 weeks (21 days) after the end of the sample month. Exceptions to this start date are
noted earlier in this chapter. All data collection for each monthly sample must be completed
within 6 weeks (42 days) after data collection begins. For mail-only and mixed-mode surveys,
data collection for a monthly sample must end 6 weeks after the first questionnaire is mailed.
For telephone-only surveys, data collection must end 6 weeks following the first telephone
attempt.
As noted earlier in this chapter, HOPDs and ASCs must provide the patient information file for
each sample month in time for the survey vendor to initiate the survey within 21 days after the
sample month closes. The HOPD or ASC can choose to submit the data needed on two separate
files. The first file must contain all patient information that the vendor will need to determine
the patients’ eligibility for the survey and for fielding the survey.The second file may contain
information needed at the facility-level for analysis, and it must be submitted to the vendor in
time for the vendor’s data submission to the OAS CAHPS Data Center.
Requirement That the First File Contain All Patient Information
The survey vendor needs to receive all patient and patient procedure information in the first file
and follow the process (described in Step 1) to remove known ineligible patients and procedures
from the frame so they are not sampled. Survey vendors should not initiate the OAS CAHPS

December 2015 IV. Sampling Procedures
Centers for Medicare & Medicaid Services 51 Outpatient and Ambulatory Surgery CAHPS Survey Protocols and Guidelines Manual
survey to all patients and determine at a later date which patients had a procedure that was OAS
CAHPS-eligible. Consultations, preadmission tests or follow-up tests are examples of ineligible
procedures. In general, vendors should use CPT codes/G codes as described in Step 1 to
determine if the surgery is OAS CAHPS-eligible but other methods may suffice. An example of
another method which could suffice is if a facility performed a limited set of procedures and all
were eligible. Please consult the Survey Coordination Team for guidance about the method you
would like to use in lieu of CPT coding to determine procedure eligibility.
If procedure ineligibility is revealed during data collection, a sampled patient can be given a
status code of ineligible. Nevertheless, survey vendors must have a process that excludes known
ineligible patients and procedures before the survey is initiated with them.
Preventing patient confusion is one reason for this policy. The OAS CAHPS survey directs
sample patients to think about the procedure that they had on a particular date. Experience
shows that patients whose reference date was for a secondary visit (e.g., preadmission test) and
not a procedure, or patients whose procedure was not OAS CAHPS-eligible, were confused by
the questionnaire topics.
The second main reason for this policy is that it ensures that the OAS CAHPS data reflect patient
experience with a surgery/procedure itself. If a patient is sampled for an ineligible procedure his
or her questionnaire data will fail to reflect the desired measures. Furthermore, patients may
only be sampled once every 6 months. If they are sampled for a visit that is later found out to be
ineligible, it is no longer possible to sample the eligible procedure visit.
Survey vendors and facilities should direct any questions on this procedure to the Survey
Coordination Team.
Sampling Issues and Errors
Based on national implementation of other CAHPS Surveys, CMS and the OAS CAHPS Survey
Coordination Team have observed some common misconceptions and problems with the
sampling process. The following is a list of some of these common misconceptions, paired with
the proper implementation method that survey vendors should use to avoid these issues during
the sampling process.
Patient Eligibility Criteria
1. Misconception: Patients with missing or incomplete mailing addresses or telephone
numbers are considered ineligible for the OAS CAHPS Survey.
Correct Implementation: Patients whose address is not a U.S. domestic address are
ineligible, but if they have an address which is missing or incomplete, or if their telephone
number is missing or incomplete, they are eligible to be included in the OAS CAHPS Survey

IV. Sampling Procedures December 2015
52 Centers for Medicare & Medicaid Services Outpatient and Ambulatory Surgery CAHPS Survey Protocols and Guidelines Manual
if they meet all other survey eligibility criteria. Vendors should attempt to obtain complete
contact information. We also recommend that survey vendors use address or telephone-
lookup services to confirm or obtain sample patients’ mailing address or telephone number.
If an address cannot be obtained the case should be finalized as a noncomplete of 330—Bad
Address/Undeliverable Mail or No Address, not as ineligible.
2. Misconception: If the HOPD or ASC did not serve any patients who met survey eligibility
criteria, the HOPD or ASC does not need to submit a sample file to its OAS CAHPS Survey
vendor for that sample month or notify them in any way.
Correct Implementation: HOPDs and ASCs participating in the OAS CAHPS Survey
should submit a monthly patient information file to their survey vendors for each sample
month or send an e-mail notification if no survey eligible patients were served in a particular
sample month. The survey vendor must, in turn, submit an OAS CAHPS data file to the
OAS CAHPS Survey Data Center for each sample month. Otherwise the HOPD or ASC will
be considered to have “missed” a month of survey participation.
3. Misconception: There is a variable called “number of eligible patients” that is part of
vendors’ data submission to the OAS CAHPS Data Center. In determining the value for that
variable, vendors should count patients who were identified as deceased or reported during
the survey that they did not receive care from the HOPD or ASC.
Correct Implementation: The “number of eligible patients” variable on the XML file must
reflect the number of presumed eligible patients who were included on the monthly patient
information file. Patients who were later identified as ineligible for the survey during the
data collection period should be noted by their final survey disposition code and should not
be removed from the “number of eligible patients” count.
4. Misconception. Patient age can be calculated based on their age as of the beginning of the
sample month.
Correct Implementation: Patient’s age must be calculated based on their age on the date of
surgery.
Sampling Procedures and Documentation Requirements
1. Misconception: It is acceptable for a survey vendor to use only the patient’s medical record
number (MRN) to identify patients who may have been listed more than once on a monthly
patient information file or to identify patients who have been sampled in the last 5 months.
Correct Implementation: Survey vendors are urged to use more than one variable to
identify patients for whom duplicate information is provided on the monthly patient
information file and to identify patients who have been sampled in the last 5 months. Using
the MRN together with another variable, including surgical code, date of procedure, patient

December 2015 IV. Sampling Procedures
Centers for Medicare & Medicaid Services 53 Outpatient and Ambulatory Surgery CAHPS Survey Protocols and Guidelines Manual
name, date of birth, telephone number, or address will ensure that the correct patient is
identified. Vendors may choose to perform the de-duplication process in multiple steps.
However, the MRN should never be applied as the sole variable in any of the steps; that is, it
should always be combined with another patient variable.
2. Misconception: SID number can be assigned more than once.
Correct Implementation: Once a SID number is assigned, it must never be used again. If a
patient is sampled more than once, a new SID number must be assigned to that patient each
time he or she is sampled. During the sampling process, all vendors should check the sample
file to make sure the same SID number is not assigned to two different patients and that the
SID has not been assigned in a preceding sample month.
3. Misconception: A survey vendor can conduct a census survey of all eligible patients during
the first sample month that an HOPD or ASC administers the OAS CAHPS Survey;
therefore, the survey vendor does not have to conduct the survey for the next 5 months.
Correct Implementation: As described in this chapter, survey vendors must select and
survey a sample of patients each sample month, including for very small HOPDs and ASCs.
Using a sampling rate and selecting a sample of patients each sample month will ensure that
an even distribution of patients is surveyed across a 12-month period.
4. Misconception: The sampling rate should be adjusted each month.
Correct Implementation: Survey vendors should adjust the sampling rate at the beginning
of a quarter unless the number of patients served is dramatically different (either lower or
higher) than for the preceding months in the quarter. The sampling rate should remain
constant during a quarter. If there is a huge difference in the number of patients served in a
month within a quarter, the survey vendor should follow up with the HOPD or ASC to make
sure that the information on the file is correct and determine the reason for the difference.
5. Misconception: The seed number (or random numbers generated) do not need to be saved.
Correct Implementation: Documentation of the seed number and the random number
generation and application process is a critical component of the OAS CAHPS sampling
protocols, as samples must be replicable for OAS CAHPS site visit team review.
6. Misconception: It is not necessary to retain documentation of ineligible sample members.
Correct Implementation: Vendors should retain a separate file or list of each patient
deemed ineligible and the reason the patient did not meet the eligibility criteria. This
information allows someone other than the person who selected the sample to conduct quality
control of the sample, checking to make sure the right patients were excluded. This
information is also subject to review during site visits.

IV. Sampling Procedures December 2015
54 Centers for Medicare & Medicaid Services Outpatient and Ambulatory Surgery CAHPS Survey Protocols and Guidelines Manual
Processing Patient Administrative Data
1. Misconception: If an HOPD or ASC changes/switches vendors, the current OAS CAHPS
Survey vendor must provide a file containing patient information about all patients sampled
in the preceding sample months so the new vendor can exclude those patients from the
sample frame.
Correct Implementation: OAS CAHPS Survey vendors are not required to provide the new
vendor with a file containing information about patients sampled in the last 5 months.
Sampling Quality Control Procedures
1. Misconception: Survey vendors who have automated the receipt and processing of monthly
patient information files and the sample selection process do not need to implement any
quality control procedures, because the programs and algorithms used for these processes
were fully tested after they were developed.
Correct Implementation: All survey vendors must have in place and implement quality
control procedures on the entire sampling process, including receipt and processing of the
monthly patient information files and sample selection for each sample month for each
HOPD or ASC client. This includes vendors who use automated systems/procedures for
sampling. One way to identify problems with the receipt or processing of a monthly patient
information file is to look at the history of the numbers of patients served and who met
survey eligibility requirements in preceding sample months.
If the numbers of patients served or eligible on the monthly patient information file is very
different from the numbers provided on files submitted in preceding months, this may be a
good indication that there may be a problem with the monthly patient information file
received. If there is an extreme variation in the number of patients served/eligible from one
month to the next, vendors are encouraged to contact the HOPD or ASC to determine the
reason for the extreme difference in numbers.
2. Misconception: Survey vendors may use the same staff who conduct the sampling process
to conduct quality control checks of the sample.
Correct Implementation: The quality control of each sample file should be performed by
someone other than the person who performed each task associated with the sample selection
process. Vendors are also encouraged to apply appropriate quality control checks on and test
all of the computer programs/systems the vendor uses to receive and process monthly files.

Centers for Medicare & Medicaid Services 55 Outpatient and Ambulatory Surgery CAHPS Survey Protocols and Guidelines Manual
V. MAIL-ONLY ADMINISTRATION PROCEDURES
Overview
This chapter describes the requirements and guidelines for implementing the mail-only mode of
survey administration for the Outpatient and Ambulatory Surgery CAHPS Survey (OAS
CAHPS). The chapter begins with a discussion of the mail survey protocol and schedule,
followed by a discussion of the requirements for producing all mailing materials, including
questionnaires, cover letters, and envelopes. Guidelines on how the questionnaire packages
should be mailed and data processing guidelines, including optical scanning and data entry, are
provided in this chapter. This chapter also provides suggestions for incorporating quality control
activities into the mail-only mode of survey administration. In this manual, patients included in
the sample are usually referred to as “sample members” or “patients.” However, in discussions
of survey processing and systems they may be referred to as “cases.”
Data Collection Schedule
Data collection for each sample member must be initiated no later than 3 weeks (21 days) after
the close of the sample month. The timing of a mail-only administration process is shown in
Table 5.1.
Questionnaires returned after the 6-week data collection period has ended should be considered
nonresponses and coded as such. Data collection must be closed for a sampled patient by six
weeks (42 calendar days) following the initiation of the survey.
Table 5.1 Mail-Only Administration Schedule and Protocol
Activity Timing
Mail initial questionnaire with cover letter to sample members
No later than 3 weeks (21 days) after the close of the sample month
Mail second questionnaire with cover letter to all sample members who do not respond to first questionnaire mailing
Approximately 3 weeks (21 days) after the first questionnaire is mailed
Complete data collection Six weeks (42 days) after the first questionnaire is mailed
Submit data files to the Centers for Medicare & Medicaid Services (CMS) via the OAS CAHPS Survey website
The second Wednesday of January, April, July, and October.

V. Mail-Only Administration Procedures December 2015
56 Centers for Medicare & Medicaid Services Outpatient and Ambulatory Surgery CAHPS Survey Protocols and Guidelines Manual
If the 21st day of the month falls on a weekend or holiday, vendors should make every attempt to
begin the survey on the business day prior to that weekend or holiday. However, it is acceptable
to mail the questionnaire on the first business day following the weekend or holiday if necessary.
If for some reason the survey cannot be initiated within 21 days after the sample month ends, the
vendor can initiate the survey within 26 days after the sample month ends. Vendors who are
initiating the survey between 21 and 26 days must complete and submit a Discrepancy
Notification Report (Chapter XV) to the OAS CAHPS Survey Coordination Team.
If the survey cannot be initiated within 26 days after the close of the sample month, CMS may
allow it to be initiated more than 26 days after the sample month ended. However, survey
vendors must first request permission to do so via e-mail to the OAS CAHPS Survey
Coordination Team. The e-mailed request should explain the reason for the delay, state when the
vendor will (if approved) initiate the survey, and request CMS’s approval. As noted in
Table 5.1, data collection must be closed 42 calendar days after the first questionnaire is mailed.
Note as well that the deadline for data submission is constant. This deadline will not shift later if
the vendor starts data collection late.
Questionnaires, Letters, and Envelopes
The mail survey version of the instrument is available in English, Spanish, and Chinese. At a
future date, the questionnaire will also be provided in one additional language, to be determined
based on the language needs of the sample members. All versions of the survey materials are
available on the OAS CAHPS Survey website at https://oascahps.org/.
Copies of the mail survey instrument and sample mail survey cover letters in English, Spanish,
and Chinese are also included in the appendices to this manual:
• sample mail survey cover letters, questionnaire and questionnaire in scannable format in
English, Appendix B;
• sample mail survey cover letters, questionnaire and questionnaire in scannable format in
Spanish, Appendix C;
• sample mail survey cover letters, questionnaire and questionnaire in scannable format in
Chinese, Appendix D; and
• Office of Management and Budget (OMB) Disclosure Notice in English, Spanish, and
Chinese in Appendix G.

December 2015 V. Mail-Only Administration Procedures
Centers for Medicare & Medicaid Services 57 Outpatient and Ambulatory Surgery CAHPS Survey Protocols and Guidelines Manual
Outpatient and Ambulatory Surgery CAHPS Survey Questionnaire
The OAS CAHPS Survey questionnaire contains 37 questions. The survey can be administered
as a standalone survey or can be combined with facility-specific questions as explained in
Chapter III. Questions 1 to 24 are considered the “core” OAS CAHPS Survey questions and
must be placed at the beginning of the questionnaire. Questions 25 to 37 are the “About You”
OAS CAHPS Survey questions and must be administered as a unit.
The OAS CAHPS Survey Questionnaire is available in Appendix B, and available in both
Microsoft Word and PDF formats on the OAS CAHPS Survey website at https://oascahps.org/.
Questionnaire Printing Requirements and Recommendations
The following are formatting and content requirements and recommendations for the OAS
CAHPS Survey Questionnaire. Survey vendors cannot deviate from questionnaire requirements.
Requirement Recommendation
Questions Every questionnaire must begin with the
core OAS CAHPS survey questions. n/a
No changes in wording are allowed to either
the OAS CAHPS Survey questions or to the
response (answer) choices.
n/a
If hospital outpatient departments (HOPDs)
and ambulatory surgery centers (ASCs) elect
to add their own questions they must follow
the guidelines in Chapter III. In terms of
placement of supplemental questions in the
questionnaire, they must be placed after the
“core” OAS CAHPS questions. They may
either be placed before or after the unit of
“About You” questions.
n/a
Formatting Questions and associated responses choices
may not be split across pages. n/a
Vendors must be consistent throughout the
questionnaire in formatting response options
either vertically or horizontally. If a vendor
elects to list the response options vertically,
this must be done for every question in the
questionnaire. Vendors may not format some
response options vertically and some
horizontally.
n/a
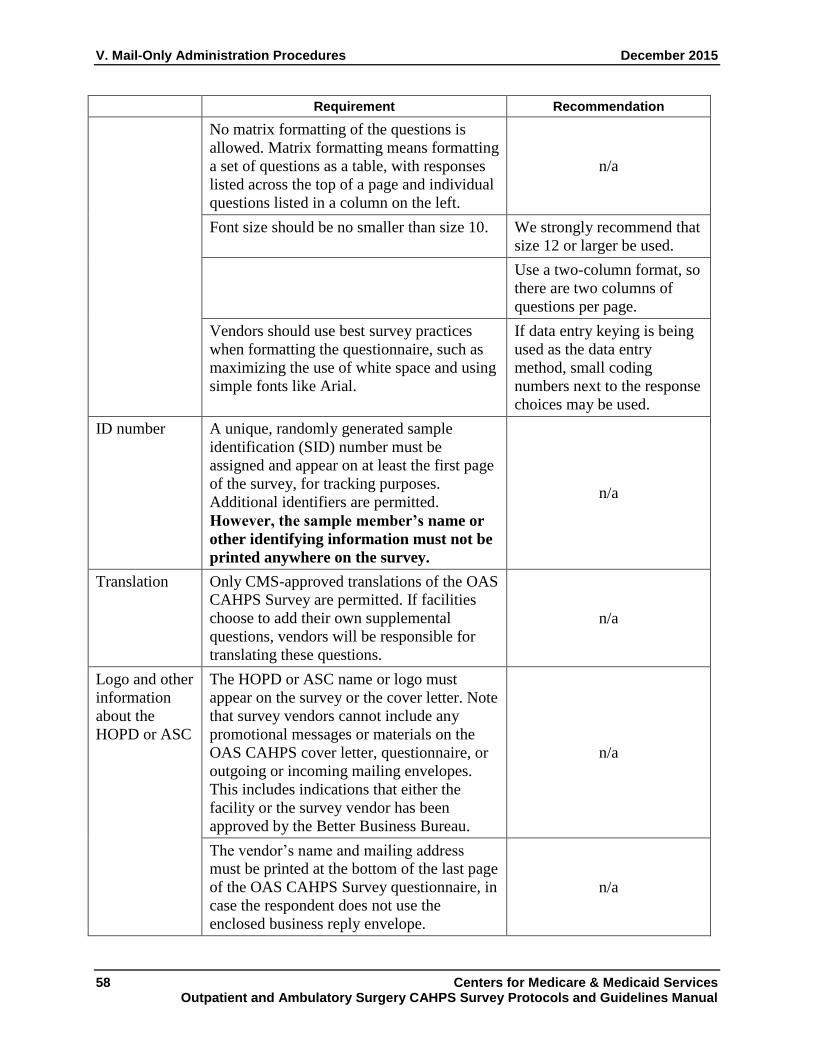
V. Mail-Only Administration Procedures December 2015
58 Centers for Medicare & Medicaid Services Outpatient and Ambulatory Surgery CAHPS Survey Protocols and Guidelines Manual
Requirement Recommendation
No matrix formatting of the questions is
allowed. Matrix formatting means formatting
a set of questions as a table, with responses
listed across the top of a page and individual
questions listed in a column on the left.
n/a
Font size should be no smaller than size 10. We strongly recommend that
size 12 or larger be used.
Use a two-column format, so
there are two columns of
questions per page.
Vendors should use best survey practices
when formatting the questionnaire, such as
maximizing the use of white space and using
simple fonts like Arial.
If data entry keying is being
used as the data entry
method, small coding
numbers next to the response
choices may be used.
ID number A unique, randomly generated sample
identification (SID) number must be
assigned and appear on at least the first page
of the survey, for tracking purposes.
Additional identifiers are permitted.
However, the sample member’s name or
other identifying information must not be
printed anywhere on the survey.
n/a
Translation Only CMS-approved translations of the OAS
CAHPS Survey are permitted. If facilities
choose to add their own supplemental
questions, vendors will be responsible for
translating these questions.
n/a
Logo and other
information
about the
HOPD or ASC
The HOPD or ASC name or logo must
appear on the survey or the cover letter. Note
that survey vendors cannot include any
promotional messages or materials on the
OAS CAHPS cover letter, questionnaire, or
outgoing or incoming mailing envelopes.
This includes indications that either the
facility or the survey vendor has been
approved by the Better Business Bureau.
n/a
The vendor’s name and mailing address
must be printed at the bottom of the last page
of the OAS CAHPS Survey questionnaire, in
case the respondent does not use the
enclosed business reply envelope.
n/a
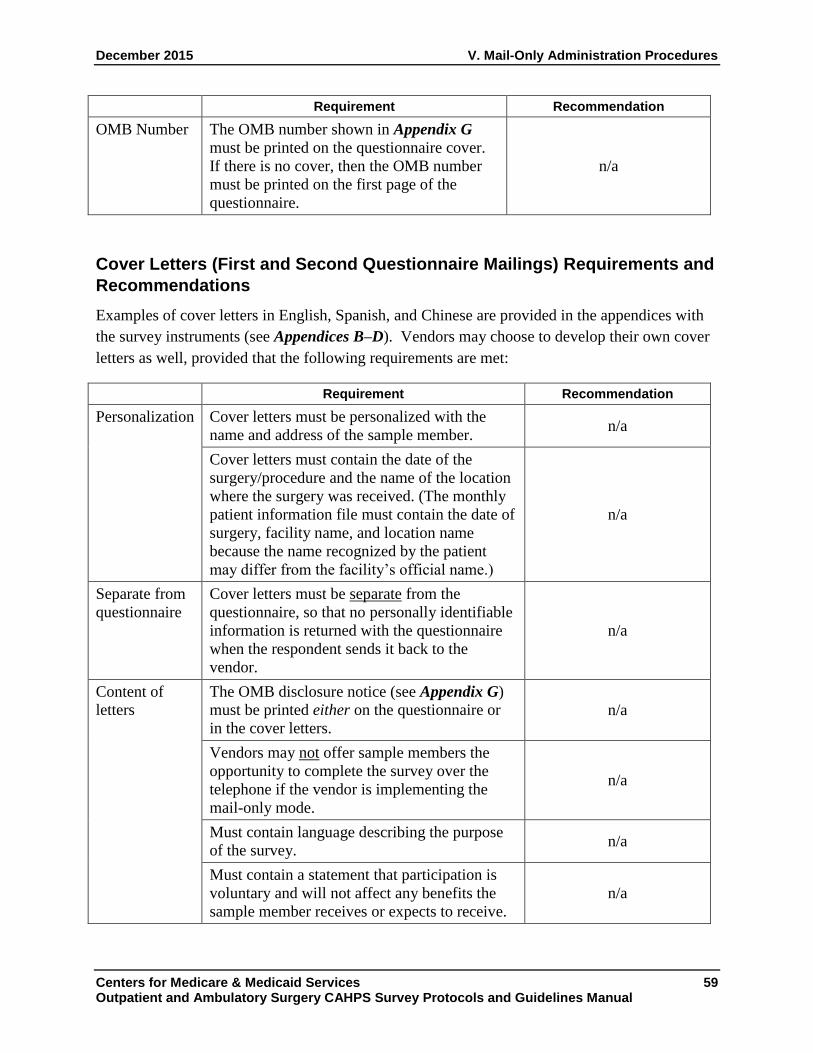
December 2015 V. Mail-Only Administration Procedures
Centers for Medicare & Medicaid Services 59 Outpatient and Ambulatory Surgery CAHPS Survey Protocols and Guidelines Manual
Requirement Recommendation
OMB Number The OMB number shown in Appendix G
must be printed on the questionnaire cover.
If there is no cover, then the OMB number
must be printed on the first page of the
questionnaire.
n/a
Cover Letters (First and Second Questionnaire Mailings) Requirements and
Recommendations
Examples of cover letters in English, Spanish, and Chinese are provided in the appendices with
the survey instruments (see Appendices B–D). Vendors may choose to develop their own cover
letters as well, provided that the following requirements are met:
Requirement Recommendation
Personalization Cover letters must be personalized with the
name and address of the sample member. n/a
Cover letters must contain the date of the
surgery/procedure and the name of the location
where the surgery was received. (The monthly
patient information file must contain the date of
surgery, facility name, and location name
because the name recognized by the patient
may differ from the facility’s official name.)
n/a
Separate from
questionnaire
Cover letters must be separate from the
questionnaire, so that no personally identifiable
information is returned with the questionnaire
when the respondent sends it back to the
vendor.
n/a
Content of
letters
The OMB disclosure notice (see Appendix G)
must be printed either on the questionnaire or
in the cover letters.
n/a
Vendors may not offer sample members the
opportunity to complete the survey over the
telephone if the vendor is implementing the
mail-only mode.
n/a
Must contain language describing the purpose
of the survey. n/a
Must contain a statement that participation is
voluntary and will not affect any benefits the
sample member receives or expects to receive.
n/a

V. Mail-Only Administration Procedures December 2015
60 Centers for Medicare & Medicaid Services Outpatient and Ambulatory Surgery CAHPS Survey Protocols and Guidelines Manual
Requirement Recommendation
Must contain language indicating that responses
from all survey participants will be grouped
together and these grouped data may be shared
with the HOPD or ASC, for purposes of quality
improvement.
n/a
Must contain language stating that if the
respondent needs help in reading the questions
or marking responses, a friend or family
member can assist them.
n/a
Must contain a toll-free customer support
telephone number, which will be staffed by the
survey vendor.
n/a
Printing The HOPD or ASC name (or logo) must appear
on the letters or the survey. Note that survey
vendors cannot include any promotional
messages or materials on the OAS CAHPS
cover letter, questionnaire, or outgoing or
incoming mailing envelopes. This includes
indications that either the facility or the survey
vendor has been approved by the Better
Business Bureau.
n/a
Signature on
the letters
A signature is required. We recommend that the
signature of an
appropriate official from
the HOPD or ASC be
printed on each cover
letter If this is not
possible, the signature
from an appropriate
official at the survey
vendor is acceptable.
Requests for
Survey in
Other
Language
n/a Survey vendors offering
an English, Spanish, and
Chinese version of the
questionnaire may add
language to the English
cover letter indicating that
a version of the
questionnaire is available
in those languages.

December 2015 V. Mail-Only Administration Procedures
Centers for Medicare & Medicaid Services 61 Outpatient and Ambulatory Surgery CAHPS Survey Protocols and Guidelines Manual
Mailing Requirements and Recommendations
Requirements and recommendations are described below. Vendors are expected to follow these
requirements to maximize response rates and ensure consistency in how the mail-only mode of
administration is implemented.
Requirement Recommendation
Questionnaire
contents
Each questionnaire mailing must contain a
personalized cover letter, questionnaire, and
postage-paid business reply envelope.
n/a
Envelopes Vendors are responsible for supplying both the
outgoing envelopes for the questionnaire
mailings and business-reply envelopes that
sample members will use to return their
completed surveys (i.e., they cannot be supplied
by the HOPD or ASC).
n/a
Mailing We recommend mailings
are sent with first-class
postage or indicia, to
ensure timely delivery
and maximize response
rates
Addresses Patients must have a U.S. domestic address to be
eligible to participate in the OAS CAHPS
Survey.
n/a
If the sample member’s address is missing or
incomplete, the vendor must follow up with the
HOPD or ASC to obtain the address. If an
address cannot be found, or the address that is
found is too incomplete for mailing, the vendor
should treat the patient as eligible and assign the
applicable final disposition code to the case: 330
– Bad Address/Undeliverable Mail, or No
Address (see Chapter IX).
To reduce the number of
missing addresses, we
recommend vendors
verify mailing addresses
obtained from the
facilities using
commercial address
update services, such as
the National Change of
Address (NCOA) or the
U.S. Postal Service
Zip+4 software.

V. Mail-Only Administration Procedures December 2015
62 Centers for Medicare & Medicaid Services Outpatient and Ambulatory Surgery CAHPS Survey Protocols and Guidelines Manual
Requirement Recommendation
We recommend vendors
attempt to identify a new
or updated address using
commercial address
vendors or the Internet
for any mail returned as
undeliverable in time to
include the sample
member in the second
mailing.
Schedule Mailings must follow the schedule specified for
the mail-only mode of administration—the first
questionnaire package must be mailed no later
than 3 weeks after the close of the sample
month; the second questionnaire to sample
members who do not respond to the first
questionnaire mailing must be mailed
approximately 3 weeks after the first
questionnaire mailing.
n/a
Data collection must end 6 weeks after the first
questionnaire has been mailed.
n/a
Incentives The use of incentives is not permitted. This
includes monetary and nonmonetary incentives.
n/a
Data Receipt, Data Entry, and Optical Scanning Requirements
The following guidelines are provided for receiving and tracking returned questionnaires and
entering the data using either data entry or optical scanning.
Requirement
Receipting The date the questionnaire was received from each sample member must be
entered into the data record created for each case on the data file.
Completed questionnaires should be logged into the tracking system in a
timely manner to ensure that sample members who respond to the first
mailing are excluded from the second questionnaire mailing.
Mailings that are returned in the mail as undeliverable must also be logged
into the tracking system. Although not required, we recommend vendors
attempt to identify a new or updated address using commercial address
vendors or the Internet for any mail returned as undeliverable in time to
include the sample member in the second mailing.

December 2015 V. Mail-Only Administration Procedures
Centers for Medicare & Medicaid Services 63 Outpatient and Ambulatory Surgery CAHPS Survey Protocols and Guidelines Manual
Requirement
If two questionnaires are received from the same sample member, vendors
should keep and use the questionnaire that has the more complete data,
regardless of which questionnaire is received first. If the two questionnaires
received contain the same amount of data (are equally complete), the vendor
should retain and use the first one received.
A final OAS CAHPS Survey disposition code (see Table 9.1 in Chapter IX)
must be assigned to each case.
Reviewing
received
questionnaires
for problems
Questionnaires should be visually reviewed prior to scanning or data entry
for notes/comments. Vendors should have more than one person who can
code or review comments and attach notes for proper disposition code
assignment.
We recommend that vendors attempt to identify a new or updated address
using commercial address vendors or the Internet for any mail returned as
undeliverable in time to include the sample member in the second mailing.
If a completed mail survey questionnaire is returned and the vendor realizes
that it was completed by proxy (i.e., there is a note written on the
questionnaire that a family member completed the questionnaire because the
patient had died, had moved to a nursing home, or had been incarcerated)
vendors should not scan a questionnaire for that sample member. This is
because proxy respondents are not permitted on OAS CAHPS. Vendors
should instead assign the applicable final disposition code to the case.
If a sample member were to die or become ineligible after completing the
questionnaire (vendors might learn of this through a comment written by a
family member on the questionnaire) that questionnaire is still an eligible
complete survey. Vendors should scan the questionnaire and assign the
applicable final disposition code indicating the completed survey.
Duplicate
questionnaires
The key entry process should not permit keying of duplicate questionnaires.
The scanning program should not permit scanning of duplicate
questionnaires.
Out-of-range
or invalid
responses
The key entry program should not permit out-of-range or invalid responses.
The scanning program should not permit out-of-range or invalid responses
Quality control For keying: All questionnaires should be 100 percent rekeyed for quality
control purposes. That is, for every questionnaire, a different keyer should
rekey the questionnaire and the data entry files of the two keyers should be
systematically compared. If any discrepancies between the two data entry
files are detected, a supervisor should resolve the discrepancy and ensure
that the correct value is stored in the data.

V. Mail-Only Administration Procedures December 2015
64 Centers for Medicare & Medicaid Services Outpatient and Ambulatory Surgery CAHPS Survey Protocols and Guidelines Manual
Requirement
For optical scanning: A sample of questionnaires (minimum of 10 percent)
should be systematically compared with the original hardcopy survey. Any
discrepancies between the scan and the hardcopy should be reconciled by a
supervisor. This serves as a quality control measure that the scanning
program is capturing the hardcopy correctly.
Additionally, the survey responses captured in the database for a sample of
questionnaires (minimum of 10 percent) should be systematically compared
to scanned image for that case. This can be done either by visually
examining the scanned image and the data to reveal inconsistencies, or by
rescanning and noting whether the data from the original matches the data
from the rescan. This serves as a quality control measure that the scanning
program is translating the response marks in the scanned image to the data
file consistently and correctly.
Interpreting
blanks and
ambiguous
survey
responses
The following apply for both keying and optical scanning:
If a response mark falls between two answer choices but is clearly closer to
one answer choice than to another, select the response that is closest to the
marked response.
If two responses are checked for the same question, select the one that
appears darkest. If it is not possible to make a determination, leave the
response blank and code as “missing” rather than guessing.
If a mark is between two answer choices but is not clearly closer to one
answer choice, code as “missing.”
If a response is missing, leave the response blank and code as “missing.”
Open-ended
responses
The decision on whether to key or scan the responses to open-ended survey
items, specifically, the “Other language” (response option 2) in Q35 and the
“Helped in some other way” (response option 5) in Q37, is up to each
individual HOPD or ASC. Vendors will not be required to key or scan and
include responses to open-ended survey items on the data files submitted to
the OAS CAHPS Survey Data Center.
CMS, however, encourages survey vendors to review the open-ended entries
so they can provide feedback to the Coordination Team about adding
additional preprinted response options to these survey items if needed.
It follows that if the vendor includes the Consent to Share Identifying
Information question in the mail survey questionnaire, we do not require that
the vendor key or scan the response to that question. However, we do
recommend it for the vendor’s own documentation.
Answers to the Consent to Share Identifying Information question will not
be included on the data files submitted to the OAS CAHPS Survey Data
Center.

December 2015 V. Mail-Only Administration Procedures
Centers for Medicare & Medicaid Services 65 Outpatient and Ambulatory Surgery CAHPS Survey Protocols and Guidelines Manual
Staff Training
All staff involved in the mail survey implementation, including support staff, must be thoroughly
trained on the survey specifications and protocols. A copy of relevant chapters of this manual
should be made available to all staff as needed. In particular, staff involved in questionnaire
assembly and mailout, data receipt, and data entry must be trained on:
• use of relevant equipment (case management systems for entering questionnaire receipts,
scanning equipment, data entry programs);
• OAS CAHPS Survey protocol specific to their role (for example, contents of questionnaire
package, how to document or enter returned questionnaires into the tracking system);
• decision rules and coding guidelines for returned questionnaires (see Chapter IX); and
• proper handling of hardcopy and electronic data, including data storage requirements (see
Chapter VIII).
Staff involved in providing customer support via the toll-free telephone number should also be
trained on the accurate responses to commonly asked questions, how to respond to questions
when customer support does not know the answer, and the rights of survey respondents. If the
OAS CAHPS Survey is being offered in a language other than English, customer support staff
should also be able to handle questions via the toll-free telephone number in that language.
Telephone interviewer training requirements are described in more detail in Chapter VI of this
manual. Please refer to that chapter for more information on training customer support staff.
Quality Control Guidelines for Mail-only Survey
The following steps are required or recommended as a means of incorporating quality control
into the mail-only survey administration procedures. Quality control checks should be
conducted by a different staff person than the one who completed the task. Some of these are
mentioned earlier in the chapter.
Required
• Check a minimum of 10 percent of all printed materials to ensure the quality of the
printing—that is, make sure there is no smearing, misaligned pages, duplicate pages, or stray
marks on pages.
• Check a minimum of 10 percent of all outgoing questionnaire packages to ensure that all
package contents are included and the same unique SID number appears on both the cover
letter and the questionnaire.
V. Mail-Only Administration Procedures December 2015
66 Centers for Medicare & Medicaid Services Outpatient and Ambulatory Surgery CAHPS Survey Protocols and Guidelines Manual
• For vendors that are scanning: a sample of questionnaires (minimum of 10 percent) should
be compared with the original hardcopy survey as a quality control measure. Additionally,
for a sample of questionnaires (minimum of 10 percent) the response data resulting from the
scanning program should be compared to the scanned image for that case. Any discrepancies
from either of these should be reconciled by a supervisor.
• For vendors who are keying: all questionnaires should be 100 percent rekeyed for quality
control purposes. That is, for every questionnaire, a different keyer should rekey the
questionnaire and the data entry files from the two keyers should be systematically compared
to ensure that all entries are accurate. If any discrepancies are observed, a supervisor should
resolve the discrepancy and ensure that the correct value is stored in the data.
Recommended
• Verify that sample members’ mailing addresses provided by the HOPD or ASC are correct
by using commercial address update services, such as the National Change of Address or the
U.S. Postal Service Zip+4 software. Cases with incomplete mailing addresses must remain
in the sample.
• “Seed” each mailing. That is, include the name and address of designated vendor staff in
each mailing file to assess the completeness of the questionnaire package and timeliness of
package delivery.
• Before submitting XML data to the OAS CAHPS Data Center, we highly recommend
vendors review a sample of cases comparing responses recorded on the hardcopy
questionnaire to responses scanned to the response codes which appear in the XML files.
This quality control step will ensure that the responses included in the XML files accurately
reflect the patients’ responses to the survey questions.
• Vendors are urged to develop a way to measure error rates for their data receipt staff (in
terms of recognizing marginal notes and passing these on to someone for review), for data
entry or scanning operators, and for coders. Vendors should then work with their staff to
minimize error rates. The Coordination Team will request information about data receipt and
processing error rates during site visits to survey vendors.
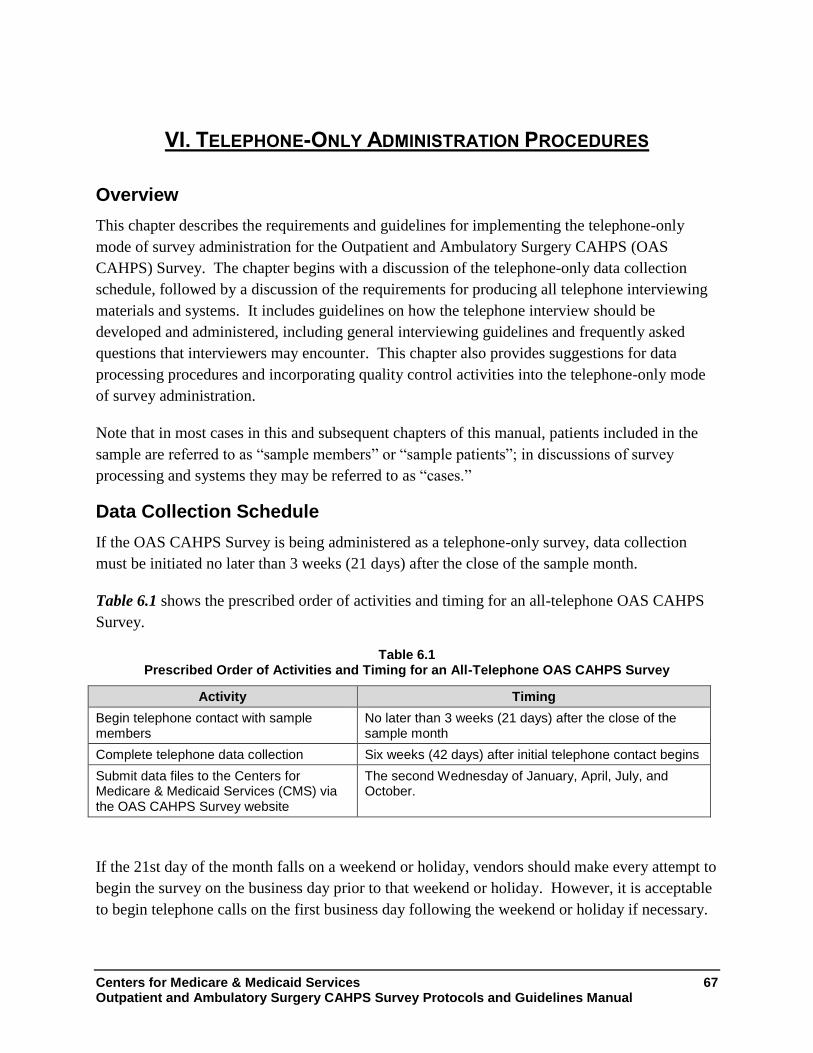
Centers for Medicare & Medicaid Services 67 Outpatient and Ambulatory Surgery CAHPS Survey Protocols and Guidelines Manual
VI. TELEPHONE-ONLY ADMINISTRATION PROCEDURES
Overview
This chapter describes the requirements and guidelines for implementing the telephone-only
mode of survey administration for the Outpatient and Ambulatory Surgery CAHPS (OAS
CAHPS) Survey. The chapter begins with a discussion of the telephone-only data collection
schedule, followed by a discussion of the requirements for producing all telephone interviewing
materials and systems. It includes guidelines on how the telephone interview should be
developed and administered, including general interviewing guidelines and frequently asked
questions that interviewers may encounter. This chapter also provides suggestions for data
processing procedures and incorporating quality control activities into the telephone-only mode
of survey administration.
Note that in most cases in this and subsequent chapters of this manual, patients included in the
sample are referred to as “sample members” or “sample patients”; in discussions of survey
processing and systems they may be referred to as “cases.”
Data Collection Schedule
If the OAS CAHPS Survey is being administered as a telephone-only survey, data collection
must be initiated no later than 3 weeks (21 days) after the close of the sample month.
Table 6.1 shows the prescribed order of activities and timing for an all-telephone OAS CAHPS
Survey.
Table 6.1 Prescribed Order of Activities and Timing for an All-Telephone OAS CAHPS Survey
Activity Timing
Begin telephone contact with sample members
No later than 3 weeks (21 days) after the close of the sample month
Complete telephone data collection Six weeks (42 days) after initial telephone contact begins
Submit data files to the Centers for Medicare & Medicaid Services (CMS) via the OAS CAHPS Survey website
The second Wednesday of January, April, July, and October.
If the 21st day of the month falls on a weekend or holiday, vendors should make every attempt to
begin the survey on the business day prior to that weekend or holiday. However, it is acceptable
to begin telephone calls on the first business day following the weekend or holiday if necessary.

VI. Telephone-Only Administration Procedures December 2015
68 Centers for Medicare & Medicaid Services Outpatient and Ambulatory Surgery CAHPS Survey Protocols and Guidelines Manual
OAS CAHPS Survey vendors must make a concerted effort to initiate the survey for each sample
month within 21 days after the sample month ends. This means that phone contacting should
begin by the 21st day after the end of the sample month.
If for some reason the survey cannot be initiated within 21 days after the sample month ends, the
vendor can initiate the survey within 26 days after the sample month ends. Vendors that are
initiating the survey between 21 and 26 days must complete and submit a Discrepancy
Notification Report (Chapter XV) to the OAS CAHPS Survey Coordination Team.
CMS may allow the survey to be initiated more than 26 days after the sample month ended.
However, survey vendors must first request permission to do so via e-mail to the OAS CAHPS
Survey Coordination Team. The e-mailed request should explain the reason for the delay, state
when the vendor will (if approved) initiate the survey, and request CMS’s approval.
As noted in Table 6.1, data collection must be closed 42 calendar days after the telephone survey
begins. Note as well that the deadline for data submission is constant. This deadline will not
shift later if the vendor starts data collection late.
Telephone Interview Development Process
The following paragraphs describe the requirements for producing all materials and systems
needed for the telephone-only survey. The telephone interview script in English, Spanish, and
Chinese in both Microsoft Word and PDF formats are available on the OAS CAHPS Survey
website at https://oascahps.org/.
A list of questions that are frequently asked by sample members and suggested answers to those
questions are included in Appendix H (English) and Appendix J (Spanish). Some general
guidelines for telephone interviewer training and monitoring are provided in Appendix I.
Specific requirements and guidelines associated with the telephone survey administration are
discussed below.
Telephone Interviewing Systems
An electronic telephone interviewing system means that the interviewer reads from and enters
responses into a computer program. Using an electronic system encourages standardized
interviewing and monitoring of interviewers. Survey vendors using a telephone-only survey
mode must use an electronic system to administer the OAS CAHPS Survey. Paper-and-pencil
administration is not permitted for telephone surveys. To ensure that sample members are
called at different times of the day and across multiple days of the week, vendors must also have
a survey management system. Ideally, the electronic system will be linked to the survey
management system so that cases can be tracked, appointments set and called back at appropriate
times, and pending and final case status easily accessed for any case.

December 2015 VI. Telephone-Only Administration Procedures
Centers for Medicare & Medicaid Services 69 Outpatient and Ambulatory Surgery CAHPS Survey Protocols and Guidelines Manual
Predictive or automatic dialers are permitted, as long as they are compliant with Federal Trade
Commission and Federal Communications Commission regulations, and as long as respondents
can easily interact with a live interviewer. For more information about Federal Trade
Commission and Federal Communications Commission regulations please visit
https://www.ftc.gov/ and https://www.fcc.gov/.
Telephone Interview Script
Survey vendors are provided with standardized telephone scripts in Appendix B (English) and
Appendix C (Spanish). These scripts include the introductory screens in addition to the survey
questions.
The OAS CAHPS Survey questionnaire script contains 35 questions. The survey can be
administered as a standalone survey or can be combined with facility-specific questions as
explained in Chapter III. Questions 1 to 24 are considered the “core” OAS CAHPS Survey
questions and must be placed at the beginning of the questionnaire. Questions 25 to 35 are the
“About You” OAS CAHPS Survey questions and must be administered as a unit.
Note that the OAS CAHPS telephone interview script contains only 35 questions and the mail
survey contains 37 questions. The mail survey questionnaire contains questions that ask if
anyone helped the sample member to complete the survey (Questions 36 and 37). These two
questions are not applicable if the survey is administered by telephone.
The following are content and programming requirements and recommendations for the OAS
CAHPS Survey Questionnaire. Note that survey vendors cannot deviate from questionnaire
requirements.
• Every questionnaire must begin with the core OAS CAHPS questions. They must be
administered in the order in which they appear.
• No changes in wording are allowed for either the OAS CAHPS Survey questions or to the
response choices.
• Hospital outpatient departments (HOPDs) and ambulatory surgery centers (ASCs) may add
their own questions, following the guidelines in Chapter III. In terms of placement of
supplemental questions in the questionnaire, note that they must be placed after the “core”
OAS CAHPS questions. They may either be placed before or after the unit of “About You”
questions.
• Only CMS-approved translations of the OAS CAHPS Survey are permitted, although if
facilities choose to add their own supplemental questions, vendors will be responsible for
translating these questions.

VI. Telephone-Only Administration Procedures December 2015
70 Centers for Medicare & Medicaid Services Outpatient and Ambulatory Surgery CAHPS Survey Protocols and Guidelines Manual
Telephone Interviewing Requirements
Telephone interviewing requirements and recommendations for the OAS CAHPS Survey
interview are described below. Vendors are expected to follow these requirements to maximize
response rates and to ensure consistency in how the telephone-only mode of administration is
implemented. Vendors are also advised to keep an eye on response rates, to assess whether calls
are being scheduled optimally across the data collection period. A low response rate may be
indicative of calls being spaced too closely together, rather than spread across a number of weeks
Telephone Contact
• Vendors must attempt to contact every patient in the sample. Vendors must make a
minimum of five telephone contact attempts for each sampled case, unless the sample
member refuses or the vendor learns that the sample member is ineligible to participate in the
survey.
• A telephone contact attempt is defined as one of the following:
◦ the telephone rings six times with no answer or an answering machine is reached;
◦ the interviewer reaches a household member and is told that the sample member is not
available to take the call;
◦ the interviewer reaches the sample member and is asked to schedule a call-back at a later
date; or
◦ the interviewer gets a busy signal on each of three consecutive phone call attempts,
spaced at least 20 minutes apart.
• Vendors may make more than one phone call in one 7-day period but cannot make all five
attempts in one 7-day period. Scheduling calls to take place over a longer period of time
could reach patients who may be unavailable the first week of the data collection period.
• Contact with a sample member may be continued after five attempts if the fifth attempt
results in a scheduled appointment with the sample member, as long as the appointment is
within the data collection period.
• Phone calls must be made at different times of the day (i.e., morning, afternoon, and evening)
and different days of the week throughout the data collection period.
• Interviewers may not leave voicemail messages on answering machines or leave messages
with household members.
• Interviewers may tell household members that they are calling about “a study on health
care.”

December 2015 VI. Telephone-Only Administration Procedures
Centers for Medicare & Medicaid Services 71 Outpatient and Ambulatory Surgery CAHPS Survey Protocols and Guidelines Manual
• Vendors must be able to provide a phone call log that keeps track of the date and time phone
calls were made for each sample member.
• If the vendor finds out that a sample member is ineligible for the OAS CAHPS Survey, the
vendor must immediately stop further contact attempts with that sample member.
• Telephone survey data collection for each monthly sample must begin no later than 3 weeks
from the close of the sample month and must be completed within 6 weeks from the initial
telephone attempt.
• The use of incentives—monetary or nonmonetary—is not permitted.
• Proxy respondents are not permitted on OAS CAHPS. If a sample member is incapable of
responding to the telephone interview because of mental or physical impairments such as
difficulty hearing, the case should be closed using code 240 or “Mentally/Physically
Incapable” and end the interview. If a sample member is capable of responding but just
needs some help to do so, a friend or family member may help, but cannot respond on his or
her behalf.
• If a respondent begins the interview but cannot complete it during the call for a reason other
than a refusal, the vendor should follow up with the respondent to complete the entire
interview. The interviewer should follow up even if the respondent answered enough
questions in the interview for the case to pass the completeness criteria. It is especially
important to complete the questions in the “About You” section of the questionnaire, because
data from some of those questions will be used in patient-mix adjustment.
• The vendor must be able to offer the interview in any of the approved languages for which an
HOPD or ASC has contracted, even if the language is different from the language that the
HOPD or ASC believes the sample member will require. That is, the vendor must be able to
easily switch to accommodate a respondent’s language preference. For example, if the initial
contact is in English but the respondent prefers to conduct in Spanish, the vendor must be
able to switch to Spanish.
• Sample members are still eligible even if they have missing, incomplete, or foreign phone
numbers. The vendor should contact the HOPD or ASC to obtain the telephone number for
the address of the patient. If the HOPD or ASC cannot provide this number, the vendor
should attempt to obtain a telephone number for the patient from other sources (directory
assistance, Internet directories, etc.). If the vendor still cannot obtain a telephone number,
the vendor should code the case as code 340–wrong, disconnected, no telephone number.
• If a respondent decides after he or she has answered some of the questions in the telephone
interview that he or she does not wish to participate in the survey any longer, the vendor
should code the case as a refusal. The vendor should not use the partial data that were

VI. Telephone-Only Administration Procedures December 2015
72 Centers for Medicare & Medicaid Services Outpatient and Ambulatory Surgery CAHPS Survey Protocols and Guidelines Manual
obtained before the interview was ended. This protocol applies even if the respondent
answered enough questions in the interview for the case to pass the completeness criteria.
Note that this situation is different from the respondent saying that he or she does not wish to
continue an interview. If the respondent breaks off the interview but does not state that he or
she does not wish to participate in the survey, the data may be used as long as the interview
meets the completeness criteria. The vendor may then code the case as a completed
interview if the case passes the completeness criteria; otherwise it should be coded as a
breakoff/partial data.
Contacting Difficult-to-Reach Sample Members
• Although not required, we strongly recommend that survey vendors verify telephone
numbers obtained from HOPDs and ASCs, using a commercial address/telephone database
service or directory assistance.
• We recommend that vendors attempt to identify a new or updated telephone number for any
sample member whose telephone number is no longer in service when called and for any
sample members who have moved so that the sample members can be contacted prior to the
end of the data collection period.
• If the sample member’s telephone number is incorrect, the interviewer may ask the person
who answers the phone for the sample member’s phone number.
• If the sample member is temporarily ill, on vacation, or unavailable during initial contact, the
interviewer should attempt to recontact the sample member before the data collection period
ends. If the sample member cannot be reached before the data collection period ends, code
the case as 350, “No Response After Maximum Attempts.”
• If the sample member does not speak a language that has an approved translation for OAS
CAHPS, the interviewer should thank the sample member for his or her time, end the
interview, and code the case as 230, “Ineligible: Language Barrier.”
• If a sample member is physically or mentally incapable of responding by telephone, the case
should be finalized and coded as 240.
• For sample members who are living in institutions (assisted living, group homes, etc.), OAS
CAHPS Survey vendors should contact the HOPD or ASC to obtain a direct-dial telephone
number. If the HOPD or ASC cannot provide a direct-dial telephone number for the patient,
try to obtain the sample member’s telephone number using other sources, such as a telephone
number lookup service, directory assistance, or Internet telephone survey directories. If
vendors cannot obtain a telephone number for the patient, they should assign a disposition
code of Missing/Disconnected Number to the case. As a reminder, sample members living in
nursing homes are ineligible.
December 2015 VI. Telephone-Only Administration Procedures
Centers for Medicare & Medicaid Services 73 Outpatient and Ambulatory Surgery CAHPS Survey Protocols and Guidelines Manual
Distressed Respondent Procedures
It is critically important that survey vendors develop a “distressed respondent protocol,” to be
incorporated into all interviewer and help desk training. Handling distressed respondent
situations requires balancing keeping personally identifiable information and private health
information confidential and helping a person who needs assistance. For survey research
organizations, best interviewing practices recommend having a distressed respondent protocol in
place for handling distressed respondents, which balances the respondent’s right to
confidentiality and privacy and providing assistance, if the situation indicates that the
respondent’s health and safety are in jeopardy.
Therefore, each approved OAS CAHPS Survey vendor is expected to have procedures in place
for handling distressed respondent situations and to follow those procedures. CMS and the OAS
CAHPS Survey Coordination Team cannot provide guidelines on how to evaluate or handle
distressed respondents. However, survey vendors are urged to consult with their organization’s
Committee for the Protection of Human Subjects Institutional Review Board for guidance. In
addition, professional associations for researchers, such as the American Association of Public
Opinion Researchers (AAPOR), may be able to provide guidance regarding this issue. The
following is an excerpt from AAPOR’s website that lists resources for the protection of human
subjects. More information about protection of human subjects is available at AAPOR’s website
at http://www.aapor.org.7
• The Belmont Report (guidelines and recommendations that gave rise to current federal
regulations)
• Federal Regulations Regarding Protection of Human Research Subjects (45 CFR 46) (also
known as the Common Rule)
• Federal Office for Human Research Protections
• National Institutes of Health Human Participant Investigator Training (although the site
appears to be for cancer researchers, it is the site for the general investigator training used by
many institutions)
• University of Minnesota Web-Based Instruction on Informed Consent
7 The American Association of Public Opinion Researchers website at
http://www.aapor.org/Additional_IRB_Resources.htmt, July 2010.

VI. Telephone-Only Administration Procedures December 2015
74 Centers for Medicare & Medicaid Services Outpatient and Ambulatory Surgery CAHPS Survey Protocols and Guidelines Manual
Telephone Interviewer Training
Vendors must provide training to all telephone interviewing and customer support staff prior to
starting telephone survey data collection activities. Telephone interviewer and customer support
staff training must include the following:
• teaching interviewers how to establish rapport with the respondent;
• teaching interviewers the content and purpose of the interview so that they can effectively
communicate this information to the sampled patients;
• teaching interviewers to administer the interview in a standardized format, which includes
reading the questions as they are worded, not providing the respondent with additional
information that is not scripted, maintaining a professional manner, and adhering to all
quality control standards;
• teaching interviewers how to use effective neutral probing techniques;
• teaching interviewers to use the frequently asked questions document so that they can answer
questions in a standardized format; and
• teaching multilingual customer support staff how to handle questions in English and the other
language(s) in which the survey is being offered.
Survey vendors should also provide telephone survey supervisors with an understanding of
effective quality control procedures to monitor and supervise interviewers.
Vendors must conduct an interviewer certification process of some kind—either oral, written, or
both—for each interviewer and customer service staff member prior to permitting that person to
make or take calls on the OAS CAHPS Survey. The certification should be designed to assess
the interviewer’s level of knowledge and comfort with the OAS CAHPS Survey instrument and
ability to respond to sample members’ questions about the survey. Documentation of training
and certification of all telephone interviewers and customer support staff and outcomes will be
subject to review during oversight visits by the OAS CAHPS Survey Coordination Team.
Telephone Data Processing Procedures
The following guidelines are provided for ensuring that the telephone interview data are properly
processed and managed.
Telephone Data Processing Requirements
• A unique sample identification number (SID) must be assigned to each case and included in
the case management system and on the final data file for each sample member.

December 2015 VI. Telephone-Only Administration Procedures
Centers for Medicare & Medicaid Services 75 Outpatient and Ambulatory Surgery CAHPS Survey Protocols and Guidelines Manual
• Vendors must enter the date of the interview with each sample member in the survey
management system or in the interview data.
• Vendors must be able to link each telephone interview to their survey management system,
so that appropriate variables, such as the language in which the survey was conducted, can be
pulled into the final data file.
• Vendors must de-identify all telephone interview data when the data are transferred into the
final data file for delivery. Identifiable data include respondent names and contact
information.
• Vendors must assign a final OAS CAHPS Survey status or disposition code to each case (see
Chapter IX for a list of these codes) and include a final disposition code for each sampled
case in the final data file. It is up to the vendor to develop and use a set of pending
disposition codes to track actions on a case before it is finalized appropriately—pending
disposition codes are not specified in the OAS CAHPS Survey protocol.
Telephone-Only Quality Control Guidelines
The following activities are methods to incorporate quality control into the telephone-only
survey administration procedures. Quality control of telephone interviewers and customer
support staff should include the following activities:
• OAS CAHPS requires that survey vendors thoroughly test the electronic telephone
interviewing system before beginning the OAS CAHPS survey. Testing will vary from
system to system, but includes at a minimum comparing each screen to the Telephone Script
to verify that the questions and answer choices are faithful to the script, checking each
question to ensure that the answers input match the data exported, and checking that a
respondent is automatically routed to the next appropriate question.
• Vendors are required to keep written documentation that all telephone interviewing and
customer support staff have been properly trained prior to interviewing. Copies of
interviewer certification exam scores should be retained as well. Documentation should be
maintained for any retraining required and will be subject to review during oversight visits.
• Although not required, we recommend that vendors conduct regular Quality Circle meetings
with telephone interviewing and customer support staff to obtain feedback on issues related
to telephone survey administration or handling inbound calls.
• Survey vendors must establish and communicate clear telephone interviewing quality control
guidelines for their staff to follow. These guidelines should be used to conduct the
monitoring and feedback process, and should include clear explanations of the consequences

VI. Telephone-Only Administration Procedures December 2015
76 Centers for Medicare & Medicaid Services Outpatient and Ambulatory Surgery CAHPS Survey Protocols and Guidelines Manual
of not following protocols, including actions such as removal from the project or termination
of employment.
• Vendors are required to silently monitor a minimum of 10 percent of all telephone interviews
to ensure that correct administration procedures are being followed.
• Supervisory staff monitoring telephone interviewers should use the electronic system to
observe the interviewer conducting the interview while listening to the audio of the call at the
same time.
• Monitoring staff or supervisors should provide performance feedback to interviewers as soon
as possible after the monitoring session has been completed.
• Interviewers should be given the opportunity to correct deficiencies in their administration
through additional practice or retraining; however, interviewers who receive consistently
poor monitoring scores should be removed from the project.
• There are federal and state laws and regulations relating to the monitoring/recording of
telephone calls. In certain states, consent must be obtained from every party or conversation
if it involves more than two people (“two-party consent”). When calling sample members
who reside in these states, survey vendors should not begin either monitoring or recording
the telephone calls until after the interviewer has read the following statement: “This call
may be monitored or recorded for quality improvement purposes.”8
• All OAS CAHPS Survey vendors are responsible for identifying and adhering to federal and
state laws and regulations in the states in which they will be administering the OAS CAHPS
Survey.
• Vendors should conduct periodic reviews of their XML data files by comparing at least 50
completed telephone interview responses directly from their computer-assisted telephone
interviewing system to the values output in the XML file. Doing this monthly review will
ensure that the responses are being accurately captured and output to the XML file.
8 The following states currently require two-party or all-party consent when telephone calls are monitored or
audiotaped: California, Connecticut, Delaware, Florida, Illinois, Maryland, Massachusetts, Michigan, Montana,
New Hampshire, Pennsylvania, and Washington.

Centers for Medicare & Medicaid Services 77 Outpatient and Ambulatory Surgery CAHPS Survey Protocols and Guidelines Manual
VII. MAIL WITH TELEPHONE FOLLOW-UP (MIXED-MODE) SURVEY ADMINISTRATION PROCEDURES
Overview
This chapter describes the requirements and guidelines for implementing a mixed-mode survey
administration for the Outpatient and Ambulatory Surgery CAHPS (OAS CAHPS) Survey. For
the OAS CAHPS Survey, “mixed mode” is defined as a mail survey followed by a telephone
follow-up of nonrespondents.
This chapter begins with a discussion of the data collection schedule that should be followed
when a mixed-mode design is used. The mail survey protocols are described next, followed by a
discussion of the protocols for implementing the telephone follow-up of nonrespondents. The
chapter ends with quality control guidelines that should be implemented throughout the mixed-
mode data collection process and describes data storage requirements.
Note that in most cases in this and subsequent chapters of this manual, patients included in the
sample are referred to as “sample members” or “patients”; in discussions of survey processing
and systems they may be referred to as “cases.”
Data Collection Schedule
Survey vendors using mail with telephone follow-up of nonrespondents must initiate the mail
survey for each monthly sample no later than 3 weeks (21 days) after the close of the sample
month. Table 7.1 shows the basic tasks and timing of activities when conducting the OAS
CAHPS Survey using a mixed-mode survey administration.
Table 7.1 Tasks and Schedule of Activities for Mail with Telephone Follow-Up
Activity Timing
Mail questionnaire with cover letter to sample members
No later than 3 weeks (21 days) after the close of the sample month
Initiate telephone follow-up contact for all mail survey nonrespondents
Approximately 3 weeks (21 days) after the questionnaire is mailed
Complete data collection Six weeks (42 days) after the questionnaire is mailed
Submit data files to the Centers for Medicare & Medicaid Services (CMS) via the OAS CAHPS Survey website
The second Wednesday of January, April, July, and October.

VII. Mail with Telephone Follow-Up (Mixed-Mode) Survey Administration Procedures December 2015
78 Centers for Medicare & Medicaid Services Outpatient and Ambulatory Surgery CAHPS Survey Protocols and Guidelines Manual
If the 21st day of the month falls on a weekend or holiday, vendors should make every attempt to
complete the survey mailout on the business day prior to that weekend or holiday. However, it is
acceptable to mail the questionnaires on the first business day following the weekend or holiday
if necessary.
OAS CAHPS Survey vendors must make a concerted effort to complete the survey mailout for
each sample month within 21 days after the sample month ends. If for some reason the survey
mailout cannot be completed within 21 days after the sample month ends, the vendor can
conduct the mailout within 26 days after the sample month ends. Regarding the telephone
survey, vendors must make a concerted effort to initiate the telephone survey 21 days after the
mailout. If for some reason the telephone survey cannot be begun by this time, the vendor can
initiate the telephone survey within 26 days after the mailout. Vendors must complete and
submit a Discrepancy Notification Report (Chapter XV) to the OAS CAHPS Survey
Coordination Team if the mailout is initiated within 26 days after the sample month closes or if
the telephone survey is initiated within 26 days after the mailout.
If the mailout cannot be conducted within 26 days after the close of the sample month or if the
telephone survey cannot be initiated within 26 days of the mailout, CMS may allow these
activities to be conducted more than 26 days after the sample month ended. However, survey
vendors must submit a request via e-mail to the OAS CAHPS Survey Coordination Team. The
e-mailed request should explain the reason for the delay, state when the vendor will (if approved)
initiate the mail and telephone survey, and request CMS’s approval. As noted in Table 7.1, data
collection must be closed 42 calendar days after the questionnaire is mailed. Note as well that
the deadline for data submission is constant. This deadline will not shift later if the vendor starts
data collection late.
As explained in Chapter IX, all cases that are not finalized as a result of the mail survey
component of the mixed-mode survey must be assigned for telephone follow-up, including both
cases that are returned blank and undeliverable mail. This means that unless the case was a
refusal or the patient was determined to be ineligible for the survey during the mail survey data
collection phase of the survey, survey vendors should follow up with the patient by telephone.
The data collection period for mixed-mode data collection is 6 weeks long, just as it is in mail-
only and telephone-only modes. All telephone contact should be initiated and completed within
the specified 3-week period noted above in Table 7.1. Questionnaires may be received through
the mail after the case has been referred for telephone follow-up. If these questionnaires arrived
before the 6-week data collection period ended they should be processed and telephone efforts
with this case should be halted. If these questionnaires arrived after 6-week data collection
period ended they should be considered nonresponses and coded as such.

VII. Mail with Telephone Follow-Up (Mixed-Mode) December 2015 Survey Administration Procedures
Centers for Medicare & Medicaid Services 79 Outpatient and Ambulatory Surgery CAHPS Survey Protocols and Guidelines Manual
Questionnaires, Letters, and Envelopes
Vendors who will be using a mixed-mode design must be able to offer the mail and telephone
versions of the instrument in each language in which the survey is being administered. Vendors
may not offer a mail questionnaire in one of the non-English languages and conduct the
telephone follow-up only in English. For this reason, the mixed-mode design cannot be used in
conjunction with the Chinese versions of the mail questionnaire, because there is no
corresponding OAS CAHPS–approved telephone interview in Chinese. All versions of these
survey materials in the approved languages are available on the OAS CAHPS Survey website at
https://oascahps.org/.
Copies of the mail survey instrument and sample mail survey cover letters in English, Spanish,
and Chinese are also included in the appendices to this manual:
• sample mail survey cover letters, questionnaire, and questionnaire in scannable format in
English, Appendix B;
• sample mail survey cover letters, questionnaire, and questionnaire in scannable format in
Spanish, Appendix C;
• sample mail survey cover letters, questionnaire, and questionnaire in scannable format in
Chinese, Appendix D and
• Office of Management and Budget (OMB) Disclosure Notice in English, Spanish, and
Chinese in Appendix G.
Outpatient and Ambulatory Surgery CAHPS Survey Questionnaires
The OAS CAHPS Survey Questionnaire used in the mail mode contains 37 questions. The
survey can be administered as a standalone survey or can be combined with facility-specific
questions as explained in Chapter III. Questions 1 to 24 are considered the core OAS CAHPS
Survey questions and must be placed at the beginning of the questionnaire. Questions 25 to 37
are the “About You” OAS CAHPS Survey questions and must be administered as a unit.
The OAS CAHPS Survey Questionnaire are available in both Microsoft Word and PDF formats
on the OAS CAHPS Survey website at https://oascahps.org/.
Questionnaire Printing Requirements and Recommendations
The following are formatting and content requirements and recommendations for the OAS
CAHPS Survey Questionnaire. Survey vendors cannot deviate from questionnaire requirements.

VII. Mail with Telephone Follow-Up (Mixed-Mode) Survey Administration Procedures December 2015
80 Centers for Medicare & Medicaid Services Outpatient and Ambulatory Surgery CAHPS Survey Protocols and Guidelines Manual
Requirement Recommendation
Questions Every questionnaire must begin with the core OAS
CAHPS survey questions. n/a
No changes in wording are allowed to either the
OAS CAHPS Survey questions or to the response
(answer) choices.
n/a
If hospital outpatient departments (HOPDs) and
ambulatory surgery centers (ASCs) elect to add
their own questions they must follow the guidelines
in Chapter III. In terms of placement of
supplemental questions in the questionnaire, they
must be placed after the “core” OAS CAHPS
questions. They may either be placed before or
after the unit of “About You” questions.
n/a
Formatting Questions and associated responses choices may
not be split across pages. n/a
Vendors must be consistent throughout the
questionnaire in formatting response options either
vertically or horizontally. If a vendor elects to list
the response options vertically, this must be done
for every question in the questionnaire. Vendors
may not format some response options vertically
and some horizontally.
n/a
No matrix formatting of the questions is allowed.
Matrix formatting means formatting a set of
questions as a table, with responses listed across
the top of a page and individual questions listed in
a column on the left.
n/a
Font size should be no smaller than size 10. We strongly
recommend that size
12 or larger be used.
Vendors should use best survey practices when
formatting the questionnaire, such as maximizing
the use of white space and using simple fonts like
Arial.
If data entry keying is
being used as the data
entry method, small
coding numbers next
to the response
choices may be used.

VII. Mail with Telephone Follow-Up (Mixed-Mode) December 2015 Survey Administration Procedures
Centers for Medicare & Medicaid Services 81 Outpatient and Ambulatory Surgery CAHPS Survey Protocols and Guidelines Manual
Requirement Recommendation
ID number A unique, randomly generated sample
identification (SID) number must be assigned and
appear on at least the first page of the survey, for
tracking purposes. Additional identifiers are
permitted. However, the sample member’s name
or other identifying information must not be
printed anywhere on the survey.
n/a
Translation Only CMS-approved translations of the OAS
CAHPS Survey are permitted. If facilities choose to
add their own supplemental questions, vendors will
be responsible for translating these questions.
n/a
Logo and other
information
about the
HOPD or ASC
The HOPD or ASC name or logo must appear on
the survey or the cover letter. Note that survey
vendors cannot include any promotional messages
or materials on the OAS CAHPS cover letter,
questionnaire, or outgoing or incoming mailing
envelopes. This includes indications that either the
facility or the survey vendor has been approved by
the Better Business Bureau.
n/a
The vendor’s name and mailing address must be
printed at the bottom of the last page of the OAS
CAHPS Survey questionnaire, in case the
respondent does not use the enclosed business reply
envelope.
n/a
OMB Number The OMB number shown in Appendix G must be
printed on the questionnaire cover. If there is no
cover, then the OMB number must be printed on
the first page of the questionnaire.
n/a
Cover Letter Requirements and Recommendations
Examples of cover letters in English, Spanish, and Chinese are provided in the appendices with
the survey instruments (see Appendices C–F). Vendors may choose to develop their own cover
letters as well, provided that the following requirements are met:

VII. Mail with Telephone Follow-Up (Mixed-Mode) Survey Administration Procedures December 2015
82 Centers for Medicare & Medicaid Services Outpatient and Ambulatory Surgery CAHPS Survey Protocols and Guidelines Manual
Requirement Recommendation
Personalization Cover letters must be personalized with the
name and address of the sample member. n/a
Cover letters must contain the date of the
surgery/procedure and the name of the
location where the surgery was received. (The
monthly patient information file must contain
the date of surgery, facility name, and
location name because the name recognized
by the patient may differ from the facility’s
official name.)
n/a
Separate from
Questionnaire
Cover letters must be separate from the
questionnaire, so that no personally
identifiable information (PII) is returned with
the questionnaire when the respondent sends
it back to the vendor.
n/a
Content of
letters
The OMB disclosure notice (see Appendix G)
must be printed either on the questionnaire or
in the cover letters.
n/a
Vendors may not offer sample members the
opportunity to complete the survey over the
telephone. Telephone interviews may only be
conducted as part of the nonresponse follow-
up.
n/a
Must contain language describing the purpose
of the survey. n/a
Must contain a statement that participation is
voluntary and will not affect any benefits the
sample member receives or expects to
receive.
n/a
Must contain language indicating that
responses from all the survey participants will
be grouped together and these grouped data
may be shared with the HOPD or ASC, for
purposes of quality improvement.
n/a
Must contain language stating that if the
respondent needs help in reading the
questions or marking responses, a friend or
family member can assist them.
n/a
Must contain a toll-free customer support
telephone number, which will be staffed by
the survey vendor.
n/a
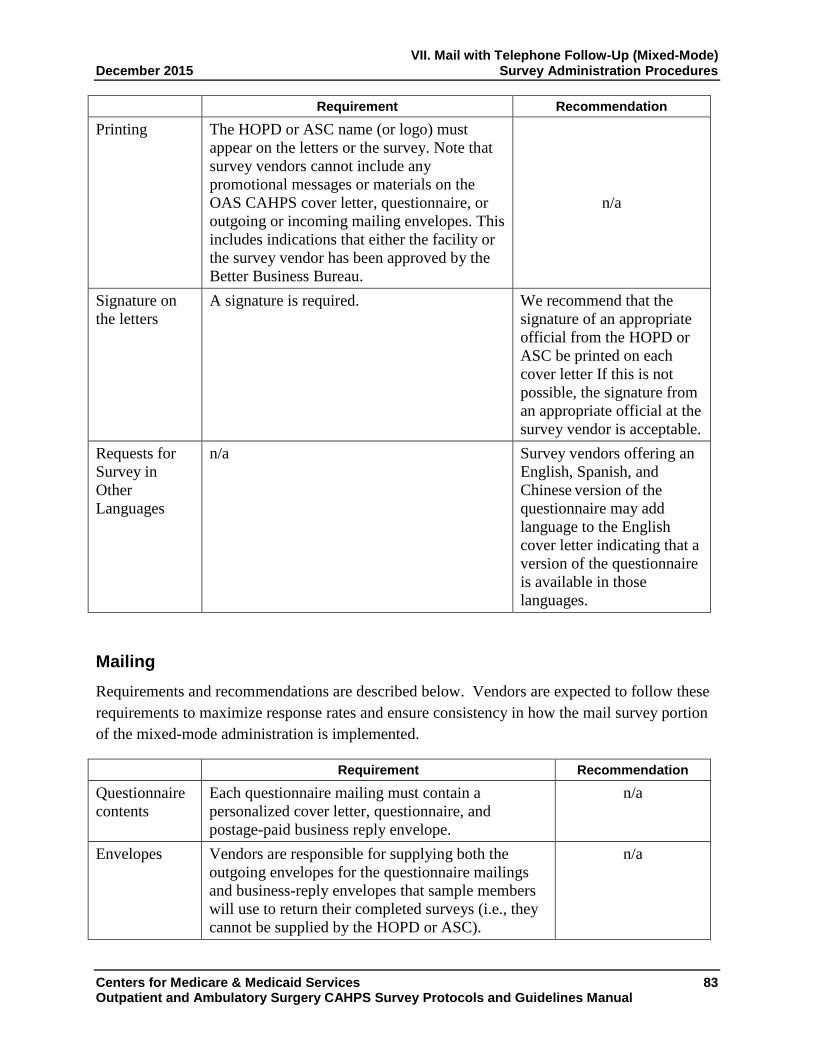
VII. Mail with Telephone Follow-Up (Mixed-Mode) December 2015 Survey Administration Procedures
Centers for Medicare & Medicaid Services 83 Outpatient and Ambulatory Surgery CAHPS Survey Protocols and Guidelines Manual
Requirement Recommendation
Printing The HOPD or ASC name (or logo) must
appear on the letters or the survey. Note that
survey vendors cannot include any
promotional messages or materials on the
OAS CAHPS cover letter, questionnaire, or
outgoing or incoming mailing envelopes. This
includes indications that either the facility or
the survey vendor has been approved by the
Better Business Bureau.
n/a
Signature on
the letters
A signature is required. We recommend that the
signature of an appropriate
official from the HOPD or
ASC be printed on each
cover letter If this is not
possible, the signature from
an appropriate official at the
survey vendor is acceptable.
Requests for
Survey in
Other
Languages
n/a Survey vendors offering an
English, Spanish, and
Chinese version of the
questionnaire may add
language to the English
cover letter indicating that a
version of the questionnaire
is available in those
languages.
Mailing
Requirements and recommendations are described below. Vendors are expected to follow these
requirements to maximize response rates and ensure consistency in how the mail survey portion
of the mixed-mode administration is implemented.
Requirement Recommendation
Questionnaire
contents
Each questionnaire mailing must contain a
personalized cover letter, questionnaire, and
postage-paid business reply envelope.
n/a
Envelopes Vendors are responsible for supplying both the
outgoing envelopes for the questionnaire mailings
and business-reply envelopes that sample members
will use to return their completed surveys (i.e., they
cannot be supplied by the HOPD or ASC).
n/a

VII. Mail with Telephone Follow-Up (Mixed-Mode) Survey Administration Procedures December 2015
84 Centers for Medicare & Medicaid Services Outpatient and Ambulatory Surgery CAHPS Survey Protocols and Guidelines Manual
Requirement Recommendation
Addresses Patients must have a U.S. domestic address to be
eligible to participate in the OAS CAHPS Survey.
n/a
If the sample member’s address is missing or
incomplete, the vendor must follow up with the
HOPD or ASC to obtain the address. If an address
cannot be found, or the address that is found is too
incomplete for mailing, the vendor should treat the
patient as eligible and proceed to the telephone
follow-up survey.
To reduce the
number of missing
addresses, we
recommend that
vendors verify
mailing addresses
obtained from the
facilities using
commercial address
update services, such
as the National
Change of Address or
the U.S. Postal
Service Zip+4
software.
Schedule Mailings must follow the schedule specified for the
mail-only mode of administration—the
questionnaire package must be mailed no later than
3 weeks after the close of the sample month; the
phone calls for telephone follow-up must begin
approximately 3 weeks after the questionnaire
mailing.
n/a
Data collection must end 6 weeks after the
questionnaire has been mailed.
n/a
Incentives The use of incentives is not permitted. This includes
monetary and nonmonetary incentives.
n/a
Data Receipt, Data Entry, and Optical Scanning Requirements
The following guidelines are provided for receiving and tracking returned questionnaires and
entering the data using either data entry or optical scanning.
Requirement
Receipting The date the questionnaire was received from each sample member must be
entered into the data record created for each case on the data file.
Mailings that are returned in the mail as undeliverable must also be logged
into the tracking system. They should then be followed up by telephone.
A final OAS CAHPS Survey disposition code (see Table 9.1 in Chapter IX)
must be assigned to each case.
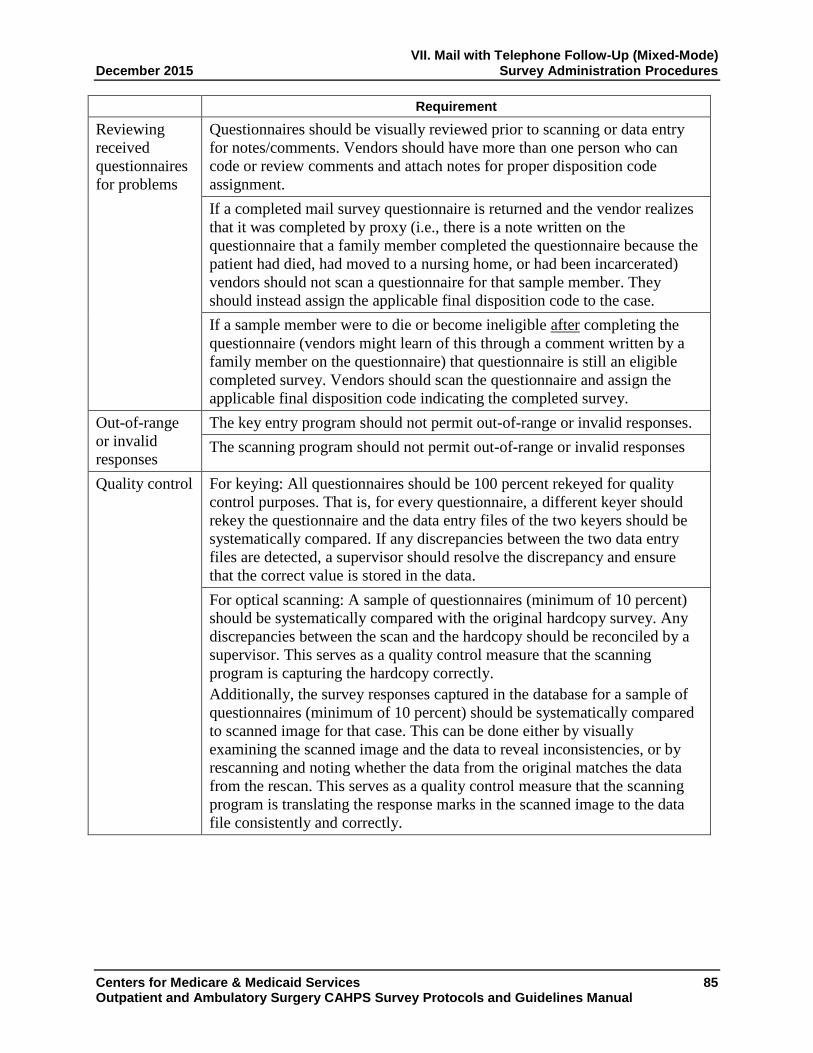
VII. Mail with Telephone Follow-Up (Mixed-Mode) December 2015 Survey Administration Procedures
Centers for Medicare & Medicaid Services 85 Outpatient and Ambulatory Surgery CAHPS Survey Protocols and Guidelines Manual
Requirement
Reviewing
received
questionnaires
for problems
Questionnaires should be visually reviewed prior to scanning or data entry
for notes/comments. Vendors should have more than one person who can
code or review comments and attach notes for proper disposition code
assignment.
If a completed mail survey questionnaire is returned and the vendor realizes
that it was completed by proxy (i.e., there is a note written on the
questionnaire that a family member completed the questionnaire because the
patient had died, had moved to a nursing home, or had been incarcerated)
vendors should not scan a questionnaire for that sample member. They
should instead assign the applicable final disposition code to the case.
If a sample member were to die or become ineligible after completing the
questionnaire (vendors might learn of this through a comment written by a
family member on the questionnaire) that questionnaire is still an eligible
completed survey. Vendors should scan the questionnaire and assign the
applicable final disposition code indicating the completed survey.
Out-of-range
or invalid
responses
The key entry program should not permit out-of-range or invalid responses.
The scanning program should not permit out-of-range or invalid responses
Quality control For keying: All questionnaires should be 100 percent rekeyed for quality
control purposes. That is, for every questionnaire, a different keyer should
rekey the questionnaire and the data entry files of the two keyers should be
systematically compared. If any discrepancies between the two data entry
files are detected, a supervisor should resolve the discrepancy and ensure
that the correct value is stored in the data.
For optical scanning: A sample of questionnaires (minimum of 10 percent)
should be systematically compared with the original hardcopy survey. Any
discrepancies between the scan and the hardcopy should be reconciled by a
supervisor. This serves as a quality control measure that the scanning
program is capturing the hardcopy correctly.
Additionally, the survey responses captured in the database for a sample of
questionnaires (minimum of 10 percent) should be systematically compared
to scanned image for that case. This can be done either by visually
examining the scanned image and the data to reveal inconsistencies, or by
rescanning and noting whether the data from the original matches the data
from the rescan. This serves as a quality control measure that the scanning
program is translating the response marks in the scanned image to the data
file consistently and correctly.

VII. Mail with Telephone Follow-Up (Mixed-Mode) Survey Administration Procedures December 2015
86 Centers for Medicare & Medicaid Services Outpatient and Ambulatory Surgery CAHPS Survey Protocols and Guidelines Manual
Requirement
Interpreting
blanks and
ambiguous
survey
responses
The following apply for both keying and optical scanning:
If a response mark falls between two answer choices but is clearly closer to
one answer choice than to another, select the response that is closest to the
marked response.
If two responses are checked for the same question, select the one that
appears darkest. If it is not possible to make a determination, leave the
response blank and code as “missing” rather than guessing.
If a mark is between two answer choices but is not clearly closer to one
answer choice, code as “missing.”
If a response is missing, leave the response blank and code as “missing.”
Open-ended
responses
The decision on whether to key or scan the responses to open-ended survey
items, specifically, the “Other language” (response option 2) in Q35 and the
“Helped in some other way” (response option 5) in Q37, is up to each
individual HOPD or ASC. Vendors will not be required to key or scan and
include responses to open-ended survey items on the data files submitted to
the OAS CAHPS Survey Data Center.
CMS, however, encourages survey vendors to review the open-ended entries
so they can provide feedback to the Coordination Team about adding
additional preprinted response options to these survey items if needed.
It follows that if the vendor includes the Consent to Share Identifying
Information question in the mail survey questionnaire, we do not require that
the vendor key or scan the response to that question. However, we do
recommend it for the vendor’s own documentation.
Responses to the Consent to Share Identifying Information question will not
be included on the data files submitted to the OAS CAHPS Survey Data
Center.
Staff Training
All staff involved in the mail survey implementation, including support staff, must be thoroughly
trained on the survey specifications and protocols. A copy of relevant chapters of this manual
should be made available to all staff as needed.
In particular, staff involved in questionnaire assembly and mailout, data receipt, and data entry
must be trained on:
• use of relevant equipment (case management systems for entering questionnaire receipts,
scanning equipment, data entry programs);

VII. Mail with Telephone Follow-Up (Mixed-Mode) December 2015 Survey Administration Procedures
Centers for Medicare & Medicaid Services 87 Outpatient and Ambulatory Surgery CAHPS Survey Protocols and Guidelines Manual
• the OAS CAHPS Survey protocol specific to their role (for example, contents of
questionnaire package, how to document or enter returned questionnaires into the tracking
system);
• decision rules and coding guidelines for returned questionnaires (see Chapter IX); and
• proper handling of hardcopy and electronic data, including data storage requirements (see
Chapter VIII).
Staff involved in providing customer support via the toll-free telephone number should also be
trained on the accurate responses to common respondent questions, how to respond to questions
when customer support does not know the answer, and the rights of survey respondents. If the
OAS CAHPS Survey is being offered in a language other than English, customer support staff
should also be able to handle questions via the toll-free telephone number in that language.
Telephone interviewer training requirements are described in more detail in Chapter VI of this
manual. Please refer to that chapter for more information on training customer support staff.
Telephone Interview Development Process
The following paragraphs describe the requirements for producing all materials and systems
needed for the telephone survey. The telephone interview script in English and Spanish are
available on the OAS CAHPS Survey website at https://oascahps.org/.
Copies of the telephone interview script can also be found in Appendix B (in English) and
Appendix C (in Spanish). A list of frequently asked interview questions is included in
Appendix H (English) and Appendix J (Spanish). Some general guidelines for telephone
interviewer training and monitoring are provided in Appendix I.
Specific requirements and guidelines associated with the telephone interview administration are
discussed below.
Telephone Interviewing Systems
In electronic interviewing systems, the interviewer reads from and enters responses into a
computer program. Using an electronic interviewing system or some other type of electronic
data collection system encourages standardized interviewing and monitoring of interviewers.
The OAS CAHPS Survey mixed-mode administration requires vendors use an electronic
interviewing system to administer the follow-up telephone OAS CAHPS Survey. Paper-and-
pencil administration of the OAS CAHPS Survey is not permitted. To ensure that sample
members are called at different times of the day and across multiple days of the week, vendors
must also have a survey management system. Ideally, the electronic interviewing system will be
linked to the survey management system so that cases can be tracked, appointments set and
called back at appropriate times, and pending and final case status easily accessed for any case.

VII. Mail with Telephone Follow-Up (Mixed-Mode) Survey Administration Procedures December 2015
88 Centers for Medicare & Medicaid Services Outpatient and Ambulatory Surgery CAHPS Survey Protocols and Guidelines Manual
Predictive or automatic dialers are permitted, as long as they are compliant with Federal Trade
Commission and Federal Communications Commission regulations, and as long as respondents
can easily interact with a live interviewer. For more information about Federal Trade
Commission and Federal Communications Commission regulations please visit
https://www.ftc.gov/ and https://www.fcc.gov/.
Telephone Interview Script
Survey vendors are provided with standardized telephone scripts in Appendix B English and
Appendix C, Spanish. These scripts include the introductory screens, in addition to the survey
questions.
The OAS CAHPS Telephone Survey questionnaire script contains 35 questions. The survey can
be administered as a standalone survey or can be combined with facility-specific questions as
explained in Chapter III. Questions 1 to 24 are considered the “core” OAS CAHPS Survey
questions and must be placed at the beginning of the questionnaire. Questions 25 to 35 are the
“About You” OAS CAHPS Survey questions and must be administered as a unit.
Note the OAS CAHPS telephone interview script contains only 35 questions and the mail survey
contains 37 questions, because the mail survey questionnaire contains questions that ask if
anyone helped the sample member to complete the survey (Questions 36 and 37). These two
questions are not applicable if the survey is administered by telephone.
The following are content and programming requirements and recommendations for the OAS
CAHPS Survey Questionnaire. Survey vendors cannot deviate from questionnaire requirements.
• Every questionnaire must begin with the core OAS CAHPS questions. They must be
administered in the order in which they appear.
• No changes in wording are allowed for either the OAS CAHPS Survey questions or to the
response choices.
• HOPDs and ASCs may add their own questions, following the guidelines in Chapter III. In
terms of placement of supplemental questions in the questionnaire, note that they must be
placed after the “core” OAS CAHPS questions. They may either be placed before or after
the unit of “About You” questions.
• Only CMS-approved translations of the OAS CAHPS Survey are permitted, although if
facilities choose to add their own supplemental questions, vendors will be responsible for
translating these questions.

VII. Mail with Telephone Follow-Up (Mixed-Mode) December 2015 Survey Administration Procedures
Centers for Medicare & Medicaid Services 89 Outpatient and Ambulatory Surgery CAHPS Survey Protocols and Guidelines Manual
Telephone Interviewing Requirements and Recommendations
Telephone interviewing requirements and recommendations for the OAS CAHPS Survey
interview are described below. Vendors are expected to follow these requirements to maximize
response rates and ensure consistency in how the telephone follow-up is implemented in the
mixed mode of administration.
Telephone Contact
• Vendors must attempt to contact every sample member included in the sample. Vendors
must make a minimum of five contact attempts for each nonrespondent to the mail survey,
unless the sample member refuses or the vendor learns that the sample member is ineligible
for the survey.
• A telephone contact attempt is defined as one of the following:
◦ the telephone rings six times with no answer;
◦ the interviewer reaches a household member and is told that the sample member is not
available to take the call;
◦ the interviewer reaches the sample member and is asked to schedule a call-back at a later
date; or
◦ the interviewer gets a busy signal on each of three consecutive phone call attempts,
spaced at least 20 minutes apart.
• Vendors may make more than one phone call in one 7-day period but cannot make all five
attempts in one 7-day period. Scheduling calls to take place over a longer period of time may
reach patients who may be unavailable the first week of the data collection period.
• Contact with a sample member may be continued after five attempts if the fifth attempt
results in a scheduled appointment with the sample member, as long as the appointment is
within the data collection period.
• Phone calls must be made at different times of the day (i.e., morning, afternoon, and evening)
and different days of the week throughout the data collection period.
• Interviewers may not leave voicemail messages on answering machines or leave messages
with household members.
• Vendors must be able to provide a phone call log that keeps track of the date and time phone
calls were made for each sample member.
VII. Mail with Telephone Follow-Up (Mixed-Mode) Survey Administration Procedures December 2015
90 Centers for Medicare & Medicaid Services Outpatient and Ambulatory Surgery CAHPS Survey Protocols and Guidelines Manual
• If the vendor finds out that a sample member is ineligible for the OAS CAHPS Survey, the
vendor must immediately stop further contact attempts with that sample member.
• Telephone interviewing must follow the schedule specified for the mixed mode of
administration, with the first phone contact initiated approximately 3 weeks after the
questionnaire is mailed and all phone contacts ending 3 weeks after phone contact begins.
• The use of incentives is not permitted in the telephone follow-up portion of the mixed-mode
survey administration. This includes monetary and nonmonetary incentives.
• Proxy respondents are not permitted on OAS CAHPS for any reason. If a sample member is
incapable of responding to the telephone interview because of mental or physical
impairments such as difficulty hearing, the case should be closed using code 240 or
“Mentally/Physically Incapable” and end the interview. If a sample member is capable of
responding but needs some help to do so, a friend or family member may help, but cannot
respond on his or her behalf.
• Proxies are also not permitted for deceased respondents. If a sample member is found to be
deceased, the case should be closed using code 210.
• If a respondent begins the interview but cannot complete it during the call for a reason other
than a refusal, the vendor should follow up with the respondent to complete the entire
interview. This follow-up should be done even if the respondent answered enough questions
in the interview for the case to pass the completeness criteria. It is especially important to
complete the questions in the “About You” section of the questionnaire, because data from
some of those questions will be used in patient-mix adjustment.
• The vendor must be able to offer the interview in any of the approved languages for which an
HOPD or ASC has contracted, even if the language is different from the language that the
HOPD or ASC believes the sample member will require. That is, the vendor must be able to
easily switch to accommodate a respondent’s language preference. For example, if the initial
contact is in English but the respondent prefers to conduct in Spanish, the vendor must be
able to switch to Spanish.
• Sample members are still eligible even if they have missing, incomplete, or foreign phone
numbers. The vendor should contact the HOPD or ASC to obtain the telephone number(s)
they have on record for the sample member. If the HOPD or ASC cannot provide this
number, the vendor should attempt to obtain a telephone number for the patient from other
sources (directory assistance, Internet directories, etc.). If the vendor still cannot obtain a
telephone number, the vendor should code the case as code 340—wrong, disconnected, no
telephone number.

VII. Mail with Telephone Follow-Up (Mixed-Mode) December 2015 Survey Administration Procedures
Centers for Medicare & Medicaid Services 91 Outpatient and Ambulatory Surgery CAHPS Survey Protocols and Guidelines Manual
• If a respondent decides after he or she has answered some of the questions in the telephone
interview that he or she does not wish to participate in the survey any longer, the vendor
should code the case as a refusal. The interviewer should not use the partial data that were
obtained before the interview was ended. This protocol applies even if the respondent
answered enough questions in the interview for the case to pass the completeness criteria.
Note that this is different from the respondent saying that he or she does not wish to continue
an interview. If the respondent breaks off the interview but does not state that he or she does
not wish to participate in the survey, the data may be used as long as the interview meets the
completeness criteria. The vendor may then code the case as a completed interview if the
case passes the completeness criteria; otherwise it should be coded as a breakoff/partial data.
Contacting Difficult-to-Reach Sample Members
• Although not required, we strongly recommend that survey vendors verify telephone
numbers obtained from the HOPD or ASC, using a commercial address/telephone database
service or directory assistance.
• We recommend that vendors attempt to identify a new or updated telephone number for any
sample member whose telephone number is no longer in service when called and for patients
who have moved so that the sample members can be contacted prior to the end of the data
collection period.
• If the sample member’s telephone number is incorrect, the interviewer may ask the person
who answers the phone for the sample member’s phone number.
• If the sample member is temporarily ill, on vacation, or unavailable during initial contact, the
interviewer should attempt to recontact the sample member before the data collection period
ends. If the sample member cannot be reached before the data collection period ends, code
the case as 350, “No Response After Maximum Attempts.”
• If the sample member does not speak a language which has an approved translation for OAS
CAHPS, the interviewer should thank the sample member for his or her time, end the
interview, and code the case as 230, “Ineligible: Language Barrier.”
• If a sample member is physically or mentally incapable of responding by telephone, the case
should be coded as a 240.
• For sample members who are living in institutions (group homes, assisted living, residential
care facilities, etc.), OAS CAHPS Survey vendors should contact the HOPD or ASC to
obtain a direct-dial telephone number for the patients who live in those facilities. If the
HOPD or ASC cannot provide a direct-dial telephone number for the patient, try to obtain the
sample member’s telephone number using other sources, such as a telephone number lookup

VII. Mail with Telephone Follow-Up (Mixed-Mode) Survey Administration Procedures December 2015
92 Centers for Medicare & Medicaid Services Outpatient and Ambulatory Surgery CAHPS Survey Protocols and Guidelines Manual
service, directory assistance, or Internet telephone survey directories. If vendors cannot
obtain a telephone number for the patient, they should assign a disposition code of
“Missing/Disconnected Number” to the case. As a reminder, sample members living in
nursing homes or prisons are ineligible.
Distressed Respondent Procedures
It is critically important that survey vendors develop a “distressed respondent protocol,” to be
incorporated into all interviewer and help desk training. Handling distressed respondent
situations requires balancing keeping personally identifiable information and private health
information confidential and helping a person who needs assistance. For survey research
organizations, best interviewing practices recommend having a distressed respondent protocol in
place for handling distressed respondents, which balances the respondent’s right to
confidentiality and privacy and providing assistance, if the situation indicates that the
respondent’s health and safety are in jeopardy.
Therefore, each approved OAS CAHPS Survey vendor is expected to have procedures in place
for handling distressed respondent situations and to follow those procedures. CMS and the OAS
CAHPS Survey Coordination Team cannot provide guidelines on how to evaluate or handle
distressed respondents. However, survey vendors are urged to consult with their organization’s
Committee for the Protection of Human Subjects Institutional Review Board for guidance. In
addition, professional associations for researchers, such as the American Association of Public
Opinion Researchers (AAPOR), may be able to provide guidance regarding this issue. The
following is an excerpt from AAPOR’s website that lists resources for the protection of human
subjects. More information about protection of human subjects is available at AAPOR’s website
at http://www.aapor.org.9
• The Belmont Report (guidelines and recommendations that gave rise to current federal
regulations)
• Federal Regulations Regarding Protection of Human Research Subjects (45 CFR 46) (also
known as the Common Rule)
• Federal Office for Human Research Protections
9 The American Association of Public Opinion Researchers website at
http://www.aapor.org/Additional_IRB_Resources.html, July 2010.

VII. Mail with Telephone Follow-Up (Mixed-Mode) December 2015 Survey Administration Procedures
Centers for Medicare & Medicaid Services 93 Outpatient and Ambulatory Surgery CAHPS Survey Protocols and Guidelines Manual
• National Institutes of Health Human Participant Investigator Training (although the site
appears to be for cancer researchers, it is the site for the general investigator training used by
many institutions)
• University of Minnesota Web-Based Instruction on Informed Consent
Interviewer Training
Vendors must provide training to all telephone interviewing and customer support staff prior to
starting telephone survey data collection activities. The telephone interview training must
include the following:
• teaching interviewers how to establish rapport with the respondent;
• teaching interviewers the content and purpose of the interview so that they can effectively
communicate this information to the sample members;
• teaching interviewers to administer the interview in a standardized format (reading the
questions as they are worded, not providing the respondent with additional information that is
not scripted, maintaining a professional manner, and adhering to all quality control
standards);
• teaching interviewers how to use effective neutral probing techniques;
• teaching interviewers to use the frequently asked questions document so that they can answer
questions in a standardized format; and
• teaching multilingual customer support staff how to handle questions in English and the other
language(s) in which the survey is being offered.
Survey vendors should also provide telephone survey supervisors with an understanding of
effective quality control procedures to monitor and supervise interviewers.
Vendors must conduct an interviewer certification process of some kind—either oral, written, or
both—for each interviewer and customer service staff member prior to permitting that person to
make or take calls on the OAS CAHPS Survey. The certification should be designed to assess
the interviewer’s level of knowledge and comfort with the OAS CAHPS Survey instrument and
ability to respond to sample members’ questions about the survey. Documentation of training
and certification of all telephone interviewers and customer support staff and outcomes will be
subject to review during oversight visits by the OAS CAHPS Survey Coordination Team.

VII. Mail with Telephone Follow-Up (Mixed-Mode) Survey Administration Procedures December 2015
94 Centers for Medicare & Medicaid Services Outpatient and Ambulatory Surgery CAHPS Survey Protocols and Guidelines Manual
Telephone Data Processing Procedures
The following guidelines are provided for ensuring that the telephone interview data are properly
processed and managed.
Telephone Data Processing Requirements
• A unique SID number must be assigned to each sampled case and included in the case
management system and on the final data file for each sample member.
• Vendors must enter the date the interview was conducted with each sample member in the
survey management system or in the interview data.
• Vendors must be able to link each telephone interview to their survey management system,
so that appropriate variables, such as the language in which the survey was conducted, can be
pulled into the final data file.
• Vendors must de-identify all telephone interview data when the data are transferred into the
final data file for delivery. Identifiable data include respondent name and contact
information.
• Vendors must assign a final OAS CAHPS Survey status or disposition code to each case (see
Chapter IX for a list of these codes) and include a final disposition code for each sampled
case in the final data file. It is up to the vendor to develop and use a set of pending
disposition codes to track actions on a case before it is finalized appropriately—pending
disposition codes are not specified in the OAS CAHPS Survey protocol.
Mixed-Mode Quality Control Guidelines
The following steps are required or recommended as a means of incorporating quality control
into the mixed-mode survey administration procedures. Quality control checks should be
conducted by a different staff person than the one who completed the task.
Mail Protocol
• Vendors are required to check a minimum of 10 percent of all printed materials to ensure the
quality of the printing—that is, make sure that there is no smearing, misaligned pages,
duplicate pages, or stray marks on pages.
• Vendors are required to check a minimum of 10 percent of all outgoing questionnaire
packages to ensure that all package contents are included and that the same unique SID
number appears on both the cover letter and the questionnaire.
• For vendors who are scanning: a sample of questionnaires (minimum of 10 percent) should
be compared with the original hardcopy survey as a quality control measure. Additionally,

VII. Mail with Telephone Follow-Up (Mixed-Mode) December 2015 Survey Administration Procedures
Centers for Medicare & Medicaid Services 95 Outpatient and Ambulatory Surgery CAHPS Survey Protocols and Guidelines Manual
for a sample of questionnaires (minimum of 10 percent) the response data resulting from the
scanning program should be compared to the scanned image for that case. Any discrepancies
from either of these should be reconciled by a supervisor.
• For vendors who are keying: all questionnaires should be 100 percent rekeyed for quality
control purposes. That is, for every questionnaire, a different keyer should rekey the
questionnaire and the data entry files from the two keyers should be systematically compared
to ensure that all entries are accurate. If any discrepancies are observed, a supervisor should
resolve the discrepancy and ensure that the correct value is stored in the data.
Although not required, vendors are urged to develop a way to measure error rates for their data
receipt staff (in terms of recognizing marginal notes and passing these on to someone for
review), for data entry or scanning operators, and for coders. Vendors should then work with
their staff to minimize error rates. The Coordination Team will request information about data
receipt and processing error rates during site visits to survey vendors.
Telephone Protocol
The following activities are methods to incorporate quality control into the survey administration
procedures for the telephone follow-up portion of the mixed-mode survey administration.
Quality control of telephone interviewers and customer support staff should include the
following activities:
• OAS CAHPS requires that survey vendors thoroughly test the electronic telephone
interviewing system before beginning the OAS CAHPS survey. Testing will vary from
system to system, but includes at a minimum comparing each screen to the Telephone Script
to verify that the questions and answer choices are faithful to the script; checking each
question to ensure that the answers input match the data exported, and checking that a
respondent is automatically routed to the next appropriate question.
• Vendors are required to keep written documentation that all telephone interviewing and
customer support staff have been properly trained prior to interviewing. Copies of
interviewer certification exam scores should be retained as well. Documentation should be
maintained for any retraining required and will be subject to review during oversight visits.
• Although not required, we recommend that vendors conduct regular Quality Circle meetings
with telephone interviewing and customer support staff to obtain feedback on issues relating
to telephone survey administration or handling inbound calls.
• Survey vendors must establish and communicate clear telephone interviewing quality control
guidelines for their staff to follow. These guidelines should be used to conduct the
monitoring and feedback process and should include clear explanations of the consequences

VII. Mail with Telephone Follow-Up (Mixed-Mode) Survey Administration Procedures December 2015
96 Centers for Medicare & Medicaid Services Outpatient and Ambulatory Surgery CAHPS Survey Protocols and Guidelines Manual
of not following protocols, including actions such as removal from the project or termination
of employment.
• Vendors are required to silently monitor a minimum of 10 percent of all telephone interviews
to ensure that correct administration procedures are being followed.
• Supervisory staff monitoring telephone interviewers should use the computer-assisted
telephone interviewing (CATI) or alternative electronic system to observe the interviewer
conducting the interview while listening to the audio of the call at the same time.
• Monitoring staff or supervisors should provide performance feedback to interviewers as soon
as possible after the monitoring session has been completed.
• Interviewers should be given the opportunity to correct deficiencies in their administration
through additional practice or retraining; however, interviewers who receive consistently
poor monitoring scores should be removed from the project.
• There are federal and state laws and regulations relating to the monitoring/recording of
telephone calls. In certain states, consent must be obtained from every party or conversation
if it involves more than two people (“two-party consent”). When calling sample members
who reside in these states, survey vendors should not begin either monitoring or recording
the telephone calls until after the interviewer has read the following statement:
“This call may be monitored or recorded for quality improvement purposes.”10
• All OAS CAHPS Survey vendors are responsible for identifying and adhering to federal and
state laws and regulations in the states in which it will be administering the OAS CAHPS
Survey.
• Vendors should conduct periodic reviews of their XML data files by comparing at least 50
completed telephone interview responses directly from their CATI system to the values
output in the XML file. Doing this monthly review will ensure that the responses are being
accurately captured and output to the XML file.
10 The following states currently require two-party or all-party consent when telephone calls are monitored or
audiotaped: California, Connecticut, Delaware, Florida, Illinois, Maryland, Massachusetts, Michigan, Montana,
New Hampshire, Pennsylvania, and Washington.

Centers for Medicare & Medicaid Services 97 Outpatient and Ambulatory Surgery CAHPS Survey Protocols and Guidelines Manual
VIII. CONFIDENTIALITY AND DATA SECURITY
Overview
This chapter describes the requirements and guidelines for (1) protecting the identity of sample
members included in the survey sample, (2) ensuring confidentiality of respondent data, and
(3) ensuring data security. The chapter begins with a discussion of how confidential data should
be handled and the importance of confidentiality agreements. The last section provides
information about the importance of establishing and maintaining physical and electronic data
security.
Safeguarding Patient Data
The Health Insurance Portability and Accountability Act of 1996 (HIPAA) is legislation intended
to protect private medical information and to improve the efficiency of the health care system.
This law went into effect April 14, 2003.
The type of information protected under HIPAA is called “protected health information,” or PHI.
PHI is defined as personally identifiable information that relates to a person’s past, present, or
future health or medical treatment. If the health information is completely de-identified, it is no
longer PHI and can be released. HIPAA also applies to electronic records, whether they are
being stored or transmitted. All vendors approved to implement Outpatient and Ambulatory
Surgery CAHPS (OAS CAHPS) survey must adhere to HIPAA requirements. That is, vendors
must safeguard any and all data collected from sample members as required by HIPAA.
Vendors should therefore stress to their hospital outpatient department (HOPD) and ambulatory
surgery center (ASC) clients the importance of sending the monthly patient information files in a
manner which adheres to HIPAA guidelines, at a minimum encrypting the patient information
files prior to sending them to their vendor.
Vendors must adhere to the following requirements when conducting OAS CAHPS. Each of
these is discussed in more detail in the paragraphs that follow.
• Confidential data must be kept secure as described in this chapter.
• Access to confidential data must be limited to authorized staff members.
• Vendors must develop procedures for identifying and handling breaches of confidential data.
• No data that can identify a sample member can be included on OAS CAHPS data files
submitted to the OAS CAHPS Data Center. That is, all file submissions must contain de-
identified data.

VIII. Confidentiality and Data Security December 2015
98 Centers for Medicare & Medicaid Services Outpatient and Ambulatory Surgery CAHPS Survey Protocols and Guidelines Manual
State Regulations and Laws Protecting Patients With Specific
Conditions/Illnesses
As indicated in Chapter IV of this manual, some states have additional regulations and laws
governing the release of patient information for patients with specific illnesses or conditions, and
for other special patient populations, including patients with HIV. It is the HOPD’s or ASC’s
responsibility to identify any applicable state laws and regulations and exclude patients from the
survey as required by the law or regulation.
Confidential Data Must Be Kept Secure
Any identifying information associated with a patient should be considered private and must be
protected. When the sample frame information is received from an HOPD or ASC, it will
contain private information, such as the name and address or telephone number of the patient,
and other information such as outpatient surgeries or procedures performed and the date on
which the surgeries or procedures were performed. HOPDs and ASCs must provide the monthly
patient information files in a manner which adheres to HIPAA guidelines and regulations, at a
minimum encrypting the patient information files prior to sending them to their vendor.
From the moment the vendor receives sample frame information, the data must be handled in a
way to ensure that the patient information is kept confidential and that only authorized personnel
have access to it. Examples of ways to keep confidential data secure include storing the data
electronically in password-protected locations and limiting the number of staff with access to the
password. For confidential information that is obtained on hard copy, data should be kept in a
locked room or file cabinet, with access restricted to authorized staff. Confidential data should
not, under any circumstances, be removed from the survey vendor’s place of business, either in
electronic or hardcopy form, even by survey vendor staff. Confidential data should not be stored
on laptop computers unless those laptops have data encryption software to protect the
information should the laptop be lost or stolen.
Limit Access to Confidential Data to Authorized Staff
Survey vendors should consider carefully who needs access to confidential OAS CAHPS data
and then ensure that only those staff have access. For example, the sampling manager will need
access to the facility sample frame to select the sample. However, information on the frame does
not need to be included in every data file—although names and addresses need to be provided in
the file used to create cover letters, other PHI does not have to be on that file.
Any staff who will be working with data about outpatient surgery patients should sign a
confidentiality agreement specific to OAS CAHPS implementation (see the paragraph on
Confidentiality Agreements for more information).

December 2015 VIII. Confidentiality and Data Security
Centers for Medicare & Medicaid Services 99 Outpatient and Ambulatory Surgery CAHPS Survey Protocols and Guidelines Manual
Develop Procedures for Identifying and Handling Breaches of Confidential
Data
Survey vendors are required to develop protocols for identifying when there has been a breach of
security with OAS CAHPS data, including when an unauthorized individual has gained access to
confidential information and when an authorized individual has distributed confidential data in
an unauthorized manner. The vendor’s plans must include a system to notify the vendor’s OAS
CAHPS Project Director in a timely manner of a security breach, a means to detect the level of
risk represented by the breach in security, and a means to take corrective action against the
individual who created the breach and any persons affected by the breach, including sample
members.
Provide Only De-identified Data Files to the OAS CAHPS Data Center
Although vendors will have access to confidential information about outpatient surgery patients,
none of the data files submitted to the OAS CAHPS Data Center may contain any confidential
information (i.e., any information that would identify a sample member). All files submitted to
the OAS CAHPS Data Center must contain de-identified data only. Therefore, only the unique
patient sample identification (SID) number that the survey vendor assigns to each sample
member should be included on the file for each data record. (There will be a data record for each
patient sampled.)
Providing OAS CAHPS Response Data to ASCs and HOPDs
When providing response data to their clients, survey vendors must provide data that are de-
identified. Survey vendors must be aware of the following requirements and exceptions.
About You Questions (Questions 25–37)
Vendors can provide de-identified response data for an About You question only if there are a
minimum of 11 responses in each response category for that question. For example, if there are
11 or more responses in each age category of Q27, it is acceptable to provide response results for
Q27, but if there are 10 or fewer responses in each age category it is not acceptable to provide
response data for Q27.
Providing Identified Data
Survey vendors can provide responses linked to a sample member’s name and other identifying
information only if the sample member gives his or her consent on the “Consent to Share
Identifying Information” question (Appendix F). This includes providing this sample member’s
responses to any About You questions which do not meet the threshold of 11 that is required for
reporting response data overall.
In the absence of this explicit consent, only de-identified response data can be provided.

VIII. Confidentiality and Data Security December 2015
100 Centers for Medicare & Medicaid Services Outpatient and Ambulatory Surgery CAHPS Survey Protocols and Guidelines Manual
Confidentiality Agreements
Survey vendors are required to obtain a signed affidavit of confidentiality from all staff,
including subcontractors, who will work on the OAS CAHPS implementation. This includes
individuals who will be working as telephone interviewers or staffing the customer support line
and individuals working in data receipt or data entry positions. Copies of the signed agreements
should be retained by the project director as documentation of compliance with this requirement.
Vendors will be asked to provide this documentation during site visits by the OAS CAHPS
Survey Coordination Team.
Physical and Electronic Data Security
Vendors must take appropriate actions to safeguard both the hardcopy and electronic data
obtained during the course of implementing OAS CAHPS, including data obtained from ASCs
and HOPDs and data provided by survey respondents.
The following are measures vendors should take to ensure physical and electronic data security:
• Paper copies of questionnaires or sample frame information must be stored in a secure
location, such as a locked file cabinet or within a locked room. At no time should paper
copies be removed from the vendor’s premises, even temporarily.
• At no time should electronic data be removed from the survey vendor’s or subcontractor’s
premises, even temporarily.
• Electronic data must be protected. Electronic security measures may include firewalls,
restricted access levels, or password-protected access.
• Access to confidential data must be limited to authorized staff members.
• Data stored electronically must be backed up nightly or more frequently to minimize data
loss.
• Electronic images of paper questionnaires or keyed data, including computer-assisted
telephone interview or alternative electronic system data, should be retained for 3 years in a
secure location at the vendor’s facility.
• Paper copies of questionnaires must be stored in a secure location at the vendor’s facility,
such as a locked room or file cabinet, for 3 years. Paper copies of questionnaires do not need
to be kept if electronic images of the questionnaires are being kept instead.
• Destroy all paper and electronic copies of questionnaire and surveys that contain personally
identifiable information once the proper time has elapsed.

December 2015 VIII. Confidentiality and Data Security
Centers for Medicare & Medicaid Services 101 Outpatient and Ambulatory Surgery CAHPS Survey Protocols and Guidelines Manual
• Protocols for secure file transmission must be established. E-mailing of PHI via unsecure
e-mail is prohibited.
• Confidential data should not be stored on laptop computers unless those laptops have data
encryption software to protect the information should the laptop be lost or stolen.
• Vendors must develop procedures for identifying if breaches of confidential data have
occurred, informing the OAS CAHPS Survey Coordination Team, and implementing a
corrective action plan.
• No data that can identify a patient or a sample of patients can be included on OAS CAHPS
Survey data files submitted to the OAS CAHPS Data Center. That is, all file submissions
must contain de-identified data.
Communicating With Sample Members About Confidentiality and Security
Sample members may wish to understand how the OAS CAHPS survey keeps information about
them confidential and secure. It is important that survey vendors on OAS CAHPS clearly and
succinctly communicate this information to sample members, when asked. The following are
guidelines of what to convey:
• the purposes of the survey and how the survey results will be used, specifically that all
patients’ survey responses will be reported at the aggregate level and absolutely no response
will be linked to an individual patient respondent;
• participation in the study will not affect the care they receive or health care benefits they
currently receive or expect to receive in the future;
• participation in the OAS CAHPS Survey is voluntary;
• they can skip or refuse to answer any question they do not want to answer;
• all information they provide is protected by the Federal Privacy Act of 1974 and HIPAA
(most patients are familiar with HIPAA);
• all OAS CAHPS project staff have signed affidavits of confidentiality and are prohibited by
law from using survey information for anything other than this research study; and
• no facility personnel will see an individual patient’s answers unless the patient explicitly
gives consent to share their answers.

VIII. Confidentiality and Data Security December 2015
102 Centers for Medicare & Medicaid Services Outpatient and Ambulatory Surgery CAHPS Survey Protocols and Guidelines Manual
This page intentionally left blank.

Centers for Medicare & Medicaid Services 103 Outpatient and Ambulatory Surgery CAHPS Survey Protocols and Guidelines Manual
IX. DATA PROCESSING AND CODING
Overview
This chapter describes the requirements and guidelines for creating and assigning a unique
sample identification (SID) number to each sample member, decision rules related to processing
returned mail survey questionnaires, assignment of survey disposition codes, and quality control
measures. In addition, procedures and steps for determining whether a returned survey meets the
definition of a completed survey and information about how survey response rates are calculated
are provided in this chapter.
Sample Identification Numbers
A unique numeric or alphanumeric SID number must be assigned to each patient included in
the Outpatient and Ambulatory Surgery CAHPS (OAS CAHPS) Survey sample. Vendors will
use the SID to track efforts to complete the survey with each sample member throughout the data
collection period. When creating and assigning SID numbers to sampled cases, follow the
guidelines listed below.
• The SID number assigned to a sample member cannot contain any combination of letters or
numbers that could link the SID with a particular sample member. For example, no part of a
sample member’s name, address, date of birth, telephone number, Social Security number, or
dates of outpatient surgeries or procedures can be included in the unique SID created and
assigned to the sample member.
• The SID number also cannot link a particular sample member with a particular hospital
outpatient department (HOPD) or ambulatory surgery center (ASC). The vendor should not
embed within the SID any items identifying the source HOPD or ASC, such as its CMS
Certification Number (CCN), its initials, or its location. Vendors with multiple OAS CAHPS
clients wishing to track the source should establish a variable distinct from the SID in which
to identify the source HOPD or ASC of the patient.
• The SID can be a numeric or alphanumeric variable. The SID must have a minimum length
of 6 and a maximum length of 16 characters.
• Vendors must assign new SID numbers to the new set of patients sampled each month.
Vendors must not reuse the same SID number.
• If a patient is sampled more than once in a calendar year or across multiple calendar years,
the vendor must assign a new SID number to that patient each time he or she is sampled.

IX. Data Processing and Coding December 2015
104 Centers for Medicare & Medicaid Services Outpatient and Ambulatory Surgery CAHPS Survey Protocols and Guidelines Manual
Data Processing Decision Rules and Coding Guidelines
Guidelines and procedures for handling ambiguous, missing, or inconsistent survey responses
from returned mail survey questionnaires are provided below. Note that these guidelines should
be followed regardless of whether the vendor is using optical scanning or data entry to enter data
from completed questionnaires.
Mail Surveys
In mail surveys, some respondents may choose not to answer particular questions, and others
may not clearly mark their answer choices. Use the following rules to handle missing or
ambiguous responses when processing completed questionnaires from the OAS CAHPS mail
survey respondents.
• If a response mark falls between two answer choices but is clearly closer to one answer
choice than to another, select the response that is closest to the marked response.
• If two responses are checked for the same question, select the one that appears darkest. If it
is not possible to make a determination, leave the response blank and code as “missing”
rather than guess.
• If a mark is between two answer choices but is not clearly closer to one answer choice, code
as “missing.”
• Note that the only survey items in the OAS CAHPS Survey where two or more answers are
acceptable are Questions 32 and 37, which ask the sample member to check all answer
choices that are applicable to him or her. For both of these questions, enter responses for all
of the categories that the respondent marked.
• If a response is missing, leave the response blank and code it as “Missing.”
Skip Patterns
Some of the questions included in the OAS CAHPS Survey instrument are “screening”
questions—that is, they are designed to determine whether one or more follow-up questions
about the same topic are applicable to the respondent. The respondent is directed to the next
applicable question by a “skip” instruction printed beside the answer choice that he or she marks.
In mail surveys, some respondents may answer the screening question but leave applicable
follow-up questions blank. In other cases, some respondents will mark an answer to follow-up
questions that are not applicable to them (based on the answer to the screening question). Yet in
other cases, some respondents will answer both the screening and follow-up questions with
responses that contradict each other. Use the following rules for completed OAS CAHPS
Questionnaires.

December 2015 IX. Data Processing and Coding
Centers for Medicare & Medicaid Services 105 Outpatient and Ambulatory Surgery CAHPS Survey Protocols and Guidelines Manual
Decision Rules for Coding Screening Questions (Qs. 10, 30, 34, and 36)
• Key or scan the response provided by the respondent.
• If the screener question is left blank, code it as “Missing (Code M).”
Decision Rules for Coding Follow-Up Questions (Qs. 11, 12, 31, 35, and 37*)
*Please note: Q. 37 is included in the mail survey only.
• Key or scan the response provided by the respondent whenever one is given, regardless of
whether the response agrees with the screener question. For example, if the respondent
answers “No” to the screener question and then marks a response to the follow-up question
instead of skipping it, that is acceptable—the response must still be keyed or scanned.
• If the follow-up question is left blank (correctly) because the respondent correctly followed
the skip instruction in the screener question, assign Code X (“Not Applicable”) to the follow-
up question.
• If the follow-up question is left blank (incorrectly) because the respondent skipped it rather
than answering it, enter Code M (“Missing”) for the follow-up question.
To summarize, when follow-up questions are appropriately skipped, the follow-up question
response should be coded as “Not Applicable,” which is Code X. When follow-up questions are
incorrectly answered, scan or key the response that the respondent provides. If a screener or
follow-up question should have been answered but was not, code the response as “Missing,”
which is Code M. Note that in OAS CAHPS, survey vendors will key or scan the response to
every question that the respondent provides.
Decision Rules for Coding Survey Responses Marked Outside of the Response Box
Although OAS CAHPS mail questionnaires use response bubbles or boxes, vendors may receive
surveys where a response is marked outside the response box. CMS and the OAS CAHPS
Survey Coordination Team acknowledge that there are some instances where it is acceptable to
consider a response “marked,” even if the response box itself is not marked. However, to
minimize the opportunity for coding interpretation errors among vendors, OAS CAHPS requests
that all responses or response boxes that are not circled, checked, underlined, or in some other
way clearly designated by the respondent (i.e., the respondent writes the exact wording of a
response to the right of the response options) be coded as “Missing.”
Although some text or marks to the right of the response options may seem to point to a
particular response, many times the respondent’s intent is not clear. This opens the door to
nonstandardized interpretations from vendor to vendor. To provide some visual guidance on

IX. Data Processing and Coding December 2015
106 Centers for Medicare & Medicaid Services Outpatient and Ambulatory Surgery CAHPS Survey Protocols and Guidelines Manual
what is expected, we have offered three examples below of when it is acceptable to code a
response and two examples of when it is not acceptable to code a response.
When it is Acceptable to Code a Response
Example 1:
In this first example, the respondent has
circled a response. The respondent’s
intention is clear and the vendor should code
the answer to Q3 as “No.”
Example 2:
In this second example, the respondent has
underlined a response. The respondent’s
intention is clear and the vendor should code
the answer to Q6 as “Yes, definitely.”
Example 3:
In this third example, the respondent has
placed a check mark very close to a
response. Again, the respondent’s intention
is clear, and the vendor should code the
answer to Q22 as “Yes.”

December 2015 IX. Data Processing and Coding
Centers for Medicare & Medicaid Services 107 Outpatient and Ambulatory Surgery CAHPS Survey Protocols and Guidelines Manual
When it is NOT Acceptable to Code a Response
Example 1:
In this example, the respondent has placed a
check mark to the right of the response
boxes. It is not clear which response was
intended. Therefore, the correct procedure
for a question presenting like Q10 is to code
the response as “M” which stands for
“missing.”
Example 2:
In this example, the respondent has placed a
check mark to the right of the response
boxes. It is not clear which response was
intended. Therefore, the correct procedure
for a question presenting like Q9 is to code
the response as “M.”

IX. Data Processing and Coding December 2015
108 Centers for Medicare & Medicaid Services Outpatient and Ambulatory Surgery CAHPS Survey Protocols and Guidelines Manual
Survey Disposition Codes
Survey disposition codes, which are also referred to as status codes, are used to track the current
status of a sampled case as it moves through the survey process. For example, a disposition code
is used to designate that the first questionnaire has been mailed, and another disposition code is
used to indicate that the questionnaire has been received. Disposition codes can be interim
(meaning that they are expected to change as the case moves through the rest of the survey
process) or final (meaning that no further action will be taken with that case). Understanding
and appropriately using OAS CAHPS disposition codes is required for successful administration
and completion of OAS CAHPS. This section provides a list and description of the final
disposition codes that are to be used on OAS CAHPS, for mail-only, telephone-only, and mixed-
mode surveys.
Survey vendors should apply pending disposition codes to OAS CAHPS cases for internal
tracking purposes only—that is, to describe the result of the most recent work or action on the
case that did not result in a final disposition. Because survey vendors may have already
developed a set of designated pending dispostion codes for tracking the pending status of a case,
survey vendors may use their own set of pending codes on OAS CAHPS.
Definition of a Completed Survey or Survey Completion Criteria
As is seen below in the description of all OAS CAHPS status codes, one of the criteria in
determining the correct code is whether the survey is “complete.” A survey is considered to be
“complete” and should be assigned a survey disposition code of 110 or 120 if at least 50 percent
of the questions applicable to all sample members (Questions 1–10 and 13–24) are answered.
• Survey items that are part of skip patterns and the items in the “About You” section of the
questionnaire (Questions 10 and 25–37) are not included in this calculation of percentage
complete.
• Responses of “Don’t Know” and “Refuse” should be recoded to missing “M” and should not
be counted as responses.
• Use the steps in Exhibit 9.1 to determine whether a survey can be considered “complete.”

December 2015 IX. Data Processing and Coding
Centers for Medicare & Medicaid Services 109 Outpatient and Ambulatory Surgery CAHPS Survey Protocols and Guidelines Manual
Exhibit 9.1 Steps for Determining Whether a Questionnaire Meets Completeness Criteria
Sum the number of questions that have been answered by the respondent that are applicable to all
patients. These include questions 1–10 and 13–24.
R = total number of questions answered
Divide the total number of questions answered by 22, which is the total number of questions applicable to
all patients, and then multiple by 100 to determine the percentage.
Percentage Complete = (R / 22) x 100
If the Percentage Complete is greater than or equal to 50 percent, then assign the applicable survey
completed disposition code (code 110 or 120) to indicate that the case meets the definition of a
completed survey. Otherwise, assign the disposition code for breakoff (code 310) to the case.
The vendor must select and assign the applicable code from the disposition codes shown in
Table 9.1 for each sampled case included on the data file submitted to the OAS CAHPS Data
Center.
Table 9.1 OAS CAHPS Survey Disposition Codes
Code Description
110 Completed Mail Survey
See Definition of a Completed Survey (above)
Assign this code for mail-only cases and for mixed-mode cases if the sample member responded by mail.
Note that respondents may receive assistance completing the mail survey and such respondents should be included in Code 110. If they are capable of understanding and answering the questions someone else can provide assistance. For example, someone could read the questions and record their answers to help a blind respondent.
120 Completed Telephone Interview
See Definition of Completed Survey (above)
Assign this code if the interview was completed by telephone and for mixed-mode cases if the sample member responded by telephone.
Note that respondents may receive assistance in completing the telephone survey and such respondents should be included in Code 120. For example, someone could translate the computer-assisted telephone interview (CATI) interviewer’s questions into sign language and state a deaf respondent’s replies to the CATI interviewer.
210 Ineligible: Deceased
Assign this code if the sample member is reported as deceased during the course of the survey period.
(continued)

IX. Data Processing and Coding December 2015
110 Centers for Medicare & Medicaid Services Outpatient and Ambulatory Surgery CAHPS Survey Protocols and Guidelines Manual
Table 9.1 OAS CAHPS Survey Disposition Codes
Code Description
220 Ineligible: Does Not Meet Eligible Population Criteria11
Assign this code if it is determined during the data collection period that the sample member does not meet all of the required eligibility criteria for being included in the survey sample. Exclude the sample member if:
• The sample member is under age 18 (note: sampling procedures direct vendors to remove such patients from the sample frame based on their birthdate).
• The sample member does not have a domestic U.S. address (note: sampling procedures direct vendors to remove these patients from the sample frame based on their address).
• The sample member resides in a nursing home or in a prison/jail (note: sampling procedures direct vendors to remove these patients from the sampling frame if this residence information is known).
• The sample member reports that he or she did not receive an outpatient surgery/procedure from the named HOPD or ASC.
• The sample member reports that he or she did not receive surgery/procedure on the sample date.
• It is reported that the sample member was discharged to hospice care following his or her surgery during the sample month.
A full listing of eligibility criteria is provided in Chapter IV of this manual.
230 Ineligible: Language Barrier
Assign this code to sample members who do not speak one of the languages which are approved for the OAS CAHPS survey.
240 Ineligible: Mentally or Physically Incapacitated
Assign this code if it is determined that the sample member is unable to complete the survey because he or she is mentally or physically incapable.
310 Break-Off
This code should be assigned if the sample member completes some responses but does not meet the definition of a completed survey (see above).
320 Refusal
This code should be assigned if the sample member indicates either in writing or verbally (for telephone administration) that he or she does not wish to participate in the survey.
330 Bad Address/Undeliverable Mail, or No Address
This code should be assigned only when using the mail-only mode. It should be assigned if it is determined that the sample member’s address is bad (e.g., the questionnaire is returned by the Post Office as undeliverable with no forwarding address).
11 See Chapter IV for eligibility rules for OAS CAHPS.

December 2015 IX. Data Processing and Coding
Centers for Medicare & Medicaid Services 111 Outpatient and Ambulatory Surgery CAHPS Survey Protocols and Guidelines Manual
Code Description
340 Wrong, Disconnected, or No Telephone Number
This code will be used in telephone-only or mixed-mode survey administration. In the telephone-only mode, this code should be assigned if it is determined the telephone number is bad (disconnected, no telephone number available, etc.). In the mixed mode, this code should be assigned because the telephone follow-up represents the last attempt to reach the sample member even if it is determined the mailing address is also bad.
(continued) Table 9.1
OAS CAHPS Survey Disposition Codes
Code Description
350 No Response After Maximum Attempts
This code can be used in all three approved data collection modes. It should be assigned when the contact information for the sample member is assumed to be viable, but the sample member does not respond to the survey/cannot be reached during the data collection period.
This code should also be assigned to completed surveys received after the data collection period ends. As explained earlier, the data collection period ends 42 calendar days after the initial mailout (for mail-only and mixed mode) or 42 calendar days after the initiation of the telephone survey (for telephone-only mode) for telephone surveys.
Mail-Only Mode
• This code should be assigned if the sample member’s address is viable but he or she does not respond to either the first or second questionnaire mailing during the data collection period. This code should be assigned if the initial questionnaire is returned blank and the second questionnaire is never returned.
Telephone-Only Mode
• This code should be assigned if it is determined that the telephone number is viable but the minimum number of telephone attempts (five) did not result in a completed interview or other final disposition code.
Mixed Mode
• This code should be assigned if it is determined that the address and telephone number are viable but the maximum number of contact attempts (i.e., the questionnaire mailing and five telephone attempts) did not result in a completed survey or another final disposition code.
Differentiating Between Disposition Codes 330 (Nonresponse: Bad
Address), 340 (Bad/No Telephone Number), and 350 (No Response after
Maximum Attempts)
Code 330: Nonresponse: Bad Address should be assigned only if there is evidence that the
patient’s address is not viable. Evidence that the address is not viable includes the following:
• the HOPD or ASC does not provide an address for the sample member and the vendor has
attempted but failed to obtain an address;

IX. Data Processing and Coding December 2015
112 Centers for Medicare & Medicaid Services Outpatient and Ambulatory Surgery CAHPS Survey Protocols and Guidelines Manual
• the questionnaire is returned as “undeliverable, no forwarding address”; and
• the questionnaire is returned as “address or addressee unknown” or some other reason the
mail was not delivered.
The vendor is strongly encouraged to use an outside address update service prior to mailing
questionnaires to ensure that the most accurate mailing address is used. Survey vendors are
permitted to ask HOPDs and ASCs to provide updated address information for all patients
treated within the sample month, if needed. The survey vendors cannot, however, give a list of
sample members to the HOPD or ASC to request this information. Similarly, if a questionnaire
is returned as undeliverable, the vendor is strongly encouraged to attempt to locate a new address
prior to the second questionnaire mailing.
Code 340: Nonresponse: Bad or No Telephone Number should be assigned only if there is
evidence that the sample member’s telephone number is not viable. This applies to both
telephone-only and mixed-mode administration. Evidence that the telephone number is not
viable includes the following:
• the HOPD or ASC does not provide a telephone number for the sample member and the
vendor has attempted and failed to obtain a telephone number;
• on calling, the telephone interviewer learns that the telephone number on file is disconnected,
nonworking, or out of order, and no new telephone number is provided; and
• on calling, the telephone interviewer reaches a person and learns that the telephone number is
the wrong number for the sample member and no new number is provided.
To ensure that the most accurate telephone number is used, the vendor is strongly encouraged to
use an outside telephone number update service prior to initiating telephone contact. Similarly,
if the vendor learns that a telephone number is not viable, the vendor is strongly encouraged to
attempt to locate a new telephone number for the sample member prior to the end of the data
collection period. Survey vendors are permitted to ask HOPDs and ASCs to provide updated
telephone number information for all patients treated within the sample month, if needed. The
survey vendors cannot, however, give a list of sample members to the HOPD or ASC to request
this information.
Code 350: Nonresponse: No Response After Maximum Attempts should be assigned if there is
evidence that the sample member’s address or telephone number is viable but the sample
member has not responded after all questionnaire mailings or telephone attempts appropriate for
the given mode have been implemented.

December 2015 IX. Data Processing and Coding
Centers for Medicare & Medicaid Services 113 Outpatient and Ambulatory Surgery CAHPS Survey Protocols and Guidelines Manual
Handling Blank Questionnaires
In handling questionnaires that are returned blank, vendors should differentiate between mail
survey questionnaires that are returned blank because the United States Postal Service could not
deliver the mail (referred to as undeliverables) and those returned blank by the sample member
or the sample member’s family or friend. The procedures described below are for surveys that
are returned blank and are not marked as undeliverable.
For the mail-only mode it is appropriate to send a second questionnaire to the sample member if
the first questionnaire is returned blank, as long as it is mailed before the end of the data
collection period. If the second questionnaire is also returned blank, the vendor should assign a
final survey disposition code “320 – refusal.” If the first survey for the mail-only mode is never
returned and the second survey is returned blank, then that case should also be assigned a final
disposition code of “320 – refusal.” Finally, if the first survey for the mail-only mode is never
returned or returned blank and the second questionnaire is not returned at all, the vendor should
assign the final survey disposition code “350 – no response after maximum attempts.”
Note that all cases that are not finalized as a result of the mail survey component of the mixed-
mode survey must be assigned for telephone follow-up, including both cases that are returned
blank and undeliverable mail. This means that unless the case was a refusal or the sample
member was determined to be ineligible for the survey during the mail survey data collection
phase of the survey, survey vendors should follow up with the sample member by telephone.
This includes cases for which the questionnaire was returned blank and those for which the
questionnaire was undeliverable.
Quality Control Measures
Vendors are strongly encouraged to implement quality control measures for every aspect of mail
and telephone data processing activities. Required and recommended quality control measures
are described in detail in the mail, telephone, and mixed-mode data collection chapters of this
manual; however, we have repeated key measures here as well. Quality control measures are
listed by topic in the paragraphs that follow. Vendors should conduct additional quality control
measures as warranted, based on their individual processes. All quality control checks should be
conducted by a different person than the one who completed the task.
Quality Control for Mail Survey Data Processing Activities
• Vendors should review at least 10 percent of the printed questionnaires for each batch of
questionnaires that are printed each sample month to ensure the quality of the printed
questionnaires. The questionnaires should be examined to make sure there are no bleed-
throughs, which can impact or cause problems when scanning the data from completed
surveys, and to make sure all pages are included in the questionnaire.

IX. Data Processing and Coding December 2015
114 Centers for Medicare & Medicaid Services Outpatient and Ambulatory Surgery CAHPS Survey Protocols and Guidelines Manual
• Vendors should check to make sure the number of mail survey packages to be mailed
matches the number of sampled cases.
• Vendors should check a sample of at least 10 percent of mail survey packages before they are
sealed and mailed. In this check, make sure that the SID number on the questionnaire
matches the SID number on the cover letter.
• For vendors that use scanning software for data capture procedures, select a sample of
questionnaires (minimum of 10 percent), rescan, and compare the scanned images against the
original hardcopy survey as a quality control measure. For vendors that use data keying as
their data capture process, all questionnaires should be 100 percent rekeyed by a different
keyer to ensure all entries are accurate. If any discrepancies are observed, a supervisor
should resolve the discrepancy and ensure the correct value is keyed.
• For coding, vendors should select and review a sample of cases coded by each coder to make
sure coding rules were followed correctly.
• We highly recommend before submitting data to the OAS CAHPS Data Center that vendors
compare the responses coded on the hardcopy questionnaire for a sample of at least 10
percent of cases with the responses that were actually scanned or keyed and with the
responses entered on the XML file. This quality control step will ensure that the responses
included in the XML files accurately reflect the sample members’ responses to the survey
questions.
• We highly recommend vendors calculate and review the response rates periodically for each
of their client ASCs or HOPDs. If a sample was selected for an HOPD or ASC but there is
no response or a very low response rate, this could be an indicator that incoming mail was
not processed, scanned data were not exported to the XML file, or other problems occurred
with the mail survey. In instances where the number of cases sampled was very small (e.g.,
10 or fewer), it is possible that all of the sample members decided not to return a completed
survey. For HOPDs and ASCs with larger sample sizes, no response from any of the sample
members could be indicative of a data collection or data processing problem.
• Vendors are urged to develop a way to measure error rates of both their data receipt staff (in
terms of recognizing marginal notes and passing these on to someone for review) and in
terms of data entry or scanning verification. Vendors should then work with their staff to
minimize error rates. The OAS CAHPS Survey Coordination Team will request information
about data receipt and processing error rates during site visits to survey vendors.

December 2015 IX. Data Processing and Coding
Centers for Medicare & Medicaid Services 115 Outpatient and Ambulatory Surgery CAHPS Survey Protocols and Guidelines Manual
Quality Control for Telephone Survey Data Processing Activities
• Vendors must silently monitor a minimum of 10 percent of all telephone interviews to ensure
that correct administration and coding procedures are being followed. Supervisory staff
monitoring telephone interviewers should use the electronic system to observe the
interviewer conducting the interview while listening to the audio of the call at the same time.
• We highly recommend that vendors calculate and review the response rates on a periodic
basis for each of their client HOPDs and ASCs. If a sample was selected for an HOPD or
ASC but there is no response or a very low response rate, this could be an indication of a data
collection or data processing problem. In cases where the number of cases sampled was very
small (e.g., 10 or fewer), it is possible all of the sample members decided not to participate in
the survey. For HOPDs and ASCs with larger sample sizes, it is highly unlikely that 100
percent of the sample cases will refuse to participate in the survey.
• Vendors should conduct periodic reviews of their XML data files by comparing at least 50
completed telephone interview responses directly from their CATI system to the values
output in the XML file. Doing this review monthly will ensure that the responses are being
accurately captured and output to the XML file.
• Vendors should generate and review frequencies of cases at the various interim and final
disposition codes for each ASC and HOPD and perhaps by telephone interviewer. For
instance, a high percentage of cases coded as “not available” after maximum attempts could
indicate that call attempts are not scheduled appropriately.
Quality Control on XML Files
• Vendors should use the XML validation tool to conduct an initial quality control of their
XML file formatting. The XML Schema Validation Tool is available on the OAS CAHPS
website under the “Data Submission” tab.
• We highly recommend that vendors conduct some additional quality control measures on the
data included on XML files to ensure that the data from completed mail and telephone
surveys are being captured accurately. This includes running frequencies of distributions on
both the patient administrative data and the patient response data to look for outliers or
anomalies, including missing values.
Examples of frequencies vendors could run include the race variable (are all respondents
coded as Alaska Native, for example) or the age variable (is there a reasonable distribution of
age categories across sample members, or do the ages lean heavily toward the very young or
very old?). By reviewing frequencies of both the patient administrative data and the patient
response data, vendors may be able to identify problems in the data they receive from
HOPDs and ASCs, their own facility data file processing, or their XML coding operations.

IX. Data Processing and Coding December 2015
116 Centers for Medicare & Medicaid Services Outpatient and Ambulatory Surgery CAHPS Survey Protocols and Guidelines Manual
• Vendors should periodically check their data processing programs to confirm that variables
on the XML files are coded properly on the XML file.
• Vendors should conduct a final check of the
disposition code assigned to all sampled cases
before submitting XML files to the OAS
CAHPS Data Center. If the vendor identifies a
case assigned either an ineligible or
noncomplete final disposition code AND there
are data included in the Patient Response
Record section of the XML file, they should check their records to determine why code 110
or 120 was not assigned to the case. If it is determined that the case is indeed ineligible or
was a noncomplete, remove the survey response data from the XML file.
• Vendors should select a random sample of
cases on the XML file and compare the
variables in the Patient Administrative Record
against the patient information that was
provided by the HOPD or ASC on the monthly
patient information file to make sure the
information was exported to the XML file correctly.
Computing the Response Rate
Survey vendors are not required to compute a response rate for each monthly sample. However,
CMS will compute and report a response rate for each ASC and HOPD when survey results are
publicly reported. For a given public reporting period (i.e., the last four quarters of collected
data), a response rate for each ASC and HOPD will be calculated as described in Exhibit 9.2.
The information below is provided for illustrative purposes only.
The Patient Response Record section of the
XML file is the patient response record,
which contains the responses to the OAS
CAHPS Survey from every patient who
answered the survey during the sample
month.
The Patient Administrative Record section
of the XML file contains data about each
patient who was sampled for the sample
month, including both those who responded to
the survey and nonrespondents.

December 2015 IX. Data Processing and Coding
Centers for Medicare & Medicaid Services 117 Outpatient and Ambulatory Surgery CAHPS Survey Protocols and Guidelines Manual
Exhibit 9.2 How Response Rates Are Calculated
Response Rate =
Total number of Completed Surveys is the number of surveys assigned a final survey disposition code of
110 or 120.
Total Number of Surveys Fielded is the total number of patients selected for the survey in the sample
month. This includes all cases with a final survey disposition code of 110 through 350.
Total Number of Ineligible Surveys is the number of sample cases assigned a final survey disposition
code of 210, 220, 230, or 240. No other cases will be removed from the denominator.

Centers for Medicare & Medicaid Services 118 Outpatient and Ambulatory Surgery CAHPS Survey Protocols and Guidelines Manual
X. THE OAS CAHPS SURVEY WEB PORTAL
Overview
This chapter presents an overview of the Outpatient and Ambulatory Surgery CAHPS Survey
(OAS CAHPS) website and the web portal within the website. The website is the official site for
the OAS CAHPS Survey with public and private sections. The private section, called the “web
portal,” is an interactive site which supports the functionality needed by survey vendors, HOPDs
and ASCs participating in the OAS CAHPS Survey. For example, it contains procedural
documents, survey materials, online submissions and authorizations, and reports for vendors,
hospital outpatient departments (HOPDs), ambulatory surgery centers (ASCs).
The OAS CAHPS Web Portal
The OAS CAHPS Data Center is maintained by RTI International, which is assisting the Centers
for Medicare & Medicaid Services (CMS) with OAS CAHPS. RTI also developed and
maintains the OAS CAHPS web portal, available at https://oascahps.org/. This web portal is the
main vehicle for communicating and updating information about OAS CAHPS to ASCs,
HOPDs, and survey vendors. The web portal has both public and secure (restricted-access)
sections to ensure the security and privacy of selected interactions. On the public page, a link to
a login allows authorized users (survey vendor, HOPD or ASC staff) access to the restricted
private sections of the web portal, where they can carry out administrative functions according to
their role. Access to the secure sections will be restricted and controlled through user
identification and password.
Specifically, survey vendors will use the web portal to submit OAS CAHPS data to the Data
Center. It will also allow Medicare-certified HOPDs and ASCs to authorize their contracted
survey vendor to submit OAS CAHPS data on their behalf, access their data submission reports,
and review their OAS CAHPS survey results before the results are publicly reported.
Exhibit 10.1 provides an overview of both the public and private links and information available
on the web portal. In the diagram private links are shown in red text and public links are shown
in black text.
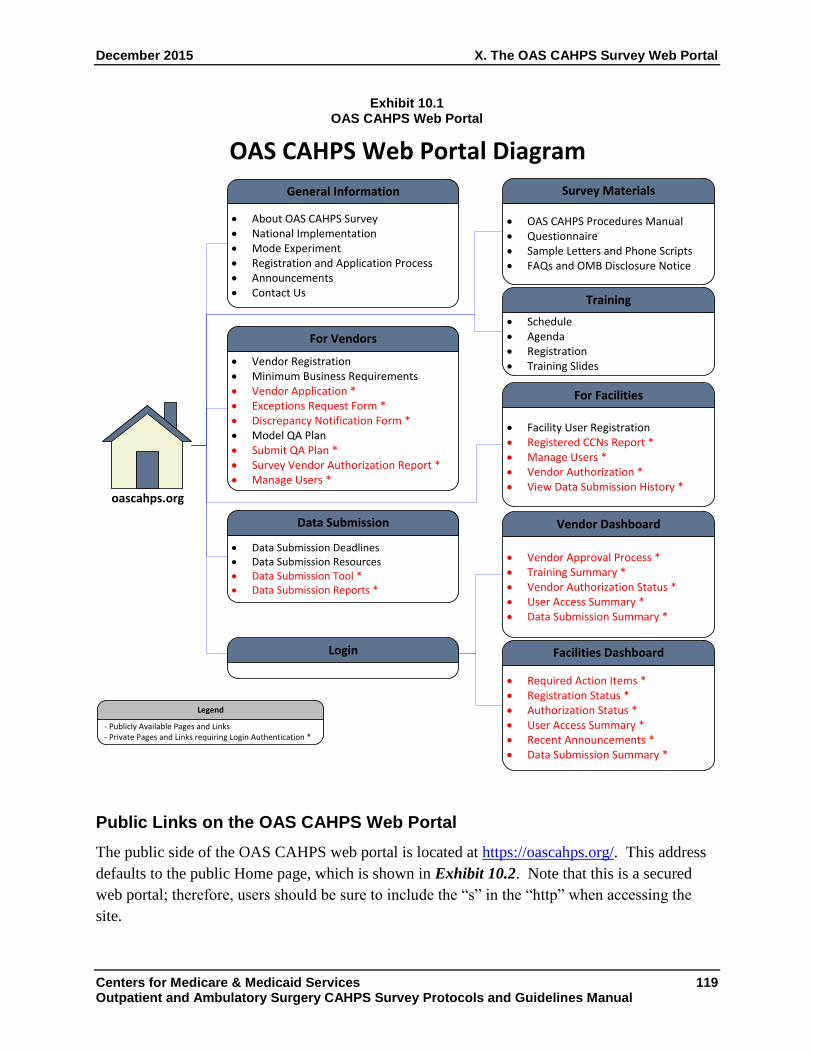
December 2015 X. The OAS CAHPS Survey Web Portal
Centers for Medicare & Medicaid Services 119 Outpatient and Ambulatory Surgery CAHPS Survey Protocols and Guidelines Manual
Exhibit 10.1 OAS CAHPS Web Portal
Public Links on the OAS CAHPS Web Portal
The public side of the OAS CAHPS web portal is located at https://oascahps.org/. This address
defaults to the public Home page, which is shown in Exhibit 10.2. Note that this is a secured
web portal; therefore, users should be sure to include the “s” in the “http” when accessing the
site.
OAS CAHPS Web Portal Diagram
· About OAS CAHPS Survey· National Implementation· Mode Experiment· Registration and Application Process· Announcements· Contact Us
General Information
· Schedule· Agenda· Registration· Training Slides
Training
· Vendor Registration· Minimum Business Requirements· Vendor Application *· Exceptions Request Form *· Discrepancy Notification Form *· Model QA Plan· Submit QA Plan *· Survey Vendor Authorization Report *· Manage Users *
For Vendors
oascahps.org
· OAS CAHPS Procedures Manual· Questionnaire· Sample Letters and Phone Scripts· FAQs and OMB Disclosure Notice
Survey Materials
· Data Submission Deadlines· Data Submission Resources · Data Submission Tool *· Data Submission Reports *
Data Submission
· Facility User Registration· Registered CCNs Report *· Manage Users *· Vendor Authorization *· View Data Submission History *
For Facilities
· Vendor Approval Process *· Training Summary *· Vendor Authorization Status *· User Access Summary *· Data Submission Summary *
Vendor Dashboard
Login
· Required Action Items *· Registration Status *· Authorization Status *· User Access Summary *· Recent Announcements *· Data Submission Summary *
Facilities Dashboard
- Publicly Available Pages and Links - Private Pages and Links requiring Login Authentication *
Legend
OAS CAHPS Web Portal Diagram
· About OAS CAHPS Survey · National Implementation and Public Rpt · Mode Experiment · Vendor Application Process · Announcements · Contact Us
General Information
· Schedule · Agenda · Registration · Training Slides
Training
· Vendor Registration · Minimum Business Requirements · Vendor Application
* · Exceptions Request Form
* · Discrepancy Notification Form
* · Model QA Plan · Submit QA Plan
* · Survey Vendor Authorization Report
* · Manage Users
*
For Vendors
oascahps . org
· OAS CAHPS Procedures Manual · Questionnaire · Sample Letters and Phone Scripts · FAQs and OMB Disclosure Notice
Survey and Protocols
· Data Submission Deadlines · Sample File Download
* · Data Submission Resources
· Data Submission Tool
* · Data Submission Reports
*
Data Submission
· Facility User Registration · Registered CCNs Report
* · Manage Users
* · Authorize a Vendor
* · View Data Submission History
* · Survey Preview Report
*
For Facilities
· Vendor Approval Process
* · Training Summary
* · Vendor Authorization Status
* · User Access Summary
* · Data Submission Summary
*
Vendor Dashboard
Login
· Required Action Items
* · Registration Status
* · Authorization Status
* · User Access Summary
* · Info for Dialysis Facilities
* · Recent Announcements
* · Data Submission Summary
*
Facilities Dashboard
- Publicly Available Pages and Links - Private Pages and Links requiring Login Authentication
*
Legend

X. The OAS CAHPS Survey Web Portal December 2015
120 Centers for Medicare & Medicaid Services Outpatient and Ambulatory Surgery CAHPS Survey Protocols and Guidelines Manual
Exhibit 10.2 OAS CAHPS Home Page (Public Web portal)
On the Home page, there is a welcome message that includes brief information about OAS
CAHPS. In that message, there are hyperlinks embedded in the underlined text that lead to other
pages that provide more specific information.
The OAS CAHPS web portal uses navigation features that include standard dropdown menus
and other navigation tools. A horizontal menu bar is displayed near the top of the Home page.
The bar has different tabs, each with its own dropdown options to allow users to perform various
functions and access more information. The navigation tabs include the following:
• General Information;
• Training;
• For Vendors;
• Survey Materials;
• Data Submission; and
• For Facilities.
The public pages on the OAS CAHPS web portal contain numerous links and information
including the following:
• Background information about OAS CAHPS, including information about the mode
experiment, national implementation and public reporting;

December 2015 X. The OAS CAHPS Survey Web Portal
Centers for Medicare & Medicaid Services 121 Outpatient and Ambulatory Surgery CAHPS Survey Protocols and Guidelines Manual
• Requirements and a description of the application process for survey vendors interested in
becoming a CMS-approved OAS CAHPS Survey vendor;
• Contact information for the OAS CAHPS Survey Coordination Team (e-mail address and
toll-free telephone number);
• Survey questionnaires and related survey administration materials in English, Spanish, and
Chinese (forthcoming);
• Survey administration protocols, guidelines for data submission, and information about the
data submission tool (including this manual);
• Model Quality Assurance Plan, which is a sample QAP outline that approved survey vendors
should use as a guide when completing their own initial QAP or annual QAP update;
• Vendor Registration Form, to be completed by the survey vendor’s designated Survey
Administrator; the Survey Administrator must complete this form so that he or she can access
and submit a Vendor Application to become a CMS-approved OAS CAHPS Survey vendor;
• HOPD/ASC User Registration Form, to be completed by the HOPD’s or ASC’s designated
Survey Administrator to create an account and credentials for accessing links in the secure
section of the web portal;
• Continuous updates in the Announcements section (shown in Exhibit 10.3) which is under
General Information. An These updates will provide vendors, HOPDs, and ASCs with any
new policies or changes in survey administration protocols and procedures, announcements
about updates to the procedures manual, a data submission schedule, and reminders of
upcoming data submission deadlines;
• A recent announcements section also appears on the home page box (shown in Exhibit 10.4);
• Forthcoming, a list of survey vendors that have been approved to administer OAS CAHPS;
• Helpful documents that are targeted for HOPDs and ASCs, including information about OAS
CAHPS participation guidelines and instructions on steps that facilities should take to
participate in OAS CAHP); and
• Training information and materials for each Introduction to the OAS CAHPS Training
Session and all vendor update training sessions, including training registration form.

X. The OAS CAHPS Survey Web Portal December 2015
122 Centers for Medicare & Medicaid Services Outpatient and Ambulatory Surgery CAHPS Survey Protocols and Guidelines Manual
Exhibit 10.3 Announcements Page on the OAS CAHPS Web Portal
Exhibit 10.4 Recent Announcements on the OAS CAHPS Web Portal Home Page

December 2015 X. The OAS CAHPS Survey Web Portal
Centers for Medicare & Medicaid Services 123 Outpatient and Ambulatory Surgery CAHPS Survey Protocols and Guidelines Manual
How to Obtain Access to the Private side of the OAS CAHPS Web Portal
All Users (Survey Vendors, HOPDs, and ASCs)
Designate an OAS CAHPS Survey Administrator. Before any participating HOPD, ASC, or
survey vendor can access the restricted portion of the web portal, the organization first must
decide which staff member it will designate to serve as its OAS CAHPS Survey Administrator.
The designated OAS CAHPS Survey Administrator’s roles and responsibilities are listed below.
• Register as the Survey Administrator for the HOPD, ASC or survey vendor;
• Designate another individual within the organization to serve as the backup OAS CAHPS
Survey Administrator;
• Remove access or approve the removal of access for users who are no longer authorized to
access the private side of the web portal;
• Serve as the main point of contact with the OAS CAHPS Survey Coordination Team and
Data Center; and
• Notify the OAS CAHPS Survey Coordination Team if your role as the OAS CAHPS Survey
Administrator will no longer be valid and identify a successor.
HOPD and ASC Users
Step 1: The individual designated as the HOPD’s/ASC’s OAS CAHPS Survey
Administrator will complete and submit the Facility Website User Registration Form. This
online form is located on the public side of the web portal. It is used to establish an account and
obtain credentials for accessing the secured sections of the web portal. To do this, click on the
“Facility Registration” link under the “For Facilities” navigation tab on the OAS CAHPS web
portal (as shown in Exhibit 10.5).
The form will collect the OAS CAHPS Survey Administrator’s name, e-mail address, and
telephone number. The Survey Administrator will also be instructed to create a username and
password that will be used to access the secured links and forms on the private side of the web
portal. Once all information is correct, click the “Submit” button.
The OAS CAHPS Data Center staff will activate an account for the HOPD’s or ASC’s OAS
CAHPS Survey Administrator immediately after the online registration form has been submitted.
Once the registration form is submitted, users will be routed to a dashboard created specifically
for their HOPD(s) or ASC(s), where they can find the other forms required to complete the
registration process. Additional links to important functions and forms, including the CCN
Registration Form and the Authorize a Vendor Form, are also available on the dashboard.

X. The OAS CAHPS Survey Web Portal December 2015
124 Centers for Medicare & Medicaid Services Outpatient and Ambulatory Surgery CAHPS Survey Protocols and Guidelines Manual
Exhibit 10.5 Facility User Registration Form
Step 2: The OAS CAHPS Survey Administrator will complete and submit the CCN
Registration Form. This online form is located on the private side of the web portal. Therefore,
the OAS CAHPS Survey Administrator will enter the established username and password to log
in. See Exhibit 10.6. The OAS CAHPS Survey Administrator will type the CCN or CCNs for
which they are an administrator into the box. Multiple CCNs can be separated by commas and
entered into the box. After the CCN(s) are entered click the “Lookup Facility Names” button
and the system will automatically display the facility or facilities name(s) in the display window.
The person filling out this form will be presented the list of roles and responsibilities of the OAS
CAHPS Survey Administrator. The OAS CAHPS Survey Administrator needs to personally
acknowledge that that he/she is the OAS CAHPS Survey Administrator for the listed HOPD or
ASC, and acknowledge that he/she accepts the roles and responsibilities for the listed HOPD
or ASC. Once all information is entered correctly click “Submit.”
Step 3: The OAS CAHPS Survey Administrator will designate a backup OAS CAHPS
Survey Administrator and create an account for him or her. The backup OAS CAHPS
Survey Administrator will have all of the same permissions as the primary OAS CAHPS Survey
Administrator. Having a backup Survey Administrator will ensure continued system use if the
primary Survey Administrator is unavailable or terminates employment with the HOPD or ASC.
The Survey Administrator or the backup Survey Administrator must notify the Data Center
immediately if the primary Survey Administrator will no longer serve in that role.

December 2015 X. The OAS CAHPS Survey Web Portal
Centers for Medicare & Medicaid Services 125 Outpatient and Ambulatory Surgery CAHPS Survey Protocols and Guidelines Manual
Exhibit 10.6 CCN Registration Form
The form to designate a backup survey administrator is also available under the Facility
Dashboard, under the menu item “Manage User Console.” This is shown in Exhibit 10.7. The
Survey Administrator can add a new user, delete a user, or edit a user. User Details collects
contact information for the user and allows them to linked with, or unlinked from, any of the
CCNs associated with the primary Survey Administrator.

X. The OAS CAHPS Survey Web Portal December 2015
126 Centers for Medicare & Medicaid Services Outpatient and Ambulatory Surgery CAHPS Survey Protocols and Guidelines Manual
Exhibit 10.7 Manage User Console
Step 4: The OAS CAHPS Survey Administrator or backup completes the Vendor
Authorization Form. After an HOPD or ASC has entered into a contract with a survey vendor,
the facility must authorize a survey vendor to submit data on its behalf before the survey vendor
can successfully submit OAS CAHPS data for that facility. Facilities should note that survey
vendors must submit their clients’ survey data to the OAS CAHPS Data Center by the following
deadlines: the 2nd
Wednesday in July, October, January and April. For further details, see Table
14.2 in Chapter XIV, Public Reporting.
To authorize a vendor, facility’s OAS CAHPS Survey Administrator must log in to the secure
web portal and proceed to the ‘Vendor Authorization” sub menu under the “For facilities” tab.
The sub menu provides three options for users:
• Start an Authorization;
• Delete an Authorization;
• Authorization Report.
A brief description and the steps in each of these actions are provided below. Note that an
automatic e-mail will be sent to the HOPD and/or ASC OAS CAHPS Survey Administrator
confirming that the vendor has been authorized soon after the authorization has been submitted.
December 2015 X. The OAS CAHPS Survey Web Portal
Centers for Medicare & Medicaid Services 127 Outpatient and Ambulatory Surgery CAHPS Survey Protocols and Guidelines Manual
1. Start an Authorization. This is used both by an HOPD or ASC that is just beginning to
participate in OAS CAHPS, as well as by an HOPD or ASC which is switching to another
vendor. The OAS CAHPS Survey Administrator will:
◦ Select an approved vendor from the dropdown list (note that the list of approved vendors
will be available beginning in December 2015 and updated on a flow basis);
◦ Select the “Start Date,” which is the first day of the first calendar year quarter (either
January 1, April 1, July 1, or October 1) for which the vendor is being authorized to
submit OAS CAHPS data. For example, if a vendor is authorized to submit data
beginning January, February or March, the Survey Administrator should choose a Start
Date of January;
◦ Select the CCN or CCNs to which the authorization applies; and
◦ Click the “Submit” button.
To change or switch to a different survey vendor, the HOPD or ASC will follow the same
process in above. The system will automatically assign an end date for the existing
authorization, based on the start date of the new authorization. This will ensure that there are
no gaps in authorization time periods.
The system will allow an HOPD/ASC to change a start date for multiple CCNs. This would
be useful for someone who is serving as the OAS CAHPS Survey Administrator for example
for several ASCs which are under different CCNs but are linked organizationally. To select
multiple CCNs, the OAS CAHPS Survey Administrator should check the box next to the
name of each CCN for which this vendor is authorized to submit data. The administrator
should click to Submit button to save the entries selected.
HOPDs and ASCs should note the following details regarding switching vendors:
◦ HOPDs/ASCs may switch vendors only at the beginning of a quarter. This is because
data for every month in a quarterly submission must come from a single vendor.
Consider the three months below.
Sample month Survey takes place Data submitted to the
OAS CAHPS Data Center
January February through April July
February March through May July
March April through June July

X. The OAS CAHPS Survey Web Portal December 2015
128 Centers for Medicare & Medicaid Services Outpatient and Ambulatory Surgery CAHPS Survey Protocols and Guidelines Manual
These sample months all go into the same quarterly delivery to the OAS CAHPS Data
Center. One vendor cannot supply January data and a second vendor supply February
and March data because that will mean that there must be two vendors for a single
submission. That is why vendors may only be switched for the beginning month of a
data delivery quarter.
◦ Survey vendors may not submit data files after the data submission deadline passes for a
quarter; therefore, it is critically important that HOPDs/ASCs make sure the End Data for
their old vendor and Start date for the new vendor are correct, well in advance of the data
submission deadlines.
◦ The Vendor Authorization form is an authorization to submit data, not an authorization to
conduct the survey. More than one vendor at a time may collect data (in the chart below,
note the overlapping times for Vendors A and B to conduct the survey). However, only
one vendor at a time can submit data. Vendor A who is collecting data through 6/2 needs
to be authorized to submit that data in the July 13 submission―which falls within quarter
3 (quarter 3 dates are 7/1 through 9/30). Vendor B who is collecting data beginning 5/21
needs to be authorized to submit data in the October 10 submission ― which falls within
quarter 4 (quarter 4 dates are 10/1 through 12/31).
Sample month
Begin conducting
survey
End conducting
survey
Quarterly data submission deadline to
OAS CAHPS Data Center
Authorization begin date
(starting day of first calendar
quarter)
Authorization end date
(ending day of final calendar
quarter)
Vendor A Feb–March 3/21/2016 6/2/2016 7/13/2016 1/1/2016 9/30/2016
Vendor B April-and on 5/21/2016 No end date 10/10/2016 10/1/2016 No end date
2. Delete an Authorization. This function will allow an HOPD/ASC to delete an existing
authorization. The reason an ASC/HOPD may want to delete an authorization is to revise its
end date or revise it to show a different vendor. After deleting the existing authorization,
follow the steps in Start an Authorization to create the authorization with the start date and
vendor that you desire. The system will allow an HOPD/ASC to change a start date or
vendor for multiple CCNs. This would be useful for someone who is serving as the OAS
CAHPS Survey Administrator for example for several ASCs which are under different CCNs
but are linked organizationally. To select multiple CCNs, the OAS CAHPS Survey
Administrator should check the box next to the name of each CCN for which this vendor is
authorized to submit data. The administrator should click to Submit button to save the
entries selected.
3. Authorization Report. This function will allow HOPDs/ASCs to view the list of facilities for
which a vendor has been authorized, and the current vendor’s name, and the Start Date for

December 2015 X. The OAS CAHPS Survey Web Portal
Centers for Medicare & Medicaid Services 129 Outpatient and Ambulatory Surgery CAHPS Survey Protocols and Guidelines Manual
each vendor. If the HOPD/ASC entered an End Date for the vendor currently authorized, the
End Date will also show.
Survey Vendors Users
Step 1: The individual designated as the survey vendor’s OAS CAHPS Survey
Administrator will complete an online Vendor Registration Form. This form is located on the
public side of the web portal. To locate this form, click on the “Vendor Registration Form” link
under the “Forms for Vendors” navigation tab on the OAS CAHPS web portal (as shown in
Exhibit 10.8). When completing the Vendor Registration Form, the vendor’s OAS CAHPS
Survey Administrator will establish an account and create credentials for accessing the secure
sections of the web portal.
The form will collect the vendor’s OAS CAHPS Survey Administrator’s name, e-mail address,
and telephone number. The Survey Administrator will also be instructed to create a username
and password that will be used to access the secured links and forms on the private side of the
web portal, including the Vendor Application. Once all information is entered and correct, click
the “Submit” button.
Once it is submitted, the Survey Administrator will be routed to a dashboard created specifically
for that survey vendor.
Exhibit 10.8 Vendor Registration Form Link

X. The OAS CAHPS Survey Web Portal December 2015
130 Centers for Medicare & Medicaid Services Outpatient and Ambulatory Surgery CAHPS Survey Protocols and Guidelines Manual
Step 2: Complete the Vendor Application Form. This form is located on the private side of
the OAS CAHPS Survey web portal. It is divided into four pages. Vendors need to save each
page in order to proceed to the next. The application will time out after 60 minutes of inactivity.
The OAS CAHPS Survey Administrator can save and return to it as many times as needed to edit
responses input into the page. When the application is complete and accurate, click “Submit” to
submit the application. The vendor application form appears in Appendix A.
After the application has been completed, a new window will appear with a copy of the OAS
CAHPS Survey Vendor Consent Form, customized for the registering survey vendor.
The OAS CAHPS Survey Vendor Consent Form is a document on which the person designated
as the OAS CAHPS Survey Administrator will acknowledge that he or she accepts the roles and
responsibilities of the Survey Administrator for the listed survey vendor. The Survey
Administrator will print a hardcopy version of the Consent Form. Then, review, sign and date
this form in the presence of a Notary Public, and obtain the notary’s signature and seal on the
form. Mail the notarized OAS CAHPS Survey Vendor Consent Form to the OAS CAHPS Data
Center at the address provided at the top of the form.
Step 3: Periodically check their Vendor Authorization Status. As explained above in Step 4
for HOPDs and ASCs, the HOPD’s/ASC’s OAS CAHPS Survey Administrator is required to
authorize a survey vendor to submit OAS CAHPS data on their behalf. Survey vendors should
check periodically to ensure that each client HOPD and/or ASC with which they have contracted
has accurately completed the online Authorize a Vendor Form and that the Start Date the facility
entered is the first day of the first quarter in which the vendor is authorized to submit data on the
facility’s behalf. ASCs, HOPDs, and survey vendors should note that CMS will not allow OAS
CAHPS vendors to submit data files after the data submission deadline passes for a quarter;
therefore, it is critically important that facilities authorize the vendor and make sure that the Start
Date is correct well in advance of a data submission deadline.
The Vendor Authorization Status report is available under the vendor’s customized dashboard.
User Dashboards and Secure (Access-Restricted) Links
The private OAS CAHPS web portal menu options differ slightly from those on the public web
portal. In Exhibit 10.1, the items with an asterisk are accessible only on the private pages of the
web portal and with proper login credentials and authorization. Access to the secure sections
will be restricted and controlled through a user identification and password, created by the
survey vendor, HOPD or ASC Survey Administrator during the registration process. Once
logged into the secure side of the web portal, OAS CAHPS Survey Administrators will be routed
to a dashboard created specifically for their organization.

December 2015 X. The OAS CAHPS Survey Web Portal
Centers for Medicare & Medicaid Services 131 Outpatient and Ambulatory Surgery CAHPS Survey Protocols and Guidelines Manual
Each of the “Dashboard” views (Facility Dashboard and Vendor Dashboard) provides the user
with links to key items on the web portal, depending on the user.
• Vendors are provided with the status of key elements of the Vendor Approval Process—
including the status of and links to their vendor application, consent form, and overall
approval status; a User console, showing administrative users within the organization; and
links to both data submission reports and reports showing the HOPDs and ASCs that have
authorized them.
• HOPDs and ASCs are provided with links to all of the documents required for the
registration and vendor authorization process, including links to the vendor authorization
form; a User console, showing administrative users within the organization; recent
announcements; and links to their data submission and latest preview reports.
Facility Dashboard
Each time the ASC’s or HOPD’s OAS CAHPS Survey Administrator logs into the web portal, he
or she will be taken to the Facility Dashboard (see Exhibit 10.9). The dashboard will guide the
Survey Administrator through the rest of the registration process, including printing out and
completing the OAS CAHPS Survey Administrator Consent Form. Survey Administrators should
note that they can register additional HOPDs or ASCs at any time using the dashboard.
The Facility Dashboard also includes:
• An Authorize a Vendor link that allows the HOPD’s or ASC’s OAS CAHPS Survey
Administrator to select a CMS-approved survey vendor to submit data on behalf of the
facility.
• A Manage Users Console link, where the Survey Administrator can add or delete authorized
users for certain functions on the web portal.
• Reports, including data submission and latest preview reports.
• Recent announcements posted on the web portal.
HOPDs and ASCs are responsible for checking the web portal announcements displayed both on
their dashboard and the OAS CAHPS web portal homepage regularly for updates.

X. The OAS CAHPS Survey Web Portal December 2015
132 Centers for Medicare & Medicaid Services Outpatient and Ambulatory Surgery CAHPS Survey Protocols and Guidelines Manual
Exhibit 10.9 Facility Dashboard
Vendor Dashboard
Each time the survey vendor’s OAS CAHPS Survey Administrator logs into the web portal with
the login credentials created during the registration process, he or she will be taken to the Vendor
Dashboard (see Exhibit 10.10). From the dashboard, survey vendors can complete and submit
the Vendor Application and Vendor Survey Administrator Consent Form during periods in which
the Coordination Team is accepting vendor applications. The Vendor Application must be
completed to be considered for approval as a CMS-approved survey vendor.
Exhibit 10.10 Vendor Dashboard
December 2015 X. The OAS CAHPS Survey Web Portal
Centers for Medicare & Medicaid Services 133 Outpatient and Ambulatory Surgery CAHPS Survey Protocols and Guidelines Manual
The Vendor Dashboard also includes the following tools or links:
• Manage Users Console, where the Survey Administrator can add or delete authorized users
on the web portal;
• Data Submission Tool, where the Survey Administrator can upload and submit survey data
on behalf of his or her client HOPDs and/or ASCs; and
• Reports, including Vendor Authorization Status reports and data submission reports.
System and Security Requirements for the OAS CAHPS Web Portal
Approved survey vendors will submit or upload OAS CAHPS Survey data to the OAS CAHPS
Data Center through a link on the OAS CAHPS web portal. The security level for users’
browser Internet zone must be set to the equivalent of medium or lower, at least during the time
that they are working in the project web portal.
Data Security
OAS CAHPS survey vendors are required to submit only de-identified data files to the OAS
CAHPS web portal. This means that no personally identifiable patient information can be
included in the data files that are submitted to the OAS CAHPS Data Center. Vendors are
required to assign a unique sample identification (SID) number to each sampled patient included
in the survey. The data submitted must include an SID for each patient included in the sample,
regardless of whether the sample member completed the survey. More information about
assigning a unique SID to each sampled patient is included in Chapter IV.
Even though only de-identified data will be submitted to the OAS CAHPS Data Center, every
measure will be taken to protect and secure OAS CAHPS data. Ensuring data security was a
concern and consideration during the design and development of the OAS CAHPS web portal.
The web portal balances a straightforward and flexible design with the need to protect the
privacy and security of OAS CAHPS data. Data are encrypted whenever vendors upload their
data files. The OAS CAHPS Survey Coordination Team has implemented a number of policies
and procedures to ensure that all communications and transfers are secure. Among these
measures are the following:
• requiring that each individual provided access to the private links on the web portal must
have a secure login;
• requiring users to create and use a strong password;
• using Secure Sockets Layer (SSL) technology to encrypt files for transmission; and
• carefully monitoring uploads, upload attempts, and web portal use in general.

X. The OAS CAHPS Survey Web Portal December 2015
134 Centers for Medicare & Medicaid Services Outpatient and Ambulatory Surgery CAHPS Survey Protocols and Guidelines Manual
When users log into the private links on the web portal, the system will automatically check and
authenticate their credentials before allowing access. This ensures that only authorized users log
into the system.
In addition to allowing only credentialed users access to the private links on the web portal, all
electronic data are stored behind a firewall in a password-protected network. All data traffic
between the vendor’s network and the Internet pass through this single connection point. This
process provides the same level of protection and monitoring to all systems connected to the
vendor’s network. The web portal firewall is programmed to allow or prevent access to the
network by using a set of rules to determine whether attempted network access is in compliance
with the OAS CAHPS Data Center’s network security policy. In addition, the firewall logs all
incoming traffic to help detect and analyze any problems or suspicious activity.
Survey Vendor’s Web Portal Security Responsibilities
All OAS CAHPS survey vendors must go through an application and certification process to
participate in the survey. In addition, vendors must agree to strict requirements to continue their
participation. By following the security procedures identified for the project, survey vendors
will protect their client HOPDs’ and ASCs’ data and those of other vendors participating in OAS
CAHPS.
All OAS CAHPS survey vendors must also abide by all requirements set forth in the Health
Insurance Portability and Accountability Act of 1996 (HIPAA), legislation intended to protect
private health information and to improve the efficiency of the health care system. The type of
patient information that is protected under HIPAA is called “Protected Health Information” or
PHI. PHI is defined as personally identifiable information (PII) that relates to a person’s past,
present, or future health or medical treatment. If the health information is completely de-
identified, it is no longer considered PHI and can be released. HIPAA applies to all electronic
and hardcopy records whether they are being stored or transmitted.
OAS CAHPS survey vendors must safeguard all data collected from patients as required by
HIPAA. However, survey vendors will not submit any confidential information to the OAS
CAHPS Data Center as all of data file submissions will contain only de-identified data. Even
with de-identified data files, vendors must still use security measures to keep the data as safe as
possible. This means that when issued credentials to access the private links on the project web
portal, survey vendors also must follow all safeguards to prevent an unauthorized person from
entering the private side of the web portal. Therefore, the OAS CAHPS Data Center has
password protected the private side of the web portal and requires that approved survey vendors,
HOPDs and ASCs use the following guidelines when creating and maintaining their password:
• When an OAS CAHPS survey vendor, HOPD’s or ASC’s account is approved, the user will
be able to log into the system and change the password on first login.

December 2015 X. The OAS CAHPS Survey Web Portal
Centers for Medicare & Medicaid Services 135 Outpatient and Ambulatory Surgery CAHPS Survey Protocols and Guidelines Manual
• Each account will be locked out after five successive incorrect password entries. If the
account is locked, the user will need to contact the OAS CAHPS Survey Coordination Team
to have the account unlocked.
If a user’s password is compromised or lost, contact the OAS CAHPS Survey Coordination
Team immediately to ask that the account be deactivated. The Coordination Team will then
issue new credentials to the user.
Web Portal Password Generation and Protection
As indicated, data security is of utmost concern to the OAS CAHPS Survey Coordination Team.
When survey vendors, HOPDs, and ASCs generate a password to access the private links on the
project web portal, they must develop a strong password. A strong password is defined as one
that contains at least nine (9) characters. These nine characters must include the following:
• one upper-case alphabet letter,
• one numeral, and
• one special character (&,%,#,!).
An example of a strong password is Mgh0721$&; it meets the required criteria shown above.
These password rules and guidelines are designed to minimize the chance that automated
password-cracking routines used by unauthorized personnel can gain access to the web portal. In
addition to the above rules, the following guidelines will help create a strong password:
• Combine two or more related words with punctuation, such as Radio-Cook.
• Use a password that looks like nonsense but allows an easy way to remember it, such as
“Thaawtsom.” for “The hills are alive with the sound of music.” (Note the end punctuation.)
• Think in terms of vanity license plates, such as “I8myfood.”
The following should be avoided when creating a password; therefore, do not use:
• a single English word;
• a scientific name, biological term, geographic name;
• a person’s name or part of name, even with slight modifications like an added character at the
end or beginning;
• known combinations (e.g., NLRB 1234, attorney1, judge111);
X. The OAS CAHPS Survey Web Portal December 2015
136 Centers for Medicare & Medicaid Services Outpatient and Ambulatory Surgery CAHPS Survey Protocols and Guidelines Manual
• words found in a dictionary, including names, obscene words, or well-known phrases;
• a password with a repeating series of characters;
• reverse spellings of dictionary words;
• a name associated with the user in any way (middle name, family names, pet’s name, sports
team name, films, etc.);
• portions of a User ID on the current or other systems; or
• simple keyboard patterns (e.g., “asdfjkl.”).
In addition, a user should never write down his or her password. If the user needs to store
passwords, there are free applications that can be downloaded and used. An application like this
can be very helpful because another password safety rule is to never use the same password
across applications or computers. Finally, do not share or give the password to anyone. OAS
CAHPS survey vendors, HOPDs, and ASCs are responsible for all access to the private links on
the project web portal that are made under their credentials.
What To Do If a User Forgets the Password
If a user forgets his or her password, simply click on the Forgot Password link on the Login
screen on the OAS CAHPS web portal. Survey vendors, HOPDs, and ASCs can request a
password by providing the username. OAS CAHPS Data Center project staff will send the
user’s password to him or her via e-mail at the e-mail address provided on the registration form.
When the e-mail containing the password is received, promptly delete it, then log in and change
the password immediately.

December 2015 X. The OAS CAHPS Survey Web Portal
Centers for Medicare & Medicaid Services 137 Outpatient and Ambulatory Surgery CAHPS Survey Protocols and Guidelines Manual
This page intentionally left blank.
Centers for Medicare & Medicaid Services 138 Outpatient and Ambulatory Surgery CAHPS Survey Protocols and Guidelines Manual
XI. FILE PREPARATION AND DATA SUBMISSION
Overview
Survey vendors will construct and submit a data file containing three sections; 1) a header
record, 2) a patient administrative record for every sampled case, 3) a response record for every
completed survey in each monthly Outpatient and Ambulatory Surgery CAHPS (OAS CAHPS)
Survey sample. Vendors will submit data files for each of their client hospital outpatient surgery
departments (HOPDs) and ambulatory surgery centers (ASCs). Data for all three monthly
samples in a calendar quarter must be submitted by a specific data submission deadline for each
quarter. Data will be submitted to the OAS CAHPS Data Center through the OAS CAHPS web
portal.
Data File Preparation
OAS CAHPS vendors will submit XML data files for each HOPD or ASC that has authorized
the vendor to submit data on the facility’s behalf. All OAS CAHPS data files must contain a
record for each patient who was sampled at the HOPD or ASC for each month of the quarterly
submission period. Survey vendors will submit data at least once each quarter by uploading
individual .xml files or a zipped file of multiple XML files. During the data file upload process,
the survey vendor’s data are encrypted (scrambled so that they are unreadable) until they are
received by the Coordination Team and checked for errors. This means that an OAS CAHPS
vendor’s data will remain secure from the beginning of the upload process onward.
The data file submission steps that OAS CAHPS vendors will follow to submit OAS CAHPS
data files are shown below.
3. Format and prepare survey data following the XML file specifications.
4. Submit data file(s) via the OAS CAHPS web portal.
5. Review and follow -up on Data Upload Reports.
Each of these steps is described in the following sections.
Step 1: Format and Clean Survey Data Following the XML File Specifications
Each XML file should contain only 1 month of survey data for all HOPD or ASC locations under
a specific CMS Certification Number CCN. The OAS CAHPS XML file structure is included in
Appendix K. The specifications in that document contain details about the data to be submitted

December 2015 XI. File Preparation and Data Submission
Centers for Medicare & Medicaid Services 139 Outpatient and Ambulatory Surgery CAHPS Survey Protocols and Guidelines Manual
such as data type, field sizes, and order. The format of each OAS CAHPS data file must match
the specification provided in that Appendix. Survey vendors can also download the XML data
file template from the OAS CAHPS web portal. The XML templates were developed based on
data elements needed for analysis and on the OAS CAHPS questionnaire.
The XML file format will allow data for all patients sampled during a given sample month to be
submitted in one file. Survey vendors should note that if a data file for a sample month is
submitted more than once, the most recent data submission will overwrite the file previously
submitted for that sample month, even if those files “passed” all checks. Therefore, the final
file submission must contain data for all patients who were sampled in that sample month
for all HOPD or ASC locations under a specific CCN. OAS CAHPS vendors should note that
a data file must pass both validation checks before the file is accepted. One check is completed
immediately upon upload and the second validation check is completed within 10 minutes of
upload. We highly recommend that vendors submit data submission files as early as possible to
allow time for any errors detected during the validation checks to be corrected and to resubmit
the file.
The data file specifications for OAS CAHPS XML files are described below and included in
Appendix K. If disproportionate stratified random sampling (DSRS) is used, approved survey
vendors must use the XML for DSRS. The DSRS data file specifications are provided in
Appendix L.
XML Data File Specifications
OAS CAHPS survey vendors must submit data using the XML format only. Survey vendors that
need assistance with the XML format should contact the OAS CAHPS Survey Coordination
Team for technical assistance at 1-866-590-7468 or by sending an e-mail to [email protected].
Each XML file will consist of three sections: a Header Record, a Patient Administrative Data
Record, and the Patient Response Record. Each of these sections is described below. There
should be only one header record for each OAS CAHPS XML file. Each patient within the
XML file should have an administrative data record. A survey response record must be included
for every sampled patient who completed the survey questionnaire (via mail or telephone).
HOPDs, ASCs, and their survey vendor should keep in mind that an OAS CAHPS data file must
be submitted for each sample month.
XI. File Preparation and Data Submission December 2015
140 Centers for Medicare & Medicaid Services Outpatient and Ambulatory Surgery CAHPS Survey Protocols and Guidelines Manual
Header Record
The Header Record contains the following data elements:
• Header Type
• Provider Name. This is the HOPD’s or ASC’s Provider Name
• Provider Number This is the HOPD’s or ASC’s CCN.
• Sample Year. This is the calendar year in which the survey is conducted.
• Sample Month. Survey vendors will select a sample of patients who meet survey eligibility
criteria for each calendar month. The Sample Month is the month for which the sample was
selected.
• Mode of Survey Administration. The survey mode, either mail only, phone only, or mixed
mode, must be the same for all sample members in each sample month in the calendar
quarter for all of the HOPD or ASC locations under the same CCN. HOPDs, ASCs, and
their survey vendors cannot change survey administration modes until a new quarter begins.
Also note that the survey mode indicated in the Header Record must be one of the modes that
the survey vendor is approved to use. If the mode is not one of the modes for which the
vendor is approved, the Data Center will not accept the data file when the vendor attempts to
submit it.
• Type of Sampling. This is the sampling method that was used to select the sample—these
include census, simple random sampling (SSS), stratified systematic sampling, proportionate
stratified random sampling (PSRS), and disproportionate stratified random sampling (DSRS).
See Chapter IV for information about each of these methods.
• Number of Patients Served. This is the total number of patients who had at least one
outpatient surgery or procedure during the sample month at the ASC or HOPD. This number
should reflect all patients who received outpatient care in the sample month regardless of
eligibility of that surgery, or of that patient, for OAS CAHPS. CCNs which contain multiple
HOPD or ASC locations should note that this value should reflect the total number of
patients served across all eligible HOPD/ASC locations. If the eligible ASC(s) or HOPD(s)
served no patients during the sample month, enter zero for this variable on the data file for
this sample month.
• Number of Patients on the File Submitted by the HOPD(s) or ASC(s). As was explained
in Chapter IV, the facility should withhold various categories of patients from the monthly
patient information file that it supplies to vendor. These types of patients are: patients who
are deceased, are not 18 years old or older, were discharged after their procedure to hospice,

December 2015 XI. File Preparation and Data Submission
Centers for Medicare & Medicaid Services 141 Outpatient and Ambulatory Surgery CAHPS Survey Protocols and Guidelines Manual
currently reside in a nursing home, are prisoners, or who requested that the facility not
release their name to anyone outside that facility. This vendor should count the number of
patients which the facility supplies and indicate that number on the data file for this sample
month. As stated regarding Number of Patients Served, this value should reflect patients
across all eligible HOPD or ASC locations in the CCN; if no patients were served during the
sample month zero should be entered.
• Number of Eligible Patients. This is the number of patients in the file submitted by the
HOPD or ASC which meet survey eligibility criteria in the sample month. As explained in
Chapter IV, patients whose CPT codes are not within the eligible range are ineligible. It is
acceptable for either the facility or the vendor to remove these ineligible patients. As stated
regarding Number of Patients Served, and Number of Patients on the File Submitted by the
HOPD(s) or ASC(s), this value should reflect patients across all eligible HOPD or ASC
locations in the CCN. This value can be zero only if none of the patients on the file provided
by the HOPD or ASC for the sample month was eligible for the survey.
• Number of Patients Sampled. This is the number of patients selected for the survey during
the sample month. This value can be zero only if all of the patients included on the file that
the HOPD or ASC provided for the sample month were ineligible for the survey. If a value
of zero is entered for this variable, the value for the Number of Eligible Patients variable
must also be zero.
If DSRS is used, the survey vendor must use the specific DSRS header. The DSRS has these
extra data elements in the Header Record:
• DSRS Stratum Name (note that there must be at least two strata identified for DSRS
sampling).
• DSRS Number of Patients on file submitted to vendor, which is the number of patients
included on the file that all of the HOPD or ASC locations that share a CCN provided for this
stratum.
• DSRS Number of Patients eligible in stratum, which is the number of patients who meet
survey eligibility criteria within each stratum.
• DSRS Number of Patients sampled in stratum, which is the number of patients sampled
within the stratum.
Please remember that approved OAS CAHPS vendors must complete and submit an Exceptions
Request Form to the Coordination Team prior to sampling if their HOPD or ASC chooses to use
DSRS (see Chapter XV for more information about the Exceptions Request Form). If a vendor
submits a data file with a DSRS Header record and does not have prior approval for using DSRS,

XI. File Preparation and Data Submission December 2015
142 Centers for Medicare & Medicaid Services Outpatient and Ambulatory Surgery CAHPS Survey Protocols and Guidelines Manual
the data file will be rejected. More information about DSRS and requirements for DSRS sample
selection and file construction is provided in Chapter IV.
Patient Administrative Data Record
The second section of the XML file contains data about each patient who was sampled for the
sample month, including both those who responded to the survey and nonrespondents. In this
section of the file, some of the information provided in the Header Record is repeated, including
the HOPD’s or ASC’s CCN and the Sample Year and Sample Month. All other information
included in this section of the file is about the patients included in the sample. There must be a
Patient Administrative Record for every patient sampled in the sample month. The sample
identification (SID) number assigned to each sample member must be included. Only de-
identified data will be submitted to the OAS CAHPS Data Center; however, the unique SID
number that the survey vendor assigned to the sample member must be included on the file. Files
submitted with missing and/or duplicate SID numbers will be rejected.
Most of the information required in the Patient Administrative Data Record is provided by, or
derived from, information the HOPD or ASC submits to the vendor on the monthly patient
information file. The vendor will calculate the sample member’s age based on the date of birth
provided by the HOPD or ASC). The survey vendor will classify each patient’s surgery as either
gastrointestinal, orthopedic, ophthalmologic, or other according to the CPT or G code. If CPT
code(s) in range 40000–49999 or G-code(s) G0105, G0121, or G0104, assign surgical category
1. If CPT code(s) in range 20000–29999 or G-code is G0260, assign surgical category 2. If CPT
code(s) in range 65000–68899, assign surgical category 3. If CPT code(s) or G codes not in the
range for surgical categories 1, 2 or 3, assign surgical category 4.
The survey vendor will also compute the lag time which reflects the number of days that elapsed
between the date of surgery and the date the survey was initiated for that patient. See
Appendix K, XML Data File Layout for instructions and coding specifications.
The information in the last part of this section is survey administration data compiled by the
survey vendor. This information includes the Final Survey Status (also known as disposition
code) assigned to each case and survey language.
Patient Response Record
The third section of the XML file is the patient response record, which contains the responses to
the OAS CAHPS survey from every patient who answered the survey during the sample month.
Note that only the OAS CAHPS survey questions should be submitted. Do not submit
responses to non-OAS CAHPS questions (i.e., supplemental questions) that were added by
the HOPD or ASC. The only records that should be included are those with a final Survey
Status code for a completed survey (Codes 110 and 120) and those with Code 310 (Break-Off).

December 2015 XI. File Preparation and Data Submission
Centers for Medicare & Medicaid Services 143 Outpatient and Ambulatory Surgery CAHPS Survey Protocols and Guidelines Manual
For all patient response records that are included on the file, all response fields must have a
legitimate value, which can include “Missing,” or “Not Applicable.”
The decision whether to key the responses to the two open-ended survey items―“Other
language” (response option 2) in Q35 and “Helped in some other way” (response option 5) in
Q37―is up to each individual HOPD or ASC. Vendors should not include responses to open-
ended survey items on the data files submitted to the OAS CAHPS Data Center. CMS, however,
encourages survey vendors to review the open-ended entries so that they can provide feedback to
the Coordination Team about adding additional preprinted response options to these survey
items, if needed.
Step 2: Data File Submission
OAS CAHPS vendors should follow the steps outlined below for submitting data via the OAS
CAHPS web portal:
1. Login to the OAS CAHPS web portal; when logged in, the system will display the
vendor’s dashboard.
2. Click the “Submit Data” link under “Data Submission” The data submission tool page
will display (as shown in Exhibit 11.1)
3. Click the “Select” button to select the file to upload. The Select button permits users to
locate and directly upload a file that has been saved in their own computer system.
Survey vendors can select either a single XML file or a single ZIP file that contains
multiple XML files.
4. After selecting the file to be uploaded, click “Upload XML” to submit the file. The Data
Submission Summary Report based on the file selected will appear. A link to this report
will also be e-mailed to the vendor’s OAS CAHPS Survey Administrator.
5. To upload more than one file at a time, click the “Add” button on the same screen.
Additional file selection rows will be added. Repeat Step 3 above for each file to be
uploaded.
6. To remove rows that have been added, click the “Remove” button to the right of the row
to be deleted.

XI. File Preparation and Data Submission December 2015
144 Centers for Medicare & Medicaid Services Outpatient and Ambulatory Surgery CAHPS Survey Protocols and Guidelines Manual
Exhibit 11.1 Link to Data Submission Tool
Exhibit 11.2 shows how the screen looks when submitting multiple files for uploading to the
private side of the web portal.
As the upload begins, the XML file will undergo validation checks. The first check will
determine whether the CCN(s) in the header record and the patient administrative file are aligned
for the client ASC’s or HOPD’s authorized survey vendor and the facility’s CCN. The next
validation checks will determine the quality and completeness of the data.
If the file fails any of the validation checks, the survey vendor will receive an error message
within seconds after a file error is detected noting that the file upload failed, giving details on
why the file failed to upload. For example, the message may indicate that there is no
authorization from the HOPD or ASC for the survey vendor to submit data on its behalf or that
the number of patient records listed in the Header Record does not match the number of sample
members for which data are provided in the Patient Administrative Record section of the file.
If a file does not pass the upload validations, none of the data on the file are accepted and stored
in the Data Center. Survey vendors must review data submission reports (discussed in
Chapter XII) and correct any data errors on the XML file and resubmit the file. CMS will not
accept data files that are submitted after the quarterly data submission deadline. We strongly
encourage survey vendors to submit their data files well in advance of the data submission
deadline for a survey period. Survey vendors can resubmit a data file for an HOPD or ASC
client as many times as needed prior to the data submission deadline. However, survey vendors
must keep in mind that each time a data file for an HOPD or ASC is submitted, it overwrites any
data for that same facility that were previously submitted for that survey period.

December 2015 XI. File Preparation and Data Submission
Centers for Medicare & Medicaid Services 145 Outpatient and Ambulatory Surgery CAHPS Survey Protocols and Guidelines Manual
Exhibit 11.2 Uploading Multiple Files
Step 3: Review and Follow -Up on Data Upload Reports
There are three reports that are available to survey vendors via the OAS CAHPS web portal.
These reports serve to inform survey vendors about the outcome of each of the vendor’s data file
upload attempts, and they also provide the vendor with a history of upload efforts, successful or
unsuccessful. The three reports are listed below:
• Data Submission Summary Report;
• Data Submission History Report; and
• Data Submission History by Upload Date.
Each of these reports is described in detail in Chapter XII.
Quarterly Data Submission Deadlines
Survey vendors have the option of submitting a data file to the OAS CAHPS Data Center as data
collection and processing activities for each monthly sample are completed or on a quarterly
basis. However, the data file for all months in a specific quarter for each client HOPD or ASC
must be submitted before the submission deadline for that quarter.
Data Center staff will check all data files immediately after they are submitted to ensure that they
pass the initial verification checks. Any files in which problems are detected or that do not
comply with file specification requirements will not be accepted by the Data Center. Survey
vendors are also reminded again that all data files undergo validation checks immediately upon
upload and the second validation check is completed within 10 minutes of upload. OAS CAHPS
data files must pass both validation checks before they are accepted. Survey vendors are

XI. File Preparation and Data Submission December 2015
146 Centers for Medicare & Medicaid Services Outpatient and Ambulatory Surgery CAHPS Survey Protocols and Guidelines Manual
strongly encouraged to submit data files well in advance of a data submission deadline in case
there are problems that must be corrected before the data file is accepted. Survey vendors are
also strongly encouraged to check the Data Submission Summary reports that are posted on the
web portal (these reports are discussed in the next chapter) to ensure that the files are accepted.
Potential Situations When Vendors Will Not Submit Data
If there is a Survey Vendor Authorization in effect (explained in Chapter X, Step 4) the OAS
CAHPS Data Center will expect the survey vendor to submit data for the contract HOPD or ASC
for every quarter. If the survey vendor fails to submit, the HOPD/ASC is considered
noncompliant for that quarter, with respect to CMS National Implementation.
However, there are situations when a survey vendor will not be able to submit data. The
paragraphs below describe those situations and instruct survey vendors how to proceed so as not
to be noncompliant
Survey Not Yet in Effect
Survey vendor authorizations (described in Chapter X) are put into effect on a quarterly basis,
and remain in effect until they reach the end date (if any) of the authorization period. Should an
HOPD/ASC authorize a vendor for Quarter 1 beginning in January, yet begin collecting data
mid-quarter (for example, March) the elapsed months between quarter start and survey start (in
this example, January and February) will not have survey data. Survey vendors must submit a
Exceptions Request Form (ERF) to the OAS CAHPS Survey Coordination Team to explain this
situation. Once this ERF is on record and approved, the survey vendor and their client
ASC/HOPD will not be considered non-compliant.
Closed CCN or Closed Location Within a CCN
If an HOPD or ASC closes or is no longer active while its OAS CAHPS vendor is still contracted
to conduct and provide survey data on its behalf, the vendor authorization that that HOPD or
ASC submitted will remain in effect for the entire authorization period. It remains in effect until
either the facility’s OAS CAHPS Survey Administrator modifies the end date of the
authorization, or, alternatively until the OAS CAHPS Survey Coordination team marks the CCN
as inactive/closed. Survey vendors should contact the OAS CAHPS Survey Coordination team
to inform them if a client facility closes or becomes inactive. The Survey Coordination team will
mark this CCN as inactive. Inactive HOPDs or ASCs are viewable on the Vendor Authorization
Report and are designated with an asterisk (*) symbol.
If the CCN remains active but one of the HOPD or ASC locations or entities within it closes, the
remaining active HOPD(s)’ or ASC(s)’ location(s) should continue participating in OAS
CAHPS.

December 2015 XI. File Preparation and Data Submission
Centers for Medicare & Medicaid Services 147 Outpatient and Ambulatory Surgery CAHPS Survey Protocols and Guidelines Manual
Data Submission Quality Control
The following issues and guidelines are provided to assist vendors in making sure that XML files
are prepared properly and that quality control measures are conducted on each file before the
vendor attempts to submit the file to the OAS CAHPS Data Center. Implementing adequate
quality control on XML files, and submitting each file well in advance of the data submission
deadline, will help ensure that each HOPD’s or ASC’s monthly data files are accepted and that
high-quality data are submitted. Quality control checks should be conducted by a different staff
person than the one who completed the task.
Verify that the vendor is authorized to submit data. Vendors should check the Survey Vendor
Authorization Report regularly to make sure that each of their clients has authorized the vendor
to submit data on their behalf and that the Start Date the HOPD or ASC entered represents the
first month of the quarter for which the vendor collected data on the HOPD’s or ASC’s behalf.
Help ensure proper file format by using the validation tools on the OAS CAHPS website.
The following can be downloaded from the OAS CAHPS website:
• Templates for the XML files
• XML schemas
• Schema validation tool
• Data submission tips
Vendors should apply the validation schema posted on the OAS CAHPS web portal on each data
file. This validation tool contains some of the same validation checks that are applied when the
data file is submitted to the Data Center. Using the validation schema to identify file problems
and correcting any problems detected will reduce the number of attempts to submit the data file.
Perform additional quality control checks. In addition to using the validation schema, survey
vendors are encouraged to make additional quality control checks on the data files before they
attempt to submit the files to the Data Center. Some suggested quality checks are listed below.
a. Check the sample month entered on the XML file to verify that the sample month is
correct. The OAS CAHPS Data Center will not accept a data file for a sample month in a
previous data submission quarter, but it will accept files for months in the current and
upcoming data submission quarters. Similarly, make sure that the sample month on the
file correctly indicates the month in which the sample patients received their outpatient
surgery or procedure.

XI. File Preparation and Data Submission December 2015
148 Centers for Medicare & Medicaid Services Outpatient and Ambulatory Surgery CAHPS Survey Protocols and Guidelines Manual
b. Select a sample of patients for whom data are entered on the XML file and compare the
data on the XML file for those patients with the data for that patient on the original (raw)
data source. For example, compare the variables entered in the Patient Administrative
Data Record section of the XML with the information that the HOPD or ASC provided
for the sample patient on the monthly patient information file. Similarly, compare the
entries in the Patient Survey Response Record section of the XML with the hardcopy
questionnaire or scanned image of the patient’s completed survey or, if the survey was
completed by phone, with the original CATI or telephone survey data file. Implementing
this quality control check on a sample of the data records will ensure that data are
correctly exported from the data source onto the XML file.
c. After the XML file is prepared, generate data distributions (frequencies of
responses/variables) on selected variables and inspect the output for data anomalies. A
visual inspection of data frequencies is a quick way to identify data problems. For
example, if the race variable for all patients entered on the XML file is American Indian,
this could be an indication that the race variable is incorrect. Similarly, response option 2
is coded for the overall rating of care variable for all patients on the file, this is likely an
indication that there is a problem with the file.
d. Check that a valid response code has been entered for all variables in the XML file. Note
if data are missing for a variable, either the missing code (“M”) or the code for not
applicable (“X”) must be entered for the variable.
e. Confirm that there have not been any assigned duplicate SID numbers assigned in the
XML files across months in the data submission period or across prior data submission
periods. An SID number can only be assigned to one patient and cannot be reused within
quarters, across quarters, or across years.
f. Verify that all final disposition codes are correct. Vendors must make sure that no data
are submitted for non-interview cases that are coded as deceased, ineligible, refusals, etc.
The reverse check – confirming that there is response data present for all patients whose
final disposition code is complete – should also be performed.
g. Vendors should change the disposition code for a completed survey that does not pass the
OAS CAHPS completeness criteria to 310 (breakoff). Also, make sure that code 340 is
being appropriately assigned to cases only when the vendor could not obtain a “working”
telephone number for the sample patient.
h. Conduct quality checks of mail survey coders’ work by having a different person recheck
a sample of each coder’s cases to make sure that they are following and applying correct
coding guidelines.
i. Check the file to make sure that all patient data the HOPD or ASC provided for a patient
on the monthly patient information file exported correctly to the XML file.
December 2015 XI. File Preparation and Data Submission
Centers for Medicare & Medicaid Services 149 Outpatient and Ambulatory Surgery CAHPS Survey Protocols and Guidelines Manual
j. Check the XML file name to make sure that it conforms to OAS CAHPS file naming
conventions.
k. Confirm that an XML file has been accepted for each sample month for each HOPD or
ASC.
Survey vendors should check the XML data files for internal logic and consistency prior to
submitting them to the OAS CAHPS Data Center. Some examples of items to check are
provided below:
a. The number of eligible patients included in the variable on the header record should
always be equal to or smaller than the number of patients the facility served during the
sample month. It should never be more than the number of patients served.
b. The number of patients eligible must be equal to or larger than the number of patients
sampled.
c. The number of patients sampled must be equal to or less than the number of patients
served.
d. The total number of patients for which the vendor has included administrative
information in the patient administrative section of the XML file must equal the number
of patients sampled.
Survey vendors are reminded that if none of the patients for whom information is provided on
the monthly patient information file is eligible for OAS CAHPS, the vendor must still prepare
and submit an XML file for that sample month (see Appendix M). The vendor must indicate on
the file that there were zero eligible cases in the number eligible variable, and enter all other
information required in the Header Record Section of the XML file. Note that OAS CAHPS
vendors are not required to submit a Discrepancy Notification Report for situations where there
are zero eligible cases; however, they are required to submit a Discrepancy Notification Report if
the HOPD or ASC did not submit a file at all (see Potential Situations When Vendors Will Not
Submit Data, above.)

Centers for Medicare & Medicaid Services 150 Outpatient and Ambulatory Surgery CAHPS Survey Protocols and Guidelines Manual
XII. WEB PORTAL REPORTS
Overview
The Outpatient and Ambulatory Surgery CAHPS (OAS CAHPS) Survey Data Center will
generate and provide via the OAS CAHPS web portal a number of reports to indicate the status
of data submissions and the quality of the data submitted. These reports are described in the
following sections.
Reports for Survey Vendors
Survey vendors will be able to access a number of reports via the secured section of the web
portal. The most important of these is tied to the data submission and file review process—the
Data Submission Summary Report. Another important report is the Survey Vendor Authorization
Report, which allows the survey vendor to view all ambulatory surgery centers (ASCs) and
hospital outpatient departments (HOPDs) that have authorized the vendor to collect and submit
data on their behalf. Each of these reports is discussed separately below.
The Data Submission Summary Report
This report is generated at two points in time. First, it is immediately available to survey vendors
after they upload data via the Data Submission Tool. Once the vendor submits data, the system
will check for the correct file layout, missing data, duplicate patient ID numbers, invalid
responses, etc. After successful file upload, the Data Center conducts a more thorough edit of
the data, which is done within an hour of the file submission. This second validation check is
also referred to as the “secondary validation.” The Data Submission Summary Report is updated
after the secondary validation checks have been made.
The first check (during upload) of the submitted data file is to make sure that the XML template
has been used and is properly formatted. If the survey vendor has an incorrectly formatted
template, the data upload process will stop immediately and display an error message to the
vendor that describes the problem detected. After the system verifies that a properly formatted
template has been used, it will begin a series of data checks. It will look for any fields in the
Header Record with missing data. If any data are missing, the file will be rejected, and the data
submission report will let the vendor know what data fields are missing. The system will also
check for any duplicate sample identification (SID) numbers to make sure a vendor has not used
an SID more than once for a given HOPD or ASC in a given quarter. If a vendor has used a
duplicate SID, the file will be rejected and the data submission report will let the vendor know
where the error is so it can be corrected. Finally, the report will check that the vendor is
authorized to upload data for the particular ASC or HOPD.

December 2015 XII. Web Portal Reports
Centers for Medicare & Medicaid Services 151 Outpatient and Ambulatory Surgery CAHPS Survey Protocols and Guidelines Manual
If the data file successfully passes the initial checks, the system will display a message saying
that the upload was successful. This screen will also provide the vendor with a count of records
received for each facility. The message will also indicate that the file will be sent through a
more formal data processing step within an hour, and that the data submission report will be
updated to show the results of this data processing step.
Files that have successfully passed the upload validation process are then subjected to a
secondary validation process. The system will check for missing data fields required for patient
eligibility determination. Each patient response record included on the file will be checked to
ensure that all entries are within the acceptable range. In addition, a completeness algorithm will
be run to verify that all patient response records included on the file meet survey completeness
criteria (although this step will be used to ensure that the appropriate cases are included as
“complete” and will not be a reason for rejecting a file).
The results of the secondary validation are appended to the Data Submission Summary Report
for each file that was uploaded. This report will provide sufficient detail, by CMS Certification
Number (CCN), of data file errors that caused data files to be rejected so that the vendor can fix
those errors and resubmit the file(s). Following the edit checks, the system will generate and
send an e-mail to the vendor indicating that the data processing step has been completed, and the
vendor can view the results on the Data Submission Summary Report. The e-mail will be
generated immediately after the secondary validation process has been completed. Survey
vendors can access this report at any time from the website by going to the “Data Submission”
menu and selecting the “Data Submission Reports” link. Survey vendors can select to view a
history of all reports, or history by upload date.
Files that successfully pass both stages of validation will be accepted and processed for public
reporting. If any problems are detected in the data file, this information will be displayed on the
Data Submission Summary Report, and the vendor will be expected to correct the errors and
resubmit the file.
As explained in Chapter XI, each XML file contains a single CCN for a single month. However,
vendors can upload a zip file containing XML files for several CCNs and several months. Files
will be accepted or rejected based on CCN. The vendor will only need to resubmit the XML file
with incorrect records.
Because of the two-part nature of the Data Center’s data processing steps, vendors are strongly
advised to submit files far enough in advance of the quarterly submission deadline to allow for
both the initial upload file check and the secondary validation checks, if they have to resubmit a
file. The OAS CAHPS Data Center will not accept files after 8:00 PM EST on the data
submission deadline date for each quarter.

XII. Web Portal Reports December 2015
152 Centers for Medicare & Medicaid Services Outpatient and Ambulatory Surgery CAHPS Survey Protocols and Guidelines Manual
Below is an example Data Submission Summary Report.
The Data Submission History Summary Reports
OAS CAHPS Survey vendors can view a history of their data submission activities via two
reports under the Data Submission Report menu option: Data Submission History and Data
Submission History by Upload Date. The Data Submission History report allows vendors to see
a summary or detailed list of all data submission activity. The Data Submission History by
Upload Date allows vendors to search for a data submission report by the actual upload date.
Below is an example of what a vendor would see upon selecting a particular file upload date.
Survey Vendor Authorization Report
The Survey Vendor Authorization Report allows survey vendors to view a list of ASCs and
HOPDs that have authorized the vendor to collect and submit data on their behalf. A survey
vendor under contract with an HOPD or ASC that has not yet been formally authorized by the
facility to submit data on the facility’s behalf should contact the facility and ask it to do so. Any
files a vendor submits for an HOPD or ASC that has not formally authorized the vendor to
submit data on its behalf will be rejected during data submission. It is the vendor’s responsibility
to ensure that any HOPD or ASC with which it is contracted to conduct the OAS CAHPS Survey

December 2015 XII. Web Portal Reports
Centers for Medicare & Medicaid Services 153 Outpatient and Ambulatory Surgery CAHPS Survey Protocols and Guidelines Manual
completes the authorization process. The OAS CAHPS Data Center will reject data files if the
form is out of date. Below is an example Survey Vendor Authorization Report.
If a facility closes or is no longer active while its survey vendor is still contracted to conduct and
provide survey data on its behalf, any vendor authorizations will remain in effect for the entire
authorization period. The authorized vendor must submit the data that were collected for the
closed HOPD or ASC to the OAS CAHPS Data Center.
Reports for Ambulatory Surgery Centers and Hospital Outpatient Departments
HOPDs and ASCs will be able to access two reports via the secured section of the OAS CAHPS
Survey website. The first report, the Data Submission Summary Report, is intended to provide a
means for the facility to monitor its vendor’s data submission activities and should be reviewed
on a monthly or quarterly basis, depending on the agreement that the facility has worked out with
the vendor in terms of frequency of data submission. The second report available to HOPDs and
ASCs is the OAS CAHPS Survey Results for Public Reporting―this report is a preview of the
OAS CAHPS Survey results that are compiled for each facility on a quarterly basis prior to being
publicly reported. These reports are discussed below.
Data Submission Summary Report
The Data Submission Summary Report is available to HOPDs and ASCs from the “For facilities”
menu on the OAS CAHPS Survey website. HOPDs and ASCs that have contracted with a
survey vendor will be able to log into the website and view, print, and download a report that
includes information on the number of submissions and the submission status of their contracted
vendor’s monthly or quarterly file submissions. HOPDs and ASCs are strongly advised to
review these reports on a regular basis.
The Data Submission Summary Report displays all of the dates on which the Data Center
accepted the data files the vendor submitted for the HOPD or ASC. Only files that passed both
the initial edit checks implemented during file upload and those that passed the secondary set of
edit checks will be listed on this report. The purpose of this report is to allow an HOPD or ASC
to monitor whether its vendor is successfully submitting data files by the required quarterly data
submission deadlines. An HOPD or ASC can use this report for reference when it follows up
with its vendor if expected data submissions do not appear. The Data Submission Summary
Report also includes a hyperlink embedded in the date of each submission that takes the user to

XII. Web Portal Reports December 2015
154 Centers for Medicare & Medicaid Services Outpatient and Ambulatory Surgery CAHPS Survey Protocols and Guidelines Manual
the data validation checks that were performed on the uploaded files for that date. This report
will give users the ability to view a list of successful data file transmissions.
To protect the confidentiality of each HOPD or ASC and the vendor it has selected, only the
facility and its authorized vendor will be able to view the submission history relating to that
facility’s data.
OAS CAHPS Survey Results for Public Reporting
The OAS CAHPS Survey Preview Reports provide HOPDs and ASCs with a preview of their
own survey results that will be publicly reported on the CMS website. The preview report is
made available approximately 2 weeks before the OAS CAHPS Survey results are publicly
reported. HOPDs and ASCs are able to access their Preview Report(s) via the secure side of the
OAS CAHPS portal. To access the reports, HOPDs and ASCs must login to the OAS CAHPS
web portal and then select the “Preview Reports” link under the “For facilities” menu. HOPDs
and ASCs participating in the OAS CAHPS Survey will have access to their own reports. The
Preview Report will not be available to the OAS CAHPS Survey vendor or to anyone other than
the HOPD or ASC.

December 2015 XII. Web Portal Reports
Centers for Medicare & Medicaid Services 155 Outpatient and Ambulatory Surgery CAHPS Survey Protocols and Guidelines Manual
This page intentionally left blank.

Centers for Medicare & Medicaid Services 156 Outpatient and Ambulatory Surgery CAHPS Survey Protocols and Guidelines Manual
XIII. OVERSIGHT ACTIVITIES
Overview
This chapter describes oversight activities that will be conducted by the Outpatient and
Ambulatory Surgery CAHPS (OAS CAHPS) Survey Coordination Team to ensure that the
survey is being administered according to required OAS CAHPS Survey protocols.
Requirements for vendor Quality Assurance Plans (QAPs), data review activities to be conducted
by the Coordination Team, communication between the Coordination Team and the vendors, and
site visit procedures are described in the following sections.
Quality Assurance Plan
All vendors seeking approval to conduct the OAS CAHPS Survey must submit a QAP, a
document that describes how the vendor will implement, comply with, and provide oversight of
all sampling, survey, and data processing activities associated with the OAS CAHPS Survey.
The first QAP must be submitted within 6 weeks of the data submission deadline date after the
vendor’s first quarterly data submission. It must be updated and submitted annually thereafter
and at any time that changes occur in staff or vendor capabilities or systems.
A QAP Outline is included in Appendix N to assist vendors in the development of their own
QAP. The vendor’s QAP should include the following sections:
• Organization Background and Staff Experience
• Identifying and Recruiting hospital outpatient departments (HOPDs) and ambulatory surgery
centers (ASCs)
• Work Plan
• Sampling Plan
• Survey Implementation Plan
• Data Security, Confidentiality, Privacy Plan
• Discrepancy Report and Corrective Action Plan
• Questionnaire Attachments

December 2015 XIII. Oversight Activities
Centers for Medicare & Medicaid Services 157 Outpatient and Ambulatory Surgery CAHPS Survey Protocols and Guidelines Manual
Within each section, the vendor must specify all key staff responsible for implementing or
overseeing the activity or activities, procedures, and methods being used, and quality assurance
activities that will be implemented. Changes to key staff must be reported to the OAS CAHPS
Survey Coordination Team. There should be sufficient detail provided for all of these
components so that the Centers for Medicare & Medicaid Services (CMS) can evaluate whether
the vendor is complying with all approved protocols. If CMS and the Coordination Team do not
feel that the vendor’s QAP has sufficient detail to make this determination, the Coordination
Team will request that the vendor make additions or edits to its QAP and resubmit it. Vendors
will also be required to submit either a copy of the mail questionnaire (for mail and mixed-mode
surveys) or the screen shots from their electronic telephone interview (for telephone surveys) as
part of their QAP. Note that the submission of a completed QAP is one of the components of
the vendor approval process.
When preparing the QAP, vendors should review and refer to the QAP Outline provided on the
OAS CAHPS website to ensure that they provide all information requested, including detailed
information about systems, protocols, and processes, so that the OAS CAHPS Survey
Coordination Team can assess how the survey is being implemented. The Coordination Team
will request that the vendor provide more information if the information provided is not
adequate. Vendors should also organize the information in their QAPs to conform to the sections
included in the QAP Outline, and make sure that the QAP is paginated for ease of reference and
review by CMS and the Coordination Team.
Data Review
The OAS CAHPS Survey Coordination Team will conduct ongoing reviews of the data
submitted by each survey vendor. As discussed in Chapter XI of this manual, data files are
reviewed immediately upon submission for proper formatting, completeness, accuracy of record
count, and out-of-range and missing values. In addition, the Coordination Team will run a series
of edits on the data to check for such issues as outlier response rate patterns or unusual data
elements.
The Coordination Team will attempt to resolve data issues with the vendor through the use of
conference calls or e-mail exchanges. If the Coordination Team believes that there are any
significant issues with a vendor’s data, or if repeated discussions and contact with a vendor fail
to result in cleaner data submissions, a more thorough review of the vendor’s data processing and
survey implementation activities may be initiated. At that time, the Coordination Team may
request copies of documentation associated with whatever the data issue is—for example, if out-
of-range values are found repeatedly, the Coordination Team may request copies of documents
showing the training program used to train Data Entry keying staff, training records, and
documentation that recommended quality assurance practices associated with keying data were
followed. Vendors are expected to comply with all such requests for documentation.

XIII. Oversight Activities December 2015
158 Centers for Medicare & Medicaid Services Outpatient and Ambulatory Surgery CAHPS Survey Protocols and Guidelines Manual
Communication Between Survey Vendors and the Coordination Team
The OAS CAHPS Survey Coordination Team welcomes communication from vendors related to
any part of the OAS CAHPS Survey implementation process. Vendors may communicate with
the Coordination Team via telephone or e-mail. The Coordination Team is also available to
participate in teleconference calls as needed to ensure vendors’ successful implementation of the
OAS CAHPS Survey. As noted in a preceding section of this manual, the vendor must provide
the facility name and CMS Certification Number (CCN) in all communications with the OAS
CAHPS Survey Coordination Team and OAS CAHPS Survey Data Center.
The Coordination Team expects that in addition to communication with vendors about technical
assistance issues, it will also schedule conference calls with selected vendors to review vendor
procedures and ensure adherence to the OAS CAHPS Survey protocols and guidelines. The
Coordination Team will make periodic calls to vendors to assess the status of sampling, data
collection, and file processing issues in general. These calls will be scheduled in advance so that
appropriate members of the vendor’s project team can participate.
Requirement for Clients
Survey vendors receive approval to conduct the OAS CAHPS Survey after their designated OAS
CAHPS Survey Project Director/Survey Administrator 1) successfully completes an online
training certification after participating in both sessions of the Introduction Training, and 2)
attends and successful completes all mandatory Update Trainings.
This status of “approved to conduct OAS CAHPS Survey” will be withdrawn if the survey
vendor does not have any clients on OAS CAHPS for two years from the Introductory Training.
If they wish to re-instate this approval status, they will need to obtain clients or repeat the
Introductory Training.
Site Visits to Survey Vendors
The OAS CAHPS Survey Coordination Team will conduct site visits to all approved vendors.
The purpose of the site visits is to allow the Coordination Team to observe the entire OAS
CAHPS Survey implementation process, from the sampling stage through file preparation and
submission.
The Coordination Team expects at a minimum to accomplish the following on each site visit:
• To review the process the survey vendor followed to determine the eligibility of their clients,
and specifically how the vendor
◦ identified the hospital/CCN, worked with the hospital management to determine the
eligible HOPDs within the CCN or within other CCNs, and gained the participation of
the eligible HOPDs within CCNs; and

December 2015 XIII. Oversight Activities
Centers for Medicare & Medicaid Services 159 Outpatient and Ambulatory Surgery CAHPS Survey Protocols and Guidelines Manual
◦ identified the ASC, worked with the ASC management to understand the CCN number or
numbers of their facilities, including different sites, and gained the participation of the
eligible locations within each CCN.
• A “walk through” of the systems and processes used from the point of obtaining a sample
frame from an HOPD or ASC to preparation of a final data file, including but not limited to a
review of:
◦ software/programs used to select and store the sample; how patient contact information
(name and address) and sample identification (SID) number are printed on letters
accompanying questionnaire mailings or provided to a call center for telephone survey
data collection; questionnaire production, mailout, and receipt facilities/processes;
telephone survey operation facilities/processes, including listening to interviews;
◦ all data processing activities, including how final status codes are assigned; and
◦ file preparation and submission activities and file storage facilities.
• A review of documentation associated with any of the above steps, as applicable. The
documentation to be reviewed includes but is not limited to:
◦ signed confidentiality forms for all applicable staff, including subcontractors;
◦ training records, such as for data entry or telephone interviewing staff;
◦ monitoring logs, with dates and times telephone interviewers were monitored, and the
results of those monitoring sessions;
◦ telephone interview scripts, including introductory scripts and responses to frequently
asked questions; and
◦ verification records, for either data entry or scanning processes, showing the level of
quality control for keyed questionnaires.
• Interviews with the vendor’s key OAS CAHPS Survey project staff, including the project
manager, sampling manager, and data manager.
The Coordination Team may make either scheduled or unscheduled visits to the vendor’s site.
Scheduled visits will be planned far enough in advance to ensure that all appropriate vendor staff
are able to participate in the site visit review process. For unscheduled visits, the Coordination
Team will give the vendor a 3-day window during which the team may conduct the onsite
review.
XIII. Oversight Activities December 2015
160 Centers for Medicare & Medicaid Services Outpatient and Ambulatory Surgery CAHPS Survey Protocols and Guidelines Manual
Generally, the site visit team will consist of two to three individuals, although the size of the
team may vary and may include representatives from CMS. All discussions, observations, and
materials reviewed during the site visit will remain confidential. Thus, although the
Coordination Team appreciates that certain systems or processes may be proprietary to a vendor,
full cooperation with the site visit team is expected so that the team may adequately assess
vendor compliance with all OAS CAHPS Survey protocols and guidelines.
After each site visit, the Coordination Team will prepare and submit to CMS a Site Visit Report,
which will summarize the findings from each site visit, including any systems and data issues.
The Site Visit Report will also describe corrective actions that the vendor will be required to take
to correct any deficiencies or problems noted. The Coordination Team will provide the vendor
with the Site Visit Report after it has been reviewed with CMS project staff. The Coordination
Team may request clarification, additional documentation, or changes to any aspect of the
implementation process, if needed. The vendor will then be given a specified period of time in
which to provide the additional information or submit documentation showing that it has
implemented the requested process or system change. The Coordination Team will follow up
with the vendor by teleconference or with additional site visits as needed.
Corrective Action Plans
If a vendor fails to demonstrate adherence to the OAS CAHPS Survey protocols and guidelines,
as evidenced by ongoing problems with its submitted data or as observed in its implementation
process during a site visit, CMS may ask the Coordination Team to either increase oversight of
the vendor’s activities (or submitted data files) or, if necessary, put the vendor on a corrective
action plan.
If the vendor is put on a corrective action plan, the Coordination Team will work out a schedule
with CMS by which the vendor must comply with the tasks set forth in the corrective action plan.
These will include interim monitoring dates, where the Coordination Team and the vendor will
meet via teleconference to discuss the status of the plan and what changes the vendor has made
or is in the process of making. The nature of the requested changes that the vendor is asked to
implement will dictate the kind of “deliverables” the vendor will be expected to provide and the
dates by which the deliverable must be provided.
Survey vendors that fail to comply with the oversight activities described above or whose
implementation of the OAS CAHPS Survey is found to be unsatisfactory after the opportunity is
given to correct deficiencies may be subject to having their “approved” status rescinded.
Further, any HOPD or ASC survey responses collected by the vendor may be withheld from
public reporting. The affected facilities will be notified by the OAS CAHPS Survey
Coordination Team of their vendor’s failure to comply with oversight activities or unsatisfactory
implementation so that the facilities will have the opportunity to contract with another approved
vendor.

December 2015 XIII. Oversight Activities
Centers for Medicare & Medicaid Services 161 Outpatient and Ambulatory Surgery CAHPS Survey Protocols and Guidelines Manual
This page intentionally left blank.

Centers for Medicare & Medicaid Services 162 Outpatient and Ambulatory Surgery CAHPS Survey Protocols and Guidelines Manual
XIV. PUBLIC REPORTING
Overview
This chapter describes the public reporting activities associated with the Outpatient and
Ambulatory Surgery CAHPS (OAS CAHPS) Survey. All publicly reported data are available on
the CMS website. Results from the OAS CAHPS Survey are published quarterly and include
each hospital outpatient department’s (HOPD’s) and ambulatory surgery center’s (ASC’s) most
recent four quarters of data.
The chapter begins with a list of the measures that are reported and explains how the results are
adjusted and reported. The chapter concludes with a discussion of Outpatient and Ambulatory
Surgery Preview Reports and a table showing the quarters included in each public reporting
period.
Measures That Are Reported
OAS CAHPS Survey results are reported for three composites and two global items:
Composite Measures
• About Facilities and Staff (Q3, Q4, Q5, Q6, Q7, and Q8)
• Communications About Your Procedure (Q1, Q2, Q9, Q10/Q11, and Q12)
• Preparations for Discharge and Recovery (Q13, Q14, Q15/Q16, Q17/Q18, Q19/Q20, and
Q21/Q22)
Global Items
• Overall rating of facility (Q23)
• Patient willingness to recommend HOPD or ASC to family or friends (Q24)
Each of the three composite measures consists of five or more questions from the survey that are
about related topics. The results from the questions that comprise a composite are reported as
one score. Composite scores are created by first determining the proportion of answers to each
response option for all questions in the composite. The final composite score averages the
proportion of those responding to each answer choice in all questions in the composite. Only
questions that are answered by survey respondents are included in the calculation of composite
scores.

December 2015 XIV. Public Reporting
Centers for Medicare & Medicaid Services 163 Outpatient and Ambulatory Surgery CAHPS Survey Protocols and Guidelines Manual
Adjustment and Reporting of Results
In 2015, the OAS CAHPS Survey Coordination Team conducted a mode experiment to test the
effects of using three data collection modes: mail only, telephone only, and mixed mode (mail
with telephone follow-up of nonrespondents).
Because some patients’ assessment of the care they received from HOPDs and ASCs may be
influenced by patient characteristics that are beyond the facilities’ control, CMS used the data
from the mode experiment to determine whether and to what extent characteristics of patients
participating in the OAS CAHPS Survey statistically affect survey results. Statistical models
were developed to adjust or control for these patient characteristics. These statistical adjustments
are applied before survey results are publicly reported. Also, some patients may not respond to
the survey, and this may impact the accuracy and comparability of results. Therefore, the data
from the mode experiment were analyzed to detect potential nonresponse bias. The results of
these analyses determined applicable statistical adjustments that are made on each quarter of the
OAS CAHPS Survey data.
OAS CAHPS Survey results are published on the CMS website. The URL of the OAS CAHPS
public reporting will be announced in 2016. Results are reported for a rolling four quarters of
data that are updated quarterly by replacing the oldest quarter of data with data from the most
recent quarter. Table 14.1 shows a crosswalk of the composite measures and global ratings
mapped to the text that is displayed on the CMS website.
Table 14.1 Crosswalk of Composite Measures and Global Ratings
OAS CAHPS Composite Measurements/ Global Ratings
OAS CAHPS Questions Included in Composite/
Global Rating Text Displayed on CMS Website
Care of Patients Q3, Q4, Q5, Q6, Q7, and Q8 Did the HOPD or ASC staff give care in a professional way?
Communications About Your Procedure
Q1, Q2, Q9, Q10/Q11, and Q12
Did the HOPD or ASC staff communicate with patients about what to expect during and after the procedure?
Preparations for Discharge and Recovery
Q13, Q14, Q15/Q16, Q17/Q18, Q19/Q20, and Q21/Q22
If after leaving the facility the patient reported having pain, nausea or vomiting, bleeding, or possible signs of infection as a result of the procedure or the anesthesia, had the HOPD or ASC staff given the patient information about what to do?
Overall rating of care Q23 How do patients rate the overall care from the HOPD or ASC?
Patient willingness to recommend HOPD or ASC to family or friends
Q24 Would patients recommend the HOPD or ASC to friends and family?

XIV. Public Reporting December 2015
164 Centers for Medicare & Medicaid Services Outpatient and Ambulatory Surgery CAHPS Survey Protocols and Guidelines Manual
Facility Preview Reports
Prior to publishing the results on the CMS website, the OAS CAHPS Survey Coordination Team
makes available a preview report posted on the OAS CAHPS website so that each HOPD and
ASC can review the results that will be publicly reported. We anticipate that OAS CAHPS
Survey data will be publicly reported for the first time in January 2018, based on survey results
from data collected for the sample months July 2016 through June 2017 (see Table 14.2). Each
subsequent quarterly public reporting period includes survey results from data collected for the
prior 12 months, as the oldest quarter’s data are dropped and the newest quarter’s data are added.
Public Reporting Periods
Table 14.2 shows the quarters included in each public reporting period.
Table 14.2 Data Submission Deadlines linked to the (Anticipated) Public Reporting Period
Vendors Data Submission
Deadline to (1)
Includes Sample
Months in…. Public Reporting
Period (#) Public Reporting Period
Covers
Date posted on CMS.gov
(2) (3)
July 13, 2016 Qtr. 1, 2016 October 2016 (1) Qtr. 1, 2016 Not posted
Oct. 11, 2016 Qtr. 2, 2016 January 2017 (2) Qtr. 1, 2016–Qtr. 2, 2016 Not posted
Jan. 11, 2017 Qtr. 3, 2016 April 2016 (3) Qtr. 1, 2016–Qtr. 3, 2016 Not posted
April 12, 2017 Qtr. 4, 2016 July 2017 (4) Qtr. 1, 2016–Qtr. 4, 2016 Not posted
July 12, 2017 Qtr. 1, 2017 October 2017 (5) Qtr. 2, 2016–Qtr. 1, 2017 Not posted
Oct. 11, 2017 Qtr. 2, 2017 January 2018 (6) Qtr. 3, 2016–Qtr. 2, 2017 Jan. 2018
Jan. 10, 2018 Qtr. 3, 2017 April 2018 (7) Qtr. 4, 2016–Qtr. 3, 2017 April 2018
April 11, 2018 Qtr. 4, 2017 July 2018 (8) Qtr. 1, 2017–Qtr. 4, 2017 July 2018
July 11, 2018 Qtr. 1, 2018 October 2018 (11) Qtr. 2, 2017–Qtr. 1, 2018 Oct. 2018
Oct. 10, 2018 Qtr. 2, 2018 January 2019 (12) Qtr. 3, 2017–Qtr. 2, 2018 Jan. 2019
Jan. 9, 2019 Qtr. 3, 2018 April 2019 (13) Qtr. 4, 2017–Qtr. 3, 2018 April 2019
April 10, 2019 Qtr. 4, 2018 July 2019 (14) Qtr. 1, 2018–Qtr. 4, 2018 July 2019
NOTES: (1) Data submissions will be second Wednesday of month. (2) Exact location within CMS.gov of public
reporting of OAS CAHPS to be announced at a future date. (3) Data are publicly released for a facility when that
facility has four consecutive quarters of data.

December 2015 XIV. Public Reporting
Centers for Medicare & Medicaid Services 165 Outpatient and Ambulatory Surgery CAHPS Survey Protocols and Guidelines Manual
This page intentionally left blank.

Centers for Medicare & Medicaid Services 166 Outpatient and Ambulatory Surgery CAHPS Survey Protocols and Guidelines Manual
XV. EXCEPTIONS REQUEST PROCESS AND DISCREPANCY
NOTIFICATION REPORT
Overview
This chapter describes the process to be used to request an exception to the Outpatient and
Ambulatory Surgery CAHPS (OAS CAHPS) Survey Protocols, including guidelines for
submitting an Exceptions Request Form. This chapter also covers the process for alerting the
OAS CAHPS Survey Coordination Team of an unplanned discrepancy in the collected or
submitted survey data. Vendors are expected to submit a Discrepancy Notification Report
whenever there has been an inadvertent or temporary deviation from the standard OAS CAHPS
Survey Protocols. The vendor is expected to notify the OAS CAHPS Survey Coordination Team
within 24 hours after the discovery of the discrepancy.
Exceptions Request Process
The Exceptions Request Form (see Appendix O) is designed to allow the survey vendor to
request a planned deviation from the standard OAS CAHPS Survey protocols. Vendors are
asked to submit an Exceptions Request Form for any exceptions to the OAS CAHPS Survey
protocol. The Coordination Team will make a determination after reviewing each request
whether to approve the exception. The OAS CAHPS Survey Coordination Team has identified
three allowable exceptions on the OAS CAHPS Survey at this time: the use of disproportionate
stratified random sampling (see Chapter IV), more frequent than monthly sampling (see
Chapter IV), and survey not yet in effect (Chapter XI). Vendors must complete and submit an
Exceptions Request Form to obtain approval to implement these exceptions.
The Exceptions Request form is designed to allow the survey vendor to request the same
exception for multiple hospital outpatient departments (HOPDs) or ambulatory surgery centers
(ASCs) for which it is responsible for collecting data. The Exceptions Request Form can be
accessed and submitted online (https://oascahps.org/).
Review Process
The Coordination Team will review the vendor’s exceptions request, evaluating the
methodological strengths and weaknesses of the proposed approach. The Coordination Team
will let the survey vendor know whether the exceptions request has been approved or denied. If
denied, the vendor will have 5 business days to appeal the decision. To submit an appeal, the
vendor needs to check “Appeal of Exception Denial” in Box 1b on the Exceptions Request Form
and update the form to provide further information about the exception being requested. The

December 2015 XV. Exceptions Request Process and Discrepancy Notification Report
Centers for Medicare & Medicaid Services 167 Outpatient and Ambulatory Surgery CAHPS Survey Protocols and Guidelines Manual
Coordination Team will review the appeal and return a final decision to the survey vendor within
10 business days.
Discrepancy Notification Report
The Discrepancy Notification Report (DNR) (see Appendix P) is designed to allow the survey
vendor to notify the OAS CAHPS Survey Coordination Team of an unplanned deviation from
the OAS CAHPS Survey protocols that will require some form of corrective action on the part of
the survey vendor. Examples of instances when a Discrepancy Notification Report is required
include the following:
• the vendor or facility inadvertently omitted from the sample frame patients who were eligible
for the survey;
• the vendor is unable to initiate the survey by the 21st day after the sample month ended and
needs to initiate it from the 22nd through the 26th day after the sample month ended;
• a variable was incorrectly coded and submitted on the XML file;
• there has been a natural disaster or event that has interrupted data collection in such a way as
to adversely affect survey outcomes; and
• the HOPD or ASC was unable to provide the vendor with a file for the sample
month. The
reason the HOPD or ASC was unable to provide the monthly patient information file must be
specified in the Discrepancy Notification Report.
The DNR can be accessed and submitted online via the OAS CAHPS Survey website
(https://oascahps.org/).
The vendor is expected to notify the OAS CAHPS Survey Coordination Team within 24 hours
after the discovery of the discrepancy. The vendor must also notify all affected HOPDs and
ASCs that a DNR has been submitted to the Coordination Team on their behalf. The report must
clearly describe the discrepancy and the action proposed by the vendor to correct the
discrepancy, along with a proposed timeline to correct the discrepancy. At a minimum, the
following information must be included on the report form:
• the HOPD’s or ASC’s CMS Certification Number;
• sample month and year;
• number of affected patients;
• a description of the discrepancy and whether the deviation from OAS CAHPS Survey
protocol was caused by the vendor or facility;

XV. Exceptions Request Process and Discrepancy Notification Report December 2015
168 Centers for Medicare & Medicaid Services Outpatient and Ambulatory Surgery CAHPS Survey Protocols and Guidelines Manual
• remediation plan for the affected month and the timeline for the remediation activity; and
• corrective actions to be taken to avoid the situation in the future.
Vendors are required to submit a DNR if an HOPD or ASC client does not submit a monthly
patient information file for a sample month. However, survey vendors do not need to continue
submitting these reports for facilities that are not submitting monthly patient information files
once the facility has failed to submit a monthly patient information file for 3 consecutive
sample months. It is the responsibility of the OAS CAHPS Survey vendor to track the number
of months the HOPD or ASC has failed to submit a monthly patient information file and to
submit a DNR for the first 3 months that this occurs.
Vendors are reminded that no DNR is needed if a facility has notified the vendor via submission
of a zero eligible file or an e-mail that it has no eligible patients in a given sample month. If an
HOPD or ASC submits a file to its vendor with no eligible patients, the vendor must submit an
XML file for that facility for that sample month indicating there were no eligible patients.
Discrepancy Report Review Process
The Coordination Team will review the vendor’s DNR and evaluate the impact of the
discrepancy on the publicly reported data. Depending on the type of discrepancy, a footnote may
be added to the publicly reported data. The Coordination Team will let the survey vendor know
whether additional information is required to document or correct the discrepancy.

December 2015 XV. Exceptions Request Process and Discrepancy Notification Report
Centers for Medicare & Medicaid Services 169 Outpatient and Ambulatory Surgery CAHPS Survey Protocols and Guidelines Manual
This page intentionally left blank.


Centers for Medicare & Medicaid Services Outpatient and Ambulatory Surgery CAHPS Survey Protocols and Guidelines Manual
APPENDIX A:
VENDOR APPLICATION FORM

Appendix A: Vendor Application Form December 2015
Centers for Medicare & Medicaid Services Outpatient and Ambulatory Surgery CAHPS Survey Protocols and Guidelines Manual
This page intentionally left blank.

Centers for Medicare & Medicaid Services A-1 Outpatient and Ambulatory Surgery CAHPS Survey Protocols and Guidelines Manual

Appendix A: Vendor Application Form December 2015
A-2 Centers for Medicare & Medicaid Services Outpatient and Ambulatory Surgery CAHPS Survey Protocols and Guidelines Manual

December 2015 Appendix A: Vendor Application Form
Centers for Medicare & Medicaid Services A-3 Outpatient and Ambulatory Surgery CAHPS Survey Protocols and Guidelines Manual
Appendix A: Vendor Application Form December 2015
A-4 Centers for Medicare & Medicaid Services Outpatient and Ambulatory Surgery CAHPS Survey Protocols and Guidelines Manual

December 2015 Appendix A: Vendor Application Form
Centers for Medicare & Medicaid Services A-5 Outpatient and Ambulatory Surgery CAHPS Survey Protocols and Guidelines Manual

Appendix A: Vendor Application Form December 2015
A-6 Centers for Medicare & Medicaid Services Outpatient and Ambulatory Surgery CAHPS Survey Protocols and Guidelines Manual

December 2015 Appendix A: Vendor Application Form
Centers for Medicare & Medicaid Services A-7 Outpatient and Ambulatory Surgery CAHPS Survey Protocols and Guidelines Manual

Appendix A: Vendor Application Form December 2015
A-8 Centers for Medicare & Medicaid Services Outpatient and Ambulatory Surgery CAHPS Survey Protocols and Guidelines Manual
December 2015 Appendix A: Vendor Application Form
Centers for Medicare & Medicaid Services A-9 Outpatient and Ambulatory Surgery CAHPS Survey Protocols and Guidelines Manual

Appendix A: Vendor Application Form December 2015
A-10 Centers for Medicare & Medicaid Services Outpatient and Ambulatory Surgery CAHPS Survey Protocols and Guidelines Manual

December 2015 Appendix A: Vendor Application Form
Centers for Medicare & Medicaid Services A-11 Outpatient and Ambulatory Surgery CAHPS Survey Protocols and Guidelines Manual

Appendix A: Vendor Application Form December 2015
A-12 Centers for Medicare & Medicaid Services Outpatient and Ambulatory Surgery CAHPS Survey Protocols and Guidelines Manual

December 2015 Appendix A: Vendor Application Form
Centers for Medicare & Medicaid Services A-13 Outpatient and Ambulatory Surgery CAHPS Survey Protocols and Guidelines Manual

Appendix A: Vendor Application Form December 2015
A-14 Centers for Medicare & Medicaid Services Outpatient and Ambulatory Surgery CAHPS Survey Protocols and Guidelines Manual
This page intentionally left blank.

Centers for Medicare & Medicaid Services Outpatient and Ambulatory Surgery CAHPS Survey Protocols and Guidelines Manual
APPENDIX B:
ENGLISH:
MAIL SURVEY COVER LETTERS, MAIL QUESTIONNAIRES,
INSTRUCTIONS FOR SCANNABLE MAIL QUESTIONNAIRE, TELEPHONE INTERVIEW SCRIPT

Appendix B: English: Mail Survey Cover Letters, Mail Questionnaires,
Instructions for Scannable Mail Questionnaire, Telephone Interview Script December 2015
Centers for Medicare & Medicaid Services Outpatient and Ambulatory Surgery CAHPS Survey Protocols and Guidelines Manual
This page intentionally left blank.

Centers for Medicare & Medicaid Services B-1 Outpatient and Ambulatory Surgery CAHPS Survey Protocols and Guidelines Manual
SAMPLE COVER LETTER FOR FIRST QUESTIONNAIRE MAILING
Outpatient and Ambulatory Surgery CAHPS Survey
To be Printed on Ambulatory Surgery Center or Hospital Outpatient Department or Vendor
Letterhead
«FirstName» «LastName»
«Address1» «Address2»
«City_Name», «State_Code» «Zip_Zip4»
Dear «FirstName» «LastName»:
[FACILITY] would like to learn more about the quality of health care that patients receive in our
facility. [VENDOR], an independent research company, is helping us conduct this survey. Our
records show that you had a surgery or procedure at [FACILITY]. The results of this survey will
be used to help us understand more about patient experiences in our facility.
The enclosed survey asks for your experiences with the outpatient surgery or procedure you had
on [DATE OF SURGERY]. We hope that you will take a few minutes to complete and return the
questionnaire to [VENDOR] in the enclosed, postage-paid envelope.
When answering the questions, please consider your visit to [FACILITY] on [DATE OF
SURGERY]. Do not answer questions based on any other surgeries or procedures you might
have had at either this facility or another.
All information you provide will be confidential and is protected by the Privacy Act. Your
answers to the survey will be grouped with answers from all other survey participants; your
name and identifying information will not be linked to your answers when the data are analyzed.
The overall survey results for [FACILITY NAME] and other facilities will be publically reported
on the Internet at https://www.medicare.gov/. These results will help people make more
informed decisions when choosing an outpatient or ambulatory surgery facility. Your
participation is voluntary and will not affect any health care benefits you currently receive or will
receive in the future.
If you have any questions about the survey, please call NAME toll-free at 1-800-XXX-XXXX. If
you need help in reading the questions or marking responses, a friend or family member can
assist you. Thank you in advance for your participation. Si desea recibir la versión de la encuesta
en español, por favor llame al 1-800-XXX-XXXX.
Sincerely,
NAME
Title
Enclosures [PRINT UNIQUE SAMPLE ID NUMBER HERE]

Appendix B: English: Mail Survey Cover Letters, Mail Questionnaires,
Instructions for Scannable Mail Questionnaire, Telephone Interview Script December 2015
B-2 Centers for Medicare & Medicaid Services Outpatient and Ambulatory Surgery CAHPS Survey Protocols and Guidelines Manual
SAMPLE COVER LETTER FOR SECOND QUESTIONNAIRE MAILING TO MAIL
SURVEY NONRESPONDENTS
Outpatient and Ambulatory Surgery CAHPS Survey
To be Printed on Ambulatory Surgery Center or Hospital Outpatient Department or Vendor
Letterhead
«FirstName» «LastName»
«Address1» «Address2»
«City_Name», «State_Code» «Zip_Zip4»
Dear «FirstName» «LastName»:
Recently, we sent you a letter asking for your help on a survey to provide [FACILITY] with
information about the quality of health care provided to patients who receive an outpatient
surgery or procedure in our facility. As of today, we have not yet received your completed
questionnaire. If you have already completed and returned the questionnaire, please accept
our thanks. If you have not completed it, please take a few minutes to do so now. Then
return the questionnaire in the enclosed, postage-paid envelope.
When answering the questions, please consider your visit to [FACILITY] on [DATE OF
SURGERY]. Do not answer questions based on any other surgeries or procedures you might
have had at either our facility or another.
The results of this survey will be used to help us understand more about patient experiences in
our facility. All information you provide will be confidential and is protected by the Privacy Act.
Your participation is voluntary and will not affect any health care benefits you currently receive
or will receive in the future.
If you have any questions about the survey, please call NAME toll-free at 1-800-XXX-XXXX. If
you need help in reading the questions or marking responses, a friend or family member can
assist you. Thank you in advance for your participation. Si desea recibir la versión de la encuesta
en español, por favor llame al 1-800-XXX-XXXX.
Sincerely,
NAME
Title

Consumer Assessment of Healthcare Providers and Systems
Outpatient and Ambulatory Surgery Survey
(OAS CAHPS)
A PATIENT EXPERIENCE OF CARE SURVEY ABOUT OUTPATIENT AND AMBULATORY SURGERIES
AND PROCEDURES
2016
ACCORDING TO THE PAPERWORK REDUCTION ACT OF 1995, NO PERSONS ARE REQUIRED TO RESPOND TO A
COLLECTION OF INFORMATION UNLESS IT DISPLAYS A VALID OMB CONTROL NUMBER. THE VALID OMB CONTROL
NUMBER FOR THIS INFORMATION COLLECTION IS 0938-1240. THE TIME REQUIRED TO COMPLETE THIS
INFORMATION COLLECTION IS ESTIMATED TO AVERAGE 8 MINUTES PER RESPONSE, INCLUDING THE TIME TO
REVIEW INSTRUCTIONS, SEARCH EXISTING DATA RESOURCES, GATHER THE DATA NEEDED, AND COMPLETE AND
REVIEW THE INFORMATION COLLECTION. IF YOU HAVE COMMENTS CONCERNING THE ACCURACY OF THE TIME
ESTIMATE(S) OR SUGGESTIONS FOR IMPROVING THIS FORM, PLEASE WRITE TO: CMS, 7500 SECURITY
BOULEVARD, ATTN: PRA REPORTS CLEARANCE OFFICER, MAIL STOP C4-26-05, BALTIMORE, MARYLAND
21244-1850.

Appendix B: English: Mail Survey Cover Letters, Mail Questionnaires,
Instructions for Scannable Mail Questionnaire, Telephone Interview Script December 2015
B-4 Centers for Medicare & Medicaid Services Outpatient and Ambulatory Surgery CAHPS Survey Protocols and Guidelines Manual
SURVEY INSTRUCTIONS
Answer all the questions by checking the box to the left of your answer.
You are sometimes told to skip over some questions in this survey. When this happens you will see an arrow with a note that tells you what question to answer next, like this:
Yes
No If No, go to #1. This survey asks about your experience at the facility named in the cover letter. For this survey, we use the term “procedure” for diagnostic, surgical or other procedures. We refer to “facility” as the place where you had your procedure.
Please answer these questions only for the procedure(s) you had on the date included in the cover letter. Do not include any other procedures in your answers.
I. BEFORE YOUR PROCEDURE
The first few questions are about getting ready for your procedure. Include any information you received before and on the day of your procedure.
1. Before your procedure, did your doctor or anyone from the facility give you all the information you needed about your procedure?
1 Yes, definitely 2 Yes, somewhat 3 No
2. Before your procedure, did your doctor or anyone from the facility give you easy to understand instructions about getting ready for your procedure?
1 Yes, definitely 2 Yes, somewhat 3 No
II. ABOUT THE FACILITY AND STAFF
The next questions ask about the day of your procedure.
3. Did the check-in process run smoothly?
1 Yes, definitely 2 Yes, somewhat 3 No
4. Was the facility clean?
1 Yes, definitely 2 Yes, somewhat 3 No
5. Were the clerks and receptionists at the facility as helpful as you thought they should be?
1 Yes, definitely 2 Yes, somewhat 3 No
6. Did the clerks and receptionists at the facility treat you with courtesy and respect?
1 Yes, definitely 2 Yes, somewhat 3 No

Appendix B: English: Mail Survey Cover Letters, Mail Questionnaires,
December 2015 Instructions for Scannable Mail Questionnaire, Telephone Interview Script
Centers for Medicare & Medicaid Services B-5 Outpatient and Ambulatory Surgery CAHPS Survey Protocols and Guidelines Manual
7. Did the doctors and nurses treat you with courtesy and respect?
1 Yes, definitely 2 Yes, somewhat 3 No
8. Did the doctors and nurses make sure you were as comfortable as possible?
1 Yes, definitely 2 Yes, somewhat 3 No
III. COMMUNICATIONS ABOUT YOUR
PROCEDURE
As a reminder, please include any information you received before and on the day of the procedure.
9. Did the doctors and nurses explain your procedure in a way that was easy to understand?
1 Yes, definitely 2 Yes, somewhat 3 No
10. Anesthesia is something that would make you feel sleepy or go to sleep during your procedure. Were you given anesthesia?
1 Yes 2 No If No, go to #13
11. Did your doctor or anyone from the facility explain the process of giving anesthesia in a way that was easy to understand?
1 Yes, definitely 2 Yes, somewhat 3 No
12. Did your doctor or anyone from the facility explain the possible side effects of the anesthesia in a way that was easy to understand?
1 Yes, definitely 2 Yes, somewhat 3 No
13. Discharge instructions include things like symptoms you should watch for after your procedure, instructions about medicines, and home care. Before you left the facility, did you get written discharge instructions?
1 Yes 2 No
IV. YOUR RECOVERY
14. Did your doctor or anyone from the facility prepare you for what to expect during your recovery?
1 Yes, definitely 2 Yes, somewhat 3 No

Appendix B: English: Mail Survey Cover Letters, Mail Questionnaires,
Instructions for Scannable Mail Questionnaire, Telephone Interview Script December 2015
B-6 Centers for Medicare & Medicaid Services Outpatient and Ambulatory Surgery CAHPS Survey Protocols and Guidelines Manual
15. Some ways to control pain include prescription medicine, over-the-counter pain relievers or ice packs. Did your doctor or anyone from the facility give you information about what to do if you had pain as a result of your procedure?
1 Yes, definitely 2 Yes, somewhat 3 No
16. At any time after leaving the facility, did you have pain as a result of your procedure?
1 Yes 2 No
17. Before you left the facility, did your doctor or anyone from the facility give you information about what to do if you had nausea or vomiting?
1 Yes, definitely 2 Yes, somewhat 3 No
18. At any time after leaving the facility, did you have nausea or vomiting as a result of either your procedure or the anesthesia?
1 Yes 2 No
19. Before you left the facility, did your doctor or anyone from the facility give you information about what to do if you had bleeding as a result of your procedure?
1 Yes, definitely 2 Yes, somewhat 3 No
20. At any time after leaving the facility, did you have bleeding as a result of your procedure?
1 Yes 2 No
21. Possible signs of infection include fever, swelling, heat, drainage or redness. Before you left the facility, did your doctor or anyone from the facility give you information about what to do if you had possible signs of infection?
1 Yes, definitely 2 Yes, somewhat 3 No
22. At any time after leaving the facility, did you have any signs of infection?
1 Yes 2 No

Appendix B: English: Mail Survey Cover Letters, Mail Questionnaires,
December 2015 Instructions for Scannable Mail Questionnaire, Telephone Interview Script
Centers for Medicare & Medicaid Services B-7 Outpatient and Ambulatory Surgery CAHPS Survey Protocols and Guidelines Manual
V. YOUR OVERALL EXPERIENCE
23. Using any number from 0 to 10, where 0 is the worst facility possible and 10 is the best facility possible, what number would you use to rate this facility?
0 Worst facility possible
1
2
3
4
5
6
7
8
9
10 Best facility possible
24. Would you recommend this facility to your friends and family?
1 Definitely no 2 Probably no 3 Probably yes 4 Definitely yes
VI. ABOUT YOU
25. In general, how would you rate your overall health?
1 Excellent 2 Very good 3 Good 4 Fair 5 Poor
26. In general, how would you rate your overall mental or emotional health?
1 Excellent 2 Very good 3 Good 4 Fair 5 Poor
27. What is your age?
1 18 to 24 2 25 to 34 3 35 to 44 4 45 to 54 5 55 to 64 6 65 to 74 7 75 to 79 8 80 to 84 9 85 or older
28. Are you male or female?
1 Male 2 Female
29. What is the highest grade or level of school that you have completed?
1 8th grade or less 2 Some high school, but did not
graduate 3 High school graduate or GED 4 Some college or 2-year degree 5 4-year college graduate 6 More than 4-year college
degree

Appendix B: English: Mail Survey Cover Letters, Mail Questionnaires,
Instructions for Scannable Mail Questionnaire, Telephone Interview Script December 2015
B-8 Centers for Medicare & Medicaid Services Outpatient and Ambulatory Surgery CAHPS Survey Protocols and Guidelines Manual
30. Are you of Hispanic, Latino/a, or Spanish origin?
1 Yes, Hispanic, Latino/a, or Spanish
2 No, not Hispanic, Latino/a, or Spanish If No, go to #32
31. Which group best describes you?
1 Mexican, Mexican American, Chicano/a
2 Puerto Rican 3 Cuban 4 Another Hispanic, Latino/a, or
Spanish origin
32. What is your race? You may select one or more categories.
1 White 2 Black or African American 3 American Indian or Alaska
Native 4 Asian Indian 5 Chinese 6 Filipino 7 Japanese 8 Korean 9 Vietnamese 10 Other Asian 11 Native Hawaiian 12 Guamanian or Chamorro 13 Samoan 14 Other Pacific Islander
33. How well do you speak English?
1 Very well 2 Well 3 Not well 4 Not at all
34. Do you speak a language other than English at home?
1 Yes 2 No If No, go to #36
35. What is that language?
1 Spanish 2 Other Language
(PLEASE SPECIFY): ________________________ (Please print.)
36. Did someone help you complete this survey?
1 Yes 2 No If No, go to END.
37. How did that person help you? Check all that apply.
1 Read the questions to me 2 Wrote down the answers I
gave 3 Answered the questions for me 4 Translated the questions into
my language 5 Helped in some other way:
(EXPLAIN): ________________________ (Please print.)
6 No one helped me complete this survey
END

Appendix B: English: Mail Survey Cover Letters, Mail Questionnaires,
December 2015 Instructions for Scannable Mail Questionnaire, Telephone Interview Script
Centers for Medicare & Medicaid Services B-9 Outpatient and Ambulatory Surgery CAHPS Survey Protocols and Guidelines Manual

Appendix B: English: Mail Survey Cover Letters, Mail Questionnaires,
Instructions for Scannable Mail Questionnaire, Telephone Interview Script December 2015
B-10 Centers for Medicare & Medicaid Services Outpatient and Ambulatory Surgery CAHPS Survey Protocols and Guidelines Manual
(Alternative Instructions for Scannable Forms)
SURVEY INSTRUCTIONS
· Answer all the questions by completely filling in the circle to the left of your answer.
· You are sometimes told to skip over some questions in this survey. When this happens you
will see an arrow with a note that tells you what question to answer next, like this:
Yes
No If No, go to #1.
This survey asks about your experience at the facility named in the cover letter. For this survey,
we use the term “procedure” for diagnostic, surgical or other procedures. We refer to “facility”
as the place where you had your procedure.
Please answer these questions only for the procedure(s) you had on the date included in the
cover letter. Do not include any other procedures in your answers.

Appendix B: English: Mail Survey Cover Letters, Mail Questionnaires,
December 2015 Instructions for Scannable Mail Questionnaire, Telephone Interview Script
Centers for Medicare & Medicaid Services B-11 Outpatient and Ambulatory Surgery CAHPS Survey Protocols and Guidelines Manual
TELEPHONE INTERVIEW SCRIPT
FOR THE OUTPATIENT AND AMBULATORY SURGERY CAHPS SURVEY
INTRO1 Hello, may I please speak to [SAMPLED MEMBER’S NAME]?
1. YES Go to INTRO 2
2. NO, NOT AVAILABLE RIGHT NOW [SET CALLBACK]
3. NO [REFUSAL] Go to TERMINATE Screen,
4. MENTALLY/PHYSICALLY INCAPABLE
IF ASKED WHO IS CALLING:
This is [INTERVIEWER NAME] calling from [VENDOR] on behalf of
[FACILITY NAME]. I’d like to speak to [SAMPLE MEMBER’S NAME] about
a health care survey.
INTRO2 [Hello, this is [INTERVIEWER NAME] calling on behalf of [FACILITY
NAME] [FACILITY NAME] is participating in a survey about patients’
experiences with outpatient surgeries and procedures. The results will be used to
help [FACILITY NAME] understand patient experiences in their facilities.
Your participation in this survey is completely voluntary and will not affect any
health care or benefits you receive. All information you provide is confidential
and is protected by the Privacy Act. The interview will take about 8 minutes to
complete. This call may be monitored or recorded for quality improvement
purposes.
[ADDRESS ANY QUESTIONS/CONCERNS THEN CONTINUE.]
INTRO3 This survey asks about your experience at [FACILITY NAME]. For this survey,
we use the term “procedure” for diagnostic, surgical or other procedures. We refer
to “facility” as the place where you had your procedure. Please answer these
questions only for the procedure you had on [DATE]. Do not include any other
procedures in your answers.

Appendix B: English: Mail Survey Cover Letters, Mail Questionnaires,
Instructions for Scannable Mail Questionnaire, Telephone Interview Script December 2015
B-12 Centers for Medicare & Medicaid Services Outpatient and Ambulatory Surgery CAHPS Survey Protocols and Guidelines Manual
[ADDRESS ANY QUESTIONS/CONCERNS THEN SELECT RESPONSE OPTION.]
1 BEGIN INTERVIEW [GO TO Q1_INTRO]
2 NO, NOT RIGHT NOW [SET CALLBACK]
3 DID NOT RECEIVE SURGERY/PROCEDURE FROM THIS FACILITY
DURING [MONTH] [GO TO Q_INELIGIBLE SCREEN]
4 NO [REFUSAL] [GO TO Q_REF SCREEN]
Q1_INTRO The first few questions are about getting ready for your procedure. Include any
information you received before and on the day of your procedure.
Q1. Before your procedure, did your doctor or anyone from the facility give you all
the information you needed about your procedure? Would you say…
1 Yes, definitely
2 Yes, somewhat
3 No
M MISSING/DK
Q2. Before your procedure, did your doctor or anyone from the facility give you easy
to understand instructions about getting ready for your procedure? Would you
say…
1 Yes, definitely
2 Yes, somewhat
3 No
M MISSING/DK
Q3_INTRO The next questions ask about the day of your procedure.
Q3. Did the check-in process run smoothly? Would you say…
1 Yes, definitely
2 Yes, somewhat
3 No
M MISSING/DK

Appendix B: English: Mail Survey Cover Letters, Mail Questionnaires,
December 2015 Instructions for Scannable Mail Questionnaire, Telephone Interview Script
Centers for Medicare & Medicaid Services B-13 Outpatient and Ambulatory Surgery CAHPS Survey Protocols and Guidelines Manual
Q4. Was the facility clean? Would you say…
1 Yes, definitely
2 Yes, somewhat
3 No
M MISSING/DK
Q5. Were the clerks and receptionists at the facility as helpful as you thought they
should be? Would you say…
1 Yes, definitely
2 Yes, somewhat
3 No
M MISSING/DK
Q6. Did the clerks and receptionists at the facility treat you with courtesy and respect?
Would you say…
1 Yes, definitely
2 Yes, somewhat
3 No
M MISSING/DK
Q7. Did the doctors and nurses treat you with courtesy and respect? Would you say…
1 Yes, definitely
2 Yes, somewhat
3 No
M MISSING/DK
Q8. Did the doctors and nurses make sure you were as comfortable as possible?
Would you say…
1 Yes, definitely
2 Yes, somewhat
3 No
M MISSING/DK
Q9_INTRO As a reminder, please include any information you received before and on the day
of the procedure.

Appendix B: English: Mail Survey Cover Letters, Mail Questionnaires,
Instructions for Scannable Mail Questionnaire, Telephone Interview Script December 2015
B-14 Centers for Medicare & Medicaid Services Outpatient and Ambulatory Surgery CAHPS Survey Protocols and Guidelines Manual
Q9. Did the doctors and nurses explain your procedure in a way that was easy to
understand? Would you say…
1 Yes, definitely
2 Yes, somewhat
3 No
M MISSING/DK
Q10. Anesthesia is something that would make you feel sleepy or go to sleep during
your procedure. Were you given anesthesia?
1 YES
2 NO [GO TO Q#13]
M MISSING/DK
Q11. Did your doctor or anyone from the facility explain the process of giving
anesthesia in a way that was easy to understand? Would you say…
1 Yes, definitely
2 Yes, somewhat
3 No
M MISSING/DK
Q12. Did your doctor or anyone from the facility explain the possible side effects of the
anesthesia in a way that was easy to understand? Would you say…
1 Yes, definitely
2 Yes, somewhat
3 No
M MISSING/DK
Q13. Discharge instructions include things like symptoms you should watch for after
your procedure, instructions about medicines, and home care. Before you left the
facility, did you receive written discharge instructions?
1 YES
2 NO
M MISSING/DK

Appendix B: English: Mail Survey Cover Letters, Mail Questionnaires,
December 2015 Instructions for Scannable Mail Questionnaire, Telephone Interview Script
Centers for Medicare & Medicaid Services B-15 Outpatient and Ambulatory Surgery CAHPS Survey Protocols and Guidelines Manual
Q14. Did your doctor or anyone from the facility prepare you for what to expect during
your recovery? Would you say…
1 Yes, definitely
2 Yes, somewhat
3 No
M MISSING/DK
Q15. Some ways to control pain include prescription medicine, over-the-counter pain
relievers or ice packs. Did your doctor or anyone from the facility give you
information about what to do if you had pain as a result of your procedure?
Would you say…
1 Yes, definitely
2 Yes, somewhat
3 No
M MISSING/DK
Q16. At any time after leaving the facility, did you have pain as a result of your
procedure?
1 YES
2 NO
M MISSING/DK
Q17. Before you left the facility, did your doctor or anyone from the facility give you
information about what to do if you had nausea or vomiting? Would you say…
1 Yes, definitely
2 Yes, somewhat
3 No
M MISSING/DK
Q18. At any time after leaving the facility, did you have nausea or vomiting as a result
of either your procedure or the anesthesia?
1 YES
2 NO
M MISSING/DK

Appendix B: English: Mail Survey Cover Letters, Mail Questionnaires,
Instructions for Scannable Mail Questionnaire, Telephone Interview Script December 2015
B-16 Centers for Medicare & Medicaid Services Outpatient and Ambulatory Surgery CAHPS Survey Protocols and Guidelines Manual
Q19. Before you left the facility, did your doctor or anyone from the facility give you
information about what to do if you had bleeding as a result of your procedure?
Would you say…
1 Yes, definitely
2 Yes, somewhat
3 No
M MISSING/DK
Q20. At any time after leaving the facility, did you have bleeding as a result of your
procedure?
1 YES
2 NO
M MISSING/DK
Q21. Possible signs of infection include fever, swelling, heat, drainage or redness.
Before you left the facility, did your doctor or anyone from the facility give you
information about what to do if you had possible signs of infection? Would you
say…
1 Yes, definitely
2 Yes, somewhat
3 No
M MISSING/DK
Q22. At any time after leaving the facility, did you have any signs of infection?
1 YES
2 NO
M MISSING/DK
Q23_INTRO The next two questions ask about your overall experience.

Appendix B: English: Mail Survey Cover Letters, Mail Questionnaires,
December 2015 Instructions for Scannable Mail Questionnaire, Telephone Interview Script
Centers for Medicare & Medicaid Services B-17 Outpatient and Ambulatory Surgery CAHPS Survey Protocols and Guidelines Manual
Q23. Using any number from 0 to 10, where 0 is the worst facility possible and 10 is
the best facility possible, what number would you use to rate this facility?
0 WORST FACILITY POSSIBLE
1
2
3
4
5
6
7
8
9
10 BEST FACILITY POSSIBLE
M MISSING/DK
Q24. Would you recommend this facility to your friends and family? Would you say…
1 Definitely no
2 Probably no
3 Probably yes
4 Definitely yes
M MISSING/DK
Q25. In general, how would you rate your overall health? Would you say …
1 Excellent,
2 Very good,
3 Good,
4 Fair, or
5 Poor?
M MISSING/DK

Appendix B: English: Mail Survey Cover Letters, Mail Questionnaires,
Instructions for Scannable Mail Questionnaire, Telephone Interview Script December 2015
B-18 Centers for Medicare & Medicaid Services Outpatient and Ambulatory Surgery CAHPS Survey Protocols and Guidelines Manual
Q26. In general, how would you rate your overall mental or emotional health? Would
you say …
1 Excellent,
2 Very good,
3 Good,
4 Fair, or
5 Poor?
M MISSING/DK
Q27. What is your age?
1 18 TO 24
2 25 TO 34
3 35 TO 44
4 45 TO 54
5 55 TO 64
6 65 TO 74
7 75 TO 79
8 80 TO 84
9 85 OR OLDER
M MISSING/DK
Q28. Are you male or female?
1 MALE
2 FEMALE
M MISSING/DK
Q29. What is the highest grade or level of school that you have completed? Would you
say…
1 8th grade or less,
2 Some high school, but did not graduate,
3 High school graduate or GED,
4 Some college or 2-year degree,
5 4-year college graduate, or
6 More than 4-year college degree?
M MISSING/DK

Appendix B: English: Mail Survey Cover Letters, Mail Questionnaires,
December 2015 Instructions for Scannable Mail Questionnaire, Telephone Interview Script
Centers for Medicare & Medicaid Services B-19 Outpatient and Ambulatory Surgery CAHPS Survey Protocols and Guidelines Manual
Q30. Are you of Hispanic or Latino/Latina, or Spanish origin?
1 YES
2 NO [GO TO Q32]
M MISSING/DK
Q31. Which group best describes you?
1 Mexican, Mexican American, Chicano/a
2 Puerto Rican
3 Cuban, or
4 Another Hispanic, Latino/a, or Spanish origin
M MISSING/DK
Q32. What is your race? You may select one or more categories. Are you…
1 White
2 Black or African American
3 American Indian or Alaska Native
4 Asian, or
5 Native Hawaiian or Pacific Islander
6 NONE OF THE ABOVE
M MISSING/DK
PROGRAMMER INSTRUCTIONS: IF WHITE ONLY, BLACK/AFRICAN AMERICAN
ONLY, OR AMERICAN INDIAN/ALASKA NATIVE ONLY, OR ANY COMBINATION OF
THESE THREE OPTIONS, NONE OF THE ABOVE OR MISSING/DK, GO TO Q33.
IF ASIAN ONLY, GO TO Q32A. IF WHITE, BLACK/AFRICAN AMERICAN, AND/OR
AMERICAN INDIAN/ALASKA NATIVE AND ASIAN ARE CHOSEN, GO TO Q32A. IF
NATIVE HAWAIIAN/PACIFIC ISLANDER IS ALSO CHOSEN, SEE INSTRUCTION
AFTER Q32A.
IF NATIVE HAWAIIAN/PACIFIC ISLANDER ONLY, GO TO Q32B. IF WHITE,
BLACK/AFRICAN AMERICAN, AND/OR AMERICAN INDIAN/ALASKA NATIVE AND
NATIVE HAWAIIAN/PACIFIC ISLANDER ARE CHOSEN, GO TO Q32B.

Appendix B: English: Mail Survey Cover Letters, Mail Questionnaires,
Instructions for Scannable Mail Questionnaire, Telephone Interview Script December 2015
B-20 Centers for Medicare & Medicaid Services Outpatient and Ambulatory Surgery CAHPS Survey Protocols and Guidelines Manual
Q32a. Which groups best describe you? You may select one or more categories. Are
you…
1 Asian Indian
2 Chinese
3 Filipino
4 Japanese
5 Korean
6 Vietnamese, or
7 Other Asian
8 NONE OF THE ABOVE
M MISSING/DK
IF NATIVE HAWAIIAN/PACIFIC ISLANDER WAS ALSO CHOSEN IN Q32, GO TO Q32B.
ELSE, GO TO Q33.
Q32b. Which groups best describe you? You may select one or more categories. Are
you…
1 Native Hawaiian
2 Guamanian or Chamorro
3 Samoan, or
4 Other Pacific Islander
5 NONE OF THE ABOVE
M MISSING/DK
Q33. How well do you speak English? Would you say…
1 Very well
2 Well
3 Not well
4 Not at all
M MISSING/DK
Q34. Do you speak a language other than English at home?
1 Yes, I speak a language other than English
2 No, I speak English at home [GO TO Q_END]
M MISSING/DK

Appendix B: English: Mail Survey Cover Letters, Mail Questionnaires,
December 2015 Instructions for Scannable Mail Questionnaire, Telephone Interview Script
Centers for Medicare & Medicaid Services B-21 Outpatient and Ambulatory Surgery CAHPS Survey Protocols and Guidelines Manual
Q35. What is that language?
1 Spanish (GO TO Q_END)
2 Other Language (GO TO Q35a)
M MISSING/DK
Q35a. What is that language? (ENTER RESPONSE BELOW. ALLOW UP TO 50
CHARACTERS)
M MISSING/DK
Q_END These are all the questions I have for you. Thank you for your time. Have a good
(day/evening).
INELIGIBLE SCREEN:
Q_INELIG Thank you for your time. Have a good (day/evening).
REFUSAL SCREEN:
Q_REF Thank you for your time. Have a good (day/evening).


Centers for Medicare & Medicaid Services Outpatient and Ambulatory Surgery CAHPS Survey Protocols and Guidelines Manual
APPENDIX C:
SPANISH: MAIL SURVEY COVER LETTERS,
MAIL QUESTIONNAIRES,
INSTRUCTIONS FOR SCANNABLE MAIL QUESTIONNAIRE, TELEPHONE INTERVIEW SCRIPT
Appendix C: Spanish: Mail Survey Cover Letters, Mail Questionnaires,
Instructions for Scannable Mail Questionnaire, Telephone Interview Script December 2015
Centers for Medicare & Medicaid Services Outpatient and Ambulatory Surgery CAHPS Survey Protocols and Guidelines Manual
This page intentionally left blank.
Centers for Medicare & Medicaid Services C-1 Outpatient and Ambulatory Surgery CAHPS Survey Protocols and Guidelines Manual
SAMPLE COVER LETTER FOR FIRST QUESTIONNAIRE MAILING
Outpatient and Ambulatory Surgery CAHPS Survey
To be Printed on Ambulatory Surgery Center or Hospital Outpatient Department or Vendor
Letterhead
«FirstName» «LastName»
«Address1» «Address2»
«City_Name», «State_Code» «Zip_Zip4»
Estimado(a) «FirstName» «LastName»:
[FACILITY NAME] participará en una encuesta nacional para saber más sobre la calidad de la
atención médica que reciben los pacientes. [VENDOR], una organización independiente que
realiza estudios, está ayudando a realizar esta encuesta. Nuestros registros muestran que usted se
hizo un procedimiento o cirugía en [FACILITY NAME]. Los resultados se usarán para ayudar a
comprender las experiencias de los pacientes de nuestro centro.
La encuesta que adjuntamos hace preguntas sobre sus experiencias con el procedimiento o la
cirugía que recibió el [Date of Procedure]. Esperamos que tome unos cuantos minutos para
completar y devolver el cuestionario a [VENDOR], en el sobre adjunto con franqueo postal
pagado.
Al contestar las preguntas, tenga en cuenta su visita a [FACILITY NAME] el [Date of
Procedure]. No responda las preguntas acerca de otras cirugías o procedimientos que haya tenido
en este centro de cirugía o en otro lugar.
Toda la información que proporcione será confidencial y estará protegida por la Ley de
Privacidad. Sus respuestas a la encuesta se agruparán con las de otros participantes del estudio.
Su nombre y su información de identidad no se asociarán a sus respuestas cuando se analicen los
datos. Los resultados generales de la encuesta de [FACILITY NAME] y de otras instalaciones se
reportará públicamente en internet en https://www.medicare.gov/. Estos resultados ayudarán a
las personas a tomar decisiones más informadas cuando eligen un centro para cirugía externa o
ambulatoria. Su participación es voluntaria y no afectará a ningún beneficio de atención médica
que usted reciba ahora o en el futuro.
Si tiene alguna pregunta sobre la encuesta, puede llamar al personal de la encuesta a la línea
gratuita 1-800-XXX-XXXX. Si necesita ayuda para leer las preguntas o marcar respuestas, una
amistad o miembro de la familia puede ayudarle. Le agradecemos de antemano por su
participación.

Appendix C: Spanish: Mail Survey Cover Letters, Mail Questionnaires,
Instructions for Scannable Mail Questionnaire, Telephone Interview Script December 2015
C-2 Centers for Medicare & Medicaid Services Outpatient and Ambulatory Surgery CAHPS Survey Protocols and Guidelines Manual
Atentamente,
NAME
Title
Enclosures [PRINT UNIQUE SAMPLE ID NUMBER HERE]

Appendix C: Spanish: Mail Survey Cover Letters, Mail Questionnaires,
December 2015 Instructions for Scannable Mail Questionnaire, Telephone Interview Script
Centers for Medicare & Medicaid Services C-3 Outpatient and Ambulatory Surgery CAHPS Survey Protocols and Guidelines Manual
SAMPLE COVER LETTER FOR SECOND QUESTIONNAIRE MAILING TO MAIL
SURVEY NONRESPONDENTS
Outpatient and Ambulatory Surgery CAHPS Survey
To be Printed on Ambulatory Surgery Center or Hospital Outpatient Department or Vendor
Letterhead
«FirstName» «LastName»
«Address1» «Address2»
«City_Name», «State_Code» «Zip_Zip4»
Estimado(a) «FirstName» «LastName»:
Hace poco, le enviamos una carta pidiéndole su ayuda en una encuesta para dar información a
[FACILITY] sobre la calidad de la atención médica que reciben los pacientes de cirugía para
pacientes externos o ambulatorios. Al día de hoy, no hemos recibido el cuestionario con sus
respuestas. Si usted ya completó el cuestionario y lo regresó, se lo agradecemos. Si no lo ha
completado, por favor dedique unos minutos para hacerlo ahora. Luego envíe el
cuestionario en el sobre adjunto con franqueo postal pagado.
Al contestar las preguntas, por favor tenga en cuenta su visita a [FACILITY] el [DATE OF
SURGERY]. No responda las preguntas acerca de otras cirugías o procedimientos que haya
tenido en este centro de cirugía o en otro lugar.
Los resultados de la encuesta se usarán para ayudar a comprender las experiencias de los
pacientes del centro. Toda la información que proporcione será confidencial y estará protegida
por la Ley de Privacidad. Su participación es voluntaria y no afectará a ningún beneficio de
atención médica que usted reciba ahora o en el futuro.
Si tiene alguna pregunta sobre la encuesta, puede llamar al personal de la encuesta a la línea
gratuita 1-800-XXX-XXXX. Si necesita ayuda para leer las preguntas o marcar respuestas, una
amistad o miembro de la familia puede ayudarle. Le agradecemos de antemano por su
participación.
Atentamente,
NAME
Title

Encuesta CAHPS sobre la cirugía externa o ambulatoria
(OAS CAHPS®)
UNA ENCUESTA DE PACIENTES SOBRE LA EXPERIENCIA CON LA ATENCIÓN DE CIRUGÍAS Y
PROCEDIMIENTOS AMBULATORIOS
2016
DE ACUERDO A LA LEY DE REDUCCIÓN DE TRABAJO ADMINISTRATIVO DE 1995 (PAPERWORK REDUCTION ACT
OF 1995), NINGUNA PERSONA TIENE LA OBLIGACIÓN DE RESPONDER A UN CUESTIONARIO QUE SOLICITE
INFORMACIÓN, A MENOS QUE LLEVE UN NÚMERO DE CONTROL DE OMB (OFICINA DE ADMINISTRACIÓN Y
PRESUPUESTO) VÁLIDO. EL NÚMERO DE CONTROL OMB VÁLIDO PARA ESTE CUESTIONARIO ES 0938-1240. SE
ESTIMA QUE EL TIEMPO PROMEDIO NECESARIO PARA COMPLETAR ESTE CUESTIONARIO ES DE 8 MINUTOS POR
RESPUESTA, INCLUYENDO EL TIEMPO PARA REVISAR LAS INSTRUCCIONES, BUSCAR EN LAS FUENTES DE DATOS
EXISTENTES, RECOPILAR LOS DATOS NECESARIOS, COMPLETAR Y REVISAR LA INFORMACIÓN RECOPILADA. SI
TIENE ALGÚN COMENTARIO SOBRE LA EXACTITUD DEL TIEMPO ESTIMADO O SUGERENCIAS PARA MEJORAR ESTE
FORMULARIO, POR FAVOR ESCRIBA A: CMS, 7500 SECURITY BOULEVARD, ATTN: PRA REPORTS CLEARANCE
OFFICER, MAIL STOP C4-26-05, BALTIMORE, MARYLAND 21244-1850.

Appendix C: Spanish: Mail Survey Cover Letters, Mail Questionnaires,
December 2015 Instructions for Scannable Mail Questionnaire, Telephone Interview Script
Centers for Medicare & Medicaid Services C-5 Outpatient and Ambulatory Surgery CAHPS Survey Protocols and Guidelines Manual
INSTRUCCIONES PARA LA ENCUESTA
Conteste todas las preguntas marcando el cuadrito que aparece a la izquierda de su respuesta.
A veces se le pide que salte algunas preguntas en esta encuesta. Cuando esto ocurra, verá una flecha con una nota que le indicará cuál es la siguiente pregunta a la que tiene que ir, de esta manera:
Sí
No Si contestó “No”,
pase a la pregunta 1 Esta encuesta pregunta acerca de sus experiencias en el centro ambulatorio que se menciona en la carta de presentación. Para esta encuesta, usamos el término “procedimiento” para procedimientos de diagnóstico, cirugías u otros procedimientos. Nos referimos al “centro ambulatorio” como el lugar en donde se realizó su procedimiento.
Por favor, responda las preguntas solo para el/los procedimiento(s) que tuvo en la fecha que se incluye en la carta de presentación. No incluya ningún otro procedimiento en sus respuestas.
I. ANTES DEL PROCEDIMIENTO
Las primeras preguntas son acerca de la preparación para su procedimiento. Incluya cualquier información que haya recibido antes o en el día del procedimiento.
1. Antes del procedimiento, ¿le dio un doctor o alguien del centro ambulatorio toda la información que necesitaba acerca de su procedimiento?
1 Sí, definitivamente 2 Sí, algo 3 No
2. Antes del procedimiento, ¿le dio un doctor o alguien del centro ambulatorio instrucciones fáciles de entender sobre lo que necesitaba para prepararse para su procedimiento?
1 Sí, definitivamente 2 Sí, algo 3 No
II. ACERCA DEL CENTRO
AMBULATORIO Y EL PERSONAL
Las siguientes preguntas se refieren al día de su procedimiento.
3. ¿Fue fácil el proceso de registro?
1 Sí, definitivamente 2 Sí, algo 3 No
4. ¿Estaba limpio el centro ambulatorio?
1 Sí, definitivamente 2 Sí, algo 3 No

Appendix C: Spanish: Mail Survey Cover Letters, Mail Questionnaires,
Instructions for Scannable Mail Questionnaire, Telephone Interview Script December 2015
C-6 Centers for Medicare & Medicaid Services Outpatient and Ambulatory Surgery CAHPS Survey Protocols and Guidelines Manual
5. ¿Le ayudó el personal administrativo y de recepción del centro ambulatorio tanto como usted pensaba que debían hacerlo?
1 Sí, definitivamente 2 Sí, algo 3 No
6. ¿Le trató el personal administrativo y de recepción del centro ambulatorio con cortesía y respeto?
1 Sí, definitivamente 2 Sí, algo 3 No
7. ¿Le trataron los doctores y enfermeras con cortesía y respeto?
1 Sí, definitivamente 2 Sí, algo 3 No
8. ¿Se aseguraron los doctores y enfermeras que usted estuviera tan cómodo como fuera posible?
1 Sí, definitivamente 2 Sí, algo 3 No
III. COMUNICACIÓN SOBRE SU
PROCEDIMIENTO
Le recordamos que por favor incluya cualquier información que haya recibido ya sea antes o en el día del procedimiento.
9. ¿Le explicaron los doctores u enfermeras el procedimiento de tal manera que fue fácil de entender?
1 Sí, definitivamente 2 Sí, algo 3 No
10. La anestesia es algo que le haría sentir sueño o dormir durante el procedimiento. ¿Le dieron anestesia?
1 Sí 2 No Si contestó “No”,
pase a la pregunta 13
11. ¿Le explicó el doctor o alguien del centro ambulatorio el proceso de dar anestesia de tal manera que fue fácil de entender?
1 Sí, definitivamente 2 Sí, algo 3 No
12. ¿Le explicó el doctor o alguien del centro ambulatorio los posibles efectos secundarios de la anestesia de tal manera que fuera fácil de entender?
1 Sí, definitivamente 2 Sí, algo 3 No

Appendix C: Spanish: Mail Survey Cover Letters, Mail Questionnaires,
December 2015 Instructions for Scannable Mail Questionnaire, Telephone Interview Script
Centers for Medicare & Medicaid Services C-7 Outpatient and Ambulatory Surgery CAHPS Survey Protocols and Guidelines Manual
13. Las instrucciones al ser dado de alta incluyen observar los síntomas después de su procedimiento, instrucciones sobre los medicamentos y cuidado en el hogar. Antes de salir del centro ambulatorio, ¿recibió instrucciones por escrito al darle de alta?
1 Sí 2 No
IV. SU RECUPERACIÓN
14. ¿Le preparó el doctor o alguien del personal del centro ambulatorio sobre qué esperar durante su recuperación?
1 Sí, definitivamente 2 Sí, algo 3 No
15. Algunas maneras para controlar el dolor incluyen medicamentos recetados, medicamentos para el dolor de venta libre o bolsas de hielo. ¿Su doctor o alguien del centro ambulatorio le dio información sobre qué hacer si tenía dolor como resultado de su procedimiento?
1 Sí, definitivamente 2 Sí, algo 3 No
16. En algún momento después de salir del centro ambulatorio, ¿tuvo dolor debido al procedimiento?
1 Sí 2 No
17. Antes de salir del centro ambulatorio, ¿su doctor o alguien del personal del centro ambulatorio le dio información sobre qué hacer si tenía náusea o vómitos?
1 Sí, definitivamente 2 Sí, algo 3 No
18. En algún momento después de salir del centro ambulatorio, ¿tuvo náusea o vómitos como resultado del procedimiento o la anestesia?
1 Sí 2 No
19. Antes de salir del centro ambulatorio, ¿su doctor o alguien del personal del centro ambulatorio le dio información sobre qué hacer si sangraba como resultado del procedimiento?
1 Sí, definitivamente 2 Sí, algo 3 No
20. En algún momento después de salir del centro ambulatorio, ¿tuvo sangrado como resultado del procedimiento?
1 Sí 2 No

Appendix C: Spanish: Mail Survey Cover Letters, Mail Questionnaires,
Instructions for Scannable Mail Questionnaire, Telephone Interview Script December 2015
C-8 Centers for Medicare & Medicaid Services Outpatient and Ambulatory Surgery CAHPS Survey Protocols and Guidelines Manual
21. Posibles señales de infección incluyen fiebre, hinchazón, calor, secreción o enrojecimiento. Antes de salir del centro ambulatorio, ¿su doctor o alguien del personal del centro ambulatorio le dio información sobre qué hacer si tuviera señales de infección?
1 Sí, definitivamente 2 Sí, algo 3 No
22. En algún momento después de salir del centro ambulatorio, ¿tuvo señales de infección?
1 Sí 2 No
V. SU EXPERIENCIA GENERAL
23. Usando un número del 0 al 10, en donde 0 es el peor centro ambulatorio posible y 10 es el mejor centro ambulatorio posible, ¿qué número usaría para calificar éste centro ambulatorio?
0 Peor centro ambulatorio
posible
1
2
3
4
5
6
7
8
9
10 Mejor centro ambulatorio
posible
24. ¿Recomendaría este centro ambulatorio a sus amistades y familia?
1 Definitivamente no 2 Probablemente no 3 Probablemente sí 4 Definitivamente sí
Appendix C: Spanish: Mail Survey Cover Letters, Mail Questionnaires,
December 2015 Instructions for Scannable Mail Questionnaire, Telephone Interview Script
Centers for Medicare & Medicaid Services C-9 Outpatient and Ambulatory Surgery CAHPS Survey Protocols and Guidelines Manual
VI. ACERCA DE USTED
25. En general, ¿cómo calificaría su salud general?
1 Excelente 2 Muy buena 3 Buena 4 Regular 5 Mala
26. En general, ¿cómo calificaría su salud mental o emocional?
1 Excelente 2 Muy buena 3 Buena 4 Regular 5 Mala
27. ¿Qué edad tiene usted?
1 18 a 24 años 2 25 a 34 años 3 35 a 44 años 4 45 a 54 años 5 55 a 64 años 6 65 a 74 años 7 75 a 79 años 8 80 a 84 años 9 85 años o más
28. ¿Es usted hombre o mujer?
1 Hombre 2 Mujer
29. ¿Cuál es el nivel o año escolar más avanzado que usted ha completado?
1 8o años de escuela o menos 2 9-12 años de escuela, pero
sin graduarse 3 Graduado de la escuela
secundaria, Diploma de escuela secundaria, preparatoria o su equivalente (o GED)
4 Algunos cursos universitarios o un título universitario de un programa de 2 años
5 Título universitario de 4 años 6 Título universitario de más de
4 años
30. ¿Es usted de origen hispano, latino o español?
1 Sí, soy de origen hispano, latino o español
2 No, no soy de origen hispano, latino o español Si contestó “No”, pase a la pregunta 32
31. ¿Cuál grupo lo(a) describe mejor?
1 Mexicano, mexicano americano, chicano
2 Puertorriqueño 3 Cubano 4 Otro origen hispano, latino o
español

Appendix C: Spanish: Mail Survey Cover Letters, Mail Questionnaires,
Instructions for Scannable Mail Questionnaire, Telephone Interview Script December 2015
C-10 Centers for Medicare & Medicaid Services Outpatient and Ambulatory Surgery CAHPS Survey Protocols and Guidelines Manual
32. ¿Cuál es su raza? Puede seleccionar una o más categorías.
1 Blanca 2 Negra o afro americana 3 Indígena americana o nativa
de Alaska 4 India asiática 5 China 6 Filipina 7 Japonesa 8 Coreana 9 Vietnamita 10 Otra raza asiática 11 Nativa de Hawai 12 Procedente de Guam o
Chamorro 13 Samoana 14 Otra raza de las islas del
Pacífico
33. ¿Qué tan bien habla usted inglés?
1 Muy bien 2 Bien 3 No bien 4 Nada
34. ¿Habla usted algún otro idioma que no sea inglés en casa?
1 Sí 2 No Si contestó “No”, pase
a la pregunta 36
35. ¿Qué idioma habla en su casa?
1 Español 2 Otro idioma
(FAVOR DE ESPECIFICAR): _______________________ (Favor de usar letra tipo imprenta.)
36. ¿Le ayudó alguien a completar esta encuesta?
1 Sí 2 No Si contestó No, vaya
al FINAL.
37. ¿De qué manera le ayudó esa persona? Marque todas las respuestas que correspondan.
1 Me leyó las preguntas 2 Anotó las respuestas que le di 3 Contestó las preguntas por mi 4 Me tradujo las preguntas a mi
idioma 5 Me ayudó de alguna otra
manera: (EXPLIQUE): _______________________ (Favor de usar letra tipo imprenta.)
6 Nadie me ayudó a completar esta encuesta
FINAL

Appendix C: Spanish: Mail Survey Cover Letters, Mail Questionnaires,
December 2015 Instructions for Scannable Mail Questionnaire, Telephone Interview Script
Centers for Medicare & Medicaid Services C-11 Outpatient and Ambulatory Surgery CAHPS Survey Protocols and Guidelines Manual

Appendix C: Spanish: Mail Survey Cover Letters, Mail Questionnaires,
Instructions for Scannable Mail Questionnaire, Telephone Interview Script December 2015
C-12 Centers for Medicare & Medicaid Services Outpatient and Ambulatory Surgery CAHPS Survey Protocols and Guidelines Manual
(This version contains alternative Instructions for Scannable Forms)
INSTRUCCIONES PARA LA ENCUESTA
· Responda todas las preguntas llenando por completo el círculo a la izquierda de su respuesta.
· A veces se le indica que debe saltarse algunas preguntas de esta encuesta. Cuando ocurra,
verá una flecha con una nota que le indica qué pregunta es la siguiente, de esta manera:
Sí
No Si contestó “No”, pase a la pregunta 1
Esta encuesta pregunta acerca de sus experiencias en el centro ambulatorio que se menciona en
la carta de presentación. Para esta encuesta, usamos el término “procedimiento” para
procedimientos de diagnóstico, cirugías u otros procedimientos. Nos referimos al “centro
ambulatorio” como el lugar en donde se realizó su procedimiento.
Por favor, responda las preguntas solo para el/los procedimiento(s) que tuvo en la fecha
que se incluye en la carta de presentación. No incluya ningún otro procedimiento en sus
respuestas.

Appendix C: Spanish: Mail Survey Cover Letters, Mail Questionnaires,
December 2015 Instructions for Scannable Mail Questionnaire, Telephone Interview Script
Centers for Medicare & Medicaid Services C-13 Outpatient and Ambulatory Surgery CAHPS Survey Protocols and Guidelines Manual
TELEPHONE INTERVIEW SCRIPT
FOR THE OUTPATIENT AND AMBULATORY SURGERY CAHPS SURVEY
INTRO1 [Buenos días/Buenas tardes/Buenas noches], ¿puedo hablar con [SAMPLE
MEMBER’S NAME]?
1. YES Go to INTRO 2
2. NO, NOT AVAILABLE RIGHT NOW [SET CALLBACK]
3. NO [REFUSAL] Go to TERMINATE Screen,
4. MENTALLY/PHYSICALLY INCAPABLE [CODE AS INCAPABLE]
IF ASKED WHO IS CALLING:
Mi nombre es [INTERVIEWER NAME], y estoy llamando de [VENDOR] en
nombre de [FACILITY NAME]. Me gustaría hablar con [SAMPLE MEMBER’S
NAME] sobre una encuesta sobre la atención médica.
INTRO2 [Buenos días/Buenas tardes/Buenas noches], mi nombre es [INTERVIEWER
NAME] y estoy llamando de parte de [FACILITY NAME]. [FACILITY NAME]
está participando en una encuesta sobre las experiencias de los pacientes que han
tenido una cirugía o un procedimiento ambulatorio. Los resultados se usarán para
ayudar a [FACILITY NAME] a comprender las experiencias de los pacientes en
su centro ambulatorio.
Su participación en esta encuesta es completamente voluntaria y no afectará a
ningún beneficio de atención médica que usted recibe. Toda la información que
proporcione es confidencial y está protegida por la Ley de Privacidad. La
entrevista se puede completar como en 8 minutos. Esta llamada puede ser
escuchada o grabada con propósitos de mejorar la calidad.
[ADDRESS ANY QUESTIONS/CONCERNS THEN CONTINUE.]
INTRO3 La encuesta hace preguntas sobre sus experiencias con [FACILITY NAME]. Para
esta encuesta, usamos el término “procedimiento” para procedimientos de
diagnóstico, cirugías u otros procedimientos. Nos referimos al “centro
ambulatorio” como el lugar en donde se realizó su procedimiento. Por favor,
responda a estas preguntas solo para el procedimiento que se realizó el [DATE]. No
incluya ningún otro procedimiento en sus respuestas.

Appendix C: Spanish: Mail Survey Cover Letters, Mail Questionnaires,
Instructions for Scannable Mail Questionnaire, Telephone Interview Script December 2015
C-14 Centers for Medicare & Medicaid Services Outpatient and Ambulatory Surgery CAHPS Survey Protocols and Guidelines Manual
[ADDRESS ANY QUESTIONS/CONCERNS THEN SELECT RESPONSE OPTION.]
1 BEGIN INTERVIEW [GO TO Q1_INTRO]
2 NO, NOT RIGHT NOW [SET CALLBACK]
3 DID NOT RECEIVE SURGERY/PROCEDURE FROM THIS FACILITY
DURING [MONTH] [GO TO Q_INELIGIBLE SCREEN]
4 NO [REFUSAL] [GO TO Q_REF SCREEN]
Q1_INTRO Las primeras preguntas son acerca de la preparación para su procedimiento.
Incluya cualquier información que haya recibido antes o en el día del
procedimiento.
Q1. Antes del procedimiento, ¿le dio un doctor o alguien del centro ambulatorio toda
la información que necesitaba acerca de su procedimiento? ¿Diría usted que…?
1 Sí, definitivamente
2 Sí, algo
3 No
M MISSING/DK
Q2. Antes del procedimiento, ¿le dio un doctor o alguien del centro ambulatorio
instrucciones fáciles de entender sobre lo que necesitaba para prepararse para su
procedimiento? ¿Diría que…?
1 Sí, definitivamente
2 Sí, algo
3 No
M MISSING/DK
Q3 INTRO Las siguientes preguntas se refieren al día de su procedimiento.
Q3. ¿Fue fácil el proceso de registro? ¿Diría que…?
1 Sí, definitivamente
2 Sí, algo
3 No
M MISSING/DK

Appendix C: Spanish: Mail Survey Cover Letters, Mail Questionnaires,
December 2015 Instructions for Scannable Mail Questionnaire, Telephone Interview Script
Centers for Medicare & Medicaid Services C-15 Outpatient and Ambulatory Surgery CAHPS Survey Protocols and Guidelines Manual
Q4. ¿Estaba limpio el centro ambulatorio? ¿Diría que…?
1 Sí, definitivamente
2 Sí, algo
3 No
M MISSING/DK
Q5. ¿Le ayudó el personal administrativo y de recepción del centro ambulatorio tanto
como usted pensaba que debían hacerlo? ¿Diría que…?
1 Sí, definitivamente
2 Sí, algo
3 No
M MISSING/DK
Q6. ¿Le trató el personal administrativo y de recepción del centro ambulatorio con
cortesía y respeto? ¿Diría que…?
1 Sí, definitivamente
2 Sí, algo
3 No
M MISSING/DK
Q7. ¿Le trataron los doctores y enfermeras con cortesía y respeto? ¿Diría que…?
1 Sí, definitivamente
2 Sí, algo
3 No
M MISSING/DK
Q8. ¿Se aseguraron los doctores y enfermeras que usted estuviese tan cómodo como
fuera posible? ¿Diría que…?
1 Sí, definitivamente
2 Sí, algo
3 No
M MISSING/DK
Appendix C: Spanish: Mail Survey Cover Letters, Mail Questionnaires,
Instructions for Scannable Mail Questionnaire, Telephone Interview Script December 2015
C-16 Centers for Medicare & Medicaid Services Outpatient and Ambulatory Surgery CAHPS Survey Protocols and Guidelines Manual
Q9_INTRO Le recordamos que por favor incluya cualquier información que haya recibido ya
sea antes o en el día del procedimiento.
Q9. ¿Le explicaron los doctores u enfermeras el procedimiento de tal manera que fue
fácil de entender? ¿Diría usted que…?
1 Sí, definitivamente
2 Sí, algo
3 No
M MISSING/DK
Q10. La anestesia es algo que le haría sentir sueño o dormir durante el procedimiento.
¿Le dieron anestesia?
1 SÍ
2 NO [GO TO Q13]
M MISSING/DK
Q11. ¿Le explicó el doctor o alguien del centro ambulatorio el proceso de dar anestesia
de tal manera que fue fácil de entender? ¿Diría usted que…?
1 Sí, definitivamente
2 Sí, algo
3 No
M MISSING/DK
Q12. ¿Le explicó el doctor o alguien del centro ambulatorio los posibles efectos
secundarios de la anestesia de tal manera que fuera fácil de entender? ¿Diría usted
que…?
1 Sí, definitivamente
2 Sí, algo
3 No
M MISSING/DK

Appendix C: Spanish: Mail Survey Cover Letters, Mail Questionnaires,
December 2015 Instructions for Scannable Mail Questionnaire, Telephone Interview Script
Centers for Medicare & Medicaid Services C-17 Outpatient and Ambulatory Surgery CAHPS Survey Protocols and Guidelines Manual
Q13. Las instrucciones al ser dado de alta incluyen observar los síntomas después de su
procedimiento, instrucciones sobre los medicamentos y cuidado en el hogar.
Antes de salir del centro ambulatorio, ¿recibió instrucciones por escrito al darle de
alta?
1 SÍ
2 NO
M MISSING/DK
Q14. ¿Le preparó el doctor o alguien del personal del centro ambulatorio sobre qué
esperar durante su recuperación? ¿Diría que…?
1 Sí, definitivamente
2 Sí, algo
3 No
M MISSING/DK
Q15. Algunas maneras para controlar el dolor incluyen medicamentos recetados,
medicamentos para el dolor de venta libre o bolsas de hielo. ¿Su doctor o alguien
del centro ambulatorio le dio información sobre qué hacer si tenía dolor como
resultado de su procedimiento? ¿Diría que…?
1 Sí, definitivamente
2 Sí, algo
3 No
M MISSING/DK
Q16. En algún momento después de salir del centro ambulatorio, ¿tuvo dolor debido al
procedimiento?
1 SÍ
2 NO
M MISSING/DK

Appendix C: Spanish: Mail Survey Cover Letters, Mail Questionnaires,
Instructions for Scannable Mail Questionnaire, Telephone Interview Script December 2015
C-18 Centers for Medicare & Medicaid Services Outpatient and Ambulatory Surgery CAHPS Survey Protocols and Guidelines Manual
Q17. Antes de salir del centro ambulatorio, ¿su doctor o alguien del personal del centro
ambulatorio le dio información sobre qué hacer si tenía náusea o vómitos? ¿Diría
que…?
1 Sí, definitivamente
2 Sí, algo
3 No
M MISSING/DK
Q18. En algún momento después de salir del centro ambulatorio, ¿tuvo náusea o
vómitos como resultado del procedimiento o la anestesia?
1 SÍ
2 NO
M MISSING/DK
Q19. Antes de salir del centro ambulatorio, ¿su doctor o alguien del personal del centro
ambulatorio le dio información sobre qué hacer si sangraba como resultado del
procedimiento? ¿Diría que…?
1 Sí, definitivamente
2 Sí, algo
3 No
M MISSING/DK
Q20. En algún momento después de salir del centro ambulatorio, ¿tuvo sangrado como
resultado del procedimiento?
1 SÍ
2 NO
M MISSING/DK

Appendix C: Spanish: Mail Survey Cover Letters, Mail Questionnaires,
December 2015 Instructions for Scannable Mail Questionnaire, Telephone Interview Script
Centers for Medicare & Medicaid Services C-19 Outpatient and Ambulatory Surgery CAHPS Survey Protocols and Guidelines Manual
Q21. Posibles señales de infección incluyen fiebre, hinchazón, calor, secreción o
enrojecimiento. Antes de salir del centro ambulatorio, ¿su doctor o alguien del
personal del centro ambulatorio le dio información sobre qué hacer si tuviera
señales de infección? ¿Diría que…?
1 Sí, definitivamente
2 Sí, algo
3 No
M MISSING/DK
Q22. En algún momento después de salir del centro ambulatorio, ¿tuvo señales de
infección?
1 SÍ
2 NO
M MISSING/DK
Q23_INTRO Las siguientes preguntas se refieren a su experiencia en general.
Q23. Usando un número del 0 al 10, en donde 0 es el peor centro ambulatorio posible y
10 es el mejor centro ambulatorio posible, ¿qué número usaría para calificar éste
centro ambulatorio?
0 PEOR CENTRO AMBULATORIO POSIBLE
1
2
3
4
5
6
7
8
9
10 MEJOR CENTRO AMBULATORIO POSIBLE
M MISSING/DK

Appendix C: Spanish: Mail Survey Cover Letters, Mail Questionnaires,
Instructions for Scannable Mail Questionnaire, Telephone Interview Script December 2015
C-20 Centers for Medicare & Medicaid Services Outpatient and Ambulatory Surgery CAHPS Survey Protocols and Guidelines Manual
Q24. ¿Recomendaría este centro ambulatorio a sus amistades y familia? ¿Diría usted
que…?
1 Definitivamente no
2 Probablemente no
3 Probablemente sí
4 Definitivamente sí
M MISSING/DK
Q25. En general, ¿cómo calificaría su salud general? ¿Diría que es…
1 Excelente
2 Muy buena
3 Buena
4 Regular o
5 Mala?
M MISSING/DK
Q26. En general, ¿cómo calificaría su salud mental o emocional? ¿Diría que es…
1 Excelente
2 Muy buena
3 Buena
4 Regular o
5 Mala?
M MISSING/DK
Q27. ¿Qué edad tiene usted?
1 18 A 24 AÑOS
2 25 A 34 AÑOS
3 35 A 44 AÑOS
4 45 A 54 AÑOS
5 55 A 64 AÑOS
6 65 A 74 AÑOS
7 75 A 79 AÑOS
8 80 A 84 AÑOS
9 85 AÑOS O MÁS
M MISSING/DK
Appendix C: Spanish: Mail Survey Cover Letters, Mail Questionnaires,
December 2015 Instructions for Scannable Mail Questionnaire, Telephone Interview Script
Centers for Medicare & Medicaid Services C-21 Outpatient and Ambulatory Surgery CAHPS Survey Protocols and Guidelines Manual
Q28. ¿Es usted hombre o mujer?
1 HOMBRE
2 MUJER
M MISSING/DK
Q29. ¿Cuál es el nivel o año escolar más avanzado que usted ha completado? ¿Diría
que…?
1 8o grado de escuela o menos
2 9-12 años de escuela, pero sin graduarse
3 Graduado(a) de escuela secundaria, diploma de escuela secundaria,
preparatoria o su equivalente o 'GED'
4 Algunos cursos universidarios o un título universitario de un programa de 2
años
5 Título universitario de 4 años o
6 Título universitario de más de 4 años
M MISSING/DK
Q30. ¿Es usted de origen hispano, latino o español?
1 SÍ,
2 NO [GO TO Q32]
M MISSING/DK
Q31. ¿Cuál grupo lo(a) describe mejor? ¿Diría que usted es…?
1 Mexicano(a), mexicano(a) americano(a), chicano(a)
2 Puertorriqueño(a)
3 Cubano(a)
4 Otro origen hispano, latino o español
M MISSING/DK
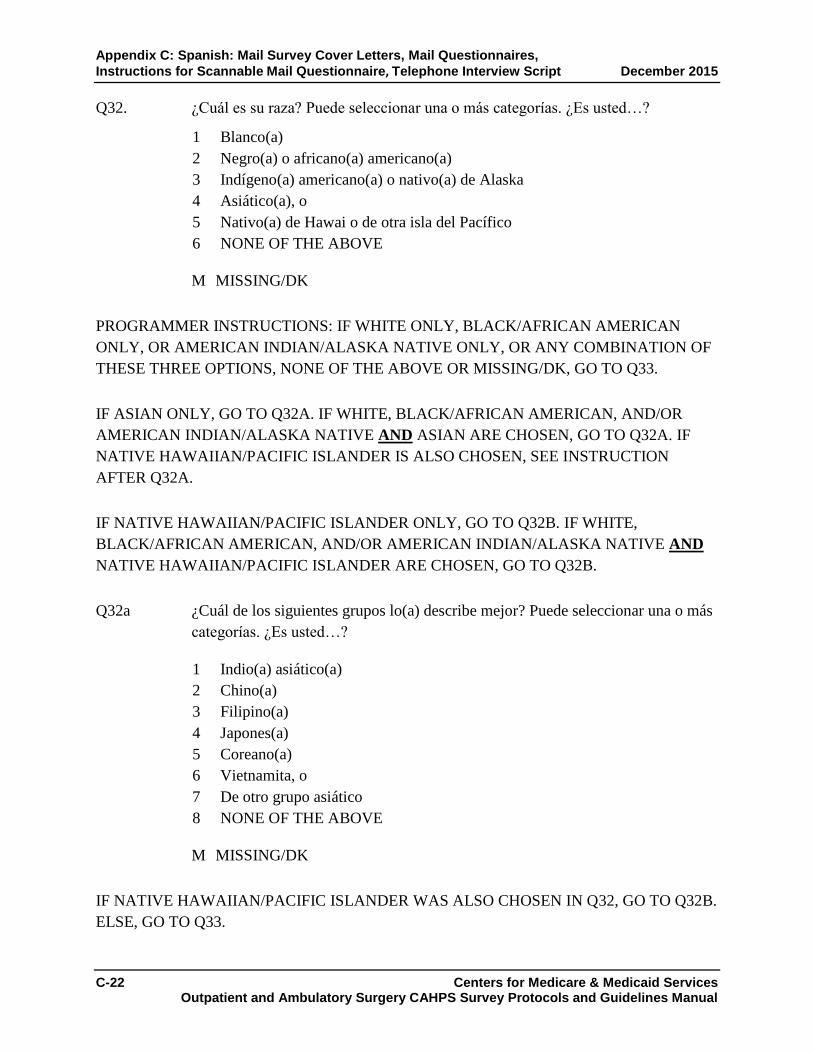
Appendix C: Spanish: Mail Survey Cover Letters, Mail Questionnaires,
Instructions for Scannable Mail Questionnaire, Telephone Interview Script December 2015
C-22 Centers for Medicare & Medicaid Services Outpatient and Ambulatory Surgery CAHPS Survey Protocols and Guidelines Manual
Q32. ¿Cuál es su raza? Puede seleccionar una o más categorías. ¿Es usted…?
1 Blanco(a)
2 Negro(a) o africano(a) americano(a)
3 Indígeno(a) americano(a) o nativo(a) de Alaska
4 Asiático(a), o
5 Nativo(a) de Hawai o de otra isla del Pacífico
6 NONE OF THE ABOVE
M MISSING/DK
PROGRAMMER INSTRUCTIONS: IF WHITE ONLY, BLACK/AFRICAN AMERICAN
ONLY, OR AMERICAN INDIAN/ALASKA NATIVE ONLY, OR ANY COMBINATION OF
THESE THREE OPTIONS, NONE OF THE ABOVE OR MISSING/DK, GO TO Q33.
IF ASIAN ONLY, GO TO Q32A. IF WHITE, BLACK/AFRICAN AMERICAN, AND/OR
AMERICAN INDIAN/ALASKA NATIVE AND ASIAN ARE CHOSEN, GO TO Q32A. IF
NATIVE HAWAIIAN/PACIFIC ISLANDER IS ALSO CHOSEN, SEE INSTRUCTION
AFTER Q32A.
IF NATIVE HAWAIIAN/PACIFIC ISLANDER ONLY, GO TO Q32B. IF WHITE,
BLACK/AFRICAN AMERICAN, AND/OR AMERICAN INDIAN/ALASKA NATIVE AND
NATIVE HAWAIIAN/PACIFIC ISLANDER ARE CHOSEN, GO TO Q32B.
Q32a ¿Cuál de los siguientes grupos lo(a) describe mejor? Puede seleccionar una o más
categorías. ¿Es usted…?
1 Indio(a) asiático(a)
2 Chino(a)
3 Filipino(a)
4 Japones(a)
5 Coreano(a)
6 Vietnamita, o
7 De otro grupo asiático
8 NONE OF THE ABOVE
M MISSING/DK
IF NATIVE HAWAIIAN/PACIFIC ISLANDER WAS ALSO CHOSEN IN Q32, GO TO Q32B.
ELSE, GO TO Q33.

Appendix C: Spanish: Mail Survey Cover Letters, Mail Questionnaires,
December 2015 Instructions for Scannable Mail Questionnaire, Telephone Interview Script
Centers for Medicare & Medicaid Services C-23 Outpatient and Ambulatory Surgery CAHPS Survey Protocols and Guidelines Manual
Q32b ¿ Cuál de los siguientes grupos lo(a) describe mejor? Puede seleccionar una o más
categorías. ¿Es usted…?
1 Nativo(a) de Hawai
2 Procedente de Guam o Chamorro
3 Samoano(a), o
4 De otra isla del Pacífico
5 NONE OF THE ABOVE
M MISSING/DK
Q33. ¿Qué tan bien habla usted inglés? ¿Diría que…?
1 Muy bien
2 Bien
3 No bien
4 Nada
M MISSING/DK
Q34. ¿Habla usted algún otro idioma que no sea inglés en casa?
1 Sí, hablo un idioma que no sea inglés
2 No.Yo hablo inglés en casa. [GO TO Q_END]
M MISSING/DK
Q35. ¿Qué idioma habla en su casa?
1 Español [GO TO Q_END]
2 Otro idioma (GO TO Q35a)
M MISSING/DK

Appendix C: Spanish: Mail Survey Cover Letters, Mail Questionnaires,
Instructions for Scannable Mail Questionnaire, Telephone Interview Script December 2015
C-24 Centers for Medicare & Medicaid Services Outpatient and Ambulatory Surgery CAHPS Survey Protocols and Guidelines Manual
Q35a. ¿Qué idioma habla en su casa? (ENTER RESPONSE BELOW)
{ALLOW UP TO 50 CHARACTERS}
M MISSING/DK
Q_END Estas son todas las preguntas que tengo para usted. Muchas gracias por su tiempo.
Le deseo que tenga (un buen día/buenas noches).
INELIGIBLE SCREEN:
Q_INELIG Muchas gracias por su tiempo. Le deseo que tenga (un buen día/buenas noches).
REFUSAL SCREEN:
Q_REF Muchas gracias por su tiempo. Le deseo que tenga (un buen día/buenas noches).

Centers for Medicare & Medicaid Services Outpatient and Ambulatory Surgery CAHPS Survey Protocols and Guidelines Manual
APPENDIX D:
CHINESE (FORTHCOMING): MAIL SURVEY COVER LETTERS,
MAIL QUESTIONNAIRES, INSTRUCTIONS FOR SCANNABLE MAIL QUESTIONNAIRE

Appendix D: Chinese: Mail Survey Cover Letters, Mail Questionnaires, Instructions for Scannable Mail Questionnaire December 2015
Centers for Medicare & Medicaid Services Outpatient and Ambulatory Surgery CAHPS Survey Protocols and Guidelines Manual
This page intentionally left blank.

Centers for Medicare & Medicaid Services Outpatient and Ambulatory Surgery CAHPS Survey Protocols and Guidelines Manual
Chinese (Simplified)

Appendix D: Chinese: Mail Survey Cover Letters, Mail Questionnaires, Instructions for Scannable Mail Questionnaire December 2015
Centers for Medicare & Medicaid Services Outpatient and Ambulatory Surgery CAHPS Survey Protocols and Guidelines Manual
This page intentionally left blank.

Centers for Medicare & Medicaid Services D-1 Outpatient and Ambulatory Surgery CAHPS Survey Protocols and Guidelines Manual
SAMPLE COVER LETTER FOR FIRST QUESTIONNAIRE MAILING
Outpatient and Ambulatory Surgery CAHPS Survey
To be Printed on Ambulatory Surgery Center or Hospital Outpatient Department or Vendor
Letterhead
«FirstName» «LastName»
«Address1» «Address2»
«City_Name», «State_Code» «Zip_Zip4»
尊敬的 «FirstName» <<LastName>>:
[FACILITY]想了解病人在我们的医院得到的医疗服务的质量。 [VENDOR],
一家独立的研究机构,帮助我们做这个问卷调查。 我们的记录表明您在 [FACILITY]
做过手术或接受过治疗。
这个调查的结果,将帮助我们更好地理解病人在我们医院的经历。
随附的调查问卷,将询问在[DATE OF SURGERY]您对您的门诊手术或医疗程序的意见。
我们请您花几分钟时间填写此调查问卷,并用随附的邮资已付的信封将其寄回给我们。
当您回答本调查问卷中的问题时,仅考虑您 [DATE OF SURGERY] 在 [FACILITY]
的经历。不要涉及您在我们医院或其他医院做其他手术或医疗程序的经历。
您在此提供的所有信息均将保密,并受到《隐私法》(Privacy Act) 保护。
您对问卷的回答将与其他调查研究参与者的回答一起汇总;当分析数据时,
您的姓名和身份识别信息不会与您的回答关联在一起。对[FACILITY
NAME]和其他医院调查的结果将于2017年在网上公布,
网址是https://www.medicare.gov/ 。
这些调查结果将帮助人们在选择门诊手术及非住院手术的医院时,做出知情的决定。
您的参与纯属自愿,不会影响您的任何医疗福利。
如果您对本调查研究有任何疑问,请拨打免费服务电话1-800-XXX-XXXX致电NAME。
如果您在阅读问卷或回答问题方面需要帮助,请让家人或朋友帮助您。感谢您的参与。
祝好!
NAME
Title
附件 [PRINT UNIQUE SAMPLE ID NUMBER HERE]

Appendix D: Chinese: Mail Survey Cover Letters, Mail Questionnaires, Instructions for Scannable Mail Questionnaire December 2015
D-2 Centers for Medicare & Medicaid Services Outpatient and Ambulatory Surgery CAHPS Survey Protocols and Guidelines Manual
SAMPLE COVER LETTER FOR SECOND QUESTIONNAIRE MAILING TO MAIL
SURVEY NONRESPONDENTS
Outpatient and Ambulatory Surgery CAHPS Survey
To be Printed on Ambulatory Surgery Center or Hospital Outpatient Department or Vendor
Letterhead
«FirstName» «LastName»
«Address1» «Address2»
«City_Name», «State_Code» «Zip_Zip4»
尊敬的 «FirstName»<<LastName>>:
最近,我们给您寄了一封信,请您帮助完成一项问卷调查,
此问卷询问您在[FACILITY]接受门诊手术或医疗程序时的该医院的服务质量。
迄今为止,我们尚未收到您填妥的调查问卷。如果您已寄回调查问卷,我们不胜感激。
如果您尚未填写该调查问卷,请现在就花几分钟时间填写。然后用随附的邮资已付的信
封将其寄回给我们。
当您回答本调查问卷中的问题时,仅考虑您 [DATE OF SURGERY] 在 [FACILITY]
的经历。不要涉及您在我们医院或其他医院,做其他手术或医疗程序的经历。
您在此提供的所有信息均将保密,并受到《隐私法》(Privacy Act) 保护。
您的参与纯属自愿,不会影响您的任何医疗福利。
如果您对该调查研究有任何疑问,请拨打免费服务电话1-800-XXX-XXXX致电NAME。
如果您在阅读问卷或回答问题方面需要帮助,请让家人或朋友帮助您。感谢您的参与。
祝好!
NAME
Title

Consumer Assessment of Healthcare Providers and Systems Outpatient and
Ambulatory Surgery Survey (OAS CAHPS)
A PATIENT EXPERIENCE OF CARE SURVEY ABOUT OUTPATIENT AND AMBULATORY SURGERIES
AND PROCEDURES
2016
消费者评估医疗服务机构和系统
门诊手术及非住院手术问卷调查
(OAS CAHPS)
关于门诊手术及其他非住院手术和医疗程序中病人经历的问卷调查
2016年
根据1995年减少纸张使用法案,如果问卷上没有有效的OMB控制数码,任何人都无须
回答问卷上的任何问题。这项问卷持有有效的OMB控制数码:0938-1240。完成这份问
卷,估计需要八分钟。这包括阅读问卷的说明,查找现有的资料,收集和整理所需的信
息,以及完成和审阅所提供的信息。如果您对完成这份问卷所估计的时间或对如何改进
这项问卷有任何看法,请写信给: CMS, 7500 Security Boulevard, Attn: PRA Reports
Clearance Officer, Mail Stop C4-26-05, Baltimore, Maryland 21244-1850.

Appendix D: Chinese: Mail Survey Cover Letters, Mail Questionnaires, Instructions for Scannable Mail Questionnaire December 2015
D-4 Centers for Medicare & Medicaid Services Outpatient and Ambulatory Surgery CAHPS Survey Protocols and Guidelines Manual
SURVEY INSTRUCTIONS
请回答所有的问题。作答时,请在问题左
边的方格内打勾。
有时问卷会要求您跳过一些问题。这种情
况发生时,您会看到箭头并注明下一个该
回答的问题,如:
是
否 如回答否,请跳到#1.
本问卷调查是关于您在我们这封信所特指
的医院的经历。在本问卷调查中,“医疗
程序”这个词指的是诊断,外科手术及其
他医疗过程。“医疗处所”这个词指的是
进行您的医疗程序的地方。
请针对印在信函上所列的的日子那天您
所经历的所有医疗程序来回答这些问题
。在您回答问题时,请不要考虑或涉及
其他医疗程序。
I.在您的医疗程序之前
最初的几个问题是关于为进行您的医疗程
序所做的准备的。这包括在医疗程序之
前和程序当天,您所收到的任何有关信
息。
1. 在您的医疗程序之前,这个医疗处
所的医生或者其他人是否给您关于
这个程序您所需要的所有信息?
1 是的,十分确定 2 是的,在某种程度上
3 否
2. 在您的医疗程序之前,这个医疗处所
的医生或者其他人是否给您让您容
易理解的关于怎样准备您的医疗程
序的医嘱?
1 是的,十分确定 2 是的,在某种程度上 3 否
II.关于这个医疗处所及其医护人员
下面的问题,是有关您医疗程序当天的经
历。
3. 办理看病登记签到手续的过程是否
顺利流畅?
1 是的,十分确定 2 是的,在某种程度上
3 否
4. 这个医疗处所很干净吗?
1 是的,十分确定 2 是的,在某种程度上 3 否
5. 这个医疗处所的工作人员和前台接
待人员是否像您想象的那样很有帮
助?
1 是的,十分确定
2 是的,在某种程度上 3 否

Appendix D: Chinese: Mail Survey Cover Letters, December 2015 Mail Questionnaires, Instructions for Scannable Mail Questionnaire
Centers for Medicare & Medicaid Services D-5 Outpatient and Ambulatory Surgery CAHPS Survey Protocols and Guidelines Manual
6. 这个医疗处所的工作人员和前台接
待人员是否常以礼貌和尊重对待您?
1 是的,十分确定 2 是的,在某种程度上 3 否
7. 医生和护士是否常以礼貌和尊重对
待您?
1 是的,十分确定
2 是的,在某种程度上 3 否
8. 医生和护士是否尽可能让您感到舒适?
1 是的,十分确定 2 是的,在某种程度上 3 否
III.关于您的医疗程序的沟通交流
注意:请包括您在该医疗程序之前和当天所收到信息。
9. 医生和护士是否用您听得懂的方式来向您解释医疗程序?
1 是的,十分确定 2 是的,在某种程度上 3 否
10. 麻醉会让您在的医疗程序中感到困倦或入睡。是否给您用了麻醉?
1 是 2 否 如回答否,请跳到#13
11. 医生或这个医疗处所的其他人是否
用您听得懂的方式来向您解释麻醉?
1 是的,十分确定 2 是的,在某种程度上 3 否
12. 医生或医疗处所的其他人是否用您
用您听得懂的方式来向您解释麻醉
可能产生的副作用?
1 是的,十分确定 2 是的,在某种程度上 3 否
13. 出院医嘱包括:医疗程序之后,有
可能出现的需要注意的症状的说明,
服药说明, 在家调养须知等等。在
您离开医疗处所之前,您是否得到
了书面的出院医嘱?
1 是 2 否
IV.您的术后恢复
14. 您的医生或这个医疗处所的其他人
是否向您解释您的恢复过程是怎样
的?
1 是的,十分确定 2 是的,在某种程度上 3 否

Appendix D: Chinese: Mail Survey Cover Letters, Mail Questionnaires, Instructions for Scannable Mail Questionnaire December 2015
D-6 Centers for Medicare & Medicaid Services Outpatient and Ambulatory Surgery CAHPS Survey Protocols and Guidelines Manual
15. 止痛的方法有处方药、非处方止疼
药、或者冰袋等。您的医生或这个
医疗处所的其他人是否给您医嘱,
告诉您如果您因医疗程序而产生疼
痛的话应该怎么办?
1 是的,十分确定 2 是的,在某种程度上 3 否
16. 从这个医疗处所离开后的任何时
候,您是否因为您的医疗程序而感
到疼痛?
1 是 2 否
17. 在您离开这个医疗处所之前,您的
医生或这个医疗处所的其他人是否
给您医嘱,告诉您如果您恶心或是
呕吐该怎么办?
1 是的,十分确定 2 是的,在某种程度上 3 否
18. 从这个医疗处所离开后的任何时
候,您是否因为您的医疗程序而感
到恶心或者呕吐?
1 是 2 否
19. 在您离开这个医疗处所之前,您的
医生或这个医疗处所的其他人是否
给您医嘱,告诉您如果您因医疗程
序而出血的话应该怎么办?
1 是的,十分确定 2 是的,在某种程度上 3 否
20. 从这个医疗处所离开以后的任何时
候,您是否因为您的医疗程序而出
血?
1 是 2 否
21. 发生感染的可能迹象包括发烧、肿
胀、发热、流脓流液、发红等。在
您离开这个医疗处所之前,您的医
生或这个医疗处所的其他人是否给
您医嘱,告诉您如果出现感染迹象
时应该怎么办?
1 是的,十分确定 2 是的,在某种程度上 3 否
22. 从这个医疗处所离开后的任何时
候,您是否有过任何感染的迹象?
1 是 2 否
V. 您的总体经历
23. 请用下列0到10中任何一个数字评
价。 0 是最差医疗处所,10 是最佳
医疗处所。您认为那一个数字最能
代表您对此医疗处所的评价?
0 最差医疗处所
1
2
3
4
5
6
7
8
9
10 最佳医疗处所

Appendix D: Chinese: Mail Survey Cover Letters, December 2015 Mail Questionnaires, Instructions for Scannable Mail Questionnaire
Centers for Medicare & Medicaid Services D-7 Outpatient and Ambulatory Surgery CAHPS Survey Protocols and Guidelines Manual
24. 您是否会向您的朋友和家人推荐这
个医疗处所?
1 绝不会 2 也许不会 3 可能会 4 绝对会
VI. 关于您
25. 总体而言,您如何评价您的整体健
康状况?
1 极好 2 很好 3 好 4 一般 5 差
26. 总体而言,您如何评价您的整体精
神或情绪健康状况?
1 极好 2 很好 3 好 4 一般 5 差
27. 您的年龄多大?
1 18 to 24 2 25 to 34 3 35 to 44 4 45 to 54 5 55 to 64 6 65 to 74 7 75 to 79 8 80 to 84 9 85 岁以上
28. 您是男性还是女性?
1 男性 2 女性
29. 您已完成的最高级别或水平的年级
或院校是什么?
1 8年級或更低 2 读过高中﹐但未毕业 3 高中毕业或有同等学业文凭
(GED) 4 读过一些大学或二年制学位 5 四年制大学毕业 6 四年制大学毕业以上学历
30. 您是西班牙裔、西语族裔、或拉丁
裔吗?
1 是的,是西语族裔,拉丁裔,
西班牙裔 2 否, 不是西语族裔,拉丁裔,
西班牙裔
如回答否,请跳到#32
31. 以下哪个族裔最适合您?
1 墨西哥裔、墨西哥裔美國人、
美國出生的墨西哥裔人 2 波多黎各裔 3 古巴人 4 其他西班牙人、西裔、拉丁裔

Appendix D: Chinese: Mail Survey Cover Letters, Mail Questionnaires, Instructions for Scannable Mail Questionnaire December 2015
D-8 Centers for Medicare & Medicaid Services Outpatient and Ambulatory Surgery CAHPS Survey Protocols and Guidelines Manual
32. 您属于哪一种族?请选一个或一个
以上的回答。
1 白人 2 黑人或非裔美国人 3 美洲印第安人或阿拉斯加原住
民 4 亚洲人 5 华人 6 菲律宾人 7 日本人 8 韩国人 9 越南人 10 其他亚裔 11 夏威夷原住民 12 关岛或查莫罗人 13 萨摩亚人 14 其他太平洋岛国人
33. 您英文说得怎么样?
1 非常好 2 还好 3 不好 4 不会
34. 除了英文,您在家是否还说其他语
言?
1 是 2 否 如回答否,请跳到#36
35. 在家还说什么其他语言?
1 西班牙语 2 其他语言
(请说明):
_______________________
(请工整地填写)
36. 是否有人帮助您填写本调查问卷?
1 是 2 否 如果否, 跳到“问卷完”
37. 那人是如何帮助您的?勾选所有适
用项。
1 为我读问题 2 写下我给出的答案 3 替我回答问题 4 将问题译成我的语言 5 以其他方式帮助:
(解释一下):
______________________
(请用正楷填写) 6 没人帮助我填写本调查问卷
问卷完
Appendix D: Chinese: Mail Survey Cover Letters, December 2015 Mail Questionnaires, Instructions for Scannable Mail Questionnaire
Centers for Medicare & Medicaid Services D-9 Outpatient and Ambulatory Surgery CAHPS Survey Protocols and Guidelines Manual
(Alternative Instructions for Scannable Forms)
(可供扫描的表格填写说明)
2015
调查问卷说明
· 请用完全涂黑答案左侧的圆圈的方式,来回答所有问题。
· 有时会让您跳过某些问题。当出现这种情况时,您会看到一个箭头和一个说明,告诉
您下一步回答什么问题,像这样
是
否 如回答否,请跳到问题#1.
本问卷调查是关于您在我们这封信所特指的医院的经历。在本问卷调查中,“医疗程序”
这个词指的是诊断,外科手术及其他医疗过程。“医疗处所”这个词指的是进行您的医疗
程序的地方。
请针对印在信函上所列的的日子那天您所经历的所有医疗程序来回答这些问题。在您回
答问题时,请不要考虑或涉及其他医疗程序。

Appendix D: Chinese: Mail Survey Cover Letters, Mail Questionnaires, Instructions for Scannable Mail Questionnaire December 2015
D-10 Centers for Medicare & Medicaid Services Outpatient and Ambulatory Surgery CAHPS Survey Protocols and Guidelines Manual
This page intentionally left blank.

Centers for Medicare & Medicaid Services D-11 Outpatient and Ambulatory Surgery CAHPS Survey Protocols and Guidelines Manual
CHINESE (TRADITIONAL)

Appendix D: Chinese: Mail Survey Cover Letters, Mail Questionnaires, Instructions for Scannable Mail Questionnaire December 2015
D-12 Centers for Medicare & Medicaid Services Outpatient and Ambulatory Surgery CAHPS Survey Protocols and Guidelines Manual
This page intentionally left blank.

Appendix D: Chinese: Mail Survey Cover Letters, December 2015 Mail Questionnaires, Instructions for Scannable Mail Questionnaire
Centers for Medicare & Medicaid Services D-13 Outpatient and Ambulatory Surgery CAHPS Survey Protocols and Guidelines Manual
SAMPLE COVER LETTER FOR FIRST QUESTIONNAIRE MAILING
Outpatient and Ambulatory Surgery CAHPS Survey
To be Printed on Ambulatory Surgery Center or Hospital Outpatient Department or Vendor
Letterhead
«FirstName» «LastName»
«Address1» «Address2»
«City_Name», «State_Code» «Zip_Zip4»
尊敬的 «FirstName» <<LastName>>:
[FACILITY]想瞭解病人在我們的醫院得到的醫療服務的質量。 [VENDOR],一家獨立的
研究機構,幫助我們做這個問卷調查。 我們的記錄表明您在 [FACILITY] 做過手術或接
受過治療。 這個調查的結果,將幫助我們更好地理解病人在我們醫院的經歷。
隨附的調查問卷,將詢問在[DATE OF SURGERY]您對您的門診手術或醫療程序的意見。
我們請您花幾分鐘時間填寫此調查問卷,並用隨附的郵資已付的信封將其寄回給我們。
當您回答本調查問卷中的問題時,僅考慮您 [DATE OF SURGERY] 在 [FACILITY] 的經
歷。不要涉及您在我們醫院或其他醫院做其他手術或醫療程序的經歷。
您在此提供的所有資訊均將保密,並受到《隱私法》(Privacy Act) 保護。您對問卷的回答
將與其他調查研究參與者的回答一起匯總;當分析資料時,您的姓名和身份識別資訊不會
與您的回答關聯在一起。對[FACILITY NAME]和其他醫院調查的結果將於2017年在網上
公佈,網址是https://www.medicare.gov/ 。這些調查結果將幫助人們在選擇門診手術及非
住院手術的醫院時,做出知情的決定。 您的參與純屬自願,不會影響您的任何醫療福
利。
如果您對本調查研究有任何疑問,請撥打免費服務電話1-800-XXX-XXXX致電NAME。
如果您在閱讀問卷或回答問題方面需要幫助,請讓家人或朋友幫助您。感謝您的參與。
祝好!
NAME
Title
附件 [PRINT UNIQUE SAMPLE ID NUMBER HERE]
Appendix D: Chinese: Mail Survey Cover Letters, Mail Questionnaires, Instructions for Scannable Mail Questionnaire December 2015
D-14 Centers for Medicare & Medicaid Services Outpatient and Ambulatory Surgery CAHPS Survey Protocols and Guidelines Manual
SAMPLE COVER LETTER FOR SECOND QUESTIONNAIRE MAILING TO MAIL
SURVEY NONRESPONDENTS
Outpatient and Ambulatory Surgery CAHPS Survey
To be Printed on Ambulatory Surgery Center or Hospital Outpatient Department or Vendor
Letterhead
«FirstName» «LastName»
«Address1» «Address2»
«City_Name», «State_Code» «Zip_Zip4»
尊敬的 «FirstName»<<LastName>>:
最近,我們給您寄了一封信,請您幫助完成一項問卷調查,此問卷詢問您在[FACILITY]
接受門診手術或醫療程序時的該醫院的服務質量。迄今為止,我們尚未收到您填妥的調查
問卷。如果您已寄回調查問卷,我們不勝感激。 如果您尚未填寫該調查問卷,請現在就
花幾分鐘時間填寫。然後用隨附的郵資已付的信封將其寄回給我們。
當您回答本調查問卷中的問題時,僅考慮您 [DATE OF SURGERY] 在 [FACILITY] 的經
歷。不要涉及您在我們醫院或其他醫院,做其他手術或醫療程序的經歷。
您在此提供的所有資訊均將保密,並受到《隱私法》(Privacy Act) 保護。 您的參與純屬
自願,不會影響您的任何醫療福利。
如果您對該調查研究有任何疑問,請撥打免費服務電話1-800-XXX-XXXX致電NAME。
如果您在閱讀問卷或回答問題方面需要幫助,請讓家人或朋友幫助您。感謝您的參與。
祝好!
NAME
Title

Consumer Assessment of Healthcare Providers and Systems Outpatient and
Ambulatory Surgery Survey (OAS CAHPS)
A PATIENT EXPERIENCE OF CARE SURVEY ABOUT OUTPATIENT AND AMBULATORY SURGERIES
AND PROCEDURES
2016
消費者评估醫療服务機構和系統
門診手術及非住院手術問卷調查
(OAS CAHPS)
關於門诊、門診手术及其他非住院手術和醫療程序中病人經歷的問卷調查
2016年
根據1995年減少紙張使用法案,如果問卷上沒有有效的OMB控制數碼,任何人都無須回
答問卷上的任何問題。這項問卷持有有效的OMB控制數碼:0938-1240。完成這份問卷,
估計需要八分鐘。這包括閱讀問卷的說明,查找現有的資料,收集和整理所需的資訊,以
及完成和審閱所提供的資訊。如果您對完成這份問卷所估計的時間或對如何改進這項問卷
有任何看法,請寫信給: CMS, 7500 Security Boulevard, Attn: PRA Reports Clearance
Officer, Mail Stop C4-26-05, Baltimore, Maryland 21244-1850.

Appendix D: Chinese: Mail Survey Cover Letters, Mail Questionnaires, Instructions for Scannable Mail Questionnaire December 2015
D-16 Centers for Medicare & Medicaid Services Outpatient and Ambulatory Surgery CAHPS Survey Protocols and Guidelines Manual
SURVEY INSTRUCTIONS
請回答所有的問題。作答時,請在問題左
邊的方格內打勾。
有時問卷會要求您跳過一些問題。這種情
況發生時,您會看到箭頭並注明下一個該
回答的問題,如:
是
否 如回答否,請跳到#1.
本問卷調查是關於您在我們這封信所特指
的醫院的經歷。在本問卷調查中,“醫療
程序”這個詞指的是診斷,外科手術及其
他醫療過程。“醫療處所”這個詞指的是
進行您的醫療程序的地方。
請針對印在信函上所列的的日子那天您
所經歷的所有醫療程序來回答這些問題
。在您回答問題時,請不要考慮或涉及
其他醫療程序。
I.在您的醫療程序之前
最初的几个问题是关于为進行您的醫療程
序所做的准备的。这包括在医疗程序之前
和程序当天,您所收到的任何有關信息。
1. 在您的醫療程序之前,這個醫療處
所的醫生或者其他人是否給您關於
這個程式您所需要的所有資訊?
1 是的,十分確定
2 是的,在某種程度上
3 否
2. 在您的醫療程序之前,這個醫療處
所的醫生或者其他人是否給您讓您
容易理解的關於怎樣準備您的醫療
程序的醫囑?
1 是的,十分確定
2 是的,在某種程度上 3 否
II.关于这個醫療处所及其醫護人員
下面的问题,是有关您医疗程序當天的經
歷。
3. 辦理看病登記簽到手續的過程是否
順利流暢?
1 是的,十分確定
2 是的,在某種程度上
3 否
4. 這個醫療處所很乾淨嗎?
1 是的,十分確定
2 是的,在某種程度上
3 否
5. 這個醫療處所的工作人員和前臺接
待人員是否像您想像的那樣很有幫
助?
1 是的,十分確定
2 是的,在某種程度上 3 否

Appendix D: Chinese: Mail Survey Cover Letters, December 2015 Mail Questionnaires, Instructions for Scannable Mail Questionnaire
Centers for Medicare & Medicaid Services D-17 Outpatient and Ambulatory Surgery CAHPS Survey Protocols and Guidelines Manual
6. 這個醫療處所的工作人員和前臺接
待人員是否常以禮貌和尊重對待
您?
1 是的,十分確定
2 是的,在某種程度上 3 否
7. 醫生和護士是否常以禮貌和尊重對
待您?
1 是的,十分確定 2 是的,在某種程度上 3 否
8. 醫生和護士是否盡可能讓您感到舒
適?
1 是的,十分確定 2 是的,在某種程度上 3 否
III.關於您的醫療程序的溝通交流
注意:請包括您在該醫療程序之前和當天
所收到資訊。
9. 醫生和護士是否用您聽得懂的方式
來向您解釋醫療程序?
1 是的,十分確定 2 是的,在某種程度上 3 否
10. 麻醉會讓您在的醫療程序中感到困
倦或入睡。是否給您用了麻醉?
1 是
2 否 如回答否,請跳到#13
11. 醫生或這個醫療處所的其他人是否
用您聽得懂的方式來向您解釋麻醉?
1 是的,十分確定 2 是的,在某種程度上
3 否
12. 醫生或醫療處所的其他人是否用您
聽得懂的方式來向您解釋麻醉可能
產生的副作用?
1 是的,十分確定 2 是的,在某種程度上
3 否
13. 出院醫囑包括:醫療程序之後,有
可能出現的需要注意的症狀的說明,
服藥說明, 在家調養須知等等。在
您離開醫療處所之前,您是否得到
了書面的出院醫囑?
1 是 2 否
IV.您的術後恢復
14. 您的醫生或這個醫療處所的其他人
是否向您解釋您的恢復過程是怎樣
的?
1 是的,十分確定 2 是的,在某種程度上 3 否

Appendix D: Chinese: Mail Survey Cover Letters, Mail Questionnaires, Instructions for Scannable Mail Questionnaire December 2015
D-18 Centers for Medicare & Medicaid Services Outpatient and Ambulatory Surgery CAHPS Survey Protocols and Guidelines Manual
15. 止痛的方法有處方藥、非處方止疼
藥、或者冰袋等。您的醫生或這個
醫療處所的其他人是否給您醫囑,
告訴您如果您因醫療程序而產生疼
痛的話應該怎麼辦?
1 是的,十分確定 2 是的,在某種程度上 3 否
16. 從這個醫療處所離開後的任何時
候,您是否因為您的醫療程序而感
到疼痛?
1 是 2 否
17. 在您離開這個醫療處所之前,您的
醫生或這個醫療處所的其他人是否
給您醫囑,告訴您如果您噁心或是
嘔吐該怎麼辦?
1 是的,十分確定 2 是的,在某種程度上
3 否
18. 從這個醫療處所離開後的任何時
候,您是否因為您的醫療程序而感
到噁心或者嘔吐?
1 是
2 否
19. 在您離開這個醫療處所之前,您的
醫生或這個醫療處所的其他人是否
給您醫囑,告訴您如果您因醫療程
序而出血的話應該怎麼辦?
1 是的,十分確定 2 是的,在某種程度上 3 否
20. 從這個醫療處所離開後的任何時
候,您是否因為您的醫療程序而出
血?
1 是
2 否
21. 發生感染的可能跡象包括發燒、腫
脹、發熱、流膿流液、發紅等。在
您離開這個醫療處所之前,您的醫
生或這個醫療處所的其他人是否給
您醫囑,告訴您如果出現感染跡象
時應該怎麼辦?
1 是的,十分確定 2 是的,在某種程度上 3 否
22. 從這個醫療處所離開後的任何時
候,您是否有過任何感染的跡象?
1 是 2 否
V. 您的總體經歷
23. 請用下列0到10中任何一個數字評
價。 0 是最差醫療處所,10 是最佳
醫療處所。您認為那一個數字最能
代表您對此醫療處所的評價?
0 最差醫療處所
1
2
3
4
5
6
7
8
9
10 最佳醫療處所

Appendix D: Chinese: Mail Survey Cover Letters, December 2015 Mail Questionnaires, Instructions for Scannable Mail Questionnaire
Centers for Medicare & Medicaid Services D-19 Outpatient and Ambulatory Surgery CAHPS Survey Protocols and Guidelines Manual
24. 您是否會向您的朋友和家人推薦這
個醫療處所?
1 絕不會 2 也許不會 3 可能會 4 絕對會
VI. 關於您
25. 總體而言,您如何評價您的整體健
康狀況?
1 極好 2 很好
3 好 4 一般 5 差
26. 總體而言,您如何評價您的整體精
神或情緒健康狀況?
1 極好
2 很好 3 好 4 一般 5 差
27. 您的年齡多大?
1 18 to 24 2 25 to 34 3 35 to 44 4 45 to 54 5 55 to 64 6 65 to 74 7 75 to 79 8 80 to 84 9 85 歲以上
28. 您是男性還是女性?
1 男性
2 女性
29. 您已完成的最高級別或水準的年級
或院校是什麼?
1 8年級或更低 2 讀過高中﹐但未畢業 3 高中畢業或有同等學業文憑
(GED) 4 讀過一些大學或二年制學位 5 四年制大學畢業
6 四年制大學畢業以上學歷
30. 您是西班牙裔、西語族裔、或拉丁
裔嗎?
1 是的,是西語族裔,拉丁裔,
西班牙裔
2 否, 不是西語族裔,拉丁裔,
西班牙裔 如回答否,請跳到#32
31. 以下哪個族裔最適合您?
1 墨西哥裔、墨西哥裔美國人、
美國出生的墨西哥裔人 2 波多黎各裔 3 古巴人 4 其他西班牙人、西裔、拉丁裔

Appendix D: Chinese: Mail Survey Cover Letters, Mail Questionnaires, Instructions for Scannable Mail Questionnaire December 2015
D-20 Centers for Medicare & Medicaid Services Outpatient and Ambulatory Surgery CAHPS Survey Protocols and Guidelines Manual
32. 您屬於哪一種族?請選一個或一個
以上的回答。
1 白人 2 黑人或非裔美國人 3 美洲印第安人或阿拉斯加原住
民 4 亞洲人 5 華人
6 菲律賓人 7 日本人
8 韓國人 9 越南人 10 其他亞裔
11 夏威夷原住民 12 關島或查莫羅人 13 薩摩亞人 14 其他太平洋島國人
33. 您英文說得怎麼樣?
1 非常好 2 還好 3 不好
4 不會
34. 除了英文,您在家是否還說其他語
言?
1 是 2 否 如回答否,請跳到#36
35. 在家還說什麼語言?
1 西班牙語 2 其他語言
(請說明):
______________________
(請工整地填寫)
36. 是否有人幫助您填寫本調查問卷?
1 是
2 否 如果否, 跳到“問卷完”
37. 那人是如何幫助您的?勾選所有適
用項。
1 為我讀問題 2 寫下我給出的答案 3 替我回答問題
4 將問題譯成我的語言 5 以其他方式説明:
(解釋一下):
_______________________
(請用正楷填寫)
6 沒人幫助我填寫本調查問卷
問卷完

Centers for Medicare & Medicaid Services D-21 Outpatient and Ambulatory Surgery CAHPS Survey Protocols and Guidelines Manual
(Alternative Instructions for Scannable Forms)
(可供掃描的表格填寫說明)
调查问卷说明 · 請用完全塗黑答案左側的圓圈的方式,來回答所有問題。
· 有時會讓您跳過某些問題。當出現這種情況時,您會看到一個箭頭和一個說明,告訴
您下一步回答什麼問題,像這樣
是
否 如回答否,請跳到問題#1.
本問卷调查是关于您在我们这封信所特指的医院的经历。在本問卷调查中,“醫療程序”
這個詞指的是诊断,外科手术及其他醫療過程。“醫療處所”這個詞指的是进行您的医疗
程序的地方。
請針對印在信函上所列的的日子那天您所經歷的所有醫療程序來回答這些問題。在您回
答問題時,請不要考慮或涉及其他醫療程序。

Appendix D: Chinese: Mail Survey Cover Letters, Mail Questionnaires, Instructions for Scannable Mail Questionnaire December 2015
D-22 Centers for Medicare & Medicaid Services Outpatient and Ambulatory Surgery CAHPS Survey Protocols and Guidelines Manual
This page intentionally left blank.

Centers for Medicare & Medicaid Services Outpatient and Ambulatory Surgery CAHPS Survey Protocols and Guidelines Manual
APPENDIX E:
ADDITIONAL LANGUAGE COVER LETTERS AND QUESTIONNAIRE
(FORTHCOMING)

Appendix E: Additional Language Cover Letters and Questionnaire December 2015
Centers for Medicare & Medicaid Services Outpatient and Ambulatory Surgery CAHPS Survey Protocols and Guidelines Manual
This page intentionally left blank.

Centers for Medicare & Medicaid Services Outpatient and Ambulatory Surgery CAHPS Survey Protocols and Guidelines Manual
APPENDIX F:
CONSENT TO SHARE IDENTIFYING INFORMATION QUESTION

Appendix F: Consent to Share Identifying Information Question December 2015
Centers for Medicare & Medicaid Services Outpatient and Ambulatory Surgery CAHPS Survey Protocols and Guidelines Manual
This page intentionally left blank.

Centers for Medicare & Medicaid Services F-1 Outpatient and Ambulatory Surgery CAHPS Survey Protocols and Guidelines Manual
HOPDs or ASCs may request that their survey vendor provide survey responses linked to a
sample member’s name. If they wish to do so, they must ask for and receive consent from the
sample member using the Consent to Share Identifying Information question (below). This
question should be placed at the end of the questionnaire as the last question.
English Mail Questionnaire Version
The facility where you received your surgery or procedure may want to review your survey
responses so that they can decide how to address any concerns that you have.
Do you give your permission to link your name with your survey responses that will be
shared with the facility where you received your surgery or procedure?
4 Yes, I give my permission to link my name with my survey responses. 5 No, I do not give permission to link my name with my survey responses.
English Telephone Interview Version
The facility where you received your surgery or procedure may want to review your survey
responses so that they can decide how to address any concerns that you have.
Do you give your permission to link your name with your survey responses that will be
shared with the facility where you received your surgery or procedure?
1 Yes
2 No

Appendix F: Consent to Share Identifying Information Question December 2015
F-2 Centers for Medicare & Medicaid Services Outpatient and Ambulatory Surgery CAHPS Survey Protocols and Guidelines Manual
Spanish Mail Questionnaire Version
Es posible que el centro ambulatorio en donde se realizó su cirugía o procedimiento desee revisar
sus respuestas para encontrar la manera de aclarar sus preocupaciones.
¿Nos da usted permiso de asociar su nombre con las respuestas a la encuesta que se
compartirá con el centro ambulatorio en donde se realizó su cirugía o procedimiento?
1 Sí, doy permiso para asociar mi nombre con mis respuestas a la encuesta. 2 No, no doy permiso para asociar mi nombre con mis respuestas a la encuesta.
Spanish Telephone Interview Version
Es posible que el centro ambulatorio en donde se realizó su cirugía o procedimiento desee revisar
sus respuestas para encontrar la manera de aclarar sus preocupaciones.
¿Nos da usted permiso de asociar su nombre con las respuestas a la encuesta que se
compartirá con el centro ambulatorio en donde se realizó su cirugía o procedimiento?
1 Sí
2 No

December 2015 Appendix F: Consent to Share Identifying Information Question
Centers for Medicare & Medicaid Services F-3 Outpatient and Ambulatory Surgery CAHPS Survey Protocols and Guidelines Manual
Chinese (Simplified) Mail Questionnaire Version
为您做手术或进行医疗程序的机构可能希望了解您的回答,以便他们了解和解除您的顾虑。
您是否同意将您的姓名与您对此调查问卷的回答联系起来,并与此机构分享此信息?
1 是,我同意将我的姓名与我对此调查问卷的回答联系起来。
2 否,我不同意将我的姓名与我对此调查问卷的回答联系起来。
Chinese (Traditional) Mail Questionnaire Version
為您做手術或進行醫療程序的機構可能希望瞭解您的回答,以便他們了解和解除您的顧慮。
您是否同意將您的姓名與您對此調查問卷的回答聯繫起來,并與此機構分享此資訊?
1 是,我同意將我的姓名與我對此調查問卷的回答聯繫起來。
2 否,我不同意將我的姓名與我對此調查問卷的回答聯繫起來。
Appendix F: Consent to Share Identifying Information Question December 2015
F-4 Centers for Medicare & Medicaid Services Outpatient and Ambulatory Surgery CAHPS Survey Protocols and Guidelines Manual
This page intentionally left blank.

Centers for Medicare & Medicaid Services Outpatient and Ambulatory Surgery CAHPS Survey Protocols and Guidelines Manual
APPENDIX G:
OMB PAPERWORK REDUCTION ACT LANGUAGE

Appendix G: OMB Paperwork Reduction Act Language December 2015
Centers for Medicare & Medicaid Services Outpatient and Ambulatory Surgery CAHPS Survey Protocols and Guidelines Manual
This page intentionally left blank.

Centers for Medicare & Medicaid Services G-1 Outpatient and Ambulatory Surgery CAHPS Survey Protocols and Guidelines Manual
OMB PAPERWORK REDUCTION ACT LANGUAGE
The Office of Management and Budget (OMB) Paperwork Reduction Act language below must
be included in the Outpatient and Ambulatory Surgery CAHPS Survey mailings. It can be
included in the cover letter or on the front or back of the questionnaire. It does not need to be
included in both the cover letter and the questionnaire.
ENGLISH
According to the Paperwork Reduction Act of 1995, no persons are required to respond to a
collection of information unless it displays a valid OMB control number. The valid OMB control
number for this information collection is 0938-1240. The time required to complete this
information collection is estimated to average 8 minutes per response, including the time to
review instructions, search existing data resources, gather the data needed, and complete and
review the information collection. If you have comments concerning the accuracy of the time
estimate(s) or suggestions for improving this form, please write to: CMS, 7500 Security
Boulevard, Attn: PRA Reports Clearance Officer, Mail Stop C4-26-05, Baltimore, Maryland
21244-1850.

Appendix G: OMB Paperwork Reduction Act Language December 2015
G-2 Centers for Medicare & Medicaid Services Outpatient and Ambulatory Surgery CAHPS Survey Protocols and Guidelines Manual
OMB PAPERWORK REDUCTION ACT LANGUAGE
The Office of Management and Budget (OMB) Paperwork Reduction Act language below must
be included in the Outpatient and Ambulatory Surgery CAHPS Survey mailings. It can be
included in the cover letter or on the front or back of the questionnaire. It does not need to be
included in both the cover letter and the questionnaire.
SPANISH
De acuerdo a la Ley de Reducción de Trabajo Administrativo de 1995 (Paperwork Reduction
Act of 1995), ninguna persona tiene la obligación de responder a un cuestionario que solicite
información, a menos que lleve un número de control de OMB (Oficina de Administración y
Presupuesto) válido. El número de control OMB válido para este cuestionario es 0938-1240. Se
estima que el tiempo promedio necesario para completar este cuestionario es de 8 minutos por
respuesta, incluyendo el tiempo para revisar las instrucciones, buscar en las fuentes de datos
existentes, recopilar los datos necesarios, completar y revisar la información recopilada. Si tiene
algún comentario sobre la exactitud del tiempo estimado o sugerencias para mejorar este
formulario, por favor escriba a: CMS, 7500 Security Boulevard, Attn: PRA Reports Clearance
Officer, Mail Stop C4-26-05, Baltimore, Maryland 21244-1850.

December 2015 Appendix G: OMB Paperwork Reduction Act Language
Centers for Medicare & Medicaid Services G-3 Outpatient and Ambulatory Surgery CAHPS Survey Protocols and Guidelines Manual
OMB PAPERWORK REDUCTION ACT LANGUAGE
The Office of Management and Budget (OMB) Paperwork Reduction Act language below must
be included in the Outpatient and Ambulatory Surgery CAHPS Survey mailings. It can be
included in the cover letter or on the front or back of the questionnaire. It does not need to be
included in both the cover letter and the questionnaire.
CHINESE (SIMPLIFIED)
根据1995年减少纸张使用法案,如果问卷上没有有效的OMB控制数码,任何人都无须回
答问卷上的任何问题。这项问卷持有有效的OMB控制数码:0938-1240。完成这份问卷,估
计需要八分钟。这包括阅读问卷的说明,查找现有的资料,收集和整理所需的信息,以及
完成和审阅所提供的信息。如果您对完成这份问卷所估计的时间或对如何改进这项问卷有
任何看法,请写信给: CMS, 7500 Security Boulevard, Attn: PRA Reports Clearance Officer,
Mail Stop C4-26-05, Baltimore, Maryland 21244-1850.

Appendix G: OMB Paperwork Reduction Act Language December 2015
G-4 Centers for Medicare & Medicaid Services Outpatient and Ambulatory Surgery CAHPS Survey Protocols and Guidelines Manual
OMB PAPERWORK REDUCTION ACT LANGUAGE
The Office of Management and Budget (OMB) Paperwork Reduction Act language below must
be included in the Outpatient and Ambulatory Surgery CAHPS Survey mailings. It can be
included in the cover letter or on the front or back of the questionnaire. It does not need to be
included in both the cover letter and the questionnaire.
CHINESE (TRADITIONAL)
根據1995年減少紙張使用法案,如果問卷上沒有有效的OMB控制數碼,任何人都無須回
答問卷上的任何問題。這項問卷持有有效的OMB控制數碼:0938-1240。完成這份問卷,
估計需要八分鐘。這包括閱讀問卷的說明,查找現有的資料,收集和整理所需的資訊,以
及完成和審閱所提供的資訊。如果您對完成這份問卷所估計的時間或對如何改進這項問卷
有任何看法,請寫信給:CMS,7500 Security Boulevard, Attn: PRA Reports Clearance Officer,
Mail Stop C4-26-05, Baltimore, Maryland 21244-1850.

Centers for Medicare & Medicaid Services Outpatient and Ambulatory Surgery CAHPS Survey Protocols and Guidelines Manual
APPENDIX H:
FREQUENTLY ASKED QUESTIONS FOR TELEPHONE INTERVIEWERS
(ENGLISH)

Appendix H: Frequently Asked Questions for Telephone Interviewers (English) December 2015
Centers for Medicare & Medicaid Services Outpatient and Ambulatory Surgery CAHPS Survey Protocols and Guidelines Manual
This page intentionally left blank.
Centers for Medicare & Medicaid Services H-1 Outpatient and Ambulatory Surgery CAHPS Survey Protocols and Guidelines Manual
FREQUENTLY ASKED QUESTIONS
OAS CAHPS®
What is the purpose of this survey?
The purpose of this survey is to learn about your experiences with the care you received for your
recent outpatient surgery or procedure. The survey results will help other patients make more
informed choices when choosing an outpatient surgery facility and help facilities in the study to
improve the quality of care provided to their patients.
I’ve already completed a mail survey. Do I need to complete this survey again?
Thank you for completing the survey and mailing it back in. However, we have not yet received
the survey and so we are following up to gather your feedback by phone. If you have some time
right now we could go through the questions. Or I can call you back in a few days if we still
have not received the survey by mail.
I lost the mail survey. Would you please mail me another one?
We are nearing the end of the survey data collection period and are not allowed to send out any
additional surveys. Because the feedback you provide will help improve the quality of the
outpatient surgery care you and others like you receive, we are asking that you please complete
the survey with us over the phone. If now is okay, let’s get started!
I already completed/received a survey about this.
Sometimes hospitals and surgeons conduct surveys of their recent patients, and you may have
received one of those surveys. The survey we are asking you to do is about your experience at
the outpatient facility where your surgery or procedure was performed. The results will be used
to help people make more informed decisions when choosing an outpatient surgery facility. The
facilities will also use survey results to help improve the quality of care they give to their
patients.
How are the results from the study going to be used?
Results from this survey will be used to help people make more informed decisions when
choosing an outpatient surgery facility. The facilities will also use survey results to help improve
the quality of care they give to their patients.
Do I have to take part in this survey?
Your participation in this survey is voluntary. All information that you give in this survey will
be held in confidence and is protected by the Privacy Act. Please know that none of your
individual answers will be shared with [FACILITY NAME], nor will they know whether or not
you participated.
Appendix H: Frequently Asked Questions for Telephone Interviewers (English) December 2015
H-2 Centers for Medicare & Medicaid Services Outpatient and Ambulatory Surgery CAHPS Survey Protocols and Guidelines Manual
It is also important that you know that your decision to participate in this survey and your
answers to the questions will not affect any health care benefits you receive now or expect to
receive in the future.
You can also skip or refuse to answer any question you don’t feel comfortable with. But, we
hope you will participate because the feedback you provide will help improve the quality of the
care you, and others like you, receive.
I did not have surgery. This survey does not apply to me.
This survey is applicable to you if you had a medical or diagnostic procedure at [FACILITY
NAME] in [MONTH, YEAR]. Examples of these types of procedures include colonoscopy,
endoscopy, biopsy and injection for pain management. [NOTE: IF NEEDED, EXPLAIN TO
RESPONDENT HOW THEY WERE SELECTED: You were randomly selected to participate
in this survey because our records show that you had a procedure at (FACILITY NAME).]
I can’t remember any specific procedure/I didn’t have surgery on that date.
For privacy reasons, we do not have access to the procedures you had at this facility during
[MONTH]. Please try to answer the questions as best as you can for the procedure you
remember the most in [MONTH].
My surgery was not outpatient/ambulatory because I stayed overnight at the hospital/facility. This survey does not apply to me.
This survey is for people who had outpatient surgeries, including those who went home on the
same day and those who stayed overnight for observation. As long as you went home after
observation and a doctor did not write an order to admit you to a hospital as an inpatient, then
this survey is for you.
What do I have to do/What kinds of questions are there?
I would like to ask you some questions about your experiences with your recent outpatient
surgery or procedure at [FACILITY NAME]. For example, the questions will ask for your
experience with the check-in process, the facility itself, the communication you had with the
facility’s staff, the information you received on your procedure, and your overall experience.
This survey takes on average about 8 minutes to complete, and I will move through the questions
as quickly as possible.
Is it okay for RESPONDENT’S wife, husband, child, legal guardian, etc.) to answer these questions?
Because you were chosen at random to participate in this important study, and because you were
the one who received care for an outpatient surgery or procedure, no other person can take your
place. But, you may skip or refuse to answer any question you’re uncomfortable with.

December 2015 Appendix H: Frequently Asked Questions for Telephone Interviewers (English)
Centers for Medicare & Medicaid Services H-3 Outpatient and Ambulatory Surgery CAHPS Survey Protocols and Guidelines Manual
How do I know this is confidential?
Your individual answers will only be seen by research staff, who have signed statements of
confidentiality. All personal identifying information, such as names and addresses, will be
removed from data records before they are analyzed. And, everyone’s answers will be combined
to produce a summary report.
Why do you want to know all this personal stuff about me (RACE, AGE, GENERAL HEALTH, etc.) if this is a survey about my outpatient surgery care experiences?
I understand your concern with the questions about your general health and background. We
have found that people’s experiences may differ based on their current health status and other
characteristics. This is a very important survey. If a question bothers you, just tell me you’d
rather not answer it, and I’ll move on to the next question.
I’m on the Do Not Call list. Why are you calling me?
The Do Not Call list stops sales and telemarketing calls. We are conducting survey research on
behalf of [FACILITY NAME]. We are not calling to sell or market a product or service.
I’m not going to answer a lot of questions over the phone!
Your cooperation is very important to us. The information that you provide in this survey will
help others make more informed choices about an outpatient surgery center and will help the
facility you visited to improve the care they give. Please know that you can skip or refuse to
answer any question you don’t feel comfortable with, and that all of your answers will be kept
completely confidential since they are protected by the Federal Privacy Act of 1974. Let me
start and you can see what the questions are like…[READ FIRST QUESTION]
How did you get my name? How was I chosen for the survey?
Your name was randomly selected from a list of patients at [FACILITY NAME] who received an
outpatient surgery or procedure in [MONTH].
I did not like my outpatient surgery center!
I understand. Your opinions are very important and will help your outpatient surgery center
understand how to improve its care. Let’s start now. [NOTE: DO NOT ARGUE BACK.
MAKE SHORT, NEUTRAL COMMENTS TO LET THEM KNOW THAT YOU ARE
LISTENING AND IMMEDIATELY ASK THE FIRST QUESTION.]
How long will this take?
This survey takes on average about 8 minutes to complete. I’ll move through the questions as
quickly as possible.

Appendix H: Frequently Asked Questions for Telephone Interviewers (English) December 2015
H-4 Centers for Medicare & Medicaid Services Outpatient and Ambulatory Surgery CAHPS Survey Protocols and Guidelines Manual
This page intentionally left blank.

Centers for Medicare & Medicaid Services Outpatient and Ambulatory Surgery CAHPS Survey Protocols and Guidelines Manual
APPENDIX I:
GENERAL GUIDELINES FOR TELEPHONE INTERVIEWERS

Appendix I: General Guidelines for Telephone Interviewers December 2015
Centers for Medicare & Medicaid Services Outpatient and Ambulatory Surgery CAHPS Survey Protocols and Guidelines Manual
This page intentionally left blank.

Centers for Medicare & Medicaid Services I-1 Outpatient and Ambulatory Surgery CAHPS Survey Protocols and Guidelines Manual
OUTPATIENT AND AMBULATORY SURGERY CAHPS SURVEY
GENERAL GUIDELINES FOR TELEPHONE INTERVIEWING
Overview
The Outpatient and Ambulatory Surgery (OAS) CAHPS Survey will be administered as an
electronic system telephone interview. As a telephone interviewer on the OAS CAHPS, you will
use the system to conduct each interview. The questions you ask are programmed into a
computer. The phone number is provided by the computer for you to make the call. You will
read the questions from the computer screen and enter the answer to each question into the
computer. Based on the answer you enter, the computer will automatically take you to a screen
with the next applicable question.
You play an extremely important role in the overall success of this study. You are the link to the
hundreds of respondents who will provide valuable information to the project team. You are the
person who develops rapport with the respondents, assures them that their participation is
important, and obtains their full cooperation and informed consent.
As a professional interviewer, your job is to help each respondent feel at ease and comfortable
with the interview. Key to accomplishing this goal is to be fully informed about the survey, the
interview, and the data collection procedures.
General Interviewing Techniques
The process of asking questions, probing, and entering responses correctly is crucial to obtaining
high-quality data for the OAS CAHPS Survey. General techniques and procedures you should
follow when conducting the OAS CAHPS Survey interviews are provided below.
Administering Survey Questions
• Ask the questions exactly as they are presented. Do not change the wording or condense any
question when reading it to the respondent.
• Emphasize all words or phrases that appear in bold, are underlined, or appear in italics.
• Ask every question specified, even when a respondent has seemingly provided the answer as
part of the response to a preceding question. The answer received in the context of one
question may not be the same answer that will be received when the other question is asked.
If it becomes cumbersome to the respondent, remind him or her gently that you must ask all
questions of all respondents.
• If the answer to a question indicates that the respondent did not understand the intent of the
question, or if the respondent requests that any part of the question be clarified, even if it is
only one word, repeat the question.

Appendix I: General Guidelines for Telephone Interviewers December 2015
I-2 Centers for Medicare & Medicaid Services Outpatient and Ambulatory Surgery CAHPS Survey Protocols and Guidelines Manual
• Read the questions slowly, at a pace that allows them to be readily understood. Remember
that the respondent has not heard these questions before and will not have had the exposure
that you have had to the questionnaire.
• Transition statements are designed to inform the respondent of the nature of an upcoming
question or a series of questions, to define a word, or to describe what is being asked for in
the question. Read transition statements just as they are presented. Don’t create “transition
statements” of your own, because these may unintentionally introduce bias into the interview.
• Give the respondent plenty of time to recall past events.
• Do not suggest answers to the respondent. Your job as an interviewer is to read the questions
exactly as they are printed, make sure the respondent understands the question, and then enter
the responses. Do not help the respondent answer the questions.
• Ask questions in the exact order in which they are presented.
• Do not read words that appear in ALL CAPITAL LETTERS to the respondent. This
includes both questions and response categories.
• Read all questions including those which may appear to be sensitive to the respondent in the
same manner with no hesitation or change in inflection.
• Thoroughly familiarize yourself with the Frequently Asked Questions list before you conduct
interviews so that you are knowledgeable about the OAS CAHPS Survey.
• At the end of the interview, tell the sample member that the survey is completed and thank
him or her for taking part in the survey.
Introducing the Survey
The introduction is of the utmost importance to successfully completing a telephone interview.
Most people hang up in the first few minutes of the interview, so if you can convince the
respondent to remain on the line long enough to hear the purpose of the study and begin asking
the questions, the chances that your respondent will complete the interview increase
dramatically.
• When reading the introduction, sound confident and pronounce the words as clearly as you
can.
• Respondents are typically not expecting survey research calls, so they may need your help to
clarify the nature of the call.

December 2015 Appendix I: General Guidelines for Telephone Interviewers
Centers for Medicare & Medicaid Services I-3 Outpatient and Ambulatory Surgery CAHPS Survey Protocols and Guidelines Manual
• Practice the introduction until you can present it in such a manner that your presentation
sounds confident, sincere, and natural.
• Deliver the introduction at a conversational pace. Rushing through the introduction gives an
impression of lack of confidence and may also cause the listener to misunderstand.
• Try not to pause too long before asking the first question in the survey following the
introduction. A pause tends to indicate that you are waiting for approval to continue.
Avoiding Refusals
The first and most critical step in avoiding refusals is your effort to establish rapport with
reluctant sample members, therefore minimizing the incidence of refusals. Remember, you will
not be able to call back and convert a refusal―your initial contact with the sample member is the
only chance you will have to create a successful interview. The following are some tips to
follow to avoid refusals.
• Make sure you are mentally prepared when you start each call, and have a positive attitude.
• Treat respondents the way you would like to be treated.
• Always use an effective/positive/friendly tone and maintain a professional outlook.
• Pay careful attention to what the respondent says during the interview.
• Listen to the respondent completely rather than assuming you know what he or she is
objecting to.
• Listen before evaluating and entering a response code.
• Be accommodating to the respondents’ needs.
• Always remain in control of the interaction.
• Understand the reason for reluctance/refusal at the start of the call, or figure it out as quickly
as possible.
• Listen as an ally, not an adversary, and do not debate or argue with the respondent.
• Be prepared to address one (or more) reason(s) for reluctance/refusal.
• Focus your comments to sample members on why they specifically are important to the
study.
• Paraphrase what you hear and repeat this back to the respondent.
• Remember that you are a professional representative of your survey organization and the
health care facility whose patients you are contacting.
Appendix I: General Guidelines for Telephone Interviewers December 2015
I-4 Centers for Medicare & Medicaid Services Outpatient and Ambulatory Surgery CAHPS Survey Protocols and Guidelines Manual
General Interviewing Guidance
The following sections provide guidance on the use of probes, avoiding bias, and entering
responses accurately. By following these rules, interviewers will help ensure that the OAS
CAHPS Survey interviews are conducted in a standardized manner.
Probing
At times, it will be necessary for you to probe to obtain a more complete or more specific answer
from a respondent. To elicit an acceptable response, you will often need to use an appropriate
neutral or nondirective probe. The important thing to remember is not to suggest answers or lead
the respondent. Some general rules for probing follow:
• Repeat the question if the respondent misunderstood or misinterpreted the question. After
hearing the question the second time, the respondent will probably understand what
information is expected.
• Use a silent probe, which is pausing or hesitating to indicate to the respondent that you need
additional or better information. This is a good probe to use after you have determined the
respondent’s response pattern.
• Use neutral questions or statements to encourage a respondent to elaborate on an inadequate
response. Examples of neutral probes include the following: “What do you mean?” “How
do you mean?” “Tell me what you have in mind.” “Tell me more about….”
• Use clarification probes when the response is unclear, ambiguous, or contradictory. Be
careful not to appear to challenge the respondent when clarifying a statement and always use
a neutral probe. Examples of clarification probes are “Can you give me an example?” or
“Could you be more specific?”
• Encourage the respondent to give his or her best guess if a respondent gives a “don’t know”
response. Let the respondent know that this is not a test and there are no right or wrong
answers. We are interested in the respondent’s opinions and assessment of the care that he or
she has received at their ambulatory surgery center or hospital outpatient department.
• If the respondent asks you to answer the question for him or her, let the respondent know that
you cannot. Instead, ask the respondent if she or he requires clarification on the content or
meaning of the question.
Avoiding Bias
One common pitfall of interviewing is unknowingly introducing bias into an interview. Bias
occurs when an interviewer says or does something that affects the answers respondents give in

December 2015 Appendix I: General Guidelines for Telephone Interviewers
Centers for Medicare & Medicaid Services I-5 Outpatient and Ambulatory Surgery CAHPS Survey Protocols and Guidelines Manual
an interview. An interview that has significant bias will not provide accurate data for the
research being conducted; such an interview may have to be thrown out.
As a professional interviewer, remaining neutral at all times ensures that bias is not introduced
into the interview. There are many things you can do or avoid to help ensure that no bias is
introduced. You should
• read all statements and questions exactly as they are written,
• use neutral probes that do not suggest answers,
• not provide your own personal opinions or answers in an effort to “help” respondents, and
• not use nonverbal language, such as a cough, pause or a yawn to influence the interview.
Taking these steps to monitor your own spoken and unspoken language will go a long way to
guarantee that the interviews you conduct are completed correctly and efficiently.
Entering Responses
The majority of the questions you will ask have precoded responses. To enter a response for
these types of questions, you will simply select the appropriate response option and enter the
number corresponding to that response.
The conventions presented below must be followed at all times to ensure that the responses you
enter accurately reflect the respondents’ answers and to ensure that questionnaire data are all
collected in the same systematic manner.
• You must listen to what the respondent says and enter the appropriate answer if the response
satisfies the objective of the question. If the answer does not appear to satisfy the objective,
repeat the question.
• In entering answers to open-ended questions or “Other (specify)” categories, enter the
response verbatim, exactly as it was given by the respondent.
• Enter the response immediately after it is given.
• If a respondent gives a range in response to a question, probe as appropriate for a more
specific answer. For example, if a respondent says, “Oh, 2 or 3 times” and you can enter
only one number, ask for clarification: “Would that be closer to 2 or to 3?”
Rules for Successful Telephone Interviewing
Remember, the key to successful interviewing is being prepared for every contact that you make.
Have a complete set of the appropriate materials at your work station, organized in such a

Appendix I: General Guidelines for Telephone Interviewers December 2015
I-6 Centers for Medicare & Medicaid Services Outpatient and Ambulatory Surgery CAHPS Survey Protocols and Guidelines Manual
manner that you do not have to stop and search for required documents. Some general rules that
you should follow every time you place a call are provided below.
1. Be prepared before you place a call. Be prepared to talk to the sample member. You should
be able to explain the purpose of your call to the sample member or his or her family and
friends. Do not rely on your memory alone to answer questions. Make sure you review and
understand the Frequently Asked Questions (FAQs).
2. Act professionally. Convey to sample members that you are a professional who specializes
in asking questions and conducting interviews. As a professional interviewer, you have
specific tasks to accomplish for this survey.
3. Make the most of your contact. Even though you may not be able to obtain an interview on
this call, it is important to make the most of the contact to aid in future attempts. For
example, if you are trying to contact the sample member and he or she is not available, gain
as much information as you can to help reach the sample member the next time he or she is
called. Important questions to ask:
◦ When is the sample member usually home?
◦ What is the best time to reach the sample member?
◦ Can you schedule an “appointment” to reach the sample member at a later time?
4. Don’t be too quick to code a sample member as incapable. Some sample members may be
hard of hearing or appear not to fully understand you when you call. Rather than
immediately coding these cases as “Incapable,” please attempt to set a call-back for a
different time of day and different day of the week. It is possible that reaching the sample
member at a different time may result in your being able to conduct the interview with him or
her. It is also possible that a friend or family member can assist the sample member with the
interview. You cannot allow them to proxy for the sample member, but you can allow them
to provide general help.

Centers for Medicare & Medicaid Services Outpatient and Ambulatory Surgery CAHPS Survey Protocols and Guidelines Manual
APPENDIX J:
FREQUENTLY ASKED QUESTIONS FOR TELEPHONE INTERVIEWS
(SPANISH)
Preguntas más frecuentes para entrevistas por teléfono

Appendix J: Frequently Asked Questions for Telephone Interviews (Spanish) December 2015
Centers for Medicare & Medicaid Services Outpatient and Ambulatory Surgery CAHPS Survey Protocols and Guidelines Manual
This page intentionally left blank.

Centers for Medicare & Medicaid Services J-1 Outpatient and Ambulatory Surgery CAHPS Survey Protocols and Guidelines Manual
PREGUNTAS MÁS FRECUENTES
OAS CAHPS®
¿Cuál es el propósito de esta encuesta?
El objetivo de la encuesta es aprender sobre sus experiencias con los servicios que recibió
durante su más reciente cirugía externa o procedimiento ambulatorio. Los resultados de la
encuesta ayudarán a otros pacientes a tomar decisiones más informadas al seleccionar un centro
de cirugía ambulatoria así como para ayudar a los centros que participan en el estudio a mejorar
la calidad de la atención que proporcionan a sus pacientes.
Ya completé una encuesta por correo. ¿Tengo que completar esta encuesta otra vez?
Muchas gracias por completar la encuesta y enviarla por correo. Sin embargo, aún no hemos
recibido la encuesta, y estamos dándole seguimiento para obtener sus comentarios por teléfono.
Si tiene tiempo en este momento puedo hacerle las preguntas. O le puedo volver a llamar en
unos días si aún no hemos recibido la encuesta por correo.
Perdí la encuesta que se envía por correo. ¿Me puede enviar otra por correo?
Estamos cerca del final del periodo de recolección de datos y no nos permiten enviar ninguna
encuesta adicional. Como las opiniones que usted proporcione nos ayudarán a mejorar la calidad
de la atención de pacientes de cirugía externa o ambulatoria que usted y otras personas reciben,
le estamos pidiendo que por favor complete la encuesta con nosotros por teléfono. Si este es un
buen momento, ¡comencemos!
Ya completé/recibí una encuesta como esa.
A veces los hospitales y los cirujanos llevan a cabo encuestas de sus pacientes recientes y usted
pudiera haber recibido una de esas encuestas. La encuesta que le estamos pidiendo que haga es
sobre su experiencia en la instalación de cirugía externa en donde le realizaron la cirugía o
procedimiento. Los resultados se utilizarán para ayudar a las personas a tomar decisiones más
informadas cuando eligen un centro para cirugía externa o ambulatoria. Los centros también van
a utilizar la encuesta para ayudar a mejorar la calidad de los servicios que dan a sus pacientes.
¿Cómo se utilizarán los resultados del estudio?
Los resultados de esta encuesta se usarán para ayudar a las personas a tomar decisiones más
informadas cuando eligen un centro para cirugía externa o ambulatoria. Los centros también van
a utilizar la encuesta para ayudar a mejorar la calidad de los servicios que dan a sus pacientes.

Appendix J: Frequently Asked Questions for Telephone Interviews (Spanish) December 2015
J-2 Centers for Medicare & Medicaid Services Outpatient and Ambulatory Surgery CAHPS Survey Protocols and Guidelines Manual
¿Tengo que participar en esta encuesta?
Su participación en esta encuesta es voluntaria. Toda la información que usted proporcione en
esta encuesta se mantendrá confidencial y está protegida por la Ley de privacidad. Deseamos
que sepa que ninguna de sus respuestas individuales se compartirán con [FACILITY NAME], ni
sabrán si usted participó o no.
También es importante que sepa que su decisión de participar en esta encuesta y sus respuestas a
las preguntas no afectarán a ningún beneficio de atención médica que usted reciba ahora o que
espere recibir en el futuro.
También se puede saltar o rehusar contestar cualquier pregunta que le moleste. Sin embargo,
esperamos que participe porque los comentarios que usted nos dé nos ayudarán a mejorar la
calidad de los servicios que recibe usted y otras personas como usted.
No tuve una cirugía. Esta encuesta no me corresponde.
Esta encuesta sí le corresponde si le realizaron un procedimiento médico o de diagnóstico en
[FACILITY NAME] en [MES, AÑO]. Ejemplos de este tipo de procedimientos incluyen:
colonoscopía, endoscopía, biopsia e inyección para control del dolor. [NOTE: IF NEEDED,
EXPLAIN TO RESPONDENT HOW THEY WERE SELECTED: Usted fue seleccionado al
azar para participar en esta encuesta porque nuestros registros indican que le realizaron un
procedimiento en (FACILITY NAME).]
No recuerdo ningún procedimiento/No tuve una cirugía en esa fecha.
Por razones de privacidad, no tenemos acceso a los procedimientos que le realizaron a usted en
ese centro durante [MES]. Por favor trate de responder a las preguntas lo mejor que pueda para
el procedimiento que mejor recuerde en [MES].
Mi cirugía no fue como paciente externo/ambulatorio porque me tuve que quedar una noche en el hospital/centro. Esta encuesta no me aplica.
Esta encuesta es para personas que tuvieron cirugía como pacientes externos, incluyendo a las
personas que se fueron a casa el mismo día y los que se quedaron una noche para observación.
Siempre y cuando se fuera a su casa después del periodo de observación y un doctor no le haya
ordenado que se le admitiera en un hospital como paciente interno, entonces esto es para usted.
¿Qué tengo que hacer/Qué tipos de preguntas son?
Me gustaría hacerle algunas preguntas sobre sus experiencias con su reciente cirugía externa o
procedimiento ambulatorio en [FACILITY NAME]. Por ejemplo, las preguntas le pedirán sus
experiencias con el proceso de registro, el centro de cirugía en sí, la comunicación que tuvo con
el personal del centro de cirugía, la información que recibió sobre su procedimiento y su
December 2015 Appendix J: Frequently Asked Questions for Telephone Interviews (Spanish)
Centers for Medicare & Medicaid Services J-3 Outpatient and Ambulatory Surgery CAHPS Survey Protocols and Guidelines Manual
experiencia en general. En promedio, esta encuesta se puede completar en unos 10 minutos y
voy a avanzar con las preguntas tan rápido como sea posible.
¿Es posible que (la esposa, el esposo, el hijo, el tutor legal, etc.) responda a estas preguntas?
Como usted fue seleccionado(a) al azar para participar en este importante estudio y como usted
fue la persona que recibió la atención médica para la cirugía externa o procedimiento
ambulatorio, ninguna otra persona puede tomar su lugar. Pero se puede saltar o rehusar contestar
cualquier pregunta que le moleste.
¿Cómo sé que esto es confidencial?
Las respuestas que usted dé solo serán vistas por el personal del estudio, quienes han firmado
declaraciones de confidencialidad. Toda la información de identidad, como los nombres y las
direcciones, serán separados de los registros de datos antes de ser analizados. Y, las respuestas
de todas las personas se combinarán para generar un reporte de resumen.
¿Por qué desea saber todos esos datos personales acerca de mi (SALUD, RAZA, EDAD, etc.) si esta encuesta es acerca de mis experiencias sobre la atención médica durante mi cirugía externa o ambulatoria?
Entiendo su preocupación sobre las preguntas sobre su salud en general y antecedentes. Hemos
encontrado que las experiencias de las personas pueden variar de acuerdo al estado salud y otras
características. Esta es una encuesta muy importante. Si le molesta alguna pregunta, solo
dígame que no desea responderla y avanzaré a la siguiente pregunta.
Estoy en la lista de no llamar. ¿Por qué me están llamando?
La lista de No llamar previene las llamadas de ventas y telemercadeo. Estamos llevando a cabo
el estudio de encuesta a nombre de [FACILITY NAME]. No le estamos llamando para vender o
promover un producto o servicio.
¡No voy a responder a tantas preguntas por teléfono!
Su cooperación es muy importante para nosotros. La información que usted proporcione en esta
encuesta ayudará a otras personas a tomar decisiones más informadas sobre un centro de cirugía
externo o ambulatorio y ayudará al centro de cirugía, a mejorar sus servicios. Por favor tenga en
cuenta que se puede saltar o negar a contestar cualquier pregunta que le moleste y que sus
respuestas se mantendrán completamente confidenciales porque están protegidas por la ley
federal de privacidad de 1974. Empecemos y usted podrá ver cómo son las preguntas…[READ
FIRST QUESTION]

Appendix J: Frequently Asked Questions for Telephone Interviews (Spanish) December 2015
J-4 Centers for Medicare & Medicaid Services Outpatient and Ambulatory Surgery CAHPS Survey Protocols and Guidelines Manual
¿Cómo obtuvo mi nombre? ¿Cómo me seleccionaron para la encuesta?
Su nombre se seleccionado al azar de una lista de pacientes en [FACILITY NAME] que tuvieron
una cirugía externa o procedimiento ambulatorio durante el mes de [MES].
¡No me agradó el centro de cirugía externa/ambulatoria!
Le entiendo. Sus opiniones son muy importantes y ayudarán a su centro de cirugía
externa/ambulatoria a entender como mejorar sus servicios. Comencemos. [NOTE: DO NOT
ARGUE BACK. MAKE SHORT, NEUTRAL COMMENTS TO LET THEM KNOW THAT
YOU ARE LISTENING AND IMMEDIATELY ASK THE FIRST QUESTION.]
¿Cuánto tiempo va a tomar?
En promedio esta encuesta se puede completar como en 8 minutos. Trataré de hacer las
preguntas tan rápido como me sea posible.

Centers for Medicare & Medicaid Services Outpatient and Ambulatory Surgery CAHPS Survey Protocols and Guidelines Manual
APPENDIX K:
XML DATA FILE LAYOUT FOR STANDARD HEADER RECORD

Appendix K: XML Data File Layout for Standard Header Record December 2015
Centers for Medicare & Medicaid Services Outpatient and Ambulatory Surgery CAHPS Survey Protocols and Guidelines Manual
This page intentionally left blank.

Cen
ters
for M
ed
ica
re &
Med
icaid
Se
rvic
es
K
-1
Ou
tpatie
nt a
nd
Am
bu
lato
ry S
urg
ery
CA
HP
S S
urv
ey P
roto
co
ls a
nd
Gu
ide
lines M
an
ual
STANDARD XML DATA FILE LAYOUT
OUTPATIENT AND AMBULATORY CAHPS SURVEY
STANDARD HEADER RECORD
The following section defines the format of the header record.
NOTE: Each element must have a closing tag that is the same as the opening tag but with a forward slash. Data element names do not contain
any spaces, underscores, or capital letters.
XML Element Description Valid Values Data Type Field
Size
Data
Element
Required
Type of Header Record
headertype
This header element should only occur once
per file.
Example: headertype 1 /headertype
Type of Header Record 1 = Standard Header
Record
Numeric 1 Yes
Provider Name
<providername
This header element should only occur once
per file.
Example: providername
SampleHOPDASCName / providername
This is the HOPD’s or ASC’s
Provider Name
— Alphanumeric 100 Yes
Provider Number
providernum
This header element will occur again as an
administrative data element in the patient level
data record.
Example: providernum 123456 /
providernum
This is the HOPD’s or ASC’s
CMS Certification Number
(CCN, formerly known as the
Medicare Provider ID Number)
No Dashes or spaces
Valid 6- or 10-digit CMS
Certification Number
(CCN)
Alphanumeric 10 Yes

Ap
pen
dix
K: X
ML
Data
File
Layo
ut fo
r Sta
nd
ard
He
ad
er R
eco
rd
Decem
ber 2
01
5
K-2
C
en
ters
for M
ed
ica
re &
Med
icaid
Se
rvic
es
Ou
tpatie
nt a
nd
Am
bu
lato
ry S
urg
ery
CA
HP
S S
urv
ey P
roto
co
ls a
nd
Gu
ide
lines M
an
ual
XML Element Description Valid Values Data Type Field
Size
Data
Element
Required
Sample Month
samplemonth This header element will occur again as an
administrative data element in the patient level
data record.
Example: samplemonth 12 /
samplemonth
Survey vendors will select a
sample of patients who meet
survey eligibility criteria for each
calendar month. The Sample
Month is the month for which the
sample was selected.
MM
(1 – 12 = January –
December)
Numeric 2 Yes
Sample Year
sampleyear This header element will occur again as an
administrative data element in the patient level
data record.
Example: sampleyear 2016 /
sampleyear
This is the calendar year in which
the survey is conducted.
YYYY
(2016 or greater)
Numeric 4 Yes
Survey Mode
surveymode
This header element will occur again as an
administrative data element in the patient level
data record.
Example: surveymode 1 / surveymode
The survey mode, either mail
only, phone only, or mixed mode,
must be the same for all sample
members in each sample month in
the calendar quarter for all of the
HOPD or ASC locations under
the same CCN.
1 = Mail only
2 = Telephone only
3 = Mixed mode
Numeric 1 Yes
Type of Sampling
sampletype
This header element should only occur once
per file.
Example: sampletype 1 /sampletype
Type of sampling used. Note:
Sample Type must be the same
for all three months in each
quarter.
1 = Census
2 = Simple random
sampling
3 = Stratified systematic
sampling
4 = Proportionate
Stratified Random
sampling
Numeric 1 Yes

Decem
ber 2
01
5
Ap
pen
dix
K: X
ML
Data
File
Layo
ut fo
r Sta
nd
ard
He
ad
er R
eco
rd
Cen
ters
for M
ed
ica
re &
Med
icaid
Se
rvic
es
K
-3
Ou
tpatie
nt a
nd
Am
bu
lato
ry S
urg
ery
CA
HP
S S
urv
ey P
roto
co
ls a
nd
Gu
ide
lines M
an
ual
XML Element Description Valid Values Data Type Field
Size
Data
Element
Required
Patients Served
patientsserved
This header element should only occur once
per file.
Example: patientsserved 600 /
patientsserved
This is the total number of
patients who had at least one
outpatient surgery or procedure
during the sample month at the
HOPD or ASC, regardless of
whether the patient or surgery was
OAS-CAHPS eligible
1 – 999999
M = Unknown/Missing
Alphanumeric 6 Yes
Patients on file(s) submitted to Vendor
patientsfile
This header element should only occur once
per file.
Example: patientsfile 595 /patientsfile
Number of patients included on
the file that the vendor received
for this HOPD or ASC.
0 – 999999 Numeric 6 Yes
Eligible Patients
eligiblepatients
This header element should only occur once
per file.
Example: eligiblepatients 500 /
eligiblepatients
This is the number of patients in
the file submitted by the HOPD or
ASC which meet survey
eligibility criteria in the sample
month.
0 – 999999 Numeric 6 Yes
Sampled Patients
sampledpatients
This header element should only occur once
per file.
Example: sampledpatients 450 /
sampledpatients
This is the number of patients
selected for the survey during the
sample month. This value can be
zero only if all of the patients
included on the file that the
HOPD or ASC provided for the
sample month were ineligible for
the survey.
0 – 999999 Numeric 6 Yes

Ap
pen
dix
K: X
ML
Data
File
Layo
ut fo
r Sta
nd
ard
He
ad
er R
eco
rd
Decem
ber 2
01
5
K-4
C
en
ters
for M
ed
ica
re &
Med
icaid
Se
rvic
es
Ou
tpatie
nt a
nd
Am
bu
lato
ry S
urg
ery
CA
HP
S S
urv
ey P
roto
co
ls a
nd
Gu
ide
lines M
an
ual
PATIENT ADMINISTRATIVE DATA RECORD
The following section defines the format of the patient level data record.
NOTE: Each element must have a closing tag that is the same as the opening tag but with a forward slash. Data element names do not contain
any spaces, underscores, or capital letters.
XML Element Description Valid Values Data Type Field
Size
Data
Element
Required
Provider Number
providernum
This administrative element also occurs in the
previous header record.
Example: providernum 123456 /
providernum
This is the HOPD’s or ASC’s
CMS Certification Number
(CCN, formerly known as the
Medicare Provider ID Number)
No Dashes or spaces
Valid 6- or 10-digit CMS
Certification Number
(CCN)
Alphanumeric 10 Yes
Sample Month
samplemonth This administrative element also occurs in the
previous header record.
Example: samplemonth 12 /
samplemonth
OAS CAHPS Survey sampling
month
MM
(1 – 12 = January –
December)
Numeric 2 Yes
Sample Year
sampleyear This administrative element also occurs in the
previous header record.
Example: sampleyear 2016 /
sampleyear
Year of sample month YYYY
(2016 or greater)
Numeric 4 Yes

Decem
ber 2
01
5
Ap
pen
dix
K: X
ML
Data
File
Layo
ut fo
r Sta
nd
ard
He
ad
er R
eco
rd
Cen
ters
for M
ed
ica
re &
Med
icaid
Se
rvic
es
K
-5
Ou
tpatie
nt a
nd
Am
bu
lato
ry S
urg
ery
CA
HP
S S
urv
ey P
roto
co
ls a
nd
Gu
ide
lines M
an
ual
XML Element Description Valid Values Data Type Field
Size
Data
Element
Required
Sample ID No.
sampleid This administrative element should only occur
once per patient.
Example: sampleid 1234567 /sampleid
Survey vendors will assign a
unique de-identified sample
identification number (SID) to
each patient. The SID number
will be used to track the survey
status of the patient throughout
the survey administration process
and to designate sample patients
on the data file submitted to the
Data Center.
Maximum of 16
characters
Alphanumeric 16 Yes
Surgical Category
surgicalcat This administrative element should only occur
once per patient.
Example: surgicalcat 1 /surgicalcat
This is the category for the
surgery, and must be one of the
following options:
Gastrointestinal (GI), Orthopedic,
Ophthalmologic, Other.
If CPT code(s) in range 40000–
49999 or G-code(s) G0105,
G0121, or G0104, assign surgical
category 1.
If CPT code(s) in range 20000–
29999 or G-code is G0260, assign
surgical category 2.
If CPT code(s) in range 65000–
68899, assign surgical category 3.
If CPT code(s) or G codes not in
the range for surgical categories
1, 2 or 3, assign surgical category
4.
1 = Gastrointestinal (GI)
2 = Orthopedic
3 = Ophthalmologic
4 = Other
Numeric 1 Yes

Ap
pen
dix
K: X
ML
Data
File
Layo
ut fo
r Sta
nd
ard
He
ad
er R
eco
rd
Decem
ber 2
01
5
K-6
C
en
ters
for M
ed
ica
re &
Med
icaid
Se
rvic
es
Ou
tpatie
nt a
nd
Am
bu
lato
ry S
urg
ery
CA
HP
S S
urv
ey P
roto
co
ls a
nd
Gu
ide
lines M
an
ual
XML Element Description Valid Values Data Type Field
Size
Data
Element
Required
Age
patientage
This administrative element should only occur
once per patient.
Example: patientage 7 /patientage
Category for patient’s age as of
date of surgery/procedure.
(Patients must be 18 or older at
the date of surgery/procedure to
be eligible for the survey.)
18–24 .......................... 1
25-29 ........................... 2
30-34 ........................... 3
35-39 ........................... 4
40-44 ........................... 5
45-49 ........................... 6
50-54 ........................... 7
55-59 ........................... 8
60-64 ........................... 9
65-69 ......................... 10
70-74 ......................... 11
75-79 ......................... 12
80-84 ......................... 13
85-89 ......................... 14
90 or older................. 15
Unknown/Missing .... M
NOT APPLICABLE .. X
Alphanumeric 2 Yes
Gender
patientgender This administrative element should only occur
once per patient.
Example: patientgender 1 /
patientgender
Patient’s gender 1 = Male
2 = Female
M = Unknown/Missing
X = NOT APPLICABLE
Alphanumeric 1 Yes
Survey Mode
surveymode
This administrative element should only occur
once per patient.
Example: surveymode 1 /surveymode
This is the mode of data
collection the patient used to
complete the survey.
1 = Mail only
2 = Telephone only
X = NOT APPLICABLE
Alphanumeric 1 Yes

Decem
ber 2
01
5
Ap
pen
dix
K: X
ML
Data
File
Layo
ut fo
r Sta
nd
ard
He
ad
er R
eco
rd
Cen
ters
for M
ed
ica
re &
Med
icaid
Se
rvic
es
K
-7
Ou
tpatie
nt a
nd
Am
bu
lato
ry S
urg
ery
CA
HP
S S
urv
ey P
roto
co
ls a
nd
Gu
ide
lines M
an
ual
XML Element Description Valid Values Data Type Field
Size
Data
Element
Required
Lag Time
<lagtime>
This administrative element should only occur
once per patient.
Example: lagtime 51 /lagtime
The number of calendar days
between the date of eligible
surgery/procedure and the date
when this patient’s survey was
initiated.
0-90
X = NOT APPLICABLE
Alphanumeric 2 Yes
Final Survey Status
finalstatus
This administrative element should only occur
once per patient.
Example: finalstatus 110 /finalstatus
Final disposition of survey 110 = Completed Mail
Survey
120 = Completed Phone
Survey
210 = Ineligible:
Deceased
220 = Ineligible: Does
not Meet Eligibility
criteria
230 = Ineligible:
Language Barrier
240 = Ineligible:
Mentally or
Physically
Incapacitated
310 = Breakoff
320 = Refusal
330 = Bad Address/
Undeliverable Mail
340 = Wrong/Disc/No
Telephone Number
350 = No response after
Maximum attempts
Numeric 3 Yes

Ap
pen
dix
K: X
ML
Data
File
Layo
ut fo
r Sta
nd
ard
He
ad
er R
eco
rd
Decem
ber 2
01
5
K-8
C
en
ters
for M
ed
ica
re &
Med
icaid
Se
rvic
es
Ou
tpatie
nt a
nd
Am
bu
lato
ry S
urg
ery
CA
HP
S S
urv
ey P
roto
co
ls a
nd
Gu
ide
lines M
an
ual
XML Element Description Valid Values Data Type Field
Size
Data
Element
Required
Survey Language
language This administrative data element should only
occur once per patient.
Example: language 1 /language
Identify language in which survey
completed
1 = English
2 = Spanish
3 = Chinese
X = NOT APPLICABLE
Alphanumeric 1 Yes

Decem
ber 2
01
5
Ap
pen
dix
K: X
ML
Data
File
Layo
ut fo
r Sta
nd
ard
He
ad
er R
eco
rd
Cen
ters
for M
ed
ica
re &
Med
icaid
Se
rvic
es
K
-9
Ou
tpatie
nt a
nd
Am
bu
lato
ry S
urg
ery
CA
HP
S S
urv
ey P
roto
co
ls a
nd
Gu
ide
lines M
an
ual
PATIENT RESPONSE RECORD
The following section defines the format of the patient response record.
NOTE: Each element must have a closing tag that is the same as the opening tag but with a forward slash. Data element names do not contain
any spaces, underscores, or capital letters.
XML Element Description Valid Values Data Type Field
Size
Data
Element
Required
Q1 Informed
informed
This patient response data element should only
occur once per patient.
Example: informed 1 /informed
Before your procedure, did your
doctor or anyone from the facility
give you all the information you
needed about your procedure?
Yes, definitely............. 1
Yes, somewhat ............ 2
No ............................... 3
MISSING/DK ........... M
Alphanumeric 1 Yes
Q2 Instructions
instructions
This patient response data element should only
occur once per patient.
Example: instructions 1 /instructions
Before your procedure, did your
doctor or anyone from the facility
give you easy to understand
instructions about getting ready
for your procedure?
Yes, definitely............. 1
Yes, somewhat ............ 2
No ............................... 3
MISSING/DK ........... M
Alphanumeric 1 Yes
Q3 Check In
checkin This patient response data element should only
occur once per patient.
Example: checkin 1 /checkin
Did the check-in process run
smoothly?
Yes, definitely............. 1
Yes, somewhat ............ 2
No ............................... 3
MISSING/DK ........... M
Alphanumeric 1 Yes
Q4 Clean
clean
This patient response data element should only
occur once per patient.
Example: clean 1 /clean
Was the facility clean? Yes, definitely............. 1
Yes, somewhat ............ 2
No ............................... 3
MISSING/DK ........... M
Alphanumeric 1 Yes
Q5 Clerk Helpful
clerkhelpful This patient response data element should only
occur once per patient.
Example: clerkhelpful 1 /clerkhelpful
Were the clerks and receptionists
at the facility as helpful as you
thought they should be?
Yes, definitely............. 1
Yes, somewhat ............ 2
No ............................... 3
MISSING/DK ........... M
Alphanumeric 1 Yes

Ap
pen
dix
K: X
ML
Data
File
Layo
ut fo
r Sta
nd
ard
He
ad
er R
eco
rd
Decem
ber 2
01
5
K-1
0
Cen
ters
for M
ed
ica
re &
Med
icaid
Se
rvic
es
Ou
tpatie
nt a
nd
Am
bu
lato
ry S
urg
ery
CA
HP
S S
urv
ey P
roto
co
ls a
nd
Gu
ide
lines M
an
ual
XML Element Description Valid Values Data Type Field
Size
Data
Element
Required
Q6 Clerk Request
clerkrespect
This patient response data element should only
occur once per patient.
Example: clerkrespect 1 /clerkrespect
Did the clerks and receptionists at
the facility treat you with courtesy
and respect?
Yes, definitely............. 1
Yes, somewhat ............ 2
No ............................... 3
MISSING/DK ........... M
Alphanumeric 1 Yes
Q7 Dr. Respect
drrespect
This patient response data element should only
occur once per patient.
Example: drrespect 1 /drrespect
Did the doctors and nurses treat
you with courtesy and respect?
Yes, definitely............. 1
Yes, somewhat ............ 2
No ............................... 3
MISSING/DK ........... M
Alphanumeric 1 Yes
Q8 Dr. Comfort
drcomfort
This patient response data element should only
occur once per patient.
Example: drcomfort 1 /drcomfort
Did the doctors and nurses make
sure you were as comfortable as
possible?
Yes, definitely............. 1
Yes, somewhat ............ 2
No ............................... 3
MISSING/DK ........... M
Alphanumeric 1 Yes
Q9 Dr. Explain
drexplain
This patient response data element should only
occur once per patient.
Example: drexplain 1 /drexplain
Did the doctors and nurses
explain your procedure in a way
that was easy to understand?
Yes, definitely............. 1
Yes, somewhat ............ 2
No ............................... 3
MISSING/DK ........... M
Alphanumeric 1 Yes
Q10 Anesthesia
anesthesia
This patient response data element should only
occur once per patient.
Example: anesthesia 1 /anesthesia
Anesthesia is something that
would make you feel sleepy or go
to sleep during your procedure.
Were you given anesthesia?
Yes .............................. 1
No ............................... 2
MISSING/DK ........... M
Alphanumeric 1 Yes

Decem
ber 2
01
5
Ap
pen
dix
K: X
ML
Data
File
Layo
ut fo
r Sta
nd
ard
He
ad
er R
eco
rd
Cen
ters
for M
ed
ica
re &
Med
icaid
Se
rvic
es
K
-11
O
utp
atie
nt a
nd
Am
bu
lato
ry S
urg
ery
CA
HP
S S
urv
ey P
roto
co
ls a
nd
Gu
ide
lines M
an
ual
XML Element Description Valid Values Data Type Field
Size
Data
Element
Required
Q11 Anesthesia Explain
anesthesiaexplain
This patient response data element should only
occur once per patient.
Example: anesthesiaexplain 2 /
anesthesiaexplain
Did your doctor or anyone from
the facility explain the process of
giving anesthesia in a way that
was easy to understand?
Yes, definitely............. 1
Yes, somewhat ............ 2
No ............................... 3
MISSING/DK ........... M
NOT APPLICABLE .. X
Alphanumeric 1 Yes
Q12 Anesthesia Side
anesthesiaside
This patient response data element should only
occur once per patient.
Example: anesthesiaside 1 /
anesthesiaside
Did your doctor or anyone from
the facility explain the possible
side effects of the anesthesia in a
way that was easy to understand?
Yes, definitely............. 1
Yes, somewhat ............ 2
No ............................... 3
MISSING/DK ........... M
NOT APPLICABLE .. X
Alphanumeric 1 Yes
Q13 Discharge Instructions
dischargeinstructions This patient response data element should only
occur once per patient.
Example: dischargeinstructions 1 /
dischargeinstructions
Discharge instructions include
things like symptoms you should
watch for after your procedure,
instructions about medicines, and
home care. Before you left the
facility, did you get written
discharge instructions?
Yes .............................. 1
No ............................... 2
MISSING/DK ........... M
Alphanumeric 1 Yes
Q14 Recovery
recovery
This patient response data element should only
occur once per patient.
Example: recovery 1 /recovery
Did your doctor or anyone from
the facility prepare you for what
to expect during your recovery?
Yes, definitely............. 1
Yes, somewhat ............ 2
No ............................... 3
MISSING/DK ........... M
Alphanumeric 1 Yes

Ap
pen
dix
K: X
ML
Data
File
Layo
ut fo
r Sta
nd
ard
He
ad
er R
eco
rd
Decem
ber 2
01
5
K-1
2
Cen
ters
for M
ed
ica
re &
Med
icaid
Se
rvic
es
Ou
tpatie
nt a
nd
Am
bu
lato
ry S
urg
ery
CA
HP
S S
urv
ey P
roto
co
ls a
nd
Gu
ide
lines M
an
ual
XML Element Description Valid Values Data Type Field
Size
Data
Element
Required
Q15 Pain Info
paininfo This patient response data element should only
occur once per patient.
Example: paininfo 1 /paininfo
Some ways to control pain
include prescription medicine,
over-the-counter pain relievers or
ice packs. Did your doctor or
anyone from the facility give you
information about what to do if
you had pain as a result of your
procedure?
Yes, definitely............. 1
Yes, somewhat ............ 2
No ............................... 3
MISSING/DK ........... M
Alphanumeric 1 Yes
Q16 Pain Result
painresult
This patient response data element should only
occur once per patient.
Example: painresult 1 /painresult
At any time after leaving the
facility, did you have pain as a
result of your procedure?
Yes .............................. 1
No ............................... 2
MISSING/DK ........... M
Alphanumeric 1 Yes
Q17 Nausea
nausea
This patient response data element should only
occur once per patient.
Example: nausea 1 /nausea
Before you left the facility, did
your doctor or anyone from the
facility give you information
about what to do if you had
nausea or vomiting?
Yes, definitely............. 1
Yes, somewhat ............ 2
No ............................... 3
MISSING/DK ........... M
Alphanumeric 1 Yes
Q18 Nausea Result
nausearesult
This patient response data element should only
occur once per patient.
Example: nausearesult 1 /nausearesult
At any time after leaving the
facility, did you have nausea or
vomiting as a result of either your
procedure or the anesthesia?
Yes .............................. 1
No ............................... 2
MISSING/DK ........... M
Alphanumeric 1 Yes
Q19 Bleeding Instruction
bleedinginstruction This patient response data element should only
occur once per patient.
Example: bleedinginstruction 1 /
bleedinginstruction
Before you left the facility, did
your doctor or anyone from the
facility give you information
about what to do if you had
bleeding as a result of your
procedure?
Yes, definitely............. 1
Yes, somewhat ............ 2
No ............................... 3
MISSING/DK ........... M
Alphanumeric 1 Yes

Decem
ber 2
01
5
Ap
pen
dix
K: X
ML
Data
File
Layo
ut fo
r Sta
nd
ard
He
ad
er R
eco
rd
Cen
ters
for M
ed
ica
re &
Med
icaid
Se
rvic
es
K
-13
O
utp
atie
nt a
nd
Am
bu
lato
ry S
urg
ery
CA
HP
S S
urv
ey P
roto
co
ls a
nd
Gu
ide
lines M
an
ual
XML Element Description Valid Values Data Type Field
Size
Data
Element
Required
Q20 Bleeding Result
bleedingresult
This patient response data element should only
occur once per patient.
Example: bleedingresult 1 bleedingresult
At any time after leaving the
facility, did you have bleeding as
a result of your procedure?
Yes .............................. 1
No ............................... 2
MISSING/DK ........... M
Alphanumeric 2 Yes
Q21 Infection Info
infectioninfo This patient response data element should only
occur once per patient.
Example: infectioninfo 1 /infectioninfo
Possible signs of infection include
fever, swelling, heat, drainage or
redness. Before you left the
facility, did your doctor or anyone
from the facility give you
information about what to do if
you had possible signs of
infection?
Yes, definitely............. 1
Yes, somewhat ............ 2
No ............................... 3
MISSING/DK ........... M
Alphanumeric 1 Yes
Q22 Infections Signs
infectionsigns This patient response data element should only
occur once per patient.
Example: infectionsigns 1 /
infectionsigns
At any time after leaving the
facility, did you have any signs of
infection?
Yes .............................. 1
No ............................... 2
MISSING/DK ........... M
Alphanumeric 1 Yes

Ap
pen
dix
K: X
ML
Data
File
Layo
ut fo
r Sta
nd
ard
He
ad
er R
eco
rd
Decem
ber 2
01
5
K-1
4
Cen
ters
for M
ed
ica
re &
Med
icaid
Se
rvic
es
Ou
tpatie
nt a
nd
Am
bu
lato
ry S
urg
ery
CA
HP
S S
urv
ey P
roto
co
ls a
nd
Gu
ide
lines M
an
ual
XML Element Description Valid Values Data Type Field
Size
Data
Element
Required
Q23 Rate Facility
ratefacility This patient response data element should only
occur once per patient.
Example: ratefacility 2 /ratefacility
Using any number from 0 to 10,
where 0 is the worst facility
possible and 10 is the best facility
possible, what number would you
use to rate this facility?
Worst facility
possible ....................... 0
.................................... 1
.................................... 2
.................................... 3
.................................... 4
.................................... 5
.................................... 6
.................................... 7
.................................... 8
.................................... 9
Best facility possible . 10
MISSING/DK ........... M
Alphanumeric 2 Yes
Q24 Recommend
recommend This patient response data element should only
occur once per patient.
Example: recommend 2 /recommend
Would you recommend this
facility to your friends and
family?
Definitely No .............. 1
Probably No ................ 2
Probably Yes .............. 3
Definitely Yes ............. 4
MISSING/DK ........... M
Alphanumeric 1 Yes
Q25 Rate Overall
rateoverall This patient response data element should only
occur once per patient.
Example: rateoverall 1 /rateoverall
In general, how would you rate
your overall health?
Excellent ..................... 1
Very good ................... 2
Good ........................... 3
Fair .............................. 4
Poor ............................ 5
MISSING/DK ........... M
Alphanumeric 1 Yes
Q26 Rate Overall Mental
rateoverallmental This patient response data element should only
occur once per patient.
Example: rateoverallmental 1 /
rateoverallmental
In general, how would you rate
your overall mental or emotional
health?
Excellent ..................... 1
Very good ................... 2
Good ........................... 3
Fair .............................. 4
Poor ............................ 5
MISSING/DK ........... M
Alphanumeric 1 Yes
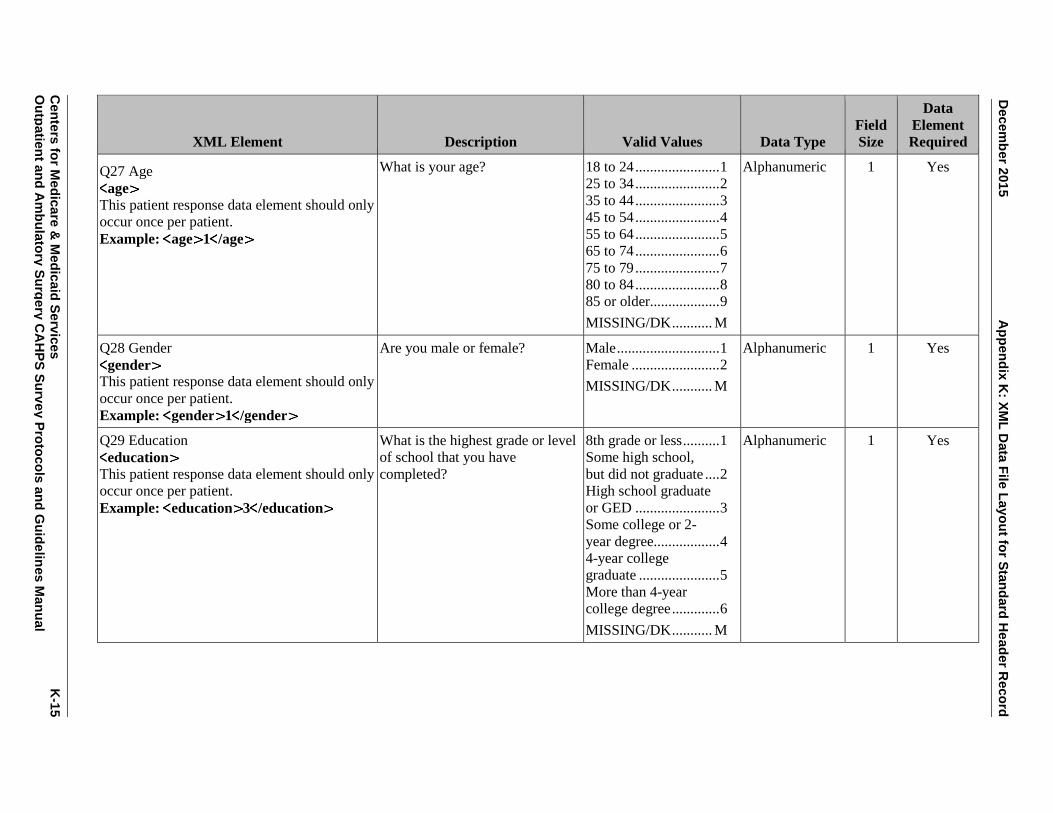
Decem
ber 2
01
5
Ap
pen
dix
K: X
ML
Data
File
Layo
ut fo
r Sta
nd
ard
He
ad
er R
eco
rd
Cen
ters
for M
ed
ica
re &
Med
icaid
Se
rvic
es
K
-15
O
utp
atie
nt a
nd
Am
bu
lato
ry S
urg
ery
CA
HP
S S
urv
ey P
roto
co
ls a
nd
Gu
ide
lines M
an
ual
XML Element Description Valid Values Data Type Field
Size
Data
Element
Required
Q27 Age
age This patient response data element should only
occur once per patient.
Example: age 1 /age
What is your age? 18 to 24 ....................... 1
25 to 34 ....................... 2
35 to 44 ....................... 3
45 to 54 ....................... 4
55 to 64 ....................... 5
65 to 74 ....................... 6
75 to 79 ....................... 7
80 to 84 ....................... 8
85 or older................... 9
MISSING/DK ........... M
Alphanumeric 1 Yes
Q28 Gender
gender This patient response data element should only
occur once per patient.
Example: gender 1 /gender
Are you male or female? Male ............................ 1
Female ........................ 2
MISSING/DK ........... M
Alphanumeric 1 Yes
Q29 Education
education This patient response data element should only
occur once per patient.
Example: education 3 /education
What is the highest grade or level
of school that you have
completed?
8th grade or less .......... 1
Some high school,
but did not graduate .... 2
High school graduate
or GED ....................... 3
Some college or 2-
year degree.................. 4
4-year college
graduate ...................... 5
More than 4-year
college degree ............. 6
MISSING/DK ........... M
Alphanumeric 1 Yes

Ap
pen
dix
K: X
ML
Data
File
Layo
ut fo
r Sta
nd
ard
He
ad
er R
eco
rd
Decem
ber 2
01
5
K-1
6
Cen
ters
for M
ed
ica
re &
Med
icaid
Se
rvic
es
Ou
tpatie
nt a
nd
Am
bu
lato
ry S
urg
ery
CA
HP
S S
urv
ey P
roto
co
ls a
nd
Gu
ide
lines M
an
ual
XML Element Description Valid Values Data Type Field
Size
Data
Element
Required
Q30 Ethnicity
ethnicity This patient response data element should only
occur once per patient.
Example: ethnicity 2 /ethnicity
Are you of Hispanic, Latino/a, or
Spanish origin?
Yes .............................. 1
No ............................... 2
MISSING/DK ........... M
Alphanumeric 1 Yes
Q31 Group
group
This patient response data element should only
occur once per patient.
Example: group 1 /group
Which group best describes you? Mexican, Mexican
American,
Chicano/a .................... 1
Puerto Rican ............... 2
Cuban .......................... 3
Another Hispanic,
Latino/a, or Spanish
origin .......................... 4
MISSING/DK ........... M
NOT APPLICABLE .. X
Alphanumeric 1 Yes
Q32 Race White-mail
racewhite-mail
This patient response data element should only
occur once per patient.
Example: racewhite-mail 1 /racewhite-
What is your race? You may
select one or more categories.
White .......................... 1
MISSING/DK ........... M
NOT APPLICABLE .. X
Alphanumeric 1 Yes
Q32 Race African American-mail
raceafricanamer-mail This patient response data element should only
occur once per patient.
Example: raceafricanamer-mail 1
/raceafricanamer-mail
What is your race? You may
select one or more categories.
Black or African
American .................... 1
MISSING/DK ........... M
NOT APPLICABLE .. X
Alphanumeric 1 Yes

Decem
ber 2
01
5
Ap
pen
dix
K: X
ML
Data
File
Layo
ut fo
r Sta
nd
ard
He
ad
er R
eco
rd
Cen
ters
for M
ed
ica
re &
Med
icaid
Se
rvic
es
K
-17
O
utp
atie
nt a
nd
Am
bu
lato
ry S
urg
ery
CA
HP
S S
urv
ey P
roto
co
ls a
nd
Gu
ide
lines M
an
ual
XML Element Description Valid Values Data Type Field
Size
Data
Element
Required
Q32 Race American Indian-mail
raceamerindian-mail This patient response data element should only
occur once per patient.
Example: raceamerindian-mail 1 /
raceamerindian-mail
What is your race? You may
select one or more categories.
American Indian or
Alaska Native ............. 1
MISSING/DK ........... M
NOT APPLICABLE .. X
Alphanumeric 1 Yes
Q32 Race Asian Indian-mail
raceasianindian-mail This patient response data element should only
occur once per patient.
Example: raceasianindian-mail 1 /
raceasianindian-mail
What is your race? You may
select one or more categories.
Asian Indian................ 1
MISSING/DK ........... M
NOT APPLICABLE .. X
Alphanumeric 1 Yes
Q32 Race Chinese-mail
racechinese-mail This patient response data element should only
occur once per patient.
Example: racechinese-mail 1 /
racechinese-mail
What is your race? You may
select one or more categories.
Chinese ....................... 1
MISSING/DK ........... M
NOT APPLICABLE .. X
Alphanumeric 1 Yes
Q32 Race Filipino-mail
racefilipino-mail This patient response data element should only
occur once per patient.
Example: racefilipino-mail 1 /
racefilipino-mail
What is your race? You may
select one or more categories.
Filipino ....................... 1
MISSING/DK ........... M
NOT APPLICABLE .. X
Alphanumeric 1 Yes
Q32 Race Japanese-mail
racejapanese-mail This patient response data element should only
occur once per patient.
Example: racejapanese-mail 1 /
racejapanese-mail
What is your race? You may
select one or more categories.
Japanese ...................... 1
MISSING/DK ........... M
NOT APPLICABLE .. X
Alphanumeric 1 Yes

Ap
pen
dix
K: X
ML
Data
File
Layo
ut fo
r Sta
nd
ard
He
ad
er R
eco
rd
Decem
ber 2
01
5
K-1
8
Cen
ters
for M
ed
ica
re &
Med
icaid
Se
rvic
es
Ou
tpatie
nt a
nd
Am
bu
lato
ry S
urg
ery
CA
HP
S S
urv
ey P
roto
co
ls a
nd
Gu
ide
lines M
an
ual
XML Element Description Valid Values Data Type Field
Size
Data
Element
Required
Q32 Race Korean-mail
racekorean-mail This patient response data element should only
occur once per patient.
Example: racekorean-mail 1 /
racekorean-mail
What is your race? You may
select one or more categories.
Korean ........................ 1
MISSING/DK ........... M
NOT APPLICABLE .. X
Alphanumeric 1 Yes
Q32 Race Vietnamese-mail
racevietnamese-mail This patient response data element should only
occur once per patient.
Example: racevietnamese-mail 1 /
racevietnamese-mail
What is your race? You may
select one or more categories.
Vietnamese ................. 1
MISSING/DK ........... M
NOT APPLICABLE .. X
Alphanumeric 1 Yes
Q32 Race Other Asian-mail
raceotherasian-mail This patient response data element should only
occur once per patient.
Example: raceotherasian-mail 1 /
raceotherasian-mail
What is your race? You may
select one or more categories.
Other Asian ................. 1
MISSING/DK ........... M
NOT APPLICABLE .. X
Alphanumeric 1 Yes
Q32 Race Native Hawaiian-mail
racenativehawaiian-mail This patient response data element should only
occur once per patient.
Example: racenativehawaiian-mail 1 /
racenativehawaiian-mail
What is your race? You may
select one or more categories.
Native Hawaiian ......... 1
MISSING/DK ........... M
NOT APPLICABLE .. X
Alphanumeric 1 Yes
Q32 Race Guamanian Chamorro-mail
raceguamanianchamorro-mail This patient response data element should only
occur once per patient.
Example: raceguamanianchamorro-mail
1 /raceguamanianchamorro-mail
What is your race? You may
select one or more categories.
Guamanian or
Chamorro .................... 1
MISSING/DK ........... M
NOT APPLICABLE .. X
Alphanumeric 1 Yes

Decem
ber 2
01
5
Ap
pen
dix
K: X
ML
Data
File
Layo
ut fo
r Sta
nd
ard
He
ad
er R
eco
rd
Cen
ters
for M
ed
ica
re &
Med
icaid
Se
rvic
es
K
-19
O
utp
atie
nt a
nd
Am
bu
lato
ry S
urg
ery
CA
HP
S S
urv
ey P
roto
co
ls a
nd
Gu
ide
lines M
an
ual
XML Element Description Valid Values Data Type Field
Size
Data
Element
Required
Q32 Race Samoan-mail
racesamoan-mail This patient response data element should only
occur once per patient.
Example: racesamoan-mail 1 /
racesamoan-mail
What is your race? You may
select one or more categories.
Samoan ....................... 1
MISSING/DK ........... M
NOT APPLICABLE .. X
Alphanumeric 1 Yes
Q32 Race Other Pacific Islander-mail
raceotherpacificislander-mail This patient response data element should only
occur once per patient.
Example: raceotherpacificislander-mail 1
/raceotherpacificislander-mail
What is your race? You may
select one or more categories.
Other Pacific
Islander ....................... 1
MISSING/DK ........... M
NOT APPLICABLE .. X
Alphanumeric 1 Yes
Q32 Race White-phone
racewhite-phone This patient response data element should only
occur once per patient.
Example: racewhite-phone 1 /racewhite-
phone
What is your race? You may
select one or more categories. Are
you…
White .......................... 1
MISSING/DK ........... M
NOT APPLICABLE .. X
Alphanumeric 1 Yes
Q32 Race African American-phone
raceafricanamer-phone
This patient response data element should only
occur once per patient.
Example: raceafricanamer-phone 1 /
raceafricanamer-phone
What is your race? You may
select one or more categories. Are
you…
Black or African
American .................... 1
MISSING/DK ........... M
NOT APPLICABLE .. X
Alphanumeric 1 Yes
Q32 Race American Indian-phone
raceamerindian-phone
This patient response data element should only
occur once per patient.
Example: raceamerindian-phone 1 /
raceamerindian-phone
What is your race? You may
select one or more categories. Are
you…
American Indian or
Alaska Native ............. 1
MISSING/DK ........... M
NOT APPLICABLE .. X
Alphanumeric 1 Yes

Ap
pen
dix
K: X
ML
Data
File
Layo
ut fo
r Sta
nd
ard
He
ad
er R
eco
rd
Decem
ber 2
01
5
K-2
0
Cen
ters
for M
ed
ica
re &
Med
icaid
Se
rvic
es
Ou
tpatie
nt a
nd
Am
bu
lato
ry S
urg
ery
CA
HP
S S
urv
ey P
roto
co
ls a
nd
Gu
ide
lines M
an
ual
XML Element Description Valid Values Data Type Field
Size
Data
Element
Required
Q32 Race Asian Indian-phone
raceasianindian-phone
This patient response data element should only
occur once per patient.
Example: raceasianindian-phone 1
/raceasianindian-phone
What is your race? You may
select one or more categories. Are
you…
Asian Indian................ 1
MISSING/DK ........... M
NOT APPLICABLE .. X
Alphanumeric 1 Yes
Q32 Race None of Above-phone
racenoneofabove-phone
This patient response data element should only
occur once per patient.
Example: racenoneofabove-phone 1 / racenoneofabove-phone
What is your race? You may
select one or more categories. Are
you…
NONE OF ABOVE .... 1
MISSING/DK ........... M
NOT APPLICABLE .. X
Alphanumeric 1 Yes
Q32a Race Asian Indian-phone
raceasianindian-phone
This patient response data element should only
occur once per patient.
Example: raceasianindian-phone 1 / raceasianindian-phone
Which groups best describe you?
You may select one or more
categories. Are you…
Asian Indian................ 1
MISSING/DK ........... M
NOT APPLICABLE .. X
Alphanumeric 1 Yes
Q32a Race Chinese-phone
racechinese-phone
This patient response data element should only
occur once per patient.
Example: racechinese-phone 1
/racechinese-phone
Which groups best describe you?
You may select one or more
categories. Are you…
Chinese ....................... 1
MISSING/DK ........... M
NOT APPLICABLE .. X
Alphanumeric 1 Yes
Q32a Race Filipino-phone
racefilipino-phone
This patient response data element should only
occur once per patient.
Example: racefilipino-phone 1
/racefilipino-phone
Which groups best describe you?
You may select one or more
categories. Are you…
Filipino ....................... 1
MISSING/DK ........... M
NOT APPLICABLE .. X
Alphanumeric 1 Yes

Decem
ber 2
01
5
Ap
pen
dix
K: X
ML
Data
File
Layo
ut fo
r Sta
nd
ard
He
ad
er R
eco
rd
Cen
ters
for M
ed
ica
re &
Med
icaid
Se
rvic
es
K
-21
O
utp
atie
nt a
nd
Am
bu
lato
ry S
urg
ery
CA
HP
S S
urv
ey P
roto
co
ls a
nd
Gu
ide
lines M
an
ual
XML Element Description Valid Values Data Type Field
Size
Data
Element
Required
Q32a Race Japanese-phone
racejapanese-phone
This patient response data element should only
occur once per patient.
Example: racejapanese-phone 1 /
racejapanese-phone
Which groups best describe you?
You may select one or more
categories. Are you…
Japanese ...................... 1
MISSING/DK ........... M
NOT APPLICABLE .. X
Alphanumeric 1 Yes
Q32a Race Korean-phone
racekorean-phone
This patient response data element should only
occur once per patient.
Example: racekorean-phone 1 /
racekorean-phone
Which groups best describe you?
You may select one or more
categories. Are you…
Korean ........................ 1
MISSING/DK ........... M
NOT APPLICABLE .. X
Alphanumeric 1 Yes
Q32a Race Vietnamese-phone
racevietnamese-phone
This patient response data element should only
occur once per patient.
Example: racevietnamese-phone 1 /
racevietnamese-phone
Which groups best describe you?
You may select one or more
categories. Are you…
Vietnamese ................. 1
MISSING/DK ........... M
NOT APPLICABLE .. X
Alphanumeric 1 Yes
Q32a Race Other Asian-phone
raceotherasian-phone
This patient response data element should only
occur once per patient.
Example: raceotherasian-phone 1 /
raceotherasian-phone
Which groups best describe you?
You may select one or more
categories. Are you…
Other Asian ................. 1
MISSING/DK ........... M
NOT APPLICABLE .. X
Alphanumeric 1 Yes

Ap
pen
dix
K: X
ML
Data
File
Layo
ut fo
r Sta
nd
ard
He
ad
er R
eco
rd
Decem
ber 2
01
5
K-2
2
Cen
ters
for M
ed
ica
re &
Med
icaid
Se
rvic
es
Ou
tpatie
nt a
nd
Am
bu
lato
ry S
urg
ery
CA
HP
S S
urv
ey P
roto
co
ls a
nd
Gu
ide
lines M
an
ual
XML Element Description Valid Values Data Type Field
Size
Data
Element
Required
Q32a Race None of Above Asian Indian-
phone
racenoneofaboveasianindian-phone
This patient response data element should only
occur once per patient.
Example: racenoneofaboveasianindian-
phone 1 / racenoneofaboveasianindian-
phone
Which groups best describe you?
You may select one or more
categories. Are you…
NONE OF ABOVE .... 1
MISSING/DK ........... M
NOT APPLICABLE .. X
Alphanumeric 1 Yes
Q32b Race Native Hawaiian-phone
racenativehawaiian-phone
This patient response data element should only
occur once per patient.
Example: racenativehawaiian-phone 1 /
racenativehawaiian-phone
Which groups best describe you?
You may select one or more
categories. Are you…
Native Hawaiian ......... 1
MISSING/DK ........... M
NOT APPLICABLE .. X
Alphanumeric 1 Yes
Q32b Race Guamanian Chamorro-phone
raceguamanianchamorro-phone
This patient response data element should only
occur once per patient.
Example: raceguamanianchamorro-phone
1 /raceguamanianchamorro-phone
Which groups best describe you?
You may select one or more
categories. Are you…
Guamanian or
Chamorro .................... 1
MISSING/DK ........... M
NOT APPLICABLE .. X
Alphanumeric 1 Yes
Q32b Race Samoan-phone
racesamoan-phone
This patient response data element should only
occur once per patient.
Example: racesamoan-phone 1 /
racesamoan-phone
Which groups best describe you?
You may select one or more
categories. Are you…
Samoan ....................... 1
MISSING/DK ........... M
NOT APPLICABLE .. X
Alphanumeric 1 Yes

Decem
ber 2
01
5
Ap
pen
dix
K: X
ML
Data
File
Layo
ut fo
r Sta
nd
ard
He
ad
er R
eco
rd
Cen
ters
for M
ed
ica
re &
Med
icaid
Se
rvic
es
K
-23
O
utp
atie
nt a
nd
Am
bu
lato
ry S
urg
ery
CA
HP
S S
urv
ey P
roto
co
ls a
nd
Gu
ide
lines M
an
ual
XML Element Description Valid Values Data Type Field
Size
Data
Element
Required
Q32b Race Other Pacific Islander-phone
raceotherpacificislander-phone
This patient response data element should only
occur once per patient.
Example: raceotherpacificislander-phone
1 /raceotherpacificislander-phone
Which groups best describe you?
You may select one or more
categories. Are you…
Other Pacific
Islander ....................... 1
MISSING/DK ........... M
NOT APPLICABLE .. X
Alphanumeric 1 Yes
Q32b Race None of Above Pacific-phone
racenoneofabovepacific-phone
This patient response data element should only
occur once per patient.
Example: racenoneofabovepacific-phone 1
/racenoneofabovepacific-phone
Which groups best describe you?
You may select one or more
categories. Are you…
NONE OF ABOVE .... 1
MISSING/DK ........... M
NOT APPLICABLE .. X
Alphanumeric 1 Yes
Q33 Speak English
speakenglish This patient response data element should only
occur once per patient.
Example: speakenglish 1 /speakenglish
How well do you speak English?
(Would you say…)
Very well .................... 1
Well ............................ 2
Not well ...................... 3
Not at all ..................... 4
MISSING/DK ........... M
Alphanumeric 1 Yes
Q34 Speak Other
speakother This patient response data element should only
occur once per patient.
Example: speakother 1 /speakother
Do you speak a language other
than English at home?
Yes, speak language
other than English ....... 1
No, speak English at
home ........................... 2
MISSING/DK ........... M
Alphanumeric 1 Yes
Q35 Speak Other Specify
speakotherspecify This patient response data element should only
occur once per patient.
Example: speakotherspecify 1 /
speakotherspecify
What is that language? Spanish ....................... 1
Other ........................... 2
MISSING/DK ........... M
NOT APPLICABLE .. X
Alphanumeric 1 Yes

Ap
pen
dix
K: X
ML
Data
File
Layo
ut fo
r Sta
nd
ard
He
ad
er R
eco
rd
Decem
ber 2
01
5
K-2
4
Cen
ters
for M
ed
ica
re &
Med
icaid
Se
rvic
es
Ou
tpatie
nt a
nd
Am
bu
lato
ry S
urg
ery
CA
HP
S S
urv
ey P
roto
co
ls a
nd
Gu
ide
lines M
an
ual
XML Element Description Valid Values Data Type Field
Size
Data
Element
Required
Q36 Help-mail
help This patient response data element should only
occur once per patient.
Example: help 1 /help
Did someone help you complete
this survey?
Yes .............................. 1
No ............................... 2
MISSING/DK ........... M
NOT APPLICABLE .. X
Alphanumeric 1 Yes
Q37 Help Read-mail
helpread This patient response data element should only
occur once per patient.
Example: helpread 1 /helpread
How did that person help you?
Check all that apply.
Read the questions
to me ........................... 1
MISSING/DK ........... M
NOT APPLICABLE .. X
Alphanumeric 1 Yes
Q37 Help Wrote-mail
helpwrote This patient response data element should only
occur once per patient.
Example: helpwrote 1 /helpwrote
How did that person help you?
Check all that apply.
Wrote down the
answers I gave ............ 1
MISSING/DK ........... M
NOT APPLICABLE .. X
Alphanumeric 1 Yes
Q37 Help Answer-mail
helpanswer This patient response data element should only
occur once per patient.
Example: helpanswer 1 /helpanswer
How did that person help you?
Check all that apply.
Answered the
questions for me ......... 1
MISSING/DK ........... M
NOT APPLICABLE .. X
Alphanumeric 1 Yes
Q37 Help Translate-mail
helptranslate This patient response data element should only
occur once per patient.
Example: helptranslate 1 /
helptranslate
How did that person help you?
Check all that apply.
Translated the
questions into my
language ...................... 1
MISSING/DK ........... M
NOT APPLICABLE .. X
Alphanumeric 1 Yes
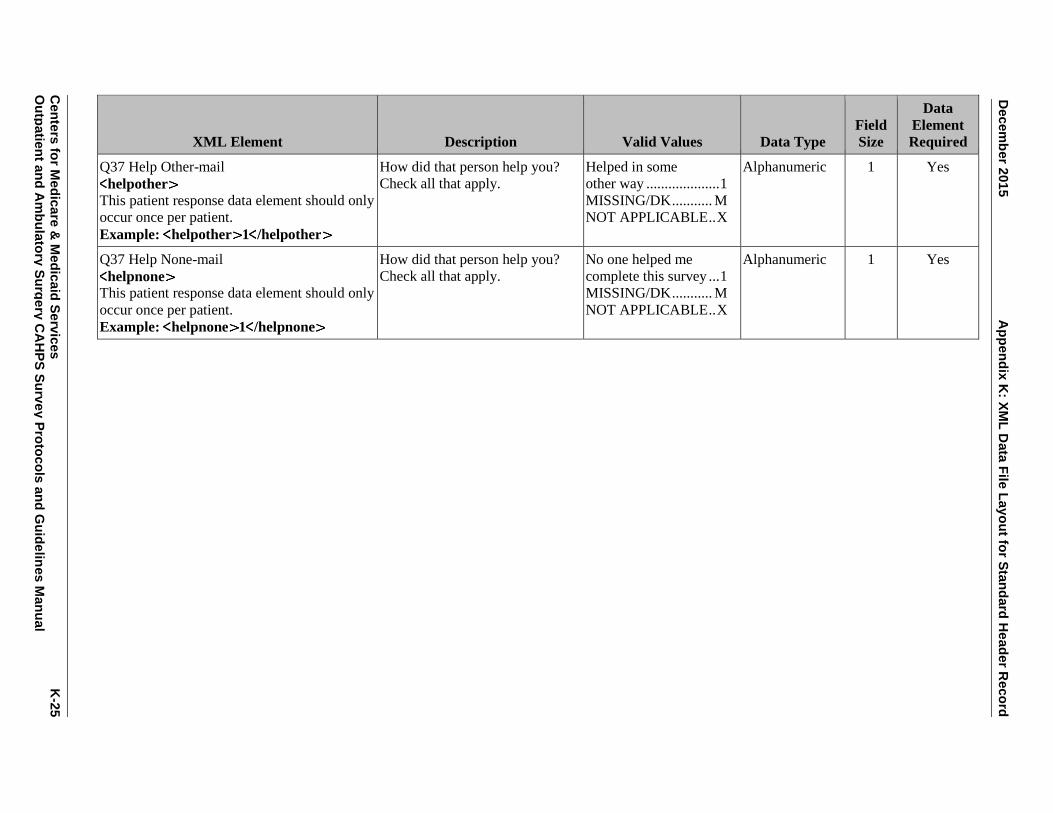
Decem
ber 2
01
5
Ap
pen
dix
K: X
ML
Data
File
Layo
ut fo
r Sta
nd
ard
He
ad
er R
eco
rd
Cen
ters
for M
ed
ica
re &
Med
icaid
Se
rvic
es
K
-25
O
utp
atie
nt a
nd
Am
bu
lato
ry S
urg
ery
CA
HP
S S
urv
ey P
roto
co
ls a
nd
Gu
ide
lines M
an
ual
XML Element Description Valid Values Data Type Field
Size
Data
Element
Required
Q37 Help Other-mail
helpother This patient response data element should only
occur once per patient.
Example: helpother 1 /helpother
How did that person help you?
Check all that apply.
Helped in some
other way .................... 1
MISSING/DK ........... M
NOT APPLICABLE .. X
Alphanumeric 1 Yes
Q37 Help None-mail
helpnone This patient response data element should only
occur once per patient.
Example: helpnone 1 /helpnone
How did that person help you?
Check all that apply.
No one helped me
complete this survey ... 1
MISSING/DK ........... M
NOT APPLICABLE .. X
Alphanumeric 1 Yes
Appendix K: XML Data File Layout for Standard Header Record December 2015
K-26 Centers for Medicare & Medicaid Services Outpatient and Ambulatory Surgery CAHPS Survey Protocols and Guidelines Manual
This page intentionally left blank.

Centers for Medicare & Medicaid Services Outpatient and Ambulatory Surgery CAHPS Survey Protocols and Guidelines Manual
APPENDIX L:
XML DATA FILE LAYOUT FOR DISPROPORTIONATE STRATIFIED
RANDOM SAMPLING (DSRS) HEADER RECORD

Appendix L: XML Data File Layout for Disproportionate Stratified Random Sampling (DSRS) Header Record December 2015
Centers for Medicare & Medicaid Services Outpatient and Ambulatory Surgery CAHPS Survey Protocols and Guidelines Manual
This page intentionally left blank.

Cen
ters
for M
ed
ica
re &
Med
icaid
Se
rvic
es
L
-1
Ou
tpatie
nt a
nd
Am
bu
lato
ry S
urg
ery
CA
HP
S S
urv
ey P
roto
co
ls a
nd
Gu
ide
lines M
an
ual
DSRS XML DATA FILE LAYOUT
OUTPATIENT AND AMBULATORY CAHPS SURVEY
DSRS HEADER RECORD
The following section defines the format of the header record.
NOTE: Each element must have a closing tag that is the same as the opening tag but with a forward slash. Data element names do not contain
any spaces, underscores, or capital letters.
XML Element Description Valid Values Data Type Field
Size
Data
Element
Required
Type of Header Record
headertype>
This header element should only occur once
per file.
Example: headertype 2 /headertype
Type of Header Record 2 = DSRS Numeric 1 Yes
Provider Name
<providername
This header element should only occur once
per file.
Example: providername
SampleHOPDASCName /providername
This is the HOPD’s or ASC’s
Provider Name
— Alphanumeric 100 Yes
Provider Number
providernum
This header element will occur again as an
administrative data element in the patient level
data record.
Example: providernum 123456 /
providernum
This is the HOPD’s or ASC’s
CMS Certification Number
(CCN, formerly known as the
Medicare Provider ID Number)
No Dashes or spaces
Valid 6- or 10-digit CMS
Certification Number
(CCN)
Alphanumeric 10 Yes

Ap
pen
dix
L: X
ML
Data
File
Layo
ut fo
r Dis
pro
po
rtion
ate
Stra
tified
Ran
do
m S
am
plin
g (D
SR
S) H
ead
er R
eco
rd
Decem
ber 2
01
5
L-2
C
en
ters
for M
ed
ica
re &
Med
icaid
Se
rvic
es
Ou
tpatie
nt a
nd
Am
bu
lato
ry S
urg
ery
CA
HP
S S
urv
ey P
roto
co
ls a
nd
Gu
ide
lines M
an
ual
XML Element Description Valid Values Data Type Field
Size
Data
Element
Required
Sample Month
samplemonth This header element will occur again as an
administrative data element in the patient level
data record.
Example: samplemonth 12 /
samplemonth
Survey vendors will select a
sample of patients who meet
survey eligibility criteria for each
calendar month. The Sample
Month is the month for which the
sample was selected.
MM
(1 – 12 = January –
December)
Numeric 2 Yes
Sample Year
sampleyear This header element will occur again as an
administrative data element in the patient level
data record.
Example: sampleyear 2016 /
sampleyear
This is the calendar year in which
the survey is conducted.
YYYY
(2016 or greater)
Numeric 4 Yes
Survey Mode
surveymode
This header element will occur again as an
administrative data element in the patient level
data record.
Example: surveymode 1 /surveymode
The survey mode, either mail
only, phone only, or mixed mode,
must be the same for all sample
members in each sample month in
the calendar quarter for all of the
HOPD or ASC locations and
strata under the same CCN.
1 = Mail only
2 = Telephone only
3 = Mixed mode
Numeric 1 Yes
Type of Sampling
sampletype
This header element should only occur once
per file.
Example: sampletype 5 /sampletype
Type of sampling used. Note:
Sample Type must be the same
for all three months in each
quarter.
5 = Disproportionate
stratified random
sampling
Numeric 1 Yes
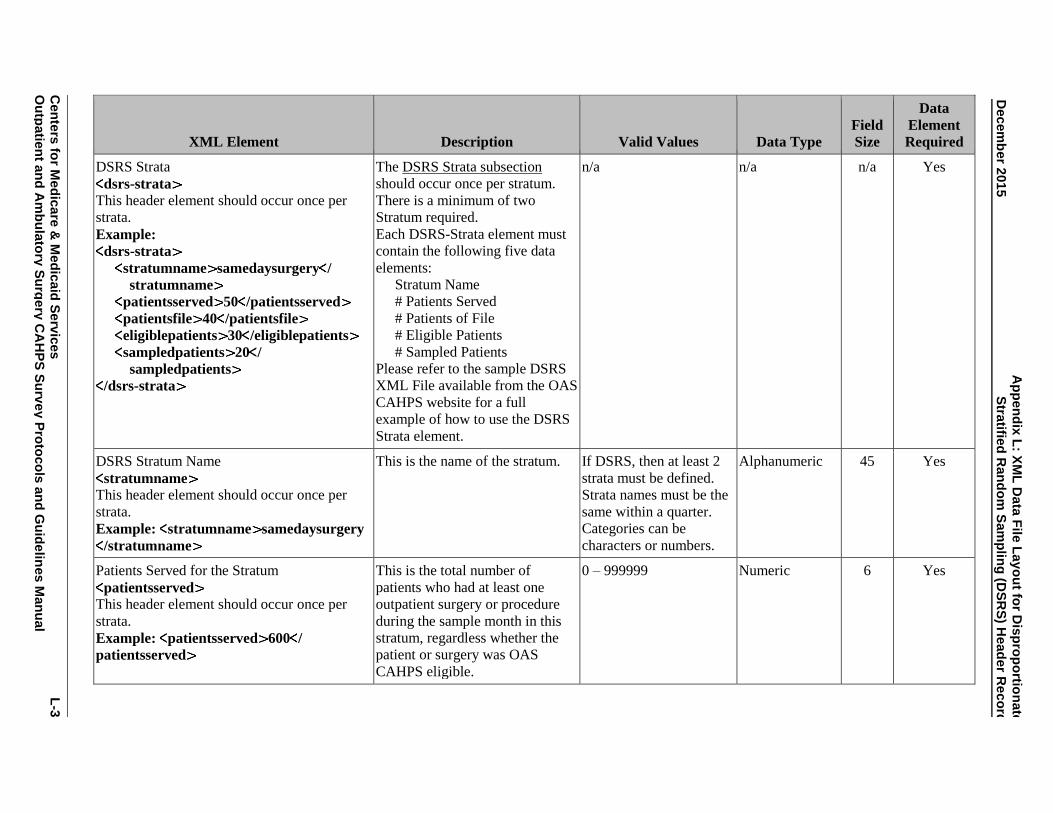
A
pp
en
dix
L: X
ML
Data
File
Layo
ut fo
r Dis
pro
po
rtion
ate
Decem
ber 2
01
5
Stra
tified
Ran
do
m S
am
plin
g (D
SR
S) H
ead
er R
eco
rd
Cen
ters
for M
ed
ica
re &
Med
icaid
Se
rvic
es
L
-3
Ou
tpatie
nt a
nd
Am
bu
lato
ry S
urg
ery
CA
HP
S S
urv
ey P
roto
co
ls a
nd
Gu
ide
lines M
an
ual
XML Element Description Valid Values Data Type Field
Size
Data
Element
Required
DSRS Strata
dsrs-strata
This header element should occur once per
strata.
Example:
dsrs-strata
stratumname samedaysurgery /
stratumname
patientsserved 50 /patientsserved
patientsfile 40 /patientsfile
eligiblepatients 30 /eligiblepatients
sampledpatients 20 /
sampledpatients
/dsrs-strata
The DSRS Strata subsection
should occur once per stratum.
There is a minimum of two
Stratum required.
Each DSRS-Strata element must
contain the following five data
elements:
Stratum Name
# Patients Served
# Patients of File
# Eligible Patients
# Sampled Patients
Please refer to the sample DSRS
XML File available from the OAS
CAHPS website for a full
example of how to use the DSRS
Strata element.
n/a n/a n/a Yes
DSRS Stratum Name
stratumname
This header element should occur once per
strata.
Example: stratumname samedaysurgery
/stratumname
This is the name of the stratum. If DSRS, then at least 2
strata must be defined.
Strata names must be the
same within a quarter.
Categories can be
characters or numbers.
Alphanumeric 45 Yes
Patients Served for the Stratum
patientsserved
This header element should occur once per
strata.
Example: patientsserved 600 /
patientsserved
This is the total number of
patients who had at least one
outpatient surgery or procedure
during the sample month in this
stratum, regardless whether the
patient or surgery was OAS
CAHPS eligible.
0 – 999999 Numeric 6 Yes

Ap
pen
dix
L: X
ML
Data
File
Layo
ut fo
r Dis
pro
po
rtion
ate
Stra
tified
Ran
do
m S
am
plin
g (D
SR
S) H
ead
er R
eco
rd
Decem
ber 2
01
5
L-4
C
en
ters
for M
ed
ica
re &
Med
icaid
Se
rvic
es
Ou
tpatie
nt a
nd
Am
bu
lato
ry S
urg
ery
CA
HP
S S
urv
ey P
roto
co
ls a
nd
Gu
ide
lines M
an
ual
XML Element Description Valid Values Data Type Field
Size
Data
Element
Required
DSRS Patients on file(s) submitted to Vendor
patientsfile
This header element should occur once per
strata.
Example: patientsfile 595 /patientsfile
Number of patients included on
the file that the vendor received
for this stratum for this sample
month.
0 – 999999 Numeric 6 Yes
DSRS Eligible Patients
eligiblepatients
This header element should occur once per
strata.
Example: eligiblepatients 500 /
eligiblepatients
Number of patients who meet
survey eligibility criteria within
this stratum for this sample
month.
0 – 999999 Numeric 6 Yes
DSRS Sampled Patients
sampledpatients
This header element should occur once per
strata.
Example: sampledpatients 450 /
sampledpatients
This is the number of sampled
patients for this stratum for this
sample month. This variable will
be used to weight the data.
10 – 999999
Must be a minimum of 10
sampled patients in every
stratum in every month.
Numeric 6 Yes

A
pp
en
dix
L: X
ML
Data
File
Layo
ut fo
r Dis
pro
po
rtion
ate
Decem
ber 2
01
5
Stra
tified
Ran
do
m S
am
plin
g (D
SR
S) H
ead
er R
eco
rd
Cen
ters
for M
ed
ica
re &
Med
icaid
Se
rvic
es
L
-5
Ou
tpatie
nt a
nd
Am
bu
lato
ry S
urg
ery
CA
HP
S S
urv
ey P
roto
co
ls a
nd
Gu
ide
lines M
an
ual
PATIENT ADMINISTRATIVE DATA RECORD
The following section defines the format of the patient level data record.
NOTE: Each element must have a closing tag that is the same as the opening tag but with a forward slash. Data element names do not contain
any spaces, underscores, or capital letters.
XML Element Description Valid Values Data Type Field
Size
Data
Element
Required
Provider Number
providernum
This administrative element also occurs in the
previous header record.
Example: providernum 123456 /
providernum
This is the HOPD’s or ASC’s
CMS Certification Number
(CCN, formerly known as the
Medicare Provider ID Number)
No Dashes or spaces
Valid 6- or 10- digit CMS
Certification Number
(CCN)
Alphanumeric 10 Yes
Sample Month
samplemonth This administrative element also occurs in the
previous header record.
Example: samplemonth 12 /
samplemonth
OAS CAHPS Survey sampling
month
MM
(1 – 12 = January –
December)
Numeric 2 Yes
Sample Year
sampleyear This administrative element also occurs in the
previous header record.
Example: sampleyear 2016 /
sampleyear
Year of sample month YYYY
(2016 or greater)
Numeric 4 Yes

Ap
pen
dix
L: X
ML
Data
File
Layo
ut fo
r Dis
pro
po
rtion
ate
Stra
tified
Ran
do
m S
am
plin
g (D
SR
S) H
ead
er R
eco
rd
Decem
ber 2
01
5
L-6
C
en
ters
for M
ed
ica
re &
Med
icaid
Se
rvic
es
Ou
tpatie
nt a
nd
Am
bu
lato
ry S
urg
ery
CA
HP
S S
urv
ey P
roto
co
ls a
nd
Gu
ide
lines M
an
ual
XML Element Description Valid Values Data Type Field
Size
Data
Element
Required
Sample ID No.
sampleid This administrative element should only occur
once per patient.
Example: sampleid 1234567 /sampleid
Survey vendors will assign a
unique de-identified sample
identification number (SID) to
each patient. The SID number
will be used to track the survey
status of the patient throughout
the survey administration process
and to designate sample patients
on the data file submitted to the
Data Center.
Maximum of 16
characters
Alphanumeric 16 Yes
Surgical Category
surgicalcat This administrative element should only occur
once per patient.
Example: surgicalcat 1234567 /
surgicalcat
This is the category for the
surgery, and must be one of the
following options:
Gastrointestinal (GI), Orthopedic,
Ophthalmologic, Other.
If CPT code(s) in range 40490–
49999 or G-code(s) G0105,
G0121, or G0104, assign surgical
category 1.
If CPT code(s) in range 20000–
29999 or G-code is G0260, assign
surgical category 2.
If CPT code(s) in range 65091–
68899, assign surgical category 3.
If CPT code(s) or G codes not in
the range for surgical catories 1, 2
or 3, assign surgical category 4.
1 = Gastrointestinal (GI)
2 = Orthopedic
3 = Ophthalmologic
4 = Other
Numeric 1 Yes

A
pp
en
dix
L: X
ML
Data
File
Layo
ut fo
r Dis
pro
po
rtion
ate
Decem
ber 2
01
5
Stra
tified
Ran
do
m S
am
plin
g (D
SR
S) H
ead
er R
eco
rd
Cen
ters
for M
ed
ica
re &
Med
icaid
Se
rvic
es
L
-7
Ou
tpatie
nt a
nd
Am
bu
lato
ry S
urg
ery
CA
HP
S S
urv
ey P
roto
co
ls a
nd
Gu
ide
lines M
an
ual
XML Element Description Valid Values Data Type Field
Size
Data
Element
Required
Age
patientage
This administrative element should only occur
once per patient.
Example: patientage 7 /patientage
Category for patient’s age as of
the date of surgery/procedure.
(Patients must be 18 or older at
the date of surgery/procedure to
be eligible for the survey.)
18–24 .......................... 1
25-29 ........................... 2
30-34 ........................... 3
35-39 ........................... 4
40-44 ........................... 5
45-49 ........................... 6
50-54 ........................... 7
55-59 ........................... 8
60-64 ........................... 9
65-69 ......................... 10
70-74 ......................... 11
75-79 ......................... 12
80-84 ......................... 13
85-89 ......................... 14
90 or older................. 15
Unknown/Missing .... M
NOT APPLICABLE .. X
Alphanumeric 2 Yes
Gender
patientgender This administrative element should only occur
once per patient.
Example: patientgender 1 /
patientgender
Patient’s gender 1 = Male
2 = Female
M = Unknown/Missing
X = NOT APPLICABLE
Alphanumeric 1 Yes
Survey Mode
surveymode
This administrative element should only occur
once per patient.
Example: surveymode 1 /surveymode
This is the mode of data
collection the patient used to
complete the survey.
1 = Mail only
2 = Telephone only
X = NOT APPLICABLE
Alphanumeric 1 Yes
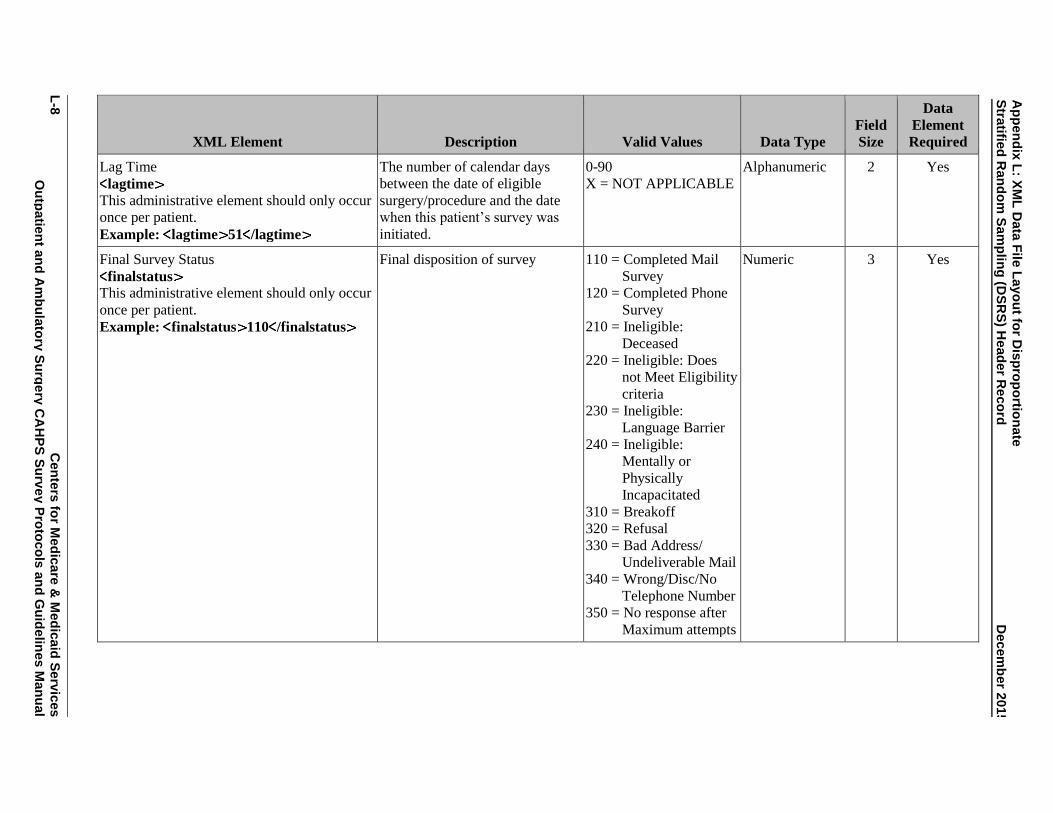
Ap
pen
dix
L: X
ML
Data
File
Layo
ut fo
r Dis
pro
po
rtion
ate
Stra
tified
Ran
do
m S
am
plin
g (D
SR
S) H
ead
er R
eco
rd
Decem
ber 2
01
5
L-8
C
en
ters
for M
ed
ica
re &
Med
icaid
Se
rvic
es
Ou
tpatie
nt a
nd
Am
bu
lato
ry S
urg
ery
CA
HP
S S
urv
ey P
roto
co
ls a
nd
Gu
ide
lines M
an
ual
XML Element Description Valid Values Data Type Field
Size
Data
Element
Required
Lag Time
lagtime
This administrative element should only occur
once per patient.
Example: lagtime 51 /lagtime
The number of calendar days
between the date of eligible
surgery/procedure and the date
when this patient’s survey was
initiated.
0-90
X = NOT APPLICABLE
Alphanumeric 2 Yes
Final Survey Status
finalstatus
This administrative element should only occur
once per patient.
Example: finalstatus 110 /finalstatus
Final disposition of survey 110 = Completed Mail
Survey
120 = Completed Phone
Survey
210 = Ineligible:
Deceased
220 = Ineligible: Does
not Meet Eligibility
criteria
230 = Ineligible:
Language Barrier
240 = Ineligible:
Mentally or
Physically
Incapacitated
310 = Breakoff
320 = Refusal
330 = Bad Address/
Undeliverable Mail
340 = Wrong/Disc/No
Telephone Number
350 = No response after
Maximum attempts
Numeric 3 Yes

A
pp
en
dix
L: X
ML
Data
File
Layo
ut fo
r Dis
pro
po
rtion
ate
Decem
ber 2
01
5
Stra
tified
Ran
do
m S
am
plin
g (D
SR
S) H
ead
er R
eco
rd
Cen
ters
for M
ed
ica
re &
Med
icaid
Se
rvic
es
L
-9
Ou
tpatie
nt a
nd
Am
bu
lato
ry S
urg
ery
CA
HP
S S
urv
ey P
roto
co
ls a
nd
Gu
ide
lines M
an
ual
XML Element Description Valid Values Data Type Field
Size
Data
Element
Required
Survey Language
language This administrative data element should only
occur once per patient.
Example: language 1 /language
Identify language in which survey
completed
1 = English
2 = Spanish
3 = Chinese
X = NOT APPLICABLE
Alphanumeric 1 Yes
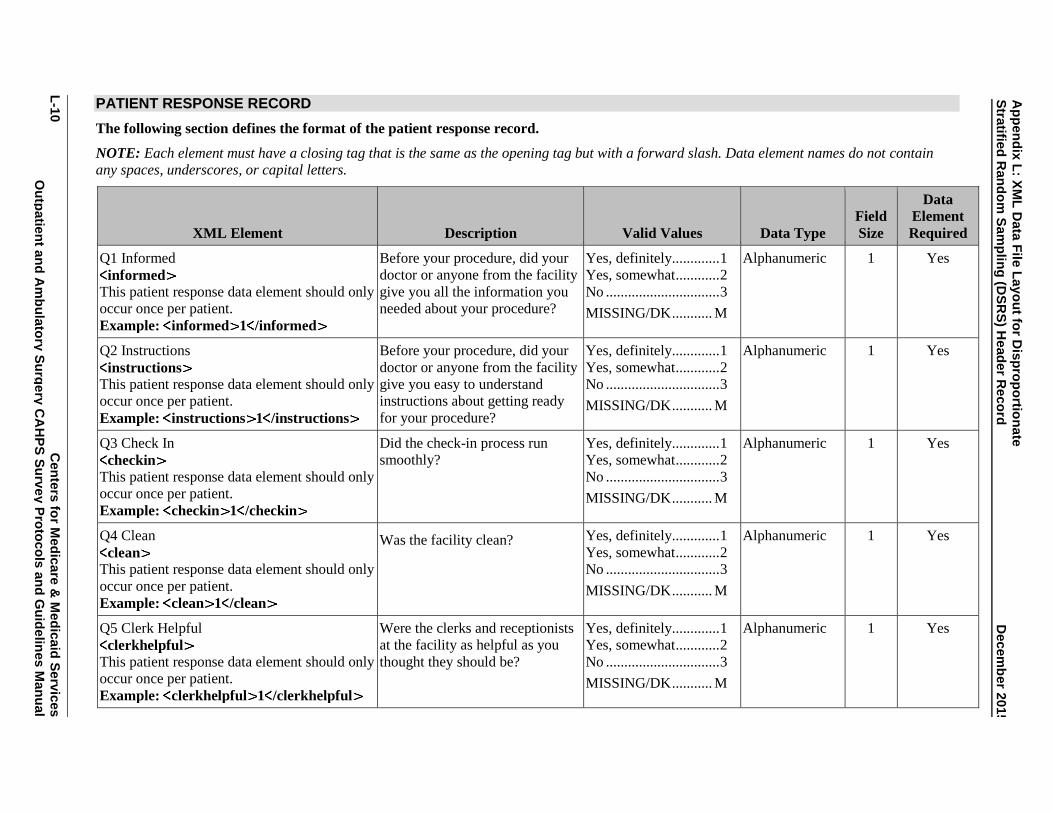
Ap
pen
dix
L: X
ML
Data
File
Layo
ut fo
r Dis
pro
po
rtion
ate
Stra
tified
Ran
do
m S
am
plin
g (D
SR
S) H
ead
er R
eco
rd
Decem
ber 2
01
5
L-1
0
Cen
ters
for M
ed
ica
re &
Med
icaid
Se
rvic
es
Ou
tpatie
nt a
nd
Am
bu
lato
ry S
urg
ery
CA
HP
S S
urv
ey P
roto
co
ls a
nd
Gu
ide
lines M
an
ual
PATIENT RESPONSE RECORD
The following section defines the format of the patient response record.
NOTE: Each element must have a closing tag that is the same as the opening tag but with a forward slash. Data element names do not contain
any spaces, underscores, or capital letters.
XML Element Description Valid Values Data Type Field
Size
Data
Element
Required
Q1 Informed
informed
This patient response data element should only
occur once per patient.
Example: informed 1 /informed
Before your procedure, did your
doctor or anyone from the facility
give you all the information you
needed about your procedure?
Yes, definitely............. 1
Yes, somewhat ............ 2
No ............................... 3
MISSING/DK ........... M
Alphanumeric 1 Yes
Q2 Instructions
instructions
This patient response data element should only
occur once per patient.
Example: instructions 1 /instructions
Before your procedure, did your
doctor or anyone from the facility
give you easy to understand
instructions about getting ready
for your procedure?
Yes, definitely............. 1
Yes, somewhat ............ 2
No ............................... 3
MISSING/DK ........... M
Alphanumeric 1 Yes
Q3 Check In
checkin This patient response data element should only
occur once per patient.
Example: checkin 1 /checkin
Did the check-in process run
smoothly?
Yes, definitely............. 1
Yes, somewhat ............ 2
No ............................... 3
MISSING/DK ........... M
Alphanumeric 1 Yes
Q4 Clean
clean
This patient response data element should only
occur once per patient.
Example: clean 1 /clean
Was the facility clean? Yes, definitely............. 1
Yes, somewhat ............ 2
No ............................... 3
MISSING/DK ........... M
Alphanumeric 1 Yes
Q5 Clerk Helpful
clerkhelpful This patient response data element should only
occur once per patient.
Example: clerkhelpful 1 /clerkhelpful
Were the clerks and receptionists
at the facility as helpful as you
thought they should be?
Yes, definitely............. 1
Yes, somewhat ............ 2
No ............................... 3
MISSING/DK ........... M
Alphanumeric 1 Yes

A
pp
en
dix
L: X
ML
Data
File
Layo
ut fo
r Dis
pro
po
rtion
ate
Decem
ber 2
01
5
Stra
tified
Ran
do
m S
am
plin
g (D
SR
S) H
ead
er R
eco
rd
Cen
ters
for M
ed
ica
re &
Med
icaid
Se
rvic
es
L
-11
Ou
tpatie
nt a
nd
Am
bu
lato
ry S
urg
ery
CA
HP
S S
urv
ey P
roto
co
ls a
nd
Gu
ide
lines M
an
ual
XML Element Description Valid Values Data Type Field
Size
Data
Element
Required
Q6 Clerk Request
clerkrespect
This patient response data element should only
occur once per patient.
Example: clerkrespect 1 /clerkrespect
Did the clerks and receptionists at
the facility treat you with courtesy
and respect?
Yes, definitely............. 1
Yes, somewhat ............ 2
No ............................... 3
MISSING/DK ........... M
Alphanumeric 1 Yes
Q7 Dr. Respect
drrespect
This patient response data element should only
occur once per patient.
Example: drrespect 1 /drrespect
Did the doctors and nurses treat
you with courtesy and respect?
Yes, definitely............. 1
Yes, somewhat ............ 2
No ............................... 3
MISSING/DK ........... M
Alphanumeric 1 Yes
Q8 Dr. Comfort
drcomfort
This patient response data element should only
occur once per patient.
Example: drcomfort 1 /drcomfort
Did the doctors and nurses make
sure you were as comfortable as
possible?
Yes, definitely............. 1
Yes, somewhat ............ 2
No ............................... 3
MISSING/DK ........... M
Alphanumeric 1 Yes
Q9 Dr. Explain
drexplain
This patient response data element should only
occur once per patient.
Example: drexplain 1 /drexplain
Did the doctors and nurses
explain your procedure in a way
that was easy to understand?
Yes, definitely............. 1
Yes, somewhat ............ 2
No ............................... 3
MISSING/DK ........... M
Alphanumeric 1 Yes
Q10 Anesthesia
anesthesia
This patient response data element should only
occur once per patient.
Example: anesthesia 1 /anesthesia
Anesthesia is something that
would make you feel sleepy or go
to sleep during your procedure.
Were you given anesthesia?
Yes .............................. 1
No ............................... 2
MISSING/DK ........... M
Alphanumeric 1 Yes

Ap
pen
dix
L: X
ML
Data
File
Layo
ut fo
r Dis
pro
po
rtion
ate
Stra
tified
Ran
do
m S
am
plin
g (D
SR
S) H
ead
er R
eco
rd
Decem
ber 2
01
5
L-1
2
Cen
ters
for M
ed
ica
re &
Med
icaid
Se
rvic
es
Ou
tpatie
nt a
nd
Am
bu
lato
ry S
urg
ery
CA
HP
S S
urv
ey P
roto
co
ls a
nd
Gu
ide
lines M
an
ual
XML Element Description Valid Values Data Type Field
Size
Data
Element
Required
Q11 Anesthesia Explain
anesthesiaexplain
This patient response data element should only
occur once per patient.
Example: anesthesiaexplain 2 /
anesthesiaexplain
Did your doctor or anyone from
the facility explain the process of
giving anesthesia in a way that
was easy to understand?
Yes, definitely............. 1
Yes, somewhat ............ 2
No ............................... 3
MISSING/DK ........... M
NOT APPLICABLE .. X
Alphanumeric 1 Yes
Q12 Anesthesia Side
anesthesiaside
This patient response data element should only
occur once per patient.
Example: anesthesiaside 1 /
anesthesiaside
Did your doctor or anyone from
the facility explain the possible
side effects of the anesthesia in a
way that was easy to understand?
Yes, definitely............. 1
Yes, somewhat ............ 2
No ............................... 3
MISSING/DK ........... M
NOT APPLICABLE .. X
Alphanumeric 1 Yes
Q13 Discharge Instructions
dischargeinstructions This patient response data element should only
occur once per patient.
Example: dischargeinstructions 1 /
dischargeinstructions
Discharge instructions include
things like symptoms you should
watch for after your procedure,
instructions about medicines, and
home care. Before you left the
facility, did you get written
discharge instructions?
Yes .............................. 1
No ............................... 2
MISSING/DK ........... M
Alphanumeric 1 Yes
Q14 Recovery
recovery
This patient response data element should only
occur once per patient.
Example: recovery 1 /recovery
Did your doctor or anyone from
the facility prepare you for what
to expect during your recovery?
Yes, definitely............. 1
Yes, somewhat ............ 2
No ............................... 3
MISSING/DK ........... M
Alphanumeric 1 Yes

A
pp
en
dix
L: X
ML
Data
File
Layo
ut fo
r Dis
pro
po
rtion
ate
Decem
ber 2
01
5
Stra
tified
Ran
do
m S
am
plin
g (D
SR
S) H
ead
er R
eco
rd
Cen
ters
for M
ed
ica
re &
Med
icaid
Se
rvic
es
L
-13
Ou
tpatie
nt a
nd
Am
bu
lato
ry S
urg
ery
CA
HP
S S
urv
ey P
roto
co
ls a
nd
Gu
ide
lines M
an
ual
XML Element Description Valid Values Data Type Field
Size
Data
Element
Required
Q15 Pain Info
paininfo This patient response data element should only
occur once per patient.
Example: paininfo 1 /paininfo
Some ways to control pain
include prescription medicine,
over-the-counter pain relievers or
ice packs. Did your doctor or
anyone from the facility give you
information about what to do if
you had pain as a result of your
procedure?
Yes, definitely............. 1
Yes, somewhat ............ 2
No ............................... 3
MISSING/DK ........... M
Alphanumeric 1 Yes
Q16 Pain Result
painresult
This patient response data element should only
occur once per patient.
Example: painresult 1 /painresult
At any time after leaving the
facility, did you have pain as a
result of your procedure?
Yes .............................. 1
No ............................... 2
MISSING/DK ........... M
Alphanumeric 1 Yes
Q17 Nausea
nausea
This patient response data element should only
occur once per patient.
Example: nausea 1 /nausea
Before you left the facility, did
your doctor or anyone from the
facility give you information
about what to do if you had
nausea or vomiting?
Yes, definitely............. 1
Yes, somewhat ............ 2
No ............................... 3
MISSING/DK ........... M
Alphanumeric 1 Yes
Q18 Nausea Result
nausearesult
This patient response data element should only
occur once per patient.
Example: nausearesult 1 /nausearesult
At any time after leaving the
facility, did you have nausea or
vomiting as a result of either your
procedure or the anesthesia?
Yes .............................. 1
No ............................... 2
MISSING/DK ........... M
Alphanumeric 1 Yes
Q19 Bleeding Instruction
bleedinginstruction This patient response data element should only
occur once per patient.
Example: bleedinginstruction 1 /
bleedinginstruction
Before you left the facility, did
your doctor or anyone from the
facility give you information
about what to do if you had
bleeding as a result of your
procedure?
Yes, definitely............. 1
Yes, somewhat ............ 2
No ............................... 3
MISSING/DK ........... M
Alphanumeric 1 Yes

Ap
pen
dix
L: X
ML
Data
File
Layo
ut fo
r Dis
pro
po
rtion
ate
Stra
tified
Ran
do
m S
am
plin
g (D
SR
S) H
ead
er R
eco
rd
Decem
ber 2
01
5
L-1
4
Cen
ters
for M
ed
ica
re &
Med
icaid
Se
rvic
es
Ou
tpatie
nt a
nd
Am
bu
lato
ry S
urg
ery
CA
HP
S S
urv
ey P
roto
co
ls a
nd
Gu
ide
lines M
an
ual
XML Element Description Valid Values Data Type Field
Size
Data
Element
Required
Q20 Bleeding Result
bleedingresult
This patient response data element should only
occur once per patient.
Example: bleedingresult 1 bleedingresult
At any time after leaving the
facility, did you have bleeding as
a result of your procedure?
Yes .............................. 1
No ............................... 2
MISSING/DK ........... M
Alphanumeric 2 Yes
Q21 Infection Info
infectioninfo This patient response data element should only
occur once per patient.
Example: infectioninfo 1 /infectioninfo
Possible signs of infection include
fever, swelling, heat, drainage or
redness. Before you left the
facility, did your doctor or anyone
from the facility give you
information about what to do if
you had possible signs of
infection?
Yes, definitely............. 1
Yes, somewhat ............ 2
No ............................... 3
MISSING/DK ........... M
Alphanumeric 1 Yes
Q22 Infections Signs
infectionsigns This patient response data element should only
occur once per patient.
Example: infectionsigns 1 /
infectionsigns
At any time after leaving the
facility, did you have any signs of
infection?
Yes .............................. 1
No ............................... 2
MISSING/DK ........... M
Alphanumeric 1 Yes

A
pp
en
dix
L: X
ML
Data
File
Layo
ut fo
r Dis
pro
po
rtion
ate
Decem
ber 2
01
5
Stra
tified
Ran
do
m S
am
plin
g (D
SR
S) H
ead
er R
eco
rd
Cen
ters
for M
ed
ica
re &
Med
icaid
Se
rvic
es
L
-15
Ou
tpatie
nt a
nd
Am
bu
lato
ry S
urg
ery
CA
HP
S S
urv
ey P
roto
co
ls a
nd
Gu
ide
lines M
an
ual
XML Element Description Valid Values Data Type Field
Size
Data
Element
Required
Q23 Rate Facility
ratefacility This patient response data element should only
occur once per patient.
Example: ratefacility 2 /ratefacility
Using any number from 0 to 10,
where 0 is the worst facility
possible and 10 is the best facility
possible, what number would you
use to rate this facility?
Worst facility
possible ....................... 0
.................................... 1
.................................... 2
.................................... 3
.................................... 4
.................................... 5
.................................... 6
.................................... 7
.................................... 8
.................................... 9
Best facility possible . 10
MISSING/DK ........... M
Alphanumeric 2 Yes
Q24 Recommend
recommend This patient response data element should only
occur once per patient.
Example: recommend 2 /recommend
Would you recommend this
facility to your friends and
family?
Definitely No .............. 1
Probably No ................ 2
Probably Yes .............. 3
Definitely Yes ............. 4
MISSING/DK ........... M
Alphanumeric 1 Yes
Q25 Rate Overall
rateoverall This patient response data element should only
occur once per patient.
Example: rateoverall 1 /rateoverall
In general, how would you rate
your overall health?
Excellent ..................... 1
Very good ................... 2
Good ........................... 3
Fair .............................. 4
Poor ............................ 5
MISSING/DK ........... M
Alphanumeric 1 Yes
Q26 Rate Overall Mental
rateoverallmental This patient response data element should only
occur once per patient.
Example: rateoverallmental 1 /
rateoverallmental
In general, how would you rate
your overall mental or emotional
health?
Excellent ..................... 1
Very good ................... 2
Good ........................... 3
Fair .............................. 4
Poor ............................ 5
MISSING/DK ........... M
Alphanumeric 1 Yes

Ap
pen
dix
L: X
ML
Data
File
Layo
ut fo
r Dis
pro
po
rtion
ate
Stra
tified
Ran
do
m S
am
plin
g (D
SR
S) H
ead
er R
eco
rd
Decem
ber 2
01
5
L-1
6
Cen
ters
for M
ed
ica
re &
Med
icaid
Se
rvic
es
Ou
tpatie
nt a
nd
Am
bu
lato
ry S
urg
ery
CA
HP
S S
urv
ey P
roto
co
ls a
nd
Gu
ide
lines M
an
ual
XML Element Description Valid Values Data Type Field
Size
Data
Element
Required
Q27 Age
age This patient response data element should only
occur once per patient.
Example: age 1 /age
What is your age? 18 to 24 ....................... 1
25 to 34 ....................... 2
35 to 44 ....................... 3
45 to 54 ....................... 4
55 to 64 ....................... 5
65 to 74 ....................... 6
75 to 79 ....................... 7
80 to 84 ....................... 8
85 or older................... 9
MISSING/DK ........... M
Alphanumeric 1 Yes
Q28 Gender
gender This patient response data element should only
occur once per patient.
Example: gender 1 /gender
Are you male or female? Male ............................ 1
Female ........................ 2
MISSING/DK ........... M
Alphanumeric 1 Yes
Q29 Education
education This patient response data element should only
occur once per patient.
Example: education 3 /education
What is the highest grade or level
of school that you have
completed?
8th grade or less .......... 1
Some high school,
but did not graduate .... 2
High school graduate
or GED ....................... 3
Some college or 2-
year degree.................. 4
4-year college
graduate ...................... 5
More than 4-year
college degree ............. 6
MISSING/DK ........... M
Alphanumeric 1 Yes
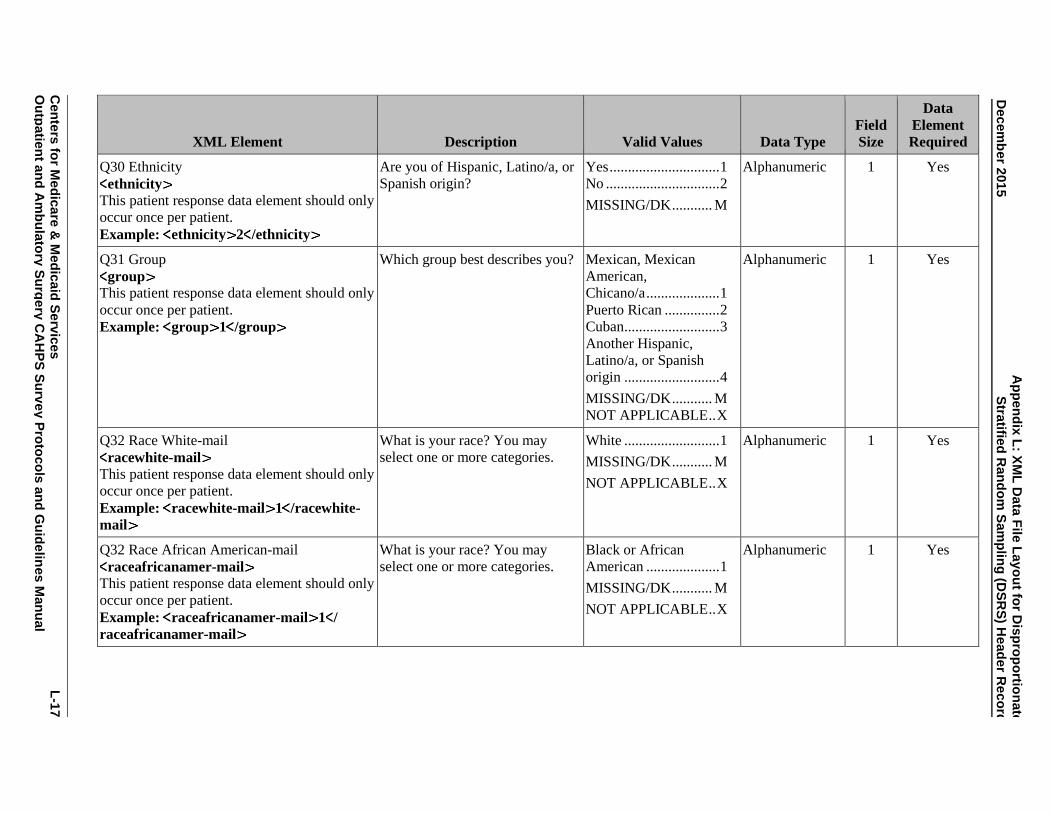
A
pp
en
dix
L: X
ML
Data
File
Layo
ut fo
r Dis
pro
po
rtion
ate
Decem
ber 2
01
5
Stra
tified
Ran
do
m S
am
plin
g (D
SR
S) H
ead
er R
eco
rd
Cen
ters
for M
ed
ica
re &
Med
icaid
Se
rvic
es
L
-17
Ou
tpatie
nt a
nd
Am
bu
lato
ry S
urg
ery
CA
HP
S S
urv
ey P
roto
co
ls a
nd
Gu
ide
lines M
an
ual
XML Element Description Valid Values Data Type Field
Size
Data
Element
Required
Q30 Ethnicity
ethnicity This patient response data element should only
occur once per patient.
Example: ethnicity 2 /ethnicity
Are you of Hispanic, Latino/a, or
Spanish origin?
Yes .............................. 1
No ............................... 2
MISSING/DK ........... M
Alphanumeric 1 Yes
Q31 Group
group
This patient response data element should only
occur once per patient.
Example: group 1 /group
Which group best describes you? Mexican, Mexican
American,
Chicano/a .................... 1
Puerto Rican ............... 2
Cuban .......................... 3
Another Hispanic,
Latino/a, or Spanish
origin .......................... 4
MISSING/DK ........... M
NOT APPLICABLE .. X
Alphanumeric 1 Yes
Q32 Race White-mail
racewhite-mail
This patient response data element should only
occur once per patient.
Example: racewhite-mail 1 /racewhite-
What is your race? You may
select one or more categories.
White .......................... 1
MISSING/DK ........... M
NOT APPLICABLE .. X
Alphanumeric 1 Yes
Q32 Race African American-mail
raceafricanamer-mail This patient response data element should only
occur once per patient.
Example: raceafricanamer-mail 1 /
raceafricanamer-mail
What is your race? You may
select one or more categories.
Black or African
American .................... 1
MISSING/DK ........... M
NOT APPLICABLE .. X
Alphanumeric 1 Yes

Ap
pen
dix
L: X
ML
Data
File
Layo
ut fo
r Dis
pro
po
rtion
ate
Stra
tified
Ran
do
m S
am
plin
g (D
SR
S) H
ead
er R
eco
rd
Decem
ber 2
01
5
L-1
8
Cen
ters
for M
ed
ica
re &
Med
icaid
Se
rvic
es
Ou
tpatie
nt a
nd
Am
bu
lato
ry S
urg
ery
CA
HP
S S
urv
ey P
roto
co
ls a
nd
Gu
ide
lines M
an
ual
XML Element Description Valid Values Data Type Field
Size
Data
Element
Required
Q32 Race American Indian-mail
raceamerindian-mail This patient response data element should only
occur once per patient.
Example: raceamerindian-mail 1 /
raceamerindian-mail
What is your race? You may
select one or more categories.
American Indian or
Alaska Native ............. 1
MISSING/DK ........... M
NOT APPLICABLE .. X
Alphanumeric 1 Yes
Q32 Race Asian Indian-mail
raceasianindian-mail This patient response data element should only
occur once per patient.
Example: raceasianindian-mail 1 /
raceasianindian-mail
What is your race? You may
select one or more categories.
Asian Indian................ 1
MISSING/DK ........... M
NOT APPLICABLE .. X
Alphanumeric 1 Yes
Q32 Race Chinese-mail
racechinese-mail This patient response data element should only
occur once per patient.
Example: racechinese-mail 1 /
racechinese-mail
What is your race? You may
select one or more categories.
Chinese ....................... 1
MISSING/DK ........... M
NOT APPLICABLE .. X
Alphanumeric 1 Yes
Q32 Race Filipino-mail
racefilipino-mail This patient response data element should only
occur once per patient.
Example: racefilipino-mail 1 /
racefilipino-mail
What is your race? You may
select one or more categories.
Filipino ....................... 1
MISSING/DK ........... M
NOT APPLICABLE .. X
Alphanumeric 1 Yes
Q32 Race Japanese-mail
racejapanese-mail This patient response data element should only
occur once per patient.
Example: racejapanese-mail 1 /
racejapanese-mail
What is your race? You may
select one or more categories.
Japanese ...................... 1
MISSING/DK ........... M
NOT APPLICABLE .. X
Alphanumeric 1 Yes

A
pp
en
dix
L: X
ML
Data
File
Layo
ut fo
r Dis
pro
po
rtion
ate
Decem
ber 2
01
5
Stra
tified
Ran
do
m S
am
plin
g (D
SR
S) H
ead
er R
eco
rd
Cen
ters
for M
ed
ica
re &
Med
icaid
Se
rvic
es
L
-19
Ou
tpatie
nt a
nd
Am
bu
lato
ry S
urg
ery
CA
HP
S S
urv
ey P
roto
co
ls a
nd
Gu
ide
lines M
an
ual
XML Element Description Valid Values Data Type Field
Size
Data
Element
Required
Q32 Race Korean-mail
racekorean-mail This patient response data element should only
occur once per patient.
Example: racekorean-mail 1 /
racekorean-mail
What is your race? You may
select one or more categories.
Korean ........................ 1
MISSING/DK ........... M
NOT APPLICABLE .. X
Alphanumeric 1 Yes
Q32 Race Vietnamese-mail
racevietnamese-mail This patient response data element should only
occur once per patient.
Example: racevietnamese-mail 1 /
racevietnamese-mail
What is your race? You may
select one or more categories.
Vietnamese ................. 1
MISSING/DK ........... M
NOT APPLICABLE .. X
Alphanumeric 1 Yes
Q32 Race Other Asian-mail
raceotherasian-mail This patient response data element should only
occur once per patient.
Example: raceotherasian-mail 1 /
raceotherasian-mail
What is your race? You may
select one or more categories.
Other Asian ................. 1
MISSING/DK ........... M
NOT APPLICABLE .. X
Alphanumeric 1 Yes
Q32 Race Native Hawaiian-mail
racenativehawaiian-mail This patient response data element should only
occur once per patient.
Example: racenativehawaiian-mail 1 /
racenativehawaiian-mail
What is your race? You may
select one or more categories.
Native Hawaiian ......... 1
MISSING/DK ........... M
NOT APPLICABLE .. X
Alphanumeric 1 Yes
Q32 Race Guamanian Chamorro-mail
raceguamanianchamorro-mail This patient response data element should only
occur once per patient.
Example: raceguamanianchamorro-mail
1 /raceguamanianchamorro-mail
What is your race? You may
select one or more categories.
Guamanian or
Chamorro .................... 1
MISSING/DK ........... M
NOT APPLICABLE .. X
Alphanumeric 1 Yes
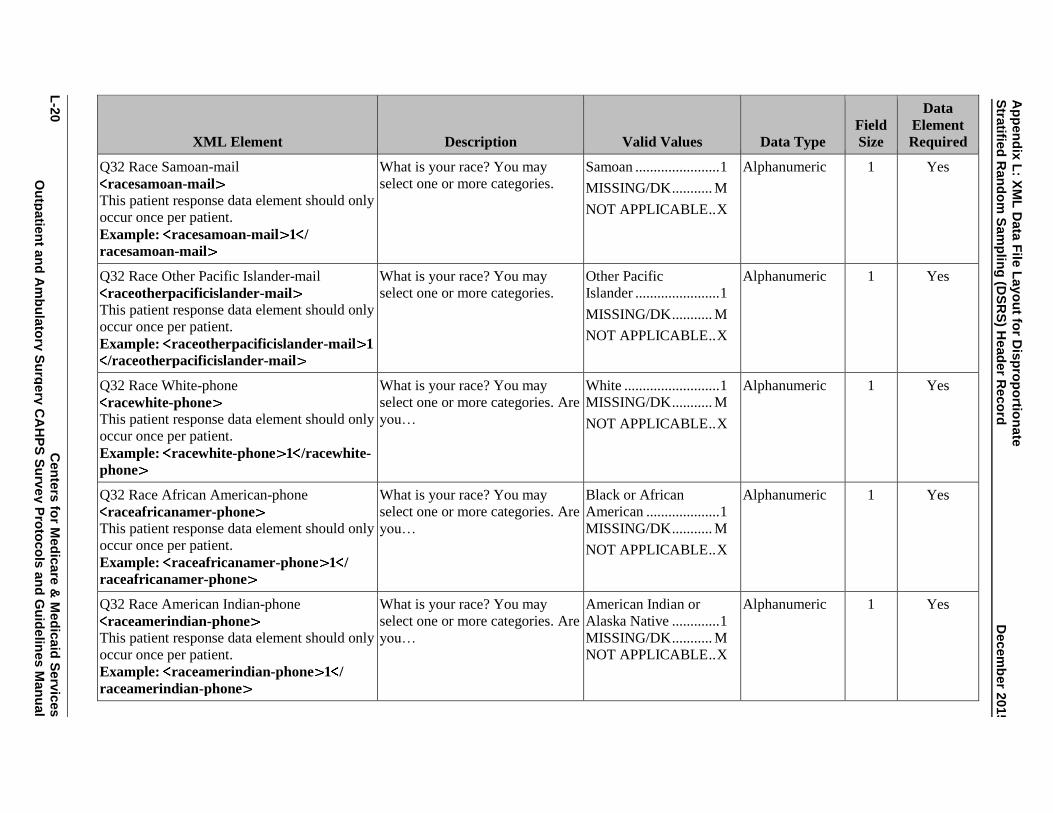
Ap
pen
dix
L: X
ML
Data
File
Layo
ut fo
r Dis
pro
po
rtion
ate
Stra
tified
Ran
do
m S
am
plin
g (D
SR
S) H
ead
er R
eco
rd
Decem
ber 2
01
5
L-2
0
Cen
ters
for M
ed
ica
re &
Med
icaid
Se
rvic
es
Ou
tpatie
nt a
nd
Am
bu
lato
ry S
urg
ery
CA
HP
S S
urv
ey P
roto
co
ls a
nd
Gu
ide
lines M
an
ual
XML Element Description Valid Values Data Type Field
Size
Data
Element
Required
Q32 Race Samoan-mail
racesamoan-mail This patient response data element should only
occur once per patient.
Example: racesamoan-mail 1 /
racesamoan-mail
What is your race? You may
select one or more categories.
Samoan ....................... 1
MISSING/DK ........... M
NOT APPLICABLE .. X
Alphanumeric 1 Yes
Q32 Race Other Pacific Islander-mail
raceotherpacificislander-mail This patient response data element should only
occur once per patient.
Example: raceotherpacificislander-mail 1
/raceotherpacificislander-mail
What is your race? You may
select one or more categories.
Other Pacific
Islander ....................... 1
MISSING/DK ........... M
NOT APPLICABLE .. X
Alphanumeric 1 Yes
Q32 Race White-phone
racewhite-phone This patient response data element should only
occur once per patient.
Example: racewhite-phone 1 /racewhite-
phone
What is your race? You may
select one or more categories. Are
you…
White .......................... 1
MISSING/DK ........... M
NOT APPLICABLE .. X
Alphanumeric 1 Yes
Q32 Race African American-phone
raceafricanamer-phone
This patient response data element should only
occur once per patient.
Example: raceafricanamer-phone 1 /
raceafricanamer-phone
What is your race? You may
select one or more categories. Are
you…
Black or African
American .................... 1
MISSING/DK ........... M
NOT APPLICABLE .. X
Alphanumeric 1 Yes
Q32 Race American Indian-phone
raceamerindian-phone
This patient response data element should only
occur once per patient.
Example: raceamerindian-phone 1 /
raceamerindian-phone
What is your race? You may
select one or more categories. Are
you…
American Indian or
Alaska Native ............. 1
MISSING/DK ........... M
NOT APPLICABLE .. X
Alphanumeric 1 Yes
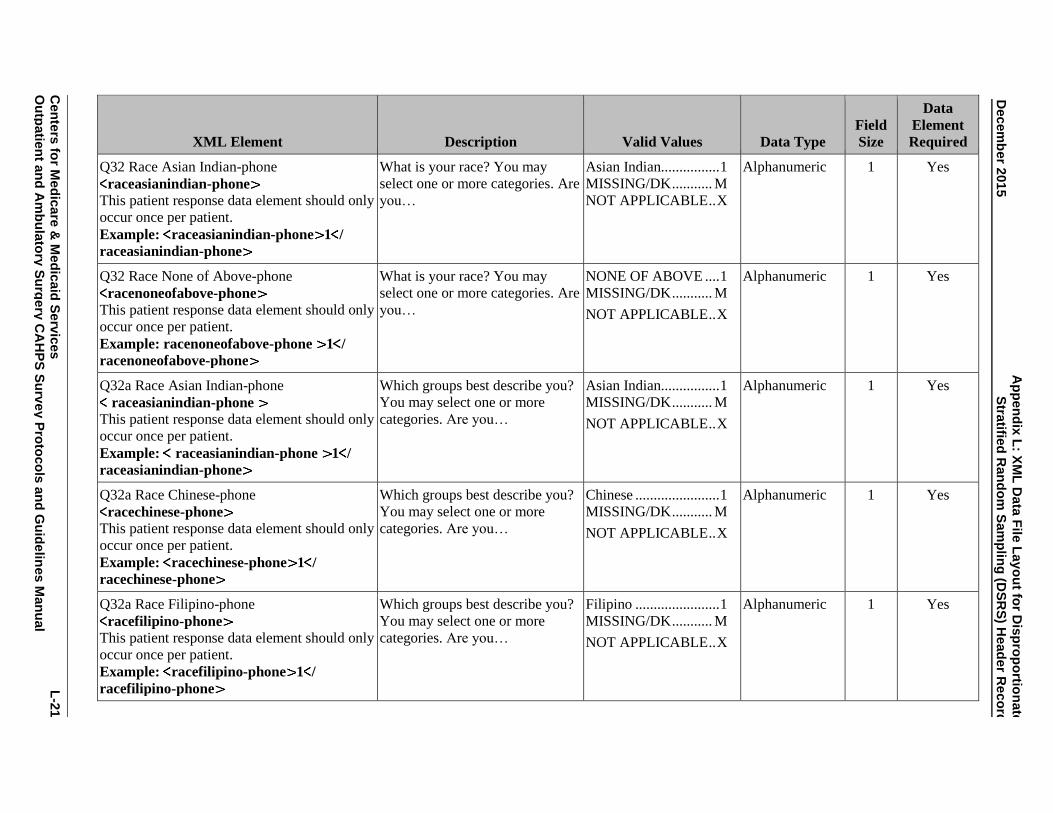
A
pp
en
dix
L: X
ML
Data
File
Layo
ut fo
r Dis
pro
po
rtion
ate
Decem
ber 2
01
5
Stra
tified
Ran
do
m S
am
plin
g (D
SR
S) H
ead
er R
eco
rd
Cen
ters
for M
ed
ica
re &
Med
icaid
Se
rvic
es
L
-21
Ou
tpatie
nt a
nd
Am
bu
lato
ry S
urg
ery
CA
HP
S S
urv
ey P
roto
co
ls a
nd
Gu
ide
lines M
an
ual
XML Element Description Valid Values Data Type Field
Size
Data
Element
Required
Q32 Race Asian Indian-phone
raceasianindian-phone
This patient response data element should only
occur once per patient.
Example: raceasianindian-phone 1 /
raceasianindian-phone
What is your race? You may
select one or more categories. Are
you…
Asian Indian................ 1
MISSING/DK ........... M
NOT APPLICABLE .. X
Alphanumeric 1 Yes
Q32 Race None of Above-phone
racenoneofabove-phone
This patient response data element should only
occur once per patient.
Example: racenoneofabove-phone 1 / racenoneofabove-phone
What is your race? You may
select one or more categories. Are
you…
NONE OF ABOVE .... 1
MISSING/DK ........... M
NOT APPLICABLE .. X
Alphanumeric 1 Yes
Q32a Race Asian Indian-phone
raceasianindian-phone
This patient response data element should only
occur once per patient.
Example: raceasianindian-phone 1 / raceasianindian-phone
Which groups best describe you?
You may select one or more
categories. Are you…
Asian Indian................ 1
MISSING/DK ........... M
NOT APPLICABLE .. X
Alphanumeric 1 Yes
Q32a Race Chinese-phone
racechinese-phone
This patient response data element should only
occur once per patient.
Example: racechinese-phone 1 /
racechinese-phone
Which groups best describe you?
You may select one or more
categories. Are you…
Chinese ....................... 1
MISSING/DK ........... M
NOT APPLICABLE .. X
Alphanumeric 1 Yes
Q32a Race Filipino-phone
racefilipino-phone
This patient response data element should only
occur once per patient.
Example: racefilipino-phone 1 /
racefilipino-phone
Which groups best describe you?
You may select one or more
categories. Are you…
Filipino ....................... 1
MISSING/DK ........... M
NOT APPLICABLE .. X
Alphanumeric 1 Yes

Ap
pen
dix
L: X
ML
Data
File
Layo
ut fo
r Dis
pro
po
rtion
ate
Stra
tified
Ran
do
m S
am
plin
g (D
SR
S) H
ead
er R
eco
rd
Decem
ber 2
01
5
L-2
2
Cen
ters
for M
ed
ica
re &
Med
icaid
Se
rvic
es
Ou
tpatie
nt a
nd
Am
bu
lato
ry S
urg
ery
CA
HP
S S
urv
ey P
roto
co
ls a
nd
Gu
ide
lines M
an
ual
XML Element Description Valid Values Data Type Field
Size
Data
Element
Required
Q32a Race Japanese-phone
racejapanese-phone
This patient response data element should only
occur once per patient.
Example: racejapanese-phone 1 /
racejapanese-phone
Which groups best describe you?
You may select one or more
categories. Are you…
Japanese ...................... 1
MISSING/DK ........... M
NOT APPLICABLE .. X
Alphanumeric 1 Yes
Q32a Race Korean-phone
racekorean-phone
This patient response data element should only
occur once per patient.
Example: racekorean-phone 1 /
racekorean-phone
Which groups best describe you?
You may select one or more
categories. Are you…
Korean ........................ 1
MISSING/DK ........... M
NOT APPLICABLE .. X
Alphanumeric 1 Yes
Q32a Race Vietnamese-phone
racevietnamese-phone
This patient response data element should only
occur once per patient.
Example: racevietnamese-phone 1 /
racevietnamese-phone
Which groups best describe you?
You may select one or more
categories. Are you…
Vietnamese ................. 1
MISSING/DK ........... M
NOT APPLICABLE .. X
Alphanumeric 1 Yes
Q32a Race Other Asian-phone
raceotherasian-phone
This patient response data element should only
occur once per patient.
Example: raceotherasian-phone 1 /
raceotherasian-phone
Which groups best describe you?
You may select one or more
categories. Are you…
Other Asian ................. 1
MISSING/DK ........... M
NOT APPLICABLE .. X
Alphanumeric 1 Yes

A
pp
en
dix
L: X
ML
Data
File
Layo
ut fo
r Dis
pro
po
rtion
ate
Decem
ber 2
01
5
Stra
tified
Ran
do
m S
am
plin
g (D
SR
S) H
ead
er R
eco
rd
Cen
ters
for M
ed
ica
re &
Med
icaid
Se
rvic
es
L
-23
Ou
tpatie
nt a
nd
Am
bu
lato
ry S
urg
ery
CA
HP
S S
urv
ey P
roto
co
ls a
nd
Gu
ide
lines M
an
ual
XML Element Description Valid Values Data Type Field
Size
Data
Element
Required
Q32a Race None of Above Asian Indian-
phone
racenoneofaboveasianindian-phone
This patient response data element should only
occur once per patient.
Example: racenoneofaboveasianindian-
phone 1 / racenoneofaboveasianindian-
phone
Which groups best describe you?
You may select one or more
categories. Are you…
NONE OF ABOVE .... 1
MISSING/DK ........... M
NOT APPLICABLE .. X
Alphanumeric 1 Yes
Q32b Race Native Hawaiian-phone
racenativehawaiian-phone
This patient response data element should only
occur once per patient.
Example: racenativehawaiian-phone 1 /
racenativehawaiian-phone
Which groups best describe you?
You may select one or more
categories. Are you…
Native Hawaiian ......... 1
MISSING/DK ........... M
NOT APPLICABLE .. X
Alphanumeric 1 Yes
Q32b Race Guamanian Chamorro-phone
raceguamanianchamorro-phone
This patient response data element should only
occur once per patient.
Example: raceguamanianchamorro-phone
1 /raceguamanianchamorro-phone
Which groups best describe you?
You may select one or more
categories. Are you…
Guamanian or
Chamorro .................... 1
MISSING/DK ........... M
NOT APPLICABLE .. X
Alphanumeric 1 Yes
Q32b Race Samoan-phone
racesamoan-phone
This patient response data element should only
occur once per patient.
Example: racesamoan-phone 1 /
racesamoan-phone
Which groups best describe you?
You may select one or more
categories. Are you…
Samoan ....................... 1
MISSING/DK ........... M
NOT APPLICABLE .. X
Alphanumeric 1 Yes

Ap
pen
dix
L: X
ML
Data
File
Layo
ut fo
r Dis
pro
po
rtion
ate
Stra
tified
Ran
do
m S
am
plin
g (D
SR
S) H
ead
er R
eco
rd
Decem
ber 2
01
5
L-2
4
Cen
ters
for M
ed
ica
re &
Med
icaid
Se
rvic
es
Ou
tpatie
nt a
nd
Am
bu
lato
ry S
urg
ery
CA
HP
S S
urv
ey P
roto
co
ls a
nd
Gu
ide
lines M
an
ual
XML Element Description Valid Values Data Type Field
Size
Data
Element
Required
Q32b Race Other Pacific Islander-phone
raceotherpacificislander-phone
This patient response data element should only
occur once per patient.
Example: raceotherpacificislander-phone
1 /raceotherpacificislander-phone
Which groups best describe you?
You may select one or more
categories. Are you…
Other Pacific
Islander ....................... 1
MISSING/DK ........... M
NOT APPLICABLE .. X
Alphanumeric 1 Yes
Q32b Race None of Above Pacific-phone
racenoneofabovepacific-phone
This patient response data element should only
occur once per patient.
Example: racenoneofabovepacific-phone 1
/racenoneofabovepacific-phone
Which groups best describe you?
You may select one or more
categories. Are you…
NONE OF ABOVE .... 1
MISSING/DK ........... M
NOT APPLICABLE .. X
Alphanumeric 1 Yes
Q33 Speak English
speakenglish This patient response data element should only
occur once per patient.
Example: speakenglish 1 /speakenglish
How well do you speak English? Very well .................... 1
Well ............................ 2
Not well ...................... 3
Not at all ..................... 4
MISSING/DK ........... M
Alphanumeric 1 Yes
Q34 Speak Other
speakother This patient response data element should only
occur once per patient.
Example: speakother 1 /speakother
Do you speak a language other
than English at home?
Yes, speak language
other than English ....... 1
No, speak English at
home ........................... 2
MISSING/DK ........... M
Alphanumeric 1 Yes
Q35 Speak Other Specify
speakotherspecify This patient response data element should only
occur once per patient.
Example: speakotherspecify 1 /
speakotherspecify
What is that language? Spanish ....................... 1
Other ........................... 2
MISSING/DK ........... M
NOT APPLICABLE .. X
Alphanumeric 1 Yes

A
pp
en
dix
L: X
ML
Data
File
Layo
ut fo
r Dis
pro
po
rtion
ate
Decem
ber 2
01
5
Stra
tified
Ran
do
m S
am
plin
g (D
SR
S) H
ead
er R
eco
rd
Cen
ters
for M
ed
ica
re &
Med
icaid
Se
rvic
es
L
-25
Ou
tpatie
nt a
nd
Am
bu
lato
ry S
urg
ery
CA
HP
S S
urv
ey P
roto
co
ls a
nd
Gu
ide
lines M
an
ual
XML Element Description Valid Values Data Type Field
Size
Data
Element
Required
Q36 Help-mail
help This patient response data element should only
occur once per patient.
Example: help 1 /help
Did someone help you complete
this survey?
Yes .............................. 1
No ............................... 2
MISSING/DK ........... M
NOT APPLICABLE .. X
Alphanumeric 1 Yes
Q37 Help Read-mail
helpread This patient response data element should only
occur once per patient.
Example: helpread 1 /helpread
How did that person help you?
Check all that apply.
Read the questions
to me ........................... 1
MISSING/DK ........... M
NOT APPLICABLE .. X
Alphanumeric 1 Yes
Q37 Help Wrote-mail
helpwrote This patient response data element should only
occur once per patient.
Example: helpwrote 1 /helpwrote
How did that person help you?
Check all that apply.
Wrote down the
answers I gave ............ 1
MISSING/DK ........... M
NOT APPLICABLE .. X
Alphanumeric 1 Yes
Q37 Help Answer-mail
helpanswer This patient response data element should only
occur once per patient.
Example: helpanswer 1 /helpanswer
How did that person help you?
Check all that apply.
Answered the
questions for me ......... 1
MISSING/DK ........... M
NOT APPLICABLE .. X
Alphanumeric 1 Yes
Q37 Help Translate-mail
helptranslate This patient response data element should only
occur once per patient.
Example: helptranslate 1 /
helptranslate
How did that person help you?
Check all that apply.
Translated the
questions into my
language ...................... 1
MISSING/DK ........... M
NOT APPLICABLE .. X
Alphanumeric 1 Yes
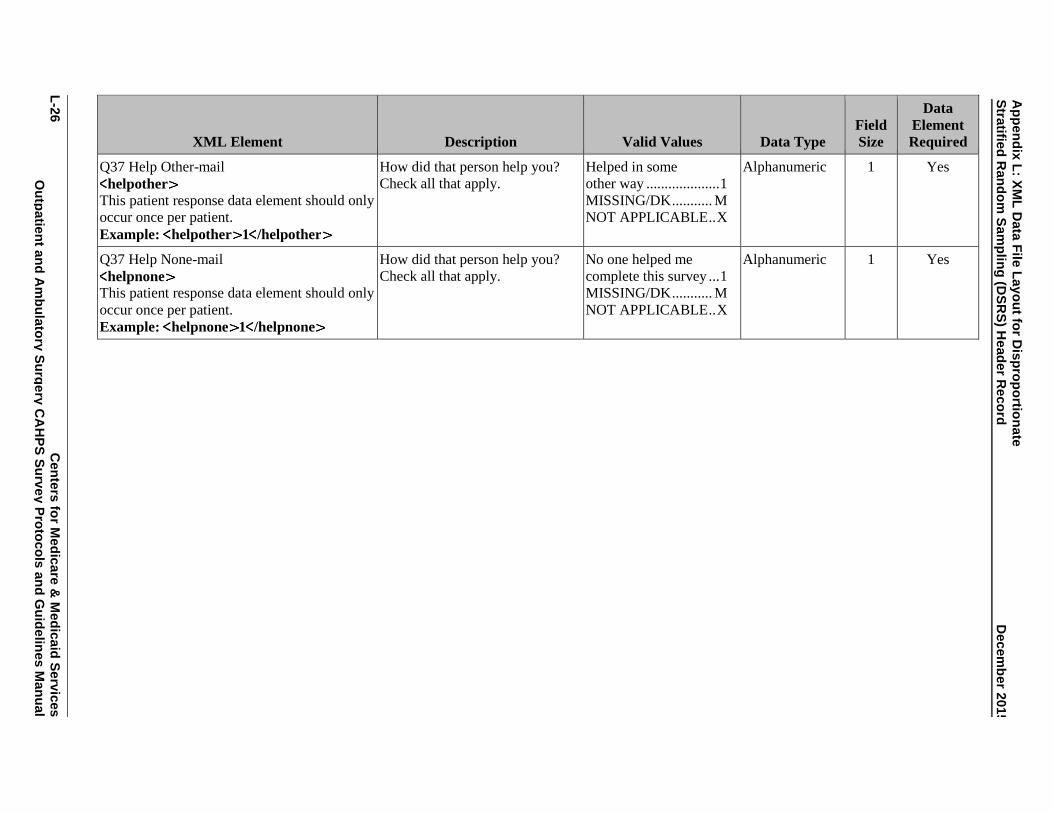
Ap
pen
dix
L: X
ML
Data
File
Layo
ut fo
r Dis
pro
po
rtion
ate
Stra
tified
Ran
do
m S
am
plin
g (D
SR
S) H
ead
er R
eco
rd
Decem
ber 2
01
5
L-2
6
Cen
ters
for M
ed
ica
re &
Med
icaid
Se
rvic
es
Ou
tpatie
nt a
nd
Am
bu
lato
ry S
urg
ery
CA
HP
S S
urv
ey P
roto
co
ls a
nd
Gu
ide
lines M
an
ual
XML Element Description Valid Values Data Type Field
Size
Data
Element
Required
Q37 Help Other-mail
helpother This patient response data element should only
occur once per patient.
Example: helpother 1 /helpother
How did that person help you?
Check all that apply.
Helped in some
other way .................... 1
MISSING/DK ........... M
NOT APPLICABLE .. X
Alphanumeric 1 Yes
Q37 Help None-mail
helpnone This patient response data element should only
occur once per patient.
Example: helpnone 1 /helpnone
How did that person help you?
Check all that apply.
No one helped me
complete this survey ... 1
MISSING/DK ........... M
NOT APPLICABLE .. X
Alphanumeric 1 Yes

Centers for Medicare & Medicaid Services Outpatient and Ambulatory Surgery CAHPS Survey Protocols and Guidelines Manual
APPENDIX M:
XML DATA FILE LAYOUT FOR ZERO SAMPLED FILE

Appendix M: XML Data File Layout for Zero Sampled File December 2015
Centers for Medicare & Medicaid Services Outpatient and Ambulatory Surgery CAHPS Survey Protocols and Guidelines Manual
This page intentionally left blank.

Cen
ters
for M
ed
ica
re &
Med
icaid
Se
rvic
es
M
-1
Ou
tpatie
nt a
nd
Am
bu
lato
ry S
urg
ery
CA
HP
S S
urv
ey P
roto
co
ls a
nd
Gu
ide
lines M
an
ual
ZERO FILE SAMPLED XML DATA FILE LAYOUT
OUTPATIENT AND AMBULATORY CAHPS SURVEY
HEADER RECORD
The following section defines the format of the header record.
NOTE: Each element must have a closing tag that is the same as the opening tag but with a forward slash. Data element names do not contain
any spaces, underscores, or capital letters.
XML Element Description Valid Values Data Type Field
Size
Data
Element
Required
Type of Header Record
headertype
This header element should only occur once
per file.
Example: headertype 1 /headertype
Type of Header Record 1 = Standard Header
Record
Numeric 1 Yes
Provider Name
<providername
This header element should only occur once
per file.
Example: providername
SampleHOPDASCName /providername
This is the HOPD’s or ASC’s
Provider Name
— Alphanumeric 100 Yes
Provider Number
providernum
This header element will occur again as an
administration data element in the patient level
data record.
Example: providernum 123456 /
providernum
This is the HOPD’s or ASC’s
CMS Certification Number
(CCN, formerly known as the
Medicare Provider ID Number)
No Dashes or spaces
Valid 6- or 10-digit CMS
Certification Number
(CCN)
Alphanumeric 10 Yes

Ap
pen
dix
M: X
ML
Data
File
Layo
ut fo
r Ze
ro S
am
ple
d F
ile
Decem
ber 2
01
5
M-2
C
en
ters
for M
ed
ica
re &
Med
icaid
Se
rvic
es
Ou
tpatie
nt a
nd
Am
bu
lato
ry S
urg
ery
CA
HP
S S
urv
ey P
roto
co
ls a
nd
Gu
ide
lines M
an
ual
XML Element Description Valid Values Data Type Field
Size
Data
Element
Required
Sample Month
samplemonth This header element will occur again as an
administration data element in the patient level
data record.
Example: samplemonth 12 /
samplemonth
Survey vendors will select a
sample of patients who meet
survey eligibility criteria for each
calendar month. The Sample
Month is the month for which the
sample was selected.
MM
(1 – 12 = January –
December)
Numeric 2 Yes
Sample Year
sampleyear This header element will occur again as an
administration data element in the patient level
data record.
Example: sampleyear 2016 /
sampleyear
This is the calendar year in which
the survey is conducted.
YYYY
(2016 or greater)
Numeric 4 Yes
Survey Mode
surveymode
This header element will occur again as an
administration data element in the patient level
data record.
Example: surveymode 1 /surveymode
The survey mode, either mail
only, phone only, or mixed mode,
must be the same for all sample
members in each sample month in
the calendar quarter for all of the
HOPD or ASC locations under
the same CCN.
1 = Mail only
2 = Telephone only
3 = Mixed mode
Numeric 1 Yes
Type of Sampling
sampletype
This header element should only occur once
per file.
Example: sampletype 1 /sampletype
Type of sampling used. Note:
Sample Type must be the same
for all three months in each
quarter.
1 = Census
2 = Simple random
sampling
3 = Stratified systematic
sampling
4 = Proportionate
Stratified Random
sampling
5 = DSRS
Numeric 1 Yes
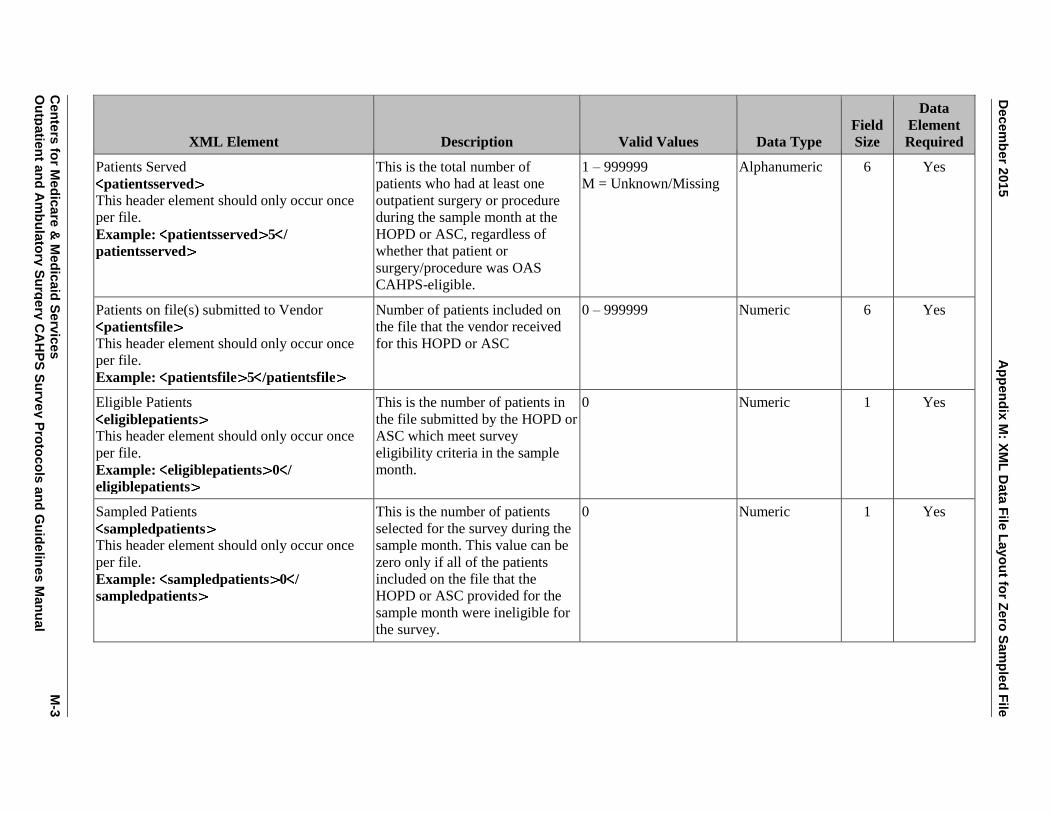
Decem
ber 2
01
5
Ap
pen
dix
M: X
ML
Data
File
Layo
ut fo
r Ze
ro S
am
ple
d F
ile
Cen
ters
for M
ed
ica
re &
Med
icaid
Se
rvic
es
M
-3
Ou
tpatie
nt a
nd
Am
bu
lato
ry S
urg
ery
CA
HP
S S
urv
ey P
roto
co
ls a
nd
Gu
ide
lines M
an
ual
XML Element Description Valid Values Data Type Field
Size
Data
Element
Required
Patients Served
patientsserved
This header element should only occur once
per file.
Example: patientsserved 5 /
patientsserved
This is the total number of
patients who had at least one
outpatient surgery or procedure
during the sample month at the
HOPD or ASC, regardless of
whether that patient or
surgery/procedure was OAS
CAHPS-eligible.
1 – 999999
M = Unknown/Missing
Alphanumeric 6 Yes
Patients on file(s) submitted to Vendor
patientsfile
This header element should only occur once
per file.
Example: patientsfile 5 /patientsfile
Number of patients included on
the file that the vendor received
for this HOPD or ASC
0 – 999999 Numeric 6 Yes
Eligible Patients
eligiblepatients
This header element should only occur once
per file.
Example: eligiblepatients 0 /
eligiblepatients
This is the number of patients in
the file submitted by the HOPD or
ASC which meet survey
eligibility criteria in the sample
month.
0 Numeric 1 Yes
Sampled Patients
sampledpatients
This header element should only occur once
per file.
Example: sampledpatients 0 /
sampledpatients
This is the number of patients
selected for the survey during the
sample month. This value can be
zero only if all of the patients
included on the file that the
HOPD or ASC provided for the
sample month were ineligible for
the survey.
0 Numeric 1 Yes

Appendix M: XML Data File Layout for Zero Sampled File December 2015
M-4 Centers for Medicare & Medicaid Services Outpatient and Ambulatory Surgery CAHPS Survey Protocols and Guidelines Manual
This page intentionally left blank.

Centers for Medicare & Medicaid Services Outpatient and Ambulatory Surgery CAHPS Survey Protocols and Guidelines Manual
APPENDIX N:
INSTRUCTIONS FOR PREPARING A SURVEY VENDOR QUALITY
ASSURANCE PLAN

Appendix N: Instructions for Preparing a Survey Vendor Quality Assurance Plan December 2015
Centers for Medicare & Medicaid Services Outpatient and Ambulatory Surgery CAHPS Survey Protocols and Guidelines Manual
This page intentionally left blank.
December 2015 Appendix N: Instructions for Preparing a Survey Vendor Quality Assurance Plan
Centers for Medicare & Medicaid Services N-1 Outpatient and Ambulatory Surgery CAHPS Survey Protocols and Guidelines Manual
INSTRUCTIONS FOR PREPARING A SURVEY VENDOR QUALITY ASSURANCE PLAN
Introduction: OAS CAHPS is a CMS-sponsored standardized survey instrument and data
collection methodology for measuring patients’ perspectives on patient care received in HOPDs
and ASCs. OAS CAHPS data provides the public with comparative information on HOPDs and
ASCs and supports quality-related activities. (A definition of HOPD and ASC can be found in
Chapter II – Introduction and Background.) Like other CAHPS programs, HOPDs and ASCs
conducting OAS CAHPS contract with survey vendors to conduct data collection on their behalf.
Survey data collection can be completed using one of three modes: mail only, telephone only, or
mixed mode (mail with telephone follow-up).
Survey vendors must meet minimum business requirements posted on the OAS CAHPS website
to become an OAS CAHPS vendor. These requirements include having experience conducting
surveys and drawing statistical samples; possessing facilities and systems for survey operations;
conducting all survey operations in the United States; and adhering to security and
confidentiality procedures. Survey vendors meeting these minimum requirements will receive
interim approval once they have (1) submitted their online vendor application, (2) satisfactorily
answered follow-up questions about their application from the OAS CAHPS Survey
Coordination Team and received CMS approval, (3) participated in the Introduction to the OAS
CAHPS Survey training session, and (4) successfully completed a written Training Certification
Form. With interim approval, vendors can begin conducting OAS CAHPS on behalf of client
facilities. To become fully approved, vendors must complete the final step in the approval
process: the submission of an acceptable Quality Assurance Plan (QAP). The QAP must be
submitted within 6 weeks of the data submission deadline date after vendor’s first quarterly
submission of OAS CAHPS data. It must be updated and resubmitted annually on or before April
30 and whenever the survey vendor makes key staff or protocol changes.
This purpose of this document is to serve as instructions for survey vendors to help them develop
a QAP that describes their specific plans for implementation and compliance with all guidelines
required to implement the OAS CAHPS Survey.
The vendor’s QAP should include the sections listed below. The specific requirements for these
sections are described in the pages that follow.
I. Organization Background and Staff Experience
II. Identifying and Recruiting HOPDs and ASCs
III. Work Plan for Each Mode of Data Collection
IV. Sampling Plan

Appendix N: Instructions for Preparing a Survey Vendor Quality Assurance Plan December 2015
N-2 Centers for Medicare & Medicaid Services Outpatient and Ambulatory Surgery CAHPS Survey Protocols and Guidelines Manual
V. Survey Implementation Plan
VI. Data Security, Confidentiality, and Privacy Plan
VII. Exceptions Request Process and Discrepancy Notification Reporting
VIII. Questionnaire and Materials Attachments
To facilitate review of the QAP, each vendor should use the outline format noted above.
I. ORGANIZATION BACKGROUND AND STAFF EXPERIENCE
In this section of the QAP, each OAS CAHPS Survey vendor must provide the following
information:
• Your organization’s name, address, and telephone number. If your organization has multiple
locations, include the address of both the main location and the address of the locations at
which the primary operations, including sampling, data collection, and data processing
activities, are being conducted.
• Describe the history and affiliation with any other organization (e.g., other company or
university affiliation). Include the scope of business, number of years in business, and
number of years of survey experience.
• Describe your organization’s survey experience conducting person-level surveys using each
approved data collection mode that is allowed for the OAS CAHPS Survey, specifically,
mail-only, CATI-only, and mixed mode (mail with CATI follow-up). Describe other CAHPS
survey experience if you have it. You must discuss each data collection mode for which you
have received approval, regardless of whether you have any HOPD or ASC clients who are
using that mode.
• Provide an organizational chart that shows the names and titles of staff members, including
subcontractors, who are responsible for each of the following tasks:
a. Overall project management, including tracking and supervision of all tasks below.
b. Explaining the nature of the project to hospitals and ASCs, including determining
whether their facility is eligible.
c. Sampling procedures, including creation of the sample frame, selection of the sample,
and assignment of a unique identification number to each sampled patient.
d. Data collection procedures, including overseeing implementation of the data collection
mode for which your organization has been approved.

December 2015 Appendix N: Instructions for Preparing a Survey Vendor Quality Assurance Plan
Centers for Medicare & Medicaid Services N-3 Outpatient and Ambulatory Surgery CAHPS Survey Protocols and Guidelines Manual
e. Data receipt and data entry/scanning procedures.
f. File development and submission processes.
The organizational chart should also clearly specify all staff reporting relationships, including
those staff who are responsible for managing subcontractors. It should designate any
individuals who have quality assurance oversight responsibility and indicate which tasks they
are responsible for.
• Summarize the background and experience of the individuals who are responsible for the
tasks listed in the organizational chart above, including a description of any subcontractors
serving in these roles. The description of each individual’s experience should include a
discussion of how the person’s qualifications are relevant to the OAS CAHPS Survey tasks
that he or she is expected to perform. Resumes should be available upon request.
II. IDENTIFYING AND RECRUITING HOPDS AND ASCS
• Describe your process for identifying hospitals and ASCs whom you will attempt to contract
for OAS CAHPS. Clarify if you contact only those institutions with whom you already have
a relationship, or if you also contact institutions you have not worked with previously.
• When working with hospitals to explain the study, how do you determine whether a
particular hospital has one or more eligible HOPDs? What questions do hospitals have and
how do you address these questions?
• When working with ASCs to explain the study, how do you determine which facilities or
sites within their institution are eligible? What questions do ASCs have and how do you
address these questions?
III. WORK PLAN
• Describe how your organization is implementing the OAS CAHPS Survey for each mode for
which your organization has been approved. This section of your QAP must describe the
entire process that your organization is following, including:
a. how you are obtaining the sample frame and selecting the sample;
b. how you are fielding the survey, receiving and processing the data;
c. the procedures that you are following to prepare and submit final files; and
d. the type of quality control procedures you are following at each stage to ensure data
quality.

Appendix N: Instructions for Preparing a Survey Vendor Quality Assurance Plan December 2015
N-4 Centers for Medicare & Medicaid Services Outpatient and Ambulatory Surgery CAHPS Survey Protocols and Guidelines Manual
• For each step above, you must specify the name of the individual who is responsible for
conducting and providing oversight of each specific activity.
• Include a copy of a schedule or timeline that you are following to ensure that you are able to
conduct all activities within the timeframes specified in the OAS CAHPS Survey protocols.
The timeline must describe when that activity will be completed (for example, x weeks after
sample selection, or y weeks after mailing the first questionnaire). The timeline must include
receipt of files from HOPDs and ASCs, sample selection, each step of the mailout or
telephone implementation, data file cleaning, and data file preparation and submission.
IV. SAMPLING PLAN
• Describe how you are working with your client facilities to ensure that the HOPDs and ASCs
understand patient survey eligibility criteria and the measures you take to ensure that all
patient information needed for sample selection is included on the file that is submitted and
that the monthly patient files are submitted in time for you to select the sample and initiate
the survey within 21 days after the sample month ends.
• Describe how HOPDs or ASCs submit the monthly patient files to your organization and
how you check those files. That is, describe the steps that you take to ensure that the ASC or
HOPD has included all required data on the monthly patient files and the checks you make to
ensure that the same patient information is not included more than once on the monthly
patient information file. Describe how the transmission is done to ensure security of these
HIPAA data.
• Describe how you create the sample frame. This section should describe the process you are
using to develop a sampling frame that complies with the OAS CAHPS Survey protocol.
Specifically, you must explain how you are creating the frame, what patient survey eligibility
criteria you are using, and the types of patients who are being excluded and how those cases
are being identified. Please make sure your QAP addresses each of the following questions:
a. How do you check monthly patient information files to determine if any required data for
a patients is incomplete?
b. What do you do if information is missing from the monthly patient information files?
c. What are the eligibility and exclusion criteria that you use to determine which patients are
eligible and which patients should be excluded from the sample frame? Refer to
Chapter IV, Sampling Procedures – Patient Eligibility Criteria.
d. How do you know whether your client HOPDs and ASCS have included all patients on
the monthly patient files? Do you obtain and retain documentation from the HOPDs and

December 2015 Appendix N: Instructions for Preparing a Survey Vendor Quality Assurance Plan
Centers for Medicare & Medicaid Services N-5 Outpatient and Ambulatory Surgery CAHPS Survey Protocols and Guidelines Manual
ASCs about who was excluded and the reasons those patients were excluded from the
monthly patient information files?
e. How do you know whether all eligible ASCs within the CCN, or all eligible HOPDs
within the CCN, are submitting patient files?
f. Do you check the monthly patient information files to ensure that patients are only listed
once on the file? If so, what information and process do you use to identify and remove
patients who may have been listed on the monthly patient information file more than
once?
g. What process (system or procedures) do you use to identify and remove patients who
have been included in the survey sample in the last 5 months?
h. What process (system, software, or procedure) do you use to assign a unique patient
identification number to each sample patient?
i. OAS CAHPS Survey vendors are expected to calculate and use a sample rate for each
ASC and HOPD client to ensure that an even distribution of patients is sampled over a
12-month period. How do you determine a sample rate for each ASC and HOPD?
j. How is the sample selected? What software program do you use to generate the seed
number and assign random numbers used for sampling?
k. What documentation about sample frame creation do you retain and for how long?
l. If the ASC or HOPD is also conducting other patient experience surveys, what
procedures do you follow to ensure that the sample for OAS CAHPS is selected first, and
is a random selection that is representative of the monthly patient records?
• Describe the quality control checks that you are performing on the sampling activities, how
frequently those checks are being performed, and by whom. Indicate what percentage of the
sample frame or sample file is being checked, and describe the documentation that you
maintain to verify that the quality control procedures have taken place. Note that this
documentation may be requested by the OAS CAHPS Survey Coordination Team at any
time.
• If applicable, describe any sampling exceptions that you have requested or for which your
firm has been approved. Explain the exceptions request and the specific procedures you are
or will be following to implement the approved exception.

Appendix N: Instructions for Preparing a Survey Vendor Quality Assurance Plan December 2015
N-6 Centers for Medicare & Medicaid Services Outpatient and Ambulatory Surgery CAHPS Survey Protocols and Guidelines Manual
V. SURVEY IMPLEMENTATION PLAN
• Describe the system resources that you are using to implement your approved survey
mode(s). This includes a description of the relevant hardware or software. For example,
describe the electronic telephone interviewing systems, mailing equipment, scanning or data
entry equipment, and case management system that you are using.
• Describe training that is being given to all staff working on the OAS CAHPS Survey project,
including telephone interviewers (if applicable), mail survey production staff, and data
receipt/data processing/data entry staffs. If you are using any subcontractors for any roles,
describe how the subcontractor’s staff are being trained. Include a discussion of quality
control procedures that you or your subcontractor are implementing during training to ensure
compliance with OAS CAHPS Survey protocols. Describe the documentation that is being
kept to provide evidence of this quality control.
• Describe the toll-free customer support telephone line that you are offering, including the
actual telephone number, how customer support staff are being trained, and who is
responsible for training and responding to questions related to the OAS CAHPS Survey. Also
include information on the days of the week and times of the day that you are staffing the
customer support line and how you are handling after-hours contacts, and include text of any
recordings that are being used. Include a discussion of quality control procedures that are
being implemented to ensure compliance with OAS CAHPS Survey protocols and describe
documentation that is being kept to provide evidence of this quality control. (Reference
chapter VI of this manual.)
• Describe the production and mailout process for mail surveys, if applicable, including who is
responsible for the process and what quality control checks are being implemented at each
stage (for example, monitoring the quality and content of mail survey packages, use of
seeded mailings, and frequency of checks). Describe all quality control checks that are being
implemented and documented to ensure that the OAS CAHPS Survey protocols are being
followed. (Reference chapter V of this manual.)
• Describe the receipt and data entry or scanning process for mail surveys, if applicable,
including who is responsible for the process and what quality control checks are being
implemented at the questionnaire receipt, data entry, or scanning phase, and how frequently
those checks are being made. Describe all quality control checks that are being implemented
and documented to ensure that the OAS CAHPS Survey protocols are being followed.
(Reference chapter V of this manual.)
• Describe the process for implementing the telephone survey, if applicable, including who is
responsible for training and monitoring interviewer performance, how training and
monitoring are being documented, and what systems and procedures are being used to ensure

December 2015 Appendix N: Instructions for Preparing a Survey Vendor Quality Assurance Plan
Centers for Medicare & Medicaid Services N-7 Outpatient and Ambulatory Surgery CAHPS Survey Protocols and Guidelines Manual
that all interviewing is conducted according to the OAS CAHPS Survey protocols (for
example, varying times of day that calls are attempted and tracking the status of call
attempts). If you are using a telephone survey subcontractor, describe oversight activities you
are conducting to ensure that the subcontractor is in compliance with OAS CAHPS Survey
protocols. (Reference chapter VI of this manual.)
• If you are approved for mixed-mode administration, you must address all of the paragraphs
above regarding both mail and telephone processes. In addition, you must include a
discussion of the control system used to monitor case status as the case transitions from the
mail phase of the survey to the telephone follow-up phase. Describe how you keep track of
surveys that are returned while the telephone follow-up phase is in effect. Describe the
processes that you have in place to ensure that sample members who have returned a
completed survey are not called after the completed survey is received. How do you
determine which completed survey to retain (mail or telephone interview data) if the sample
member returns a completed survey and participates in a telephone interview? (Reference
chapter VII of this manual.)
• Describe the processes you are using to create data files and submit them to the OAS CAHPS
Survey Data Center through the OAS CAHPS Survey website. Discuss quality control
checks that are being implemented during file creation, including how these checks are being
documented. (Reference chapter XI of this manual.)
VI. DATA SECURITY, CONFIDENTIALITY, AND PRIVACY PLAN
• Describe the measures that you are taking to ensure data security, including a discussion of
the use of passwords, file encryption, backup systems, and any other measures to ensure the
security of OAS CAHPS Survey data. Describe how often passwords are changed. For both
hardcopy questionnaires and electronic data files, describe how and for how long these
materials will be stored and when and how they will be destroyed. (Reference chapter VIII of
this manual.)
• Describe how individuals will be authorized and de-authorized to access personally
identifiable information (PII). Include information about how confidentiality agreements are
being implemented among vendor staff and any subcontractor staff. Describe how affidavits
of confidentiality are being documented, background checks are being conducted, and
confidentiality training procedures are being implemented. Include a copy of the
confidentiality agreement that is being used as an appendix in your QAP. Describe the
measures that are being taken to protect respondent privacy and ensure compliance with
HIPAA requirements. Include information about how unauthorized individuals are being
prevented from accessing PII and the survey data in physical and electronic format.
(Reference chapter VIII of this manual.)

Appendix N: Instructions for Preparing a Survey Vendor Quality Assurance Plan December 2015
N-8 Centers for Medicare & Medicaid Services Outpatient and Ambulatory Surgery CAHPS Survey Protocols and Guidelines Manual
• If you are approved for telephone surveys, include a screenshot or text indicating the
voluntary nature of the sample member’s participation.
VII. EXCEPTIONS REQUEST PROCESS AND DISCREPANCY NOTIFICATION
REPORTING
• Describe any Exceptions Requests that you have or plan to request or document that you
have none but agree to comply with the process outlined in chapter XV of this manual.
• Document your understanding of the Discrepancy Notification Reporting protocol outlined in
chapter XV of this manual and that you agree to comply with the process.
VIII. QUESTIONNAIRE AND MATERIALS ATTACHMENTS
• Attach a copy of your formatted mail survey questionnaire if you are approved for mail-only
or mixed-mode administration. Be sure to include the cover page and back page.
• If you are approved for telephone-only or mixed-mode administration, attach all screen shots
from your telephone interview program—beginning with the introductory screens and ending
with the last question in the interview. If your interview includes the Consent to Share
Identifying Information question, please include a screen shot of this question as well.
• If you are approved for mail-only or mixed-mode administration, include a copy of your
cover letter(s).

Centers for Medicare & Medicaid Services Outpatient and Ambulatory Surgery CAHPS Survey Protocols and Guidelines Manual
APPENDIX O:
EXCEPTIONS REQUEST FORM

Appendix O: Exceptions Request Form December 2015
Centers for Medicare & Medicaid Services Outpatient and Ambulatory Surgery CAHPS Survey Protocols and Guidelines Manual
This page intentionally left blank.

December 2015 Appendix O: Exceptions Request Form
Centers for Medicare & Medicaid Services O-1 Outpatient and Ambulatory Surgery CAHPS Survey Protocols and Guidelines Manual
OUTPATIENT AND AMBULATORY SURGERY CAHPS SURVEY EXCEPTIONS REQUEST FORM
Use the Exceptions Request Form to report a planned deviation from the standard OAS CAHPS protocols. You may request the same exceptions for multiple Hospital Outpatient Departments (HOPDs) or Ambulatory Surgery Centers (ASCs) with which you contract, if applicable.
To submit this form online, please go to https://oascahps.org/.
I. Exception Request
Please provide today’s date, select an exception request classification, and provide the specific reason for your exception request
1a. Date Submitted _______________________
1b. Exception Request Classification (Select one)
New Exception Request
Update list of applicable HOPDs and ASCs on a previous Exception Request
Update other information on a previous Exception Request
Appeal of denial of a previous Exception Request
1c. Specify Reason for Exception Request:
For example: “We request 5 additional business days to complete the phone attempts for three of our contracted facilities.”
II. Description of Exception Request
2a. Purpose of requested exception (e.g., sampling, data issues).
For example: “The purpose is to allow us to complete the required telephone attempts for three of the facilities for which we collect data. A flu epidemic has spread through our area resulting in many telephone interviewers being unable to work for several days in a row.”
2b. How and when will the exception be implemented?
For example: “Instead of the final calling day being Friday, February 6, 2016, we will continue calling Friday, February 6 through Wednesday, February 11. The extension in the data collection period will allow us to finalize all outstanding phone cases.”
2c. Provide evidence that exception will not affect survey results.
For example: “This procedure will not impact survey results because it only applies to the mail cover letter.” Or “If the extension is granted it will not impact our ability to meet the data submission deadline.”

Appendix O: Exceptions Request Form December 2015
O-2 Centers for Medicare & Medicaid Services Outpatient and Ambulatory Surgery CAHPS Survey Protocols and Guidelines Manual
III. Which HOPDs and ASCs are impacted by this Exception Request?
Vendor should revise the Exception Request if additional facilities (CCNs) need to be added after the initial Exception Request was submitted. If you have multiple CCN numbers, please enter them as a comma-separated list, as shown in the example below. Do not include dashes in the CCN number. After entering your CCN number(s), click on the "Lookup Facility Names" button.
For example: “111111, 222222, 333333, 44C4444444, 55C5555555”
Lookup Facility Names .
To submit this form, visit the Outpatient and Ambulatory Surgery CAHPS Survey website at https://oascahps.org/. If you have any problems completing the online Exceptions Request Form, please e-mail the OAS CAHPS Survey Coordination Team at [email protected] for assistance.
Centers for Medicare & Medicaid Services Outpatient and Ambulatory Surgery CAHPS Survey Protocols and Guidelines Manual
APPENDIX P:
DISCREPANCY NOTIFICATION REPORT

Appendix P: Discrepancy Notification Report December 2015
Centers for Medicare & Medicaid Services Outpatient and Ambulatory Surgery CAHPS Survey Protocols and Guidelines Manual
This page intentionally left blank.

December 2015 Appendix P: Discrepancy Notification Report
Centers for Medicare & Medicaid Services P-1 Outpatient and Ambulatory Surgery CAHPS Survey Protocols and Guidelines Manual
OUTPATIENT AND AMBULATORY SURGERY CAHPS SURVEY DISCREPANCY NOTIFICATION REPORT
Use the Discrepancy Notification Report to notify the OAS CAHPS Survey Coordination Team of any unplanned deviation from the OAS CAHPS protocols that occurred.
To submit this form online, please go to https://oascahps.org/.
Date Submitted: inserted by system
I. Discrepancy Notification Report
One Discrepancy Notification Report (DNR) is required for each discrepancy reason. If you have multiple CCNs with the same discrepancy reason, please include all CCNs on one DNR. If you have more than one discrepancy reason, you will need to submit a DNR for each discrepancy reason. To complete this form, please complete the following sections:
• Section I—Select the affected Survey Period and the reason for the discrepancy from the
drop down boxes.
• Section II—Indicate how many facilities, and which CCNs, are impacted by the discrepancy
reason.
• Section III—Provide a detailed description of the discrepancy being reported for each CCN
and include the number of affected patients. If you do not know the number of affected
patients, please enter UNK. If the number of affected patients is not applicable, enter NA.
• Section IV—Include a description of the corrective action your organization has taken to
address the discrepancy.
• Section V—Provide any additional information about the discrepancy that you feel the OAS
CAHPS Survey Coordination Team will need.
• Section V—Submit.

Appendix P: Discrepancy Notification Report December 2015
P-2 Centers for Medicare & Medicaid Services Outpatient and Ambulatory Surgery CAHPS Survey Protocols and Guidelines Manual
II. Affected Facility or Facilities
How many facilities are affected? Enter number: . .
Please enter the CCN number(s) for which you are filing this discrepancy. If you have multiple CCN numbers, please enter them as a comma-separated list, as shown in the example below. Do not include dashes in the CCN number. After entering your CCN number(s), click on the “Lookup Facility Names” button.
Example: 111111, 222222, 333333
Lookup Facility Names .
III. Describe Discrepancy
Please complete the items below in detail for each facility listed. Include adequate information so the OAS CAHPS team can fully understand this discrepancy and its root cause.
For example: “We had to mail out pre-notification letters after the deadline, because our vendor offices were closed due to inclement weather.” Or “It has come to our attention that an error occurred during data collection and the answers to Q8, Q9, and Q10 were all recorded as “refused” due to a programing error.”
IV Corrective Action
Describe the corrective action(s) that will be taken to address discrepancy. Include the proposed timeline for the corrective action(s).
For example: “We have increased staff hours ensure that all pre-notification letters are sent no later than 2 days after the deadline.” Or “We have implemented quality control procedures and automated checks to prevent this type of programing error in the future. The CATI system now allows data to be recorded for the Q8, Q9, and Q10. In future survey periods the CATI instrument will be tested in both the development and live survey environments.”

December 2015 Appendix P: Discrepancy Notification Report
Centers for Medicare & Medicaid Services P-3 Outpatient and Ambulatory Surgery CAHPS Survey Protocols and Guidelines Manual
V. Additional information
Provide additional information that will help the OAS CAHPS Survey Coordination Team understand the discrepancy.
For example: “Due to a blizzard the data collection facility was closed for two days before the pre-notification mailing deadline.” Or “This has been corrected for the current survey period. All additional survey data collected will not be impacted by this problem.”
VI. Submit.
A Discrepancy Notification form will be submitted for the CCN number(s) listed above when you click the "Submit" button below. Please verify that the list is correct. If it is not correct, please edit your CCN number(s) above and click the Lookup button again.
To submit this form, visit the Outpatient and Ambulatory Surgery CAHPS Survey website at https://oascahps.org/. If you have any problems completing the online Discrepancy Notification Form, please e-mail the OAS CAHPS Survey Coordination Team at [email protected] for assistance.

Appendix P: Discrepancy Notification Report December 2015
P-4 Centers for Medicare & Medicaid Services Outpatient and Ambulatory Surgery CAHPS Survey Protocols and Guidelines Manual
This page intentionally left blank.





























