Embed Size (px)
Citation preview

Gut, 1992, 33, 976-981
Protein synthesis rates in colon and liver: stimulationby gastrointestinal pathologies
S D Heys, K GM Park, M A McNurlan, R A Keenan, J D B Miller, 0 Eremin, P J Garlick
AbstractRates of protein synthesis in vivo in normaland pathological tissues of the gastrointestinaltract, were measured using the 'flooding dose'technique with the stable isotope L-[1-'C]leucine. The rate of protein synthesis innormal colonic mucosa was 9.4 (1.2)% (mean(SEM)) per day but was significantly raised inbenign and malignant colorectal tumourtissue, and in colonic mucosa from patientswith inflammatory bowel disease (p<0.001).Furthermore, the rate of protein synthesis wassignificantly greater in benign colorectaltumour tissue, 36.7 (2 5)% per day, than that ineither malignant tumour tissue, 21.7 (1.9)% perday, or in inflammatory bowel disease mucosa,24.7 (2.5)% per day (means (SEM) p<0001).Liver protein synthesis rates were alsomeasured in separate groups of patients withbenign disease of the gastrointestinal tract, inpatients with colorectal carcinoma, and inpatients with inflammatory bowel disease. Thefractional rate of liver protein synthesis was20O7 (1.9)% per day in patients with benigndisease and 23.1 (1.6)% per day in patients withcolorectal cancer. In patients with inflamma-tory bowel disease, however, liver proteinsynthesis was significantly increased to 35 4(2.3)% per day (means (SEM) p<0.01).
Rowett ResearchInstitute, Bucksburn,AberdeenS D HeysKGM ParkM A McNurlanP J Garlick
Department of Surgery,University ofAberdeen,AberdeenJ D B Miller0 EreminR A KeenanCorrespondence to:Mr S D Heys, FRCS(Glas),Department of Surgery,University Medical Buildings,Aberdeen Royal Infirmary,Foresterhill, AberdeenAB9 2ZD.
Accepted for publication11 November 1991
The development of weight loss and malnu-trition, with a concomitant loss ofbody nitrogen,reduced nitrogen intake and reduction in leanbody mass, are well recognised findings inpatients with benign or malignant disease of thecolon.'2 With inflammatory bowel disease, theloss of protein through the gastrointestinal tractis also a contributory factor.23 Previous investi-gations of protein metabolism in these clinicaldisorders have centred on measurements ofwhole body protein turnover. In the presence ofa malignant tumour - for example, lung or colon,increases in whole body protein synthesis andbreakdown have been reported,45 although otherstudies have detected no change.67 Rises inwhole body turnover rates have also been seen inpatients with inflammatory bowel disease. More-over, the increased rate of protein synthesis andbreakdown correlated with the severity of thedisease activity, as assessed from the patientserythrocyte sedimentation rates.8
These studies of whole body protein meta-bolism, however, simply reflect an average ofevents occurring in all individual tissues. In thepresence ofmalignancy it is known that differenttissues can respond in different ways. Forexample, Pain et al9 have shown that in experi-mental tumour-bearing animals, protein
synthesis was decreased in skeletal muscle butincreased in liver when compared with non-tumour bearing controls. Similarly in man, inpatients with bronchial carcinoma there was adecrease in skeletal muscle protein synthesis butno change in whole body protein synthesis, whencompared with control patients without malig-nant disease.'0 Measurement of protein synthesisin individual tissues is therefore advantageouswhen further investigating these abnormalitiesin protein metabolism, but in the past this hasusually required animal studies.Tumour protein synthesis has been previously
measured in man by constant infusion of ['N]glycine or ['4C]leucine, "11 In order to calculaterates of protein synthesis accurately, however, itis necessary to correctly measure the isotopicenrichment of the precursor free amino acid.Compartmentation of free amino acid poolsresults in different isotopic enrichment in theintra and extracellular pools when traceramounts of label are given. Moreover, theenrichment of neither of these alternatives maybe representative of that of the true precursor,so that erroneous rates of protein synthesismay result.'4 The problem was minimised inmeasurements on cells and tissues in vitro,however, and in small animals in vivo, by the'flooding dose' technique, in which all aminoacid pools are rapidly equilibrated to similarenrichments.We have further developed the 'flooding dose'
technique for measurement of tissue proteinsynthesis in normal and pathological tissues inman, in vivo,'5 '7 and have now applied it to thestudy of normal and diseased colorectal tissue.Additional measurements were also made of liverprotein synthesis to determine whether thepresence of gastrointestinal pathology affectedprotein synthesis in this tissue which was notdirectly affected by the disease.
Methods
PATIENTSThis study was performed in the Grampiangroup of hospitals and was approved by theJoint Ethical Committee of the University ofAberdeen and the Grampian Health Board, withall patients giving informed consent.
STUDY 1The patients studied were both male and femalewho had been admitted to hospital for electivesurgery. Patients with colorectal tumours(benign and malignant) and inflammatory boweldisease underwent standard bowel preparationwhich consisted of a low residue diet for two days
976
on January 11, 2021 by guest. Protected by copyright.
http://gut.bmj.com
/G
ut: first published as 10.1136/gut.33.7.976 on 1 July 1992. Dow
nloaded from

Protein synthesis rates in colon and liver: stimulation by gastrointestinal pathologies
and Picolax (Nordic Pharmaceuticals, Feltham,Middlesex) on the day before surgery. Patientsundergoing haemorrhoidectomy received onlyphosphate enemas on the day before surgery.
Details of patients are given in Table I andthey were divided into four groups: group a:colorectal carcinoma; group b: benign colorectaltumours - that is, tubulovillous adenomas;group c: inflammatory bowel disease (fivepatients had ulcerative colitis and one patienthad Crohns disease, with stool frequencies rang-ing from four to six motions per day; all patientshad diffuse pan-colitis and were histologicallyreported as 'moderate active chronic colitis'; andgroup d: haemorrhoidectomy. All patients werefasted before surgery. Measurements of proteinsynthesis in biopsies of colorectal tissue weremade. The tissues sampled were malignantcolorectal tumour tissue (group a), benigncolorectal tumour tissue (group b), rectal mucosafrom patients with inflammatory bowel disease(group c), and healthy rectal mucosa from thosepatients undergoing haemorrhoidectomy (groupd).
STUDY 2The patients studied were both male and femaleand their details are shown in Table II. They hadbeen admitted for the surgical treatment of thefollowing conditions: group e: benign disease(comprising patients with benign colorectaltumours (two), plus those with chronic chole-cystitis; group f: inflammatory bowel disease (allpatients had moderately active ulcerative colitiswith diffuse involvement of the whole colon, butno evidence at laparotomy or on liver functiontests of hepatic damage); group g: colorectalcarcinoma. Liver protein synthesis rates weremeasured, at the time of surgery, as describedbelow.
MEASUREMENT OF PROTEIN SYNTHESISIn study 1, protein synthesis was determined bythe 'flooding dose' technique, as described pre-
TABLE I Clinical details ofpatient groups in whom proteinsynthesis was measured in normal and pathological tissues
Patient group Age Body mass Serum albumin(n) (yr) index (kglm2) (gll)
Normal mucosa (5) 49 (10) 23 (1) 41(1)Tubulovillousadenomas (6) 67 (7) 23 (1) 42 (0.6)
Inflammatory boweldisease (6) 38 (8) 21(1) 39 (1)
Colorectal cancer (6) 71 (4) 21 (1) 39 (1)
Values shown are means (SEM).
TABLE II Clinical details ofpatients in whom liver proteinsynthesis was measured
Patient group Age Body mass Serum albumin(n) (yr) index (kglm2) (gll)
Benign disease* (5) 58 (4) 22 (0.5) 39(1)Inflammatory bowel
disease(4) 40(10) 21(0.6) 36(1)Colorectal cancer (5) 71 (2) 21 (0.2) 38 (1)
Values shown are means (SEM)*, patients in the benign diseasegroup comprised three patients with chronic cholecystitis and twowith benign colonic tumours.
viously.'5 16 A bolus of L-[1-'3C]leucine (4 g/70 kgbody weight, 19.4 atom %) was given at aconstant rate in 200 ml 0 9% saline over 10minutes. Venous blood samples (5 ml) weretaken at 10, 20, 30, 60, and 90 minutes after thestart of injection of isotope for measurement ofthe isotopic enrichment of plasma free leucine.After allowing between 45 and 90 minutes forincorporation of labelled amino acid into pro-tein, anaesthesia was induced and biopsies ofrectal mucosa or tumour were taken immedi-ately, through a sigmoidoscope (therefore thepatient was anesthetised for only five minutes ofthe 45-90 minute period available for incorpora-tion of isotope). The biopsies were immediatelyfrozen in liquid nitrogen and stored at -20°Cuntil analysed.
In study 2, the same 'flooding dose' procedurewas carried out except that an operative liverbiopsy, approximately 200 mg, was takenimmediately after the abdomen had beenopened. This biopsy was taken from the anteriorsurface of the right lobe of the liver. There wasno evidence of hepatic metastases in thosepatients with colorectal carcinoma at the time ofthe study, and serum bilirubin, and aspartateaminotransferase, alkaline phosphatase andgammaglutamyltransferase activities werenormal.
ANAESTHETIC TECHNIQUEA standard anaesthetic regimen was used in allpatients. Anaesthesia was induced with suxa-methonium and propofol, and maintained usinga combination of nitrous oxide, oxygen andisoflurane.
SAMPLE PREPARATIONThe free and protein bound leucine in the tissuebiopsies were separated by pulverising the frozentissue, homogenising in 0.2 M HC104 at 4°C andcentrifuging at 2800 g for 20 minutes. Thesupernatant containing the free leucine wasneutralised with 1 M KOH at 4°C and centri-fuged to remove excess KC104. This supernatantwas used for measurement of isotopic enrich-ment of free leucine. The protein precipitate waswashed with HC104, dissolved in 0.3 M NaOHat 37°C for one hour and then reprecipitated with2 M HC104. The protein pellet was washed againwith 0-2 M HC104, before hydrolysing in 6 Mhydrochloric acid for 24 hours at 110°C. Afterhydrolysis, the hydrochloric acid was removedby evaporation in vacuo, and the remainingsample used for the measurement of isotopicenrichment of leucine in protein.
Preparation of plasma for determination ofisotopic enrichment of free leucine was per-formed as described previously.'5
MEASUREMENT OF "3C ENRICHMENTS
Plasma and tissuefree leucineThe enrichment of plasma free leucine wasmeasured using a VG 12-250 quadrupole gaschromatograph mass spectrometer (VG,Masslab, Manchester, UK), after conversion to
977
on January 11, 2021 by guest. Protected by copyright.
http://gut.bmj.com
/G
ut: first published as 10.1136/gut.33.7.976 on 1 July 1992. Dow
nloaded from

Heys, Park, McNurlan, Keenan, Miller, Eremin, Garlick
16
a 14x8)- 12E0
10 _
8
l0 10 20 30 40 50 60 70 80 90
Time (minutes)
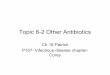
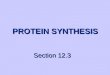
Figure 1: Time coursefor the fall in plasma free leucineenrichmentfollowing administration ofL-[f1-C]leucine.Values shown are means (SEM).
the tertiary butyldimethylsilyl derivative. Theion peaks at m/z 302 and 303 were monitoredunder electron impact and selective ion record-ing conditions.18The enrichment of tissue free leucine was also
measured using GCMS after conversion ofleucine to the N-butyl heptafluorobutyrylisobutyl derivative.19 Chemical ionization, withmethane as the reactant gas, and selective ionrecording ofthe ion peaks at m/z 363 and 364 wasused.
Protein bound leucineLeucine was separated from other amino acids inthe protein hydrolysate by preparative ionexchange chromatography. Leucine-CO2 wasliberated by reaction with ninhydrin at pH 2.2,20and its enrichment measured along the linesdescribed by Halliday and Reid2' using a gas
isotope ratio mass spectrometer, SIRA 12 (VGIsogas, Middlewhich, Cheshire, UK).
CALCULATIONSThe fractional rate of protein synthesis in thetissue was calculated from the formula describedby McNurlan et a122;
ks=(p(t)-P(o) x 100/Awhere, ks is the fractional rate of proteinsynthesis (% per day), P(o) and P(t) are theenrichments of leucine in tissue protein at thebeginning and end of the incorporation period(atom %) and A is the area under the curve forprecursor enrichment (atom % excessxtime indays), assuming a linear increase from 0 to themeasured value at 10 minutes. P(o) was taken toequal the enrichment of a zero time sample ofplasma proteins.23
STATISTICAL ANALYSISThe significance of differences between means
was assessed using the Mann Whitney U test.
ResultsThe clinical details of the patients studied are
shown in Tables I and II. The mean age ofpatients in the colorectal cancer and benigncolorectal tumour groups was higher than that ofthe inflammatory bowel and normal rectal
CDo
h-
a)0.
C0
..-
40
36
32
28
24
20
16
12
8
4
0
Normal Benign Malignant Inflammatorymucosa tumour tumour bowel
disease
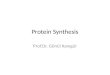
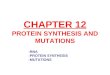
Figure 2: Rates ofprotein synthesis in normal colorectalmucosa, mucosafrom patients with inflammatory boweldisease (IBD), benign tumours of the rectum and in malignantcolorectal tumours. (Values shown are means (SEM),*p<0.001 compared with normal colorectal mucosa.)
mucosa groups, as would be expected from theage distributions of surgery for these differentpathologies. The nutritional status of all groups,however, as assessed by body mass index (bodyweight/height2) was comparable.
PLASMA AND BIOPSY FREE LEUCINE "3CENRICHMENTSThe time course of the plasma free leucineenrichment after the 'flooding dose' (Fig 1),showed peak enrichment immediately after theleucine infusion had finished followed by a linearfall in all subjects.One of the criteria for 'flooding' is that
different amino acid pools should reach similarenrichments. In order to determine if this hadoccurred, the biopsy free leucine enrichmentswere measured and compared with the plasmafree leucine enrichment at the time of taking thebiopsy. This was expressed as a ratio of biopsy/plasma free leucine enrichment. These ratioswere 0.92 (0.03), 0.88 (0.02), 090 (0.02), and0.85 (0.02) (means (SEM)) for normal mucosa,benign tumour, malignant tumour and inflamedmucosa, respectively. In the liver biopsies theratios were 0.84 (0.02), 0-86 (0.04), and 0.81(0.05) for benign gastrointestinal disease,colorectal cancer and inflammatory bowel diseasegroups of patients respectively.
TISSUE PROTEIN SYNTHESIS RATESThe fractional rate of protein synthesis in normalcolonic mucosa was 9.4 (1.2)% per day (mean(SEM)), but was significantly raised in all thepathological conditions studied (p<0-001). Thevalues were, 36.7 (2.5)% per day in benigncolorectal tumour tissue, 21.7 (1-9)% per day inmalignant colorectal tissue, and 24.7 (2.5)% perday in rectal mucosa from patients with inflam-matory bowel disease (Fig 2).
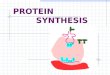
Liver fractional protein synthetic rates in thethree groups of patients are shown in Figure 3.The values were 20-7 (1-9)% per day in patientsin the benign group, and 23-1 (1.6)% per day in
978
18r
on January 11, 2021 by guest. Protected by copyright.
http://gut.bmj.com
/G
ut: first published as 10.1136/gut.33.7.976 on 1 July 1992. Dow
nloaded from

Protein synthesis rates in colon and liver: stimulation by gastrointestinal pathologies
40r-
*)' L
4' 24
- Ol
0-
2-
-h 1 60
_i
8
T
_
0l
Benign Colorectaldisease cancer
Inflammatoryboweldisease
Figure 3: Rates ofliver protein synthesis in patients withinflammatory bowel disease (IBD), colorectal cancer and acontrol group with benign disease. (Values shown are means(SEM), p<O0O1 compared with colorectal cancer and benigngroups ofpatients.)
patients with colorectal cancer. In the patientswith inflammatory bowel disease, however, liverprotein synthesis was significantly raised to 35.4(2-3)%/day (p<0 01).
DiscussionThe development and application of the 'flood-ing dose' technique to the measurement ofprotein synthesis is rapidly turning over tissues,such as tumour tissue, has facilitated a furtherevaluation of rates of protein synthesis indiseased tissues derived from patients withgastrointestinal pathology. In order to obtain'baseline rates' for colonic mucosa, a group ofpatients who were undergoing a haemorrhoidec-tomy (all without evidence of colorectal tumouron barium enema and sigmoidoscopic examina-tions) consented to undergo measurement ofprotein synthesis. The rate of protein synthesisin disease free colonic mucosa from non-tumourbearing patients has not been reported pre-viously, although Stein et all" did measure
protein synthesis in the macroscopically 'normal'colonic mucosa of patients with colorectalcancer. These workers reported a wide range ofrates, from 2 to 26% per day, with a mean (SEM)of 9.4 (2.5)% per day (seven). This is similar tothe rate for normal mucosa obtained here, butwith more interindividual variation. Disease freemucosa from cancer patients was not studied inthe present investigation because of the technicaldifficulty of taking a second biopsy after thetumour had been removed.The protein synthesis rate in localised malig-
nant colorectal tumours of 217 (1-9) per day(mean (SEM)) is similar to that reported pre-viously. 16 The rate in benign colorectal tumours,however, has not been previously documented.The value obtained in these benign tubulovillousadenomas was significantly raised relative toboth normal and malignant tissues. The reasons
for this are unclear, but there are two possibleexplanations. It is known that approximately30% of benign tumours will become 'invasive'and therefore it is possible that an increase inprotein synthesis, which would be needed forfurther growth, might herald the development of
the malignant phenotype and invasion by thetumour cells. The histological appearances wereall benign, however, and showed changes ofmildor moderate dysplasia only, with no evidence ofmalignant change or invasion into the underlyingtissues. Furthermore, experimental studies haveinvestigated cell kinetics in normal mucosa andin benign and malignant tumours of the humancolon by labelling with bromodeoxyuridine.24These studies have shown that the labellingindex was significantly lower in normal mucosathan in benign and malignant tumours, and thatof malignant tumours was significantly greaterthan that in benign tumours. In addition, thelabelling index ofbenign tumours with low gradedysplasia was significantly lower than that inthose with high grade dysplasia. It is thereforeunlikely that the increased protein synthesis inbenign tumours represents a metabolic markerfor the malignant phenotype and more aggres-sive tumour. A further possible explanation,however, lies in the well recognised productionof large amounts of mucoprotein by villoustumours of the rectum. It may be that theincreased protein synthesis by these tumoursrepresents an increased production of secretorymucoprotein, the synthesis of which has beenmeasured, in addition to the structural proteins,by the 'flooding dose' method.
Previous investigations of protein metabolismin patients with inflammatory bowel disease, likethose in malignancy, have centred on whole bodymeasurements. Powell-Tuck et all measuredwhole body protein metabolism in 19 patientswith ulcerative colitis, while they were receivingenteral or intravenous nutrition. It was foundthat increases in protein synthesis and break-down could be correlated with the progressionof disease severity, as judged by erythrocytesedimentation rate and clinical symptoms. Nomeasurements of protein synthesis in individualtissues or intestinal mucosa were carried out inthese studies, however. The contribution, there-fore, of the pathological colon to this increasedwhole body protein synthesis and breakdownwas unknown. Moreover, there are no data inhealthy man regarding the contribution that thecolonic mucosa makes to whole body proteinsynthesis. Studies in experimental animals haveshown that in the rat, the fractional rate ofprotein synthesis in normal colonic mucosa is62% per day, but this only contributes 2-6% ofwhole body protein synthesis.25 If a comparablerelationship between protein synthesis in colonicmucosa and in the whole body existed in man,then colonic protein synthesis would have toincrease by a factor of 80 to account for adoubling of whole body protein synthesis.26 Asthe increase in synthesis in rectal mucosa frompatients with inflammatory bowel disease wasvery much less than this, the increase in wholebody protein turnover in such patients is notsolely because of an increase in colonic proteinsynthesis.
Synthesis of proteins by the human liver, bothstructural and secretory, is of interest andrelevance in patients because of the hepaticinvolvement in the acute phase response.Indeed, animal studies have shown that thepresence of a tumour results in increased hepatic
979
r-
on January 11, 2021 by guest. Protected by copyright.
http://gut.bmj.com
/G
ut: first published as 10.1136/gut.33.7.976 on 1 July 1992. Dow
nloaded from

980 Heys, Park, McNurlan, Keenan, Miller, Eremin, Garlick
protein synthesis.9 Before measuring liverprotein synthesis with a 'flooding dose', it wasnecessary to confirm that the ['3C]leucine enrich-ments in the liver tissue were comparable withthose of plasma, after injection of isotope. Theratios of liver to plasma free leucine enrichmentat the end of the measurement period were lowerthan the value of 95% seen in muscle with thesame protocol,'5 which compares with 50%27 to80%1' in muscle when ['3C]leucine is infused as atracer dose. Our previous studies have shownthat at 10 minutes and 30 minutes after a floodingdose of ['3C]leucine the enrichment of liver freeleucine was 102% and 95% respectively ofplasma values, falling to 81% at 90 minutes.28Similar values have been reported for tumourtissue. 16 Thus, over the entire measurementperiod the flooding procedure was successful inbringing the tissue and plasma free leucineenrichments to similar values.A further consideration when measuring
protein synthesis by taking liver biopsies at thetime of surgery has been what effect, if any, theanaesthetic agents themselves would have onprotein synthesis. This remains unknown inman, but we have investigated the effects ofcommonly used anaesthetic agents on tissueprotein synthesis in the rat and found thatalthough halothane causes a significant depres-sion of liver protein synthesis, isoflurance did nothave such an effect.2930 A standard anaestheticregimen, using isoflurane, was therefore used inall patients in order to standardise and minimiseany potential effect of anaesthetic drugs on liverprotein synthesis.The rate of liver protein synthesis in patients
with non-metastatic colonic carcinoma reportedhere was not significantly different from the ratedocumented in patients with benign disease ofthe gastrointestinal tract. The rates obtained,however, are higher than those measured in fivecolorectal cancer patients by Stein et al," whichwas 13-4 (2-0)%/day (mean (SEM)). Stein et al"used a constant infusion of ['5N]glycine whichmeasures only intracellular proteins and notsecretory proteins. The 'flooding dose' method,with its relatively short period of measurement,will measure both fixed and secretory proteinsynthesis.22 Different results may be explainedby the 'flooding method' allowing a moreaccurate determination of the enrichment ofthose amino acids used for protein synthesis (afull discussion of the potential advantages anddisadvantages of the 'flooding dose' techniquefor measuring tissue protein synthesis can befound in references'4'7. The ['"N] is not dis-tributed uniformly among the different aminoacids, being largely confined to glycine, and theconcentration of glycine in the free pool relativeto the other amino acids is not only variable, butdiffers from that in protein. Thus, the enrich-ment of the total mixture of amino acids will bedependant on variations in the concentration ofglycine, making the procedure unreliable. Morerecently, Fearon et al3 also estimated rates ofliver protein synthesis by a constant infusion of["5Niglycine, with measurement of the enrich-ment of free and protein bound glycine, in sevencolorectal cancer patients with liver metastases.The rate was only 7 5 (0*8)%/day. The reasons
for this difference may be partly explained bythe different techniques of measurement. Alsothe presence of metastatic disease may havemodulated protein synthesis by the non-affectedhepatocytes, although further studies are neededto clarify this.The rate of liver protein synthesis in patients
with inflammatory bowel disease was 43% higherthan the control group of patients. It is knownthat in inflammatory bowel disease the serumconcentrations of acute phase reactants such asorosomucoid, alpha-l-acid glycoprotein, alpha-l-antitrypsin and alpha-l-antichymotrypsin, areincreased.32-35 The increased rate of liver proteinsynthesis may therefore be explained, in part, byan increased synthesis of the acute phase react-ants. Studies in experimental animals haveshown a similar rise of liver protein synthesisduring inflammation36 and after injection ofendotoxin37 or recombinant cytokines.38 Therelative contributions of the hepatocytes andcells of the reticuloendothelial cells to theincreased rate of liver biopsy protein synthesisremains unknown, and further studies will berequired to clarify this.Could this increase in liver protein synthesis,
however, account for the increase in whole bodyprotein synthesis that Powell-Tuck et al1reported in their series of patients? As for thecolon, the contribution of liver to whole bodyprotein synthesis in the absence of pathologicalconditions in man is unknown, but in the youngrat the liver contributes only 13% of whole bodyprotein synthesis.25 If similar figures wereapplied to man, then clearly an increase of only43% in liver protein synthesis would not accountfor the reported increases in whole body proteinsynthesis. Therefore, protein synthesis in other,as yet unidentified, tissues must also haveincreased.The results of these studies therefore provide
further insight into the changes in protein meta-bolism, at the tissue level that occur in patientswith gastrointestinal pathology. In addition,they extend the observations from whole bodystudies of protein metabolism that have beenpreviously reported. The tissue biopsies in thesestudies are made up, not only of hepatocytes orcolonic epithelial cells, however, but also com-prise many other cell types - for example,reticuloendothelial cells, fibrous tissue. Thetissue biopsy rate ofprotein synthesis is thereforea summation of that in all these cells. The furtherdevelopment of current techniques for measur-ing protein synthesis, in vivo, will be required toallow the contribution ofeach cell type to the rateof protein synthesis in the whole biopsy to bedetermined.
Rates of protein synthesis in tissues derived from colonic mucosahave been published in abstract form in the Proc Nutr Soc 1990;49: 135.
We are grateful to Mr E Milne and Mr A G Calder for massspectrometric analyses and to Mrs V Buchan for amino acidanalyses. We thank the Wellcome Trust, Grampian Health Board,Scottish Hospitals Endowment Research Trust and Nestec Ltd,for their financial support.
1 Brennan ME. Uncomplicated starvation versus cancercachexia. CancerRes 1979;,37: 2359-64.
2 Dickinson RJ, Ashton MG, Axon ATR, Smith RC, YeungCK, Hill GL. Controlled trial of intravenous hyperalimenta-tion and total bowel rest as an adjunct to the routinetreatment of acute colitis. Gascroenrerology 1980; 79: 1199-204.
on January 11, 2021 by guest. Protected by copyright.
http://gut.bmj.com
/G
ut: first published as 10.1136/gut.33.7.976 on 1 July 1992. Dow
nloaded from

Protein synthesis rates in colon and liver: stimulation by gastrointestinal pathologies 981
3 Welch CS, Adams M, Wakefield EG. Metabolic studies inulcerative colitis. J Clin Invest 1937; 16: 161-8.
4 Herber D, Chlebowski RT, Ishbashi DE, Herrold JN, BlockJB. Abnormalities in glucose and protein metabolism in non-cachectic lung cancer patients. CancerRes 1982; 42: 4815-8.
5 Melville S, McNurlan MA, Calder AG, Garlick PJ. Increasedprotein turnover despite normal energy metabolism andresponses to feeding in patients with lung cancer. Cancer Res1990; 50: 1125-31.
6 Herrmann VM, Garnick MB, Moore FD, Wilmore DW.Effect ofcytotoxic agents on protein kinetics in patients withmetastatic cancer. Surgery 1981; 90: 381-7.
7 Glass RE, Fern EB, Garlick PJ. Whole-body protein turnoverbefore and after resection of colorectal tumours. Clin Sci1983; 64: 101-8.
8 Powell-Tuck J, Garlick PJ, Lennard-Jones JE, Waterlow JC.Rates of whole body protein synthesis and breakdownincrease with the severity of inflammatory bowel disease.Gut 1984; 25: 460-4.
9 Pain VM, Randall DP, Garlick PJ. Protein synthesis in liverand skeletal muscle of mice bearing an ascites tumour.Cancer Res 1984; 44: 1054-7.
10 Emery PW, Edwards RHT, Rennie MJ, Souhami RL,Halliday D. Protein synthesis in muscle measured in vivo incachectic patients with cancer. BMJ' 1984; 289: 584-6.
11 Stein TP, Mullen JL, Oram-Smith J, Rosato EF, WallaceHW, Hargrove WC. Relative rates of tumor normal gut,liver and fibrinogen protein synthesis in man. Am J Physiol1978; 234: E648-52.
12 Mullen JL, Buzby GP, Gertner MH, Stein TP, Hargrove WC,Oram-Smith J, et al. Protein synthesis dynamics in humangastrointestinal malignancies. Surgery 1980; 87: 331-8.
13 Shaw JHF, Humberstone DA. Cancer: a metabolic parasite.BrJ Surg 1988; 75: 1262.
14 Waterlow JC, Garlick PJ, Millward DJ. Protein turnover inmammalian tissues and in the whole body. Amsterdam: NorthHolland Publishing, 1978.
15 Garlick PJ, Wernerman J, McNurlan MA, Essen P, LobleyGE, Milne E, et al. Measurement of the rate of proteinsynthesis in muscle of postabsorptive young men byinjection of a 'flooding dose' of [1-"C]leucine. Clin Sci 1989;77: 329-36.
16 Heys SD, Park KGM, McNurlan MA, Calder AG, Buchan V,Blessing K, et al. In vivo measurement of tumour proteinsynthesis in human colorectal and breast cancer and itsvariability in separate biopsies from the same tumour. ClinSci 1991; 80: 587-93.
17 McNurlan MA, Essen P, Heys SD, Buchan V, Garlick PJ,Wernerman J. Measurement of protein synthesis in humanskeletal muscle: further investigation of the 'flooding'technique. ClinSci 1991; 81: 557-64.
18 Calder AG, Smith A. Stable isotope ratio analysis ofleucine and ketoisocaproic acid in blood plasma by gaschromatography/mass spectrometry. Use of tertiarybutyldimethylsilyl derivatives. Rapid Comms in Mass Spec1988; 2: 14-6.
19 MacKenzie SL, Tenaschuk D. Gas-liquid chromatography ofN-heptafluorobutyryl isobutyl esters of amino acids.J Chromatogr 1974; 97: 19-24.
20 Van slyke DD, Dillon RT, McFadyen DA, Hamilton P.Gasometric determination of carboxyl groups in free aminoacids. J Biol Chem 1941; 141: 627-80.
21 Halliday D, Reid WWC. Mass spectrometric assay of stable
isotope enrichment for the estimation of protein turnover inman. Proc NutrSoc 1981; 40: 321-34.
22 McNurlan MA, Tomkins AM, Garlick PJ. The effect ofstarvation on the rate of protein synthesis in rat liver andsmall intestine. Biochemnj 1979; 178: 373-9.
23 Heys SD, McNurlan MA, Park KGM, Milne E, Garlick PJ.Baseline measurements for stable isotope studies; an alterna-tive to biopsy. Biomed Environ Mass Spectrom 1990; 19:176-8.
24 Risio M, Coverlizza S, Ferrari A, Candelaresi GL, Rossini FP.Immunochemical study of epithelial cell proliferation inhyperplastic polyps, adenomas, and adenocarcinomas oflarge bowel. Gastroenterology 1988; 94: 899-906.
25 McNurlan MA, Pain VM, Garlick PJ. Conditions that alterrates of tissue protein synthesis in vivo. Biochem Soc Trans1980; 8:283-5.
26 Powell-Tuck J. Protein metabolism in inflammatory boweldisease. Gut 1986; 27 (suppl): 67-71.
27 Bennet WM, Connacher AA, Scrimgeour CM, Smith K,Rennie MJ. Increase in anterior tibialis muscle proteinsynthesis in healthy man during mixed amino acid infusion:studies of incorporation of [1-'3C]leucine. Clin Sci 1989; 76:447-54.
28 Ballmer PE, McNurlan MA, Milne E, Heys SD, Buchan V,Calder AG, et al. Measurement ofalbumin synthesis in man:a new approach employing stable isotopes. Am J Physiol1991; 259: E797-803.
29 Heys SD, Norton AC, Dundas CR, Ferguson K, Garlick PJ.Anaesthetic agents and their effect on tissue proteinsynthesis in the rat. Clin Sci 1989; 77: 651-5.
30 Ferguson K, Heys SD, Norton AC, Dundas CR, Garlick PJ.Effect of volatile anaesthetic agents on liver proteinsynthesis. Proc NutrSoc 1990; 49: 182.
31 Fearon KCH, McMillan DC, Preston T, Winstanley P,Cruikshank AM, Shenkin A. Reduced rates of hepaticprotein synthesis, the acute phase protein response, andelevated circulating interleukin-6 and tumour necrosis factorin advanced malignancy. Proc Nutr Soc 1990; 49: 167A.
32 Weeke B, Jarnum S. Serum concentrations of 19 serumproteins in Crohns disease and ulcerative colitis. Gut 1971;12: 297-302.
33 Lubega J, Davies TJ. A comparison of serum mucoproteinwith serum al acid glycoprotein, haptoglobin, and atlantitrypsin assays in monitoring inflammatory boweldisease. ClinChimActa 1990; 188: 59-70.
34 Buckell NA, Lennard-Jones JE, Hernandez MA, Kohn J,Riches PG, Wadsworth J. Measurement of serum proteinsduring attacks of ulcerative colitis as a guide to patientmanagement. Gut 1979; 20: 22-7.
35 Cooke WT, Fowler DI, Cox EV, Gaddie R, Meynell MJ. Theclinical significance of orsomucoids in regional ileitis andulcerative colitis. Gastroenterology 1958; 34: 910-9.
36 Ballmer PE, McNurlan MA, Southorn BG, Grant I, GarlickPJ. The effect of human interleukin-l(3 on liver proteinsynthesis in comparison to a systemic inflammatory insultinduced by turpentine in the rat. Proc Nutr Soc 1990; 49:162A.
37 Jepson MJ, Pell J, Bates P, Millward DJ. The effects ofendotox4emia on protein metabolism in ske letal muscle andliver of fed and fasted rats. Biochem3r 1986; 235: 329-36.
38 Charters Y, Grimble RF. Effect of recombinant humantumour necrosis factor ct on protein synthesis in liver,skeletal muscle and skin of rats. BiochemJ 1989; 258: 493-7.
on January 11, 2021 by guest. Protected by copyright.
http://gut.bmj.com
/G
ut: first published as 10.1136/gut.33.7.976 on 1 July 1992. Dow
nloaded from