Embed Size (px)
Citation preview

PROTEIN AND CALORIE
REQUIREMENTS
THE SURGICAL PATIENT
Prof Christian Simoens, MD, PhD
Head of the Department of Abdominal Surgery
UZ Brussel

SURGICAL METABOLISM AND NUTRITION
Energy utilization
In short- and long-term starvation
Inflammatory response (SIRS-CARS)
In critical situation
ERAS guidelines
Nutritional support in the surgical patient

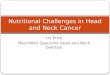
SHORT-TERM FASTING
glycogen
gluconeogenesis
oxidation
protein
triglycerides
brain
RBC
WBC
Nerve
Kidney (m)
Heart
Kidney (c)
Muscle
glucoseAmino
Acids(ala, gln)
glycerol
FFA
Pyruvate
lactateketones
muscle
Ad tissue
Liver
REE ↓ 30%
8-30 g N/day
Glucose ↓
FFA ↑

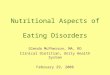
LONG-TERM FASTING
glycogen
gluconeogenesis
oxidation
protein
triglycerides
brain
RBC
WBC
Nerve
Kidney
HeartRenal cortex
Muscle
glucoseAmino
acids
glycerol
FFA
Pyruvate
lactate
ketones
muscle
Ad tissue
Liver
gluconeogenesis
kidney
REE %
2--5g N/day
Glucose ↓
FFA ↑↑

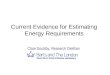
INFLAMMATORY RESPONS TO INJURY
DAMPs
PAMPs
Myeloid cells
Somatic cells
endothelium
SIRS
CARS
ORGAN DAMAGE
MOF
Homeostasis and
tissue repair
Pituitary
Adrenal
CNSGH
Aldosterone
insuline
Infl cytokines
TNF-α, IL, IFN
Inflammatory
response
ACTH
glucocorticoids
Epi, norepi
acetylcholine
DAMP damage-associated molecule patterns
PAMP pathogen-associated molecule patterns
CNS central nervous system
SIRS systemic inflammatory response syndrome
CARS counterregulatory anti-inflammatory response syndrome

SIRS - CARS
MOF
recovery
SIRS
CARS

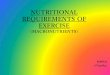
ENERGY METABOLISM FOLLOWING INJURY
glycogen
gluconeogenesis
oxidation
protein
triglycerides
Wound
RBC
WBC
Nerve
Kidney
Heart
Kidney
Muscle
glucoseAmino
acids
glycerol
FFA
Pyruvate
lactate
ketones
muscle
Ad tissue
Liver
gluconeogenesis
kidney
REE ↑↑ 10-80%
15-30g N/day
Glucose ↑↑
FFA ↑↑
50-80%

WHAT IS MALNUTRITION?
There is no universally accepted definition
Malnutrition ? nutritional risk ?
~40% of patients undergoing major surgery should be at nutritional risk
~8% severely malnourished
5,4% average weight loss during hospitalisation
Malnutrition is often either not recognized or not viewed as clinicallysignificant by many surgeons
McWirther JP et al, BMJ 1994;308:945
Hiesmayr M et al, Cl Nutr 2009;28:484

IMPACT OF MALNUTRITION
Independent risk factor for poor postoperative
outcome
↓ lean muscle mass
Alterations in respiratory mecanics
Impaired immune functions
Intestinal atrophy
↑ infectious complications
poor wound healing, ↑ anastomotic leakage
↑ LOS, ↑ Costs
↑ mortality

SCREENING OF MALNUTRITION
All patients are screened on admission. Role of dietitian in the
assessment of nutritional requirements and the identification
of appropriate nutritional options
NRS (Nutritional Risk Score)
1. BMI, weight loss, food intake
2. disease severity, age
NRS ≥ 3 increased postoperative complications
Anthropometric tests
Biochemical parameters (e.g. albumine, prealbumine)

Nutrition des patients chirurgicaux11 3-5-2018

Nutrition des patients chirurgicaux12 3-5-2018
SUIVI DE L’ÉTAT NUTRITIONNEL CHEZ LES PATIENTS CHIRURGICAUX

INDICATIONS FOR NS IN SURGICAL PATIENTS
NS in the surgical patient aims to meet the energy requirements for essential metabolic processes and tissue repair and to prevent or reverse the catabolic effects of disease or injury
Only a minority of surgical patients will need routine NS
Enhanced Recovery After Surgery (ERAS) guidelines Measures aiming to attenuate the metabolic stress induced
by starvation and surgery.
ERAS was first developped for colon surgery but now extendsto other GI interventions and even to other surgicaldisciplines.

ERAS GUIDELINES /1
Avoid mechanical bowel preparation
Dehydration, fluid and electrolyte abnormalities
Increased risk for anastomotic leakage
(Preserve colonic microbiome
Role of the microbiome in glucose metabolism, immune
functions, fuel for colonocytes,…)
Lassen K et al, Arch Surg; 144: 961

ERAS GUIDELINES /2
Avoid preoperative fasting from midnight
Allow intake of clear fluids 2h and solid foods 6h before
induction

ERAS GUIDELINES /3
Preoperative carbohydrate loading
↓ preoperative thirst, hunger and anxiety
↓ postoperative insuline resistance
↓ protein loss
shorter hospital stay

ERAS GUIDELINES /4
Avoid opioids, long-acting sedatives and hypnotics
Avoid general anesthesia by gas inhalation
Epidural anesthesia
Prevention and treatment of nausea and vomiting
Avoid routine naso-gastric intubation
Effect of epidural analgesia on postoperative insulin resistance as
evaluated by insulin clamp technique
I. Uchida, T. Asoh, C. Shirasaka, H. Tsuji. Br J Surg 1988

ERAS GUIDELINES /5
Avoid perioperative IV fluid overload
Delayed return to normal gastro-intestinal function
↑ risk of anastomotic leakage
Early oral or enteral feeding
(Prefer protective colostoma to ileostoma)

ERAS GUIDELINES /6
Avoid drains (peritoneal cavity)
Prevention of postoperative ileus
Early mobilisation

ENERGY – PROTEIN REQUIREMENTS
Harris-Benedict
BEE (♂)= 66.47+13.75(W)+5.0(H)-6.76(A) kcal/day
BEE (♀)= 655.1+9.56(W)+1.85(H)-4.68(A) kcal/day
- calculated BEE x 1.2 - 2 (depending on severity of injury)
Approximative estimation of requirements
Energy: 25-30kcal/kg.day (severe stress 30-40kcal/kg.day)
1.2 – 1.5 g/kg.day protein
(nonprotein calorie : nitrogen ratio of 150:1)
Indirect calorimetry in selected patients
Weimann A. Cl Nutr 2006; 25: 224
Braga M. Cl Nutr 2009; 28: 378

ROUTES FOR NS
Oral nutritional support
Enteral tube feeding
Nasogastric, nasojejunal, PEG
jejunostomy
Parenteral feeding
Prefer enteral routeLower cost, no risk associated with IV route (vascular access, infections,…), maintained
mucosal defenses, maintained IGA and cytokines production, no bacterial overgrowth

TIMING OF NUTRITIONAL SUPPORTPREOPERATIVE NS
Patients with severe nutritional risk
Oral or enteral NS for 10-14 days (A)
or 7–10 days TPN if EN contra-indicated) (A)
Consider feeding jejunostomy (e.g. neo-adjuvant radio-
chemotherapy in obstructive esofageal cancer patients)
Pre-op oral nutritional supplements in mildly to
moderately malnourished patients
Preoperative carbohydrate load
Immunonutrition (arginine,nucleotides, n-3FA) (A)
5-7 days preoperatively to all cancer patients (and prolonged for 5-7 days postoperatively)
Weimann A. Cl Nutr 2006; 25: 224
Braga M. Cl Nutr 2009; 28: 378

TIMING OF NUTRITIONAL SUPPORTPOSTOPERATIVE NS (ORAL)
Early oral food intake (A)
Within 24h
to reach nutritional target within 5-7days
~ type of surgery
Nutritional supplements (2x200ml) untill adequate
food intake
Weimann A. Cl Nutr 2006; 25: 224
Braga M. Cl Nutr 2009; 28: 378

TIMING OF NUTRITIONAL SUPPORTPOSTOPERATIVE NS (ENTERAL)
Early tube feeding (< 24 hours) (NJT, PEG) (A)
patients at nutritional risk
severe surgery
if anticipated oral intake <60% of target for >10days
consider placement of jejunostomy at time of
surgery
Weimann A. Cl Nutr 2006; 25: 224
Braga M. Cl Nutr 2009; 28: 378

TIMING OF NUTRITIONAL SUPPORTPOSTOPERATIVE NS (PARENTERAL)
Indications for post-operative parenteral nutrition
severely malnourished patients (A)
when postoperative complication impairing
gastrointestinal function for > 7days (A)
combination EN and PN if nutritional target cannot be
met by EN alone (<60%)
Avoid overnutrition! ↑ O2 consumption, ↑ CO2 production, need for ventilatory support, fatty liver,
↓ WBC function, hyperglycemia, ↑ infections
Weimann A. Cl Nutr 2006; 25: 224
Braga M. Cl Nutr 2009; 28: 378

TYPE OF FORMULAS (ORAL – ENTERAL)
ONS
High calory, high protein diets
Enteral feeding
Standard whole protein formulas appropriate for most
patients (C)
High-calorie, high protein, elemental, renal, pulmonary,
hepatic formulas
EN with immuno-stimulating substrates (A)
Glutamine?, arginine?
Weimann A. Cl Nutr 2006; 25: 224
Braga M. Cl Nutr 2009; 28: 378

TPN COMPOSITION
Standard (3in1) mixtures appropriate for most
patients (50/30/20)
Administered over 24h (glucose control)
High output fistulas
Metabolic and electrolyte disturbances
May necessitate supplementation Na, Mg, vitamins,…

TPN COMPOSITION
Choice of lipid
n-6 FA (soy oil) pro-inflammatory, immunosuppression
MCFA (coconut oil) rapidly cleared from plasma and promptly oxidized
n-9 FA (olive oil) slower plasma clearance, ↑anti-oxydant defenses
n-3 FA (fish oil) anti-inflammatory, ↓cardiac arrhythmias
Amino-acids
Dipeptiven? (alanyl-glutamine)
Vitamins and trace elements
Supplemented on a daily basis

MONITORING NUTRITIONAL STATUS
Daily monitoring of diatary intakes
Weight
Weekly nutritional screening and/or re-assessment
Clinical parameters
Blood analyses
Glucose, triglycerides
Hematology, CRP
Liver function, renal function
Albumine, transferrin
Ionogram, P, K, Mg

REFEEDING SYNDROME
Initiation of EN or PN in a malnourished patient
Electrolyte abnormalities (PO4--, Mg++, K+)
Thiamine deficiency
Na+ and water retention (oedema)
Heart failure, respiratory failure, delirium, death
Slow increase of calorie intake in patients at risk
Close electrolyte monitoring (supplementation as
required)

OPTIMAL DURATION OF NS
Well nourished patients: untill normal feeding
Malnourished patients: ONS for 8 weeks

SUMMARY
Malnutrition substantially increase postoperative
morbidity and mortality
An appropriate postoperative NS has beneficial
effects on postoperative outcome
The implementation of ERAS guidelines has
substantially decreased postoperative morbidity
In malnourished patients the nutritional status
should first be corrected and surgery delayed