Embed Size (px)
Citation preview

Despite progress in prevention, ischaemic stroke remains a major global health burden1. Brain damage after ischaemic stroke can be limited by rescuing the ‘ischaemic penumbra’ — that is, the severely hypoperfused and hypoxic, electrically silent, at risk brain tissue2,3. Evidence based treatments to salvage the penumbra all involve restoring blood flow as early as possible4; otherwise, with time, the penumbra evolves into a ‘core’ of irreversibly damaged tissue until it has vanished entirely3,5. Intravenous thrombolysis (IVT) with tissue plasminogen activator (tPA) has been in use since 1996, but its therapeutic time window is only 4.5 h, and the early recanalization rate is only ~30%6. In 2015, direct clot removal by retrograde catheterization, also known as mechanical thrombectomy, administered within 6 h of stroke onset was consistently shown across six randomized control trials (RCTs) to considerably improve functional outcomes over and above IVT alone across the whole range of modified Rankin Scale (mRS) scores and immediately became the standard of care4. However, despite an early recanalization rate of > 80%, over half of the treated patients did not achieve functional independence (mRS score > 2)7, mainly because the ischaemic core was already too large at the time of recanalization. Therefore, one potential way to further
enhance the benefits of mechanical thrombectomy is to stop or limit core growth — that is, to ‘freeze’ the penumbra — until recanalization is achieved.
This article reviews approaches to freezing the penumbra as an adjunct to mechanical thrombectomy. Although several pharmacological agents, including the neuroprotectant N A 1 (ref. 8), are being tested for this purpose, the focus here is on nonpharmacological approaches. In contrast to the pharmacological agents, which often have multiple molecular targets, these nonpharmacological strategies aim to restore the physiological balance between oxygen delivery and oxygen demand in the penumbra. Readers who are interested in pharmacological approaches are referred to recent topical reviews9,10. As summarized in Table 1, nonpharmacological approaches are mostly non invasive, easy to administer and innocuous, have few or no contraindications and could potentially be delivered ‘in the field’, even before a diagnosis of ischaemic stroke is firmly established11. Although the feasibility and safety of most of these interventions has been established in proof ofconcept RCTs, their efficacy has not yet been documented. In addition, as discussed below, the penumbral freezing paradigm has rarely been specifically addressed, which might account for the alleged failure
Protecting the ischaemic penumbra as an adjunct to thrombectomy for acute strokeJean- Claude Baron
Abstract | After ischaemic stroke, brain damage can be curtailed by rescuing the ‘ischaemic penumbra’ — that is, the severely hypoperfused, at- risk but not yet infarcted tissue. Current evidence- based treatments involve restoration of blood flow so as to salvage the penumbra before it evolves into irreversibly damaged tissue, termed the ‘core’. Intravenous thrombolysis (IVT) can salvage the penumbra if given within 4.5 h after stroke onset; however, the early recanalization rate is only ~30%. Direct removal of the occluding clot by mechanical thrombectomy considerably improves outcomes over IVT alone, but despite early recanalization in > 80% of cases, ~50% of patients who receive this treatment do not enjoy functional independence, usually because the core is already too large at the time of recanalization. Novel therapies aiming to ‘freeze’ the penumbra — that is, prevent core growth until recanalization is complete — hold potential as adjuncts to mechanical thrombectomy . This Review focuses on nonpharmacological approaches that aim to restore the physiological balance between oxygen delivery to and oxygen demand of the penumbra. Particular emphasis is placed on normobaric oxygen therapy , hypothermia and sensory stimulation. Preclinical evidence and early pilot clinical trials are critically reviewed, and future directions, including clinical translation and trial design issues, are discussed.
Department of Neurology, Hôpital Sainte- Anne, Université Paris 5, INSERM U894, Paris, France.
e- mail: jean- [email protected]
https://doi.org/10.1038/ s41582-018-0002-2
Corrected: Author Correction REVIEwS
© 2018 Macmillan Publishers Limited, part of Springer Nature. All rights reserved.
NATuRe RevIeWS | NEuROlOgy volume 14 | JuNe 2018 | 325

of some of these interventions. Therefore, one aim of this Review is to advocate repurposing of such ‘failed’ interventions towards effective penumbral freezing.
In addition to constraining the core volume in patients who are eligible for mechanical thrombectomy, penumbral freezing could ‘buy time’ by preventing the core size from reaching the recommended exclusion threshold4,12, thereby making more patients eligible for this therapy, not only within but also beyond the 6 h time point. Indeed, the DAWN and DEFUSE3 trials recently showed that patients who were selected by imaging to harbour a large penumbra — determined directly13 or inferred by a clinical–core mismatch14 — and a small to moderate core volume (so called ‘slow progressors’ (ref.15)) could benefit from mechanical thrombectomy up to 24 h from the time that they were last seen well.
This article critically reviews both preclinical and clinical trials of nonpharmacological approaches and indicates new directions for research. With regard to the preclinical trials, we focus o n clinically relevant focal c e r e b ral i s c h a emia r e s u l ting f r o m m i d dle c e r e b ral a r t ery occlusion (MCAO).
Freezing the penumbra: the conceptThe penumbral freezing concept is outlined in box 1. As illustrated in fig. 1, the penumbra is characterized by severely reduced perfusion and, hence, oxygen supply2,5, together with relatively preserved oxygen consumption3 — a ‘mismatch’ that results in severe tissue hypoxia16–24 and an increased oxygen extraction fraction3. Accordingly, the main nonpharmacological penumbral freezing approaches aim to either enhance oxygen delivery or reduce the tissue’s oxygen demand. Importantly, although the benefits of penumbral freezing are expected to be optimized by pre hospital initiation, starting the therapy in conjunction with IVT to limit core growth during transfer for mechanical thrombectomy25, and even during mechanical thrombectomy
itself, is still likely to be beneficial, in line with the ‘time is brain’ concept26.
Improving oxygen supply to the penumbraAs the complex ischaemic cascade that ultimately results in infarction is triggered by severe persistent hypoxia27, increasing the blood’s oxygen carrier capacity or enhancing retrograde collateral perfusion would be expected to maintain the penumbra until reperfusion occurs and, in turn, reduce the final damage.
Increasing oxygen transport capacityHyperbaric oxygen (HBO) therapy was initially tested in patients following positive findings in experimental models28,29, but small scale pilot clinical studies were largely negative30, perhaps in part related to the known adverse effects of HBO31. However, given the logistical barriers, no clinical study to date has tested HBO in accordance with the penumbral freezing paradigm. An alternative approach that has been investigated is normobaric oxygen (NBO) therapy (also known as normobaric hyperoxia), alone or combined with perfluorocarbons (PFCs).
Normobaric oxygen therapy. Although reviews on NBO therapy in stroke are available32–34, no critical review reflecting the rapid growth in the literature on this topic has been published recently.
Although NBO does not result in major increases in total arterial oxygen content, a rodent study showed that NBO — administered as 100% oxygen added to ambient air via a nose cone — increased the arterial partial pressure of oxygen (PaO2) fourfold and increased the oxygen saturation to 100%35. Similar observations have been made in humans36. In various rodent models of ischaemic stroke16,22,23,37,38, NBO administration doubled the brain tissue partial pressure of oxygen (PtO2) and significantly increased penumbral PtO2 from ~10–15 mmHg to ~25 mmHg (physiological value in rats: ~30–35 mmHg). Interestingly, in one study, PtO2 increased less in brain areas that were assumed to represent the core than in the penumbra22.
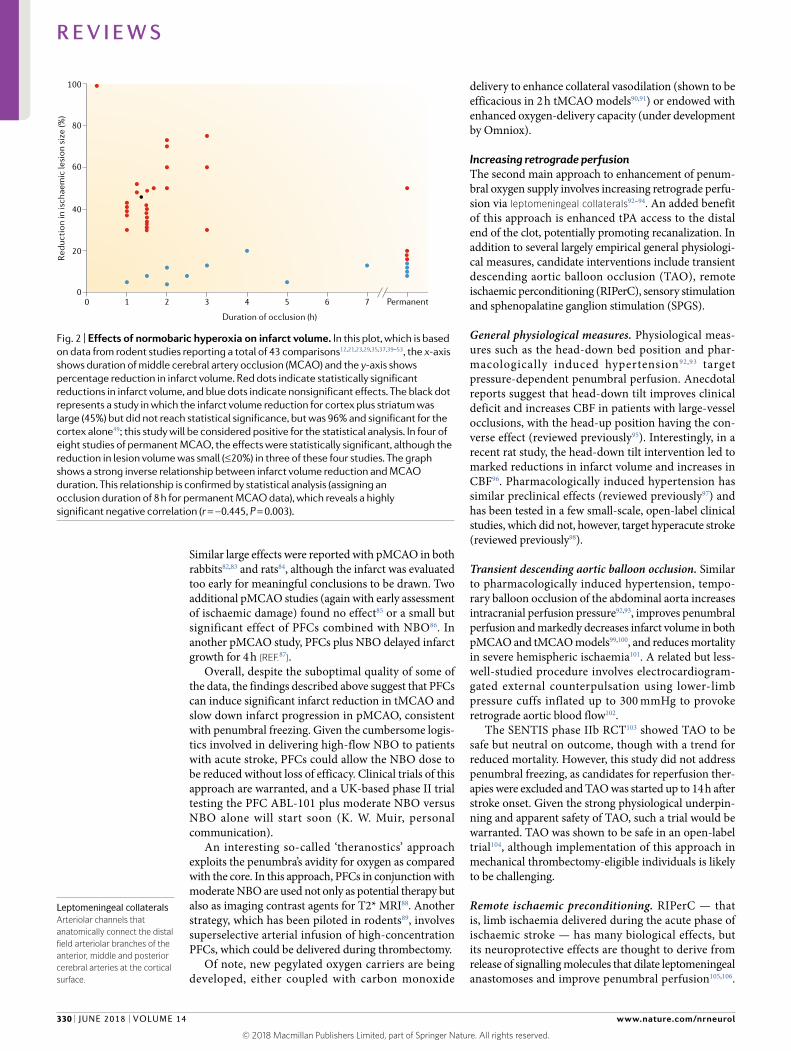
The effects of NBO on infarct volume in rodents is summarized in Supplementary Table 1 and depicted graphically in fig. 2. A literature search on this topic recovered 21 full articles in the English language12,21,23,29,35,37,39–53, reporting a total of 43 comparisons. As fig. 2 shows, a strong negative relationship exists between effect size and MCAO duration. This relationship persists if the data are binned by MCAO duration, with significant effects observed in 17 of 19 studies of temporary MCAO (tMCAO) < 2 h, 7 of 11 studies with tMCAO of 2–3 h and 4 of 11 studies with MCAO > 3 h (P = 0.0057, Fisher test). Note that although significant effects were reported in four of eight comparisons of permanent MCAO (pMCAO)29,41,42,53, in three of these, the reduction in lesion size was ≤ 20% — the generally accepted cut off point for a clinically meaningful effect. Regarding modern preclinical stroke research quality criteria54, randomized group allocation was mentioned in the majority of studies and blinding in roughly half (Supplementary Table 1), reinforcing the overall validity, although sample
Key points
•The extent of brain damage following an ischaemic stroke can be limited by rapidly rescuing the ‘ischaemic penumbra’ — that is, the severely ischaemic, at- risk but not yet infarcted tissue.
•Intravenous thrombolysis, which was licensed for clinical use in 1996, can salvage the penumbra if administered early after stroke onset; however, the recanalization rate is low.
•endovascular thrombectomy increases the likelihood of penumbral salvage and considerably improves outcomes; however, around half of the patients who undergo successful thrombectomy do not achieve functional independence, mainly because the infarct is already too large at the time of recanalization.
•Novel therapies that aim to ‘freeze the penumbra’ — that is, to prevent infarct growth until recanalization is complete — hold considerable potential as adjuncts to thrombectomy.
•This article focuses on nonpharmacological approaches to freeze the penumbra, which directly target penumbral hypoxia, are mostly non- invasive and easy to administer, have few or no adverse effects and might be delivered before hospital admission.
•emphasis is placed on normobaric hyperoxia, hypothermia and sensory stimulation, but other potential approaches, including transcranial direct cortical stimulation, perconditioning, perfluorocarbons, aortic balloon occlusion and sphenopalatine ganglion stimulation, are also presented.
Clinical–core mismatcha mismatch between clinical presentation and size of the core on imaging, such that the clinical deficit appears larger than would be expected from the core alone, indicating that a large penumbra is also present.
Hyperbaric oxygen(Hbo). oxygen delivered at a pressure higher than atmospheric pressure.
Normobaric oxygen(Nbo). oxygen delivered at atmospheric pressure.
© 2018 Macmillan Publishers Limited, part of Springer Nature. All rights reserved.
www.nature.com/nrneurol
R e v i e w s
326 | JuNe 2018 | volume 14

size calculation was only rarely mentioned. Although in several studies infarct assessment was carried out at 24 h, which some consider to be too early, especially for pMCAO, the benefits of NBO seemed to be independent of infarct assessment time point (Supplementary Table 1).
Only one study has looked at the effects of timing of NBO initiation44. In a 2 h tMCAO paradigm, NBO was efficacious if started ≤ 30 min after MCAO but not at 45 min, suggesting that the intervention is beneficial only if started early. However, across the tMCAO ≤ 3 h studies listed in Supplementary Table 1, only a trend towards significant advantages of early intervention with NBO is present (Fisher’s P = 0.06 for NBO started at < 30 min versus ≥ 30 min). Also, the extent to which penumbral dynamics in rodents translate directly to humans is uncertain55. Whenever performed, neurological and behavioural tests showed benefits that paralleled the reduction in lesion size, indicating that NBO does not interfere with plasticity related delayed behavioural improvements.
Importantly, three studies that employed serial MRI41,42,44, with lesion volume being determined by apparent diffusion coefficient (ADC) values, documented arrest of lesion growth or even partial lesion reversal during NBO, signifying effective penumbral freezing. Also
consistent with penumbral freezing, under pMCAO conditions, the ADC lesion subsequently resumed growth despite NBO, with no difference in ultimate ADC lesion size, whereas with recanalization at 180 min, the gain from NBO consolidated as a reduction in infarct size41,42. Similar findings have been reported in humans (see below).
Despite mild vasoconstrictive effects under physiological conditions, NBO was not found to reduce cerebral blood flow (CBF) in ischaemic areas12,41,42,44–46,52,56; in fact, significant increases in CBF were seen16,23,37,41,44. NBO was also found to increase penumbral oxyhaemoglobin and ATP stores, prevent core growth and reduce both the CBF threshold for tissue survival23,51,57 and the occurrence of peri infarct depolarizations (PIDs), which are known to facilitate penumbral demise58.
Also contrary to expectations, NBO did not promote oxidative stress12,37,48, which is detrimental after reperfusion59,60. Equally critical for clinical translation, NBO was consistently found not to be detrimental if continued into reperfusion37,39,45,56,61,62 — a scenario that mimics early spontaneous or therapy induced recanalization. Only one study failed to confirm this finding63. In two studies, continuation of NBO led to further reductions in infarct volume50,61, possibly because NBO
Table 1 | Potential nonpharmacological interventions to freeze the ischaemic penumbra
Intervention Mechanism of penumbral protection
Effect on infarct volume in rodents
Penumbral freezing directly documented
Translatability Ongoing RCTs directly testing the penumbral freezing paradigm
Normobaric oxygen (NBO)
Increased oxygen delivery
Strong effects if given early after tMCAO; little or no effect in pMCAO or tMCAO > 3 h
Yes (also in humans)
Excellent (including pre- hospital)
One (PROOF)a
Perfluorocarbons (PFCs) Increased oxygen delivery
Strong effect in combination with NBO (mainly in tMCAO), but few good- quality studies
Yes Excellent (including pre- hospital)
None
Transient descending aortic balloon occlusion (TAO)
Increased collateral perfusion
Strong effects in both tMCAO and pMCAO, but few studies published
No Limited (complex logistics)
None
Remote ischaemic perconditioning (RIPerC)
Increased collateral perfusion
Strong effects (stronger with tMCAO than with pMCAO), but few studies published
No Excellent (including pre- hospital)
One (RESCUE)a
Sensory stimulation Increased collateral perfusion
Strong effects in rats (both tMCAO and pMCAO) if given early
No Unclear, as sensory stimulation is detrimental in mice or if started late, but could be started pre- hospital
None
Sphenopalatine ganglion stimulation (SPGS)
Increased collateral perfusion
Clear effects (only pMCAO tested)
Yes Good, but difficult to apply in the field
None
Therapeutic hypothermia Reduced tissue energy requirements
Strong effects; larger in tMCAO (any duration) than in pMCAO and larger with deep hypothermia
No Good, but deep hypothermia is associated with more adverse effects; pre- hospital delivery difficult
One (ICTuS-3)a
Cathodal transcranial direct cortical stimulation (C- tDCS)
Inhibition of peri- infarct depolarizations
Mild to moderate effects in both tMCAO and pMCAO, but few studies published
No Excellent (including pre- hospital)b
One (STICA)a
pMCAO, permanent middle cerebral artery occlusion; RCT, randomized controlled trial; tMCAO, temporary MCAO . aSee main text for details. bGiven its dual effects — that is, both freezing the penumbra and preventing reperfusion injury — hypothermia can and probably should be administered both before and after recanalization (see main text for details).
Apparent diffusion coefficient(aDC). Mri- based physiological variable expressing the diffusion coefficient of water molecules in brain tissue, which is restricted in acutely ischaemic tissue.
© 2018 Macmillan Publishers Limited, part of Springer Nature. All rights reserved.
NATuRe RevIeWS | NEuROlOgy
R e v i e w s
volume 14 | JuNe 2018 | 327

counteracted microcirculatory compromise. Likewise, in rodent models, NBO did not interfere with — and did in fact promote — the fibrinolytic effects of tPA without increasing the risk of brain haemorrhage42,43,56,64,65. NBO also prevented tPA related deleterious effects on the neurovascular unit43. Importantly, NBO was not detrimental if administered after intraparenchymal haemorrhage40,66, which can be mistaken for ischaemic stroke in pre hospital settings before imaging.
NBO has been tested in a number of clinical trials, but this Review addresses only RCTs that explored NBO as a neuroprotective strategy in hyperacute ischaemic stroke. Accordingly, four trials that aimed to prevent secondary hypoxic episodes by means of oxygen supplementation up to 24 h after stroke onset67–71 will not be reviewed.
Note that the current recommendation is to administer supplemental oxygen only whenever saturation falls below 95%72. Breathing 100% oxygen can depress respiratory drive and cause hypercapnia and acidosis; therefore, this intervention is contraindicated in patients with chronic pulmonary disease or conditions that cause reduced respiratory drive. Pulmonary complications occur only if NBO is administered for > 16 h.
Two small scale, phase II RCTs that meet the eligibility criteria for inclusion in this Review have been published to date36,73. These trials documented the feasibility and safety of NBO but showed no clinical benefit. However, neither trial specifically tested the penumbral freezing paradigm, although one did document penumbral freezing during NBO.
Box 1 | The penumbral freezing paradigm
The figure depicts an idealized time course of the ischaemic penumbra and core in various scenarios after stroke. In the real world, accurate mapping of the penumbra and core is challenging.
The top row shows the typical natural history of tissue evolution after acute middle cerebral artery (mCA) occlusion. By 3 h after stroke onset, the centre of the mCA territory, where perfusion is lowest, is irreversibly damaged. This ‘core’ is surrounded by a rim of ‘penumbra’, where perfusion is better preserved owing to leptomeningeal collaterals, which are fed by the neighbouring anterior and posterior cerebral arteries. Without recanalization, more penumbra progresses to core tissue. eventually, the at- risk penumbra turns into core, and no salvageable tissue remains. The final infarct, which comprises the initial core and penumbra, is large, causing severe disability (modified Rankin Scale (mRS) score 5). The final infarct size is not the only determinant of final outcome: infarct topography, age, comorbidities, previous stroke and white matter ischaemic changes are also important factors.
The second row illustrates the benefits of recanalization achieved at 4.5 h, which stops core growth, resulting in a smaller final infarct and an mRS score of 3 — much better than with no reperfusion but still above the threshold for functional independence (mRS score 2). If recanalization fails, the outcome is the same as in the natural history scenario.
The third row shows the effects of freezing therapy initiated on hospital admission, which enables core growth to stop until recanalization is achieved 1.5 h later. owing to extensive penumbral salvage, the final infarct is the same size as the core on admission, and the patient achieves functional independence (mRS score 2). Again, if thrombectomy fails, the final outcome is the same as in the natural history scenario.
The fourth row illustrates the theoretical effects of efficacious freezing therapy started in the field 1.5 h after stroke onset. This strategy allows maximal penumbral salvage and minimal final infarct, resulting in mild residual symptoms but no functional disability (mRS score 1).
Freezing therapy
3 4.5
Final infarctHospital admission(3 Recanalization 1.5 h later Failed recanalization
Final infarct
Penumbra
mRS score 3
mRS score 5
mRS score 2
mRS score 1
mRS score 5
mRS score 5
mRS score 5
Pre-hospital
Natural history(no reperfusion therapy)
Standard management
Penumbral freezingstarted on admission
Penumbralfreezing started inthe field
Freezing therapy
Core
© 2018 Macmillan Publishers Limited, part of Springer Nature. All rights reserved.
www.nature.com/nrneurol
R e v i e w s
328 | JuNe 2018 | volume 14

The first trial36 recruited 16 patients with proximal occlusion and diffusion–perfusion mismatch (DPM) up to 12 h from stroke onset. Candidates for IVT were excluded a priori. Eligible patients were randomly assigned to high flow NBO (45 l/min) for 8 h or to standard care. At 3 months, NIH Stroke Scale (NIHSS) scores were nonsignificantly lower in the NBO group than in the controls. The primary end point was lesion growth, as assessed by diffusion weighted imaging (DWI), at 4 h (that is, during NBO). The controls exhibited a mean 49% increase in lesion volume compared with a 12% decrease in the NBO group (P = 0.004; subsequently confirmed in a slightly larger sample74). As the hypo perfused tissue volume was stable in both groups, one can conclude that penumbral freezing was truly achieved in the NBO group. However, the differences in lesion volumes between the two groups had vanished on the 24 h, 1week and 3month follow up MRI scans.
These observations36, which are strikingly similar to those reported above in rodents, provide documentation of penumbral freezing in humans under high flow NBO. However, as in rodents, and as predicted by the penumbral freezing paradigm (box 1), with persistent occlusion the benefit vanished after a few hours, and the penumbra eventually progressed to infarction despite continuing NBO. The clinical deficits mirrored the imaging findings. By the 4 h time point, NIHSS scores had decreased in the NBO group and increased slightly in the control group (P = 0.099). These effects reached statistical significance at 24 h and 1 week but vanished thereafter. Interestingly, magnetic resonance spectroscopy revealed that NBO prevented lactate build up in the ischaemic tissue, indicating improved aerobic metabolism75. Once again, this effect was lost after NBO was discontinued. Although these studies did not report the exact timing of NBO initiation relative to stroke onset, they suggest that in patients with DPM, the therapeutic window for NBO is at least 4 h if the therapy is started within 12 h of stroke onset, which is a promising feature and should encourage trials combining NBO and thrombectomy.
The other RCT73 had a similar design and included 40 patients with DPM ≤ 12 h from stroke onset who were ineligible for IVT. The participants were randomly assigned to NBO (10 l/min) for 12 h or standard care. At variance with the RCT described above, monitoring during NBO was not planned. The mean time from stroke onset to randomization was 8.5 h. NBO had no significant effects on NIHSS scores at day 7, mRS scores at 3 months, or lesion volumes at 24 h and 3 months, as measured by MRI. Recanalization was not assessed.
A larger phase IIb RCT of NBO has now been carried out; this trial has not yet been published, and only fragmentary information is available76. This trial enrolled patients within 9 h of stroke onset and excluded candidates for IVT until 60 participants had been recruited. High flow NBO (30–45 l/min) was delivered for 8 h. Unfortunately, the trial was stopped prematurely after 85 participants had been recruited, owing to increased mortality in the NBO arm. This finding was not directly attributed to NBO but was thought to be related to inclusion of patients with massive infarcts. Although it is difficult to draw firm conclusions until the results are published, a possible lesson from this trial is that patients with severe strokes should be excluded from NBO RCTs.
In a pilot RCT of NBO (10 l/min for 4 h), which recruited nine IVT eligible patients per arm77, significantly better neurological recovery was found up to 1 week poststroke in the NBO arm. However, later assessments and mRS data were not provided, and recanalization was not evaluated. In an independent sample, NBO was found to significantly reduce blood markers of blood–brain barrier damage.
In summary, although none of the above trials were designed to test the penumbral freezing paradigm per se, the fact that high flow NBO achieved prolonged penumbral freezing in appropriate candidates, even when started hours after stroke onset, is a strong incentive to test NBO in patients who are eligible for mechanical thrombectomy. A proof ofconcept RCT known as PROOF, which is designed to test the penumbral freezing hypothesis by including only candidates for mechanical thrombectomy in whom perfusion imaging will be conducted, has recently been funded78. This trial will primarily test whether NBO started ≤ 3 h from stroke onset and administered for ≤ 4 h reduces core growth. Pre hospital NBO administration might be considered as the trial progresses, possibly using mobile stroke units (MSUs) equipped with CT79,80.
Perfluorocarbons. PFCs are inert chemicals that are administered as an intravenous emulsion. They have a large oxygen carrying capacity and can release oxygen into hypoxic tissues. PFCs substantially enhance the effects of inhaled oxygen when the two interventions are administered in combination. In addition, owing to their small molecular size, PFCs can carry oxygen more freely to tissue with compromised microcirculation than can erythrocytes.
In a 2 h tMCAO model, PFCs combined with NBO significantly reduced infarct size 2.5fold to 4fold in a dose dependent manner compared with NBO alone81.
Cerebral blood flow CMRO2
Oxygen extraction fraction
a b c
Fig. 1 | The ischaemic penumbra in humans. Single- slice depiction of the ischaemic penumbra (arrows) in a patient with acute proximal middle cerebral artery (MCA) occlusion showing severe hypoperfusion throughout the cortical MCA territory (part a), which constrains the oxygen supply , together with relatively preserved oxygen consumption (cerebral metabolic rate of oxygen (CMRO2); part b), resulting in severe tissue hypoxia and increased oxygen extraction fraction (part c). These images were obtained using 15O2 triple- gas PET3. Figure adapted with permission from ref.175, Oxford University Press.
© 2018 Macmillan Publishers Limited, part of Springer Nature. All rights reserved.
NATuRe RevIeWS | NEuROlOgy
R e v i e w s
volume 14 | JuNe 2018 | 329
Similar large effects were reported with pMCAO in both rabbits82,83 and rats84, although the infarct was evaluated too early for meaningful conclusions to be drawn. Two additional pMCAO studies (again with early assessment of ischaemic damage) found no effect85 or a small but significant effect of PFCs combined with NBO86. In another pMCAO study, PFCs plus NBO delayed infarct growth for 4 h (ref.87).
Overall, despite the suboptimal quality of some of the data, the findings described above suggest that PFCs can induce significant infarct reduction in tMCAO and slow down infarct progression in pMCAO, consistent with penumbral freezing. Given the cumbersome logistics involved in delivering high flow NBO to patients with acute stroke, PFCs could allow the NBO dose to be reduced without loss of efficacy. Clinical trials of this approach are warranted, and a UK based phase II trial testing the PFC ABL101 plus moderate NBO versus NBO alone will start soon (K. W. Muir, personal communication).
An interesting so called ‘theranostics’ approach exploits the penumbra’s avidity for oxygen as compared with the core. In this approach, PFCs in conjunction with moderate NBO are used not only as potential therapy but also as imaging contrast agents for T2* MRI88. Another strategy, which has been piloted in rodents89, involves superselective arterial infusion of high concentration PFCs, which could be delivered during thrombectomy.
Of note, new pegylated oxygen carriers are being developed, either coupled with carbon monoxide
delivery to enhance collateral vasodilation (shown to be efficacious in 2 h tMCAO models90,91) or endowed with enhanced oxygen delivery capacity (under development by Omniox).
Increasing retrograde perfusionThe second main approach to enhancement of penumbral oxygen supply involves increasing retrograde perfusion via leptomeningeal collaterals92–94. An added benefit of this approach is enhanced tPA access to the distal end of the clot, potentially promoting recanalization. In addition to several largely empirical general physiological measures, candidate interventions include transient descending aortic balloon occlusion (TAO), remote ischaemic perconditioning (RIPerC), sensory stimulation and sphenopalatine ganglion stimulation (SPGS).
General physiological measures. Physiological measures such as the head down bed position and pharmacologically induced hypertension92,93 target pressure dependent penumbral perfusion. Anecdotal reports suggest that head down tilt improves clinical deficit and increases CBF in patients with large vessel occlusions, with the head up position having the converse effect (reviewed previously95). Interestingly, in a recent rat study, the head down tilt intervention led to marked reductions in infarct volume and increases in CBF96. Pharmacologically induced hypertension has similar preclinical effects (reviewed previously97) and has been tested in a few small scale, open label clinical studies, which did not, however, target hyperacute stroke (reviewed previously98).
Transient descending aortic balloon occlusion. Similar to pharmacologically induced hypertension, temporary balloon occlusion of the abdominal aorta increases intracranial perfusion pressure92,93, improves penumbral perfusion and markedly decreases infarct volume in both pMCAO and tMCAO models99,100, and reduces mortality in severe hemispheric ischaemia101. A related but less wellstudied procedure involves electrocardiogram gated external counterpulsation using lower limb pressure cuffs inflated up to 300 mmHg to provoke retrograde aortic blood flow102.
The SENTIS phase IIb RCT103 showed TAO to be safe but neutral on outcome, though with a trend for reduced mortality. However, this study did not address penumbral freezing, as candidates for reperfusion therapies were excluded and TAO was started up to 14 h after stroke onset. Given the strong physiological underpinning and apparent safety of TAO, such a trial would be warranted. TAO was shown to be safe in an open label trial104, although implementation of this approach in mechanical thrombectomy eligible individuals is likely to be challenging.
Remote ischaemic preconditioning. RIPerC — that is, limb ischaemia delivered during the acute phase of ischaemic stroke — has many biological effects, but its neuroprotective effects are thought to derive from release of signalling molecules that dilate leptomeningeal anastomoses and improve penumbral perfusion105,106.
0
20
40
60
80
100
0 1 2 3 4 5 6 7
Duration of occlusion (h)
Permanent
Red
ucti
on in
isch
aem
ic le
sion
siz
e (%
)
Fig. 2 | Effects of normobaric hyperoxia on infarct volume. In this plot, which is based on data from rodent studies reporting a total of 43 comparisons12,21,23,29,35,37,39–53, the x- axis shows duration of middle cerebral artery occlusion (MCAO) and the y- axis shows percentage reduction in infarct volume. Red dots indicate statistically significant reductions in infarct volume, and blue dots indicate nonsignificant effects. The black dot represents a study in which the infarct volume reduction for cortex plus striatum was large (45%) but did not reach statistical significance, but was 96% and significant for the cortex alone49; this study will be considered positive for the statistical analysis. In four of eight studies of permanent MCAO, the effects were statistically significant, although the reduction in lesion volume was small (≤20%) in three of these four studies. The graph shows a strong inverse relationship between infarct volume reduction and MCAO duration. This relationship is confirmed by statistical analysis (assigning an occlusion duration of 8 h for permanent MCAO data), which reveals a highly significant negative correlation (r = −0.445, P = 0.003).
Leptomeningeal collateralsarteriolar channels that anatomically connect the distal field arteriolar branches of the anterior, middle and posterior cerebral arteries at the cortical surface.
© 2018 Macmillan Publishers Limited, part of Springer Nature. All rights reserved.
www.nature.com/nrneurol
R e v i e w s
330 | JuNe 2018 | volume 14

Accordingly, RIPerC substantially reduces early damage106 and infarct size in tMCAO107,108. In embolic MCAO, RIPerC significantly improved CBF and reduced both infarct size and neurological deficit109,110. These effects were enhanced by coadministration of tPA, consistent with penumbral freezing. This straightforward and directly translatable intervention has definite clinical potential and could be easily implemented in the field by paramedics using a simple pressure cuff.
In a phase IIb trial of pre hospital RIPerC within 24 h of suspected ischaemic stroke, post hoc adjustment for baseline perfusion and diffusion lesion severity revealed significantly larger penumbral salvage (the primary end point) in the tPA treated subgroup. However, after stratification for evidence of recanalization on 24 h imaging, no differential benefit was observed111; in fact, contrary to the expected effects, RIPerC seemed to benefit patients without occlusion and individuals in whom recanalization was unsuccessful. Of note, the samples were small and therapy was started before baseline MRI, which, together with the low recanalization rates from IVT and the delayed assessment of recanalization, might account for these disappointing findings. Importantly, this study confirmed the safety of RIPerC in this setting. Another phase IIb trial, RESCUE, in which leg ischaemia is started ≤ 6 h after stroke onset and both IVT and mechanical thrombectomy are permitted, is ongoing112. The primary end point is lesion growth on DWI. Though not designed to directly address penumbral freezing, this trial should provide important information.
Sensory stimulation. Sensory stimulation has recently emerged as a potential nonpharmacological acute stroke therapy. As no clinical studies have been published so far, only preclinical findings are addressed here.
Similar to physiological stimulation113, sensory stimulation is predicted to increase penumbral perfusion owing to at least partially preserved neurovascular coupling (NVC). A long held belief was that under ischaemic conditions, the brain vasculature would be fully vasodilated as an autoregulatory response to low perfusion pressure. However, in a cat model, Strong et al.114 documented the occasional presence of marked CBF responses to direct electrical stimulation in the penumbra, pointing to a vasodilation reserve that can be harnessed by neuronal stimulation. Although the absolute CBF increase was modest, it was sizeable considering the severe hypoperfusion that prevailed in the penumbra. Preserved — though markedly reduced — CBF responses were subsequently found in rats115,116 in proportion to ischaemia induced attenuation of somatosensory evoked potentials (SSEPs), suggesting maintenance of NVC. Stimulation induced increases in CBF should extend the lifetime of the penumbra5, but the accompanying increases in neuronal energy requirements could lead to worsening of neuronal ischaemia. Supporting this potentially detrimental scenario, the linear relationship between CBF responses and SSEPs was found to be preserved in severe ischaemic conditions115, and in another study, sensory stimulation failed to evoke local PtO2 increases116.
Supplementary Table 2 summarizes the findings from the 15 rodent acute stroke studies on sensory stimulation that have been published to date. The 13 published rat studies117–129 originate from 3 groups based in Irvine, Singapore and Philadelphia (seven, four and two studies, respectively). Six of the rat studies implemented contralateral forepaw stimulation and the other seven (all from Irvine) used whisker stimulation.
All but one117 of the rat studies investigated pMCAO, which is suboptimal with respect to the penumbral freezing paradigm. Nevertheless, most studies showed significant and sometimes spectacular effects of sensory stimulation on infarct volume, which depended on the timing of the stimulation relative to MCAO induction. Sensory stimulation that was started immediately or within 15 min of MCAO (+0 h) had significant effects in 10 of 13 studies117–125,128 (including the tMCAO study117), a large effect (P values not reported) in 2 studies127,129 and no effect in 1 study126. These inconsistencies might have been attributable to differences in the sensory stimulation protocol: the Irvine team used whisker stimulation, whereas the others stimulated the forepaw. All seven of the Irvine studies118–124 reported complete protection (100% reduction in infarct volume). This finding, which was replicated in aged rats122, is virtually unprecedented in the stroke neuroprotection literature, especially with respect to pMCAO. The benefits of immediately applied sensory stimulation did not depend on the anaesthetic regimen124. Importantly for clinical translation, the Irvine group achieved complete neuroprotection with ‘natural’ sensory stimulation (that is, spontaneous exploratory behaviour in an enriched environment) versus usual environment in awake rats123.
Sensory stimulation that was started 1 h into MCAO (+1 h) provided complete protection in one Irvine study120 but produced only small, nonsignificant reductions in infarct size in a study from Singapore125. With sensory stimulation started at 2 h, effects were inconsistent in two Irvine studies120,121 and absent in one Singapore study125. Studies of sensory stimulation that was started at 3 h (all from Irvine) reported significantly larger infarcts relative to the no stimulation group in four studies118,120,121,124 and no difference in one123. In summary, immediate sensory stimulation was beneficial in most studies, a 1 h start was less effective but still beneficial, a 2 h start had neutral effects and a 3 h start seemed to be detrimental.
The Philadelphia group found that sensory stimulation improved behavioural outcomes in their tMCAO study117 but not in their follow up pMCAO study126. The Irvine team found that behavioural outcome on day 7 was significantly better in the + 0 h group than in the + 3 h group120 and was normal at 4 months in + 0 h rats. However, this study did not include no stimulation controls. In the Irvine study on aged rats, behavioural function at day 7 was significantly better in treated animals than in no stimulation controls on some but not all tasks122.
Limitations of the studies include the occasional lack of no stimulation controls; the absence of P values in some of the articles from Singapore; and the fact that infarct assessment was often carried out at too early a
Neurovascular coupling(NVC). a physiological process whereby neuronal activity, which increases neuronal energy metabolism, leads to dilation of the neighbouring vascular tree, causing increased local perfusion and, hence, delivery of energetic nutrients.
Somatosensory evoked potentials(SSePs). Discrete electrical responses to somatosensory stimulation occurring in the specialized neurons of the somatosensory cortex and recordable using various techniques.
© 2018 Macmillan Publishers Limited, part of Springer Nature. All rights reserved.
NATuRe RevIeWS | NEuROlOgy
R e v i e w s
volume 14 | JuNe 2018 | 331

stage (24 h), especially for pMCAO. In addition, randomized group allocation and blinded infarct assessment were mentioned in a minority of studies, and sample size calculation was mentioned only in one study (Supplementary Table 2). Finally, publication bias130 cannot be ruled out.
Information regarding the underlying mechanisms of sensory stimulation related neuroprotection is scarce and inconsistent. The Irvine group reported improved surface cortical blood flow in + 0 h treated rats, both during sensory stimulation121 and 24 h later120. These findings suggest improved ischaemic territory perfusion during stimulation, consistent with preservation of NVC. However, two studies from Philadelphia using forepaw stimulation reported no increase in CBF during sensory stimulation117,126. The Irvine group consistently found complete recovery of SSEPs — assessed by the haemodynamic response — during sensory stimulation, which again indicates NVC preservation. At 24 h, consistent with reported tissue outcomes, SSEPs were normal in the + 0 h group but absent in the + 3 h groups. Similar findings were reported by the Singapore group127,129 (Supplementary Table 2).
At first sight, the observation that sensory stimulation can afford neuroprotection despite permanent occlusion conflicts with the notion that any benefit is bound to vanish unless the hypoxic tissue is eventually reperfused131–133. In one Irvine study, CBF at 4 months was 40–50% of the normal value distal to the pMCAO119, indicating moderate chronic hypoperfusion. Sensory stimulation, delivered acutely, might permanently ‘reset’ the NVC, for example, via vascular remodelling or altered neuron–vessel coupling, which in turn would permanently protect the tissue despite persistent occlusion. Another more mundane possibility is that the improved penumbral perfusion that results from sensory stimulation (or any other intervention with a similar target) is a consequence of an increase in blood pressure following withdrawal of general anaesthesia, such that tissue originally defined as ‘penumbra’ while under anaesthesia permanently adopts a benign hypoperfusion status.
Two mouse studies of sensory stimulation have been published to date134,135. In one study, forelimb stimulation that was started 10 min after pMCAO consistently induced larger infarcts relative to controls, whereas whisker stimulation had no significant effect134. Interestingly, the former but not the latter paradigm was associated with markedly increased PIDs, together with a twofold larger area in which CBF was < 30%, and reduced oxyhaemoglobin levels. These findings suggest the occurrence of PID induced increases in neuronal activity in the face of decreased perfusion, which in turn worsened tissue hypoxia and abolished NVC. Interestingly, in one rat study, forepaw stimulation also doubled PID frequency in parallel with no CBF improvement or infarct size reduction126. The neutral effects of whisker stimulation on both PIDs and infarct volume in mice134 were thought to reflect the topographical difference between the barrel field, which lies well within the MCA territory, and the forelimb area, which lies at its borders. Thus, in mice, whisker stimulation would target irreversibly injured
tissue, where PIDs cannot occur, whereas forelimb stimulation would target the MCA penumbral border, where PIDs can be generated. Another observation from this mouse study, which could have translational implications, was that concurrent NBO prevented the increased PIDs that were observed with forelimb sensory stimulation.
In a recently published study135, the Irvine group subjected two different mouse strains to the + 0 h single whisker sensory stimulation paradigm that had proved strikingly effective in their rat studies. However, no benefits with regard to infarct volume or SSEPs were found in either strain. These marked species differences in the effects of early sensory stimulation may reflect the less welldeveloped collateral system — in particular, fewer pial collaterals and intra- tree anastomoses and a frequently incomplete circle of Willis — in mice135,136. It would be interesting to assess the effects of sensory stimulation in spontaneously hypertensive rats, which also have fewer functional leptomeningeal collaterals and show more rapid transition from penumbra to core than do normotensive rats55,137–140. This model would have clinical relevance, as spontaneously hypertensive rats represent the untreated hypertensive condition. Given that the benefits of sensory stimulation seem to depend on collateral status, sensory stimulation might not benefit patients with chronic hypertension.
When designing pilot safety and feasibility studies of sensory stimulation in humans, investigators must consider several factors. First, patient selection should be based on the presence of penumbra and/or good collaterals together with a small core on admission imaging, so as to enrich the sample with potential responders. Second, different sensory stimulation modalities, including somatosensory, verbal and visual, should be evaluated. Third, the most appropriate ‘control’ condition (no stimulation or limited stimulation) requires careful assessment. Fourth, the time window for the benefits and safety of sensory stimulation seems to be narrow, which could make implementation of this approach challenging. However, as the technique is fairly straightforward, initiation in the field before hospital admission might be feasible. Fifth, the possibility of combining sensory stimulation with mechanical thrombectomy, as per the penumbral freezing paradigm, needs to be explored. Last, patients must be monitored closely for potential deterioration during and early after sensory stimulation.
Although the single tMCAO study published so far117 supports the idea that sensory stimulation can freeze the penumbra, the data await replication, and different sensory stimulation modalities and tMCAO durations need to be assessed. As all the preclinical rat studies to date originated from the same three groups, replication by other groups is warranted.
Sphenopalatine ganglion stimulation. By activating the parasympathetic fibres that travel along the facial nerve, SPGS triggers vasodilation in the anterior circulation92,93,141. In rats with pMCAO, SPGS was found to freeze the penumbra, reduce infarct volume and
Intra- tree anastomosesVascular connections similar to leptomeningeal collaterals but occurring between arterioles belonging to the same vascular system (for example, the middle cerebral artery).
Circle of WillisThe vascular channels connecting the anterior and posterior circulation and the right and left hemisphere arterial systems, situated at the base of the brain and, when complete, forming a continuous circle of connecting arteries.
© 2018 Macmillan Publishers Limited, part of Springer Nature. All rights reserved.
www.nature.com/nrneurol
R e v i e w s
332 | JuNe 2018 | volume 14

improve behavioural outcomes despite only modest increases in CBF142,143. Similar benefits with regard to infarct volume and behaviour were also found after photothrombotic infarction144, a model with marginal clinical relevance.
Although replication of these positive findings is warranted, clinical translation is already underway, as SPGS is easy to implement. Following a positive feasibility study, a phase IIb/III RCT (ImpACT24 (ref.145)) is ongoing146. Unfortunately, this study is not designed to test the penumbral freezing paradigm, as reperfusion therapy is an exclusion criterion, and treatment can be started up to 24 h after stroke onset.
Reducing the tissue’s energy needsTwo main nonpharmacological approaches that aim to reduce the penumbra’s neuronal activity and energy needs — hypothermia and cathodal transcranial direct cortical stimulation (C tDCS) — are currently being considered.
HypothermiaHypothermia is the single most potent known inhibitor of neuronal activity and has provided strong neuroprotection in various subtypes of experimental acute brain injury, including stroke147,148. Consequently, therapeutic hypothermia forms part of the routine management of patients with cardiac arrest or global brain ischaemia. The effects of therapeutic hypothermia in focal cerebral ischaemia have been extensively studied since the mid20th century, with well over 100 published rodent studies reporting more than 200 comparisons in the past 25 years alone. Critically, therapeutic hypothermia not only affords protection against ischaemic injury but also potently inhibits post reperfusion deleterious events that affect the neurovascular unit, including endothelial injury, blood–brain barrier opening, entry of blood borne white cells into the brain tissue and production of oxygen free radicals60. This unique dual effect makes hypothermia an extremely attractive stroke therapy that could be administered both before and after recanalization.
Rather than present a detailed review of the experimental and clinical literature on therapeutic hypothermia in stroke, I shall highlight several recently published high quality and detailed progress reviews, systematic reviews and meta analyses131,147–153.
Preclinical studies. In a 2007 meta analysis of therapeutic hypothermia, van der Worp et al. reported an overall infarct volume reduction of 43.5% (95% CI 40.1–47.0%) in animals that received this intervention151. Relevant to the present Review, this effect was much larger with tMCAO than with pMCAO (mean ~46% and 37%, respectively), consistent with the aforementioned idea that neuroprotection is of limited benefit unless early perfusion takes place (box 1). Two particularly well designed studies that used identical experimental protocols clearly demonstrated this differential effect154,155.
Subanalyses in the seminal review by van der Worp et al. highlighted several salient points151. First, no clear
effect of tMCAO duration on effect size was observed. Second, the effect size was largest with hypothermia that straddled the ischaemia and reperfusion phases, although therapeutic hypothermia was still efficient if delivered only during reperfusion. Third, the effect was most robust if hypothermia was started before or at the time of MCAO. Fourth, a significant relationship between effect size and target temperature was observed, with the lowest temperatures having the greatest effects, although even modest cooling to 35 °C had significant benefits. Fifth, adverse effects were more prominent with the lowest target body temperatures. Last, improvements in neurological and behavioural functions paralleled the positive effects on infarct size.
In a subsequent meta analysis of 216 comparisons149, therapeutic hypothermia was associated with a mean infarct volume reduction of 44.4%, which is very close to the figure reported by van der Worp’s et al.151. In the studies that were included in this meta analysis, therapeutic hypothermia was started from 60 min before MCAO to 180 min after MCAO, and the target cooling temperature ranged from 14 °C to 35 °C, with a duration of up to 24 h. Accordingly, substantial heterogeneity in effect size was reported. No significant effects of cooling degree, modality (whole body, focal intra arterial or local), delay or duration were observed, although the samples were often small. Again, highly significant beneficial effects of therapeutic hypothermia on behavioural impairment were consistently reported. Unfortunately, no attempt was made to separate pMCAO from tMCAO in this meta analysis.
Given the in vitro effects of cooling on coagulation, including fibrinolysis, an important translational issue is whether therapeutic hypothermia is safe in conjunction with tPA. Experimental studies have shown that moderate hypothermia does not interfere with thrombolysis156,157 and does not increase the rate of parenchymal haemorrhage131. Several RCTs have combined thrombolysis with intravascular cooling (via a central catheter), with no complications reported (see below). In 2010, van der Worp et al. reviewed the implications of the animal work for trial design150.
Clinical trials. A 2013 review148 summarized nine pilot or phase II trials of therapeutic hypothermia in hyperacute stroke. Importantly, these trials documented the feasibility of both surface and endovascular cooling in this setting. Early trials that assessed surface cooling reported no clear effects on outcome, although several problems were experienced, including slow achievement of therapeutic hypothermia, partly due to skin vasoconstriction, and marked shivering (even with modest cooling to ~34 °C (ref.158)). In addition, serious adverse effects were reported, especially with low target temperatures (~32 °C). Subsequent trials implemented endovascular cooling via cold saline infusion into the vena cava in association with anti shivering medication (meperidine). All four endovascular cooling neuroprotection trials were small scale and only three were actual RCTs; no indication of efficacy was observed148. Two further RCTs have been published since this review appeared. One used a combination of surface and
© 2018 Macmillan Publishers Limited, part of Springer Nature. All rights reserved.
NATuRe RevIeWS | NEuROlOgy
R e v i e w s
volume 14 | JuNe 2018 | 333

endovascular cooling159 and the other used endovascular cooling only160. Neither showed significant benefits; however, both were underpowered, and one was stopped prematurely.
Importantly, most trials have documented serious adverse effects of therapeutic hypothermia delivered for 12–48 h with target temperatures of 33–35 °C. These effects included increased mortality and incidence of pneumonia, with the latter being attributed mainly to aspiration from the anti shivering agents when administered to non sedated and non ventilated patients160. In the ICTuS2 trial160, pneumonia rates were not substantially reduced despite daily clinical assessments, which enabled early antibiotic treatment. Although reducing the duration and depth of therapeutic hypothermia decreases the chance of pneumonia, this benefit is offset by reduced neuroprotection150.
Unfortunately, no therapeutic hypothermia trial has specifically tested the penumbral freezing paradigm by delivering hypothermia to candidates for mechanical thrombectomy. In the two recent RCTs cited above159,160, therapeutic hypothermia was administered to IVT treated patients but was often initiated several hours after IVT, and early recanalization was not assessed in either study, precluding evaluation of benefits in conjunction with reperfusion. Given the low recanalization rates associated with IVT, negative findings do not preclude the possibility that moderate therapeutic hypothermia could improve outcomes if administered as an adjunct to mechanical thrombectomy. A phase III RCT of endovascular or surface cooling at 34–35 °C started at ≤ 6 h (Euro HYP1)161 is ongoing, but does not specifically target candidates for reperfusion therapies and is being hampered by slow recruitment, probably because of the recent shift in emphasis towards mechanical thrombectomy. Interestingly, in a nonrandomized study that compared cohorts from two different centres where patients routinely underwent endovascular therapy162, moderate endovascular therapeutic hypothermia — implemented at one centre only — was significantly associated with reduced oedema formation and haemorrhagic transformation and fewer poor outcomes. Though anecdotal, this study points towards potential benefits from therapeutic hypothermia deli vered both before and after mechanical thrombectomy. ICTus3, a trial to test endovascular cooling in association with mechanical thrombectomy, is reported to be at the planning stage160. However, implementation of hypothermia before thrombectomy will probably prove to be logistically difficult given the increasingly rapid care pathways, the time consuming procedures involved in therapeutic hypothermia, such as vena cava catheterization, and the need to swiftly achieve target temperatures.
Selective intra- arterial cooling. Selective intra arterial cooling (SIAC) might afford more rapid and profound local brain hypothermia than whole body hypothermia while limiting the associated adverse effects163. In animal models, this approach, whether administered during or only after tMCAO, resulted in markedly reduced lesion volumes (reviewed previously163). In clinical practice, SIAC would be started in
conjunction with mechanical thrombectomy and, given the typically short procedural time for thrombectomy, its main target would be reperfusion injury, perhaps including capillary obstruction causing the no reflow phenomenon164. However, as alluded to above, even short lasting penumbral cooling might be beneficial. Therefore, SIAC would represent an attractive double edged therapy. A pilot study has demonstrated the feasibility and safety of this approach165, and RCTs are now warranted to test efficacy.
Cathodal tDCSC tDCS is a non invasive and painless neurostimulation method in which application of a weak direct electrical current to the skull between anodal and cathodal electrodes allows modulation of the excitability of underlying cortical neurons. C tDCS hyperpolarizes neuronal membranes and, consequently, has inhibitory effects on cortical networks166,167. Given its poor spatial resolution, C tDCS is likely to induce widespread effects across the hemisphere, even in humans, which is relevant to stroke therapy.
Three rodent studies have examined the effects of C tDCS delivered over the ischaemic hemisphere on infarct volume. In one study168, C tDCS delivered for 60 min, starting 30 min into 90 min tMCAO, significantly reduced infarct size (by 37%) relative to controls but was not effective if applied 4.5 h after MCAO. By contrast, early applied anodal tDCS, which increases neuronal activity166,167 and, hence, might aggravate neuronal oxygen deprivation in ischaemic conditions, mildly increased the lesion volume. In another study169, C tDCS significantly reduced infarct volume (by 20–30%) when administered for 4 h or 6 h after pMCAO. In parallel, PID density was markedly reduced by C tDCS and correlated with infarct volume. In the third study129, C tDCS again resulted in mild reductions (~25%) in infarct volume after branch pMCAO.
Taken together, these early studies suggest that C tDCS only modestly reduces infarct volume, apparently via PID blockade. Given its widespread hemispheric effects and non invasive nature, which potentially allows pre hospital administration, the translational potential of C tDCS is high. However, further studies are needed to replicate the above findings and test other stimulation protocols. STICA, a single centre, hospital based pilot safety and feasibility RCT targeting candidates for mechanical thrombectomy, with infarct growth as the primary end point, was recently initiated in Paris, France.
ConclusionsTable 1 summarizes the main features of the interventions detailed above, including factors with clinical implications, such as strength of preclinical effects, translatability and potential adverse effects.
While acknowledging the limitations of the preclinical studies and clinical trials conducted to date54,170, this Review has highlighted a number of nonpharmacological interventions that hold promise to slow down the demise of the penumbra as an adjunct to mechanical thrombectomy and to improve functional outcomes over
© 2018 Macmillan Publishers Limited, part of Springer Nature. All rights reserved.
www.nature.com/nrneurol
R e v i e w s
334 | JuNe 2018 | volume 14

and above the documented benefits of thrombectomy. By constraining infarct growth, these interventions might also make patients who are normally excluded from mechanical thrombectomy eligible for this treatment, thereby increasing the number of treated patients, not only within but also beyond the currently approved time windows171,172. Importantly, delivery of these interventions at the pre hospital stage, in the ambulance or in an MSU, would maxi mize the benefits (box 1). Pre hospital stroke trials are feasible11 and will be facilitated by national stroke trial networks such as STROKENET in the USA173 and the international pre hospital stroke treatment network174. Pre hospital trials of nonpharmacological interventions are particularly attractive given the expected innocuity of these interventions in patients with ischaemic stroke (but see the caveats outlined above) as well as in those with haemorrhagic stroke or stroke mimics, although confirmation in pilot studies is required. Any concerns might be further allayed if MSUs with both a CT scanner and a stroke physician on board become routine.
Crucially for trial design, none of these interventions have any added adverse effects if continued into the
reperfusion phase — a situation that might occur in the clinical setting owing to spontaneous or IVTinduced reperfusion. Importantly, continuation of hypothermia into the reperfusion phase seems to enhance the benefits of this intervention.
The design of clinical trials of potential penumbral freezing interventions poses substantial challenges, including pre hospital treatment delivery, consent in the emergency situation, care pathways (notably with the ‘drip- and- ship’ paradigm), patient selection, whether therapy should be continued during and after mechanical thrombectomy, clinical versus imaging outcomes as a primary end point and whether the clinical end point should be functional outcome or number of patients receiving mechanical thrombectomy. Funding is an added challenge with respect to trials of nonpharmacological therapies, although the EU funded PROOF study has set an important precedent in this regard. Given the major potential benefits of penumbral freezing, these challenges should not be seen as obstacles to progress.
Published online 19 April 2018
1. Feigin, V. L. et al. Global burden of stroke and risk factors in 188 countries, during 1990–2013: a systematic analysis for the Global Burden of isease Study 2013. Lancet Neurol. 15, 913–924 (2016).
2. Astrup, J., Siesjo, B. K. & Symon, L. Thresholds in cerebral ischemia — the ischemic penumbra. Stroke 12, 723–725 (1981).
3. Baron, J. C. Mapping the ischaemic penumbra with PET: implications for acute stroke treatment. Cerebrovasc. Dis. 9, 193–201 (1999).
4. Powers, W. J. et al. 2015 American Heart Association/American Stroke Association focused update of the 2013 guidelines for the early management of patients with acute ischemic stroke regarding endovascular treatment: a guideline for healthcare professionals from the American Heart Association/American Stroke Association. Stroke 46, 3020–3035 (2015).
5. Jones, T. H. et al. Thresholds of focal cerebral ischemia in awake monkeys. J. Neurosurg. 54, 773–782 (1981).
6. Seners, P. et al. Incidence and predictors of early recanalization after intravenous thrombolysis: a systematic review and meta- analysis. Stroke 47, 2409–2412 (2016).
7. Goyal, M. et al. Endovascular thrombectomy after large- vessel ischaemic stroke: a meta- analysis of individual patient data from five randomised trials. Lancet 387, 1723–1731 (2016).
8. Cook, D. J., Teves, L. & Tymianski, M. Treatment of stroke with a PSD-95 inhibitor in the gyrencephalic primate brain. Nature 483, 213–217 (2012).
9. Fisher, M. & Saver, J. L. Future directions of acute ischaemic stroke therapy. Lancet Neurol. 14, 758–767 (2015).
10. Tymianski, M. Combining neuroprotection with endovascular treatment of acute stroke: is there hope? Stroke 48, 1700–1705 (2017).
11. Saver, J. L. et al. Prehospital use of magnesium sulfate as neuroprotection in acute stroke. N. Engl. J. Med. 372, 528–536 (2015).
12. Kim, H. Y., Singhal, A. B. & Lo, E. H. Normobaric hyperoxia extends the reperfusion window in focal cerebral ischemia. Ann. Neurol. 57, 571–575 (2005).
13. Albers, G. W. et al. Thrombectomy for stroke at 6 to 16 hours with selection by perfusion imaging. N. Engl. J. Med. 378, 708–718 (2018).
14. Nogueira, R. G. et al. Thrombectomy 6 to 24 hours after stroke with a mismatch between deficit and infarct. N. Engl. J. Med. 378, 11–21 (2018).
15. Albers, G. W. Late window paradox. Stroke 49, 768–771 (2018).
16. Baskerville, T. A. et al. Influence of 100% and 40% oxygen on penumbral blood flow, oxygen level, and T2*-weighted MRI in a rat stroke model. J. Cereb. Blood Flow Metab. 31, 1799–1806 (2011).
17. Crockard, H. A., Symon, L., Branston, N. M. & Juhasz, J. Changes in regional cortical tissue oxygen tension and cerebral blood flow during temporary middle cerebral artery occlusion in baboons. J. Neurol. Sci. 27, 29–44 (1976).
18. Harris, R. J., Richards, P. G., Symon, L., Habib, A. H. & Rosenstein, J. pH, K+, and PO2 of the extracellular space during ischaemia of primate cerebral cortex. J. Cereb. Blood Flow Metab. 7, 599–604 (1987).
19. Hoffman, W. E., Charbel, F. T. & Edelman, G. Brain tissue oxygen, carbon dioxide, and pH in neurosurgical patients at risk for ischemia. Anesth. Analg. 82, 582–586 (1996).
20. Hoffman, W. E., Charbel, F. T., Gonzalez- Portillo, G. & Ausman, J. I. Measurement of ischemia by changes in tissue oxygen, carbon dioxide, and pH. Surg. Neurol. 51, 654–658 (1999).
21. Hou, H. et al. The effect of oxygen therapy on brain damage and cerebral pO2 in transient focal cerebral ischemia in the rat. Physiol. Meas. 28, 963–976 (2007).
22. Liu, S. et al. Interstitial pO2 in ischemic penumbra and core are differentially affected following transient focal cerebral ischemia in rats. J. Cereb. Blood Flow Metab. 24, 343–349 (2004).
23. Shin, H. K. et al. Normobaric hyperoxia improves cerebral blood flow and oxygenation, and inhibits peri- infarct depolarizations in experimental focal ischaemia. Brain 130, 1631–1642 (2007).
24. Boisserand, L. S. et al. Multiparametric magnetic resonance imaging including oxygenation mapping of experimental ischaemic stroke. J. Cereb. Blood Flow Metab. 37, 2196–2207 (2017).
25. Boulouis, G. et al. Clinical imaging factors associated with infarct progression in patients with ischemic stroke during transfer for mechanical thrombectomy. JAMA Neurol. 74, 1361–1367 (2017).
26. Saver, J. L. Time is brain — quantified. Stroke 37, 263–266 (2006).
27. Moskowitz, M. A., Lo, E. H. & Iadecola, C. The science of stroke: mechanisms in search of treatments. Neuron 67, 181–198 (2010).
28. Veltkamp, R. et al. Hyperbaric oxygen induces rapid protection against focal cerebral ischemia. Brain Res. 1037, 134–138 (2005).
29. Veltkamp, R. et al. Oxygen therapy in permanent brain ischemia: potential and limitations. Brain Res. 1107, 185–191 (2006).
30. Bennett, M. H. et al. Hyperbaric oxygen therapy for acute ischaemic stroke. Cochrane Database Syst. Rev. 11, CD004954 (2014).
31. Lou, M., Eschenfelder, C. C., Herdegen, T., Brecht, S. & Deuschl, G. Therapeutic window for use of hyperbaric oxygenation in focal transient ischemia in rats. Stroke 35, 578–583 (2004).
32. Poli, S. & Veltkamp, R. Oxygen therapy in acute ischemic stroke — experimental efficacy and molecular mechanisms. Curr. Mol. Med. 9, 227–241 (2009).
33. Singhal, A. B. Oxygen therapy in stroke: past, present, and future. Int. J. Stroke 1, 191–200 (2006).
34. Singhal, A. B. A review of oxygen therapy in ischemic stroke. Neurol. Res. 29, 173–183 (2007).
35. Ejaz, S. et al. Normobaric hyperoxia markedly reduces brain damage and sensorimotor deficits following brief focal ischaemia. Brain 139, 751–764 (2016).
36. Singhal, A. B. et al. A pilot study of normobaric oxygen therapy in acute ischemic stroke. Stroke 36, 797–802 (2005).
37. Liu, S. et al. Electron paramagnetic resonance- guided normobaric hyperoxia treatment protects the brain by maintaining penumbral oxygenation in a rat model of transient focal cerebral ischemia. J. Cereb. Blood Flow Metab. 26, 1274–1284 (2006).
38. Fryer, T. D. et al. Effects of hyperoxia on 18F- fluoro-misonidazole brain uptake and tissue oxygen tension following middle cerebral artery occlusion in rodents: pilot studies. PLoS 12, e0187087 (2017).
39. Beynon, C., Sun, L., Marti, H. H., Heiland, S. & Veltkamp, R. Delayed hyperbaric oxygenation is more effective than early prolonged normobaric hyperoxia in experimental focal cerebral ischemia. Neurosci. Lett. 425, 141–145 (2007).
40. Fujiwara, N. et al. Effect of normobaric oxygen therapy in a rat model of intracerebral hemorrhage. Stroke 42, 1469–1472 (2011).
41. Henninger, N., Bouley, J., Nelligan, J. M., Sicard, K. M. & Fisher, M. Normobaric hyperoxia delays perfusion/diffusion mismatch evolution, reduces infarct volume, and differentially affects neuronal cell death pathways after suture middle cerebral artery occlusion in rats. J. Cereb. Blood Flow Metab. 27, 1632–1642 (2007).
42. Henninger, N., Bratane, B. T., Bastan, B., Bouley, J. & Fisher, M. Normobaric hyperoxia and delayed tPA treatment in a rat embolic stroke model. J. Cereb. Blood Flow Metab. 29, 119–129 (2009).
43. Liang, J. et al. Normobaric hyperoxia slows blood–brain barrier damage and expands the therapeutic time window for tissue- type plasminogen activator treatment in cerebral ischemia. Stroke 46, 1344–1351 (2015).
44. Singhal, A. B., Dijkhuizen, R. M., Rosen, B. R. & Lo, E. H. Normobaric hyperoxia reduces MRI diffusion abnormalities and infarct size in experimental stroke. Neurology 58, 945–952 (2002).
45. Singhal, A. B., Wang, X., Sumii, T., Mori, T. & Lo, E. H. Effects of normobaric hyperoxia in a rat model of focal cerebral ischemia–reperfusion. J. Cereb. Blood Flow Metab. 22, 861–868 (2002).
‘Drip- and-ship’ paradigman acute stroke referral pathway in which a thrombolytic agent such as tissue plasminogen activator is administered in a community stroke unit and the patient is immediately transferred to the nearest comprehensive stroke centre for mechanical thrombectomy.
© 2018 Macmillan Publishers Limited, part of Springer Nature. All rights reserved.
NATuRe RevIeWS | NEuROlOgy
R e v i e w s
volume 14 | JuNe 2018 | 335

46. Esposito, E., Mandeville, E. T., Hayakawa, K., Singhal, A. B. & Lo, E. H. Effects of normobaric oxygen on the progression of focal cerebral ischemia in rats. Exp. Neurol. 249, 33–38 (2013).
47. Jin, X. et al. Normobaric hyperoxia combined with minocycline provides greater neuroprotection than either alone in transient focal cerebral ischemia. Exp. Neurol. 240, 9–16 (2013).
48. Liu, C., Weaver, J. & Liu, K. J. Rapid conditioning with oxygen oscillation: neuroprotection by intermittent normobaric hyperoxia after transient focal cerebral ischemia in rats. Stroke 43, 220–226 (2012).
49. Miyamoto, O. & Auer, R. N. Hypoxia, hyperoxia, ischemia, and brain necrosis. Neurology 54, 362–371 (2000).
50. Flynn, E. P. & Auer, R. N. Eubaric hyperoxemia and experimental cerebral infarction. Ann. Neurol. 52, 566–572 (2002).
51. Shin, H. K. et al. Endothelial dysfunction abrogates the efficacy of normobaric hyperoxia in stroke. J. Neurosci. 34, 15200–15207 (2014).
52. Tiwari, Y. V. et al. Effects of stroke severity and treatment duration in normobaric hyperoxia treatment of ischemic stroke. Brain Res. 1635, 121–129 (2016).
53. Geng, X. et al. Ethanol and normobaric oxygen: novel approach in modulating pyruvate dehydrogenase complex after severe transient and permanent ischemic stroke. Stroke 46, 492–499 (2015).
54. Kilkenny, C. et al. Animal research: reporting in vivo experiments — the ARRIVE guidelines. J. Cereb. Blood Flow Metab. 31, 991–993 (2011).
55. Baron, J. C., Macrae, I. M., Adams, H. P. Jr & Dirnagl, U. ESC- BRAIN: experimental and clinical stroke research — do they connect? Meeting report of the ESC- BRAIN joint symposium held in London and Shanghai in May 2013. Cerebrovasc. Dis. 36, 306–321 (2013).
56. Fujiwara, N. et al. Combination therapy with normobaric oxygen (NBO) plus thrombolysis in experimental ischemic stroke. BMC Neurosci. 10, 79 (2009).
57. Sun, L., Strelow, H., Mies, G. & Veltkamp, R. Oxygen therapy improves energy metabolism in focal cerebral ischemia. Brain Res. 1415, 103–108 (2011).
58. Mies, G., Iijima, T. & Hossmann, K. A. Correlation between peri- infarct DC shifts and ischaemic neuronal damage in rat. Neuroreport 4, 709–711 (1993).
59. Weaver, J. & Liu, K. J. Does normobaric hyperoxia increase oxidative stress in acute ischemic stroke? A critical review of the literature. Med. Gas Res. 5, 11 (2015).
60. Bai, J. & Lyden, P. D. Revisiting cerebral postischemic reperfusion injury: new insights in understanding reperfusion failure, hemorrhage, and edema. Int. J. Stroke 10, 143–152 (2015).
61. Geng, X. et al. Synergetic neuroprotection of normobaric oxygenation and ethanol in ischemic stroke through improved oxidative mechanism. Stroke 44, 1418–1425 (2013).
62. Eschenfelder, C. C. et al. Neuroprotection by oxygen in acute transient focal cerebral ischemia is dose dependent and shows superiority of hyperbaric oxygenation. Cerebrovasc. Dis. 25, 193–201 (2008).
63. Haelewyn, B. et al. Moderately delayed post- insult treatment with normobaric hyperoxia reduces excitotoxin- induced neuronal degeneration but increases ischemia- induced brain damage. Med. Gas Res. 1, 2 (2011).
64. Sun, L. et al. Oxygen therapy reduces secondary hemorrhage after thrombolysis in thromboembolic cerebral ischemia. J. Cereb. Blood Flow Metab. 30, 1651–1660 (2010).
65. David, H. N. et al. Prothrombolytic action of normobaric oxygen given alone or in combination with recombinant tissue- plasminogen activator in a rat model of thromboembolic stroke. J. Appl. Physiol. 112, 2068–2076 (2012).
66. Zhou, W., Marinescu, M. & Veltkamp, R. Only very early oxygen therapy attenuates posthemorrhagic edema formation and blood–brain barrier disruption in murine intracerebral hemorrhage. Neurocrit. Care 22, 121–132 (2015).
67. Ali, K. et al. The stroke oxygen pilot study: a randomized controlled trial of the effects of routine oxygen supplementation early after acute stroke — effect on key outcomes at six months. PLoS ONE 8, e59274 (2014).
68. Mazdeh, M., Taher, A., Torabian, S. & Seifirad, S. Effects of normobaric hyperoxia in severe acute stroke: a randomized controlled clinical trial study. Acta Med. Iran. 53, 676–680 (2015).
69. Ronning, O. M. & Guldvog, B. Should stroke victims routinely receive supplemental oxygen? A quasi- randomized controlled trial. Stroke 30, 2033–2037 (1999).
70. Rincon, F. et al. Association between hyperoxia and mortality after stroke: a multicenter cohort study. Crit. Care Med. 42, 387–396 (2014).
71. Roffe, C. et al. Effect of routine low- dose oxygen supplementation on death and disability in adults with acute stroke: the Stroke Oxygen Study randomized clinical trial. JAMA 318, 1125–1135 (2017).
72. Jauch, E. C. et al. Guidelines for the early management of patients with acute ischemic stroke: a guideline for healthcare professionals from the American Heart Association/American Stroke Association. Stroke 44, 870–947 (2013).
73. Padma, M. V. et al. Normobaric oxygen therapy in acute ischemic stroke: a pilot study in Indian patients. Ann. Indian Acad. Neurol. 13, 284–288 (2010).
74. Wu, O. et al. Evaluating effects of normobaric oxygen therapy in acute stroke with MRI- based predictive models. Med. Gas Res. 2, 5 (2012).
75. Singhal, A. B. et al. Magnetic resonance spectroscopy study of oxygen therapy in ischemic stroke. Stroke 38, 2851–2854 (2007).
76. US National Library of Medicine. ClinicalTrials.gov https://clinicaltrials.gov/ct2/show/NCT00414726 (2017).
77. Shi, S. et al. Normobaric hyperoxia reduces blood occludin fragments in rats and patients with acute ischemic stroke. Stroke 48, 2848–2854 (2017).
78. Poli, S. et al. Penumbral rescue by normobaric oxygen administration in patients with acute ischemic stroke and target mismatch profile (PROOF). Eur. Stroke. J. 2 (Suppl.), 335–336 (2017).
79. Fassbender, K. et al. Mobile stroke units for prehospital thrombolysis, triage, and beyond: benefits and challenges. Lancet Neurol. 16, 227–237 (2017).
80. Kunz, A. et al. Functional outcomes of pre- hospital thrombolysis in a mobile stroke treatment unit compared with conventional care: an observational registry study. Lancet Neurol. 15, 1035–1043 (2016).
81. Seiffge, D. J. et al. Improvement of oxygen supply by an artificial carrier in combination with normobaric oxygenation decreases the volume of tissue hypoxia and tissue damage from transient focal cerebral ischemia. Exp. Neurol. 237, 18–25 (2012).
82. Culp, W. C. et al. Dodecafluoropentane emulsion decreases infarct volume in a rabbit ischemic stroke model. J. Vasc. Interv. Radiol. 23, 116–121 (2012).
83. Woods, S. D. et al. Progress in dodecafluoropentane emulsion as a neuroprotective agent in a rabbit stroke model. Mol. Neurobiol. 48, 363–367 (2013).
84. Brown, A. T. et al. Dodecafluoropentane emulsion (DDFPe) decreases stroke size and improves neurological scores in a permanent occlusion rat stroke model. Open Neurol. J. 8, 27–33 (2014).
85. Schneider, U. C., Karutz, T., Schilling, L. & Woitzik, J. Administration of a second generation perfluorochemical in combination with hyperbaric oxygenation does not provide additional benefit in a model of permanent middle cerebral artery occlusion in rats. Springerplus 3, 32 (2014).
86. Woitzik, J., Weinzierl, N. & Schilling, L. Early administration of a second- generation perfluorochemical decreases ischemic brain damage in a model of permanent middle cerebral artery occlusion in the rat. Neurol. Res. 27, 509–515 (2005).
87. Fitzgerald, R. T. et al. Dodecafluoropentane emulsion delays and reduces MRI markers of infarction in a rat stroke model: a preliminary report. Magn. Reson. Imag. 33, 236–239 (2015).
88. Deuchar, G. A., Brennan, D., Griffiths, H., Macrae, I. M. & Santosh, C. Perfluorocarbons enhance a T2*-based MRI technique for identifying the penumbra in a rat model of acute ischemic stroke. J. Cereb. Blood Flow Metab. 33, 1422–1428 (2013).
89. Woitzik, J. & Schilling, L. A new method for superselective middle cerebral artery infusion in the rat. J. Neurosurg. 106, 872–878 (2007).
90. Cipolla, M. J., Linfante, I., Abuchowski, A., Jubin, R. & Chan, S. L. Pharmacologically increasing collateral perfusion during acute stroke using a carboxyhemoglobin gas transfer agent (SanguinateTM) in spontaneously hypertensive rats. J. Cereb. Blood Flow Metab. https://doi.org/10.1177/0271678X17705567 (2017).
91. Zhang, J. et al. Transfusion of hemoglobin- based oxygen carriers in the carboxy state is beneficial during transient focal cerebral ischemia. J. Appl. Physiol. 113, 1709–1717 (2012).
92. Shuaib, A., Butcher, K., Mohammad, A. A., Saqqur, M. & Liebeskind, D. S. Collateral blood vessels in acute ischaemic stroke: a potential therapeutic target. Lancet Neurol. 10, 909–921 (2011).
93. Winship, I. R. Cerebral collaterals and collateral therapeutics for acute ischemic stroke. Microcirculation 22, 228–236 (2015).
94. Rocha, M. & Jovin, T. G. Fast versus slow progressors of infarct growth in large vessel occlusion stroke: clinical and research implications. Stroke 48, 2621–2627 (2017).
95. Ali, L. K. et al. Heads Up! A novel provocative maneuver to guide acute ischemic stroke management. Interv. Neurol. 6, 8–15 (2017).
96. Beretta, S. et al. Cerebral collateral therapeutics in acute ischemic stroke: a randomized preclinical trial of four modulation strategies. J. Cereb. Blood Flow Metab. 37, 3344–3354 (2017).
97. Shin, H. K. et al. Mild induced hypertension improves blood flow and oxygen metabolism in transient focal cerebral ischemia. Stroke 39, 1548–1555 (2008).
98. Regenhardt, R. W. et al. Blood pressure and penumbral sustenance in stroke from large vessel occlusion. Front. Neurol. 8, 317 (2017).
99. Noor, R. et al. Partial intra- aortic occlusion improves perfusion deficits and infarct size following focal cerebral ischemia. J. Neuroimag. 20, 272–276 (2010).
100. Winship, I. R. et al. Augmenting collateral blood flow during ischemic stroke via transient aortic occlusion. J. Cereb. Blood Flow Metab. 34, 61–71 (2014).
101. Ramakrishnan, G., Dong, B., Todd, K. G., Shuaib, A. & Winship, I. R. Transient aortic occlusion augments collateral blood flow and reduces mortality during severe ischemia due to proximal middle cerebral artery occlusion. Transl Stroke Res. 7, 149–155 (2016).
102. Guluma, K. Z. et al. Feasibility and safety of using external counterpulsation to augment cerebral blood flow in acute ischemic stroke — the Counterpulsation to Upgrade Forward Flow in Stroke (CUFFS) trial. J. Stroke Cerebrovasc. Dis. 24, 2596–2604 (2015).
103. Shuaib, A. et al. Partial aortic occlusion for cerebral perfusion augmentation: safety and efficacy of NeuroFlo in Acute Ischemic Stroke trial. Stroke 42, 1680–1690 (2011).
104. Hammer, M. D. et al. Safety and feasibility of NeuroFlo use in eight- to 24-hour ischemic stroke patients. Int. J. Stroke 7, 655–661 (2012).
105. Hess, D. C. et al. Remote ischaemic conditioning — a new paradigm of self- protection in the brain. Nat. Rev. Neurol. 11, 698–710 (2015).
106. Ma, J. et al. Prevention of the collapse of pial collaterals by remote ischemic perconditioning during acute ischemic stroke. J. Cereb. Blood Flow Metab. 37, 3001–3014 (2017).
107. Hahn, C. D., Manlhiot, C., Schmidt, M. R., Nielsen, T. T. & Redington, A. N. Remote ischemic per- conditioning: a novel therapy for acute stroke? Stroke 42, 2960–2962 (2011).
108. Ren, C. et al. Limb remote ischemic per- conditioning in combination with post- conditioning reduces brain damage and promotes neuroglobin expression in the rat brain after ischemic stroke. Restor. Neurol. Neurosci. 33, 369–379 (2015).
109. Hoda, M. N. et al. Remote ischemic perconditioning is effective alone and in combination with intravenous tissue- type plasminogen activator in murine model of embolic stroke. Stroke 43, 2794–2799 (2012).
110. Hoda, M. N. et al. A 2 × 2 factorial design for the combination therapy of minocycline and remote ischemic perconditioning: efficacy in a preclinical trial in murine thromboembolic stroke model. Exp. Transl Stroke Med. 6, 10 (2014).
111. Hougaard, K. D. et al. Remote ischemic perconditioning as an adjunct therapy to thrombolysis in patients with acute ischemic stroke: a randomized trial. Stroke 45, 159–167 (2014).
112. Pico, F. et al. A multicenter, randomized trial on neuroprotection with remote ischemic per- conditioning during acute ischemic stroke: the REmote iSchemic Conditioning in acUtE BRAin INfarction study protocol. Int. J. Stroke 11, 938–943 (2016).
113. Muoio, V., Persson, P. B. & Sendeski, M. M. The neurovascular unit — concept review. Acta Physiol. 210, 790–798 (2014).
114. Strong, A. J., Gibson, G., Miller, S. A. & Venables, G. S. Changes in vascular and metabolic reactivity as indices of ischaemia in the penumbra. J. Cereb. Blood Flow Metab. 8, 79–88 (1988).
© 2018 Macmillan Publishers Limited, part of Springer Nature. All rights reserved.
www.nature.com/nrneurol
R e v i e w s
336 | JuNe 2018 | volume 14

115. Burnett, M. G., Detre, J. A. & Greenberg, J. H. Activation- flow coupling during graded cerebral ischemia. Brain Res. 1047, 112–118 (2005).
116. Sutherland, B. A. et al. Multi- modal assessment of neurovascular coupling during cerebral ischaemia and reperfusion using remote middle cerebral artery occlusion. J. Cereb. Blood Flow Metab. 37, 2494–2508 (2017).
117. Burnett, M. G. et al. Electrical forepaw stimulation during reversible forebrain ischemia decreases infarct volume. Stroke 37, 1327–1331 (2006).
118. Davis, M. F., Lay, C. C., Chen- Bee, C. H. & Frostig, R. D. Amount but not pattern of protective sensory stimulation alters recovery after permanent middle cerebral artery occlusion. Stroke 42, 792–798 (2011).
119. Hancock, A. M., Lay, C. C., Davis, M. F. & Frostig, R. D. Sensory stimulation- based complete protection from ischemic stroke remains stable at 4 months post- occlusion of MCA. J. Neurol. Disord. 1, 135 (2013).
120. Lay, C. C., Davis, M. F., Chen- Bee, C. H. & Frostig, R. D. Mild sensory stimulation completely protects the adult rodent cortex from ischemic stroke. PLoS ONE 5, e11270 (2010).
121. Lay, C. C., Davis, M. F., Chen- Bee, C. H. & Frostig, R. D. Mild sensory stimulation reestablishes cortical function during the acute phase of ischemia. J. Neurosci. 31, 11495–11504 (2011).
122. Lay, C. C., Davis, M. F., Chen- Bee, C. H. & Frostig, R. D. Mild sensory stimulation protects the aged rodent from cortical ischemic stroke after permanent middle cerebral artery occlusion. J. Am. Heart Assoc. 1, e001255 (2012).
123. Lay, C. C. & Frostig, R. D. Complete protection from impending stroke following permanent middle cerebral artery occlusion in awake, behaving rats. Eur. J. Neurosci. 40, 3413–3421 (2014).
124. Lay, C. C., Jacobs, N., Hancock, A. M., Zhou, Y. & Frostig, R. D. Early stimulation treatment provides complete sensory- induced protection from ischemic stroke under isoflurane anesthesia. Eur. J. Neurosci. 38, 2445–2452 (2013).
125. Liao, L. D. et al. Rescue of cortical neurovascular functions during the hyperacute phase of ischemia by peripheral sensory stimulation. Neurobiol. Dis. 75, 53–63 (2015).
126. Luckl, J. et al. The biological effect of contralateral forepaw stimulation in rat focal cerebral ischemia: a multispectral optical imaging study. Front. Neuroenerg. 2, 19 (2010).
127. Bandla, A. et al. Peripheral sensory stimulation is neuroprotective in a rat photothrombotic ischemic stroke model. Conf. Proc. IEEE Eng. Med. Biol. Soc. 2016, 6086–6089 (2016).
128. Liao, L. D. et al. Improving neurovascular outcomes with bilateral forepaw stimulation in a rat photothrombotic ischemic stroke model. Neurophotonics 1, 011007 (2014).
129. Liu, Y., Liao, L., Chan, S., Bandla, A. & Thakor, N. V. An integrated neuroprotective intervention for brain ischemia validated by ECoG- fPAM. Conf. Proc. IEEE Eng. Med. Biol. Soc. 2016, 4009–4012 (2016).
130. O’Collins, V. E. et al. 1,026 experimental treatments in acute stroke. Ann. Neurol. 59, 467–477 (2006).
131. Yenari, M. A. & Hemmen, T. M. Therapeutic hypothermia for brain ischemia: where have we come and where do we go? Stroke 41 (Suppl.), S72–S74 (2010).
132. Chavez, J. C., Hurko, O., Barone, F. C. & Feuerstein, G. Z. Pharmacologic interventions for stroke: looking beyond the thrombolysis time window into the penumbra with biomarkers, not a stopwatch. Stroke 40, e558–e563 (2009).
133. Minnerup, J., Sutherland, B. A., Buchan, A. M. & Kleinschnitz, C. Neuroprotection for stroke: current status and future perspectives. Int. J. Mol. Sci. 13, 11753–11772 (2012).
134. von Bornstadt, D. et al. Supply- demand mismatch transients in susceptible peri- infarct hot zones explain the origins of spreading injury depolarizations. Neuron 85, 1117–1131 (2015).
135. Hancock, A. M. & Frostig, R. D. Testing the effects of sensory stimulation as a collateral- based therapeutic for ischemic stroke in C57BL/6 J and CD1 mouse strains. PLoS ONE 12, e0183909 (2017).
136. Faber, J. E., Chilian, W. M., Deindl, E., van Royen, N. & Simons, M. A brief etymology of the collateral circulation. Arterioscler. Thromb. Vasc. Biol. 34, 1854–1859 (2014).
137. Reid, E. et al. Penumbra detection using PWI/DWI mismatch MRI in a rat stroke model with and without
comorbidity: comparison of methods. J. Cereb. Blood Flow Metab. 32, 1765–1777 (2012).
138. Brint, S., Jacewicz, M., Kiessling, M., Tanabe, J. & Pulsinelli, W. Focal brain ischemia in the rat: methods for reproducible neocortical infarction using tandem occlusion of the distal middle cerebral and ipsilateral common carotid arteries. J. Cereb. Blood Flow Metab. 8, 474–485 (1988).
139. Chan, S. L., Sweet, J. G., Bishop, N. & Cipolla, M. J. Pial collateral reactivity during hypertension and aging: understanding the function of collaterals for stroke therapy. Stroke 47, 1618–1625 (2016).
140. McCabe, C. et al. Differences in the evolution of the ischemic penumbra in stroke- prone spontaneously hypertensive and Wistar- Kyoto rats. Stroke 40, 3864–3868 (2009).
141. Hennerici, M. G., Kern, R. & Szabo, K. Non- pharmacological strategies for the treatment of acute ischaemic stroke. Lancet Neurol. 12, 572–584 (2013).
142. Henninger, N. & Fisher, M. Stimulating circle of Willis nerve fibers preserves the diffusion- perfusion mismatch in experimental stroke. Stroke 38, 2779–2786 (2007).
143. Yarnitsky, D. et al. Sphenopalatine ganglion (SPG) stimulation in acute stroke model: a novel method for neuroprotection. Stroke 37, 728 (2006).
144. Levi, H. et al. Stimulation of the sphenopalatine ganglion induces reperfusion and blood- brain barrier protection in the photothrombotic stroke model. PLoS ONE 7, e39636 (2012).
145. US National Library of Medicine. ClinicalTrials.gov https://clinicaltrials.gov/ct2/show/NCT00826059 (2017).
146. Khurana, D., Kaul, S. & Bornstein, N. M. ImpACT-1 Study Group. Implant for augmentation of cerebral blood flow trial 1: a pilot study evaluating the safety and effectiveness of the Ischaemic Stroke System for treatment of acute ischaemic stroke. Int. J. Stroke 4, 480–485 (2009).
147. Lyden, P. D., Krieger, D., Yenari, M. & Dietrich, W. D. Therapeutic hypothermia for acute stroke. Int. J. Stroke. 1, 9–19 (2006).
148. Wu, T. C. & Grotta, J. C. Hypothermia for acute ischaemic stroke. Lancet Neurol. 12, 275–284 (2013).
149. Dumitrascu, O. M., Lamb, J. & Lyden, P. D. Still cooling after all these years: meta- analysis of pre- clinical trials of therapeutic hypothermia for acute ischemic stroke. J. Cereb. Blood Flow Metab. 36, 1157–1164 (2016).
150. van der Worp, H. B., Macleod, M. R., & Kollmar, R. European Stroke Research Network for Hypothermia (EuroHYP). Therapeutic hypothermia for acute ischemic stroke: ready to start large randomized trials? J. Cereb. Blood Flow Metab. 30, 1079–1093 (2010).
151. van der Worp, H. B., Sena, E. S., Donnan, G. A., Howells, D. W. & Macleod, M. R. Hypothermia in animal models of acute ischaemic stroke: a systematic review and meta- analysis. Brain 130, 3063–3074 (2007).
152. Krieger, D. W. & Yenari, M. A. Therapeutic hypothermia for acute ischemic stroke: what do laboratory studies teach us? Stroke 35, 1482–1489 (2004).
153. Lyden, M. P., Colbourne, P. F., Lyden, P. & Schwab, S. Preclinical and clinical studies targeting therapeutic hypothermia in cerebral ischemia and stroke. Ther. Hypothermia Temp. Manag. 3, 3–6 (2013).
154. Morikawa, E. et al. The significance of brain temperature in focal cerebral ischemia: histopathological consequences of middle cerebral artery occlusion in the rat. J. Cereb. Blood Flow Metab. 12, 380–389 (1992).
155. Ridenour, T. R., Warner, D. S., Todd, M. M. & McAllister, A. C. Mild hypothermia reduces infarct size resulting from temporary but not permanent focal ischemia in rats. Stroke 23, 733–738 (1992).
156. Kollmar, R. et al. Combination therapy of moderate hypothermia and thrombolysis in experimental thromboembolic stroke — an MRI study. Exp. Neurol. 190, 204–212 ( 20 04 ).
157. Tang, X. N., Liu, L. & Yenari, M. A. Combination therapy with hypothermia for treatment of cerebral ischemia. J. Neurotrauma 26, 325–331 (2009).
158. Geurts, M. et al. COOLIST (Cooling for Ischemic Stroke Trial): a multicenter, open, randomized, phase II, clinical trial. Stroke 48, 219–221 (2017).
159. Piironen, K. et al. Mild hypothermia after intravenous thrombolysis in patients with acute stroke: a randomized controlled trial. Stroke 45, 486–491 (2014).
160. Lyden, P. et al. Results of the ICTuS 2 Trial (Intravascular Cooling in the Treatment of Stroke 2). Stroke 47, 2888–2895 (2016).
161. van der Worp, H. B. et al. EuroHYP-1: European multicenter, randomized, phase III clinical trial of therapeutic hypothermia plus best medical treatment versus best medical treatment alone for acute ischemic stroke. Int. J. Stroke 9, 642–645 (2014).
162. Hong, J. M. et al. Therapeutic hypothermia after recanalization in patients with acute ischemic stroke. Stroke 45, 134–140 (2014).
163. Esposito, E., Ebner, M., Ziemann, U. & Poli, S. In cold blood: intraarteral cold infusions for selective brain cooling in stroke. J. Cereb. Blood Flow Metab. 34, 743–752 (2014).
164. Dalkara, T. & Arsava, E. M. Can restoring incomplete microcirculatory reperfusion improve stroke outcome after thrombolysis? J. Cereb. Blood Flow Metab. 32, 2091–2099 (2012).
165. Chen, J. et al. Endovascular hypothermia in acute ischemic stroke: pilot study of selective intra- arterial cold saline infusion. Stroke 47, 1933–1935 (2016).
166. Cambiaghi, M. et al. Brain transcranial direct current stimulation modulates motor excitability in mice. Eur. J. Neurosci. 31, 704–709 (2010).
167. Nitsche, M. A. & Paulus, W. Excitability changes induced in the human motor cortex by weak transcranial direct current stimulation. J. Physiol. 527, 633–639 (2000).
168. Peruzzotti- Jametti, L. et al. Safety and efficacy of transcranial direct current stimulation in acute experimental ischemic stroke. Stroke 44, 3166–3174 (2013).
169. Notturno, F. et al. Neuroprotective effect of cathodal transcranial direct current stimulation in a rat stroke model. J. Neurol. Sci. 342, 146–151 (2014).
170. Fisher, M. et al. Update of the stroke therapy academic industry roundtable preclinical recommendations. Stroke 40, 2244–2250 (2009).
171. Jovin, T. G. & Nogueira, R. G. DAWN in full daylight (DWI or CTP assessment with clinical mismatch in the triage of wake up and late presenting strokes undergoing neurointervention) [abstract]. Eur. Stroke J. 2 (Suppl.), LB33–001 (2017).
172. Albers, G. W. et al. A multicenter randomized controlled trial of endovascular therapy following imaging evaluation for ischemic stroke (DEFUSE 3). Int. J. Stroke 12, 896–905 (2017).
173. Broderick, J. P., Palesch, Y. Y. & Janis, L. S. & National Institutes of Health StrokeNet Investigators. The National Institutes of Health StrokeNet: a user’s guide. Stroke 47, 301–303 (2016).
174. Audebert, H. et al. The PRE- hospital Stroke Treatment Organization. Int. J. Stroke 12, 932–940 (2017).
175. Agarwal, S., Warburton, E. A. & Baron, J.-C. From Time is brain to Physiology is brain: a case for reflection in acute stroke treatment decisions. Brain 138, 1768–1770 (2015).
AcknowledgementsThe author thanks M. Bruyère for typing the supplementary tables.
Competing interestsThe author declares no competing interests.
Publisher’s noteSpringer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Review criteriaA PubMed search of original and review articles was per-formed using the following search terms: “normobaric hyperoxia and stroke” or “hyperoxia and stroke”; “hypother-mia and stroke”; “sensory stimulation and stroke”; “tran-scranial direct cortical stimulation and stroke” or “tDCS and stroke”; “per- conditioning and stroke”; “perfluorocarbons and stroke”; “aortic balloon occlusion and stroke” or “aortic occlusion and stroke”; and “spheno- palatine ganglion stim-ulation and stroke”. The articles that were selected for this Review used middle cerebral artery occlusion as a stroke model, were published in the English- language peer- reviewed literature and were published between 1975 and 2017.
Supplementary informationSupplementary information is available for this paper at https://doi.org/10.1038/s41582-018-0002-2.
© 2018 Macmillan Publishers Limited, part of Springer Nature. All rights reserved.
NATuRe RevIeWS | NEuROlOgy
R e v i e w s
volume 14 | JuNe 2018 | 337





![Realistic Soft Shadows by Penumbra-Wedges Blending · Penumbra-wedges X + Specular & diffuse Visibility buffer Modulated spec+diff Ambient Final image. Penumbra-wedges [3/4] Penumbra-wedges](https://img.pdfslide.us/doc/110x75/5f543a4c0135c76e2b226697/realistic-soft-shadows-by-penumbra-wedges-penumbra-wedges-x-specular-diffuse.jpg)