Embed Size (px)
Citation preview

1
PROSTATE CANCER: PROSTATE CANCER: The Diagnostic DilemmaThe Diagnostic Dilemma
Christopher R. Porter, MDCo-Director Urologic OncologyVirginia Mason Medical Center
Seattle, WA
The Dilemma
Common diseaseSensitive, non-specific screening testAlmost everyone gets a biopsyTumor is invisible
It’s a shot in the dark…
and hopefully not a miss!
In an Ideal World
Who to shoot and where to shoot them
We would know…
Who needs a biopsy
and where to aim
OR

2
A Big Deal
Why is prostate cancer so important?
Because a lot of people have it…
Worldwide Incidence
*Incidence per 100,000 population. Parkin DM, et al. CA Cancer J Clin. 1999;49:53.
39.5539.55
16.7516.75
8.518.51
49.7049.70
1.081.08
5.135.13
31.0331.03
92.3992.39
Eastern Eastern EuropeEurope
JapanJapan
AustraliaAustraliaNew ZealandNew Zealand
ChinaChina
Northern Northern AfricaAfrica
Southern Southern AfricaAfrica
North North AmericaAmerica
WesternWesternEurope Europe
Incidence in US
230,000 new cases in 2004*28,900 deaths in 2003#1 cancer and #2 killer in men4.5% decline per year since 1994
*Jemal A, Tiwari RC, et al CA Cancer J Clin 2004;54:8-29.
Screening Tools
Oesterling J, et al. Cancer: Principles & Practice of Oncology. 5th ed. 1997;1322-1386.
MethodMethodSensitivitySensitivity
(%)(%)SpecificitySpecificity
(%)(%)
PositivePositivePredictivePredictiveValue (%)Value (%)
DRE 69-89 84-98 26-35
PSA* 57-79 59-68 40-49
TRUS 36-85 41-79 27-36
*Using a 4-ng/mL cutoff.
Prostate Specific Antigen (PSA)
<4 ng/mL considered “normal”4-10 ng/mL 22% positive biopsy rate>10 ng/mL 66% positive biopsy rateMay be elevated by any prostate disease or manipulation
Oesterling J, et al. Cancer: Principles & Practice of Oncology. 5th ed. 1997;1322-1386. Kassabian VS, et al. The American Cancer Society Textbook of Clinical Oncology. 2nd ed. 1995;311-329.
Brawer MK. CA Cancer J Clin. 1999;49:264-281.

3
ROC Curve for PSA
Bellorofonte C, et al: European Urology 2005;47:29-27.
The problem is that PSA is sensitive but not specific
PSA 4 -10 ng/dlPositive biopsy: 24%
CaP Prevention Trial: Results
FINASTERIDE24.8% decrease in CaP
“Higher grade” CaP (6.4% vs 5.1%)
Sexual side effects slightly more common
(BUT high in placebo too! (50%))
24.4% with PSA <3 had positive biopsy
Surprisingly…
One in four men with PSA <3 have CaP
The prostate cancer prevention trial: current status.Higgens et al J Urol 2004;171(Part 2):1517.
Consider the Cost…

4
Consider the Cost
8% have PSA >4¼ will be positive US: 38 million men age 45-748% of 38 million = 3.04 million¼ of 3.04 million = 760,000 prostate cancer2.28 million unnecessary biopsies
Grizzle WE et al, J U Onc. 2004; 22: 337-43
It gets worse…
Consider the Cost
The Prostate Cancer Prevention Trial (PCPT)Placebo Arm
After 7 years those with PSA <4 (-DRE)15% positive end of study biopsy
and Re-consider the Cost
If we screen EVERYONE:38 million only 8% (3 million) screened35 million remain15% of these will be positive (5.24 million)Total number with cancer 6 million
32 million unnecessary biopsies!!
What can we do to PSA to improve accuracy of cancer
detection?

5
Improving PSA
Lower the cut-off pointUse Free/Total PSA ratioUse complex PSAUse precursor forms of PSA
Free-to-Total PSA*
PSAPSA Probability of CancerProbability of Cancer
2 ng/mL 1%
2-4 ng/mL 15%
4-10 ng/mL 25%
>10 ng/mL >50%
Brawer MK. Prostate-specific antigen: Current status. CA Cancer J Clin. 1999;49(5):264-281.
% FPSA% FPSA Probability of CancerProbability of Cancer
0-10% 56%
10-15% 28%
15-20% 20%
20-25% 16%
>25% 8%*Men with non-suspicious DRE results, regardless of patient age.
Free PSA ROC Curve
Bellorofonte C, et al European Urology 2005;47:29-27.
Even with the most advanced use of molecular forms, one still cannot predict who will have a positive biopsy.
Using PSA Forms to Improve Accuracy
Free PSA at least 3 precursor forms:• A full length & two truncated• Precursors can be expressed as % of free PSA
(%pPSA)• Accuracy of %pPSA vs % free PSA is 64% vs 53%
Improving PSA
PSA densityPSA velocity Free PSAPSA precursor forms etc
The fact of the matter is…
They are really not much better.

6
The Problem
INDIVIDUAL CLINICAL
PARAMETERS ARE UNRELIABLE
Gestalt
MENTAL PREDICTION
Personal experience
Personal knowledge
Prior outcomes
Mental prediction/human decision-making subject to inherent biases
Hogarth, R: Judgment & Choice, The Psychology of Decision. 2nd Ed. New York. John Wiley & Sons
Predictive Models
Not subject to same inherent biasesMaximize predictive accuracyOutperform human experts
Miehl P, Causes & Effects of my Disturbing Little Book. J Pers. Asses. 50: 370, 1986Larkin, M, Cancer Prognostic tools..Oncol Times, April,2002, p58
Predicting the Outcome of Prostate Biopsy in a Racially Diverse
Population: A Prospective Study
American Society of Clinical Oncology Orlando, Florida, 2001
Porter CR, et al.
Contributors
Colin O’DonnellE David CrawfordEduard GamitoChristopher PorterAshutosh Tewari
DOD Grant: ANN’S in CaP Project
Methods
Prospective study (1999-2001)
IRB approval
319 men: Indication for TRUS Biopsy
Single attending surgeon
Clinical & Ultrasonic Exams
DRE & TRUS: Level of Suspicion, 1-5

7
Methods
AgeRaceFamily HistoryAUASSBiopsy HistoryPotency
PSAFree PSAPSA DensityProstate VolumeDRE (LOS)TRUS (LOS)TRUS: Calcium
PARAMETERS:
Methods
STATISTICSUnivariate Analysis
PREDICTIVE MODELLINGLogistic Regression Analysis (LR)Artificial Neural Networks (ANN)
Methods
Pre-biopsy parametersSelection: Stepwise LRInputs: PSA/VOL/DRE/TRUS/BX HXModel training
Five Logistic Regression models *Five ANN models ^
* 1.2.1 R Development Program^ Brainmaker version 3.72 Calif. Sci 1988
ANN Model Training
Data set divided: Training & Validation Set
Cases with known output are presented
Training algorithm adjusts the weights
Weights based on error actual vs. expected
Training set data presentation continues
Weights adjusted to minimize error
ANN Model validated on “virgin data”
YDRE + BX
Neural Networks
PSA
TRUS
XInput Layer Hidden 1 OutputHidden 2
Receiver Operator Characteristics (ROC) Curve
Measure of PredictabilityROC: performance compares predictive capability with actual outcome.Sensitivity vs 1-SpecificityArea under ROC (AUROC)
Value of 1.0 = Perfect resultValue of 0.5 = Toss of a coin

8
Predictive Models
0.040.77Artificial Neural Network
0.040.76Logistic Regression
SDAUROC (MEAN)MODEL
Predictive Models
Logistic Regression (LR) Artificial Neural Networks (ANN)
Equivalent good performanceRobust modelsAUROC= 0.76
Porter CR et al, Urology, 60, 5, 831-4, 2002
Predictive Models
Both LR and ANN(+) bx vs (–) bx randomly selected76% of men with (+) bx would have a higher predicted probability of (+) bx
Porter CR et al, Urology, 60, 5, 831-4, 2002
Benefits of Neural Nets
No arbitrary method of variable reductionNo decrease in degree of freedomComplex variable interactions capturedAmerican Joint Committee on Cancer : Endorsed Neural Nets for PCA
– Bostwick D, Semin. Urol Onc. 17,4,1999
Predictive Models:An International Prospective Multicenter Model Involving
4,788 Men
Virginia Mason, WashingtonStanford University, CaliforniaUniversity of Innsbruck, Austria
Presented at ASCO, 2004
Methods
Tyrol, Austria (n=3814)Virginia Mason (n=491)Stanford (n=483)

9
Tyrol
Screening StudyElevated PSA: Age-specificRepeat PSADRETRUS TRUS Biopsy (Sextant)
Reissigl A, et al, Cancer 80: 1818-29, 1997
VMMC & Stanford University
Referral populationElevated PSA Abnormal DRETRUS Biopsy (10 core)
Methods
Input variablesAgePSAGland volumePSADDRETRUS
Methods
Tyrol modelData split randomly into three 1200 setsThree ANN modelsThree logistic regression models Cross-way internal validation The median ANN model selectedThe median LR model selected
Methods
Extramural validationMedian ANN & LR models selectedValidated individually against VMMC and SU data sets

10
0.3-1,300Yes0.75/0.75
Age, PSA, volume, DRE, TRUS, prior biopsy
ANN/LR4,788Porter CR
0-389Yes0.77/0.76Age, PSA, volume, DRE, TRUS, race, prior biopsy
ANN/LR319Porter CR
4-10Yes0.91/0.90PSA, PSAD, free PSA, PSA TX, DREANN/LR974Djavan B
2.5-4Yes0.87/0.85PSA, PSAD, free PSA, PSA TZ, DREANN/LR272Djavan B
0-4Yes0.75Age, race, PSALR700Eastham JA
2.5-4Yes0.74Age, creatinine kinase PAP, PSA, free PSA
ANN151Babian RJ
>4YesN/AAge, PSA, DRE, TRUSANN1.787Snow PB
PSArangeValidatedAccuracy
ROCInput variablesModelnAuthor
Critique
Study populationsScreening (Model)Referral (Validation)
BiopsySextant vs 10-core
Predictive Models
Accuracy in predicting the outcome of the biopsy75% overall
Porter CR et al., Proceedings of ASCO, 2004
Now we know
Who…
But WHERE??!!
A Patient’s Question
“So, let me get this straight…patients with PSA 2-10 have about a 25%
chance of positive biopsy…
…That means 75% have a chance of negative biopsy.”
A Difficult Sell
“Well Sir, we can’t see the cancer,so we will take more biopsies –
say 10-12…
If we miss it this time we’ll need to do it again, because we miss about 1 in 3.”

11
Grey Scale Ultrasound
InaccurateFew targets30-50% false negativeWeather map
Spectral Analysis for Detecting and Evaluating
Prostate CancerErnest J. Feleppa, Andrew Kalisz, SK Alam, Stella Urban
Riverside Research Institute, New York, NYChristopher R. Porter
Virginia Mason Medical Center, Seattle, WAJohn Gillespie
National Institutes of Health, Bethesda, MDPeter Scardino, Makato Ohori
Memorial Sloan-Kettering Cancer Center, New York, NYsupported by:NIH grant CA53561
Prostate Studies: Rationale
MotivationsInability to image prostate cancerInability to target treatment
ObjectivesTo characterize cancerous vs. noncancerous tissuesTo image cancerous regions of the prostate
Prostate Studies: Rationale
To more effectively:Guide biopsies Treat cancerous tissues Spare non-cancerous tissuesMonitor treatment

12
SCANNER
COMPUTERSYSTEM
probeand
biopsyneedle
RFechoes
timing andcontrolsignals
SYSTEM FOR ACQUIRING U/S DATA:-- RF echo-signal data (3-D and Bx)-- instrument settings (gain, etc.)-- B-mode-interpretation LOS values
GOLD STANDARD:-- histology biopsy
Spectral Analysis: The Basics
Returning sound wave capturedInstead of using volume (Grey scale/B mode)Entire radio frequency signal analyzedSlope, y intercept and mid band RF values Machine Learning Mathematical Model (ANN)ANN weights the RF values (Look-up table)New RF values analyzed and the probability of the region of interest harboring CAP is calculated
Processing GUIROI and Spectrum
(basis for characterizing tissue)
Power Spectrum: Tissue Properties
Slope = f (size, attenuation)Intercept = f (size, concentration, relative impedance)Midband = f (size, concentration, relative impedance)
General Approach: 3 Steps
1. Build data base
2. Classify tissue types
3. Generate tissue-type images

13
General Approach 1: Data Base
Compute spectral
parameter values of RF
data in known location (e.g., biopsy site)
Obtain “truth”data from
histology (e.g., pathology report)
Obtain “general”data for case (e.g., age, race, or PSA)
DATA BASE
Obtain “baseline”data (e.g., LOS) to
assess efficacy
Clinical Data-acquisition System
0
0.2
0.4
0.6
0.8
1
0 0.2 0.4 0.6 0.8 1
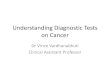
best neural net curve: area = 0.848 ± 0.047
average neural net curve: area = 0.804 ± 0.052
B-mode-based curve: area = 0.662 ± 0.034
TPF
FPF
Early ROC Curves for 1005 Biopsies ROC Curves
0.7213
0.4580
0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
1
0 0.1 0.2 0.3 0.4 0.5 0.6 0.7 0.8 0.9 1
FPF (1 - specificity)
TPF
(sen
sitiv
ity)
RBF = 0.810 +/- 0.02595% confidence = 0.757 to 0.855
LOS Area = 0.647 +/- 0.02995% confidence = 0.589 to 0.702
Accuracy of Spectral Analysis in Identifying CaP
0.66 +/- 0.030.80 +/- 0.05MSKCC
0.66=/- 0.03O.81 +/-0.05MSKCC
0.67 +/- 0.040.78 +/- 0.05SUNY
AccuracyGrey scale
AccuracySpect. Anal
Site
3-D Multi-Modality Studies
U/S + MRS (+ MRI ) in 3-DIndependent information, e.g., MRS choline/citrate ratio
Radical-prostatectomy patientsData acquired in vivo and in vitro
Correlate with histology in 3-DRegion-by-region (volumetric)
Develop more-powerful classifiersLinear (?)Nearest neighbor (?)Neural network (?)

14
3-D Spectral Analysis
Men prior to prostatectomy undergo TRUS using Spectral Analysis
0.2 cm Spectral Analysis cuts are obtained
RRP specimen pathology compared to pre-op Spectral Analysis scans
Anterior Tumor:2-D Images and Histology
(apical view)
Targeting: Anterior Tumor
ppm 2.0 3.5 3.0 2.5
CholineCreatine
Citrate
Cancer2.0
1.5ppm3.5 3.0 2.5
Choline
CreatineCitrate
Healthy
Prostate Cancer
Decreased Citrateloss of cellular function
loss of ductal morphology
Increased Choline + Creatineincreased proliferationmembrane changes
increased cell density
Role of MRS
John Kurhanewicz, Ph.D.MSRC, UCSF
OrlaidCholine Image +
Citrate Image
OverlaidCholine/Citrate
image
Cancer
NormalOverlaidCitrateCholineImages
MRS Displays
In 47 patients who had sextant biopsies and combined MRI/MRSI prior to radical prostatectomy and step-section histopathology, we demonstrated significantly (p< 0.05) improved* localization to a sextant of the prostate (i.e. left/right base, midgland and apex) when combining the information.
Tumor Localization using MRI/MRSI and Sextant Biopsy
Sensitivity SpecificityBiopsy Alone 50% 81%MRI (+) + MRSI (+, > 2 s.d.) 56% 82%MRI (+) or MRSI (+, > 2 s.d.) 88% 40%MRI (+) + MRSI (+, > 3 s.d.) 41% 91%MRI (+) or MRSI (+, > 3 s.d.) 78% 52%MRI (+) + MRSI (+) + Biopsy (+) 34% 98%*MRI (+) or MRSI (+) or Biopsy (+) 94%* 38%

15
ROC Curves: MRS vs. MRI
sens
itivi
ty
1-specificity0.2 0.4 0.6 0.8 1.0
0.2
0.4
0.6
0.8
1.0
Radiology 1999;213:481-488
MRI+MRSI, Az=0.83
MRI, Az=0.77
Conclusion
Tissue-type images (TTIs) show promisebiopsy guidance and planning (real time)therapy targeting (escalation and sparing, w/ MRS)monitoring therapy (potentially, w/ MRS)
Conclusion
Payoff for biopsy is largefewer missed cancersfewer unnecessary biopsies
Payoff for therapy targeting is largereduced deleterious effects on non-cancersenhanced desired effects on cancers
We’ll know who to shoot and when to shoot’em



![ProstateMRI,withorwithoutMRI-targetedbiopsy,and ...doccdn.simplesite.com/d/a7/85/281756459332109735/8... · [Diagnostic Test Accuracy Review] Prostate MRI, with or without MRI-targeted](https://img.pdfslide.us/doc/110x75/5e67d4d211dfb66b806b9099/prostatemriwithorwithoutmri-targetedbiopsyand-diagnostic-test-accuracy-review.jpg)