Embed Size (px)
Citation preview

Ava i l ab l e on l i ne a t www.sc i enced i r ec t . com
ScienceDirect
Journal of Crohn's and Colitis (2014) xx, xxx–xxx
CROHNS-00992; No of Pages 9
Prospective validation study of theInternational Classification of Functioning,Disability and Health score in Crohn's diseaseand ulcerative colitis
Rupert W.L. Leonga,c,⁎, Tony Huanga,c, Yanna Koa,c, Ari Jeona,Jeff Changa,c, Friedbert Kohlerb,c, Viraj Kariyawasamaa Gastroenterology and Liver Services, Concord Hospital, Hospital Rd, Sydney, New South Wales 2139, Australiab Department of Rehabilitation Medicine, Braeside Hospital, Sydney, Australiac Faculty of Medicine, The University of New South Wales, Sydney, Australia
Received 21 January 2014; received in revised form 23 February 2014; accepted 25 February 2014
Abbreviations: CD, Crohn's diseaseInflammatory Bowel Disease QuestionnUC, ulcerative colitis.⁎ Corresponding author at: Concord H
6767.E-mail address: rupertleong@outlo
http://dx.doi.org/10.1016/j.crohns.201873-9946/© 2014 European Crohn's an
Please cite this article as: Leong RWLHealth score in Crohn's disease and ul
KEYWORDSDisability;Inflammatory bowel disease;Crohn's;Colitis;Work;Employment
Abstract
Background and aims: Inflammatory bowel diseases (IBD) may result in disability. We aim tovalidate a novel scoring system for the IBD disability index (IBD-DI), and identify predictors ofdisability and its correlation with work absenteeism.Methods: This prospective IBD ambulatory clinic cohort study measured IBD-DI, Crohn's DiseaseActivity Index (CDAI) for Crohn's disease (CD) or partial Mayo score (pMayo) for ulcerative colitis(UC), IBDQ quality-of-life, and Work Productivity and Activity Impairment. Negative IBD-DI
represented greater disability. Validation tests were performed and predictors and extent ofwork absenteeism were determined.Results: 166 consecutive subjects were recruited (75 CD, 41 UC, 50 controls). IBD-DI correlatedwith CDAI (r = −0.77, P b 0.001), pMayo (r = −0.82, P b 0.001) and IBDQ (r = 0.86, P b 0.001).IBD-DI differentiated CD, and UC from controls (medians −7, −4, +10; P b 0.001) with a score ofN3.5 identifying controls with 94% sensitivity and 83% specificity (area-under-curve 0.92). Stablepatients had unchanged IBD-DI (P = ns) but not in those who relapsed (P b 0.001). Intraclasscorrelation was 0.89 and Cronbach's alpha of internal consistency was 0.94. Diagnosis age, sex,phenotype, perianal disease, prior surgery, steroid-use and disease duration did not influencethe IBD-DI but active use of biological agents significantly reduced disability (P = 0.03). 21.6% of; CDAI, Crohn's disease activity index; IBD-DI, Inflammatory bowel disease disability index; IBDQ,aire; ICF, International Classification of Functioning, Disability and Health; pMayo, partial Mayo score;
ospital, Gastroenterology and Liver Services, Sydney, Australia. Tel.: +61 2 9767 6111; fax: +61 2 9767
ok.com (R.W.L. Leong).
14.02.028d Colitis Organisation. Published by Elsevier B.V. All rights reserved.
, et al, Prospective validation study of the International Classification of Functioning, Disability andcerative colitis, J Crohns Colitis (2014), http://dx.doi.org/10.1016/j.crohns.2014.02.028

2 R.W.L. Leong et al.
Please cite this article as: Leong RWHealth score in Crohn's disease and ul
IBD patients had moderate-severe disability equating to missing N25% of work hours in theprevious week. Multivariate analysis identified that only IBD-DI to be predictive ofunemployment status (OR: 0.94; 95% CI: 0.89–0.99).Conclusions: The IBD-DI is a valid tool measuring disability in both CD and UC and correlates withworkforce participation. It is a potential useful tool in the assessment of participation restrictionand activity limitation. Trial registration: ACTRN12613000903785.© 2014 European Crohn's and Colitis Organisation. Published by Elsevier B.V. All rights reserved.
L, et al, Prospective validationcerative colitis, J Crohns Colitis
1. Introduction
Disability is defined by the World Health OrganizationInternational Classification of Impairments, Disabilities andHandicaps (ICIDH) as “any restriction or lack (resulting from anyimpairment) of ability to perform an activity in the manneror within the range considered normal for a human being”.1
Disability, therefore, more accurately reflects impairments,activity limitation and participation restrictionwhich correlateswith the lost work productivity and increased health resourcesutilization. Reversal of disability to minimize or eliminate suchlimitations and restrictions then becomes an important drivingforce of any intervention as a marker of successful treatment.This in turn allows the cost of newer treatments to be directlyincorporated into the regulatory approval process as a trade-offfor the reduction in disability. In contrast, “quality of life” is apatient-reportable outcome on their feeling of their limitationsand restrictions. Quality of life is heavily subjective based uponinter-individual coping strategies.2
Inflammatory bowel diseases (IBD) are chronic incurablegastrointestinal diseases that typically affect the youngworking-age population. Active disease, progressive coursewith cumulative intestinal damage, development of compli-cations, the presence of extra-intestinal manifestations andtreatment adverse effects may result in disability. Functionalassessment is an essential consideration in chronic illnesses; assuch theWorld Health Organization (WHO) is currently revisingthe International Classification of Diseases to include func-tional properties for disabling conditions.3 The WHO devel-oped the International Classification of Functioning, Disabilityand Health (ICF), a structured and complete frameworkthat classifies body functions, structure, activity and partic-ipation.4 This framework has been endorsed for use as theinternational standard to describe and assess health anddisability. Disability data can be correlated with medical andrehabilitative service requirements. Studies on rehabilitationand rheumatology have previously used the ICF as an outcomemeasure.5–9 The ICF Comprehensive and Brief Core Sets,with the latter termed the IBD disability index (IBD-DI), haverecently been developed for IBD to measure its functionalconsequences and disease burden.10,11 The IBD-DI was devel-oped following an extensive literature search and consensuspertaining to disability in IBD. This questionnaire, however,has not yet been tested clinically or validated to capture thefull spectrum of issues in IBD. To date no scoring system hasbeen designed for the IBD-DI, which ideally must reflectthe fluctuating nature of both Crohn's disease (CD) andulcerative colitis (UC), demonstrate reversibility followingsuccessful medical and surgical therapies, and capture themulti-dimensionality of IBD. This score should be objective, has
stu(20
a sufficiently wide range to be useful, correlate with workabsenteeism, and correlate withmeasures of quality of life anddisease activity.
The primary objective of this study was to design andvalidate a numerical scoring system for the IBD-DI tomeasure IBD disability using standard statistical tech-niques. Secondary endpoints were to describe the extentof disability in IBD, correlate the disease index with workabsenteeism, and identify significant exploratory predic-tors of employment status.
2. Materials and methods
2.1. Subjects
Consecutive ambulatory patients aged 16 to 80 years oldwith established CD and UC of at least 6 months wereprospectively recruited from the IBD clinics of Concord andBankstown Hospitals, which are tertiary IBD referralcenters in Sydney, Australia. Subjects were excluded ifthey were unable to comprehend the questionnaire, havean active psychiatric disorder, significant symptomatic co-morbidity that might influence disability, with stomas orileoanal pouches were excluded. Age- and sex- group-matchedcontrols without a gastrointestinal disorder or gastrointestinalsymptoms in the preceding month were recruited to deter-mine baseline function. They were recruited from the samecatchment area as cases, typically hospital visitors andrelatives of patients. The Australian unemployment rate atthe time of the study was b5%.
2.2. Inflammatory bowel disease disability index(IBD-DI) score
The ICF IBD-DI consists of 19 items divided into 28 partscovering the 5 domains of Overall Health, Body Function,Body Structures, Activity Participation and EnvironmentalFactors.10 The IBD-DI was specifically designed to excludethe use of any questions that examine patients' subjectivecoping and feelings. It explores the severity of disability andlimitations in the areas of sleeping, mood, abdominal pain,bowel frequency, regulating defecation, participation insocial events and work or school and exacerbating effects ofmedication, food, family and healthcare professionals. Inline with other ICF scores, positive scores were proportionalto the lack of difficulties and the alleviating effects ofmedication, food, family and healthcare professionals. Anovel composite scoring system was designed and imple-mented to test the IBD-DI to represent the presence and
dy of the International Classification of Functioning, Disability and14), http://dx.doi.org/10.1016/j.crohns.2014.02.028
3IBD Disability Index Validation Study
severity of disability in the previous week with lower or morenegative scores indicating greater disability (Appendix A).The response of each item on the questionnaire was eitherdichotomous “yes” versus “no” or ordinal on a 1 to 5 Likertscale (1 being no difficulty and 5 being extreme difficulty).Scores from each question were combined into domain totalsand a final composite score representative of the overalldegree of disability ranging from −80 (maximum degree ofdisability) to 22 (no disability) with ‘0’ as the anticipatedpoint of neutrality. Scores of severe, moderate, mild andminimal disability correlated with the ability to work b50%,50–75%, 76–99% and 100% of work-hours in the previousweek.
Pilot testing was performed on 5 IBD patients todetermine the questionnaire script, test the protocol andthe scoring system. The questionnaire was administeredface-to-face by a single trained research assistant (TH)blinded to the clinical encounter and the subject's IBDhistory. Subjects completed the questionnaire prior to theirphysician interview to ensure independent self-reporting.The face-to-face questionnaire administration ensured thatthere was no missing data. IBD subjects were invited toprovide commentary relating to the questionnaire and torepeat the questionnaires 4 weeks later to capture anychanges to the IBD-DI.
2.3. Demographics and comparative assessment tools
Clinical information obtained included demography,smoking status, disease duration, IBD phenotype, 12 thepresence of extra-intestinal manifestations (EIM), medicaltreatment, prior hospitalization and surgery. Subjectscompleted the Work Productivity and Activity ImpairmentQuestionnaire: General Health that measured the impact ofhealth problems on employment status, number of hoursworked, work productivity and daily activities in thepreceding week. Employment was defined as labor forceparticipation of at least 1 day per week with 35–40 hregarded as full-time work.
Patients also completed the 32-question InflammatoryBowel Disease Questionnaire (IBDQ) measuring theirsubjective disease-related quality of life.13 Disease activ-ities were measured using the Crohn's Disease ActivityIndex (CDAI) for CD 14 and partial Mayo Score (pMayo) forUC.15 The CDAI assessed the parameters of soft/liquidstool frequency, abdominal pain, well-being, EIM, fistulas,abdominal mass, use of anti-diarrheal agent, anemia andweight loss. The pMayo was scored according to diarrhea, perrectal bleeding and physician global scale of disease severity.Higher scores represented greater disease severities.
2.4. Power calculation
Using social security system data covering 93% of theGerman workforce, the disability rate of IBD patientsrequiring rehabilitation was 9%.16 Power calculation wasbased on the ability to detect a difference in overall severedisability of 9% with 80% power and a 1-sided alpha level of0.05. Recruitment using a 2:1 ratio of cases versus controlsrequired a sample size of 115 IBD cases to 50 controls.
Please cite this article as: Leong RWL, et al, Prospective validation stuHealth score in Crohn's disease and ulcerative colitis, J Crohns Colitis (20
2.5. Statistics and ethical consideration
The IBD-DI total score and domain sub-scores were analyzedusing non-parametric tests of Spearman correlation, MannWhitney U, Wilcoxon signed-rank test for unpaired andpaired median comparisons respectively and Kruskal–Wallistest for comparison of 3 or more continuous variables.Discriminant ability refers to how well the IBD-DI differen-tiated active IBD from controls. Construct validity refers tohow well the IBD-DI correlated with the IBDQ (convergentvalidity) and clinical disease activity indices (divergentvalidity). Paired IBD-DI of a subject's index and repeat scoreswas tested for test–retest reliability in those with stabledisease activity. Responsiveness was assessed by comparingpre- and post-treatment in those with clinically relevantchanges in disease activity (defined as a CDAI change of N70points in CD or pMayo score of N2 in UC) and measured byWilcoxon signed-rank test, effect size and responsivenesscoefficient. Reliability assessed the homogeneity of theIBD-DI using intra-class correlation coefficient (ICC), andstandardized Cronbach's alpha for internal consistency. AnICC of N0.8 indicates excellent reliability. Data reduction,dimensionality and variance testing was performed byfactor analysis using principal component analysis with anEigenfeld value N1 and the varimax rotation method.Receiver operator characteristics (ROC) was performedand measured by area under curve (AUC) to identify thebest statistical cut-off differentiating IBD from controls.Subjects provided commentary on disability and the IBD-DIand the time to its completion was recorded. Thequestionnaire readability was tested using the Fleschreading scale. Binary logistic regression was performed todetermine independent predictive factors of employmentstatus.
Statistical analyses were performed using IBM SPSS version20.0. A P value of less than 0.05 was deemed statisticallysignificant. Informed consent was obtained for all subjects.The study was approved by the Concord Hospital EthicsCommittee and registered with the Australian New ZealandClinical Trials Registry (ACTRN12613000903785).
3. Results
3.1. Study population
Over a 6 month period, 192 consecutive subjects wereprospectively approached for the study. Of these 10 wereexcluded due to limited comprehension, 13 declinedparticipation and 3 failed to complete the full studyprotocol. There was no missing data. Of the 166 subjectsrecruited, 116 were IBD patients (75 CD, 41 UC) and 50 werecontrols. In the patient group, 35 (21 CD 14 UC) patientsconsented for a follow up survey. Of these paired cases, 20 hadstable disease and 15 had significant clinical changes in theirdisease activities. The mean ages of IBD subjects and controlswere 40.5 and 41.2 respectively and male sex proportion was52.6% and 56.0% respectively (both P N 0.05). Only 59.5% ofIBD subjects (61% CD, 56%UC; P = 0.30) were in current full- orpart-time employment or study compared to 100% of controls.Only 1 control (2%, 95% CI: +/−3.9) had a negative IBD-DI score(Table 1).
dy of the International Classification of Functioning, Disability and14), http://dx.doi.org/10.1016/j.crohns.2014.02.028
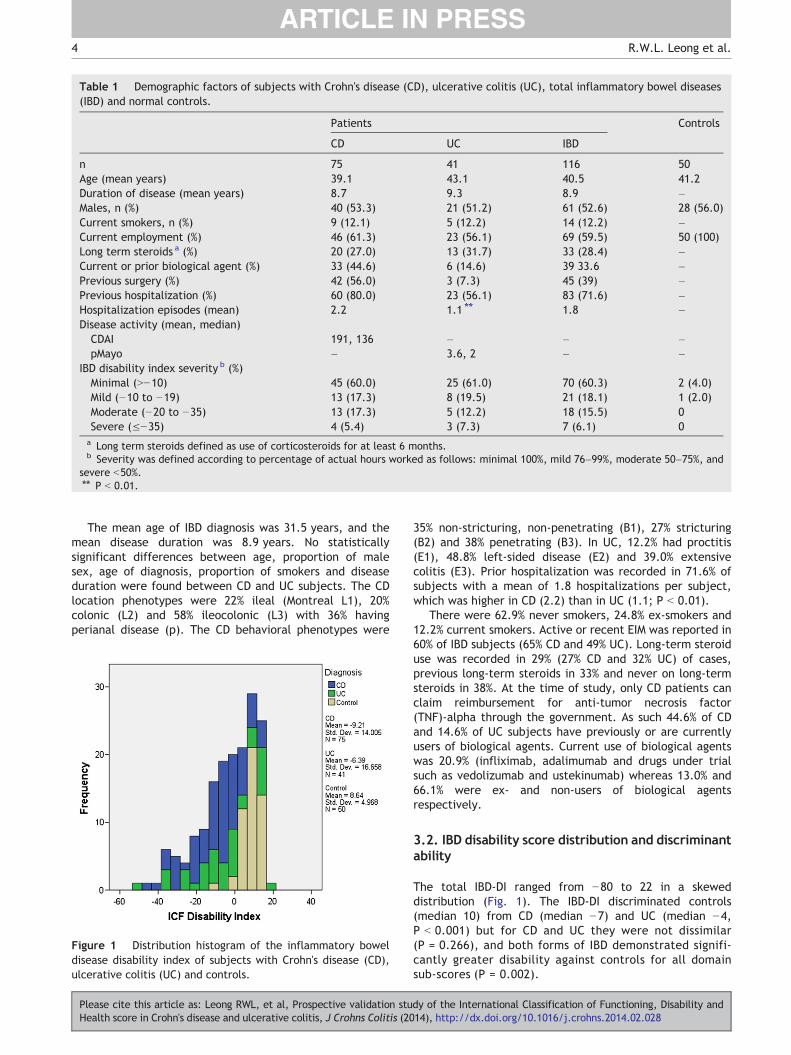
Table 1 Demographic factors of subjects with Crohn's disease (CD), ulcerative colitis (UC), total inflammatory bowel diseases(IBD) and normal controls.
Patients Controls
CD UC IBD
n 75 41 116 50Age (mean years) 39.1 43.1 40.5 41.2Duration of disease (mean years) 8.7 9.3 8.9 –Males, n (%) 40 (53.3) 21 (51.2) 61 (52.6) 28 (56.0)Current smokers, n (%) 9 (12.1) 5 (12.2) 14 (12.2) –Current employment (%) 46 (61.3) 23 (56.1) 69 (59.5) 50 (100)Long term steroids a (%) 20 (27.0) 13 (31.7) 33 (28.4) –Current or prior biological agent (%) 33 (44.6) 6 (14.6) 39 33.6 –Previous surgery (%) 42 (56.0) 3 (7.3) 45 (39) –Previous hospitalization (%) 60 (80.0) 23 (56.1) 83 (71.6) –Hospitalization episodes (mean) 2.2 1.1 ⁎⁎ 1.8 –Disease activity (mean, median)CDAI 191, 136 – – –pMayo – 3.6, 2 – –
IBD disability index severity b (%)Minimal (N−10) 45 (60.0) 25 (61.0) 70 (60.3) 2 (4.0)Mild (−10 to −19) 13 (17.3) 8 (19.5) 21 (18.1) 1 (2.0)Moderate (−20 to −35) 13 (17.3) 5 (12.2) 18 (15.5) 0Severe (≤−35) 4 (5.4) 3 (7.3) 7 (6.1) 0a Long term steroids defined as use of corticosteroids for at least 6 months.b Severity was defined according to percentage of actual hours worked as follows: minimal 100%, mild 76–99%, moderate 50–75%, and
severe b50%.⁎⁎ P b 0.01.
4 R.W.L. Leong et al.
The mean age of IBD diagnosis was 31.5 years, and themean disease duration was 8.9 years. No statisticallysignificant differences between age, proportion of malesex, age of diagnosis, proportion of smokers and diseaseduration were found between CD and UC subjects. The CDlocation phenotypes were 22% ileal (Montreal L1), 20%colonic (L2) and 58% ileocolonic (L3) with 36% havingperianal disease (p). The CD behavioral phenotypes were
Figure 1 Distribution histogram of the inflammatory boweldisease disability index of subjects with Crohn's disease (CD),ulcerative colitis (UC) and controls.
Please cite this article as: Leong RWL, et al, Prospective validation stuHealth score in Crohn's disease and ulcerative colitis, J Crohns Colitis (20
35% non-stricturing, non-penetrating (B1), 27% stricturing(B2) and 38% penetrating (B3). In UC, 12.2% had proctitis(E1), 48.8% left-sided disease (E2) and 39.0% extensivecolitis (E3). Prior hospitalization was recorded in 71.6% ofsubjects with a mean of 1.8 hospitalizations per subject,which was higher in CD (2.2) than in UC (1.1; P b 0.01).
There were 62.9% never smokers, 24.8% ex-smokers and12.2% current smokers. Active or recent EIM was reported in60% of IBD subjects (65% CD and 49% UC). Long-term steroiduse was recorded in 29% (27% CD and 32% UC) of cases,previous long-term steroids in 33% and never on long-termsteroids in 38%. At the time of study, only CD patients canclaim reimbursement for anti-tumor necrosis factor(TNF)-alpha through the government. As such 44.6% of CDand 14.6% of UC subjects have previously or are currentlyusers of biological agents. Current use of biological agentswas 20.9% (infliximab, adalimumab and drugs under trialsuch as vedolizumab and ustekinumab) whereas 13.0% and66.1% were ex- and non-users of biological agentsrespectively.
3.2. IBD disability score distribution and discriminantability
The total IBD-DI ranged from −80 to 22 in a skeweddistribution (Fig. 1). The IBD-DI discriminated controls(median 10) from CD (median −7) and UC (median −4,P b 0.001) but for CD and UC they were not dissimilar(P = 0.266), and both forms of IBD demonstrated signifi-cantly greater disability against controls for all domainsub-scores (P = 0.002).
dy of the International Classification of Functioning, Disability and14), http://dx.doi.org/10.1016/j.crohns.2014.02.028
IBD-Disability Index200-20-40-60
IBD
Q
250
200
150
100
50
0
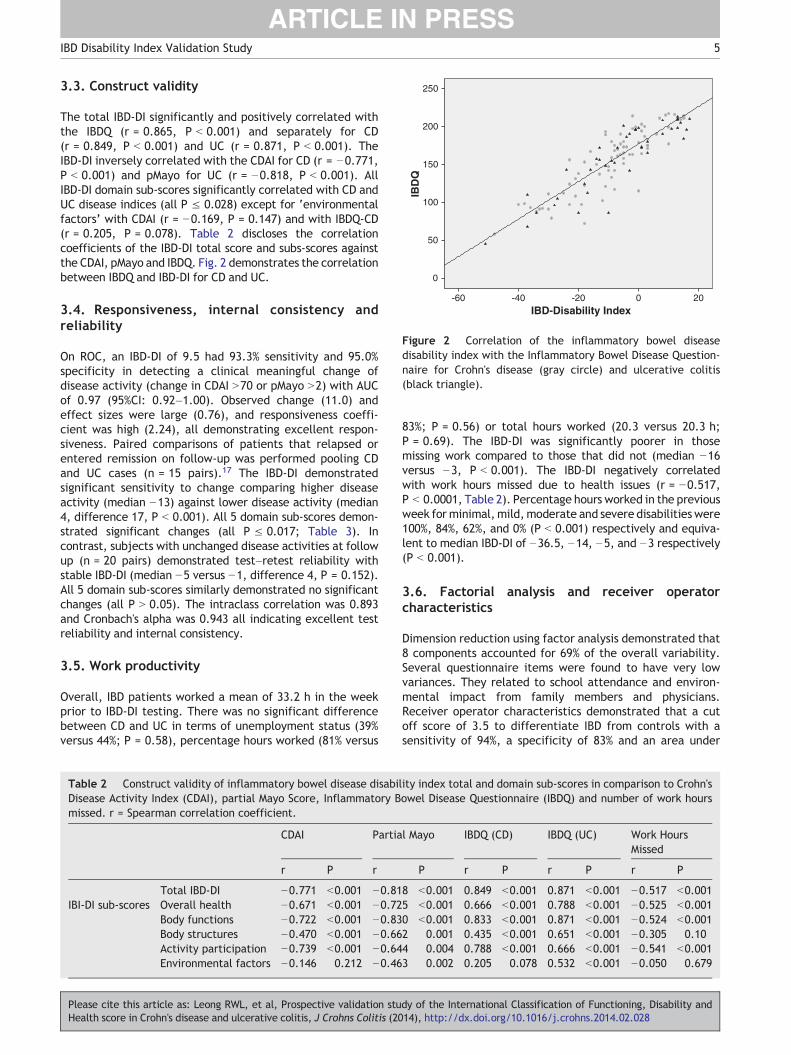
Figure 2 Correlation of the inflammatory bowel diseasedisability index with the Inflammatory Bowel Disease Question-naire for Crohn's disease (gray circle) and ulcerative colitis(black triangle).
5IBD Disability Index Validation Study
3.3. Construct validity
The total IBD-DI significantly and positively correlated withthe IBDQ (r = 0.865, P b 0.001) and separately for CD(r = 0.849, P b 0.001) and UC (r = 0.871, P b 0.001). TheIBD-DI inversely correlated with the CDAI for CD (r = −0.771,P b 0.001) and pMayo for UC (r = −0.818, P b 0.001). AllIBD-DI domain sub-scores significantly correlated with CD andUC disease indices (all P ≤ 0.028) except for ‘environmentalfactors’ with CDAI (r = −0.169, P = 0.147) and with IBDQ-CD(r = 0.205, P = 0.078). Table 2 discloses the correlationcoefficients of the IBD-DI total score and subs-scores againstthe CDAI, pMayo and IBDQ. Fig. 2 demonstrates the correlationbetween IBDQ and IBD-DI for CD and UC.
3.4. Responsiveness, internal consistency andreliability
On ROC, an IBD-DI of 9.5 had 93.3% sensitivity and 95.0%specificity in detecting a clinical meaningful change ofdisease activity (change in CDAI N70 or pMayo N2) with AUCof 0.97 (95%CI: 0.92–1.00). Observed change (11.0) andeffect sizes were large (0.76), and responsiveness coeffi-cient was high (2.24), all demonstrating excellent respon-siveness. Paired comparisons of patients that relapsed orentered remission on follow-up was performed pooling CDand UC cases (n = 15 pairs).17 The IBD-DI demonstratedsignificant sensitivity to change comparing higher diseaseactivity (median −13) against lower disease activity (median4, difference 17, P b 0.001). All 5 domain sub-scores demon-strated significant changes (all P ≤ 0.017; Table 3). Incontrast, subjects with unchanged disease activities at followup (n = 20 pairs) demonstrated test–retest reliability withstable IBD-DI (median −5 versus −1, difference 4, P = 0.152).All 5 domain sub-scores similarly demonstrated no significantchanges (all P N 0.05). The intraclass correlation was 0.893and Cronbach's alpha was 0.943 all indicating excellent testreliability and internal consistency.
3.5. Work productivity
Overall, IBD patients worked a mean of 33.2 h in the weekprior to IBD-DI testing. There was no significant differencebetween CD and UC in terms of unemployment status (39%versus 44%; P = 0.58), percentage hours worked (81% versus
Table 2 Construct validity of inflammatory bowel disease disabilDisease Activity Index (CDAI), partial Mayo Score, Inflammatory Bmissed. r = Spearman correlation coefficient.
CDAI Partia
r P r
Total IBD-DI −0.771 b0.001 −0.81IBI-DI sub-scores Overall health −0.671 b0.001 −0.72
Body functions −0.722 b0.001 −0.83Body structures −0.470 b0.001 −0.66Activity participation −0.739 b0.001 −0.64Environmental factors −0.146 0.212 −0.46
Please cite this article as: Leong RWL, et al, Prospective validation stuHealth score in Crohn's disease and ulcerative colitis, J Crohns Colitis (20
83%; P = 0.56) or total hours worked (20.3 versus 20.3 h;P = 0.69). The IBD-DI was significantly poorer in thosemissing work compared to those that did not (median −16versus −3, P b 0.001). The IBD-DI negatively correlatedwith work hours missed due to health issues (r = −0.517,P b 0.0001, Table 2). Percentage hours worked in the previousweek for minimal,mild,moderate and severe disabilities were100%, 84%, 62%, and 0% (P b 0.001) respectively and equiva-lent to median IBD-DI of −36.5, −14, −5, and −3 respectively(P b 0.001).
3.6. Factorial analysis and receiver operatorcharacteristics
Dimension reduction using factor analysis demonstrated that8 components accounted for 69% of the overall variability.Several questionnaire items were found to have very lowvariances. They related to school attendance and environ-mental impact from family members and physicians.Receiver operator characteristics demonstrated that a cutoff score of 3.5 to differentiate IBD from controls with asensitivity of 94%, a specificity of 83% and an area under
ity index total and domain sub-scores in comparison to Crohn'sowel Disease Questionnaire (IBDQ) and number of work hours
l Mayo IBDQ (CD) IBDQ (UC) Work HoursMissed
P r P r P r P
8 b0.001 0.849 b0.001 0.871 b0.001 −0.517 b0.0015 b0.001 0.666 b0.001 0.788 b0.001 −0.525 b0.0010 b0.001 0.833 b0.001 0.871 b0.001 −0.524 b0.0012 0.001 0.435 b0.001 0.651 b0.001 −0.305 0.104 0.004 0.788 b0.001 0.666 b0.001 −0.541 b0.0013 0.002 0.205 0.078 0.532 b0.001 −0.050 0.679
dy of the International Classification of Functioning, Disability and14), http://dx.doi.org/10.1016/j.crohns.2014.02.028
Table 3 IBD disability index total and domain sub-scores of subjects with paired results divided into those with changed diseaseactivities and those with stable disease activities.
Domain First IBD-DI Second IBD-DI P
Changed disease activity a Total IBD-DI −13.0 4.0 b0.001Overall health −2.0 −1.0 0.013Body functions −13.0 −3.0 b0.001Body structures 0.0 2.0 0.011Activity participation −8.0 −2.0 b0.001Environmental factors 4.0 8.0 0.017
Stable disease activity Total IBD-DI −5.0 −1.0 0.152Overall health −1.0 −1.0 0.782Body functions −5.5 −4.0 0.252Body structures 0.0 0.0 0.726Activity participation −1.5 −2.0 0.655Environmental factors 6.0 6.0 0.253
a Pooled IBD cases with CDAI change of N70 points or pMayo change of N2 points.
6 R.W.L. Leong et al.
curve of 0.92 (95% CI: 0.87–0.97). This cut-off score wasconsidered close to the original score of “0” design torepresent neutrality.
The IBD-DI was not influenced by patient sex (P = 0.31),phenotype of CD or UC, peri-anal phenotype (P = 0.78) orprior surgery (P = 0.82) indicating current disease activity tobe a greater influence on disability. The presence of EIM,especially arthralgia, significantly worsened IBD-DI (P b 0.001).Smoking had no overall effect on IBD-DI but current smokingadversely affected the ‘body structure’ domain in CD and hadthe inverse effect in UC. Ex-smokers demonstrated improve-ment of disability in CD but worsening in UC (P = 0.047, Fig. 3).Younger subjects had significantly poorer IBD-DI (r = 0.244,P = 0.016) as did younger age of IBD diagnosis (r = 0.253,P = 0.028). Biological agents significantly improved IBD-DIcompared to ex-users (median IBD-DI −4 versus −13, P = 0.03).A trend towards improving IBD-DI between current biologicalagent users and non-users was found (median IBD-DI −4 versus−7, P = 0.052). Only the IBD-DI was an independent predictorof employment status (odds ratio [OR]: 0.94, 95% confidenceinterval [CI]: 0.89–0.99, P = 0.042; Table 4f). The IBDQ, use ofbiological agents, EIM, age, previous surgery, and diagnosis ofCD versus UC were not independent significant predictors ofemployment status on multivariate analysis.
3.7. Qualitative analysis
The questionnaire's completion time was between 10 and15 min with a Flesch reading score of 67 equivalent to a grade9 level of English. Respondents considered the questionnaireto capture many issues surrounding their disability but manycommented the redundancy of some items such as thatreferring to schooling. No patients felt the IBD-DI to beintrusive or disagreed with the need to identify and measuredisability.
4. Discussion
Functional limitations and restriction in participation corre-late with the economic impact of IBD. Work absenteeism andrequirement for financial support add to the mounting costof these diseases.18,19 Measuring disability is relevant to
Please cite this article as: Leong RWL, et al, Prospective validation stuHealth score in Crohn's disease and ulcerative colitis, J Crohns Colitis (20
patients, support organizations, lobby groups, social securityagencies, health insurance companies and government healthdepartments.20 High unemployment rates of 35% to 39% havebeen identified in IBD subjects from the USA, Netherlandsand Sweden 21–23 and are similar to the rate in our cohort of40%. Reversal of disability, therefore, becomes an essentialpatient-centered goal for medical and surgical treatments. Assuch, there needs to be a valid tool that measures disability.The IBD-DI was developed from the universally acceptedWHO International Classification for Functioning, Disabilityand Health.1 Using similar methods, core data sets havebeen developed for other chronic diseases such as systemicsclerosis, 8 and cross sectional cohort studies have assesseddisability such as in osteoarthritis.9 This is the first validationstudy using the ICF methodology on IBD and is the first studycorrelating a disability score with work productivity in IBD.Importantly, the IBD-DI was valid in measuring disability forboth CD and UC.
Recruitment from specialized IBD clinics provided thefull spectrum of disability necessary to validate the IBD-DI.Recruitment of controls also determined baseline levels offunctioning to which IBD patients can aspire. Patients inremission had IBD-DI similar to controls indicating thereversibility of disability. The IBD-DI correlated to both CDand UC clinical disease activities (negatively), work hoursmissed and with quality of life (positively) (all P b 0.001).The IBD-DI correlated closely with IBDQ, but only the IBD-DIwas an independent predictor of employment status onmultivariate logistic regression. It demonstrated test–retestreliability and excellent responsiveness to change. Priorsurgery, hospitalization and IBD phenotypes did not predictdisability levels, signifying the importance of current diseaseactivity in influencing disability. A previous study had alsorevealed that surgery, IBD location or behavioral phenotypesdid not influence quality of life.21 Arthralgia, the commonestEIM in our cohort, significantly increased disability. This wasalso seen in a previous study that found arthralgia to beassociatedwith unemployment (OR: 2.27; 95% CI: 1.27–7.14).24
Younger age, but not sex, was associated with greaterdisability, which was similar to a previous study on quality oflife.21,24 Current-smoking exacerbated the IBD-DI in CD and hadthe opposite effect in UC. This provided internal validation thatIBD-DI can detect the inverse smoking-related effects on CD
dy of the International Classification of Functioning, Disability and14), http://dx.doi.org/10.1016/j.crohns.2014.02.028
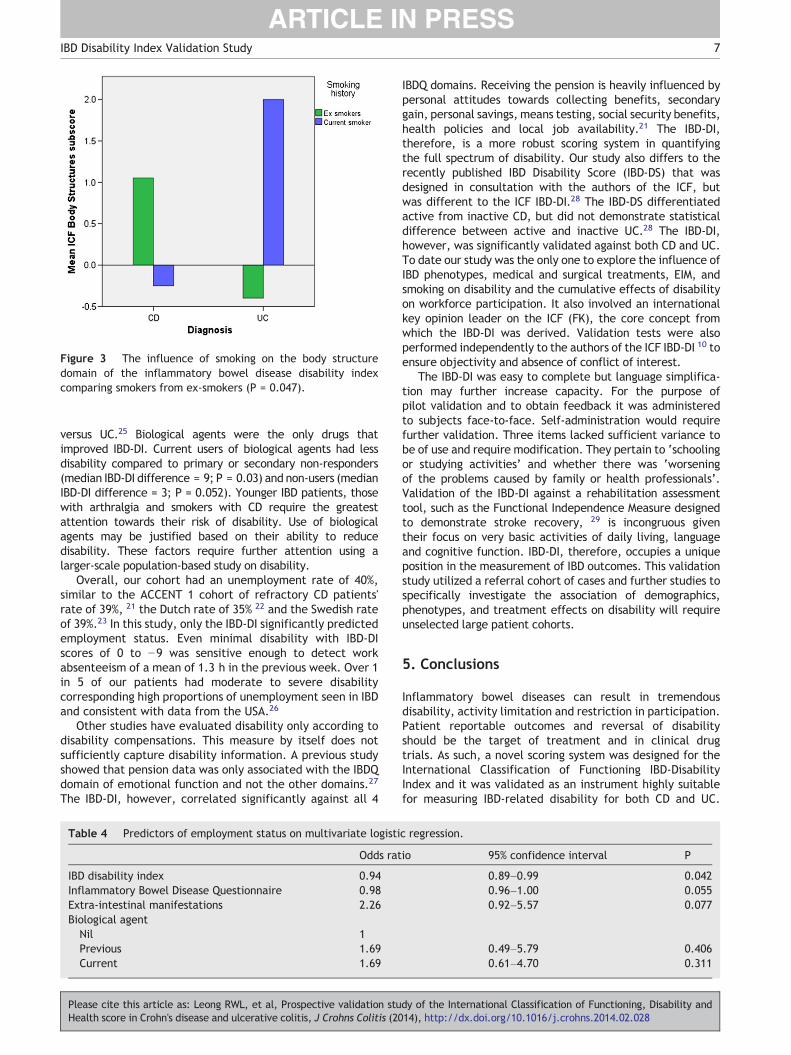
Figure 3 The influence of smoking on the body structuredomain of the inflammatory bowel disease disability indexcomparing smokers from ex-smokers (P = 0.047).
7IBD Disability Index Validation Study
versus UC.25 Biological agents were the only drugs thatimproved IBD-DI. Current users of biological agents had lessdisability compared to primary or secondary non-responders(median IBD-DI difference = 9; P = 0.03) and non-users (medianIBD-DI difference = 3; P = 0.052). Younger IBD patients, thosewith arthralgia and smokers with CD require the greatestattention towards their risk of disability. Use of biologicalagents may be justified based on their ability to reducedisability. These factors require further attention using alarger-scale population-based study on disability.
Overall, our cohort had an unemployment rate of 40%,similar to the ACCENT 1 cohort of refractory CD patients'rate of 39%, 21 the Dutch rate of 35% 22 and the Swedish rateof 39%.23 In this study, only the IBD-DI significantly predictedemployment status. Even minimal disability with IBD-DIscores of 0 to −9 was sensitive enough to detect workabsenteeism of a mean of 1.3 h in the previous week. Over 1in 5 of our patients had moderate to severe disabilitycorresponding high proportions of unemployment seen in IBDand consistent with data from the USA.26
Other studies have evaluated disability only according todisability compensations. This measure by itself does notsufficiently capture disability information. A previous studyshowed that pension data was only associated with the IBDQdomain of emotional function and not the other domains.27
The IBD-DI, however, correlated significantly against all 4
Table 4 Predictors of employment status on multivariate logisti
Odds rat
IBD disability index 0.94Inflammatory Bowel Disease Questionnaire 0.98Extra-intestinal manifestations 2.26Biological agent
Nil 1Previous 1.69Current 1.69
Please cite this article as: Leong RWL, et al, Prospective validation stuHealth score in Crohn's disease and ulcerative colitis, J Crohns Colitis (20
IBDQ domains. Receiving the pension is heavily influenced bypersonal attitudes towards collecting benefits, secondarygain, personal savings, means testing, social security benefits,health policies and local job availability.21 The IBD-DI,therefore, is a more robust scoring system in quantifyingthe full spectrum of disability. Our study also differs to therecently published IBD Disability Score (IBD-DS) that wasdesigned in consultation with the authors of the ICF, butwas different to the ICF IBD-DI.28 The IBD-DS differentiatedactive from inactive CD, but did not demonstrate statisticaldifference between active and inactive UC.28 The IBD-DI,however, was significantly validated against both CD and UC.To date our study was the only one to explore the influence ofIBD phenotypes, medical and surgical treatments, EIM, andsmoking on disability and the cumulative effects of disabilityon workforce participation. It also involved an internationalkey opinion leader on the ICF (FK), the core concept fromwhich the IBD-DI was derived. Validation tests were alsoperformed independently to the authors of the ICF IBD-DI 10 toensure objectivity and absence of conflict of interest.
The IBD-DI was easy to complete but language simplifica-tion may further increase capacity. For the purpose ofpilot validation and to obtain feedback it was administeredto subjects face-to-face. Self-administration would requirefurther validation. Three items lacked sufficient variance tobe of use and require modification. They pertain to ‘schoolingor studying activities’ and whether there was ‘worseningof the problems caused by family or health professionals’.Validation of the IBD-DI against a rehabilitation assessmenttool, such as the Functional Independence Measure designedto demonstrate stroke recovery, 29 is incongruous giventheir focus on very basic activities of daily living, languageand cognitive function. IBD-DI, therefore, occupies a uniqueposition in the measurement of IBD outcomes. This validationstudy utilized a referral cohort of cases and further studies tospecifically investigate the association of demographics,phenotypes, and treatment effects on disability will requireunselected large patient cohorts.
5. Conclusions
Inflammatory bowel diseases can result in tremendousdisability, activity limitation and restriction in participation.Patient reportable outcomes and reversal of disabilityshould be the target of treatment and in clinical drugtrials. As such, a novel scoring system was designed for theInternational Classification of Functioning IBD-DisabilityIndex and it was validated as an instrument highly suitablefor measuring IBD-related disability for both CD and UC.
c regression.
io 95% confidence interval P
0.89–0.99 0.0420.96–1.00 0.0550.92–5.57 0.077
0.49–5.79 0.4060.61–4.70 0.311
dy of the International Classification of Functioning, Disability and14), http://dx.doi.org/10.1016/j.crohns.2014.02.028
8 R.W.L. Leong et al.
Active disease, younger age, smokers with CD andarthralgia were significant predictors of disability. TheIBD-DI correlated with IBDQ and inversely with clinicaldisease activities. It was also the only significantindependent predictive factor for employment status.As such, the IBD-DI is suitable for health economics research,regulatory approval processes, or for clinical drug trialendpoint to ensure new treatments generate improvementin patient outcomes.
Conflict of interest
Rupert WL Leong declares no conflict of interest and hasapproved the final draft.
Tony Huang declares no conflict of interest and hasapproved the final draft.
Yanna Ko declares no conflict of interest and hasapproved the final draft.
Ari Jeon declares no conflict of interest and has approvedthe final draft.
Jeff Chang declares no conflict of interest and hasapproved the final draft.
Friedbert Kohler declares no conflict of interest and hasapproved the final draft.
Viraj Kariyawasam declares no conflict of interest and hasapproved the final draft.
No writing assistance was required.Potential competing interests: none.
Acknowledgments
Financial support: no specific support was provided for thisresearch project.
RWL is partly funded by a National Health and MedicalResearch Council Career Development Fellowship and is onthe advisory boards of Ferring Pharmaceuticals, AbbVieAustralia, Janssen, Takeda and has received honoraria fromFerring Pharmaceuticals, AbbVie Australia, Janssen, andShire.
Guarantor of the article: Rupert Leong.Specific author contributionsTH, YK, AJ, JC, FK, VK have no conflicts to disclose.RWL: study concept; study design, study supervision.RWL, TH, YK, AJ, JC, VK: patient recruitment, acquisition
of data, data entry.RWL, TH, JC, FK, VK: manuscript drafting, critical revision.RWL, TH, VK: statistical analysis, analysis and interpre-
tation of data.
Appendix A
The inflammatory bowel disease disability index scoring keyQuestion 1
• Very good = 0 score• Good = −1 score• Moderate = −2 score• Bad = −3 score• Very Bad = −4 score
Please cite this article as: Leong RWL, et al, Prospective validation stuHealth score in Crohn's disease and ulcerative colitis, J Crohns Colitis (20
Questions 2–13
• None = 0 score• Mild = −1 score• Moderate = −2 score• Severe = −3 score• Extreme = −4 score
B525: number of liquid/very soft stools in last week
• 0 = +1 score• 1–4 = −1 score• 5–8 = −2 score• 9–12 = −3 score• N12 = −4 score
BMI
• b15 = −2 score• 15.1–19.9 = −1 score• 20–24.9 = 0 score• 25–29.9 = −1 score• N30 = −2 score
B515: do you feel that you've lost weight in the last week?
• Yes = −1 score• No = +1 score
S540: blood in stool?
• None = +1 score• Little = −1 score• A lot = −2 score
S770: is arthritis or arthalgia present?
• Yes = −1 score• No = +1 score
Questions 14–18Positive/alleviating effects
• NA = +4 score• No positive effect = 0 score• Mild positive effect = +1 score• Moderate positive effect = +2 score• Severe positive effect = +3 score• Extreme positive effect = +4 score
Negative/worsening effects
• NA = 0 score• No negative effect = 0 score• Mild negative effect = −1 score• Moderate negative effect = −2 score• Severe negative effect = −3 score• Extreme negative effect = −4 score
Questions 18–19
• No = −1 score• Yes = +1 score
dy of the International Classification of Functioning, Disability and14), http://dx.doi.org/10.1016/j.crohns.2014.02.028
9IBD Disability Index Validation Study
References
1. World Health Organization. Document A29/INFDOCI/1; 1976[Geneva, Switzerland].
2. Peyrin-Biroulet L. What is the patient's perspective: howimportant are patient-reported outcomes, quality of life anddisability? Dig Dis 2010;28(3):463–71.
3. Kohler F, Selb M, Escorpizo R, Kostanjsek N, Stucki G, Riberto M.International Society of Physical and Rehabilitation MedicineSub-Committee Implementation of the ICF; Participants ofthe São Paulo ISPRM – World Health Organization Workshop.Towards the joint use of ICD and ICF: a call for contribution.J Rehabil Med 2012;44(10):805–10.
4. World Health Organization. International Classification ofFunctioning, Disability and Health: ICF. Geneva, Switzerland:WHO; 2001 [http://www.who.int/classifications/icf.appareas/en/index.html (accessed 28 May 2013)].
5. Okochi J, Takahashi T, Takamuku K, Escorpizo R. Staging ofmobility, transfer and walking functions of elderly persons basedon the codes of the International Classification of Functioning,Disability and Health. BMC Geriatr 2013;13:16.
6. Grill E, Stucki G. Scales could be developed based on simpleclinical ratings of International Classification of Functioning,Disability and Health Core Set categories. J Clin Epidemiol2009;62(9):891–8.
7. Kohler F, Xu J, Siva-Withmory C, Arockiam J. Feasibility of usinga checklist based on the ICF as an outcome measure inindividuals following lower limb amputation. Prosthet OrthotInt 2011;35:294–301.
8. Saketkoo LA, Escorpizo R, Keen KJ, Fligelstone K, Distler O.ESUSTAR. International Classification of Functioning, Disabilityand Health Core Set construction in systemic sclerosis and otherrheumatic diseases: a EUSTAR initiative. Rheumatology Dec2012;51(12):2170–6.
9. Oberhauser C, Escorpizo R, Boonen A, Sticki G, Cieza A.Statistical validation of the brief International Classification ofFunctioning, Disability and Health Core Set for osteoarthritisbased on a large international sample of patients withosteoarthritis. Arthritis Care Res 2013;65(2):177–86.
10. Peyrin-Biroulet L, Cieza A, Sandborn WJ, Coenen M, Chowers Y,Hibi T, et al. International Programme to Develop New Indexesfor Crohn's Disease (IPNIC) group. Development of the firstdisability index for inflammatory bowel disease based on theinternational classification of functioning, disability and health.Gut Feb 2012;61(2):241–7.
11. Achleitner U, Coenen M, Colombel JF, Peyrin-Biroulet L,Sahakyan N, Cieza A. Identification of areas of functioning anddisability addressed in inflammatory bowel disease-specificpatient reported outcome measures. J Crohns Colitis Jun2012;6(5):507–17.
12. Silverberg MS, Satsangi J, Ahmad T, Arnott AD, Bernstein CN, BrantSR, et al. Toward an integrated clinical, molecular and serologicalclassification of inflammatory bowel disease: report of a workingparty of the2005MontrealWorld Congress of Gastroenterology.CanJ Gastroenterol 2005;19(Suppl A):5–36.
13. Guyatt G, Mitchell A, Irvine EJ, Singer J, Williams N. A newmeasure of health status for clinical trials in inflammatorybowel disease. Gastroenterology 1989;96:804–10.
Please cite this article as: Leong RWL, et al, Prospective validation stuHealth score in Crohn's disease and ulcerative colitis, J Crohns Colitis (20
14. Best WR, Becktel JM, Singleton JW, Kern Jr F. Development of aCrohn's disease activity index: National Cooperative Crohn'sDisease Study. Gastroenterology 1976;70:439–44.
15. Schroeder KW, Tremaine WJ, Ilstrup DM. Coated oral5-aminosalicylic acid therapy for mildly to moderately activeulcerative colitis: a randomized study. N Engl J Med 1987;317:1625–9.
16. Sonnenberg A. Disability and need for rehabilitation among patientswith inflammatory bowel disease. Digestion 1992;51(3):168–78.
17. Leong RW, Lee YT, Ching JY, Sung JJ. Quality of life in Chinesepatients with inflammatory bowel disease: validation of theChinese translation of the Inflammatory Bowel Disease Ques-tionnaire. Aliment Pharmacol Ther 2003;17:711–8.
18. Ward FM, Bodger K, Daly MJ, Heatley RV. Clinical economicsreview: medical management of inflammatory bowel disease.Aliment Pharmacol Ther 1999;13:15–25.
19. Feagan BG, Vreeland MG, Larson LR, Bala MV. Annual cost ofcare for Crohn's disease: a payor perspective. Am J Gastroenterol2000;95:1955–60.
20. Picone D. Disability — people with a disability: responding toneeds during hospitalization. revised Jan 08, http://www0.health.nsw.gov.au/policies/pd/2008/pdf/PD2008_010.pdf [accessed Jun2013].
21. Feagan BG, Bala M, Yan S, Olson A, Hanauer S. Unemploymentand disability in patients with moderately to severely activeCrohn's disease. J Clin Gastroenterol May–Jun 2005;39(5):390–5.
22. Boonen A, Dagnelie PC, Feleus A, Hesselink MA, Muris JW,Stockbrügger RW, et al. The impact of inflammatory bowel diseaseon labor force participation: results of a population sampledcase–control study. Inflamm Bowel Dis Nov 2002;8(6):382–9.
23. Blomqvist P, Ekbom A. Inflammatory bowel diseases: healthcare and costs in Sweden in 1994. Scand J Gastroenterol1997;32:1134–9.
24. Casellas F, Vivancos JL, Sampedro M, Malagelada JR. Relevanceof the phenotypic characteristics of Crohn's disease in patientperception of health-related quality of life. Am J Gastroenterol2005;100:2737–42.
25. Lunney PC, Leong RWL. Review article: ulcerative colitis,smoking and nicotine therapy. Aliment Pharmacol Ther2012;36(11–12):997–1008.
26. Longobardi T, Jacobs P, Bernstein CN. Work losses related toinflammatory bowel disease in the United States: results fromthe National Health Interview Survey. Am J Gastroenterol2003;98:1064–72.
27. Bernklev T, Jahnsen J, Henriksen M, Lygren I, Aadland E, SauarJ, et al. Relationship between sick leave, unemployment,disability, and health‐related quality of life in patients withinflammatory bowel disease. Inflamm Bowel Dis 2006;12(5):402–12.
28. Allen PB, KammMA, Peyrin-Biroulet L, Studd C, McDowell C, AllenBC, et al. Development and validation of a patient-reporteddisability measurement tool for patients with inflammatory boweldisease. Aliment Pharmacol Ther Feb 2013;37(4):438–44.
29. Hamilton BB, Granger CV, Sherwin FS, Zielezny M, Tashman JS.A uniform national data system for medical rehabilitation.In: Fuhrer MJ, editor. Rehabilitation outcomes: analysis andmeasurement. Baltimore, MD: Brookes; 1987. p. 137–47.
dy of the International Classification of Functioning, Disability and14), http://dx.doi.org/10.1016/j.crohns.2014.02.028