Embed Size (px)
Citation preview
Prospective study of risk factors for ventilator-associatedpneumonia caused by Acinetobacter species
Julio Medina MDa,*, Carlos Formento MDb, Julio Pontet MDb,c, Andrea Curbelo MDd,Cristina Bazet MDe,f, Jorge Gerez MDd, Eduardo Larranaga MDd
aCatedra de Enfermedades Infecciosas, Instituto de Higiene, Facultad de Medicina, Universidad de la Republica,
Montevideo CP 11600, UruguaybUnidad Cuidados Intensivos del Hospital Pasteur, Montevideo, UruguaycPhysiology Department, Facultad de Medicina, Universidad de la Republica, Montevideo, UruguaydUnidad Cuidados Intensivos del Hospital Policial, Montevideo, UruguayeLaboratorio Clınico, Departamento de Microbiologıa, Hospital de Clınicas, Facultad de Medicina,
Universidad de la Republica, Montevideo, UruguayfLaboratorio de Microbiologıa, Hospital Pasteur, Montevideo, Uruguay
0883-9441/$ – see front matter D 2007
doi:10.1016/j.jcrc.2006.06.010
* Corresponding author. Tel.: +598
E-mail address: [email protected]
Keywords:Ventilator-associated
pneumonia;
Acinetobacter spp;
Intensive care unit;
Antibiotics;
Specific risk factors;
Prospective cohort study
AbstractSummary: The incidence of ventilator-associated pneumonia (VAP) by Acinetobacter spp (VAPA) is
increasing and has high morbidity and mortality. It is imperative to identify risk factors to be able to use
prevention policies.
Objective: The aim of this study was to identify specific risk factors for VAPA.
Design: Prospective cohort study.
Interventions: None.Setting: Two medical-surgical intensive care units.
Measurements: During a period of 36 months, all patients with more than 48 hours on mechanical
ventilation and suspected of having a VAP were enrolled. Only VAP with microbiological confirmation
was analyzed.
Results: Two hundred eighteen consecutive patients with clinical suspicion of VAP were enrolled.
One hundred twenty-five VAPs were confirmed by culture—46 by Acinetobacter spp and 79 by
other pathogens.
The 36 potential risk factors for Acinetobacter spp were analyzed by univariate analysis.
Logistic regression identified previous use of ceftriaxone (relative risk, 5.1; 95% confidence interval,
1.47-17.82) and previous use of ciprofloxacin (relative risk, 9.1; 95% confidence interval, 2.29-36.63)
as significant independent predictors for the development of VAPA.
Conclusions: Previous use of ceftriaxone and ciprofloxacin are independent risk factors for the
development of VAPA.
D 2007 Elsevier Inc. All rights reserved.
Journal of Critical Care (2007) 22, 18–27
Elsevier Inc. All rights reserved.
2 4876981; fax: +598 2 4876981.
y (J. Medina).

Prospective study of risk factors for VAP caused by Acinetobacter species 19
1. Introduction
Although there are various studies evaluating risk factors
associated to ventilator-associated pneumonia (VAP) by
Acinetobacter spp (VAPA), only a few are prospective or
case-control. The number of enrolled patients with VAPA is
also small in some studies [1-4].
With respect to mortality, there are authors that still
question the attributable mortality due to VAPA [5].
Although, some studies have showed increased mortality
[6] and even a 5-fold increase in mortality risk [7].
Infections by Acinetobacter spp determine new resis-
tance patterns forcing the use of broad-spectrum antibiotics,
which, in turn, increases economic costs and helps the
emergency of new multiresistant pathogens [8,9].
Acinetobacter spp is a nonfermentative, oxidase-
negative, aerobic, Gram-negative coccobacilli. It is an
ubiquitous resident, which grows preferably in moist
environment and has been isolated in food and inanimate
objects such as tap water faucets, sinks, bedside urinals,
hospital air, andmedical equipment. Little is known regarding
the pathogenesis of Acinetobacter spp infection [10,11].
To be able to develop prevention strategies, risk factors
related to VAPAwere sought: head trauma, acute respiratory
distress syndrome (ARDS), neurosurgery, copious pulmo-
nary aspiration, Glasgow Coma Scale (GCS) score of 9 or
lower, previous infection, severity of illness, previous use of
antibiotics (especially ceftazidime), and intravenous use
of fluorquinolones [1-4,12,13]. The emergency and spread
of Acinetobacter spp vary in each hospital, depending on
these factors.
However, there was a progressive increase of the
incidence of VAPA in our intensive care unit (ICU) without
a clear relation to the classic risk factors. Our aim was to
prospectively identify other specific risk factors for VAPA.
Table 1 Criteria for the diagnosis of VAP
1. New and persistent infiltrate in CXR
2. 2 or more of the following criteria:
Rectal temperature z 38.58C or b368CLeucocytosis z12 � 103 /mm3 or V4 � 103/mm3
Purulent respiratory secretions
3. 1 or more of the following:
BAL z104 CFU/mL
Positive tracheal aspirates plus CPIS N6
Microorganism isolated in z2 blood cultures with
identical sensitivity to tracheal secretions and in absence of
other possible infection
Positive culture of pleural fluid in absence of previous
pleural instrumentation
VAP was considered suspected when I and II were positive. VAP was
considered confirmed when 1, 2, and 3 were positive. BAL,
bronchoalveolar lavage; CXR, chest x-ray.
2. Materials and methods
2.1. Study design
Prospective cohort study.
2.2. Patient selection
This study was conducted during a 36-month
period (from May 2000 to May 2003) in 2 ICUs at Hospital
Pasteur and Hospital Policial in Montevideo, Uruguay.
Hospital Pasteur is a 23-bed medical-surgical ICU with
10 ventilated beds. Hospital Policial is a 14-bed medical-
surgical ICU with 8 ventilated beds. Hospital Pasteur is a
general surgical ICU but differing from Hospital Policial; it
does not include neurosurgery.
2.3. Inclusion criteria
All successive patients with 48 hours or more on
mechanical ventilation and suspected of having a VAP were
enrolled [14].
Only VAP with microbiological confirmation were
analyzed and divided into 2 sets—VAPA and VAP by
other pathogens.
Only the first episode of VAP was considered to avoid
the wrong diagnosis of VAP with a previous radio-
logic image.
2.4. Exclusion criteria
All nonconfirmed VAP and VAP developed within
48 hours of admission in patients transferred from other
centers were excluded.
2.5. Diagnosis of VAP
The diagnostic criteria for VAP used in this study were
modified from those established by the American College of
Chest Physicians [24] and the ones used by Ibrahim et al
[15,16]. These criteria are presented on Table 1.
The most common diagnostic criteria were bronchoal-
veolar lavage of 104 CFU/mL or higher and a positive
tracheal aspirate plus clinical pulmonary infection score
(CPIS) higher than 6, adapted by Flanagan et al [17].
For processing endotracheal aspirates, we used a
semiquantitative culture method. For semiquantitative
analysis, purulent aspirate was inoculated in conventional
agar media. The number of colony forming units (CFU)
was determined by the 4-quadrant method and classified
as follows: no growth, 1+, 2+, 3+, or 4+ [18]. The bacterial
growth in 1, 2, or 3 quadrants of the culture dishes was not
taken into account. Only the 4-quadrant growth was
considered because it had a good correlation with
quantitative methods and was equivalent to 106 CFU or
higher [19].
Patients with bronchoalveolar lavage below 10 4 CFU/
mL were not included.
When it was not possible to perform a bronchoalveolar
lavage, the diagnosis of VAP was done with tracheal
aspirate plus CPIS higher than 6.
J. Medina et al.20
2.6. Definitions
Consensus definitions for ARDS, severe sepsis, and
septic shock were used [20,21]. Community-acquired
pneumonia (CAP) was considered severe, using criteria
described by Ewig et al [22]. Patients with CAP and
multiple organ dysfunction syndrome (MODS) were con-
sidered to have severe respiratory sepsis.
Previous antibiotic use was considered if the patient had
received 48 hours or more of intravenous antibiotics within
the previous 2 weeks. So, patients who received antibiotics
as preoperation prophylaxis therapy were not taken into
account. In no case was the use of selective digestive
decontamination performed. We did not use any specific
oral care agents to decontaminate oropharyngeal cavity.
We considered VAP cured if the leukocyte count
decreased to below 10000/mm3, temperature was below
388C, Pa/Fio2 was below 250, and if there was a decrease
of purulent tracheal secretions and decrease or disappear-
ance of the etiologic microorganism from the cultures of
tracheal aspirates or nonbronchoscopic bronchoalveolar
lavage. We did not take into account the chest radiographs
for assessing the resolution of the VAP [23] We assessed
the resolution of the VAP between the sixth day from the
beginning of the antimicrobial treatment and 72 hours after
completion of therapy.
Crude mortality was considered as total number of deaths
with VAP. Related VAP mortality was defined as death by
VAP or deaths that could not be attributed to other causes.
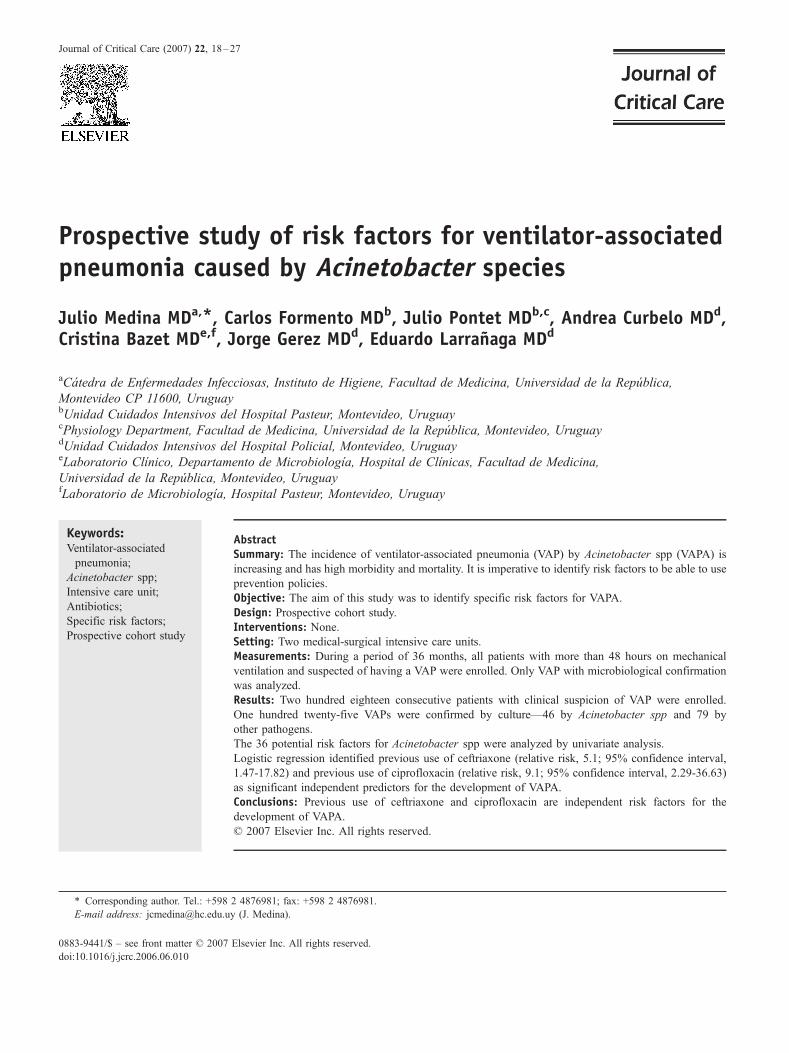
Table 2 Characteristics of the patients included in this study
Variables VAPA (n = 46) Other
Age (y)
Mean (SD) 54.5 (19.2)
Median (interquartile range) 56.5 (46.25-69.75)
No. (%) of women 18 (40)
APACHE II at admission
Mean (SD) 21.0 (7.8)
Median (interquartile range) 20 (16-27)
Criteria proposed by McCabe and Jackson [22]
Rapidly fatal disease (n [%]) 0
Ultimately fatal disease (n [%]) 5 (10.8)
Nonfatal disease (n [%]) 41 (89.2)
Diagnosis at admission (n [%])
Nontraumatic ABI (n [%]) 10 (21.7)
Severe CAP (n [%]) 5 (10.8)
COPD exacerbation (n [%]) 4 (8.6)
Severe trauma (n [%]) 5 (10.8)
Severe sepsis (n [%]) 10 (21.8)
Drug overdose (n [%]) 0
Thoracoabdominal surgery (n [%]) 6 (13.0)
Miscellany (n [%]) 6 (13.0)
Day VAP
Mean (SD) 9.9 F 6.2
Median (interquartile range) 8.5 (5.25-12)
ABI, acute brain injury.
2.7. Microbiology
Microbiological sampling processing and identification
of isolated microorganisms were performed by standard
methods [24].
All nonfermentative, oxidase-negative, catalase-positive,
strictly aerobic, motionless, Gram-negative coccobacilli
were considered belonging to Acinetobacter genus [24].
Phenotype identification was completed with API 20 NE
system (Biomerieux, France).
Susceptibility tests were performed following recom-
mendations of the National Committee for Clinical Labo-
ratory Standards [25].
2.8. Data collection
All patients included in the protocol were followed up
daily until discharged from ICU.
The following variables were recorded: sex, age, nutri-
tional status, smoking habits, alcoholism, use of cortico-
steroids, hemodialysis, presence of diabetes, cancer, chronic
obstructive pulmonary disease (COPD), AIDS, heart failure
functional class III to IV, lung aspiration, use of positive
pressure at end of expiration, use of anti-H2, reintubation,
previous surgery, head trauma, neurosurgery, and GCS.
We also recorded the need of mechanical ventilation,
following criteria by Zwillich et al [26]; previous medical
condition by criteria proposed by McCabe and Jackson [27];
days of mechanical ventilation; diagnosis of VAP;
CPIS [17] the day that VAP was diagnosed; responsible
pathogens (n = 79) P Standardized difference [31]
56.1 (17.0) .61 0.09
56 (45-73)
21 (26.6) .16
19.5 (6.8) .26 0.2
19 (14.5-25)
1
10 (12.6)
68 (86.1) 1
26 (32.9) .22
10 (12.6) 1.00
5 (6.3) .72
10 (12.6) 1.00
4 (5.1) .007
5 (6.3) .15
8 (10.1) .76
11 (13.9) 1.00
7.2 F 5.5 .012 0.47
5 (3-9.5)
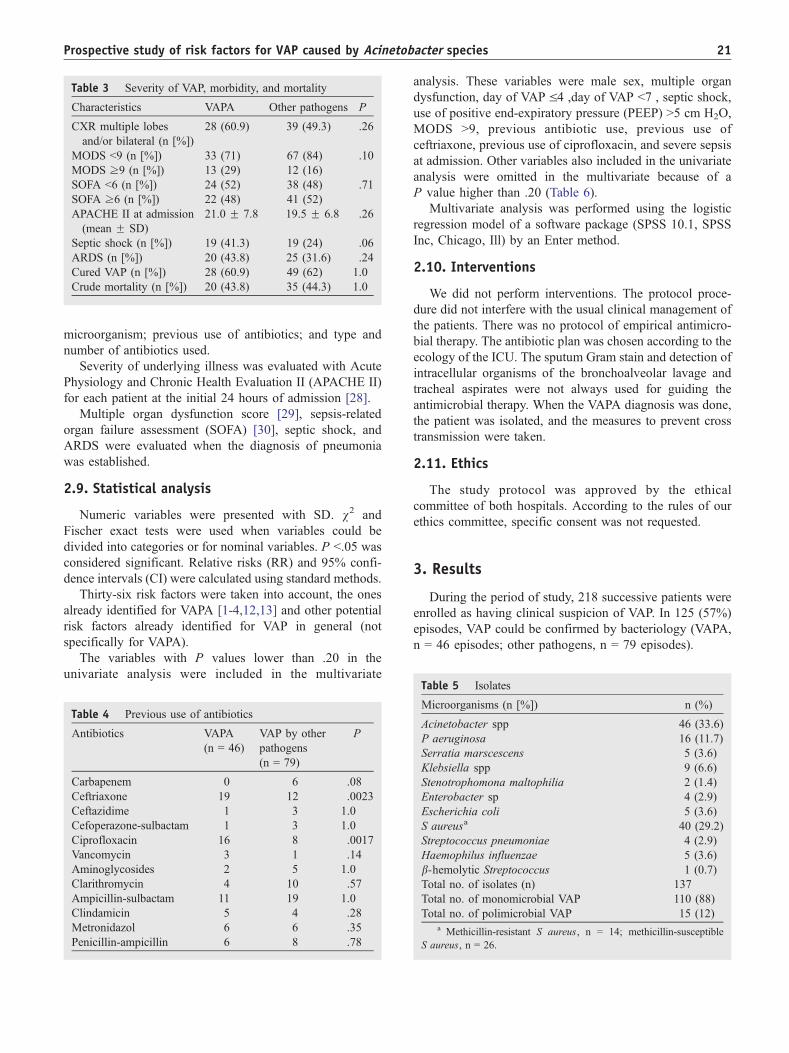
Table 3 Severity of VAP, morbidity, and mortality
Characteristics VAPA Other pathogens P
CXR multiple lobes
and/or bilateral (n [%])
28 (60.9) 39 (49.3) .26
MODS b9 (n [%]) 33 (71) 67 (84) .10
MODS z9 (n [%]) 13 (29) 12 (16)
SOFA b6 (n [%]) 24 (52) 38 (48) .71
SOFA z6 (n [%]) 22 (48) 41 (52)
APACHE II at admission
(mean F SD)
21.0 F 7.8 19.5 F 6.8 .26
Septic shock (n [%]) 19 (41.3) 19 (24) .06
ARDS (n [%]) 20 (43.8) 25 (31.6) .24
Cured VAP (n [%]) 28 (60.9) 49 (62) 1.0
Crude mortality (n [%]) 20 (43.8) 35 (44.3) 1.0
Prospective study of risk factors for VAP caused by Acinetobacter species 21
microorganism; previous use of antibiotics; and type and
number of antibiotics used.
Severity of underlying illness was evaluated with Acute
Physiology and Chronic Health Evaluation II (APACHE II)
for each patient at the initial 24 hours of admission [28].
Multiple organ dysfunction score [29], sepsis-related
organ failure assessment (SOFA) [30], septic shock, and
ARDS were evaluated when the diagnosis of pneumonia
was established.
2.9. Statistical analysis
Numeric variables were presented with SD. v2 and
Fischer exact tests were used when variables could be
divided into categories or for nominal variables. P b.05 was
considered significant. Relative risks (RR) and 95% confi-
dence intervals (CI) were calculated using standard methods.
Thirty-six risk factors were taken into account, the ones
already identified for VAPA [1-4,12,13] and other potential
risk factors already identified for VAP in general (not
specifically for VAPA).
The variables with P values lower than .20 in the
univariate analysis were included in the multivariate
Table 4 Previous use of antibiotics
Antibiotics VAPA
(n = 46)
VAP by other
pathogens
(n = 79)
P
Carbapenem 0 6 .08
Ceftriaxone 19 12 .0023
Ceftazidime 1 3 1.0
Cefoperazone-sulbactam 1 3 1.0
Ciprofloxacin 16 8 .0017
Vancomycin 3 1 .14
Aminoglycosides 2 5 1.0
Clarithromycin 4 10 .57
Ampicillin-sulbactam 11 19 1.0
Clindamicin 5 4 .28
Metronidazol 6 6 .35
Penicillin-ampicillin 6 8 .78
analysis. These variables were male sex, multiple organ
dysfunction, day of VAP V4 ,day of VAP b7 , septic shock,
use of positive end-expiratory pressure (PEEP) N5 cm H2O,
MODS N9, previous antibiotic use, previous use of
ceftriaxone, previous use of ciprofloxacin, and severe sepsis
at admission. Other variables also included in the univariate
analysis were omitted in the multivariate because of a
P value higher than .20 (Table 6).
Multivariate analysis was performed using the logistic
regression model of a software package (SPSS 10.1, SPSS
Inc, Chicago, Ill) by an Enter method.
2.10. Interventions
We did not perform interventions. The protocol proce-
dure did not interfere with the usual clinical management of
the patients. There was no protocol of empirical antimicro-
bial therapy. The antibiotic plan was chosen according to the
ecology of the ICU. The sputum Gram stain and detection of
intracellular organisms of the bronchoalveolar lavage and
tracheal aspirates were not always used for guiding the
antimicrobial therapy. When the VAPA diagnosis was done,
the patient was isolated, and the measures to prevent cross
transmission were taken.
2.11. Ethics
The study protocol was approved by the ethical
committee of both hospitals. According to the rules of our
ethics committee, specific consent was not requested.
3. Results
During the period of study, 218 successive patients were
enrolled as having clinical suspicion of VAP. In 125 (57%)
episodes, VAP could be confirmed by bacteriology (VAPA,
n = 46 episodes; other pathogens, n = 79 episodes).
Table 5 Isolates
Microorganisms (n [%]) n (%)
Acinetobacter spp 46 (33.6)
P aeruginosa 16 (11.7)
Serratia marscescens 5 (3.6)
Klebsiella spp 9 (6.6)
Stenotrophomona maltophilia 2 (1.4)
Enterobacter sp 4 (2.9)
Escherichia coli 5 (3.6)
S aureusa 40 (29.2)
Streptococcus pneumoniae 4 (2.9)
Haemophilus influenzae 5 (3.6)
b-hemolytic Streptococcus 1 (0.7)
Total no. of isolates (n) 137
Total no. of monomicrobial VAP 110 (88)
Total no. of polimicrobial VAP 15 (12)a Methicillin-resistant S aureus, n = 14; methicillin-susceptible
S aureus, n = 26.
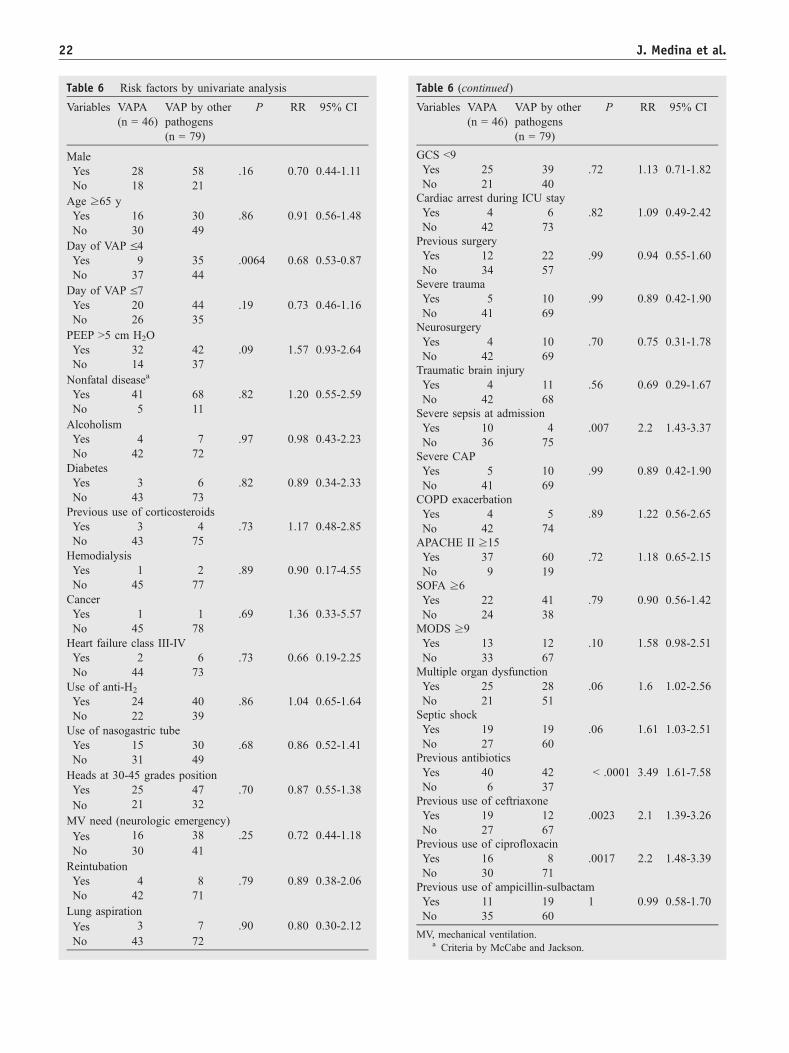
Table 6 Risk factors by univariate analysis
Variables VAPA
(n = 46)
VAP by other
pathogens
(n = 79)
P RR 95% CI
Male
Yes 28 58 .16 0.70 0.44-1.11
No 18 21
Age z65 y
Yes 16 30 .86 0.91 0.56-1.48
No 30 49
Day of VAP V4Yes 9 35 .0064 0.68 0.53-0.87
No 37 44
Day of VAP V7Yes 20 44 .19 0.73 0.46-1.16
No 26 35
PEEP N5 cm H2O
Yes 32 42 .09 1.57 0.93-2.64
No 14 37
Nonfatal diseasea
Yes 41 68 .82 1.20 0.55-2.59
No 5 11
Alcoholism
Yes 4 7 .97 0.98 0.43-2.23
No 42 72
Diabetes
Yes 3 6 .82 0.89 0.34-2.33
No 43 73
Previous use of corticosteroids
Yes 3 4 .73 1.17 0.48-2.85
No 43 75
Hemodialysis
Yes 1 2 .89 0.90 0.17-4.55
No 45 77
Cancer
Yes 1 1 .69 1.36 0.33-5.57
No 45 78
Heart failure class III-IV
Yes 2 6 .73 0.66 0.19-2.25
No 44 73
Use of anti-H2
Yes 24 40 .86 1.04 0.65-1.64
No 22 39
Use of nasogastric tube
Yes 15 30 .68 0.86 0.52-1.41
No 31 49
Heads at 30-45 grades position
Yes 25 47 .70 0.87 0.55-1.38
No 21 32
MV need (neurologic emergency)
Yes 16 38 .25 0.72 0.44-1.18
No 30 41
Reintubation
Yes 4 8 .79 0.89 0.38-2.06
No 42 71
Lung aspiration
Yes 3 7 .90 0.80 0.30-2.12
No 43 72
Table 6 (continued)
Variables VAPA
(n = 46)
VAP by other
pathogens
(n = 79)
P RR 95% CI
GCS b9
Yes 25 39 .72 1.13 0.71-1.82
No 21 40
Cardiac arrest during ICU stay
Yes 4 6 .82 1.09 0.49-2.42
No 42 73
Previous surgery
Yes 12 22 .99 0.94 0.55-1.60
No 34 57
Severe trauma
Yes 5 10 .99 0.89 0.42-1.90
No 41 69
Neurosurgery
Yes 4 10 .70 0.75 0.31-1.78
No 42 69
Traumatic brain injury
Yes 4 11 .56 0.69 0.29-1.67
No 42 68
Severe sepsis at admission
Yes 10 4 .007 2.2 1.43-3.37
No 36 75
Severe CAP
Yes 5 10 .99 0.89 0.42-1.90
No 41 69
COPD exacerbation
Yes 4 5 .89 1.22 0.56-2.65
No 42 74
APACHE II z15
Yes 37 60 .72 1.18 0.65-2.15
No 9 19
SOFA z6
Yes 22 41 .79 0.90 0.56-1.42
No 24 38
MODS z9
Yes 13 12 .10 1.58 0.98-2.51
No 33 67
Multiple organ dysfunction
Yes 25 28 .06 1.6 1.02-2.56
No 21 51
Septic shock
Yes 19 19 .06 1.61 1.03-2.51
No 27 60
Previous antibiotics
Yes 40 42 b .0001 3.49 1.61-7.58
No 6 37
Previous use of ceftriaxone
Yes 19 12 .0023 2.1 1.39-3.26
No 27 67
Previous use of ciprofloxacin
Yes 16 8 .0017 2.2 1.48-3.39
No 30 71
Previous use of ampicillin-sulbactam
Yes 11 19 1 0.99 0.58-1.70
No 35 60
MV, mechanical ventilation.a Criteria by McCabe and Jackson.
J. Medina et al.22
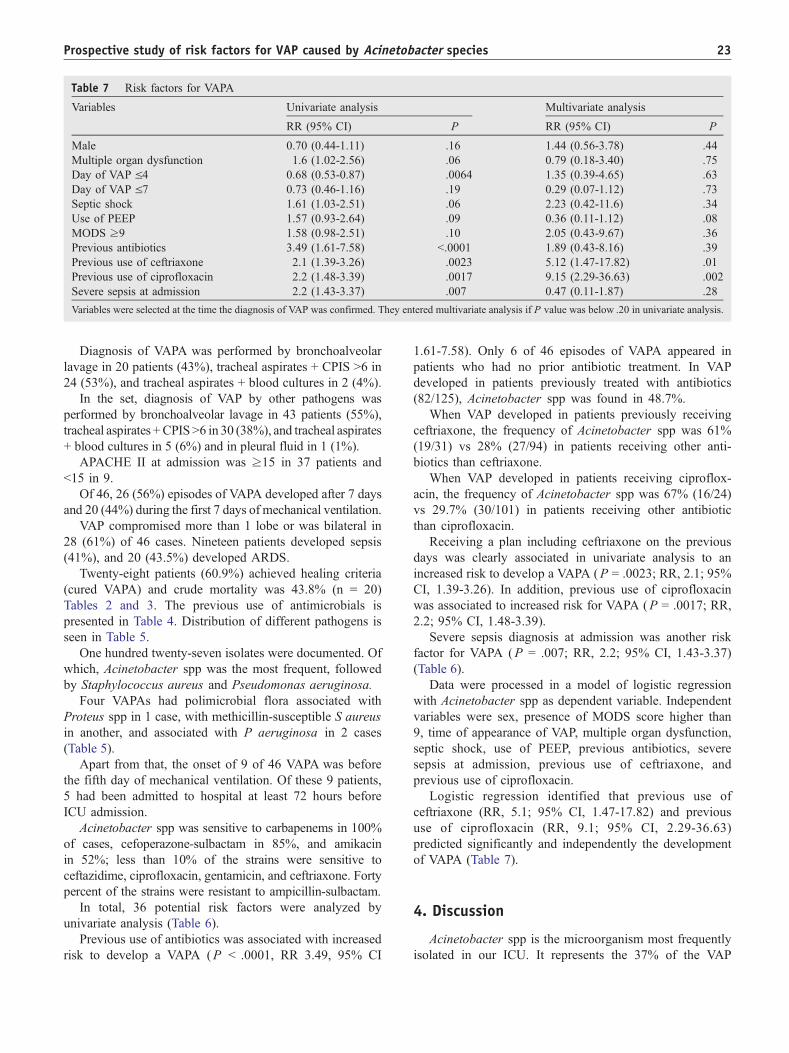
Table 7 Risk factors for VAPA
Variables Univariate analysis Multivariate analysis
RR (95% CI) P RR (95% CI) P
Male 0.70 (0.44-1.11) .16 1.44 (0.56-3.78) .44
Multiple organ dysfunction 1.6 (1.02-2.56) .06 0.79 (0.18-3.40) .75
Day of VAP V4 0.68 (0.53-0.87) .0064 1.35 (0.39-4.65) .63
Day of VAP V7 0.73 (0.46-1.16) .19 0.29 (0.07-1.12) .73
Septic shock 1.61 (1.03-2.51) .06 2.23 (0.42-11.6) .34
Use of PEEP 1.57 (0.93-2.64) .09 0.36 (0.11-1.12) .08
MODS z9 1.58 (0.98-2.51) .10 2.05 (0.43-9.67) .36
Previous antibiotics 3.49 (1.61-7.58) b.0001 1.89 (0.43-8.16) .39
Previous use of ceftriaxone 2.1 (1.39-3.26) .0023 5.12 (1.47-17.82) .01
Previous use of ciprofloxacin 2.2 (1.48-3.39) .0017 9.15 (2.29-36.63) .002
Severe sepsis at admission 2.2 (1.43-3.37) .007 0.47 (0.11-1.87) .28
Variables were selected at the time the diagnosis of VAP was confirmed. They entered multivariate analysis if P value was below .20 in univariate analysis.
Prospective study of risk factors for VAP caused by Acinetobacter species 23
Diagnosis of VAPA was performed by bronchoalveolar
lavage in 20 patients (43%), tracheal aspirates + CPIS N6 in
24 (53%), and tracheal aspirates + blood cultures in 2 (4%).
In the set, diagnosis of VAP by other pathogens was
performed by bronchoalveolar lavage in 43 patients (55%),
tracheal aspirates +CPISN6 in 30 (38%), and tracheal aspirates
+ blood cultures in 5 (6%) and in pleural fluid in 1 (1%).
APACHE II at admission was z15 in 37 patients and
b15 in 9.
Of 46, 26 (56%) episodes of VAPA developed after 7 days
and 20 (44%) during the first 7 days of mechanical ventilation.
VAP compromised more than 1 lobe or was bilateral in
28 (61%) of 46 cases. Nineteen patients developed sepsis
(41%), and 20 (43.5%) developed ARDS.
Twenty-eight patients (60.9%) achieved healing criteria
(cured VAPA) and crude mortality was 43.8% (n = 20)
Tables 2 and 3. The previous use of antimicrobials is
presented in Table 4. Distribution of different pathogens is
seen in Table 5.
One hundred twenty-seven isolates were documented. Of
which, Acinetobacter spp was the most frequent, followed
by Staphylococcus aureus and Pseudomonas aeruginosa.
Four VAPAs had polimicrobial flora associated with
Proteus spp in 1 case, with methicillin-susceptible S aureus
in another, and associated with P aeruginosa in 2 cases
(Table 5).
Apart from that, the onset of 9 of 46 VAPA was before
the fifth day of mechanical ventilation. Of these 9 patients,
5 had been admitted to hospital at least 72 hours before
ICU admission.
Acinetobacter spp was sensitive to carbapenems in 100%
of cases, cefoperazone-sulbactam in 85%, and amikacin
in 52%; less than 10% of the strains were sensitive to
ceftazidime, ciprofloxacin, gentamicin, and ceftriaxone. Forty
percent of the strains were resistant to ampicillin-sulbactam.
In total, 36 potential risk factors were analyzed by
univariate analysis (Table 6).
Previous use of antibiotics was associated with increased
risk to develop a VAPA (P b .0001, RR 3.49, 95% CI
1.61-7.58). Only 6 of 46 episodes of VAPA appeared in
patients who had no prior antibiotic treatment. In VAP
developed in patients previously treated with antibiotics
(82/125), Acinetobacter spp was found in 48.7%.
When VAP developed in patients previously receiving
ceftriaxone, the frequency of Acinetobacter spp was 61%
(19/31) vs 28% (27/94) in patients receiving other anti-
biotics than ceftriaxone.
When VAP developed in patients receiving ciproflox-
acin, the frequency of Acinetobacter spp was 67% (16/24)
vs 29.7% (30/101) in patients receiving other antibiotic
than ciprofloxacin.
Receiving a plan including ceftriaxone on the previous
days was clearly associated in univariate analysis to an
increased risk to develop a VAPA (P = .0023; RR, 2.1; 95%
CI, 1.39-3.26). In addition, previous use of ciprofloxacin
was associated to increased risk for VAPA (P = .0017; RR,
2.2; 95% CI, 1.48-3.39).
Severe sepsis diagnosis at admission was another risk
factor for VAPA (P = .007; RR, 2.2; 95% CI, 1.43-3.37)
(Table 6).
Data were processed in a model of logistic regression
with Acinetobacter spp as dependent variable. Independent
variables were sex, presence of MODS score higher than
9, time of appearance of VAP, multiple organ dysfunction,
septic shock, use of PEEP, previous antibiotics, severe
sepsis at admission, previous use of ceftriaxone, and
previous use of ciprofloxacin.
Logistic regression identified that previous use of
ceftriaxone (RR, 5.1; 95% CI, 1.47-17.82) and previous
use of ciprofloxacin (RR, 9.1; 95% CI, 2.29-36.63)
predicted significantly and independently the development
of VAPA (Table 7).
4. Discussion
Acinetobacter spp is the microorganism most frequently
isolated in our ICU. It represents the 37% of the VAP

J. Medina et al.24
episodes, with similar incidence in both ICU. This problem
is also seen in many South American countries where the
VAPA represents the 14% to 29% of the total VAP [32,33].
The most important findings of this prospective, obser-
vational study are identification of previous use of
ceftriaxone and ciprofloxacin as independent risk factors
for VAPA. It is noteworthy that our population (n = 46) is
bigger than other published series [1-4,34].
VAPA is important because of added morbidity and
mortality; it is also associated with increasing incidence and
resistance, forcing the use of broad-spectrum antibiotics that
generate selection pressure favoring development of new
multiresistant pathogens, which is a major problem in
infection control [6-9,35].
Different authors have documented the impact of
previous antimicrobial agents in the development of VAPA.
Lortholary et al [4] found that 75% patients colonized or
infected by Acinetobacter spp had received antibiotics
previously, whereas in our population the relationship was
40/46 (86.9%).
Fagon et al [12] found that the frequency of VAP due to
species of Pseudomonas and Acinetobacter spp was higher
in patients with previous antibiotic therapy (65% vs 19%).
The antibiotics related to higher risk differed; in a
retrospective study of 15 episodes of VAP by Acinetobacter
baumannii in mechanical ventilation for at least a week,
univariate analysis found that the previous use of ceftazi-
dime was a risk factor for VAP [3]. This was not found in
our study. The infrequent use of ceftazidime in our ICU was
the difference between the 2 studies.
Similar to the findings of Villers et al [13], we found that
the previous use of fluorquinolones (in our case, ciproflox-
acin) was associated with an increased risk of developing
VAPA. These authors recommend caution in the use of
fluorquinolones and that its use should be discontinued in
units with high resistance to this antibiotic and with high
prevalence of nonfermentative Gram-negative bacilli, as is
the case of the 2 ICUs analyzed in this article.
Trouillet et al [34] found that the previous use of broad-
spectrum antibiotics (including third-generation cephalospo-
rin, fluoroquinolone, and carbapenem) was an independent
risk factor for VAP caused by potentially resistant bacteria.
The resistant bacteria most frequently isolated in this study
were P aeruginosa and methicillin-resistant S aureus.
Contrary to the findings of Lortholary et al [4], previous
infection and severity of illness were not statistically
significant risk factors in our population. Other authors
have identified other risk factors different from the previous
use of antibiotics for VAPA. Baraibar et al [1] found, in a
logistic regression analysis of 12 VAP by A baumannii, that
head trauma, ARDS, neurosurgery, and large-volume
pulmonary aspiration were independent risk factors for
VAP by this microorganism.
This work analyzed VAP in ICUs both in Europe and
Uruguay. In our work, these risk factors were not found, but
the populations analyzed are not comparable because
Baraibar et al [1] had higher number of patients with
myocardial infarction, severe trauma, and severe head
injuries, whereas our population had more patients with
severe sepsis, postoperative abdominal surgery, and non-
traumatic acute brain injury. We included patients from
2 different ICUs because in 1, there were no neurosurgical
patients that are a known risk factor.
Akca et al [2] analyzed 9 pneumonias by Acinetobacter
spp, identifying pulmonary aspiration and a GCS of 9 or
lower as risk factors, which were not found in this work.
Comorbidity, general characteristics of the population,
severity scores, diagnosis at admission, nor interventions
such as PEEP, reintubation, use of anti-H2, and nasogastric
tubes were not associated with increased risk of infection by
this pathogen.
Forty-three percent of VAPA developed before day 7 of
mechanical ventilation, explaining why, in endemic situa-
tion, this pathogen quickly colonizes and infects the
patients. Critically ill patients are the reservoir of multi-
resistant microorganisms, and the documented infection is
only the tip of the iceberg of the relation between
colonization infections. Therefore, emphasis should be
placed in trying to decrease selective pressure by ceftriaxone
and ciprofloxacin.
To decrease the increasing incidence of Acinetobacter
spp, restriction or rotation with similar molecules policies
for this antimicrobial agents should be applied. This has
shown benefit in decreasing incidence of VAP [36,37].
Of nineteen patients, 8 had received ceftriaxone and had
a severe CAP either as severe respiratory sepsis. Therefore,
emphasis should be placed in reevaluation of the empirical
use of ceftriaxone for CAP in the ICU. Alternative plans of
restriction and or rotation with aminopenicillins plus
b-lactam antibiotics could be proposed.
The acquisition and dissemination of Acinetobacter spp
varies in each ICU, depending on multiple factors, as
mentioned above.
This leads us to hypothesize that risk factors for VAPA
are characteristic of each ICU, and thus, each ICU must
know their own ecology and also those specific risk factors
for the acquisition of VAPA. The growth of a subpopulation
of microorganisms in previously colonized patients could be
favored by previous use of some antimicrobial agents and
produce infection [38].
Especially, ceftriaxone and ciprofloxacin have high
digestive elimination, approximately 40% to 50% for both,
and this could favor digestive colonization and ulterior
development of VAPA via an endogenous mechanism.
Future studies are needed to confirm this hypothesis.
According to our study, the 3 antibiotics most frequently
prescribed were ceftriaxone, ciprofloxacin, and ampicillin-
sulbactam. The different use of antibiotics in each ICU
could determine different risk factors.
Furthermore, because Acinetobacter spp is an endemic
pathogen in Uruguay and the rest of Latin America, this
could determine different risk factors.
Prospective study of risk factors for VAP caused by Acinetobacter species 25
We suggest that restriction of these antibiotics accompa-
nied by rotation with other molecules of similar spectrum is
a valid strategy of infection control and, thus, decrease the
incidence of VAPA. Each ICU should know its own specific
risk factors for acquiring VAPA.
Limitations of the present study are that we have done
the typification of genus but not the species identification,
and no molecular typification was performed.
We also ignore if during this period, there was an
outbreak of a monoclonal strain in units having Acineto-
bacter spp as an endemic agent, and thus, other risk factors
different from the ones analyzed could not be found. We
emphasize that our population consists of 46 prospectively
collected VAPA, which represents a high number of cases,
and that a strict methodology was used for the diagnosis of
VAP. This gives us a high clinical significance to the risk
factors found in our study.
5. Conclusions
In summary, previous use of ceftriaxone and ciproflox-
acin are independent risk factors for the development
of VAPA.
Acknowledgments
The authors thank Alejandro Arroliga MD, FCCS, for his
exhaustive revision of the manuscript and his suggestions,
and Stella M. Calvo, MD, and Graciela Perez, MD, for
translating and designing this manuscript.
References
[1] Baraibar J, Correa H, Mariscal D, et al. Risk factors for infection by
Acinetobacter baumannii in intubated patients with nosocomial
pneumonia. Chest 1997;112:1050-4.
[2] Akca O, Koltka K, Usel S, et al. Risk factors for early-onset,
ventilator-associated pneumonia in critical care patients: selected
multiresistant versus nonresistant bacteria. Anesthesiology 2000;
93(3):638-45.
[3] Husni R, Goldstein L, Arroliga A, et al. Risk factors for an outbreak of
multi-drug-resistant acinetobacter nosocomial pneumonia among
intubated patients. Chest 1999;115:1378-82.
[4] Lortholary O, Fagon JY, Hoi AB, et al. Nosocomial acquisition of
multiresistant Acinetobacter baumannii: risk factors and prognosis.
Clin Infect Dis 1995;20(4):790 -6.
[5] Garnacho J, Sole-Violan J, Sa-Borges M, et al. Clinical impact of
pneumonia caused by Acinetobacter baumannii in intubated patients:
a matched cohort study. Crit Care Med 2003;31(10):2478-82.
[6] Fagon JY, Chastre J, Hance AJ, et al. Nosocomial pneumonia in
ventilated patients: a cohort study evaluating attributable mortality and
hospital stay. Am J Med 1993;94(3):281 -8.
[7] Koprnova J, Svetlansky I, Babel’a R, et al. Prospective study of
antibacterial susceptibility, risk factors and outcome of 157 episodes
of Acinetobacter baumannii bacteremia in 1999 in Slovakia. Scand J
Infect Dis 2001;33(12):891-5.
[8] Kollef MH, Fraser VJ. Antibiotic resistance in the intensive care unit.
Ann Intern Med 2001;134(4):298 -314.
[9] Landman D, Quale JM, Mayorga D, et al. Citywide clonal outbreak of
multiresistant Acinetobacter baumannii and Pseudomonas aeruginosa
in Brooklyn, NY: the preantibiotic era has returned. Arch Intern Med
2002;162(13):1515-20.
[10] Bergogne-Berezin E, Townern KJ. Acinetobacter spp. As nosocomial
pathogens: microbiological, clinical, and epidemiological features.
Clin Microbiol Rev 1996;9:148 -65.
[11] Arnow P, Flaherty JP. Nonfermentative gram-negative bacilli. In:
Mayhall CG, editor. Hospital epidemiology and infection control. 2nd
ed. Philadelphia7 Lippincott Williams & Wilkins; 1999. p. 431-51.
[12] Fagon JY, Chastre J, Domart Y, et al. Nosocomial pneumonia in patients
receiving continuous mechanical ventilation: prospective analysis of
52 episodes with use of protected specimen brush and quantitative
culture techniques. Am Rev Respir Dis 1989;139:877-84.
[13] Villers D, Espaze E, Coste-Burel M, et al. Nosocomial Acinetobacter
baumannii infections: microbiological and clinical epidemiology. Ann
Intern Med 1998;129:182-9.
[14] Johanson WG, Pierce A, Sanford J, et al. Nosocomial respiratory
infections with gram negative bacilli: the significance of colonization
of the respiratory tract. Ann Intern Med 1972;77:701 -6.
[15] Pingleton SK, Fagon JY, Leeper Jr KV. Patient selection for clinical
investigation of ventilator-associated pneumonia: criteria for evaluat-
ing diagnostic techniques. Chest 1992;102:553S-6S.
[16] Ibrahim EH, Ward S, Sherman G, Schaiff R, Fraser VJ, Kollef MH.
Experience with a clinical guideline for the treatment of ventilator-
associated pneumonia. Crit Care Med 2001;29:1109-15.
[17] Flanagan P, Findlay G, Magee J, et al. The diagnosis of ventilator-
associated pneumonia using non-bronchoscopic, non-directed lung
lavages. Intensive Care Med 2000;26:20 -30.
[18] Montravers P, Fagon JY, Chastre J, Lecso M, Dombret MC, Trouillet
JL, et al. Follow-up protected specimen brushes to assess treatment
in nosocomial pneumonia. Am Rev Respir Dis 1993;147(1):38 -44.
[19] Bergmans D, Bonten M, Leeuw P, et al. Reproducibility of
quantitative cultures of endotracheal aspirates from mechanically
ventilated patients. J Clin Microbiol 1997;35:796-8.
[20] Bernard GR, Artigas A, Brigham KL, et al. The American-European
Consensus Conference on ARDS. Definitions, mechanisms, relevant
outcomes, and clinical trial coordination. Am J Respir Crit Care Med
1994;149(3 Pt 1):818-24.
[21] Bone RC, Balk RA, Cerra FB, et al. Definitions for sepsis and organ
failure and guidelines for the use of innovates therapies in sepsis. The
ACCP (An American College of Chest Physician), SCCM (Society of
Critical Care Medicine) Consensus conference committee. Chest
1992;101:1644-55.
[22] Ewig S, Ruiz M, Mensa J, et al. Severe community-acquired
pneumonia: assessment of severity criteria. Am J Respir Crit Care
Med 1998;158:1102-8.
[23] Dennesen P, van der Ven A, Kessels A, Ramsay G, Bonten M.
Resolution of infectious parameters after antimicrobial therapy in
patients with ventilator-associated pneumonia. Am J Respir Crit Care
Med 2001;163:1371 -5.
[24] Schreckenberger PC, Von Graevenitz PC. Acinetobacter, achomo-
bacter, Alcaligenes , Moraxella , methylobacterium, and other
nonfermentative gram negative rods. In: En Murray P, Baron E,
Pfaller M, Tenover F, Molken R, editors. Manual of clinical
microbiology. 7th ed. Washington (DC)7 American Society of
Microbiology; 1999. p. 539 - 60.
[25] National Committee for Clinical Laboratory Standards. Performance
Standards for Antimicrobial Susceptibility Testing. Eleventh informa-
tional Supplement NCCLS M 100 S 11 Wayne, Pa, 2001.
[26] Zwillich C, Pierson D, Creagh E, et al. Complications of assisted
ventilation. A prospective Study of 354 consecutive Episodes. Am J
Med 1974;57:161-70.
[27] McCabe W, Jackson G. Gram-negative bacteriemia. Arch Intern Med
1962;110:847-64.
[28] Knaus WA, Draper EA, Wagner DP, et al. APACHE II: a severity of
disease classification system. Crit Care Med 1985;13:818 -9.

J. Medina et al.26
[29] Marshall JC, Cook DJ, Christou NV, et al. Multiple organ dysfunction
score: a reliable descriptor of a complex clinical outcome. Crit Care
Med 1995;23:1638-52.
[30] Vincent JL, Moreno R, Takala J, et al. The SOFA (sepsis-related organ
failure assessment) score to describe organ dysfunction/failure.
Intensive Care Med 1996;22:707 -10.
[31] Mamdani M, Sykora K, Li P, Normand S, Streiner D, Austin P, et al.
Reader’s guide to critical appraisal of cohort studies: assessing
potential for confounding. BMJ 2005;330:960-2.
[32] Costa SF, Newbaer M, Santos CR, Basso M, Soares I, Levin AS.
Nosocomial pneumonıa: importante of recognition of etiologic agents
to define an apropiate inicial empirical therapy. Int J Antimicrob
Agents 2001;17(2):147-50.
[33] Santucci SG, Gobara S, Santos CR, Fontana C, Levin AS. Infections
in burn intensive care unit: experience of seven years. J Hosp Infect
2003;53(1):6 -13.
[34] Trouillet J-L, Chastre J, Vuagnat A, Joly-Guillou M-L, Combaux D,
Dombret M-C, et al. Ventilator-associated pneumonia caused by
potentially drug-resistant bacteria. Am J Respir Crit Care Med 1998;
157:531-9.
[35] Chastre J. Infections due to Acinetobacter baumannii in the ICU.
Semin Respir Crit Care Med(24):69 -77.
[36] Gruson D, Hilbert G, Vargas F, et al. Rotation and restricted use of
antibiotics in a medical intensive care unit. Am J Respir Crit Care Med
2000;162:837-43.
[37] Raymond D, Pelletier S, Crabtree T, et al. Impact of a rotating empiric
antibiotic schedule on infectious mortality in an intensive care unit.
Crit Care Med 2001;29:1101-8.
[38] Petri Jr W. Antimicrobial agents: penicillins, cephalosporins,
and other h-lactam antibiotics. In: Hardman JG, Limbird LE, Gilman
AG, editors. Goodman and Gilman’s the pharmacological basis of
therapeutics. 10th ed. New York7 McGraw-Hill; 2001. p. 1171-88.
antimicrobial treatment [16]. Most patients with pneumoniacaused by resistant bacterial strains have a history of
Commentary
Ventilator-associated pneumonia by multidrug-resistantbacteria: Pathogen-specific risks versuscare-related risks
biotics. However, they found out that antibiotic resistanceconsistently caused an increase in hospital stay [15,16].
Within the Gram-negative bacteria identified as patho-
gens causing ventilator-associated pneumonia (VAP), mul-
tidrug-resistant ones, especially Acinetobacter species,
present specific challenges for the caregivers in intensive
care units (ICUs). Acinetobacter species consist of strictly
aerobic, Gram-negative, oxidase-negative cocobasillary
organisms. The DNA/DNA hybridization studies have
revealed 25 genomic species of Acinetobacter, 17 of which
have been confirmed and 10 of which have been named [1].
In clinical practice, because most species cannot reliably be
separated by phenotypic testing, the genospecies 1 (Acine-
tobacter calcoaceticus), 2 (Acinetobacter baumannii), 3,
and 13 are grouped together under the name A baumannii-
calcoaceticus complex (ABC). The ABC is the source of
approximately 80% of Acinetobacter infections [2-4].
Traditionally, ABC was considered a low-virulence
microorganism given that most clinical isolates reflected
colonization rather than significant infection [5,6]. Howev-
er, recent experience suggests that members of ABC can
cause outbreaks of hospital-acquired infections (including
multifacility outbreaks) [7]. Although there is controversy in
the reported mortality attributed to ABC, it is associated
with an elevated crude mortality in a subset of high-risk
patients [8,9]. The unique characteristics of ABC, such as
diversity of reservoirs, tolerance to desiccation—hence
survival in hospital conditions—and the capacity to acquire
antimicrobial-resistant genes leading to multidrug resistance
are the reasons why it is an emerging cause of health care–
associated infections.
In this issue, Dr Medina and colleagues conducted
a prospective study to identify specific risk factors for
VAP caused by Acinetobacter species [10]. Similar to
previous studies [11-13], this study confirmed that the use
of broad-spectrum antibiotics—namely ceftriaxone and
ciprofloxacin—is associated with increased incidence of
Acinetobacter VAP by creating an environment favoring
multidrug-resistant pathogens.
Although intensivists have an increased awareness about
pneumonia induced by multidrug-resistant pathogens, in the
light of current evidence-based medicine, it is hard to con-
clude whether these pathogens play a definite role in in-
creasing morbidity or mortality. In addition, there is no clear
evidence that a more resistant bacterial strain is more
virulent than its susceptible counterpart. Therefore, the
outcome differences between the 2 strains [14,15] are often
suggested to relate to patient characteristics at baseline or at
time of infection onset and to the effect of empirical
antibiotic use and a longer time of hospitalization. In 2 large
series of severe Staphylococcus aureus and Pseudomonas
aeruginosa VAP outbreaks, Combes et al [16] showed that
antibiotic resistance did not significantly affect ICU
mortality of patients receiving appropriate initial anti-
Similarly, we found increased length of stay in the ICU, but
no difference in mortality with VAP as a result of multidrug-
resistant pathogens [17].
With the findings somewhat similar to previous studies,
the real importance of this study is that it raises awareness
about the severity of the patient’s status and the importance of
preventive measures instead of specific risks for resistant
pathogens as they relate to causes of VAP. Assessment of
severity of status, clinical suspicion and diagnosis of
pneumonia, appropriate empiric antibiotherapy, and deesca-
lation approach are the key elements in managing pneumonia
in the ICU. The management of VAP in the ICU requires
knowledge of when to start the antibiotic, the dose and
duration needed, and most importantly, institution-specific
empiric coverage [18]. Healthcare facilities are recommen-
ded to provide their own preventive pathways according to
their own epidemiological and surveillance data [19].
Another important issue is how to handle the endemic of
multidrug-resistant species in the ICU. Multidrug-resistant
pathogens including Acinetobacter species usually cause
pneumonia in the late phase (N5-7 days) and possibly in










![Pneumonia (Ventilator-associated [VAP] and non-ventilator](https://img.pdfslide.us/doc/110x75/61c3dfa934191a172140c0d5/pneumonia-ventilator-associated-vap-and-non-ventilator-.jpg)










![Ventilator Associated Pneumonia Treatment[1]](https://img.pdfslide.us/doc/110x75/577d23921a28ab4e1e9a2bfc/ventilator-associated-pneumonia-treatment1.jpg)