Embed Size (px)
Citation preview
Prospective Evaluation of Surgeon PhysicalExamination for Detection of Incisional Hernias
Rebeccah B Baucom, MD, William C Beck, MD, Michael D Holzman, MD, MPH, FACS,Kenneth W Sharp, MD, FACS, William H Nealon, MD, FACS, Benjamin K Poulose, MD, MPH, FACS
BACKGROUND: Surgeon physical examination is often used to monitor for hernia recurrence in clinical andresearch settings, despite a lack of information on its effectiveness. This study aims to comparesurgeon-reviewed CT with surgeon physical examination for the detection of incisional hernia.
STUDY DESIGN: General surgery patients with an earlier abdominal operation and a recent viewable CT scanof the abdomen and pelvis were enrolled prospectively. Patients with a stoma, fistula, or soft-tissue infection were excluded. Surgeon-reviewed CT was treated as the gold standard.Patients were stratified by body mass index into nonobese (body mass index <30) and obesegroups. Testing characteristics and real-world performance, including positive predictivevalue and negative predictive value, were calculated.
RESULTS: One hundred and eighty-one patients (mean age 54 years, 68% female) were enrolled. Herniaprevalence was 55%. Mean area of hernias was 44.6 cm2. Surgeon physical examination had alow sensitivity (77%) and negative predictive value (77%). This difference was more pro-nounced in obese patients, with sensitivity of 73% and negative predictive value 69%.
CONCLUSIONS: Surgeon physical examination is inferior to CT for detection of incisional hernia, and fails todetect approximately 23% of hernias. In obese patients, 31% of hernias are missed by surgeonphysical examination. This has important implications for clinical follow-up and design ofstudies evaluating hernia recurrence, as ascertainment of this result must be reliable andaccurate. (J Am Coll Surg 2014;218:363e366.� 2014 by the American College of Surgeons)
Currently, there exist no standardized criteria for thephysical or radiologic diagnosis of incisional hernia.One widely accepted definition formulated by the Euro-pean Hernia Society is, “any abdominal wall gap with orwithout a bulge in the area of a postoperative scar,palpable or perceptible by clinical examination or imag-ing.”1 Until the advent of high-quality CT, surgeon phys-ical examination (SPE) was the primary modality used fordiagnosis of incisional hernias. Traditionally, this clinicalexamination includes abdominal wall inspection andpalpation with the patient supine and standing, as wellas during Valsalva maneuvers. The examiner looks for abulge and, if a hernia is believed to be present, the exam-iner attempts to define the fascial edges. In cases where
Disclosure Information: Nothing to disclose.
Presented at the 99th Annual Clinical Congress, American College ofSurgeons, Surgical Forum, Washington, DC, October 2013.
Received October 4, 2013; Revised December 3, 2013; Accepted December8, 2013.From Vanderbilt University Medical Center, Nashville, TN.Correspondence address: Rebeccah B Baucom, MD, Vanderbilt UniversityMedical Center, 1161 Medical Center Dr, D-5203 Medical Center North,Nashville, TN 37232. email: [email protected]
363ª 2014 by the American College of Surgeons
Published by Elsevier Inc.
the fascial defect is small and/or the patient obese, herniascan be missed on physical examination.Within the past several years, CT has been increasingly
used to diagnose and characterize hernias, particularlythose that necessitate a complex operative repair. Usingthis imaging technique, one can determine the contentsof the hernia sac and the relationship of the hernia toother abdominal wall landmarks, such as bony structuresand the linea semilunaris. A few small studies fromGreece and Spain evaluating the use of CT as a follow-up after incisional hernia repair have found that CT hasa sensitivity of 100% and specificity of 97% for detectionof recurrence.2,3 However, due to the relatively high costand the exposure to ionizing radiation, CT is not widelyused in follow-up after hernia repair, particularly if thepatient is asymptomatic. Our group has previouslydemonstrated the use of ultrasound to detect incisionalhernia formation using dynamic abdominal sonographyfor hernia with results comparable with CT.4
Several experts have questioned the need to rely on anyadjunct imaging test to detect incisional hernia. Researchstudies have primarily relied on SPE for determination ofrecurrence after repair. However, in the few publishedstudies evaluating SPE for detection of hernia recurrence,
ISSN 1072-7515/13/$36.00
http://dx.doi.org/10.1016/j.jamcollsurg.2013.12.007
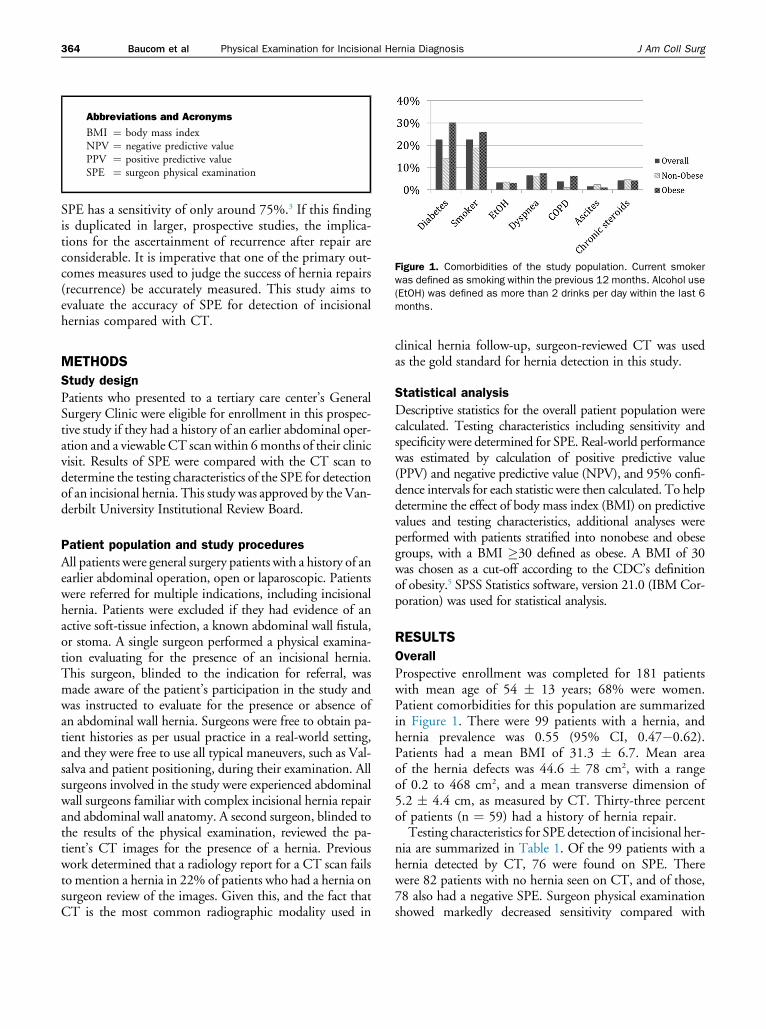
Figure 1. Comorbidities of the study population. Current smokerwas defined as smoking within the previous 12 months. Alcohol use(EtOH) was defined as more than 2 drinks per day within the last 6months.
Abbreviations and Acronyms
BMI ¼ body mass indexNPV ¼ negative predictive valuePPV ¼ positive predictive valueSPE ¼ surgeon physical examination
364 Baucom et al Physical Examination for Incisional Hernia Diagnosis J Am Coll Surg
SPE has a sensitivity of only around 75%.3 If this findingis duplicated in larger, prospective studies, the implica-tions for the ascertainment of recurrence after repair areconsiderable. It is imperative that one of the primary out-comes measures used to judge the success of hernia repairs(recurrence) be accurately measured. This study aims toevaluate the accuracy of SPE for detection of incisionalhernias compared with CT.
METHODS
Study design
Patients who presented to a tertiary care center’s GeneralSurgery Clinic were eligible for enrollment in this prospec-tive study if they had a history of an earlier abdominal oper-ation and a viewable CT scan within 6months of their clinicvisit. Results of SPE were compared with the CT scan todetermine the testing characteristics of the SPE for detectionof an incisional hernia. This study was approved by the Van-derbilt University Institutional Review Board.
Patient population and study procedures
All patients were general surgery patients with a history of anearlier abdominal operation, open or laparoscopic. Patientswere referred for multiple indications, including incisionalhernia. Patients were excluded if they had evidence of anactive soft-tissue infection, a known abdominal wall fistula,or stoma. A single surgeon performed a physical examina-tion evaluating for the presence of an incisional hernia.This surgeon, blinded to the indication for referral, wasmade aware of the patient’s participation in the study andwas instructed to evaluate for the presence or absence ofan abdominal wall hernia. Surgeons were free to obtain pa-tient histories as per usual practice in a real-world setting,and they were free to use all typical maneuvers, such as Val-salva and patient positioning, during their examination. Allsurgeons involved in the study were experienced abdominalwall surgeons familiar with complex incisional hernia repairand abdominal wall anatomy. A second surgeon, blinded tothe results of the physical examination, reviewed the pa-tient’s CT images for the presence of a hernia. Previouswork determined that a radiology report for a CT scan failsto mention a hernia in 22% of patients who had a hernia onsurgeon review of the images. Given this, and the fact thatCT is the most common radiographic modality used in
clinical hernia follow-up, surgeon-reviewed CT was usedas the gold standard for hernia detection in this study.
Statistical analysis
Descriptive statistics for the overall patient population werecalculated. Testing characteristics including sensitivity andspecificity were determined for SPE. Real-world performancewas estimated by calculation of positive predictive value(PPV) and negative predictive value (NPV), and 95% confi-dence intervals for each statistic were then calculated. To helpdetermine the effect of body mass index (BMI) on predictivevalues and testing characteristics, additional analyses wereperformed with patients stratified into nonobese and obesegroups, with a BMI �30 defined as obese. A BMI of 30was chosen as a cut-off according to the CDC’s definitionof obesity.5 SPSS Statistics software, version 21.0 (IBM Cor-poration) was used for statistical analysis.
RESULTS
Overall
Prospective enrollment was completed for 181 patientswith mean age of 54 � 13 years; 68% were women.Patient comorbidities for this population are summarizedin Figure 1. There were 99 patients with a hernia, andhernia prevalence was 0.55 (95% CI, 0.47�0.62).Patients had a mean BMI of 31.3 � 6.7. Mean areaof the hernia defects was 44.6 � 78 cm2, with a rangeof 0.2 to 468 cm2, and a mean transverse dimension of5.2 � 4.4 cm, as measured by CT. Thirty-three percentof patients (n ¼ 59) had a history of hernia repair.Testing characteristics for SPE detection of incisional her-
nia are summarized in Table 1. Of the 99 patients with ahernia detected by CT, 76 were found on SPE. Therewere 82 patients with no hernia seen on CT, and of those,78 also had a negative SPE. Surgeon physical examinationshowed markedly decreased sensitivity compared with
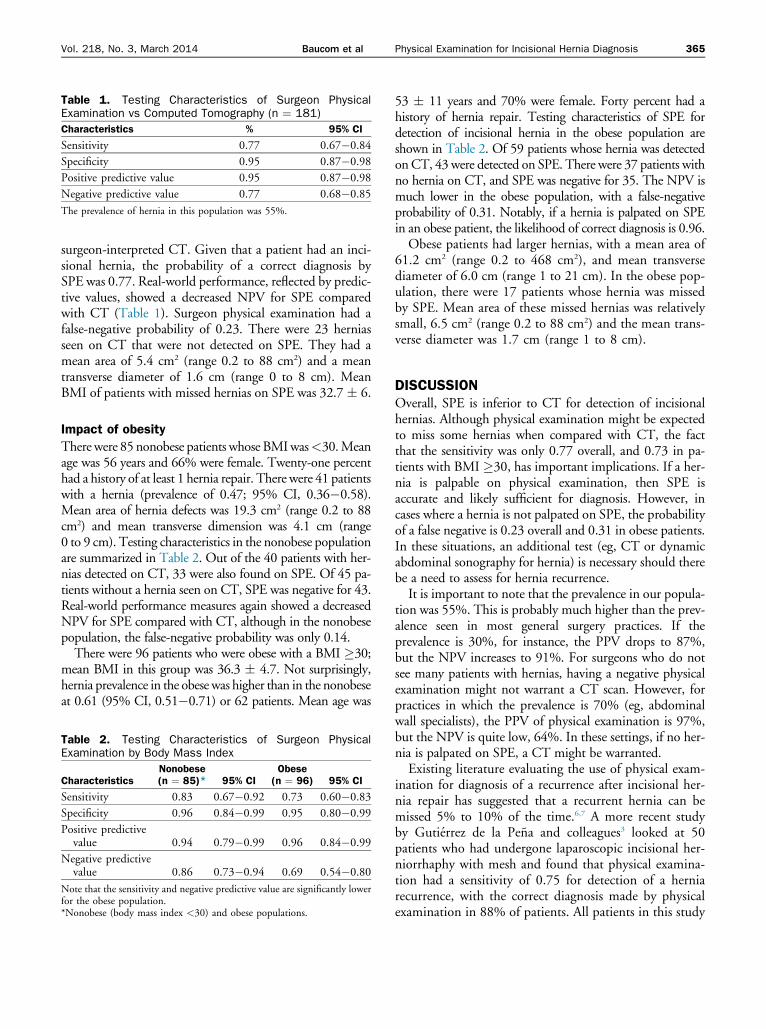
Table 1. Testing Characteristics of Surgeon PhysicalExamination vs Computed Tomography (n ¼ 181)
Characteristics % 95% CI
Sensitivity 0.77 0.67�0.84
Specificity 0.95 0.87�0.98
Positive predictive value 0.95 0.87�0.98
Negative predictive value 0.77 0.68�0.85
The prevalence of hernia in this population was 55%.
Vol. 218, No. 3, March 2014 Baucom et al Physical Examination for Incisional Hernia Diagnosis 365
surgeon-interpreted CT. Given that a patient had an inci-sional hernia, the probability of a correct diagnosis bySPE was 0.77. Real-world performance, reflected by predic-tive values, showed a decreased NPV for SPE comparedwith CT (Table 1). Surgeon physical examination had afalse-negative probability of 0.23. There were 23 herniasseen on CT that were not detected on SPE. They had amean area of 5.4 cm2 (range 0.2 to 88 cm2) and a meantransverse diameter of 1.6 cm (range 0 to 8 cm). MeanBMI of patients with missed hernias on SPE was 32.7 � 6.
Impact of obesity
Therewere 85 nonobese patients whose BMIwas<30.Meanage was 56 years and 66% were female. Twenty-one percenthad a history of at least 1 hernia repair. There were 41 patientswith a hernia (prevalence of 0.47; 95% CI, 0.36�0.58).Mean area of hernia defects was 19.3 cm2 (range 0.2 to 88cm2) and mean transverse dimension was 4.1 cm (range0 to 9 cm). Testing characteristics in the nonobese populationare summarized in Table 2. Out of the 40 patients with her-nias detected on CT, 33 were also found on SPE. Of 45 pa-tients without a hernia seen on CT, SPE was negative for 43.Real-world performance measures again showed a decreasedNPV for SPE compared with CT, although in the nonobesepopulation, the false-negative probability was only 0.14.There were 96 patients who were obese with a BMI �30;
mean BMI in this group was 36.3 � 4.7. Not surprisingly,hernia prevalence in the obese was higher than in the nonobeseat 0.61 (95% CI, 0.51�0.71) or 62 patients. Mean age was
Table 2. Testing Characteristics of Surgeon PhysicalExamination by Body Mass Index
CharacteristicsNonobese(n ¼ 85)* 95% CI
Obese(n ¼ 96) 95% CI
Sensitivity 0.83 0.67�0.92 0.73 0.60�0.83
Specificity 0.96 0.84�0.99 0.95 0.80�0.99
Positive predictivevalue 0.94 0.79�0.99 0.96 0.84�0.99
Negative predictivevalue 0.86 0.73�0.94 0.69 0.54�0.80
Note that the sensitivity and negative predictive value are significantly lowerfor the obese population.*Nonobese (body mass index <30) and obese populations.
53 � 11 years and 70% were female. Forty percent had ahistory of hernia repair. Testing characteristics of SPE fordetection of incisional hernia in the obese population areshown in Table 2. Of 59 patients whose hernia was detectedonCT, 43 were detected on SPE. There were 37 patients withno hernia on CT, and SPE was negative for 35. The NPV ismuch lower in the obese population, with a false-negativeprobability of 0.31. Notably, if a hernia is palpated on SPEin an obese patient, the likelihood of correct diagnosis is 0.96.Obese patients had larger hernias, with a mean area of
61.2 cm2 (range 0.2 to 468 cm2), and mean transversediameter of 6.0 cm (range 1 to 21 cm). In the obese pop-ulation, there were 17 patients whose hernia was missedby SPE. Mean area of these missed hernias was relativelysmall, 6.5 cm2 (range 0.2 to 88 cm2) and the mean trans-verse diameter was 1.7 cm (range 1 to 8 cm).
DISCUSSIONOverall, SPE is inferior to CT for detection of incisionalhernias. Although physical examination might be expectedto miss some hernias when compared with CT, the factthat the sensitivity was only 0.77 overall, and 0.73 in pa-tients with BMI �30, has important implications. If a her-nia is palpable on physical examination, then SPE isaccurate and likely sufficient for diagnosis. However, incases where a hernia is not palpated on SPE, the probabilityof a false negative is 0.23 overall and 0.31 in obese patients.In these situations, an additional test (eg, CT or dynamicabdominal sonography for hernia) is necessary should therebe a need to assess for hernia recurrence.It is important to note that the prevalence in our popula-
tion was 55%. This is probably much higher than the prev-alence seen in most general surgery practices. If theprevalence is 30%, for instance, the PPV drops to 87%,but the NPV increases to 91%. For surgeons who do notsee many patients with hernias, having a negative physicalexamination might not warrant a CT scan. However, forpractices in which the prevalence is 70% (eg, abdominalwall specialists), the PPV of physical examination is 97%,but the NPV is quite low, 64%. In these settings, if no her-nia is palpated on SPE, a CT might be warranted.Existing literature evaluating the use of physical exam-
ination for diagnosis of a recurrence after incisional her-nia repair has suggested that a recurrent hernia can bemissed 5% to 10% of the time.6,7 A more recent studyby Gutierrez de la Pena and colleagues3 looked at 50patients who had undergone laparoscopic incisional her-niorrhaphy with mesh and found that physical examina-tion had a sensitivity of 0.75 for detection of a herniarecurrence, with the correct diagnosis made by physicalexamination in 88% of patients. All patients in this study

366 Baucom et al Physical Examination for Incisional Hernia Diagnosis J Am Coll Surg
underwent diagnostic laparoscopy as the gold standard.Authors concluded that CT should be performed aspart of the regular postoperative assessment of symptom-atic patients after hernia repair, citing obesity and fibrosisfrom mesh implantation as substantial contributors to thecomplexity of the physical examination.The findings of our larger, prospective study confirm
the relatively low sensitivity of SPE for detection of inci-sional hernias. In particular, SPE most often failed todetect small hernias in large patients. Although Gutierrezde la Pena and colleagues did not specifically analyze theirresults in obese patients, our findings also reveal thatobesity contributes to the difficulty of diagnosis withSPE. Interestingly, we found comparable size estimationof the mean hernia for CT and SPE (CT mean transversedimension 6.2 � 3.1 cm and SPE mean transversedimension 6.0 cm � 3.5 cm). However, only 18 patientshad complete information for SPE estimated size.The findings of this study are important clinically for
several reasons. First, the rate of obesity in the UnitedStates continues to increase, so physical examination willmiss an increasing number of incisional hernias. Althoughthese hernias might be relatively small, they are not insig-nificant. As surgeons, we have a responsibility to counselpatients about the risks of hernia incarceration and stran-gulation, particularly in the increasingly complex medico-legal environment. Although data are conflicting, somereports suggest that smaller hernias pose a greater risk ofstrangulation once incarcerated.8 In addition, herniastend to increase in size over time. If a patient is a candidatefor hernia repair, the potential for improving value in man-agement and decreased patient morbidity by performing arepair when the hernia is small could be substantial.These findings also have implications for research.
When evaluating new and existing therapies for herniarepair, it is imperative that hernia recurrence be accuratelyassessed. If the outcomes of interest cannot be measuredwith certainty, how can the therapy be deemed effectiveor ineffective? If SPE is used as a stand-alone measure-ment for detection of hernia recurrence, 31% of herniasmight go undetected. This number will be even higherif the prevalence of hernia in that population is >55%.If a hernia is palpable on SPE, then no follow-up studyis needed for confirmation because the sensitivity andPPV of SPE are >95%. In those cases where the SPE isnegative, additional investigation is necessary to accu-rately determine whether a recurrence is present.This study is not without limitations. The results are
representative of a group of patients at a single institution,which can introduce referral bias. Multiple surgeons per-formed the physical examinations, which means that theremight have been some differences in evaluation for the
presence of a hernia. However, all of the surgeons involvedare experienced with evaluation and repair of complexabdominal wall hernias and abdominal wall anatomy,and attempts were made to standardize the study proce-dures. Lastly, it is not known whether these results aregeneralizable to the population of patients with primaryventral hernias (ie, epigastric or umbilical hernias). Thestudy population included patients who had undergoneprevious surgery and had a visible scar. This, and the factthat primary umbilical hernias tend to be quite small, sug-gest that SPE in primary abdominal wall hernias might beeven less sensitive, but this is unknown.
CONCLUSIONSSurgeon physical examination is inferior to CT for detec-tion of incisional hernias, with particularly low sensitivityand high false-negative probability. In the increasinglyobese population of surgery patients, a more sensitivemodality for hernia detection should be used if the SPEis negative and concern exists for hernia recurrence.
Author Contributions
Study conception and design: Holzman, Sharp, Nealon,Poulose
Acquisition of data: Beck,Holzman, Sharp,Nealon, PouloseAnalysis and interpretation of data: Baucom, Sharp,NealonDrafting of manuscript: Baucom, PouloseCritical revision: Baucom, Poulose
REFERENCES
1. Muysoms FE, Miserez M, Berrevoet F, et al. Classification ofprimary and incisional abdominal wall hernias. Hernia 2009;13:407e414.
2. Gossios K, Zikou A, Vazakas P, et al. Value of CT after laparo-scopic repair of postsurgical ventral hernia. Abdom Imaging2003;28:99e102.
3. Gutierrez de la Pena C, Vargas Romero J, Dieguez Garcıa JA.The value of CT diagnosis of hernia recurrence after prostheticrepair of ventral incisional hernias. Eur Radiol 2001;11:1161e1164.
4. Beck WC, Holzman MD, Sharp KW, et al. Comparative effec-tiveness of dynamic abdominal sonography for hernia vscomputed tomography in the diagnosis of incisional hernia.J Am Coll Surg 2013;216:447e453.
5. Centers for Disease Control and Prevention. Overweight andObesity. Atlanta, GA: Centers for Disease Control and Preven-tion; 2012.
6. Miller PA, Mezwa DG, Feczko PJ, et al. Imaging of abdominalhernias. Radiographics 1995;15:333e347.
7. Ghahremani GG, Jimenez MA, Rosenfeld M, Rochester D. CTdiagnosis of occult incisional hernias. AJR Am J Roentgenol1987;148:139e142.
8. Bloemen A, van Dooren P, Huizinga BF, Hoofwijk AG. Com-parison of ultrasonography and physical examination in thediagnosis of incisional hernia in a prospective study. Hernia2012;16:53e57.