Embed Size (px)
Citation preview

Prospective Comparison of Catheter-BasedEndoscopic Sonography versus StandardEndoscopic Sonography: Evaluation ofGastrointestinal-Wall Abnormalities andStaging of Gastrointestinal Malignancies
Johannes Koch, MD,1,2 Robert A. Halvorsen, Jr., MD,2 Scott D. Levenson, MD,1 John P. Cello, MD1
1 Division of Gastroenterology, Hepatology, and Clinical Nutrition, Department of Medicine, San FranciscoGeneral Hospital, University of California, San Francisco, 1001 Potrero Avenue, San Francisco, California 941102 Department of Radiology, San Francisco General Hospital, University of California, San Francisco, 1001Potrero Avenue, San Francisco, California 94110
Received 2 June 2000; accepted 9 October 2000
ABSTRACT: Purpose. Endoscopic sonography (EUS)is an important imaging modality for evaluating be-nign and malignant luminal gastrointestinal-tract ab-normalities. The objectives of this study were toevaluate the feasibility of catheter-based EUS (C-EUS)during standard upper and lower endoscopy in pa-tients with malignancies and other abnormalities ofthe gastrointestinal-tract lumen, to assess the imagequality obtained with the 12.5-MHz catheter-based ul-trasound transducer, and to prospectively comparethe interpretations of C-EUS images with those of thestandard EUS (S-EUS) images.
Methods. One hundred thirty-seven consecutivepatients referred for EUS were evaluated with C-EUSfollowed by S-EUS. The patients were assigned to 1 of2 groups: group A, patients with intramural masses orintestinal wall thickening, with biopsies negative formalignancy; and group B, patients with esophageal,gastric, duodenal, or rectal cancer referred for staging.
The results of C-EUS and S-EUS were compared foreach group.
Results. C-EUS was completed in 134 patients: 81patients with 83 lesions in group A and 53 patients ingroup B. For group A, C-EUS image interpretationconcurred with that of S-EUS in 74 (89%) of 83 lesions.For group B, C-EUS concurred with S-EUS for tumordepth (T) and nodal (N) classifications in 19 cases(36%) and 26 cases (49%), respectively. The depth ofinvasion was underestimated by C-EUS in all 34 casesin which the T classifications by C-EUS and S-EUSwere discordant. In 1 of 6 patients with stenotic cancerthat was nontraversable by S-EUS, C-EUS identifiedlymphadenopathy (incorrectly classified as N0 by S-EUS).
Conclusions. C-EUS was easily performed, and theC-EUS images were comparable to the S-EUS imagesin assessing mucosal and intramural lesions. Thelimited depth of penetration of the catheter-basedtransducer resulted in understaging the extent oftumor invasion and underestimating the nodalspread. © 2001 John Wiley & Sons, Inc. J Clin Ultra-sound 29:117–124, 2001.
Keywords: endoscopic ultrasonograph; ultrasonogra-phy; instrumentation methods; comparative study;gastrointestinal malignancy
Endoscopic sonography (EUS) has emerged asan important imaging modality for the evalu-
ation of luminal gastrointestinal-tract abnormali-ties. High-frequency (5–12.5-MHz) ultrasound
Correspondence to: J. Koch, San Francisco General Hospital,NH-3D-5, 1001 Potrero Avenue, San Francisco, Califor-nia 94110Grant sponsor: National Institutes of Health (to J. K. andS. L.)Grant number: NRSA T32 DK07007Presented in part at the annual meeting of the American So-ciety for Gastrointestinal Endoscopy, New Orleans, Louisiana,May 1994 (abstract published in Gastrointestinal Endoscopy1994;40:A207 and Gastrointestinal Endoscopy 1994;40:A208),and at the World Congress of Gastroenterology, Los Angeles,California, October 1994
© 2001 John Wiley & Sons, Inc.
VOL. 29, NO. 3, MARCH/APRIL 2001 117

transducers incorporated into the tips of endo-scopes can provide detailed images of benign andmalignant disorders. EUS depicts the discrete5-layered structure of the gastrointestinal wall.1
The high-resolution EUS images can provide im-portant information for determining therapy inpatients with mucosal and intramural abnormali-ties of unclear etiology, such as abnormal gastricrugae, intramural masses, strictures, and surgi-cal anastomoses. EUS is also known to providereliable staging of the tumor depth (T classifica-tion) and nodal involvement (N classification) ofgastrointestinal malignancies.
EUS is routinely preceded by “forward view-ing” endoscopy to determine the exact sizeand location of the lesion. EUS is then performedwith a dedicated ultrasound endoscope. Themost widely employed ultrasound endoscopes(GF-UM20 or earlier series, Olympus Corpora-tion, Melville, NY) have an outer diameter ofnearly 13 mm; a long, rigid distal tip; and obliqueviewing fiberoptics. These echoendoscopes aremore cumbersome than and often not as well tol-erated by patients as are forward-viewing endo-scopes.
Technologic advances have led to the miniatur-ization of ultrasound transducers.2,3 Transducershoused inside small catheters, developed for in-travascular imaging, have been used for transna-sal evaluation of the esophagus4 and “through-the-scope” imaging of a wide variety of gastro-intestinal lesions.5–11 Catheter-based EUS(C-EUS), which can be done during the forward-viewing endoscopy, addresses the limitations ofstandard EUS (S-EUS) by eliminating the needfor the echoendoscopy, with its associated risks,discomfort, and cost, and by permitting imagingof stenotic lesions that cannot be traversed by anechoendoscope. However, the accuracy of C-EUShas not been compared to that of S-EUS for be-nign lesions of the gastrointestinal tract. Studiesof C-EUS in esophageal cancer,12–14 ampullar tu-mors,15 and colonic cancer16 have yielded contra-dictory results.
The objectives of our study were to evaluate thefeasibility of C-EUS during standard upper andlower endoscopy in patients with malignanciesand other abnormalities of the gastrointestinal-tract lumen, to assess the image quality obtainedwith the 12.5-MHz catheter-based ultrasoundtransducer, and to compare the interpretations ofthe C-EUS images with those of the S-EUS im-ages in a prospective manner.
PATIENTS AND METHODS
From March 1, 1993, until August 1, 1996, 137consecutive patients referred for EUS of theesophagus, stomach, duodenum, and/or rectumparticipated in the study. Patients were assignedto 1 of 2 groups. Group A consisted of patientswith intramural (or submucosal) masses or intes-tinal-wall thickening, with endoscopic biopsiesnegative for malignancy. Group B consisted of pa-tients with a known esophageal, gastric, duode-nal, or rectal malignancy referred for staging.C-EUS and S-EUS were performed, and the re-sults were compared for each patient group. Allpatients provided written informed consent priorto the procedures, and the study was approved bythe Committee on Human Research at the Uni-versity of California, San Francisco.
Each patient underwent either routine endos-copy with conscious sedation or nonsedated sig-moidoscopy to evaluate and localize the lesion.During the endoscopic examination of gastric,duodenal, and rectal lesions, 100–500 ml of salinewas instilled into the intestinal lumen to providean acoustic interface covering the lesion. TheC-EUS transducer was passed through the biopsychannel of the endoscope; sonography was per-formed, and the findings were interpreted. Imme-diately following the endoscopy and C-EUS, thesame physician performed the S-EUS examina-tion. The sonographic procedures and interpreta-tions were all performed by the same investigator(J. K.).
The endoscope-based systems for S-EUS werethe GF-UM3 and GF-UM20 (Olympus) andthe FG 32UA (Pentax Precision Instruments,Orangeburg, NY). S-EUS was performed using a7.5-MHz transducer. The Intravascular Ultra-sound imaging system (Diasonics, Milpitas, CA)was used for C-EUS. C-EUS utilized 220-cm long,6.2-French catheters containing 12.5-MHz trans-ducers (Microvasive, Endosound; Boston Scien-tific, Natick, MA). The transducer was attached toa mechanically rotated 1.3-mm core, providing360° images with an axial resolution of 0.1 mmand a depth of penetration of about 2 cm. All in-struments were decontaminated and disinfectedusing standard hospital procedures for endoscopicequipment between applications.
RESULTS
During the study period, 137 patients were eli-gible and gave written informed consent; 2 pa-tients were excluded owing to probe malfunction2
KOCH ET AL
118 JOURNAL OF CLINICAL ULTRASOUND

and 1 because a complete S-EUS examinationcould not be performed.1 In 134 patients, imagingwas completed with both C-EUS and S-EUS.There were 88 men and 46 women, with a meanage ± standard deviation of 58 ± 15.1 years. Ingroup A, there were 81 patients with 83 lesions (2patients with 2 distinct lesions); in group B, therewere 53 patients with gastrointestinal malignan-cies (Table 1). Twenty-seven patients were exam-ined with the GF-UM3, 101 patients with the GF-UM20, and 6 patients with the Pentax FG-32UA.
C-EUS added 5–15 minutes to the time re-quired for the endoscopic procedure. The cath-eters were easily passed through the workingchannels of the endoscopes. The appearance ofthe intestinal-wall layers on C-EUS was similarto that on S-EUS. The images obtained within 2cm of the transducer on C-EUS were comparableto the S-EUS images. C-EUS required endoscopi-cally guided positioning of the catheter in prox-imity to the lesion. The C-EUS image quality de-teriorated when the C-EUS transducer wasfarther than 2 cm from the area of interest orthe probe was in direct contact with the intestinalwall. The first 3 intestinal-wall layers were ill-defined or obscured if the catheter was placedonto the mucosa. In contrast, excellent imageswere obtained during S-EUS with the transducerseveral centimeters away from the lesion.
In group A, the diagnostic impression by C-EUS concurred with that by S-EUS in 74 [89%;95% confidence interval (CI), 80–95%] of 83 mu-cosal and intramural lesions (Table 2). There wasan 84% concordance (Figure 1) between C-EUSand S-EUS in the diagnosis of intramural masses(95% CI, 71–94%), with the interpretations beingdiscordant in 7 of 45 of these masses [2 esopha-geal, 3 gastric, and 2 duodenal]. There was a 95%concordance between C-EUS and S-EUS for diag-nosing suspected wall thickening (95% CI, 82–99%), with the interpretations being discordant in2 of 38 cases (both gastric). C-EUS images of 4masses (2 esophageal and 2 duodenal intramuralmasses) were inadequate owing to difficulty withacoustic interfacing. This led to misdiagnosis byC-EUS in 3 patients.
For group B, the 53 patients with gastrointes-tinal malignancies referred for staging included48 patients with primary malignancies: 23 esoph-ageal cancers, 9 gastric malignancies, 1 duodenalcancer, and 15 rectal cancers (Table 3). The other5 patients had persistent or recurrent tumors af-ter therapy given prior to the EUS evaluation: 3patients had received chemotherapy (2 for esoph-ageal cancer and 1 for gastric lymphoma), and 2patients had had an intraluminal recurrence fol-lowing surgical resection of the primary cancer (1esophageal cancer and 1 rectal cancer). The T andN classifications by C-EUS were concordant withthose by S-EUS in 19 (36%; 95% CI, 23–50%) of 53patients and in 26 (49%; 95% CI, 35–53%) of 53patients, respectively. There was concordance ofboth T and N classifications between C-EUS andS-EUS in 15 (28%; 95% CI, 17–42%) of 53 casesand discordance of both T and N classification in21 (40%; 95% CI, 26–54%) of 53 cases. The depthof invasion was underestimated by C-EUS in all34 cases in which T classifications by C-EUS andS-EUS were discordant (Figure 2). Involvedlymph nodes were missed by C-EUS in 19 pa-tients. In 1 of 6 patients with stenotic cancers that
TABLE 1
Location and Nature of 136 Intestinal-Tract Lesions
Evaluated by Catheter-Based Endoscopic Sonography and
Standard Endoscopic Sonography
Site ofLesion
No. Benign LesionsNo.
MalignantLesions
Intramural orSubmucosal Mass
Suspected WallThickening
Esophagus 12 12 26Stomach 18 21 10Duodenum 9 1 1Rectum 6 4 16Total no. 45 38 53
TABLE 2
Concordance of Diagnoses by Catheter-Based Endoscopic Sonography and Standard Endoscopic Sonography
in 83 Benign Lesions
Site of Lesion
No. Lesions with Concordant Diagnoses/Total No. Lesions
Intramural Masses Suspected Wall Thickening Both Groups Combined (%)
Esophagus 10/12 12/12 22/24 (92)Stomach 15/18 19/21 34/39 (87)Duodenum 7/9 1/1 8/10 (80)Rectum 6/6 4/4 10/10 (100)Total no. 38/45 36/38 74/83 (89)
CATHETER-BASED VERSUS STANDARD ENDOSCOPIC SONOGRAPHY
VOL. 29, NO. 3, MARCH/APRIL 2001 119

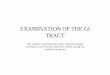
FIGURE 1. Gastric leiomyoma. (A) Catheter-based endoscopic sonogram shows normal multilayered appear-ance of the gastric wall (mucosa and submucosa) (arrow). There is a suggestion of a mass with significantshadowing possibly developed in the muscularis propria (open arrow). The mass is poorly defined, and itsdeep margin cannot be demonstrated. (B) Standard endoscopic sonogram of the mass shows normal mucosaand submucosa (arrow) overlying a round, well-circumscribed hypoechoic mass (open arrow) consistent witha leiomyoma measuring 2.5 cm.
KOCH ET AL
120 JOURNAL OF CLINICAL ULTRASOUND

were nontraversable by S-EUS, C-EUS identifiedlymphadenopathy (incorrectly classified as N0 byS-EUS). C-EUS defined the distal margin in the 6patients with stenotic cancers that were evalu-ated with both systems.
DISCUSSION
EUS is an important imaging modality in thestaging of luminal gastrointestinal malignanciesand the evaluation of mucosal abnormalities andintramural masses. C-EUS has 2 distinct advan-tages over endoscope-based sonography: ultra-sound catheters are easily used during routineendoscopy, without the cost and risks of addi-tional procedures inherent in S-EUS; and cath-eter-based transducers cost less than echoendo-scopes, although the C-EUS transducers arelikely less durable.
The endoscopic diagnoses of luminal massesand wall abnormalities whose initial biopsies arebenign are often uncertain. Some examples in-clude abnormal gastric rugae, esophageal stric-tures, irregular intestinal anastomoses, and in-tramural masses. To confirm the nature of theseconditions, repeat endoscopy, contrast radiogra-phy, CT, and other tests are frequently per-formed.
C-EUS was easily performed and provided ad-equate images to accurately assess the majority ofgastrointestinal-tract intramural masses andmucosal lesions. C-EUS findings did not concurwith S-EUS findings in 7 of 45 masses; the inabil-ity to obtain an adequate acoustic interface dur-ing C-EUS presented the most consistent obstacleto diagnostic imaging. Air between the catheterand the mass impaired imaging when the cath-eter was near but not touching the lesion. Withthe catheter placed against the intestinal wall,C-EUS did not resolve the mucosa and submucosaas distinct layers since they were not in the opti-mal focal zone. These 2 limitations would havebeen eliminated with the use of a balloon-tipped
catheter, which was unavailable during the studyperiod but is available in recently commerciallyreleased ultrasound catheters.
C-EUS findings concurred with S-EUS find-ings in the vast majority of patients with a sus-pected infiltrative process, ie, wall thickening,which in this series was most commonly a gastricabnormality. C-EUS offers an accurate and easilyperformed means of diagnosing or excluding aninfiltrative process (most of which are malignant)as the cause of abnormal rugae. The ability ofC-EUS to evaluate suspected wall thickening inthe esophagus and duodenum is limited owing tothe lack of an acoustic interface. The sonographicdifferentiation of benign from malignant esopha-geal strictures is based solely on the presence orabsence of hypoechoic infiltration extending be-yond the muscularis propria as a likely indicatorof malignancy.
The T classification of gastrointestinal tumorsby EUS is often based on subtle differences be-tween tumors. In this study, the C-EUS classifi-cation of the depth of malignant wall-invasion didnot agree with the S-EUS classification. The Tclassification was underestimated by C-EUS inevery instance of discordance, and in several pa-tients C-EUS failed to identify invasion into ad-jacent organs (T4). The deterioration of imagesbeyond 2 cm from the transducer on C-EUS pre-vented the accurate assessment of the differencesbetween T2, T3, and T4 tumors. The smallertransducers used with C-EUS operate at a higherfrequency (12.5-MHz) than do the transducersused with S-EUS (7.5-MHz), accounting for themore limited depth of penetration and represent-ing a significant limitation of C-EUS in cancerstaging.
The C-EUS nodal classification of gastrointes-tinal malignancies also did not agree with the S-EUS classification. However, in 2 patients withnontraversable cancers (rectal and esophageal),C-EUS images depicted an oval structure mostconsistent with an involved lymph node that was
TABLE 3
Gastrointestinal Malignancies Evaluated by Catheter-Based Endoscopic Sonography and Standard Endoscopic Sonography
Site of Lesion
No. Malignancies
Primary MalignancyPostsurgical Carcinoma
RecurrencePostchemotherapyPersistent Disease Total No.
Esophagus 23 1 2 26Stomach 9 0 1 (lymphoma) 10Duodenum 1 0 0 1Rectum 15 1 0 16Total no. 48 2 3 53
CATHETER-BASED VERSUS STANDARD ENDOSCOPIC SONOGRAPHY
VOL. 29, NO. 3, MARCH/APRIL 2001 121

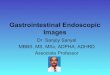
FIGURE 2. Esophageal adenocarcinoma. (A) Catheter-based endoscopic sonogram scan shows a hypoechoicmass (open arrows), which involves the mucosa and submucosa and extends into the muscularis propria. Thepenetration through the muscularis propria was not seen, and the tumor was classified as T2. Curved arrowsshow the outer margin of the muscularis propria without adequate resolution to suggest invasion of theadventitia. (B) Standard endoscopic sonogram shows the hemicircumferential hypoechoic mass, which in-volves the mucosa and submucosa and clearly extends through the muscularis propria (arrow). The tumorwas classified as T3.
KOCH ET AL
122 JOURNAL OF CLINICAL ULTRASOUND

not noted on the S-EUS examination of the proxi-mal tumor margin. In all 6 patients with stenoses,C-EUS permitted imaging of the total length ofthe tumor, imaging which may be useful in se-lected patients. While C-EUS cannot be advo-cated for routine EUS cancer staging, C-EUS mayin selected individuals provide additional infor-mation that is inaccessible by S-EUS.
During the study period, only 1 experienced en-dosonographer was available, and therefore, thisendosonographer had to interpret both the C-EUS and S-EUS images. We cannot exclude thepossibility that the endosonographer’s knowledgeof the C-EUS results may have biased the S-EUSinterpretations. However, any bias resulting fromknowledge of the C-EUS results could be expectedto influence the interpretation of S-EUS to agree,not disagree, with that of C-EUS. Because S-EUSwas used as the reference standard and the ex-pected direction of the bias would be to increasethe observed concordance between C-EUS and S-EUS, the lack of independent interpretationlikely did not affect the conclusions regardingstaging of the gastrointestinal malignancies.
Three previous studies directly compared C-EUS to S-EUS for staging esophageal cancer.12–14
In a series of 43 patients, Chak et al12 reportedthat C-EUS was convenient, easy to use, and mostuseful for small tumors and early cancers. C-EUSimage interpretation resulted in understaging ofthe tumor in 5 of 13 patients in Chak et al’s study.Although the accuracy of C-EUS versus S-EUSimages for 22 patients with mucosal or submuco-sal lesions was not reported, the endosonogra-phers who performed the examinations in 14 of 22patients preferred the catheter system. Ha-segawa et al13 reported results using both EUSsystems in 22 patients with 25 mucosal and sub-mucosal esophageal carcinomas. Their catheter-based system included an endoscope modifiedwith a balloon to facilitate filling of the esophaguswith water. The overall accuracy of C-EUS versusS-EUS in establishing the T classification as mu-cosal or submucosal was 92% versus 76%, respec-tively, and in establishing the N classificationwas 56% versus 67%, respectively. The advan-tages of C-EUS imaging in evaluating early can-cers in this Japanese study by Hasegawa et al areprobably less meaningful in the United Statesgiven the predominance of advanced esophagealcancers in this country.
Menzel and colleagues14 reported a series of 53patients with stenotic esophageal cancers usinga 15-MHz miniprobe (Aloka, Tokyo, Japan).The investigators noted that the C-EUS determi-nation of T classification was more accurate than
the endoscope-based determination (87% versus57%). In the Menzel et al series, all errors in C-EUS staging (7 of 53) were due to overstaging.C-EUS images were least accurate for the T1 le-sions (43%), unlike in previous studies from Ja-pan,13,17 in which C-EUS was more accurate forsmall, early tumors. In Menzel et al’s study, 2clinicians interpreted the images independently,and differences in their levels of expertise werenot assessed.
Comparisons of C-EUS and S-EUS for evaluat-ing ampullar tumors and colon cancers have beenpublished.15,16 Two studies reported C-EUS to bemore accurate than S-EUS. Neither study ad-equately addressed why C-EUS images of ad-vanced esophageal cancer, duodenal tumors, andcolon cancers, all of which are usually larger than2 cm, had been more accurately interpreted thancorresponding S-EUS images. The smaller trans-ducers with a focal depth below 5 mm that areused in C-EUS are unlikely to be more accuratethan the transducers used in S-EUS for assessingcancers greater than 2–3 cm thick. In our reportand the report by Chak et al,12 all errors were dueto inadequate tissue penetration and understag-ing, findings that are consistent with the theoret-ical limitations of C-EUS. The optimal role of C-EUS in cancer staging remains uncertain pendinglarger, multicenter studies.
In conclusion, C-EUS images of the gastroin-testinal tract appeared to be comparable to S-EUS images for the evaluation of intramuralmasses and suspected wall thickening, but C-EUS was less accurate for cancer staging in thisstudy. Balloon-tipped catheters have recently be-come available and may enhance EUS in theesophagus and duodenum by improving theacoustic interface. The C-EUS system we evalu-ated consistently understaged advanced gastroin-testinal luminal malignancies owing to poor reso-lution in deep tissues. Larger, lower-frequencytransducers may improve C-EUS’s accuracy fordetermining the T and N classifications of malig-nancies, although the diameter of the probes andassociated depth of penetration are limited by thediameter of the endoscope’s channel. The rela-tively inexpensive, easy to use C-EUS systemsstill allow highly accurate evaluation of superfi-cial mucosal and intramural lesions and shouldbe a useful complement to routine endoscopy andto S-EUS for some gastrointestinal-tract tumors.
REFERENCES
1. Tio TL, Tytgat GNJ. Endoscopic ultrasonographyof normal and pathologic upper gastrointestinal
CATHETER-BASED VERSUS STANDARD ENDOSCOPIC SONOGRAPHY
VOL. 29, NO. 3, MARCH/APRIL 2001 123

wall structure. Comparison of studies in vivo andin vitro with histology. Scand J GastroenterolSuppl 1986;123:27.
2. Silverstein FE, Martin RW, Kimmey MB, et al. Ex-perimental evaluation of an endoscopic ultrasoundprobe: in vitro and in vivo canine studies. Gastro-enterology 1989;96:1058.
3. Rosch T, Classen M. A new ultrasonic probe forendosonographic imaging of the upper GI-tract.Preliminary observations. Endoscopy 1990;22:41.
4. Liu J-B, Miller LS, Goldberg BB, et al. TransnasalUS of the esophagus: preliminary morphologic andfunction studies. Radiology 1992;184:721.
5. Akahoshi K, Misawa T, Fujishima H, et al. Preop-erative evaluation of gastric cancer by endoscopicultrasound. Gut 1991;32:479.
6. Furukawa T, Tsukamoto Y, Naitoh Y, et al. Evalu-ation of intraductal ultrasonography in the diagno-sis of pancreatic cancer. Endoscopy 1993;25:577.
7. Maruta S, Tsukamoto Y, Niwa Y, et al. Evaluationof upper gastrointestinal tumors with a new endo-scopic ultrasound probe. Gastrointest Endosc 1994;40:603.
8. Itoh A, Tsukamoto Y, Naitoh Y, et al. Intraductalultrasonography for the examination of duodenalpapillary region. J Ultrasound Med 1994;13:679.
9. Alexander AA, Miller LS, Liu JB, et al. High-resolution endoluminal sonography of the analsphincter complex. J Ultrasound Med 1994;13:281.
10. Yoshida M, Tsukamoto Y, Niwa Y, et al. Endo-scopic assessment of invasion of colorectal tumorswith a new high-frequency ultrasound probe. Gas-trointest Endosc 1995;41:587.
11. Van Dam J. Endosonographic evaluation of the pa-tient with achalasia. Endoscopy 1998;30(suppl 1):A48.
12. Chak A, Canto M, Stevens PD, et al. Clinical ap-plications of a new through-the-scope ultrasoundprobe: prospective comparison with an ultrasoundendoscope. Gastrointest Endosc 1997;45:291.
13. Hasegawa N, Niwa Y, Arisawa T, et al. Preopera-tive staging of superficial esophageal carcinoma:comparison of an ultrasound probe and standardendoscopic ultrasonography. Gastrointest Endosc1996;44:388.
14. Menzel J, Hoepffner N, Nottberg N, et al. Preop-erative staging of esophageal carcinoma: mini-probe sonography versus conventional endoscopicultrasound in a prospective histopathologicallyverified study. Endoscopy 1999;31:291.
15. Menzel J, Hoepffner N, Sulkowski U, et al. Poly-poid tumors of the major duodenal papilla:preoperative staging with intraductal US, EUS,and CT—a prospective, histopathologically con-trolled study. Gastrointest Endosc 1999;49(3 pt 1):349.
16. Tsuda S, Hoashi T, Yao T. Endoscopic ultrasonog-raphy versus probe for diagnosis of depth of infil-tration of colorectal cancer. Endoscopy 1998;30(suppl 1):A85.
17. Murata Y, Suzuki S, Mitsunaga A, et al. Endo-scopic ultrasonography in diagnosis and mucosalresection for early esophageal cancer. Endoscopy1998;30(suppl 1):A44.
KOCH ET AL
124 JOURNAL OF CLINICAL ULTRASOUND