Embed Size (px)
Citation preview

8/6/2019 Pros Tho Don Tie 2003 05 En
http://slidepdf.com/reader/full/pros-tho-don-tie-2003-05-en 1/3
The Evaluation of Occlusal
Vertical Dimension
PROSTHODONTICS THE DENTAL CHRONICLE OF THE ASSOCIATION OF PROSTHODONTISTS OF QUEBEC
concept espouses that there aresometimes changes in the OVD, followingdental wear or the loss of posterior teeth.The disciples of this theory feel that thepatient’s neuromuscular system canadapt to changes to the dento-alveolarcomplex.1,2,3,4,5
Without knowing the initial positionof the stable bony points of referencebefore the dental changes, it is difficult,even impossible, to determine withcertainty if there is a loss of OVD. Thenone has to ask how does one render adiagnosis?
The methods used are not new. Infact, they are the same methods that areused in complete prosthetics since the
beginning of the century.13,14 Individually,the resultant diagnosis of each one of thetests is of little value, but by combiningall the clinical observations a dentists canestablish a diagnosis.
Facial proportions 15,16
Divine proportions or the golden rule :According to the sculpturer Phidias, thegolden number is the relationshipbetween two measures that when they
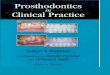
are respected generate divineproportions, namely, a harmony of formsagreeable to the eye. According to thegolden rule, the relationship between thepupil-commissure of the lips and thecommissure of the lip-chin measures1.618:1. Also the distance between thepupil and the commissure of the lips isgenerally equal to the distance betweenthe inferior edge of the nose and the chin(nasion to gnathion).15 (FIG 1)
Among the most complexrestorative challenges for a dentist is thatrelated to occlusal vertical dimension(OVD). In order to get the necessaryrestorative space and offer the patient agood long term prognosis, it is sometimesnecessary to make changes to the
OVD.1,2,3,4,5
The OVD is defined as the distancebetween two points when the occlusalsurfaces are in contact.6 It goes withoutsaying that it is a measure that isestablished by the position of the teeth.
The decision to change the occlusalvertical dimension should not be takenlightly as a change in a patient’s OVDautomatically necessitates the resto-
ration of a complete arch and even two.
Does dental wear automatically cause
the loss of OVD?
Two concepts exist in response to thisquestion.7 The first was conveyed byNiswonger8 in the 30’s who, fromexperience with patients, concluded thatnature conserves a constantinterocclusal distance of 4/32 of an inch(3mm) from birth to death.
This distance is maintained by anextrusion of the dento-alveolar complexto compensate for dental wear. Thedisciples of this theory9,10 feel that achange in the VD can cause seriousproblems at the dental, muscular andarticular level.
Another concept supported bycephalometric studies is that of thevariability of facial proportions.11,12 This
241Journal dentaire du Québec Volume 40 Mai/Juin 2003
FIG 1 : Old Photo. Facial proportions AC=BD
Geneviève Guertin, D.M.D.,Cert Prostho, M.S.Ed

8/6/2019 Pros Tho Don Tie 2003 05 En
http://slidepdf.com/reader/full/pros-tho-don-tie-2003-05-en 2/3
PROSTHODONTICS THE DENTAL CHRONICLE OF THE ASSOCIATION OF PROSTHODONTISTS OF QUEBEC
Profile : A profile with a Cl IIItendency where the chin seems to beprognathic can be a sign of a loss of OVD.
Contour of the lips : The loss of OVDcan produce a weakening of the labialcommissures and in and in occlusion, thelips then have an appearance of overcompression and the vermilion of the lipis thinner. (FIG 2)
Old photos : Old photos are excellentguides to allow the clinician to have anidea of what were the facial proportionsbefore dental wear or the loss of teeth.(FIG 1)
Phonetics
/SSSS/ and closest speaking space
Place the patient in the sittingposition.
With a lead pencil, make a mark onthe lower incisor of the position of theupper incisor edge when the patient is inocclusion (maximal intercuspidationposition). Then mark the position of theincisal edge when the patient makes the/SSSS/ sound. The distance between the
two lines corresponds to the closest speaking space .17 (FIG 3 and 4) When apatient’s measures are greater than thefollowing measures there could be a lossof OVD.
Cl I : 1.5-3.0 mmCl II : 3-6 mmCl III : less than 1 mm
/MMMM/ and Freeway Space
Place the patient in the sittingposition.
Mark off two precise points, one onthe nose and one on the chin.
Measure the distance between thetwo points when the patient is inocclusion (maximal intercuspidationposition) and when the patient is in aneutral or rest position.
242 Journal dentaire du Québec Volume 40 Mai/Juin 2003
FIG 4 : Patient saying the /s/ sound
FIG 2 : Weakening of the labial commissures, thinning of the lips
FIG 3 : Patient in the maximum intercuspidation position

8/6/2019 Pros Tho Don Tie 2003 05 En
http://slidepdf.com/reader/full/pros-tho-don-tie-2003-05-en 3/3
PROSTHODONTICS THE DENTAL CHRONICLE OF THE ASSOCIATION OF PROSTHODONTISTS OF QUEBEC
The position can be obtained byasking the patient to keep their muscles
at rest by pronouncing the /mmmm/sound or having the patient swallow.
The inter-occlusal distance is equal tothe distance between the two lines, thatis, RVD-OVD.
According to studies by Miswonger8,83% of patients measure 4/32 of an inchfor inter-occlusal distance. An increaseddistance signifies the possibility of a lossof OVD.
It is important to remember thatindividually these methods of evaluatingOVD have no scientific value. It is whenall these evaluations are combined that adentist can render a diagnosis and anapproximate OVD therapeutic value canbe determined.
Bibliography
1. Kois JC et Phillips KM. Occlusal Vertical
Dimension : Alteration concerns Compendium
1997 ; 18(12) : 1169-1180.2. Rivera-Morales WC. Restoration of the vertical
dimension of occlusion in the severely worn
dentition. DCNA 1992 ; 36(3) : 651-664.
3. Rivera-Morales WC et Goldman BM. Are speech-
based techniques for determination of occlusal
vertical dimension reliable? Compendium 1997 ;
18(12) : 1214-1223.
4. Lee RL et Gregory GG. Gaining vertical
dimension for the Deep-Bite Restorative Patient.
DCNA 1971 ; 15(3) : 743-755
5. Turner KA. Restoration of the extremely worn
dentition. JPD 1984 ; 52(4) : 467-474.
6. The Glossary of Prosthodontic Terms. 7e edition
1999 Mosby (Traduction)
7. Swerdlow H. Vertical dimension literature
review. JPD 1965 ; 15(2) : 241-247.
8. Niswonger ME. The rest position of the mandible
and the centric relation. JADA 1934, 21 : 1572
9. Thompson JR. The Rest Position of the mandible
and its significance to dental science. JADA
1946 ; 33 : 151-180
10. Dawson P. Evaluation, Diagnosis, and Treatment
of Occlusal Problems. 2e ed 1989. The C.V.
Mosby Co. St-Louis, Baltimore, Toronto. Chapter5 : 56-71.
11. Tallgren A. The continuing reduction of the
residual ridges in complete denture wearers : A
mixed-longitudinal study covering 25 years. JPD
1972 : 120-132.
12. Atwood DA. A cephalometric study of the clinical
rest position of the mandible. JPD 1956 ; 6 : 504-
509.
13. Pound E. Controlling anomalies of vertical
dimension and speech. JADA 1976 ; 36 : 124-
135.
14. Boucher C. Swenson’s complete dentures. St-
Louis CV Mosby Co 1964 : Ch 4 et 14.
15. McGee GF. Use of facial measurements in
determining vertical dimension. JADA 1947 ; 35 :
342-350.
16. Mack MR. Facially generated occlusal vertical
dimension. Compendium 1997 ; 18(12) : 1183-
1193.
17. Silverman MM. Determination of vertical
dimension by phonetics. JPD 1956 ; 6 : 465-471.
243Journal dentaire du Québec Volume 40 Mai/Juin 2003
In Memoriam Le docteur Maurice Mercier
est décédé le 26 mars 2003 à l’âge de 84 ans. Dentiste retraité du gouvernement fédéral et
capitaine du Canadian Dental Corps durant la guerre 1939-45.
Le docteur Patrick Hector Corcoranest décédé le 7 avril 2003 à l’âge de 85 ans. Il a été capitaine au sein du corps dentaire
de l’Armée Canadienne et a aussi pratiqué la dentisterie pendant 42 ans
dans le quartier Limoilou à Québec.