Embed Size (px)
Citation preview


- --
8 Preprosthetic Surgery: l m p d n g the Patients' Denture-Bearing h a s and Ridge Relations, 100
The M b n t ~ k s Predhment, 3 Geoqp A. ZarbI S. Ross Bryant
9 Immediate Dentures, 123 Nancy S. Arbree
10 Overdenture, 160 George A. Zarb, Rhnda K h o b , John I! Zawb
1 1 Building Rappork The Art of Communication in the Management of the Edentulous Prediament, 177 Howard M. La4mman
&Wd&&J- 12 Materials hescribed in the Managemem of Edentulous Patients, 190 Rmda R, Dinan -
REHABILITATION OF THE EDENTUMUS PATiENT: FABRICATION OF COMPLETE DENTURES, 209
% 13 omloping an *nalgue/Substitute for the M d l tary DentureBearing m a , 211 David M. Da*





the h W b &ilk and h- m. M ~ ~ h a \ P e ~ ---% m physidogd ~a~lses. * * ~ C ~ ~ i m p ~ ~ Wfiationa @id with ocmwid surgical -np--h-m=%- j f ~ ~ ~ ~ t o ~ ~ a t W ~ p t i ~ h P w e ~ ~ a ~ ~ a n d ~ ~ g g ~ ~ c o m p I ~ , a n d r n
pychmhic wp to cope with ~ f h P @ - - -
~ d e m ~ ~ a d a p t S v e ~ i n ~ end The hiwon L that
h s - u e n t p b l i h imght-- tics was d m o m m k d a s a ~ W a t m e n t ~ o n for any adaptive denture-maring p&att ars well. The mso d 4 of ~~, be that @w ptient should be willing to undergo the required m- thetic mgid p w a h m and incur the m c e m q additional expmm 1-2).
In the tml%th edition of this text, we continue a halfeatmy-ol8 @adition of kbhg the obj- d m&tbisLof mal@ complete ~ . M b d s o ~ a c i m w ~ ~ e ~ o f implsot-mpporbed pmstbm on Cmml decioa ~ f o r m a n a g l n g t h e & t u l o u B ~ ~ S i m 1 9 8 5 w e ~ ~ ~ ~ u f ~ ~ ~ d sckntif~: wacept that can place the fqthd nmn- k 0 f i m p l m t s i t t ~ I 1 ~ ~ ~ t D ' * ~ " t b e e&mlous pm&m& Nmrthebs, we amt that this spp& L clearly a* ~~c nor W i l e for all pakm bcetwc W t i o d corn- plcte dentura t h m has compeIljngly ah& p e n its merib, We also mmrh cmwhdfhmrt the clinid skih and judgmmt required M m k c o m p l * ~ m ~ s ~ t b & ~ ~ - t i o n ~ q u t . T h e y a m & e t w o s W o f t h e ~ min- th -emtvthat -+
h OW pa-. ~ o f t h e s e ~ ~ t s , t h e r e i s r n e e d
for this text and its inmdn@y dual purpose. Today's dentkt can o f k dl edmtdcpus patients two wmlent apttons: CmqItte dtnmes or implant- Wdmd or impw--ed proshem (nbb 1- l ) . C ~ i t b e b w t ~ o f t h e r a p y i s l a d t d w a ~ w mr clawcut seIdon. The c W decision &odd Ideally r&ect the dedst's larowledge of de g e l d hatment efficaq rrnd dkchnm, as well as a patient's un- of trahmt fish and cost-effahnesk Biological, fb&ond, per- sonality, and fhd cmu&dons may ~~ ~ ~ o r ~ o s h e r e r A d m i r t d y , t h e ~ r e t e demm option kds itselfto mom fmpd wli- cation than a i d i m p 1 ~ ~ pshehc o a e , ~ ~ ~ t l ~ d e t e r m i n r m t ~ f ~ choice. On the oSlwr hana rn impht-mppbd


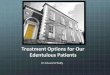
PWe 1-2 Pre- and postprosthdantic photographs, A and 0, of a woman who ephibited chronic maladaptive complete denture behavior. Although this gratifying esthetic result might have been readily achiwed with conventional complete dentures, in the p m t case, a more stable support mechanism was required for the mandibular prosthesis, whlch was attained by the uw of five oaointegrated implants, whose transepithelial abutment components are shown in C. The articulated working mt (D) incorporated implant abutment analogues to support a customdesigned, rigid, silver-palladium framework.
Continued



Chapter 1 The Edentulous Predicament 5
IauIc I- I a Treatment Optionr for Edentulour Patientr
#rplodr -- - W d a a d W I
Edentulous ifi me w both a r t h A; 'Cpmgkte dentu~stw ,hndiml wthetic and 8. Irnphnt&pMted d e n t u r e s or perceptual consequences C. Imptankupported fixed prosthesis that am encountered on a
tindependtnt and walating-basis
I. Wrthwt prior denture experience A, 0, or C It. With an adaptive complete A, B,urC
denture exertnce Ill. with a curmi history of 8,ar C
maladaptive dentun-wearing experiem
f r w t m m t d r e i c c b k r f l ~ ~ ~ ~ ~ ~ a n d ~ ~ : ~ , t A t h p p r t o f ~ t ~ G h p R g C s i n 4 h e p m h d d t d a p k h ~ r t c e Eon be mkdy nrl&tbk&an ~ r n d a r n ~ d n e d p-
? I
, :
' I , I
1 ,I
-



~~~ of^^
~ f b a p ~ b o m ~ r ~ ~ t i h w g L w * q - g r o u p a i o f ~
~ ~ p ~ o n E y i f & q ~ I y ~ d , a n d t h i s s u p p w t i s p r m d e d b y the pefiodontim, an organ cmpmd of soft and ~~w~
T h e ~ ~ ~ ~ ~ b t h e Boneoftkjjawa,flrrovidingadehaauspensory a p p a b s mismt tu M o n a l fbma. It allows

-'- wsw intemtim.amoRgthe~ ,&hperuls bf the rnwibtory q%t& k ttte -'d ~ a d m g e in L e mcs)panlm o E u & d

tbt the rnH&tiw fmm mtiw on a pros&& ~h am not Mwly to be -11ed or &mu- ~ ~ ~ ~ t b e y ~ t o b e b y t h e ~ d dmwa- mluxxpe* 4h -epadmt mpmw &ahm &me will aknxmst its& m d y h m t h e d m g m cbwd in the+& dentition.
. *
m v - . d o - w e - & ~ o a ~ W ~ W i t h ~ ~ &&om, mag&&, and- of differ- e n t f ~ m o f a c c ~ l ~ O r r t f a c o f b e a h m d , the unsuitability of* tisaw mppdng complete dmtum for lad-bewing f u m h d bt imme- diately recqnhd becaw fh mucaw membrane i s f o r c b d t o s w w a n i d e n t i d ~ m ~ p w i - odonldli-.
The area d mwmm d & e to receive the had f r o m c o m p h * i e l i m i ~ * ~ with the cmeqmding areas of wppm& available for natural dentitiom. Rewanhem turre computed the mean dentumbeamg area to be 22.96 cm2 in the M o u s mdae aad approximately 12.25 cm2 in an edentulw mandible. These figures, par- W a r l y t h e r ~ ~ m e s , a r e m ~ i c m n - ~witllth845-Fm2areaofpe&do~1igament W a M e in eacb htd arch (Figure 2.3). It dm ~ b e ~ d ~ t t h e ~ ~ ~ (basal seat) becomes pmgmwively d e r m &dud ridgea morh Fwbmm, tbe m w m demomtmtes little tolerance or &pi&lity to den- ture wearing. This minimal tolerance can be ~ a t i l l ~ t r p ~ ~ e n c e o f s y ~ c diseases such as a m & hprhmipn, or *, m weU as nutritional deficiencies. In hct, any dia- turbance of the normal matabolic pracei3w m q lower the upper firnit of m u d bkmm m d ini- tiate infhmdon.
~ c a h r y l & a r e m u c h ~ ~ t h a s e a b a t c a n b e p d u c e d b y ~ e f f b r t a n d a r e i n t ~ m s ~ m o f 4 4 l b ( 2 0 ~ f m t b e n a t u r a l ~ m u m forces of 13 to 16 1b (6 to 8 kg) d m q chewing have hem ~ P d e d with oomp1ete deq* t l l r e s , b u s t h e ~ W a r e ~ l y ~ ~ t h a n ~ w , I n ~ ~ b i t e f o r c e s ~ t o b e f w e t o s i x ~ l t s a s f o r ~ o m ~ l ~ ~ wearem than for pfmom with lm&rd tceq. Moreover, the forces requlred for dmhg vary w i t h t h e t y p e o f f o d b e h g ~ h h t a with prostheses hquently limit the lading of

eigure 2-3 The area of periodontal ligament supporting an intact natural dentition has been computed to be approximately 45 cm2 in each arch W. When t& are lost, and a patient becomes edentulous (81, aspects of support for an occlusion are severely compro- mised both qual'itively and quantitatively.

'k ~ f $ w t o a a 5 ~ i e u s e d t o ~ ~ ~ - b&289t&ptk~ @ tb (ad sWIiQ),of-. h f'act, the bucciaa-
1 Flgum 24 A, Panoramic ndlographs showing 'the jam of four edefltulous patients. aesiduat ridge reduction has occurred to variable extents,
hntinued

-re 24 m t Y 8, The rate d rlugc duction is quantified bewen IWO stages of observation (a and b). The difference between a and b represents the reduction in height of the alveolar ridges between of obswvation. The shaded area denotes wrption. C is a reproduction of progressive residual ridge reduction as refI&ed in a composite of five different laierd wphatograms. (B, Modified from Tall n A: j Prasthet Dent 27:120-132,1972.) Y=

iusn. This %c$wum &m& on the imrwtiotls ofthemany mnpma& mpmw~ted in P i 2-2. l % e ~ W o n u & a ~ d e r t t u r e f b r t h e -a&&gmttw#h&malmahis@i ~ h ~ ~ ~ ~ i g ~ W s f O f u n ~ ~ ~ ~ ~ * w atste.
The primary wmpmmb of hman dental acclmion are (1) the dentition, (2) h mmmtas- d a r s y s b q and (3) the cmniofkial smtchm. The devdqment and mtmtian of t h m mnpo- n a b are itWrrelat4 BO tb! $r67wtb, a@Wion, and change activeiy parkipate in the dew@- ment of an &t d w i o n . Dabition dmlop- ment is chamcte&wd 4 a period of dental alwand-
~ u k ~ ~ ~ ~ i c d t x e a t - m e n t & t a t ~ m y ~ & ~ ~ f ~ h r e d &d@w Trwwm; 89a example, ~ c s n ~ ~ & ~ ~ ~ ~ t b y -c-
Hgum M ~~ and adaptation of the &usion.


PamfarndJa10d CornSi&ratiohs No&dmd 4p * habits irwox* rcpotsdne=the*ost lb hamnfitlbtheww* ofthe- t i c r r t o r y ~ ~ ~ a o ~ ~ ~ ~ c r t l ~ ~ ~ i a c i d e a c e d ~ ~ ~ 6 : l ~ ~ m ~ w i t h ~ ~ o t w i t b ~ ~ , c ~ d ~ i n d i ~ t b a t ~ ~ i s c w m n m n a n d i s a ~ quent- o f t k c o q l a & d ~ o f & e d e n - tw-basring mums& In the damre wemm, p a d I & i d M c a n ~ ~ ~ r n t h e d a m 3 ~ - ~ % l > T h e & & U t y o f t k ~ O f ~ ~ h sad^
The n e u ~ p h p ~ i d q g i d bask underlying b n a t i a m h b m n s ~ e x p h ~ l y b s t h i n m i n d s and k humm beingst and pmt of itti m ~ c a n ; b e ~ b y a n ~ i a t h e tonic activity k &E jaw rrru%c1a. It irs a vay corn- p l ~ m e a d ~ l r n a ~ b e a a s h a w n t ~ result fronmpychm~cia3fackm (such aa shms or ~ ) o r t Q b e a ~ t i p a t O ~ ~ o I t s @g., anger, fh8Won). . It nwy be ~~ with specific meW cmdi$iorus (oral h&ve dyskbda, Parkhsonb' dkaw) w with st+ pamamh (e,g., lmahm [sooth gmdhg], rapid eye mmmmt pEbq behavior d b d m t , ar+ madbdar mywbnw) or sleep disorders (stpea). It msy be found comombtly with c* ilmad cmditiw sncb as p a h orsl b&n8, xtromn.& and discwnfort* prmthe- as or wlusion.
m ~ ~ ~ * ~ m d e ~ 1 ~ i s ~ t Q ~ ~ ~ ~ ,

w- r t wmd#a -dmHwo Mainly vertieaI Mm&entand light I i . I
Diurnal on{y Frequently korhtal as well 9s vettical P r o l o p pod bh/ &ve
WI d umal and nocturnal
behavior in the surrounding musculature. Frequently, the complaint of a sore tongue is related to a habit of thrusting the tongue against the denture. The patient usually is unaware of the causal relationship between the painl l tongue and its contact with the teeth. Similarfy, patients tend to occlude the teeth of new dentures frequently at first-perhaps to strengthen confidence in reten- tion until the surrounding muscles become accus- tomed or to provide some accommodation in the chewmg pattern-and experimental closure of the teeth is part of the process of adaptation. A strong response of the lower lip and mentalis muscle has been observed electromyographically in long-term complete denture wearers with impaired retention and stability of the lower denture. It is feasible and probable that the tentative occlusal contacts result- ing may trigger the deveIopment of habitual non- functional occlusion.
The mechanism whereby pressure causes sore- mss of the mucous membrane is probably related to an interruption or a dimnution of the blood flow in the small blood vessels in the tissues. These vas- cular changes could very welt upset the metabolism of the involved tissues. The relationship between parafunction and residual ridge reduction has not been investigated. Nevertheless, it is tempting to include parafhction as a possible significant pros-
ridge reduction.
CHANGES IN MORPHOLOGICAL I FACE HEIGHT AND THE I TEMPOROMANDIBULAR JOINTS
I The terminal stage of skeletal growth is usually accepted as being at 20 to 25 years of age. It is also
~ t h a t g r o w t h ~ d ~ o f ~ ~ skuletan contin= well into adult life and swh ~ a ~ ~ ~ u n t s f o r ~ ~ m i n * ~ t f a c i a l ~ ~ l t h b t e n r e p w z e d t h a t m o r - pbhgical face bight krmsa with in per- sons pslaessing an intgot or relatively intact htit ioa N e l e s s , a premature duction in morphulogicd fwe height mm with amition or &mian of teeth. Thh reduction is even more cons pi^^ in c lo us a d ~~ denture ww&g patien&. F i 2-5 pimis s flaw chart ofthe p m s m e d m of chmgestbtbke place during the dwelopmmt and dqt&on of the o&lusiofi. It also sma to u~derwme the ~ 0 f ~ ~ ~ ~ ~ i ~ a e l a p t s t o hm@3 aslmciahd with disease a d a#wdant teeth low.
MaxIllomandibdm morpholugical, changes ta laep~ lm~yowraper iodof~anddepend an the balance of osteobWc and ~~c activity. Th& * aurfaca of tempom n m d i i j o b WL) we also ipvolwd, ad at ~ ~ , ~ r p r d ~ ~ w ~ through the paolifedve activity d the articular ~ ~ . X n i h e W S k e ~ , wnydimdmd ~ i n ~ ~ f a a a ~ t o r t b e j w - ~ b ~ o f t h e ~ o f W a r e ~ t & i y -bthCmd.xtibltl&-m ~ ~ a x t i ~ ~ u a d ~ e s i a w b u t wntinu01~~ remodeXing t h r o w He. Such r e m a d e ' h g i S ~ b a r b l y & ~ w ~ b ~ - gruity oftheopphg! dab Is main- tained, even in the pmmm of' dimensional or ~ o n a l c h g e s i a o ~ ~ a f t b e f a o i a f shletotl.
The reduction of the residual xiagPrs slnder pIete dentures mi the ac- M o n h

imwkEMq4M- jaw wltdiQmm-Bt
t m 9 ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ m e n t o f ~ a ~ i e ~ ~ . w a ~ piat for devehphg a p m s t h e t i e ~ ~

p r h d most of the ~b~ m o e y a b e e n ~ a t l ~ a o t i n
me- ~ 8 c c I ~ o f c o m p ~ ~ ~ i S ~
, ~ d w i a t ~ t h a r t c . o d d ~ ~ ~ & f h W m d ~ ~ g ~
ia close to, in oemtric m i a n , or the I
I Xt is callxxtgd, mtrsvarttxe* a f ~ ~ c ~
@WW k a xwdmlw position autariar to d psition referred to as uattric-
L in cmpbdenta te prdmdontics,
&&,piition d plarmed maximum ma on k&.h ie e&Wli&sd to coincide with the
tric relaiiw. The W d m c e of ccn- and centric ocalpsiun is cmsqmtly a wtric relation &usion (ma),
Tb centric 0 1 x 1 ~ ~ ~ position cmupkd bJI the m d i b l e in the dentate patient cem& be regis- ter& wi& d1cient & m m q when the *at l3aQmM e d e d d a cme~uen* , ~&~ r i e n c e s u ~ W t h e ~ Q f m t € & ~ tionistbe~tartingpuixttinthe Wgndan artificial 0 ~ I U s i o ~ l .
N ~ e 1 w 1 , olle mufit r e a b that aa inkgd part of the W ~ r n of centric d8ti-t the ~ l i a k d ~ d ~ k ~ f o r dmnge* Thh change is brought shout byalt8nakm i n ~ ~ ~ B l a d ~ ~ ~ w e l l a s ~ m a r p b ~ ~ c ~ t w i n t h e T M J a A n ~ ~ f o r t h e ~ c ~ o f d c d a - tion in dmtumwarhg pati* @ d u l y k an raging con- mo&ms the clm& fmt&d ~ o f t h e ~ ~ ~ I t ~ accomts for di&mt o o n ~ ~ agd tcdmqlm of design of occwm.
Tempom~~fd ibu i~r b in t Changes N- drsscriptiw of TMJ -tion have c V O h d ~ c r f d ~ h x n e 0 S E Q d s . T h e basic ~ o l q k a l r e l h d p qmmg tire condyles, the &da, and theit: glen& f m w m b k -
* . d u r i n g m d d ~
contacts and during dl mmmnmtia guided ly o c c t u s a l e l ~ . ~ t : t l ~ ~ i n ~ t r e a t - mernt with coqlek deatures, the dm* W d seek to maimin or restore this M c physioIogicd ~ a t i 6 m . n e ~ m ~ o f t I r e ~ ~ am qmduciMa, d all other rnomnmb take p l m e c e w i t h h ~ ~ a f t h e ~ ~ " e d ~ e 1 ~ of motloaM Remhers haw cmclwied that the p a a s i v e h i r a g e ~ ~ t s h a ~ d defInib dd tard rqwddbie chmshr. T h e ~ ~ ~ f ~ p o ~ ~ p s t h i s of tremmbw practical s i ~ ~ in the -- m m t d ~ ~ B ~ h i t t h i s r e p r o d u c M ~ h ~ d ~ i n ~ p t m g p w s w o e I t m u s t b e d e d h t m o s t ~ o m ~ ~ ~ ~ d a ~ o f . . vamhomon the themeof amuiihtdddtim T n f h e ~ d ~ h p e r i o d $ ~ ~ o r a 8 o t p - t i w ~ ~ m s a r c h a n g e s o f t b e T M J s m a y h a v e ~ T h m u i a ~ ~ ~ ~ based on mtqg &a tbe d t a me only qmuhtwe.

ESTlKIlC, BEHAVIORAL M D ADAPWE MPUMSES
Morpholegical Changes m t e d whb tho
Edentuluuo State i, Deepening of nasolabial gmrrve i; Loss of labiodental angle 3. Deckease in horizontal Iabiat angle 4. Narrowing of lips 5. Increase in columella-philtral angle 6. Prognathit appearance
dhilkm d e & mfbcialch&I#&x- ~~ of or -t, = p a for ~IW.
~ ~ ~ s a m e ~ ~ o a ~ t e t h e ~ ~ t ~ 0 f t h e i r f r r e E s r f ~ f o r w h i c h t h e y a r e ~ o ~ l u u i r r P 1 ~ ~ l y m a g - n i f i e d ~ ~ ~ ~ s a m u n x e W t o t $ a i r ~ - law pmtieammt. h recent yeas, tlulrnerautl plastic surgical intervdm, W m l adcbs b i d cm= d c i ~ , h m b e e n ~ O n e o r m o r e o f t b e ~ ~ ~ w m a y p r u v i d e ~ s o r t o f mlut io l ides imihyb~mdvPbichisnot~ d m t i d b r e m i t . J n ~ a ~ ~ d a d t m a s t bepmqmdtoguideEhe@mtwitha=femlto €#l-mwin*mdof- WmY.
b p r r l i e a t $ ~ ~ ~ ~ d ~
& & m t a ~ d e ~ d m u I r l k thwiskl to m i d htm -. Meatswb*toprrrvide-of w-?€v=mmd CWb h t l m B p h & q p @ W M d b e ~ ~ d & m x d * b * I f & h ~ ~ ~ o f s i ~ m o f ~ * ~ thm=Yb*.
~ f k d ~ ~ o f ~ c o b j ~ andmethodsrat~Wforg80dccam=wm
. . w i t b a l l ~ . ~ k & e c t w w k m a b e p d ~ % ~ c ~ ~ m ~ l p h s ~ ~ w f i m c - t i d d m

I ~ * b a a i o n o f ~ ~ ~ a a d I q w d i w b m d i s m w b ~ p a t i e n t % ~ / **@-*d-b-Pt
~ ~ b o ~ ~ ~ ~ ~ d f f E o n n i n e I &-of-rrfMm-w*
~ ~ ~ t Q Q Q r n P l ~ ~ ~ b e o n e 0 f ' ~ ~ ~ ~ ~ ~ 0 f ~ ~ t l m t ~ 1 ~ ~ d ~ d d e n t i m y T h e ~ o f I ~ ~ ~ b j ~ ( ~ ] i n a a ~ I h3taoatbbMta&Citdiff&WaDthe I ~ t o r s y s t s m , w h i ~ h i n M n h f l v e n c g t b s
' ~ & ~ ~ ~ , ~ ~
i +EsrSaadrn-m*Wbh W dupe, witi~a, p m aad mow@
I & f # % ~ . ~ ~ ~ r o l e 9 n d ~ W c e of m d stimuli in the mum1 ofjm
I ammmnts need clarification, but it has been damwbhd &Fit control of h t m m by
WW to the oral mucous rnemhne. AM#& it L teqhg to as~~rne that there is a ~~ be&men oral s t a q n w i s and pupwefisl oral ~ ~ , ~ t h e d t s o f ~ i t w ~ u p omoar indicate that smcessful denha WEdQ ~ i w o I ~ ~ d h e r t h a n o r a l ~ ~ o r a l ~ . 1 t ~ ~ ~ ~ d m d t & ~ l y I q t h e o r y ~ w f b e ~ e d ~ , w h i c h a p a t i e n t u d a g o m w h i l e hmhg to war cmpIete den-.
Learnityt means the acquisition of a new a&- ~ o r O p ~ f a n ~ o n e . M w d m s R U I ~ r 0 t b e ~ m ~ m ~ ~ - -@ to mcW movement. The &cce@me of com- @f& den- i8 d e d b a of ~ ~ n , ~ b d e f ~ ~ & ~ ~ dfmimr- ,ioa Jmpmm to sohtinued or qeabd ~ ~ e r 9 ~ f h a t a r i s e f m m t h o w n a a c t o f d x
w i t b ~ r k h l y ~ t s d ~ ~ ~ a r e i~medafkwashort t ime.~useeach
~ o f t b ~ i n m ~ e L r e ~ t o t h e wm afthie prwi~ls app1ioation ofthe storage of Momation froin the h e d i - mintegratpt ofhabiuatioa Wid@
k ~ ~ e o f i n f ~ o n o f t h i s t y p e ~ & w o l & x a g e , a d ~ s i e a h e ~ w h g t o ~ & g@imh have difflEulti&s b e c o d q m m f W b q @ h ~ F u a h m ~ , s w m w b n r p ~
I * & w h a e v e w o a . % k z w b t pWly prwents the tnm&er of hbihdon
I
2 ~ o r n ~ n l a of the Menhleus m e
t z v d d B y m ~ l d ~ ~ b a m ~ w h i c h ~ ~ r i s e t o a n e w ~ O E ~ ~ ufi, and d clinicid applications of &@&an p r o b ~ ~ ~ ~ T h e ~ e g l t ~ ~ w m r ~ l & e u p p e r d t m w ~ a ~ ~ u r a l ~ ~ ~ ~ w i l I ~ r c a m p 1 * t ~ ~ ~ ~ a d a p t t ~ . S g c h ~ . ~ h w ~ ~ l l r r i t b * e d ~ s a s d ~ - tation of the tmgim- The topgw f q u e d y m p a h t o t h e b o f p t & ~ ~ t e e & ~ a l m u I s r bom~~ging*tObringitsl8tfd~ i r u t o ~ ~ & e ~ ~ T l w ~ n r r f a n e w d e n t a t e j a ~ a s a n u w ~ t & t 8 e t o a g r a e , a n d t f a e m ~ b ~ ~ ~ & e ~ o f t h ~ t o ~ t o t h e a k d q a c e ~ l e , A d e @ e e ~ o f ~ tongue wWty also @a place. Furth- tbe ~ ~ ~ d u d t i d g m a m ~ ~ t o n s w a e n s a - tiom h m lh owdying p8thmis. Pramms t m s f k m d ~ ~ ~ & ~ h ~ ~ ~ & ~ u l i f x o m t b e ~ a t a d f r i e t i d ~ * f o o d l a a o n , ~ ~ ~ l ~ l o f t h e l t p p e r ~ * quentEp.mmtbe~8becmwthepaster ioa ~ o f t h e t o P g u e i s n o I o n g r e r ~ t g ~ thedi-effactomthea-by W ~ g l l l a I d i ~ ~ ~
B d e n k r f o t r s ~ e x p a c t , ~ s r e e x ~ b ~ t o t h e ~ ~ m l ~ ~ ~ . ~ ~ ~ t a k e p ~ i n t b w a t e x t o f th patiaatb om& oy&dcI emtima& and pycbo- logicat m s *
The facility for Iegtning and c-an appears to dimirrlsl)r with rtge. Mysmeing age b m d s t o b e z 1 c ~ b y ~ s i v e a t m p h y of e l m # in the cerebral mrtex, and a @om-
qaent 1088 in the facility of caordbmtion occm. Certainly, patient motivation dictates the qmd w i t h w h i c h ~ ~ f l t u ~ ~ p k e . h is imperative that, the dentist d e t a m h tbe pa%imt's m&&bn in seeking bedmmt, d& vatu tfiismotidon, md seektofwtwibifitis klring or a b n k /
A ~ a e e d e x i s t s f o x d e n ~ ~ t o b a M e t a ~~ a patieat% &dcpt~ k seeking prosthodontic care and to identi@ pbkmbtfm ~ ~ r r t . ~ ~ n a l ~ ~ ~ t o p l a y a ~ & i n t h e W e g y o f d m t d p r o b h m . T h a i n t # i ~ m d M ~ m o b v i ~ q 7 3 t o ~ t h ~ p a t i ~ m d h m

1 t ~ a E s o ~ ~ ~ t ~ ~ @ f f w w y ~ m ~ - W d
fOt--~-~m
t h e ~ S e ~ t i ~ m ~ ' ( r e ~ h m - m ~ k M b e e a * c a d
r n i m ~ ~ i n ~ o n d & m b n t ~ i n f a p e -
4xadkhmbw*-intbeat I m l w e b ~ ~ ~ b a f d e n m ~ 1 d W @ h l h h ~ & & h S , b
+ s m & t h , M t . Z l i n i c a t ~ m & I ~ - t m ~ &dim indicate that a cmnbimtim of @lmh-e p r o s w t i c protwds, and qmpri-
@mmmk&cd and supportive therapy, are lamdly aiiqmte tQ pmide plien€s with d
~ 0 f ~ ~ t i e S i a ~ ~ ~ h j d kcdv& is achieving j& rest. F k c w l e ~ d t y f a r ~ o 8 t i ~ t l & f m t h e . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . & ~ U , v o ~ Q r ~ ~ ~ ~ b e ~ c u E t t 0 ~
ETH€TiC, BEHAVIORAL, AND A M W E RESPONSES
Amdated the Ec)renXsbds State
1. Deepening of nasolabial g m 2. Loss ~f tabiodental angte 3. Decrean in horimntal labial angle 4, Narrowing of lips 5. Increase in columella-philtral angte & Prmathic appearance
Behayioryll and Adffpti~e Respnl~e~

Chptw 2 Biomechanics of the E d c m t u h State 21
~ ~ a n o f l e t t t n J a & n U l ~ ~ a n d i w w O t l ~ i a r r e ~ t o t h e ~ t b ~ # w . m ~ t ' $ ~ d l n d ~ w b ~ ~ l ~ ~ ~ t h e r t a n ~ ~ i y ~ ~ ~ o f ~ a f c w ~ a n b . b 1 p i a g ~ , ~ a d a p t b c o m p l e t e d e n ~ s w b e w e o f tbemblt mcuuw~ oneofthembstrmard-
I w p t a of clinical daihtry, The pmsunce of - * &t&um& foreign obj- (dentum) in an ederatu- r ~ m w u t h b b o a s l d t o e l i & d i ~ s t ~ u l i t o t h @ I ~ r s y s t s m , w h i o h i n a u n i A n - ~ t h s
wlic masticatory stroke pattern. Both atmocep ton? and pmprioccpta are probably d%$edbythe i h , shape, pision, pressure &om, olnd mobility d the prosthesa. Ths exact role artd p0W-m hportmx of mucod stimuli in the control ofjaw nwvmmh need ~ l ~ c a t i o n , but it has besn c w y ~ ~ t h a t ~ l o f d e n t t l r e s b y muscle a&Q is d c d if d a c e mmthetic is applied to the oral muoous membrane. ~~ it is bm@ting to a s s u m that t h e is a camlation betweem 4 stereqyosis and p r p e f u l oral &&or activity* th muh of most hv&&ons up to now indicate that euccessfd dentuff maring m b l y involves factom other than d m a n mrd oral &oman#. It &emf- mmah very diScult to appiy leatning theory con- to tbe p w d proms, whi,ch a patient undqoea while teaming to wear complete dentures*
Learaing means the @sition of a new d v - ity or change of an one. h h x l a r s&ll ~ t o t Z r e ~ i i t y t o ~ t e m u s c u l a r r r c t i v - &y to b o b movement. The amepmce of com- p b dentures is accompanied by a promis of Iiabhtdo4r whichis Wmd as aMgmdual diminu- tion of nqmsm ta c d n u d or qwaed stimulr." TheWestimntiihatarkfmntbemWofthe pmh& with the richly innmated o d cavity mrre
. probably ignmed a short time, h w e each s&ge o f t h ~ b a s ~ i n ~ e i s m l d t o t b e m&mq met? of the prwiow application of the M m , stmige of i n f o d o n from the immedi- wpttis an integral part of habituation. Diculty i a t l x e s t ~ 0 f f n f ~ o n o f ~ t y p e ~ - ~ o l d ~ ~ a g e , d ~ i s t b e ~ n w h y o ~ d e r patien& have dBculties becoming comfarhble wikh dmhxm. Fmfkmore, stimuli rnW be spe- WIG and i c h f i d to achieve habituation, This is wWt probably p m a s the hmfsr of habituation
~kedbyanaldfdardenturetoamwdentrrre, ~ c h ~ t & y $ I ~ r i m t o a ~ m n @ o f s t i n m - utf, and sewed c h i d a p p l i ~ t i ~ of a d q m m p r o b ~ m r t y k ~ t e r e d T h p a t i e n t w h ~ wwnarompleteuppethtureqqmingafewrsmt- Urat mk&r mmdktk teeth d y will find a complete 1- dmbre dSlcutt to nrlrlpt to. Such a patient has to contend with dtered she a d orien- '
tation of the tofl'gue. The tongue frequently reqmnds ta the 10s of @or Wth and alveolar bomby~gsirsetnbrhgitalatedbarders into contact with tfie h c d mucosa. The imtertion of a new denklre in* a n m ~~t far t h e t o n g u e , m d ~ ~ i c t m g w ~ t twrgmh the shap ofthe bngmtodmnto the altered space available. A degree of rebin& tongue activity also takes place. Furthermore, the posterior residual ridge^ are e x p d to new scam- tim from the werIyhg prosthe~is. h m e s m m f d through the denture base tactile stimuli from the tongzle and fiictiod contact with ~ h l a d d i t i o n , c o n t r o l ~ f t h e u p p e r ~ f r e - quatry must be unlearned kame. the p k r i w partoftbtungueismlonger~uhedtoco~ the dislodghg effect on the denture p d u d by the mmhhg amul ib dentition.
~ t u E o u % patien& e x p a and am expect4 to adapttothedentummoreorh'
-021 most taLe place in-; the patient's d, systemic, dd, rtnd psych Iogicd staten.
The facility for learning and coordination appears to diminish with age. Advancing age tends to be accompttnied by progressive a p h y of elements in the cerebral cortex, and a conse- quent loss in the facility of coordination wcm. Certainly, patient motivation dictates the speed with which adaptation to denhues takus we. It ia imperative that ,the dentist determine the patient's motivation ia seeking treatment, culti- vate this motivation, and seek to fmtm it if it is h h g or absent.
A d i s W IW&&&X~OT den&& to bes&to u u h t a n d a patient's motivdoa in wdung p m h d d i c care End to ide* probram befbre strrttiagtreabnenL Emti& factom areham to pIay a sipificaat role in thtt etiology of dental prd>lms. The inthew a d dinid emination ~ o b v i o ~ w a y a t ~ o ~ t h e ~ e n t 8 n d f o r m

t t h g W t i W m a ~ ~ . ~ ~ ~ ~ ~ ~ o a a f ~ ~ ~ ~ ~ ~ s r n d d & ~ ~ ~ t x J ~ ~ ~ s r n d ~ ~ ,
' ~ m ~ ~ ~ ~ ~ t f a e ~ e o ~ t m e ~ B ~ , ~ t o ~ ~ m d w h m t o ~ ~ ~ e n t ' s ~ ~ , A n ~ ~ o f a d e n t u r e
b t h physically oorapatii with the orrrl a god in-rsonal r e l a t i d p
tistandpatient. Etisqtotbehtistto ~ t b ~ f ~ a n d ~ ~ ~ . m w q . i b p h t t M e s other i h e s a anddental . . ~ ~ ~ i n * ~ o f ~ ~ I Q b l l g . k ~ ~ ~ ~ ~ s s e c u r e @ m t w i i l w # w t ~ y Y c a p e w i t h d i s c ~ d b w,
U h ~ ~ b m m ~ f h a t ~ a ~ o m - p k ! t e ~ ~ o m ~ ~ ~ ~ - ~ ~ o f & ~ i v e ~ m ~ f a u n d awmagegrq~wwatZlee t $ 3 t ~ a f ' ~ ~ , A ~ ~ f i Y on ~ t b e ~ ~ l ~ y ~ e x p h i n ~ c u l - * I t i d - patient satiWop1 with denhm, ~ ~ o n e f a g r o b l e m , ~ d m a l c e p s - ~~ m f e d fm diagnmia and treat- ~ & t 4 t a @ s n t I s flqmmm
Zs the howledge, W, and M b w & ~ ~ ( 1 r w e a r ~ ~ d s t : ~ W ~ ~ ~ t U ~ ~ ~ - @ . ~ ~ ~ a f a ~ h i ~ ~ b e o ~ a ~ ~ u f e ~ P e r ; t m c e l a n d t r s r i n t n g ~ ~ ~ ~ r m ~ & ~ ~
wi pz&&ly, unfm*, Ohg rigors of d m h l p m t i c e ~ m o s t d m ~ f r c m t & n g ~ - t h w t a ~ o n t a ~ p ~ ~ e w . Bmuw ammstbn Wiwem mati@ problem ~ ~ p m b I e m s ~ e x i $ t , a ~ t h & m - ~ & m l d b o u m d w a ~ f o r ~ ~ p e r - ~ ~ W i L t h e ~ L I t i s s u s e f U l ~ b w b b l i ~ a ~ f o a ~ ~ -

~ W A : ~ ~ : ~ ~ ~ W o i n ~ u b J . B m t B : O n l ~ a a r t u a i n ~ W t d ' " ' & M - m W t i o a m - states tooth hrr atad euhmdiam, J Dent Gduc 49:


Chapter 3 The Effem of Aging on the Wentubw State 25
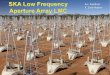
ed (ZQZO) Distribution of the Population 65 Years of Age and Older - - Australia mafia France -Y Iwn Elew Zealand United Kingdom tSnW S t a m
DtSlTlBUTlON AND IMPACT OF EPENTULlSM IN OLD AGE W b u r i o n 'fhe pmvdence of edentullm is declining. Todag, ~ ~ ~ ~ t O o n % ~ ~ f t h e ~ a n 6S years of age and older in most indus tdbd m e s are he, but there are hge -04 ad age-related d a d o m (Table 3-21, More older ~tt ian~pmenm~IytahaveteptfgprobaBly ~ m a n y w o m e n h r r v e l w r d d ~ ~ ~ e d e r i n l i f e , T h e l o ~ o f d ~ i s
with less d u r n pmpIe. For exam- * i n t h 8 U n i t e d ~ w i t h i z l ~ l a s t t t w o ~ ~haIf(51075) of the Iw educatedpqmhon w m ~ . I ~ w i t h a b o u t o n e q w t e r (29%) of @e mom big&& educated population (Burt, 1992), which most W l y reflects the mpe of M t h &ces a c d b i e to individuals. Quite aimply, those who hiwe less education and less *mImqdhp-deataIinfor- r s l t t t i o n a n d ~ d e 0 p a f f a r d r e ~ ~ ~ -
many coutltsies @W%tee, 1985). The damme in total a 1- in the U M State$ for example, hasctroppedby&utlW%eachWfortheht 3 0 ~ , ~ 0 * ~ w i a . ~ a n e t ~ f n the number of edeatufow popit for the fomee- able future with the growing numbers of older pet+ pie werall@- Shih. QW, 2 W .
Redud alveoltw ridge.s c o n t h e to resoh for aw- e d * a f k r ~ o f ~ y e t o I d e r p e r - Sow m&4y seek treatmat for problems with ~ ~ b l y ~ ~ ~ f t h e m ~ ~ ~ f i e d w i & ~ ~ ~ ~ e t d , 1991). M m okpeopIe u=b =wpoorry r a n m ~ ~ ~ p f O b I l b l y & ~ ~ ~ * * hold^,^^ ~ p ~ w h m ~ d o e ~ m p l & i & i t b ~ * t h e ~ o f ~ h w d ~ * ~ I w E e d e a t u r e s o n ~ ~ l . i d g e s .
'Bbm*dd@uBcMscEnta'm2)m THEIMPACTOFAGEONTHE mite thc benefh of mter flddaaioo olad abwt-offour~~derpertmswitb EDENTULQUSMOUTH
$$iwht&ix& w m using complete dmtum in at MUCOW bWv orra jaw (Mojm and MacEntea 1892; -l&wBnbq and Glick, 19931, but men thb is Stmmti t i~ and other mild hhmatim m the
lower than tb prevsllence of complete mucosal lesions ammtmd moet in &mtdh re- only a few dm& ago h m older edentuloas mouths, of older men

- . Table 3-1
Thc Dlst~+button ul tdenti~lirnl i r ~ Oltl Age
D m r k Fintand Gemny Ireland Jaotan N m win
wen
U R M States
PsRU (2001) Todd h lader (1491) Walls & Steele (2001)
Charme (1 993) Hawkins, Main and Locker (1998) Ainamo & h e m (1 992) AInarna & herberg (1992) Nitschke (2001) OtMu1hne and Whdton (1990) Ministry Hlth and Welfare (1993) Ainam 6r herberg (1992) Bourgeois, Nihtila, and M e d (1998) The Spanish Geriatric Oral H e a l i b
Research Group goo?) Ai namo k berberg (1 492)
Miller et al. (1981) Marcus et al. (1996)
Douglass et at. (1 993) MMWR (1999)
~ w z a r ~ , s m o k e f o ~ , a n d d ~ + & d > - bl exmwively (MwEnW, Glide, and S W , 19%). Qml G3nCer or p m c m v lesions are l m s d inwestern c~ltltrim, ahhough they are &a m m t ~ f o m o f o ~ o n t h e ~ m b - - t b m t & i n & e r ~ o f A s h . I t i ~ d t y clear tht the incidence of oral cmer is hi& m ~ A & m ~ c a n s ~ ~ ~ ~ o f the U.S. a d C&m popuIatl0m of o t h laces mddmtthe~&is~opcareramongAfrican Americans, whbh probably refl- tbe innuace & hw 9ocioeconomic SWU mom than genes or w b e (&Lw.s et d., 1999; b g a r d et at., 2W). B & m d ~ c ~ , mch as nicotine and alcohol, shwldbemoredamagingtutbeordmucosahold a & h i w e s f a ~ & ~ m i t o d s w i t h s l a w
of ceh a d h u r a d number of elastic ~ . ~ o r e i t h ~ l y t f i a t t h e ~ o f o r d
cancer is increased among edentdous denture w m espwidly a m ~ l g those who drink doohd t o e x c e s s d g m o h ~ , ~ p l y ~ m a n y oftfiemarepoorandtheymsrkelittleuseof~ ing services for early datmtba
Bone Bone maw is at it^ maximum in midlife, with & starrtially mure in men than in women, and in some racial groups mora than o h m . Howem, even withinindiviw, theq~ofboneinal lparts of the bWn, inc- the jaws, d a gtwdy and decreases with age (Estww, 1994). The ~ o c c ~ ~ g b e c s r u s e ~ b ~ ~ ~ e f f f - c i ~ t s b g e n ~ o n d e o l h m , a n d ~ i a m ajerall reduction of d d u m dmrpthn from the inkathe in old age.


TaSCE AND SMELL l h s @ d d m w y - w u g e d3e smtwry- im cbmlyrelated a d d q d e n L The stmation of mly - i n ~ ~ ~ b u t ~ t s f r o m ~ i n ~ o n a f ~
~ , ~ 8 ~ n d t T ~ i s f ; e f t , b F--mte,&d- ~ E ~ , ~ m E , a n d d t y ~ ~ =w--,~-lmykbe@ *la disntrbing the otherrs. Q l f a w y cells d ~ ~ ~ ~ ~ ~ h t a i a s 0 ~ ~ B e ~ - ~ ~ d o r r g t h e w E y .
~ t y t o ~ ~ w i t h a g e , a n d e s p e - cidly in alder p o r n with AlzheimerB d b a ~ (Murphy, 1993)). Also, the prefermice for 5pecif1c ~ c h m g a o w r f i m e t o f m r ~ ~ - wm of mgiw a d d t CompIainf of an imp&- ~ ~ ~ ~ o f ~ $ t ~ ~ & m I d h h ~ t h o ~ y ~ w ~ ~ a a ~ E w p i m k q ~ o r & ~ m n e u r o - ~ ~ . ~ t h # e & n e w e s ( V I , ~ ~ ~ ~ g m ~ o f m ~ ~ b e d i 5 - ~ ~ b g r - q - t e - g . , ~ ~ * and =wh m d &.&, heid *@=wdh&,but, f-&b dmage i n - W a f d t % l m m w b ~ & - ilybyinmxtwd--.
AGING SKIN AND TEETH
T l w s c a r s o f a l i f ~ a m ~ d e d ~ d y o n the skin as wddmi, pufFlpess, and p ~ ~ ~ , but the c h g w ate not dl manifestahm of+- eratim. For example, fewer hngxhw' ells in 0 l d e r r k i n o m p r c r e n t u n d s s i r s M c ~ ~ w - % - m a # l f n g o f ~ M ~ ~ g a h a t t h c s r m . T h e ~ I a o k ~ & h i the o l ~ ~ w ~ ~ 4 k y e p i d m m l -*his-IrUlmtw=- t t M d t h i ~ m ~ ~ . Q r a d u a l E y t h e ~ t h i m , ~ b I v e c o h g e n a a d ~ a a d wtinkleBqprtarthen~~fhtmeb!3k
A g e ~ ~ ~ v i t y d " p o n t " o f t h e upper lip, and it flattens the phihum. The - E m - d * * a * gbghktothemiddlethirdofthetbe,whet.aaa
1

G Ffgura 3-1 A n k ~ ~ a r cheifitis (A and an and sfomatitis (q in an elderly man caused by malnutrition andlor liver dysfunction (white b l o d cell count, 3.79; hemoglobin, 12,4; hematocrit, 36.3; vitamin B, , 203).

The .dw sf healthyI mbrd teeth In hue &%n pMow b o q , ~& k& whtion in dm&ul a d value (M&cmt& ma lW1). The cbma, and occarimdly&=
d e a ~ t o ~ m w b ~ b j f a s p k d c d i s b ~ o f v w - h -0- W U ~ *=--telx--*crlr* ~ ~ ~ ~ ~ e o f l u t ~ ~ w ! l W h m l * W * ~ W & ~ h - ~ ~ e a r t r i n s I ~ ~ * I t . h n o t ~ ~ b ~ t h i s r u g g d ~ k a @ ~ ~ Z n f ~ , ~ p a t i e s t s i n ~ ~ t h e ~ i l e r m e o f t h e i r ~ ~ p r e f e r t o ~ ~ ~ - w i t h t e e t h w = d e g ~ , md*fhatlnatnr&tteeth.
c€WCEWf FOR W O N A L APPEMUMCE fM W AGE Qldur p5mom wrry &€a their s e I f - h @ as m + i f ~ t m m , ~ 2 t t ~ O t h e r ~ D f ~ . ~ m a y b e d ~ ~ u t g r o w i n g 0 1 4 b ~ t ~ ~ ~ ~ b b & b ~ ~ d b d - aace b&mal th@ good and the bad effects. U n f M y , a mpt m&d d m d y to older pwpb can be d . . . 1byfwJhgsof mid n&&m a d p h p i d c- by kk stigma of bdqwte den- {OoBmm, 196-3).
The prom3 of* coslneti~ industry, including plastic and e&&c dentistry, d the pop- M t y of tbe *fit Wulry, attest to a wide- spmd-tbrat*,shriffingbadyfat,and other " M ~ ~ ' ' msy inhibit w damp per-
'
s d relationshipa, Concedmmt of age has become a p w q a t i o n of tbe Western wnrId, a fixation that seemsit0 & M Y mmm mom directly t b a ? r m e n , T h e a g i n g ~ i s m m J M ~ - t r a C t i ~ m d j n d g e d , ~ b y ~ ~ w o m e n , m o r e h m h l y ~ h ~ m m , * m ~ i n gamd suem lwi repelled by the grayins w %latWWdfbb3okman.
Society fmms an anyone, young or old, (but
Figure SZ Appeannce of the Lower two thirds of an elderly perm's face demonstrating 8 the fypiarl droop of the upper lip that accentuates the mandibular incison.

v?l;! , , ,
I ' j . , I :. , ,
I , ,- I ' .." .
, ' I , .
, if ::: ,
i i , : , 1 ' ' 1
, , ,
, '. " . 1 : 1 ' ,>: , .,; , , , , , ,
: , !< , : , , , ; , " , , : I - . ,- - I
,, , I I: I ..I,. . I , I I,.:. 1,: :-, ,,I,.,!
1 , : ' ' ,; , 1,; ,:: ,> , ,., ,, :I:, ! ,. I IN: '""I I '-1.1 '\"I' :,, , ! I ,111, ! . :I, , 1 , s , l'!P ! \ I , : , ,
Figure 3-3 A and B, The influence of the vertical dimension of occlusion on the 'yauthfu)" appearance of the face.
,&m cmdmafd of age. Appmdy, we a h h . b e w h o d o n o t h a v e t o c o v e r u p ~ d e ~ , & m q u m t I y , m e n a r e m ~ t h a o ~ &out seeking improvemen& to their qpe&rmcece BMhemm, age coxx~mhent is acwptaMe Ew W but not for othas, a clear Wcatim that &we+ are double sbndtd opmthg mtkeppbli~
Atl attractk appuarwe is considered impor- to batis is fa^^ Healthy older pmm fie-
~ ~ t W t h e y t r y h a t d t o & e l & l o o k n . A b d t h y p m q will acceptthe natirral wseqwnw of aging without undue. dhtuhnce, $Mmgh psychosoc~ pressures can came an
a-ion with appmmnce, wen to the pghtdwrex ia ~ ~ f o r t h e & s t timeinoId _= (Nicholson slnd lhlhce, lW), U d
f o r ~ r n ~ b o ~ a r a n c e ~ h with caution and m b d dimly to the
~ d t h e ~ t . h d e & ~ : ' ~ t h a t ~ @ b e h ~ ~ ~ ~ , ~ ~ - ~ i f ~ p r r t i e n t i s d e p r e ~ o r & ~ W d ' v * a v w y g u a t d e d m % @ o $ k A w , a . * ~ ~ ~ ~ t h e a S % e ~ ~ o f t l l e .&&ian and the patient offem a valuable d b g m s - hie to aprabIem, assuming ofcame that the
clinician has a r a t i d rather than a view of aging.
SUMMARY The naed for complete dentures in the Westem world will IeEmse aver the next quartar of a m- tury &pita the Durretlt ttumewes of p v d v e dentistry and $m apparent &heme of cotlbempo- racy society, Management of edmtUro08 eld&y patients involves a constant sensitivity to the w- tial impact of a r n u l t k k of msdicolI disorders. ~ ~ f e w ~ ~ a m ~ l ~ ~ ~ t o ~ l d e r individuaIs; n e v d I s s , the mouth is a fine sen- sor of systemic stability, md ommionally it offen h e f~ physical mimif&&on of a d i m . For example, the edentuhus mwth cm s* h n a very p d u l m k of dingles invO1vhg mmory ~ o f t b e f r a c e , n e x k , a n d ~ a r d i s p l a y ~ - lar c m t i s with a denture-* amlatitis w- d y w i t t m t ~ ~ d s h e a l m o r e ~ l y and possib1y less @ecthly in old age became of d m w i e d k n n m o f c e b o r p o m b l ~ cirmIa- ti~n. Com~quently, the mucosa and &lying h e suppdng complete d a t u m hmi more dowly from the trauma of ill-fitting denbra.


! b ! h U k & k n & ~ d o f ~ ~ Wa &-& IG, k PC, BAm &fp &.C%oaa; gggp&m.gP,J-aarc-m

Sequelae Caused by Wearing Complete Dentures
THE DENTURE IN THE URAL WWRQNMENT w t of a rm&b psibe& in oral ~ p F S d u ~ e s p ~ ~ ~ s O f t h e ~ e a v i - ~ t ~ m s r y h a v e a n ~ e E e e k o n t h e
of the oral ti- (Box 4-11. MucosiaI mctims wddmdt bin amechanical MWion
the damns, an on of microbial plaque an the d- or, m i o d y t a toxic or ~ d ~ i t o c o m t i ~ o f ~ e h t u r e ma&id 'J[Pme c~1tinum m&g of dentures may haw a negatme effect on residual ridge form btmmM of bone mmpin. F ~ e f m m , \nvearing; c o m p l e b ~ b u r e s thatfunctimpoortyandthat imp& nwiwory frmction could bt a wgative ~ S p f t h E g a d t Q ~ 0 f ~ m ~ - & fundion d nutritiwal stam, prkalwly in older-.
T h m a r e ~ ~ ~ o f t h e i n ~ o n ~ t r l e ~ ~ ~ ~ ~ f a l ~ ~
W a c e propaties of the prosfhetic materid m y dfwt plaque formation on the prosthesis; h e , the. original s d a a cbmhtry af the
matorid'is modified by the a q & d geIlicle a d thus k d minor impmtm~ce for the e&&ILbent of plaque (Box 4-2). Qn tbe con- Wry, surfme irregularities or mimporositiea @wly prom* flaque m w m by enhlc- ing th ~Brrrfacce area apased to mimMal calo- &&on and by enbeing the mchment of phqwe- F u r t h m , plaque formation is greatly h f b m d by mvimmnmtal conditions such as $le dew of the prosthesis, health of adjacent
m u m , compo&tion of dm, salivary secretion rate, ol.et hygiene, and denture-weadng habib of tbe patient.
The presence of diffbrm Q p a of d d mat- in the oral cavity may give r b to elec- trochdcaI corrosion, but c h g a in the oral enviromnmt due to bacterial p l q w may cawti- tute an important cofactor in this process. C m s i v e galvanic c m e w have been ipipIicared in the burning mouth syndrome (BMS), oral lichen planus, and a k e d taste pept ion . Moat often it is dificalt to establish a deTmite c a d relationship because mechanical irritation or infection may dm be involved. Fox &hmw+ I o d irritation of the mwow by abe m y incmse m m d petmeability to dIqens or microbid antigem. This makes it diff~cult to dis- tinguish be?mm a simple irritation and an aller- gic reaction against the prosthetic material, microbid antigens, or agents absorbed to the prosthesis capable of eliciting an allergic respam. The matter Ia further compliatetl by the fact that certain mimorgmism {e.g.$ yeasts) are abh to me. metbyhdumylate aa a cttrlqm some, tbarcby musing a chemical &gradation of the denture resin.
Z n t b e ~ ~ n s p r o a ~ a n d t h e odmucosa ,micfrobidp~may~impmtant ne@w or hmdd dbts (QUIZ 4-1). Thus a prosthesis m y prom& infection of the underlying mucosa, d e s , and ~ m t d &sew adjacent to overdentme abutments, periimplant @gkkh, and chedcd degradation or c m i m of pro&tic materials.


wagnds m ~ ~ o f ~ ~ ~ s t o m a t i t i s i s ~ d t g f t b e ~ o f m y c e l i a c a ~ o h y p h i n a ~ ~ o r t h e isohtion of Cad* specits in high h Ban the leaions (250 wloniee) (Figure 46). U d l y , ~ a m r e # v d i n h i g b O r d e r s ~ t h e fi* surface of the dmuC4x3 than from come- - ateas of the palatal nmosa. This indi- cates tbat cadido miding on &e f ~ ~ a c e of the d ~ i r a ~ ~ ~ ~ f b i n f & ~ n .
Eti- ,id Wdhmlng Factm T%Le direct ~ ~ f b r ~ ~ ~ L @ ~ ~ f & ~ & - t h e M a l wdty (Baa b3). This tb iu%shn pmaih in ~ * r r e e ~ t h e i t ~ ~ ~ a r # l n i g W t b ~ W i ~ i f t b ~ ~ m - I t h m * w * a - t h e m j # p t w t o f * ~ ~ o f ~ p ~ ~ ~ ~ w ~ k ~ ~ ] j l a & l b t i o a , t r a u m a d d * b ~ ~ f * palatal q i W celf$ tlteffrby reducing the d e p o f ~ & h b a r r i € ? r ~ 0 1 1 o f t f t e s p i t l l e ~ ~ ~ ~ o a o f ~ ~ ~ rial anti- am t a b place mom mdy?
Tfie m 1 M m of the fitting denme adwe b y C Q n d l r d a s ~ e s d g i p e n d s o n s e v e f l J ~ , inch&& adhemwe of* W, -with o r o l l ~ b a c ~ & * c r f t h e s h , a n d ~ ~ d $ b w r y ~ c r e s h T h e
poor oral @&@a#$ b&$3 a m - hk *-*@dm- wmrbg,Ttge--htElgam@
suacu@&biy to ~~~~ den- stom atitis m y be aging, mhmtdtion, hmmmppm- ion, -on -, diabetes ~Ui tns , and possibly tmtmmt wilh antibterhl mtibiotics,

4
ChWw 4 Squelae Cau& by Wearing Complete Dentures I
Hg~m u A, ~ y p e Ill denture stprdth, papillary hwerplasia, the d u b r type. 0, Type Ill denture StMllgtitis, papillary hyprplasia, the mossy type.
b IJ F&re 4 s terions of tlrr! mucm in patients with Cmdidu-maiated denture stomatitis. A, DDrffu5e atrophic glossitis. 8, Median rhomboid gtwsitis. C, An&at &titis. D, Erythema of the soft palate.

F Part One On Being Edentulous
A 8 F b m 44 A, Culture on OriPufey: Ilrft, positive culture in a rroddedd wier of Csd* &ht, hi* number of yeast colonies from a patient with denture *matitis indi- * a Gad!& infection, B, 5mar from the fiing d m surface yWd4 pseudamydum.

Clwhr 4 Sequelae Caused by Wearing Com pktc Dentures

* Meat B n ~ n g ~ w r s
44 &Type Itl denture dmatitkshowing mdular M s i a with sewe infhrnmatian. %, After on!y a 2-wdWmmenf with amphoteridn 8 which are usually pmdhd fpt 4 weeks, tbw! #y&em has declined, but the hyprphda has pwshd,
dabby Ridge Flabby xi& (ie., mobile or extrmdy mht ~ * ~ ~ ~ t o r e g ~ O f ~ b y ~ ~ . I t i a ~ m m t ~ i n ~ ~ o p ~ d ~ ~ ~ ~ ~ a . r e ~ ~ m e & I m t h e ~ a , a n d i e ~8secp%bdm&IdM~* $ i Q & * a e r n J d mlditim 4-91.
~ ~ ~ ~ r i ~ % ~ ~ L ~ d ~ t h e V e 8 t ~ m ~ b Q
A wmnm m p k afwearhg ill-fitting htms is * OFF-& BS h t w hyperpbia qf the mucoasa in G Q n W with the denme b ~ * pigun% 4-10]. T%e k b are the muh of c h m l k , ~ b g r - l b - ~ ~ b y t h i n ,
<um flange. The pro- *f ti- m take p h rewvdy qaicw *
placement of new & n m s and is nemdy not w&wd with tqnq-. The lesiom ~ b u ~ g k o x q u i t e ~ a n d a r e m m - posed af flqw of IgperpWc connective tbmc, Jnflammation is variable; botkevur, in ~e bottom of deep fiames, smm -on and alcmtion m y ocew.
~ r e p ~ o r ~ t o f ~ ~ t h e M a t m & m d ~ q W d p d u c e s o m e c ~ ~ o f b ~ ~ m g i d ~ ~ ~ ~ a n d r % p ~ o f ~ d e n t u c e , b ~ m ~ l y ~ ~ ,
When pmmm u b d m s dewlop d irrita- tion fbm mhbial products is severe, the patient m~ 3lWhd disGomforL p b d m p # y i 3 ~ t , f h e * ~ b a ~ l & w ~ a a a o p ~ ~

4 -at Caused by Cwnpktc Dmbw 41
~ ~ ~ , o r o r x e r o s t o m i a ) . I n ~ B y s t e m i c a l l y b sore spots QVU heal a few
1 Om1 Cancer in Denture W ~ I P T S A t l ~ ~ n r a l ~ d ~ c i r r i ~ m o f ~ ~ ~ t h e ~ h a s o ~ b e e n ~ ~ ~ n o W m i t r : p r o o f ~ t o ~ F w 4-12). WIG rqmts have detailed the devel- opment of oral carcimmw in patients who wear ill- I I ~ d ~ m ~ ~ $ ~ ) ~ * fitting d m ~ o p dentures. in partially ~owwm, or tufa~y mait Exhmhus ora~ caDcan patients, do The rsaa~ms appear to include m msociatim with
Figure 4-10 k Soft tisue hymbsia of the maxillary wlws. & T h e h a W o n is mured bf chronic irrbthn by the denture flange. C, Fibmma psoduced by the l i l denture Range.

P
' -mC.ll k , A N t e u u i ~ p m d ~ ~ t h e m ~ x i f l a r y d e ~ r e i n t h e h r n u ~ r n P t c R region d i d to the tuberosity {am@, B, Wi h r produced by the lingual denture flaw.
I J L 1 .
BURNING MOUTH SYNDROME BhdSmnMkr~Lof&ntumwdqsf ld is t-.&*,- dm in me or ~ o w a l a r w t m s h m ~ w i t h t b e d e n - hms. lthdmao- b8twuabrrm- @ a n d B k 1 9 . b ~ ~ group, h -8'8 oral mucosae we often ~ d ~ o f ~ c h W h i # h , h f ~ - d n , o r m ~ I & g h a C t i m . i n ~ * m s , ~ ~ m ~ ~ * ~ c M y ~ y y ~ W ~ ~ Q ~ , ~ ~ ~ ~ BMS i8 older Wn 50,- of a@, is fanate, aud weam oomp1W den-. In the e&atU1ou#
Figure 4-12 A, Basocellular carcimrna of the floor of the mouth, early stage. 8, Carcinoma involving the alveolar ridge and the vestibule.


qgmt e~hinition of the fm. T h patient's ~ & o o l d ~ b e ~ ~ ~ ~ b u t w - h w - h w wal3nw with ~~ wEmbwM, ~ b d e d o a t o n l y a i r a ~ v e e f m r t ~ ~ ~ ~ d ~ s r t ,
Th~gagdexia amma&heaItiy defemernech- auh, Tta function hi to m t foreis bodies &#gatahgffietrackG&ngmbetfig~ &by tactile Stimulatio~lof themft*, th$
part of the mgm, and tba bees. ather sbWi wch aa sight, We, noige,
~ t s w e l l a s ~ o ~ f a c b m , o r a ~ t i m o f ~ ~ ~ ~ . l n s e & i w p ~ t s , ~ g m r g r e f l e J r i s ~ i l y r e l d a R a r p ~ t o f mdmtms,bPtit usually dhqpears h a few ~ a s ~ ~ ~ b ~ e d e n t u r e ~ . ~ i s t e n t amphints af gagging may be due to amextended kadatas@iptlt7*&-partafhd- k y and the ~~ of the
LongWind sntdie of tbe form aad weight of the ~ ~ r e s i ~ ~ i n ~ ~ f c o m p l e t e h t u m hiwe demomtmtd a G&WUS bass of bone htw after tooth extndofl md p h m e n t of cwnpletc dentures, The reddon is a sequel of alveolar remodeling due to altered functional dm- ulus of the bone tissue. It foUows a c W c pro- gm&e arad kvere~ ib l~ c o w that oftan & in ~ ~ a o f ~ ~ ~ m a n d d M 0 a ~ 4 l 3 b ~ ~ o f ~ i @ c u I a x i y ~ i n ~ w i t h t h i n ~ d bane(e ,g , , thE~BLbdl&bia lpar t so f the~ and tb.e lingumrl of the mandr'ble). a the f i r s t ~ * ~ ~ o n , t h e ~ ~ n a f ~ ~ d l I a l r i d @ f t e i * i t f ~ ~ p ~ i a r t b a r r t 2 t o 3 m m f o r t h e ~ s a d 4 t 0 5 ~ f o x b man&e. Aftm h d h g ofthe midual ridge, b r e m & ~ ~ d ~ b r r t w i t a W d i & m & y . h h d k s r m d & o f * -
u J-13 A, Severe midual rldge reductIoh--a sequeb of w r i n g complete
4 !&@m wer wed 'years. & N o i e tlrc b t h n of the mental faramina near the top of the &tea1 r*.

I ~ ~ i n h e i g M i r ~ 0 . 1 t c O . l i m s ~ i . ~ . : 4 w ? h e B k % & h e h e ~ ~ B ~ , **- . .
mw- t: ~ ~ b o f ~ ~ ~ * ~ ,* *d I l m l e M 4-5). It is d ~ & e ~ a f ~ ~ ~ e ~ m ~ t s . .b a m m b W ~ a of
redactim of t i le tlldlhI8 0 small goni&t angle (I.e.,
k m m d mdibdw b m bend a d a postdm of the lower Wid dgm b reladm to
b.aQYl)* Women are p&iculwly flreqtmq rtnd extat of.midmd
I on, and it hm been suggostd b t @uge&w loss o f W u m k dentures is a martc
fa& is a slEBMbsr#ededc-
h.&mmmipidr&Wrldge -*a- hr@irltik-
l l w m c h d d ~ ( i , e . , ~ u r ~ ~ a a a l ~ ~ ~ t t a d b y t l a e ~ a r ~ t c m g u e t 0 ~ ~ T i d g a ~ ~ e d w k ~ t a u t ~ i n & m w k b g p w x m T l n w a ~ ~ ~ b e t w e G n ~ ~ o f ~ ~ ~ t $ e ~ o f ~ a m d E b e ~ * ~ m m i m p o n i s a t i n ~ ~ ~ o f ~ t h s n i a d a y ~ . ~ & b l t g ~ ~ ~ i s t a a ~ e 9 i k ~ t b ~ i o f * d e n - ~ a r t h a t ~ m * h a r e : M e ~ - o f & G T Z o n ,
n W m ~ @ f * r i * & w ~ ~ 1 ~ 0 f d ~ * 8 Q b ~ w i t h *- of the lnusde a t t a c w closer to h & ~ f b ~ ~ ~ ~ h B ~ Q f & C d C d G b u l s h of on, duction of the r m w k e hui&aadormt&mofthemandible,& iTuxwle k reA&iV% pmgdlia; *m in m* dmiar rids& ~~~ &r pmgewion oftbe resi&dmMon,*b-- t r i p Q t a l i a ~ ~ ~ ~ , i b b e
t m d = l J b ~ ~ ~ * d ~ -a **@kt w--
~ d ~ 0 f ~ ~ W ~ ~ t O theh=pofthadW*
A b - l M ~ a @ h ~ t i c m w i & ~ e n d t h e ~ ~ a f t b E r # ! S i W * L l a o t ~ ~ ~ , in l m & ~ cosnp1e w u r e wm8mrf3* ths -- p h w - , d * - & * d d - . . I f i ~ ~ ~ w ~ ~ * ~ t m h w t r r ~ ~ ~ ~ f and retention of new den-. T d t h a l l y , them p r o ~ - ~ ~ b g r p t e ~ ~ p r e p r o s - w i c 8 * i p i i * ~ b f s ~ d a * ~ ~ ~ d ~ m , i n ~ ~ m t i ~ , B y p e - W l ~ ~ ~ ~ ~ . ~ ~ ~ h r n r e b e e r r * e c I i p ~ t r q . rho hmdwtbl of the 0 ~ h ~ mhmque, w h d ~ i ~ a t . t d
t W & h = t u & W n E s = Cswa and ~ h n P o l D & m ? m ~ o t w h x t c d teeth to $eve aa abut- ~ ~ ~ d m t u x m i s a n ~ ~ t p r o d m h t i c technique (sse Chaplur 10) pigwe r E - l 4 ~ . ? n t h h ~ ~ a f e w & & h i n a ~ ~ ~ g m d p e s i h a r e ~ m d m ~

madwhticdy Woxe the cmwn is modified The ~ ~ ~ a n d ~ w r e f i l l e d w i ~ ~ o r a e o ~ i t e ~ ~ . I n t h i s ~ ~ ~ g d o n t a u y ~ ~ ~ ~ a n b e ~ e d ford~teatrsinarelctiwly shpkway, ~~ mttaue& not n e c m
~ ~ * d ~ h n i ~ f 4 t i l ~ ~ ~ d e n - ~ ~ m l w w f ~ ~ . H m w w r , t b e ~ o f ~ s i s ~ ~ w i t h a ~ r h k o f c & r i a s m d ~ o f p e r i a d o ~ diiaeaereoftheabumatee&.UneofEberaasons fotthis i sWthehtd&d~t ionbeneatha ~ ~ f t ~ & t a m ~ ~ a n d g # d ~ % d o f t h e f w n g ~ s ~ ~ L g ~ ~ ~~~. Onemumtiisthatthe ipmtesof
d A * m p s preduuhw in d E n t u j e p ~ a w w l l k n m f o r ~ i r ~ o r ~ MWims b dmtd plaque on moo& mum1 sm-
f~,aa~~~08ZGIOtcwnenkrm.M~- t w y p o m t i a t o f ~ ~ i s i r ~ b y B h e fm&g tlpat plaque (in which
3 d a y s o f p l a q u e ~ g ~ ~ ~ ~ ~ i s ~ T & s c ~ ~ I d ~ ~ i t i s d i f f i o u l t t o m i n t a i n h d t h y ~ ~ c&itb$-t to a v m d a l m a b ~ . - ~ g f e a - W e of denture plaque flora is its hj@ pmpda18 of lactobacilli and Stnpt~cocm mu&iw1 which muld explain why c& is d iMdt b mntml ~ u s e ~ ~ ~ 0 f a p t 0 3 0 O J o ~ l ~ ~ been obwmed in patient8 waaring medmtm%.
For the of weadenhms to be @mu& eff& prav€mb of caries aad peri- & easewisn~,Tkprinc ipdaimofthepmm- t i v e ~ ~ ~ u I d b e t o ~ I ~ d phqw ontbe e x p o ~ & n & ~ o f l i ~ e ~ ~
C F@m 4-3 4 k, Complete wdetltures in a patient with muftiple aplasia, B and C, The I
datums haw been in piam br a5 years, and the remaining teddrook have prevented I
midud rid@ reduction. I


E p $ d r m m (B C h @ a 6) Aging is OM d a t e d Twfth a signifiant dm- fn energy ~ ~ t 1 ~ ~ o a f r ~ ~ h m m t e ~ ~ ~ ~ ~ ~ T g u s a 3 P h ~ - i k n j a ~ d W d b d ~ i s
by a 3003 &tion of f d intalce* >with the exception of mbohydmW the
~ f o r ~ ~ t l l r n n t r i ~ ~ ~ ~ s i g a i f i c € m t l y w i t h a g e . A $ e ~ ~ ~ ~ ~ b y ~ w w
rwah evidence of befichch, whi& $ ~ ~ W t o t k d ~ c r r p ~ ~ ~ . !Wea mtriticmd d e k i d e s am w e smmg h e a y illwdl&, even with paor &* ~ ( g t , ~ , i n c W ~ ill 0rJlcaPwd @at9 nu td id defwimias are hpmt. h * p&iiwEi, fmm & m m-fitting danm, ~ ~ ~ ~ ~ o r - - w -
- M 4 M k M q r n d t r r - Onsof t h e m n p d k & m f Q a m w c w t bBom--,In,tadle-,
ill@ il3 fox'= m d -
h . m b s k ~ * ~ h b b e - a g # i w a @ & y 5 0 * M d a m n l q ~ h p E w h d y ~ ~ d g u f ~ b cbwwg-@-~w- ~ ~ ~ ~ ~ ~ w i f h e ~ i h a - t i m ~ ~ t e e t b ~ t . T b e r e b n o ~ ~ ~ ~ ~ E i o n c o u l d b a ~ ~ a 6 f ~ ~ . ~ , ~ ~ ~ h m a ~ ~ ~ d f a t a f t d a ~ ~ t i a n o f m f & d a l m r i W b o f m & i c d ~ ~ W i t h ~ * ~ ~ t h e ~ w m*. NMddmaf Status anel Mastkatory F m c d ~ ~ ~ ~ ~ ~ - t o ~ ~ ~ d ~ sm&hid%tawdfflearers of^^: ~ ~ t i o n a n d o p a i l h a s t l l b , ~ ha&, mciwmnomic sWq and U C . In ~ y i n d i ~ s t b e r e i s n o ~ ~ h t t b e ~ i n ~ ~ ~ i t e d i n ~ o f c o m - pbb-wtbatrep1mt of i l l - f ~ ~
rtum WMI ~II-fitihg new demhms will
a q i o r h i p v m a t o f n ~ h ~ - ~ ~ 3 0 m e a m d h t i g n a f h m d i & h c o u M t & e p h e & p r ~ ~ b e c a ~ s e ~ e ~ t s t m e l i l r e l y t s ~ ~ m ~ d t Q ~ x ~ w e ~ ~ s u o h ~ ~ - . & d f t w i & .
m&-of-e-- t i m ~ ~ ~ ~ m ~ ~ ~ w i t h p w r ~ ~ p ~ w ~ ink&&-,d*-m ~ ~ , ~ ~ ~ ~ ~ - i m g ~ u a t i w h a s r n q g a t h ~ o n ~ a b i l i t y a a d e E i ~ ( B m 4 4 ) .
F o r t 5 2 e ~ ~ d ~ ~ ofthe n ~ ~ ~ J t ~ o f t e n ~ ~ t o ~ dietary habits. This r d u d m of d M y &&m ~ ~ k e v e r y ~ f c u l t ~ 1 3 8 e t h a i r ~ h a b i t a a m o ~ m f ~ f i x e d a n d ~ h y b a u e a d c m d appdh. In dditiun, poorly adapted -maatt@-*-imfmnred dbwy lmbits* M-4 - d m d fwd b t f o r e e a t i B g ~ h r p ~ t i ~ ~ d ~ ~ influam on food selection. Ehwmur* it will not S t i m d & ~ d h m r n * . % mhtwawa orrewhbhmmt of QFe3 beattb and ~ ~ ~ ~ a n ~ p a r t d
Assaciatims among Xerostomia, Denlure Wearing, Impaired Masticatory Fumcth, and UndemsytritJon in Frail and
Dependent OIder Pemns ~ e d u a d Stknalaited &Pwq flow Rate Assodated wlth: Complaints of x~mtomia Chewing difficulties Complaints related to wearing urmplek den-
t u r s Increaed number of chewing Eyrles befife
swallowing Lass of appetite ~Pduted %rum albumin level R e d u d body m a index Reduced skinfold thickness

~0-
CONTROL W SWUElAE WITH THE USE Of COMPLETE DENFUES & - c a s a i a l F - ~ f ~ - P ~ ~ ~ ~ 0 f ~ ~ W r i ~ l t n d p a t h ~ ~ ~ f h d ~ . T h i p ~ & ~ ~ p s o r ~ e n t ~ ~ - th Opthe mludon, m c i e n t b- t & @ , d - c p r o b l - * w , b m mrrynotlmabl~tuwmrdmtwsaadwillwoeivea
m~tb &me wqwl$e of ridge . ~ b b e ~ ~ f o U ~ ~ b -&?I&


,I I I I' I(
Temporomandibular Disorders in Edentulous Patients Thuan Dao
Temporomandibular disorders (or TMDs) is a col- subjects, but it is certainly not of the epidemic pro- lective term that is used to designate a group of portions reported in earlier studies. musculoskeletal conditions affecting the temporo- mandibular area, These include muscular condi- tions, such as myofascial pain, and disorders affecting the temporomandibular joint complex, such as disc displacement disorders and arthritic diseases. The term TMDs was introduced by Dworkin and LeResche (1992) and replaces numerous misleading terms that were previously used.
€?IDEM IOLOGY OF TEMPOROMANDIBULAR DISORDERS IN EDENTULOUS POPULATIONS The reported prevalence of TMDs in edentdous ppuhtions appears to vary considerably, ranging &om 0% (LoiseUe, 1969) to 94% ( A m and YiIdund, 1989). The wide discrepancies abswved are largely &o to differences in the criteria, or the taGk of specific criteria, that were used to ddne TMDs. Although the prevalence of TMDs in the h t u l o u s popuiation still needs to b ascertained, &I app isa l of the epidemiological literature on TMDs and related symptoms from different popu- l & u n M studies reveals consistently that it is primarily a condition of young d middle-age adultg (mainly female) and that its prevalence tends to diminish in the older-age p u p @e&&e, 1m1 where @a1 or complete -rn pre- vails (Macmtee, 1985; W m I Watkins, and C h e q 2002). These obsemtipns suggest that TMas are encounted in elderly and edmtulous
ETIOLOGICAL FACTORS The presumed association between edentulism and TMDs resulted fiom the traditional mechanistic notions that tooth loss is a predisposing factor to mandibular dysfunction. This association has been further reinforced by reports that the severity of such dysfunction is positively correlated with the loss of occlusal support and the number of remain- ing teeth or occluding pairs of teeth. It is therefore not surprising to see that the loss of vertical dimen- sion of occlusion has also been assumed to play an important role in the etiology of TMDs in elderIy and edentuIous patients. However, if tooth loss or edentulism is a direct cause of TMDs, the preva- lence of TMDs should be higher in the edentulous population as compared with the dentate one. This is clearly not the case, and in the Iast decade numerous reports have refuted this assumption (Bibb, Atchison, Pullinger et al., 1995; De Kanter, Truin, Burgersdijk et al., 1993; Gray, McCord, Murtaza et al., 1997). In addition, the lack of cor- relation between the humber of remaining teeth and the prevalence or severity of TMDS has been rqeatedy reported (Bibb, Atchson, Pullinger et al., 1995; Tervonen and Knuuttila, 1988).
Although the effect of the dentition and eden- t u b on changes in the temporomandibular joints (TMJs) has been questioned, an age-related increase in the prevalence of degenerative diseases is a well-known fact, whether in inthe TMJs p a se (Pereira, Lundh, and Westesson, 1994) or in other

My joints $3owq ZOUi), WOW because ~ i i p m o r P t ~ e n t a m o n g o I d a p e r ' b i o n s , i t f - ~ b ~ m t h l F t t h e - o f dqmemtb &sews in the e d a t r J . 0 ~ ~ popdatiun i s m m e ~ t o b e ~ ~ ~ ~ w i & eda&m itgetf.
A @w &dies have reported a higher p m - h in edentulm versus dentate s u b jwb. H m w m , the data eiwr were not ab4mWed by stathtical analysis (Temnen and KnWIih, 1938), or group differences failed to & *tical s i g n i f i v (Hmhan, Snow&, Mmm et d., 1990). There me also compelling data thrtt TMkehed sigu and symptoms are mild in e c h h h w mb~mts (Bergmm and Carbon, 1985; Lwxhq ~ , M ~ e y etd., 1990; Rtwtk, PeItoh, and Salonen, 1997; Wdding and owlen, 1987) md me relatively law' in the wha do not
B e n t m s (Wilding and Owen, 1987). A lack of a b r & t h betmen the severity w p e n c e of TMI3B ans e d e m - - w fwm (dlmion,
+"ty d number of m q h pmdmes, d e wldon+entric mIatiw c&cidmm, and d e n t u r e ~ m m d ~ t y ) h a s & o b € a l ~ - quently r e p t d in rbe Iimme @Bb, A t c W , m g e t at d., 1995; M a c h , we&, M&n et d, 1987; bwth, Peltoh, md bbmn, 1997). W w ~ c e , ~ ~ ( I ~ 7 ) ~ M , ~ - &on b&mm the ciiical signs of dysfhwion and w1d M g t or denftae &. In their search fw etiologid f&brs for TMDs itl H h t l l - Ions dentUtewearing patients, FauIkner and M e (lm) failed to show signifloant associa- ~ ~ ~ m r m b e r o f ~ ~ t p a ~ ~ txmplm-,ahearge#f&ehm+ ween- t t iG a w l u 4 i d rewtnl ~ ~ c c , and ~ ~ m r r n e l ~ ~ . ~ T h e I r d t i s w n - ~ w i t h z h e ~ t ~ ~ v i m t h a t questions the role af mMon in the pathophysiol- ogy of m a e , Z(101).
Mmw d~fogical concepts have nsw h m wli@ by biological vwiablas, which W& ceII&r, mlecdar, nmmphysrological,
~ U U U ~ ~ , 4 genetic ~ u f j o i n t d i ~ . ~ m f ~ e r n d
c h i d and basic science d.
~ a a ~ t u r s o f p a i n d i a f l a m m a -
t ioninarthr i t icp indin~11f l intheTUJs I hm m e i d incmshg attention (Kopp, 2001). P r o p o S e d n e u r a I m e c ~ f o r T M D p a i n n o w b1ade ' * in mttd inhibitory niacha- ~ = ~ r n a l u l a k d b y p c d p h - e r a l ~ ~ t ~ a n d ~ ~ i n ~ n e t * v o w s y & m ~ & a t ~ h e t m p d prom& of pin (Makm, Fillingim, I Booker et d., 1995). In the case of mle-related TMD$ m i h t i o n of peripheral tissues, n e w I
plasticity in pronaciwpthe and antinociceptive cir- , clrits, and behaviaml aeaaitizatIon associated with 1 i n m a d mtionality and with pain-specific mu- roenddne md autonomic reqmsivity have been a h been m i d (sbbler, 1999). Same newer lines of evidence atso suggest that tbe above pain systems may IW >e by the female hor- mones. One such example is the interaction between e d q e n and mumadim a* i m p l i d in h t h peripheml atxi central pain procmsing maimisms (Dw, Knight, and Ton-That, 1998; Dao and L~Resche, 2008). Momwx, the use of exogenous hormones (e.g., d conimepbs and hormone replacement therapies) has also h e n qorted to be associated with increased rish for TMDs, and a dose-response relationship was a h evident (LeResche, Saunders, Von Korff et al., 3997). The role of female hormones h h e patho- ptrysidagy of TMDa is an aitirmg resea& area; however, it mu& IM r e a g m d that the etiology of TMD conditiom is still unclear.
MANAGEMENT OF TEMPORO- MANDIBULAR DISORDERS IN THE EDENTULOUS PATIENT The dental approach to TMD m.&nmk m the eden- tuIous patimt bas tmditimdy consisted of 9- mizbg the stability, miaticm, and occlusion of the complete prostheses. This is still zt vaIid approach to the adjunctive mmgment of the TMDs. However, this d m not imply a presumed oecIusal etiolagy, M m e d of T M h should p h a d y be dhckd toward p l W o n of the condidon, The gmidelhes for ~~f are weU s u m m i d ia the offwid alcientic Infomation Statement pub- lished by the Atmriean Amciation of Dmtal R e ~ m h ( m e , 280 1 ).

Uwpbr 5 Temporomandibular Dborde~~ in Mentubus Patients 53
I ' ~ m R I t h e ~ c h i c d c l i r r i c a l & [ f TMDs]. . . it is s t rw$y &at, d m thm slre spacific and justifiable indica- t i ~ t o t t a e ~ ~ ~ b e ~ o n ~
cmmmiw &rev&& &empetdie . W E h no -c brapies have
of the condi- atld until dmlopment of specific tbmpies,
mmct and prudent consemtive ctymptomatic p a g m e n t of TMDs in drmtur~ wearers M d Ore h i k to the management stmkgies prescribed &mest TMD patien% p his includes patimi miu- ~ ~ ~ ~ c e a b u t t b e b e n i g a n a ~ o f & condition, selfam, short-term phmmmther-
19973, and'c&&tive and be.haviod intar- won oworkin, 1997).
went education, medications, oral glints), tfiie former patiunb &awed s i m d y chcmwd pain, d d pain-related activities, I redud number of paMd msticatoxy m w h , and reduced a d d i t i d visits for TMDs baa- IDworldn, vugghls, W h & f , 202).
P-pymyh- whenthepvi- ous strategies fail to kcrase h e patient% comfort lever. Far - pin statem, ~~ !no& corn- monly p m d i i medications with d p s i c - d m , as well as znlwcb m b t s , ms- anti-inflammatory b g s (NSAlDs) , and the recently introduced selective cyclooxyg~c-2 (COX-2) inhibitor These medications am pdcu- larIy useful for the tmdmmt of &tic cwditiom invohing the M s . Patiah should be f o U d clody for the titration of the medication, to enstm r a d e q u a t e p a i a ~ l d m i n i m i 7 a r n ~ t e d ~ i d e effects. It ia impmmt to note that although the h t e n n e m of t h e medidma is well ~~ their long-tam efficacy h not well dommaented For @tent and nampathic d- d p a i n , ~ e m e n t w i t l l ~ ~ a n d opioids may play an imporlant role. As for other m e d i d o m that are pmdbd on a long-lmn basis, howwer, the Urn Wwtxx~ W thettrpeu- tic benefit and toxicity should be carefully weighed, and their nlfminibt&m &add be sup- ported and coordinated with he family physician or a p&n spechist, The dentist should additionally be a w m of the potential intewtias of tha p scribed medications with other dmgs that am d by the patient for comwbid conditions.
A wide range of ph$ical modalitim can b mag- gested to patients, including the use of hat rrnd cold therapies, ul-4 rtwaagc, joint rnoBiliza- tian, and passive &etching, and can be &mink tered either by the patient or by a clinician. Although local heat application is widely wed fm pain relief, its benefit has ken questioned because raised kqemture increases tissue inflammation. On the other hand, the superiority of cold mer heat therapy for reducing inflammation and welling

~ ~ d o ~ ( ~ r e v i e w b y F e i n e d W 1997) Ahugb the long=km &cotcy of physid mdditie8 for m d u h l pain con- d i t i u m h n o t b e e n ~ ~ ~ ~ , & o@&dshort-livedbemfiiinpmvidkgpainrelief jw their we. as pdiatire maurea far TMDs.
TMQB a n RI%W the &nidon8 and elddy p o p hihi, dtbqh their pmalmce and severity do t E O P ~ ~ a f t h e d m E a t e m b j ~ i n a l ~ w e r - m. The shift fiom a mechanical etiological
~ ~ a m ~ o n e , i P c ~ g e m p ~ m ~ p d b b stiS1oghl role of f h h b m m e s , bas ~ ~ l n a hifi ia t m h m t focus. Although pmihdu& hmtm~nt mms at acM- o@md
mbd improvanent-of dK pht% orofa- ewmmfwdhtiion. theinterventimDwsek
Diottria ICA: &lpsit treahenb for d i d e m W ~ ~ ~ t k r J P a a h U I O w l ~ 1 ~ % 3 : 1 5 4 - I 4 & 1997.
~ S P : ~ ~ ~ ~ ~ S k a $ QmiAaedCkalpplfpOlOnrlffPdBd~$3:I2&133, 1997997
~ S F , ~ K & W ~ L s t a l : A ~ c l i n i - d c a l ~ ~ ~ ~ f m # m g o r o - ~ 8 f ~ I l ~ ~ ~ o e ~ f a e a M d f m W m ) s - p g ~ ~ , JO&aeM 15;68*63,2002.
D t # o r k i t r s F , ~ L : ~ d i ~ ~ c r I ~ f o r t w & pmm&ndiMr dlaprdem: r t u i q d t d , 5mnhaIioils and u p h a t i o m , mifiqm, J Wom&& D M Fadd Od M &MI-355.1992.
F a u b w KD, MD: AetM&csl facm of csen- i w n a n d i b u l a r ~ i n c ~ y ~ ~ ~ ~ c l e s $ r b mwhg p&&, J h I R&5111243311, IW*
F c i n e J ? 3 , L ~ ~ A n ~ t o f t h e s E c w y o f ~ ~ a n d p @ b I ~ f w t h e c o n t r p I o f ~ c t n u d a b M p r r i a , M 71543,1997.
~ R l , M ~ J F , ~ G a t a t : T h B ~ o f ~ ~ - ~ ~ ~ ~ c w n p I e t = ~ ~ t o ~ w i t h a D a t c a a t ~ d M I , B ~ J ~ ~ ~ W 9 * - 1 [ 1 3 , 1 9 9 7 .
l f r a e n e C S : T h B ~ e g y e g y o f o f a r '
inrpu~* hmt - t , J *M i 5 : s r r o E & 1WI16,ZWt.
Harrimaa LP. Snowdon DA, M e LH et 4: %mpm ~ ~ j o i a t ~ W & c k d h a a l t h p r w n & m i n t h a ~ W ~ ~ M d U t u l ~ 7-13, 1990.
Le-b, Sanad#sK~brEmdal: U r n o f a m ~ l r n d o t r i k o f ~ * p a l n , P& 68:153-160, lW,
W e t l e W J : ~ ~ ~ r O ~ f o E a t d y s f d h t h e ~ u i ~ 3 A a p ~ h 7kl45446,lW.
L d E m T P , s a m g g 3 R % ~ m & & m & ~ ~ ~ ~ p a t i ~ , J ~ b m o r d 4 : w , 1990.

~ M : a f l r w o ~ ~ o f * ~ k ~ 8 p s . m& hiom, C!#r ~&InRkiwwami 13:44741,2001.
Stohla CB: Mde-relatad ~~ dbmb, 13:m-m, 1999,
~ T a n ~ M : P E e v a l g l o t o f ~ M u ~ o f ~ W ~ ~ B r n o a s ~ ~ d Z & ~ % M & 65 pars in WmWmia, Fmhd, I 15:455-463,1988.
W a a a n n , W ~ ~ ~ # r n t & T ~ m i n t b o r w T y oEd: I3-1S-year incidence m q ddsrb Imam, CBmmvnzry Dew Otd E@a&fd m29-37,2002.
Wil- RJ, Owes CP: The of t e - b joint d y m in ~ O U B aon-btnro we&g M- viduaIa, J W Re&& 14: 175-1 82,1987.

Nutrition Care for the Denture-Wearing Patient Mary P. Faine
Enjoyment of food is regarded as an important d&miwni of an adult's quality of life. Loose teeth, U s m , or U-fitting dentures may pre- clude eating favorite foods, as well aa limit tht intake of emmM nuttieah. D e c r e d chewing ability, fear of c h h q while eating, and irritation of the oral mucosa when food particles get mder dentures may influence food choices of the denture wearm Cmmmly, the nutritional slatus of a patient with dmtum affects the health of the ord tissues md the patient$ adaptation to a new prosthegis. In fad, mlldesigned mi constructed dentures or an implant-supported prosthesis may prove to b ~~ for a patient because of poor toler- &e by the unhlying tissues and bone. Hence, denture failures c2m be h e not only to imperfect desiga, but also to poorly nourished tissues. W d symptoms of malnutrition are often
&emd first: in the oral cavity. Became of rapid cell tumwer [every 3 to 7 days) m the mouth, a @, balanced intake of essential nutrim& is required for fhe maintenance of the oral qib l ium. hdeqwite long;-tetm nutrition m y r e d t in angu- h chdt is , glosaitis, md slow tisaw healing. The mount of dveoIar bone morptiw that accnrs after tooth extmctions may be exacerbated by low calcium and vitamin D hWm.
Ne9tly half of older indivibh have clinically imabk nukition problem. Undernutrition h a s with ahwing age. Persons older than 70 p a n of age are more lihly to have nutritiodly poor diets. Dentate stam can affect eating ability
,and t l n ~ tbe diet quality. In eldedy persons, ord h d t h p r o b l ~ s may contribute to involunw
weight loss and a lower body mass index. Because most edentulous adults are of advanced age, a large number of patients with dentures can be expected to have nutritional deficits. The nutritional status of a denture wearer also is influenced by economic hardship, social isolation, degenerative diseases, medication regimens, and dietary supplementation practices (Figure 6-1). An understanding of the nutritional requirements, symptoms of malnutri- tion, and environmental factors that influence food choices will assist dental clinicians in identifying denture-wearing patients at risk for malnutrition. Dietary guidance, baaed on the assessment of the edentulous patient's nutrition history and diet, should be an integral part of comprehensive prosthodontic treatment. Nutrition support will improve the tolerance of the oral mucosa to new dentures and prevent rejection of dentures. Because denture fabrication requires a series of appoint- ments, dietary analysis and counseling can be eas- ily incorporated into an edentulous patient's treament plan.
d
THE IMPACT OF DENTAL STATUS ON FOOD INTAKE The food choices of older adults are closely linked to dental atatus and masticatory efficiency. Although an intact dentition is not a necessity for maintaining nutritional health, the loss of teeth aRen leads adults to sdect diets that are lower in nutrient density. Investigators in the United States and S& have reported that adults with mupromid

& e , ~ m o t o r ~ a a , ~ sah,aad t h e n ~ o f o c c l u d i n g ~ o f t ~ i n t h mouth mainly detr.
" an indiviwrp d* abil- i@ Whan cumpad to those with natural ~~ persms with &18 complete denrum hid greatly reduced cbwhg we. Denture - mu& complete a greater nlmzber of chewing s t r o ~ t o p r e p s r e f o o d f o r ~ * E ~ ~ ~ additionat &wing, the avma.ge dentuFe doe# nai ~ f d ~ t o a s d a p w t i d b d z e ~ H 3 s ~ uttil dentition. The &wing ddhty of kdhkhds w i t h % c ~ l & ~ i n o n l y o n e ~ h , o p p o s e d b y ~ W d e a t i t i o n , ~ t ~ k ~ t o ~ l y t h c s o u n e ~ t ~ ~ w i & ~ ~ m p 1 * datum in both arch. En a Ve&mn's Artmini- Strasion longitdid study, &mition s&m and nutrient intake3 were eignificmtly raid to d- caiory function. m m complete d a m I e 5 replace old ones that had poor m t i q pathla subjectively tba? &,cat@ performance ~ e & ~ ~ b & a r a n d c h ~ ~ e r m t foods. However, nu* in* ww nat impHwad c ~ e f f t u ~ i s ~ b y ~ g pwticlesizeaftmsubjwbhm M a t e s t f o o d ~ ~ 0 n g a s n ~ t o p r e p a r e ~ ~ l e f o r ~ - lo*.
T ~ m l d h a r d n ~ ~ t b a n ~ a n d md, d e t : d e a c c w of a food for many patiem witb den-. Geneaally, the intake of hard fmds (xa-wveget&l# orfdb, f h m Inmts, h a d b r e & , d , a n d n u t s ) i s ~ ~ ~ intake of soft: fods (pound beef, brads, d s , pastries, md calmed fruits ebnd vegetabb) is mcmsd Whether these changes in food wlectb wg-b d e c t nutritional status d& on nnttient density of the food mWtub4 bat wfi f& 3xe often low& in nuixient b i t y and fiber. For example, rqhciag stads with ground Wpm vides simifar nmimp, but dw&Mkg f o r a g r e e n d a d d t a m k n u t t i t n t h b b ,
Replacing a compl@te datum dL msminb grated implants m u h in sigiSmnt in masti&rp l i m c t i ~ I n d hake&- f r u i t s m d ~ b r d m ~ ~ r r m l group of Swedish abhs wha rewiwd timue- ~ t i ~ p s ~ i a t h e l o w w ~ . ~ ~ m o w @ ware dentures reputed that their chew- ing ability was ~~ h p m d after Man of a madii* f d pl-dwh on owdnfe-

ZZ!, h t x d mphb. However, impmmd oral n does not lead to se ldon of a higher qual-
%diet. Some incfhidwb will ~amotevaFied && mid increase their intake of h i @ and -eta- #% but d e n t intake of i m p k t warera is gen- d& to wmplek demture subjects. To ppm did quality, individual *t!3 under&*
plwdwdmics aecrd diemy counseling. The M & t y to distinguish the senmy Wi-
tk offood r e d m a p&t'a enjoyment of eating m d ~ l ~ d t o ~ e d c w i e i n t a k e . B e c ~ a h e m in tm?e md $mall acuity bquently mmqmies aging, it is M " ~ c u l t b separate the ~afaginganddmtwewewingonsernsofy ~ . N e d y a l l d m b m ~ q m r t a ~ t hb in W e acuity when dea- are fiest ~ T k i s i ~ d l y a ~ u t d t o d e n t u r e b a s e ~ ~ £ t h e M ~ ~ . H ~ , W a b i l i t J r t o W d y @mvm as ?he patient adapts to the
~ c a m p d w i t h * ~ ~ demk adults or partial b k a e wearers,
~ ~ l & c h e h m t e s d taste, aexhrre oftest foo& andmeiwd ease of chewing (by mapla dentrrre wearm) were rated the Iaffleat. In ma m, dmmre rflemhtre are 3igmCmtly 1 ~ 5 5 ~ t o ~ ~ e e i n ~ a n d ~ e s s d ; c e r t a i n f f o o d s ~ h t a t e s t l b j ~ ~
DehyQation is a major pMm for d m ~ t h e ~ t o s e n s e t b i r s t i s d ~ i n t h e m y popdon, H ~ ~ m eEevated body tctapemtum, a d mentoll codmion may occur w h a fluid intake is -. The m f o r t of ~ ~ i s d e p n d e n t o n t E s e h d x i ~ ~ d d i v a i n ~ m o n t h . I f t b e o t a f m ~ L drg, h w q k difficult, denture W o n is cum- - & m u c d soreness or ulceration8 k&p , Bwause &vary flow f-tes nnastioa-
dthe h o d bolus, swallowing, d a xmjw mibutor to the pleasure
0faiQg. PIcmtomb, mom c m m o d y called dry mouth,
C 3 &id ~ t i m d ~~ g h d dys- fbmb. ~s~ may cumi'bute to ger idc jmimtri~on. Thm me @weld causes of dry &* the we of rnedicatim, thqleut ic radia- ih ta the h d and neck, diabetes, dqmssion, &&@m, pernicious anemia, mwopame, vita-
orvitanh B complex Mciency, HIV infec- ~ ~ a u t o ~ ~ ~ s u & ~ S j ~ ' s
syndtom. A#ng aa &e mIe m s e of d e c m d ~ ~ ~ i s ~ , T k e ~ c O r n m r n ~ ofdrymouthi8thewofdrugsto~~chronic &eases. Xerostomh is a possible side effecrasso- ciakd with more th 408 drugs includmg antihy- pertensives, mtfdepmwnta, antihistamines, bronchodilators, anti^^^, antispamod- ics, anticholin~cs, 4 ~ W ~ W S . ~ o u t h ~ ~ g b s , alcohol, tobacco, and caffeine my alter flow or cause dryness of the oral mucorn
Management of trarostomia dqmde on the cause of the condition. If a d q is suspected to be the muse, cmsdting with the patient's physician may result in prwriptioo of an alternate drug or modification ofthe dasage schedule. Sat in substi- tutes pmvide tempomy relief but have not p v m to be acceptable for many patient$ and b y am -he. Milk h a s b m n p @ a s a d h & stitute, Milk not only a i 6 in lubricating tha tissues and increasing the pleame of eating, but aIso has Wering capaciw. This Me&g capacity may be o r n ~ t b e n ~ t i f a p e r d e n t u r e ~ t t e e t h a r e ~ h e d r y ~ a ~ u L m r r y m a l t i n i n a d - equate autritimd in&, dm use of milk not only serves as a s a h suwtute but also is sn excellent source of nutrhb.
Sidogogum (agents that stimulate salivary flow) sueb ss sugar-fm grmq lWng6?3, or augw- free candiets confahing &c acid may be rcmco- mdgd SorbitoI- or x y ~ ~ ~ e d prodwts may decrease tha risk of candidhis developing in susceptible adults. Additianal recommcmWons i n c l u d e ~ g e s h t ~ ~ m o ~ e ~ such as water with P slice of hmq lmomb, or Ilmaade. C a q h g a sport bottle when 1- t u n n e w i l l d ~ f o f f t e q u e r r t s i p 5 0 f ~ * S ~ Popsictes w ice chps will hmase &rt and provide lubricatiq sauces, gmks , rmd dremkgs w i l l m o i s t e n f ~ & ~ t h w n e ~ , t o ~ h* Chewing f i h u 6 1 foods sRlcfi as dery or w h ~ l e ~ b m d s w i I L r 9 s o ~ & p r c ~ d u o t i ~ . ~ a ~ e ~ t o c ~ * ~ u x l ~ a t ~ t e i g h t ~ u f w t m , j i i c e , a r m i f l r d d y i s t h e ~ ~ ~ t O l e 1 l t m d l y m a u t h .
GASTROINTESTINAL FUNCTIONING Littie rmmh exiw on the e&ct of moth 108% on gastmintatind function w ttbe likelihood of

OF OLDER ADULTS
~ ~ a ~ i n ~ l i c ~ . & ~ n i c $ i s ~ w * l * w a phydad mmhe, €lms- wtr-

pm&h irtbake ia reduced, protein metabohm is
-i~ieficimcim in the el- -tian ~ a p t f 0 h ~ L i n i ~ ~ a a y b o r E y ~ ~ ~ ~ d i n a n i n d i v i M h a v l n g ~ e ~ . . . I l ldmbb who haw leW-calori8 inblm, inpa rnuitipto drugs, or have disease stam that cause l m w % a @ m a ~ e & ~ r i s k f o r h ~ - ~ ~ ~ d d e r p e r s c m s a f b e n r e p o r t ~ o w d b b q &&s of vitamin D, vhmh E, folk acid, calciam,rrnd@um. O r a l ~ y m p t O m S ~ f ~ ~ f r i twhare~duetoa tackof thev i taminB ~ ~ ~ p m e J s vitamin C, iron, or protein mble 6-1). In one study* chid symptoms of barning mouth syndmme @MS) were resolved in 24 of 28 Pat;- ~ p m v e a ~ d e f i c i . m c y w h e n v i ~ B cumpk supplmmtation was g h a Fslic acid p h p mimportantroleiu~lidik-irnandin~d Mmdd~tion;memiam&skmaninade- ~ ~ ~ . h 4 a n y d r U ~ a n d a t ~ ) h o l ~ fsrit =id absmpirm and r n e h b o b hstividuh w i t h a ~ i n t a b a f f o l i c a c i d w h a r e u a d a - p @ ~ - ~ d r u g t h ~ a p e a t ~ ~ r i S k o f
Table 6-1 ' Oral Signs of Nutrier~t Deficic~icicr I
N m t d e m t ~ OrrlSylapOsm
Protein Decreased s a l i ~ r y flow Enlarged pilroiid glands
Vitamin 3 complex, tips: * iron, protein Cheilosis
Angular stamatitis Angular s a r s Inflammation
Tongue: Edema Magenta tongue Atrophy of filiforrn papillae Bwning remation Soreness Pale, bitkd
Vimin C Edematous oral mucow Tender gingiva Spontaneous bleeding of gingival Hemorrhages in interdental
papillae
~ a ~ ~ o f t h i s ~ O r r m ~ e ~ ~ ~ ~ , ~ I i . ~ h , apm@K,zlraddtkd beansareg&sowcwdfoli~&d.
W r t 3 r t h e ~ 0 f ~ ~ ~ o f v k n h BIZ, a prmkmx d mihagnored v i t a m i n B l z & f m i e n c p h & 8 k n & d ~ t h e eIderly popalblioa. ~ - ~ u t r d v i e B ,, d- ~ l ~ t ~ a v i ~ B , ~ M C i ~ ~ often dm r 1- v i a BIZ =take m h k of i P t f i f i g i C f ~ . A ~ 8 1 2 d e P ~ ~ m n r y l d ta problems w i t h ~ t i a h o l d * r ~ . V i t m i n BI2 is found only in a n i d pr&wm. G p W c wt&nBl2 o b t a i n e d h fortifiedfbads or- ~ ~ i s ~ ~ t b z r n ~ b o m t d vitamin BIZ.
Because ofits role in C O ~ sptkus, asc#lr- bic wid (vitamin C) is esgentlal for wound healmg. ThepeiI3awidevariationinvi~Cintakesof aduIts. h me ~utvey, low umrbic acid i n t a b w o c h t d with low p b lev& w m reported in one faWh of older Mvkhds. Heavy &, a l c o h o I ~ m ~ w i t h h i g h ~ i n h k h a h i ~ r d d y ~ f o r a s l c a r b i c a & k The denture- patient &ould be enconaged t 0 0 ~ f o Q d s r i c h i n v l ' ~ C ~ s u c h a &us fruits, m, d o n s , kiwihit, mangos, ppya,andstmbmia
W ~ E ~ & s m a n t i ~ m ~ U m e m ~ . B y ~ r t s w ~ o f f m ~ d s , v i ~ E ~ ~ o f ~ c e l I pho5pholipEP. ~~ OfviwnhE inch& ~ ~ a i f s , ~ * ~ a t l d ~ .
Mapmiurn is a compmat of the body s3rele- f o ~ , i $ a ~ 0 ~ f o r m o m ~ 3 o o ~ g o d pw a role m ~ t l % c u ~ mwmiwioa The highest momas of magnesium am found in veg- etables and unrefined gmh. Milk is o mmkmtely good source.
~ 1 ~ ~ m b e a s e r i o u d t ~ p r o w among ~ * ~ ~ A l ~ ~ ~ i I E i d e n C e o f a E E * i s ~ d - mates of alcohol ablm in imkpld&w older ~ a r e l % t o 8 % 0 f ~ o I ~ t h a n M ) ~ o f ~ ~ A k ~ ~ o f k m i s ~ ~ ~ ~ l o s s o f a ~ h ~ ~ o n , ~ m e n t , 1 ~ 0 f ~ , ~ t e r f t l P e d ~ o r t l c c o a - tribute to excess d o b b o l ~ By oldm adults. E l d a r l y ~ t e n d b & i n k a d r x w b e d d c o h o l b u t d r i n t r m . ~ . % ~ d

~ ~ r s o ~ f o r
in,py&xhe,fob and acid are
~ t o ~ h a ~ e s i s r u e ~ 11oPrldbemmi&d.
' -1,
~@letuM AND BONE HEALTH
b o d y ~ w . ~ ~ 0 f ? M i c r t n d c 3 ~ d ~ is c l d y sti l l h 1 o p k g .
Resorption of the &eoIar* i s a- problem ~ d e D . ~ ~ patiem awl m m h in, uwkabk dmttm~ the alveolar gnvasms occ dd--wi&-*w&h o f ~ t h e d v t m h r h u m h n o ~ ~ f o r ~ w m G - ~ - P i ~ b t % c d & d a p a d b a r p e ~ ~ l s - A ~ d # g R ? e d ~ ~ ~ ~ ~ - ~ mrwomenthsninmen.Bomelmsisaaelem&d i n l h e f b t Q m o d w a # e r t o o t h ~ d m e k d m i n t h e & i t h a n i n ~ ~ T h e ~ ~ d ~ h ~ * q a e n t l y m a l e a s i t a n o p . e d i f E ~ t o ~ a m&*athatbwwQrttad remlti~~.
D i ~ c a l c i u m ~ ~ c r i t i o a l t o ~ t h e ~ ~ ~ . ~ r n o & ~ m w m o f p ~ ~ ~ b o n e ~ L a c q ~ a d e r m P & e l ~ b y ~ s i n a e b a e ~ ~ ~ 3 0 l r n a Q ~ d a g e . A w o m a n ~ b a ~ ~ ~ a t 3 5 ~ Q f ~ w i U ~ p r o - ~ ~ t e l y m o ~ e ~ m i n e r r d ~ m d b less subicepWe to fraEtrrme a* mm~qmt~ , c a k i U m ~ 0 f ~ ~ ~ ~ r e w ~ ~ ~ ~ ~ ~ dealhm who hrrve tzc#sive ridge rempbn ~ l < r w e r ~ G i ~ ~ ~ ~ 3 5 , ~ 75% af U.& wormerm harw ilwhqww - ~ A ~ W c s l c i m n ~ ~ ~ ~ & ~ i a w p t i v e ~ e i u m ~ . F w d l e t r n n ~ I e w - e ~ t o b e ~ ~ w i U b e ~ ~ ~ e , r s m d t h i s ~ t o ~ ~ Q f ~ W e t o a ~ ~ € l ~ & i a m ~ h y ~ I d w ~ W i l ' m t & t i ~ ~ ~ m a s s , i t d l ~ e c a l c i ~ ~ a a d d ~ ~ mofboneloss.
Etllw7&Natadaal-&-- o l m & w a n ~ - xaen&wmm 1 9 1 S ~ ~ e f q p and i r n m g f 0 r ~ 5 1 ~ ~ 0 ~ mbk 6-2). T b frtr ib ~ & i m ~ o f U . S . w m m a n d ~ 4 * f O a d 610 mspe&ivelyely W aging a d ~ e a o p a ~ l w l b o r e d o c e d ~ r ~ t n ~ # s l t s d ~ M y ~ ~ ~ ~ i r l ~ ~ h ~ ~ ~ ~ ~ t m f o u n d i a r h u b b a n d ~ d

phywa h d in *Oie-gmb products and m n p k X 3 8 with d- mount of oalcim
& t m x b d ~ * o f & * - ~ ~ ~ ~ ~ u m b i n ~ ~ , h m & W & d a i n e ~ [ 3 0 0 m g o r I e ~ p e a
fow-fat d i k Pm *'
BJ)d-*ht&ta 15pg&ag~?1(680ItJ).
Table &2 The 1997 Dietary Reference Intake Values I
l f a n ~ I a c b ~ ~ m e , i s ~ i n t d - - t , 1 r x d i i p ~ ~ ~ , a v i ~ ~ 6 t u g p 1 ~ mentof 10pgiatbiadde.
For t h e women who wnsumc minimal % m ~ o f d a i r y ~ ~ ~ ~ - ~ o e , o r h a v e ~ t o d e i r y f o o d s f d ~ ~ p l ~ ~ o n ~ b e ~ - supp1- am welltolerakd, a r e i m x p & e , r r t r d ~ f 8 ~ 5 i & ~ ~ t s . The most cammoa farms d -1- are dcium Eatboaate, cakhunciWak, calcium lac- tate, calcium glwmmte, and &ium diphqhte, Calcium dxmte co&h the &best mwatm- tion of alemental calcium (4Mh but in older women, M y aorptim J calcium utrab k bet- ter. Hmwer, h s demenatl d c i m n is ohbsimd from each d C h l c&@ @I&. ~ t h s r t ~ ~ m h ~ h d n D t o & t ~ t i ~ o f ~ c i u m i n ~ g u t o l r e ~ f u l i f v i ~ D L n o t ~ ~ o t h e r m ~ * A d o w o f 1m mg of ehmmtal dciwn bkm with meah k cam- m n n t y p x s c r i w . ~ ~ d e r i v e d d ~ ~ - bonate or d i m c h b is the &st mwm; bane meal, oystm &dl, atad dolode cdoim supple- m e a t n r ~ b e ~ ~ ~ W b e c ~ t h e y m a y b e ~ t a m h a witla heavy me€& BWh as lead or m w -
Few advass &ch of d c i u m s u p p l e - tion have been - Some d& wwnen have ~ n a u s w a , ~ o r ~ ~ I n ~ ~ d * i Q * d t R i a m - l @ o f calcium, A ~ p a r w P m a u f t 8 e ~ a n , m h l y men, afe bo formtng kidney mnw h o w w e r , a h i g h i n t a k n f ~ ~ ~ n o t appear to a i k t stone fomation, A physician W d modtar t h ~ use of &urn ~upplefllmts by t k e persons. The rnmimum ~~i~ intaka that ~ n o ~ o f ~ ~ k 2 . 5 g .
VITAMIN AND HERBAL J
SUPPLEMENTATiON


~ ~ n o t ~ t o ~ t i n m w h ~ ~ i n C Q t O h a f ~
I t ~ ~ i s ~ ~ t m r ~ u a l ~ o r m ~ e # , t e ~ ~ # s m ~ o f n u f t i - t i d ~ . M Q s € ~ w a l ~ t h e h t i s t t h a t t h c y e a t a h ~ ~ ~ ~ ~ ~ d C ~ ~ f o s m ~ ~ ~ t o r s a t t h e f h t ~ s o ~ ~ ~ a n d foflw-lap can accarrdmhg the of^ ' T ! h e ~ ~ ~ b y ~ ~ t f f b o ~ ~ ~ ~ i n b w i c n ~ m c 4 i t u ~ ~ ( 1 ~ , ~ . h t h e U ~ g t a a e s F , ~ l i n i 4 s i@safhk ~ ~ ~ ~ v e r y o f t e n . ~ , c m t & i d % Q ~ ~ @ ~ r n ~ t o k a t
~ U I ~ I I O ~ ~ 6-11, DieE8t'Jr ~ d ~ ~ h i n c I u d e d i n ~ m t i f p & ~ h a v e a a y o f ~ f & w h g p h y + i C a t m a o c i a l ~ o l d e r ~ 7 5 ~ o f ~ , I w v ~ , l i t d e d ~ t a c t , h l ~ ~ * l o ~ i s , w ~ m u l , ~ e d f i r g $ o r ~ E q a withdaily Sdf-CaKu.
The maita obj- of diet comdhg for ptiemt3 mdergoiq ppo&&ntia mre is to a-
im- in nutrient h* - ia . tdm w i t h ~ a d ~ h e a l t h , T b ~ i s n o t expea& rn &@w gplf~ifIc nwimt Mlci*, h t t o d c r t e r m i n e J * @ ~ o f * & . I f t h p a t i e n t ~ ~ l ~ t a r y ~ g h t loss or g a i n ~ ~ 1 0 1 b ~ t b e p t s t 6 ~ ~ ~ a ~ c ~ ~ r & m Q u ~ ~ ~ ~ ~ ~ 0 f ~ -
I Risk Factam For Malnutritiu~ in Patiem with Denturn
Eating less than two meab per day Difficulty chewing and wallowing J
Unplanned weightgain or loss of mare than 10 lb tn the ha 6 months
UndeWng t h f h w a p y or radaisn therapy toox denture or save qm?r under ddntrlre Oral lesions (gloeitis, cheilsis, or burnlng
f araguej 0,:
Sevetely r e w r k l mandible Alcohol or drug abuse Unable to shop for, conk for, or feed oneself

OWin n nBarition him d an aecmk, ' relrord of fd intake over n 3- to 5&y ~ o r c o m p ~ a f o a d ~ ~ f m n Evaluate tlre diet; assess nutxiti~flal risk
4 Te&abovtthecoxrxpom& of adiet that o t i l l s u p p o t t ~ o r a l m ~ b o n ~ ~ ~ W b a i y ~ t h
~ p a ~ e s ~ ~ g ~ ~ ~ t h
b diet FoUaw-up to s u p p t patient in efforts to ~ W b e h a v i m
~ , a l l d & f r o l a t h e b r e s d - c e m l ~ . T h f ¶ minim- r€amlmdad Mlmber of s d n @ d e a c h f i D o d g r o u p w i l l ~ d e ~ l B O f E ~ ~ o f ~ ~ h t & i n d t ~ m I ( n d ~ s b o u l d b e & F i s h , g r o u a d ~ ~ , ~ ~ ~ , O T ~ l ~ m a d e ~ ~ ~ ( # 1- ~~@~ mllrcel o f p t e h within the ijndt and vqekible graupi, one saving of a ck- m f n r i t a n d o n e ~ o f ; a v i ~ A - r i c h ~ o d , ~ ~ c h ~ ~ @ h ~ ~ r W ~ f n r i b a n d ~ - . etabh, irs d e d daily.
- A t t h e ~ m d ~ t h m l a t i m & i p o f & t o t h e h d t f i o f t h e o r a l ~ s a n d d ~ ~ n ~ f t h e p a t i e n t ' $ d i e t ~ b @ ~ T h i r r w i l l ~ abut 30 to 45 d u t e s , W m e i c M c d termss should b e u a c d ~ ~ ~ ~ t 9 ~ t h e & ~ w & m M - . M w m t o b t s M FaI the epiblhil mils in the mouthhsve rr rapid himover. Secmd, tfse hcdh of tSle W M e and maxilla &pi& on a mmtmt supply of dcim and vitamin D. Lack of d t h n tnrry iweIcmte boa0 ~ h c ptieila owtk tradl-h crtn beusedtoN~k€mmtofBomm?&hg in the mandible. This W 1 y k d i g b k w g for @mts beam they have probddy never canaid- ered dm systesnic role of e t a in maintaining the orrtl t i~ues.
When &cussing the qutllity af the padmtk di* always begin by pointing out positive m. I d a i @ w h i c h f d ~ g u o t a s m ~ m & Z f t b a d i e t L ~ y p m r , ~ o n o n a o r t w a o f the most dtid deficiencia. L m a h i u , h i t , vegetable, or d&ry h d hhkes, or ~xcemive use of &t-soluble vitamin mpp1emanb would b of pri- pary ooraaern. Do tfot mawhelm patient9 wi* mfimdm or dam by peenting a 1- list of dietary wedmesea. RmmW W older patients with dentures often aze pwtiwhrly semi- t i v e m p s s ~ ~ t o t b e i t h e a h h d m a y ~ f o r e ~ f ~ l ~ ~ I f ~ ~ u d l ~ prob1ms d&m@ r e f d to a physician m ~ ~ i s ~ e .
N u t r i ~ @ f m ~ ~ @ m a m t o e a t a a a r i & y o f s f ~ 1 , ~ ~ ~ mme~, &iq fmb, fkuit$, vegetable, and c a ~ , a n d t o ~ t ~ t , M , a r p d ~ ~ ~ 6 - 2 ) . ~ 0 f d i e a ~ i @ , t h a t i a , ~ ~ o r m c l r e ~ g r o ~ ~ t h e d d y ~ h b t e n ~ w i t b ~ r i t l k o f ~ w l e r ~ .

1
9, . D o ~ ~ r y o u f ~ w b x Q o o d F d r Paor. : k k b w W y d d p ~ M a g e h W W h e n a F e y M l r ~ ~ ? ~ t k m m o s t ~ ~ ?
3 . R a ~ 4 & & ~ *mly t mkB8nds 4. O o y s u ~ ~ ~ ~ B # E v e r y d a y S e l d w n Nsver
mtfmeol* mmwr SrrPsdcs: 6 . 5 . , a t m * 3 r w u E 4 Q m , F # h ( n t s , ~ ~ ?
~ k k i d ? 6, ~ ~ ~ ~ ~ Y O u a b d ~ ~ Q x ?
W h a t ~ ~ d o ~ ~ ~ ~ ~ ? 7., & e ~ o n + ~ ~ Y a No- Hym.WMtsd7 - ~ ~ W a m 1. A w # b m w f m E y o i m ? w t m Y m No-
-:
f ) rbmdnerate,&-:
4 1 mmids,~other%r: I Q . ~ y w r c a w c t h @ ~ Y e # N o m r ~ d p l p o u ~ ~ w ~ ~ m o r ~ ~ ~ ? 1 1 . i h y w ~ ~ ~ o r ~ Y - No- DasuW:-
mure 6-2 A nutrition history questionnaire that could be completed by the patient at tke time the halth Wry is &aid. #
l W y t o b e ~ B d d t a g m e g l o r s s o f x d k o r ~ e j u i F e w i U ~ ~ ~ m n t ~ t o nutrient intake. W h it is *ed what i b l ~ ~ b e l a a d t b o ~ t h e ~ m f s d i e t , t h e ~ o r ~ ~ a n ~ a & ~ p m m i p - ~ i b r a h e ~ t e r t a k e h . T h e ~ o f t h e diet wwmmt anrf the diet pmmiptk a h

*AdUlbB 2 M o ym
Rgure 6-3 Form used for evaluating a %day
- " -
1st 2 n d 9 r d 4 t h 8th 6.Qly tklay hodgroups Portion Wmenlng dmy day day day dmy ?QW totd Dlmmw
Mllk group 1 1 1 2 ~ I c e c r e a m (mlik, cheese) 1 cup milk, yogurt ' 5*
3-4 wlngdday 1 112 pz cheddar dww 0+ 2 02 pmcms ch-
m W P 2-3 ol cooked lean Imeet,ftsh, m=t,ffsh,poultry poum, ew, 2- W m , w 4Tbppeanukbutbr 10
b n Q I cup cc&ed dry beans 2-3 &&day or lentil8 - group 1 orang% 24wnAngdday l/2 med grapehutt 5
a'4 cup hurt j u b
1 med apple, pear, banana 6
112,wrpcodadfruit
Vwembgroup l I 2 a u p ~ d r u k 3-6 servlngs/day green, orange, or 5
yellw vegetable
112 wp cooked peas, bans, cam, potatoes 10
1w-
&ma- 1 pamake, 1 tortllla Om* 1 dice bread, 112 3 5 serutngdday 1 oz dry dryreal
112 eup mked w, 30
rice, -, mecaron1
I food diary submitted by the patient. The I group is compared with the recommended
w e n t dietary inqdvement Witbcoahud g d - ante and encomagamnt k m the dentlrl Wm, p a t i ~ a E ~ a p t ~ ~ ~ ~ i n t b k r f o d ~ h I n ~ m ~ ~ s h o u l d b e m ~ p a r t u f t b w d l p r o ~ dontic tmatmeat*
F m ~ h W o r ~ o ~ ~ ~ r n c U f m d y ~ n r r t t i t i o n ~ M * f a a d ~ ~ d m d s , a n d ~ m e a l ~ ~ i n l d ~ c a ~

1. Eat a variety of foods. 2, Build diet araund mmpkx dehydrdtes
(fruits, vqetables. whole grain breads, and enriched cereals).
3. Eat at leastfivesewjngroi fruit$ and rtegeta- bles daily.
4. sded fish, poultry, kan mat, or dried peasand beans werq day.
5. consume four servings of calcium-rich foack d Jly.
6, Limit i+ke of bakery produrn high in fat and sfmple sugars.
3'+ Limit intake of prepred and processed foods high in sodium and fat,
8. Consume eight glasles of water, jhice, or
&- ot community centers. Nutrition e&m- tion, w w l l its food, is pmvidd These tlimition d c e s can have a signif~cant impad on nutrient hitake and ndtional status of participating alder a&ts, Dental pmvidm can refer patients to these programs.
DIFfARY MANAGEMENT WHEN TEETH A H mRAClEu h&mta who are candidates for implantrs or imme- dh& -S regUire & tooth tiom. The pathit who is well nourished dl aperim more rapid tiwue healing and will be at lower risk of i n f h afkr surgery. If a patient 4m=m~-C~~w*&t,d ~~ cognition, nnwrplained skin lusion~, @ads, lsxttgery should k cb11pi _iwiiIthe-$w-mm*
+- i t k d w 1 ~ ~ e n t s w i t h uncon- Ati$%m*,dpd-wi~-m-
f w g complhtim ~~~b t b i r h & k f o r n f e w
@mlh~pmdlmonthaRer-Cd~On
with the physician of the d M d c or hypermsive patient wilI aid the dentist in d e m h h g if the ptiunt is stable enough to undergo the surgical pmcdm, Tke a&qwcy of a patient's diet a n be ~ w i t h t h @ ~ t e p s j y s t d ~ I b e d T p s u p port M y functi* aod to irrrpxwe the 0- of surgery, malnourished patients '&odd be instructed to wmmne highealorie, high--in f& before surguy. &-baeed cooked meals and soups, canned fruiB, mashed vegetab1e5,
ice meam, comga chew, grormd meat, d e g g s are ~ f o r p a t i ~ w i t h c h e w i n g d i f f i - culties to w&A rsmjtivitdn oontaining 100% of
. the value wm bprumibed for the high-hk patient.
A generous suppiy of emmthl nhents in the body is bmic to ti- h d b g . It has been clearly shown that when the immune system is depreered, the risk of infection after m g ~ l y is greater. Rotein, vitamins A and C, folk acid, pyridoxine, vitamin B1 , iron, and zinc must be &able to ~y oeus hr the support of p h g o ~ c aotiuity, cell-mediated immunity, collagen synthesis, rand regeneration of epithelial cells. The mount of protein and dories required by the postoperative patient will depend on the amount of metabolic strms experienced during surgery. For the fmt 24 hours after d o n s , the patient should be counseled to cvnsme nutrientdam liquids. A blender is in m h g meam soaps, miik- s w s , mt drink& or ia8tmt breakf88t drinks with whole or milir with 2% fat. A high- protcinrzliIIccanbemadebyaddingonecupofdry milk powder to one quart of fluid whole milk This fortified milk a n be d for cooking, for adding tu beverages, or for &&ng by iraeIf. By using this milk, the patient csn boost calories, protein, vitamins, and minerals without increasing serving aim. Howewer, mi& is a p r some of vi- 9, an -tid nutrient for coIhgen *h, sa Me- NS h i t juices or atlother saurce of &ic acid mudit be included in the S d , b p n t mads throughout the day (every 2 hours) may be ~ i o ~ ~ ~ ~ d a t i t s . T h i s i ~ n a t a deslirabLtimeforan~ttotrytoIosewu@t;
P e o p l e ' S l ~ ~ for solid foods s m vasies greatIy. If blood cIot formafion is satishe- tory, the patient &odd k emmuaged to progress toaof i foodebyth~third~.Am&yofsof t

h r t g & a ~ M ~ f ~ C k ~ W ~ m d a s i o g era& m~, JdM4 186:20&215.2001.
a r P a e a r S M , h & Q V a l l e e R & & W h e d * - *tdatCdtQ-* s- dlw, J- h u t 70:468-473,
1993. ~ D M , & ~ . ~ ~ a t r ~ s t a l : ~ h s ~ ~ o f ~
k ~ ~ ~ ~ ~ ~ & . m J 1 8 % ~ m.
~ ~ H ~ B , f ~ P , S h i p p C : D i e t a r y ~ ~ a n d ~ ~ f h t i w ~ i a e i n ~ ~ wome~, AM J C h Nrrh &%85-687,1987.
D a P q r v B , ~ s i n ~ ~ m i e A h k ~ t t o f d t i v l t y t o o ~ f h m "pplicathminadudy o f a g b g a n d h - tima, QiaAl &wus 24:671-#7,19R.
D w y s r r n ~ * ~ ~ ~ ~ m prrstricca fbkaa pmuwih, w- DC, 1991, N a m I r i o D ~ ~
~ W c , ~ a K : P o a d ~ ~ NI&I JAfd~8142 ,1973+
C ~ d i c t P r y ~ w i t h ~ ~ ~ d e n t i t i ~ ~ : howpeq,k EEq#q C ~ W D ~ w 18:33-39.1998.
~ W W s l l l 9 K : m ~ o f n c w ~ t e t s ~ a n ~ thh d A& 7rr M 43357-268, 1985.
H r r o d E ( : T h s w e d m i l k s s t a d h ~ J P l r M I c H & h r W.184.184,1B4.
I n ~ o f ~ F c u d a n d ~ t i o n B a a r d D i ~ ~ ~ f o t ~ ~ ~ ~ b a n d ~ ~ D C , f 6 9 7 , N a t m d --
J & o o a t M & ~ C I I : S ~ ~ a t P d d b # ~ # i ~ ~ ~ * ~ J h h t h t24A9-56+1992a
J O ~ K T ~ ~ ~ C , h q h s 6 C W : T b ~ of edsnm- ~ o n ~ ' s n d m t t r i e n f ~ 1 A m D s r r t A B s g c 127:4%457,1996.
~ K & s o m m S D : ~ ~ ~ t ~ r c i c m ~ ~ rn denture- J P m i h l h t 14:687&4,19&.
~ I I A , ~ ~ B , ~ 1 9 5 o t r r l : ~ h ~ &dotal bm -I& in h d @ m e n o p a d woman -Int4:Wl09,1994.
W ~ ~ C , ~ R : H o w d e m r i t i o n s ~ d d - eabwy f5mh a$f&i n m h t in*, J A m &ntAsw 1Z9:1261-1269,19%.
KtWr PJ: b q a r h of ~ b o n e i n n w r m ; l d mmpmtk wanarra,$msrk#ht 63:218-222,1990.
~ D , ~ J l l d , ~ J , e t a l : P I b r e ~ i n e ~
EM< mdcatw-,J- 349,199rl.
~ ~ w a m l J l , A , I S , a t a l : ~h~~ ~ d ~ @ t y i n ~ v w y o I ~ J - A n r h t A S B ~ ~ I33: 1369-1379,m.
M o j w P , ~ ~ E , R a p i n ~ ~ a t t o m s h i p ~ clral Wthrmdrmtri.atrm invoryaldpaopb, Age-g 2&43-468.4999.
M ~ P , 3 r a d b m y I : ~ d a d A m c t i o n a o d i\rPr#fbton lT:I77-X78,2W.


1 :T FOR
' 7 ~
I . .
t :: ,,

IDiagnosis and Treatment Planning dl -
for ~dentulous or Potentially Edentulous Patients
d c pmdures a d &dings that $q @culwIy relevant to edmtdous and nearly &knhdw patients. d.
@Milb~ with the Patient f&p+ntwh~isaeeking~mstlmdmticcareie
b y ~ ~ ~ $ g d o r w . I f t h e
$b&& dentist and patient b e the of . The dentist also ha^ the potentid pro&g on w*m. Both
~ & m m h g patiat3 need thedr comprete ~ C p r t ~ t a k m o r r e v i ~ w n d n e e d t o mdm bmu& mamati
. * 008. '
7
&PCLFCpfionwillbetheprimarymdeofdata in the ~ ~ 0 1 1 . . A variety of theorla
on have hen advanced but it ia m&T- i n t e e with the
f&$~ T @ d 05th i i m h identified in this grocwrs -on, d i a c ~ t h , mopition, idenmi-
aid judgmant. It is not d i f i d to atend totbother~nw,wchastoucband tbhsks arehtqmbd in a littlemore
. . (i.e., detammq its presence). Discrimination rapha distinguishiag that which h been noticed h m sanething e h . Recognition quires decid- ing whether this, or at last surding &imilar. hi been perceived on mme previous occasion. Iden@iation moves the p e w s into specifkity; w h a t b a s b m ~ o b d c a a a o w b Mgmmt allw something that has been obmed to be p h d wi- r mctrmn of bowledge. In everyday Ufk, the% fasb usually p d arxtomat- id ly , ornd mtahdy no attempt is moade to fully@- wive dI aspeats oftbe ewhmn~flt. In diagnosis, there is a professional responsibility to omit noth- ing of consequence. A comigtent, mthdical ~ h t o e x a m i n i n g p a t i t m t s i s ~
Healab qua ti^ aad identification data a n kt gathered ha the mqt ion The dentist's review and cW1c~tion of the responses Qn the qraestion- naire, as well as the. emmination o f k patient, am appropriately carried out in the private qwratq. The opmbry &odd be comfortably equipped, twtefullydeaabd, andwalllit Itshouldhfteeof ~ m d p r o f j i d e p a t i e a t s w i t b ~ ~ d s e c u r i t y s i n d ~ y t b a t w i l l a l l m ~ ~ o communiate h m t l y and cwnpletely,
Diagnosis, in its broadest s q is an mahalion af &&q cmd~tions. More specifically, dia@wing hvalves identifytng, a d making judgments about, ~ ~ f r o m a ~ ~ . T i t w e ~

might simply be thought of as pmbl$mg. 'Zlae bt&w of these problems jdi the e s d a l f - *, but tbe dentist% pmqtiQn of them must mwe through the p m q t d to judgtnent. Tbe la tk~magrn&bacwmpl ishdtmti iaf fer &U ex&a The W& have to use ad&- t i o n a l ~ t a ~ b ~ ~ o f a problem ad whether it requires trea-t. Most imporCaae, the dentist cannot act on oh-rn that have not h e n ma&, It is dangerous and i m p pm@k ta auwtute $wtmptions for observa- W s . lh importtsnce of a thorough examination wi .~acwrate%ylecordedo~011~caonotbe
e n d s and Treatment Planning Mthgh logic suggests fhe tidy secpam of data gatherhg, intqmhtiw into a diagnosis, then mmmt plamhg, the experkaced omcian d l b~g~eadduringtbdatagatherhgandita imp#i011. me mmmCBB ofboth tlmment a n d ~ ) ~ w i U ~ b a r n e b m i n d w i & ~ c - ~ w ~ t o h a w s u c h ~ a n m n i g h t c ~ t h e propa&. The objectiw of the psocess is the -1- o p m t of s treatment pIm that specifically id tkesm the d h l g n d needs of the patieat and acmmm&W tmment as it progresses.
CONTRIBUTING HISTORY: THE PATIENT'S STORY
A messary first step for all pdents is the estab- lishmerrt of their identity. Infomation received in m W Men, by recepttonists over telephones, or evenonfarmscampletedbythepatienthddbe c d m e d . The staff can check a d m i n i a m infwmratian such a klqhane numbers a d atdmsm. The dentist should address the patient by qwm and wflmmore v n a I infomalion such M date of birth, Revitwing already compItl3d
~ p r o v i ~ e o m e ~ e s f o r ~ ~ colmmtion and directly, or indimsly, w n f l the. contained infomdon. A qudm about hours o f w o r k ~ w e l l p m p t a ~ e n t ~ h ~ a n ~ o n O f ~ 1 b a d + ~ ' ' t b ~ '1 work in the, cafeteria, so f am off at 230." N w t h @ d e n t i s t n s t ~ ~ * t h e ~ e n t ~ h available for appointments but also knows that the patient w o h in a h&&& area far i?equeag eahg.
Knowledge of patients' social settings cern help the dentist lmderstand patients' apectatjm and the evolution of their dental status. Famity and social circle norms influence people. There are sb;U mrs of society that are not distmmd by both loss or by the prospect of wearing complete den- tares. ahet patients come fFom dorhmk &- cumsmces where cam has been bacbpak, b~ g i v e a t b e m o n r c a s , ~ w a d d ~ d o n e ~ . Mast people have close ftimds or rektiva whw j-t they d u e . It L helpful bo have patients identlfy these p q b drrring the amht ion and, if possible, gain gome insight into their vim.
An exploration of a patient's habits will help identify those who might have contributed to their present condition aad those3 who will help mure success or failure far the treatment to be supplimd The potentid fur -cation or reinforcement of habits should be mted for inclusion in tbe trab m a t p h . The dentist will lib to h o w a patient's oral and den- hygierne prOQedwes. The duntist can also f d out 8mne Of the patient's less fhvm able habits by q l a i n h g their si-wce for tmimmt. SoPolring is an ample. A patient who has not been mnvind of the long-tmn ddmen- tal e m uf smoking might reqmnd when learning of its dethaental efEds on wound heding and tbe durability of tissue c ~ ~ .
Patient ex-tim are fmded in the realities a n d p e p c e p t l m s ~ f t h e ~ m d ~ ~ d ~ knowledge and d m ofthe present but are Val- idated only in the dmmvm of the frrture. P r O & * b W M ~ s e ~ t o f b tigtry. Its intelligent use of m d m technips aad materials justifies raihg the apeatations of patients with poor cbtd histories d inadcqwk knowledge. of denthey today. T h e pertieats a h great practice builders when htmnt e x c d h i r m~tixtiwls. Bther people hawe exptatbm

dkppkr 7 Diagnosis and Tleaknwtt Planning for Mentulaw or Potentially ~ W ~ l o u s Meats 75

o f ~ * w ~ ~ B f ~ * ~ t a r e t m
are farely f w d ia h m diBimlty d t h
Thatmen? planning is &fmed later in this chapter a s a p c e s s o f m a t c h i n g ~ q t i o n s w i & a patierrtb-51cdm-bymM diagnosis. Par& of that W d diagnosis m u i n o I n d e ~ Q f a n y ~ R 3 ~ ~ ~ ~ t i a I t o p F . r f e a t t h e ~ r y d r ~ i m b l e ~ - ment. l h t d d a a d d y t i d ~ m f w t k e ~ ~ t i E ~ b o ~ e h n & ImowIedge to spudfk hawledge of itte patimi ~ ~ S a m e ~ ~ ~ d d b ~ - imd am anatomid, phpidogicd, pathdogid pyc~1ogicaI, mketic, a d P d .
The caminadon d the p-t's itnabmy fo~usmmontbehead&*~kmtbo dentuFe-supm &udxm4 for the patiaut Be&-
ing pposth~tic cart. H m w , the m's p d a p p ~ e ~ b e ~ f o r ~ - taristiw suaa as - ,-gaif,=d pwd defects. &T-s, W t i a in jaw size and mmmfdcity, Memmh space, ridge sbpe,*md-te-m examplw of i t n a t d d ti^ & m m p h p r a p ~ e t i c ~ o r s p e ~ a c ~ ~ ~ in a treatment plm.
Normal -010gid functioning eontrilmks t o d e n t U r 6 w ~ . F a r ~ r e , h ~ ~ o f ~ ~ s ~ m ~ ~ c o n - t d . hfi~imcies must therefom be noted ansf cam
measarea planned. The quality md ~ t y a f ~ w m d s ~ o f a c t o m i n a p a t t m t ? i ~ - @W of datum, Thick, r o p y ~~'~ ~ ~ s , d ~ ~ m l u w ~ ! 3 m m d t o p m i d e a n ~ t f ~ & r m - ~onofdenaYairQtIW&ofb- Althongh**m-tabetnM for p-c pmposes, an oxplatpation d&& effects can ~~ l n l d m m d r n ~ d ~ b - ~ s a n d ~ b y ~ W ~ b accept the -W limiwions on fmatinmt sllcwsB.

D d a f o r a n w t W i c
hma. s&tQ p k
smile'' extedwly. hematiye mewam W a h e I p e d i a m d n g ~ d ~ b t o ~ ~ ~ ~ ~ ~ * ~ C ~ emblJ demwy to p m d E l i w m prewk E p l f m m m f i o r d ~ A U ~ ~ - m h e d p t i e t r t ~ * $ ~ b m - m & b l C ~ ~ ~ ~ ~ m m g d * i @ i n g t h m t o m w t t h e m l i t y s f a m e & p r m f b d d e - . X t L - ~ h & di-ia ta addrew patient eqecwiona fbr ~ m ~ o f ~ m ~ d ~ b o ~ ~ ~ a l s o ~ ~ ~ f 4 i W % d r n o f r t f e w ~ - * k e t h t B a B r e t a i n e r f a d 1 e p d a l ~ s a t - i ~ c a n ~ r w r y ~ ? , d Z l l W ll~~ew, complete denture sitdon. All ~ ~ ~ t e o f ~ € # ~ ~ ~ m i a o l @ e n t v r h o ~ r C b s I I j m v r e ~ ~ ~ g a ~ c a m p ~ * ~ t o r e p l a c e ~ t ~ ~ partial denture, but harp mmhthg m m p t e d teeth in the anterim mmdi131e. Attho@ the m a a Q ~ ~ c a n ~ ~ ~ r ~ h e p a r t i a l - & % - - ~ t s f w ~ ~ ~ ~ d ~ o E t h e ~ o r ~ m a l t e t h e ~ l ~ o f a ~ d& very dimeult
Both, the dentist and patient b m m m to cmsidsr the fhmoial implidmu& of traa- plans. The best -mat p b are if* ptisntcmmt a E d the h a m e & The dia@~& must therefore d e l b m h &e sigptificasw of pmbIems the prisri~y of the need far t?m& m a 4.0 p m & tbe dsvelopnxmt of a plan &at addma- h e patienth nee& k W i ~ a n W t y t e r ~ ~ $ i ~ ~ must be d w t d to dlow edder&wi , & hWim care, Warred --& and d+ezdb h a t m u a
DATA COuECllON AND RKm?b&

78 M Two PrepatingthePatiem for Complete Denture T r m e n t , * I
. .
b% mip&ed for their c m t n i o n to the diagnosis. They must be kept confdmtial as a fundamental
' I Mcip1e of dmtist/ptient relations. Office staff -,. must be made aware of these principles. They
s h d d how tbat no patient i n f o d o n should he s h a d with d e n , neither through conversation nor through careless exposure on computer smem or written records that can be viewed by other patients.
Record keeping is rapidly moving to computers instead of the traditional paper chart. Computer- based record keeping offers some definite advan- %es in formatting, manipulation, and data #&id. Unfortunately, some program can limit mkud expression and thereby presmt a risk of lhithg the scope and depth of information &- d. It is not the role of this text to debate the mer- &a and te~hnology of computerization. The f6Ilmhg discussion of gathering and moding ~~w will not be s p d ~ c to either form&
I. P I a . . I
Questions The g a t b e g of inform~~tim &rta with the first 80~1taGt h t , or with, the patient. The informticm may came in a referral letter or a telephone d l $om the patient or another dentie Whatever the mm, the record keeping sbauld begin with this cmwa
A xeghttion form facil- the capturing of b& information &u& as the patient's name,
and talephone numbez. The name and ddm$ of the patient's physician, insurance infor- d m , rderral smrce, and any other information Wmightnwdhqumtorqukkrlccessdsucstn b re~oEded here, Gathering information with health qtwhmbs h a s e v d advantam, but ~ ~ d r t o t b e ~ a l m e . T b e i r r & n ~ - bga are wdstemy of pdetmmhd qwt;ons aid ease of patient response. They therefore pro- vide o quick m e w for the dentist. Staff should be d v k d to try to detect people wha might have wading problems ari- h m lack of education, ~~ disabihties, or language problems because the patient's f& language is different from the lan- g u g ~ used in the q ~ c ) ~ . For m t p p l e , a veFbal ahhimation of the quest lo^ will overcome the problem, but for some people the
help of family, a a or or ininterpreter may be
t t qdd . However completion of the q w h m a i m ia achieved, the dentist &odd review it and discus it with the patient. Because the responses pmi& only an overview derived h m s t x m k d i d ~ tions, tbe bbt must qh any suspicious incomplete responges in more M. Dimt a- v d w with p p l e will prohbly be more wed- ing #an written communication Thb h partly dm to its spontaneity and interactive nature If alu, overcomes a nmm1 reluctance by some peop1u to put candid or c ~ ~ d e n t i a l lnfomtion in writing The referring p m is the fm source of infoma- tion. If t h i ~ is anorher dentist, somethiug of the patient's attitudes or behavior might be M e d . If the referring person is a f d y member or &kd, it is wise to be m a cautious in fhe qudohg. H m , that person might reveal something of the new patient's hopes and f em and, specifid& the reason for the referral. Gimn a chance, mok patients will tell Wu own story. Indeed, most patients will have at l a s t at lay idea of their diag- nosis and a possible treatment plan. The dentist will learn this through cmful listening. An inter- pretation of this Wormation will assist the dentist in detemining what the patients' dental awarenerss is and how much education will be required to help patients understand their problems and what dentisw can do for them. Patients muat be assisted in this process by addmssing them at theit level of understding, avoiding unnecessary den- tal jargon or m approach that might inhibit the conversation. Some patients are reluctant to rwd information in heir health or social histories tU they feel is not pertinent to dentistry. A simple expht im of dentistry's reaponaibility for the health of the whole patient as dental treatment might a f f ec t it, or might be influenced by it, usw ally will help.
Whether patients have been edmtulous for long oP short periods, or are h u t tu be rendered edenw law, it is kimpottsnt bo d e w information a b d their progression from a full mmpietllmt of n&i- rd teeth to their present state. The primary pw- pose of thig review is to enable the dentist to b m restoration on original information and avoid replication of errors in existing prostheses. Sow

Cb@w 7 O l a m s k and Treatmaat Planuhg for hien- or PmntktI%lly Edmtuiw
mmixs*Eaq l i f b , ~ B ~ l f i r r ~ d ~ ~ ~ , x n ~ ~ ~ i ~ ~ b e U % e d GonhUdy. M m W d b dtsignd far ~ e ~ ~ ~ i s e a g Q l a Z i a f f a x ~ ~ v i s u a I ~ . ~ ~ * i t y d ~ m e ~ t . ~ ~ l y ~ U l i ~ b ~ W ~ r o o m ~ @ T ~ ~ d ~ ~ n , ~ ~ ~ b t w o ~lLOtbe~ps&m~t~attouIdbe ~ t o ~ t h e ~ t i m Q f ~ sbdmfi.Tbta&figlltmgwm~ ghumV~ItGUityMRh~srWifb~,snd~ I#& ef ,f am r€qnid CoIa l?&um is ~ a # m t ~ ~ ~ M o n b u t ~ f o r t h a ~ t d w h n o f m f t h . O m the p a t i e n r t & d d ~ ~ ~ y .
~ h m r r c h t o b l e a n a e d ~ ~ g t f i e ~ m t ~ t h ~ ~ a n d ~ t t i i l g i n f h e ~ c t i r . A m t b ~ b m o v ~ ~ orbpmdPBatbep&a=adEngwmor m d a p ~ o t l ~ ? X S ~ p d l r n o r ~ o f ~ f a d ~ t b ~ a p p e a r b b e s h m t o f ~ t h ? A m ~ a n y ~ o f r $ j w y o r ~ - m e n t ? B ~ p a t i a t ~ ~ g l a s s e s ? L t h e p&at o h t h g aid? Do the patient's h d ~ -c? & tbm f&d a m - -Are - t i f w l w m t e 4 suppkd?
~ ~ ~ e D d ~ ~ ~ , ~ ~ & ~ t b e ~ ~ a n , m a ~ ~ m d ~ o f t h e s a f i m d h d ~ ~ & e & j e c & o f a c m f u i v W ~ t i o n o f ~ m w & ~ ~ t i s t ~ u l d a d q v t a ~ ~ ~ - t h w ~ 9 6 t . ~ ~ t O m i d ~ . ~ ~ ~ ~ t a ~ ~ . ~ & i & f m p l & t . T h i a ~ a a d i & w t ~ ~ ~ a c a m p d m h a ~ n . B i f f * e s - 2 ~ ~ W t h e ~ w ~ ~ e ~ l a t e ~ t i o n i s 9 n S ~ t i l i z ? ~ m f o r ~ ~ c b i e f 0 o m g W i t l t i m ~ t of$iepatient%dad m ~~
ubn+ aid& kl Woti m btpM. The moufh ~ h & s b E t i a t h e ~ I o f ~ b ~ tia respwSiWti%$ %r many years. It allow fsF

80 ParITwa Pregarhrgthe Patient for Complete DcntunTmelrt
comfmtitblo viewing angles. It atPo enables the dentist to direct light to s t r u c w and recesses of inter&.
Magnifimtian is a. simple aid to vision A hand- held lens will m e in some instances, bud many dmtists flnd lowp convenient for most tasks, Beyond mapifmation, Ioupea can improve the viewing dis- and, with mare sapbisticated @a, cm adjnpt the viewing angle. The latter f- enable the dentist to work using less -8s- fid patme ahan might be possible with unaided
Still ~ ~ h y can be an i d in diagnosis 2and tteratment phmhg @ m d y by allwing the den- tbt to haw recorded imam available for study dur-
tbtt development of a treatment plan ttttt.aomal vihogaphy ia promoted as a meum
far pdmt educatioa I& well-lit, -4 image &@@xi on a m o w also prwides the dentiet with an excellent image f6r immediate viewing or for storage md ~~. The stored images supple- ment d m records for a variety of usea h m patient &ation to legal defenses. Tbe ability to view such rich visual iuformation when developing a treatment plan is a major asset.
Digithation of images makes computer- w h d vision possible. Although video images can be converted for tbb purpose, still digital pho- tography has developed to a practical state.
The mition from emulsion-based film radiogra- phy to p h o ~ u a b l e phosphor-based f h , CCD (charge couple device) atld CMOS (mlrnplemen- kry metat mride Bemiductor) image sensing, is well umhmay. Thh tmsitiw is mbhg patient exposure to radiation; is e h i d n g h g e incon- sis;tmcies related to c w c e n ~ o m , depletion, and m p m t w e of chmi&; and also is ehhating chemical &sposd as a problem. Eqerimcd den- tists will fd that diqlayed digital images dBer in ;~ppetuance f h m coxmatid mdiogmphs viewed with irmmittal light on a viewbox. Direct viewing of the mall fh image gives the perception of pre- cision in the image that m y appear to be lacking in h e dprged digital image displayed on a monitor. Tfbe qprent lack of predsion is a function of
~tnagtS~&rn and the resolution of the digital
image. Any digital image can be enhanced to bring out specific features.
Radiographs am important aids in the evalua- tion of s u b m d conditions in patients seeking p m ~ n t i c care. The presence of abnormalitits in edentulow jaws, or in the edentdous sqgmb of partdly edentulous jaw, may lm wuspectd because of the abseoce of clinical signs or symp- toms. A b n d i t i e s do occur and can be seen on radiographic emmhtion. These m y be fareign bodies; r e W tooth TOO&; mmpted t e a or various pathoses of developmmhl, Manmatmy, or neoplastic origin. Wogra* aid in dotemin- ins; the depth of periodontal pockets. They provide information about the bone surrounding the apices of pulpleas teeth. They can show the mount of bone lost around the remaining teeth and in the edentulow regions Figure 7-1). Thay also can shaw the relative thickness of the submucosa cov- ering the bone in dentdous regions, the location of the mandibular c a d , and the mental foramina in relation to the basal seat for dentures. They can uve an indication of the quality of the h e that supports the teeth md will support the dentures. Unfortunately, this information is not always reli- able because of variation# in radiographic tech- niques, exposure times, and developing pcedum. H m r , the denser (radiopaque) the bane appears to be, the batter the bony foundation. Sharp spicules of bone on ridge mats and spiny ridges also are appatent on dental radiogm&. These conditions may affect decisions about the types of impreasions and den--bw design that should be used
E x h o d radiographs can provide a general sur- vey of a patient's dentme foundation and m u d - ing smctum. Pmramic dental dogmphy is madily available far the convenient exambiion of dentulous and ehtulous patients. The dmht m,m be aware that such radiographs incorpoe ina~cu- racies d t h g from the tomographic principles of dGs type of dagraph Modem machines have adjustmenu to cmpemate for some. of t h e pmb lems, but they do not pro- precisely accurate pictures of the anatomical structupes. Mecation of struchlres is wmmon with this technique and is of the order of 25%. Because the machines are pro- grammed to caphue a predetermined "slice" of a m t o m y , ~ o u t s i d e t h a t s l i c e c a n b e m i d

J mrmr- 0
Figure 7-1 Radiographic evidence can be combined with clinical observations to enable the dentist to prescribe optimal treatment. The patient in A and Band the one in Care partially edentulous, and each requested complete denture treatment. In A and 8, clinical and radiographic examinations indicate that all the teeth can be retained and a maxillary removable partial overdenture can be prescribed, rather than a complete denture. In C and D, a minimum of two
I bilaterally located and suitable abutments to support an overdenture is not present. This patient was I therefore treated with immediate dentures because of the untreata ble periodontal disease present.

82 M l h Preparing the Patient lor Complete Denture Treatment
~ ~ ~ c ~ . ~ p e t ~ f i l m h o l d m d d ~ a i m t n g w m & l e f a r m k h g ~ ~ , C c p ~ c s r n d t e m p m m d h h joint ~~ are exsun- p b . Some largefamat views, such as the latad j o e w p r o j & i o n , c a u ~ ~ e d ~ ~ ' t h e ~ e a t h l d a c ~ l o r t d e d w i t h f ~ ~ t f t e f a m W e ~ i m r t d e w i t h h ~ c h a i t - si& dmd X-rag mru:hine.
I n h m I ' d r a d i ~ ~ b t h e M ~ ~ format k den&ryI with the mcd qpmch ~ ~ t i d f b r c a r i e s ~ s l n d & e ~ w i m o f ~ s q p o r t ~ p e r i n t p i - d ~ h ~ ~ f i t a l r p a b ~ o abnfaga. The d film size a l h s placement close a0 the struchm of Wwt, resulting in less magnification than ~IIOP&O mdhpqlyb s ~ , ~ s m a l t f ~ c € a ~ ~ ~ ~ ~ avoiddhhthofthehaq$ ~ ~ t h e v a l ~ d t M o r ~ t $ i s f o m p a t ~ ~ b ~ ~ i n edddow patients. M a x i k y tuhwi$iW, for ~ l ~ a r e ~ ~ ~ E n . g ~ ~ h s b u t c . m b e ~ ~ i t l p f d e o n ~ ~ f h . X n f & c $ W f Q m a r r a ~ ~ t r s e d ~ ~ ~ ~ ~ ~ a a y ~ ~ n o b ~ ~ ~ ~ f r m r r t ~ I ~ ~ ~ ~ b*&b,w--m*b t h l a f c l r m a t - M * w o f a - 0 d d b - m to ~ B e l d a m t l r e o c c I ~ ~ ~ f ~ b e e t h s n d e x p d ~ ~ ~ o r ~ t h e j a m i o ~ d e a v i e w o f a ~ m h L k W ~ a p i - d ~ , i t ~ a I l ~ h ~ p & o f ~ m ~ f ~ i t ~ i s ~ E y ~ I p - f a r l f b r d i ~ ~ e x p ~ o n o f t h e b o r a t ~ o r I m g u a f l y , ~ ~ ~ ~ o c c u r ~ a r ~ ~ .
~ i t L ~ t t a w e a l l a ~ i n d i a g - a ~ s i s , buch is p h b l y second only to vision in
i a r r t l o n , r n * ~ a o ~ * i S ~ f u l . M ~ & w ~ - d v e a l a r rid- and znylohydd rim, t y p i d y are tadw W o r e ~ ~ p a l p a t d t W ~ d b a t o l d c ~ ~ . T h e y ~ d l P e ~ d i a ~ ~ ~ & d w o f ~ ~ ~ a r r d ~ T ~ o r p a i n , i n ~ - of itrtrsoral pl#m to avoid amissio~. W~Ealfy, gna~W*I*aadCbks ,asovingto*
amas, the floor of.& TIPO*
and the tongue, Aside from noting the of & ~ i t i ! 3 ~ t O ~ n o t e m ~ o %QHl&ecmhwmd-,
~ ~ ~ ~ d a r y ~ ~ ~ wm# s h d d b &a&& The sides of midual d ~ ~ ~ h a f a l p ~ i n ~ t i m t r , the ~ ~ e a 8nd patient racfions ~ b m ~ T i w ~ 0 f ~ ~ f l a o t 0 f t h s
m ' i p W at$ p h c t m n of salivot by b w ~ ' M Shdd br: hbxk5&ated 4 ~ f 6 t ~ ~ i p n 0 f s a l h t k o m ~ dttct o r i f b aa tb and duct we gently qumd. Palpat@ of the tongue is essential fat' a f h m q & . ~ W ~ b e b i n s ( : q u e m ~ & e ~ l t a l ~ ~ ' R ~ e ~ & a t , L ~ e d t a p t r u Q e ~ ~ ~ m ~ ~ A i ~ b y & e ~ a ~ e , ~ ~ ~ ~ l d t b ~ w h i l E ! , wing a &nor &Y examine it, Palpation of h~ t~shwrdbdotsebdthI&to*mdri&t:; to left, O b v i o ~ , w mu5t be d w e qomy , ~ ~ ~ l a r e ~ b ~ ~ a n d ~ . r @ c w r o f t b e ~ u ~ T ~ d e n f i s t w i l l w r axtrawal p~~ to m b m w hd W? i n g s a a d e x p h & s ~ m c h a r e & e T W

Cbptcr 7 Diagnoris and Treatmaw Planning Por Edmubus or Potentially Eden~Iws miem

84 P u t W PnpadngttK Patient for Complete Denture Treatment
how the information is obtained, the objective is the gathering of specific Momtion h r n specific observations.
T h e p r t t i s a t % e x t s t i n g ~ s h u I d b e ~ d y . The obj- of th examhation are to determinemthe&tyof&deraturesmd how that relates to &e experkma aited earlier by the patient and to detamine the potentid for inpmmmt. If h e dentist armo of identify specific ~ a f t b e ~ t h ~ t c a a b e ~ e d t o ~ ~ f ~ p m b b , ~ o a t h e ~ - ingofnerrwdmtawL ~antmmmt taanbddngm a d i n g myage with~ut a mvig&oa chart. The m&mdarh&Wspoitedtlm btvqage we gmb&ly ming to pPoduFe failure k, l h f l m & m d ~ & m ~ ~ b e ~ b y v i r i s a a l ~ o n o r E g k t ~ w i t h e ~~~~~~t~~ the ~ p i n s o f ~ h h ~ S e O ~ & e ~ of the dmm a d the matetid of tbe oppmhg g c c I ~ o a , d l ~ m d ~ ~ o f ~ u s e a n d a ~ o f ~ ~ c a n ~ ~ . F ~ ~ , p Q r c e - ~ ~ ~ ~ ~ ~ t h a a ~ t i c ~ ~ ~ t h e r e a 2 n t t e t h w i l l ~ m m w e a r ~ ~~ teeth over the same of m. ~ ~ p ~ r ~ ~ f a f a t e e t h m d m ~ ; * ~ ~ ~ b t ~ l f t h e ~ e n t ~ n o t b e t o ~ fd, et#@aUy demlemhg them. Chppimg dm ~ I x ! t € t e ~ ~ f l a c k ~ f h ~ n y intfreoecru- h A n e v a l u a t i a n o f t h e f i t c r f a ~ w i l l ~ h o w w e , U i t L ~ t o t h e d m t u m ~ a m a $ h a w w e U t & e f h g ~ f d I t h e d c i , W ~ t h e b O t d e r ~ ~ 1 8 o u e , ~ d ~ ~ ~ o f ~ ~ a t i s l ~ d . ~ ~ ~ fbguEYw m3 d&ck$lt in extat or thi~hmis fail t o ~ m ~ ~ f b r $ ~ p o & * ~ , & ~ m L A ~ a f ~ ~ ~ l c a n b e - l id b tb t i a m d o e of the deoture Wore seating that will d &e distribution of tissue wntact, These pmdmts inch& pmam-indimting ~ s W d +d fmul&wts of *a- sim materials. A thin & of hv&ible bdrncol- loidhpre&on&d also &.Acbbopom ~ b f i t b h f ~ o f g ~ ~ n w ~ * d ~ ~ s u r f a G e ~ f t h 3 ~ , m t i ~
w u d h o f t h e l a b i a l ~ i s a t y p i c d ~ t i o a
The most important observation that must be made of the occlusion is whether the occlusion is in k- many with the patient's jaw relatiom. Large dis- crq?ancies will be immediately obvious if the patient is guided into contric relation and the occiu- sion is observed as the patient brings the teeth together and subsequently is guided into eccentric contacts. Small discrepancies may only be sug- gested by tooth wear patterns. The level and orien- ration of the c~clusd plane must be assessebo must the tooth-to-tooth and tooth-to-ridge relation- ships. The length of the plane relative to the size and shape of the denture-bearing m a also must be assessed. Denture teeth set aver the slope of the mandibular ridge as it approaches the retromolar pad are recopkd as a source of denture instabil- ity. Tissue trauma and a patient's inability to suc- cessfully use dentures can k p e n t t y be traced to errors in occIusion.
An evaluation of the esthetics of existing den- tutes should be approached first from the perspec- tive of the knowledge and professional judgment of the dentist. Second, there must be an evaluation in the light of infomation about the patient's natural teeth. The third phase of the evaluation must take into c&&ration the patient% views. These per- spectives must dl be reconciled to achieve success in the making of new prostheses. A patient will sometimes be slitidid with esthetically inappro- priate dentures because of conditioning through long-term me. patients often are reluctant to have sigmf~cant changes made because they would be noticeable to otba people. Patiants who desire change muBt have their expectations clarified because these expectations may not correspond with the dentist's intentions or abilities. The esthetic appropriateness of a patient's existing den- tures md the possibilities for improvement can be determined by camping the observed and cgn- ternplated characteristics with the recommenda- tions d e later in this book for selecting and arranging prostbetic teeth.
Soft Tissue Health Complete dentures are entirely dependent for sup- port on sofi tissue (mucoperios~) and undedy- ing hard tissue (bone). The heaIth and quality of those tissues gte therefore very important deternri-

I
C Plate 7-1 An extensive range of morphological tissue health variables must k dia- before treatment planning is finished and complete denture fabrication is started. Six different dentulous maxillae underscore some of the frequently encountered variables, A, This residual ridge shows minimal resorption and is covered by firm, healthy, soft tissues. Hamular notches are well defined, and no tissue adhesions are pment. This mam'llary bawl wt area offers an excellent morphological prognosis. B, This midual ridge, though substantial, is irregular, with b ~ n y undercuts and mall most- present. The left tuberosity is pendubus and mobile, and a large tows is present. A denture can be built on these foundations, but surgical considerations also should be addressed to optimize the b a d seat area. C, Anterior localized ridge mxption has occurred and been replaced by hyperplastic tissue. This tissue is usually wised before impmion making. When a patient's health precludes this option, a mod' id impression technique is employed.
Continued

Ft*iwr 7-1 d B 4 Home -re and a regular recall program were not instituted for this p&w Conwquemtk,, the basal seat am became inflamed, and an epulis multed. Tissue rest, massage, and the pmuiption of a tmiment liner should precede a surghl astsment in this patieM. E, Advanced midual ridge resorption is evident, with low mobile pwipheral tissue attadr. ments and &lieration of the barnu far nvtches. As a resutt, compmrnise In both peripheml and pxmior H a l seats will nqate a favorable prognosis for a retentive and &Me denture. F, A mrphologbf picture similar to the one in E has been rectified by a prepmithetic sulcus deepening with skin g d t placement This p d p t i o n used to k frequently u d in the mandiMe but has k n uirtrta1ly &tip& by implant wament.


7 mt'd D to F, Hyperplastic replacement of the entire residual ridge does not usually provide a firm denture-bearing area. However, surgiwl excision may result in a significantly duced basal area, as in E Extension of the denture's posterior lingual flanges usually will allow for a stable denture in E. This objective may not be fulfilled in F W u s e of the unfavorably high attachment of the floor of the mouth. Also notice the virtual continuity of r n l i l e mu- in the floor of the mouth and the labiatlbuccal vestibule. They are separatd by a thin, mobile, fibrous band. From a rnorpholagic. paint of view, this does not provide a favorable prognosis. Preptofthetic surgery for placement of osseointegrated implants is likely to be needed in these situations.


86 Part Two Preparing the Miant for Complete Denture Treatment
h m g die m m emmm hsions f a d in the IIIQII& of sdmtuhs pathb rn padoepithe- ii-~t$ hypqbm, pnrpiltary hypaphsh, apht- h u ~ lichen plauw, hprkaatosiq 1- sad e p a s flwmmm (hpxpbm-f. ~ b b l S ~ b e r n 0 r e @ 0 ~ h ~ l 8 , ~ W 8 d c a 8 a n b e ~ ofmalipanciers. ~ ~ b e ~ d ~ i n ~ d ~ . i f ~ a m n 0 t ~ ~ ~ ~ C a n ~ P o r ~ p a t i ~ d - E o r t h e ~ I f ~ i - W I W ~ O W ~ ~ ~ ~ ~ ~ P S Z ~ ~ ~ ~ W ~ ~ . T h E i e ~ ~ d ~ f ~ ~ t e S B 8 . W
a r e n m t ~ i a p e o p t e w h o a m ~ ~ ~ - w * ~ b u t : *
all ages. 'XZter ~~~ of ~ t h d o g o t ~ w h e m ~ theylxmlerrmimpm-
oagt. Mmb matt be qudoned a w t their k n t w l ~ ofmy tmpicim fia- Qumtiming # t k O M r n & & ~ ~ t ~ ~ f ~ - w ~ ~ ~ w w - , ~
The ptim's pmxption uf WWIW a or^^^.
T##,m101: o f b m w m a revad d h t &-*-ill
~ a f * ~ W ~ , I t ~ ~ d b e w h i t e s m r ~ ~ a ~ f h a t h l x m t m u - ~ S n d L n o a r ~ G S m ~ ~ ~ ~ ~ ~ ~ l ~ m a ~ s e e d
~ ~ ~ b & ~ t o t l l t ~ ~ ~ ~ o n ; $ ~ ~ . A l ~ ~ ~ a r k f m n a v a r i G t y o f m m . e s , f m r - ex in^^)^^,
c & t m r m m t ~ b o f k - o f t h e
m o a a f i ~ ~ ~ c i o a s o f C . a&m* t i ~ A ~ m q b e m n d e ~ a n d ~ ined for pseudohypiae. Smears also may b C U I ~ t o ~ ~ c l i n i d ~ .
HyptSpW bfohe t b tm UmAated with &fib+ i i n g ~ i s a ~ m f f t l ~ . H ~ ~ o y i l l b 8 ~ h * W U n f 1 9 ~ ~ r i d ~ a n d b d e r ~ , m a ~ o n e i t h e r t u ~ ~ o r t a ~ ~ 0 ~ 1 o f s q q w r t @ b a e . w h i m b o r m e ~ , i f ~ r d d i n ~ ~ f Q ~ ~ a s ~ b y $ r e . & i q % d e a t u m . m ~ o ~ w i U t e ? n a i n a t W ~ W w i L ~ b tic time, Thie mmdition seems to appm appearom tb ~ i n i n ~ mareb. Onthe mandibb,itis ~ ~ ~ i n ~ a n b e r i u r ~ ~ ~ e ~ ~ a m d ~ y ~ i e r b u t ~ ~ ~ a o t r e W i n m m ~ a n k r b r exmcticm sites. W I u d tmm fmm dmw& v a t i c a d ~ i m o f t h e j s w s ~ d p o r r t e r i o r t o & w a r ~ ~ t e d i n t b d o r r u & i o n s a d c w * t O W p r o b i e m . ~ ~ ~ - calry-*-flwW,~kY ~ 0 f ~ . t I r a t h a v e ~ d ~ ~ t s f l ~ ddgemppo&&.mwNpmluwa~hypeat g ~ w ~ ~ ~ ~ ~ ~ ~ f ~ s w f u n r , S i d m l y , the will @ifem& h i & a loow-feg fhge. The labial &e of the ~ ~ & ~ 1 a r t i d g e L a ~ s i t s , P ~ ~ i s ~ ~ h ~ m c e ~ ~ t o ~ 5 i ? & e ~ Q f t b p @ l a ~ , i n t h e a w & o f t h e ~ o f h g 4 m n b k t r e ~ . ~ t b i s f i s ~ i B ~ ~ d ~ t b s e n d ~ k a s ~ p @ l l m y h p r " p w u . % d a q cwvh3 of p r r p m y ~~ m p r o n e t o i n f e G t i i o n . T h e M ? & d l ~ y L found to b C. aZ6Wm. Olwbuly, -tion must b e t r e o l t e d b e f o r e n ~ d ~ a r e ~ b u t x e c u p . retlce is like& dm3 &I hyperpwc t ime a mrld .
E x c e s s ~ s t i s s u e ~ m ~ & way n d - m mcom Mthwgh t is s ~ ~ ~ i t d i o e s n o t ~ ~ ~ ~ , m i s i n g a r t ~ t o i t a ~ di&€nlfh. Theltldhy**, ifflbrw, m a y ~ o n t y ~ P - ~ ~ b u f m g ! W b e m l q g e a a r t o i n ~ w i t h d l e ~ p ~ ~ a f ~ d m l p l a r s e . Iftheg.a~emob& ~ w i l l ~ ~ s t a b i l i t y o f t h o ~ * m a n ~ r @ o n o f t b e m a x i l l r t r y ~ d u d ~

ChqW 7 W s i s and Tm&mmt Planniq for WWilous or Potantrally EdenWm-
Blone Bone is the rum, y& physiologically @anlie, suppost for b* and . Ib hand^^^^^ ~ s ~ d l d ~ B m ~ * l e ~ a m ~ a a k d ~ ~ ~ s w h a a M B a d W , W W k * & e o * l m s p r o $ e i n & ~ t a d w i t h ~ a k r Q - b w a $ Q a d ~ - a n d ~ ~ . A t h w f o r o g h c I i s ~ o f b # a % & i ~ o f s ~ * h ~ @ ~ d ~ ~ ~ ~ ~ ~ ~ h ~ w

M Psrf T*m Preparing the Patient for Complete Derrture Treatment 1 especially &after menopause, are particularly inclined to have osteoporosk. Local bone hsease and anatomy can be significant factors in prostho- dontic care. Retained roots of teeth, abscesses, cysts, and neophsms bave to be iden=ed and dif- ferentially diagnosed. Appropriate tmsmnt must then be p h e d . Some retained roots will be par- tially resorbed and dr fficult to distinguish h m sur- rolrnding bone. Atternpts to remove these surgically often am frustrating and only padally successful. If such roots are asymptomatic and appmtiy cov- ered completely in bone, they are usually best left uixbmbed. The patient should be made aware of their presence and the rationale for leaving them. Roots covered only by mucosa and roots with clearly &fined periodontal ligaments, associated cysts, or abscesses should be remwed. Neoplasms q u i r e complete diagnosis and treatment.
The anatomy of strucnrres particulariy related to tb -on of prosthodontic t r e e e n t is dmchd and ill- in Iater chapters. Diagnosis in prepamtion for new dentures requires a detailed
''on of the specific anatomy of the individ- ual patient. Many h t i a m wilt be found. Some will present: no special problems. 0th- will require accommodation in impression making. Still
tl 1 others will require surgical correction. Sharp and spiny residual alveolar ridge cmts can be products
t of preexhctiotl h n e destruction, trauma during L extractions, or postextraction resorption. Ctestal
bone irreguldties and increasing radiolucency toward the ridge crest suggest this in radiographs showing the ridge in profrle. Palpalion usually will reved the sensitivity of the mucoperiasteum over the crest. Because of the sensitivity, spiny ridge crests cannot contribute much to the support of a denture. Surgical reduction is tempting and some- t h a indicated, but the redudon in ridge height adversely a£fects the stability of a denture. The ridges an sometimes be kept for their contribution to stability if they are relieved of direct pressure by using a sel& pressure impression technique that gains support far the denture from other areas. Severe resorption will expose the mental foramina on the crest of the m&Ibuiar residual alveolar ridge. This may be seen radiographcally. The expo& mental nerve is sensitive to pressure. The patient wearing dentures may report a sporadic
*hooting pain in the distribution area of nerve.


80 Part Twa Preparing the Patient for Complete Denture Treatment
at its mferior border than at the residual aiveolar ridge in the posterior part of the mouth, resorption, in effect, moves the left and right ridges progres- sively farther apart. The mandiular arch appears to becam wider, while the maxillary arch b m e s namwer, The cross-wtion shrinkage in the molar region is downward and ourward. The cross-section &idage in the anterior region at first is downward and bachad. Then, as shrinkage continues, the anterior part of the basal seat for the mandibular den- im mwes forward These changes must be noted at the time of the examination to plm for the resultant problems of leverage, occlusioa. and tooth position for esthetics.
Dentuse stability is d a n c e d by parallelism of the prhmy denture-behg areas. When natural teeth contact in centric occlusion, the surfaces of the maxiUary md mandibular arches are, in effect, parallel. This is a very stable relationship. Even though denture teeth wilI be set to contact evenly in centric occlusion, the surface of the arches that support the dentures may be resorbed ou? of paral- lelism. This dimhushes the stability of the dentures. This problem must be noted at examination for consideration in denture design. For example, implant-supported dentures are especially helpful in this situation. To determine this relationship, the paaim should be coached ta position the jaws at the d c a l dimension of occlusion and hold the position. while the exmining dentist parts the lips with fmgers and mouth mirror to observe the ridges, The relationship also will be obvious on mounted diagnostic casts. Mounted diagnostic casts &o will m a 1 the amount of interarch space. This is important information because a lack of space can lead to denture failure from improperly positioned teeth. Excessive space usually is related to mere ridge resorption. The resulting instability aIso limits denture success. Evan when severe ridge resorption indicates excessive interarch space in the anterior of the mouth, the posterior should be examined to determine if there is sufficient space. If some teeth are present, they must not interfere with the placement of the occIusal plane. Extraction m y be indicated if a tooth is so extruded that its occlusal surface is above the desired occlusal plane, unless it can be shortened mfficiently to be on the same pIane with the other teeth in that dental arch.
Iftbemmikrytuberositiesatesohrgethat t h e y w i f l ~ t t h e ~ l & o n d t h e ~ c c l u s a t plane or q u i r e the omission of some teeth or pre- vent the correct distal extensions of the dm- bases, they could be ~~ reduced The fad t f i a t o p a t i e n t r n a y h a v e ~ ~ g d e n ~ ~ not rule out these m~deg, I h t p r e b w a r on old denturea over the retromolar pads and the maxillary tuberosities suggests m intmmh space deficiency. Radiographs will srhow whether hgp tubmsities are bone w an owgmwth of fibrous connective tissue. Where possible, the reductim should be Wted ta the fibrous tissue. The resul2- iog closed soft tissue wwnd heds quickly and pr~&ctabIy, S M d bone have to be removed, remodeling is initiated, m a b g the result leas p dictable and proloqing the haaling. Scrmebm spm can be gained by dissecting out nonemential contents from large retrornolar pa&.
Border h e s R&m!hn of a co~pfete denture is partiauy I y d e n t w an effedw hrdex d, The mil is mated by close!iy adapting the den- to its surrouuag tbmes. Th&ore the tissues that will surround th denture flanges and the spaces that will accommdate them should be e x a d m i thoroughly. Noting their specific anatomical char- acteristics and &nemie - the ~~ wiU help in designing the dm*, in detemhhg the size and ship of a mstm tray, and in d u 8 t ~ hg of the ixqmmiollg,
The labial d c i anterior to the b d h u h are o h obliteroraed by the lips resthg against the midual dvw)br ridps. With severe ridge resorp- tion, the 1-1 boundmy is undefined An d* mate of the dq@ and I&- wi& of each d c u s will help by setling an objective for impre+ sion mafring and ul-ly for the height aud thickness of tbe labial The goel is to prp- vide a denture flange that correctly supports, but doesmtdistort,thelipwfiile&mcregtingabor- der-sediq contact with the bwndary ti- with out imp'qmW. EswntiaUy the aame can be said of the buccal sulci, wfiich are I ~ t d distztl to @ buccal h u l a . Howver, some r e b d stmtms must be examined for their influmm an the spw. Latad jaw mmemunt will advance the comoid process of &a mandible toward tb maxillary tubemdty. In BO doing, it m y obIit the aulcw, T

&Kva Saliva a M dom not the ~ k m v a . ~ t h e h m r a t e d t b e & w s i t y a r a ~ t o ~ ~ N ~ ~ & ~ ~ i 8 ~ 1 m Y m i n . A f l o w a f ~ * ~ ~ d l i s ~ ~ ~ ~ p t n d ~ ~ o n o f ~ ~ ~ ~ ~ e s r t r u f i e t a . t h e ~ l e a t e , b a t & g I s m ~ ~ - d k o b o a ~ f m t m h ~ f h . Many patien& of d m t u r e e *, llowwtw,
~ ~ t e d ~ ~ ~ * raoeived mdi&cm * kkm

92 Part I'W W?p#rhgdx Patient for Camplete Denture Treatment - m@lon ofthe s d h r y glands u d y have glandular
hmct ion with resulting reduction in d i - ~ f l a w . h I n a a b s e n c e o f a h i s t w y o f ~ m or a n t i s i a t ~ ~ drags to aqdah didllish€ld flows, f w t b r invwtigatim is warranted. The g a n d s ~ ~ m a y b e ~ d m d u & c a n b e Madad, dhgh the latter d d wud@ prodwe &ate distrer~a Often the palatal gands are d a t m p i in patients who have wrrrn a complete ~ ~ f o r r n q f l y ~ . T h ~ a w i s m l l y ~ a t r a p h y ~ t i n g f m m l o s t ~ d ~ ~ ~ p p o x t o f t h e d e n ~
TheWwvityismrroundedbym~les. J a w d m~~~ atethepmdum of muscle acthitye If the muscles are mmg aad their wdl w d h t d , thq will help the @enf we a cor- w ~ - - C - @ I p a o r - ~ ~ ~ ~ e s , ~ p w r ~ l ~ ~ o n & l ~ f r o m d e n t u r e ~ t y a n d ~ ,
M t d e t o l l u s %tweafthefa<iawsis ~ ~ ~ s ~ o f ~ ~ o n , T ~ t o n e ~ i s e ~ t o o i x t r o q o r t o o w d t i s -.As a resuh, completing clisxical proce- ~ ~ r e q u k m m t h s n ~ u s d r r r n o u n t o f he. If the muscles are too tense, ch& atld lip -&this will be di8iculG if SWK, the lipg ~ ~ ~ k * l e ~ y ~ ~ 0 1 1 ~ P ~ ~ m y ~ e r n e r e t i m e t h a n u s u a l t&m to aee the den-. Opmnd Optlmaffurmctioning of &B~Ittbdfacidetrpre~mmuscla~ ~mpprtfnrmtb%m~teethandridg€aar h c m d y da@d and built ~~,
M ~ ~ l m w s a k r Wrdinatbn Good mwcular ~ i a r a d ~ ~ f ~ m t r e ~ ~ ~ t h e & e c : - * ~ 0 f G D r n p ~ ~ * & r n h ~ M ~~ cmstmctim. Fot example, wkm tongue
of a ~~ i q m s s i a n , the thing, dh4hz1,mdrrmol~ntofmwmmt arecritical to - s w a s a of Xhe mol- Similarly, modmion Q*-isiInq--con- mmiunwtlduse.
. h~~ lar t ;k iarg~ty tomwethemmdib1e ~ 4 b ~ p l a c r ? a t t l w ~ h e ~ o r l s t h e ~
Tongw Apart EfDm the -1e of n l o w m m c m a h a t i 8 p l ~ ~ ~ ~ *owly menti& tolrpluep3sitim ~~ ~ m d w ~ a i n ~ e t e ~ f u a g t i & l g . i % ~ ~ ~ ~ ~ ptientofattborderof*lmgtlal~~* m a b I ~ & 0 ~ ~ ~ ~ ~ & 1 * k j g f o r c e e O n ~ ~ ~ o f W ~ flan$@. Norkn&y, t h G tmgue w b


94 M TWa Preparing the Patient for Compplete Denture Treatment
&%lip Adentam withan ~ b u i y ~ c l r h b b i r t t mg(t~metgie*Hp~tokmm* ~ ~ ~ t h i ~ ~ ~ ~ ~ ~ * E f p ~ t h i c k , o t s h o r f . A n oblitemt&d $Wtmm or mtOl&ial fold suggests -ssiw qqmh T b problem mi lip fdbss is
~ B a c b g w . I f ~ € ? B l d s t i n g
& $ l ~ ~ t b e n e # a n d c a ~ ~ ~ b l i p ~ f p l l . ~ t i m e w i I l ~ ~ i a a f t h e w a x * .
Wdigjht ~~ in the labiolingud to& psition ~ m ~ d m g e . i n t h e h p m t o u r , T h i a d a h b & ~ W t h g t e v e m m e r @ p h g o f ~ g & @ ~ t h d a u e o f t h e l i p . B o t h ! h e a r c h
individual tooth positions we l i p give thebtbt,aWnaora ~ ~ i n ~ a r G h f o n n g a d --wiw=t-*-
* ~ i a ~ I i p ~ u ~ . on d tooth p & n is dwrt or iwmpem @. The for a l-naW show of
~ ~ ~ m d ~ o f ~ ~ b w a s w % l l .
I: 't
DIAGNOSTIC FINDINGS 1:611
Obvlous, Congwe* or lnmgnrent? Some diagnohc f-s have obvious sign& came mdsuggmttrewwntthatiS j~9t'aaobvhw, 'We incidence of this wil l hmem as a dW& becomes more q e d d in treating aimbulotw r m d ~ ~ ~ . ~ ~ ~ ~ ~ i ( l I 1 8 ~ k b a s h f o t ~ l ~ a W e n t plrm Hmwm, such a tramenk plm $ l l ~ u l d b e l ~ m ~ o ~ ~ i n ~ o f ~ i n g . T h e ~ r n a J r l e a d t 0 ~ ~ ~ ~ fmtmtdtheoW~isbdekmhifwchfm& wm cmsismwitf t&f- thath been&.Dtberer-bhxatbedb eraethgtappearstobepmxWdthepWe& ology? wmgmity of iBfmdm gabred w a ptient ~ i g d s the need fdr fmihr irwestigatim
Summary A&agnoskmustktrasedonmWinf- tionandrmt wmmthrtlae F ~ g a f r o m t h ~ ~ tory and - * . W k o findings carmot be accollnkd faa, fu r tk ilmsrim may b i n ~ f p m a t e d i n t o ~ ~ p ~ p r ~ d a d s ~ action wMhd not be in ja r i~~~i to &e patient. A irumt m a r y u f t h e ~ ~ i n d e v e l ~ o ~ ough dagp~osis can serve as a primer ad
* . cbmmmg patiat pmblms (Box 7-1).
TREATMENT PIAN W 1 NG ~ t m # t t p I ~ i s ~ ~ o f ~ ~ - b I e ~ o p t i a n s w i t h ~ & d ~ &&y anan& the &&mat in order of ppimity b u t i n k e e p i n g w i t b n ~ d a r ~ ~ !Kquenm.Thep~o~ess:q~abrlwad~l*U t r d m d possibilities and W e d knowledge of p a t k n t d - b a m - A ~ ~ ~ p l a n n i n g w i L r def"i&ncy in dbrddaese a@c&s o f k n ~ w ~ p b m t b & p a t i t n t i n j m p n q ~ ~ O r ~ ~ L T h e ~ a l s a ~ l e s i @ ~ ~ ~ b i n o h r d e m a ~ p h * t b t ~ t b E s t t h e ~ f ~ ~ tenttabliWhtimaTeqrxiring-~

y-
apkr 7 Diawosb and Tremenl Psanning for €&Wlous or ~ i a l t y MmwlPus M @
TREATMENT PUN
that will a d k w a partidm patient%
7-2).ThattreatmentwinbW in a logid sqwace snd wilt include adjmctb care. Its detd rrnd clarity wil l pen& estbatm of qwr- e t t o ~ t i m e a n d ~ t f m a , a t ~ a s ~ i - aMfm.Ftt ihrretohfwers@aplsnmh idhued -consent by the pdmt imposaiile. Roceeding without Mmned m t expm+s the dentist to p r o b 1 ~ ranging b m loa$ of patient ccmmalm to m~ulty with fee mudon or even liwon. hdqua te plans dso ma3ce it difficult
or -ibIe for staff to do their part m maiatain- hg a dolivery of ptient m e .
Tmafnrent Planning Is Problem Solving hblem-dying techniques w d y inv01w I L 1 ~ i s o f a ~ e m , ~ i t i a t o c o m p o - ~ w h e r e p c m i b l e , ~ ~ a n d ~ a list of possible comporteat mhhm to dtimately construct a cmphensi.re ~Iu t ion . Th0 proMems are not salved until tbe ~l~~ are implemented. U n W mfutlans might reasonably k thought af as hypotheses in need ufteshg. DmaI treatinent pIanuing might be &ou&t of in the same manner. The first step is a carem analysis of the diagm- tic findings, paying particular attuntion to sp i f i c curupcm- (see Box 7-11, With howledg% of these needs, the second s&p iav~lw~ developing a lhst of possible means of addressing them @ox 7-2). Although this may be a -he, tiaePe are times when a written list #gists fhinkinn. The integration of these c;mnponent solutions info a mmpkmive t e e m plan mydm an s b - tim of the impad of the components on each Qther.
The hfutching Pmas The i n fodon &odd be gathered on in&- vidual patients and 1 e techniques for gathering it are d i s d earlier in this chapter. The &b of the p s c OMS debmine the d&&
--+-~-~).AB~E&M sapply a set of oomp1ete dentures a an d d & w patient does not require very m p M s h a i i hit&- kg. Left at that iwl , ,the reid& might be a p d l p unsqixistimtd Truly profemid are require& the dentist to consider dl information @wed and appropriately address it iu the tmbnent plan.

I %6 )rtl2 Two Pmng the Patient for Cmplae teture Treatment
. I
Hgure 7-2' Why treatment pian.

tJllptM 7 Dia#m& a d fm#?wnt Planning for Edmulous or hteda t ly 6demuh Wenis 97
Figure 7-3 The treatment planning process.
%re are many occasions when the patient will benefit from preparatory care such as the treat- lent of candidiasis, the repositioning of frenula, &id the reduction of fibrous maxillary tuberosi- -am. The presence of active periodontal disease
make prediction of the form of the postex- .&action ridge impossible and thereby suggest the me of an interim immediate denture for the patient who is about to have remaining teeth atracted. A history of denture dissatisfaction, the b c i a l meam to afford quality care, and find- ings of a deficient, denture-supporting foundation but adequate bone suggest the patient would ben-
efit from implant-supported prostheses. Design, fabrication, and-delivery of prostheses as the focus of proathodor$ic care are discussed later in this book. The dentist must customize ihe care for each patient.
The information accumulated from the diag- nosi~ must be systemrttically analyzed to identify each patient's problems and to determine their related needs, A problem list for a patient might include (I) large areas of dentulnas residud alveolar ridges and (2) tbtee remaining teeth that can be restored only with the aid of enddontic and periodontal treatment. When a patient is

g8 Raft Two Preparing the Patient for Complete Denture Treatment
' Patlent Edmtioa: an W and conthing activity i n k p l to, d supporthe of, a ~~t pIan
Should facilitate
lrigum 7 4 Patient education.
unhappy with his or her a p p k e and mpresses o &ire for replacemmt of missing tea& the den- tist* k l m q b d t o decide the p h t needs a&&w @dodontic, peridontic, and grostho- don& wmmnt s address all problem. EWwq if the patient hati limited fmmcial rewums, be at she is more likely to d a t e the prdhm into a need for ~~ and complete dentmi. A g m a m t must be m h e d an the 9
nee* and tho oP& to qplieii This may require modifmtions in a treatment plan as Fust conewid by a dentist One might think of this prwess as transforming a dentist- oriented lmatment pfan to patientsriented -- merit plan in light af a variety of hfhmcing facton such as ~ [ ; ~ d b ' u i & aind fin;tnces. However, the modificati~ should not be such that they would jeoprndiaa the health of & patient.

mkhg dmtd do so with of tln&&ming and expidlcc. The
~ ~ & 9 n s r i u c a t i o n a l t a o 1 t o ~ t h e iikt's h d of U n i i m t a n ~ g of w&y and & - o f h o w ~ p ~ ~ e n t B m T % v i d d n e a d a i H d m m r g h
~ e n t ~ m i s r r a d d e l e m a n t &sht polre that & ~ d d start with the cm- kd**(F*7-6).
i n g ~ W m ~ d 1 b e ~ m d W ~ t i o n s t h a f $ o w i t h i t , T t i s d t o ~ W BpQd treatment plans are conducive to g O d car6 r r n d t o r n u t r r a ? ~ ~ ~ b ~ prrti*.
~ J P . ~ A A : ~ ~ ~ ~ ~ P ~ u ~ Q - Isms: a mmmy, Br &at 3 f 89:1284 W 2400.
~ D A , ~ T P , ~ \ r e a ~ B R L ; ~ w ~ d und ~&Uofmial m&la#, M I & , 1992, WB SaunderaL
Morris R& PrkdpI~s qf $&tat tmdnwt p l d w , ~ I W , W & ~ .
Owdl B, Kay* AF, Cluleaou a hsth~dorrrtm: principle a d d f m t e g h , Lodon, 1996, Mosby-Wo*
~ A S , N ~ I C , ~ H H : Gwh~&dsnw:mg d a # l h d & S t ~ 1 9 9 1 . ~ ~ ~
unitsa---mm* ~ ~ ~ ~ ~ , d 6 , R D c ~ W 19%-
~ B p e i a l C a n v e a t i o n , ~ . r n ~ ~ 4 $ ' d m P d w = -

hprosthetic Surgery! Improving the Fatiento' Dentum4karing Areas and'
k arb, 5, R045 Bryant
Y'" - . 1 1 .
The vast majority of patients for whom complete denture therapy is have already k e n weamg dentures. As suggested earlier, there is a risk in patients wearing dentures for prolonged periods. Thls risk, or biological price, manifests itself in a number of adverse changes in the dentures' founda- tions. Consequently, sweral conditions in the edentu- Ious mouth should be corrected or treated before the construction of complete dentures. Often, patients are unaware that tissues in the mouth have been damagd or deformed by the presence of old prostheses. Other oral conhtiom may have developed that must be managed to increase the chances for success of the new dentures. The patient must be made cognizant of these problems, and a logical explanation by the dentist, supplemented with radiographs and, where quire4 diagnostic casts, usually will convince the patient of the necessity for the suggested treament.
Treatment methods to improve the patient's denture foundation and ridge relations are usually either nonsurgical or surgical in nature, but can be a combination of both methods.
NONSURGICAL METHODS Nonsurgical methods of edentulous mouth prepara- tion include the following methods.
Rest for the Denture-Supporting Tissues
Rest for the denture-supporting tissues can be achieved by removal of the dentures fiom the mouth for an extended period or the use of tempo- rslry soft liners inside the old dentures. Both proce-
dures allow deformed tissue of the residual ridges to return to normal form (Figures 8-1 and 8-2). Clinical reports and experience also support the merits of regular finger or toothbrush massage of denture-bearing rnucosa, especially of those areas that appear edematous and enlarged.
It has been demonstrated that tissue abuse caused by improper occlusion can be made to disappear by (1) withholding the faulty dentures h m the patient, (2) adjustu@correcting the occlusion and refitting the denture by means of a tissue conditioner, or (3) substituting properly made dentures. When the latter is undertaken, it is necessary to allow the soft tissues to recover by removing the dentures for 48 to 72 hours before impressions are made for the construc- tion of new dentures. However, it generally is not fea- sible to withhold a patient's dentures for an extended period while the tissues are recovering. Therefore
VL temporary soft liners ha been developed as tissue treatment or conhtioning materials. The sohess of these materials is maintained for several days while the tissues recover. Tissue conditioners consist of a polymer powder and an aromatic ester-ethanol mixture (see Chapter 12). They have been widely used in dentistry for years and provide the dentist with an expanded scope for short-term resolution of patient problems.
The major uses of these tissue-conditioning materials are tissue treatment, liners for surgical splints, trial denture-base stabilizers, and optimal arch form or neutral zone determinants. Clinical experience indicates that soft Iiners also can be used as functional impression materials when relining or refitting complete dentures (see Chapter 24).

Delayed elask Instantaneous elastkreeovery
Wrm 8-1 Typical behavior of tissue under a constant pressure tuad for 10 mlnutes. Notice the 90% recovery within 8 minut16 after removal of the pressure Total recovery requlres 4 hours. {From Kydd WF, Daly CH, and W h e e t jB: Int Dent) 21:43O-l41,1971.)
Minutes Figura S2 Comparison of respan= to tissue loading and removal of the load in an
, .~l efderly adult and a young adult. The compression curve is essentially the same. Howwer, the removal of load shows definite in rate of recovery. The load was 11 glmm?. (From - . Kydd WL, Dab CH, and Wheeler 18: lnt DeRt j 21 :430-441,1971,)

102 R R h a Preparing the Patient for Complete Denture Treatmefit
Occlusal Correction of the Old Prostheses
An attempt should first be made to restore an optimal vertical dimension af occlusion to the den- tures presently worn by tbe patient with an interim resilient lining miterial. This step enables the dentist to prognosticate the amount of vertical facial support that the patient can tolerate, and it allows the presumably deformed tissues to recover. The decision to create room inside the denture depetlds on its fit and the condition of the tissues. The tissue treatment material also permits some movement of the denture base, so its position becomes compatible with the existing occlusion, apart from allo\krmg the displaced tissues to recover their original form. Consequently, ridge relations are improved, and this improvement facilitates the dentist's eventual relation registration procedures.*
It also may be necessary to correct the extent of tissue coverage by the old denture base so dl usable supporting tissue is included in the treat- ment. This cumtion can easily be achieved by use of one of the resin border-molding materials combined with a psue con&timer.
Good Nutrition A good nutritionaI program must be emphasized for each edentulous patient. This program is espe- cially important for the geriatric patient whose metabolic and masticatory efficiency may be compromised (see Chapter 6) .
Corsdjtioning of the Patient's Musculature The use of jaw exercises can permit relaxation of the muscles of mastication and strengthen their coordination and help prepare the patient psycho- logically for the prosthetic service. If at the initial appointment the dentist observes that the patient responds with difficulty to instructions for relax- ation and coordinated mandibular movement, a program of mandibular exercises may be pre- scribed. Clinical experience indicates ihat such a program m y be beneficial and the subsequent regismion of jaw relations facilitated.
%8 will in !am M t a t e a0 occlusd adjustment thar can ke acpom- @ h d intrmdy m extraorally (with an articuktw).
SURGICAL METHODS FrquentIy, ccertain conditions of the denture.-bearing tissues require edmtdous patients to be treated sur- gically. These cwditions are the result of u n f a d l l e morphological &OI~S of the denture-- area or, mon commonly, mult h n long-tan wear of ill-fitting dentures. The obj&w of prescribmg a preprosthetic s ~ c a l procedure are listed in Box 8-1. It must be ernphasizgd that these intewentiom are hkqumtly mandatory undertakings. It is often far easier to make alterations in the prosthetic tech- niques and materials used than to subject the patient to a surgical intervention. The key consid- eration is whether a good prosthodontic prognosis will result from the surgical outcome. In fact, it is only the provision of dental implants that has been shown to have the best prognosis for morpbologi- cal problems associated with maladaptive denture-wearing behavior.
Correction of Conditions mat Preclude Optimal Prosthetic Function Hyperplastic Ridge, Epulis Fissuratum, and Papillomatosis The premise underscoring sutgl- cal intervention is that mobile tissues (e.g., a
Obj ytives of Preprosthodontic Surgical Prescript ions
1. Correcting conditions that preclude optimal prosthetic fundion Lmld or generalized hyp~plastic wlace- ment of resorb4 ridgs Epulk fissuratum Papillomntosis Unfavorably located frenular attachmnts Pendulous maxillary tuberosities Bony prpminences, undercuts, a d ridges Discrepancies in jaw size relationships Pressufe on mental foramen
2, Enlargement of denture-bearing areats) Vestibu loplasly Ridge augmentation
3. Provision for placing tooth root analogues by means of oswintegrated dental implam

chapter 8 Preprusthetic Surgery: Irnpming the Patieng Denture-Ewn'ng Areas and Ridge Rdatlom
8 Figure 8-3 Preoperative tA) and postoperative (6) views of the maxillary buccal frenum (arrowhead) in an edentulous patient with an unrepaired palatal cleft. Excision allowed for optimal extension of the denture flange into this area.

1w Part Two Preparing the Patient for Complete Denture Treatment
ideal atadon and border of the flange of the denture. Tbe upper labial h n u m in particular may be cotspmd of a strong bmd of !~IYMu$ comec- tive tisaw that attaches on the lingual side of the ad sf the residual ridge. This tissue should wWy be removed surgically. Frena o h became *en? as a result of reduction of the residual ri&w+ If muscle fibers are attached close to the crest of the ridge when h n a are removed, the muscles d y are detached and elevated or & p m d to expose the amount of desired ridge height The hnaectomy can be carried out before prosthetic treatment is begun, or it can be done at the time of denture insertion when the new denture a n act as a surgical template. The former is pre- fPaTed because the patient wilI not have to contend whh postopaative discomfort dong with adjust- mat to the dentures.
Pendulous fibrous maxillary tuberosities (Pigwe 8-4) are frequently encountered They occur un ib td ly or bihml1y and may interhe with dmhm construction by excessive mmxhment on
or obliteration of ~e interarch space. Surgicd exci- sion is the l rafmat of chaice (Q-tm 8-5), but occasionally maxiUacy bone must be remwed. Care must be used to avoid opening into the maxillary sinus. In those imhwes in which the sinus drps down into a pneumatized and elongated tuberosity, it may be possible to colhpae the sinus floor upward without danger of opening into it. This technique also is used when a bony undercut exists on the buccal side of the tuberosity and the sinus has pneu- matized into the undercut (Figure 8 4 ) .
Bony prominences, undercuts, spiny ridges, and mandibular tori may have to be m o v e d to avoid painful denture flange impingement and to achieve a border seal beyond them a g e t the floor of the mouth (Figme 8-7). They hquently occur so close to the floor of the mouth that a border seal cannot be made. Oa the other band, w r l l a r y tori are rarely removed. Satisfactory dentures can be made over most of them by careful relief of the palatal denture base material. The following are indications for the r e m d of maxillary tori:
-re 84 A, A pendulous, fibrous, mobile rkght maxillary tuberosity ?hat is easily ctiqbwl. 0, Two elptic incisions undermine the m a mi aliwv fw a~ximaticrn of
3 the rn-I wrfaces (0) mr a firm, bony haw.

. . kyt"!xn,i&'
I f ~ s ~ k ~ . T b C, Indhns made just tr& W. 0 and E, Thin mJ

106 Plrt w- mparing the Patient for Complete Denture Treatment
n Flgure 8-6 Legend on oppmite page.


108 Part TWO Preparing the Patient for Complete Denture Treatment
E Figure 8-7 Conspicuous rnandltrular tori (4 a n surgically exposed (B). A mucoperiosteal flap (C) is replaced and sutured interdentally. 0, Prominent mandibular tori on an edentulous cast (arrowhwds). E, lntraoral view of the tori that murt be excised before denture construction.
&sure oa dm M c d Fommm ifbane usually are more dense and mistant to resorption in ihe mmiibh has hm a&me, the mental than the bone anterior or postmior to the foramen is.
P ~ n t p ~ r ~ ~ a r ~ a t d a e m o f t I a e Thiscausesthemarginsofthemmtalforam~ta m d d hmy p m m ~ (Figure 8-17). When this extend and have very sharp edges 2 to 3 mm higher 'bappm~, the bDny mar&w of the foramen than the surrounding mandibular bone. Pressure

--
A B Flgum 8.8 The sheer bulk of a tom may prwent cunventianal palatal roverage by the denture base 0. This situation can be amlioPatJ in a pattially denentulous mouth by modMQtian af the design of major connectors 0, or (less frequently] the torus may be considered for surgical removal.

110 Part Two Preparing the Patient for Complete Denture Treatment
b e surgical tecbiquezt of veatt'burqhty and ridge augmentation have k n largely eclipsed by

8 d 3 d a Z ~ i n W ~ i t h ~ ~ - m & a ~ ~ ~ ~ ~ M ~ ~
be be en pro- w i l a # a m a - *-,- de€a&%a tfie **W\W~U
a r ~ ~ o f ~ ~ ~ ~ . ~ d ~ h r m ~ h ~ ~ e a h t e n - -4fm chatwe *~h l .wb -bmry *hiug*pmmiatb--~w, ~ ~ ~ i & ~ ~ a n d i t s ~ ~ f m q i s ~ ~ e t o t h e & o d i f i ~ of tb # amtab BwCleb acwy. .The ti8k ofakmdlwwr16gandchinsmatm r % s d t % m l $ u 0 h ~ u l a r ~
, w O P t e r t h e ~ c l o s e ~ t i i o n ~ t h e
tm bM db@has h muitad in a clctrrer *
~ o e ~ ~ ~ ~ t i o n ~ ~ A w i d e m d ~ d c u s i s n o t ~ & ~ ~ % n A d ~ ) , d * ~ I a s t y 8 a n b e ~ ~ ~ i a t t r p ~ & @ m a h - m w t ~ l u l e W ~ ~ o r ~ o f t h c ~ ( s e e F i g u r e
.of the mentab &ow for the pro-
d a Q d o a o f a l ~ ~ & , l & m g w i Q a l o w r w o a t s d - w k h m @ m -
aad of.^^ flange. The i n & e ~ w f t w c a ~ n u s c 1 e
-a,fZlPQQBIbt&=wm$ The ~ o f ' ~ a a y H c r e s i a ~ ~ o r
~rn'lecl@mdenturebm&b p @ y h k & ' b I b h ~ . T h a s e ~ ~ are umdy fastened to the mandible with. cimm- & U * f o r 1 mkorImgw.CareirHy

1 E FIgure 8-1 1 A ptminent and painful superior genial tubwcle (A, amwheud~ is surghlly aposql (B) and excised (tg Cephalometric radiographs @ and q shaw the thinness of the mandible. In D, notice that the superior genial tubercle (am4 is higher than the smsf of the hony ridge. Notice also the extreme interarch distance at the rest position. E, After the tukrde had .been removed.

Qpter B PtFprosthetlc Surgery: Improvkog the Writs' DeRtumBearkrg h ? a ~ and Rehim ftg
M@ spw will reduce infl-tion, r a b pompdve mmhg , md maintain muscles in the &bdp~tion,~@iglpmhgtberesult,The di%t of nundiinlar v m t b ~ s i o n q e g r on n u d e &ty and pmskdix retention has ka im%@wd.rZaee 'C a d ~ i t y of the d & d i & & M ~ U 8 C k S W s h o w togndergoodydightdmgadspitethernentah rnuercBt'sbe@&mmpZetelyfroanits~in &a amiible. The p m m e d muse of this minor ~ ~ ~ t h e ~ s m u s c l e w g i v e n a a e w ~ i u t b e l u m r l i p , w i ~ ~ y t h e s a m e ~
ere 8-1 3 Anterior mandibular alveolar ridge p&mn Homwq a whble cbauge in the apparent lmti larrowhwdr) are rarely excised. ~ o f o f ~ ~ h i n c a n ~ T h e d W
has been &smW as a ' M ' s c k n
Flfurr 8-34 Unclercuts frequently occur on the lingual of the mandibular second and third molars. Occasionally, they ate wry tender, and a sharp rnylohyoid ridge of hone must be excised (A, arrowheads). 3, .A sutvgror is used to emphadze the undercut that such a ridge can create.
A POgawrt *lI ?osWhmadlsubIingual undmubSA,awcows),oc#rr~uend31and r;an be used ta enhance mandibular detpnte st;lMlity IB) via MYB r e d u d of the &it resin ftdngtfs).

114 FwI Two Preparing the Paiitnt for Complete Denture Treatment
mrn 10-16 ~mpmtive and p~&pmtiw (8) views of a man whu undement mandibular & m f m y , C, The pnmpmtive diagnostic cast.
Contin&

F Q Figure 8-16 comY Preoperarive (D) and postoperauve (y pror~les and cephalomettic views (F, 6) of a woman treated in a similar manner. (Courtesy Dr. P. Symlski.)

w m aid WiaghpIhk @) vkw afmdmW&b m W i e with w p r f i e t a ~ . ~ m $ W fmmim t$ mfti~xg@mWdve &dual ridge dudion , l$x%miw ~lrmquite NWte 'in wth dtmtioa
~ ~ ~ ~ d ~ ~ B l X S B ~ ~ ~ ~ r i d g e m o p t l o n b y p l r r ~ m & t b b ~ p f 4 h ~ A ~ T b i s on&ba%gm$tiifromtillilimorribmm6
&me ar bekv tb madible. unfo- f d f l ~ - w w wh d m m l ~ r n ~ b b ~ w i t h r e s p ~ t t o p w ~ ~ & r i 8 % p : h w $ h t ~ d ~ maxhiclity m a wmmt mame. Conside&%
am- k ~~~b old dmtm or cmtign is mcummmded with h e a ~ ~ ~ $ F l s B d & t h e ~ t o ~ d u m ~ a t b y a r e a ~ l e ~ Aain tbe of the mwly foPtaed, yet d particularly fbr elderly ~~. NmrWm$ &rr$wnWh cummt gnrgical re- suggM m a for wm
b i n i n g ~ w i & i m p ~ t o r e c t i f y ~ w ~ P ,R##e AwgmWatiom For many years oral and ual ridge mwr@ion pbletwj @&1y in l W & b f ~ d , ~ b v e @[email protected] to mBtme !n&b.
I -

Replacement of Tooth Rwfs with Osmintegmtid Derl fa1 Implants Whemver complete denhaw are prescribed, th o ~ w of a dmhm-bearing area is a logid and gompdhg objective* For some patients this d d a p q m s t W c mqgical prescription. T h dedes of s t d m about m t outcome with mehkgdw have provided hfutable evideme to support this typc of p r q m h t i c surgery. This
u & d in a new era of efi- in pnqrosthetic - The
b murce af suppit, and the focus has now shifted to an a d m e o w one. Different numbers of i t nphb are prem'bed for different prosthesis @, srrch an ~ h d h d y fixed prosthesis, which is emtidy implant borne (Figure 8-2 11, or an overdenture, which relies both on imphut and mid- ual ridge mpport (Figure 8-22). Implant =- merit of edenldous jaws is described in Part 4.
ged character of the ridge (amha&).

118 krt Two Preparing the Patient for Complete Denture Tmtrnent
I
L A
I
D E I
Figure 8-18 Legend on opposite page.

Ckaptm B Ple~rwthetic Surgery: I m r t g the Patients' k n t n m ~ n g ~ and &$ge Relations
e 8 . 1 9 Sagttalsertiansth~ttrelowlwIip # d o r part of the mandible (A and fl shaw the ~:mi+aCh for a labia I flahge and the e f W c# the Wlb muscle $M) on this spire. The muscle $&ta on ihe h e and inserts into the MI. @r&bn of the mu& l i i the lip ;md red- the bmfWe for the a dmdentu* A beta!
( $ s h o w s ~ m t o u r d t k ~ u a l mhr ridge f rnrndately aftef tooth mction ('I) @itheorigfn af the mentalis m w l e (simulated a Wen 1 r e s ~ b s to its pmmt twef, the n l a t i i &&of origin d this muscle now obiittmtes the
subs, V and E, A niandtbulat Wibulaplasty Wicks for dramatic in- in the labial fbnge W n .
C D Ftgum 8-20 Deepened facial mandibular (A and 8) and maxillary vestibules (C) with skin gnfts in place. Note that current procedures do not aim at achieving such a wide area of operation and restria the intersection to inferlorarnina site in the mandible. Mandibular dentures before and after sulcus deepening are compand (a).

120 Part TWO Preparing the Patient for Complete Denture Treatment
C ' C 0 : Fi#we 8-21 A, After two preprmeuc surgical stag&, the osseointegsated implants are
used as abutments for an electively removable fixed prosthesis. P m h t i c cylinders are matched to the implants and joined together by means of a wax d a l d i n g (B), which is cast to provide support fsr the final prosthesis (C and Dl. Notice that access to the retaining sews allows for ready removal of the pr06thsis and that the dngival surface design allows for hygiene maintenance as with standard fwd prostheses.

I
0 Figure &22 A, Stabilimtion of a complete denture by means of thm osseointegrated implantsjoined togetherwith a cast gold bar #. Clip attachments inside the mandihlar prosthesis ensure retention and stability without compromising the esthetic ~ u l t (C and D). The qwhy of a patient's prosthetic experience a n be gmtly enhanced by prescribing his m s t - e k h method,

122 M M W r i n g the Patient far Complete Denture Treatment
-mmwhY B ~ Q ~ I , ~ R ~ b ~ d d s m r a m
~ ~ ~ & ~ ~ , O B p r n f ~ 1%I%*f#, lW.
C ~ J & ~ ~ A ~ ~ o f t b e ~ j ~ * 2 w w * IRa32-rn, 1988.
de ~ . ~ ~ P J W , ~ f I & a k hitrp$%d IwwWt admumdon of tEae amphie maa&hl:0. J&W&k *7:129* 1V9,
~ A : ~ ~ m & i a k a n w i m o f t h & ~ &&utJ tSlfl2)4J%42& 1M1.
~ S : ~ ~ I h a r v e ~ ~ ~ L #wd= gI& atwp.ym f0lIm-q *,Ini ford
1@2?70478q M7. ~ 8 i ~ ~ E , ~ B e t d : X n m a e t l c e o f ~
@ pthlogy on m k t ridge midon a k ~~ . a 5-w c W and r a d i m fohw-np --w 1921a21s. m. ~ ~ w i l b b a k h w f k r f i w - p e a r
& h k d # & W p ~ 4 J ~ k l & & i k ~ 4 1 : 173-176,19#.


124 Plrt Two Preparing the Patient for Complete Denture
~ W ~ ~ ~ ~ W i t h ~ t h e s e ) i . a P y ~ m b e - ~ & o p r r & ~ ~ k ~ ~ . ~ e r z ~ t h e l i ~ r s f e ~ f o r t 8 s ~ k W * ~ f b r ~
I l h h ~ u y ~ n a t ~ ' b a d ~ ~ t h e y d a nQt wwUy ww c-od denture be& and prwmiq tedmiqws. Tho main Uyanwgt of
WI hag la#% &g., in wear and color stability) as d w a l denture teoth ornd pctssed bases.
ADVANTAGES AND DtsAWANTAGEs FOR A&L TYPES OF I MMEDMTE WNmm
t . m e ~ ~ o O f a n i m m e d i ~ ~ k t t a e m a h t e m m o f a p a t i e n t ' s ~ ~ ~ i s n o ~ m wad.
2. C h m d support, muwlc tone, v d c d dbmdon of ~ l a s i o p , jaw rel&mk&p, a n d ~ ~ t r t ~ k ~ ~ ~ w i I l n o t ~ w t ~ a ~ t o f wd.h Eom.
S k . ~ i s ~ t o b e ~ t a r r d r t h e exhadim rdtrs M pro-
L ~ ~ ~ ~ ~ ~ B T f s a t w w a - m - p i d g e
i @earhd, I%5; &bm, I*, 1958; CmpbIl, 1960; C d a w ,
IMn 4, &L@erto@hafe(ifdesimd)tknata-
~ 9 o o e h ~ a n d p o ~ t i o n , p l w h f m m a n d ~ I f * ~ t l l e ~ ~ w e r - . C i d & t i ~ a n g o f t h e m t e e t h c a n b e --&w-
5. T t a e ~ ~ m ~ b r r c t a p t ~ ~ i l y a o ~ ~ d x c ~ t i m e r h a t ~ i % u m ~ i S ~ . S ~ t r n d & ~ tiun am rarely wmpmn&& srmd nutrition be^.
6. ~ ~ t y o f ~ ~ m a t o - rialdlmfor " M ~ v m d i t y i n h ~ ~ ~ e m t ~ f t h e ~ B ~ m r W e , b t h a t t b h m b n s t a g e
L & ~ ~ W i l t a p p o ~ .
Treat

f#IAGMW4,~ 'rREAPAilEW PIANNI NG,
l m g - & h ~ s a & m * ~ . W ~ - timely In svme awes*.& pawme f m s k r k u ~ a n d h ~ W ~ - ~ * ~ a r a d

1 6 Patt Twa Preparing the Patient for Complete Denture Treatment
soft tissue d a t e d pmechm can campli~ate tnatment. Im some patients, tile squelae of advaawd pmiwimtd &me, includmg & e m ~~~ WMOWS, might require a "staged"
I surgical approach to the fmal objective of s definitive prosthesis. Extracting the poshxio~ teeth and performing other mmsary prscedwes f a in patien& a n Id to pmdictabb mdta for the CID.
Hmevm for o t k patients, the idea of a penmi withorrt posterior teeth L imposible to imagine. The I D esmtially recmcilea these w m i d e m k (1) expwlitmq for tbe patient whede d e , oscupa- t i o n , m d ~ - d s M l * ~ o f t d l $t dl times and (2) fwqpitim of the
a g l l 4 s m & ~ a p i ~ ~ q r ~ t ~ r p e f ~ . T h e ~ ~ ~ t o ~ - ~ p a t i ~ r r n B ~ ) i a
t h a t i f t b e ~ w n d ~ l ~ o ~ i s n o t ~ i f w = t m y a m e w ~ ~ ~ ~ b e m T n t h i s ~ I a ~ a t l t c s n b e m s d ~ e ~ ~ ~ t Z t e h h ~ a x i ! & 3 i n ~ a : of wrvi#.
M m t i n d ~ p a t i ~ m e o p t h g f o r t h u e vwience of the m3 &LC& lfthe dm& perfa t h e ~ e ~ c ~ a x l d t h e @ i e n t i z i r n d v e , & e ~ t h g U D c a n k v e r y ~ T h e ~ d ~ ~ a l l o w ~ of the end redt .
T h e f m d ~ a s t o w h i c h ~ o f ~ a t e d m t u r e b a S S u i t a t t i e ~ ~ ~ a n d g 0 h i s t o r y o f t h e @ m t m b e ~ . W l e s u m m h m a ~ n a f ~ C D , e m B ~ a s s i ~ ~ ~ ~ ~ and at the fmd ~ e n t - p h d h g visit,
C fsgum 9-i Advanced (Class McG .; Nirnmo, and Skiba, 2002) candidate for immediate denture treatment. A, Natural tooth display. aI, Teeth in centric ocdusion. C, ~axillary OCCIUS~I view. Continued

Oral m@h&fi
F I . Ftgure 9-1 d d D, Mandibular occlusa~ YIW. Panoramic (E) and full mouth IF).

Intended as definitive or long-term prosthesis Transitional or short-term prosthesis After healing is complete, it is relined After healing, a second denture is made; the IID is kept
as a spare denture and may be relined for use as a spare
At the patient's initial pmntation, usually only anterior At initial presentation, usually both anterior and teeth (plus possibly premolars) are 'remaining posterior teeth are remaining
Usualb has good retention and stability at placement, Usually has only fair retention and stability at which is possible to maintain during healing insertion, which must be improved by provisional
relines (tissue conditioning) during healing The overall cost of CID treatment is less than IID The overall cost of 110 treatment is greater than ClD
treatment because it is the cost of the CID plus a reline treatment because it indudes the cost of the interim denture and a second denture
Treatment process takes longer than the IlD because Treatment process takes less time than the CID as there is a delay of 3-4 weeks for the postericlr teeth denture fabrication procedures can begin right away extraction areas to heal partially before making the final impression.
Generally indiated when only anterior teeth are Generally indicated when there are multiple anterior present or few posterior teeth remain that do not and posterior teeth remaining or full arch extractions support on existing removable partial denture andlor thee teeth support a removable partial denture
that the patient desim to main until insertion Generally indicated when patient can function without Generally indicated when the patient cannot or will not
posterior teeth for approximately 3 months go without posterior teeth or an existing removable (3-4 weeks p t e r i o r area healing time plus 2 months partial denture because of esthetic or fundional to fabricate and place the CID) concerns
At placement of the ClD, usually only anterior teeth are At placement of the 110, usually both anterior and extracted (passibl y also one premolar on each side posterior teeth are extracted that had been retained to preserve the vertical dimension of occlusion)
Indicated when two extraction visits are feasible Indimted when only one surgical visit is preferable (e.g., to meet "one hospital surgical visit" insurance benefits or when the patient's medical condition warrants) only one surgical andlor hospital visit.
Esthetia of the CID cannot be changed The second denture procedure after the It0 allows an alteration of estheticu and any other factors if indicated.
At the end of the treatment, the patient has one denture. At the end of the treatment, the patient has a spare denture to use in mse of extenuating circumstances
If all posterior teeth are initially removed, the vertical Because posterior teeth need not be removed before dimension of occlusion is not pmerved; opposing fabrication of the llD, the vertical dimension of premolars can be maintained for this purpose occlusion may be preserved
Contraindicated for a patient who has a complex Indicated when the patient will become edentulous irv treatment plan (e-g,, periodontal therapy, crowns, one arch and become partially edentulous in the fixed partial dentures and removable partial dentures opposing arch for the first time or complex in the opposing arch) or for changes in the vertical procedures are needed (such as crowns, fixed partial dimension of occlusion dentures, and removable partial dentum) or changes
in the vertiml dimension of or changes in the vertical dimension of mlusion; an upper 110 against a transitional lower partial denture can be made; then any periodontal procedures, crowns, and fixed partial denturn can be done during the initial healing stage
Yot useful for converting existing prostheses such as Can be useful in converting existing prostheses to an IlD removable partial dentures

'E* + - , - v > l -- -1 -A - -: 4 1 1_ 'I
Explanation to the Patient Concerning immediate Dentures
1. They do not fit as well as complete dentures. tion, different chewing sounds, and fac~a l con- They may need temporary lin~ngs with tissue tour. conditioners and may require the use of denture 6. It may be diff~cult or impossible to insert the adhesives. immediate denture on the f i f i t day. Every effort
2. They will cause discomfort. The pain of the will be made to do so. I f rt is not possible, it will extractions, in additian to the sore spots caused be inserted or remade as quickly as possible. by the immediate denture, will make the first 7, Immediate dentures must be worn for the first 24 week or two after insert~on difficult. hours wlthout being removed by the patlent If
3. It will be difficult to eat and speak initially, almost they are removed, they may not be able to be like learning to eat and speak all over again. reinserted for 3 to 4 days. The dentist will remove
4. The esthetics may be unpredictable. Without an them at the 24-hour visit anterior try-in, the appearance of the immediate 8. Because supporting tissue changes are unpre- denture may be different from what you or the dictable, immediate dentures may loosen up dur- dentist expected. ing the flrst 1 to 2 years. The pattent i s
5. Many other denture factors are unpredictable responsible far all fees lnvolved in refitting or such as the gagging tendency, Increased saliva- relining the dentures
t k ~ t s h o d d i a ~ c l ~ a n d ~ a n d a n ~ v i m o f ~ probin@,aPlilldwtbglof ~ i a ~ u m d ~
a note af need for frenm T i m e U b m - W I r p m P l l i l t n r m ~ I ~ ~ f ~ ~ ~ ~ ~ ~ , r r n d a s l s p l m t d m t h ~ i n ~ o n W ~ t h e p a t i e m t ~ & a $ l ~ ~ d ~ . N d ~ ~ o f t h e f o f i ~ ~ # i l l h e f p h l ~ ~
1. The patient's eKisting mi& grid need for d l ~ ~ of h pairition (aewtlg teeth n q h n e d r i ~ e g p l I y i f a ~ t o o f h baabxalustfurwmtime)
2. Tbe patients e x w q wrtM dimtlu?b of o c c l ~ a u d ~ t ~ i n t e m c c l ~ d i s - ~ ( ~ ~ ~ a n d ~ a e e d f 0 r ~ - ~ t o w d m g k g i t , a c w ~ t o whether tha patient's e&ling Inmiroam ~ M p a ~ u W & ~ & t h e ~ ~ ~ m ~ m f o r t h e ~ d e n ~ ~ h ~ ~ i t i s t o m a n i e p - Me or ~CWB pasitios f o r m
3. T h e ~ t ~ t d ~ a n d ~ i - c a l ~ o f ~ ~
4. A n ~ o f t b ~ e ~ ~ d c p o f occlusiotl for tbe patient
aapmtdthepmanant 5 , ~ p ~ o f ~ p r t o o t h i n t f P e b l l c 4 a t -dm face and pfde , Iip cumidor

- 130 Part Two Preaarina the Patient for Comulete Denture Treatment
I Example of Informed Consent for Immediate Dentures
An immediate denture is a denture that is inserted immediately on extraction of your remaining teeth. The fit, appearance, or com- fort of such dentures is very difficult to predict. There is no way that teeth can be fitted in advance to show you what the denture will !oak like, how well you will be able to bite and chew, and how they will fit.
Immediate dentures often require tissue con- ditioning or temporary liners during the heal- ing phase as the natural process of gum and bone shrinking takes place. After several months, the immediate denture will need a definitive reline or a new denture. The costs of these liners, relines, or the new denture are not included in the fee for the immediate denture. The fee for each of these services has been dis- cussed with you.
Every effort will be made to duplicate or improve: an the pusition of your natural teeth, but if the immediate denture b not quite what you expected, you may hdve to have a second
Eramination of kisting Prosthesis
Any existing prostheses should be examined for shade, mold kmfh position, lip support, and smile line. The shah of the denture base should also be noted
Tooth Mod~ication Many immediate denhim will require modification of w i n g teeth to correct the occlusal p h e or to ebimie prematupities in centsic relation. Occiusal plane adjustment is necessary because the factors that necessitate twth extraction (e.g., extensive caries, perihtal disease, and extrusion or drifting) often are associmd with occlusal discrepancies (Figure 9-2). Tbese can affect the correct regstration of centric relation, especially when they interfere with guiding the patient into the centric relation
pasition. They can also interfere with the propea dekdnation of the occlusd verticaI dimensioa. These tooth mdif~catim should be made to the patient in a h - of the final impressions.
At times it is determined that the analysis of the occlusion and the p h e of occlusion ia best & by pafonning a diagnostic mounting of the p liminary cam (impression technique for these is described later) to carefully evaluate the planned changes, The esthetic didogue initiated at the ord examination visit can be m d e d and madied on the mounted diagnostic casts, These casts are alw used to plan and mark the occlusal tooth modifla- tions that will need to be done at the final imp= sian visit later (Figure 9-3). These preliminary casts dso serve as apmxtmction record
Prognosis All of the foregoing features will allow the dentist to determine a prognosis for the immediate den- ture. The professional fee should be quoted only after this thorough examination. At this point, them will be a good indication of the best type of imme- diate denture for the patient, the anticipated diffi- culties (e.g., idability to achieve a reliable centric relation position), esthetic demands on the part of the patient, a compromised residual ridge for den- ture support, syhtemic diseases and medications that may affect denture success, sensitive tissues or sharp, bony prominences that may necessitate more sore spot adjustment, and other concerrls. The Amerim College of Prosthodontics Classif~catiioa for Partially Edentuloua Patients (McGarry, Nimmo, Skiba et d., 2002) should be noted; it is helpful ta both the dentist and the patimt fa use this ~ystem to understand the nature of the patient5 diagnusis and prognosis. It also w e a as a basis to refer to special- ists (prosthodontists) when indicated. Once the patient understauh and accepts the diagnosis, d- ment plan, and prognosis, treatment can begin.
Rt.feralr/Adjunctive Care I f other dentists are to be involved in the patient's treatment, referrals for required cond- tations are requested at this time. When required, a surgical consultation should occur early in the treatment to establish good communication

, Fhum B;L & The lower anWb teePR Wuirinn d f i & n ?o t)lm ?a an wen ptci of ocdtlsion. & Note the w~~ must b~ m r d in the finai planned prosth
, * h e W g b t a p t n e s ~ a r G ~ teeth fm (w- fhmeds)* d c d cmsidepo~tim~ le.g.. h t d
dy cotqromisd adjacent teeth fkquendY i m p v a and &as the periodontal treat- m t ~ m y b ~ h t h s , ~ f e e t h ,
mats for m ~ ~ e t y , where tiat to do Q d hwh*
. <
t & d s e a i l l p d t h k c a n b e ~ r h - T h e - & h + w Ma ' 3 l r ~ a a t k h d ~ ~ t h a t r m - l i P a ~ - w e a t k L p ~ h ~ ~ r e o e i v e i n p u t a a d ~ ~ ~ b m ~ ~ B ~ w o f t h B k
aldfdon* eullsd-n aoncetping atly Wnxt mded for planned overden- abut- & &odd be done, if neceaiq. The endodon-
O R e a , p t i a t s w i t f i ~ t c ~ * & * resto&oabi, cmww,'w d b partid d f m t l l m , ~ m a ~ e m & ~ * c i h t with the immediate datule prodma.
For the patient with a single CID, r&~mtkxt~- a n d c r o w n s ~ b e ~ ~ ~ # @ 3 b , S weeks of healing a h the first s@cd vi&md ~ ~ i n c f d a n t W i t h ~ i m m e d i $ t e ~ ~ d u r e s - F o r ~ ~ e n t w i t h a ~ l X r X , tiom, aad the Befiaitiw rtww&b* denhafa pm@dma *.wm opgmdllg:.d .am h e afkrphmwnt of ofxm), Tb* tionto this L i f a t m w i t h d ~ . ~ d e n ~ t a l ~ E o x ~ ~ ~ ~ k

132 Part Twa Preparing the Patient for Complete Denture Treatment
S3 Mounted diagnostit asts of the patient "i f % @ ~ 41 an M p evaluate the pigneafocd~ion,&rudedteeth, d h a t a , and r d W t h . T k y m kmarkedfw . mile tine, midline, Wetidr firhi$ and planes of d w i o n such as intwpugillary and +
&-warn Thw serve a gqtrrnanont W a c t i o n record. A, Front vim with marks k r midline, intetpupitlaq line, and mile Ine, 8, RigM k r a l view with ah-tragus line. C, Left l a t d vim
P
First ~ ' & W g i t a l Yi&


134 Part Two Ppparing the Patient for Complete Denture Treatment
Figure %3 A, Maxillary tray border molded with periphery (rope) wax to extend into undercuts and onto the vestibular roll area and patatal area (6). C, Mandibular tray similarly prepared.
3. The tray is outlined to be 2 to 3 mm short of the vestibular roll and to extend and include the posterior limit (posterior palatal seal and hamular notch area).
4, Autopolymerizing acrylic resin or light- wed resin is adapted aver the cast, into the stops, and to the planned outline. A handle is added to the anhior palate or to the mid- palate. The latter is regarded as advanta- g e m because if the anterior handle is too long, it may interfere with proper anterior vestibuie border molding. A sketch of the cross section of a full arch tray for a CID is shown in Figure 9-8. The full arch tray for an IID would be similar except that it would have teeth under the posterior section as
well as under the anterior section, The lxay is allowed to polymerize (Figure 9-9).
5 . As with the usual techniqu! in complete dentures (see Chapters 13 and 14), the tray is polished, tried in, and relieved. Border molding is accompli~hed, the appropria,te adhesive added, and a final impression 'is made in any preferred eIastomeric material (irreversible hydrocolloid, polysulfide rub- ber base, polyvinyl s h o n e , or polyether) (Figun: 9-10).
Type Two: Two-Tray or Sectional Custom Impression Tray The type two method is used only when the posterior teeth have been remmd (CID). It cannot be used in the IID technique because usually

Flgure 9-5 Maxillary fl and mandibular te] preliminary irnpteyions f o r t h IIR tech- nique and maxillw (4 and mandibular (Dl preliminaw irnpmions for the CID technhue. 04 conventional immediate denture; 110, interim immediie d h r e .
Ious ares, This section or posterior tray s h d d cwer the lingual surfaces of the te& (only) and extend up beyond the incid edges of the teeth to include a h- dle (Figure 9-1 1).
4. ForthemtE6qrdmortrmry,~e~earemry- ing teebniqu~: one is to adapt a cwWm tray, EUMI mather is to cut and modify a plastic W (Fm 9-12). dm&&, s ~ m e
opmtom prefer ta not use a tray, Instead, they adapt p h impression mabaial or a heavy mix of aa elastomeric impression materiaJ directly in the mouth. The W o r sectionl'imuiw makrial must caver h hbid surfam of the teeth and the v m t i i . M miations can be used successfully.

136 Part TWa Preparing the Patlent for Cornptete Denture Treatment
D Figurn 9 4 Preliminary maxillary W and mandibular [e) casts for I10 technique. Pdtminary maxBhv (q and mandibular (0) wsts for the a0 technique. CID, ~onventlonal ' immediate denture; IID, interim immediate denture.
5. The posterior sectional w y is tried in, reliwed as with a cony,lek denture tray, barb molded, Etnd adhesive applied; then the posterior impm~ion is made in my impression materid &sired (zinc mide-agm1 paste, polysflde rubber b e , poIyviay1 silicones, polyether) (Fw 9-13). This materid dues not have to be ela;shmmic bemuse it will nat lock into tooth undexc~ts because it includes only the l h g d mare of the teeth and the -or r i d g ~ . If severe posterior ridge +dsxouis orre pmsent, an eIsstomeric W &old be used
6. I'Im pea-r impression is m d and inspected. Excess material is removed,

F@J= 9-7 Wax block-out of d U a t y W and mndibbr (B) casts for on interim immediate denture (IIP).
The p d u m fbr Iaoahg the pogrerirn limit and j ~ r e ~ n mod3 am*tbLl to thosefcrr eom- p l e t e ~ ~ ~ ~ 1 5 ) . if^^^ anterior and postmior teeth remaitling (in same patients w i t h l I D s ) , t h a ~ n o t k a n e e d f o r a recaxdbm.and~e~lw&nrinm.Ktlot(asinsmm I#rdenb ~4th'- a d dl with CIDs),
Figure M Sketch of outline and wax block-out of a single full arch custom i rnrn'on tray for a conventional immediate denture (UD]. A, Wax fw spazer, I, Stop. C, Wax black-out

138 hfl Two Preparing the Palient for Cgmplae Denture Treatment
A B Figure E&9 Maxillary IA) and mandibular (B) full arch custom impression trays. This view would look the same for either a ClD or an IID. In the IID, teeth would also be present under the posterior sections. CID, Conventional immediate denture: 114 interim immediate denture.
C D Figure 9-10 Border molding (A) and final impressions (0) for maxillary IC) and mandibu- lar ID) immediate dentures (110) in full arch custom impression trays. In the CID technique, porterior teeth would not usually be present in the full arch final impression. CID, Conventional immediate denture; !ID, interim immediate denture.


140 Part Two Prcpdrirlg the Patlet11 lor Co~nl)let? I l~ntur? Trpainieril
C D Figure 9-13 The posterior component of the seclional impression technique (conven- t~onal immediate denture [CID]). Maxillary posterior section is border rnolrled (A), and the final impression i s made (6). C, Mandibular border molding. D, Impression.
~ ~ m s ~ , ~ ~ u r ~ a ~ * % y e y e : y
3. An tmh~&m of the patient's existhg verti- cal dimwdm of mlwim is ~ l i s ~ dWmWg K it should be retained, On occasion, tf8e qxmh may wish to restom it by o p i n g h w e the p*t$ U n m t#& loss, lQmellQ of the mmhing and tooth wear mated uvsrclosure. At &ms, the d a d dimension of occlusim ~ ~ v e t o b e c l ~ ~ ~ ~ a n d ~ o n o f t h e ~ m t - $ ~ o f a e n e d i t .
'I'hc latter can hc accnmplished by grinding thc t i i ~ t i ~ ra l IH. st0110 tcctll 011 tlic mastcr cast.
4. Tl-ic r )cul~~sion rims (and tcctli if nccussary) are tri lrlmcd to thc dcsired vcl-tical dimen- sion o f c~cclusion. A facc-bi~w t ran~ fc r and a recording of cc~lrr ic relotiun arc niadc (see Chapter 16).
5. Thc casts arc mountud un thu al-tici~lator ( Figrlrc 9- 1 8 1.
6. Protrusive relation rccords arc madc, if desired. to translkr to the articulator in order to set the coridylnr guidance.

C D Figure 9-14 The anterior component of the sectional impression technique and reassembly with posterior section (conventional immediate denture [ClD]), A, Maxillary poste- rior impmion rwated in the mouth, B, Try-in of the anteeor section of rnaxlllary tray. C, Sectional maxillary final impression remwed (by unhinging) together and reassembled. D, Mandibular completed final sectional impression.
Wm the Denture Teeth/Verifyng law ~ M I S and the Patient Try-in Appointment h e articulated casts are used for setting any ante- ~ t a i o r teeth that are missing so that a try-in mbe ~ x t p b h d with the patient. A try-in is pt d w q pposaible (e.g., when all teeth in the arch lm.pmmt as in som patients with IIDs), but the b t m g should st i l l be canfmed at a patient && Xn Figure 9- 19, the posterior teeth are missing m) rn that a try-in is possible. P
b Set the posterior teeth as described in Chapter I 17, Set the teeth in tight centric occlusion.
2. The trial denture bases are bid in the mouth and used to verify vertical dimension of occlusion and centric relation as with complete denture#. If necessary, the l o w Gast is remounted with a new centric relation mord until the articulator mounting and the patient's centric relation coin- cide. Teeth are reset to any nnv mounting and tried in again. For patiem whm a try-in is not possible, a verifying centric relation record should be taken ta d m the jaw relationship.
3. Now it is important to take t ime witb the patient to record landmarks on the casts and to confm the patient's esthehr: desires. Much of what fol- lows has already been done mi a preliminary

142 M T w a Preparing the Patient far Complete Denture Treatment
~ & ~ ~ W & ~ ~ - ingphw. If WWle, t&nmmsd&$pst~c ~ ~ ~ ~ w ~ m % a a mm?&m. Q % m * m @ w * i s
~ ~ ~ ~ ~ s f ~ m s r s t a ~ T h e m i & h o f t h e h e L d l y t h e b t &obfbr*>**W~Mdkcon- Fmmd with the patient It &odd be pointed o a t b h * i f * W W d a e s o r ~ n o t & d e w i ~ t h e m i ~ o f t h e p h i i t n r m m t h e ~ o f b l o w e r ~ ~ ~ ~ ~ p t r : f e r t b a t i t h .
b. T h anbxior plane of oc~lusion (wing the intapqillary h ots a guide) is determined & ~ ~ n t h e k u f f h e ~ t + m e mminhg canill- may not be ~oincident with &is pktw. Two teeth sbdd be found
are pamild to the dwire:d anterior plane d cmchsim Jf m a r tee& are still pres- e a t a t ~ ~ ~ ~ b e e x ~ n , w w a w d d dim &a bid ~ccrusaf p h . btzad lmsbwks that m r q a n d tethie ~ p l ~ d ~ ~ u l d IX M md ~ ~ c a d b ~ e s s a n e t i d m d m w a&&-WgwWan t h e ~ o f ~ ~ I f ~ o r ~ ~ ~ a t t t c f i i s s t a g e , itis t # s y t o ~ l d ~ ~ & ~ ~ ~ w i t h ~ ~ t s r i ~ ~ t m t h ~ u p .
c. The high lip line should be determined A discussion can then occur with the patient as to lhe display of toothlgiagiw that will be attempted w the need for a localid antmior dvedectomy if too much toothlgingiva display is anticipated (we patient in F i p 9-1, A). Also note and show the patient the posterior tooth why in the buccal corridor. Make sure the patient sees and approves this.
d A discussion of placement of diatemata, rotated te&, notches, and other m t d arrangements should occur so that the patient is actively involved in the esthetic decisions. Some patients want perfect-look- ing teeth because they never had them, whereas ather patients will prefer a mom natural arrangement. They may not wait friends and colleagues to h o w that any change has occurred
e. Note the existing anterior vertical and h& zontal overlap. Often, in patients in whom driRing and e x d o n have occurre4 tkb will be severe. Most patients will want t~ duplicate the position of their natural teed$ but some da have rather umsthpic amqb mmts, the result of adwced periodontal disease md driffing of teeth.
Determine how much vertical overIq needs to be maintained for esthetics d p b netics. Deep vertical overlaps are detrimental to denture stability, Zf it is excewive, ~IS-
with the patient the possibilitJi of denUte retentive loss during excursions. Using e posterior matomica1 tooth or increasing the horizontal overlap to minimize the hid guidance may be able to help here.
I f horizontal overlap is excessive, d e k ~ mine if maxilIary anterior teeth need top placed farther back into the mouth to elimi- nate an mesthetic position or if the h o b tal overlap needs to be preserved for @ support and phonetics. Lower anterior deo3. ture teeth can he tipped forward to elidat& some of the excess horizontal overlap Discuss with the patient the fact that ante& teeth in dentures do not have centric relati@ contact; this wiU be especially m e if tb horizontal overlap is excessive. Make

0 P@am 946 Maxillary W and d h h r @ f i d asis WW from the SiqtefuP
wsbm irrrprdan tmy m&J shown in F ~ M 9-90, ~ c ' i ~ r n immediate ckm blw, The final casts for a maxillary W and m d h i a r (B) mnwfithnal irnmedia denture KID) are also shown.
tmm fiehion is wnfmed raafi t6s @at (Figm 9-20).
6. A diwwion of dy ~ u q i c a l and denttw p1m- plane or for better lpentric ment protocol &odd wmu to pqmu the
~ t ~ f i r e t h e r ~ t o m y ~ ~ ~ P a t i e r y t i n q b w h a d ~ ~ ~ w r i t - ten immctiom leartia. it is d ~ q 5 w i ~ t o ~ t o ~ ~ ~ ~ ~ t i s s u e s wdl became &matom a d dimlored in the f e w d a y s o r e v e n ~ ~ ~ o n . O l l c e ~ damwtoy repm ia rewlved. tfie patient w i I l s t i l l ~ a I d m n s e o f u p p e r l i p puffiness, due to the pnwnca of a flange, which

W W Two heparing the Patient for Complete Denture Treatment
figure A, Mandibular record base with occlusidn rim for an 110 that uses the remaining teeth and halfway up the height of the retromolar pad as a guide to location of the posterior plane of occlusion. Maxillary (6) and mandibular ICj final casts and record bztm for conventional immediate dentures (CIDs).
is necessary for denture retention. This can be "every other " tooth setup is suggested thinned after sore spots are eliminated, and the duplicating the exact position of the patient should be reassured that the full upper tooth is not the goal. Some authors have Lip d o n is usually temporary until the soft the removal of all the tseth at this stage an tiasue~ rtdapt. setting of the denture teeth with the desire
7. If a change in in vvertical dimension of occlu- arrangement irrespective o sion is desired, and indeed feasible, the denture were. Howwer, this metho teeth are reset or modified to the preferred ver- able f irmation provided tical dimension of occbion. The following toath @-up
1. Mark with an " X (overdenture ab
Setting the Mterior Teeth: L~bor~tory Phase can be marked with an "0") and with a saw or cutting disk every other
~ m t d o r ~ f m i m m e d i a o e d e n ~ d i f f e r s tior tooth (in the case of IJDs, every &om that far ~ompIete dmtms. An a l~mt iw or posterior tooth as well) from the

a F l ! . %. I -8 %-I8 A, Mounted m t s for immediate upper anrt lower clmm {IlD). MgH
Ia&nl view 18) and left lateral view M, Fw upper and hwet C I k Q, Fmntai vkw 5 Rigkt I a r a l vie* F, L& lateral view. #D, Conventiod immediate denture: la, i w i m immed'ie denture.

146 Part IWa Preparing the h t b t for Complete Denture Treatment

amount of trimming possible is usudly p ~ t h e ~ ~ , ~ ~ . B r i q ~ ~ ~ ~ ~ ~ ~ h 4 ~ ~ forwstrd, cl&m dhbmata if d w d p a W i d ~ W ~ . M ~ fEas imthe~Fimahmrlancedocc f~
, a f t b e ~ m M t W ~ k & d a t ~ ~ medad (Figure 9-22). A Bow gau@ or Wqut stage, often by tk deeu &&mi- ~ n p b e u s e d t o ~ ~ c i a The prescription to the W ~ * r t n pieexistingdismce-thehrn ahodd note that thi~ trimming should be the pieexhetion dmguoatic cast a d #a
new tooth ~~t (Figure 9-23). 4. An extra visit to recall the patient for
a look at the final wax-up is a g d idea i n t h e ~ f m t m d at this- tima. Thh serves to rmwmre
mfmhg to the notes and some apprehensive patients a d nuy Watthetry-inPtiskThegodhm wen provide them an o p p t d t y to ta-
duce minor artistic refinement# in the

148 Part Two Preparing the Patient for Complete Denture Treatment
E F Figure 9-22 A, Every other tooth is set on the maxillary and the mandibular casts. B, The remaining teeth are removed. C to F, The setup is completed and waxed-up.
Wax Contouring, Flusking, and Boil-Ou t material for strength during future deflasking. Also, when denture insertion is first attempted,
1. The wax contour is similar to that for complete it will undoubtedly bind on undercut areas. dentures, although the immediate denture may Thickness of the acrylic resin is needed to
. be thinner, especially in the anterior. Make sure - provide room to trim from the inside to relieve that wax is added to provide a thickness of the sore spot or to seat the denture.


t50 Part Two Preparing the Patient for Complete Denture Treatment
Ftgure 9-24 At boil-out, a knife is used to smooth the extraaion sites to a harmonious rounded contour.
F@m W A su-I template is made at boilbout from the W e r cast W by making an inewrstble h f i d b i d (a9gim?@ impression. 0, %is b poured in stone. C, A wax-up 15 done?, & This OA be procad in c h r aaylic &n.

1 posterior wdercuts at o f f e n ~ d s n o 4 &
~ ~ W z E t e ~ s h d be placed in a &emid
g sohion in a bag for delivery.
ry and Immediate Denture Insertion
(Figure 9-26) or sectioning of any preexist- ing fixed partial dentures. The dentist perfmmhg tabe operatian then extracts the
i ~emainhg teeth, taking care to preserve the labial plate of bone. Usuatty, no bone
'3. The surgical tmpb is used as a guide to enrrure that the presmied bone ttimming ia &mu adeqmtefy. The template h u l d fit rmd be in contact with all tissue ~~I l r faces. bdquately trimmed areas plauned for bone reduction will Manch h m the pres- sure and be seen through the clear kmplate.
T h e ~ ~ i s d ~ * ~ o r r & t i s s u e t t i m m e d t d l ~ ~ t e ~ utsmdy srnd camptetely. This indhm t h a t t h e d & k m w i l l s & a s i t m s ~ i a w s ~ p m p e r ~ c c : I ~ ~ ~ ~y~~
3. S u b m are placed where mamy (Figure 9-27). (Wdh simple m u m , none ar;e -1
4, If the d t r r r e abutments ru s t be r e d . a c e 8 a i k t $ e ~ , t h e e x t r a c t i m l w c k e w m b a : ~ & g ~ ( 3 t l b y ~ ~ ~ 3 u f I e w f o i l .
5. Umdy, the the or surgeon p l m ~ the dwtuPesothatitseatswe1Iwithgoodfmn b W wlnsim rtnd no gross deflective c ~ a ~ , ~ a m t s ~ i b ~ e (indicated by m c b g ) can be hated with prmwe-iadi- and trimmi. If the ~colmfm ie n& csrrect, the denture sti~uid h mbcbd for seating, paz?tipu- ~ ~ , e h e m c d d d m t t m h e e l mas, Wch are clwksd fix inWmce, W h ~ M ' e a r e d & , a qoick acclaral z s to BnOW s i m u I ~ ~ b i b d mtmt (Pigum P- 28). Further rePmemmnt of the m d d o n d y is done at a later date. ?be h a &odd be h k e d far proper relief.
Wrs The overdmwre abutnwmareka reduced by the applicatjon of a rubber dam to prevent amputated crowns from entering the throat or airnay.

1!iZ M F w e Preparing the Went for Complete Denture Treatment
' u ' .
- CAk pmpf b e tdamin& the template will seat uniiimnly. 4 Smm can then be Je. 1

Ire more WwIt ia the clinical
t b m ~ t ~ ~ ~ g o i m g to remw3tb dm&
tnre md that this will cause wme d i m - fora mve m m dilute l n o u h d d y for the patient to rinse wiL, Remove &e ~ d ~ i t .
2 . ~ & y c ~ k t ; h e ~ ~ ~ ~ . ~ ~ ~ d ~ , ~ ~ ~
as strawbemy-red qets. Usnally, W ar8aBiactude canine tdnmc&, to tubemiti~s; posterior f i t ~IMS; and ~ b y o i d ~ ~ H F e i t a s ~ y o h &ut ridge areas.
3. T l w ~IW m y be related to the denture barn v h d y or with the djmctive pse uf p m indicator paste. The c o m e ~ a r e ~ l i e w d i n t b e a c r y k ~ . T h e d e n ~ ~ b e h p t w t a f t b e ~ odyfwaveryabrttinae.
4. Adjust my gmm occlusai d i w in ceotric telatim or exulrsions.
S. ~e~-dentnre formimt ion . 'kea tissue conditim~r if dentwe is undswmy.
. --
semiadjustable @ t i & ~ wing the m b W ~ d b t f o r e & & i n g , r - m n t s i o d a t h

151 PPrt Two Prepring the Patknt for Complete Denture Treatment i
A C BZB The patient W rmd maxillary # and mandisldar N archa 24 4 r s
a W rnmtion. Sm spots are evident on the mandibular an* buccal ridge.


f 1 W Part TW Preparing the Patient for Complete Denture Treatment


t# Port Two Preparing the Patient for Complete Denture Treatment
:, - :~&Mw 5M3 c m t W ci,&dwWn Wkcats of tk%&tim denture s e w a5 a sufght wr the p w f b l r r a t l y ~ M p s to plan t)te k t iraplnntlbar 2tssemMy
ant m a & W i n g , t y i n of final hnpiant barasrembb 1, Anal ,-- owkittle. l, Fatid$ smile with { m d j irnent wdmmre. lf ,WW,wdl, tht patient3 itlteritlt Ww can ah be dined t~ W the bat assembly,
.d B W gwhmt's maanent plan iooludea BtBhwm impw - w d e m r e ,
~ ~ t p ~ ~ ~ d b a ~ iijr&thrs&wsmind
t i m e * h p h t ~ ~ ~ 1 ~ a e ~ . T h e ~ ~ ~ b e - &m
I- r e l i e tissue-conditiming p=. A h ~~ tmwvdngP tbe immHw3 dm-
a U r e i s r e l i & t o b t b e h & g s b u t - d zerve iw he prosthis until replacement
ly the implement pmsthesia Figute 9-33 shows
SUMMARY 1 today3 treatment modalities patients with esthetics, fimcd
phase. The technique is ular camplete dentures for both the patient denti& If the patient is well prepmi and ~


A. arb, Rhonda F, Jamb, John R h r b
halists haw long rwognkd the &Eimwe that ~ ~ o f b e e t h ~ t o ~ t i e ~ o E a h e - o h ridge integrity @ i i 10-1). It appm ?hat the prwmce of a treaEttry periodonrorl ligainmt maintains alveolar tidge morphology, hereas a ~ p e r i & t d ? i ~ o r i t s ~ e , k d a t e d with variable but inwitable time- dipmdeat reduction in residual ridge dimensions (see Chqter21. Enthe past& d o n ~fentIre &&tiQny wit$ ~l~ denture -1- ~ t o b ~ a a a n k ~ i w m d ~ - B a solufhn for orat hdth care, The 1-acy of t& bas^ amajor oral ~opphalog- ical: pmbZem: d m u d residual ridge wwrptiun (Rm). aqpii and fqlmtIy rapid reuction in edW&lh& a g e s h appears to be mdtifaatwid and is mq&cx&y ufl- H m , clinical expximce and w q w U i n g f y dwnnmtad r e d haw mdmmred the merits of retaining mturd to& to stme an isolbutments under complete den- tnres or e l ~ e under eartensive ot distal extension areas of&le partial denhum. The premise is that a c c l d forces of a functional and p w a f ~ c - t h d n a t u r e t h a t e x e r t ; ~ n a c t v e r s e ~ e a n ~ ~ 6 ~ d t o b e ~ u a t e d o r redud and that a#empis to d W y d d r a this p d e m are an iqmhnt pslrt of the RRR para- d@n that the dm& can control. Thns we have the bdmique of desigtbg omdmtum, mch also bave ba de& as hybrid dentures, or teeth- qqmkd or as&std complete dentures. The ~ ~ ~ e n t s m a y b e f e w o r n ~ u s , mmnally &aed or reshed, and Wuently ~~ prepred. The o b w v e is to di&
tribute stress ccaacentxation between retained teeth ablbmm and d m ~ r n p p o * lkw (Figure 10-2).
T h e a v m h m t e c ~ m o ~ & m duced to reconcile a negd for maximum wlpaort;in m o r p h p 1 0 ~ compromid dental archa witb a desire to qually
re~dthg from M- ~h- dm. C o n ~ t l y , p a t i ~ w i f h c ~ ~ a n d m w h as clefi palabs or thoat with 6- ~ o f ~ o f ~ ~ ~ w e r e t h e u s u a l d - dates for the d c e (RQure 10-3). EvmbAIy, t& merits and ingenuity of the technique encowaged dent& to p m m i i it for d e n t s who had worn dentiti- or anomalies that iacludd missing tgatgl and when ~ v m b b jaw or position 4 not: be rectified by orthagndu~ surgery (Fiw 10-4 and 10-5). Above all, the technique was in- pomtcd into the management of patients * partial M terminal dentitions, especially WW complete dentures seemed a likely therapdc option. In fact, in today's dental practices, it is nmd unlikely that immediate dentures are e m pm scribed without diligent efforts made to retain ab# m a t teeth (even if provisionally) for an imrnedidh overdenture service (see Chapter 91,
Most prosthodontic edumtos and me8pch
now recognize that the technique helps redw tb impact of some af complete dentute-wwhg wm sequence$: RRR, lass of occlusslr stability, udm mind esthetic appearance, and cornpromid ~ ~ t m y f n u c t i o n . The tecbniqwhmahabiw regardmi as a gentler t r ans i t . to the complete$r eckintulous state,

~ e m a cited iuhmbga of owrdmmi inclade the Following: (1) 'mere ias m&&mm of mare miduaI ridge hte& &m if rm ' k p p o a e d " ~ i s w o t n . m ~ f r a m : ~

7
161 Part Two Preparing the Patient for Complete Denture Treatment
I A B
Ffgure 10-2 The entrre notion of the classic overdenture technique is depicted in A and A Two mandibular canines ate morphologically altered afler mot anal therapy and extmtion of adjacent teeth that demonstrated advanced pertodontal disease. Their retention and use as overdenture abutments ensure dentogingival support for the complete denture
, and an expected reduction in residual ridge resorption (UUR) at least around and between the ' abutments. Overdenture treatment planning reconcil~ dinical decions regarding number
. and location of potential abutments, their restorative and endodontic status, and their use " for retention and support. A management stategy for their continued health status is also . a required considetation. - . ... .
imprcreRed o c c l d streas rtighhtiw. (2) Denture protocoI and the presence of re 8hbiMy and even retention (parbcuIarly in the dimwe are Serious dekmnts mzmlibl~) may be danced (3) Patients' mbjec- the p m p t i o n s regiwdbg a retained '"nattrral * W d t o b p & t i v e a n e s . M m q m t e
bmm ~ccIUsal-8, biting fQrce, md comqalt xteumrmesmJar wmhl f h n ifthe abut- meats in& w- - h t . (41 The tech- n i q m i s a ~ a n d s ~ b a l ~ t o ~ ~ m p i e t a dmtm tbapy, a d it is fquently self-mpmd as providing immense pSph0logi~d sapport for patients. (5) 1b application is virtually unIitnited a d dep& on the dmtist's jtdpmt and skill The? pmmtin of gingival and m ~ a b a v e a l l , o n t b e ~ e n t ' s m O E i ~ n t o ~ - dbmeisaveaycmpelhgconcaa tain an impeccable oral ewkmment (Figure 10-6). mdns the @entb responsibility, and T h e r e m e ~ d k d ~ t a ~ t o t h e ~ u e , a n d i t k ~ t o r e g d i t a s a l h l y p m v h i o n a l o n e . The Iikiely .y-t tramition ta cut@&
tmtawnt is Wly related to the patient's dbp@e818ccmmbmaad&e-ofk m w - b . ~ t m ~ ~ w i ~ t r h e mvcd b t h ahmnem' mimummi is not con- restorative ducks fa s g a plaque-frw milieu with its Serious dsk of & d m wqueb. F u r t h m r e , the

mra q0-3 Clinical management strntegy =flied out on this 44ryear-old man whose aB$mital anomaly was wrgMIy repaid k his youth & to 9. Note that angenbtty impaired hwbnhl a d vertka I dimembm of the facial prafile were estMicalIy corrected VrriihailtNfmiemre.

164 h r t Two Preparing the Patient for Complete Denture Treatment 1
I#DICATIOMS AND TREATMENT M N I N G T h vemtiIity of the overdenma ~ervice ia demon- in Figures 10-2 to 10-8. These
mamples were selected to emphdze the mng3 of treatment pwties. Above A, they
< ,
undodontic xequkemmb (if any) in the

FIgura 104 Wmts with vertical or horizontal dimedon deficits of their rnaxitbry ad16 can be managed prosthodontically by overlaying their maxillary dentition, This approach perm& lmprwed horizontal facial support and increased wrtiat dimemian of miusion. A, 8, D, and E, Pretreatment views of a patient WhoK complaint of corn promid masticatory funaion and poor h e t i c appearance was attributable to a discrepancy in facial dedopment. C and F, Post-treatment results were achieved without surgical oiUwgnathic i w t l o n s . Comtinucd

068 hrt Twa Preparing the Patiem for Complete Denture Treatment 1
bwe i d s if wh teeth are r6ml-h for their early exlradiou. Such an serve to impmve the p m i h d status ofthe caretainedtaeth.
SELECTION OF ABUTMENT TEETH I
1. Periodontal and mobility status: An ment root or tooth must be ehnm smlmded by healthy period0 The tissues may already be


rmlHI hrtm Preparing t k satlent for complete fcnture Treatment
Maw of hms the
.&&nenta are summed
I

Excesziw lip UrppMt FQw#Mw- t l t e -Maf
tllat&aB&Xmw
pl-ent of WK;M be&
too& can be restored ~ t l i an alloy or a corn- W* popbtion, d WE of psi&, ieshaped, and pohhed with fme m W & d d not preclude ti^ &a@pr disks. Xn moa s h t i ~ 1 8 , o bare ~ f f ~ ~ s , S ~ o f a m y o f fmth root preparation can provide &qua& t h e ~ n a W & ~ E s u t i a R W - u p t a

. , - Hpwe 1M A and I, Advanced, symptomatic teeth wear and pulpal recession in a patient whose dentition %wed considerable rndrphologEcal changes and neglect. C and D, T h M maxillary anterior teeth were retained, and an overdenture was constructed IE). b m e of the badly worn anterior mandibular teeth were duced/reshaped, polished, and partially "restormi* with a cast removable partial denture d the overlay type.

dm8 hive an additional e%gmB, I@ m m e ~ a m ~ 1 e ~ ~ sight of ~ ~ 1 0 ~ ~ " r m m ' ' rws i n t h e h ~ p t h ~ ~ ~ ' r p ~ . . &
C *~~~~~~ of a wing does8 n&
redmid caries T d prqmtiw h s h k b thatfwamq~eh gokimm, w i & w t r ~ u t ~ o n a l p i n ~ o n , a a d it h I & s a combhiim af &oddur and C l l m f l e r a d ~ ~ a d i M ~ t f r e a f m u n t d ~ M t o o t b ~ I t m ~ t r e ~ ~ that themainobjective i n p ~ z r n d ~ ~ a b a t - meatsistoprolongthetwfilllife~of tbe d e d abutments an8 the pmmwtiion

172 Part Two Preparing the Patient for Complete Denture Treatment
~ ~ * m t t ; a h n n t - t o ~ r ~ ~ f o r ~ ~ - comwudy,.~ dmpk d m 4 convex &umw%t prepamtion or w i ~ a ~ ) ~ t o t r e t t m e ~ root^^
3. Prmish of some sort d &achment mech- a n i ~ m a c a s t c o p i n g ~ L ~ (Figwe 10-10). This is a II of the p M - e - q t u s e d i n ~ e ~ ~ ~ ~ I s d f b r w w i t b ~ ~ t s . X t h i a W h - Itically ingmiow idea d offers a h i t y 0 f t & m i ~ * &example, mod and
4m#mrcd-chahdham m ~ o r ~ a ~ ~ a s c @ h @ L w w # - a - 4 a M e h3 midwt aad l l d b ~ T f s e n o t i m o f ~ ~ u o f ~ ~ e n t s ~ t h e ~ ~ dmgn h &t&bilify lttad rehwia, I z R l l ~ t a m a ~ * ~ f ~ o n ~ ~ ~ r e t e t l t f o n . ~ 6 r o s n ~ ~ i q e m e , t h e * ~ ~ ~ demrards and diffhtlti#, p& W Z t e g ~ a r e ~ o r a Z h ~ mamknawe rqukmmts may be ma demanding, aud esthetic plus in&m
-re 10-10 A t t ~ ~ ~ t r i n ~ ~ ~ m t b e ~ , i h q c a n i m p r r w e support, stability, ad r&Wtm &&&wedentitre. Some dirih1 &#& are shown. A and B, The bIlw b f a chairside atfstchmeni w: male partion cemented in the abutment teeth and h a F e busing emMd in the aayiic of the dentwe . C and D, The Q b m - m t k e a r a k W-type-is-bawing W o n is & i d by ttte f howiw embedded in the ( W l a r y ) wedenture.


W4 pprr JWo pre@&g the Patient for Complete Denture
gel is prescribed for daily appfi&n to the h i d e d&e mmhture to bring the fluoride into inti- ~ c m t a c t w i t h h e ~ t o a t f i ~ u . I t i s udmtmd hat the effdmaess of fluoride on ~ a n d d d d ' ~ ~ C S h 8 9 l l ~ b e e n ~ ~ e ~ Mid as ff d d e mnhmdhtion and incurpa- timi in e m w L Studies of root surfaee caries in patiem exposed tu lifelong fluori-d water spply rewid n damme in caries activity, Its we
bersa prosmibed for patients with ovedm?mm aod seems t~ &mme c d e s activity. As in warnel, &e grater the fhmide concaht im, the gre~kr the e0?1&m~y afthe fhwride.
An in vitm evaluation was performed by lhtiqys et al. ( 1997) f o simulate overdenture abut- mWnt root surf- caries, and the depth of miner- ~ o r l ~ ~ d ~ w i t a p o ~ l i ~ t t%lkofmpy. flu^ prepmations w m 5000-ppm &dtWA phosphate flu&& (pH 5.6),5WO-ppm & d u r n fluoride, and t000~ppm neutral sdhm fluoride, with a d M b d warn cmktol. ~ 1 8 d e r y s t h e ~ ~ I s t i t h ~ r o o t ~ \ a f e r e ~ p l # e d i n f t n a r i d e h 4 ~ t h e n i u a ~ ~ ~ m h t i o n f w 6 ~ a a d ~ i n a ~ 1 ~ s o l u t i o n f a r 1 7 h o ~ . ~ ~ m i u ~ 5 m p p m ~ ~ w had sW&id@ shalhwr bsims. All grolups wept t h ~ ~ mntrd group exhiitad m n i n d b - tion bands. Ihhction of deminerttlimtim was fomd to have a dose m w s e in favor of the p a e r 5000 ppm. m w findings am c*t fait$ in viwo fluoridated & W c e stu&ef~ on root swfwecaties.
CSim th- fmdings, MK should consider the pnqmltiw wilil gr&m fluoride Than3 la also dmx1Ga with 5WD= t t E a t ~ b e ~ T h e m I e o f ~ m t i m ~ i s ~ ~ ~ f n r o o t a u r f a c e G a r i e ~ IF&&$* Tk'thmgM that the dtmm m y be ~ ~ t & d b y S h e ~ y u s e o f ~ ~ w i ~ ~ p H i s a n ~ ~ o k ~ p a l i ~ ms€kqping irdirrtkan b e been UB* dB& mtan- BOW Pluwide pqmmtiom (pH 4.0) in tray alrplica- tors& 10 minutes -for many ywswithaut d d u tissue irritatb or patient complaints. In addition, stannous fluoride (SnPd ~ a r a ~ h e been sbawa to inhibit plaque formation and peti- mkmqpismr~ in multiple peridon- tal stwhx Ifp- complain abut time irrita-
Treatment
tiom, n d pqaratim can be m s i clinician should continue to &wte the co cially fluoride p r e p d m and the fluoride twe as it relates to root surface &e overdenture ah-.
CLINICAL PROCEDURES .I The procedures will vary dependrng on wh a tooth-suppmrted complete denture is be= ~tructed or a tooth-supported immediate- complete dGntrrre is p b e d (see Chapter
Tooth-Supported Complete benture 1 The important principles of compl a d o n must be mpectd d
hygiene measures of the patient. If untreated, the codtion may precipitate a series of adverse cha a d actually progress to pwiodontal disease.

TREATMENT OUTCOME STUDIES ' The d m h ~ t o p m l q the useM rifs of at leaart a f b w o f s u r ~ h t h ~ t a ~ ~ ~ d i s ~ i n ~ ~ c s l w l e p t ~ r s p m e n - t h e M * b w * l i s l I e d M ~ ~ ~ b d # d r e c ~ ~ ~ ~ & ~ B f ~ 1 0 ~ ~ dinid foww* sf t h e ptiemtsh c u m m ~ h m t o - % w w ~ t u m a r e a n ~ d t t e r n a t i v e t o ~ ~ ~ ~ d a t u x e t h ~ , m d ~ u = m i n routhe practice o o n ~ to bu egdmd H m a o , t t l e ~ ~ ~ t t m - o f ~ ~ ~ a n d i t a i m ~ ~ b p ~ m W ~ s b e b p t i n m i n d i f ~ ~ s t z e a b m ~ q i a t o ~ i t e p o k t l W ~ t h a ~ e a a d * ally m d & t 4 " b ou-6s repmd in i m p l # t ~ ~ ~ w- siudks me wrw beginning to alipsu the Wonal role of talth-auppow me?&mm.
SUMMARY ReMely hm-tam favorable outcoma with the oxdenture tdmique am we11 demmtr8te-d and e m h e routine p+on of the technique. Furthermore, the recent inhbtian of the 0~6e0integdm technique created the podbility of m v d n g patients with dadapthe complete dentures into ones with adaptive mrdaatures when implants rue to sMWe "affeW@" prostheses. As a dt, the hKin teclmiqaes (tradi- tianal complete deuture f a b i d o n with mhd teeth &utnmts or with implants) now 04%~ dm- W and patients a n w standard of proghdodc * l= 4).

176 Rrt T m Preparlmhe Patient for Complete Defitu~ re Treatment
f ~ ~ t a m m T P e m k P t memu, J M )LT:S$I-S~~. 5999.
E c I ~ e n 5 ~ ~ ~ Y a n d c r ~ e Q a t f f l l i n ~ ~ : 1 on W& and ~~

bilding Rapport: The Art of bmmunication in the Management of be Edentulous Predicament
d e n t a l k l p . T h e ~ o f t b i s c ~ w L b o ~ - tize the practicing dgltist t~ bhe ' of &e dootm/patient rehtimship by sq
ii h no lottger n v for tbo h b-m~hN&lbfbr t o ~ c o r t n t l e ~ h ~ w i t h ~ ~ l i ~ , J u h u ~ k ~ t k t ' ~ . . & e y m
o ~ ~ ~ a n 8 ~ ~ g ~ ~ o f ehisrmnltaumeht& of ~ d o f ~ w ~ ~ . , n - . amrlcmk-
w45, a f c o ~ , ~ =im6f=1 * kmmr* OV(.
a c u r m y ~ ~ ~ h h ~ a m ~ t h r a o f ~ a r t w i t h h ~ a f f e r m g f ~ ~ i t y . Cmumicntiofl and umbmm&g am not the sole ~ e w o f ~ ~ ~ ~ , b ~ m ~ ~ ~ ~ ~ f ~ h ~ ~ f e f r o m ~ ~ ~ b t w ~ s a c i a l , d p ~ o n a l .
For Mth - ~f~~ hL8pidh, f b r ~ ~ t i o m r t o d e c ~ r u c h ~ m & ~ d ~ i m p ~ e c f i n i c a l
k d ~ c ~ m m d m b ' w i t l a t d n i q u e b e u ~ ~ ~ m m d ~ d -
mdd poporibm of biological and physhl sci- oncwtobe & s o f b e . d f r o m ~ w u i B h t y ~ ~ u m and tb eqadly daunting tesk of Rcquititw and h t m i q g c W ~ ~ t o ~ ~ t h h a ~
p v i & quick sd&m to problem. s c r i ~ ~ ~ . T h ~ ~ h t ~ ~ , s i q ~ m ! 4 r e t p l i r c "with ~ t i s k ~ ~ e d ~
eBdw c o m m d d h n &ch- ~~ witb tbaaie "problem patients" W l i s t e H 2 r r g t o t h e t a e c d s o f t b w ~ ~ e n c o u & d b p . ~ W t i - .

178 -Wire Preparing the Patient for Complete Denture Treatment
(1) what is a€mmddm*F @),I*-* ,4$:.h@lm-
MMWNICATION?

senders and reaiwrs of messages, many of which are distort& by external, physiologial, and pwcholwical noise, (From Adlw RB, Towne N: i m h g orrt'Imking iir, ed 5, New Yark,
I Encoded Decc&s
Noise Nolre
*re 11-1 Communimtion is a continuous, irreversible, transactive process involving L"
participnts who occupy different but werlopping environments and are simultaneously
1987, &It, ~inehart and Winston.) - -

4 8 b Palt Two Preparing the Patient for Complete Denture Treatment
i t m p & i r n d t h e ~ d ~ ~ - ~ w I m i n t e ' l n t i O n t r l ~ b o r ~ ~ ornowerbrrl # e ~ * b 6 c o m s fhEmxhx, d B r a s s h e ~ * P ~ wpaa send d receive mewages IlIim-
*. T b p q m e o f i h d i d o g a e i s t o e x ~ g e
illmnairn that is tmhmud cmeqmnt?ys the ~ u f ~ ~ & a n ~ a ~ bmm of &n mB13tB1 imaga of each participant. PUI @ & m u $ ~ ~ d o W ~ E P e c a l l i w t h i ~
is @endent w the partioipmt~' &my b q r e s s and inkqm acculmb
These cqddties are affected by the two hm to amid sdenthts as emirommr
pd m & ~ Ewhmmt h twofold: in addition to t t a C t ~ l ~ e , i t m m q w s e a & e i n t e r a a l
the dhbgue. h P i p 11-1 iIIwtmtes, c l w k m m t s werlap, Init only t4 the
~ ~ B r e ~ * o r n f s ' ~ c e d l w r w f - ~ s r e ~ I f ~ e ~ ~ w o m a n ~ ~ t h e ~ ~ g l a a n ~ ~
IfoneortheotherIzadklr- m w e L M b y c r m .
Tknsmtjorportion ofeach k t w d tmvimment bmt ommm to both pa&iprrr~ts. DiBimnces in
maw, soci-c status, and among many *, create varied inter-
~ ~ t h a t a ~ ~ C M r n n n n i 0 8 - %M. h b wq1e WO, the quality and content
~beafFtxtdifthewomm's wmrumwnt is h t of a chief W v e
asrro&yI~.WhaZifbisfaBcinated@b W $ P d a h e i s u n i a ~ i n i t , o r s h e i s m ~ ~ ~ ~ ~ h e r L a 4 U - y e m - o l d bmhew
m ~ d f a c m ~ ~ s u c ~ o f ~ - mm?won, m* * Itas two aspects: the ex&-
i n k m d Th eff- of exkmal noise are , Lowi mUBic4 for example, Mts the
m a ' to hem ad, Gonmpmtly, %#he @ityoftheirdhkmcth
~ ~ M U O , ~ m k e i s to d a d p~@~lq@l factors. The f+hw&&
~ ~ & ~ ~ ~ t h e ~ c - ~ @ @ o l e g i c a l c d i t k m (e.g., t be ill? is she
hearing impaired?). The latter includes elements such as a participant's preoccupation, emotiod state. d defensiveness. In short, anything hap- pening in a participant's consciousness that didorla attention or distracts it from the cornmunicah process is psychological no& and impinges on both the accuracy of expression and of reception, Adler and Towne define this transactional model of communication as ''a continuous, irreversible, transactive process involving participants who occupy different but overlapping enviromnents and are simultaneously senders and receivers of mee sages, many of which are distorted by external, physiological, and psycholugical noise."
WHY IS COMMUNICAT1ON IMPORTANT? "Man is the talking animal." Speech and gestm saturate every facet of human existence. Why m the only animals that obviously and continuoudy engage in symbol making so occupied with this complex activity? Since the first tribal g~oup agreed that certain noises would represent spd- fied external objects or internal states of Homo sapiens have used language as a tool for fuh filling needs.
Abraham Maslow sd forth a hierarchical tax- onomy of human needs: (1) life, (2) safety, (3) belongingness and affection, (4) reapect and self-respect, and (5) self-actualization or the real- ization of individual potential. On the most basic level (need for life), the ability to communicate, bo share sensory impressions, played a substanh role in the sucem of the species by expanding tb limits of individual perception to include senmy data from others' nervous systems and by support- ing the cooperative activity necessary to sumid People warned one another of danger by shoutiqg wo& that meant "watch out"; they shared ad passed to their progeny stores of knowledge b facilitate life. Part of a tribal repertoire that M shared by symbols included Information such what plants to eat or make soap or baskets from ad what dangerous animals or places to avoid, Through verbal and nonverbal exchanges with immediate family, shamaus, and chiefs, people leamed and Willed needs for safety, inclusion, affection, and esteem. Because the basic net&


182 hrt Two Preparing the Patient for Complete Dentun Treatment
feehgs. Unexpressed emotions we likely to be ignored and may ultimately be relegated to the realm of the ~ 1 1 ~ c i o u s . The inaccurate and often negative mythology surrounding the acceptance and expression of'emotion can close the door on self-awmnms. For example, people often beIieve that their fmlings come from others. b4Yo~ make me happy" or 'You make me angry'' are c m o n expressions. Hawever, emotions, which are based on thoughts in response to situations and circum- stances, are generated from within. We are respon- sible for how we feel, Rqlacing "you" statements with "I" statements, such as "I feel happy (angry) when you call," conveys the notion of responsibil- ity and defuses the threatening implication of emo- tional control from without and msultant dependency. In adhtion, "I" statements ~ d u c e the risk that the receiver will react defensively.
Another common myth is the belief that being aware of a feeling or expressing it is synonymous with acting on it. Acknawledging anger does not commit one to yelling and throwing things. Rather than a call to immediate action, a feeling is a message from the inner self, an invitation to self-awareness. How or if to act on it is subject to the discretion of the inQvidua1 relative to the situation.
Awareness of physical reactions, followed by introspection, assists in recognizing and defining feelings. Strong emotions elicit rapid heartbeat, perppiring, and a shaky sensation-signs of both fear and anticipatiori. Subtle feelings are most fre- quently felt in the solar plexus or heart. A flutter or a pang here is a feeling message. Another way to tune in on feelings is to monitor h e r dialogue. mt are you saying to yourself: that you are worthy and capable? Feedback fi om others can also bring emotions and other unknown aspects of self into awareness and clarity. Genuineness, a quality of self-awareness, is expressed when comuaication accurately portrays inner experi- mce. Sir Francis Bacon stated the essence of gen- uineness when he wrote, "Be so true to thyself as thou be not false to others." Communicators who display genuineness inspire bust by exhibiting spe- cific behaviors. They are free from playing roles; that is to say, they do not disguise themselves or play games to manipulate others. They are aware
nesses; they tend not to react defensively; and they are open and consistent in thought, feeling, and behavior.
Attending behavior meam paylug attention ta I
or belug with mother and communicating this n m verbally with physical proximity; relaxed, opem posture; turning toward the partner; and eye contact. It includes sensitive interpretation of now I verbal messages. Attending behavior speaks of affection, respect, and esteem.
Listening, which is closely related to attending skills, is not merely hearing the other's words while waiting impatiently for a hlrn to talk. Effective lis- tening means being committed to understanding another. It also requires attention to, and accurate decoding of, both verbal and nonverbal messages. Nonverbal lauguage (proxemics, kinesics, and par- alanguage) conveys feelings and attitudes. Prox- emics is the study of the space between commuuicaton; kinesics concerns postures and facial expressions; and paralanguage is the use of sounds other than words, such as pause, pitch, and intonation. Accurate decoding of nonverbal lan- guage requires understanding that its mesmges an? ambiguous and sensitivity to their meaning within the context of the situation. Listening is essential for empathetic responding.
Empathy is the ability to see a situation from I
another's frame of refaence and to understand and appreciate someone else's feelings, perceptions, w attitudes. It does not necessarily connote agreement but does relay respect or the belief that the other is a worthwhile and capable individual. It functions to promote and communicate undewtandmg , l a m the groundwork for trust. It is a difficult skill because personal feelings and attitudes must be exchanged for openness and acceptance.
Self-disclosure broadens the base of un&r- standing and increases rapport. Persons wd hemseives contiauously through nonverbal behav. ior, but people hquently feel that self-disclosum means confessing faults and weaknesses. It is mom accurately a shanng of experience and resulting feelings within the context of an interaction Self-disclosure promotes trust in a relationship and encourages others to respond in kind.
Deep understanding combines the slalls of' attending, listening, and empathy to perceive and communicate information about another that me$
I


181 Part Twa Preparhrg the Patient for Complete Denture Treatment
d i m d y eFeabeamda&@verespoase to t h e p m ~ . T f w f $ s t f € ? w m i n u t e s o f m i n ~ m m critical in matihg inst. A warm relatimshp &odd be generated at the greeting before the initial inkmiew st-. Tbis is a c o o m p ~ by mtpthetic nwvetbal and verbal communications, a ~ ~ e ~ h m e i n t u i t i v e l y a a d o t h m h m e ~ i n l ~ t h e m l e o f s d o c t o r a n d wdng t h m l w to mmbhg it.
Bwlby'a research sug- that attachat behavior is a m q the htindve responses that qmw at b f i This mpome i~ bialogidy preset and therefope not dependent on pior learning. A W b t behavior is &fed as "seeking and mainhining proximity to mother individual." Attachment behavior is one set of instinctive mspomm that operates in the service of species d v a l . For the reminder of one's life, seeking md main- proximity to another individual wil l be a matkt of mhl importance. to existence.
All relatitionahips of comequence include &eat behavior and trust if they are to effec- tively d y e . When patients require the help of care p r o v i h (such as a dentist or physician] to c o ~ e for their most prized poswsdon (effective physical functioning), attachmat a d trust needs are activated The m y in which the clinician rec- qphs and responds to such needs can make a crucial difhmce in outcome.
A pattent may view a prodesis prescriphon with saw degree of dm. Wefs regard the pre- smipth as the ultimate disaster because prerioua experiences have indicated a maladaptive reyam#. This can be the case wen when an initial prosthetic qmience is an adaptive one, only to undergo a pmgn~dc change as a result of a con- tinwm of adverse morpho1agical sequel%. Hope- fully, b t &a&mmt M o m are ~timulated as ~ P . t ; g n t ~ f b r a ~ w h ~ i s c o n f i d u n t , &g, m s i b , sad supportive. The dentist who
I can gatigfy W w attadmmt behaviors is likely to have a considerable advantage in preparing a denture that is acceptable to the patient, both physidy a d emotimally,
THE IATRQSEDATIVE l NTERVI EW The hhwdative inkmiew is designed to help .dentists mobilize their resources so that they
operate in the mo& efficient way to mate tb climate of invohent and ?rust indhpmmble de altering malalapti-.
The iaxoaedative modd is a systematic, matic, "cherished" interaction used to reduce at eliminate most of the dental f m encountered ilC, practice. The definition of iatrowdation h " m a calm by the doctor's behavior." The word is a combination of iatm (doctor) and sedation (the act of malring calm). The goal of iatrosadak tion is to creata a relearning experience w b d a the feelings originfly learned will be m l e d and a new set of feelings generated as a conm qumce of the interaction between the &tor ad the patient. The iatrasedative interview is com- posed of four parts: (1) recognizing and acknowl- edging the probIem, (2) exploring a d iden- the problem, (3) interpreting and explaining t#e problem, and (4) offering a solution to t'tne problem.
RECOGNIZING AND ACKNOWLEDGI HG THE PROBLEM The following example started as an opm-emkd initial interview. The patient immediately i n d i d that emotional factors wen an important camp nent of her request fbr a n a denture. The doctq recognized this and acZmow1edgd it by s M h g & an iatrosedative interview. Had the Q c h responded to the patient's opening statement $ =king, "WeIl, what's the problem with yea denture?" this would indicate n o n a + % n o w l ~ and the desire to mwe the interview into the td nical-cd arena
EKample A 57-year-uld woman has an appointment to + a dentist concerning her inability to adapt 'to dentures. Mher d m this in fodon , he lamws v i ~ t d l y nothing abwt this patienL When he enters &a opmhy, his first hpmsion is of an petite woman who seems younger than age. She is seated, her face is expressiodess, and f& doctor infmthtsheis~ousordepressed~ begins with a g r d q and w e brief p l d q the continues:
&tor: What k i d of dzftculties m you having?


486 Pprf Tlwo Preparing the Pafknt for Complete Denture Treatment
d o r t ' t ~ w k y I c a m e ~ s t w ~ . g ~ p ~ t @ competent spaialists m l d not M& me & a m
* I c a r t U ~ ~ ~ ~ t h e ~ ~ B f f h e ~ m ~
patient appmd tmw and anxious. Her emo- k k d W d to a more aggr~sive p i - O r o a ~ w r h i ~ t b ~ e o f ~ m d ~ a g e ~ ~ ~ i a b o t b t h s ~ o f h m m i c e a n d t U e r ~ . 2 b ~ ~ t m ~ M a ~ 8 . ~ E i m i ~ t a ~ l y a s k k * ~ r e q ~ ~ n wmIidon despite her p s U r n , k wmnd ~ i a t o ~ u p o n k W y v e i l e d a n ~ . FM &e moment, fie doctor chows the iintt v Howem, he will keep in miad the ~ a n d ~ ~ f o r ~ ~ ~ t i n t k e inwvkw,
%W: W I k n t @ m u p . & & i kme &e &ehg th&$ m1*eone wt hgve u m w fo w p k . WpaustzJ Pi m hdp.
P E e r ~ i s n o t t o t a l , b u t ~ ~ m u s t be cautigYrr. what lqpmed with the prRtiws "very#aq?&&-**vf$ir& d d ~ b @ t h e f w u f W d w ~ .
lkkbr: T ~ a r e ~ ~ h a p p y w - t h the@- ~ ~ y o s r ~ t b q ?
r 9 a ~ d e ~ , h e r ~ ~ ~ ~ . . . I s ~ ~ a f
~ r m m f r m k p a s t ~ a 0 0 ~ ~ ~ - t h e ~ o n d i r ~ t o t h e tha or link to
~ ~ : ~ a n e ~ ~ t ~ # ~ ~ k g rdwmthtI#wsl ldkhppy~&h. I M&g t h m dhas I b e d weariw
a m ht*k&tdtkat tHeyaol l ldmab o m U d # C .
T h i B ~ L i t h e x : ~ d t i i e ~ b A m w w h s ~ m * d W @ m t m *nat difikmt I f d s * h l n h instam, @ ~ * f w u f w d o n f a , b & ~ ~ 2lbautemothda
D@am h wae ~ i & n g W b Q U t ~ m * ~ n r r J
The- Explicitly inimpre& what &patient ~ b m & s ~ B i m . A t t h i s ~ h e ~ t h a t i f & m j S ~ ~ c e Q f ~ , b e ~ ~ ~ l=tsdwu$a-tpb*-
P a - t d t l w ~ l ~ w f t h e p r o stated in the prcwhs @on of the
Wlpkthm.Irmw&wma
e a e t i ~ ~ I ~ W f b m e . I a m m m m h ~ i k m y ~
~ r : W ~ n r s t a m P s b ~ ~ f o us 4 child. D i d w rn ga used to the idea?

den WJ the feel den to '
efft
~ ~ t h n o n ~ w y t o u s e t h e i n f ~ o n and aoth Tim
~ & ~ i e 8 0 ~ ~ i n v o ~ t ~
F f k m M d s e ~ I t w m a ~ & M ~ ~ r ,
and F 9 .
i t P t ~ f n & ~ e n e d ~ ~ ~ c k i h i w J i t m ~ ~ lm b~ -1 k fm &.* m&ng her fwk w y old m&Wy. h f i a r - - o f m , d w e Tk -&b fw wfm&.t fD d lo*w wiw- irr~a+pal~tm.rn-m~rrn s m t m e of thgt bss* und your@Uw q h w m ~ ~ C t a n ~ & i ~ & ~ ~ ~ t ~ Y o w w k f f V B k m d t 8 $ w ~ n g d ~ kuweqfpwmderk- -e . 2% m a y h a w ~ t h & s ~ & r y m u m t W n g ~ t o mcept~m*pW?Mg F U Y W the- dilioq # ~ a a d ~ o f p u ~ ~ porting timum, may aut be qtbd$w m u&@w dentam q e r i a a . A th0mugh m i n a t h n will eroabie me to defmiw d d t w d&mth mihmb ofde- q p p r . b*yck tw h p b a ~ ~ w bt!pa~l&inpurpr&ula*cw. Nkidow hi&? Dam th& m a h 9-e tom?
Fwd: that sound~psdbb. m e exam& nation is d wt.)
D ~ 0 f : I w u n t g w r t u ~ ~ * 1 i a @ c a n &age, rzlld with that c h g e w can w t * u ta be &e to w the h t u m with c-rt. Tow gum, althwgh rmdw am heal* 7 % q are not u$mad, b u z ~ ~ o f ~ ~ p i ~ with the ~ ~ ~ d ~ ~ t h e ~ ~ ~ ~ ~ i ~ t h e p m ~ o f ~ d a ~ . m ~ m den- and s m ~t of+-, it i~ Z&.& that p u will rw haw the sammsgrou haw n m . kt$ t u i k a b o u t ~ w e r a a n d a
OFFER1 NG A SOUITfON TO THE PROBLEM
Doetor: I% w i l l , w d together in d n g ~~, df rn pikeonfdmt rhat, as we +wk things out i ~ q e h + yorrr faliugs aborrl p u r ~ e c ars$yourdenrwres wSIIcbgeso thatymwtllbe a M e t o i ~ ~ ~ ~ y . ~ t I i ~ h g t o tak timE to f&m wzi@tthg &tarmj%rpu. r a ~ ~ n s h g t s s 3 t 8 4 ~ u m t A s .
?'&&I h b ~ wb $0 h g ? I ) o c k c f t ~ ~ ~ ~ m a h ~ r h a t m
w e I l p ~ , & m ~ t a p t p ~ b e & f g * tion w i t h e mdIutaan tym to b w t A r t t t b d & y I p ~ t k ? * ~ h ~ ? ? l a r l f h c f n ~ ~ t f i T S t d a y o f m a ~ m t a i h t t t i m w s ~ ~ b8 avaliahie to he@ make you m-

188 hrt Two Preparing the Patient for Complete Denture Treatment 1 Patient: I really appmciate that, doc to^ f ie
other doctors wen so impatient with me and didn 'r seem to realize that I wrrr suffering so much emo- tionally. IIfed hopefuI and would like us to start.
The patient is grateful that the dentist is willing to spend the necessary time to make a good set of dentures. The great advantage is that the patient WIU get involved with the dentist as the helping, understanding, and supportive figure, reahzing that the dentist is extremely concerned about her long-term well-being. She also realizes that this dentist is maintaining an open-door policy. This cuntinues the building process toward an ever-mare-positive trusting relationship.
Doctor: Good. I am glad you feel optimistic about our working together. Let's set up an apa inhent to start treatment. J would like you to bring some photograph ofyou when you had your natural (own) teeth. They will be of great help to both of us in determining what your teeth looked Jib before and also help us in determining how to mmnge the new teeth.
&bent: I'll start looking for them. I think I h e wedding pictures whe~! I had a big smile on v & e . Tlx patient is now involved in the fabrication
of the new dentures, which adds another increment of mlationship building. If, after a considmble mount of treatment, it becomes apparent that the patient# adaptive ability is not increasing suffi- c idy , it would be in her best interest and the dentist's to address the issue. The timing is impor- tant h. This is a difficult issue. Most patimts reject the initial recommendation of dealing dire& with the emotional aspects of the problem. Nevertheless, with an understantllng approach, coupled with a strong relationship, such as exists with this patient, an initial rejection may change to -=.
Doctor: I am very concerned about our pmgms at this point. We have done e v e f i i n g that we can togethec and things are not going as well for you as they shorsld. My aperience has been that most patients would be able to manage these denturn. I am quite confrdnt that the stress you haw mderg~ne in losing your teeth a d struggling w'th the denturn is still afecting you. Themfore I think we should Bring someone in to help w with
1
I hose s t m s factors.
Patient: No, I don 't think I want to do this. I don 'r think I am emotionally disturbed.
Doctor: I did not mean to imply that you was an emotionally disturbed individual. We a12 haw specrfic areas in our lives that arz upsetting, ad for many people, accepting dentures is very d~j?- cult. I need to discuss this with you at this po-k because without solving this emotional aspect, we chance failure again, and you may be spending time, efort, and money unnec~psurily, What I would like you to do is think about it becawe I sin- cerely be l~ke it would be in your best inter& Perhaps share these thoughts with someone who is particularly close to you and whose opinioln you value. Call me next week, and let us discuss dti8 h e r the phone. One last point: next week you q still be opposed to my suggestion; however; in 4 or! 6 months you may fee2 differently about it and umt to explore my suggestion further. If that happens, feelf ie to cull me, and I'll be happy to help you k arty way I can.
There are a small percentage of patients who cannot adapt because they need their symptom Patients maintain symptoms for a variety of reasons. The symptoms may represent a way of rationalizing other problems and manipulatiq people, and they may be an exhibitionistic attempt to draw sympathy from other people. These symp toms may be absolutely necessary to maintain a precarious psychological equilibrium. If the patient cannot relinquish such symptoms, th dentist will fail.
SUM MARY Some patients are maladaptive because morpho- logical or neuromuscul~ deficits preclude successr fd wearing of dentures. Other patients am emotionally maladaptive. For these patients, eff* tive verbal and nonverbal communication is sig& icant in maximizing an effective doctorlpatient relationship and minimizing the maladaptive response. Often, patients who seek technical advice relative to a prosthesis are s e e h g emotional soIutions.
If the patient is maladaptive, the dentist cannot conclude that the patient is "neurotic'' and beyond the dentist's capacity to help. The dentist who sh& off the patient's desire to share his or her feel*

I' I
Ill

Materials Prescribed in the Management of Edentulous patients
The selection of rnateriaIs is based on a reconcilia- tion of their biocompatibility, optimum physical and mechanical properties an4 where indicated, their superior esthetic qualities. A fundamental howledge of the properties, as well as the lirmta- tions of dental materials i s crucial, so that dentists cm carefully manipulate those materials to the best benefit of the patient. This is further underscored by the fact that none of the materials used in den- tlstry or medicine are totally inert. Biodegradation of materials in the oral environment has been fre- quently related to chemical or mechanical factors prevailing in the oral cavity such as bacteria, saliva, and other oral fluids.
The aim of ths chapter is to present a synthesis of key information regarding biomaterials prescribed in the management of the edentulous patient. It is organized in five sections: denture base materials, denture teeth materials, Iining materials. denture cleansers, and cast metal alloys.
Fulfilling the requirements listed in Box 12- 1 may be a challenge for dental practitioners, consid- ering the number of new materials available on the dental market, often with unproven claims of supe- riority in biwompatibility, physical, and mechani- cal properties. The clinical efficiency of all prosthodontic materials should essentially be based on long-term, large-scale clinical trials, as well as strict adherence to internationally recognized spec- ifications and standards that gauge the quality and properties of those materia15 to ensure maximum safety, durability, and effectiveness.
DENTURE BASE MATERIALS Over the years a variety of materials have been used for the fabrication of denture bases. The most commonly used materials are polymers such aa polymethylmethacrylate (PMMA) or acrylic resins. Popularity of PMMA accrues from the fact that the material exhibits favorable working char- acteristics, has acceptable physical r n e c h c a l and esthetic properties, and is easy to fabricate with inexpensive equipment. However, as with all atheir known denture base materials, acrylic resin has its inherent limitations and does not fulfill all the requirements of a hypothetically ideal denture base material (Box 12-2).
The polymerization pmess of PMMA involves the conversion of low molecular weight monomers to high molecular wight polymers. Denture base resins are formed by a process of adhtional p o l y m e ~ m through the release of free radicals. The reaction passes through three stages, namely, activation and initiation, propagation, and fmally, termination. An initiator hke benzyl peroxide yields free radicals, which sets off the cham reaction. Activation of the initiator can be achlevsd through the application rif heat (heat-activated or cured PMMA), chemicah, such as tertiary amines (chemically activated PMMA), or by other sources of energy, such at^
visible light-activated (VLC) urethane dimehacry- late, or tbrough electromagnetic rahation such as in the case of microwave-activated resins.
Copolymers sue formed when monomers of two or more compatible types are joined. The vast

, General Requirements of I: Blmateda b for Edbntulo~s Patients
1. The material must k biotompatible: i. Noharmfule~~tsontheoraltissues
Norotoxic, nonirritairrrt Momllergenie, nancardnogenlc
2. The material mud fulfill dinical objective: OptirPlum physical and mechanical pmpedes:
Adequate hardness, rigidity, strength Y igh abrasion resistance Adequate thermal properties Adequate viscwlastir properties Chemical nondegradability
Superior &hetic propertis Hi@ kallsability Ea$y to fabricate and rnanipulatf: Readily avai table and economical to use Remits aasy and inexpemive maintenance
such as repairs and additions
I
rnajoriw of today's dentma are rtaade of h&- activated f MMA and c o p o l ~ , swh as m h r reinforced PMMA. The Mer is a hi&h-hp&$ acrylic reah, when the P W f o m gz& c ; s p o l ~ with pdystpne-butdiae niWez The rubber h d d m s s i w a m t l y impme i m p ~ ~ d t h o p o ~ ~ d e a k r r e ~ .
F o l p ? m with ckmicai bonds behuml differ- ent o h a h ape t e m d m-bki- This p m c a ~ aEe& phyddpmpdes oftbpo@m. In& caseofPMMA,ithuwwri~asm11ascraze ~ , w h i & b s t h a ~ o f ~ t o f o r m minutesurfam mch, andrdms&ereainh d u - b i h ~ in m g d c solvents. The chemical wmpi- t i o n o f ~ t l y u d ~ h e & i s W in Box 12-3.
W c r t t d W P M M A Powder-tiquid *ern Powder: prepomrized spheres vf BM MA
Initiato~ benloyl peroxide 4~0.5%) Pigments and dyed synthetic fibers
LiquU: methyl methamylate monomer Inhibitor: hydmquinone (tract$ Croslinking agent: &hytene glycol dirmetha-
wlak (-1a4e) ~ctiv-r-~Nimdfifl-ptoluidine'
' M k e A d W d PMMA ~owder4iquid system sitmitar to hmi-hated PMMA: with slighr
mdiWcatiatmr,to accommodate 'the micro- wave aadwation pmdure
r J g h t ~ m C ~ MNglc 4mnWmmi phed C s l r e e ~ a d nrymd Matrix: urethane dinmetkatrylate, microfine silica fiHh; acrylic rein beads Photolnitlatar: camphomquine-arnint
"Only in chemimlly activated rwihs. I RbMnPR?lurodbvlmwI~te-

192 Part- Reparing the Patient for Complete Denture Treatment
Techd@ Considemtions and Properties of Bsse Resins
PMMA Thew resins are commonly @#&wed in a brass flask usmg a compression- i W h g techdque (dough technique). The polymer @monomer are mixed in the proper ratio of 3:l by volume or 2.5:l by wight. The mixed material groes through four stages: fm a wet, sandlike stage; &wmxl, a tiicky fibrous stage as the polper dis- wives in the monomer; third, a smooth, doughlike m, suitable for packing into a mold; and fourth r stiff, rubberlike stage. Dough formation is w i d by i n t d plasticizers chemically attached to the polper beads that locally s o h tbrm and facilitates monomer diffusion,
After wax ehhation, the dough is packed in a gypsum mold The flasks are placed, under pres- am, in a time-kmpmatwe controlled water bath to initiate polymerization of the resin.
The plymerimtion reaction is exothermic in mhre ispd should be carefully coatrolled to avoid a m a d d increase. in temperatuw, which may exceed - tbe boiling point of mracted monomer (1 OO.SmC), W i n g to denture porosity. Gaseous porosity due to rapid heating and manoma evaporation a- as fine, d o r m spherical porn, l&ed more offen ia the thicker portions of the denture.
Inadqwdo pressure during £lask closure, an - insufF~cient mount of dough present on packing of
the mold, or impqm mixing of pcrwderfliquid mnpmta may also result in derrture porosity. The d t h g porosity will inevitably compromise the phyaicd and denture esthetics and mrry promote the accumulation of dature deposits, wbich muld adversely affect tbe health of the t 3 f m l m - m g tissues.
In peneral, heat-activated acryh resins are plymend by placing the flasks in a constant- bmpmdwe water bath at 74'C (165'F) for 8 horn ar longer with or without a 2- to 3-hour tamhd boil at 1 W'C. A shorter cycIe imfolves processing 4b resin at 74'C for approximately 2 hours thm W i n g at 100°C for 1 hour or longer.
Rapidsure type resin^ have been recently btmduced in the marlat, The resins are polymer- id by rapidly heating h e packed in bniling w&r for 28 minutes. The materials are hybnd acrylics, in which activation of the polperization
reaction is carded out through both chemical and heat activators, allowing rapid palymerizatioa withut porosity.
It &odd be notsd, however, that processing $ ~~s that are too low or for shorter timee inereases the residual monomer content in thj processed denture base. Exass residual mown& in the polymerized resin baae could lead to tisw irritation, sensitivity, or even allergic r e a c h $ in some patients. The plasticizing effects of m e s s monomer could also adversely S e c t lh# properties and dimensional stability of the dun- Fortunately, allergies to residual monomer = relatively rare, and most patients are welI able C tolerate the 02% to 0.5 % of residual monomer W often remains, even in a properly p o l y m d bas&
After tbe polymhtion procedure, the den# flasks are cooled slowly to mom temperam t# allow adequate rel- of internal stresses and thw minimize warpage of the bases. Defiasking theg follows a d should be done carefully to avoid h hue or flexing of the dentures.
The popularity a d relative simplicity of th compression molding technique are uwlly over- shadowed by the hi#-prmessing stresses that W induced in the resins during polymerization. ThW stresses result from various factors. First, pol? imtion shrinkage, which occurs as polymer c m are formed, accounts for a volumetric sbrkhge d about 7%. Second, t h d shrinkage follows ah the resin cools. h addition, differences in b m d contraction of the rerin and gypsum mold c o l l ~ tively yield stresses in the resin. Tt ia tmpthg 1 assume that the release of such cumulative sirem may give rise to dimensional changes and inacm racies in th~ fit of the denture base. However, th@ changes have been found to be c~~ insip& cant in the fit of heat-activated acrylic resin bases, and in most imtauces they do not cause. & comfort to the patient. O c c l d errors that d commdy encountered &er pmwssing are ei% tively corrected and fbe predetermined vertid dimension of occlwim restored through TOUW laboratory remount procedures. I
Denture base ~~ are also subjected to 4 variety of stresws muring function. Midline fM4 tures of dexlhms during funct~on have been e; ered a flexural fatigue failure because of cycI& deformation of the base during functiwt This &

h a r h e d in the Managemant d €dmWIotls P a W s
H ~ t h m i P M M A i l 5 l ~ ~ ~ ~ ushg $n ~ ~ n t r n ~ tdmiqiw. Tha resh t m i x L ~ i t l C o a ~ ~ ~ u n d e r
demo&mb m i n i m r r m p o ~ t i l a n *. ~ p ~ s ~ ~ ~ m m o ~ ~ p o 3 ~ , @ n , ~ ~ = Y ~ * Wer p b t b muM.be dM tn patients with a c d h n e a i allergy .ta the # d m a y h ~ . m w * c - a r t d d * ~ o f ~ w ~ ~ b a p p ~ ~ ~ ~ fdxkatim
T h ~ ~ ~ ~ f t e n r e f e r r e d t u t l z ? c o ~ M-, ur ampo+mbhg dm. As pointed o u t ~ * t h e ~ 1 ~ ~ m o ~ ~ - tains a chemical initiam, a Wwy m h , which *tea p~1-on pmmw ~~~ d o f U n y h € & ~ ~ ~ m ~ ~ much lem fmpnilqused fw denme f&hihn as cumpared with the h ~ t - ~ w b d mbs, ~ o r * m i m s d b ~ m b g . ~ ~ ~ h a ~ ~ ~ a t ~ ~ o f t h e r e a r i n ~ p e c i ~ 3 Q ~ ~ f b k ~ l ~ ~ ~ , ' P f i e ~ o o P l d d m ~ u s w d ~ ~ ~ u s i n g ~ p W ~ W ~ ~ . T l X e ~ ~ ~ h ~ ~
, . 0 f ~ ~ t t s e d i ; a t h i a ~ q U e i s ~ ~ ~ 0 f ~ ~ ~ ~ Q ~ flWtyaft€W&

i m P o 1 ~ pouring the fhlid of a rwmi'bIe hydm
kmpmtworatasligbtly q. Pdym* is cam-
5 & W b . The k C h * ~ &
~ m d ~ b u f i s p r o a e t o ~ , s u c h . a a p ~ o f ~ ~ r h n r i a g ; ~ o f t h e ~ i n @ ~ m o i d . T h e ~ o f a ~ f l a s k ~W-S m-c PS- m14 ~ ~ a i x ~ m i n ~ m i x , ~ ~ 1 * a & w e r & b . h eomparimi with heat-activated resins,
chedd lpdwtdras ineb , ittgmed,hwea & & r ~ ~ ~ o f 3 % t o S O / a . Wymeiidm in dwm resins is never as q i e t e sk ~ 4 v a e a d ~ s , T h i s & x % i a i & r i o r ~ a k l p t o p e r t i e s a n d ~ c a l l y c o m p r o -
bb@bllity of the dentwe bases. lb matehis exbibit higher so1ub'U-y; they h a v ~ h&rh mIm &Mhty* due Eo oxidation of the B w w - ; a n d ~ - ~ t ' e ~ h l & ,
d e r ilfcfmsed mEsses. H
i m h x d ~ g ~ ~ ~ ,
&dbwms are ~ ~ e c ~ c waves in the ~ ~ m n g e ~ ~ k r t c e n t l y tuactiraBetk.potpexbthn~ of
r e s i n ~ . T h 4 3 ~ ~ ~ ~ i m - @i&dhI9&,withtlrr,' afa@ ~ F ~ ~ ~ ~ ~ e f w ~ m ~ ~ a ~ e n . T h e ~ i c : & & i ~ i a a
~ ~ ~ ~ m t i ~ s ~ a h d c h e ~ i - ~ ~ ~ ~ m ~ a ~ i s ~ ~ t o ~ ~ ~ u f m o n o r n e r , h a ~ & m t ~ G y & o P ~ u & 3 m i n u t e s . h ~ ~ ~ ~ k p r r p ~ g ~ w i ~ t h e m o n ~ ~ a m W . ~ ~ u s rapid intend- c o r n s . th &gma of pdylnerimtion iiwIwm3,
~ ~ ~ ~ p ~ , a n d ~ m q g y i s ~ ~ h ~ m o n a m e r

MATEREALS USED IN THE FABMCBTlON OF PROSTHR'IC DENTURE TEETH ~ e t i c o r ~ ~ m p ~ h a v a r i e t y o f W ~ ! & 4 & ~ * ~ 1 * ~ ~ -
pwoew acryli~ mills, mOdit%d WxyEi~, IurdGompDsh~hfnW&h~ fabrimtion of dmhm ~houfd den~m&atu o p t i m m n p ~ a n d m d m i d ~ t a w ~ ~ w ~ o f ~ ~ f r m c - t i ~ 1 8 , & a a ~ W t i n & ~ , o r c r u s h - ing of food, aad shmbwnuly miW @or ~ ~ h * ~ n ~ o t ~ d W mu& @ax f 2.4).

Processin: rrdmlqd R d a Method d kthatlon
7 , s
-tPllcr
-tional heat- adi~twl PMMA
Corn pression-mo tdedldough Gwd biocompatibility Low technique density Flask and gypsum mold Good esthetics, color Water bath short or stability, surface finish lang cycles Insoluble in oral fluids
Chemical bond with resin teeth
Acceptable dimensional stability
Easily repairedlmodified Easy to fabricatellow cost
ntbber Compression molded High impad strength bhforced WMA Water bath short or long
cycles I
Low thermal conductivity lp impaa and flexural strengths
Short fatigue life tow abrasion
resistance Radlolucent
Reduced stiffndrigidiw Mom expensive than
conventional PMMA
. M-actimtd fiber Compression molded High impact and flexutal Unesthetic color of Carbon r e i n f d PMMA Water bath short or long strengths and Uvlar fibers
Wle~ Good fatigue resistance Inferior surface finish i High stiffness Increased production time
Difficulty in handling and placement of fi bet%
Cmph:rxroWw Dimensimlfy wrq@ High residual monomer @ PPW~~UM & out Imsl- eag-to Mask content
.zFM twcessinjg is less time- High creep rates Qlly adhated tomim Reduced stifFnw
. .. Lower impadfatigue strev 1 , r . . . I + I - , , COIW instability tfigh duMI LW.\ -: - I 2 h, 1 : Tooth m o w w m t h h I d
. . : - , , .. failures in pour resirms
Mkcrowawactitivated Compresion molded Short processing time High mpital cost PMMA Fiber r e i n f o d plastic Rask Pmcwing technique Flasks easily fractured
Microwave energy in an easytclean limited serviceability wen at 500-600 W Dirnensiona l accuracy Porosity if tirn%temperaCure
Curing time as short as Comparable physicall of oven not controlled 3 minutes mechaniml properties
to conventionally prpcessed resins
Ught-mated PlWMA No flask required 9 --h i.l. .:: High intensity visible light
--= F I Y ~ W , (wavelength 400-500 nm) -2, .U .-# : In special light chamber i,,,: ,,, ,, . , , , , , Curing time 10 minuta *,.I ,, . : -, .., ,., * , l l . . * J ; . l . ! .,:, :. ,\ , ,-,
- I ' . . '.' . 1 1 7 , ; ;,,. ,* ' , i , ., ,, , t $ I V \ . / i l k 1. - - , ).
>,:. .! , ;...: . b y , . ; ) l # p L! w * , . - : l . . t . ; ~ . . ' I
Simple processing technique High capital Cwt Shwt processing time inferior bond to resin No methacrylate monomer denture Low polymerization Decreased elastic
shrinkage teeth modulus Slightty Improved fit lower flexural strength Comparable impact strengh ', and hardness to conven- ' tionally p r o c d resins

Penture Teeth ;.a D u a b l ~ band with the denture base material . -2. Reslsme to oral fluiddsalwnts ,3. High impact strength to withstand forces '. during masriation 4, High abrasion reristame with little or no
weat to maintain the predetermined verticaI dimension of occlusion and withstand parafunctional movements
5 Whetidly pleasing, inconspicuous, ade- w&tC tramluancy, color stability, goad
. surfa* ietmwre, and ease d characterization to pradweq natural appearance
6, Easily adjuBkd and . easily polished
I --- grinding of the teeth to abie interocclusal S p c a
@ws mhaping of the teeth to fit d l spaem
s qditim of acrylic resin teeth
dimension of occlusion, #uWy k ka&w denture wearers. However, n w t &e&@k~ modifled acrylic miin teeth am mom war mi&-- ant and * m u c h l w Wn wlia-dm& teeth.
C Q m p o s i t e r e ~ m k a t h h a v e a l s o b s e n ~ d a o e d ~ a a k m f ~ r - d d f m t l u c w T b q r ~ m i w y ) f m f i t I e r ~ c ~ w r o f d i c a a a d h m ~ & a a e a ~ ~ ~ ties that rue c l i n i d y -1e. ClMlthpd i m p ~ i n t h e p o l y m e r s ~ m q ~ iatz ib d e s p d we+ by most cligichs in the future.
Porcelain is another m&&d that has k m q h p o p u l a r f O r f a b E i ~ ~ ~ f ~ ~ ~ m E @ y yeam. Pamelain teeth, in pd, exhibit q e r k dW£ic qnalbm d l e n t color Nahlq, andldgh aas ion -. They am m e e h d d y ~ t a r e s i n ~ b y m ~ o f p i U s Q r ~ hob$ and this attachment p d u d e s h i r aW& to b o g r o u n d , o r ~ t o f i t ~ t e d i n ~ , p e a . Bonding of ~~ teeth to acrylic lsasea has been reoently enhaaced by a combinaaim of micromechanical retention atld c h d d boding. TkiacarriedoutbytPearingthxidgelap~of thetQothwiaha$t*dahyM*d gel, f h d pr 1 l?ihwoupw agent,
A n o ~ l r m i t a t r o n a f ~ ~ ~ ~ their ability to cause significant wear of opfwshg cmme1 and M c occlW surfaces* The t d am quite brittle, ean wsdy cmk or chip on and ue mcttlt to &d for ooclnsd 4j-B beFaw thy 1- their d m glaze end repolish-
is q u h &Ficarlt. P o d & taeth produce noisy clickhg som& on mntact witb each other. ~ , t h e ~ a r e n o t w i t h & m e r i t s , T h q a m d h e m i d y stable; am hard, in m q h o n with the ~ o f t e p auylic rash; exhibit no permanent d t f ~ a n ~ o c c ; l ~ loading; andare kl- u b l e i n o r a I ~ d a a x i d i n m o s t ~ s o 1 ~ .
In the seMonof dentnretee&forwnpl&e denture$ and c- the d y m a t i d properties of the mriom mamiah, the M s t should avoid c o m b ' i @or reein tmth with p o ~ ~ m ~ . T b e s ~ ~ i n ~ i o n ~ i n b o t h ~ * a c t y l i c m i n ~ n a o r e m p i d l y t h a n ~ ~ d ~ ~ y ~ t e d e & u c t i v e ~ ~ i n t h e m t & r & ~ ~ . o f t h e ~ 7 h b l e & 2

Ptrt Two Reparing the Patient far complete Denture Treatment
~ t h e p m p & ~ o f a t . z y l i c a n d p w c e l a i n - m i & m m a p m a d teeth. -m DENTUBE-LlN I N G MATECUAW Short-Tern Soft lines (E1ss1xe Condition IkntuwMng m a t e d 8 am used to refxt he sur- Them materids are mR, resilient materids
I. Shoa-tam soft h e m (time conditioners) 2. L a n g - m soft liners
these materids inside the mouth p d d a them process, wi& a whole m g e of diagnostic, adjunctive, and or any monomeric mbtmces hi cud
tissue iniEatia Upon mixing the pow
reduceniVD0 -on o#p&ngd&on Can oppos haturn1 teeth or
@&&c propertlec
=$$gwnss

1 Linersmssue Conditioners
ment and conditioning of abusedlirri- denture supporting tissues lining ill- denlures allows the tissues to rest and
rep in their health prior to impression making for new dentures
2. For provisional adjundiveldiagnostic pur- poses such as recovery of the vertical dirnen- sinn of occlusian and correcting occlusion of old prosthesis; also to assess the necessity of using a permanent soft liner for patients with chronic pain or soreness associated with denture wearing
3. Temporary relining of immediate den- tureslimmediate surgical splints
4. Relining clefi palate speech aids 5. Tissue-conditioning during implant healing 6. Functional impression materials
1CLU
char
posr q17R
with a fn proc rial dete
sive fitLij coel as a a y w condixw

200 Parl lh Preparing the Patient for Complete Denture
propdm; some fuIfdI the requirements of an optimum functional impression mtdd more e f i - cimtly than others. The choice of materials should be based on a thorough understanding of their properties in conjunction with their effective ch i - d applications,
&#Mmini$tmd Home Refhes lhnttmw m-the-eounter tempmy reline mate- r&& aae awdlable for patients' use and are mar- ~ a $ ' ' h e r e h . ' ' T h e m a ~ allow the ~ t P d j u s t t h e f * l t o f t t r e i r d ~ ~ . T h e y a r e ~ a s p r e ~ t h g r m a p I & c p a d s o r i n a pawdsdiw fwm and b e a simh compidan F m d ~ o n a r s ~ l i a a s , T h e ~ l b i ~ ~ d d a n g e r o f ~ ~ r u e t h e h i & ~ f o r $ l e i r m i s u ~ . h p ~ a & m i c e b ~ b ~ o n ~ p r o p e ~ m i p i n g of* CMhplem or lmg~#rm use of h+$$ ltnees
k d to tmma, can cause irritation to tfie &lying tissues, may adversely affect the derrture bme materials, and may muse occlusal emmi. There is a unanimous consensus that ~ ~ d b e ~ discmuraged fromusing ~ ~ a s r a & ~ i u t e f o r m l d n g ~
w.
Treatment
Requirerrrenb af an !deal 4 ~ T m I I .k€k Unslr
1, ~iaomp&&1'* 2. Cwod dirn&u~l stability 3, Lm WB wr~tion md water solublity 4, Good wettaUlW by saliva 5. R r m a m a saftnesslcompl~mW~i~t~ela~
ticity 5.. Atkqupte abraion ralsistance and tear
resistance 7, God Md tv$he denture base B UnzrfftxW b,qu&us environment and
ctemxrs, easy $0 dean 4. Simple to #anipulakv,
la . , Calorstilblc and &bits good , 1 1 ~ Inh&its mhbtiarl. of fungi and @tiler
rnirm~pnim

I M i r e d hi the hdanagwnantof BkntdwsWiW

2 Part Two Preparing the Patient for Complete Denture Treatment
b
,:*-& Fig"c 12-1 A, Recently amp teed resilient liner on a mandibular denture. i B, A 6-month-old resilient liner with foci of yeast co tonier already apparent. C, A neglected
12-month-old resilient liner with a l m d total coverage by yeast colonies.
d h denhimam be cleaned a9 &scribed, b u t h l i n e r i W c a n b e ~ w i t h ~ u n d e r c d d wakz Box 12-7 p v i & a comparison of proper- th o £ p W h k d acrylics versus siticme r u b k .
Q i a i c a l ~ i n d i c a t e s a l m a p t I m i d iimetohmm OPsufiWn rmdacqtablepatient &m.H-+-,the-traveta b e ~ m ~ ~ ~ n o n e & ~ ~ ~ s o f t ~ ~ n li&ape&mqmmpmbletotttatoftb~& ?sum h e . Impmmd strength, permaaent millmay, h p m d adhesion to the #mtme h, the ability to inhXf f#mtb of micmqmkms, W M d d i l i t y & f ~ b & h fbcua of ongoing rM?w2h. Thew ammp hcMe s T l r & e . ~ d b * ~ w h m t h t - ah&ed capo1ygxers and intqration with antifnn-
anponents. Wico~se rubw, w b properly
wed, may be the mmt appropriate of the !ype+s available, lnd they too are only ten expedienb and mu& be inspected regularly dentist and replaced when unsatisfactc painfed out earlier, fithe application of deansem and home am habib has mtr ib the UBB of t h e mat&& wilh significanq fichl &&s:. It must be q h a a i d , howm using thae materids d m nat p l u d e d to thu fundauld principles of comple& comtnu:tion. N~rtheless , Man used gene, soft i i i ape an exceilmt 4- in able prssthodontica.
DENTURE CLEBNSERS Education of patients irS crucial to mhm ~ 0 f b o t h t i m i ~ ~ a a d ~

physical r indmechddpmpdes of prtwhis. Fd-, it mast be
id pbqm awmufa- *tissue *-
r p m m adverse
ofdenkrreds@tsdthirr&
Patients am routinely imtmctd to ohan their den- E1 IEe [ ibyUg#t~wiE f tamf i~brushar ~ r n u l ~ s u ~ nyhn brush withmudden& and and wa& Tfie m~~ cleaning d o n o f k h a h i s ~ d y ~ c i e m t o r s m a v e l m d y - w f t M - , - w tbdeatwbaauandketh H-, i t ia in* t i v e f o r ~ & ~ T h e r a m d a f W ~ ~ ~ p ~ a a d ~ ~ ~ vigomls-lwchablh~ua~offmma- s i o n c l r ~ ~ d ~ m ~ ~ d i t u ~ acid cleantiem
T h ~ u s e a f b s r d ~ ~ , f O W ~ i n g , c r * d e n M m , d m d W c a r - ~ o r h y d m b d s ~ m r r y ~ e ~ o f p o ~ m a ~ ~ d t h ~ o n t l t a i r surfam, TBe rolrgh, lrn?@ar ~~ prom*

2 P . r ~ Two Preparing the Patient for Complete Denture
W ~ ~ o ~ U # d ~ ~ h d d h t m e clwmsers w e immersion tddqw~s; these includa alkaline peroxides and b ~ o r i t ~ . Adwantages of immmion c l e a m a inch& Ml lacsElssiw@ of the salutiona to dl 8Ea of tbe dameI xlhimm damage i3om m i s b d l @ &a- mes, m3nimum ahdun of dentme befi a d mt& amd uae dqlicity af the technique.
-Ratlag Cleamsm Ahline ~~ am pmided in powder md tablet f m The materid m x ~ t a b &dine oompmh, d&qpta, sodium ~ a n d f l a v o r i n g ~ . ~ ~ w i t h ~ ~ u m ~ d e m ~ * i & g ~ ~ ~ i n . ~ ~ ~ r u ~ y ~ C b & g is atesuEt of the oxidizing ablllty of the p&d&&mmpmitimrtnd h t b e ePlFemm&
of the evolved oxygen, This eff&ly dmn, &ssolves, and floats away organic
m. Peroxides are
solution ia n safe, effeclive ~ d e & q d ~ m , p a f -
h h l y amone geriatric or &bled patients, ~ I i m i t d d i k k d Q q d e t e r t h e m ~ ~ m e c W ~ ~ B t n g ~ p .
& y p d t h k Wlrrtiuns Diluted household (fludim hypochl-) 0re wmmnly
~wardear~urel~forIsmwingpZaqueand I&& MI, atid are q x & e of lrilling denture dh6mt ~ $ m . me technique i w o w the ~ o f f h e ~ i n a ~ ~ m a f a m p s r t @ 5 ! m o & m ~ % h ~ p r r t r s ~ f ~ a t e r Q : 3 m m ) f b l l o w d ~ ~ ~ l l r ~ &
' * - i s - k a - m
Treatment
~ ~ ~ h o s p i a DilW wid8 (cftdc &a,
d t h e ~ P w & ~ s l ! h may^^
8 DEmw cleaasem con- (mulanene auti pk-) haw -

Table 12-3 7 n i c . r l t r 3 n b 3 n o c ~f tha Il=r;n#ac Twnnc nf n a m t ~ h r n r l m - n c ~ r r
Alkaline perbarate ineffectice for removal of heavy ta tabs deposits; harmful to wtt liners
Dilute sodium hypochlorite May bleach denture base resins May discolor soft liners Cormion of base-metal alloys Unpleasant odor Cormion of mme alloys

206 WTWO m n g the Patient fur Complete Dentur
B Figure 12-2 sletal bases for complete dentures. A, Gold, stellite (cohaitlchmrniurn), or titanium alloy covers the palate and residual ridges with the borders farmed in acrylic resin. It should be noted that many dentists prefer to no? cover the residual ridges with metal 50 as to facilitate relieving and relining proceduw for acrylic resin covered sites in the future. B, Also m e that the posterior palatal seal area need not be made of metal, Many dentists prefer a "mesh" am here to provide a d l e n t retention for an actylic posterior palatal seal. The tuberosity regions may need to be entidy covered in metal or a mesh plus acrylic as &mted by the interarch space.
included we aluminum, copper, iron, and platinum, Molybdenum, tungsten, and carbon are fso & as hardening and strengthening ele- men&. Tbe resulting alIoys @lay high strength, h h w , high modulus of elasticity (stiffness), low dwity, and high cornsion resistance, and they have a substantially lower cost than gold
'allays.
r Treatment
Nickel&mium alloys contain h u t nickel and a lower inclusion of beryllium (0. lowers the melting range the allay. The ixacluaion D the formation of pound that increases the strength d h d n the allay. Box 12-9 lists the advantages aud vantages of base metal alloyti, as compared resin complete denlure bases as listed in Table
The controverq stmounding 'the bi bility of cobalt- and nickel-containing potential allergenics and the biological metal ions re lead in the mouth during corn (such as beryllium, a carcinogenic hazard) the mwits of another cast base metal, titmi rtn alternative. Superiority of titanium stem its remiirkable biwmpatibility and high c resistance. In addition, it exhibits high dimens stability, low density, and mechanical that are comparable to those of cobalt alloys. The main drawback of titanium as a

W M In the Ma- of EdenCuhs Patkilt rn
W S ' 3 1 U P L , ~ A , R l b o B e t a l : ~ ~ ~ ~~l~~~ ;tt:Ul-135, m*
- B C ; H s t r i a b n & ~ K t l : m t ~ p f ~ JtkdRehMZa.185-144, 1999.
K a k m o $ ~ ~ - @ h m A m a a I : M u m w o f ~ d w d g n 0 n c d l h h - J
arm of &@Em. In thig m, ~ ~ , a b k r # s , ~ d m t d ~ e d l l , ~ t **-+
~ & ~ m i @ , ~ ~ , ~ . l i d s r l : ~ k d w ~ f ~ d l ~ - & r * a r t ~ ~ n * ~ ~ ~ ~ o t a
h 4 n m h & ~ ~ ~ ~ T o t I ~ ~ ~ ~ ~ ~ ~ ~ . J O n d ~
O m a h Wk Dmd m t d d s a d tk& Midon, Cd 3.
bEpn-&ulm &%1%7-190,1992.
JnBrladenWWIlt, ~ P D ~ f e & l ~ ,
W'u15Fl%- ,
~ m ~ ~ ~ b e c h n t c a i ~ ~ a r t d h L % v h ar, rditQE FhlW'
WBtWdm" ~ ~ ~ ~ , b & w ~ m w i g - ~ i a p s t -
8-h! J~ I%&&M 3i477-483, mL. WE- """*"%+ r ~ a a d ~ J ~ ~
PnrePld341, m&&iX~&@aWaTaal:B~ofvisreoelogtie
pmpstb&&-~wpresantlaatrahb mf ~~~1m~IOOS,2(#1I.
T s ] e a t i e s h i Y , ~ T . ~ T a t a l : Thekrndstm@oI * w b m w w r ~ y h - 13:M,ZMO.
~ T , ~ J Q ~ d # k ? m b a d w a ; ~ Q f ~ a a 8 ~ ~ o f ~ 0 a . bt J P w r k d M 2i 555-%0,19@.
T a a H & w & ~ s s ~ & ~ Q f ~ ~ ~ - &i&sad , * M o m P w B B ~ ~ h b ~ d ~ - 9:14&153, aowl.


I f l J ~ f l ~ ~ i ~ ~ ~ i ~ l l f l ~ ~ f l ~ [ ( ~ ~ \ IN I , ... 1 . . . - I l l , . , , , ,
ing an AnalogueISubstitute for I the Maxillary Denture-Bearing Area David M. Davis
If dentures and their supporting tissues are to coex- ist far a reasonable length of tirne, the dentist must fully understand the anatomy of the supporting and limiting structures involved, for these are the foun- dation of the denture-bearing area. The denture base must extend as far as possible without inter- fering in the health or function of the tissues. It is convenient to regard the impression surface of a denture as comprising two areas: a stress-bearing or supporting area and a peripheral or limiting area. h h of these is discussed separately, but like the sides of a coin they are inseparable.
ANATOMY OF SUPPORTING VRUCTURES The foundation for dentures is made up of bone of the hard palate and residual ridge, covered by mucous membrane. The denture base rests on the mucous membrane, which serves as a cushion btween the base and the supporting bone.
Mucous Membrane The mucous membrane is composed of mucosa and submucosa. The submucosa is formed by con- nective tissue that varies in character from dense to h s e areolar tissue and also varies considerably in thickness. The submucosa may contain glandular, fat, or muscle cells and transmits the blood and nerve supply to the mucosa. Where the mucous membrane is attached to bone, the attachment mius between the submucosa and the periosteal covering of the bone.
The mucosa is formed by slratified squamous epithelium, which often is kerahmd, and a subja- cent narrow layer of connective tissue hown as the lamina propria. In the edentulous person, the mucosa covering the hard palate and the crest of the residual ridge, including the residual attached gingiva, is classified as masticatory mucosa. It is cbaractmked by a welldefined keratinid layer on its outermost surface that is subject to changes in thickness depending on whether dentures are warn and on the clinical acceptability of the dentures.
Although the importance of the mucosa from a health standpoint cmnot be neglected, the thick- ness and consistency of the submucosa are largely responsible for the support that the mucous mem- brane affords a denture because in most instances, the submucosa makes up the bulk of the mucous membrane. In a healthy mouth, the submucosa is firmly attached to the periosteum of the underlying supporting bone and will usually withstand suc- cessfully the pressures of the dentures. When the submucosal layer is thin, the soft tissues will be nonresilient, and the mucous membrane will be easily traumatized. When the submucosal layer is loosely attached to thy periosteum or it is inflamed or edematous, the tissue is easily displaceable, and the stability and support of the dentures are adversely affected
Hard Palate The ultimate support for a maxihy denture is the bone of the two maxillae and the pdatine bone. The palatine processes of the maxillae are joined together at the medial suture (Figure 13-1). The

M T h m e Rehabilitation of the Edentulous Patient: Fabrication of Complete Dentures
la-7 Both We maw lhe ana Phe palahlw bone g r W w o r t fw w upper den- Wre. Indvidlral diffemces is form W r m i m how forces should k directed to these bones dudrig function. A, Spiny p r s j m that would Irritate ti- under a denture. B, Rough ad trc-lar bone of the M l l a r y ridges. C, Incisive foramen, whicfi comes to lie doser to the tmt d !he ficlg~ as resorption €ab place. Thus the loation of the incislye papilla, which carpers the Lcisive foramen, In relation to the crest of the ri@ b a guide to the anmnf of re~rption that has ocntmd. D, Greater palatine h m e n , which often has a spiny oyedwtging edg& to it.
~ ~ u f t b ~ U l l e m d ~ p a l ~ e andd&oughitmnf&ubtothe ~ ~ ~ ~ o n f o r t h e h a r d ~ ~ a n d ~ ~ , ~ ~ t s r t ~ m a f ~ ~ b f r : s u p p o r t f b r a h e d e l ? t m . M o r e ~ t o t f t e m i ~ p m i d e s t b ~ ~ ~ ~ ~ f k t i ~ ~ t i n c r e ~ areaforthedenture.Tnhmao ofthe^^ he^^ palateiss&atanangletoth
A~aectionof&ehtrrdpslaetedmwthatthe ~ ~ ~ b y s o f i ~ i b l ~ b y ~ t i ~ a f ~ t h i o ~ , t r i b u t e s t o t f r e ~ ~ g f ~ m ~ b e p I W u m L k m t i d d t b q g b o m h y colpobciQ. Ttre submucaosa ~ h ~ ~ g i g n o f t h e ~ ~ ~ , t h e ~ s i v e p a p i U a m d ~ ~ e s u b m c m i s ~ * w i t h ~ ~ t ~ t h e l l a c p w h d o m d - . t h s d l ~ i s ~ i n ~ k & t h e mdrdym% bone. For this EwQQ tho eaA tissve *ha, ~ ~ m e d i a l ~ ~ i s ~ ~ ~ dnyrtkdtoberdiandmawidtrrrrm.hm ~heshapoanhsheoffalalveolsr
when tht? mfml teoth am moved.


214 M Xlm* Rehabilitation of the Edmtulous Patient: Fabrication of Complete Dentures
is an indieation chat ~ ~ 1 1 - f w h q dm- 4 u m ~ b e i m p r W i n m i n t a h h g t b a : n w m a l ~ ~ ~ ~ o f ~ m o ~ ~ o f E t r e ~ ~ f ~ r e f i W ~ r h r o ~ ~ t o o t f m - b m h ~ ~ * ~ t h e ~ o f . . kemmmd rm&d. ~ ~ c ~ , remncwing !he biWra 6um the mmth fw 6 to 8 hours a day, pib&y during perms of deep, allows Ifem- W a t i u n ~ inmiwe andthe signs &Mamma- d m , P P t e n ~ i u t b e s ~ ~ ~ w b n d m t u r e s m ~ t o b c ~ c a l l y ~ .
af the S u p p d n g Structure Wm &qgw&otl of the bone that prwides the &ippwt J$r &a m i d h y denture varies cmdder- ddy with & p&mL F a c h that iaflwm the tb~mdslizeoftbe sup- bone include (1) its o@W s k 8Pd wd&noy; (2) the pmn$ gat- &he&@ ( 3 ~ ~ d e m 1 ~ b y t b e ~ 6 i q g m m , (4) d@ 4 I d o n of phdmtal disease ( ~ f r e q u o n t ~ ~ f , f l ~ ;
- (3) ibms awuing from the w&g of dental I ; (6) aurgay at the t h e of md of the . d (7) the relative length of time different i pwts of th jaws h e ken edentulous. In addition, 1: a namber of aubmical features influence the
dwpe of th W palate d midual ridge. These ~ d l m x i k d i n t h e f o l l ~ m a ~ d .
b d d ~ F a r a m This is located b e n d the in&h p@la, Mch is d m on a line h e . - ~ b d h d d ~ t h e o 6 1 1 t r a l i n c i s o r s . I ~ b ~ t ~ t h e ~ t ~ f t h e r ~ d g e a s f ~ o n @qrm&s {see Rgm 13-2). Thnrs the location of ~ ~ ~ ~ s a n ~ d o n a s t o ~ ~ o f ~ & 3 t h % ~ ~ p f a c s e . T h e ~a~ m a d M o d w t i s d & ~ through h ~ ~ d ~ s h d b a t a k e n W t h d e n - # m e k E t o e r s * @ & a a & a
4WdUaw T~bwosHy Tb0 fgbmsiry region caa. ~ d g w a ~ I m ~ * & % ~ - i h y posterior teeth are retained after the nmdibular e r h have bem m&ed and not P e p h d , the max* t&h o v q t , bringing tila m e s s with thmn (F ire 13-31, These
sfeeam f s b r o u ~ b u t ~ b e h n y . LW excess h u e csm pmmt proper Imtim of
Flguw f 3-3 The efihrgd tubemiti space available and will compromise the and distal extension of the mandibular
the occlusal p h e d may M e r e with the d-, if it is not surgically removed.
Sharp, Spiny Processes Frequently, sharp, spiny pmmws MI the IILaxiuary tine bone8 (me Figure 13-1). These usuall no problems baawe they are soft tissue. Hmwer, in iadivid able reswption of the midud spines can irritate the soft tissue d the denture he, The posterior p ina o h have a sharp, spiny m t a a n may irrihb the coveting soft b s pressure fiom the denture.
Tams Falathus The torus palathus is rr ~ ~ e m e n t i h a t o c c w s i n t h e m i ~ e o roof of the mouth and is found in h u t 20% o gopdatittion ~~ 13-44). It is layer of mucow membrane tbat is tiaedbythedentnrebaeunlessarel This relief &auld conform ac of the tom b&cwse an e x t m h e arbitmy robs the &Wm ofput of its Bupport a m .
ANATOMY OF PERIPHERAL OR LIMITING STRUUURES The limiting structures of the upper dmture divided itmw three areas: (I ) the labial

be labial vestibule is divided kto a I& and right l r r b i l W ~ b y t h e ~ h u m , w h i c h i s a ~ 0 f ~ ~ ~ * ~ m e d i a n r i n e . H c o n ~ n o x a ~ l e m d ~ t b g $ C t i O f l o f ~ ~ ~ ~ ~ , ~ t ~ ~ y i n o i m ~ a n d ~ a s i t ~ t o i ~ ~ ~ e n t o n t h e l ~ side of tha ridgu. The Wid notch in the labid flange of 6 dentw must be jut wide ~ ~ ~ d $ e p e ~ ) * t o d o w t h e f k e n u m to pesa &mi@ it without mmipulstion of b lip mure 13-a - -
A twus palittlrms k covered ttl, a thin The mucous membrane lining the labial emham Mich is easily tmuma- v & h h bas a reWvely thin m w c a The submu-
c o s a t ~ b t h k k d ~ ~ ~ l ~ ~ a n t o u n t s o f l o o R e ~ l a r ~ r r n d ~ W ~ . T h e ~
m m 13-5 Correlation of anatomical landmark A, lntraoml drawing of the mwillaty &, I , labiat frenum; 1 labial restlbule; 3,. b u d fwurn; 4, huccat W*bute: 3, coronoid ' bulge; 5, residual afveolar ridge; 7, m d l bry aikm & hamular notch; 9, posterior Ijatatal w l won: 70, foveae pabtinae; IT, median psldne *he; 72, i n d v l ! gagilb; 13, qw. % M d I a v final imprtdon shews the ~~ denture fadmarkx f, labial W 4 Mlal b-; 3, hml wch; 4, buccal Ram 5, cornmid anbur; 4 akdar $mw p, am & t ~ , 8, w l l a r y seal in arm of hamukr twt& 4 ma of - *or Natal mf; 10, fmae plfim; 71, m d i palatine grwuae; 12, in* fo~sa;

216 Part t)mt Rehabilitation of the Edentulwr,Patient: Fabrication of Complete Denhrm
pwB lwrimndly through the Ups & anotsco- mix w&h the .films of the buccinator muscle. Bmmm&e f h run in a horizontal direction, i .tho ,orbWark oris has only an indirect effect on


218 Part Three Rehabilitation of the Eder~tuluus Patient: Fahr~rat io~l o l Curn~lete Dentures
- 3 3 4 4*WQP&e~isdmefoZtreMMWMduala~rridge ~ u s e ~ ? k ~ w r r t ~ ~ n o f f h ~ a l m 1 a r t i d g e . T h b n e i i t t h i n t y d by m u m s manbane ad m y relief of the denture bar& to ~~, B, Hamulaf W. C Hamuhr d the medial pWy@d @ate6
-PIX5 A I D OBJEtTlVES @ &@@%!ON MAKING
following concepts shonld be adhered to, tive of tbe selected technique:
the oral mactms. 4. A physiological type of border-=
procedure should be performed by the tist or by the patient under the @dm
&a. m m , w the dentist.


ZEO RH Tfrme RehsbHRation of the €dentubus Patient: Fabrimion of Cwnplctc I h m m
Hgum 13-10 A, The mrw'lbry tuhemity. 6, The ptetygomandlbular raphe, which is pulled forward when the mwth is opened wide. C, The retromolar pad of the mandible. The cheek lies to the right in this picture and the palate to the left
e to devise different
&ma dedsedto cWncmkmUed disphemm of , ander the d m . hpmsim tbat
. - thm wiL minimtun displacement are as is, whereas tbsu that a-
is, huwmr, no wideme to indicate that one . W h @ e p r d w s htkr lmg-km results b
The cbiw is ma& by the dent is^ on the oral conditiQm29, wwrept of the function
~ ~ ~ m d h g ths denture, and ability impression materiala.
em of the t y p of impmion being
impression-making procedure. If the a y is tm large, it will distort the tissues around the bo& of the impremion and will pull the soft tism 111lder the impression away from the bone, distor$i ing the dimensions of the sulcus in the process. If% is too d, the border tissue will cohp~e h a d onto the miW ridge. This too will distort tb acm& d g of the border extension of b denture and prevent the proper support of the lip& by the denture flange. A properly formed q enables the dentist to carry the impression maw to the mouth and co-1 it without distodng &E soft tissues hat md it. 1
Individual or custom trays have h r d m tk@ can be adjusted so they control the movable mfl ti% sues around the impression but do not distort At the same time, space is provided inside the Uq so that the shape of the tissues covering the d q ture-bearing area may be recorded with mmhd 04 selective disptaament, Because each mouth is diil ferent, thew cannot be achiwad stl$s


ZZ2 PPtt Thrre Rehabilitation of the Mentulous Patient: Fabrication of Complete Dentures
F@um I&II The stock tray must b of proper size and mwt be mmckly positioned in tke m a t h . A, T k patienf b asked ta open the mouth halfway, a d the tray k M d into the aawtth in the horizontal phne using the handle. B, The tray is centered by @timing tke &t nakh over the hbil fmurn. C, The handle of the tray is dropped downward to perma visual inspection of the posteriar extension across the palate and hamuhr notches.
~ h D . ~ f i ~ ~ ~ k ~ ~ h ~ ~ ~ o f t h e stdtmytomede a r h n ~ 3 A p ~ t h e ~ o f t b e ~ t o ~ ~ ~ . ~ ~ a ~ ~ d w p mts &@e bxdm fsmw ~fmn the ria of the
ofthe oray, wax i ~ ~ t 0 ~ ~ ~ f * ~ o r ~ d ~ ~ ~ ~ ~ < ~ ~ ~ ~ f ~ ~ i t l - * ~ a n , ~ ~ ~ o ~ ' p o u t a f i h € ? t m y i a & e ~ ~ t i ~ Aph, tke !x&wof&e t rayamobsavJ~~y ~ t a ~ ~ ~ ~ ~ ~ I%l3)..Tlre & m e is to OW a prellminsry
t t w r t i a s ~ t l y ~ d ~
trnpmsiofl Muking &fore making the preliminary impmssiw1 advisable to practice placing the tray in pa Thepatiat isasWtuopenthemwthhdfwa the tray is W m t m d b e l o w theupperre r i d g e . T h e u p p e r l $ r ~ e ~ ~ t t r e t r a y r i e d l q 4 w a r d & o P 1 y i n t o ~ w i t b ~ ~ r a n & a s o r ~ ~ W I t e a ~ locat& pmp& WWiQrIy, tb i n b f w p W i n t h e ~ m o l a r ~ o n o n & ~ t r a y , d w i t f i ~ p r e s ~ ~ ~ ~ u p w a r d ~ n ~ t h e W a X a ~ ~ s t h e ~ ( ~ ~ t b e t m y c e m e s ~ ~ t w i t h ~ t i ~ posterior seal ma The fhgem of om

the alginate h p s i o n The irpewraible hydro- to th3 nunu-%
the practice sussim (Figure t 3-13, B, C, and cethematerialh&,the&~ttndupper lifted away from the bdm of the impres- htduwairbeWeen the softtimatthe
t d n i q w h t f i e ~ ~ t t t l w t h ~ ~ f ~ s m k t t % r y ~ n O t ~ i w i t h ~ * ~ ~ t a o n e g d t o u s e a t t a y ~ f i x ~ ~ p o t i n d , ~ ~ o l n e L ~ f o r ~ ~ . R B b m W g o f * ~ W d * M a ismtm&&&n.Thetrayktoadadwirhthe imprwsibabammial&wWmthsmu&in ~ & ~ ~ ~ ~ f ~ d ~ ~ ~ = t e a
T h e r ~ o f f h e ~ t t s q r ~ ~ b e dgttrmined. %a choiceti are mailable. Either t$e pbripky is outlined with a diqmable indeli- b l e ~ o n t h e ~ a t t b ~ ( t b e p r e f d option), m the outline is somewhat arb- tmilymarkedonthepwredcast in . tbe~ry. The 00mpIeted knprwiion &odd b shewed next to the patient's mouth and the jumtion of the ertEach~d aad lmtwhed m n c d tiEwe v i s d y i ~ e d a n & a ~ o f & u ~ i o n (Figure 13-14). Tbe~ibpBltrPadinarti f icM~tone, and~m#mntmyout l inesbouIdnwbeevi~ o n ~ c a s t , T f t h e ~ e h a s n o t b e e n m a t k d o n t b ~ o n , i t e a n l m ~ ~ o n t h e m t , Howem, with the patient not p m d for n cornla- t i ~ ~ ~ f e a ~ ~ t h e c ~ m becomes an &Gated guess.
C l h i d a p e r i m has &own 4hat a large number of ademtulom pati8nts Souking mltment for new comp1W dentures ara a h @ wearing complete dentures, If these h e been worn sac- casfuUy for a mrmbex of pars and if the extension of.thebawissatisfactory,~llogic3uggeststhat thedentm~cstlbeuwdasestdqpointfor developing an acumk impression of the denture bfmingwaface.
As part of the protocol for restoring the health ofshesupp@thm,thedenhlrewillhavebeen relined with a thm conditioner. The result can be ~ l i s t h e ~ i m p r e e i o n a n d ~ ~ t o produce &the preliminary caat by pouring MI&I stme into the fittin6f surface of the dwtare. If ~ t s ~ o n t h e f i t t i n g ~ o f t h e d m h m (e.g., d the hkmsities), then artificial sbne &odd not be ukd. It w d d be impodbk to remove the den- from the cast witbut dams& either &el cast or, men worse, tb $13lttare.
' The undercuts can, of course, b removed before adding the tissue mditioner, but this mans that the fitting surface of the denture has- been

224 Part Thm Rehabilitation of the Edentulous Patknt: Fabrication of Complete Dentures
Flwm t**s r b A d ~ o f ' i ~ b l t ~ . f j : ~ w t k e ~ i ~ ~ e & + ' W ~ t h e ~ . W ' p r $ & f t ~ ~ e r B p i s d ~ d ~ $ ; r y ~ t l p w a l p l a a t e r i -
' e * M - w , w & * w i ~ + & % w i k ~ ~ b y * ~ ~ i n * ~ r X * f i n ~ ~ r ) , W h a . i ) l u l d i n p l s o w a h a R ~ ph& W the d p&k. h The wmpletPd irnpresrion.


ZZ6 Pan Thm Rehabilbtbn of the Edenh~hs Patient: Fabrication of Complete Dentures
A -*a 13-1 8 rC Relief wax covers the basal mt area except for the posterfor palatal seal area and the labial and bucal reflections. B, The custom tray should be 2 to 3 mm thie and the handle shaped so that it does not interfere with the position of tlre upper lip
Mgwe 'C346 The curtom tray mrs the entire .bassi se& area The wax spaEer has heen kit inside the ,bay to allow the tray to ibe properly positioned in the muth during border molding.
~zpoldable impression materid that is properly ~ d ~ l l E d b y t h e ~ . T h e a m o l m t o f sbprL8upplied by themya@b a m t offaPce
' ; I ~ ~ t h e t i s e n e s * am%d@to the &- Gr vi&ty ofthe o don^.
For border moldding to be &ed ont ~ u a s 5 IWy, space must Be created for the border molding mimid Therefore the flanges of the catom b y ~ b ~ ~ u n t i l t h e y a r e 2 m m s b o r t o f t h e &&&m Once the buccal and labial W g m of the ai&m tray have been adjwted, the posterior pWl ia dmked. The my must contain b&& bmdar w h m md extexld approximately P m m ~ t o t b e v i ~ l i n e . T h e v i h t i n g
line ibl o b s e d in the mouth as the patient rays P a d a o f ehortUahs."Thepohm bo*d* impression ttay is marked with a diqmsable W bte mar?m, tbe ~~~ ape dried quickly, w tray i s P h d i n t k mouth, andthepatient i s 4 ~ ~ 4 4 a h ~ T h e t t r r y L m o v c d ~ t k ~ andthemkthathasbcentransfdhrn?hets@ tothemouth is caqardwi tbtbe wTbratingbd and the hamdm notch%. Tf it is undammded, &8 length is corrected by the addition of modeiiq wII1POUI1C1. 1
The tray ia n w ready for border molding, dm ing which the borders of the tray are molded to a form that wilI be in harmony with the physiologid cd ation of the biting anatomicd smctum! This may be carried out in sections eitfier re one part of the border at a t h e or recording puts of the border &ndtanmwly.
"""gm Recordurg dl of the border simultaneously Isaa!
two general admtagm: fm the number of k tions of the tray h educed to one, a d sec4
;' developing all bodera simuhmusly &"o& pmp 4 agation of mrs cawed by a mistake in one d
' ? affecting the border contours in mother. Therequimnentaofamterialtobewd&
sim~ltanm molding of ~II h r h olre w 4 should (1) h e d ~ c i e n t body b dm it kl remain in p i t i o n on the borders dwhg lmdqg J the my, (2) d1ow some preshaprng of the fm of the bodem without adhering to the f w (3) have a setting time of 3 to 5 minutes, (4) adqua& flow whilethetrq£swtedinthemad&

HgmwIrnP h p a t y e w t m d b ~ a c ~ o s ~ t h e ~ ~ ~ ~ a s r d ~ arwnd the d r e Wgr d;&e tray.

228 h H Tbrac RebaWfiCith of the Edentulous BtietR Fabrication of cornptete t e r n
A iigura 13-18 A, Border molding in the anterior region is achieved by moving the lip outward, downward, and inward. 6, The left buccal Range is molded by moving the cheek outward, downward, inward, and then backward and forward to simulate movement of the frenun.
i F>< ' G
be pmumed that the tray already reflects tbe bor- tissues wil l help the dentist &ermine whetlm det mo1& developed with the tissue conditioner additional segmental border molding is requid ebat has been med to reline the denhue. Thus fur- Patients are able to wear complete dentures with
bank molding is very Wly unnecessary. apparent success even though the bases are n@ T~I ~B is a k d n g that the prmow denture base extended correctly. Accepting an incorn& b wm&y eatended and that care has been extended base just because the denture baa becaa taken wi& the thme conditioner to obtain the cor- worn previously is nat good practice d excIudtg W border ahape. A careful scrutiny of the tray's the possibility of providing something better. p iphey in the mouth whiIe mwing the peripheral
Preparing the Tray to Secure the Final impression Space must now be created for the final impressicill material; d e m i s e , the borders will be wmw tended and the mucous membrane displaced unnecessarily.
has flawed over it. Any
raer molding has been com- pi&&, Muding the posterior palatal seal area. The RIM wax is stlll in the impression tray.
u 1 1


230 pprt 'fhrrc Rehabilitation of the Mentulous Patient: fabrication of Complete Dentures
I I
G F@we 13-20 & W n g w;rx has h n attached just below the border5 of the final impraton. B, The vertical wall of the boxins is securely attached to the boxing strip, The height of the wall wiil allow the base of the cast to be from 10 to 15 mm thick. C, fhe cast provides an accurate positive record of the basal seat and reflections. The thickness and form of the cast permit easy adaptation of the materials used in making the occlusion rims.
1. lhmeabe~mafthe~mmq* a Uphim the present d&mw with tissue
m m e m d m l t r s a t ~ ~ . b. B t w m a p t h e * b l e f t v u h ~
o u t ~ ~ m ~ k . c. hutmet th& patient in oral md denture
h&mmtdm-the-balring tismw.
d -w==wpPeprostheticw.
2. Malcrt p r e b h y impmim. a. Use a stock tray, m d h d with wax m
th i border, and irreversible h y b d i m m i m material.
b Use a stock bay with impression a pound ~~ or silicone putty b p r e ~ mamid.
c. On the impression% border, id&@ periphd & of the p r o p o d cI3sa tray.Thh willconformto aline- attached and umthched muww membrt Maksahbmmrystonecast,
diftlmdmturehasbeenoptimi2led,tht ftmctimdybordermuldedwitha~c ditioner, reregard it as the preknmq imp sion. Make a hhratory cast in stme aegne p w .

6. M a s w cast W o a EL Box and pour the f d impmion. b ~ t h e c w L
Bifelfo$rop&y x
lad K: A -ME Gomgariaon of pala$]. ~~ bafom d sfm w&ng bmploto dRamms, J Pms&et Deut 36:25+264,1976.
h m y W R , U o m k J B : T b c ~ ~ : i t 8 ~ relief and w r palatal a, J Am Dwrt W 75:1182-1187,1967.
t y o m m ~ o f ~ f b w e ~ f n e o m p k ~ hrre J h W h t 33:S[)rlU)7, 1975.
~ A L ~ a p p ~ O f ~ p f ~ ~ ~ v = h - @ c o m p l - - e dmh, JPma& k t 13:433,IW,
W a m n l I 3 , ~ d m O r a l ~ a n d ~ b m p k s t e f h iwas, J B w h f parJ 47: 133-140,1982.
Wa- IB, MacDmdd W: WoDai variatha ie kb a e l a t r j ~ B f d ~ W ~ ~ ~ r n t 50.%53-859,1983.

. ,
- -. m .- ,I ,. >,,, ~I,:,..;;I L:,:!# I,.. .,I tlA1.d . , . *k:,.
Devek "ng an A - ' - -ue/Substitute for the ~ h d i b u l a r entire- ear in^ . . Area . . ,
, ! . ' .#. . , David M. Davis -
L ( ' ; - 1 , .-I, . .<
{*- + ' I '
' 8 :. , - ' . . - -. , . I . -
, . . . ,.=
1 -
~r& of the ~ U Q I Ridge ' I

at the time the teeth were remod,
Shw of the Sup@rting Structure The ~)nfigmtion of support for a maadibul


Chptm t4 Dewdoping an AnalogudWstitute for the Mandibular DentumWng A m a 5

of lhe ridge. Ehwa, with moqtiotl, ttae gm1l b h c i t s h c m e incremingly prominent (see s of the denillre. Bgw 14-51.
W- T h e . t o r a s ~ a r i s i s a
d mead pmmhm midway *Is& tissm of * noor of the mutH bbifl, v&jh!C a t a k E * ~ o t f h w k ~ s , h E t m wkm m n s i d d d e m s m p h has t%lren The labial M b u I e runs h m the labial
with thew d m s i d d ridge (Figwe 14-5). length and thickness of the labid flange T b tom & a W b h b is covered by an extremely the amount of titme that has been lost. ~ ~ a f f ~ ~ ~ b m e . I t a f t e n ~ t o o f t h e ~ ~ i n t h i s a r e a o f i m
mqhdly ham it can be W~dt to because of the muscles that are k e & d c
kalriag &e border 4 darly ~tctive muscle i n t b region. Th flangewinhd-tr)rhtum
I W i Y OF PERiPHEElAL OR w fa14 , Q C ~ is the liba af a L tlMtT1?& srRUCTURSS to thelip. 1 1 T h e m a n d i b ~ ~ ~ n u m

If,.' 7.1 &id
1 : . ,
P J - I FIgwo l+7 Cormlation of anatomial land- A, Inhod drawing of th
mmdiby4r arch; 7,Md fmum; & M&tl sw!bute; a &tmt kenurn; $ h-l Wbuk !$ r&uai a b l a r ridge; b u d sh&, 7pret10mobr &; $ ~ m d i b i a r raghe; $,, ~~~4 m; $0, bnm,ll, ~ I o l l n @ a l sufcus; lZt tima! b p m ; 13, r q k n 'admmy$+yqid wnlnetm. B, EdaMbular Rnal M n Wng the mWpmdFng ' " ' h u e h m : 1, hbEd tpotcR; 2j labial flangq3, bum1 tpotth; 4, bucrarl &gq 5 , a h r m $ , ~ ! f I a ~ , ~ a ~ \ f e ~ ~ t h e b u ~ l s h e ~ ? , remmiarp& >&mmibUknatch;%itngu$l t langewith-nln~o-m::~ i n c h d mfgt.the tatgut; I?, -1 T4 Iingual'mW~: P3, pm@oRyoU e m h a . W ~ - w d ~ ' w r w w ~ m w , )


T h g ~ ~ o f f h e ~ ~ i l l l ? & w b y * . ~ d h ~ ~ b y t $ e ~ * ~ ~ a t i a t ~ ~ ~ t r a s a r l S W & & * > W * < ~ W * P W ~ wd**--,Bnd$t& ~ o P ~ . ~ ~ ~ a f ~ r c # m o l m o l a r m W h M b y a m g P , * b W m I M m ~ * ~ * ~ . V h ~ r n e Q d e g l a s ~ W ~
m a a i o i e . ' W a ~ e d h t d ~ i e a t i g h t I y k t h e ~ o f ~ ~ ~ a n d i n c ~ t l l e p ? w h p e d ~ & ~ M ~ a soft tima b m k d Pigam 14-9).
T l t a e ~ k p t a Q i s ~ ~ ~ ~ f t p d d ~ @ t * W s e d c r f ~ ~ ~ ~ . ~ m ~ is-ofa*-epith- e m 8 i n ~ t o ~ ~ ~ ~ ~ cantadns g W a r h, fibm of fhe b u d tor and &or d c t o r mwIes, the -0- l k U t w b u l a r . @ e , d t h e t a m i n a l ~ ~ f ~ k m h of the @mpab muscle. The action of ~ ~ e ~ Z i m i t s ~ e ~ o f t b ~ d p m ~ t s p l a e t m e n t d e x ~ p x e ~ oatbedistal p a r t O f ~ ~ I r r r p a d ~ ~ ~ f l p r 0 - ~ . ~ a f ~ t h e d & x m ~ ~ d ~ ~ ~ 0 n a h a l f t Q t w p ~ o v e p the relmmih pad.

-34-9 The mandibular denture.
'ointh1)s~fromthemy10byoid~l~d m ~ ~ o 1 p a n d w d o a m t ~ t h e : b i t i d e , ~ ~ w l y ~ ~ u e t o €he~in~r&mex~ept irtdi tcct ly .
gum 14-10). Themutole lies deep H m v e r , t h e ~ o r p a r t o f b l q ~ a d o t Z m e r ~ i n ~ m u s c b i n t b m h r m g i m ~ t h e l ~
tu F$- 14-10 M&omh& of the mylohyaid rnuwlc in various regions. The letters with ~ r n e stgrrs denote c& sedans of the dsi- arms. A, €mine Man. 8, Premolar
I region. t, First molar, Q, Third mI2tr. At Wnt D, n d a that mylohyoid ridge approaches .. the k d &theahmlar crest. The angle of the p t e h r U n g d flange in the molar region is r A h ~ b y f t d s m u s d e ; & k ~ , o n l y ~ ~ p f t h e f l a n g s i s ~ .


Fimre 1411 Diagmm shows ttre relationship of the medial wrygoid muscle to the wperior constrictor mu&. 8, Buccinator muxle; M, mameter muscle; MF: medial pterygoid musde; Plt, ptetysornandibular raphe; RM, ramus of the mandible; RMC, posterolate
superior constriaor mude W. T portion of the retromylahyaid curtain formed by the mumus membrane w r i n g the
Figure 1412 The lingual side of the mandible shows the positions of the sublingua[ gland relative to the mylohyoid muscle, at r& (4) and when contracted (8). The mylohoid ridge is denoted by C.


FDprm 3 4 4 3 Prtdimjna~ tmgrwb mak'ing.,& A W r my O placed in the mouth by a t d o n of one corm of the mouth wlfh the index finger, The side of the tray is placed in the w e corner imd the tray is rotated into positton. &, The tray is raised anWorIy far observation of whether thereere la adequate space b&wn the lingual flanges [B* a d the. ti@ sl' the Wual ridge'h aommrnodake d k i w t t bufFd i m w m material.
confines the impfedon material In the tray. Note the Hngua l shape of the tray to a w m r d a t e the &ion of the mylohyaid musdes and to fit into the retromytohyoid fossae.


anteriw handk shaped to avoid interfering with the lower lip and ttre tw finger rests in the molar won.

1
t h i s , ~ ~ ~ ~ g e t ~ e ~ e m t o ~ a " l r s c w a d ~ t h i s ~ ~ ~ 0 -
iwllmgw-d-the@*- @id mtwle, Gd a&% wbi& dm the floor of efae H W - - W u p m t h e
insi&of*Iplguarld-kW&it t t w t b e m m & m , i t w t r a h m k w i t h t h e a & m d t b ~ ~ ~ l e . i t i s ~ t o h e m ~ ~ ~ * t o o m w h d o p t o w d t b ~ i n ~ ~ I'
region tban with tao little lxmme SfPe f l m h p m i a ~ ~ f i t l b ~



@&-
SUMMARY

f f i l s f t l q ~ ~ f l f ~ ~ ~ ~ ~ & e ~ ~ ~ ~ i # ~ WhmPhY
~ ~ ~ ~ ~ s o f ~ ~ ~ ~ a a B ~ S G , . ~ ~ H R : ~ o f W ~ ~ ~ ~ ~ ~ * , * ~ C ~ ~
1 b-a t M q " @ ** B* Jmt&nCI2:835-M7,1%% I w q a m d w a o a e - ~ ~ M q u e ~ t b n
mhbermaterisrl. ~ a a d ~ ~ t p ~ ~ ~ ~ I f ~ t r a y h B a s ~ e d o n a a s t . donth, J h a k t M t3&33,1%3.
~ f r m t b e ~ p r e v i o u s ~ , F % b k m k i Z , ~ h k . ~ l a r ~ ~ g o ~ tooth a&wtb, J R w & M 17QlP7,1%7.
h m d d I n g m a ~ d h n - o r S e h ~ ~ . f . t , ~ ~ ~ ~ ~ k d m i ? q u w ~ ~ ~ h U r ~ B . &Pem J L44:31%314,1938.
& final impmion d& the p r e f d Shsnaon St: Tbe @Is d e in mIatia ta sdenhrlws ~ s s i o n ~ ~ ~~, JPros~h den^ 37:4774#, 1972.


Chapter 15 Idemifitation of Shape and Location of Arch Forln
E Figure15-1 ~mplefeden~havethreesurfacesthatmusthwmonizewithaheod biologist environment A, The dentures' polished surfaces are xl contoured as to support and contact the cheek lip, and tongue. Band C, The impreion w b a d s u W are fitted to the bal seats D and E, The ocdusal surfaces of one denture must fit those 01 the opposing denture.


I . dusPcd with talcum powder as a separating medium. $ Ten-puge reinfmement wire k ! ada~tottle~~rp~Iamto.extend~m~thehmuIarnatshes,Pmu3ia~ I o f h M n e i i n e . C a n B B , A s h r n d ~ ~ w m ! i s p d ~ ~ W 1 & ~ S o n m t h e r e ~ o d i n g h ~ ~ ~ l o f ~ ~ i s ~ l e d b S k i s h d Y m.twml to the desired arch form, The rim $ W t t~ a h-t dQWy gmter.than#e W
length of the teeth and the amount of Mdual alveotar ridge s h r i n e .


Figure 1 S-B Wax template technique for making a trial denture base PDB). A, Master casts prepared by waxing out the undercuts and applying a separating rfiedium. B, Wax templates are farmed and lined with autopolymeriring acrylic resin {C and 0). E, The completed (well-fitting and stable) trial baw is ready for the addition of ocdusion rims.

a d p l y m e r a r e ~ ~ @ ~ & y t h i c ) c ~ i 6 d ~ . ~ h e b a s e M a M 1 cast IW are dared mhm&Mm. E'Phr denture base Is
?!?,, ,d , I
dimmion of &bIun m), and (43 make a preliminary d c relation (CR) record.
Arrk FQrm 3oh t h e ~ o f t h e occluding s&aws and the matour' sf the wh form of the o~~lwiun & should tw ~~ ~~ for each patient



i n6 are frequently 61 mrn anterior to incisive papilla ('dotted circle), B, On st, the papilla is cirdd because it' guidi to position tng the maxillary
~ r i m t o ~ t h e ~ ~ ~ ~ W ~ ~ o t l ~ ~ ~ ~ -
~ 1 8 W w t p p o r t p M & ~ m ~ c ] 2 a e l r ~ & m u c h a & l t @ ~ ~ t h e ~ ~ ~ ~ e ~ ~ ~ the pwyg~m&ndiwar mpb a d the luo&h nnuwh. I t m u s t b e ~ ~ t h a t t h e ~ t h o piodofedentulism,the grater will betheWaf the m s ~ I 6 tone, Comqumtly, the re1- of b h e ~ r n u s c l e ~ a a d r e c w e t y o f ~ L likely to be insufflcieat even if the best den^ m ptwIded. The more wurak the position of teeth repkemntaadthesoonait occurs, thetw&wiIl b e t h e ~ o f r e l ~ ~ g a n d ~ ~ - = d l i p w
A n & d m m g e d u e i s a n ~ m ~ b d t w e e n t h e ~ ~ o f t h e ~ ~ infheregionsof themaxi l lmuywnd~bp- ~ ~ A # m m f i g u r e i s a g & p l e r c e t o ~ t s r t , w i t h a n ~ m t g e ~ t o ~ 2 0 m m f b r ~ ~ ~ r i m , ~ ~ ~ ~ n o t ~ ~ ~ a W ~ e d d e p e o B i r m g a a ~ c a l ~ o f the pwticutar Mat btirmg treated (Fim 15-10).
-1- l X @ m M w s k i n d m @ s ~ virtual Mwmn Le nwlabilalW anci the mrner af the mouth.

262 Part Three Rehabilitation of the Edentulous Patient: Fabrication of Conil)letr Denlurrs
I S l O Two ocdusion rim haw k e n tmtaured and adjusted and are n w ready to k used for making ?he @minary mtric rrlatlon record. The tfimm J md contoud wax rim sem as ill) analogue fwthe mouth's n m l zonee They m be used to
tan Pi the prosthetic teeth.
lwei of ihe tAeIumI Plane h h y d m t h b u s e a ~ ~ ~ t h e smthg pint for eshbhhing the o c c W plane is the mat- i h y acclwiun rira The peduru entails shaping ihe occlusion rim so the incis4 p h e is parallel to ih kteqnp11lary line aid is at s height that dlws f 0 r ~ ~ Q f t h c m ~ ~ p h I s ~ a m c 3 m r t ~ ~ ~ - d x e k t b s t s ~ ~ ~ f i p csndmIsaguubifitisofavemgeTqgthTb d W * p w e r i * , k & t 6 ~ t b e . ~ ~ b o n ~ W s d h ~ o f * m w t nahral dW p h s (Figure 15-11). TIM& the m e r k m l * & b ~ b M ~ d & ~ u p p W r l m ~ ~ n n t i f & f c i e n t ~ - ~ ~ l m a e h ~ . r n r i ~
dea$uresh It wmhdy cmmt b qg&d as qplicabie ta dl pdenta, however.
are o h approach to meld p h e ~ ~ 1 m ~ d m e t h o d ~ ~ f j r s t a e e k to ~eooncile tongue function and its relatimi to the
taped on. The ocdusal plane is &ahfished when wax wduslon rim is made parallel to this 1 planeguide or similar device may be used patallding.
o c c 1 d plane 2tnB mandibular W h n t H s ~ h i s m W t o
0 ~ d e o a r ~ ~ , ~ ~ * ~ dl%& m w W ~ Q ~ L S f%&

~ . a a d W : ~ ~ p r o p e r l ~ ~ I i p ~ in-dkem* rims. Farher- * *
, ,sf
1. -$d$awat ofthe ~ l ' ~ mppmt 2 ~ , ~ m oftlwqlwe -:* -
, k m i m t h e j aw are at- J . M ~ t s b e t w e e a c J O t s 0 4 * ~

1
r owlusion dm W is trimmed to conform to two pairs of mprs of the mouth (B and Cj and a point two thirds of the


wibmd -k and place the d b u - hrocc1whiimin~mdh.
3. T b c o m f w W y M r t a d r r g r i g h t p ~ h a s b o r h e s h o l d s ~ b y a s u i ~ @ lwudmt The btht guides t#e patiat's mmilible into a CR position. Stabilize the r i l d b u h trial base with the foreikger ~ t b ~ o f o n e ~ a n d a a e t h e t h t r m b d F ~ o f t h e ~ h a n d t o g u i c l e t h e m d W e . The f- stabking the base &caabemcwedupwardtost&ilhth~ m d k y base, if& In this mmrm, the bases' stability is ensured, and the m d i i l e rn be guided M e visibility k mhbd. Altcmative band poshmi are t by twermt c l i t l i a .
a T h e ~ t t a d ~ m a s t b ~ t i m m o - b * w h i l e t h e : ~ i s ~ , T h i s m n u q ' simply not b possible for some patients, ape&& where nmd ihhr reskhul ridge lBlmptim is extemitre or n m - l u WiW is compKIlniaed CWly, implant- &hid wbiw r i m d m &is problem quhatsily, T I r e ~ s f a ~ ~ - ~ ~ l ~ t n l i ~ i n ~ ~ t h e ~ r t o $ a i d e ~ b ~ o p d n g a n d c ~ s w e i n t a ~ ~ ~ t o v e r i f y d l e r e c o r d ' s ~ .
B h ~ t o m h ~ t h e p r e v i ~ 1 y d e ~ b e d llrraneawetrr b e f b afte m h g medium is m t d y hlmhwd The iid bases should be tab out of t & ~ ~ r e c o * g m a t & l r e m o v l e d , a a d t h e ~ a n m o f t h e b ~ c h e c k e d t o ~ u t e t h a t thy do not co?ltact distally. This is a fmyent site ~ ~ g ~ T h e accuracy ofthis record M d b checked and r e c h h d be* pmcd- hqg to @n Wimlator mounting. The ofkqumt trid c-, p h a practical d &cutousIy a@kd twhique, will yield am- MU. Any ~ I c b d a x o r t e s f s t b a t ~ a n ~ C R ~ ~ ~ m d m d h ~ W q u o for thtp pugme is the use of c d o c m i a t s .
Tnfhqumtly, the pre- CR m r d is an iacorrect one and undiagnused at this appointment. It will, h m r , became apparent at the try-in a p p b ~ w h anewrecordstndremouut will hmtobeatade,TWis ahe-cmiumingstep and should hqddly not be r e q u i d However, it must
be recalled that clinical detamhation of o &@m is more d immibe with prc ~ i n p l a c e t h m w i t b ~ w c l ~ i o n r i n probtem can bt d f i e d , dtrlwgh addhiom ~ & w n d l a ~ t w y t i m e i s ~
SUMMARY 1. Ensure mli-fitting, retained, and &able Tbe mtdm may haye to be aid& dentam adhesive. The stability will be en a f k &sign of the arch form, or n d :
2. Establish the neutral mnd by consid& fallowing: i~ Arch fum' lation in @ous dent
P-I b. A n ~ t o f t h e a m o u n t a a d p a l
bone loss c. Use of anatomical landmarks d. Fre- esthetic evaluation
3. Determine the height of the occlusal p the mandibular occlusion rim a. Use corners of the mouth as the a
l a a . m b. Use the retromohr pads (two liidi
the pastmior lemdmarb c. Join all faur points with a hot, bm
spas 4. Establish L a MO by modifying the he
the d m i a n rim while ensuring the foil a AnmmmeethgafbothrimsinCRp h An i akmce ld distance that the
judges as being W o n a l l y adequate patient in qw&w
5. Prepare rims for a CR regisIration with in tho maxillaty wax and opposing box- arem ts in6 mandibular wax
6. Return the occlusion rim to the moi repred trial cloms. The CR rprd i with the dentid's seImted medium T record is c&med and remade, if req until a repatable CR record is establish


Biological and Clinical Considerations in Making Jaw Relation Records and Transferring Records from the Patient to the Articulator lames D. Anderson
~ ~ t o ~ d e ~ c o m p k ~ h r ~ l u f i t ~ F 0 r
REGUMTION OF MAMPIBUUR
pmwed M a t l m W m Q v 6 m ~ -~~~~~

~ n ~ ~ W s r e m c u n t a c t a n d r m W u - k m x e m ~ ~ ~ t h e ~ ~ 1 1 0 f t h e m a v e
&t b camrollod by the neuromusculsr system ~ ~ d ~ P h e ~ ~ f ~ ~ c o n d ~ h ~ t h c ~ g i n i l ~ o f t h e ~ ~
~ m n u t i n c o n p a c t t l n d the &c th of
~ b i o n , w h e n ~ ~ ~ ~ ~ w i t h ~ ~ ~ d ~ ~ ~ k ~ t h s i n e w p ~ a f t h e k # $ l s h o x t 6 d ~ w e t ~ ~ ~ ~ a o d p o t d i m @ ~ i d * ~ 0 f ~ ~ E a r ~ ~ r m d ~ ~ B a i ~ ~ ~ . , R w m d l b * t f P r m a , ~ k ~ b l h i @ d n o t s o 2 e & ~ t h w ~ O p t h e t m ~ d s o b y ~ o o n w t # a f ~ ~ ~ m i n ~ l a r ~ t h a v e ~ ~ 0 ~ ~ oomitantly as &&dive o d d ccmh$ or s & q ~ g u i d a t m f r o n r ~ g ~ ~ the patbay of mndbhr mmaami. Thus I& i n c l i n ~ p ~ d ~ ~ ~ b e m * t i d ~ t h q w i l I ~ m ~ * ~ ~ famm that regdate jaw raotion. A failwe to h e l o p this k i d d ooclaim can dhtd OEPa b i l i Q 0 f ~ l e b ~ a n d ~ ~ ~ t o ~ m ~ ~ ~ s o f t h e ~ ~ *
S e v d dentists h o b d W patients a d ~ ~ t t8 c o m p b dmmm by midiag e c a m i c t s o t b - w - & e d b y m o n ' b o t h . ~ ~ & ~ ~ b i m s 4 ~ r ~ ~ ~ ~ ~ * * * & ~ ~ I ~ f t m r e q r * ~ * ~ @ a p p e a r i o ~ ~ w i # h ~ ~ h ~ a b h i e n c e o f a ~ ~ ~ o u l ~ ~ h n g e , I ~ d ~ - i a W - - S i o b , ~ ~ ~ ~ ~ i a ~ ~ w i ~ a ~ ~ ~ ~ ~ ~ a

- . ..
Figure 181 Mandibular hrder movements in the sagittal plane. The mandibular pasition in centric occlusion (COj is depicted in I, and centric relation or the most retruded $wMpn (81 in 2. Rotation, the tery inal hInge movement (3) tilh piace between B and t, from which fk tmaslation phase of the posterior opening occurs to D, the maximum o@hEt& w o n 0, The most protrusive closure from D ends in E, maxtmurn protrusion .with mth atat ts , 5. The postural d position (BRJ and the IwMual dosure (H) are I d H inside the $orders. (Wmwn from Mohl ND, hrb WI, Cwlss&n GE Hal. editors: A
rlf &don, Carol Stmrn, iL,1988, Quinmnce P ~ b l i ~ n g . ]
another. The activity and interaction of the mi for shes of jaw movemeats have been extensively by marchem with electromyog (ETMG). Xn c W p m t k h-, 4 pation and o b d m of the mwement p d y are enough for d u a t i o n of the mu involvement in jaw Motion.
Mux~rlmr Imkmnd in law Motion Neuromuscular Rqgulotion of Mandibda
T i t e m ~ % f ; l e s ~ i b l e k m a ~ l & ~ ~ ~ lWotion ~ y s h c w h d a c t M y d u r i n g a y j a w
T b s ~ i n & & y m y b e m i - M a s t i ~ n i s a p r o t g 3 d e v e n t z e s i ~ aid V&#I wmmunt of k mtudible, f d o n on a "chwKing csnter" located within the brain g k n ~ o r ~ m m m ~ t ~ U ( p ~ i n t h e ~ f o m a t i m o f t b be mmth and d t e d h m one positim to (Figure 16-2). The cyclic natrrre of d r

~ ~ ~ o ~ o f d o r ~ ~ e ~
Centnl h r s l Pwtl*xn
t&&!G&ry M W Momwm J
*
Z The masticatory muscle motoneumns
s jmmL%-w&* I d G#n pmdwE ~f~ ~ v o m w y m ~ ~ & m ~ g t g . & ~ - ~ ~ ~ ! 1
c # H b o d y o f l h e ~ ~ ~ b e ~~~~~~ - ."I (H&Wb 16-31, h m tk l m ~ , ~ ~ ~ ~ ~ ' ~ ~ ~ 0 ~ , ~ 1 ~ ~ ~ ~ ~ a -
the ~ i o 1 ~ m& p d i ~ f l of th mble-
Figure 16-3 Tracing of mandibular rnowments in the saggital plane. Far further explanation see Figure 16-1.

272 mme hhahitbtion d the ~dentulws Patient: Fahimtion of Camplett Dmtura
wba st&bd h e p l a h am us& to suppart ~ a p u w h g e ~ b u t i n v & e ~ ~ ~ d e v i s a . E n v e I o p m i o f t a r m w ~ a n d ~ m w m t mtim (mdmum twxder r n o v ~ ) in the sagrttaldbtdphmmasecribadbyachnhtu R Q ~ ~ ~ ~ ~ ~ ~ ~ ~ m ~ J n F i g w a 164 165.The dotted line mpwnts the M a a t m y cyck. 'Illis The mst wition (or phS'&k@d rest, ~ ~ ~ ~ a * o * a d ~ o f d d f m ~ o n , m ~ ~ p o s i t i o n o f t l t b ~ u m ~ ~ . h % t i ~ i s v e r y k ~ ~ b y ~ l ~ d & ~
I,. .?.
Hmam 164 Wdqe d d m Wndibular border movement a m ) in the sagittal . pkne, QmMc &a&%% tent& relation; MHO, m i m u m hinmpening position; MQ W1of- W g Q T tha jbm; P, most protrudd position of the mandible wiPh the teeth in contact; Rat, -I rat position.




Hgwb lg8 PrmpwWv M d y md& mounted to mmsure estimates or me, shape, m ~ a ~ ~ s f ~ .
-- krcisk Papiria to Wndibrtk fn&a The
i & i w $ l a p a k a h & & e ~ w c ~ e s
' ~ & f ~ ~ ~ ~ f ~ s a ~ o b l - -'-
c e n ~ ~ ~ ~ ~ d 6 r n m ~ l m ,
* '
,

Hgum 18-1 0 Sectioned casts, wwiar view. A, When the teeth ark in centric occlusion. the inch1 edges of the rnandibubr ceMml inkisom are on awapDe 4 mm Fnrm the incisive papilia. 8, Sagittal view of the central iticisors; the vertical overlap is abwt 2 mm.

Figure 1641 The cmt of the lower residual ridge will be approximately parallel to the crest of the upper ridge when the jaw are positioned at the vertical dimension of ocdusion. This relationship is regard4.a~ ideal for the stability of dentures.
at the rest position should be between 2 and 4 mrn when viewed at the premolar region The intemch space and rest position can be measured by means of indelible dots or adhesive tape on the face. If the difference is greater than 4 mm, the occlusal verti- cal dimension may be considered too small; if less than 2 mm, the dimension is probably too great. The occlusion rims are adjusted until the dentist is satisfied with the amount of ftemch space and until other requirements of an acceptable v d c d dimension have been obtained, such as patient c o d and phonetic md esthetic considemtiom (Figure 16-14). It is worth noting that the presence or absence of dmtrrres or occlusion r h i and the v d d dimension of these can affect the physio- logical rest position. The method w d for deter- mining the position (e.g., relaxdon, swallowing, or phonetics) also may modify its vertical 1-1 (see Figure 1 6- 14). Dentists must keep this in mind when using the rest position as a guide for estab- lishing vertical maxillomandibular relations:
capacity of the masticatory It should be combined with
Phonetics Phonetic tests of the verti sion include listening to s p c h sound and observing the mlatiwships of te speech. The production of ch, s, and j sow

qab.32 n is a common finding in d e n t u b pa$entsthardw mandibular rid@,-- bemmes progressively wider, and the maxillary ridge narrow, as bone rimpdon continuer, This is exemglifid in this edentulous skuit, I
c l a @ q # h e r * W h m ~ o ~ n m u r o f * u g a . ~ e . ~ i n h i e s l o $ r u o - t m d t 2 r e ~ @ u p p d ~ * ' ~ w e t a B mwmitriw-*w-d b ~ * ~ f k q ~ - t % m e &tmpm&rwpo-d*-of ~ ~ o f ~ d e n ~ . ~ ~ ~ ~ r c q , b ~ ~ k ~ ~ ~ Iyi.4~ aahd shwdum [Figure 1615& Jf&wBp m m p p f y ~ ~ y , t h r a $ ~ ~ b
b ~ ~ f ~ ~ ~ > & ~ ~ ~ a w m & v e l ~ f ~ b * m ~ ~ s a3 - ~~~.~ * m 2 z m s o m w m * ~ h : w ~ ~ ~ r t c r d , a m d , ~ ~ ~ ~ ~ O f t h s w W ~ ~ ~ t a r ~ ~ m c m t ~ ~ w * - d
~ ~ # b ~ ~ . ~ & a

ZSO Fart Thm ~ a b i i ~ of the Edentulws Went: Fabrlcath d oftompletc Dentures

Figure 1614 Change in postural face height with insertion (or removal) of dentures.
1-35 1 ne -mq MdusWvmrn k aWd b tSMa1 surface will k similar to ttta of the finished b e and the artificial tee&. Lateral @ and occlrrsal (Bj views show the c o r n md djtn#&m Of the neutral m, whkh haw been approximated in this oEdusion rim. m # a t gtCdpJes.are used tn antouring mandibular occlusi~l rims. (Fmm He& MR, BWm MM: The influem of pmstk is on mandibutar posture in edentulous patlentsi I PW&t i)crrt 51: 6152-Wd 1984.)
vertical hemian of occl~lod. The length Tmik S e e and P a t k n t - P e d d Comfort b h e t o c o m p l e t e t b i s a c ~ a d & r e f r i - T h e ~ f t & l e s m e c a n b e d a s t a g u i 6 f u r mftnessofthewaxcones willaffectthe t h e ~ w d t h e 0 4 ~ 1 ~ ~ ~ db. No comistenyy in tbe final v h e d p i - ion. Witb this metbod, m a d j d t 6 central l i n g d t h e ~ h a s b e e n f o u ~ d ~ t b i i r b e a r i n g s c r e w i a a ~ t o ~ o f t 3 1 e ~ o n hod. r h , a n d l a c m t m l ~ p h t e L ~ M b ~ &

H & & n l . e * l G ~ a f & t r w a c ~ ~ f o t h e mandibular base form an intmcdud -gs they are fopEed against the maPam ocdusion rim when the patient swaltows. Swallovring dmld Wish f he pmpx horimtal and wrtid dadm d fhe mmdik to the max?Wa& ,
o t b r m u m I81'F).Tfitmtrdbdqj i s ~ f ~ r n t t h ~ y r n ~ , r n ~ & p , t h s c m w i a r ~ ~ d a w & & e ~ ~ s t h a t t h e j a w s ~ a b o f a r . r n ~ h ~ i n h q ~ d t h e ~ t t ~ ~ r n fesrtwlm&The~atraaladjustsddow ~ M t n t b e ~ ~ t t u r s t h e I e n ahtt* .The4-at 'e& naOefyrmtif the h e a o f t b wnmfwls ca die to the patient The @1em with thh n ~ ~ t 8 e ~ ~ f h i g t I d o j e c t s ~ $ n d t h e ~ ~ , ~ m a I m ~ ~ ~ m t h e ~ o f t f i i s m R t i ~ ~ ~ i n * & ~ t o ~ ~ m l ~ i o n ~ ~ ~ d however, lmame them are both pltysi~logic m M w w b a -
I
~ a g ~e v-1 jaw &oms wtt~ Odusion Rims Nome of the ,methuds just used done, will yield an approp&b w



OF PATIENT RECORDS
ad@wtmenb m mpiw b-d

rim, The ear rods are over the markings on the skle of the face.
~ i t i s e a s y ~ ~ g e t b e ~ ~ -of- a b b o w to orientthe& to the ~ of h d e ( F m 16-21). It s h M b e ~ h m , h t t h e s e t h e r r r e t i - d ~ b t h e w e o f a f h w h m i g b n o t nwsady m e a Wer cinictil d result. &@k3 d0ne of b f e ~ S Y B ~ ~ C Eh&S made b ~ ~ ~ t o ~ m i n ~ ~ ~ t o ~ ~ ~ ~ ~ c e ~ hwen w "&'OBchnique iwof* hinge& baibfkaFaoebawWertOihearticulatord a ~ m ~ 4 ; u e ~ ~ ~ a n d w i t h a a
mormthg, S i m k c h i d d t s with b- ~ ~ b y t h e t w o t d m i q t e s w m f o d a t ~ ~ ~ I o n g - ~ d ~ . ~ * .
b1udi3d ckxl*' walwtion of occlu- = stability, retmhg, and edition ofthe
~ t h e ~ # f Y h e ~ ~ w i l ~ ~ ~ better diiial d for: W paxknt with d-


h d M t Tlne relatimahip of the mmdi'ble to the ~ r h i n g e a x i s i s g c h i e v e d i n d i r e c t l y b y ~ g t h e m 5 2 n d i b l e b h m a x i ~ h t h ~ - lwapatien~, tfiir~mwmhip it3 morddby means of a d l c reldm record tab bmmn the t3cchmbrims.
W i n g Centtic Relation registtation of centric relation is considered
diftimkanditistrueht iitmpzire1tminingand q d m w to $c:M &le d S . Tkm am ~ ~ ~ ~ e s t h t ~ f i m n a ~ o f c o o r - diWm of mdibuloa mscalm pycbIogicd ~ W ~ h e t o a p ~ o r ~ t w b ~ ~ u r ~ b w w e o f b ~ o f tb mmhg, and n w c h d d difficuldes that are
to mshW and sometimes poorly fitking base- ~ d w u y h g h m i h c y . h a d t , ~ c m i s k d y m p d & e c e n g i c r a W m m m b c€q.in%fct,beinm.
H # w m ,9622 The completed face bow m r d ready to k matched to the articulatar.
~ ~ d ~ D c M u r n
~ f b U o w i n g ~ c a a ~ ~ In r d d i q the mandible:
1. h t m C t t h e p a ~ b y ~ ' r n * relax, pulI it badq and ~1056 srowb, e a d y o n y m r W W m
- 6. T i h t h e ~ t B h e d b a c k ~ t f a e exerciw? jut listed are carrid out.
7. Palpate thetemporal andmasseter m to relax them.

Labummy Steps
Figure 1- The width between the articulator mndylar elements can be adjusted to fit the intercondylar width recorded on the W b o w .

D F&um 1- rCrRtc&WT rim, and cast, and u p p e v ~ r M W ~ f the Whip Mix
th 1-r~- to facilitate mukrritiw of th upper cast. The h fib #fcdurg.ka bweiiience ohly, S, With d e opper member
r a i d * $a&ter kdWhM mrt&/#p of the upper rrtR C, The' u r n member d the . aWcuWr has ken k k Info @tion, Hngingthe mounttry @M irYto the plaster.
D, Wlovntim d fhe upgw mt on the aitblmr m p l d . Notice the neat appearance of the pl&er that attaches the upwr ad to the mountiq r'mg,

C D FDgwr qa-25 A, o c d u h nms and lower rast are placed in gwition on the upper cast, whkh & atladred to the upper member d the artitlllator. B, The h r member of the alzicufator,is positioned ern the inwrted upper m e m k , leaving adequate space beewewr the mounting ring on the lower m e m k and the lower cast. C, With the 1- m e m k of the a1.ticuhr remoresf, plaster is distributed ovw h e surface of the h w a. h e r m m b , i s p i a d on the upper mm&. The condylar sphm must be firmly d In M condylar hudw, and the indd guide pin must be fmdymtd in the in&l W. The tower C k s t k ~ t o t h e ~ i n g r i n g o n t h e lowercftemberof~earticubrbythe p&w.


lm obtained a~mat~ ly , what lhe imtnmat As nsted earlier* it d d ba ~ ~ ~ t o ~ ~ ~ ~ t h a t ~ t o ~ ~ g m p h i c ~ g ~
ang oftbe masticatmy s y $ k m curve soft he^^^^


.A v - -
figure 16-28 The incisal guide table and lateral lates set perfectly Rat. 1
A?mary smlngs All arhwors eufPer h m $ ~ ~ ~ ~ a n d c a n M l I y ~ ~ ~ ~ ~ % i n t b pati~~masticatorysy- c--%%-
ogddag thdt the denture bww~.m.m
m-a L B - r

mwof&ia tqtb anaugment (and thus the choice dth a&gWm used) i a clinical ju-nt that & d d be made in advance, A more complex &trmhnt is thus wt aeeessdy a better choice,
-mmmPm
mudex wmlogy, d o n , Imd -1 ~ d ~ ~ ~ J ~ J ~ t & l O I : 3 1 & 6 . 3 3 1 .
a m s-C?& Ihhw aA: E* of wIl im and mid
,- J- 233-43, t 993. ~ ~ , P . H n C : R ~ r n o f ~ ~ M
maris, J h t k s t h t 68537- *1,r992
~ J P , ~ G C , ~ T W e t a k ~ Q a ~ ~ t m d b p m & m , J h d & ~ 67:493&, 1992.
lmmln la Jh#he?W64:64&


rig and Arranging Prosthetic awl Occlusion for the Edentulo
A l w h i g ~ a n d ~ g o f a n u m b e r o f p h y s - kd $dd bia- faczors duectly reW to the ~ o r m e ~ 8 0 ~ l y s e ~ a ~ c i a l ~ ~ ~ ~ m l w i o n . ~ g Q a i s f o r t h ~ o f ~ a r e t o c x r n s t r u c t c o m p 1 & d e n t u r e s
dowthepatienttopak b pleasing, and (4) will not
mwpmmto tmitnulae mh, and e d u m & bhm&tuid infomation so that tbe &tificial ad ~ ~ w i l l ~ h i n d i v i d u a t ~ o f t k the ~ ' P l a e d d i m ~ f ~ c i a l ~ i s a r e h - ~ ~ b ~ ~ ~ , ~ i t ~ ~ ~ t o f ~ ~ a n d c o n f f * ~ T b R s 3 e t l i a g o f ~ w 1 ~ t e e t h i n w a x ~ ~ ~ o f ~ h t s i o n h a ~ ~ * ~ ~ u s e ~ f ~ r e o c a d ~ d w G & w ~ o f ~ L . ~ ~ h e 9 p m i t ~ ~ t o ~ t k . t a o t h ~ e n t o r ~ ~ t w c k ~ h ~ t o t h e ~ k ~ f o r a f d ~ m o f h e m a x i t - -jaw relat idips, an evaluation of the xahdmwqg m d t h e p h i l ~ o f 0 ~ ~ 1 w i o n b h ~ ~ ~ ~ f S & # p e r f o r m e d ~ ~ i a ~ ~ b y i n ~ ~ e f f f .
ANTERIOR TOOTH SELECTION A ~ i a r t f r e ~ v b s i b l e r e c a r d o f a ~ t i s t $ c a r e 0PetrefhmlOw~ent . I t ~ ~ p r e s a n t a u t o ~ , i b W k W ~ 1 . + (ATS) has been based on theah that twtb shqe relates to head shape, and tooth-& Mumoedka@wtlt%age, sex,


Figam 17-2 Photocopy a patient's phhgmp;k help in selecting tooth size and positioning.
Hgw'a 17-3 A, This patient's childhood photqraph p d d d assistanre In selecting + denture teeth for her at agZ 54. B and C, Magnortic casts d e of kr 30-yearsld daughter
furniahd additional assktana. The daughfer's t& shade (Vim A1 for the centrals and laterals, A2 fw the canines) atso substantiated her mother's request for a light math shade.


302 ParS Ig#w tcekPB#Ptstiwr of the EWkrus Palllent: Fabdadon of Compkw DwthrPes
teeth on the right are from different molds. can see them in the mirmr, and he is pointing
be selected based on this evidence. ones that he prefers,

~ a ~ T s Q t h hmW'm-Nm &wive* Um-+,WTsra ww- n t r h t i s l t t d k ~ ~ ~ m * m ~ ~ w i l f ~ , b u t t h e y a n b a ~ ~ . T h i a t p M e to the porcelain dahgAi6n of enamel. ~ a c a y l i c ~ a r % l ~ W d ~ ~ w b Wtid @utme@ is mp&d to tmt& fald wGQ~,
The tooth positioned just a m a ~ t o o t h r o o t o r i m p l a n t a ~ h a s t u b e " h o l l & m n a little e,xttst toooh volume is ~ ~ ~ D ' b i & a ~ ~ n w I d i n a f m n t w ~ ~ . ~ o r & ~ ~ m ~ ~ a # d ~ ~ c b e r ~ ~ . ~ ~ o r ~ w m ~ ~ - s £ l a y m ~ W ~ * ~ ~ ~ ~ m k 3 0 t b n p ~ ,
~ ~ ~ s t r a a ~ a r e m a a r o ~ ~ w i t b ! I & m @ w m w - m h f i j l l t & t h e P=w@f+dmw=5=mPwwapgQsed f o i ~ ~ m P ~ l h i ; a ~ m i s o ~ r o d l p a i i e n t $ b l y , m o r a p a t i ~ ~ t o ~ f e a a r n ~ ~ ~ d ~ - c o ~ teeth Fgwerpatids bpt fortoo-vfgibl&-- tion, N w M w , mEetiOr both cuwtddm c m ~ ~ ~ e f f e r c t s * * ~ patient's smile look u s i t b emm1, &tin, and ~ m T e e t h m n b e ~ e d t o m e & ~ ~ d e h a n m k r o f ~ d c o m W ~ , ~ a s &mgainddotandpitbon(F@m 17-gXhdidud grltBding and placmmt (Figure 17-91, pla- ~f mtmhs 4 wmn a p p a w m (Pigum 17-10), ,and nataral *on aed subtle ~ O P S in pe&.tion ( F ' i 17-1 1).

364 hst W W r i t i o n of the Edemlous Went Fabrkation of Complete Dentwes

- ~ 1 7 e d C , ~ g ~ ' t e e t h a r e ~ m r n e d t o ~ t h e ~ a t ~ ~ . It m l d not be faurrd in my mold *I&. U, The comgfetsd pmthesCs Whfuffy replimtcsdw tr~gufarity of tooth cotor, sire, and Angle Class It pQsith. Thk patient's sm& b k s
f
of the upper tight canine, the upper left lateral indsor is rotated prominently, and the incM i s ~ , w i t h a n k n g l e a a l [ D i v E s i o n 2 t o o t h a m ~ a T h e M a r e a s i n & ttndtatqaerid shade, but all the other natural effects make them a p v r red,


W m i Height qf'& W d S u m qf Posterfor T&k
Types of m r AcMJng to Yateddls
Tbe cuspd illclinw for posterior teeth were -dedM earlier in pat MI. haePiur a r t i f i d

308 PPrt Tbrss RehabilWen of rhc EPlentulws Went: Fabri-n of Garmplctt Dentures
Table 17-1 I r,lnn.>l iuln 111 n r r r l ~ ~ r ~ Tnnf II h l r r l r l k l l ~ r l i l r r lair 1 1 C t l n ~ s ~ n t r
hitRM6IN6 TEEM FOR COM DENTUM OCCLUSION
posterior teeth, then lowers ta cross-arch contact or 'balanced occlusion"
Monopfane Centric relation jaw Simplest of all Odegree teeth record only recordings
Simple artitulator Simplest articulator Set 12 anterior teeth with r Quick arrangement of teeth in chewing tests overjet but no overbite Wide range of posterior Anterior esthetia nePri W lower teeth in fiat plane tooth pbsitions possible more we j e t and no to middle of retromo tar pad No latenl stresses on Set upper to match; no mucosa with parafunction attempt on mtatt on a Easier for patients with excursions uncoordinated dosures
(e.g., patients with
wive or second and slight overbite rn The posterior point contact visible molar ramp Posteriors set to tontact maintains denture base
on at least 1 point on stability on excursions or nonworking or balancing parafundion contad
Combinations or • Centric jaw record Upper premolars appear 8 *lingualhd" 8 Monoplane lower natural omlusion posterior teeth set to Some range of posterior
retromolar pad tooth position allowed Anatomical upper Reported slightly better
chewing than monoplane

Figure 17-13 Indications of correct antempwterior positioning of artificial anterior teeth. A, Bymeasurement from the middle of the indsive fossa on the trial d e n w e base ts the labial surfam of the central incisors. 8, By visualization of the fmginary roots of artificial anterior teeth, The imaginary mts will be further in front of the midual ridge when a gmt m u n t of T~SD~JWI has aamd. C By d-iningthe relationship of a tramrse line &ending ktwm tttc m W e d the upper canine and the incisin tussa.

376 papvpkrar ~ ~ a f ~ ~ h ~ ~ f ~ o f ~ k ~ ~
lhwftrw rep---*
these muselea depend on f ie
FWwe l7-13 The Wfte wpilia is usd to help l d e the midline of the -1 arch. A, A mark is made on the casl through the center of the papilla. 8, The mark is tm&ed to the occlusion rim as a guide to placement of the maxillary incisors.


312 T%M Rehabilitation of the Edentrlhs Patient F a b M o n of Cornple~e Denturer
WibuM CetlPtal lnatsor Mtim tile central ~ n e x s t t o ~ ~ e a n d t i p it slighdytothe l ~ , ~ ~ l o n g ~ s a f t h e t o o t h ~ t h e ~ ~ 8 e ~ r t a i n t h a t ~ e n ~ O f t h e t e d h are mthaitheyaminfromtheedgeof the mmd b. The incisal edges of h e teeth muit be at the height of h e mandibdar wax ~ r i x n . ~ w i l l ~ t i n a 0 . 5 - m m ~ c a i o v w @ ~ b & a r y ~ ~ a a d ~ tee&, A 1- to 2-mm h o r k d metlap must exht tmwa the lingual & of the diary ante t i w t & h a n d f h e ~ i d s u r f ~ o f t h e ~ ~ ~ & k t h S u & a n ~ e n t w i l l m a t e n
A 6 Pigurr 17-14 A, 0.5 mm of vertical overlap and 1 to 2 mm of horizantal overlap must - exist between the maxillary anterior teeth and their mandibular antagonists to achieve a low Indsal wan<& which is n d d for anterior teeth tohmaion in harmony with most posterior tooth forms. B, The low incisat @de an& is both &hetie and funatonal.


Wrrf*-dflM~rb*by OCCLUSAL SCHEMES FOR COMPL ""mmdLdlowimofthe DENTUREOCQUSION
~ ~ ~ t a t h e # f i ~ s ~ t ~
qre%Tlwdbthef fna l
A
, , *p lY4B %kWdibuM~~iodt~far809kadtheWofWri tJgef l W * t w a d t h c li*f&&, PaiQlls of the ~bortaribortarteeth corrected from &me
sbWf.il3 R J

war 17 W 4 n g and hmm& M e t i c Teeth and ocdudon for he E k & h Wimt a11
f 7-16 & The m n residual ridge, as well as s t l d maWdd t a w , provides the guictances used in the buccdiwal a d antemmldur positionin# of the mndibdar posbriot teeth. IS, Centering the wax d u a l dm on the mandibutar d base w3h the anatomid ids is e w n l l ta the agpmgtiate p k m e n t ob the a m a l teeth. The b a d mt, or mean residual rfdap, and,& retromolar pads biIaWmlly are used to develop the positioning and height of the wax dm1 rim.
o f ~ b m d a o l l a m t e and43) wgxu&%d-- and - ~ c d m t 3 l d a ~ ~ ~ W & w ~
on tbe Manoed artitndadon; b w m r , mwww&d

articulation, ddmug'h teeth with c u q ~ dm ~ a a be usad. F o r t 3 r e ~ o c c l u m l ~ acorn- W o n of upper -miad and Iwer am- ~ m o I d s h ~ h ~ ~ ~ -- T f P e a n t e r i o r h t h a r e s e t w i t h a ~ W c d mdapofO.Sto l m m a n d l t 0 2 m m o f b o ~ - ~~~erIwJptoestablishaIowinc~guidance(we Figure 17-14). AAer these re&menOB are s&s- F.& the teeth be rotaid, @pd, overlapped, or atpaoed ta whim zlawdna. h the ~ e m e n t of the posterior teeth, most clinicians set t h e ~ b ~ t e e t b ~ f i m t h e ~ a r y ~ u s e tbis pmkks h ~gatrol of tbe ohtation of the p h of duaim both d 0 M y and sqxmhferiorly.
Wumk of Posttrim Teeth 5et decifion on t 3 1 e - o f ~ M w m ~ m & d - d e space forposterior teeehfiwnthe dishlofthe ~ ~ t h e ~ ~ . P ~ ~ o n t 4 ~ residual ridge &line aa it a d t o the pad s h o d d b e m i d e d I f o n l y ~ ~ a m t o b e ~ e d , i t i s m w e ~ & e n t t o d m p ~ f i f s t F mch a n d p b t h e s e c o n d p ~ ~ o l a r d t b e f ~ and second mohrs into the milable space. EWmamg the f*lrsS $mmlw is a logical choice because this b f h harp 1- o c c l d surfwe for the Tndidm of food.
MI@ !he Mandibular Teeth Arsl The primtrry CMMmtim ia pitioning the premolars Is that [email protected] s l r r f a c e o f t h e ~ o ~ s t t o u f d b e ~ ~ ~ ~ t o t h e o c M r i n s , & p t ~ y f a c i a l t o b c a n i n e , b u t n m e r ~ ~ d l y ~ t h e ~ ~ ,
Zn the idad situation, the ~~ First and eecond p r m o h , with their central grooves, are poSition&onaIine fromthe canine tipto 1 to2 =belaw the top of the m m o h pad (Figure 17 - 17). wm the fubd pmmhr is @tionef& rt mall #&on ofthe &Ww ir w r a s l ~ rim is ~ t o ~ t e t h e f " l t e r t m d ~ p m - m o h ~ A d u r n e o f s o f t p ~ ~ l a t e w a x is ~ t o t h e n e c l e ~ f t h e f m t ~ t m t h ~ a d

'anSuo8 a q Suipmar3 p!ane al [ w n q aql or 4M!p p a u q ! d aq & r ~ l a u I ~ J I U ~ ~ aq$ re# lg~uassa q li 'pa&ma w ybaat
~ouaamd a t p Alua UWM *pW ~e~ourayal ayl lo q p ~ u ay* pue dp p!dsm qa uaa~yaq au!l a uo pauogpd are ywa rolr;rlwd aw p sa~oo48 p ~ u a a u '8 'qaaa$ myatsod
retnq!puew a y l p lualumfl ayl u! pasn safin8 al! p!dsn> Jepq!puw pauojpd aql 40 d!$ aql pul pd JrlOMOJlaJ 40 do1 W Wlq utu f 03 L V *tl Lt-L L a*
a

318 M T b e W a b i H b t h d ob BhtulousPatient: F a b r b t i o n d o f CwngleQeDenaars
the mmdtiuk wcludal the Arranging N ~ n u t v r n i c ~ 1 Mandibular - m"lu ia in posipiofl pO*fiof m& BajCInd rn*CII,lohn @oit&tg tee&, it is pomile to determine its
cmnkL- position more wily, If the The wangernemt of notmatomical posterior nun&bah Cnst w k is positioned fmt, tk with both antmqmterior md mediohtud hcmskat v d d oveslap might m d the tooth pensating mes p e d t s the establishment
~ r m d $ l i s ~ d b e ~ u ~ d t h r o u ~ u t ~ the ~~~. Therefare placement o f t h e ~ ~ ~ k i S l e f t u n t i I I a s t t p ~ r r p ~ t h e ~ m i n ~ c a l a n d ~ m h p of fk mWor tee&. The fmt premolar is thengroundtofitthe-space. n a ~ m i c d teeth. The
The m d m o k is placed &ex positioning of the the p ~ ~ i t b r h g of the &st molar, tlmreby msrrring develop the compensating m s . its ankmpmMor cmectwss. TBe mandibular d pmm1ar is naplac& after anaaher block O f W a x ~ b e e n ~ ~ t ~ f r o m t h e ~ l d T i m . The mdibulgs Mpmmolaris the last tooth to be lation with p M . it h p n t l y n& to be mud because of three, It k the m b h l space mmhing be!muea the m d m o b and premolar aad the a n h e &r them tee& bewe been and seco mmgd iu xlldmum inmMc#r. For thh E ~ r q ~ t s Q t h f l l l E s t b B g r o t m d a n d ~ t 0 f " r t t h e ~ ~ . T h e t e & w b o t h s i & o f t h e d e n t a l ~ i t r e ~ g d i n a ~ m a n r a ~ :
Emhdmg ~~l Wanred Articuiatlon The molars eligfiUr to tlse facial. ~ceofabalanoedart i~oncaubeinspeded a f f e r d 1 ~ ~ a n d m t 3 n d i b ~ t e e t h h a v e b m l ~ e d . H o w e v e r , i r i t b e ~ ~ e d ~ ~ ~ t e e t h a r e p o s i t i d i n d y t h e s m ~ 1w&o11 in the articuhtw w they were when ~ p ~ f o m s w e r e ~ i n t h e c l r # i r r g imhmmt, thy wiIl eot balance, Furthemore, if the end^^ factors recorded fmm the ~ ~ ~ ~ ~ ~ b ~ t ~ ~ ~ t h e ~ ~ ~ ~ i n ~ ~ t h e t o o t b molds, m e & d d mi expeFt a p m M bilateral balance to b pmak W& b k what me will see duriugtbirr~iseistBatlwmeminorM~ 8 n Z ~ d ~ ~ t a D t h m a t e r i d i r r ~ ~ * for d q i n g &r prwming to addm the requid bahced adiculatim tfie w&w nwmats. The amount of movement MedMateml Compensating C u m A d t b e ~ i a a l ~ d i r e c t i m d u r i q g t h i s mhatbn p m w W d be minimal, usually
m e n d - ~ r e k i m t o # c h ~ d ~

FIgwm 17-18 The antqop9steriox cob~pemthg: gwe invpb the cuspid tips and the wtmmplar pads as the mtomlcal gukds. The cum begins W the -1 d the rhoktr positioned fd with'the plane of a&-n and tive dfstal Sutpaw E e i y el#aped. The c m e mnthues Wh the placemt ef lhe second molar with the d i h i sdm'htd at or above the top of the retmobr pad. The Went of t b awe rarely e x a d s 20 d m
I
Ffgurt 17-1 J The mdiolatetal cwve is formed by slightly elevating the buccal cusps of I the posterior teeth above the lingual cusps. The a w e usually d m not exceed 10 degret5
from the horizontal plane.

~~ ~ a w ~ ~ ~ f ~ ~ ~ ~ t a s e ~ h r w i t h t b e ~ ~ ~ ~ e ~ o h e ~ l e v e l a s ~ ~ ~ r i d p d t h e patemolsrr ad its M qmqgiml d g e slightly ele- ~Thhwi l l~t io lr tbeboothwi&ibi~ong& dbcw ~~~. The fmmpwbim c-t- i n g l x m ? ~ ~ ~ ~ . ~ d i d o f t h e ~ ~ ~ 9 h ~ u M ~ ~ Z ~ ~ l m m ~~~~p~~~ f#it&IiidBg?h m ? & T a n d ~ ~ * . T h e ~ B f e k w i o n m r q p ~ ~ b ~ ~ ~ ~ o n ~ ~ ~ d f o r ~ ~ ~ ~ h r ~ ~ . A ~ ~ ~ ~ w i l l ~ s ~ ~ - ~ ~ . T h e c e n t P a l m s $ s t d t h e f h t ~ I a t i s f i ; a u l d b e ~ t o t h e ~ i n r a f a t i m t o theref- ~ ~ ~ ~ d a n i n e t ~ t . h % ~ ~ &
amid pskdbh aw&g of the tmgw. W b e r a p i e w d i n t h ~ p ~ , L e ~ ~
' w r v e , ~ * ~ ~ a f =&odd be mainaincd by a Wt cle- ~ d ~ ~ ~ ~ t h e ~ c u s p . I b W h s l z a l e d a r i t h ~ h o f ~ I ~ . ? ~ a n d ~ ~ w f s e n i t s m a a g a m t h ~ ~
Arranging ~ 0 r w n o ~ I t c r i Maxillary Teeth to B a 1 1 d A ~ C u I ~




~ i n ~ ~ h ~ d O ~ # C ~ I molar ~~~ will not k p a m t . Such a f e l w l i ~ i~ aot aecesrsary, and positioning of fhz teeth to erabbh such a relationship is discour- ~ ~ 0 n o E ~ ~ ~ p w i t h ~ ~ - ~ ~ ~ f ~ o f ~ ~ ~ ~ ~ ~ h e pdmq m d e d m Position of the tooth ~~g maximrn htercwpatim will can- timse t& aaedialarfd mrqmdng CRrVe mw- bhd in the mmgemmt of the maaQ'buk teeth.
W a d War The mesial mm&d ridge of the d m o k is placed level with the d&al of thefmntaolar.m~atmpmrb~ F u r v e L ~ ~ ~ ~ t h e ~ t h i s ~ l o s e d i B t o c o n W with the mmdibular tooth. Again, ~ ~ ~ m s ~ , a s i s t h e & - ~ 0 f ~ ~ ~ ~ ~ .
Amtt3h18 the k)surlmrm Contact Mdd Im the ~ o f t h e M C r n 0 ~ 4 t h e ~ ~ ~ positioned with th incisal pin &gWy open wbm t b e ~ c u g p s a f e i n ~ w i t h W ~ b u - l a r ~ s t a . T h e ~ o f ~ ~ h n g d cusprrwilIrequh some a o c ~ ~ a f t h e ~ f ~ ~ a a d ~ * c s ~ f t h e l ~ kethtaal&hhmaaimtaninm&Aftw e & ~ t o o t h i s p w i t h p d , a t h b & e e t o f h b h g papsr is interposed between the tooth d ~ ~ l a r ~ ~ ~ ~ i s ~ ~ t t m e f i r s t w n t a c a p o i n t . ~ ~ ~ o n t h e ~ W ~ o f t b e ~ b u h r & o o t b i s ~ b y ~ w i t h a m u n d b u r t o p e a m i t t b e ~ c w p t o & t a h p o s i t b e ~ w i t h t h e ~ ~ ~ ~ i s ~ ~ m a x i - mmninterd&&mf & d m d & W p i n i s i n ~ * t h e ~ ~ .
Remining Maxillary Pwtrrior Teeth The remaining dm ~ter ior teeth are arranged ~ t h e ~ & i l f e o f & e a r c h w i t h t h e ~ e c r i ~ d prwdmq aa pdoudy outlined,
ocauw MODIFICATIONS AND THE W I V E R W I N G PROCESS
Framing *[email protected], caupl8d with the lack of a c c l d b h c e before procsssing, requires a
cies and to obtain a b a h d
the mouh After the clinical remount of
lary lingual q s . Premature contacts m are at the central fosaae or margid ridg
achieved at centric jaw refation position (F 17-21).
Adjusting the Working and Balandng Conbcts W o r m side inMepenms will mdt h m between the lingual inclines wp and the facial inch= mmdibdw tooth in W e d

+$!&w*Lm-w
m juaptu snop~uap aqa ro) uolsnpm pue ylaai ?laWmd %u@uelw PUP su!pa~;y L% &erg


Flgwrur 17-23 During the W m t #twemm the mrtkIlky lngraal cusps ahtact the lingual ir~dinfl ,-if the malP8klar bum4 cusps to create a bala-4 aatksrhtb. I
Y
W~&QU~ d i S t d I & trrry of the a- p m til* and of the hfXUHl.
the m t e r i m O e e t h C Q n w ~ ~ in the prom- brought into she rnowma~, the aterior m m d i h k am i t i s d e s s e t I i e t e d h u s u a U y r n ~ d , ~ t b e ~ o f
t bilaterally to the b tu res in mind


C
The Try-in Appointment Charles L. Bolender
I SECTION I: PERFECTION AND VERl FlCATlON OF JAW RELATION RECORDS I
The vertical dimension and centric relation (CR) of edentulous jaws are tentatively established with the occlusion rims, as described in Chapter 16. After the preliminary arrangement of the artificial teeth on the occlusion rims, it is essential that the accu- lacy of the jaw relation records made with the occlusion rims be tested, perfected if incorrect, and then verified to be correct. The dentist must assume that the preliminary jaw relation records were iacorrect until they can be proven correct. This mental attitude of the dentist+attempting to prove tfrat the jaw relation records are wrong-is essen- tial in perfecting and verifying jaw relation records.
Patients should be advised to leave existing dentures out of the mouth for a m u m of 24 burs before the jaw relation records are perfected rtad vded at the time of the fry-in appointment. Unfmbnately, most patients will find this to be an umeasonable request. An acceptable alternative is to haw the existing dentures rehed with a soft temporary material. Whichever approach is taken, the soft tissues of the basal seat will be rested and in the same form as they were when the final impressions were made. If this procedure is not fol- lowed, the distorted conhtion of the soft tissue can prevent the registration of accurate ~interocclusal records.
It is almost impossible to overemphasize the importance of perfection and verification of jaw relation records. The appearance and comfort of the patient, occlusion of the teeth, and health of the supporting tissues are all directly related to the accuracy of jaw relation records.
VERIFYING THE VERTICAL DIMENSION The maxillary and mandibular trial dentures are placed in the patient's mouth. The patient is instructed to dose lightly so the mwiIlary labial frenum caq be checked to see that it is absolutely free. This is necessary before the relation of the lip to the teeth can be observed. If the denture border causes binding of the h u m , the labial notch should be deepened.
Next, a tentative observation of the centric occlusion (CO) is made. The mandible is guided into CR by a thumb placed hrectly on the anteroin- ferior portion of the chin with patient instructions to "open and close until you feel the first feather touch of your back teeth." At frst contact, the patient opens and repeats this closure, only tbis time stop- ping the instant a tooth touch is felt and then clos- ing tight. The procedure will reveal errors in CR by the touch and slide of teeth on each other. Errors in CR can interfere with tests for vertical relations.
The vertical dimensions of occlusion and of rest must now be given careful consideration because the f jnd positions of the anterior and pos- terior teeth will depend to a great extent on the amount of space that is available vertically. Unfortunately, there is no precise scientific method of determining the cprrect occIusal vertical dimen- sion. The acceptability of the dentures' vertical relations depends on the experience and judgment of the dentist. Nevertheless, the factors that govern final determination of this relation can be said to hang on careful consideration of the following:
1. Preextraction records 2 . The amount of interocclusal distance to which
the patient was accustomed, either before the loss of natural teeth or with old dedum


W e n trpm md tower trial kdum The\~e&~$ ~ p o f a h t e r i u r W t h i s a g u J d ~ ~ P w t k e d r k d ' d i m e m W a ~ h k f t ~ w i l l b e ~ ~ A w w s indiate the k w a ~ tripod of stops.

&dd ima, the M mfmw ~ ~ S L T position & t t t s e d e c t s d ~ ~ ~ ~ ~ t t r e u p p e r ~ ~ ~ i a d a n t ~ s o R e n d o p p & g ~ ~ T h 4 ? ~ ~ ~ P e r n o e m ~ ~ the^^^^^ in a.
Tlte m h h rim$ with the t t d in good ~ O O , ~ ~ t o t h e n m u e h , a n d t f t e i l a m e ~ ~ ~ ~ ~ f o r e . I f t b e ~ ~ ~ ~ d a ~ z m d u n i f D t m I y ~ t h e ~ o w a r j m i s ~ ~ i & s f a r a s i t w i l l g o , t h e C T R m o u n t i n g m @ y ~ ~ a d ~ ~ ~ T h m s h o ~ ~ ~ - f o r m ~ ~ l a ~ c ~ m ~ ~ a o f ~ m o & h a b e f P O Q t d b ~ k d 7 K i ~ ~ deht&d touch md slide.
I t ~ ~ a l ~ t h i s ~ ~ d u r e t h & t t h e B s n t b t ~ h ~ m d r m e m w i n t h e p r u v i m m ~ T h e ~ m u s t k d t o b e i n o o r - reet d e s r s no touch and slide rn be detected
fI.epeateduaaif.Idldoabtas
mi '3.6.
"p .
C f P a i n k ~ & m M & b y m - ~ ~ i i l ~ ~ a p e ~ ~ m t h e -W&tbaa k&&;trabaTb-g~e b ~ M W ~ W * r n an
4wamm&qL& in
R&mhlm The pixrpom of the extraoral IWM 4s to derteratine whether ?he. psition of W teeth en the &1aor (Figwe 18-4) is the w at in the patiat's mouth (Figure 18-5). & mentioned pmiowly, it is difficult to detect ~ 0 1 ~ erras by clinical abmwtio11, 90 wax, pbtar, w ID bit~.reg&ation pwte must
.';, >' x-'
$.#$+: i: ,>,,
;A

&d A smnd layet of warmed Alum is the firs4 layer, which has been mrefully
to the pmterlor teeth,

- .
1W Part T h e 8ehabilWon of Ih Wntukur Patient: FaMEatim of Complete OcWrm I
"I- The mandible is guided inPb centric datbn dtth the thumb on the ankroidwiw portion ofthechlnandtheinkfirrgensmting the lowertrial d&um in a downward and forward d i d o n .
Figure ?&I0 The patient is instructed to close lightly into the softened wax. The index fingers should be slightly raised from the buccal flanges at this point.
dned. It is important that the imprint of the oppos- ing teeth be crisp and about 1 mm deep, with no penetration of the wax by a maxillary tooth (Figure 18-12). If penetration occurs, it will likely deflect the mclusal contact as well as shift the bases or change the rnaxilIomandibdar relation horizontally and vertically. The chilled dentures are returned to the patient's mouth, and the patient is guided into CR. The record is acceptable if there is no tilting or torquing of the trial dentures from initial contact to
Figure 18-11 The occlusal record should be approximately I-mm deep and free of any penetration by the underlying teeth.
complete cIosure (Figure 1 8- 1 3). Underlying soft tissue displacement may cause a slight movement of the bases and must be taken into account when evaluating the contact. If the record is unaccepf- able, the procedure must be repeated.
After the wax has been chilled, the triaI dm tures are placed on their casts, and the locked artic- uIator is closed in CR; the opposing teeth should fd into the indentations in every way (anteriorly, p teriorly, laterally, and vertically) (Figure 18-14), When the original CR interocclusal record and ih check are both correct, these teeth will f i t into h! indentations surprisingly well.


E ~ ~ ~ ~ x s ~ t f i t ~ d y ~ ~ ~ t h e ~ ~ r d , i t ~ W ~
~ ~ ~ ~ ~ ~ ~ ~ e r r t d i d n a t ~ c l e a n q g ~ ~ ~ ~ ~ w ~ . T a e v a w B t h i $ b i m e d e n t i & ~ r e t t t m t h e ~ t r i a l ~ a a d w a x ~ t a t h e ~ ~ a u f h ~ l , w a m e w ~ 1 8 8 ~ M b e d , r f & & ~ ~ ~ a o t w ~ h l $ l e pstiat&*w-mmtion, ~ o r W ~ h ~ X n ~ ~ , ~ ~ ~ m h ~ a e e t ~ ~ ~ * m d ~ ~ ~ ~ b y m ~ a f m h e ~ ~ h l ~ m T h e ~ m ~ ~ ~ k g ~ ~ B e e ~ t o ~ o r ~ f CaTmm8.
Xf the initid ragiatdon @re- CR ~ ~ ~ i n p ~ o r a b i t e ~ - tian paste, the same recording medium should k w d t ~ ~ h ~ ~ ~ m c y o f t h e m o u 1 1 ~ o n t h e ~ . ~ , i f w a x ~ ~ d , w ~
I b u M k the vwifyhg medium. HoweverS it is d e r ta &sort wax the mmd is removed from the mouth and t d on the dculabr @@ 18-15),
SECTION 11: ECCENTRIC IAW RELATION RECORDS, ARTlCU LATOR AND CAST ADJUSTMENT, ESTABLISHMENT OF THE POSTERIOR PALATAL SEAL
. .-
FROTRUSIVE AND LATERAL RE
dentists as to what a protmke intmhdto att&The idea& the


338 P*Ft fkrw WWIwt dthe Bdentulous Patient: Fabrication of h m p h Denturn
the postmiar twh R t the wy-in appatamnt. mafely 3 mm Mml ta its pwitim in m ~ ~ ~ o n ~ ~ ~ f ~ r h a s m a s t b e ~ i d - m ~ I & r t o & w i u h a P e m o v e d ~ y 3 e r e d ~ ~ ~ t h e ~ c d a n 8 ~ n t a l ~ u s e i t t ~ b l y m i d w a y b e t w E e i r ~ ~ f t h e ~ ~ ~ m t a s y e d h e e n tracingandtkwdhg~sidecondyle. ~ ~ t h e . ~ ~ o f ~ o t l a n d the lcML Pt twth an ~ 0 - PmtnisIw I n t m u ~ l Rcmrdr jbr the
ThrPa-rsaods per- Mix ArUmIatiar &- TypeJ €eawve a@ml%nt o f h d y k g u i w m*shllhm.
~ ~ ~ ~ ~ ~ a f f e r t b e a r t i d ! ~ . ~ W ~ ~ h ~ k a ~ f b ~ ~ c s a n d ~ ~ C R a n d t h u ~ c d ~ o n ~ b e e n wxifxd If the ho&mnhl wmhp is d ~ i c n t to a b t a i n ~ * ~ - o f t I l e l m j m ~ k ~ ~ ~ ~ u ~ ~ s L e c o r d pa willbeiukqme. r t d ~ ~ h m ~ r e c o r d ofofml&mofthejmduhginckiw.Ifthe b o r i z o n t s t t ~ q o f d r e ~ i s t m d t o
mentafthecadykguidmce, thepaticntmustbe hdrwkd to pmlrude the jm farther when the recordismade.-mtnimnm-tBfprm- sion fm m&yh guidruloe adjudmmt is 6 mm. T b hitation is,mwswry k w e of mechanical dclfhiencia of m o a t d d d n g i n m e n t s , anterior teeth.
L & e ~ d ~ l d m ~ r d s c a n b m a d e t o s e t t h e 6 ~ i n c l i n a t i W I t o d t h e I n d i b ~ k ~ a a ~ ~ ~
aa the dcuhtm. However, a corn- of the uppet and I p ~ ~ , i t ~ ~ d i f f i c l t l t t a s e o u r e a c c u - ~ f u l l y ~ rate and reproducibIe W e d xecorb t b u m v e - , in part h u e o f f h e dispI- Mi@ of& Eidge mmma. En addition, mast mmi- ~ ~ ~ m n o t & e t o ~ ~ W d eccmtric p e c k It is therefore gemdy
far p t i e m with complete hmBs i3 aot p t i m l r i m d p r d ~ b l ~ n a t ~ t e d . When the dentist hmts become f d k
~ ~ W ~ m a y b e & mlatirmofthelowertothelxpperd w E e b & e ~ o f ~ t r a c h s g s , W e d x e bi&g &via f;51 &if1 a t m h d to the o ~ c l ~ o n & n s , d K ~ o f ~ m ~ L d e t e r - mined by obsmation of the distam between the
of h c i q md the d e point, The ~ a g l d d i r e c t i a m ~ f t b e l a ~ ~ n t ~ b e ~ e d b y ~ b ~ g Z b e d i ~ c e d t b e n e t +
~isonoaeofthearcsofthetracing.Wtien t k n e e C L & e ~ i s 6 m m f f o m t h e a p ~ t h e o t r ~ o n o f t h m ~ d p mart&% in the fifst m o k region will be approxi- on dm ~ ~ r T The patimt


349 Park- U ~ ~ m of lhe W u b u s Patient: Fabrimtlon of bmplcte Delrtures
c Figum 18-9 7 Trie l denture bases pasitioned by an intemcclusal protrusive record (impression plaster) are returned to the Whip Mix arfialator. A, The horizontal condylar guidance mtchanisrn i s not in contact with the condylar sphere ( a m ) . B, The condylar meehanlsrn is rotated imo contact with the condylar sphere (arrow), thus establishing hori- -1 condylar guidance on the articulator. C, An intemclusal protrusive record has been made In wax, with the articulator adjusted as in B.
m h f & l s ~ttm hyws of ~luwaxsealed with a 4%.m WZ)PrdlllWaXpoiWnC warm spatula.


M2 Part Rm RdwMWiadPhe MBenatlous Patient: fabrkatlon of Gnnpkte Dentures
ESTABUSHMENT OF THE H E B t O R PAWN. SEAL
notch on both sides slightly a


1&25 wnf'd C, The trial denture base shQm the a&- length of the m- pt& demm X Lnm the lmhn of tire vibating tite that ~lils t~~ from the ~ ~ ' 3 wth.
f 4 0 * , P ~ o f ~ W d l J e ~ ~

I- The groove in the cast (arrows} foms a bead an L c finished denture (Figure 18-28).
1&31 lhe denture snds on the cast at A. Thebead 0, lumed 2mmin frontoftkeuibdng line, is extended hra1ly through the centet of the hamutar natdxs.

I SECTION Ill: CREATING FACIAL AND FUNCTIONAL HARMONY WITH 4NTERIOR TEETH I
ANATOMY OF NATURAL APPEARA

Hguw t&33 Facial landmarks, A, Plrrrw; 8, rima oris; C, bww tip; 0, menturn; E, men- tdabiial w tcus; f, anguhs wis; G, upper lip; #, phtlfrum; C nasolabll subs; 1, ala mi.

' , i' ' / '
~ ~ ~ ~ 0 f ~ ~ a n b o r - ' I
drqm.philman.andib.mmtOIWalh tdsnuhw @en&.
T b ~ ~ l c t r o , w g m c w e , f adeprere r
s i O n i r m ~ ~ m ~ * d b b * ~ & ~ ~ ~ h t b E d & o f t h e l m e t o i@p&mddy*m* t t t e ~ d t h e m o ~ (m@i oxis) (m Figure 18-33), The z y ~ ~
I rmmle o&iwus on the z y p m t i c h e and ~ a a w n ~ a n d f o r w e r d t o ~ ~ i t ~ n e z o f t b b ~ i n t a & u ~ & ~ i e . The d m of zbe two zygmmtbi m w k in el+ Patiagfheoomdthemwrthfoasmilingprp.
th w&bial dew @im 18-34), Many
& & e m t e d ~ ~ i t ~ e 8 a d i $ a s t k ~ 1 ~ ~ . ~ O f t b e ~ l o r l f o l d h a s
~ 0 1 ~ ~ ~ ~ ~ ~ s m d e r t h e f o ~ ~ ~ ~ b u n t i n ~ ~ t i o n ~ a m y ~ ~ ~ , T h e d ~ t r r c w m a t a n d ~ & k ~ = ~ t % % h e n t i s ~ ~ * ~ ~ b @ l d ~ t o i b ~ ~ ~ ~ m ~ ~ ~ ~ t a * t h e ~ ~
be~tii&~,&?~erpoP.ttosg,~**Haa~ilJ n o t n ~ c ~ a w ~ ~
T h ~ ~ ~ 0 t ~ t b ~ ~ w d t b e ~ ~ ~ d ~ h ~ o n ~ l ~ ~ ~ d ~ ~ ~ ~ a n d ~ & m a f t f m e ~ ~ f b r ~ ~ & e ~ 0 f ~ l ~ I i p ~ d ~ ~ ~ ~ h & ~ h A ~ m o f & l m i z d a l d d * t b ~ i s ~ ~ hrof&el@ti@igam 18-35).
A ~ ~ a f h i m h a t i d o f t k ~ I r t n r c - m ~ t f i e ~ ~ ~ ~ ~ ~ i n ' m w t ~ t b s ~ c a l m w n s o f t b l ~ ~ g , l a b i a l t o ~ b a n e ~ ~ r i s

I
I
I
I
B -,?%& 1 he polyfundional W d . A, UndAyhg wfmfkial rnusaIlmre. Ah, An&kW; DN, d i W r wtls, D@ k m septi d , , i k , inftiaohkhl kid; N, nasalis; oO.E+~w,~taris li: UQ& orbiculak a& P, pl-i Pr, proct~s; 'Wk la infenow Qfi quadmtur Iabii wperioris; R, 7, Wngulark Z -ti- =matic h e . s, Surfm.anamw. AN Ma nasi; AB, q l h s d$ AM, rae# mk bllfc, bash Q&; mu, &mum mi; klc, menturn; Mnf, mnrfftiufarrfip; MS, rnentdihl -slrkm d t y fib; mmlabiai sutcus; H, pbihrn; aO, h a or% a red zone or wrdim 'bad& Tu, W k t e . (From Martone Al, Edwards : h s & d Dent 11:1089.lOt8,1961.]

Rgum 18-3s h Rep,roduction of a patient3 far- re~oi~tio'n c o h n k . m e r h o b n ~ I o w k p wtth the cdrrea fadal contour. 8,HwiEonlittw&pchangedw,#edIhqanterSsr &&I conWthu m d b l a r teeth, with mw~ttant damam to the u p p lip
~ ~ ~ a ~ t o ~ e m ~ m a i n ~ d ~ 1 & 3 a ) , k ~ a o h l l n m v o u s r y ~ o u s ~ r b o n o n h U d k f a c t m a f f e c k t h e f a c e i n
.-.-.---- -. -.-- -.,--..-. -... ."... ...-.- -..- B bony ti& linmralh at first and then i&ialli 65--

A FCIplra 18-37 A, Muscles that maimin facial suppoft When artificial teeth and the dew hlre $ase M e r i a l restore the lips to their correEt contour, the facial muscles will L at their physiologist length, and contraction will mate the normal facial expression of the patient.
fontitwed



354 M Tgma Rchabilitatioil of the Edentulous Patient: Fabrication of Complete Dentures
-re 1&40 GOMY C The bulk is needed for correct support of the upper lip.
facial expression that may be more damaging to the q p e m c e of the patient than the slightly protruding teeth. Individual pronounced irregu- larities may be improved, m long as the position oftbe dental arch in its support of the orbicuiaris 0148 muscle and attaching muscles is not percep- tibly altered.
Thus d facial expression d proper tone of the of the f'ace depend on the position and fuuctioa of the facial muscles. These muscles can function physialogically onIy when the dentist h positioned and h p d the dental arches cor- rectly aad has given the m&& a favorable verti- cal ~~ h addition, the ~~ themselves must have. a pleasing and W m d appamce in t h e p ~ t m t t m ~ a c ~ t h a t i s ~ d e n t u n amnghg the ~ W ~ c i a l teeth in a plan that simulates nature. This, then, is the challenge of mating facial and functional harmmy with anterior teeth
BASIC GUl DES TO DEVELOPlNG FAClAL AND FUNCTIONAL HARMONY Affer an acmpthle &d dimmion of occlusion bm been &mnined and the hmkmtal relation of the casts w the arti~ulator has been vded for CR, the appmm of the patient is studied and mu- d m are made in the mgement of the teeth to obtain a harmonious effect with & patient's face.
The guides that are cons and functional harmony
3. The vertical orientation of anterior 4. The inclination of anterior teeth 5. H m m y in the general compositiay
anterior teeth 6. Refinement of individual tooth p 7. The cmmpt of harmony with sex,
and age of the patient 8. The correlation of esthetics and
guidance
Although these factors are discussed indi ally, for simplicity they are interrelated in actual clinical situation.
Preliminary Selection of the Adificial The prebiaary selection of teeth evaluated for s k , fbrm, and color arranged in the kid denture. The six upper tee&, when properly suppormg tbe
be of sufficient overall width arch to q p x h a t e l y the pos
the face so the teeth point of the face. The
time to ensure
Horizontal Orientation of the Anterior The position wid expression of the lips

# &!I F l '! ' A B
FI&ICCb 1841 A, Corm positioning of arl artificial central incisor to restore the physio- logical length of muscles for pmpw funrtionlng. Dotted outline shows the m t h incorrectly positioned to follow the residual ridge. B, Position of the original natural central incisor,
Figure 18-42 A, Artificial anterior teeth positioned too far posteriorly. Notice the lackd' tone in the skin of the upper lip. B, Artificial anterior teeth positioned c m e d l y in an anteroposterior direction. Notice the imp& skin tone.

7
3!% PPOt T b a l k h a b i m of the Edentulws Patient: Fabrimtion of fompkta Omhues
d o 1 1 br&m become f i b l a , the mmm o f t h e ~ ~ a d ~ m a n y o f t h e ~ ~ ~ a b o v e t h e ~ o f t h e ~ & m M r n - a & - o f t b * # w m m d h g t h e ~ W a n r & - ~ ~ a o W 0 f t h e ~ f n ~ ~ ~ f t l rebnotr f f eddbg . tbpo&ion~f the t e 4 4 & ~ ~ ~ i a t ~ ~ ~ i l l ~ g m a t , t h e d r w p @ ~ o f h i c r r n b e a m & e m M y * W I a l m M ~ b e ~ a n d t b ~ m ~ B e ~ f u l ~ t b e ~ b i o f l t h e ~ t ~ i n ~ ~ ~ , p t i ~ ~ d ~ ~ ~ t o t h e o t h e r i m ~ ~ t h r z t ~ b e ~ b y t k ~ t h s t w i l l p r o d u o z a x n o r e y u u t h f d qpearmca.
~ ~ l i p ~ u E p a r t ~ f r o m ~ r ~ f o c r t a e d t o o f r l r ~ o 1 1 y i s ~ b y a stmbhd tight appmance of the Iip%, a temiemy f a r d l e : l r p f s t o d i d ~ t h e ~ d ~ f r m c - tion, d i m h f b n of the normal conbum of the Iip, and &tdm of the philtrum and sulci (Figure 1843). A pbqgaph of the patient with ~ ~ c a n ~ m o m a t ~ ~ f u t i n ~ e p ~ g o f a r t i f i c i a l ~ T b e ~ ~ b e m w , t i l a t & e a ~ ~ o o ~ o f t h ~ a e d I o w e r p m d $ d e f a c e ~ l e t ; t a o s e ~ i n t h e ~ ( @ e w e 18-1, C). .
m. W W 3 A stretched a p m m of h lips and phiIt~m indtats thal arkifid J anterior teeth are positioned too far anteriorty.
base. Such a guide aha will be he
-re 1- Correct inclination of the teeth incisal edges in a moderate prognathic relation.

I C Y
Plate 18-1 The teeth used for both these patients are Vitapan hdrd dcrylic resin (Vita Zahnfabrik. Bad Sackingen. FRG]. A and 6, With preextraction recurds d> d guide, Ihi5 patienl's upper canines are shade A3.5, but her other anterior and posterior teeth are AL. Fretlucntly, thr upper natural canines will be darker than the other teeth. C and D, Her high rchool gradu~tion picture, showing her nati~ral lecth, was used as a guide in selecting arranging the anterior teeth for replacement dcntures dl agc 64.
Cotrtinlruii

E F Plate 184 mt'd E and F, She requested a light shade, which was used, with a pleasing result. 1

froPn w If*
~ t D Q & ~ ~ Q n ~ ~ ~ h * 1 8 4 , B ) , * * o f b w h i n n & & i u n b & e ~ d ~ r i d g e * s f n ~ t i a n o f " c i e b a m 0 m t d ~ d h ~ d u a l ~ : d a t ~ & a ~ ~ ~ i t P ~ t ~ f m ~ t h Q ~ ~ ~ d -
A o i m a ~ ~ r e : k b e t w a t n $ r e uppar canines, as \ t i d &om the t i ~ n ~ hg su&e of the upper bid bnture W, & d d ~ s $ . ~ * ~ d f f b w ~ ~ w ~ ~ ~ ~ f ~ ~ ~ m ~ ~ c o f - l w 3 y ' * & e m H u # w t d w ~ ~ ~ 18- 4 6 , ~ E ~ ~ ~ ~ W & ~ ~
& h d t h a ~ a ? d l n a a y wtrbbard- ~ ~ + m t o ~
p @ # # t b d w i m o f * ~ t e e t h n w y b t o o ~ ~ o r t h e t e e a i t ~ i ~ t o o f a r kwk

B C Hgam t8-A6 I W b w of wmt afiterqmterlor positioning of artificial anterior teeth. A, By measurement from tfie middle @ the incisive h on the trial denture base to tfre b W sui#am of tke. central incisors. 3, By visuiizatian of the imaginary roats of attiii- ciad amatlor teeth-h imginary ram will be farther in front of the. midual ridge when a gteat amouw J mwpth has murred . C, By determining the relationship of a tranwm firle Wending kW&n the middle'd the upper mines and the incisi* fom.
40paaofageandolderandmwatoa extmtinmmthminwomen.
A ~ e t u s t c a n b e P s e d t o ~ ~ OftheupperIipin~onPotheresidrald Theirmdexfingerisplaeedunthehisim w i t h t h s m h d u p p e r f i p ~ d i n g ~ r
(Fm 1s-47, a. Tbanmsuntaf th e d by the upper hp gives an hitida i e n ~ ~ f t f r C F f i p * b b ~ r i r ~ ~ t o * & i t w i l l ~ ~ u p p l

&?r (Figwe 18-47, D). An- d b bunt of msidual ridge resorption must fie @ d e d i a t h e c a l e u t a t i o n . f i * ~ ~ o f ~ ~ ~ ~ ~ b e e n o u t w m ~ m a k e #&c?&mak.
H o w e v e r , ~ k r a v l s x l i p i 6 ~ ~ ~ d e f o r t h e ~ o r i ~ t i w o f m t 4 3 r i ~ ~ ~ ~ ~ ~ k T n ~ ~ t a , ~ ~ e d g m o f ~ n a t - J E a w e r ~ e s a a d ~ c u s p t i p s o f t k e 1 ~ k ~ ~ r r r t o v e n * ~ e ~ o w m l i p a t t b e ~ o f t h e ~ * t i a e m w t b i r s ~ ~ @m (FQm fW8, A). HdfIc iP fmm -or ~ a r u l ~ h s r M O w ~ l m 1 , t b e i r LfAd pi th iq d l pbabIy Im incomct
Y
Flwm 1847 4, t h i s long upper lip obscures the natural uppet anterior teeth wen dur- ing sp&h. B; X relatively shoTt upper Ifp exposes atniost all the crowns of the uppw cenim1 and lateral irrciwrs, C, fhe upper lip is allowed to drape wer the index finger, which has been placed on the incisive @pitfa. The thumb is in contact with the wrmithn krdcr. 0, T k am~tmt of index finger that kas been mered Lpl the u r n lip is an indiczlh of the length of the upper lip relatlve to the upper residual ridge.

360 h t Tbrca t(eW1Miond the Edentutous Patient: Fabrbhn of Complete htum
F@ra 1W A, incisat edge of the natural bwqr m i n e st ttm led of ihe 1-r lip. & Wianship of artificial lower teeth to the W Ig. b& COW he$ht; middleI toQ high; d&teQiow, /
I
mfs, in relatimtothe


H#m 1- LahbI and lingual inclination of the anterior teh. A, The natural M h h e varyikg of itIdl&~h, B, Nodte the i n d i d o n and position cf t k anterior
in rehion to the indination of the hVml plate of bone. C, The indination af this kwr &dual ridge -ides the M o w n that the lower anterior teeth, wWch it onre summtd, had s I d a t indination.

~ S a 1 Ttle indimtian Of anterior teeth often wmIlek the WIe h e of the h t M r d d t h e f a a .
-re 1S52 Ovoid.
c e
Varying shapes of the natural dental arch. A, Square, 3, Tapering. C,

364 Part tgrsa lgehabiliOntion of the M~tulous Patient F a b r i d n of CMnpiete DeWres 1
~ ~ i n c i m i n t h e t a p e r i n g a r c h m a ~ d i s t a m a e ~ h t h e ~ a x t i a e ~ t h a a i a anyotherarchThereusuallyis~i~lemtathg d h p p i n g a f l h e ~ i a t h e ~ a r c h ~ w e . of lm space, Thdm crowding results. The m~pas i~reducethemamtof tmths lrrFace &mhg,~thetgethdonatappraswideasin other setups. This nrrrrowed is d l y in har- morrywithammwrtaperingfwe (Figure 18-53, B ) . I n f u & t h e v a y ~ s o f t h e t a p e r e d a m h d ~ t o ? h e T l a r m m H d ~ o f t h e f a c e . N d teeth move in function, and hi5 f r i . & h d m o v e m e n t w e m t h e w n h t a r e a s . M u a l ~ needtobagmdmthecorresponchngmtact ~ b d m t h e ~ ~ o n a l ~ m a n d give fhe d e h d effect of a tapefhg setup.
Tbe mmlWmin the midarchare far- ward of the &es in a position - that of thesquamandtbatofthetap&g&Thebeth in thh form of are seldom ~~ and daey ~ ~ a ~ ~ t a f l a b i r r l ~ c e t h a n i n t h h p h g a & p d , a s r t ~ h n r v e a h d e r e ~ ~ ~ b a n n w i z e w i t h m P w i d face (Tigum 18-53, C).
The forrn af the @aM Wt gives an iadica- t i o n @ s l ~ t L e ~ f m m o f t h e ~ ~ ~ removd of the namd teeth and mwqdon of the ~~ ridge. A b d and Wow edentulous ~ ~ ~ ~ t h ~ d l e ~ t a l ~ h P o f m oripdly may have been square; a high, Y-shaped ehtulow vault p b a b I y indioates a tapring den- ~ ~ d a r r w n d e d ~ o f ~ ~ ~ h e i g h t ~ in&& owid &mtal arch. Most patients exhibit same mmbidon of these classifications.
The arch form of the artificial MOT teeth ~ b e R i m i l a r i n ~ t o t b e d f w m o f ~ ~ ~ i f u n e a a a u n r e ~ t h e r e ~ a o ~ ~ a m f g e r y w ~ t h e 8 1 1 t e d o r ~ ~ r e m w e d (F ipe f El-54). This h p b matomicat fiwt ofkn is ~ t n i t i t s h o u l d b e o b s m e d c m f d l y . W b e n ~ ~ ~ ~ a r m g e d i r m a n ~ k f f m t b a t corraspondoEa&fmmaf*re~U*,natu- ~ ~ ~ a r i t i ~ t h o t t ~ ~ b e e n ~ ~ i n t b e ~ e p t ' s ~ w i l l ~ f h b e ~
~ & t h e s h a p e ~ p o 9 i t i o n o f t h e M 1 ~ ~ ~ ~ l f w t t y h l n a h e f o r m o f ~ n a ~ m h ~ a h i g h l y ~ f ~ l o s s o f E a c e f o n n ~
c m A a q m m m h f o r m w h e r e t h e d m h w a s m o r e ~ w i l I ~ ~ u s e a ~ ~ o f
Figure 1843 Anterior arch forms, A, Square. . Tapring. C Ovoid. 7
Rgun V 8-54 Domd ~ i n n indiate that the 4 h form oi artifrdal anterior teeth on the trhl dmtq bsre is brsielly simihr to that of the anteriw ?I the residual rid& - the lips, with elimimti~]. of the Atapmingarehformwherethe mw=-wt-lyw of &e mouth for proper facial

A, Buml corridor inadequate per placement of the uppw teeth. in proper position to support the the adequate b u d corridor.


Hmra I&-= Hamtony of the line fwmd by the ineisai edges of the upper amrbr Wth I w i ~ t h a t f w m e d b y t h e a ~ u r e o f ~ h l i p ~ L i ~ e s i n ~ n y ~ a n d n o t i ~ k a r r a o r t y
I , @gh#. Results are a pleasing and a d ispkbq appearam. B, Notice the hammy in tMs Gw.

I I I- T k labial face ef the M r a l i&r pmlIeb the pwfile line sf the kc&
t4otia btheinckdthiddthetooth hreab I ingwlIy~theprofikline,


A B Figure 18-63 A, Indsal wear on artificial teeth. B, The pamm of wear in A has been dcvelopd to Improve the appearance of the denture and aakt in balancing the ocdusion, Wear on the upper m i n e is placed to cormpond with wear on the lower canine in a balanced occlusion.
depict you #and 6 e f f l i ~ i n ~ , ~ t f r e d w e e a n ther@h?arcwiWforanoldetmascu- tikdhielml. 8, amsand indsal dgts of artifidat t&h must be m d H 4 tu pmvb a natural wpemm


IFiwm 1- Mesiodistal inclination of anterior teeth relative to the perpendicular.
I B
l M 7 LttdCjOal view 0f anterior teeth showing their angte of rotation. Wllary W and mandibulaf iE$
foreign ta any that miwe has estZlbIished For exam- ple, a m d h y & is seldom in at the cervical end and will appear ~~y aditcia1 if this h g - *ty is atmrptd The patient cannot point out the exact cause of the u x m a ~ ~ s bui will Be

w#mny of S p a a s and Ihdividwal Twth &bn T h e w e o f ~ ~ ~ a u t b e Iww far f n d i w tooth p d -
A B mrs 9 8 4 9 A, Notice the mesial rotation of the central incisors, the rotation and posi- tion of the lateral incisors, and the mesial aspect of the canines avwlapging the distal of the lateral inEiS0t-s. B, These mandi bu tar anterior m t h appear natural in the patient's m t h .

- h ~ & h Rclmbilitation of W Hm~tulow Patient: Fabrication d C o m p k Omtures
*%.70 A, Space hewen the upper mtral indsors can be df&w in maintain- ~ 8 h e ~ d a ~ i f i t w a s p r e s e n t b c t w e e n t h e n a t u r a l ~ i i n h . ~ , ~ p a a between the cenml and b m l incisors helps create a natural appearance in the arnnge- W d artificial anterior teeth. C, Space lwtween ?he Meml incisor and mine p m v i d ~ a
esthetic effecf when m fm the side. Hwver, it is not visible M e n seen fmm the f b v & (Compare with Wre I&%,&)

B C mLplaa 1- A, The central tnumn uorninate this srmngement of artifidal anterior Wh. B, The rounded incisal edges and relative sites of the upper lateral inc'hrs provide a corngasidon that Is feminine in appearam. C, Notice the la t ion of the u r n left anine relative to the smiling line. Wear on this bath is compatible with the patient's age, MtIm alw the anteriorly facing rneial surface and the vertical long axis of this tmih.

F@mr8-73 i * ~ t ~ d f l a p p a t d a & & , l o e t k r t h e ~ ~ l i n m t h i n . ~ . m!~ps h a w b g ~ W6d .ltatuFalpWm, xcmmi ;ed by an h w d appearance a f W z f l i n a t p d ~ & & % ~ w f e t l s . C T h e ~ a ~ r . t e e P R a r e amam an an i * . m m ta.M. Hp Notire W r d&mq ln fmt of the rddual WWIP~~.. ~iptnw &=me*= muxiem r n ~ -1 a p e hiwe twa m,W,praQler lerugth. The teeth a b appear natural be#& ~f-w ~ ~ ~ f w n t , m k w * m 4 . a ~ 9 ~
A *ompromhe M w s slightly s b r t d r q U p p r m d l o w e ~ c ~ w h i I e
balance m the prdrwive positioa ma). not be sible, &hgh it can be whiwed in the 4 occiusims. Protmivu b h c e is l e ~ impn than b W balance because incisionis pesfal c ~ i o t t s l y , The paw can contml the am md drectim of b e rapplied When b i food. On theothrnhd, chewingis done a t r co&ous l e d . P s t i m ~ do not think d

-ant and &&tion of the force they apply. they c a t protect ~ l y e s
wwLd &l* their delmms. p i h e for W d , O C L I ~ ~ ~
b ~ b e ~ s o ~ ~ ~ r i O r E a & ~ ~ c t a t ; $ w ~ t i n w t h t ~ u p p e ~ d l o w o r ~ ~ a r e !@ to end I R v e n w h e n ~ v w t i d m e r l a p o f t h e ~ ~ ~ ~ b e ~ f o r p r o p e r ~ $ t h e I ~ ~ ~ s b w l d n o t b e i n ~
1E the pstaiur teeth rn in CO (Figure 18.74). cmwtwin eventudly cause aces8 pressum occIusi011 of fhe $nkrior teeth when the mid-
14 ridges mmb and th vertical dimmi011 of *ion is decreased. &ce&e fmcu m d y
h ?
~ t b e € Q l e t a t & b y t h e m ~ r i ~ ~ p a r t o f t h e ~
lb74 O@posinpanteriot teeth should th ~ w h ? n t h e ~ r t e t h are in mtricocdusion.
u d r i d g e s a n d w t H I i b l y ~ ~ m o + tion of bone md dw&pn&t of- lhtm in this region.
PATENT ACCEPTANCE OF THE ARRANGEMENT OF ANTERIOR TEETH Fatimts must given the qpmt&y to, obrserve and approve the final ~~t of* W o r teeth tat the try-in appointment. The denhm s h d d n a t b e e ~ m p I s t e d u n t i l ~ & ~ E v e n w b m @ ~ * ~ t t b e y " b o n 9 t ~ h m t h e i r ~ l o o k , " t h e y m u s t b e ~ ~ ~ t y m ~ ~ m * - w + ~ T h e B e p a t i e n t s & ~ ~ ~ C e d n e d w i t B t f i e i r ~ c u w h ~ ~ ~ w e a r t h e ~ . ~ t s s k o u L d n a b b ~ t t o d t o o b ~ t h e i r i a i ~ i n t h e m m t h ~ t h e ~ t i s s a M d ~ t h e c o ~ h ~ i t ~ c m h d . m ~ w b k & e ~ m h f ~ ~ a n d t b ~ 1 1 2 ~ d e n t x m ~ d m d d b G8med to appmhate the Fmal fQm. Zlaitierl madions of patie* can be I m g b h g , and an ~~ reaction to a p d d y e o m p M ~ 0 f ~ ~ r n ~ ~ ~ - probIemsm-thefiarrl-af* dentum i s ~ ~ ~ ~ t y 4
Bemwehdentwa will k seen- oftenby otbr p p l e during norrmrl C Q n v d o n , patie& a h w t d & S t o ~ ~ h i n ~ d ~ ~ p & & i s ~ d 3 t o 4 f o e t ( l b 1.3m)in b n t o f a ~ ~ w i t h t b c k h l ~ i u t 3 1 e mouth md @en the oppo*v to o h e m the d e n t l m s ~ h ~ 0 n d U apmsion. The d m at U s time can be &cd to the eventual m of the b t u m , so this p h a s e m u s t n o t . h e d o n e ~ y m ~ . T h e ~ ~ t ~ u l d b ~ d t a ~ d o n g t b e m m t c r i t i d ~ ~ o r ~ ~ ~ i n d u a t i n g t h ~ o f t f r e ~ . ~
I'hedenthtshodd 1 ~ ~ b d l ~ - ~ t s ~ b y ~ p a t r e n e ~ d n e v e r ~ ~ s r f ~ ~ ~ m o f n o ~ ~ ~ t b a t h p a t i r n m a y ~ ~ c a n b ~ Howwet; other suggmtions may notbe &vis&le, a a d i t d k ~ b e x p w W * m M anatomidly feasible and wautd pwent tbet m w c l m i a t b e c h e e h a n d Q w h ~ ~ the face. Many paii&& will be pleasad with Xbs

- ,,,
?m Three WaPtWmOf the k h t u b Went fabrimhn of Cwn* htur is
T S 7 1 Went's s#atement of sathhctim with the amngmmt of artifidal re&.
reqae& *, ,ifany, ~ b ~ ~ P & Y the artificial tgeta! teeth
w-M&m-d**-* ~ i s ~ p o h a v e t 6 0 ~ ~ a ~ ~ t ~ will b iat the ptient$ c b t Ipm 18-75),
? % ~ t ~ t h & ~ ~ t ~ e ~ ~ w a t a w i l l c ~ ~ ~ ~ t y ~ n o l E ~ t o u i m P h e ~ w h i l e ~ ~ ~ m ~ t 3 a e ~ ~ w e r e m t b *

beech Considerations with Complete
or^^^
basic lmdqmnd facton we bribed to provide ~~~~
by the fabrication and wearing of ~mptete ~~.

-*a 19-1 khmatic piare of the d M n t w h d arkiculators.
NEURUPHYSiOLQGKAL BACKGROUND A v e r y ~ r r n d ~ * ~ t o o d ~ ~ 1 ~ ~ g ~ h ~ d m A @ & o f d - - h-3(iade and&mtWic) are W v e d k i 4 ~ ~ ~ T k e f Q P e d l ~ ~ n t i c ~ ~ m m e o r I e s a , h w e a a M ~ o n zpech @mmm bemuse E Amber of ~ ~ a T i l l b ~ ~
Qmth pwktioa includes huge numbers d ~ m Q t ~ l i c t s r p r o - of 12 to 16 per
~ i a - * ~ W O r , ~ a r t o ~ ~ ~ h * ~ * * ~ f ' l e a a t & a r t " * b h---iuthefieldIt h a a k h y - & a m d a l ~ - - t ~ f o r ~ ~ ~ o f ~ m ~ ~ autOm&c* ume aw- speech ooukol l ! m m w I ~ i n ~ ~ & m t h e
peGhI3 mtlva- dm p y d d a l
~ ~ ~ t h e p l i m a r y m h . s t i & ~ h ~ , * m mpl& fully €be lrwcha- ~ ~ t f h e a t ~ r @ d l y o e ~ ~ t s I
~ ~ a ~ ~ ~ d l e i n ~ c o n t r o l n f ~ ~ f m m , i n c l ~ ~ ~ ~
SPEECH PRODUCTION AND THE OF TEFM AND OTHER ORAL STRUCTURES
B ~ e ~ ~ o n c a n b u s e d a s ~ to position df~d te&, it is ncwasary

Q p t a r . ~ 9 ~ ~ m w i t h ~ - ~ 8sl
Ustenet
Figurc 19-2 Speech production and communication,
T£~sow& b, p,;W:m & made b cmmt &th ~ . b a b a n d p , ~ a i r ~ h w u p ~ w


CkPpaw19 5 p m R c o n s i d d m w k h G w n p l e k ~
m i m ~ w i t h o r w i ~ r v d o e ~ f r o m & e l o w e r t w t b d u r i n g s p d , h W ~ r i o r ~ a x o ~ ~ l y ~ * ~ i a l % l ; a ~ I f , o n ~ ~ ~ ~ d ' t f w ~
. ~ Q f ~ l ~ ~ ~ m ~ j t l ~ rn~mmbmteo£thehmllp~~if&e&W ~ p ~ ~ ~ ~ i ~ ~ m , ~ ~ ~ d m p r o ~ t a o f r # F o r w a P d , d ~ ~ ~ ~ u p g e t W ~ ~ ~ f a r ~
I f t h e u p p e r ~ ~ a r e s e t t w h r b d m t t m w & , * d - & ~ & o f h ~ l i p ~ f # d * m m ~ m m a g r ~ ~ f l ~ ~ ~ w a r e m F a x ~
FOgura 19-3 Effm of tooth @onin$ on fand v. A, Uppw antetior teeth too long, wringthe pmundatioh af f, they MI cantact the loww lip in a p w M slmlar to v, and the sau& may w n d alike. 8, ofarrtepoposWh p&idonhgeS.theted~ hwn M right are fomd, too far posterior, and antah?,

the mglw akn& out lx?hvmn the teeth when ~ ~ ~ m ~ , t h e ~ ~ p r o b a b l y t o o &k&.
U n p a h l a r S~unds Alwk mmds Ce.g., t, d, s z, u, and J) ate mada w & t h e v a l . ~ e f m e B b y ~ o f t h e t i p o f t h e but tagu6withhm08t anterior part of t h e p b (the ~ P ~ ~ Q J w ) w the h g d side of the atmior teettr. The sibilants @arp sounds) s, z, ah, ch, and j (with
M o r e ~ a f a i l u r e o f t h e ~ e d g e ~ t o approach m d y end ?a d h k i e s a pom'ble 3. Thetuqwrlarslrmiaflat. e m r i n ~ ~ o f h ~ ~ o f t h e a n t e - 4. Mmmdy, tbe mdMe will move *teeth (Pigum 19-5). This test wil l rwal the m m andupward, withthe teethalmstin
Figure 'f9.4 Vertical length of the anterior teeth during sibilant production from left to right are correct, excessive, and inadequate vertical overlap.

~ ~ ~ s p m t i ~ i o n s ~ m p l t a t ~ s5
1Y-6 HwimQl relatiah crf the antefir t&h during dbilimt @mdu&n Imm I& to rOgOrt are mnwt, ~~ a& d&mt owlapping.
€ h ~ € m M h q u d @ . F ~ r ~ Z a ~ i f i b d p a f i h ~ 1. The m n p a d d y t o u & S * ~ m ~ w H a b *
-swnd-is b p d r a m d i ~ w * ~ ~ p ~ ~ ~ --nsh--w-Witb w @ h - ( h i s d & h u , b 'stespmnnoffaf*M'b4- dew -t$s 4 .smdynsmioa a
dm--
I I 1. T h e ~ L f & t l y h t d , ~ a ~ ~ i - 1 wl-le. lhgrnmhtd @OA B1grrow& W&
MmflUOS FOR SPEECH WBtS

3W pprt W Wbilitation of the Edenhlorrs Writ: Fabrication d Cornptete mtum
tain difficulties in
~ & ~ ~ p o s i ~ d ~ . A mnm;Bsad~~areverqrexclusiveandftot ~ ~ ~ ~ ~ o ~ , ~ as & d i e , may have desirable side ~ B m - I Q i ~ f o r ~ o n S o f ~ ~ farxW--w=h-andamap- p @ d & - d b e & & p ~ l % ) .
~ s f ~ ~ i $ , ~ r d m e d ~ ~ h ~ ~ ~ e W x a t t t e r ~ ~ f a i t s r e 0 f
m e r t n s ~ ~ a n ~ ~ A prudent way to cwercome p Iems L to study fhe profile f m aud lip
PROSWETIC CONSIDERATIONS
~ ~ ~ a a c t i m y ~ a , a n d ~ - fomasimpIedtorytestmig6th~fulinsuch ~ ~ ~ a p r o p e r d i ~ . I t a I s o h ~ - ~ - t o ~ t o a n d ~ ~ m ~ ' ~ h m ~ d s ~ ~ ~ ~ a u d ~ m o r e i m p D r -
~ m a y d f m m t h e o r a l r e h b i l M ~ 1 wtmdqas l rdmak
Figure 19-6 Typical eledropatatography diagrams for the sounds in oh sadist. Shaded area represents the contact between tongue and palate. Note the sagittal groove created when the s sound is uttered.

1. IfttaepatWhwapviouswmpWW- w e ~ , ~ * m * * t b d d m e p&le&&c#f- he&#$& h n . l f , m ~ o t h e r o t h e r a ~ ~ ~ i s t Q b e ~ ~ s r ~ l & e d c a t x m , r ~ o f ~ ~ @ d m d t b e d ~ t o t h e & ~ &a&w-
2 . 1 . h t e n ~ ~ p a t h d t h ~ t r y t Q p r o - d w B * v 4 q ~ ~ m F m d y o a r s e i f . Qbemthepsifionofyourmeai& tory s l m t w s , -@=, -1% s 0 ~ ~ ~ ~ s o x r n d d ~ -
' f o r m ~ t o ~ ~ f ~ ~ ~ ~ B l e ~ i d e n t i q r t b e ~ ~ a m m c t ~ p m d W m . .
3. Make b m a t r y M~ soff- might be MpfuI*
4. H e the paticnta bearing &&e& h d- ttJry deficit will prolong the a&p&b period and n d r it mom M1col.t.
5. Jfthenpmd&&vedprobh-b mlved by dental methods, the patid tlbwld be ref& ta a tpmh p b W s L


I Waxing and Processing the Dentures, Their Insertion, and Follow-up
I Rhonda F. Jacob, George A. Zarb, Charles L. Bolender
SECTION I: WAXING AND PRT)TF<<INT. THF DFNTI IRFC I
I WAXING AND POLISHING SURFACES M e principal s d c e s are involved in the fun* t i d stability of dentures: the basal or impmion antrface (offen called the intaglio surface), the mhsd d a c e of the teeth, and the polished sur-
The latter is defined by the width of the bor- dm, the bmolingual position of the t&h, and the fullness ghem the wax to obtain ~anvexity or con- cavity both facially and lingualiya These three sur- i b s of the denture are: positioned in harmony with facial form and the wtomy rand physiological mmments of the tissues and muscles of the o d why. Apppriate positiun of the Wtim and wrrxing of the polished surface contourn and bods hichess should be determined at the try-in appointment. This will give the patient and the den- & ?he qqmdmity to evaluate &tics, phonetics, &d canfort. Ided position of the prosthetic denti- ~ h a s ~ ~ g ~ ~ ~ s e d i n p r e u i o w c h a p k m , b u t t & ahpterdismssesthedetaiIsofthef~fwmofthe polished surface as it relates to wbieving optimal phonetics and enhmced stability and retention.
The form of the polished surfaces of a denture hfhmcm its stabiiity and retentive quality. In &ition, it influences dentwe ~thetics. The den- hue bases between h e teeth and the border should b e ~ i n s u c h a ~ m a s t o a i d m t e n t i o n b y tlie mahmicd directional forces of the m l e s tad t imes . Generally slpe.ahg the contours are W on the buccal aspect of the denture but are
became of the! f u n c t i d and "at reat" space requhmmts of the tongue.
Because the mandibular denture m l y whims the desired retention and has a limited e h e area compared with the m a x j h y denture, the tongue and chwk muscles can eacsdy dislodge it. Muscles of the cheek and tmgue ~~B the extend denhlre surface and wrert f o m on the lsrteral inclined plmm of the dentition and the polished surfaces. Figure 15-1 suggests ation of the cheek and tongue in gripping a bolus of food This action may be described by tha illustration of a patient chewing a small grape, with the tongue d cheek holding the grape in place wer the o(;cld su- faces of the teeth while dosing pmure b exert& on it. In addition, s horimntal force is wrerted along tbe o~clwal plane by the tongue aad cheek.
A frrrtber study of Figure 15-1 suggests these rnwcular forces on the inclined planes of the pol- ished surfaces dmt can serve as a mechamid aid or a ddmmt to retention. For instance, when the lin- gual and buccal borders of a mandibular denture arubehgshaped,theycanbe~concavetocon- form to the tongue and check so their muscles wilI g r i p a n d t ~ d t o ~ t b e d e n t u r e . h ~ % ~ t e situation in wfricb tJle lhgud and buccal mfb asemdeconvexbeyondtfiedlnesofthelmt&, the inclined p b f m w resulting from presslaes o f t h e t # g u e a t t d e h e k s w i l t t e n d t o ~ t h e ~ - ture. The correct b u c c o ~ position of the teeth is h p m n t because hknd forces are also ewrkd on the Wtiw during function. Teeth pmitiod t o o b u o c & y m t o o ~ t y d a w ~ m ~ of &the cheek or tongue to create unfammbIe f o m on the inclined plane of the surface of the taeth and the polihed denhue. These forces will tend ta

face, known as the anatomical portion, f o d in such s way as to lose none o

A B C D m1 e and B, The amount of wax to be added. C and D, The mrpect redudon b
enhance both stability and esthetic result
d b a r d e r w i d t h o f t h e ~ s i ( ~ f l h ~ ~ d ~ h t e m k i ! 5 & p n h ~ & W ~ - ~ o f t h @ ~ a n d ~ ~ ~ ~ Q ~ t f r e o r a O i c a l o Q l l a r s o f t h e ~ T h ~ i & a t b & t u i r ~ b r ~ o f t h e a s t ~ i g u r e 2&1),rrndthen&edeadofalenifeisheIdata 45-d$$m*totbedoofh&tOfm& wax &dd lmrgh (Figm 20-2). Care W d b ~ t o ~ ~ ~ 1 ~ c l i a i d crownofthe b ism. This &a to the &hetics because most adult m t k d dentition m v d s the teeth to the -1 jmctiuri (CEJ). A h , the less mylit; mitt tht is visible around t h ~ teeth, the zmru d tbe appearanoe b. The common ten- ~ i s ~ c u t t h e l i n e t o o s t r a i g h t f b m i n ~ - M b i n t e q m h d , n o t l e a v i n g ~ m i n
-re 20-2 The angle at which the wax knife , h u l d be held for cutting the gingival line.
the* ' ?3pa#$~203) .TBiswi l l the W datum, nuking them
W W + I ~ ~ ~ B E s m f l t o b a ~ . o f w a ~ d m g t h e ~ ~ B P d ~ t o ~ ~ a o o m p h t e v h v a f ~ m € h ~ h p s s i ' b l e , l k h g u k ~ ~ h ~ r t s t a ~ ~ b t e ~ a n d ~ o n ~ f ~ ~ i n d i ~ t i o n s , m ~ o n g ~ i t i a r ~ i n ~ d ~ t h e r o o t o f r h t ~ ~ i s l h l ~ ~ r o o t ~ f ~ h ~ i n c i 8 0 r i ! & t b ~ ~ t h e r o o t o f t h e c e n - tral incisor is a length b - t h e s e bwo (pigum 204 and2015), O n t b e m a r d b d a t ~ t h 1 . w t o f t h e e r r n i u e i s t h c I ~ t , t h e ~ o f ~ Ixmkd ~ r h ~ s h o ~ a n d t h e ~ o f t h u ~ ~ m r i s b e t m m t h e s u t w o C T h e ~ i s s ~ o u t o f ~ ~ ~ , ~ ~ t h e r o o C Mcatians gpiu becMne manifest (Fignre 206). The sharp and mugh iodi~ations are now rounded with a large scrap ad the s m (Figure 20-7). T h e y W d n o t b e ~ d ,
Figure 20-3 Gingival linecutwiththe ptopw contour. The dotted line shows incorrect cutting.

F b r 0 Z4M A, Rsat indidam on the 51 wmurof the giagiwl fine.
The hgual ~ u l f & x af tbe muldibulzlr denture m r t y b e m a d e d i @ t f y c ~ w i t h t ~ the depth afthe ~ ~ ~ l w i t f u n d e r $ l e h g l d d a m of the bth. A projection of ths moth beyond the ~ & a c e a & w a n ~ ~ i n t o w h i c h t h e ~ b ~ ~ I l s f i p , ~ b y c ~ g t h e d e e -
, B, mntinwi gingival prominences. C,
he^^^^^
RXWAT~ON AND PREPAMnON WE AQOlD

Figure 20-6 Preliminary removal oi wax from between the root indication lines (arrows).
' often taken during the investing procedure to allow the multiple portions of the sto~le mold to ''fdll
apart" during deflasking. 'This offcrs case in deflaskmg the denhlre and decreases the risk of fracturing the denture or teeth during removal nf the denture frotn the flask (divesting). Thcsc optional steps are described as such.
The denture with nlastcr cast is placed in the flask to establish its height in rclation to the height of the drag of the flask (Figurc 20-1 1 ). The cope of the flask is placcd in position to ensure that the tccth do not projcct beyond the top of the flask.
Ideally. approximately to '/4 inch ( 3 to ti mm) of space should be available between the occlusal sur- face of the teeth and the top of thc flask. If thc tecth are too high, the cast must bu rcduccd in thickness. The artificial rim of the cast (land arca) should be flush with the drag of thc flask to prcvent possible breakage of thc caat in latcr separation 01-the two halves of thc flask (Figure 20- 12).
Thc distal cnds of thc lower cast may be high in relation to thc rcnlaindcr of the cast and extend closc to the posterior edge of the flask. This condl- tion causes the distal ends of the cast to be at an
I Figure 20-7 Depressions between the root ind~cation lines (arrows) that will be smoothed with the wax spatula.

3% h r t T h m WWnDR of the edeRtubus Patient: Fa13rira*n d Dm?ures
- - Filplre A, Proper form of the lingual polished surface contour. B, Position of the tongue retative to the lingual surfam of the denture base is accommodated In the concavity . designed in the denture's lingual polished surface.
~ # a g b t @ o _ * o f & 4 a r a B E , m t h a w t m h a r e ~ h O . g e w h f b f k s k i s d m w b * * M e m
- ~ o f ~ e 4 t e , a n d ~ t p 9 ~ ~ f w i s ~ i n ~ T h t ~ ~
narural mi ur ute pauern s wngue.
Flgurq 20-9 The normal lingual contour of ieznl incisor is reertabliad it artificial posterior teeth is established during the This particular contour will aid pfionetit . . =- - I - &L . .. .-I-.- waxing procedure.

p m ~ l r - 4 1 T4eIoweavraxdenWwfr;zrtteraand cast in the bottom half d the tower flask W i n g the posterior height of the land area can reduce tho Lr of creating an undercut in this area when investing emst.
mt~.ThenamixofwWcidstoneLppured ~ a o ~ I e r r e l a f d w ~ d g e s o f t h e r m x e r i a r * a r s d f h e t t p s o f f b e u l s p s o f ~ ~ ~ igmm 2bl5). Tha a p e d i~ painted with ~ ~ u r n , ~ f l a ! & i s ~ ~ m kdfattificipJsbnqendhcqdtheBa&isetin
C 0 *re 20-12 First half of flaking of the maxillary trial denture, A, Cast too high in a m I and 2. %, Areas I and 2 at a fwomble level. C, Areas I and 2 shouM k kveld. D, Areas 3 and 4 to be beveled.

I
5 1
-, ,
-YS '- M u m appfid WMI a a m d Wbrd~m'W expobatSstone'of the tad.
W#u with a camel hair brush (Eigm 20-26). T h e ~ ~ m ~ n o t ~ e i n o o a t a c t w i t h t h e ~ ~ p o ~ i L 1 t h e m o l d a r o u n d ~ ~ . I t ~ ~ t a d r y , d a ~ & i s ~ t e d o n t h e insib offbemold The flaskis allowed to cml to room tqmahm. When acrylic resin teeth m used, & e ~ ~ o f ~ ~ m u s t b e ~ o f w a x 0 r n B ~ ~ m d s t t r j o t h e r d e b r i s . W ~ on i&e teeth is the main cam far adhesive failure.
Flgure2P14 Labial, buccal,andlingualmres with V-shaped grooves coated with a separating - medium.
PACKING THE MOLD


should extrude from the entire periphery of the denture. If it does not extrude on the first pressing, that area requim the addition of more dough. Trial packing with excess removal should continue until no more flash appears.
PRESERVING THE OR1 ENTATION RELATIONS D e m is usually carefully completed with an air chisel, d the processed dentures are Iefl on the casts. The casts and dentures are returned to the mountings w the artidator, and the processing changes are observed. UsualIy the change is noted by obsadng the occlusal pin on the anterior guid- ancephfatform~isoReainthe&oflto2 mm. h o r processmg changes are usually wr- Sf.EAPlM& AND WMINQ 'F)IE rected at this time. However, new intaocclusaf

Chapter EO Waxing and Ptmdng the Denrurs, Their Indon, and Fdlowup
Figure 20-19 A, The upper cast and p m m e d upper denture are returned to the articutator mounting and attached with sticky wax. The remounting jig is positioned on the lower memkr of the articulator. I, The upper denture is dosed into the plaster on the remounting jig so the ocdusal surfaces of the teeth will make an imprint in plaster. This will permit the denture, after removal from the artificial stone cast, to be repositioned in proper relation to the upper member of the articulator.


w m Waxing and Proceging the i M t m s , Thdr Irrw~h , and m p 4Ul
SECTION II: DELIVERY OF THE COMPLETED DENTURES
1TlQUlNG THE FINISHED ,.m b e moment new dentures rn placed in a &tienth mouth, dl af the procedures involved in
construction are subject to review and -WaMw. Tbe choice of materials, the techni- :#d agd c E c d e&&veness of procedures wd, ~ W t b ; e ~ i n ~ r r u t t h e p m ~ s r t r e wed to three 4untions. These are by the :&nth who rendered the service, &c patients ~ a m t o u m t B e d e n ~ s , & t f i e ~ & m d fhmdy of the patients who will be viewing the *tures.
Bvddms made by Qentists should be the most did because these mu the profession& d o bow th potentialities and limitations irl the treat- ineat of the patiant. Dunti& must r e q a i m &!?+ & d e a in the pmthodontic d c e pmvidrd hnw of % h e may become mdfmt at deliyery, iBld smm! may become evident rttaing fop~w-up ~wn%batim. E dantists nd hwldgmble
the type of obamatims that should be'made dmaotdidofthe r d of tbe tmtmnt,
am not md&g a truly profes~iod V c e . E*-findmmtbat*tArDuId ~ e i n ~ ~ s a m e p a ~ t a g a i n w i t h c o m - ~ ~ t h e y a m a o t b e i n g ~ & d a f t M r m ~ a s t h ~ s b ~ b e . n % ~ ~ o f ~ u f ~ ~ d o d l t i c ~ c ~ ~ r n a c x m ~ $bt vigilanoe and mIf-#b@line, A critical Wu- ~bythedent i s to fep .erypthodont5c~ce ~ w i l I t e n d t a w a r d a c ~ t ~ ~ t ofthi? MxviGe.
ktknts* evaluations bf- their new dentures are p m l l y made in two phases. The fht is the e o n to tbe completed dentares whm they are &st p k d in their mouth. This can range from enthusiastic acceptance to fear and apprehension,
The patient's frame of mind will depeJPd on the &tist's t m p h g the patient's t i m , b n t i t q b e & c t e d b y ~ e x p d - e n c e s i n Q o n h r e ~ t t a d b y c ~ o f der people. If dqu& dia-s m t e ma& bfore any treatment wws s b r t d all rnkmq- tims and -kmumte information should haw been d i d LimiWioas in h t u r e war as a result of the plttkmt'g pmtkalat anatomy and function d l have been It is m y important to spend m u a t e time at the try-in appointment to avoid patient diswthbztion at insertion. If codidma cannot be d snd established before the day the den- are placed in the mouth, the merit after thhi time will be more complicated. Skilled practitioners will have dermon&rated to their patients that they are treating them profesdoady and that they h e used the utmost care in the clinical and technical procadum inwived in fabricating their dentures,
Friends' Ewluutio~~ When patients leave the dental office with their n w de-, it ia generally with mixed m o t h a . They want thek friend^ b notice h i r h p m 4 V e ; they hop^ heir friends aad mMws wil l complrment: 'them and d m their pigment m d c h o b o f ~ d ~ e y ~ w o n d w h o w ~ w i l l ~ ~ & g a n d s p e a l a r t g . L f p ple comment a h t the new teeth, some patients mayw*iftheteeth, I ~ k ~ ifthey donot ~ ~ * p a p m t s m 8 y ~ i f ~ ~ ~ ~ a r e j u s t ~ W T b e d ~ ~ ~ ~ ~ notbeaccmttu .Fr i&cap lnot~bPw~den- tum feel. Tfaey cannot judge the effichq of the d m t u r e s i n ~ m l ~ . T h u y ~ ~ ~ ~ ~ e s ~ ~ ~ t h e b ~ ~ t ~ offhepoor ~ d ~ o a ~ o a s n a r t mdmtand tbe p i b l e lack of cmd&mn
. . dtbd ~ m o r i n ~ ~ f ~ p a t i ~ i n ~ inp to foliow h t r d o n s or to use the dmtms. The patients themselves may mugdm these d i E 1 c u l t i e s a s ~ W m ~ ~ , ~ ~ a o r ~ t - mmts of f r i d may causa them to bkame the den- tist for proMenzg that may been byold the dentist's conW1. Such wll-mmixlg & i d s can add to a patient's difficulties bemuse b y have

*--w@a-sagpmb@ p t k m t b Y * ~ ~ - p n p ~ A u t d ~ E M ~ ~ ~ ~ ~ f r ~ ~ t o ~ t h e W S 9 4 6 ~ ~ W ~ ~ k ~ i t J h m X L ~ ~ h 8 ~ ~ i n g a a e d t t h d t % ~ ~ t t ~ t i m e ~ h i s m a d e . ~ ~ ~ o f a ~ b ~ ~ ~ f r i a d m a i E l ~ t f B e ~ a t f i e t i y - i n o r h & g ~ p m m ~ ~ & e m m ? y ~ ~ ~ ~ b e v # y h % t p f u l .
TREATMENT AT THE TIME OF DENTURE 1NSERTlOM m e ~ ~ t s d m l ~ ~ s t h a t ~ k & e d o u t b ~ m a ~ W ~ tic d m . lmwmcia in the mt&h and f l m ~ s when the dentures are trimmed a d m ~ ~ d t o g & t h e d e n ~ s b ~ ~ g e m t ba reco@zd and e h h k d befm the p & n m m m h b ~ ~ . ' X 2 r e ~ ~ be the result of (1) technical mm or BRYKP~ in judgment made by tho dentist, (2) technical errors M o p e d in the labaratory, or (3) Wmnt defi- ciencies of the materials used ir! the fbricathn of thedmIm3.
1- the patient should be instruct& to kmq my pdm dentma out of the mouth far 12 ta 24 ham immediately before the insertion ttpphbnmt. TI& is assentid if the new denims s c l e b k ~ s n h ~ ~ t l x l & ~ t i s - ~ . E f t b ~ ~ ~ ~ h g & ~ d b y u l d ~ ~ * ~ ~ t m e s ~ n o t ~ ~ B c t l y , ~ ~ ~ f i t ~ ~ . ~ s e a t i n g d d m - innthin ~ t & t t t ~ ~ ~ & # ~ ~ f rantbe cmasia&Wmwfit&&dnetexistifatie t i s a m d & a d r Mjwtmlts of Of fypc madeatthis att this tirras,*h-wdw-irrepm* ~ e ~ t o ~ ~ . T & ~ ~ n i s p r e d i ~ CaM on the lqlwmt dl&? the patient be ~ a n y ~ f t ~ 1 4 l m a r s ~ ~ *Jto**hW*W~tbeftnal ~ i o m m &.
h m m d d h ~ 18,18,ptimSwil$ A R d ~ ~ ~ 1 a u t d r w m o u t h f o t I 2 o 2 4 ~ a a ~ ~ . P L n ~ ~ l e
witb a ssff ?empomy r W e d to mhitnhe time adjustments s h d d be d e d i ~ ~ . with the wc lud

Hgum -23 ' A, The premutk spots h Wre 20-22 havq bm apfully relieyed with a m 8 mnd bur. A rnlnlmum of denture base d d was ntpovd* 6, The w d y uYIBe&ut we9bTh~m&rl&hngem&Zleca&l~&disctosedm~~phWy&W- naI w e t t d d t e priw. Each ~ S t r ~ bemkktted it&pendmw9s mot todiskltb r w ~ i a c e ~ ~ o n i ~ o n , ~ ~ ~ s h a t r l d b e ~ i g k t l r l . ~ & ~ ~ * ~ w t h i s a m h w e W ~ r e m k ~ t o m w e W ~ . T h h thin lingual muma surfare b very wtnerak to ukwdtion with denture ttmmmt


the^
acGumb1- - w b d cq-or*---F ~~~,~~~~ cl-by*p&m ~ C = ~ t l M f r o t n ~ ~ ~ . M & * s d & i w ~ ~ t a * ~ ~ t ; o paper^^^^^ the amount of error in &a uc~lusim. Ordudmi ~ 9 t e i ~ ~ l a x m d ~ w h m the den'tures we 1 c ~ ~ I y mounte$ iP1 th ardmdatur.
INTEROCCLUSAL RECORDS FOR REMOUNTING DENTURES



*M a u l a r denture with the d e d is ~~ on and ar mounting airst with sticky
w;slt Th&MlIzrry dehtuie has pwbnly W S H ~ OR &e upper member of the areitulatot Wiph *'- i m k fsek Figure Z&W) and mted to ~ - r w i a t r - s t ~ . ~
Figure Z&33 The maxillary teeth are secured to th wax index with a drop of sticky wax in the canine and second molar areas and secured with fast-setting plaster,#
VERIFYING CENTRIC RELATION The CR record should be verified for a c a m q before any tooth adjustments. The Aluwax is @, and the CR recording is repeated. After chilling ad drying of the wax record, the dentures are r e m d to the articulator, With the articulator locked in the maxillary te& should fit precisely into the & wax record (Figure 20-34). If all the teeth simultaneously into the wax record, the mounting$ correct. If the opposing teeth do not fit exactly iaQo the indentations in the new record, either the rial mounting was incorrect, or the patient gave&-: incorrect relation when making second mod Tt :

LA*

Fi@m 2fMt6 Articulating paper marks made in centdc &&ion show interceptive or deflective mlusal mnm'in centric occlusian. Grinding should be done onty in fwure and not on cusps.
d exumim. 4 % i b & % c R ~ ~
tlae pin is pl& in mwt with ~ l e d i s k e p t i n c m t a c t ~ u t t h e ~
2&38). Care bbkmnoi to grind on wo& * m * ~ W m w o ~ @ s ~ a n e r e ~ ~ C B

-38 Artiutlating paper is usml to locate w otdu4at cantacts in ieft lateral acdtlsion, IlDZ
Wee the position of the incisal wide pin, which has LWM fm movement d the atticulator into a left d n g position.
EO-40 The atTimlator is moved behvetn right lateral Md& and centric occluolon, whb articulating paper bdwm the t&h to locate deflective d u a l contacts in the lateral m r d o h . Notice tht ~ W m n of the ph on the Indsal guidance table.
as marmy as eight erram in excursive nmvments. The qp~ of htmeptive m1d contacts and the n- adjwtmmb are depicted in F i i 2042 h u g h 204. In most W c e s the h t e d move- ment of the incisal@& pin need not exceed 3 mm. This mmt of faberrrl movmmt usualty moves the ~ ~ ~ ~ t ~ g p t i P Q i n s a e n d ~ ~ ~ a n d m e e E B b W o n a l ~ o f ~ P s f t i & .
hamuch as denture Wth am fastmed togettier asamit , i t i s~ ibbbrei ievethecentr icm- tact of the four incisor$. This relief may be made at the time of s m r ~ the teeth, which will permit
. -39 Ma* on the buccal cusps of the , m*I lary &cth and the lingual cusps of the mandibutar Mposteriw teeth indiatte contacks in left lateral -on. These wrlam are ground to dewlop
I . m h contacts, The lingual cusps of maxillary teeth a the bucal cusps of mandibular teeth are not ,#mud, even though they shmv marks from the athxlating paper.
the of lt verticd-mrb without inmash t j ~ h e i d guide angle. D q d h g w rhe amount of a n t e r i o r ~ ~ , i t w i l l o f t e n l b e ~ t o ~ w t t i e p d a ~ ~ o f t h e ~ ~ and the lea@ and cuspal hcha of the d i c a n i n e s a n d I n c i a K l r s . I n ~ v e ~ d ~ sive c m h d s in the anterim area must be eliminsfea The dice o f t o o ~ ~ ~ i ! 3 ~ 8 * ~ p w w t t K ~ ~ a a t e r i o r t e e ~ ~ a o a e ~ cornpromhe mturillary estheti~, ahtmgh bid w e a t p a ~ o n t h e m r n x i t l a p y ~ O r & e t h ~ k v a y ~ ~ g * ~ d e n t i s t z n q ~ ~ o make anterior djus4men& on h t h &.

Hgum M Cmection of wmrs on the d r r g Mee S h q m interfering as indicated by the shaded weas A, Buccdl and lingmi cusps too Icng. & Weal cusp Mo long. C, Lingual cusps ha long.



mmm= ~ ~ ~ l l R t R e s r r t l ~ ~ ~ ~ ~ W 1 A . 1 . I I
& ~ k ~ B , ~ b i c ~ ~ , ~ I a d U ~ g u a i ~ ~ n n s l & R l g h t ~ i . 1
dusiefi, MI stnd lingual views. Mtke in the li@ h bhwe has b E e n ~ , . i a .- tk m&r w b n . E PmBwh mUnn, Here, multiple W-w%mw& l a m ~ ~ @ ,
t h stwe of the cgrnpwtxtting a m F, In {hi dinial W n@&e the uni64neiaf aotscts amkWsM an the articubtor w, tdor phobgnphs of thii pathtam in Plate lB1,pkF.

krP RehaMlitatjon of the Edentulous Patlent F a M d o n Of tompeclr Denture

~ w k f ~ ~ m a s t i ~ L M ~ o a ~ l e ~ o f f o o d w r c h u ~ m f t ~ w ~ m w t d t b t n o ~ W d b e ~ t@ nmtiaite mom &mIt GodiR Filsbm den- t t m 3 - - b € t M w e & t f & M r q u i r e l i t t l e d & b t r t & o * t h & t a i e ~ b r ~ w i t h e ~ I e ~ o f & e ~ ~ t h e ~ a t e . ~ m g i V t ~ ~ e n b d - h c e in stabilizing &e dentures. Ah, ckrring the l ~ g p a i o d , ~ ~ a d ~ b o m i d ~ - ~ ~ a b y ~ w ~ u f ~ ~ ~ h ~ ~ b e m ~ i n ~ ~ ~ o f ~ g a n d ~ l e t a ~ ~ ~ ~ t , ~ b u t m i ~ ~ j o h d n g ~ d ~ ~ ~ & t h a ~ a o e ~ ~ l ~ a p a t i m t b ~ ~ - ~ ~ ~ t t b e ~ , d t h i a ~ h ~ i n ~ ~ ~ t h e d e & t ~ t h e lkltuR%.
Wbea biting with ckmhm, patients &odd km ~ ~ p l a c e ~ f d ~ t t a e i r c e e t h towad the comers of the moubh, rather ~ t h e a n s e r i o r ~ T b n t h t ~ ~ a l d b e p w h d i a W a s d ~ t o W i t a p & r a t b e r ~ d ~ ~ m d ~ m ~ ~ $ e ~ i f m ~ w e r e ~ a . ~ d ~ ~ t B Q i a t o W t b e d e n t u m o n ~ ~ i d u d ~ ~ ~ t h s m ~ b ~ .
o c d m d l y , o ~ o u s p&ientB have gone i ~ d e n ~ f o r l o n g @ o d s a r r d ~ l ~ ~ g U s h f m d ~ - t h e d ~ r i ~ ~ p e r - ~ ~ ~ t o m g o a ~ t h e h o l r d ~ ~ . T b ~
I W y &ace in& diffcw in ~ t a ~ ~ n e w d e n t u x e s , ~ ~ t h w f a r a d j ~ w i l l ~ l y b e e x t e n d 9 d .
pngue&sm@mhntmMf~intheddity6fa loroer dWlftyg, prthlarly daring ~~~ ~ ~ w h o s e a O ~ e ~ y ~ i n a ~ pmitim relative to tbe laever anterior && &add ~ m p o ~ t i r n ~ ~ f ~ f ~ ~ ~ a r d s o i t ~ o n ~ l i n g u a d ~ s v f t h e l o w e r ~ f ~ ~ W i l l ~ ~ e ~ a p ~ ~ f o r ~ ~ &amre.
I $pmfing with New D m W m &wtun&ely, thuplobh of speaking with new den- ~ i s m a s d i f f ~ u l t a a l n i g h t b e ~ T h e


SECTION Ill: MAINTAINING THE COMFORT AND HEALTH OF THE ORAL CAVITY IN A REHABILITATED EDENTULOUS PATIENT I

- .
A ~ Q & i m k % . ~ rew h'tb81 $ i a l l i m W
~ ( ~ t l ~ k ~ ~ ~ a . Ledonsinthe mghofihe
'
IiWy due tu mrs in the dus ian that caused the denture base to J t r i and thus impinge rra the rnucwa. A, Sublingual carundes; B, mandibular labia1 hnum.


Hgwm tQ-M Labial notches must k suffidently part of &e maxillary denture and help all deep, with borders that ate rounded and smooth. situation. Them the modeling compoun



.-- . w . w m d a ,aWilk$q QMw Wh.m,the brdw wzss shwfmed to *.appdmm hg€h i-ted by the dotted litre, '&a denture no longer c a d the patient to &a&
,#@gtm -I W w the- Wiknes d the $@t buccal border in the h g b of the bucd notch #mws). The b u d hnurk, rhwing pos teW aver
border &wing bda l @Won, can lomen or ~ a ~ ~ r y ~ ~ n t k a m a n k ~ W n p e t i e n t a h t i k t i n t a & ~ r e m e o n t h e ~ .
SUBSEQUENT OWL EXAMINATIONS JkND TREATMENTS

426 Plrt T ~ L W RehbilWion of the Edentulous Patlent: Fabrication of Complete Dentures
Periodic Recall for Oral &amjfiatlun

1 Sinele Dentures
' t
mMlti& earlier, tlm edmtulow stab can ba I w w i ~ &dent to w absenw ofa ~y pert W I qSdf1c tmrphO1- - ad psy-
I z W f@ipk. This &apm d i m the Ilpht wi& a shgb txhtufow mlt. For such a ; ~ , t h a ~ ~ i s o n e o f a p p r e o i ~ g I:##$ I i o m e G M clifawnc~s inthe s q p r t h g tis- , ~ f o ~ t h e h w ~ ~ a ~ ~ 1 ~ g ~ ~ - @e management prowdms to p d w and -&ahbin t& -tiam nmmmy for long-temx I I ~ w m ~ . ~ n t h i s ~ , a ~ ~ t m t m t &&m1Lbdwmibd
VMGLE EDEHTULOUS ARCH :'Thpm&na of the conditioa in which one eden-
h c W m t a ~ m ~ o o a f m ~ ~ t i m s t b a t ~ ~ t b i h ) ~ i f i c # e n t ~ Q n t o c o m p ~ ~ ~ ~ ~ d l m - e m a l mlpIete demm~. Such an utl*-
~ m o t h s t t r d ~ ~ ~ h k e n r p m & w i n & h k % * e a c e k ~ o f ~ ~ ~ * t h e n a a t r a l b t i b i s w o f * m m p o m t o ~ ~ : w * t h a t ~ e % J r ~ f m c t i o n d ~ , ~ m u c a p e r i o * ~
bap&de of swh favorable adapt&a 1 e m ~ ~ w & ~ o f ~ -
md racial ~ b g 0 9 , ,tb *a@ m p i y , to -- p ~ d e n t u m a s e ~ b ~ ~ ~ ~ ~ appear to b the caw for p ih ts 'w i th T I p r d m e s i n ~ ~ ~ r r p ~ w a r a & be-@--d4c-wbb r e p l & m u m t a f & ~ w ~ ~ q ~ t i m ~ E r r k e # m ~ ~ ~ i n mdmka4==

occm becaw of hngstdbg m m w 0c5;tusd ffma (pigum 214). This eli& a cq nation of mofpiwbgid a d Wal thy ~ p l e , s ~ o o m p I e t t d e n t u r e ~
d&tme f#m the t- to the ridge and the potential for tiithg to rault, &m the lack of . ,I -. . -. ., . . . ..




:&lidon d tornpkc Dentures
c@hniaaccoanpliM at the f d prosthe& inser- t h a&mmat. If, h m a , it is d-ed that &e amral toofh modification that is required to emam a a b l e denaxre pmthesis would result in ~ o f t k ~ a t i d a m t a a h o f t h e ~ ~ i s ~ , ~ s ~ w i t b ~ e ~ # a p & ~ f f t f a e w d ~ ~ p l a n a r i l l b e ~ I t ~ m a y l b o ~ ~ ~ ~ WhpitimB p h €he In&ky@e& t l t * ~ ~ 0ftequired~W reh- t i C m ~ * ~ ~ I f r n h - ~ a ~ ~ ~ ~ d b ~ ~ ww*.
m ~ m h p l ~ i s ~ r a p ~ e d ~ t f m ~ ~ s r ~ t ? ~ ~ - ~ i s p & o f t h e ~ ~ , i t i s f ~ a t t h i s
h b s t m b l e controlof the mluslon cmbspq18edifihepthe8e~ are h M d s n d ~ a t W ~ ~ n n o . k ~ ~ ~ o f t f i e ~ ~ b o n h ~ ~ ~ ~ $ t e ~ M ~ ~ * p - k ~ & ~ 8 5 ~ a n , e h e P l s s u e s ~ c e i s ch@&€d*f~.and-an, hborde r s Me ~ f w ~ ~ ~ i o n , a n d t h s ~ ~ i s ~ f b r ~ m o f ~ a r t i ~ m t n m t -
~ I W d &W& should be
%%kw!@wd*w--wgaa ~ . ~ 8 1 t h i a ~ p g p s r t o ~ b w ~ ~ W ~ d j ~ t h e ~ a t e ~ ~ W @ t l I e ~ t ~ g s , a n d d u a d t o the prdehrmin~d inclination. ~ ~ ~ a m b e l t ~ ~ ~ l i ~ w i t h a dimaid &a; f o l l d by fine adj-ent with ofitae&i&m&mar~dltone.%@d c w l w s ~ ~ c ~ d ~ & e ~ c a s t t o * ~~ uf tbe m adjnstmenh. Weart, simhtd remmive movemmb are perf~med and djuse with the m e procednm. The objec- tive at this stage L to provide smooth excursive movement within a 2-nrm functional range with cmis &rch tooth contacts to mwe prosthesis stdAi@. Colnpletiun of tbe occlusd refmement i?wQlWs careful, pumicing of die occlusal m- fbet3. Xfthe * chmer to allow the p h n t to c o m p b the mfiammt by ming an inttaaral pstz (cwbamnb pate) rn the patient goes t h q h oxcurshe m m e n M , care must be taken

i:, **%? . t:. ?: F---
t -re 21-4 cesf'8 [C, D, a d IT]. Clinical management demands optimal mlusal tions which wwe readily inaqwbted into a remowable partial werdenturelRPD type of mandibu tar prosthesis opposing a complete maxillary denture, F to 1, Optimal eithetiagnrl
1 functirrn were Festered to predude further morbidity. COm'md

MANDfBUIIAIZ SINGLE DENTURE

C D I
Fig~m T1-5 Composite illustrations of an edentulous maxilla in a patient svuggling with maxillary denture stability due to the mmbinatian of an intact mandibular natural dentition and a r-ilrg edentutws maxilla. Placement of implants a l W cwrrtructim of an overdenture with enhanced furtctional stability. A and B, Panalnmic radiographs of an edentulous -1la before and after placement of eigM well-distributed implants with o connecting bar that supparts the overdenture prosthesis. C, Clinical vim of the imphnt connecting br, D, Owrdenture prosthesis in ~dusion with natural mandibular dentition.
vmtimaI treatment nearly impossible (Figure 21-6). The edentulous mandible is always at a didis- gdvmmge becmge of a limited guantity of mucow, &e amount of dentme border adjacent to moveable mrtcosa, a d the impact of o c c I d forms h m +be moving mmdihle contacting the static dentate m d h y arch. These conditions lkquently make m m t i d treatment unwise and have been b s t ddmd thraugh the use of endosgeaw dental @laW to provide retention and support for the mndibuIar complete denture and to retard residual b e mqtim.
When the clinician is unable to pmvide the option of endosumus dental implants, lmtmmt with a sin- gle denture should prdceed only after or e l m discus- sion of the potential for prob1ems, given the clinid fmdings, htmm the patient and dhicim. The ch- ical and laboratory procedm itre very similar to those kribed earlier in this chapter. Ebwvi$ ~ c l i n i c i a r t s ~ t h a t t b e u s e ofamdkntliner in the mmdbuhr denture is beneficial. With such a p ~ t h e d e n t i a t a t a e m p t s t o p v i d e a ~ reducingelementinthedenbmbasetotesisth force% of fLmctid a d ~ c t i d I d s .

F@rm 2 9 4 The mandibular denturebring area hasken &&y affected by long[.term wear of a mmpiete l ~wer denture opposing a partially edentulous maxillary dentition restored with a removable partial denture.
SUMMARY ~ ~ m t ~ ~ amnghdentmopps- h g * ~ o r ~ d e n t i t i a n ~ ~ ~ c k i b i a m nwe daa the sq le t e i y edentu- lmwpthntdm.lMsis&ewthebi~~~~cal diflkmms 3n Ihe BY& tissues for the i n g ~ ~ c w 1 ~ ~ m u g t b e 8 V s r l ~

I The Retention of Complete Dentures
Qphd outcome of Wmplete denture - ~ 0 n t h e s ~ f u I ~ g m t i o n o f t h e p r m ~ Wia dtb the p-tB d hwtions plus ~~~- c a l ~ o f t b ~ ~ ~ ~ ~ ~ ~ t b a t ~ p e t o e m e W ~
' ~ a 3 ~ m w ~ ~ ~ randrn&e m d ~ ~ o a t h e f w -*-BBBdm-- a f t h e p ~ I n t i t h ~ , ~ ~ ~ i n ~hiewhg &&we ~~~ (the mistance to ~ i n a ~ o n o p p o s i t e b t o f ~ ~ ~ a n d t h & ~ a d e n ~ ~ a p n t
I maypl@yfh-&&*t-b I r m d ~ ~ f ~ ~ i l 3 m ~ ~
F T O R S fWOLVED IN THE RPfEMTlON OF DENTURES
~ E o m i s ~ ~ i ~ t o ~ m o f & w a ~ e l m f a c e s W L ~ b y a f b o f l i q a t d l m v m l * . A m o f - ~ k # ~ b r O h i n t o ~ ~ ~ o n kmf&al ~ ~ a n d v i w o u s ~
W ~ c i a i surfwe tension mdts h m a thin h y e r o f f l u i d t h a t i a p n m n t ~ t w o ~ ~ p h e s of rigid W a l . b is * k t m the EM- ityoftlwfluidto'Wttae&id8urmmd&~ & l . r f t h e - m ~ ~ d b l o w ~
~ ~ a s d r w ~ ~ f h i d ~ l ~ bwntmtwitbtbemmkrid,thereby~itd ~ ~ s p w d l n g r n i n a t h i n f I l m . I f t h e ~ b high wrhe tadon, fluid will m h h h e its emtact with h e d, r e d h g in ~e fomation &beads on the lnakrid's surface. Dmtm kmm
~ & v m y i n t t r e i r ~ ~ i o n ( I s o t e r m e d ~ W & ~ S e d 3 ~ ~
~~~~~~~~ h b a a o r a l m s $ & - m b a t ~ p e l l i - ~ l e , t h e i x ~ ~ i s ~ w h i c h ~ m ~ ~ t & e ~ ~ b e t w l e e n ~ d ~ b r i s e . T h e t h i n ~ ~ ~ t t t e ~ ~ s n d t h 3 m u 9 0 s a & & e ~ ~ ~ ~ f l u - n b h a r ~ ~ b y y j r f p ( : g f ~ ~ o f t t P e f l u i d b ~ i & ~ w h h b o t h ~ ,
~ v m y t o ~ ~ ~ a f ~ ~ o n i n ~ ~ i a ~ ~ ~ o r ~ C ~ i a w M ~ a l i ~ t o r i s e i n a ~ t u h ~ i n ~ ~ will^^^^ t h e w d h ~ f t i a e ~ ~ , ~ b y r i s i t i g d m g the tabewdl I t t tb$m~bBtFk$CP, l i&d& ~ * W t a e a ~ ~ c f ~ d m l t m b s s E t Q d M m u a a on which it rests is dlcimtly close, the ~fiMwithathinfihofsalivaactslikeacap- ~ ~ i n ~ t h e ~ ~ t o ~ i ~ c u n - ~ ~ ~ ~ ~ & ~ d ~ . r#*q , capqwi l lwCd?he - .
Eaterfadal & tension may not play ahl impottantarofeiaEetainingtbman~dea- hm as it fur ti& tnmiky one. htefhhl s ~ ~ m & ~ ~ d e n t o n t h e ~ o f v f e l i ~ a i r M a m a t t h e ~ o f ~ ~ ~ I i d ~ m i f ~ ~ ~ w i ~ ~ w mitnmersedintbesamefl&&~,wiUlmrw ~ ~ t o ~ ~ ~ h ~ ~ , ~ m i s ~ c h t ~ t o k w p & e ~ b bofthe-m--in&m thereby e h n k t h g the effW of M d a l d m tension. This is not ioo in the maxilla Interfa&

~ o l ~ ~
m a r of 4hmion is
m a i n can bo
Coh&ion is the physical attraction of Iik
h q o d fluid. NO& diva is not ~ i v e $ o K ) ~ O f a f t h e t i ture-mumat int- wmes

- - C
mra 22-1 Complete dentures have three surfaces that must harmonize with the oral biologiml envimment. A, The &nard polished surfaces are so m t w d as to support and wntaa the cheeks, lips, and tongue. Band C, The i m p d o n or h t surfam are fitted to the basal seats. Continusued

M tlvac Rehabilltation of the Edentulous Patknt: Fabricatim of Complete Dentures
rn
FEyrs 222 Hwrtal jectSon M n $ denhim pry&& filling h e milable spare. A, The buc- dmt~r. 4 The lingua1 flange and hder are p a under t h ~ tongue. C The mylohpd ridge. * Z h a t M ~ a n d I w ~ a n s r r s h a p e d W t t r e a c t i ~ l o f f i e t o f i g u t a n d cheelcr ten& mtherthn urneat them. ff -rim artificial te#h ate too wkle Mingual ly , the forra of the denkim will be &ngd and the tongue a d cheeks will t d bo unseat them, I



Bemhgetdbim~*-- ~ d @ y ~ w P t e n a ~ k they^^^^^ i l S k d d h ~ ( l ) ~ ~ ~ m & d d v t properties and vismit~r of the merdirnn 8 . i n g b e b w m t b e d a n a u r a d f t g M ~ d @ ) e h i m h g & m h d a n t u r e b d i B ~ ~ ~ ~ ~ m m t e ~ * t h s ~ ~ d ~ ~ i s ~ w h e n r r a ~ ~ i n t o ~ ~ ~ ~ o r ~ ) a r e ~ ~ ~ r d i l y t n ~ ~ t i s s u e ~ s f a t a e ~ d ~ m d s u r f a c e u f ~ ~ ~ * Furhmmq beawe kydrated &wives are mom desive t h n diva, physical f m a ~ in-c to W ~ ~ i v r d 1 ~ n ~ ~ p u f J ~ ~ y ~ ~ ~ f o r c e s a c i t 3 x i n ~ T b a ~ ~ i n o r e a s e s t h e ~ i a f t b e ~ w i t h w l ? i & i t ~ , a a d i h e h y d m t e d ~ ~ ~ i n ~ ~ ~ f ~ d ~ a n d f l o w r g u D d e r ~ , W L ~ t h e & r n b a s e s n d bearing thws m -fore oblikratd
~ g d h e i v e m a ~ i n a s a b e f w e t f i e w1y 1960s were based on vi@able gurns (eg., k m 4 y a , ~ ~ m t n d ~ a ~ ~ * p h y ~ m ~ o n i ~ ~ o f l t 9 b o d b d e n t u r e a n d n l a C m l a a a d ~ ~ ~ M 0 ~ b ~ CSrrmkwxl adhiws (still commercially a d - able) am highly wta soluble1 @&ly in lmt ~ d s ~ u l c h a s c o ~ , & a , a n d s o u p , d ~ m s h a u i d y ~ ~ t b ~ . A U % r & i c ~ e 8 ~ t i ~ t l ~ h e b e e a , ~ t o ~ a { a a d t o * p a m h p r e ~ t h a t t b v e ~ e ~ -1, aud fbmdati- with Jcaraya impart a marked odDr r m b b n t of mtic acid Owdl, the &wive perform$nce of the vegetable jgmAad mwri& ia short-lived and relsttkdy
8 y n t h e t i c ~ ~ ~ ~ ~ - t a t e a ~ i V % ~ T h e ~ ~ ~ n d ~ W ~ c o n S i s t o f ~ o f ~ ~ t 8 o f shotw&g (ChaC) and lq-wtbg @wnyl m&y1 &ha Ideate], or "gmhd') gmiymep~i. In
pru5efxm af warn CMC hycwes and displays Q u i & ~ t i o n i c ~ ~ m ~ ~ mrrcous epithelium. The a&ind h i d inmuses its vismsiw aad CMC h~remes ha v ~ l ~ ~ ~ ~ v o i d s b e t w e e n p ~ a ~ d W ~ ~ ~ ~ t i m ~ y ~ t t x E
~ f ~ a e t i n g o n ~ d e a ~ * ~ Ipyrddone C w h e n ) is ?u~dm, hw m w &ydagmtthatbehrevewrlhCMC,~a m a r s ~ t e d t i a a e ~ t h a n ~ E o r ~ a n s e t o f ~ ~ o f C M C , ~ ~ ~ d i n m a s e ~ m d v k a s & . T b % n g - acting" 0.e.; b m u ] * a h * m o ~ ~
. . radthlgip,l- inmwein~WWorw'T'hbdfMis&ai f - i~~ mom p w m w d 1ongez E d in oaldd--Win* d u r n gmm. B m t d y , all &e b e E o m e f a ; l y & W a a d ~ ~ ~ s r r l i v a ; t b i s & ~ u $ o n i 1 3 ~ b y ~ ~ Q P h o t liquid
O t h e r ~ ~ f d e d t u f e ~ ~ ~ ~ ~ ~ u b r ~ w l a t i r i b ~ t o ~ f ~ o m ~ ~ ~ o i I , a d ~ L y e 4 b y l e n e u x i b ~ w ~ i o ~ t o b i n d ~ mt&h and to mrrlgt their p k e n t Silicone dioxide md d u u m stewate am used in powdm to qhhnize dumping. Menthol md pep. pEmint&mW*iImrin&d*& ~ l o r ; a n 8 ~ m ~ ~ ~ m b e n . o r P-M-.
W ~ - t h t e x C a p t i 6 n ~ f ~ ~ ~ ~ n ; ~ t o ~ I r a r a y a o r ~ a s j w t ~ t h w e & a v e k n ~ ~ o f t i t S w a ~ i Q ~ t x b s i ~ ~ p r o d ~ . E b r ~ 4 ~ 1 4 M , a h of the ' d l e dmtm adhmiw m - h b of -, * is ~ a s a ~ ~ ~ ~ ~ r e c a l l e d b y t b e F s a d a n d ~ ~ ~ba&&wereeitber&of-m- * ~ a m o t m t S ~ t o b ~
eye sensifity and oral toxicity befm b y &e e for sale to the public. ClinicaI &dies of -bI
mucod tissw &lying a&- dim- t l i m d l d ~ m i n ~ ~ F-f---hslw*= mmaaureUlat thNnnwpplzpdofy ,~ be^*^^ m&r& used in mu& dahl pmctick

444 r#tThmt Mabititation d Mt Menatlous Pahimt: Fabrication of Complete Mum


P%yu*s ZZ-!8 #m the emess powdet is shaken off, a thin. even coat remains.
denture in function, the dots should be distributed farther apart.
Hwwer, mom wen on

hbugh deaniw Q the denture la; essential. R e t n d is faciNtaM hy runntng warm or hot watw rrvet the t h e surface of the denture wfiile saubbing with a suitable hard-bide denture hysh. The sink should be partiaily filled with W, or a wrtshdoth w Wel should be p l a d in the sink h t h the denture ta p m n t accidental damage Ln the event the p&m is dropppcd during deanJng,

W3 PrPr'lkan of the€den&torts +%ti&: Fabricah d mpl& Dentures

$ ' $ - '
Maxillofacial Prosthodontics for the Edentulous Patient Rhonda F. Jacob
Maxillofacial prosthodontics focuses on optimizing the rudimentary fimctions of speech and swallow- ing. These functions are disrupted because of con- genital, organic, baumatic, or surgical abnormalities involving the ord cavity and related anatomical structures. M-ng routine dental procedures, the dentist creates static prostheses to fill voids created by missing tissues or to approximate organs with suboptimal function. Although rehabilitation of these rudunentary functions often is considered the primary goal by the health care provider, no less important to the patient is restoration of normal esthetics and mastication. These prostheses can be critical requhments to improve quality of life for individuals whose rehabilitation will be a lifelong proposition. Normal function may not be achieved, but optimal function should always be attained, and normalcy should always be sought.
ANATOMICAL AND PHYSIOLOGICAL CONSIDERATIONS: NORMAL FUNCTION The superior aspect of the oral cavity includes the hard and soft palate. As the beginning of the upper aerodigestive tmt, the oral cavity serves to move air for speech and respiration and food and liquids for nubition. The hard palate is the static ''roof'' of the oral cavity and the "floor" of the nasal cavity and maxillary sinuses. It serves to separate the oral cavity from the nasal cavity as required for speech, respira- tion, and swallowing. The soft: palate is a dynamic aqmtm of the oral cavity and nasal cavity.
During respiration, an individual either inspires or expires through the nose or the mouth, but never
both simultaneously. During expiration, air passes from the lungs, through the pharynx, and then through the oropharynx. Either the air then passes behind the soft palate into the nasopharynx, the nasal cavity, and out the nose, or the soft palate cle- vates to block the nasopharynx and the air passes out the oral cavity. During inspiration, the air passes in the opposite direction, through either the nasal cavity or the owl cavity.
For appropriate separation of these cavities during speech, respiration, and swallowing, the soft pdate elevates in the middle third to separate the oropharynx and nasopharynx. The soft palate musculature extends from the pharynx at the level of the palate, inferiorly to the tonsillar area. The right and lefi muscles of the soft palate attach to the distal aspect of the hard palate and then inter- mingle on the entire midline length of the soft palate, forming an aponeurosis. Simultaneous con- traction of these bilateral muscles causes the mid- line elevation of the soft palate. As the soft palate elevates, the pharyngeal wall simultaneously moves anteriorly and medially at the level of the soft palate elevation. which is in line with the plane of the hard palate. The sphincter formed by the soft palate and pharyngeal wall tightly closes and prevents any passage of liquid or fwd into the nasopharynx during deglutition, During phona- tion, the soft palate also elevates, and the pharyn- geal wall moves anteriorly and medially; however, the movement of both structures is usually less dramatic than the sphincteric movement that occurs in swallowing. These functional mwe- ments of the soft palate and pharyngeal walls during speech and swallowing are called velopha- lyngeal closure (Figure 23-1). In the English

*'I These Metal r i d e o f l m p i t frame s@w #he "oP& padtian of the soft W t e mtirat p@umsminat the &ase of thetonlye and kw the mapharynx @pen hr respiration. During ~ M g M#, the soft wlate sharply efewtes as tik phdqngA wall constricts, thkrebv fwrrting a ~ ~ t ~ W ~ ~ h a r y n x a n c t -rym
l a m g W g e , h ~ v e r y f e w ~ & t h a t r e q u i f f air to -1 £mi the oral cavitr, behind the mfi ~ d e c a p e f m m t h e ~ ~ ' h a s a l mmds"mn,m, mdngaadrmcmakinthFnaSat mtp Wm d i n g the nose, AU "oras sounds" mquhWairbeimpaundedinthesFalcavityby ~ * O f ~ $ o f t ~ a a d c ~ o f ~ e
W a T k ~ ~ o f t h e o F a Z c w i t g r i n c b
tb &@W, lllWC1a, 8md dS-8 0f &3 flflos lrf ~ P l C d t 3 8 & ~ ~ b b ~ ~ ~ € i # i n ~ ~ ~ T b ~ a d s a r r * p & n l q - * - d b d - *-**-*-* ~ ! ~ d g 4 ) 8 3 2 W O t d ~ m 0 f t e e ~ * ~ h % r d ~ , ~ ~ ~ ~ ~~ and tb dmitloa Accurate 4 rapid t q p movamens trm requid fix idhgible
I a r t h h t i a Draing matieation, the tangue c w s W y
mmsthehodtmha mihe occlusaf s & a . It f ~ ~ r h e f o o d i n i o a ~ a n d ~ f t i e ~ ~ ~ I y ~ t h ~ p d a t e ~ i n t o
TiwmftpIate s i m d ~ ~ e l e - ~ & t b e ~ ~ S . m ~ ~ ~ t t n t f o o d ~ ~ e s o ~
abrimdeiamplae w t t ~
FklN~lOPIAL DEMITS OF SPEECH AND SWALLOWING
waning, or damation of m a or smke can c m l d y denemate:


R w t k R t k t b ~ m d the Edanhrlous W t : F a b r i ~ a h of Complete Oentrr~
~ l b @ l y b o ~ ~ a t e ~ o r r , ~ th awbr e b b is positioned inferiorly
-Brises bmwed base3 hm e t e a d m k a p l in the
with a maKillufzdd prosthesis. Nunemus ~ ~ d ~ q ~ ~ ~ t a f b s r 9 n d ~ s n q m y o r ~ e m n y t h a t m a y b e & a s pro&&ie-baring m r f h s . When cowentiad ~ ~ a t e ~ , t h e ~ t s m b l & e d ~ t o ~ o w ~ e m ~ n f t h e ~ d ~ s s ~ ~ mastw cad. Bkkin$, out of undercub can d t i n h c k o f t i s s u e ~ o f t h e r e c u d b e wihthn~heryandtbabearingslIxfaceswithin W wgid site (Figm 23-3). Wrtbout bearing sur- fbe the whwl p h and the centric rehion {CR) mod o h are imwumh. Using ~ b w s ~ ~ ~ i n b o t h t h u m&ky md mdidar will aid in fd&Wiag 8mmm records. withopt petiphml ~ o n d ~ ~ , i t i s ~ ~ t m ~ ~ i n ~ e ~ ~ ~ m d i t i s w t ~ % l e t o - f # r w ~ ~ &khai tip and wport ~ f & & A l ~ ! & h g Pedphm I)f M l r x i k y ~ ~ W * t ~ t o o t h . ~ ~ w i ~ ~ ~ f i ~ g ~ ~ ~ ~ ~ d h th &n^~tl P ~ B I ~ S ernd m.m Mmss p i ? i a l o f d - - b y b b . A t t h e ~ 4 n ~ ~ t b p ~ e t s t a n d t f i e c l i n i c i t a n w i n . T h ~ h a r d ~ i i ~ a u f a t i c ~ f m e k ~ e t a & ~ p a t & e i d ~ ~ p a s i t i m t b c a n - i n g ~ B o n y ~ ~ r w
-re 23-3 The conventional triaI base (Iefrl has keen blocked out at the peripherie of the maxillary resection to allow removal from the master cast. The processed base (right) made from the same master can allows maximum tissue contad and stability for the arrangement of teeth and jaw relationship records.

like "hbb bade lebnjdx." T h e are the giDenoh d o f a ~ ~ t h ~ c o m m o n c u l d a n d ~ ~ t b r r t a i r ~ a o u ~ i t l g ~ t h e ~ w k s h o u l d o n d ~ , l a ~ ~ ~ ~ d t i ~ b e ~ t ~ o r ~ ~ ~ ~ , ~ ating h m speech with rm &tumor Is u n o o l m ~ a ~ t h ~ ~ ~ ~ ~ o b t u r a o o r h m t i ~ , h t t h t t h 8 p t h t d l y i ~ ~ ~ in d ~ u d passaga.
M A X I W OBTURATOR PROSTHESIS A n o ~ ~ s k ~ f a r ~ w h o B r r V e d g o n e - d o n d * M * fot n e o p w that originate in the pzimmd s h e s or saperior asp?& of the orsl wdty. ~ o a o f t h e h a r d ~ ~ ~ ~ n o f artidathn and aidlaw during speech pmbt~m aad &ow$ nagal r d u x dmhg dcgwd011. The o b t m ? m ~ ~ t o ~ & t y a f ~ h a r d ~ ~ ~ ~ ~ ~ a v i t y a n d ~ s i n u s f r o m t h e d ~ t y This- erirrdsof usedfbkhwdpalrttecbfEChi'tfaepatient with a ck&@ate.
The patient who miergmi ind lmy m d m i srehabiWatedfnt#reephams.Jbchpb~ %n obmafm pro&& that supptts tfie pati& thmughvaiout~ stags ofhdhg. Theaethepm+ tka are mq$d o W r , in- &mator, and def* obtxmw.


-234 h 1 4 b o I ~ m m p a l a t a l h e m ~ w mn h p k d into the mmer of the edentulous maxillecbmy patient, the hole should be drilld in the midline with sufficient space to allow the screw to move freely in the hole, but not allow the head of the screw to pass through.
Interim Obturutor Prosthesis The in& obtmtor is delivet& d e n the s@- d oboe is mwed. The prostbetic goals am to rest- -on and speech & re- palatal contours and - tha d ad$ M a x i n a r y ~ w , a n d ~ ~ f t O m ~ ~ cavity. The patient and &Uhtm&mWd Mfhk prosthe& W be altered coaeidmbly the patient heda trnd facial ~ ~ c ~ . Wpm- willb be in^^ 2mS mwths. A bwq10td w i m = ~ thc p&ient$eKistiagd4zlm8mkd**~- i l l e ~ ~ i n ~ ~ p ~ t . ~ o f t h @ & t o l m o ~ ~ L ~ a problem. The cbntistwd be wrt& bhatt?~ k- d e r ~ i m m d ~ ~ ~ ~ e p t i - md for maximal c u n ~ ~ t l t b R B W ~ the existing &amre map be reipi& b e f ~ m o d i f y i n g t h e ~ ~ ~ ~ sivea d i y me requa. c!Ommt uglmlms m d r e l i n m g w e n ~ b e ~ ~ ~ b r - der overextension in &e edentulm m d f x i a l proathemis will ummt the pro&esis. Keeping the prosthesis hojlaw in the mqgiml site will decrease weight and dd retention.
T h e ~ i s m o d i A a d ~ t h w n a t e d e n t m f i n e r t o ~ ~ t h e ~ ~ ~ ~ a l ~ ~ . T h e b U l b p o ~ W d ~ ~ ~
~ 0 1 1 o f ~ ~ . m ~ p d i n z a r y ~
~ w 1 8 t e t i l e ~ ~ ~ ~ ~ a bordm. The greater the volume of M e remet& t h e ~ t h e a m c a m t o f ~ d s o ~ ~ ~ ~andthemomtimoitwil l tBkebef~t&lih# f4wgical site is Wle. As the tissue CdmGB, l i l % ~ b ~ W i t I b e ~ ~ d ~ patient will b e difkdty &eating the pmdleml. The iatmdbk denture liner badem &odd then be relieved and r m d a c d The patitat n%am, complslining that there i% discomfort on ~~~ g i c a l ~ o f t h e m a x i l h a r t h r t t t h ~ p ~ h m longer retentive. Adjustmenb should not be ~UIB to the nonsurgical side of the pmthe~is b w w ~ theprob1amisblcdytobehsuechaagesintk
V J ; t s ; r e k ~ e r t t u ~ b a s e p h e k ~ mold4 with a Iw-YImsky tissrre d- maWM that can be relieved and modified as faW ~0rttrazhH.e occurs Fru-W Henly J. Bxwwth, Wle; MI),

7- a mk- R w m a s # : d % ~ M F - p S ~ D c n t u r s s
t h h @ m o r - m - & w!M
d d d b U , ~ W ~ a i l a a ~
-re 23-7 The ptlt. _... 3 qiginal denture has normal anatomid borders (/&I; however, the obturiltor prosthesis 'kllncd at 4 weeks after surgery (right) has marked1 y altered contours in the anterior of the prosthesis because of facial contracture. A tray extension wer the soft palate into the pharynx was added to support an impression of the pharynx in funaion, which was necessary because the patient's velar movement was inadequate in the weeks after surgery (see Figure 23-1 1).

&w#er ?rP Madlofacial Pm!h&ntks fw the ~ t w s 4@
2 t t e t h e ~ ~ ~ c a l ~ g i s c a m p b . T h e s l q i d b a s e p i * m b e b w r B e r d ~ g l r d m W w i t h a ~ c o n d i t i Q n e r m a t e r i a l o n ~ nonmghl sib. 'Ms step smhlims the pmthds, d t h e n t h s m r @ o a l s i i # ~ b e r e W ~ b a s e - p t o r f e m k f l ~ k e d a t i a w a x ~ . T h e ~ ~ heplate is tben mamed from the fla& dmq the bsil-oot procedure and r q h e d with resin. This hhiqw mums s well-fitting bwplafe dtaing
inbrim o ~ t o s phase. Sukqumt relining wil l b nectssary in the s a c J site.
aefnitive Obturator fmtkai> Thb prosthesis is fabricated when tissue heding end contm&w are compfete. When irradhtim %I- TOIArS -, retiohtion of radiation r n u d t k also h newsmy. P m a d q with a definitive pro& ds tissue cwtours are stable may r q h major djmments that will involve cbangiug tooth pasitions or $ m s adjustments to the prosthesis Wphwy. ft m y be 2 to 6 months postoperatively Wm the ~~ are die.
Preliminary imprumim are m d ~ with irre- versible hydrwolloid It k desirable to capture the
and height af the surgical 8ite in the pre- hinary impression so thai maximum atmsioa of the definitive impmsiw tray is possible (Figure 23-8). It is not necmmy tr, Mock out the mgic111 defect with gauze b prevent the impres8im mte+ xiat h m mtering this space. ('The only time the ~ g t o t h e s i n u s n e e d s t o b e p r o t ~ i s ~ the opening ia a f d . ) %me impreion &- & lack body and therefore Q not "carry" iato the &d defect witbmt d h g wax or compound qpmt iaSo the defa or injection of the nuterid with a large cu&mn syinae. Them ate h w s i b l a Irgdrocdlords with & d d d e viscosity. Thee give g o d b d e r e x ~ o l l s for edentutous a d max- illofacid impressions without wrppwt h m the tray or need to inject the materid. This ~ ~ i ~ c a n t l y redma operator time.
~ ~ ~ k o f t c s n a p m b t e m in tb patient mkgoing a maxiilectomy kcawe of mcd h u m md fibroais d the muwles of mmtkutiotl in proximity totbe dlfsryres&on. It m y be difficult to carry impression material into the @caI defect &awe of the limited orsrl open- ing, but because of the lack of dentition, the clini-
-20% I t i s d f ? s i r j s l e t o a l ~ t C l t W maxillary cavity in the pmlirninary impression for adequate extension of final impmion trays. It is not n m r y to 'block wt* the cavity with gauze
'
(Supergel, Harry J. Wworth, Skokie, HI).
despite the decreased opQaiag.
i n t o ~ ~ l o u y d e ~ ~ ~ q m a t 4 r time when fahim&@ the ftnal imprudw. The preliminmy cmt should "Mocked o d ' to atlow space f o r e md d m v i o n muat. Umbcuts in the cast atgo must be blocked mt: before making the tray, or a f k the W impmaion ispmed,thctrrr~fwillnotsep~abfromthema~- ter c a e t . a o n d e r m o ~ t h e ~ d sidead ~ t k e f ~ ~ i o r t ~ ~ b o t . d e t m o l ~ t b e ~ c r d ~ ~ t h a t t h e t r a y i a d ~ a consistent matm~t. when the weal site ist i m p m w d T h e c 2 a i c i m d d d ~ b e ~ b t d - p m m o f h * e b da molding and iqmsion &odd &e obliquely m d dgtht the mddag &lsr r i d @ a n d n o t ~ f h e ~ ~ ~ i s ~ * s & n g a t w r m a l ~ d e n t m ~ ~ ~ t b t ~ ~ ~ ~ f t e n ~ t b a ~ ~ ~ i n t o ~ ~ c a l ~ a n d ~ ~ ~ ~ dvm181: ridge wihut opmtm w.
C U m p l n d i f i ~ ~ ~ t f P e ~ todthepenpheryofthe@*.Theelitri- ~ i r l n ~ p u p p o t . r t h s ~ d w b g t h w e m a v e - ments~usetkptientmWperfarma~etyaf

m g thm matom toque, which will then

of f l e t d n . Owmtmion of h i e m in an- istehereeFtrltofsoR~ue ~ ~ E b e ~ e S i s ~ W ~ t a b e mlieoed md r d b d A d b i m am &mt &rys &@red frst my ~ ~ o u % obtumm prdmis. The patients &?add be advised to masticate EIS lit* t k a i i ~ ~ e a a t #e defkct side bccauare this mds to unseat the prasthmh. Retention is a very M- eult p d k m Eor the edentul~l~~ patient Whm phdngtbtttreatmentfbrapatientwith~~~f'dm- ~ $ e ~ n d l l ~ , t h e p h s h o u l d ~ t ~ save t& for denture mtmtion. smmly carim ~ s u p e b t e n p P o b I ~ t i o b G c a ~ 0 f ~ a f r o r r t c a n s r t , r t e e d f b r m a w n ~ , a n d t h e ~ k o f -ad ~~ tifta fwgery mld pmtqmiiw xadi-. For &is rmon grossly w * d o t m y imtolved mofars im of limited v&e. H o a t e v e a , - - d o t * a h r w e a t l t m t ~ ~ ~ ~ w i t f i l i m i ~ ~ ~ pekeit8 can meUte adqwt€I &on md 1- wm. h h S o f ~ h l @ ~ T O V f d ~ h ~ e ~ n l a x i l l a m h d ~ - A i l l $ I f * ~ O o ~ t e e t h m ~ , ~ ~ F w i f h ~ ~ ~ ~ ~ m n - sided. Them amtdmmta, in addition b adheshe, ~ ~ ~ e n b p v l e m y ~ U . T t i i s i s ~ f c l r ~ * ~ s ~ d o ~ *
(Figma 23-9 and 23-10].
m Z P 9 thipaaignthadtwtdtwith 7 recession and W r . & a t A - W were fe&ml wMM need for root anah. A kmus metal was used to create copings.
leum jelly on the prosthesis mfim and fimctiw the a m with a viscous ti- d t i c m m , a ~
previmlydesffibed.if~tissuedti~~er~ c i d i s t h i c k a n d ~ ~ ~ f h u r , ~ ma should be addressed for a relining p m d ~ . W t t e n ~ ~ r e ~ a n ~ i s o n t y l t 0 2 g n & t h e r e m h k o f t h e ~ t o r ~ k d f ~ achahidereIhingshouldbecms&d CutP& i i n e s t o ~ t e t h e a r e a ~ ~ b y t h e ~ oondilioner. Tbw f i n i l h m will confine h e mlh-
I
the denture. This magnetic system was k se&W* '
aver 10 years until the patient died of J ~ M M S L

M Thw R e b a b i M of the Wnfukurs Mht: Fabrimtion of Complete hntwa
Figrra Bl l This patient who underwent a maxilltaomy had lack of appropriate velar movement after surgical rontradure of the velum. A pharyngeal &emion was added to the prosthesis to obturate the pharynx and correct hypernasaiity.

' Ftgurs Z342 Passavarkt's ridge (umvs) is Ppominent iri lhis piltient wfw h@d U-W. a tcital soft palate Pesection. The pRaryqea1 ohtuntor pmtkds Is appdmbly I an In height, and the tidge i s evideht in the posterior contour of the prosthesfs.
pstdmly. If any of the acrylic resin my projectg tbm@ the m&xi& it &odd be gcwr~usiy ~ a n d ~ p m t i o n a f h ~ o n ~ . The inficaior amit of h e p h q m g d extension ~ d b e a t o r ~ b e l o w ~ i x l k l i m 8 1 1 ~ o f a the overall heightofhe ext~mahouldnotbemoretbn1m.Thiswill ~ ~ ~ t h a ~ o f p ~ ~ ~ -
' ~ ~ ~ e X ~ ~ g h ~ T f i e C o r n - p F m d q b e ~ & ~ d w i t d i ~ o a ~ I f ~ * ~ ~ w a x t o n . ~ ~ t h e ~ i u n , b w a x e w t e d ~ o n w i J l ~ t o k@&ly~inah&watmbatbbt fwher- ~ o r t h e p ~ W i l l l m F e d t o & p e a r t b ~ br appmhahly 30 minutes while repeatedly ~ ~ ~ d ~ d ~ ~ . ~ * ~ ~ ~ ~ ~ f o r C l ~ ~ f W ~ k ~ i ~ ~ ~ t h e ~ b d r i n I c ~ ~ t y a n d ~ ~ b ~ a t t b i s t i m e . I d e a l l y , ~ a i r f l o w r i n ~ h ~ b e ~ b .
~Cfesk0053ng the Soft fWa& ObtuMtw 'Pmsthsis
&odd h d i d & with a W d tissue d ~ e r r a t h a t h t l a ~ ~ ~ . A p a & e d m i n o t d t h e ~ n ~ ~ m t i f i s w & t i ~ w * I f t h e ~ ~ ~ tQmw p l % i n , i t m a g b e ~ D o r & w t h e & ~ i a n r m d ~ s n e w f u o & o n a l ~ m .
rcorclclkpechTooLDng apariawmp* PAUTAL AUGMENTATION PRUSMES1S ~ t b a v 4 ~ f s e l t k ~ e s i s i n t h e ~ f C ' o f t h e x r

M d e s €?Xpdatlced with thek new pmsdmwa t h e a p p ~ ' ~ ~ s t . e p i n ~ l r ~
r n - m = ! d - - w 1 M rmfmsmy to optimize i h & t L FhllyI thu~dogaj a i m m q k ~ t u & h a ~ ~ ~ became of mandihlar retention
augmentation h r frm&n and a t h e t k s may ~~~c ewe. a -
Uarcratdaude fabridon t c d l n i ~ tbuhtP
w h F n t i w g a ~ ~ p t 9 t b e s d a h ~ C nomud. At the try-in w, the magmen
~ e t h c b u l k o f a c r y l i c ~ n ~ i t t & palate could cause c d h b l e p m c d q tion if the base and augmentation are pmxW s ~ ~ r y * 7
If a speech and ~~ tbmpiat is d able, he or she can wkt ia d u g the m&mi T h e a r e a ~ f l ~ ~ f ~ b u l k ~ d
sure indicator m, loo ---mor~r ~ o f ? t h e m s a t h , 8 0 ~ ~ n o t b ~ ~ ~ o f ~ ~ a n ~ ~ ~ ~ mtgmmmiax. P b h ~ rti- c m d i h m m

B R d i ~ ~ w i & r ~ a a # e n i n % t h ~ ~ f w t h e & i b I s a r r n d ~ ~ r ~ ~ n r r v g r * b % a b l @ r o ~ t l ~ l t h e ~ o r ~ ' ' the ~ ~ i n ~ ~ . P l a o i n g a ~ i n d d m a r ~ d ~ p & & ~ ~ ~ * ~ ~ & ~ ~ I . T b i s ~ * w i j 3 . ~ ~ k b e i s i ~ %

Figure 23-14 This patient had a free soft tissue flap from the forearm placed over a marginal rnandibulectomy, replacing missing soft tissue of the floor of mouth and mandible. The right cast reveals the contour changes after connective tissue debulking 1.5 cm of soft tissue; however, because the flap does not attach to the mandible, the tissue isvery mobile, and the patient could not successfully wear dc tu res.
A m&om bmder mow:-,


TmubIdaodng Prwtliesafir the M S . , with err &ktWbs kkandihIe&my '

tdmdous pwtiw with a maxilhfwbl p ,&e& wi l l aqwbly bBnefit f bm impw m m

b d m of thafibyk g d t and ttim'hfrfitW p t a d in the patient in Figure 2347.
LABORATORY PROCEOU RES 8m'ng and Pouring impressions Because of the musuat three-dimensional shapes of soma of tha maxillofacial prostheses and became impression WRX is some he^ used, boxing t h e ~ i o n ~ ~ a t h i c k ~ p l m t e r ~ b a l f p d c e m k t m may be preferred to using a wax- bettdingtechaique.ExmsWBterin&emix~be m l w e d with paper'towels and the phterfplrmiee matmid positioned around k iqres~ion. The
mra 23-79 The debulking of soft tissues and skin graft were completed, as well as implant placement, in the patient in Figure 23-17. This patient ktmtiofls wry we1 l with an implant-assisted mandibular hetupe; howew, lack of normal tongue movement predudes a diet requiring heavy mastiation.
pumiceistbentrhndtoc~eatetheappr@ I d area, boxed with wax, coated with a -,-pwred.
Using P m c e s d Basts Adding Teeth, A& Paldul Augrne~fatiPns, or Relining obfurrtrurs During flasking, the e n h p r o c e d b&Be
ished &d plmd on the r&u~lt cu& that $ bem n h t a h d on the dcuhtm &m tlk:r i n ~ ~ t . T h e F r n a l o c c l w s i m ~ h s r e and the prosthem hmskd withapt 4 l l l w f i m - m d ,..A


ws muid to ohirate the hard and soft palateh -rag a mandibular Kennedy O w I partial denture.
~ ~ U l d h b ~ q v e d a n d ~ t o ~ f o r ~ i a g i d e t h e ~ d ~ t o r . Ifwater b ~ ~ ~ t o s b a k e ~ p r o s t h e s i s o r pl&q it u u h pressure again in a dry presem- potwill force thewater4kmghth+a maofthe lid that is leaking. Usdyj fhe leak is in a very small ~ m d l i m i t d t o o n e w f w o p k e s . T h e l ~ mw can be opened with a no. 8 wund bur, then warn is blown out of the bulb (at least two hales are n m to blaw t+e water out of the hollow pmthmis] and the boles sealed with a smaU amount of l i & h t 4 resh Again, the prosthesis ~ b e ~ f o r l e a k s b e f ~ r e f ~ d e l i ~ ~ ~ f ttme to Ih patient (Figure 2343).

Prolonging the Useful Life of Complete Dentures: The Relining Procedure George A. Zarb, Rhonda F. Jacob
I MI biologiml Blrpporting tissues and mataids wed in complete den- Waation are vubmble
r # O i m ~ c h m g e s . T h e d e n t m ~ n W e - rial may dkwlor or demimte, ~~ the d t - I cidtamoanalsodiacolm,frpctun,orboonne
r abraded. These material chmpa be HE& how- ever, irrwedle b g e in the ~~s -
I t h e p m s t h s s e a c a . d y b a ~ ~ ~ e d 1 f ~ ~ , T h i s p o i n t w a s ~ $ t M I % s s n I urnavoidable sequela of the sdenhrfous state. ' M & c u t o u s a t t e n t i o n a n d ~ i n t h c ~ o n o f I camplete dentures can nrinimizt adverse changes I h ths q p r f h g tismm rrnd in assoctated h i a l I ~ a s w & , b u t i t ~ ~ L e m . , ~ S l a e ~ f o r " & ~ ~ l e t e ~ ~
k # p ~ * t h e ~ e u r r w n d i n g a n d ~ pmhg b u t s lmmrms m~ddmly, m c w ~ ~ t h a t ~ a t ~ g t h e l l 5 e f u t l i f e o f cmlple€c *h01ve aref*ofhiqmk s i Q n ~ d ~ ~ o c c l u s a l ~ o n , and a minor spatial ~ t b n of the prosthesis. Two aechiquea are adable: (I) dine, a p r a e dtrreused.torumf~t~&the~~sues&ofndenture w i i h n e w ~ ~ ~ t h & p r o v i & s ~ ~ a n t o b ~ d e n t u t e - f o e o n - and (2) m b , the bbmwy process of repking ~ e n a i r e d e n t m ~ ~ i n a n ~ ~ t h w a . T h e d & m a h ( a t m ~ a n ~ onw) t o € h i S ~ o f " ~ ~ i s ~ ~ ~ - she paWk mmk of the complete deffturrwi.
TREATMENT RAT1 ONALE The foundation that supports a denture admnely ai a d t of- degrees and rates of midud ri&e mwption @RR). T h e
m t r y b e i n s i d i o u s a r m p i d , b u t t b e y m ~ and inevitable, and tbey d l y are a c c ~ e d b y o n e a r m o r e o f t f t e c ~ ~ l l s t d i n P i p 24-1. The wrhbh -on in vertical dimmion of wlwim (7030) mi &tmt spa- tial rewhwirn of the damm dm Id Eo ~ c ~ i n ~ ~ ~ ~ q u & y , i n i n p & i e m t ' s ~ . T h e ~ i wfusd relatioaship rn dm induce -more o r d v e r n e ~ o n t h e ~ ~ e $ w h i c h in-the riskofhrthrridge resobption.
u n e ~ c o n c l d m t t t a t ~ ~ ~ from clinlcat expdeam ami march hl* denw-vmihg path# h tW datum need reg U h atmtioa fbr ~~~ pwpu#a. Such attention can be aditwed anIy by patient ducation a n d a ~ ~ ~ d u l ~ . D a s i n g t h e ~ appointme& the dentist rt%otlcaeS a paht'a reported ~~ 8xpei~a.m with infortmiion derived from cliai~ral aminatha The mag&& o f t h e o ~ e d ~ a t l m a b i s i m t o b e made a s t o ~ t k W ~ b e d ~ b g o f t h ~ p r o ~ w i U ~ a ~ t o r y m ~ a m h ~ , oramnab.
T b e r e l i n i n g ~ i s t h ~ m o s t f i e q m d y pmmihdintervmtipdhlvesaddingamm b y e r o f ~ ~ t u r e m a ~ t u ~ ~ ~ . T h i ~ ~ b e d o n e ~ t b w t a b v ~ ~ ~ the oocluad relationships or tha e&& a f t h e l i p E r t n d ~ . w h m m i n i m a r w ~ c L m g e s ~ e v i d e a t , ~ ~ ~ ~ o f c l m o i c e . A t t s i n ~ o f ~ i m ~ i i r ~ to earnpensat0 far m@Ye dmqgw that hmx o c r m r r e d i n & e ~ w t t . T h ~ i r n r h e ~ ~ r a m y , t h e ~ a l i s r e p h c d b y a m ~ o f & c r y U ~ ~ t n t h a t B o a d e t u t h e ~ ~ ~


msuhtion of tlre soft tissue hypertrophy wifkmkt
Ths atuoupt of ~ m g e in the o c c 1 ~ v d d d h d o n & a t h d t e d & o m t h e 1 m d w r p ~ g ~ ~ b e ~ a ~ ~ ~ n o C e d , T h c p M e m i s ~ s i m g ~ y a ~ i n t h e o o c h a s d ~ - t i c a l ~ o n ; i t & o c m b e r t c h a n g e i n ~ h - ~ r t t e t i ~ d # $ d a n ~ t o ~ o t h e r g 0 d t o ~ b m d ~ A 1 0 ~ 0 f ~ ~ i o n will a u h m d d l y w the d b l ~ to have a m u m f ~ ~ ~ i a ~ ~ ~ ~ t h e ~ than it wodd at6 tb oP3gid omfwd verticaI d b a w i m m ~ ~ ~ e v t l l ~ * jm we &t&& bemiric mMon {CR) posi- tim W h t m ~ m t . b e ~ o o M is W- &ability of b tn+mlu&d chug&. Thfs o ~ w i l l k ~ ~ t k r e ~ & lim (Eigm 24-2).
l a o r p & n d * w o f k - m ~ ~ a a p s t d m t e m t o m o v e u p a n d b a c k i n * t o ~ ~ ~ ~ , ~ ~ m a y o o m - ghin of pain pain tb anterior v w t i i e below r m s e . ~ & e ~ b n a l s o m a y f o r c e t h e ~ ~ ~ ~ T h e ~ ~ t u p e ~ - a l l y m o v e s d o P c m ~ f i m m r d , b u t i t ~ m v e ~ & ~ * ~ t b a ~ d i b i a B ! 3 ~ t i m ~ ~ , t b e ~ ~ d ~ ~ ~ ~ ~ r n i s l ~ ~ ~ t e a t h ~ i a o c e h m h ~ ~ ~ d ~ Gmlpid*WMh-~m-*
s r r o u n d & ~ ~ t h r o P g h t h e ~ ~ ~ ~ ~ t h e ~ o T ~ d b l e a r e ~ b e l o F l l ~ l e w l o £ ~ ~ o B ~ o n , t h e ~ ~ m p w e s f d ~ & ~ ~ t ? l 5 m a x i I l a e ~ ~ E e i s ~ ~ t h a t ~ ~ t l z e ~ ~ ~ ~ ~ p u y * S I B F ~ ~ * - ~ . B ~ * ~ 0 f ~ ~ L n o t a e ~ m ~

7 Part Three Rehabilitation of the Mentulous Patient: Fabrication of complete Dcntun
&&&66d 8 - 2 days a b extraction - 5 years after rxfracfion
- 29 years after extraction
Ftfure 2&2 Bergman's and Carlsson's research comprised cephabmetric tracings from the mandibular symphysis region. They studied 13 patients who had been treated with Immediate complete dentures and obrerved the patients for 21 years after their extractions, All 13 composite tracings underxore the range and unpredicbbility of the morphological outcome. All patients wore opposing complete maxillary dentures. Clinical judgment regarding the mandibular denture's repositioning for relining purposer requires an understanding of resultant bone mrpt ion outcomes. Comparable information of similar changes in edentulous maxillae is not as compelling,
forward movumemt of the mandible; rather the CR position af tbe d y I a may h retained deslpite the apparent forward movement of tbe mandible when observed in relntion to the maxilla,
The effects of this rotary movement vary from patient ta patient and appear to result h u a com- plex hkmction of several f ~ ~ , particularly the duration md magaitude of bone resorption and the mandibular p0stw-d habit. The mandible's roWm may be awociated with a number of consequences that fmpnfly occur simultaneous~y: (I) losing centric relation occlusion (CRO) in the dentures; (2) changing tlae structures that support the upper denture; (3) forcing the lower denture backward so it impinges on . ha lower ridge or forcing the lower
denture anteriorly, with an ensuing pm@c appearance (Figure 24-3).
It appears then tbat maadibular rotation am elicit s e v e ~ damage in the denture-supporting tiy sues wer a long period of mupervised dmw wear. The stresses ate probably a&pented by tb use of cusped posterior teeth and by the r e d & incisal guidance, which now loch the m a n d h h denture into the maxillary denture. Although pros ponents of the 'hommp'' school of thought-&. quently indict the other school8 choise of "cw@ teeth as accelerating tissue damage in such Sim- tions, no research evidence is adable to mppW either school's claim that its tooth choice d- mizes changes in the denture-supporting t i s~ua.

ti, I i' .
) I , I
id.;# k - 1
11 r, II .- kl;. , , I - , .I . I . ., \; tl,, ,
C F i v 24-3 Loss of bone structure under both dentures permits the mandible to move upward a corresponding amount. As the mandible rotates to a dosed @tion w%Wt translation of the condyles, it frequently mows forward. The pmblem is to detemiw the amount of change that has occurrd in bath basal seats. The occlusion not appear to be correct when o b w d in the moufh of patient 6, or it may appear dffefluely adequate a d in patient C. The extraoral dose-mouthed appearance an be almost identiel in lsoth cases.

476 P*rt Tkrca Mabiilitatlon of the Edenhilou Pntirmt: Fabrication of CompletE OMtuw
f the M c h chooses to go fwward by rembbfishhg a normal inbmcchssd dis- existing denture modifications of b a d seat
W.Again, h e P r ; n c i p ~ u s e d i n t b ~ ~ ~ 8 ~ o n o f ~ d e n t u r e a ; m & o n , ~ a o f
PREUMlWARY TREMMEM I t ~ ~ l h a t i f t h a ~ ~ w m ~ $ Y t b e * w i t b i n w w * ~ d a ~ m


& ~ ~ 3 d ~ ~ f t h e u p p e r dmm4
retruded pitim, which is one cuspation, to help stabilize h e

Denture b e rmwpd6 to fuWoW pmmm~ ~ ~ W W I G fft IS w p m
I
(Few eun to taw dayel
Surface Is slmllar to pdymePlzed main surtaorr, %xc~pt It is vulnembk
to deb-
Fllprra 244 The physical staw of tisue t to use them for different objectives.
~nditionedtreatment liners allow the dentist

T h making of a new CRO md and the procedure we recommended to mure an
q d m d pro&odontio occlusion. Rtwwchera haw tlemmmw that the funotiwal status of &mlm dined with tmdment linm used as impression ~ a I S i s ~ $ o o d a s ? h e 9 ~ h I s o f d e n h l r e s rebed by border moldkg and tben rdmed with a figfit-bodied impression material.
The mcmt intdu&m of visible light--cd (VLC) mitl gystems has produced promising d t s w h e n ~ i n a w i d e m g e o f ~ o d o n t i c wthi?im. Biologi~al testing Wcates that they are nontoxic and biacompahIb1e. Ongoing resemcb' atso appears to kam improved their propdm (such as fit, strength, ability to polymerize witbout residual components, eaae of fibrication and manipulation, patient accepttanm, ability to bond with other denture base resins, and low b-d -1.
One @sing upplication of VLC resin mate- rial is b use for &hide relining. It is used in a M a r m m m as a tissue. conditioner, witb dl the p m i i t i w of ktmt d f i m t i o m bwnw the flow of the materid can be regulated by ~IBction of appropriate viscosity, warming and cooling ~ i n w r r t e r b a t h $ ~ d p a & l M p o l y - merhdoa with a handheld curing light. The m~~ is then taken to the laboratory for ilnv&e ~ ~ g o P t b e n e w ~ o f m d l ~ r i a l ~ ~ b a v e ~ l m a w n t o b e q u i t e brittle, but when supported by the original pmcaed denture h e , the VLC material within the denture and at the dabre p e d p h d rob has &ppc@m clinical ~~ far denture longevity M u m tbk mthm' clinical experience. Although tam clinical resub on ttatmmt efktive- -88 Wkd -4 bk&v &tmMltE WX wamhbb, the VLC materids seam to hold con- ~ ~ e ~ .
Both the static teahip (or versions of it) and the hct ionrt l hppessirn technique are well
8nd e x p & n c + p r o v e d p ~ . They ma be w d for simple sitwdiuns (denture settling i9 tnhb l ) and ~~ situations (excessive ~ ~ e s h a v e ~ p l $ ~ ~ ) . ~ t ~ e a r s t h a t t f i e ~ ~ ~ t h e t w o ~ i s ~ o n t h e dentist& skill in ~u~ the materhh and the ptkntk m d - .
kbhtim of C m p k Dmtrrres
Chairslde Technique


I ilant-Su 3 rn orted Pros-' ~d;ntulous Patients George A. Zarb, Steven E. Eckert, Regina Mericske-Stern
I MALADAFTIVE DENTURE BEHAVIOR
i for

Figurn ZS9 ' TmZTtjng the edentuious state with comp!ete d w t t w s presumer that acrylic d a is a reasonable substitute for the a k n t periodontaf ligament and its partidpation in the maintenance of its surrounding a h f a r bone. The shadow behveen the prosthetic teeth and the underlying bony support in A reflects the reduced and profoundly changed support for an ocdusiolr. Attempt3 to cumpensate far this inherently cornpromired support mechanism have included a diversity of implant designs, such as 3 and C, k p t m b l y , this rn d endosmus anchorage yiddad unpredictable results because of the high risk of the bne in-w hanging to a poorly dmereniated mnedive tissue one. introduction of the oneointegration technique led to a prediaable and lon%.lasting interFacial osteagenesjs hat ensure predictably favorable and prolonged functional outcomes as in 0.
allopWc tooth mot substitutes b stabilize and a -&S 25-11,
presented to the scientific de at the 1982 TQ& Confenme.


PatiCAtr' Iignr and Symptoms That Freq~nf by Pmdclde
ad Adaptive CampJete Denture EXpetiehce
1. Sevmw rnerpho~ogical comprombc d the kntvre-supporting areas that significant1 y u n d q i n a dmure rdcnriun
2. b a r aral rnwular mardihation 3. Low tolerance of the mlacwf tissues 4, Para#undimal habits Itad@ t~ recurrent
dielaesael inhtability oftllc pr6sthesis 5- Uwnlistic funniolsal pmsthationtir expec.
Wions 6. ktiw hypmttive ga& refib elRittd by a
r ~ D v ~ k p r o ~ h ~ i '
7 , PsyrhologhlitmbifEtyW w r a dCauw, wen if adequate denture rekntion or Aabitity is pmt?nt:

I s f * i n t e r f a x x . T f r e P L i s ~ ~ t o f I t ~ a p ----htalp ~ t o f a ~ p b s n * e d a n 4 t o a ~ ~ mmei l , haling m. This pmfaagld e- ~ ~ ~ f o r b ~ ~ s f ~
! r- or^ xwmie an inBucsd '**lotie
ld-&lytokwhmbletopsi- ~ ~ ~ ~ s u s p e c t ~ i m p ~ W o n l y ~ $ m e ~ h e a l I n g ~ i s a n imp&tone.T3isL*inthe*that~ implant occurdutingh bed^ i a t e a y a l . O f h a r f d m s ~ ~ a f a w ~ ~ ~ i a ~ b o b e e a m p l e t e m e h m a f b a a Y a r i a b I e p e A o d o f ~ o c c l s a l ~ ~ d m n tbe imperfectly b l e d M a c e is w l o n d d ~ t l ~ ~ ~ s e c o n d a r y ~ ~
I ~ t o ~ ~ ~ d l ~ ~ . T h i s s ~ o f %vmbhaa been m i s w bmany ~ ~ o f t m ~ a P L ~ - s e r t o h ~ -
I mthg debah on the infmqmtly imcmnkmd ~ o r k ~ ~ o n ~ .


The Science of Osseointegration
Osseointegration, or prehctable long-term anchor- age of tooth root analogues in bone, is defined as "a time-dependent healing process whereby clini- cally asymptomatic rigid fixation of alloplastic materials is achieved, and maintained, in bone dur- ing functional loading" (Zarb and Albrektsson, 199 1). Such stable bone implants have an interface that consists mainly of bone tissue. This attachment mechanism differs from the one retaining the natu- ral dentition because teeth are anchored to their surrounding bone by means of a highly differenti- ated connective tissue attachment with ordered fibers: the periodontal ligament. To this day, nobody has succeeded in creating and maintaining a replica of a periodontal ligament around an implanted allo- plastic tooth root, In fact, past implant efforts ended up anchored in poorly differentiated soft tissues, with unpredictable clinical results. Consequently, typical 5-year survival figures were in the order of 50%. This predicament provided the backdrop for the breakthrough introduction of osseointegrated oral implants in the early 1980s. It became possible to insert oral implants with a favorable predictable outcome, for example, a success rate of more than 90% over a follow-up of 5 years in the anterior region of the mandible. At the beginning of the 1980s, oral implants were prescribed in small n u - bers and rarely in university clinics. Today, the sit- uation is quite different, and the science and clinical epidemiology underscoring osseointe- grated implants are an integral part of most univer- sity curricula. The current popular notion that every commercially available osseointegrated implant system will result in a success rate of more than 90% is, however, misconceived. In the absence of
scientific evidence, there is a serious risk that some commercially available systems will yield long- term failure as a likely treatment outcome because of adverse reactions to untested irnplant materials, designs, surfaces, or diverse therapeutic prescrip tions. Furthermore, secondary failures have also been reported to occur in previously osseainte- grated implants.
Considered in this chapter k the unique self- repairing ability of the surgically prepared bony interface, which, if not unduly disturbed, will remodel d~ciently to carry clinical loads. The specific nature of the osseointegrated interface and its bonding implications are also discussed to provide informa- tion about how the osseointegrated interface is sus- tained or threatened.
OSSEOINTEGRATED INTERFACE In the past, direct contact (without interposed soft tissue layers) between bone and metallic implants was regarded as impossible to achieve. The operat- ing notion was that a soft tissue interface was inevitable, which in turn implied that the interface was of maximal strygth at the time of surgery and thereafter gradually lost holding power. Experimental studies performed at our Iabmtories by the late 1960s indicated that tbis notion was not necewdy correct, even if the methodological shortcomings of those days did not allow for defmite evidence of dmct contact between bone and implant, In the 1980s, when the bone and implant specimen cut- ting and grinding techniques were developed at the laboratories of Karl Donath in Germany, it was f h t possible to clearly demonstrate that metallic

~ ~ d t w ~ O F e d i n b m e w i l h o u t r r ~ m h & & ~ ~ ~ 2 & 1 ) . slbseqw
(-)r4&&m ht&m developad a stronger attach- mat with time because of incmmhg bone form- t 3 m ~ I y e a t r m b ~ , G e p e r a d i n g o n t h e $#i#hWion site, :, stmqth is developed wer &a htdae. The mique capacity of bone to ~ i u a E c o r d a n c c : ~ i m ~ f u n c t i w a l ~ ~ t o b e o r ~ ~ p ~ , bash d p e d i s a w r y s t r o n g ~ a c e i f t h e imphut is W u w r W during ib incorpmtion @r inwhcid orgmidirm. If ~verroEtding acmI t W ~ i s ~ d a ~ y d i f f - -
+re 2- Portion of a b l a k vent implant, surrounded hy soft tissue with sdme inflammation. The implant waa mobile, had for years caused pain, and was remwed for this reason.

~ ~ b e ~ t f o r p r o a e r l d ~ g 2 3 m @ O H W e mgg@d ' W ~ ~ ~ b o a d s m a y d e v e l o p ~
~ a n d c e r t a i n o a k m i c i m p l a n t ~ ~ d I 8ttggtsW Buch ~1~ to be " b b i o m , Efmew, thm i5 M, conclde ~~ of at&
cemiEal bonds, evam if they mmah tbmmidy pmible. The mailable evidence for chemical bonds is r€qmwd by el- mimw p h o c o ~
o f 4 ~ ~ e g r : e n c e w i t h f h e i m p t n t o r a n ~ wise mexpIahb1e Wdhcial atkdmmt
Qxidized implaw bve l&ewm b n suggested rn beiog c a m e of bioa&iQ (lee., establishing a c h m h l bond between f d g n mal md h a -1. sul(2m1 u d e r n ~ t e d a v a y s t r o n g b m c & o n t o ~ rmodid irnpLants with s- duiw ions. A h implantation, d c h catim will maw
FIm -3 €tone tissue I n d u w p u n d substance and cellular components will need pares of a minimal size of 100 prn for ingrowth. Ca k i B 4 gratrnd sulbstarlre of bone responds differently to irregularities in the mkrometer size that are important for the strength of the meointegratd response, Implant irregularities in the micrometer range are, to date, of undetermined signifimnce for osseointegration.

~ ~ i r r q ~ ~ ~ ~ e ~ ~ ~ ~ W y & & IUskmMh ion bsading ofailM'm i t n a a w i & ~ ~ o f b o a e ~
~ ~ t w Q s m a o t b e ~ a d b y t h e i r ~ d m . H m e r htemfing thaw must be OW hi published
e&dd.sautirmy ofsuch imphints is limited ta a %I- * ~ ~ d ~ a ~ .
Hgum 264 A k a l l ~ , ~ n d r i d imphnt that may l ad to wse bone m i o n

o o a ~ i m p ~ . W i t h ~ ~ t € u m p ~ s p r + g f b r ~ ~ , i t o o u b d ~ p o ~ &
I w m u c h ~ ~ ~ ~ ~ a M i d f h e ~ ~ ~ ~ ~ t h ~ n € i ~
wwem cp tiwm&m-dAl4V mofall& other c r t t d u m p ~ remain wmmtk mdrs- B i v e ~ u ~ a r a r e ~ ~ i a t l t h a t t b a t d b e p r o ~ f i v t k =cultbtefl. Hmmf, at^^^ bone hcda (e.g., msxillnry b e , whioh hu lmp,onfOesrbn ~ e ~ q ~ ~ ~ ) ~ a s e aeedsassn~bmewpprtmpo~"b2efwclhi:- Tbewstm&&yof ~ e f c i d y a n d a b b cal success, q titanium appears to be the dht implants c b i n g ' sWaare-
d r i ~ i n ~ . ~ Z ~ ~ ~ a TE&atite ~ ) , r m c t y p c o f ~ c i m n b ~ ~ k j m i $ r t n i m m o p i c ~ - p h o s p h s & ~ ~ ~ ~ t y t r i a a ~ kwpe&s, such^, H A o m a r t l a t , h w B solid m M d for we as $n Orat implant. ~~ primary o s m i n ~ m and, in Howvet ,~~f thebr i t i l enatureofHAand m a n y ~ , ~ t e ~ d r s a l a t 5 ~ . a&er m a , such as aluminum oxides, hctwes Unf&tm&bL the @lem is hat no such d&a ~ ~ ~ ~ t g O Q ~ f o r ~ ~ ~ t o k d ~ ~ ~ e v e t b e e n ~ ~ ~ h i n ~ ~ * l d * devim in tfi& solid fom HA is par- ble bone Imls. RepWs i d i a t e a Q O Q ~ b tieuhly interesting &cause there is clear tiow- saucerimtion of 1.5 mm &g the frrst year aad m&on that & +c d c mdts in a about 0.5 mm ~~ thmafbr, with ewn a tat- m m e m p i d b o n e ~ h s e m w i t h c p t i t a - d e n c y o f ~ ~ i n g ~ o f r ~ r p t i o n i n t h e ~ nium. U m y , t3wb fmdhgrr fmm short- mpmh of such implants that rua avm more d a a n i a a s l e - a m - M m ~ 0 f f i u o ~ - ~ p ( ~ i 9 9 3 ) . m ~ suBdmt ~~ f h intductiiw of HA-coahd m d & d bone loss mey not be dramtic at 5 d ~ i n t h e m i d - i 9 0 ~ . L o n g - ~ ~ b u t ~ p o s e a ~ p b l m ~ . S o i u Q w & k H A d i m p h t s h e v e k r i @ h n t l y ~ ~ ~ l a i n t h e I a ~ k o f a ~ s t e d y ~ ~ t o ~ ~ f n r c p t i ~ i l l ~ " ~ W , d b y o v ~ l o a d ~ t o m i ~ ~ f ~ ~ y ~ s m e ~ W i m s b ~ e h s d m W d t h e H A ~ 1 ~ d e s i g a s , w ~ o t h e r s ~ ~ ~ f s r t h e p m r c l i a i d o ~ . H ~ ~ e a m m t ~ o r d ~ w cmd pr tbhdy by the vmy m d u & ~ & * * m & f o r & e ~ ; ~ g h ~ o ~ i c a l f o r t h e s e ~ ~ l f ~ & ~ c ~ ~ m c h w 4 % p - I n -MdWbtshwe- f e l r r a i 8 a y I l n & P ~ h n t d e s i g n . M ~ ~ i t s t r a t e d ~ o f s d m r ~ s f ~ W ~ b c ~ ~ . t e ~ ~ d ~ m h e ~ a f t e T t h e f m t y a t r o f ~ ~ ~ ~ ' of a mm typ8 of implant on mulC of ~hort-tmn
lapanncnts am* (199*d- Impfan* krrlbce i e d a h o r t - d b g ~ ~ t o H A d i m p h t s i n & ~ a a d d ~ ~ p o s - T h e d a c e ~ b e o f h ~ itive byother^ other^- qualitative or ~~ c h g a 3 .

-re 2 6 5 aft tissue penetdun (4 and bone tissu~nchored portfon (0) of a postmortem preparation of a threaded implant design with excellent dinkal documentation. There are no adverse readlons to the implant seen in the soft or hard tissue.
dmnga may bg amplifi& by h e topograph- a ate~~tiwa~. -aw ap mfer to pokmw W v e surfam b& mmplifid by o x i d k t iqlmb or & doped with paten- timlUy active wfbstmce~. Todayj new clinical implants mmdcckxl that are eittrer quantit&iwly o r ~ ~ l y ~ ~ a l ~ a r t b a t a r e w e n a * . -of&*.
Sur ih m g h s s k hphnhhtdpropaty t h a t h s l x m ~ ~ I y i n ~ r t i v e r r r e m l i m p M t ~ . - ~ ~ ~ ~ i a ~ ~ ~ e s , h h p h t m m u f a m have mmbined ~ ~ a ~ a r ~ ~ , ~ i r t p d l m o n ~ ~ h h t h e g ~ ~ f o r - w m .
h s d # o f ~ & s t u d i e s p e r f d i a ~ b , a s m l l a s i n a f e w h u m a n e x p i m m ,
moderately rough impimts developad the l m t b fixation as described by peak Eemcwal toque bone-to-implant contm (Wennerberg, I sad), "Moderately rough" swbea were produd-& blastrng to an average height M o n ( m u m PEtrameter sJ of 1.5 8ll -8 butween the individual irregularities of 11.1 ym (S ) a n d s d e v e ~ o p e d ~ a r e a r a t i o o f 1 . 5 ~ (ST (~igun X-Q, were positive@ ~ 3 % smwther (hrmed mi b ~ ) as wu m rou&e~bbkd implafit mikes. Very mmothw faca (S, xdua h1ow 02 pm), which are itl Be! only used mqmimmtdy for abutment and m h o ~ a g e ~ e a , w i l I ~ b e 8 ~ ~ ~ u m i e d b y a i w f t t b sue i?&m imhtjm of irmninent ~~ m rema as to why rough su&m {S, values d and above 2.0 Ctm) demonsme 18s firm bone P* ation w h c m p a d with less rough mrfaaa still

Flgura 2- A mrted sunace wltn a mugnness correrponding to the expimental ideal of 1.5 pm.
need to be investigated (Figure 26-7). The m c m with any aurfw roughening involve an increased risk of corrosion. Hawwer, current howledge about such increased corrosion a p p m to be only a theoretical and not a practical problem.
In tbis context it is worth e m g ~ ~ that r careful topographical cham&&&n is emtial for a mW1e hqmtation of the role of implant m- face roughness for bone i a c e m (w4?dlm&q d ~ ~ 2 0 0 0 ) . T f i e r e ianeedfwcequip ment that can be used to meaure arbitrary designs and dfferent surfaces. For example, only some optical instruments such as c d w a l profdometry
Summary of thwls
S A ,-",,-,*,,A ,. . ", , A * .> .,,. * =-A -I,I ,I . . . . _. I,IIX ... Roughness O . I . O . g :., . ..* . .. (Sa)
Wgum 26-7 &perimenQlly the strongest bone response has a sutfxe roughness of about 1.5 p (S,).
amd interferometry can be mommended for threaded implants at tbis time.
In recent expukents remarchers have iwesti- gated the possibility of doping surfaces with differ- ent kinds of bone-stimulating factors. Such dopings can be done with implants of any d a c e roughness. A number of these he-stimulating factors, growth factors, are present in our bodies and serve as important stimuli for the initiation of healing processes. H m , external W t r a - tion of growth factors may not necessarily improve the healing situation. We have doped implants with bone morpllogcnetic proteins (BMPs) and other growth factors and f o d no influence on the h e response (Franke Stenport, 2002). One- po~ible explanation of this lack of a positive influence of growth factors m y be the fact that we d y tried them on regularly placed implants (i.e., a kind of press fit healing situation). However, one cannot exclude a positive Muam of external admidstxa- tion of growth factors in gap healmg cases, such as a tooth socket.
A rapidy growing number of publications underscore the clinical popularity af certain oxi- dized implants, and these implants may show strong bone responses quite independently of their surface roughness (Sul, 2002). Hawever, other types of oxidized implants depend mainly on their surface roughness (Sul, 2002). In fact, oxidized implants are manufactured in galvanic element setups (thus the term anodized), md the used electrolyte will influence subsequent tiaue res- ponses. The clinical use of oxidized oral implants started some 10 years ago, but long-term out- come data are still laclung (for review see Sul, 2002).
In essence, it is still unknown how much bone contact is needed for an implmt to be successful. Comequently, the clinical relevance of different surface (roughened and/or anodized) implants can only be verified in controlled clinical studies. However promising these surface alterations are, to date, there is in most cases rr lack of support- ive &ta from such studies to verify my clinical superiority of them. In fact, so far, only one sur- face roughened system has been positively docu- mented in controlled, randomized clinical studies (Gotfredsen and Karlsson, 2001; Bngquist et al. 2002).

~ ~ w & l m ~ ~ B e w l ~ ~ ~ ~ t i ~ t l f O ; hyw-ent
M m imdidon k s &Mve cuaWn&a- t h & r m & n i m ( J - , 1989.- ~ ~ ~ ~ p a t r ~ p e a t e d ~ t b ~ ~ C f b e r ~ ~ ~ ~ c ~ & with &cknt experitam wi& such patien& A I-par a* a f l e irwdiatim before hsating hpkm& is rwnmmbd. Expected stmew ratm are &out 10% I w r &tm for nmimdmd padem. HypxWic a y g m tmmem in divema
h b e e a M # c t & m e in srt least ane plwsw 5-yea wtal fallow-up ~ . ~ r n & ~ ~ t f a e r ~ ~ ~ e . i m p ~ t S ~ i i l ~ a r r d ~ i n ~ ~ t h e ~ & & r t 3 k a z q & ~ - a ~ o f t h e &&mk3 = M* is i8 mofmlm& ~ i ~ ~ ' t $ a t ~ ~ d ~ t s w i I l ~ ~ i t i b o t l e ~ i t e ~ - ~ ~ ~ ; n n p ~ ~ * ~ i m m e d i -
a b e b f ~ ~ ~ w i l l ~ a t ~ ;,
rate. A
J t b ~ d ~
~ d ~ ~ w z ~ f n p o o r t c o n e ~ ~ h t Meal h &hod with r fied wgicd tdmk#m will yidd p d d d y able long-km outcoma. Both a u b n of d -bin@-turnad h ~ p h a , whi&
~ f o # r m e i t h e r ~ ~ o r ~ (A Ibrebm 2001)
mandible betweca the mental fmmim Hmm& great c d o n is reoomntePBed with such an b k i d

diate loading protocol in the mailla, p d c d d y if the bone is judged b be of a poor q d t y . Fmdmnme, such loading puts a special e m p h i 8 ontheMsofthesurgeos~whichirJwhywrec- ~ d ~ l y ~ e d s u r g ~ ~ n s t o ~ ~ a ~
operation A promising approach for those who prefer a om-- a q i d protocol in &i- nation with direct or rapid loading is to use res+ name frequency analysis in an effort to difbatiate potentidy mobile impianta h m sta- ble ma.
SUMMARY It iis hporhmt to &serve that new biomatmiah are in need of d physical and enghdng hvesti- gadom to clarify if thy arc suitable for implmta- tin In vim W e s may provide Emportant Wormtion, but o m must memb that h i s is r e l d +a h controlled laboratory emhimeat, W h i c h ~ f m m i n v i v o ~ w i t h i ~ h o i m ~ w flow, and loading hflm. It is tkefm not mmnmun that m vim l%dhgs are quite dif- fmmt h m those o-d in dtm. Short-tern and rOng-tem in vim axpmhmtat d e s am impere- tive before ~ o m i a I clinical testing of an imphint system is initiated It is only when a bio- materid is fwad acceptable in such studies that clinical W should be stark& The most im- s t q in &e t d n g p d w e r a n a h the conttolled, preferably prospectivF, c h i d study that should spanan ahpate period, which is wnventionrrlly at Lemt 5 yeam.
I n t b e ~ 0 f ~ t h ~ 1 e d g e a b O u t ~ factors eontpolltng implant function m the bdy, it is easy to say M the scienmc community has made a gcat number of important fm- in the past 21 ye.m. Howsm, m r n m q very wll be climb'i fbR h e r slopes of a mountain of amknaum height, Major owtr ibut im will be g&- ere. inthe future hPPQfOPBCtiVBand aonded treatment outcome d e s in patient%. TBe h d a -
mental message in clinical epidemi&ogy is &at without effectiveness usurps fhc notiotl af
a compelling s c i d i c clmrin
we- A t ~ T ; O n l o n s ~ - o f b -
grated mponue, Arrst PrasL, 3 ?@~ppI):I5-24,1993. A I m o n T : Is s u g i d skU mom Importantfm cliniedmm
~ t h a u ~ i n ~ b a r d w a r e ? c ~ n I ~ ~ Rdat lPss 3:174-175,2001.
A l b m ! & m T , ~ P I . H a n a d w a H - A a t a l : '
t i ~ h n p l m B k @ a t t b f o r s a a u d a p ~ direct boae &dmag@ in man, Acfa &hop ScMd 52: 155-170, 1981.
B l - h m & ~ m C t A , A ~ T : m u e i ~ ~ t h a a : 091eoln@&un In &wl dmtiw, Chicago, lWS,
S & l : ~ b o g a ~ t o o r a I i m p ~ A ~ w c ~ ~ o f a P h a o p C h d ~ ~ i m p ~ , C C U A O m l I m p l ~ 1350-37,2002.
PrankbSMnpmtV:On~~Eudt ismfmImplaDt intk g r s t i o n i n b o n e , P h D ~ . ~ ~ ~ 2002, Udvmiw ofmtdmg
QodfredsenK, ~ ~ s o n U : A ~ 5 - ~ s t u d y of- ~ p ~ ~ ~ b y h p ~ w i t h u m % & m 3 d and no2-b1Wkd &ce, d m - 10-2-7,2001.
~ s a l a n d e r ~ : ~ n h d t h ~ ~ ~ ~ ~ timiurn iraplanrh PbD thesis, Biomakdddhdcap research, 1994, U n h d y of W&org.
JaCdsmM:OnbonebohaviourattgiaadIatiw,rnThesis, Fawardq 1985, U W of &tcbg.
J o h m s 6 m C : [ 3 n ~ ~ r o ~ ~ P h D ~ -rw#ad& 1 9 9 1 * ~ d ~
~ L : G a t k a b o l a e r i s w l e r e s p o n a ~ t o t i C a n i u m h p i a n f a , PhD Wai$ B- & 1991, U- of -.
S u l Y T : O n t t t e b w s ~ C * ~ ~ ~ , P h D t k s i n , B ~ & 2 ~ ~ o f wbmabma

I
reatment with Implant-Supported Overdentures George A. Zarb, Regina Mericske-Stern
s r o a m & & o f m * * tbwd*- t
Of OVERDENTURES TREATMENT GOW * h t p r o t s a o E h s s ~ ~ ~ ~ p ~ ~ ~ ~ . M ~ i n a O v m h t u x e ~ ~ b y m b d --of-
~~~W~~ term---be+ € x d m d * & i q H a l i t y ~ f * ~ ~ ~ l O ) , .

Altlmugh tooth aPd implant abutmat attach- m a t llm- dm%, &tit proshdc role is q r r i t e ~ . B o t h c a n @ d e ~ ~ sm l-eituntin stability* and positively Mumm adjacent bone lev&, although psiadontat dimad ~ d ~ a r e c l ~ y n o t r i r S k ~ f o r t h o u ~ - lotic-tiken ~ i a ~ abuhmmk la ebad- ies of mmdibdw overdtmtures mtahed by imploln~ have &own &at h e Mght ia very well maintained in the m a where implant8 were l d It Id& hmmr, k painted out &at resorption of the -or residual ridge. was k w m d when c& with similar sites in @mts mted-with implant-- fixed pros- ~ m * I t t h e & m ~ ~ p r u d e n t t o ~ ~ ~ ~ ~ ~ ~ m p 8 t i m t , t h e ~ t h e beaefitfr0mW-fd-b r e d a o e a v e r a l l l ~ t e m i ~ r i d g e ~ C k & e & e r ~ ~ ~ s h o u l d b m m - mended row@ far eIdsrly dentdous- p b t s becaw d&d ridge rdwion offheirbd bone appears to be less &&le €o midud ridge reeorpdou nu wcation of ~1~ denturesI @c-
dady mmdibda oaes fbr e&!y pati- with matadaptive den-, complex and difficult. Tbemfare a aimple protocol m y b readily applied to dl elderly patiah is a prudent abjec- tive. Such an approach inchide$ the fbUowhg considerations:
dl& cormeotim to remdm d$vices. Them is l i tdedonbtaboutthegmttmms~ ,
which esthetic abjoctive8 can be addmwd and~~evsd*os jng~wsds l l hno i ~ q ~ m s ~ n o t ~ ~ ~ - 1 with the €d premip?ion, TmEe p d * larlyinthemdh, w h e n ~ t e ~ r i d g e m h a o * n a r e d
5. The d d s t staould miowly cconsider man- a g i n g b o t h t h e p a ! i e n t $ m & d d ~ ~ ~ ~ ~ ~ o n a f ~ ~ ofMs c m & t i m m p f O d m M ,
INCLUSION AND EXLUSlOW CRITERIA ~ ~ t m a t m e n t ~ i s i ~ ~ l ~ ~ k ~ f w ~ * ~ r o W ~ . T h e major inclusion criteria mdmmm the quashmi- 4 pahunt digibiry. fix &€I h o d @ox27-1), A g e ~ l f ~ n o t r a n m w ~ ~ ; ~ 3 =#18kd f- phmhg in elderly path&. Cumrim problem ~~ include cmmmidon d f l d ~ s (e.g., m m p d d h d n g a d aspitive &Us) W i t h ~ ~ W 0 f ~ t i o n ; ~ ~ I y d for ah& e; special &&on tu presurgical nmmm such as general b d t h ststus ttnd infomath; d hygiene atate; aad hwne care ~ ~ ~ ~ t h i s o f t e n f o l m d i n elderly p&iBtltS- Vpith C O m dekiwdon iP M 8 E s g i c a l ~ d l W i a * ~ W ~ Q & ical age. T4scfm id#l cmdWn i is h- ~ t t y ~ a n d ~ o f ~ ~ f m a s w U £ y & m i c d l y ~ & a n d ~ ~
lrdurion Criter4a for lmpfant ~mxkdontic Tmatment
Patient desire for implant treatment Systemic health status, whlch permits a minw
surgial procedure Sufficient bone quantity to atcommpdate
prescribed implant dimensions Patient willingness and dKiity to maintain oral
health status


C Figure 27-1 Corm Imagmg ot potential host h n e sib% requires a mix of radiagaphs, whih can be rendered mwe armrate 4y using a template with metattic markers of known dimensions &). These markers will show up on a frontal [B) or sagittal i m w a d allow for measurement adjustments in bane height or dttth. Required sagimi views of anterior edenfutous sotw are provfded by mwns of rephalometric film or, I- frequently, corn puted tornogram M,


rPElDura 27-3 A, Mandibular owdenturn have been shwt~ to pehrrrl W when ~ I s y m ~ m i m @ ~ ~ ~ e s e s a r c ! i m g l a R t l ~ ~ a a d m k ~ designed when implants are placed asfar apt3 as pmik Mwem tb -1 hmim. U g of a bar &at allow for towion ai ahe prosthesis o w n d the 4ntspinqht axis an be a h i d it anterior ddml ri&p shape k -1M to an atbihwily- Urvgeds thaP h only dWy cwed. B, W#l idge curvature (as q p m d to the "flaV m , i n gart A) usually nwm pbemnt of three or mare impbnts to pwW W *Wing; WS a n m d m e n t on tongue space. HWUM, a t M MWS if the bats sqm@s f o l k the rklge contotlr, the prosthis Is then viMP, entirely itqpbt supported. SBIIW effect pd&y results even if altmadve mtdw metknlm are pre%p3M,

f s a a l ~ 0 ~ 0 f t h e B a r . T h e ~ ~ o f ~ ~ l i p ~ b f y a r e f ~ ~ H t h a ~ ~ daring the laboratory p r w s ~ i q pmmb@t$ (F'i274). S o m c l i n i c i a t l p d a t o a o a I . hmmmk embedded in the acrylic win b h m b w . ~ n ~ t a s t ~ ~ e ~ t s ~ ~ not be soldered to the metal h n w r k . T h y m r e f p l i n e d i n e h e t k n W e h w i t h a f f y l i c d I facilitata future &ages or repah. clinical a d Iabmtory pmceutes fm faMmt@ the imphnt-sqpmkd overdenaae are ethawn @ BOX 27-4. I
'.f
S ~ ~ f a p ~ ~ o l l a m d ~ i t y o f o w m i m l W a p t ~ k . T h q ~ a@iy eff*t. Bmmr, & c o r a s i M a r n & & h o f ~ e W t . ~ includ~ (1) number of mppdng hpht#r d t h e i r d S . ~ ~ ~ i h e r i * ( 2 ~ ~ b r r r ~ ~ ( 3 ) ~ a n d S h 0 f ~ ~ h & 8 ment orbam, ( 4 ) ~ b a a f ~ ~ ~ d ( 5 ) d e g r e u d f ~ c r f t h e ~ ~ ~ empirid €llmwh ed& regwbg the of^^^
a ( ~ i l i t n e ~
rigid) @OX 27-51, A m&i& rebntim k widely morn* for amhoqe m e S t o h p ~ ~ h e ~ ~ $ t h a t ~ ~
m d t s o f ~ y e i n p a t i ~ w f r h ~ ~ b h I g a n ~ & ~ one type of anchorage dwh or

Chapter 27 Clinical Protocol for Treatment with I m p l a n t - S u ~ & W & m & t
234 The acrylic Fcsin pmtW may W M may not M b . r d W : - a ~teflk'$lloy fmwyork; this appeam to tie a su wmomk implications, flte retentive clips [SOitl dip h k j a h pmitsed and "fixed" r*n the aayl d i ~ ~ a t e m n t requirements a tektTvety easy pmdure.
W e ' s lrrdexiw of setups to allow f& optimal bSK . I
Prpli@tl+ary frrlpres<mn with irrevmibk dkgn : :, ", h-~fioid ;for c u m ttay fabrimion laboratory: artectlons as detemrinePl at 'try-in , . I Qb@@W- tbsbrn traF with openings wet agpdntmmtt bar fabrication , implititti: k t i a n
' . Five ,w obtain consent of tfic *>~butmenj cmpsne~ts selected [may P
: indude addtiom1 prosthetic mpingsj Twin of bar awrnbty, wrectian of a t - - . h kaurlfi&g of f ran5fer coping 3 ingif a passive fit t not obtained
. ," +:;a FM arch br w q e Impmion with Laborabry: final corrections, pxepizratian for . : " , &artmy I processing the denture: assembly of
t,,k&mWy rnaqr'cast with implant ana- + c - ctiplbar campownts
, . ~ ~ , y z i x , d u s l p n rr'rns R M n g the denture, accklal equil ibmtfan , , > : . , . an artla taWr to rectify processing m)s i , i * .
; ' a - ~ . m l & records Slx I
.;. +-@&j&igp1 * ~ d i r y of dentures b q the patient .:.v ':L@bmLry;.~ntiwthe&antfreafiicu- ImtmctErm about handling of ahe&Mrrer , . .
: . = . IMf* p r a l l d ~ €oath *up I I, I ..
Cleslcihg in#ruaiom for hphnts, retek
:, ,:GAL; - >
Eion devices, dentures r Jnformation a k t and eemttment in fhe
1. . . . * @ri?i&idifoT [pcdiw~ rerods malntmncs care prograin " ' * f$k&tic, and fundipnal asswmcnt of m. Basdine radialgraphs for comparative
monitaring purposes (optional)

Some Anchorage Devices Used for Overdentures
Uagle Elements Single retentive anchors (stress-breaking mechanism) Single magnet anchors (stress-breaking mechanism) Individually cast telescopic coping (rigid mechanism)
Splinted r U-shaped bar (rigid)
Round dip bar (stress-breaking mechanism) Egg-shaped Odder bar (stress-breaking mech- anism)
F i v 27-5 AMhmhaurped maxiitary '
pPosthesis 39 made out of a cumbination d prosthetk teeth, Stdlite a l h {fbr m @ h with minimal bulk), and plnk ~ I i c rein as a substitute for wft tiwe dudion and for &hetic support. The undersurfxed this prosthesis Indud& fire retentive dips that the bar segments shown in Figure 29-3. Note that the dips are retained in the acrylic rein segment b facilitate any htture repair
f o r m p c m y w ~ r h e & d ~ ~ ~ a n d w m f h e ~ u n o f t e c h n i ~ ~ consuming prosthetic recotutm&m. It W d pointed out that the belief that spWd &t&y m e n t s r n $ y b ~ t o c m n p ~ t e f o r & ~ ~ d n o n ~ ~ t 6 - t h e i m p ~ ~ tobeamistabone.
The objeatiw ofmplttr n d h for all p2lti- %4@ ~ k t o ~ ~ b e a l L a f ~ @

A b i ~ m f r e r & . # k h ~ d # h ~ @ ~ h ~ 5 ~ b : m&#e#w&-etrflance and diwii$wdahhWml b m l W ~ ~ ~ W . M
Ffgwrm my'71 Ar@kmdw- u - p l e d k a d l e - w piedti&! by rmliiht m g r o m i d tissues mi$&k b r ~ a t i d & l & a f a m p t g t e & m ~ ' l t t e pmmipti~ard&oi 3 connected by a @JM bar rrrettkis@ena'$ f o x t o m f o ~ p ~ f u d f ~ ~


a p r e m t & d b a a s ~ i n ~ h 4 ~ 5 - ~ follow-up !m?y, Cttrr Olol ikpbm Rss 121825, *I.
W ~ P $ . ~ R b A . ~ r n ' f b e ~ d ~

, . . I, .: -:
Clinical Protocol: Implant-SL lorted ' " ""71
m I
Fixed Prostheses George A. Zarb, Steven E. Eckert
Sw#ssful atio ion enables tfre dentist and fhR e&&dw patient to d d e r one of two alter- ~ E o ~ ~ t i o n a t ~ f ~ d e n t u r e ~ r i - epee. These rd- are an lnrpfant-appmed f f r t a d o t m a v e r h m ~ . T h i a ~ r w i m ~ e d ~ ~ ~ h a Y e m i m p a c t on the c W decision m h g and protaco1 for f d ~ ~
Paw who fiavt beenshomtohdfimostsig- niFm f h n w~~ bave beefl those dthaddaptwdmbe mprknm. Thistndm hirar dm led maey &llm adaptive patient8 'Yo
in" h i r prosthais for implant-suppml fd-. Consemy, fhis thmpmtlc a @ h * ~ k p r ~ t ~ ~ e d e n t a l ~ ~ s Went txxhng p r o s t h ~ t i c &atmat as m a h - Wive to complete dentures; Current
wggmts that any patient whose ayshmic health does not preclude a minor waI surgical hbrvensiw a d w h m proposed host b e sites cat^ ~~ and qualitatively accmmmcb the dimdm of the dentist's selected impht ~ a n d t h e e n ~ e d s u q & c u l ~ l , as wellas afhd the prodme$ expense, may be regar&d as a c a d d a b for mscointqgmtion.
A clinical wewment iderntial to the protocol art fc i ibd in this book's wly chapters is carried a. MXU@OUB c W ~ m M 0 n b dug- mated with diagnostic crast a d @OW prost6s w* -?s @ox 2&1). It is tben matched by a
i m g i y awessmmt. Usually, panmmic cq&hmtm ~ W S provide emugh inform-
appears to bc a soxwmbt more compe.lhg amam iothemaxilIarytdcnkrlous&
PRELIM I NARY PROSTHODONTIC DESlGN The decision to an L n o u s arch with sp impWuppmbd --isis i n t l d k p the foIIwriag five cnrcid o d & r a h
1. The nrunhr of the implant abuhmfs, W early, P W compllin&ly docwnmW * i d f3umemes with implaat-mppomd fws 1

Cortddetatisar far Systemic Lscal and Prosthodontic Treatment
~dimcal hbtoPy Contmindlfathg treatment Systernlcmdition that predudesa minw oral wrgial procedure{e,s+, brittle d i i r w , H o d dywasia, immrmol@ically compromised) History of chem'cat dependency HistM)t of ordacial irradiation Certain psychiatric ldiswrders Heavy smoking [pwsiMy)
Local Ewrftderattow Size- of oral opening and Intmrdr space
rn Status of opposing dentition, if present (peri- mima4 health, overeruption, bcclusal nta- tiom) WalW,and quantib af propod host sltes, which dso requirw a radiographic evaluation
r Height of arnle line icirtumalal activity]
PYoSthdir Cerrrlderatitlons 8 PqgibIe shsrt~mings in appearam, du- . ,
sioh a d fidupg~&fpWws dentures. Will the green= a! implants mify such proMm? R&+qnslaip ot pmttnenicteeths' pwitions to uderl$ng resi$ual ridges. WiH a fixed pms- t h a b resolve the perceived complaints
- , earfi&.y*sr,wM e~msiue anterior and poste- @br @kti&rim he required3
w I$ t&eWrer t optimal poM~111 and suppoa oi tkiEircumoral,tkues compatibk with the propmd prostlletit teeth p!acemsnt and the tatafi6n d $he impla&' support?
2.
3.
o quasi-@ fox- m * f # 8 ~ I ~ ~ ~ m m t d f ~ t o J > a l 1 0 - ~ 1 2 - r m i t 4. f d l w m d h h p x o ~ . IbWEvm, tbas f d a did not addma cansidepatiom of arch form conPption (flat vmw varying d e g m of curvature), length of implants, length of cantilevers, and specific consider- ations regarding d i m ~1~ fumes plus the d ~ g u d o n of the itpplmdarch form. The same applim to tr-t p h d n g the maxi14 with tbe additional proviso k t six
o r ~ ~ t s s h o u l d w m p r i ~ e a ~ - ~ ~ - f w a . ~ ~ g n . T b k$&n of the implants. Implant low ~ i s ~ f a w w a b b w h e n i t s d i s t r i i o f ~ i s a c u r v e d ~ e r h u s ~ me-m ~ d l o w s formoxe occw ~ d ~ ~ ~ ~ ~ $ n . A W bnpht Wfom ie probably a b mn- didate fbr .as mdmture design. The qwlity b the host sites. Ckkd e x p riema t $ a t ~ y ~ F a n c e s - , tousbone-fart-- omminte@atd response. &mquenttg; ~ ~ t 8 f u ~ o n o f ~ ~ ~ ~ l a a t o # b a * b ~ ~ ~ : *
j l ~ ~ a f ~ ~ f ~ i s * * t Q b c r n ~ I y m - tioned"%ndan <b in t h ~ mmdibie, six i n t h e ~ ) ~ ~ ~ ~ p b 1 ~ a n b c ~ ~ ~ , ~ i t b-w--h- calm, F- Wd wi5 d m h ~ ~ ~ a i d e d b y improved and' enhswd aec$ns*, &x m t & , & ~ i a r p W W i & m ~ ~ p h w a r q e o f ~ 1 a m o f --It-wP=gm- d e n t & m d n ? & t Q w a ~ ~ i m p W ~ ~ ~ a ~ ~ f o r a f I x d p m t b k T b ~ d t h e p W c w ~ W ~ o n & ~ patiat ~~ activity kmwm moat p # i t h m w * m d o l r r g n i - h&,-asrd-~fAmCfiDLtal l&g. Hmmq the # h b clp.rwt ~ t o . ~ p m & c t t i a e ~ t c o m e of implants h t&qmphimrtlgt ,&amin& p m ~ b w @ g g e s @ r d f o r e m ~ Sidmm&rn*-e*. T h q s r W M t b & M k w ~ o r t h e m Q u m f M ~ - t b a t h ~ T M 8 i s ~ y a ~ t i o n i u t h ~ k ~ ~ # l e a d i ~ IeBstbsn 1 0 ~ f n ~ ~ I n h intermental foramina region ate hh- q m d y enoopmtaed It is, hmmr, a &+ quent problem In the d a , Prtxerne g & Q techniques may be requid if a fixed p r o h i s L planaed. Alkmati*

H$un 28-1 A mrnprehensive radiographii survey of edentulolajaws will enable the dentist to erwre the presence of a healthy host bone s i te compatible with both q wlity and I
quantity considerations. More than one view is necessary if a three-dimensional -merit i s to be made ( u n k there is accm to tomography). All three views-panwamic (A), cephalometric [B), and dm1 (C and D)-provide magnified dimensions of differing degrees. E and F are the spec if^ preoperatiw films, and 6 is the postoperative film of the patient in Hate 7-1.


Pkta Sl d d Frontat, p d l e , and cimm-oral dowup views of the patient provide airrent widace of the need for restoring the Wient's &id isthetit appearance of his srni te.
Cantinud

Plate 28-1 colrtkl The sequence above illustrates the fitting surface appearance of the maxilla (A), Pre- and postextraction views d the rnandfbufar supporting areas are shown in % and C, The recammended approach for a surgical guide's design is illustrated in 4 E, and F. First, the approved set-up is indexed (0); then the teeth's positiows are wplimted in autb-polymeriring resin in the index 0. The completed surgbl y lde is now ready for sterilitation and has been t i m m d to permit stable seating during the surgial procedure and an easy accommodation of the necessary instrumentation m, Such a surgical template guides the surgeon in optimal implant placement
Continued

Plate 28-1 coatY The matian of a maxillary impmsion following surgical exposure of the omintegrated implants is illustrated in the sequence above. Healing abutments are placed at the se~oncl stage surgical procedure in 6, and following a suitable healing perid (H), they are fitted with the selected abutmen8 [i] and pmtdive plastic copings (J), The healing abutments are then fitted with transfer copings (K) for the final impression. The last illustration (U shows the tissue surface of the impression in a custom tray, which incorporates the transfer copings.
Continued

Plate 28-7 corrt'd The protocol for managing the mandibular impression is similar. Transfer copings are attached to the selected abutments (M); the impression is registered (NJ and poured in stone with labratory Implant analogua fitted into the transfer copings in the final impression (N and O), This provides for very stable "overdentured" occlusion rims and t k making of jaw relation records (P) (see Chapter 15).
Continued

Plate 28-1 cont'd In Q and A, the sequence for ensuring an optimal esthetic try-in of the teeth arrangement is illustrated. Jaw relation records are next confirmed, and the laboratory phase of indexing the set-ups and using the index to design the frameworks in wax and then casting them in the selected metal is completed (S and T). In U and V, the silicone putty index is employed to confirm the relationship between the original "tried-in" teeth positions and the cast mandibular framework.
Continued

T
9 co~rY The processed prostheses are mid on the implants via screws and the access bles filled with a choice 04 one of several materials available for the purpose and )o. L a t d \rim in Y and Z show shortened dental arch designs for this patient. This protocol h2ts been tharougfi1y researched in dl d h many phases and has yielded extraordimrily favorable and predictable results. It c~mbines the traditional skills and techniques ob complete denture fabrication with the availability of substitutes for tooth roots.
Continued

Plate 28-1 ront'd The subtleties of the patient's dental appearance are modified as demonstrated in the sequence of iltustrations above. In this particular case, the patient's old photographs were used to meet the patient's expectations as suggested in Chapter 17.

Ch#w 28 dinial Protacoi: Implant-Supported Axed Pnoztlrcsas W3
~ d ~ ~ h l ~ ~ ~ p r a c s - & m s a d a m d d m & m d p W o f ~ t B i n t k e q ~ w p Y & q @ a p ~ . ~~ boah appomh ofer -king pwdbilidm, them is stH a I& of WU- ~ p r o a ~ ~ t o j u r m t i f y *mdinepm&tioa
5, ~ u f ~ ~ ~ o r U g e m ~ i t y W a f & ~ ' s ~ ~ . ~ d ~
I tim applies dmst ex4IUsiwiy to tht ~ ~ ~ a k e ~ o a o f a E g h l i p b d - t e g w * -an, or w w e d y , vhhdly m ~ m a t & , m y i n d i c a t e ~ ~ T h & ~ w i l l ~ t h e ~ ~ f a v s l e w - b - f . ~ ~ ~ . ~ ~ s m d ~ i @ s f ~ a ~ n u y p r e c 1 u d e ~ y ~ t p $ ~ r e - nance and tiwefore ~ ~ n t m h b t e a fixed
A s a n r l e , p a t b t s w i t f t ~ v€&d aad llolizmM &or d W ~~m cmdidms lkr h p h t - ~ r k d ~ d a o f ~ p F o s - ~ . O n t h e ~ ~ P K h e f e l i ~ w n o ~ o n i s ~ ~ h i g h s m i l e I h i s a a t d y ~~o with ideal implant loea- t i a r r r r o t r i m ~ ~ ~ w b a n ~ ~ p r o f i f m t h e ~ ~ ~ k m h ~ ~ ~ f ~ ~ e ~ ~ ~ ~ o t b ~l~ inehemtaiorpsrrtofthmdU~~ if&- &b, areplaced in theposttrirzwe.
PRESURGICAL TREATMENT
SURGICAL STAGE(S) The surgical technique is well described in the -1 literature and ~omi$tB of& satrile prpracedure in which &pa are raised a d holes ae carddly and gently W e d i n t ~ the selected host bone sites. The holm mnfwm to the chosen implant%' dimen- sions and accammodaoe the threaded both root m s l o ~ , which ape fiequeutly tielf-bppud into place. The xfl- mucoperiod f laps are readapted to completely cover the imphuts if they arc to be s l l b r g s d &'unloaded during; the healing period Note that the impI.mts arc prwi- s i d y sealed with a ixwwwmv br ing this interim Mi period This is m h e d eo as the two-stage surgicd p-um. Alternatively, the implants may be fitted with a "heding dmfment'' and the flaps readapted mrmd them if the one- stage surgical procedure i~ dected, In either case, the soft tissues are sutured and the tissues left to heal uudisbbed. t h~ 4- to 6-month haling perid, the designated time required for osseointegmtion to occur in the mandible and maxilla, respectively3 the denture is relieved liber- f l y and a tissue condifioaer used to refit the dm- ture. When a second-stage surgery is required, hmwpithelirrl abutments of s e l d dimemions are attached to the implants and the prottthodontic procedures stwed.
PROSTHODONTIC PROTOCOL The ptosbdmtic phase of tmdment has m its objective ?he W d o n af a cast prmthesis b e (metallic *e) that joins the implmta together m d providm distal cantilewr mendm (PW 28-1). Artificial teeth and a soft tissue mdqpe couldthenbepmsedontothe ~ ~ T b l s procedure'allaws for an electively mmvab10 pros- thesis that could be &rewed Co the o~~ abutments. 0th techniques haw a h baa &I- o p ~ d to allow the use of screw- or c~~ metd ceramic prostheses. The dbwsiun of such prowhwes' mmwtion is I& to publications that specifidly d m m -tion of implant- supported prosthesis.
The design of the prosthesis, b d h m both F d and removable protocols, & to reconcile traditional principles of wht- sim with optimal design for sofk tissue health

IOU MFmrhphn&-
tbmowhg~:
~ i n ~ ~ t ~
~ m ~ O r ~ w & ~ l & ? 4 i $ r e ~ k - I t t w <
3- ~~~ ~ o f t l m e ~ ~ d t h e n f i l m d s d b y re& The metdic fmmm are & in a dm-*ordwwpM

SUMMARY
H s a r g P J . m A B , U ~ S : m i t Q f ~ ~ ~ ~ f i x e d p a a i a l ~ f a b d ~ ~ ~ l e v e ~ ~ o m m a d e a t ~ l ~ , J ~ M 77:265-270, 1997.
J c m t T : L V h . o ~ o f ~ w o f ~ ~ h p W m p p r k d w i n b - @ , I M J Oml MaxiUqk hphm t1:ISl-158,1996.
J o m t T , B m k K : h o s ~ i a m i ~ t a n d ~ m ~ i n e d c n m I w r n i m p W ~ , I ~ J C A r J ~ I ~ ~ 11:620625,1996.
~ L , ~ M , ~ B ~ a k ~ d ~ r i o r ~ ~ a a d ~ i m p l a n t s f o r i m p r w e d p - thein suppoet, Int J W MrodIlofbc 15:4&414, 2000
kmgmt B: Biomechmk of tba Brbmmd system, k t hddhtt J 9(sapp1]:3948, 1995.
~ ~ B , K r ~ & P H . ~ B o t l d : B t D d i n g ~ a r r d i m p l r t n c f m d u m a ~ d h h l ~ I ~ J ~ Mdk$kc ImplancP 10:326-334,1995.
k i n g & B , S m C m y L , M N e t a k ~ ~ and b i 0 m o ~ b k . d in implant p m D d U~e2k416-424 Im.
&d& R: Bimdmkid m m i d m & m m w m v prmbma, J U M 49:84284%. 1983,
Whh GB: Oswintqmid &#I m h o b -, 1993,
ztm=A:mwcitni*al-d ~ i n ~ ~ ~ t h T w . o a r t a ~ , P s r t I ! ~ mu@ J-1 h w t 63;451457,1Wh.
Z a r b Q A , S & d t A : ' l l h e ~ ~ c l i n i c a l e f t W ~ r o f ~ i n ~ i m p ~ ~ T o r o n t o ~ . P a r t a : ~ pathetic rmb, 3 P r d M Deat 64:5341,1!M%.
m b Q A , ~ k T h e ~ ~ I . A ~ study m the mffwtiymm of ~~ ftxwl
JAm Death f 2TS8-M, 1996.

Managing . ., . . Problems and C~~m~l icat ions I,l L ~ I I ~ ~ , - ~
& & & $ w e n ~ , k k r t ,, *r.L.Izl,* L- a , i L l
Acthe &eatmat with owmkgrated implants ~ r s p o u l s a p e r i o d a f ~ m w t h s , 4 m d i t i s pwiW that pbIems or cmnplimticm may occur a t w y - t i m e ~ m p h d w - t . m ~ her t in of tfte f d e d prostbasis marks the a d of actim tm-t, ~ O ~ I I W - U ~ wm- and mmhxhg of the pro-s, the implants, and the host tissue8 m p m w mast c~ntinue for the life of the pdmt f'T"le 29- 1).
Thedmd;mPhfieldisinundatedwitha * OftecW-, dw&m and, of CUrn'Be, man- ufactmm'dahrm h l ~ a t t h i s ~ f i e M t h e ~ h 0 ~ c O ~ b y ~ d i f f ~ ~ d to place mi mmre dental implants. Likewise, ale c m q A h t b s h i can occur with dental * W ~ t O t r e g u i t r : & d
AII 411- to wddm of tbe d h c e s k ta dimw the sigailarities among be-authored hphts. All dmseow implants arre p l m d in a ~ ~ . I all must be made of a materid &at is ~ i 1 0 aad powssa favorable phys- fd m d m k a I p p d e s l Po function as reten- tive md m p p t h g mec$&m for dental ~ ~ ~ a l l m u g t u a d e r g o a ~ p m e s s b € a ~ a m lmg-tmn nwivd. Mtboagh &ere are dtim on mgkd tecfiniques and implant mate- d, h w &fRmmm ate generally minor, The mphd implant healing i n M bufm o c c ~ oftendoessh does show^ variety.
Implants that are daigued to h d to the jaw- bone m y da so && a period of no mechanical ~ W ~ o h e c l r a s a i c ~ h u s e d h d&ve d t e g d m and re* a period of mdiskiiutd implant plamme~t bbanea~ the oraI m c m l far 3 to 4 months in the d b l e aad 6 lmn& inthe maxilla. A t h end of that healing
I
p e r i o d t h e d & g e o f ~ t ~ ~ w h i e h 5 h e ~ m e r i n g t h e i m p ~ k ~ ~ c d I y r e d a n d - d c - & ~ t o ~ ~ t . ~ i s t h e * ~ I ~ h t o ~ ~ . l a ~ ~ t a ~ ~ c e d u r e , s o m e ~ W a r e p ~ i n s r s c h z t ~ ~ to allow an attadled hading abutmeat to pgQ ' ~ u g h t h e d ~ ~ t t h e ~ m t s t a g e d t x d ~ mm.t 3ecause khm is no mwwa cmxir@ &oh . i m p l a n t , t h e r e i ~ m s t a g e ~ ~ t h u s ~ ~ ~ i ~ ~ a s ~ o ~ 6 a g e # . X t l ~ silwthm, efbm am made to m i d fumhml I ~ g o f t h e i m p l m t l m C i l t h e b o n c b a r s a ~ to heal a d j m to tbe implant md tmm lbs 0 s h - m .
~ t d w a c P r r e n t a n d m d u l ~ . f o r t h e w ~ o f i m t m e d i r t t e ~ l a r r d i n g . ~ ~ ~ a r i g i d c ~ o f i m p ~ 1 & o r f ~ y a f k r ~ & p t o m s e m e n t ~ t h e j a w . ~ . r ig idinapiarrt~**eimplantsmb l r s s d t u ~ t l p p r k a ~ s i s ~ o s t i m m ~ r a f k r s t a g e I ~ e a y , T h e i m p ~ ~ m ~ I
h m d t a & Id imp2ants. In another q p m & 1 implants arc placed a ~~ suppdng m e c m P b r m i d i a d i v i t k a a i - w ~ e s e a . T h e s e s h g I e i m p h t s o r r e ~ n o a ~ n e ~ t s d t o r e e t h a r t o ~ ~ b p r t a r e ~ ~ retain provisid mmations tbat are pha&$i m&~, but not Mod 1e cancWm This appmch L ~ l u a s of an itmediatip& siolenl haplat&
Although it seems that there are many a p ~ t o ~ W ~ ~ c d ~ o f W d i f f e P e n t ~ d e m o n s t r a t e g a n ~ c d &tie%. In the -*en inme&@ l d , x t E d M a t e ~ d ~ t & t h e m i s a ~ o d ~ w h i c h t h u ~ h t m w ~

ChPptcr 29 M a d f i g Pmblems and CompliQliom
Stage 1 Q W r Y Unfawrak implant positionlalignment
~w-stage I sutgery . kvettfnghhymosls Infedon Suture remnans, wound dehiscence W ~ P *
Stage II w ~ w y Failure to osmintegmte Unfavorable position or angle makes implant unudle
Postpm#hodontic Pmsthodontic complications insertion M tissue complications
Delayed Delayed toss of complications o w integration
Component fracttrre Soft tissue complidm
pmckd from functional loading, The f im two approaches address this pmbiion by avoiding farce tmnmission to the impkt drrriag the early p W of healing* The hmedh load approach splints the implants to each other thereby CI'E&I# a rigid body that k relatively resistant to movemat. In the immediate p r o v i i d implant therapy the implant is placed u&r minimal functional load ~~ asnmpih thattBis load wi1l notdisplace the implaut dflciemtly to intarfete with bone-to- implftrlt heal@. Wfthout bowto-implaat healing the 1oag.W mdml dthe implant is d h l y to
bS&W h -8 of m u t i O I l will be campmid or pmmted This campbtian, fail- So &eve or mthhin osseaktegrati~n, is qg&d as the must crucial problem in implant denthtTy.
~ m ~ ~ s t o ~ f h e p o * sibIe compli&m can k awuntmd. lkty ~ ~ r e f ~ b ~ d y a r w ~ o r pro&&-, biohgxal or muctmd, funchrd or&eti.c, o r h a r d t i a u e o r s o f t t i s s u e ~ In this dqkr, b y are divided under the mrria h d - fngs of *Fei I or ~ O d o n t i c origin. This m b prhtim relates to the phase of treatment rather than the ageeifb @pe af cmqlidm &hat is encmmrd Hawever, it mat be ~~ dm
cornpfi~ona in one arearmy affect the de r* & cormwhy, at times there is no e l m diE& tion between them.
SU RGICALLY RELATED COM PLlCATlONS En&=wimph m g e q ctra b8 deBmiW as tr om- or r tm4aga procedw, Both Wmiquw demand placement af the implant witbin the elM host bQns sib with a mdculw mgicd prodwe. A two-stage implant k placed in a @- tion Ehd allown tha d mimsa to be &oared pi- marily over the implant, where= a one-stage implant is one that p a s through the I P o t h a p p a & s ~ ~ ~ ~ o f # e urd tisslaes in tbe hwhplmt qmea. LWwisu, b o l h ~ q u e s ~ a p e r i o d o f ~ h ~ l h g ~ f m t h e i n r p ~ ~ ~ ~ ~ A m ~ tian.
Surgically related problams can, in turn, be subdivided into c ~ ~ c r r l order thorn dated to w e I surgery, to the mmhkgrat i~f l time b a ~ t b r s ~ d ~ aadtumgeIImg~.The surgeon will prhteafi'Iydd WiththeseaGfxmmm; howwer, it is ~ ~ d e n t i s t , b a v i n g ~ tbe original di ios i s and treatment p h for the patient, who will be d t e d when a problem a e s . As the pmmibing and refem@ &nth& the patient's closest awmWon b with him or her. The pr#cri%ing dentist must fhfxefore be m g d d as that treatment p1mk architect and &ouM be aware of the pmibie compl idmi that m y occm dm- ing this early phaare of katment. The dantist &e should be prqmed ta deal with the patientb bensims and concerns amd tb & neceswy referrafs to the sqemn.
Any ~urgical pm& carries *th it the risk of bleeding, hfkction, mlling, and e d y m o & , and surgery for the placement of osscoinktpted i m p h b is no mcqptim. A meticuloudi A l e mr- gical technique, accompkd with appmphte m'bioticpmxiptiaa a n d i n s ~ t u t h e ~ t regarding hygiene and oral rims, h the W p m ~ v e m e a s u r e a o ~ t h e c h a n c e s o f ~ sequelm. EXCUB& bleed@, if it o c m , isumdy noted at the time of surgery or sorar &. If

Intern1 trehbaeen Siage 1 and %age It I t i s u r r u a l f o r ~ ~ t o ~ ~ t o ~ f i o r n ~ t b i r ~ p r o s t h ~ f o r a ~ t a o a t t i m e ~ ~ ~ A t ~ ~ o f ~ p e r i o a t f a e ~ w a f a o e o f & e d e n t u t e i s ~ suffIcientmy to dm for the plamlm of * ti5sw ~ o n d i i i o n e f o r ~ l i n i x l g a t least 112mut ?%i&inthenq&naftbimplauts.Anksting~ ~ t h t ~ o f ~ ~ c b ~ k ~ ~ ~ ~ ~ f l r r n l ~ i t ~ ~ ~ ~ k e r ~ t h u ~ i o n o f ~ i c ~ b i ~ g o ~ r ~ bm:famh6 B=useth~ mgid M s i q n n q v b ' ~ i u r h e w ~ ~ f " x r s a l ~ r u l i o n 0 f t B i a ~ i n ~ ~ & ~ i s n o t c ~ n p ~ ~ 2 ~ ~ ~ ~ . X n t h i s ~ i t ~ a s l ~ ~ s & y w a m - M k w & t h e W ~ ' E D ~ @ e n t d i b m f o r t M ~ ~ f h E W m s i b e . ' I h i s k t i p e i n e i t l t e P ~
~ ~ ~ e s o f t h e ~ t , t h e ~ ~ a r ~ ~ ~ ~ ~ ~ d ' ~

R d p a for Vmish for Tissue Condjt h e r
f4 anl 1-1-1 trldWtmant i rnl wioplymerizingauylic r&n powder Uringa g&w httlewith a tightly closing lid, add
the ail-merizing wlir wsin powder to lfie tti&kiw&hane satvent. This s ill tak a few h a m u dissalve rempletdy. The result- ity sfiQuld k as rbc~us as glycer- ha #,it O found that it i s tQo thick, adadd dwenc if it b im thin, add powder.
A small ;rrhwa&oJd be &-d into a p b I . : tk nr&cin~ cup 4 applied ta the entire wr- , face d t b tisssle mditiomr, paying qs&l , attention ~a the m m between the &nure
W mid the tinug anditvmer.
&*- Sire-

-%Wf Wr$$jDIbcmqsurmi&ding the imt&*thtI&ofofmdb@aph k M W v e o f a ~ i*M has nst osdmaedb rn implant was *,and* p a h t mrt4 wid ~ ~ f & t w h e n W i B ~ . . , 6 n t h g ~ a f t h e r r a d b @ a p h i r a n iW!t?nt.tbkt * and ha6 W %rnPtclm or &ps d Wun.

FI- 2S2 One week a h H s u w , the healing abutment, which w a s attached ta the center impknt, is partially mred by mucost, The patient r e W d mte pain and d i amfort as the covering tissue was pinched duri@ w a r of hi$ dimture (A). Replacement of the sh- haling aktmervt with a one eliminated the $IsEMmfort and a J I d the inflmd m u m to heal @),


Chapter 29 M a w 8 Roblems and compliatbns S 3
fik%@WW
al ly p l l d q 9 n d ~~y dBqmk3 mkh ammgmnmt, it rimy becum evident that sn orid- n a l l y p ~ f ~ ~ & ~ ~ ~ ~ m t a be altered to a himtble dmp (q,, an ove&n- me), B m of such casa am implants that b t w e h a d t p ~ b p h c a i i n a ~ l h e ~ t h e front of the mandible a& m@Tamt 1- ~ ~ ~ ~ a e d d b u - karcha
INSERTION OF PROSTHESIS

modate both the soft tissue anatomy of tfie poste- rior part of the m o d and the implant abutment and hardware connection in the aukxior. It may & newsary to mDmu the othefwise useful men- siom into the retrornylohyoid space to oomplctely seat the overdenture.
Som ptienb with implant o v d d m s fmd that hod will collect under the anterior part of the denture, whether it be &ed by a bar and clip ~ M y o r b y b a U ~ h m e n t s . T h i s i s d u e p d y t o the relatively imamate impression of tbe aaatomy ~ ( ~ t h a t t h e i l n ~ s i o l l t r a y h a d ~ ~ madewi&thusualinthis a r e a t u ~ o d p l t e the impression copings and was t h h r e too wide to achieve an acmde impression of mucosa) and partly to lhe blockat around fb mention hard- that was done befbre the fmai pessing. A chair- side addhion of aa a ~ I y n ~ ~ acrylic resin to the lingual and labial flanges in tbis a m usually wives this problem.
If a bar and clip assembly is we4 the clip may make it very Widt to remove the overdenture, dm it is l m d slightly before the first inser- tion, It cm easily be tightened after the othm usual procedum of insertion of a compIetI: denture are c0mpIeted.
In the im daya after W o n of tbe d e n - ture, the patient m y experience minor denture irri- tations under the soft tissue-qqorted area of the psthe6i.j. This i~ correchd as the denw is relieved and adjusted in the customary fashion,
Dahg the years of prosthesis wear, there are a number of p i b l e complications that may occur. Some of these are common to both f m d and removable pmthmes, whereas &em are more specific. The mmpfi~tions fall under the broad hadmgs of bi01ogic.d and ploshdontic mechani- cal anes (Table 29-2).
Biological compfidons include failure or lotis of integration and soft and hard tissue complica- tions. W u s e ossmiakgration appears to result fiom an induced and controlled healing response, it is not mprking that three fo& or more of all repwted implant failures caur during the early heding .phase. The remaining failures occur after mIW loading takes place and are in all likeli-
1 0 9 1 F L Z - i a Pmrthadontic Pmblernr and Complications
Structural Prosthesis fracture Fracture of prosthesis retaining xrew Fracture of abutment screw Fracture of implant
Cosmetic As perceived by patient and dentist Functional Speech problems
Transient rnusde discomfort or tempommandibular diwrders
hood caused by an inadequate healing response becoming compromised by subsequent loading demands. Meticulous treatment planning addresses the remote possibility of the small, if inevitable, failures. This will ensure successful p r u s ~ t i c treatment outcomes even when fewer implants than hoped for actually ossointegmted. The obvious exaq1e d d be tbe c o n v ~ o n of a proposed five- u n i t f i x e d p s t h e s ~ t o a t w o - o r ~ u n i t o v ~ - ture if two or three imphta should fail. Sofi axtd hard tissue problem are a h encountered and m a source of same mtroversy. A periodontic type of mindset cafisidm such changes as a version of @- odontal dkaselilre sequelae. On the otherbarn4 gOr, ed research, including d&i book's editam, argue for a mhPmical and microbiological cause that challengesthe implant's m m d i n g gingival tissues rather than its mkylotic-lih attachment.
Structural All of the three levels of components of the cam- pleted implant-retained system are subjected to repeated stresses of acclusal and pmfmctional loading, and it is possible for these stressa fo cause fractures of my of theae components: the prosthdic retaining screw, the abutment screw, or the implant itself (Figme 29-4). Most common is the fracture of the gold alloy screw, usually at the trase of the head of the screw, If the tcp of the threaded area is acces- sible, the s c m fragment can be moved by care- fully touching the outside- of the top of the h t m d piece, whch is remaining in the center screw of the abuaent, with a taped fm bur in either a slow-speed hnmdpiece or a high-speed handpiece

r m l h k g a i ~ l m ~ ~ ~ h ~ c u l t o f i f t b R ~ ~ ~ b ~ * w e a ~ ~ t o g r a s p ~ & ~ m d ~ e n t b ~ t d ~ ~ ~ b a ~ t m i t c o w m m ? ~ t o r m m a ? i e r ~ . I f & e d t h e g 4 d ~ ~ e a n ~ b s ~ l p l n t b e ~ h ~ ~ E h e ? q t a f t h s ~ , benchmmwf Wpatbnt'Brmuth i t m a y b e ~ Q u t k y u n ~ t h e t a p a f t h C e m ~ a ~ ~ ~ o f ~ -with mapiumemd rotating tbe explum tip preclude ~ o f o f ~ b u t i m m h g i n a ~ ~ ~ a a F ~ p w s ~ ~ - o f t h e t e s t m b c a ~ . ~ m l e r p o p -

c l ~ t o r e m o v e t h e a s c r e w f c a ~ f r o m t l l 4 b , implant. C M b this prowdm is not as ~ l i ~ as this W p t i o n suggests, wpcd dally if the abutment screw fragment seems to have bonded itself to the interior of tbe b&mQ Another approach is to very carefully pqwe s "well'" at the top of the screw hgment with a d
F&tm 3 B 4 mntV The clfnkl p h o x m h (g shows twg implants with amchd abutments me abutmnt-dning xrwv in tRe ImpIant on h.fIght is imt&, whereas the head of the retaining svew in the mldrtle implant is fractured. On the left of this ghow
the abutment is off b u s e its mining screw hasfmured at the thtwded area, thus iluminating the ~ f u n c t i o n b f W m ~ e ~ I d a n . n n t x m w ~ k a s f r a d u d ~ ~ i ~ m p M ~ k d ~ n e ~ g m t m t o ~ r t a n m a g e r o i h e ~ a r ~ e d
&theimplant.
~ e s t o a i n t d ~ a s k l n d a r d ~ d r i v e r i s P r t t & ~ ~ ~ d s f f e w ~ h b e e a s i f y ~ outo f tbe impkt
~ o f m & ~ ~ ~ t L ~ u r e d k k x dawn 3s lm@ is more rtifficult, and p a t care must be taken to m i d the intend tlm&a of the Implant. The we of an explorer to
the- o u t o f i ~ seat is demkd in the ~~pmgmph.An&mneataffewrsXrievdor ~ k i t i ~ ~ e t o w i n c ~ ~ e r e r e m o v a I i mori: diffimk. The kit can& an end- t o o l t b a t ~ t h e t u p o f ~ ~ ~ n t when premm b applied Tt isr then rotated comb-
round bw (accompanied by generour, m&m) and then to uece a larger round bur, held either in a handheld toque driver or in the cutting tool h o b provided in the rebigvat kit. The h e r mmd bur is pressed onto the prepared top surface of &the smw and turned c w ~ ~ I o c k w i s e to remove it.
Removal can be further complicated by soft tis- sue oveqmvh or cohpe iuto the p t immedi- ately above the implant. Not only does this p m w t a c lm view of the bop of the fractured abutment, but also tihete is o h some bleeding became with a h c b d retaining component, the implant- s u p p d bridge - ia d e and pinches the mucosa, causing it to W
m e i l R m m W i r r r r ~ 1 v w d i n m ~ t ~ r e m w e t b e b m k e m ~ t m e n t ~ m i s t b e u a e d withexkemecaretoavrriddamgeto the threadsm the h&or d&e implant. If the intenad h x u h of- the. implant have been damaged, it will be dif&xdt t o ~ ~ ~ l ~ t s t b u t r a e n t ~ . I n m c h a case, the fahre tap, alao inchled in he kit, can then be used to repair the theads.
The implant itself is also subject to m, though fbrhmtely this is a wry me occurrence. The hw upper Imld of tbe system act as '%sea" and uswuywill hartwebefore damaging s ~ e s ~ can c a w fracture of the imphut. If an implmt does &lure, it is w d l y at the level of the base of the abutment cemtw screw, aad, in most cases, it happens when the bone hl dm has reached this point. The e g implant fbgmmt must be removed by the mgem using atrqiine becausu it almast always mnab o s s e o ~ c
W h e p l w e r c o q m m t ~ h a r d w a r e ~ the implant-qpmed bridge and its r e l s r t i o ~ to the mmining -an, ttBe m c W scheme, and t h e p r e s e n c e a r a d ~ o f d m ~ u l d b e a s s e s s e d v e r y c a r e f d y t o ~ i f i t i s ~ to make akmtiom 80 p m a t f d h r camplidom. L o I l g d e V w ~ ~ l l ~ , egpecially*impws have hold to be plaoed in d&t-Iine w d g u & ~ ratherthaninasemihmarmmgmept,semtoix

B ~ m a r k P l , ~ P , ~ U : ~ . N ~ a ~ e w ~ t c a n c e p t f w ~ ~ $ w ~ m a n d i b l e . ~ ~ h m e ~ c t t o i e a t follow-up EQdy, aim I*h#R%bt Rts k 2-16 1999.
s r o w n m , ~ D P : ~ ~ ~ m s l l t h ~ t i c r a a I i m p h t b f m ~ & m k l o t a ~ r ~ ~ P m & W A P s d L X ) s n t 13:123-7, a001.
~ ~ u , m i a e , w ~ P : ~ ~ r o p o r t ~ f ~ M y lmkd P U h N W Tsoth Waphmmt d5m
4h M ~ e ~ a l 3 : ~ - l a , m1. (=arlUon B, car^^ UE PMddoBtk m- in ~~~ k t a l imp18Qt manant, lnl 3 Drclt iu'adw* 9:w, 1994.
~ ~ ~ E , L t a J t t a l : T h e H a n g K m g B r i ~ R . o t d o o l . ~ ~ 0 f ~ B h r a s m i u l c ~ ~ a F d provisional pm- CItn I m p h l DmI R& RP3 3:I*I'M,,rnl.
s c k s r t s E , M m v S f , C M I J a ~ d A m I y d s o f ~ d d a t e d W * $ r r e n t r w i @ W l a W, Int J W MaiIi!&c Implants 1 5 6 6 2 - 6 6 r
Eck& &,?Woliaa PC: -ti* rwiw of ll?O -$aptaatawinpatfiaIIy-m J w & a t 7 9 & l W l , 1898. . & q m ~ & $ , ~ l M , b & & n U e t a l : Dih-mbd a d ~ ~ f o t b i o t o g f c
u
M d I u & bphm lkfl3.490, ~~. b p p 4 @ R d , ~ ~ ~ h n U s t a l : B ~ ~
527-%1,1998. ~ M , ~ J A d , ~ h U s t a l : B ~ d ~
m E , Ew JQmlW 1#6:721-164,1998, Fr~rrm S. E @ h S, B ~ P Pd3 st al: The w of tramitid
@lanUfmbme&ak f i x t d ~ ~ i n c a m

implant Prosthodontics for Edentulous Patients: Current and Future Directions Emad 5. Elsubeihi, Nikolai Attard, George A. Zarb
Oswhqpdcm has h;ad a dramtic influence on ~~c practice, With its emphasis on &en- tif~ rigor, osmintegration now provides expaned Oreoltment management strategies far virtu@ dl partially and comphelly &ntulou~ patients @WM 30-1 thou@ 30-5). The ctini~d yieM &om osaseahtegration as summed up in Box 30-1 refk4s tbe res& of n m w studies on its effl- Cwy snd effectvmss.
In 19% w repmd the m l t s of the first Nu& American long-term prospdve implant study in prosthtically rndahpthe edentdous patients (W and Sch& 1990). Om p ~ ~ l y w w f* W W fbllt S U C W S S ~ ~ prOgth0- b $ c ~ t m m t dmmes exceeded inctividul ~ p ~ m ' v d ones, and alI ofthe treated patients ikmmsWd ongoing Ioag-term comforkble and Eiumw&l pnwahesm wear, TI& study lrud s u b queotaWa stroll& m&g##d k t the pmi5ion of n fixmi a quasi-Fmd (wdmtm] prosthis was the Qptimal m1utim to romp1&e dentme problems of a funchad mtm (pmWc dadaptatim). It w a s 4 % m d u & d b t & x a a j Q r d ~ o f ~ - ms in w d x g mmowiMe ~~ wa3 patimt- p m i v d cmSm and mbiliw. The latter objwtke wwldberdilywhiditrr#ipectivedthentmrber of sumssfblly 0 8 ~ i n ~ ~ f-m and nu&- s w r e d ~ m e r i t s o f ~ t y r p ~ o n s o f a ~ - n i q u e t h a t h ~ l y m l u t i ~ ~ o d o n t i c tlwamt.
Furthermore, d d m o e now continms the con- tributh of ossmintqption @ a slowing down, or d u d o n , in the kw mesorptive y s that d d ~ b e ~ ! i y t o o c c u r i n ~ ~ t u l o u s s i t e ( a ) of pimped implant plac-. Additimdy, the dm& virtual h e of even minimat mor-
bidity has also become a ~ i ~ c a n t midemtion when prescribed surgical and pro&* dontic protocols are followed This enc~mps the ~ ~ w i o n , albeit a largely anecdotal but very fnquentIy enmmkd we, that a Meat's He quality k significantly eabanced by implant prostbodontics,
Bhenwk's pioneering work in o s s e o ~ - tion ~atFtlpd the conclusions in Box 30-1 d quite understandably led to sawad dewlopmental a n d ~ i n i t i a t i v e s , w h i c h m ~ u p i n Box 30-2. Regrettablyy, very few of the a-bk systems have been validated in the litemme (Eke* Parch, Myshin et d., 19971, and c b for predictab1y We site development tend to remain long on anecdote, if somewhat short on sci- mtificauy dacummtd outcomes. As 21 result both patients and dentists cawnot readily answa the basic question that must be a & d about any SF- t e m ' s o r & d t e c ~ B e f f i x t i v e n e s s ~ Do the pnylossd btomhzolagy and hmvmionr lead to m o ~ gad t h Amrn in hse-le lo whomi it is @d? Tiis has became a dilemma in clinid ~ c e w h m ~ h y p e r i s k s o u ~ the quality of required long-term evidence, which led to the compelling documented outcornea found in Bm 30-1, It is boped hat continued effortsfat scientific validaoion will ewlve into the p r d d c k that dmtists and patients will routinely we when malung ctinical decisions on pmaib'mg implant- supportedretained ptheses & the assochid protocoL.
It is ene-g ta note that siguificant clini- cal march initiatives continue to provide a better understanding of tnaiment outcomers with our pre- ferred implant system, dong with systemic and

- - .- I I:. . . .:.:lg",;
6 - Ptata mq A, The patient with anterior partial edentlrlism (Uan IV Kennedy) was adequate@ restored by the use of a temovable partial denture (Bb This patient had always desired a fixed prosthds, but the ten@ of the edentulous span coupled with inter-arcwrpace considerations precluded a fixed ~ I u t i o n (C and 0).
Continud

Plate 30-1 m t ' d Scrupulous treatment planning, which included comprehensive imaging of the proposed implant sites (not shown), trial teeth set-up, and patient approval, thorough occlusal analysis and fabrication of a surgical splint, permitted design of a porcelain baked to metal fixed prosthesis (E, F, and 6). The optimized esthetic result (H) was achieved via a combination of patient approved prosthetic teeth and a partial labial flange to compensate for ridge morphology deficit and ensure circurn-oral support. The extent of the upper lip movement did not expose the junction of gingival replacement material and actual gingival tissues.
Continued

Plate 30-2 A, Posterior mandibular partial edentulisrn (Class H Kennedy) multd from a failed three unit fixed bridge which necessitated the extraction of both previous abutments. Three osseointegrated implants permitted a new Rxed prosthesis (B, C, an$ D).
Continued

mie 3B-Z &d The pre and past-lrnplitht treatment panoramic fnm shown in E and F reflect the%ccrpe for considering implant prostkodontia for routine partial edentulim involving the posterior mnes of either jaw, I
Continued

Plate 30-3 A, B, and C, This patient with oligodontia underwent preprosthodontic orthodontic treatment, The completed prosthodontic treatment as shown in D, E, and F attests to the versatility of implant prosthodontics for such partially edentulous challenges. This remains the most ecologically prudent treatment, especially for young patients whose natural teeth adjacent to any edentulous span can be spared being prepared.
Continued

H Plate 30-3 wt'd The patient's pre- and post-implant treatment panoramic films (G and H) reflect the post-orthodontic teeth alignment required to facilitate optimal implant placement, as guided by a suitable surgical guide.

Plam 3 0 4 The uw of miniaturized osseointegtated implants for extra-oral use permits variations on a theme of employing ingenious retentive devices to support and stabilize different types of prosthetic replacements for missing facial parts. The implantretained prosthetic eye seen above and the implant-retained prosthetit ears seen in Plate 30-5 r d e d the ingenuity of prosthodontics at its highest level of clinical skill and artistry.

PIak 90-5 Implant-mined silicone prosthetic ears (Bars and dips).

HOST BONE RESPONH
implam in difhmt spmic cmtBb&- ~ 8 i m l t o ~ ~ w o u n d ~ ~ may--- d o a ~ a n d ~ ~ 2 ) . A l ~ t h s ~ o f ~ a f t h e & e ~ l w e ~ ~ ~ t i o n s m ~ m ! ? t h r l t c s m ~ ~ tion ('We 30-21, most did not prwl& #acluiw ~ c e w t h e i m p a c t o f ~ c ~ o n * impm- .Tba~bw-Qf the ~ s t a ? a - & ~ ~ a ~ - ~ ~ ~ ~ s s s f & B a f m p l e ~ . T h i s i s ~ ~ w k d k y t k e f h d f a c t f h a t m ~ about l d bmond, mdmUc, and c d h k p m c e s s e s t n t f m e ~ . T h e r e E e r e n c b ~ p ~ m o r o ~ o f ~ @ ~ a a d a b , 2 0 0 2 ; ~ a n d ~ 1 ~ E B p o s i t o , ~ h , ~ ~ d , , 19%).
Smoking
Table 30-1 l f " 321,l I - I I I I~ I I I I I I I ~ I H .
Total number of implants 2812 Early failure 3.6% Late failure 4.1 % Overall hilure 7.7%
hi eta-analysir d 73 published studies over a 5-ycar period (Erpmito, Hirxh, Lclrhotm, Thomen, 1998). +Data from p q t d i w follow-up studies at the Univerdty ot Toronto slnre 1979.

Maul= J W 1
S U ~ I ~ W gf fnfluerlct$ of Various Factors on Implant Prosthodontic Treatment Outcomes
F d w R b k o f hltPrt Jaw site
tacrarobd I k of Isdlltrd Cornpromid
h e quantity cMnprorni4
boneqmlir,
Age and gender Incision technique Controlled diabetes mellitus Immediate loading Controlled cardiovaxular Exposed threads
disease Lack of bimrtial stabiliration Controlled hypothyroidism Number of supporting implants Hereditav ectodermal disease HlVlAtDS Systemic wrticosteroid
therapy
Mai l la in postmenopawl C~~n~ctanr swll and experience Implant diameter m e n not receiving HRT Compromised infection control tmpbnt dedgnt
Vitamin Mependent rickets lack of initial stabilkdon wren's syndrome Immediate placement in infected DiphOsphonate therapy extraction sodcets
Dieributian of implants
Cisrette smoking k k of antibiatic prophylaxis implant length Irradlatd maxilla Recent chemotherapy lmplarrt materia0
'Mate that with the WR of mokhg and dlBbetes meHitur, the Influence of other sysf~mk mditklm on L ~ & M failure Is basad on casa tepmrr Mi WMl mall ~~rrtpk Sires.
+ h & M mic=mmpic d a r M m am d i d in clmptn 16. Hm, Hormone fephmmt thaw.
m . S u b ~ ~ ~ e ~ W ~ t h e c o n - clusion that dgmW smoking is mmckted with increased risk of implant Mh, inma4 mar- ~ b a r s e ' f ~ k m # p a o r ~ t ~ f t * u e M ~ i n ~ c i ~ ~ ~ ~ b m s h m t a ~ ~ d ~ w o u n d ~ b y ~ e c t - ing i%e chuhtory a d immune symms aod impairing n'mmal cellular function. Fwthmore, it a p p m l h a t c i a r s # e m o ~ ~ s d u l ~ i s associatedFvi&-hipmd*bone density lakr in l i i in both women and men, Howwer, tht watt mecbaaisrn by which mking
its negative e&t on bone is not yet fully rmdmtood. Bone loss occurs if there is an imbal-
ance betlfiulaen the momf of born mmbd and the of of h l l f o r m e d T h -16 &-
e x a m i n i n g ~ e t h e r m e o r B P t b o f ~ m w ~ - ~ ~ ~ t o t b b g s l e l m a ~ i a t & w & ~ g h w ~ T t ~ ~ ~ h l ~ b o n e ~ a t ~ e h r m b a r s p i n e i u ~ ~ ~ ~ ~ h i * ~ ~ ~ d urine p j r d h m h levels, which is cashtent with ~ r m e d ~ ~ m F ~ , i t w u ~ ~ t e d t h a t ~ ~ r e s o r p t i 0 n ~ - a t 8 d w i t b ~ i $ i a p a t t ~ t o ~ p r o - duction md acc:eImati~~ O ~ ~ O X L of eatfosea leaditmg to early menopause an3 higher rate of bone h, On the 0th hand, ~~F


Other Systemic Conditions Cur*sadrraorpkm.Hawith.rarP p t i ~ s m p 1 e s b ~ ~ O f r a t ~ i s ~ m ~
of implant failure ib p@tkrits witb S@gm% @ w n I q ~ b * ~ ~ W * - @ b , d i n l w & € m b ~ & ~ ~ d ' ~ * o n ~ & € x b a n Q ~ -= risk of implant ha. b m ~ h ~ ~ c Q n t r o l i e d ~ hew 1~1- €xatrouaal cfsdbaardar diseetse, controlled hy@yddQ f3XV/xDs, hypphss-
scteroderm9, Erdbim- dimm, a a d l 3 s m w W y ~ ~ W . X t M d b e
hawewer, ibtwi&tbe =@on of the * m b r m ~ ~ ~ a n d ~ - ~ ~ a e , t h e q u d i t y o F m o & ~ d m s m t a f f ~ f& firm m~hSh8, d W lwdd
The SURGICAL PRUTOCOL
i n ~ a a t o r i Q t ~ 0 a a d ~ W l ~ ~ ~ j l l * ~ m c ~ o ~ ~ d ~ t o ~ ~ ~ & clinical s i tua40~~ poor bone is m c o ~ . &mph b i d e the foil-
1. Modifidon of the su@d t e c a mdmppadmof ha sites and& we d ostmbms* Tho p m m e d advan- & sUFh mhniques are h e premtion aa8 l d i d h m a s e k bone Wty of the osteomly a h .
2. M-cation of fb implant design: wider diamm, c h g a in thread design, imodu&on of SeIf-tapping implants*
3, Momcation of implidat topography @ htroduchg roughened ~ W B bo bone to imp- cotzta~t,
B w , the toq4mn benefits of such m o d E i t i m , @ * ~ * ~ d ~ ~ ~ ~ cation, am &ll to be detemhtd c f i d i y . To 1ong-m p- mdks b e nwdd rn ctichble prqposcs for mschined surface imph&j e v e n ~ h e n t h e i m p l a n t ~ ~ e x ~ ~ o r a flm as a B t of bone -on 011 the o&m hand, a m g h & e , P r l t h m & ~ t o i n d u c e more initial bone -tion, xmy in the long-term be prone to infedon-related pmbfem% due to the ~ ~ ~ f ~ 1 0 5 e ~ ~ r i a j adhesion. Further m d i s c ~ e a d y ~ t o t w t t e t ~ d t h e elEct6 of hlpimplmt $llrfm @ogm& in situ.
Thm are cumntly no qmfi~ tools that con- clusively determirae bone quality before the impW surgical ktmendon. Although computed tom%- mphy mmhs a helpful diagnostic h g h g tech- ~ ~ t p m V i ~ i n s i @ t i n t n t h e ~ ~ ~ f h b m e , t h t s ~ ~ ~ ~ ~ y ~ ~ * asful ossmhtegmth Further d at tba ceUuIar level hi also requid to determine the ar- iou steps of the h a k g phenomeruM and to d&w methods of humsing an8 improving it (W- olad Grutwr, 2802). NumBrous -pts to a i m p h s u r f w s w i t h o r g r m c ~ ~ mor- ~ ~ ~ ~ M P s ] ) a n d ~ ~ (=h=yTww**==&d pmgenitw mil migdm and dlfhnwion h m h ~ p r o p o ~ , ~ ~ , ~ e d ~ are still ~ I u s i v e . Clinid qmi- inb ted

CbapPcr 9D Implant Prosthodantics for FdenMew pptientF: Eum d Wure Dirtmbrn 5B
Figurn 301 Lekholm-Zarb dassification of edentulous anterior jawbone quantity and quality, Types A through E reflect a range of wrp t ive patterns relative to the presumed demarcation of the alveolar and basal jawbone (dotted line). Quality mpes 1 through 4 reflech a range of cortical and mncellous patterns, which haw been consistently used in plannlng oral implant treatment.
that implant fadm is a locttlized phenomenon, bew suggested for ddge -ern- S ikqea i f~ haaInnIg potential is yet to be deter- tion, with the gold standard far bone - W i mind Wh at a morphological and cellular Id. autogenous bone. F u a h - i f e & ~ t a & s o m @ - ResemhhacddiuMfhatahealingpbfbr b l e , t f i i s d o e $ w t ~ ~ t e e t b m m t s ~ ~ h t h e g r a f t i ~ ~ ~ p ~ ~ ~ . b e ~ ~ d o r s o f ~ ~ ~ ~,~~~~~~ @m. p h a s e b d b m p W ~ L y e t b b e W -
~ e d ~ ~ a l r r d y , h immw 8une Quantify diate heding pbw is 6 mods.
Maewa, the imp& of t z i l l m d c w Ridge reduction is ru! ongoing and amuhtive ~ & ? 8 d m o F b i d r t y ~ ~ t o b e ~ pmem, and the resultant &dual bone quantity in ~~ p&mb. T%- 18 pt comm c m c o m p n k ~ b p ~ t , ~ , ~ ~ ~ o o h o r t w i l l ~ b e t h e ~ * ~ ~ * m ~ i n n e e d o f ~ ~ ienttoi*t. ~ ~ ~ b o r a e ~ . V a r i Q ~ s ~ a e e d t o f m d a l ~ v c s t o ~ ~ c d ~ i n t h e e d e n t u l o u s p a d e n t ~ b o n e ~ h m & l e d t o v t r r i ~ ~ i n t *

a w h d f ~ ~ ~ ~ w ~ o f T ~ a ~ ~ ~ T h e ~ ~ ~ o f a ~ O # - - ~ y d m ' B e B ~ + a g d ~ t b & n d d d e m n h a m o f a p h p i o - b@Whm-h-**<prn SJ)W* -, aukon, eef, I%%)*
is limited by the health and mtm of ?h@ otal mu~bsa and dae morpho1ogy af b h - a t . e a . A s r a d f pathfsuc- cmrl accepmce of conventional pmdmes, ~ l O w e r ~ l e ~ e d e ~ , r e m a i n s a ~ u ~ ~ ~ ~ a a d i n t h e p a s t l e d t o r n r m ~ i q & d ~ ~ ~ mugid tdmiqm to enlarge Ihe den- m w w -
1. Acceptable inrerarttuul distance 2, Stable jaw r&lationshlp with hilaterdl contach
in retrwded closure
SW* - =-&! *- ~ ~ ~ p w i t h ~ n t f n i m m n ~ f * t Q ! s k i m p l a @ i n ? h ~ m w & ' t , 1 a d m & h , m p t i w ~ * y . M w ~ * ~ of likely favomm site d b e a s k L nla i m p W " ~ t i U n I ~ t h e ~ d h ~ ~ * ~ ~ ~ f D ~ ~ ~ f t # t b e ~ & ~ a f t e r a ~ ~ t p r s M d C 4 t o 6 ~ 1 , ~ h p ~ ~ W ~ w i & a ~ ~ .
Efficacy and k d m h e m s s studies on patient3 with dadaptwe prosthetics who were tm&d with fix& restomtim atrow that these patients ware nipfiwtly Wpd with this techuiqw (see C ~ ~ ) . ) . ~ I t & o u l d b ~ d ~ ~ ~ a t ~ i s ~ , ' d a m * m e m an that the €tram& h?@a of O s d m &at- m e n t & ! U l d b W r ~ l ~ * a p g I i - cation of the technique, S h e mrmy q d m d Imdh- ~ t ~ ~ ~ t mwi pthnts' dantriradiffioultha ~ r s l a b ~ ~ f i d i f ~ ~ ~ h ~ ~ q ~ ~ ~ t b a t ~ e d l e p a t r m & & o n o t ~ ~ a ~ ~ ~ f t h e i r ~ ~ e ~ ~ i n t o a f ~ ~ 0 ~ o n e . M ~ ~ t o ~ ia a sauce of prostheses stability that can be read- ily achi&ed with the presence of twd or more overdentwe abutmmtp,. It is therefole tempting for tht pr~stb-st to inch& such an "Ah&- ated" use of o~smhtqgration in the form of implant-suppmtd ovdentures. Such an applica- tion o h bdtt pt i ca l dinicd and financial advantages, The surgical operatim becomes a r e d u d one, both time rtnd money wise, and the ~ t p p m & h i s k i t a d c t . t o t h e p ~ t ~ ~ i n t h e context of the @mi'# state of hdth or as. Considmible widmice now idmm the M o d benefits obtained by @etrts who w implant- retained overdentures. These benefits hide improved denture stability, expanded scope for aesthetic solutiom, enhanced patient cofi&me and comfort, and retardation of loss of the residud bony ridge height (see Chap- 27).
Th@ initid proposed healing periods for the b u r i e d ~ t s w e t e a n o u t g r o w t h o f e a d y ~ based an extrapolated o h m ? i m h orthopedic d The migimd Br&um&K o s s # ~ t i m technique reqnired a two-stage surgical qipmch

semd ~~ stdim wggest that immedim witb fixed or o v e r d e m
Om1 EtoIoglr and I m p h t Pmhdontia Emlogy is described ta that b m d of biology &lmg with rewm'of mi-- to om ~ e r r t m d e 8 t h e i r ~ ~ , h a bmukr mue it alrw kludm tlre rehti- ~ ~ i u a ~ e t w i r w m a e n t a r s d ~ r e d ~ ~ o r n ~ M c ~ orpar- w ? - a w -hm - to prosthodon- t i c ~ t i ~ x ~ s m t n ~ o r e b e ~ a s a lxlmx Mwwm the-*licit ~ v e n e s s of my prodme @d&q mmm p p m k h s with sub- gingival margins, * m k W m s ridges for wlwd sopport, implwmg twll mot substitutes) a n d * M t i g s m & ~ . c o n s e ~ , ~ t ~ ~ ~ a a t t r e ~ m e n t i w e d may elicit e h g ~ ~ that Id to specific ~~ up&$ mmifmbed as chid camphationur. These inch& recurrent c&a and prMmta1 &sew ~ ~ ~ u n d a ~ ~ a r ' wd mor- pholcgical c l m q p i. e-& cm- pl**hm-ofmch- eoalqical are time;. but also retwpiatierd-smd**ju-tand s l d l l a . I t i e m * - t o w h verymininaatlocdorsystemicmorbidityrecor- ded in long&nn pqective s t u b in impkt p r m h d o ~ i l .

. ,
, , . I . . . .
Figu*a A, In natulml teeth, the structural continuity of tooth and periodontal tissues Is the prod u d of a well-imgmted series of developmental events.

d a, m contrast to natural W, the stmcbd Eontinuity W a n an d - e d implant and its host site is the result of a m n d W t q ptoct~s and not a development81 one.
fable 30-3 3 niffprpnrp~ hptwppn f p p t h and lmalants
AttaEhment mechanism (periodontal ligament) is the result of evolution and has not been replicated
Variable mobility is present; increased mobility m y be reversible
Can be intruded, extruded, or moved In young patients, teeth continue to erupt
Proprioception Has a rich plexus of blood vessels and nerves
in the periodontal ligament Data present to show progress of mucosal
inflammation to periodontal disease
Interfacial osteogeneris (ankylotic-like) is an induced healing response that is readily replicated
Immobile (ankylotic-like)
Cannot be intruded, extruded, or moved (ankylotic-like) In young patients, implants are "left behind" while
surrounding tissues change So-called osseoperception A relative absence of such a sophisticated circulation and
probably innervation Similar data are not present ..
necessarily act as periimplant pathogens. We quencies, and d d o n s of occlugal Io*. In abis regard available evidence as circumstantial at best, cantext, interfacial cracb may result, and these more particularly because i t appears to ignore the eventually coalesce and lead to implant likelihood of a compromised heding or o s s e o b - motion and in time a s ~ t i o n at the inkrfm. grated response, which could eventually succumb Secondary infection is then the likely outcome, to the diverse and unpredictable magnitudes, fre- with complete loss of bony support the inevitable

wmqumce. It is not surprising therefi ding implants &manstrate a microorganism
environment usually associated with periodmbl disease. At this si~ge: crf our hmiBdge h e it may men be tempt@ ta c o n o l ~ that the cause of implant failure is m u l t i f W d and perhap thttt even genetic factors may play a role, Harwevar, our prception is that a reconciliatiqn of the heding p e s s around an implant with the time-dependent nature of the load it is subjected to remains the ma,jur d e t d n m t of implant mc- w s or faiIure. This coavictiun does not ignore the fact that pathogenic rnicroargrmisms in plaque around teeth or implants mtiy have qs- temic health implicatiag,g,@tl~t plaque ~hodd therefore be conm1ldlr .;
SUMMARY ScimtSdly acceptable Weabmnt outcome time hmm for implant loading cover a apectnun of possibilities. This spectmm mgm from wer 20 pars f a &ed c~nmercw pure titanium implants slad ttadithd surgical potowls with dalayed loadhg, to vir t ld iy imnedi& loading - ~ u s ~ v a r i w ~ ~ ~ o f ~ s i t e i l n p m m t md i m p l i m with rnglumd sur- faces. Time, and even b&tm mearch that includes economic benefits, will dtimteIy dotermhe to
extent theccrmplete d m t m e w i l l k ~ ~ by the implant-supported prosthesis. In the mean-
time, there is fit& doubt tbt bth techniqw .cm addrefis the *- ~ d a a l ' s needs. Both ptimta and dentis# ham a h d y b e n e W @nor-
w=n= ~ S Z 1 p a r a $ l A , ~ H L a t a l : V W c r n o f a a a t a I
~ W ~ ~ u t . e v i e s P 0 f ~ s u g p ~ t r y J M - 77271-279,1997.
E k w H I I S . m G A : J m p l a n t ~ a h ~ ~ ~ ~ U ~ o f ~ O ~ 3 C h i h t h 68r103-10% ZW2,
~ M , ~ ~ ~ I m U e t a l : B P l o g i c a l ~ ~ b ~ Q f ~ ~ o r r a l i m p ~ R . ~tiop-~~rtwrn 106:n1-7~, 1 ~ 8 . - ""~=&~geama~[WBdfaaa i n g o r d b p l a t & x a m i m o f & e ~ I g l J G w l MdIo& 1- 1&11-, 1W9,
t e k h o h U , Z a r b G A : P s t i a a t s a s c t i w m d ~ a h ~ P I , ~ T , ~ U A , ~ 3 S s ~ e - pKd -: m m d n ~ h EUdcal dm-, -, 1985, ~ s e r a c o .
M d N D , h f b G A , ~ s a u a r G E ~ a l a d i ~ : A ~ b o o k g f =hm, mw, 1% -
s ~df&ca~-01 WiaWdtHe~brrt
w a t & O , ~ R : ~ C & i l l ~ ~ ~ of bcaw tpd& A&M M, 35-14 20112,
Zwb OA, Sahmitt A: The ~~ clinIcd c£fecfivmss of om&qwdM*ts : theTorontoS~.PmII: 'I% pmtbth rksrdtir,Jm# Dmt 645361,1490.