Embed Size (px)
Citation preview
12 T H E ESSENTIAL D R U G S C O N C E P T
(ii)
treatment (1997). Azithromycin is not on the WHO Essential Drugs List because of its high cost' (quoted from 'Access to essential drugs, background paper, May 1999, Health Technol- ogy and Pharmaceuticals Cluster, E D M Depart- ment, WHO). 'Triple therapy is beyond the budgets of most drug programmes . . . ' 'All [statins] remain very costly but may be cost-effective for secondary prevention of cardiovascular disease as well as for primary prevention in some very high risk patients .. . none is included on the list' (quoted from the 1 l th WHO EDL).
Every day, access to essential drugs becomes a higher priority for governments. This is reflected, for example, in the final statement on health adopted by govern- ments attending the G 8 0 l d n a w a Summit in 2000. In addition, on 17 August 2000, the U N Sub-Commis- sion for the Protection and Promotion of Human Rights adopted a high profile resolution on 'Intellectual property rights and human rights'. The Sub-Commis- sion declared that ' . . . implementation of the TRIPS Agreement does not adequately reflect the fundamental nature and indivisibility of all human rights, including the right of everyone to enjoy the benefits of scientific progress and its applications, the right to health, the right to food, and the right to self-determination . . . ' ,
'requests all Governments and national, regional and international economic policy forums to take interna- tional human rights obligations and principles fully into account in international economic policy formulation.' and 'recommends to the World Intellectual Property Organization, the World Health Organization, the Uni- ted Nations Development Programme, the United Na- tions Conference on Trade and Development, the United Nations Environment Programme and other relevant United Nations agencies that they continue and deepen their analysis of the impacts of the TRIPS Agreement, including a consideration of its human rights implications'.
The EDL is yet again confronted with scientific and political challenges, similar to the ones encountered when the list was first launched more than 20 years ago. It seems that more and more political decisions are taken with the aim of improving access to essential drugs considered as a basic human right. The WHO not only has the challenge of defining a EDL that addresses today's epidemiological reality, but also the responsibility to assist countries in gaining access to these treatments. This assistance will include addres- sing the effects of international trade agreements both at the national and international levels.
Received 20 May 2002; accepted for publication 15 November 2002
T R A N S A C T I O N S OF T H E ROYAL SOCIETY OF T R O P I C A L MEDICINE AND HYGIENE (2003) 97, 12 -13
Debate that "This house believes the essential drug concept hinders the effective deployment of drugs in developing countries"
Proposing the motion
John Horton Tropical Projects, 24 The Paddock, Hitchin, UK
Keywords: chemotherapy, drugs, Essential Drugs List
The WHO essential drugs concept had its beginnings in a Statement by its Director General at the 28th World Health Assembly in 1975. In it, he identified the concept as being a model for countries to develop their own lists in the future. The first Essential Drugs List (EDL) was produced in 1977, and was truly a list of essential drugs, identifying as it did the minimal com- ponents for a system of basic health care. The first list had 206 items listed, and since that time there has been an increase every 2 years that the Committee has met, with the list standing at over 360 items in 2001. While the increase is to be welcomed, it should be noted that only 33 of the additions have been developed in the 25 years since the list was first produced. This includes a number of anticancer agents, and of course anti-HIV drugs, together with some antibiotics which only ap- pear on a restricted list. Thus much of the list com- prises products that were 'old' even in 1977.
One could therefore argue that the EDL encourages the provision of outmoded medicines for the people of the developing world, and essentially excludes them from advances in medical science. This is brought
Address for correspondence: Dr John Horton, Tropical Pro- jects, 24 The Paddock, Hitchin, Hertfordshire SG4 9EF, UK; e-mail [email protected]
home with force when it is realized that most countries will not consider using any drug (even in emergency situations) that is not on the EDL, despite evidence that newer drugs may be more effective and/or more cost-effective. It seems that the EDL concept is being driven not by cost-benefit (or cost-efficacy), but by cost alone. Thus, all but a few products on the EDL are available as generics, and are often of very low cost. That makes sense in a world where health budgets are very limited, and drugs are often 'out of pocket' ex- penses for the user. Nonetheless, this can be a double- edged sword if controls are not in place to ensure the quality of the drugs that are being purchased by either the public or private user. While a great many products are undoubtedly easy to formulate, and there is no question over their bioavailability, for others, such as the benzimidazole anthelmintics and the antimalarial pyrimethamine, there are major problems with formu- lation. There is therefore a need for a testing network to support countries that do not have the resources to establish and properly staff their own quality control laboratories. Without this, and following purely the cost indicator 'cheapest is best', limited resources may be wasted, and, furthermore, drug resistance can be en- couraged.
A detailed examination of the changes that have occurred in the EDL over the past 25 years raises a
T H E E S S E N T I A L D R U G S C O N C E P T 13
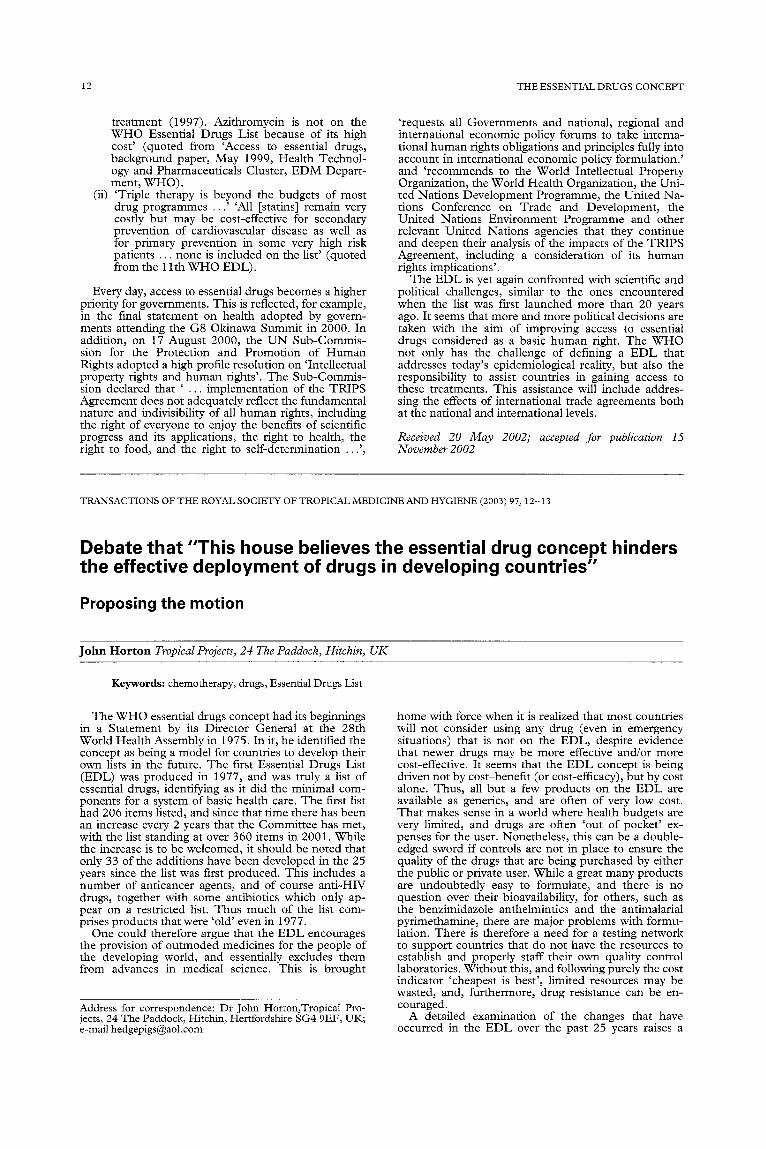
Bephenium TCE Piperazine Tiabendazole Pyrantel Levamisole Mebendazole Albendazole Niclosamide Praziquantel
Licenced 1950s 1920s 1949 1961 1966 1961 1974 1981 1960 1976
~ 1983 1985 1987 1989 1992 1995 199
Fig. 1. Anthelmintics on the WHO Essential Drugs List, date of licensure and of inclusion/exclusion. Key: solid shading, main list; hatched shading, supplementary list; A, albendazole was not registered for hydatid at this time.
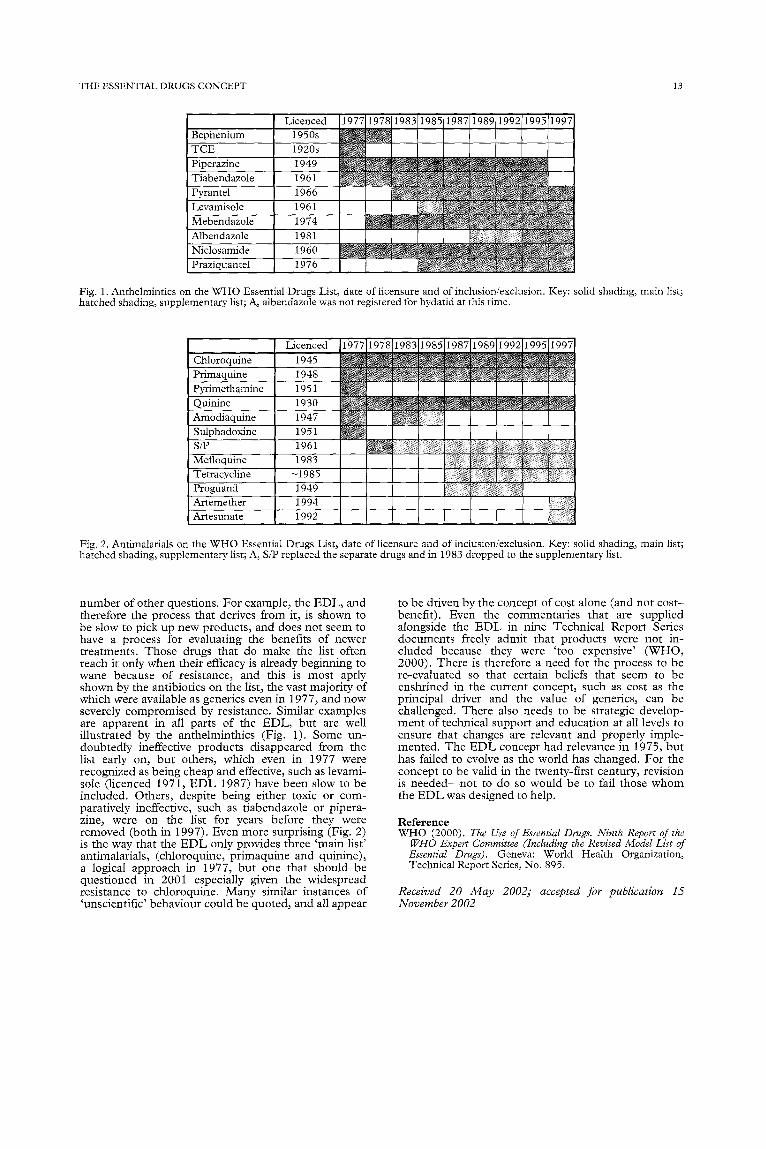
Licenced Chloroquine 1945 Primaquine 1948 Pyrimethamine 1951 Quinine 1930 Amodiaquine 1947 Sulphadoxine 1951 S/P 1961 Mefloquine 1983 Tetracycline ~1985 Proguanil 1949 Artemether 1994 Artesunate 1992
~ 1983 1985 1987 1989 1992 1995 1997
............ ~ ! ~ ! ........ ~ % ~ : i N~
ii !iiiiiiii i!i: i!i ; ! ,ii!i:iiiiii!ii }ii?iiiiiii!iiiiiiii:i:iiii :!iii!) i!; [ I i!!iiii!!iiiii!i:iiiill ! iii!!iii:!iillili iiii!iii!ii, iiiiiiii iiiliiiii:!iiiiiiii!i! I I ::iii!!ii!i!ii!!i!i i!!iii : i!iiiiiiiiiiiii!iii!iiiilil I [ !iiiii!iiii!iil)!:iii ii!ii!i!?iiii!i! !ii!iii!ii!!li!!i?i!i
!i!iii:!ii!ii!i~i!ii!!~!iii:
Fig. 2. Antimalarials on the WHO Essential Drugs List, date of licensure and of inclusion/exclusion. Key: solid shading, main list; hatched shading, supplementary list; A, S/P replaced the separate drugs and in 1983 dropped to the supplementary list.
number of other questions. For example, the E D L , and therefore the process that derives from it, is shown to be slow to pick up new products, and does not seem to have a process for evaluating the benefits of newer treatments. Those drugs that do make the list often reach it only when their efficacy is already beginning to wane because of resistance, and this is most aptly shown by the antibiotics on the list, the vast majority of which were available as generics even in 1977, and now severely compromised by resistance. Similar examples are apparent in all parts of the E D L , but are well illustrated by the anthelminthics (Fig. 1). Some un- doubtedly ineffective products disappeared from the list early on, but others, which even in 1977 were recognized as being cheap and effective, such as levami- sole (licenced 1971, E D L 1987) have been slow to be included. Others, despite being either toxic or com- paratively ineffective, such as t iabendazole or pipera- zine, were on the list for years before they were removed (both in 1997). Even more surprising (Fig. 2) is the way that the E D L only provides three 'main list' antimalarials, (chloroquine, pr imaquine and quinine), a logical approach in 1977, but one that should be quest ioned in 2001 especially given the widespread resistance to chloroquine. Many similar instances of 'unscientific ' behaviour could be quoted, and all appear
to be driven by the concept of cost alone (and not cos t - benefit). Even the commentar ies that are supplied alongside the E D L in nine Technical Report Series documents freely admit that products were not in- cluded because they were ' too expensive' (WHO, 2000). There is therefore a need for the process to be re-evaluated so that certain beliefs that seem to be enshrined in the current concept, such as cost as the principal driver and the value of generics, can be challenged. There also needs to be strategic develop- ment of technical support and education at all levels to ensure that changes are relevant and properly imple- mented. The E D L concept had relevance in 1975, but has failed to evolve as the world has changed. For the concept to be valid in the twenty-first century, revision is n e e d e d - - n o t to do so would be to fail those w h o m the E D L was designed to help.
Reference WHO (2000). The Use of Essential Drugs. Ninth Report of the
WHO Expert Committee (Including the Revised Model List of Essential Drugs). Geneva: World Health Organization, Technical Report Series, No. 895.
Received 20 May 2002; accepted for publication 15 November 2002

![Strategic Behavior in Unbalanced Matching Marketsscholar.harvard.edu/files/ran/files/cgs_0.pdf · strategy for the proposing side [6, 18]. The choice of the proposing side has received](https://img.pdfslide.us/doc/110x75/5fbac33e7c968e6af2799faa/strategic-behavior-in-unbalanced-matching-strategy-for-the-proposing-side-6-18.jpg)



























