Embed Size (px)
Citation preview

Effective Jan. 2016
Proposed 2022 Updates to Field Treatment Guidelines
Public Comment Package

Field Treatment Guideline 2022 Summary of Updates Reason for change/evidence/other notes
AC05 - Symptomatic Bradycardia
1. Change name to "Bradycardia"2. Increase Initial dose of Atropine to 1mg3. Add hypotension/shock arm with push dose epi4. Add definition of unstable
AC06 - Narrow Tachycardia 1. Change name to "Tachycardia"
AC07 - Wide Tachycardia 1. Delete AC07 and combine with AC06 into single Tachycardia FTG
AC06 - Tachycardia1. Combined both tachycardia FTGs into one.2. Add definition of Unstable3. Add immediate synchronized cardioversion for unstable patients
* Cleaned and clarified algorithm* The concern about NTG causing hypotension in the setting of an inferior wall MI was not seen in two large retrospective studies. (Links to articles below)
Prehospital NTG Safety in Inferior STEMI
Safety and Effectiveness of Field NTG in Patients with Suspected STEMI
Clinical Care and Restraint of Agitated or Combative Patients by Emergency Medical Services Practitioners
* Intranasal delivery may be inconsistant or not immediately effective in uncooperative patients.
A06a - Post-Partum Hemorrhage 1. New FTG for this 2022 The WOMAN Trial: Early TXA in Post-Partum Hemorrhage
Clinical Care and Restraint of Agitated or Combative Patients by Emergency Medical Services Practitioners. Retrieved from NAEMSP.org
* Intranasal delivery may be inconsistant or not immediately effective in uncooperative patients.
T04 - Extremity Trauma 1. Include exit to T09 - Major Hemorrhage control2. Remove references to tourniquet or hemostatic gauze * Moved Major Hemorrhage to new FTG - T09
T06 - Multi System Trauma 1. Include exit to T09 - Major Hemorrhage control2. Remove references to tourniquet or hemostatic gauze * Moved Major Hemorrhage to new FTG - T09
T09 - Major Hemorrhage Control 1. New FTG for this 2022 Effects of Tranexamic Acid on Death, Vascular Occlusive Events, and Blood Transfusion in Trauma Patints with Significant Hemmorhage - Crash-2 Trial
FP30 - TXA Administration 1. New FP for 2022 Effects of Tranexamic Acid on Death, Vascular Occlusive Events, and Blood Transfusion in Trauma Patints with Significant Hemmorhage - Crash-2 Trial
Drug Reference - Page 6 1. Update NTG2. Add TXA * Updates to FTGs required an update in this reference
Drug Reference
* Cleaned and clarified algorithm* Consistent with 2020 AHA guidelines
Adult Cardiac
Adult Medical
Pediatric Medical
Trauma
Field Procedure
1. Update history, s/s and ddx2. Add NTG in STEMI when indicated3. Remove base contact for additional fentanyl4. Add NTG contraindications5. Add indications for fluid administration 6. Clarified STEMI definition to >= 2mm ST elevation in anterior and/or lateral leads
AC08 - Chest Pain and STEMI
A03 - Adult Behavioral
1. Add "Suggested Agitation Categories"2. Increase initial dose of midazolam (10mg IM) for Excited Delerium 3. Increase max dose of midazolam (10mg IM) for Severe Agitation4. Add "caution" direction for reassessment prior to sedation administration5. Removed IN route for Midazolam administration6. Removed from Pearls: "Limit IN administrations to ½ dose in each nare."
P04 - Pediatric Behavioral1. Add "Suggested Agitation Categories" Levels2. Add "Caution" direction for reassessment prior to sedation administration3. Removed IN route for Midazolam administration

Contra Costa County Emergency Medical Services
Symptomatic Bradycardia
Treatment Guideline AC05Page 1 of 2
History• Past medical history• Medications • Beta blockers • Calcium channel blockers • Clonidine • Digoxin• Pacemaker
Differential Acute myocardial infarction Hypoxia Pacemaker failure Hypothermia Sinus bradycardia Athletes Head injury (elevated ICP) or stroke Spinal cord lesion Sick sinus syndrome AV blocks (e.g. 1o, 2o or 3o) Overdose Hypothyroidism
Signs and Symptoms• Heart rate < 60 with:
• Chest pain• Respiratory distress/acute CHF• Hypotension or shock• Altered mental status• Dizziness/Syncope
Cardiac monitor
Establish IV/IO, do not delay pacing for the unstable patient
P 12‐Lead ECG
Transcutaneous pacing
Normal Saline bolus 500ml IV/IO, may repeat as needed Maximum 1L
Consider sedation Midazolam 1mg IV/IO
Titrate in 1‐2mg increments may repeat if neededMaximum 5mg
Notify receiving facility. Contact Base Hospital for
medical direction, as needed.
Effective Jan. 2022
P
EtCO2 monitoring
Consider Push Dose Epi 5mcg (0.5 ml) IV/IOEvery 3 minutes, titrate to a BP > 90
Observe and monitor
Unstable due to BradycardiaHypotension/shock often with signs of poor perfusion Altered mental statusChest pain highly suggestive of ACS:
Severe crushing chest painPale/diaphoreticWith or without evidence of ischemia on EKG (STEMI, T‐wave inversion/depression)
StableIs the patient stable?
P
Consider Atropine 1mg IV/IO while waiting for TCP
May repeat every 3 – 5 minutes as needed
Should not be used in wide‐complex rhythms or in 2o or 3o
heart blocksMaximum 3mg
Consider pain control if BP > 90 Fentanyl 25 – 100mcg IV/IO
in 25 – 50mcg increments May repeat 25mcg every 20
minutes if neededMaximum 200mcg
P

Effective Jan. 2016
Contra Costa County Emergency Medical Services
Symptomatic Bradycardia
Treatment Guideline AC05Page 2 of 2
Pearls
Worsening bradycardia in ROSC may indicate signs of impending rearrest.
Instability due to bradycardia is typically seen with heart rates < 35 bpm. Prehospital treatment is directed toward the unstable patient, otherwise monitor and reassess frequently.
Identifying signs and symptoms of poor perfusion caused by bradycardia is paramount.
Atropine vs. pacing: Caution should be exercised in the setting of a suspected acute MI. The use of Atropine for PVCs in the presence of an acute MI may worsen heart damage. Providers should NOT DELAY transcutaneous pacing for patients with poor perfusion in the setting of an acute MI or 2o or 3o heart block.
For patients who are not in 2o or 3o heart block, pacing may be considered for bradycardia not responsive to Atropine. Prepare to utilize transcutaneous pacing early if the patient does not respond to Atropine.
For wide complex, bizarre appearance of QRS complexes with slow rhythm, consider hyperkalemia.
Consider treatable causes for bradycardia (e.g. beta blocker OD, calcium channel blocker OD, etc.)
Hypoxemia is a common cause of bradycardia. Be sure to oxygenate the patient and support respiratory effort.
Sinus bradycardia in the absence of key symptoms requires no specific treatment; monitor and observe.
Sinus bradycardia is often seen in patients with STEMI or ischemia. An early 12‐Lead ECG should be obtained to assess for STEMI.
A fluid bolus may address hypotension and lessen the need for pacing or treatment with Atropine.
Sedation prior to starting pacing is not required. Patients with urgent needs should be paced first and sedated afterwards.
The objective of sedation with pacing is to decrease discomfort, not to decrease level of consciousness. Patients who are in need of pacing are unstable and sedation should be used with extreme caution.
Monitor respiratory status closely and support ventilation as necessary.
Atropine is not effective for bradycardia in heart transplant patients as there is no vagus nerve innervation in these patients.
Patients with wide QRS or 2o or 3o heart blocks will not have a response to Atropine because the heart rates are not based on vagal tone. An increase in ventricular arrhythmias may occur.
Effective Jan. 2022

Contra Costa County Emergency Medical Services
Tachycardia
Treatment Guideline AC06Page 1 of 2
History• Medications (e.g. Aminophylline, Adderall, diet pills, thyroid supplements, decongestants, and Digoxin)• Diet• Drugs (e.g. nicotine and illegal drugs)• Past medical history• History of palpations/heart racing• Syncope/near syncope
Differential• Dysrhythmia• Sick sinus syndrome • Myocardial infarction• Electrolyte imbalance• Exertion, pain, or emotional stress• Fever/sepsis• Hypoxia• Hypovolemia or anemia• Drug effect/overdose (see History)• Hyperthyroidism• Pulmonary embolus
Signs and Symptoms• Hypotension• Palpitations, dizziness, chest pain, shortness of
breath, altered mental status, or diaphoresis• CHF• Potential presenting rhythm: • Atrial/sinus tachycardia • Atrial fibrillation/flutter • Multifocal atrial tachycardia • Ventricular tachycardia
P
If rhythm change, repeat 12‐Lead ECG
Effective Jan. 2022
PUnstable due to TachycardiaHR typically >150Hypotension/shock often with signs of poor perfusion Altered mental statusChest pain highly suggestive of ACS:
Severe crushing chest painPale/diaphoreticWith or without evidence of ischemia on EKG (STEMI, T‐wave inversion/depression)
If symptomatic, consider
Amiodarone 150mg IV/IO drip
over 10 minutesMay repeat x 1 dose
if needed
P
Consider sedation pre‐cardioversionMidazolam 1mg IV/IO
May repeat if needed in 1‐2mg incrementsMaximum 5mg
Establish IV/IO
Immediate Synchronized CardioversionNarrow Regular: 100J, 150J, 200J…Narrow Irregular: 150J, 200J, 300J…Wide Regular: 150J, 200J, 300J…Wide Irregular: Defibrillate 360J
If any delay in synchronized cardioversion and the patient is critical, defibrillate 360JContact Base Hospital for further direction if recurrent or resistant to initial three (3)
shocks
Notify receiving facility. Contact Base Hospital for
medical direction, as needed.
P
12 lead or Rhythm StripP
P
Narrow or Wide
QRS?
Regular rhythm?
Cardiac monitor
NOE.g. A‐fib/A‐flutter
Yese.g. SVT
Regular rhythm?
Yes
12‐Lead ECG or repeat if rhythm change
Monitor for recurrence. Treat with adenosine
Look for and treat underlying conditions(e.g. dehydration, CHF
exacerbation)
12‐Lead ECG or repeat if rhythm change
Establish IV/IO
WideNarrow
No
Stable
P
P
Continue to monitor, reassess
If patient becomes unstable, go to
appropriate armAdenosine 6mg IV/IO
rapid pushMay repeat 12mg IV/IO
Attempt Vagal maneuver (FP22)
Is patient stable?

Effective Jan. 2016
Contra Costa County Emergency Medical Services
Tachycardia
Treatment Guideline AC06Page 2 of 2
Pearls
In unstable patients with fever or other signs of sepsis, the underlying cause of the rapid heart rate is more likely fever and hypovolemia. This is particularly true in wide irregular tachycardia which is frequently underlying A fib with a bundle branch block. Initial efforts should focus on treating appropriately for underlying sepsis.
If at any point the patient becomes unstable, move to the unstable arm of the algorithm.
For ASYMPTOMATIC patients (or those with only minimal symptom, such as palpitations) and any tachycardia with a rate of approximately 100‐120 with a normal blood pressure, consider CLOSE OBSERVATION or fluid bolus rather than immediate treatment with an anti‐arrhythmic medication.
If patient has a history or if 12 lead ECG reveals Wolfe Parkinson White (WPW), use caution with Adenosine and give only with a defibrillator immediately available.
In Polymorphic VT: torsade de pointes, etc., the variation in QRS morphology may make it difficult to synchronize. If you cannot synchronize, move to defibrillation.
In Wide IRREGULAR rhythm such as AFib with left or right bundle, etc, synchronize cardioversion at 360J is more likely to yield first shock conversion.
Symptomatic tachycardia usually occurs at rates of 120‐150 and typically >150 beats per minute. Patients who are symptomatic with heart rates <150 likely have impaired cardiac function, such as CHF.
Search for underlying cause of tachycardia such as fever, sepsis, dehydration, hypovolemia, etc.
Monitor for respiratory depression and hypotension associated with Midazolam.
Continue pulse oximetry and ETCO2 monitoring is required for all wide complex tachycardia patients.
Providers must export ALL MONITOR DATA to EHR when caring for and treating tachycardia patients.
Effective Jan. 2022

If SBP <90 or drops >30 from baseline after NTG
Withhold further NTG administrationand
Normal Saline bolus 500ml IV/IOMay repeat as needed
Maximum 1L
Effective Jan. 2016
Contra Costa County Emergency Medical Services
Chest Pain: Suspected Cardiac or STEMI
Treatment Guideline AC08Page 1 of 2
History Age Medications Past medical history (e.g. MI, angina, diabetes,
CAD, HTN, hyperlipidemia) Recent physical exertion Provocation Quality (e.g. pressure, constant, sharp, dull,
etc.) Region/Radiation/Referred Severity (0 – 10 scale) Time (onset/duration/repetition)
Differential Acute coronary syndrome (MI, unstable angina) Pulmonary embolus Aortic dissection Pericarditis Pneumothorax Pneumonia Tamponade
Signs and Symptoms Chest pain Shortness of breath Pale, cool, diaphoretic Nausea, vomiting Hypotension or shock Possible bradycardia SyncopeAtypical presentations for elderly patients Epigastric pain Generalized weakness
Cardiac monitor
Aspirin 324mg PO
P
Consider Fentanyl 25 – 200mcg IV titrated in 25 – 50mcg increments
for pain relief if SBP > 90
If initial SBP > 90 Nitroglycerin 0.4mg sublingual May repeat every 5 minutes as needed. Maximum 3 doses.
Use caution and consider base contact if HR >120 prior to administration.Do not administer if patient has taken erectile dysfunction drugs
(e.g. Viagra, Levitra) within the last 24 hours or (e.g. Cialis) within 36 hours.
ApprovedSTEMI Receiving Centers
John Muir – ConcordJohn Muir – Walnut CreekKaiser – Walnut CreekSan Ramon Regional
Sutter DeltaHighland – OaklandKaiser – VallejoMarin General
Summit – OaklandKaiser – Oakland
Valley Care – Pleasanton
Establish IV/IO
P
Notify receiving facility. Contact Base Hospital for
medical direction, as needed.
Effective Jan. 2022
Titrate O2 administration to min needed to maintain goal of 94%‐99% SPO2
Definition of STEMI > 1mm ST segment elevation in inferior, or> 2mm ST segment elevation in anterior or lateral leads,In 2 or more contiguous leads(See 12‐Lead Procedure)
Immediate transmission of 12 lead to STEMI receiving facility
Primary assessment indicates chest pain or signs/symptoms consistent with
cardiac ischemia
STEMI?No Yes
Make STEMI ALERT notification to STEMI receiving facility
P
12‐Lead ECG

Effective Jan. 2016
Contra Costa County Emergency Medical Services
Chest Pain: Suspected Cardiac or STEMI
Treatment Guideline AC08Page 2 of 2
Pearls• Patients with a STEMI should be transported to the closest most appropriate STEMI receiving center.• Many STEMIs evolve during prehospital care and may not be noted on the initial 12‐Lead ECG.• An ECG should be obtained prior to treatment for bradycardia if patient condition permits.• Transmit all 12‐Lead ECGs whether STEMI is detected or not.• If a patient has taken their own Nitroglycerin without relief, consider potency of medication. Provider maximum
doses do not include patient administered doses.• Monitor for hypotension after administration of nitroglycerin and opioids.• Diabetics, geriatric, and female patients often have atypical pain, or only generalized complaints. Suspect cardiac
etiology in these patients, and perform a 12‐Lead ECG.• Document the time of the 12‐Lead ECG in the EHR as a procedure along with the interpretation.
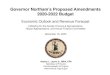
ST Elevation in 2 or more leads: Leads II, III, aVF Inferior wall MI (vessel likely RCA or LCx) ST Elevation in 2 or more leads: Leads I, aVL, V5, V6 Lateral wall MI (vessel likely LCx or LAD branch) ST Elevation in 2 or more leads: Leads V1, V2 Septal wall MI (vessel likely LCx or LAD branch) ST Elevation in 2 or more leads: Leads V3, V4 Anterior wall MI (vessel likely LCx or LAD branch)
**Look for ST DEPRESSION in reciprocal leads (opposite wall) to confirm diagnosis. **Isolated ST elevation in aVR with ST depression in all other leads should raise suspicion for a proximal LAD Artery injury or Left Main Coronary Artery abnormality. This is not STEMI criteria, but the 12‐Lead ECG should be transmitted to the ED for consultation. Consider transport to a STEMI receiving center.
Lateral
LateralInferior
Lateral
Septal
Anterior
Anterior(RVMI)
Effective Jan. 2022

Effective Jan. 2016
Contra Costa County Emergency Medical Services
Adult Behavioral
Treatment Guideline A03Page 1 of 2
History• Situational crisis• Psychiatric illness/medications• Injury to self or threats to others• Medical alert tag• Substance abuse/overdose• Diabetes
Differential• Altered mental status• Alcohol intoxication • Toxin / substance abuse• Medication effect/overdose• Withdrawal symptoms• Depression • Bipolar (manic‐depressive)• Schizophrenia• Anxiety disorders• Hypoglycemia
Signs and Symptoms• Anxiety, agitation or confusion• Affect change or hallucinations• Delusional thoughts or bizarre behavior• Combative or violent • Expression of suicidal/homicidal thoughts
Exit to appropriate TG, if indicated
Altered Mental Status TGDiabetic TG
Overdose/Toxic Ingestion TGHead Trauma TG
Assume patient has medical cause of
behavioral change
Consider IV
E
Consider restraints
Monitor restraints and PMSif indicated
P
Monitor and reassess
Assess patient’s level of Agitation
Blood glucose analysis
P
Midazolam Contact Base Hospital Physician for
additional orderMD
Cardiac monitor
P
If patient is hot to touch or suspected hyperthermia, initiate cooling measures
Notify receiving facility. Contact Base Hospital for
medical direction, as needed.
Effective Jan. 2022
Mild Moderate Severe Excited Delirium
Reassess prior to administration
Reassess prior to administration
Overtly confrontationalPhysically combative (fighting,
spitting, biting)Has little controlNot easily directedNot able to be deescalated
Extremely aggressive or violentPoses immediate and grave danger to self or providers and exhibits the following: Possibly confused or incoherent Unable to maintain attention Significantly increased strength Impervious to pain or fatigue Diaphoresis Hot/flushed skin Tachycardia
** Patients are often found in a protracted physical struggle requiring physical restraint by multiple providers.
Approach patient with caution and begin verbal de‐escalation. Exhaust de‐escalation techniques prior to consideration of physical restraints. Provide continuous reassessment of situation to ensure patient and provider safety.
Anxious/agitated but cooperativeNot aggressive (verbally or physically)Has the potential to be easily provoked or triggered
Verbally confrontational UncooperativeEasily provoked or triggeredThreatening physical posture
(clenched jaw, fists)Not physically combativeDisruptive without danger
Midazolam 5mg IM May repeat 2.5mg every 5
minutes to effectMaximum 10mg
ORMidazolam 1‐3mg IV in 1mg
incrementsAge ≥ 65 years of age 1mg IV/IM May repeat every 5 minutes to
effect. Maximum 5mg
Midazolam 10mg IM
Maximum 10mg

Effective Jan. 2016
Contra Costa County Emergency Medical Services
Adult Behavioral
Treatment Guideline A03Page 2 of 2
Pearls
Crew/responder safety is the main priority. See Policy 1008 – Managing Assaultive Behavior/Patient Restraint.
Use least restrictive method needed to manage patient and to ensure safety.
Use caution when administering Midazolam for postictal patients or patients with alcohol intoxication. Apply waveform capnography and frequently assess for depressed respirations and level of consciousness.
All patients who receive either physical restraint or chemical sedation must be continuously observed by EMS personnel. This includes direct visualization of the patient as well as cardiac and pulse oximetry monitoring.
Consider all possible medical/trauma causes for behavior (e.g. hypoglycemia, overdose, substance abuse, hypoxia, seizure, head injury, etc.).
Do not irritate the patient with a prolonged exam. Be thorough but quick.
Do not overlook the possibility of associated domestic violence or child abuse.
If patient suspected of excited delirium and suffers cardiac arrest, consider fluid bolus and sodium bicarbonate early.
Do not position or transport any restrained patient in a way that negatively affects the patient’s respiratory or circulatory status (e.g. hog‐tied or prone positions). Do not place backboards, splints or other devices on top of the patient.
If restrained, the extremities that are restrained will have a circulation check at least every 15 minutes. The first of these checks should occur as soon after placement of the restraints as possible. This shall be documented in the EHR.
Excited Delirium Syndrome:
This is a medical emergency. The condition is a combination of delirium, psychomotor agitation, anxiety, hallucinations, speech disturbances, disorientation, violent/bizarre behavior, insensitivity to pain, hyperthermia and increased strength. The condition is life‐threatening and is often associated with use of physical control measures, including physical restraints, and tasers. Most commonly seen in male patients with a history of serious mental illness or drug abuse, particularly stimulant drugs such as cocaine, crack cocaine, methamphetamine, amphetamines, bath salts, or similar agents. Alcohol withdrawal or head injury may also contribute to the condition.
Effective Jan. 2022

Effective Jan. 2016
Contra Costa County Emergency Medical Services
Post-Partum Hemorrhage Control
Treatment Guideline A06aPage 1 of 2
History Bleeding < 24 hours after delivery Out of hospital delivery Quantity and duration of bleeding Placenta delivery
Differential Trauma (vaginal or cervical laceration) Uterine atony Retained tissue/placenta Coagulopathy
Signs and Symptoms Bleeding Dizziness/syncope Weakness/dyspnea Confusion/ALOC Hypotension or other signs of shock
Supplemental oxygen as required
Establish IV/IO
P
Notify receiving facility. Contact Base Hospital for
medical direction, as needed.
Effective Jan. 2022
P
Cardiac Monitor
Initiate gentle fundal massage to encourage delivery of placenta. If placenta delivered, massage until uterus is firm.
Encourage breast feeding
Visualize for and manage bleeding from external laceration
E
Primary assessment indicates post‐partum (within last 24 hours) ongoing hemorrhage or
hemodynamic instability
Estimated blood loss >500mlAnd initial SBP < 90?
No Yes
Consider TXA 1gm in 100ml IV/IO over 10 minutes
Normal Saline 500ml ‐ 1000ml bolus to maintain SBP > 90
Maximum 1L

Effective Jan. 2016
Contra Costa County Emergency Medical Services
Post-Partum Hemorrhage Control
Treatment Guideline A06aPage 2 of 2
Effective Jan. 2022
Pearls
PPH is the leading cause of maternal mortality in the world.
Primary Post‐partum hemorrhage is excessive bleeding within the first 24 hours of birth. It is defined as either:
The loss of more than 500 ml of blood following vaginal birth;
Minor: 500 ml to 1 liter
Major: More than 1 liter
The loss of more than 1 liter of blood following a caesarean section; or
Enough blood loss to cause the mother's condition to deteriorate.
Clinical signs of shock may not manifest until considerable blood loss has occurred. Recognition is critical.
Secondary PPH is defined as a loss of more than 500 ml of blood between 24 hours postpartum and 12 weeks postpartum
Fundal massage is the most important intervention for primary post‐partum hemorrhage. It helps contract the uterus and encourage delivery of the placenta.
Breast feeding helps release the hormone, Oxytocin, which also helps contract the uterus.
Causes of Post‐Partum Hemorrhage The Four T's of Post‐Partum Hemorrhage (PPH) include:
Tone – (70% of PPH incidents) Is uterine atony which occurs when the uterus fails to contract after delivery of the baby. Contraction of the uterine muscles helps deliver the placenta, and compresses blood vessels to prevent hemorrhage.
Trauma (20% of PPH incidents), which includes:Lacerations of the cervix, vagina or perineum;
Tissue (10% of PPH incidents), which includes:Retained products, placenta, membranes or clots; orAn abnormal placenta
Thrombin (less than 1% of PPH incidents), which is caused by issues with coagulation.

Effective Jan. 2016
Contra Costa County Emergency Medical Services
Pediatric Behavioral
Treatment Guideline P04Page 1 of 2
History• Situational crisis• Psychiatric illness/medications• Injury to self or threats to others• Medical alert tag• Substance abuse/overdose• Diabetes
Differential• Altered mental status• Alcohol intoxication • Toxin/substance abuse• Medication effect/overdose• Withdrawal symptoms• Depression • Bipolar (manic‐depressive)• Schizophrenia• Anxiety disorders• Hypoglycemia
Signs and Symptoms• Anxiety, agitation or confusion• Affect change or hallucinations• Delusional thoughts or bizarre behavior• Combative or violent • Expression of suicidal/homicidal thoughts
Effective Jan. 2022
Exit to appropriate TG, if indicated
Altered Mental Status TGDiabetic TG
Overdose/Toxic Ingestion TGHead Trauma TG
Assume patient has medical cause of
behavioral changeConsider IV
E
Consider restraints
Monitor restraints and PMSif indicated
Monitor and reassess
Assess patient’s level of Agitation
Blood glucose analysis
P
Midazolam Contact Base Hospital Physician for
additional orderMD
Cardiac monitor
P
If patient is hot to touch or suspected hyperthermia, initiate cooling measures
Notify receiving facility. Contact Base Hospital for
medical direction, as needed.
Mild Moderate Severe Excited Delirium
Reassess prior to administration
Overtly confrontationalPhysically combative (fighting,
spitting, biting)Has little controlNot easily directedNot able to be deescalated
Extremely aggressive or violentPoses immediate and grave danger to self or providers and exhibits the following: Possibly confused or incoherent Unable to maintain attention Significantly increased strength Impervious to pain or fatigue Diaphoresis Hot/flushed skin Tachycardia
** Patients are often found in a protracted physical struggle requiring physical restraint by multiple providers.
Approach patient with caution and begin verbal de‐escalation. Exhaust de‐escalation techniques prior to consideration of physical restraints. Provide continuous reassessment of situation to ensure patient and provider safety.
Anxious/agitated but cooperativeNot aggressive (verbally or physically)Has the potential to be easily provoked or triggered
Verbally confrontational UncooperativeEasily provoked or triggeredThreatening physical posture
(clenched jaw, fists)Not physically combativeDisruptive without danger
For patients ≥ 12 years of ageMidazolam IM
Use Pediatape and refer to dosing guide
Contact base for additional doses as needed

Effective Jan. 2016
Contra Costa County Emergency Medical Services
Pediatric Behavioral
Treatment Guideline P04Page 2 of 2
Pearls
Crew/responder safety is the main priority. See Policy 1008 – Managing Assaultive Behavior/Patient Restraint.
Use least restrictive method needed to manage patient and to ensure safety.
Use caution when administering Midazolam for postictal patients or patients with alcohol intoxication. Apply waveform capnography and frequently assess for depressed respirations and level of consciousness.
All patients who receive either physical restraint or chemical sedation must be continuously observed by EMS personnel. This includes direct visualization of the patient as well as cardiac and pulse oximetry monitoring.
Consider all possible medical/trauma causes for behavior (e.g. hypoglycemia, overdose, substance abuse, hypoxia, seizure, head injury, etc.).
Do not irritate the patient with a prolonged exam. Be thorough but quick.
Do not overlook the possibility of associated domestic violence or child abuse.
If patient suspected of excited delirium and suffers cardiac arrest, consider fluid bolus and sodium bicarbonate early.
Do not position or transport any restrained patient in a way that negatively affects the patient’s respiratory or circulatory status (e.g. hog‐tied or prone positions). Do not place backboards, splints or other devices on top of the patient.
If restrained, the extremities that are restrained will have a circulation check at least every 15 minutes. The first of these checks should occur as soon after placement of the restraints as possible. This shall be documented in the EHR.
Excited Delirium Syndrome:
This is a medical emergency. The condition is a combination of delirium, psychomotor agitation, anxiety, hallucinations, speech disturbances, disorientation, violent/bizarre behavior, insensitivity to pain, hyperthermia and increased strength. The condition is life‐threatening and is often associated with use of physical control measures, including physical restraints, and tasers. Most commonly seen in male patients with a history of serious mental illness or drug abuse, particularly stimulant drugs such as cocaine, crack cocaine, methamphetamine, amphetamines, bath salts, or similar agents. Alcohol withdrawal or head injury may also contribute to the condition.
Effective Jan. 2022

Effective Jan. 2016
Contra Costa County Emergency Medical Services
Extremity Trauma
Treatment Guideline T04Page 1 of 2
History• Type and time of injury• Mechanism (crush, penetrating, blunt, or amputation)• Open vs. closed wound/fracture• Past medical history• Medications
Differential• Abrasion• Contusion• Laceration• Sprain• Dislocation• Fracture• Amputation
Signs and Symptoms• Evidence of trauma• Pain, swelling, deformity, or bleeding• Altered sensation or motor function• Diminished pulse or capillary refill• Decreased extremity temperature
P
EPlace splints and cold packs to stabilize fractures as necessary
Exit to Airway TGif indicated
Cardiac monitor
Establish IV/IO
If SBP < 90 in adultsNormal Saline bolus 500ml IV/IOReassess patient for criteria aboveMay repeat to a Maximum 1L as long as criteria above exists
If poor perfusion or shock in pedsNormal Saline bolus IV/IO
Use PEDIATAPE and refer to dosing guide
Repeat to age dependent goal SBPMay repeat to a Maximum 1L as long as criteria above exists
In the absence of head trauma, age‐specific hypotension, poor perfusion
or AMSConsider pain control
Control hemorrhaging
Exit to Pain Control TGif indicated
Crush injury?
P
E
Secure airwayand support respiratory rate
Place splints and cold packs to stabilize fractures as necessary
Cardiac monitor
EtCO2 monitoring
Establish IV/IO
If SBP < 90 in adultsNormal Saline bolus 500ml IV/IOReassess patient for criteria above
May repeat as long as criteria above exists
If poor perfusion or shock in pedsNormal Saline bolus IV/IO
Use PEDIATAPE and refer to dosing guideRepeat to age dependent goal SBP
May repeat as long as criteria above exists
In the absence of head trauma, age‐specific hypotension, poor perfusion or AMS
Consider pain control
Prior to release of entrapment
Control hemorrhaging
For suspected hyperkalemia:• Peaked T‐waves; or
• QRS > 0.12 seconds; or• Loss of P‐waves
Albuterol nebulizer 5mg in 6ml Normal SalineCalcium Chloride 1gm over 60 seconds
20ml flush IV/IO prior to pushing next med
Sodium Bicarbonate 1mEq/kg
YesNo
Albuterol nebulizer 5mg in 6ml Normal Saline
Notify receiving facility. Contact Base Hospital for
medical direction, as needed.
Effective Jan. 2022
Exit to Major Hemorrhage Control TGif indicated
Early transport after releaseLimit scene time to 10 minutes
for critical patients

Effective Jan. 2016
Contra Costa County Emergency Medical Services
Extremity Trauma
Treatment Guideline T04Page 2 of 2
Pearls
For partial amputations, splint affected extremity in anatomic location and elevate extremity.
For complete amputations, place amputated part in a dry container or bag and place on ice. Seal or tie off bag and place in second container or bag. DO NOT place amputated extremity directly on ice or in water. Elevate extremity and dress with dry gauze.
Penetrating trauma to an extremity may hide significant vascular injury and hemorrhage. Early application of a tourniquet should be considered.
In cases of clear‐cut traumatic arrest, epinephrine is not indicated in PEA or asystole. Epinephrine will not correct arrest caused by a tension pneumothorax, cardiac tamponade, or hemorrhagic shock. If there is any doubt as to the cause of arrest, treat as a non‐traumatic arrest.
Hypotension is age dependent. This is not always reliable and should be interpreted in context with the patient’s typical BP, if known. Shock may be present with a seemingly normal blood pressure initially.
Neonate: < 60mmHg or weak pulsesInfant: < 70mmHg or weak pulses1‐10 years: < 70mmHg + (age in years x2)Over 10 years: <90mmHgOver 65 years: <110mmHg
If vigorous hemorrhage is not controlled with elevation and direct pressure on wound, apply a tourniquet. Tourniquets may be used in pediatric patients.
Tourniquets and hemostatic gauze may also be appropriate for hemorrhage control in multi‐casualty incidents.
Consider the use of hemostatic gauze to pack the wound. More than hemostatic agent may be needed. Secure hemostatic gauze in place with a compression bandage.
Crush Injury Syndrome is caused by muscle crush injury and cell death. Most patients have an extensive area of involvement such as a large muscle mass in a lower extremity or the pelvis. May develop after one (1) hour in the presence of a severe crush, but usually requires at least four (4) hours of compression. Hypovolemia and hyperkalemia may occur, particularly in extended entrapments.
Avoid hyperventilation. Maintain an EtCO2 of 35 or greater, which may be unreliable if the patient was subject to multisystem trauma or poor perfusion.
Hypotension usually indicates injury or shock and should be treated aggressively.
An important item to monitor and document is a change in the level of consciousness by repeat examination.
Do not overlook the possibility of associated domestic violence or abuse.
Effective Jan. 2022

Effective Jan. 2016
Contra Costa County Emergency Medical Services
Multi-System Trauma
Treatment Guideline T06Page 1 of 2
History• Time of injury• Mechanism (blunt vs. penetrating)• Damage to structure or vehicle• Location of patient in structure or vehicle• Restraints or protective equipment use• Past medical history• Medications
Differential• Chest: • Tension pneumothorax • Flail chest • Pericardial tamponade • Open chest wound • Hemothorax• Intra‐abdominal bleeding• Pelvis or femur fracture• Spinal injury• Head injury• Hypothermia
Signs and Symptoms• Evidence of trauma• Pain, swelling, deformity, lesions, or bleeding• AMS• Unconscious• Respiratory distress or failure• Hypotension or shock• Arrest
P
Spinal Motion Restrictionif indicated
E
Secure airwayand support respiratory rate
Place splints and cold packs to stabilize fractures as necessary
Exit to Airway TGif indicated
Cardiac monitor
EtCO2 monitoring
Establish IV/IO
If SBP < 90 in adultsNormal Saline bolus 500ml IV/IOReassess patient for criteria aboveMay repeat to a Maximum 1L as long as criteria above exists
If poor perfusion or shock in pedsNormal Saline bolus IV/IO
Use PEDIATAPE and refer to dosing guide
Repeat to age dependent goal SBPMay repeat to a Maximum 1L as long as criteria above exists
In the absence of head trauma, age‐specific hypotension, poor perfusion
or AMS
Control hemorrhage
Do not delay transport
Early transportLimit scene time to 10 minutes
for critical patients
Needle Thoracostomyif indicated
Notify receiving facility. Contact Base Hospital for
medical direction, as needed.
Exit to Pain Control TGif indicated
Effective Jan. 2022
Exit to Major Hemorrhage Control TGif indicated

Effective Jan. 2016
Contra Costa County Emergency Medical Services
Multi-System Trauma
Pearls• ALS procedures in the field do not significantly improve patient outcome in critical trauma patients.• Basic airway management is preferred unless unable to effectively manage with BLS maneuvers. Utilize jaw
thrust technique to open the airway.• Intubation of head injury patients is best addressed at the hospital. Advanced Airways should not be used in
traumatic arrest. • In cases of clear‐cut traumatic arrest, epinephrine is not indicated in PEA or asystole. Epinephrine will not
correct arrest caused by a tension pneumothorax, cardiac tamponade, or hemorrhagic shock. If there is any doubt as to the cause of arrest, treat as a non‐traumatic arrest.
• Hypotension is age dependent. This is not always reliable and should be interpreted in context with the patient’s typical BP, if known. Shock may be present with a seemingly normal blood pressure initially.
▫ Neonate: < 60mmHg or weak pulses ▫ Infant: < 70mmHg or weak pulses
▫ 1‐10 years: < 70mmHg + (age in years x2)▫ Over 10 years: <90mmHg▫ Over 65 years: <110mmHg
• Avoid hyperventilation. Maintain an EtCO2 of 35 or greater, which may be unreliable if the patient was subject to multisystem trauma or poor perfusion.
• Hypotension usually indicates injury or shock and should be treated aggressively.• An important item to monitor and document is a change in the level of consciousness by repeat examination.• Do not overlook the possibility of associated domestic violence or abuse.
Treatment Guideline T06Page 2 of 2
Effective Jan. 2022

Notify receiving facility. Contact Base Hospital for
medical direction, as needed.
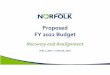
Treatment Guideline T09Page 1 of 1
Contra Costa County Emergency Medical Services
Major Hemorrhage ControlHistory Quantity and duration of bleeding Meds (anticoagulants) Recent trauma Pregnant or menstruating Recent Surgery
Differential Trauma Coagulopathy GI bleed Urinary tract pathology Vaginal bleeding (all causes)
Signs and Symptoms Visible external bleeding Melena Rectal bleeding Hematuria Vaginal bleeding Dizziness/syncope Weakness/dyspnea Confusion/ALOC Hypotension or other signs of shock
E
Cardiac monitor
Establish IV/IO
Normal Saline bolus 1L IV/IOMay repeat to maintain SBP >90
For poor perfusion or shock in pedsNormal Saline bolus IV/IO
Use PEDIATAPE and refer to dosing guideRepeat to age dependent goal SBP
Secure airway and support respiratory rate
if indicated
Effective Jan. 2022
Hemorrhage controlled?
E
Extremity injuryWound amenable to tourniquet(s)
Apply tourniquet(s) (FP21)
Junctional injuryWound not amenable to tourniquet(s)
Consider Hemostatic Gauze (FP28)
P
No
Tranexamic Acid
Indications (all three must be met)1) Age ≥ 152) Blunt/penetrating trauma and injury within 3 hours or postpartum hemorrhage3) BP < 90 presumed due to hemorrhage
Contraindications1) Isolated head injury (blunt or penetrating)2) Cervical cord injury with motor deficit3) Traumatic arrest (with > 5 minutes CPR without ROSC)4) Isolated drowning or hanging victims
E
Yes
Apply direct pressure/pressure dressing to injury
Consider TXA 1gm in 100ml IV/IO over 10 minutes

Effective Jan. 2016
Contra Costa County Emergency Medical Services
Tranexamic Acid
Field Procedure FP30Page 1 of 1
Clinical Indications: 1) Adults, age ≥ 15 years old, and; 2) Any sustained blunt or penetrating trauma within 3 hours of injury and systolic blood pressure < 90 mmHg at scene, during transport, or upon arrival to appropriate hospital due to suspected
hemorrhagic shock, or; 3) Post-partum hemorrhage with > 500 ml blood loss and systolic blood pressure < 90 mmHg in the first 24-hours following delivery.
Contraindications:1) <15 y/o with injury occurred > 3 hours ago2) Isolated head injury (blunt or penetrating)3) Cervical cord injury with motor deficit4) Traumatic arrest with > 5-minute CPR without ROSC5) Isolated drowning or hanging victims
Procedure:MUST BE ADMINISTERED WITHIN 3 HOURS OF INJURY
Mix 1gm of TXA in 100ml of Normal Saline Administer 1gm IV/IO over 10 minutes (No IV push) Monitor the patient while continuing the treatment protocol Contact receiving hospital to notify them TXA has been initiated Document the procedure, time and results in the Prehospital electronic health record.
Adverse Reaction/Side Effects:Hypotension with rapid IV injection, giddiness, nausea, vomiting, blurred vision
Treatment and Field Procedure Guidelines: M06a, T09
Effective Jan. 2022
P Paramedic
Applies to:

Effective Jan. 2016
Contra Costa County Emergency Medical Services
Drug Reference
ReferencePage 6 of 6
Drug Indication Dosing Cautions Comments
OndansetronVomiting or severe nausea
4mg IV/IO/IM/ODT
May repeat after 15 minutes
Administer IV/IO dose over 1 minute as rapid administration may cause syncope.
None
Refer to pediatric dosing guide
Sodium Bicarbonate
Tricyclic antidepressant overdose 1mEq/kg IV/IO
Can precipitate with or inactivate other drugs.
Use only if life‐threatening or in the presence of hemodynamically significant dysrhythmias.
Administer 20ml flush IV/IO when delivering in conjunction Calcium Chloride.
Crush injury
Hyperkalemia 50mEq IV/IO
Nitroglycerin
Pulmonary edema
0.4mg SL
May repeat to a max of 3 doses
Can cause hypotension and headache. Do not administer if systolic BP < 90mmHg.
Do not administer if patient has taken Viagra, Levitra, within past 24 hours or Cialis if taken within 36 past hours.
Use caution and consider base contact if HR >120.
Perform 12‐Lead ECG prior to administration.
Chest pain
0.4mg SL if systolic BP > 90mmHg
0.8mg SL if systolic BP > 150mmHg
May repeat appropriate dose every 5 minutes
Effective Jan. 2022
Tranexamic Acid (TXA)
Blunt or penetrating injury with significant blood loss within 3 hours.Postpartum hemorrhage with> 500 ml blood loss.SBP < 90 presumed due to hemorrhage.
1gm in 100ml IV/IO over 10 minutes
Do not administer to: Isolated head injuryCervical cord injury with motor deficitTraumatic arrest > 5 min CPR without ROSCIsolated drowning or hanging victims
Must be administered within 3 hours of injury.Tranexamic
Acid (TXA)
Blunt or penetrating injury within 3 hours, OR Postpartum hemorrhage with> 500 ml blood loss,
AND
SBP < 90 presumed due to hemorrhage.
1gm in 100ml IV/IO over 10 minutes
Do not administer to:Patient < 15 years old
Isolated head injuryCervical cord injury with motor deficitTraumatic arrest > 5 min CPR without ROSCIsolated drowning or hanging victims
Do not delay transport to administer TXA.