Embed Size (px)
Citation preview
Proposal to Substantially Revise the National Kidney Allocation
System
Sponsored by: The Kidney Transplantation Committee
High discard rates
Access variability due to geography and biology
Mismatch in graft/patient survival
Current System Limitations

The Growing Waiting List
OPTN data as of September 1, 2012

Over time, waiting time has become the primary driver of kidney allocation Histocompatibility components have diminished over time
This overreliance led to a system that does not accomplish any goal other than transplanting the candidate waiting the longest Doesn’t recognize that not all can wait the same length of time Fails to acknowledge different needs for different candidates (e.g., speed
over quality)
Unbalanced System Components
Make the most of every donated kidney without diminishing access
Promote graft survival for those at highest risk of retransplant
Minimize loss of potential graft function through better longevity matching
Improve efficiency and utilization by providing better information about kidney offers
Proposed Policy Objectives

Provide comprehensive data to guide transplant decision making
Reduce differences in access for ethnic minorities and sensitized candidates
Proposed Policy Objectives
Date Sentinel Event
2003 Board requests review of kidney allocation system; public hearings held
2004 Board directs investigation of benefit use in a kidney allocation system
2007 Public Forum held in Dallas; main topic LYFT2008 RFI released: main topics KDPI/LYFT2009 Public Forum held in St. Louis; main topics LYFT/KDPI 2009 Donor/recipient age matching reviewed as possibility2011 Concept document released: main topics EPTS/age
matching/ KDPI2011 Age matching no longer under consideration2012 Public comment proposal
The course of policy development

New system forecasted to result in: 8,380 additional life years gained annually Improved access for moderately and very highly
sensitized candidates Improved access for ethnic minority candidates Comparable levels of kidney transplants at
regional/national levels
Preview of Expected Outcomes

SYSTEM DESIGN
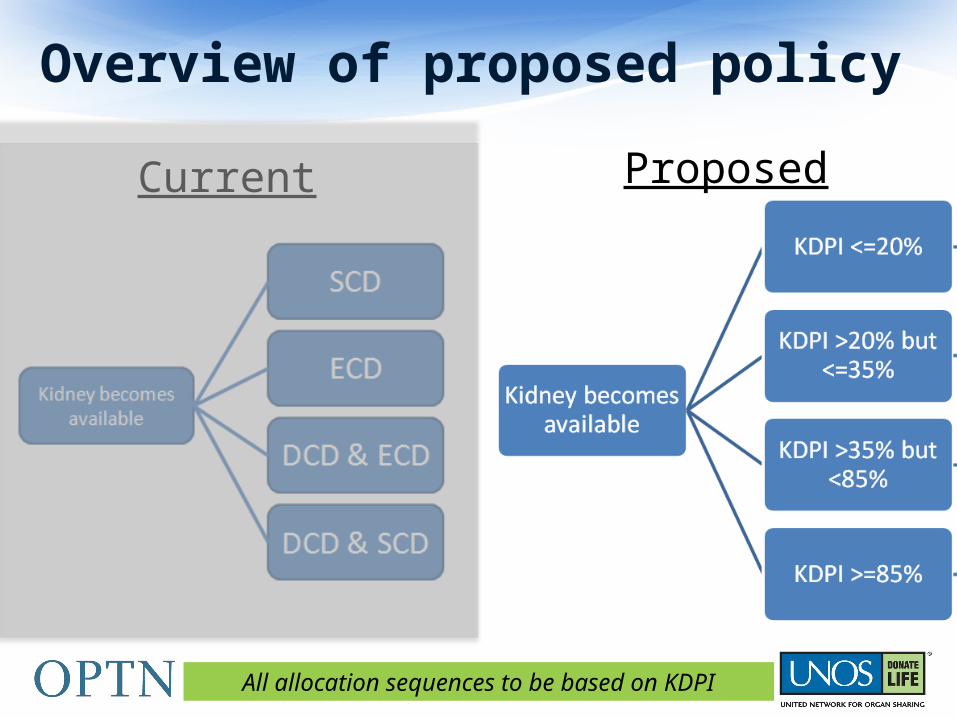
Overview of proposed policy
Current Proposed
All allocation sequences to be based on KDPI

Kidney Donor Profile Index (KDPI)
KDPI Variables
•Donor age•Height•Weight•Ethnicity•History of Hypertension•History of Diabetes•Cause of Death•Serum Creatinine•HCV Status•DCD Status
KDPI values now displayed with all organ offers in DonorNet®
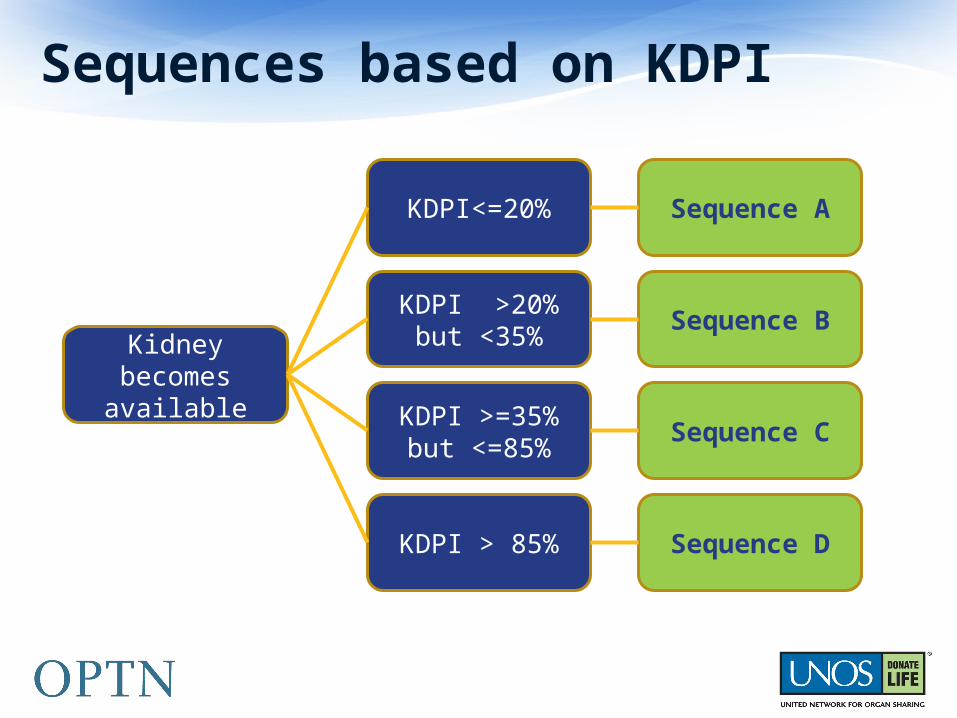
Sequences based on KDPI
Kidney becomes available
KDPI<=20%
KDPI >20% but <35%
KDPI >=35% but <=85%
KDPI > 85%
Sequence A
Sequence B
Sequence C
Sequence D

Sequences based on KDPI
Sequence AKDPI<=20%
Sequence BKDPI >20% but <35%
Sequence CKDPI>=35% but
<=85%
Sequence DKDPI>85%

Sequence AKDPI<=20%
Sequence BKDPI >20% but <35%
Sequence CKDPI>=35% but
<=85%
Sequence DKDPI>85%

Sequence AKDPI <=20%
Sequence BKDPI >20% but <35%
Sequence CKDPI >=35% but
<=85%
Sequence DKDPI>85%
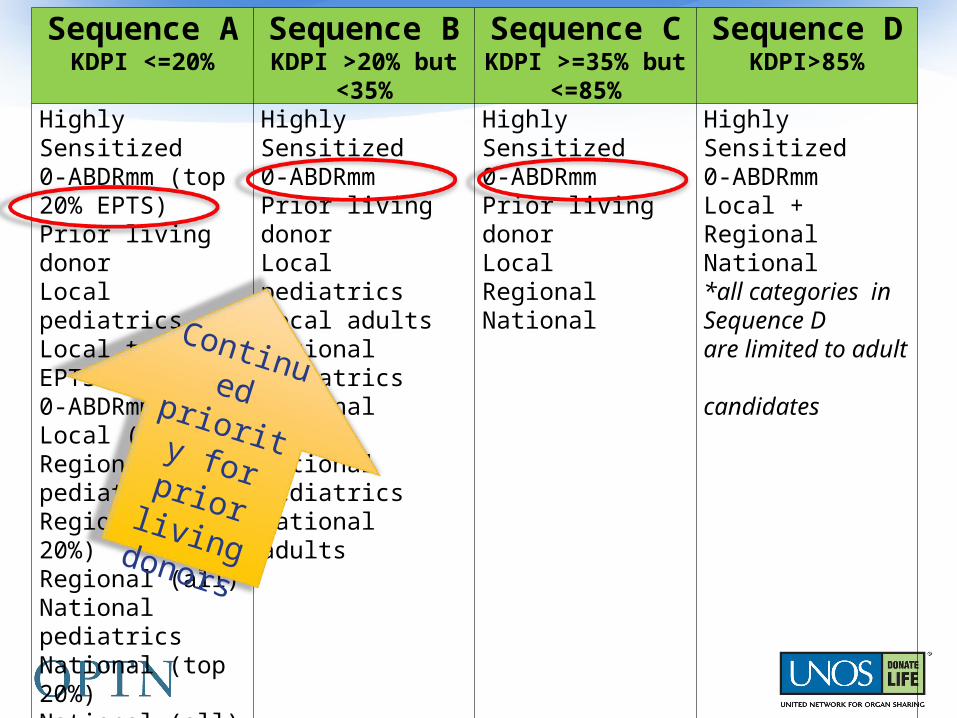
Highly Sensitized0-ABDRmm (top 20% EPTS)Prior living donorLocal pediatricsLocal top 20% EPTS0-ABDRmm (all)Local (all)Regional pediatricsRegional (top 20%)Regional (all)National pediatricsNational (top 20%)National (all)
Highly Sensitized0-ABDRmmPrior living donorLocal pediatricsLocal adultsRegional pediatricsRegional adultsNational pediatricsNational adults
Highly Sensitized0-ABDRmmPrior living donorLocal RegionalNational
Highly Sensitized0-ABDRmmLocal + Regional National *all categories in Sequence D are limited to adult candidates

Estimated Post-Transplant Survival Candidate age, time on dialysis, prior organ transplant, diabetes status
Top 20% of candidates by EPTS to receive kidneys matched on longevity
Applies only to kidneys with KDPI scores <=20% not allocated for multi-organ, very highly sensitized, or pediatric candidates
Proposed Classification: Longevity Matching

Sequence AKDPI <=20%
Sequence BKDPI >20% but <35%
Sequence CKDPI >=35% but
<=85%
Sequence DKDPI>85%
Highly Sensitized0-ABDRmm (top 20% EPTS)Prior living donorLocal pediatricsLocal top 20% EPTS0-ABDRmm (all)Local (all)Regional pediatricsRegional (top 20%)Regional (all)National pediatricsNational (top 20%)National (all)
Highly Sensitized0-ABDRmmPrior living donorLocal pediatricsLocal adultsRegional pediatricsRegional adultsNational pediatricsNational adults
Highly Sensitized0-ABDRmmPrior living donorLocal RegionalNational
Highly Sensitized0-ABDRmmLocal + Regional National *all categories in Sequence D are limited to adult candidates
Propose
d
Longe
vity
matching

Candidates with CPRA >=98% face immense biological barriers
Current policy only prioritizes sensitized candidates at the local level.
Proposed policy would give following priority
To participate in Regional/National sharing, review & approval of unacceptable antigens will be required
Proposed Classifications: Very Highly Sensitized
CPRA=100% NationalCPRA=99% RegionalCPRA=98% Local

Sequence AKDPI <=20%
Sequence BKDPI >20% but <35%
Sequence CKDPI >=35% but
<=85%
Sequence DKDPI>85%
Highly Sensitized0-ABDRmm (top 20% EPTS)Prior living donorLocal pediatricsLocal top 20% EPTS0-ABDRmm (all)Local (all)Regional pediatricsRegional (top 20%)Regional (all)National pediatricsNational (top 20%)National (all)
Highly Sensitized0-ABDRmmPrior living donorLocal pediatricsLocal adultsRegional pediatricsRegional adultsNational pediatricsNational adults
Highly Sensitized0-ABDRmmPrior living donorLocal RegionalNational
Highly Sensitized0-ABDRmmLocal + Regional National *all categories in Sequence D are limited to adult candidates
New
categories
for highly
sensitized
candidates

Prior living organ donors receive the same level of priority as current policy
Requirements remain the same for registering a prior living organ donor Policy proposal to allow priority with subsequent registrations to be
considered by Board in November 2012
Proposed policy will base qualification on date of procurement not date of transplant Would provide priority for prior donors whose organs were removed but
not transplanted
Unmodified Classification: Prior Living Organ Donor
Sequence AKDPI <=20%
Sequence BKDPI >20% but <35%
Sequence CKDPI >=35% but
<=85%
Sequence DKDPI>85%
Highly Sensitized0-ABDRmm (top 20% EPTS)Prior living donorLocal pediatricsLocal top 20% EPTS0-ABDRmm (all)Local (all)Regional pediatricsRegional (top 20%)Regional (all)National pediatricsNational (top 20%)National (all)
Highly Sensitized0-ABDRmmPrior living donorLocal pediatricsLocal adultsRegional pediatricsRegional adultsNational pediatricsNational adults
Highly Sensitized0-ABDRmmPrior living donorLocal RegionalNational
Highly Sensitized0-ABDRmmLocal + Regional National *all categories in Sequence D are limited to adult candidates
Continued priority for prior living donors

Current policy prioritizes donors younger than 35 to candidates listed prior to 18th birthday
Proposed policy would Prioritize donors with KDPI scores <35% Eliminate pediatric categories for non 0-ABDR KPDI >85%
Provides comparable level of access while streamlining allocation system
Modified Classification: Pediatric

Sequence AKDPI <=20%
Sequence BKDPI >20% but <35%
Sequence CKDPI >=35% but
<=85%
Sequence DKDPI>85%
Highly Sensitized0-ABDRmm (top 20% EPTS)Prior living donorLocal pediatricsLocal top 20% EPTS0-ABDRmm (all)Local (all)Regional pediatricsRegional (top 20%)Regional (all)National pediatricsNational (top 20%)National (all)
Highly Sensitized0-ABDRmmPrior living donorLocal pediatricsLocal adultsRegional pediatricsRegional adultsNational pediatricsNational adults
Highly Sensitized0-ABDRmmPrior living organ donorLocal RegionalNational
Highly Sensitized0-ABDRmmLocal + Regional National *all categories in Sequence D are limited to adult candidates
Continued
priority
pediatric
candidates
(now based
on KDPI)
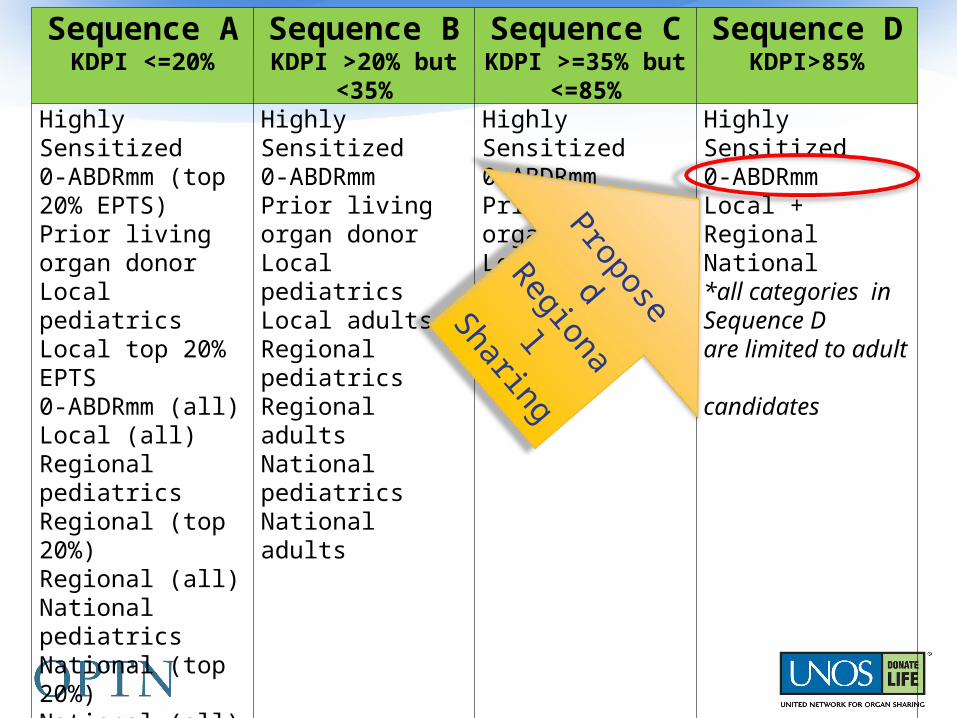
KDPI >85% kidneys would be allocated to a combined local and regional list
Would promote broader sharing of kidneys at higher risk of discard
DSAs with longer waiting times are more likely to utilize these kidneys than DSAs with shorter waiting times
Modified Classification: Local + Regional for High KDPI Kidneys
Sequence AKDPI <=20%
Sequence BKDPI >20% but <35%
Sequence CKDPI >=35% but
<=85%
Sequence DKDPI>85%
Highly Sensitized0-ABDRmm (top 20% EPTS)Prior living organ donorLocal pediatricsLocal top 20% EPTS0-ABDRmm (all)Local (all)Regional pediatricsRegional (top 20%)Regional (all)National pediatricsNational (top 20%)National (all)
Highly Sensitized0-ABDRmmPrior living organ donorLocal pediatricsLocal adultsRegional pediatricsRegional adultsNational pediatricsNational adults
Highly Sensitized0-ABDRmmPrior living organ donorLocal RegionalNational
Highly Sensitized0-ABDRmmLocal + Regional National *all categories in Sequence D are limited to adult candidates
Proposed
Regional
Sharing

Candidates with blood type B who meet defined clinical criteria will be eligible to accept kidneys from donors with blood type A2 or A2B
Reported anti-A titer values required on regular schedule
No titer values of greater than or equal to 1:8 allowed for candidate participation
Modified Classification:B Candidates receiving A2/A2B Kidneys

Current payback policy was evaluated and found to be Administratively challenging Unfair in that it affected all candidates in an OPO even if
only one center was responsible for accruing debt Ineffective in improving outcomes of recipients
Kidney paybacks would no longer be permitted.
All payback credits and debts would be eliminated upon the implementation of the revised kidney allocation system.
Removed Classification:Kidney Paybacks

PRIORITY WITHIN CLASSIFICATIONS

Candidates are rank-ordered according to points within each classification.
Proposed Changes to Point System
No proposed point changes for
Proposed point changes for
•HLA-DR•Prior living organ donors•Pediatric candidates
•Sensitized candidates•Waiting time

Proposed Point Changes: Sensitization
Current policy: 4 points for CPRA>=80%. No points for moderately sensitized candidates. Proposed policy: sliding scale starting at CPRA>=20%
0 0 0 0.08 0.21 0.34 0.48 0.81 1.091.58 2.46
4.05
6.71
10.82
12.17
17.30
02468
101214161820
0 10 20 30 40 50 60 70 80 90 100
Poin
ts
CPRA
CPRA Sliding Scale (Allocation Points)(CPRA<98%)
4 points
Proposed
Current
(CPRA=98,99,100 receive 24.4, 50.09, and 202.10 points, respectively.)

Current policy begins waiting time points for adults at registration with: GFR<=20 ml/min Dialysis time
Proposed policy would also award waiting time points for dialysis time prior to registration Applies to both pediatric and adult candidates Better recognizes time spent with ESRD as the basis for priority
Pre-emptive listing would still be advantageous for 0-ABDR mismatch offers
Proposed Point Changes: Waiting Time

SIMULATED POLICY RESULTS

Scientific Registry of Transplant Recipients (SRTR) simulates proposed policy changes
Kidney-Pancreas Simulated Allocation Model (KPSAM)
50+ KPSAM runs conducted throughout policy development
4 KPSAM runs presented here for comparison
Evaluating Potential Policy Changes

Proposed Change N1 N2 N3 N4Enhanced definition of waiting time to include pre-listing time since initiation of dialysis
X X X
A2/A2B donor to B candidates priority X X XLongevity matching (based on KDPI and EPTS) X XCPRA sliding scale point assignment X XNational Priority for CPRA>=98% XTiered Priority for CPRA>=98% XRegional sharing for kidneys with KDPI scores >85%
X X
Major Proposed Changes by Run
N1 represents simulation of the allocation rules as they existed in 2010

Average for 10 iterations N1 N2 N3 N4 Number of candidates (on waitlist at start or joining during run)
122,669 122,669 122,669 122,669
Average number of primary KI+KP transplant recipients (min, max of runs)
11,531 (11,463-11,586)
11,595(11,526-11,655)
11,386(11,359-11,429)
11,365 (11,324-11,409)
Average median lifespan post-transplant (min, max of runs)
11.82(11.75 - 11.85)
11.72(11.68-11.83)
12.63(12.3-12.45)
12.73(12.65-12.79)
Overall KPSAM Results
Average(min-max)
of runs
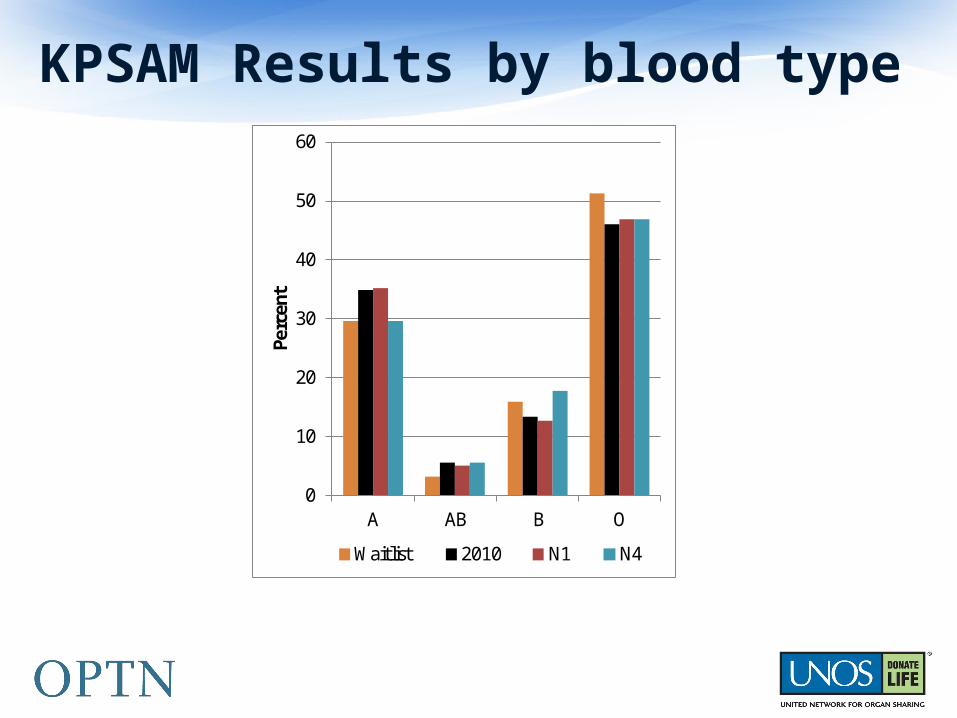
KPSAM Results by blood type
0
10
20
30
40
50
60
A AB B O
Perc
ent
Waitlist 2010 N1 N4

KPSAM results by candidate age
0
5
10
15
20
25
30
35
40
45
<18 18-34 35-49 50-64 65+
Perc
ent
Waitlist 2010 N1 N4

KPSAM results by ethnicity
05
101520253035404550
Pe
rce
nt
Waitlist 2010 N1 N4

KPSAM results by 0-ABDR mismatch
0
1
2
3
4
5
6
7
8
9
10
0 Total HLA mismatches
Perc
ent
2010 N1 N4

KPSAM results by CPRA
0
10
20
30
40
50
60
Perc
ent
Waitlist 2010 N1 N4

KPSAM results by CPRA (95-100%)

KPSAM results by degree of sharing

New system forecasted to result in: 8,380 additional life years gained annually Improved access for moderately and very highly sensitized
candidates Improved access for ethnic minority candidates Comparable levels of kidney transplants at regional/national
levels
Summary

Submit comments online:
optn.transplant.hrsa.gov
Access webinar schedules
Download educational materials
Participate in Policy Development
Publiccomment period ends December 14
John J. Friedewald, MDCommittee Chair
Richard N. Formica, Jr, MDCommittee Vice Chair
Ciara J. Samana, MSPHUNOS Committee [email protected]
Committee Leadership and Support

BACKUP SLIDES
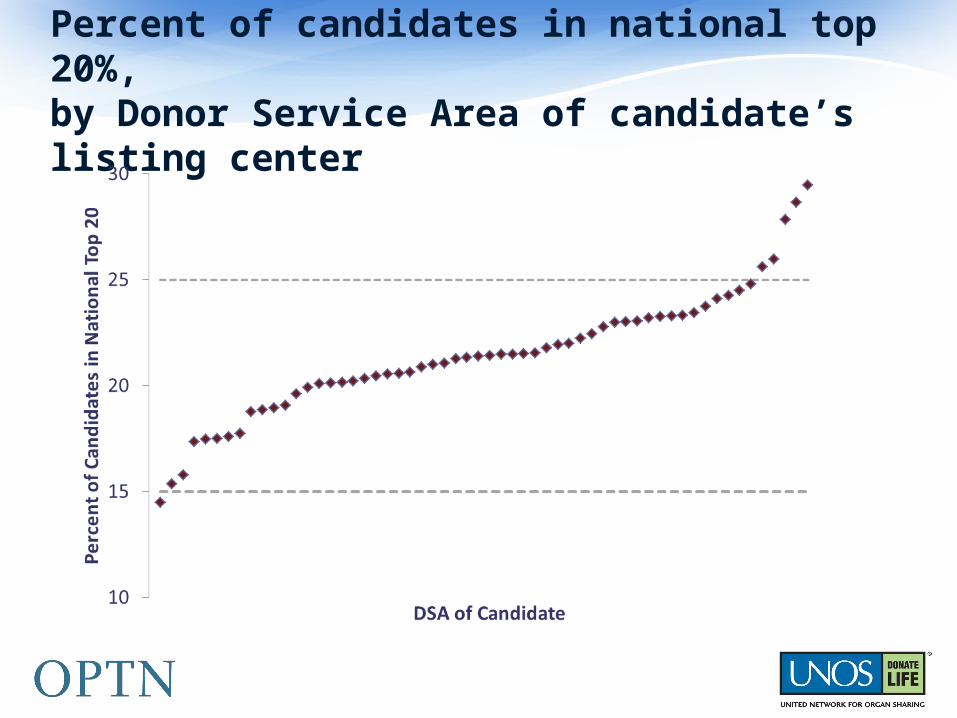
Percent of candidates in national top 20%, by Donor Service Area of candidate’s listing center
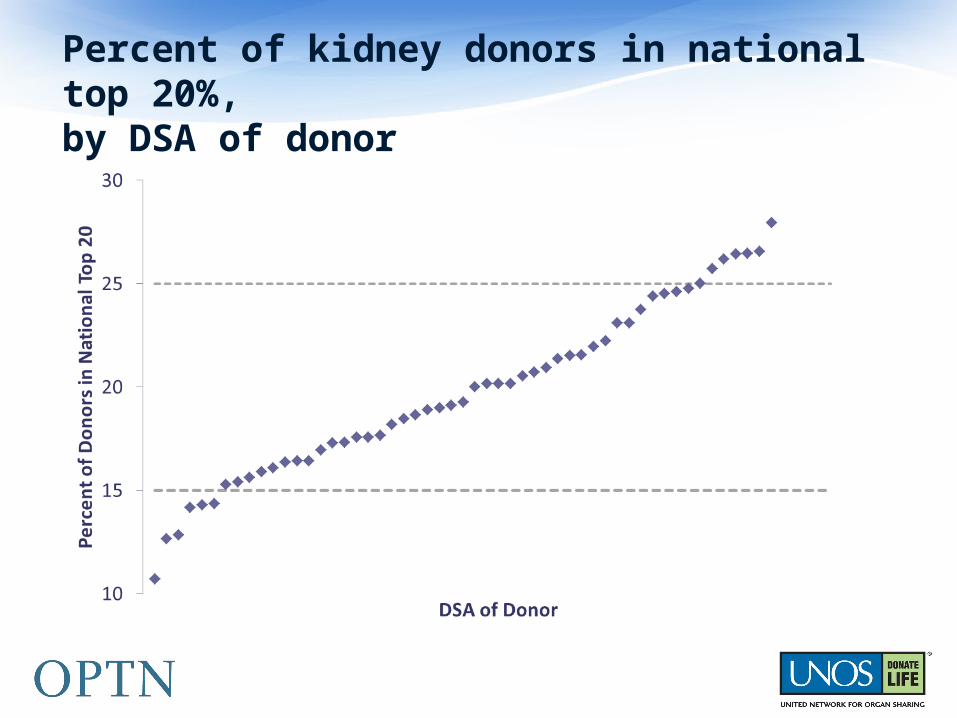
Percent of kidney donors in national top 20%, by DSA of donor





























