Embed Size (px)
Citation preview

• Prophylaxis
• Diagnosis
• Treatment
Venous Thromboembolism Management

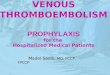
Spectrum of Venous Thromboembolism
Biologiconset Asymptomatic Symptomatic Outcome Death
Recovery
Disability
Primaryprophylaxis
Screening Clinical suspicion
Treatment
Management

“Pulmonary embolism remains the most common preventable cause of death in the hospital.”
Hull
1986

Venous Thrombosis ProphylaxisRisk Factor Equivalents
1 Factor
Age 40-59
Bed confinement >48 hrs
Varicose veins
Leg edema/ulcer/statis
Obesity (>20% ideal wt.)
MI (current)
CHF (current)
Severe COPD
Crystalliods (>5L/24 hrs)
Confining travel >4hrs
Pregnancy/postpartum (1 month)
Inflammatory bowel disease
Severe infection
Estrogen Rx
Operation >2 hrs

Venous Thrombosis Prophylaxis
Risk Factor Equivalents
2 Factors
Age > 60
Stroke (current)
Trauma
Pelvic operation
Joint replacement
Hip fracture
Malignancy
Pelvic/long bone fracture
Hypercoag. state
Hx DVT/PE
Spinal Cord Injury
3 Factors

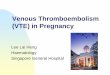
Venous Thrombosis RiskWithout Prophylaxis
1-5%40-80%>6Highest
0.5-1.0%30-40%4-5High
0.1-0.5%10-30%2-3Moderate
<0.01%<10%0-1Low
PE DVT*Risk Factor
EquivalentsRisk
OutcomeRisk Profile
Modified from: Geerts W et al CHEST 2001
* Includes calf DVT

• Bioavailability of LMWH – Reduced HIT
• Fondaparinux results– 50% reduction VTE (ortho patients)– Reduced HIT
• Intermittent pneumatic compression– Mechanical venous velocity– Alters coagulation– More effective w/ GCS
Considerations / Observations Considerations / Observations VTE Prophylaxis

1. Prophylaxis is effective…Should be considered in all patients
2. Pharmacotherapy: consider renal function– LMWH (enoxaparin)– Fondaparinux
3. Mechanical methods– Stockings (8 -15 mm Hg) plus IPC– Risk of bleeding
– Combined w/pharmacoRx in high and highest risk patients
Considerations / Observations Considerations / Observations
VTE Prophylaxis

4. Caution with pharmacoRx in patients undergoing neuraxial anesthesia
5. Post-discharge prophylaxis should be considered in patients with continuing high risk
6. Aspirin alone as prophylaxis…
…NOT RECOMMENDED!
4. Caution with pharmacoRx in patients undergoing neuraxial anesthesia
5. Post-discharge prophylaxis should be considered in patients with continuing high risk
6. Aspirin alone as prophylaxis…
…NOT RECOMMENDED!
Considerations / Observations Considerations / Observations Considerations / Observations Considerations / Observations VTE Prophylaxis VTE Prophylaxis

VTE Prophylaxis VTE Prophylaxis
Recommendations Recommendations Recommendations Recommendations
RiskRisk RecommendationRecommendation
Ambulation (all pts)Ambulation (all pts)
IPC/GCS or,
UFH 5000 SQ q 12 hrs or,
Enoxaparin 40mg SQ daily
IPC/GCS or,
UFH 5000 SQ q 12 hrs or,
Enoxaparin 40mg SQ daily
IPC/GCS plus…
UFH 5000U SQ q 8 hrs; or
Enoxaparin 40 mg SQ daily or
Enoxaparin 30mg SQ q 12 hrs
Fondaparinux 2.5 mg SQ daily
IPC/GCS plus…
UFH 5000U SQ q 8 hrs; or
Enoxaparin 40 mg SQ daily or
Enoxaparin 30mg SQ q 12 hrs
Fondaparinux 2.5 mg SQ daily
IPC/GCS plus…
UFH 5000 SQ q 8 hrs
Enoxaparin 40mg SQ daily
Enoxaparin 30mg SQ q 12 hrs
IPC/GCS plus…
UFH 5000 SQ q 8 hrs
Enoxaparin 40mg SQ daily
Enoxaparin 30mg SQ q 12 hrs
Low (0-1)Low (0-1)
Moderate (2-3)
Moderate (2-3)
High (4-5)High (4-5)
Highest(>6)
Highest(>6)