Embed Size (px)
Citation preview

Promoting Smoking Cessation in Women
Hal Strelnick, MDDept of Family and Social Medicine
David Lounsbury, PhDBruce Rapkin, PhD
Dept of Epidemiology and Population Health
Department of Obstetrics & Gynecology Grand Rounds10/20/2009
The Toll of Tobacco Use
Tobacco use is the leading preventable cause of premature death in the US
Tobacco is responsible for:• 21% of coronary heart disease deaths• 30%+ of all cancers
o 70-80% of oral cavity & pharyngeal cancerso 90% of lung cancer deathso stomach, cervix, kidneys, pancreas, AML & others
• 90% of COPD deaths

Maternal Smoking during Pregnancy
o Healthy People 2010 goal: 2% prevalence of smoking among pregnant women
o "Maternal smoking remains the single most important modifiable cause of poor pregnancy outcome in the United States, accounting for a significant portion of babies with low birth weight, pre-term births, and perinatal death such as sudden infant death syndrome (SIDS)." Institute of Medicine, Ending the Tobacco
Probem: A Blueprint for the Nation, 2007

Environmental Tobacco Smoke (aka Second-Hand Smoke)
• Same toxic exposure as First-Hand Smoke• Health effects include:
o Lung cancer, heart disease, eye & nasal irritation
o Suggested relationships to cervical cancer, miscarriage & decreased lung function
• Effects on childreno Causes & worsens asthma
o Increased risk of Sudden Infant Death Syndrome (SIDS)
o Direct effect on bronchitis, pneumonia & otitis media
o Increased probability of becoming smokers
Max et al., 2009

Epidemiological Overview
Women and Smoking

Declining Rates of Smoking in NYC
NYCDHMH EpiQuery HealthData website(http://a816-health3ssl.nyc.gov), accessed 5-13-09

Smoking Prevalence Trend for Men & WomenNew York City vs. Bronx, 2002-2008
Source: NYCDOHMH EpiQuery, Annual Community Health Surveys, 2002-2008

Reduction in Smoking Prevalence in New York City by Demographic Groups, 2002-2008
Male
Female
18-24
25-44
45-64
65+
White
Black
Hispanic
Asian
Other
Bronx
Bklyn
Manhattan
Queens
Staten Island
Source: NYCDOHMH Tobacco Control Program, Annual Community Health Surveys


Bronx NeighborhoodsNYC Department of Health
Female Smoking Prevalence 2006-2007
11.7%
12.7%
23.3%
17.6%
18.5%
South Bronx

Prevalence of Smoking Before, During, and After pregnancy
MMWR, 2009: 58(SS04); 1-29

Prevalence of Smoking during Pregnancy
MMWR, 2009: 58(SS04); 1-29

Prevalence of Smoking during Pregnancy by Race and Ethnicity
MMWR, 2009: 58(SS04); 1-29

Prevalence of Smoking during Pregnancy, by Maternal Age Group
MMWR, 2009: 58(SS04); 1-29

Postpartum Relapse
(Mullen et al., 1990)

Percentage of Women Relapsing* Post-Partum after Quitting during Pregnancy
* Assessed 4 months after deliveryMMWR, 2009: 58(SS04); 1-29

Tobacco Use and Cancer Riskin Women

What’s in a Cigarette?
+ 4000 MORE
chemicals!!

Cancer Risk and Tobacco Use in Women
• Smoking is directly responsible for 80 percent of lung cancer deaths in women in the U.S. each year
• In 1987, lung cancer surpassed breast cancer as the leading cause of cancer deaths among women in the US
• Compared to nonsmokers, men who smoke are about 23 times more likely to develop lung cancer and women who smoke are about 13 times more likely
• Smoking causes about 90% of lung cancer deaths in men and almost 80% in women
• For women, the risk of cervical cancer increases with the duration of smoking
HHS, 2004
Tobacco Use and Cervical Risks
• Increased risk with tobacco use and cervical cancer when HPV is presento Dose-adjusted increased risks seen
o Results in increased virion synthesis and genome copies
• Nicotine has several potential effects on oviduct and oviduct functiono Effects oocyte complex pickup, embryo transport, and
implantation
• Tobacco use has positive relation on clinically diagnosed PMS incidenceso Incidence rates and disease are dose-adjusted
o Supported by research of tobacco effects on FSH, estrogen, and progesterone metabolite levels

Treating Tobacco Use and Dependence in Women

Health Risks during Pregnancy• Significant evidence that smoking causes:
o Stillbirtho Preterm birtho Placental abruptiono SIDSo Fetal growth retardation
• Associated with increased risks of:o Spontaneous abortiono Ectopic pregnancieso Placenta previa
MMWR, 2004; Cnattingius, NTR, 2004

Health Risks after Pregnancy
Children of smokers have increased risk of:o SIDSo Hospitalization within first yearo Serious respiratory infections
Bronchiolitis, pneumonia
o Otitis mediao Asthmao Language delayso Hyperactivity

Why Women Continue to Smoke
• Pharmacologic addiction to nicotine• Psychological dependence on smoking
o Behavioral cueso Mood regulation, coping with stress,
emotions• Concern about weight gain
• Women tend to gain slightly more weight than men
• Assist with diet and exercise

Pharmacological Addiction:Tobacco Dependence vs. Other Chemical
Dependencies
Similarities• Compulsive use• Continued use despite harm• Impaired control over drug use• Tolerance• Withdrawal• Mediated via dopamine release• Rapid release• Rapid reinstatement of
dependence
Differences• No behavioral intoxication or
adverse behavioral outcomes• Does not cause other mental
disorders• Giving up or reducing activities
to use is rare• High intensity of use• Little euphoria• Spending lots of time in
obtaining/using/recovering from effects is rare
• Dependence is rare in adult non-daily users
• Pro-social beneficial effects

Psychological Dependence:Characteristics among Pregnant Smokers
• Young (< 25 years)• Non-Hispanic white• ≤ 12 years education• Unmarried• Annual income < 15k• Underweight• Unintended pregnancy• First-time pregnancy• Initiated prenatal care later• Medicaid enrolled• Enrolled in WIC during pregnancy
MMWR, 2009: 58(SS04); 1-29

Psychological Dependence:Characteristics of Relapsed Smokers
Post-partum• Spontaneous quitter during pregnancy
o 45% relapse within 3 months
o 60-70% relapse within 6 months
o 80% relapse within year
• Partner or household member who smokes
o 44% have partner who smokes
o 33% have household member who smokes
Merzel et al., 2009. Maternal Child Health Journal.
Importance of the Role of Providers in Smoking Intervention
• Brief counseling intervention by health care providers effectively promotes smoking cessation
• Counseling intervention especially important among pregnant smokers:o Park et al., 2004:
66% report being counseled on quitting 37% reported materials given
o Park, 2007 29% reported provider discussed medication use 10% of smokers used medication in pregnancy
(Fiore et al., 2008; Park et al., 2007)

Pharmacological Interventions

Smoking Cessation Interventions During Pregnancy
• The efficacy & safety of pharmacological approaches during pregnancy are unknown
• No medication has been observed in a sufficiently large number of pregnancies to determine what might occur with large-scale use
• Use of counseling & social support• Successful RCTs: Significant Other Supporter
(SOS), Quit Together, self-help programs• Cochrane Review (July 2009)
• 56 RCTs (N=20,000) & 9 cluster randomized trials6% smoking reduction, 17% LBW & 14% preterm birth reduction, 54 gm mean increase in birthweight
• No effective relapse RCTs

Tobacco Cessation Medications
Nicotine Replacement (D)
• Patch *• Gum *• Lozenge *• Oral Inhaler ^• Nasal Spray ^
Non-nicotine medication (C)
• Bupropion ^+o (Zyban/Wellbutrin)
• Varenicline ^+o (Chantix)
*Available OTC ^ prescription only+ FDA Black Box warning as of 7/1/09

Use of NRT in Non-pregnant Women
Reasons for using NRT• Doubles the success
rate• Treats nicotine
withdrawalo Helps patient feel more
comfortable• Safe
o Patient receiving same drug (nicotine) in a less addictive form over a relatively short period
Reasons for NOT using NRT• Medical conditions requiring
caution/physician input o i.e. recent MI, pregnancy,
current arrythmia• Age
o Under 18s require physician/parental input
• Specific issues o Allergy to patcheso Personal aversion to
medication• Questionable efficacy
o i.e. those smoking less than 10pd
Important Points about NRT
• Nicotine is the addictive part of tobacco smoke but NOT the most dangerous part
• People do NOT generally become addicted to medication
• People DON’T use enough medication or stop TOO EARLYo Medications are SAFE and EFFECTIVEo Plan on minimum of 2 months of medication
• Combinationso Work better than single medications
Use Long acting + Short acting

Plasma Nicotine concentrations for Nicotine-containing products
Time (minutes)
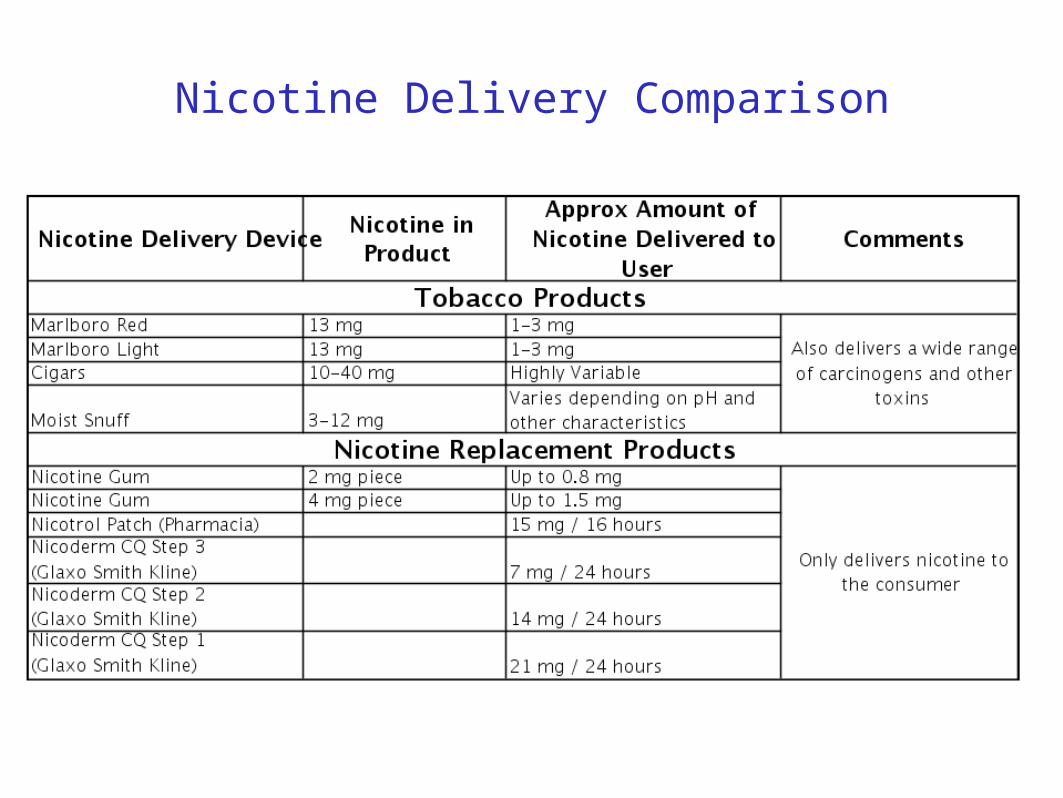
Nicotine Delivery Comparison

Important Points about Pharmacology
• In non-pregnant smokers, NRT and Bupropion each double cessation rates, compared to behavioral methods alone
• In very limited studies in pregnant women, NRT was not associated with adverse outcomes, but did have a short-term influence on fetal breathing movements and fetal heart rate variability
• Smoking nicotine has adverse effects on the fetus o Smoking exposes women to nicotine plus other chemicals that are
harmful

Training, Technical Assistance, and Resources for Clinicians
Bronx BREATHES
NYSDOH Tobacco Cessation Center

Bronx BREATHES Team
Hal Strelnick, MD – Principal Investigator
Barbara Hart, MPA – Project Manager
David Lounsbury, PhD – Co-Investigator
Shadi Nahvi, MD – Co-Investigator
Claudia Lechuga, MS – Research Associate
Shaniyya Pinckney – Academic Detailer
Bronx Einstein Alliance for Tobacco-free Health

Bronx BREATHES:Supportive Services for Clinicians
1. Tobacco treatment training: 5As, 5Rs, pharmacotherapy, NYSDOH Quitline
2. Academic detailing: Tailored consultation regarding the design and implementation of systems that identify tobacco users and manage their treatment
3. Linkage to provider and patient services: Promote referral to NYSDOH Quitline and local smoking cessation treatment services in the Bronx

Transtheoretical Model: Stages of Change
Prochaska and DiClemente

Brief Counseling Intervention: the 5 A’s
1. Ask about tobacco use Identify and document tobacco use status for every patient at
every visit
2. Advise to quit• In a clear, strong and personalized manner urge every tobacco user to
quit
3. Assess willingness to quit• Is the tobacco user willing to make a quit attempt at this time?
4. Assist in quit attempt• If willing to quit, use counseling, pharmacotherapy, and/or other
resources to help patient quit
5. Arrange follow up• Schedule follow-up contact, preferably within the first week after the quit
date
(Fiore et al., 2008)

Motivational Interviewing: the 5 R’s
1. Relevance to quitting smoking Most helpful to make it personal and specific
2. Risks associated with cont’d smoking• Highlight risks that seem most relevant to the patient
3. Rewards to being tobacco-free• Identify potential benefits to being smoke-free
4. Roadblocks to successfully quitting• Address elements of treatment that could alleviate barriers to
quitting
5. Repetition of assessment• Unmotivated patients should be asked each and every visit
(Fiore et al., 2008)

Does the patient now use tobacco?
Is the patient now ready to quit?
Provide treatment
Promote motivation
Yes
YesNo
Did the patient once use tobacco?
Prevent relapse*
Encourage continued abstinence
Yes
No
No
*Relapse prevention interventions not necessary if patient has not used tobacco for many years and is not at risk for re-initiation.
Fiore et al., 2008.
Algorithm for Brief Intervention

Provider Barriers• Too busy• Lack of expertise• No financial incentive• Most smokers can’t/won’t quit• Stigmatizing smokers• Respect for privacy• Negative message might scare away patients• Smoker
Fiore et al., 2008
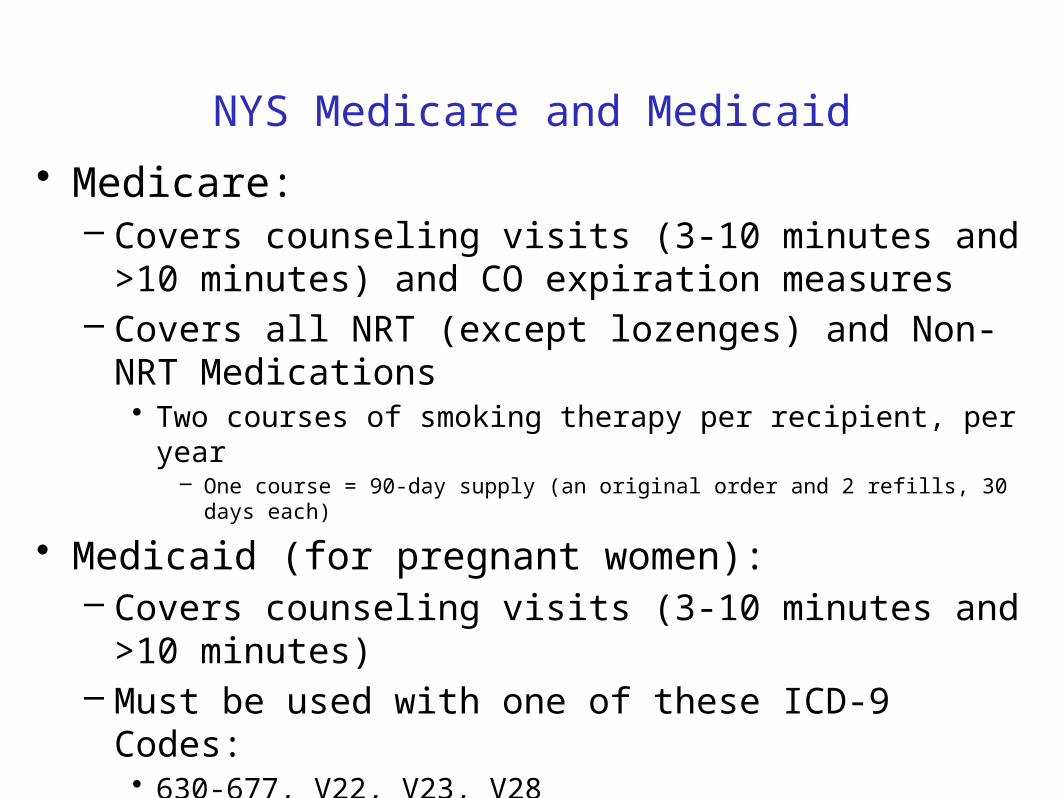
NYS Medicare and Medicaid
• Medicare:– Covers counseling visits (3-10 minutes and >10 minutes)
and CO expiration measures– Covers all NRT (except lozenges) and Non-NRT
Medications• Two courses of smoking therapy per recipient, per year
– One course = 90-day supply (an original order and 2 refills, 30 days each)
• Medicaid (for pregnant women):– Covers counseling visits (3-10 minutes and >10 minutes)– Must be used with one of these ICD-9 Codes:
• 630-677, V22, V23, V28

Reimbursement Codes
Medicare Codes Description
Payment:Facility
Non-Facility99406
Smoking and tobacco use cessation counseling visit; intermediate: >3 mins, up to 10 mins $12.94 $13.93
99407Smoking and tobacco use cessation counseling visit; intensive: >10 minutes $25.73 $27.21
94240/50 Billing for CO measure N/A$48.77 / $33.69
Medicaid Codes
DescriptionPayment:Office
APG Statewide Average
99406Smoking and tobacco use cessation counseling visit; intermediate: >3 mins, up to 10 mins $10 $20
99407Smoking and tobacco use cessation counseling visit; intensive: >10 minutes $19 $20

Patient Referral Services: Phone Counseling
NYS Quitline: 1-866-NY-QUITS• Services:
– Free telephone counseling in English, Spanish and several other languages
– Free NRT– Referrals to local counseling and cessation programs– Free educational materials
• Efficacy of Quitlines– Multiple calls: OR 1.41 (1.27-1.57)– Efficacy for long term cessation– Effective at reaching racial/ethnic minority smokers
Stead et al., Cochrane Library, 2007

NYS Fax-to-Quit Referral Service
• Available in paper and online forms– Provider-referred patients are contacted by Quitline services and
offered the same services as above– Progress report sent back to you

Clinical and TranslationalResearch in Tobacco Treatment

Future Tobacco Research in Smoking and Pregnancy
• Relapse prevention with pregnant women and women who have recently given birth
• Effectiveness of psychosocial treatment provided via nonface-to-face modalities (quitlines or web-based programs)
• Safety and effectiveness of cessation meds during pregnancy for the women and the fetus, and during child nursing
• Effectiveness of economic incentives to promote and sustain quitting
• Linking preconception, pregnancy and post-partum interventions
• Co-morbidity studies (tobacco use, depression/anxiety) among pregnant women
Fiore et al., 2008

Einstein/Monte Tobacco Think Tank
• A monthly, transdisciplinary forum for investigators and clinicians interested in tobacco prevention and control research
• Co-facilitated by Lounsbury, Rapkin, and Strelnik (Chetali Gupta, MPH, Coordinator)
• Thematic focus: Tobacco cessation among vulnerable populations who have not benefited from more universal efforts

Populations of Interest: Recalcitrant Smokers
• Methadone maintenance patients• High risk pregnancy• Head and neck cancer patients• Persons living with HIV• Homeless persons• Alcohol and tobacco co-users • Others . . .

TTT Domains of Research
• Genetic predisposition to nicotine dependence
• Pharmacogenomic differences in response to nicotine replacement
• Personality characteristics related to stress and coping
• Health status and quality of life• Family, work, and social support networks• Health systems interventions

TTT Research Approach
• Experimental and quasi-experimental clinical trials
• Comprehensive Dynamic Trials (CDTs)• Community-based Participatory Research
(CBPR)• Systems methodologies
– System dynamics modeling– Agent-based modeling– Geospatial coding– Network analysis

Acknowledgements
• Claudia Lechuga, MS• Chetali Gupta, MPH• Peter Bernstein, MD• Tobacco Think Tank Members

THANK YOU

IOM Report of Effects of Exposure to Secondhand Smoke (Oct. 2009)
• Case–control and cohort studies in multiple populations indicate that:– Exposure to secondhand smoke increases the risk of
coronary heart disease by about 25% to 30%– Increased risks were detected at even the lowest
exposures and a steep initial rise in risk is followed by a gradual increase with increasing exposure
• Effect of legislation to ban smoking and its effects on the cardiovascular health of nonsmoking adults remains a question

‘From Cells to Society’: A model for analysis of population health and health disparities.
Warnecke et al. (2008) AJPH.

The Society-Behavior-Biology NexusA developmental stream of causal influences flowing from distal social factors to proximal, individual factors. Glass and McAttee (2006). Social Science & Medicine.

The Society-Behavior-Biology NexusDetailed view of the sphere of human behavior and action.
Glass and McAttee (2006). Social Science & Medicine.





























