Embed Size (px)
Citation preview
Cathy Bremer, RN
There is no way to prepare a patient for trauma. Patients who, under ordinary circumstances, would be considered poor or unacceptable surgical risks are often subjected to stressful operations to save their lives. They may face long and complicated therapy.
Trauma covers a wide range of in- juries. Some injuries have widespread systemic effects, whereas others involve only a single organ system or tissue type. Personal and environmental characteristics have implications for treatment. These include age, nu- tritional status, existing disease, and contamination, to name a few.
All of these complicated factors have a bearing on wound healing. The nurse may be better able to promote wound healing for these patients if he or she understands the different types of traumatic wounds, the effects of mas- sive injury on body systems, and nurs- ing interventions.
Promoting healing of trauma wounds
Classification of traumatic wounds Abrasions. An abrasion occurs when epidermal cells are torn away by fric- tion. The depth may be uneven but no deeper than the accessory skin struc- tures. Abrasions normally heal by mi- gration and proliferation of epithelial cells from wound margins and surviv- ing skin appendages. Basal cells replace the migrated cells, and the remaining epidermal cells begin mitosis upward,
forming a thickened epidermal layer. The process takes about ten days and is completed with sloughing of the scab if one exists.’
Abrasions should be meticulously cleansed to remove any foreign material imbedded in the dermis that might cause “traumatic tatooing.”2 This oc- curs when the wound heals over the foreign material. If it is not removed before healing, the debris is visible through the dermis and can only be re- moved surgically. Obviously, facial ab- rasions are a special concern.
Laceration. This is an injury that ex- tends to tissues below the epithelium. The edges of a laceration may be smooth, as with knife wounds, or they may be jagged, as in excessive stretch- ing. A laceration is termed superficial when only the dermis and epithelium are involved, and deep when the injury extends to the tissues below the dermis.
Lacerations heal by the process of in- flammation, fibroplasia, contraction, and scar maturation. The edges of su- perficial wounds are easily approximated and may not require sutures, while deep lacerations tend to gape and will usu- ally require ~ u t u r i n g . ~ Whether a lac- eration should be closed or left open is based on the age of the injury and the degree of contamination. Wounds on the trunk or extremities over six hours old are usually left open, whereas those on the head and scalp are closed even up to 12 hours old because of the rich blood
dc 1150 AORN Journal, May 1982, Vol35, No 6
supply to this area.4 If contamination is known or suspected, a bacterial count should be done. If the count shows more than lo5 organisms per gram of tissue, the wound should not be c10sed.~
Stab and puncture wounds are types of lacerations. Most stabbing weapons that produce injury in soft tissue are short and narrow and cause minimal damage, although the outward appear- ance of the wound may be deceptive.6 Superficial stab wounds generally heal in the same manner as other lacera- tions. If the wound is deeper than 2 to 3 cm, however, it should be packed open to allow for drainage and complete heal- ing. Puncture wounds are deep and nar- row and tend to seal at the surface, hid- ing pockets of infection. If the wound appears heavily contaminated, the opening should be widened for thorough cleaning, debridement, and drainage.'
Avulsion. Avulsion is a tearing injury that usually involves loss of skin and other tissues. Most avulsion injuries re- quire skin grafts or flaps for closure once underlying structures are re- paired.
Amputation. Traumatic amputations generally result from industrial, farm, and motorcycle accidents. The ideal treatment for digit and upper extremity amputation is reimplantation. Prog- nosis for favorable reimplantation is de- termined by four factors. The first is the type of amputation-guillotine, avul- sion, or something in between. The cleanly severed guillotine injury has the best prognosis. The second factor is the initial handling of the amputated part. The part should be packed in a
Cathy Bremer, RN, MS, is a clinical nurse spe- cialist at Cook County Hospital and faculty member at Rush University College of Nurs- ing, Chicago. She received a baccalaureate in nursing from DePaul University, Chicago, and an M S from Rush University.
sterile, watertight container, which is put on ice. The container should be clearly labeled and transported with the patient. Related to this is the third fac- tor of warm ischemic time of the part. While the part remains warm, meta- bolic processes continue at the normal rate under anaerobic conditions, in- creasing necrotic areas. The final factor is the amount of muscle in the ampu- tated part, since muscle tissue is the most sensitive to ischemia.*
Crush injuries. A contusion is the simplest form of crush injury, with capillaries ruptured and blood released into the surrounding tissues. The age of the injury can be determined by the color of the skin. Treatment is usually not required other than application of first cold and then heat. More serious crush injuries are often difficult to evaluate initially because of the mas- sive edema, interstitial hemorrhage, questionable tissue viability, and the number of structures involved. In addi- tion to skin and muscle, vessels, ten- dons, and nerves are often also involved.
Treatment priorities include restora- tion of circulation and prevention of compartmental syndrome. When com- partment pressures (measured trans- cutaneously) exceed diastolic arterial blood pressure, fasciotomy is indicated. This can be lifesaving as well a s limbsaving. Further treatment in- cludes early repair of other deep struc- tures. The injury is left open for reeval- uation in 48 t o 72 hours. The wound can then be closed if all tissue appears via- ble and infection is not present. Recon- struction of finer structures is usually staged and may take years.s
Blast injuries. The most frequent type of blast injuries are from handguns or shotguns. The extent of an injury from a bullet depends primarily on: (1) lacera- tion, (2) cavity formation, and (3) tissue and bone destruction. Laceration is the tissue destruction as the bullet moves
1154 AORN Journal, May 1982, Vol35, No 6

along its path. A bullet passing through brain tissue will cause a more serious injury than one passing through skin and muscle. Cavity formation occurs as energy is dissipated outwardly from the bullet as it moves along its path. The violent propulsion of tissue away from the tract can damage structures at con- siderable distance from the tract itself. When the cavity collapses, after 5 to 10 milliseconds, a suction force is created, and foreign material and debris may be drawn into the wound. Tissue and bone destruction are determined largely by the wounding potential of the weapon. This is directly related to the velocity of the bullet.
Shotgun wounds are responsible for more deaths than other types of firearms. The most important deter- minant of magnitude of injury is the distance from which the injury was re- ceived. Wounds received from a dis- tance greater than seven yards seldom cause significant injury, while those re- ceived from less than three yards pro- duce massive tissue destruction.l* Shotgun wounds also carry a greater threat of subsequent infection than other gunshot wounds because of con- taminated wadding used in the shells."
A local infection can impair systemic host defenses.
Burns. Burns can be divided into thermal, electrical, and chemical in- juries. Although the cause may vary, the goals of all burn wound care are: (1) prevention of infection, (2) restoration of hemodynamic stability, and (3) providing adequate nutrition.
Most burns are classified as either partial thickness or full thickness. The
epidermis and superficial layers of der- mis are destroyed in a partial thick- ness burn. This injury can be further classified as superficial or deep partial thickness burn. In a full thickness burn, the entire depth of the dermis is de- stroyed.12
Because they are often diffuse, ther- mal injuries produce systemic responses similar to those associated with shock states. Therefore, restoring hemody- namic stability is of utmost importance in the acute phase.
Wound care depends on the extent and depth of the burn and is too exten- sive to discuss in detail in this article. Current therapeutic regimens include early removal of eschar, covering the wound with topical antibiotic, daily tubbing, and grafting following the ap- pearance of granulation tissue.13 Dur- ing the healing phase, a Jobst-type garment is often used in patients with a tendency toward hypertrophic scar for- mation. This provides constant, pro- longed, external pressure over the heal- ing area and must be worn at all times for one year.14
The extent of an electrical burn is de- termined primarily by the amount of current and duration of contact. An electrical burn causes three typical types of burns: (1) contact burns, (2) arc burns, and (3) thermal burns. In a con- tact burn, the current passes through the body from entry to exit point. This is the most serious type because the cur- rent produces vascular coagulation as well as deep muscle damage and pro- gressive tissue necrosis. Treatment may include early escharotomy, fasciotomy, and amputation in extreme cases. In an arc burn, the current passes outside the body from entry to exit point. The injury it causes is usually not extensive unless the voltage is extremely high. Thermal burns that result from electrical injury are incurred when the victim's clothing ignites, and the wound is similar to that
& 1156 AORN Journal, May 1982, Vol35, No 6

from other thermal burns.15 Chemical burns are caused by contact
with an acid or alkalai substance. The injury resembles a thermal burn. The duration of contact with the substance determines the severity of the burn. Therefore, the most important step in care is removal of the noxious sub- stance. In most cases, this is accom- plished simply by copious water irriga- tion.16
Frostbite is another type of thermal injury. Tissue destruction is thought to occur during thawing since frozen tis- sue is at metabolic standstill. There are two theories of how the damage is caused. The direct theory states that tissues are damaged directly by the ice crystals that form in the intracellular and interstitial tissues. The vascular theory states that a sequence of vaso- constriction, vasodilatation, red cell sludging, and necrosis causes the in- jury. l7 Treatment includes rapid re- warming in 90" to 106" water bath fol- lowed by measures to reduce or prevent edema. If the injury is deep, it is then treated like a full-thickness burn.'*
Healing of traumatic wounds Four of the most important factors af- fecting local wound healing are con- tamination, infection, time of treat- ment, and tissue loss.
Contamination. All traumatic in- juries are considered contaminated be- cause they occur under uncontrolled circumstances. Although a wound bacterial count of greater than lo6 organisms/gm of tissue normally indi- cates significant contamination and the likelihood of infection, in the presence of severe multiple trauma, the number that will cause infection may be much lower.
After severe injury, the patient's local defenses against contamination may be significantly compromised. Studies
have shown that in addition to local vasoconstriction, trauma can cause leukocyte dysfunction and wound hypoxia. Other factors that impair local responses are incomplete hemostasis, hematomas, dead space, and necrotic tissue.lg
Infection. When local defenses cannot adequately fight bacterial contamina- tion, infection takes hold. In the pres- ence of infection, healing not only comes to a halt, but the area of damaged or necrotic tissue can increase greatly. A local infection can impair systemic host defenses which can, in turn, affect local responses to infection. If the infective process is not reversed, it can progress to baderemia and sepsis, now recog- nized as one of the leading causes of death in the trauma patient.20
Time of treatment or repair. Research has shown that the early inflammatory period is critical in local defenses against bacterial contamination. Ani- mal studies have demonstrated that the host's efforts to suppress a developing lesion are greatest during the first few hours following contamination.
This seems to be due to leukocyte chemotaxis and oxidative killing of bacteria. These antibacterial mecha-
The single most important factor in healing is shock. nisms are most active in the first two to three hours after wounding, and it ap- pears that the ultimate size of the lesion is determined in this early period. These data suggest that enhancing these sys- tems during this critical time can signif- icantly alter the size and nature of the lesion. Restoring adequate circulation and administering antibiotics are the
1160 AORN Journal, May 1982, Vol35, No 6

most effective ways to augment the host’s antibacterial mechanisms.21
Tissue Zoss. Tissue loss or destruction delays wound healing because of the additional time required for its catabolism and clearance. Absorption and clearance of debris places further stress on other injured systems such as the kidneys, and this in turn can affect local wound responses.22
Wounds with considerable skin loss allowed to heal spontaneously, will do so by an inflammatory response (fibro- plasia, epithelial regeneration, and con- traction). Contraction is especially im- portant in the healing of open tissue defects. While the process assists greatly in healing wounds, it does not always completely close the defect. The wound‘s ability to contract is limited if the surrounding skin is not mobile, as in the pretibial area. In such areas, a de- bilitating contracture may result. Grafts and flaps are usually required when skin loss is significant.23
A final problem of skin loss is that often prolonged exposure of deep struc- tures may result in their injury even though they may have been healthy ini- tially.
Shock and wound healing The single most important systemic fac- tor in healing of a traumatic wound is whether the individual has been in the shock state. Shock is defined simply as a state of inadequate tissue perfusion. This affects every tissue of the body, some more than others, because of selec- tive compensatory mechanisms. Shock may have serious effects on the body’s most important organ systems, and these hypoperfused organ systems can, in turn, affect wound healing (Figs 1 and 2).
Cardiovascular. One of the progres- sive changes during shock is a shunting of blood from the periphery and gastro-
intestinal tract in an attempt to perfuse more vital organs. If the hypovolemic state is not corrected, the individual will become hypotensive with decreased myocardial contractility and decreased vascular responsiveness to catechola- mines. Eventually, this causes arterial hypoxemia, decreased microcirculation, and refractory
In the early compensatory phases of shock, peripheral vasoconstriction and shunting of blood not only produces wound hypoxia but impedes delivery of leukocytes and other antibacterial agents. Direct vascular damage in the wound area can rapidly cause progres- sive necrosis until vascular integrity is restored.
Lungs. If the lungs are subjected to severe hypoperfusion, a condition known as posttraumatic pulmonary in- sufficiency may result. The exact pathophysiologic mechanism of this syndrome is still being debated. The re- sult is arterial hypoxemia and hyper- carbia. This contributes t o wound hypoxia and leads to acid base distur- bances.
Gastrointestinal tract. Prolonged vasoconstriction in the splanchnic bed can cause loss of the protective mucosa in the GI tract. At worst, this produces a hemorrhagic necrosis and at best, a pro- longed ileus. This impaired functioning unfortunately occurs when the patient is in a hypermetabolic state. A patient’s caloric needs following severe trauma may increase by a s much as 50%. Wound repair is influenced by the nu- tritional disorders that may arise from this altered metabolic state. Wound healing may be delayed, and there may be wound dehiscence. 26
Liver. Hepatic failure, one of the com- plications of hypoperfusion during se- vere shock, brings about hypoprotein- emia and coagulopathies. Both have an effect on wound healing.27 Hepatic changes are degenerative, with areas of
d- AORN Journal, May 1982, Vol35, No 6 1161
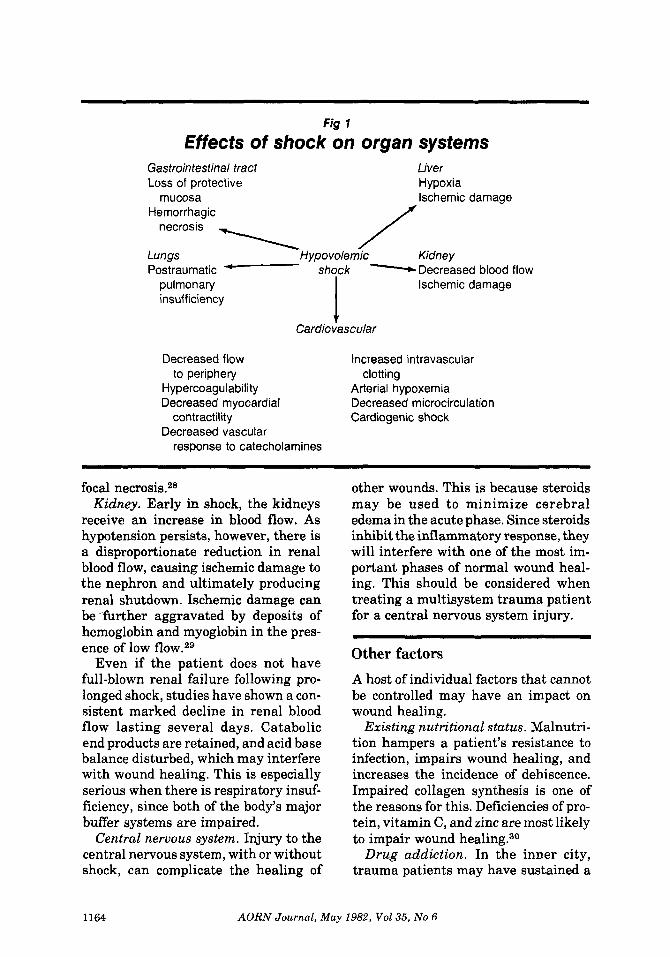
Fig I
Effects of shock on organ systems Gastrointestinal tract Loss of protective
mucosa
Liver Hypoxia Ischemic darnaae -
Lungs Hypovolemic / Kidney
Hemorrhagic
Postraumatic - shock Decreased blood flow
necrosis \ pulmonary insufficiency
Ischemic damage
t Cardiovascular
Decreased flow Increased intravascular
Hypercoagulability Arterial hypoxemia Decreased myocardial Decreased microcirculation
contractility Cardiogenic shock Decreased vascular
response to catecholamines
to periphery clotting
focal necrosis.28 Kidney. Early in shock, the kidneys
receive an increase in blood flow. As hypotension persists, however, there is a disproportionate reduction in renal blood flow, causing ischemic damage to the nephron and ultimately producing renal shutdown. Ischemic damage can be further aggravated by deposits of hemoglobin and myoglobin in the pres- ence of low
Even if the patient does not have full-blown renal failure following pro- longed shock, studies have shown a con- sistent marked decline in renal blood flow lasting several days. Catabolic end products are retained, and acid base balance disturbed, which may interfere with wound healing. This is especially serious when there is respiratory insuf- ficiency, since both of the body’s major buffer systems are impaired.
Central neruous system. Injury to the central nervous system, with or without shock, can complicate the healing of
other wounds. This is because steroids may be used to minimize cerebral edema in the acute phase. Since steroids inhibit the inflammatory response, they will interfere with one of the most im- portant phases of normal wound heal- ing. This should be considered when treating a multisystem trauma patient for a central nervous system injury.
Other factors A host of individual factors that cannot be controlled may have an impact on wound healing.
Existing nutritional status. Malnutri- tion hampers a patient’s resistance to infection, impairs wound healing, and increases the incidence of dehiscence. Impaired collagen synthesis is one of the reasons for this. Deficiencies of pro- tein, vitamin C, and zinc are most likely to impair wound healing.30
Drug addiction. In the inner city, trauma patients may have sustained a
1164 AORN Journal, May 1982, Vol35, No 6
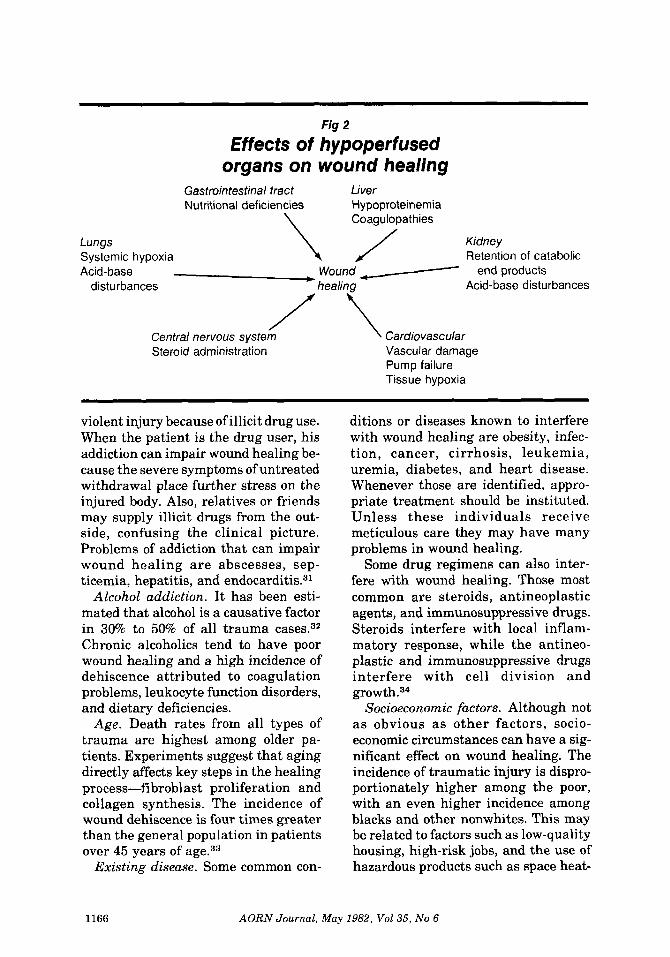
Fig 2
Effects of hypoperfused organs on wound healing
Gastrointestinal tract Liver Nutritional deficiencies Hypoproteinemia
Coagulopathies Lungs \ / Kidney Systemic hypoxia Retention of catabolic Acid-base Wound end products
disturbances healing Acid-base disturbances
Central nervous svstem Cardiovascular Steroid administration Vascular damage
Pump failure Tissue hypoxia
violent injury because of illicit drug use. When the patient is the drug user, his addiction can impair wound healing be- cause the severe symptoms of untreated withdrawal place further stress on the injured body. Also, relatives or friends may supply illicit drugs from the out- side, confusing the clinical picture. Problems of addiction that can impair wound healing are abscesses, sep- ticemia, hepatitis, and end~card i t i s .~~
Alcohol addiction. It has been esti- mated that alcohol is a causative factor in 300/0 t o 50% of all trauma cases.32 Chronic alcoholics tend to have poor wound healing and a high incidence of dehiscence attributed to coagulation problems, leukocyte function disorders, and dietary deficiencies.
Age. Death rates from all types of trauma are highest among older pa- tients. Experiments suggest that aging directly affects key steps in the healing process-fibroblast proliferation and collagen synthesis. The incidence of wound dehiscence is four times greater than the general population in patients over 45 years of age.33
Existing disease. Some common con-
ditions or diseases known to interfere with wound healing are obesity, infec- tion, cancer, cirrhosis, leukemia, uremia, diabetes, and heart disease. Whenever those are identified, appro- priate treatment should be instituted. Unless these individuals receive meticulous care they may have many problems in wound healing.
Some drug regimens can also inter- fere with wound healing. Those most common are steroids, antineoplastic agents, and immunosuppressive drugs. Steroids interfere with local inflam- matory response, while the antineo- plastic and immunosuppressive drugs interfere with cell division and growth . 34
Socioeconomic factors. Although not a s obvious a s other factors, socio- economic circumstances can have a sig- nificant effect on wound healing. The incidence of traumatic injury is dispro- portionately higher among the poor, with an even higher incidence among blacks and other nonwhites. This may be related to factors such as low-quality housing, high-risk jobs, and the use of hazardous products such as space heat-
1166 AORN Journal, May 1982, Vol35, No 6

ers and gas stoves.3s The poor may delay in seeking treat-
ment. Medical care may be inaccessible, or treatment may be postponed because the injury was sustained during a crime. They have poor medical re- sources for adequate follow-up care and lack money for obtaining supplies or medication necessary for proper wound care at home.
Nursing implications Early identification of the patient who is at the greatest risk for develbping problems in wound healing is the most important factor in promoting healing. Five other points are also worth re- membering.
Circulatory stability. If the length and degree of hypoperfusion can be reduced during the early stages following in- jury, many of the problems related to shock can be lessened. The nurse must have skills to initiate fluid therapy and hemodynamic monitoring and a thor- ough understanding of the mechanism of shock. This includes the fluid shifts that occur during and after shock and the way these changes are reflected in the patient's hemodynamic parameters. Charting intake and output is essential for picking up and correcting trends pointing toward deterioration of the pa- tient's condition.
Maintaining tissue perfusion. Al- though restoring fluid volume is paramount in maintaining tissue per- fusion, preventing hematoma or local edema formation can aid in this as well. Ongoing assessment of the injured tis- sue includes checking the patency of drains, and assuring adequate circula- tion distal to circumferential wounds or dressings.
Maintaining adequate arterial oxy- gen. Any severely injured patient should be provided with supplemental oxygen during resuscitation. If the pa-
tient is in shock or has any sign of respi- ratory distress, oxygen should never be withheld until blood gas values or other test results are received. Meticulous pulmonary hygiene should be standard during all phases of trauma care. I t should be especially aggressive if the patient has thoracic or pulmonary in- juries.
Infection prevention. This requires meticulous wound care especially dur- ing the two- to three-hour period follow- ing injury when local defense systems are most active. Infection at sites dis- tant from the injury can affect wound healing, so all catheters, drains, and in- vasive monitoring equipment should be handled aseptically.
Maintaining adequate nutrition. In the period of hypermetabolism follow- ing severe trauma, caloric needs in- crease by as much as and can go as high as 80% in the burn patient. Provid- ing for nutritional requirements not only promotes healing directly but also supports the immune system. In the first few days after injury, attention is direct.ed toward restoring hemodynam- ic stability. When this is achieved, a comprehensive and progressive dietary program should be instituted. Ideally, feeding begins by the oral route. In pa- tients with extensive gastrointestinal tract injuries or malfunction, par- enteral nutrition will be required.
Because trauma includes such a wide variety of injuries and may involve a number of organ systems, promoting healing of these wounds is complex. Each of the types of traumatic wounds requires appropriate management. The five nursing interventions described, however, can apply to any traumati- cally injured person. 0
Notes
Clinical Symposium 29:3 (1 977) 4. 1. W Michael Bryant, "Wound healing," Ciba
2. George J Hill, Outpatient Surgery, 2nd ed
1168 AORN Journal, May 1982, Vol35, No 6
(Philadelphia: W B Saunders, 1980) 109. 3. Bryant, "Wound healing," 6. 4. Hill, Outpatient Surgery, 113. 5. John M Finley, Practicai Wound Manage-
ment (Chicago: Year Book Medical Publishers, 1981) 8.
6. George Zuidema, Robert Rutherford, Walter Ballinger, The Management of Trauma, 3rd ed (Phil- adelphia: W B Saunders, 1979) 13.
7. Bryant, "Wound healing," 20. 8. Zuidema, Management of Trauma, 543. 9. Ibid.
10. lbid, 541. 11. Hill, Outpatient Surgery, 466. 12. Zuiderna, Management of Trauma, 541. 13. Ibid, 703. 14. Finley, Practical Wound Management, 78. 15. Zuidema, Management of Trauma, 713. 16. Ibid, 716. 17. Betty J Alexy, "Problems due to cold," Jour-
nal of Emergency Nursing 6 (JanuarylFebruary 1980) 23.
18. Alexander Walt, Robert Wilson, eds., Man- agement of Trauma: Pitfalls and Practice (Philadel- phia: Lea 8, Febiger, 1975) 457.
19. Thomas Hunt, J Englebert Dunphy, eds., Fundamentals of Wound Management (New York: Appleton-Century-Crofts, 1979) 183.
20. Donald E Fry, "Infection in the trauma patient: The major deterrent to good recovery," Heart and Lung 7 (March-April 1978) 257; Hill, Outpatient Surgery, 134.
21. Hunt, fundamentals of Wound Manage- ment, 195-197.
22. Zuiderna, The Management of Trauma, 39. 23. Bryant, "Wound healing," 20. 24. Zuidema, The Management of Trauma, 48. 25. F W Blaisdell, "Pathophysiology of the respi-
ratory distress syndrome," Archives of Surgery 108
26. Hunt, fundamentals of Wound Manage- ment, 292.
27. Walt, Management of Trauma: Pitfalls and Practice, 564.
28. Zuidema, The Management of Trauma, 60. 29. lbid, 59. 30. Hunt, fundamentals of Wound Manage-
ment, 187, 292. 31. Walt, Management of Trauma: Pitfalls and
Practice, 83. 32. Zuidema, The Management of Trauma, 796. 33. Ibid, 794. 34. Walt, Management of Trauma: Pitfalls and
35. Zuidema, The Management of Trauma, 797.
(1 974) 44-49.
Practice, 11 3.
Audiovisual review Nurse-Physician Communications This video seminar for nurse managers is presented in the form of a conversation between Ann Marinner, RN, PhD, a nurse educator, and Emmett C Murphy, PhD, a management consultant. Murphy analyzes the difficulty in nurse-physician relationships in terms of a theory of communication that states that communication occurs on three levels: child, parent, and adult.
In this seminar, Murphy states his belief that because the physician has been deprived of necessary stages of socialization and emotional development due to the intense nature of his training, he is unable to communicate on an adult level but instead communicates as a child, "I want," or as a parent, "do it." Murphy feels that because nursing education permits the student to pass through the stages of emotional development in a more normal fashion, the nurse is better equipped than the physician to communicate at an adult level.
Murphy states that the nurse must take the initiative to control relationships with the physician because she is in a better position to handle stress in a positive manner. Several examples of nurse-physician communication problems are discussed, with recommendations for appropriate action in each instance.
This seminar is especially valuable for nurse managers in any area but could also be used by staff nurses, unit secretaries, and other personnel with extensive physician contact. It is very appropriate for areas of high stress such as the operating room where there is a great deal of nurse-physician interaction.
The 30-minute videocassette, made in 1981, is available from Communications in Learning, Inc, 2280 Main St, Buffalo, NY 14214. The price is $225.
Susan Puterbaugh, RN, CNOR Audiovisual Committee
1170 AORN Journal, May 1982, Vol35, No 6