Embed Size (px)
Citation preview
912 BRIT. J. SURG., 1969, Vol. 56, No. 12, DECEMBER
GREEN, P., and RUBIN, L. (Igsg), Am. J. Obstet. Gynec.,
HALLENBECK, G. A., and ADSON, M. A. (1961), Archs
HERMANN, R. E., and ESSELSTYN, C. B. (1967), Ibid., 95,
HOFFBAUER, F. W., BOLLMAN, J. L., and GRINDLAY, J. H.
HUGGINS, C., and OKAMATO, R. (1960),J. exp. Med., I 12,
JARVINEN, P. A., MAAMIES, T., and TERHO, J. (1969,
PALMER, E. D. (rg61), Am. J. med. Sci., 242, 223.
78, 141.
Surg., Chicago, 83, 370.
956.
(IgsO), Gastroenterology, 16, 194.
883.
Annls Chir. Gynaec. Fenn., 54, 119.
PATTON, T. B. (1965), Sth. med. J., Nashville, 58, 1447. SCOTT, N. M., and DEUTSCH, D. L. (1g55), Am. 3. SHALDON. S . . and SHEIUOCK. S. (1962). Lancet. I. 61.
Gastroent., 24, 305.
STATHERS, 6. M., MA, M. H., ~ ~ ~ B & K B u R N , C. k. B.
WALKER, R. MILNES (1962), Proc. R. SOC. Med., 55, 770. WHELTON, M. J., and SHERLOCK, S. (1968), Lancet, 2,
(1968), Australas. Ann. Med., 17, 12.
995.
Gynec., 19, 44. WILBANKS, G. D., and KLINGES, K. G. (1967), Obstet.
YARBOROUGH, C. T. (1967), Trans. Pact$ Cst oto-ophthal. SOC., 48, 193.
PROLONGED pH RECORDING IN THE STUDY OF GASTRO-OESOPHAGEAL REFLUX*
BY J. SPENCER HAMMERSMITH HOSPITAL, LONDON
IN spite of extensive studies of the physiology of the cardia little is known about the causes and character- istics of gastro-oesophageal reflux. In patients with hiatal herniae the timing and duration of reflux are not known and inevitably management remains mainly empirical. Clinical and radiological assess- ments of reflux are often at variance and this emphasizes the need for a simple method to deter- mine whether or not reflux is taking place. The most sensitive method available is monitoring of oesophageal pH (Tuttle and Grossman, 1958; Weber and Gregg, 1959; Morgan, Hill, and Selby, 1963) but technical difficulties have proscribed its routine use. Recently the development of composite elec- trodes in which reference leads are incorporated have reduced the difficulties and have made possible prolonged recordings of oesophageal pH. In this study they were used to record the timing and duration of reflux in patients with ‘sliding’ hiatal herniae and in control subjects.
SUBJECTS AND METHODS Twenty-six subjects were studied. Fifteen had
symptomatic ‘ sliding’ hiatal herniae which had been demonstrated unequivocally by barium studies. Eleven others were studied as ‘controls’; only I was healthy and asymptomatic, the others having duodenal ulcer, gall-stones, or undiagnosed upper abdominal pain (Table I ) . In none of this group was there any serious clinical or radiological suspicion of hiatal hernia.
The p H electrode used was the Cambridge Instruments Company gastro-intestinal glass elec- trode, which was connected through a pH meter (E.I.L. 23a) to a pen recorder (Everett Edgcumbe Dwarf Recorder) which wrote on paper moving at 6 in. per hour. Before each study the apparatus was calibrated by immersing the electrode in buffer solutions (pH 4 and 9.1). The electrode was then passed transnasally into the stomach and the gastric pH noted. It was then withdrawn into the oesophagus
* Based on a paper delivered to the Surgical Research Society in Leeds in July, 1968.
under radiological control until the recording tip lay at the junction of the middle and lower thirds of the oesophagus. Patients were returned to the ward with the electrode in position, and the recording continued under normal ward conditions. Normal hospital meals and drinks were allowed, but care was taken to avoid constituents of low pH such as vinegar, canned fruit, and fruit juices. Alkaline medicines were forbidden. At night sodium amytal (200-300 mg.)
Table I.-SUBJECTS STUDIED Diannosis
‘Sliding’ F t a l hernia ‘ Controls
Normal ( I ) Duodenal ulcer (6) Gall-stones ( I ) Dyspepsia {radiograph
negative) (3)
Total
No. ofCares 15 I 1
- 26
was given to encourage sleep, and patients were positioned to sleep flat on one side for 3 hours, after which they were turned on to the other side for 3 hours. Patients were randomly allocated to sleep first in the right or left lateral positions.
In 21 subjects an 18-hour recording was obtained, which for analytical purposes was divided into a 12-hour day (11.00 a.m.-II.oo p.m.) and a 6-hour night (11.00 p.m.-5.00 a.m.). At the end of this period the electrode was withdrawn. Three patients were unable to tolerate the electrode for the full period, and in these a It-hour day recording was obtained. In I control subject a 6-hour night record- ing only was made.
The recordings were analysed to determine the duration of reflux, which was said to have occurred if the pH fell below 4. This level was chosen as it indicates unequivocal reflux and may also be of some significance as regards peptic digestion. The total period during which pH was below 4 was defined as the reJZux period, measured in minutes. Reflux periods were determined for the 12-hour day, the 6-hour night, and for the total 18-hour period of the test.
SPENCER: PROLONGED pH RECORDING 913
In 15 patients maximal acid output (MAO) in mEq. per hour was determined by the use of an intravenous histamine infusion, 0.04 mg. per kg. per hour (Lawrie, Smith, and Forrest, 1964) or intra- muscular pentagastrin 6 pg. per kg. (Johnston and
H m i l hernra Lunch
O/--rI--zz ____
12.30 p m 1.00 p.m. 1.10 p.m
7- ,i-------- 1 2 3 0 p m l W p m ~ I 30 p r m
Tlme
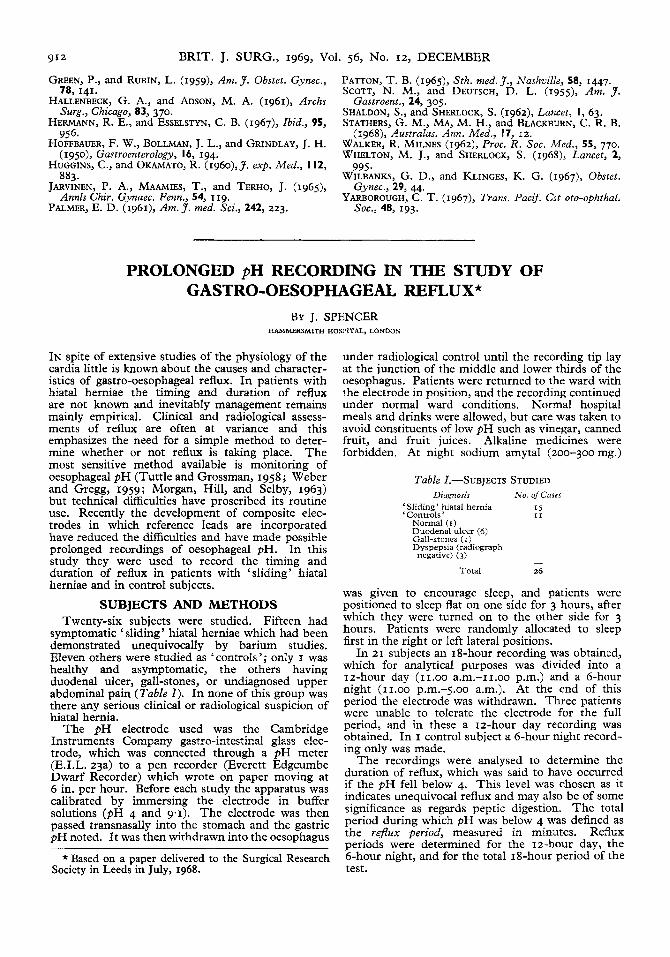
pauents with hiatal herma (A) and & d e n a l ulcer (6) . FK 1 --Extracts from typical recordm s of oesophageal pII in
Jepson, 1967). It was then possible to relate the duration of reflux to the maximal acid output.
RESULTS Extracts from typical recordings in subjects with
duodenal ulcer and hiatal hernia are seen in Fig. I . The period illustrated includes the midday meal, which was followed in the patient with a hernia by
7hble II.-REFLUX PERIOD
I .. 1 MEAN REFLUX I 1 I PERIOD
average of only 3 7 per cent of the recording period, and the difference between the mean reflux periods in the two groups was significant.
b. Mean Iz-hour day reflux periods revealed very similar differences, with significantly longer reflux in patients with herniae (Table ZZ).
c. Night reflux. Ten of the 12 subjects with herniae experienced some episodes of reflux, with a mean
Duodenal ulcer H m a l hernia
loo- " 5 - P 0001
'% 40-
I0
0 388 0 1
0 10 10 30 40 Maximal acid output (mEq. per hour) Maximal acid ourpul (mEq per hour)
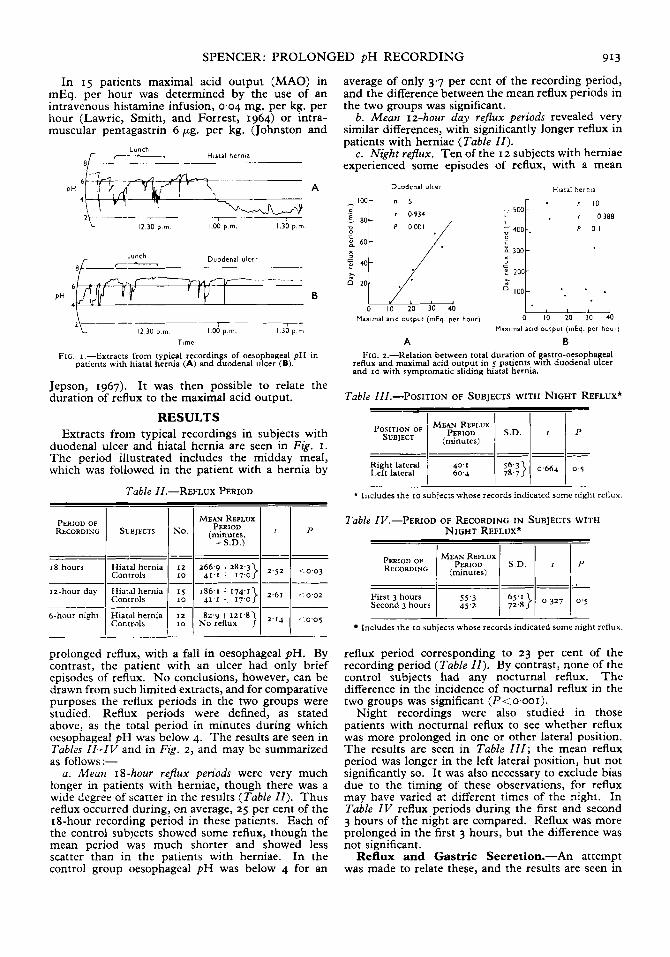
A B FIG. z.--Kelation between total duration of gastro-oesophageal
reflux and maximal acid output in 5 patients with duodenal ulcer and 10 with symptomatic sliding hiatal hernia.
Table III.--POSITION OF SUBJECTS WITH NIGHT REFLUX* I I I I
--- --- Right I.eft lateral lateral 1 : z i 1 $.:)I 0 6 6 4 1 0 ' 5
* Includes the 10 subjects whose records indicated some night reflux.
Table IV.--PERIOD OF RECORDING IN SUBJECTS WITH NIGHT REFLUX*
I I I I
First 3 hours Second 3 hours I i::: I ;:::} 1 0'327 I O"
Includes the 10 subjects whose records indicated some night reflux.
prolonged reflux, with a fall in oesophageal pH. By contrast, the patient with an ulcer had only brief episodes of reflux. No conclusions, however, can be drawn from such limited extracts, and for comparative purposes the reflux periods in the two groups were studied. Reflux periods were defined, as stated above, as the total period in minutes during which oesophageal pH was below 4. The results are seen in Tables ZZ-IV and in Fig. 2, and may be summarized as follows:-
a . Mean 18-hour rejhx periods were very much longer in patients with herniae, though there was a wide degree of scatter in the results (Table ZZ). Thus reflux occurred during, on average, 25 per cent of the 18-hour recording period in these patients. Each of the control subjects showed some reflux, though the mean period was much shorter and showed less scatter than in the patients with herniae. In the control group oesophageal pH was below 4 for an
reflux period corresponding to 23 per cent of the recording period (Table ZZ). By contrast, none of the control subjects had any nocturnal reflux. The difference in the incidence of nocturnal reflux in the two groups was significant (I-'<o.ooI).
Night recordings were also studied in those patients with nocturnal reflux to see whether reflux was more prolonged in one or other lateral position. The results are seen in Table 111; the mean reflux period was longer in the left lateral position, but not significantly so. I t was also necessary to exclude bias due to the timing of these observations, for reflux may have varied at different times of the night. In Table ZV reflux periods during the first and second 3 hours of the night are compared. Reflux was more prolonged in the first 3 hours, but the difference was not significant.
Reflux and Gastric Secretion.-An attempt was made to relate these, and the results are seen in
914 BRIT. J. SURG., 1969, Vol. 56, No. 12, DECEMBER
Fig. 2. Five of the patients with ulcers had gastric secretion measured. Although the number was so small, Fig. 2 A suggests a highly significant correla- tion, patients with higher maximal acid output having longer total periods of reflux by day. By contrast (Fig. I B), 10 patients with hiatal hernia but without concomitant duodenal ulceration were studied, and no such correlation was found.
DISCUSSION The measurement of oesophageal p H is a sensitive
means of detecting gastro-oesophageal reflux, and often gives information which is not available by radiology alone. Morgan and others (1963), in a study of 115 patients with hiatal hernia, found that only 26 (23 per cent) had reflux revealed by barium studies. Oesophageal p H measurements confirmed the presence of reflux in 24 of these patients and also revealed reflux in another 69 (60 per cent). These and other workers have attempted to plot the ‘pH profile ’ across the gastro-oesophageal junction and to detect reflux on a short-term basis. The use of prolonged recording adds a further dimension to these studies, making it possible to determine the timing and the duration of reflux. Such prolonged studies have been found feasible and technically straightforward, with minimal discomfort to patients. The clinical usefulness of such procedures depends on preliminary studies to establish the pattern of reflux in patients with hiatal hernia and in control subjects.
The most striking difference in the present study was in the incidence of night reflux. Ten of 12 patients with herniae experienced some nocturnal reflux, though in some reflux was very brief. By contrast none of the control subjects experienced reflux at night; this is perhaps more surprising since only one of the control group was healthy and asymptomatic.
During the day control subjects showed episodes of reflux, particularly after meals, with a mean reflux period of just over 40 minutes. The equivalent period in patients with herniae was just over 3 hours.
If the whole 18-hour period is considered, reflux in patients with herniae lasts an average of just over 4 hours over all. By extrapolation it is possible that in each 24 hours a patient with a hiatal hernia may have gastric juice in contact with his oesophageal mucosa for over 5 hours. The equivalent period in our control subjects would be less than I hour. This is clearly in accord with current theories concerning the role of reflux in the aetiology of oesophagitis.
It is often recommended that one aim of surgical treatment for hiatal hernia should be to reduce gastric-acid secretion; vagotomy or gastric resection are employed to this end. This presupposes that a high gastric secretory capacity is associated with
increased gastro-oesophageal reflux. It is known, however, that neither basal nor maximal acid secretion is raised above normal levels in patients with sympto- matic hiatal hernia, unless there is coexistent duodenal ulceration (Williams, Lawrie and Forrest, 1967). It is of interest in the present study that patients with duodenal ulcer had day reflux periods which were directly related to maximal acid output; although the number involved was very small, this correlation was highly significant (P< o-001). In patients with hiatal hernia no such correlation existed. It must, however, be remembered that this analysis is based on the periods of reflux and does not take into account the volume of fluid regurgitated into the oesophagus. Large and small quantities of gastric juice may be of the same pH, but might have quite different effects on the oesophageal mucosa.
SUMMARY A method is described for the continuous monitor-
ing of oesophageal pH over periods of up to 18 hours. Recordings of this kind have been carried out in
patients with sliding hiatal hernia, and the results compared with those obtained in control subjects.
The results indicate that during the day reflux occurs for significantly longer periods in patients with herniae than in controls. Nocturnal reflux occurred in the majority of patients with herniae, but in none of the control subjects. In 5 patients with duodenal ulcer there was a significant positive correla- tion between maximal acid output and the duration of reflux, but no such correlation was present in patients with hiatal herniae.
Acknowledgements.-I wish to thank Mr. R. H. Franklin for encouraging me in this study; Professor R. B. Welbourn for his continued interest and help; Dr. F. G. Pattrick for advice on the technique of pH recording which we used; and Mr. R. A. Sellwood for helpful criticism of the script. I am also indebted to the laboratory nurses, Mrs. Shearman and Mrs. Pope, for their skilful assistance.
REFERENCES JOHNSTON, D., and JEPSON, K. (1967), Lancet, 2,585. LAWRIE, J. H., SMITH, G. M. R., and FORREST, A. P. M.
MORGAN, E. H., HILL, L. D., and SELBY, D. K. (1963),
TUTTLE, S. G., and GROSSMAN, M. I. (1959, Proc. SOC.
WEBER, J. M., and GREGG, L. A. (19591, Gastroenterdogy,
WILLIAMS, C. B., LAWRIE, J. H., and FORREST, A. P. M.
(1964), Ibid., 2, 270.
Dis. Chest, 43, 367.
exp. Biol. Med., 98, 225.
37, 60.
(1967), Lancet, I , 184.

















![The Retroactive Heartburn-Gastro-Oesophageal Reflux Disease · reflux esophagitis [1,2]. Gastro-oesophageal reflux disease (GERD) is a frequent condition and demonstrates a prevalence](https://img.pdfslide.us/doc/110x75/5f16ecc61df9c2748c704a75/the-retroactive-heartburn-gastro-oesophageal-reflux-disease-reflux-esophagitis-12.jpg)











