Embed Size (px)
Citation preview
The Editor interviews:Lawrence Sherman, M.D.Associate DirectorDepartment of MedicineQueens Hospital CenterJamaica, New York
Editor: The onrushing pace of nett developments has made the possiblerelation of prolactin, a single chain polvpeptide hormone, andliuniati bfl'(Ist ((i?i(('i (ifl itiipOt't(Itit (‘.Vp('?'i?tic?ital subject. ‘¿�@%/l(utis
kiio till about prolactuti (111(1/)l.('(i@t ancer in ant nut!
In the C3H strain of mice, which is infected with mammary tumorvirus, mammary cancer develops spontaneously in females fromhyperplastic alveolar nodules that arise from apparently normalglandular epithelium. The progression of hyperplastic nodules tomammary cancer is at least partially dependent on prolactin. Inrats, both prolactin and estrogen seem to be of primary importancein influencing the growth of breast tumors, which are chemicallyinduced. High doses of estrogen stimulate pituitary secretion ofprolactin in rats, yet paradoxically result in tumor regression. probably through the peripheral effects on breast tissue. Some of thestrongest evidence for the role of prolactin in rodent breast cancerhas been obtained by the manipulation of serum levels with L-dopaor the ergot derivatives.
Editor: I)o these (It'lU.,'@.S!Illuul/(it(' (it' (Iil1u1?uiXllJ)l'O!aitllI /ei'el,s 10 ho
Dr. Sherman: L-dopa .and ergot derivatives increase secretion of prolactininhibiting factor, thereby inhibiting hormone release and loweringprolactin levels in the blood. Ergot drugs, such as ergocornine and2-bromo-alpha-ergocryptine, may act directly on the pituitary torestrict prolactin production.
Lowering serum prolactin with ergot drugs or 6-methyl-8-betaergoline-acetonitrile, a synthetic ergot, suppresses the development of nodules and decreases the frequency of mammary lesions,but has little effect on established tumors. Welsch and Griblerfound that ergot drugs reduced the growth of hyperplastic nodulesand the incidence of mammary cancers in both nulliparous and
258 CA—ACANCERJOURNALFORCLINICIANS
ProlaCtinand Breast Cancer
Dr. Sherman:
multiparous mice, although effectiveness was greatest in youngvirgin mice. Tumors developed in only one of 90 mice treated withergot for one year and discontinued for 10 months, as comparedto 24 of 90 untreated controls. Reduced prolactin levels decreasedthe rate of mammary tumors in the presence of normal ovarianactivity and estrous cycles. A study by Yanai and Nagasawa confirmed that ergot drugs inhibited the growth of hyperplastic alveolar nodules in mice and greatly decreased the number of tumors,if the drugs were started early. Once mammary tumors are established in the mouse system, prolactin does not appear necessaryfor their maintenance or growth.
Editor: I-laic the effectsof increased serum prolactin been studied?
Dr. Sherman: Yes. In rats, high fat diets raised both prolactin levels and induction rate of mammary tumors by dimethylbenzanthracene(DMBA), implying that prolactin may be a mediating factor inthe increased frequency of tumors. Supporting this hypothesis isthe observation that 2-bromo-alpha-ergocryptine, which lowersserum prolactin, negates the higher incidence of tumors in rats onhigh fat diets.
Paradoxically, in female Sprague-Dawley rats, both increasesin prolactin (produced by pituitary grafts, drugs, median-eminencelesions, handling, ether anesthesia, or administration of estrogenand progesterone) and decreases in prolactin (caused by hypophysectomy or ovariectomy) inhibit induction of mammary tumors bydimethylbenzanthracene, but only if administered before the carcinogen or soon thereafter. Stimulation of breast tissue by superphysiologic amounts of prolactin apparently “¿�protects―the breastfrom dimethylbenzanthracene; low levels of prolactin and estrogenmay limit tumors because a sufficiency of these hormones maybe necessary for tumor development.
VOL 25, NO 5 SEPTEMBER/OCTOBER1975 259

In rats, once tumors are established, their size and number continue to be influenced by the hormonal environment. Smaller lesions respond more rapidly and completely to ergocornine thanlarger ones, suggesting that even induced cancer becomes morehormone independent with age.
Editor: Ho it, appli('ab!e a me these e.vperu imuemutat studies' 1(1liutiuioiii.s'?
Dr. Sherman: It has recently been hypothesized that human breast cancer proceeds along lines similar to murine mammary tumors in the progression from hyperplastic nodules to cancer. Wellings and Jensenfound hyperplastic lobule-like structures and early foci of ductalcarcinoma in situ in the terminal ducts and lobules of human breasttissue. Hyperplastic changes occurred most often, and showed ahigher grade of atypia, in cancerous breasts.
However, the hormonal role in breast cancer in humans is muchless straightforward than in animals. First, the actual carcinogens(inducers) such as viruses or chemicals are not known; therefore,the time of induction of breast tumors is not ascertainable. Second.prolactin is one of several hormones (including estrogens andgrowth hormone) that may function as tumor promotors by activating transformed mammary cells. (Figure.) If one looks only atfasting serum levels of prolactin to indicate its role in human breastcancer, one is quickly disappointed. There is no difference in thismeasurement between patients with breast cancer and matchedcontrols. Yet, Kwa and his coworkers, who noted this, also foundhigher prolactin levels in 64 members of nine families with a highincidence of breast cancer, defined as more than two first-degreerelatives with a history of breast cancer. This suggests that prolactin may be a factor in certain high-risk populations.
Editor: iJoe.s t/u(' h!1(u/)uliiV to) (1('!flO!lStt'(lt( .t('.@thtl,u@'e!eu'(uted J)P()l(i('tull 1(t(!,s
i/u patuent.s' nit/u bi'east (‘(1110(1'mimIc(Ill! its /105 S11)10'!nuf)(lrt(ulu('c!
Dr. Sherman: No. It must be remembered that absolute levels of prolactin maynot be the essential element. The ability of prolactin to stimulatemammary tumor growth may depend more on the number of receptor sites in the tumor tissue that are able to react with the hormone.In turn, the number of these sites may be influenced by otherhormones including estrogens. In fact, it was recently shown thatprolactin stimulates estrogen receptor binding capacity in explantsof rat DMBA-induced tumors. The growth of such estrogenresponsive tumors may therefore depend in part on the numberand functional integrity of prolactin receptor sites in breast tumortissue.
Editor: I-las nuamuipuilatiomu0/ /)l'o)l(u('thlu1)5'(11'11,0,'.5Iteo'n.s'tut(/i('(/ill 111011?
Dr. Sherman: L-dopa hasbeen found to produceobjective and subjective remissions in only a few patients and for a very short time. Frantz andhis colleagues found it necessary to treat some patients as often
260 CA—ACANCERJOURNALFORCLINICIANS
Malignantalveolar cell
Malignant
alveolar cell
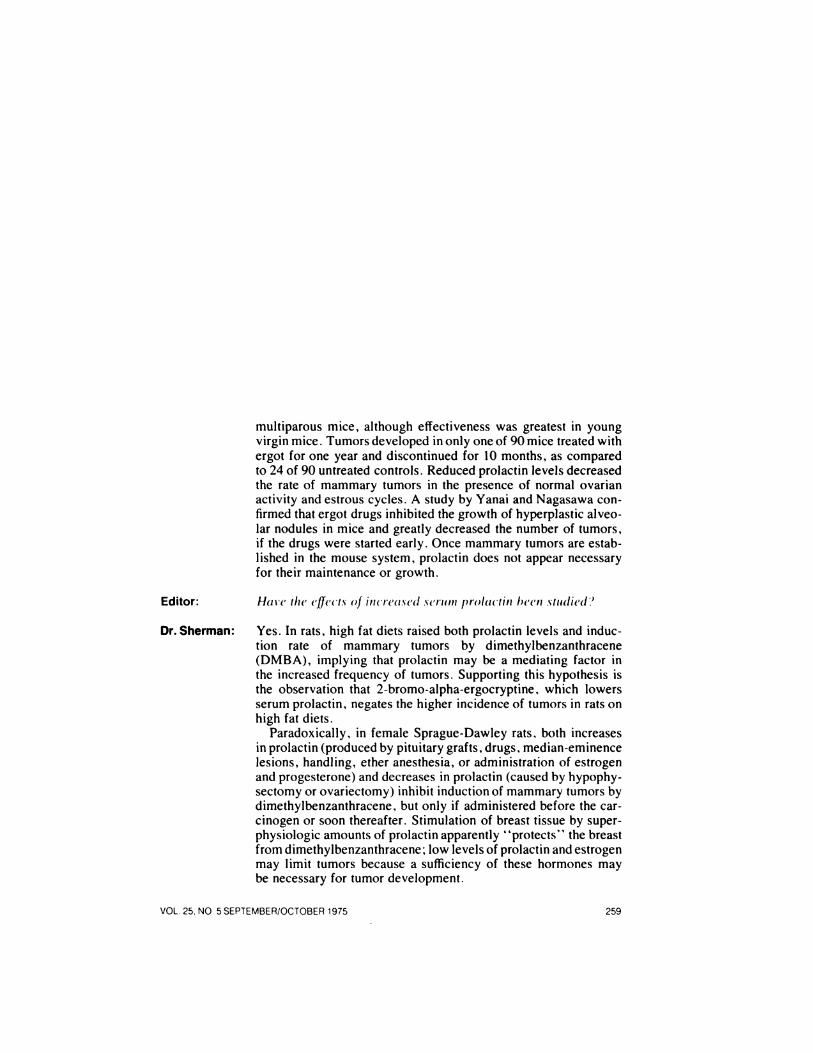
Figure. Hypothetical role of hormones and environmental carcinogens in the biochemicaltransformation and later neoplastic degeneration of human breast cells.
Route A shows possible fates of an alveolar cell transformed to one with malignant potential.Route B shows fate of an alveolar cell protected by early hormonal stimulation. Open triangles indicate onset of menopause.
Unknown carcinogen(s)(?viral, ? chemical)
alveolarcell
Normalalveolar
cell B
Normal, untransformed@ alveolar cell
Involutednormal
alveolarcell‘¿�Unknowncarcinogen (s)(?viral, ? chemical)
+
Protective hormonal
- stimulation
(?early pregnancy)
as every two hours to maintain low serum prolactin. Since prolactin levels peak during sleep and early in the morning, continuouscontrol is extremely difficult.
A study of 30 patients by Minton evaluated the ability of L-dopanot only to ease bone pain in metastatic breast cancer, but moreimportantly, its potential role in predicting response to endocrineablation. Three of his 10 patients with relief of pain were operatedupon. One had an oophorectomy and subsequent remission foreight months. Twenty months after adrenalectomy, another patient was tumor free, and following hypophysectomy, a thirdresponded but only for one month. Unfortunately, this studycannot substantiate the value of L-dopa in predicting response,since only a small number of patients, and only those with reliefof pain, underwent surgery.
Editor: %%‘¿�hatis' i/u effect 0/ utuo't'eu seil pP'ola('ii!u levels lii luuun(u!u.s ?
VOL 25, NO 5 SEPTEMBER/OCTOBER 1975 261
Early cE@1lnvolutedmenopause (@‘@transformed
alveolar cell
.@
Menopause

Dr.Sherman: Womenlivingincountrieswithhighfatconsumption,whichraisesprolactin levels, do have a greater risk of breast cancer. However,in a study by Turkington and colleagues, previously undetectableprolactin was subsequently found in very high concentration insome patients who had an objective remission after pituitary stalksection, which increases serum prolactin. Herein lies a seeminginconsistency with the prolactin hypothesis of human breastcancer.
Editor: Can this he explained?
Dr. Sherman: The perplexing effects of stalk section are possibly explained bythe varying prolactin dependence of tumors. Hormonal requirements of breast tumor tissue obtained by biopsy and cultured invitro have been studied by the Tumour Biology Group at Westminster Hospital in London. Prolactin was needed to maintain cellviability in 32 percent of the tumors, as measured by continuedhigh activity of the pentrose-shunt pathway, which is essential forcancer tissue survival. Later, it was reported that preservation ofviability was found in eight percent of cultured tumors with alow-normal concentration of prolactin in tissue-culture fluid (6 ng.per millimeter). Such concentrations are difficult to achieve withhypophysectomy alone, perhaps explaining the failure of thisoperation in some patients who may have prolactin-dependenttumors.
Editor: Vu/'hvmight sonic tuLfliOF.s'he J)P'Ola('tuli (Iej)endelut (In(I othiei'.s'iuot.@
Dr.Sherman: I wish I knew. Prolactinreceptorshave been identifiedin bothmouse and rat mammary tissue and tumors, and their number hasbeen correlated with the prolactin responsiveness of tumors. However, these receptors have not yet been detected in human breastcancer cells. Cytoplasmic estrogen receptors have been found inhuman breast tumor cells; their presence correlates with tumorregression after endocrine ablation, while their absence correlateswith refractoriness to such ablation. The hormone responsivenessof breast tumors, therefore, seems linked to the presence of theirspecific hormone receptors in the tumor tissue.
Editor: (“anthe prolactin dependency of a tumor he exploited clinically?
Dr. Sherman: Evidence indicatesthat some prolactin-dependenttumorscan survive on low levels of prolactin, but when zero serum levels areapproached, breast tumor regression can occur. Further work, particularly on tumors demonstrated to be prolactin dependent invitro, is necessary in order to evaluate the effect of low serumprolactin levels in patients with breast cancer. By determining thedependence and responsiveness of breast tumors to serum prolactinand growth hormone, it may be possible to predict the eventualtherapeutic effects of hypophysectomy, other endocrine ablationor drugs.
262 CA—A CANCER JOURNAL FOR CLINICIANS

Editor: Will oIru,u@'sbe used in the future to (‘ontrolJ)rola('tun s'e('retuOn (111(1induce tumor megm'e,s',s'iomu?
Dr. Sherman: L-dopa and ergot derivatives only reduce prolactin secretion; lesstoxic and more effective substances will probably be required before the drugs become useful in long-term treatment. New ergotalkaloids, causing less vasoconstriction, and ergoline derivativesare currently being tested in animals. It may be necessary to usecombinations of drugs that simultaneously lower serum prolactinconcentration and antagonize the hormone's effects on the breast.
I must add a caveat here. Just a year ago, the group at Westminster Hospital reported that there was in vitro dependence on growthhormone in the same human breast cancers that demonstrated prolactin dependence. This may explain in part why prolactin inhibition alone can fail to induce complete regression of tumor growth.It certainly re-emphasizes the interrelation of hormones that promote breast tumor growth.
Editor: Mighut prolactin be utilized to) predict thu occurrence of l)rea,s't(‘(ill('('?'?
Dr. Sherman: Because prolactin may be an important factor in certain populations, its measurement in peripheral blood may help identify thoseat high risk before cancer develops. It may even be possible toprevent breast cancer in women by suppressing the developmentof hyperplastic nodules—if they are proven to be forerunners ofcancer in women, as in animals.
Furthermore, the hormonal responsiveness of atypical nodulesin humans must be determined. Because responsiveness to hormone therapy is usually lost once frank breast cancer develops,and because remissions are temporary, suppressing atypicalprecancerous lesions hormonally would offer the best chance ofpreventing breast cancer. Continued work on the relationship ofprolactin and breast cancer should help answer some of these questions and realize some of these hopes.
Editor: “¿�J'buimukson. Dr. Shuem'nuin
VOL 25, NO 5 SEPTEMBER/OCTOBER 1975 263

![Prolactin-induced PAK1 tyrosyl phosphorylation promotes ...[17], while expression of kinase dead PAK in highly inva-sive breast cancer cells significantly reduces cell invasive-ness](https://img.pdfslide.us/doc/110x75/60c3c5a94ad51777967f2e9b/prolactin-induced-pak1-tyrosyl-phosphorylation-promotes-17-while-expression.jpg)



























