Embed Size (px)
Citation preview

Journal of Neurology, Neurosurgery, and Psychiatry, 1975, 38, 849-854
Progressive myoclonic epilepsy due to Gaucher'sdisease in an adult
J. 0. KING'
From the National Hospital for Nervous Diseases, Queen Square, London
SYNOPSIS A 39 year old Jewish male with a 22 year history of progressive myoclonic epilepsy wasfound to have Gaucher cells in his sternal bone marrow. The diagnosis of Gaucher's disease was
confirmed by the demonstration of beta-glucosidase deficiency in fibroblasts. Although neurologicalinvolvement is extremely rare in adults with Gaucher's disease, this disease is another lipidosiswhich should be considered in patients with progressive myoclonic epilepsy.
By progressive myoclonic epilepsy is meant thestriking combination of grand mal seizures andgeneralized myoclonus which, in some instances,may be associated with intellectual deterioration.A mild degree of myoclonic jerking is common inepileptics, particularly before a seizure (Hodskinsand Yakovlev, 1930), but in myoclonic epilepsyit may be prominent, continuous, and disabling.Recording of cerebral evoked potentials (Halli-day, 1967) is a useful confirmatory investigation,as in myoclonic epilepsy the responses are usuallygrossly enlarged. The clinical entity was origin-ally reported by Unverricht (1891, 1895) andlater by Lundborg (1903, 1913) whose workpointed to an autosomal recessive pattern of in-heritance. Lafora and Glueck (1911) describedthe amyloid cytoplasmic inclusion bodiesthroughout the nervous system, but later reportssuggested that at least three different underlyingclinical and pathological groups were presentand these have been reviewed by Halliday (1966).
Lafora body disease is characterized by onsetin the second decade with rapidly progressiveintellectual deterioration, incessant myoclonus,grand mal seizures, and death within 10 years.Parental consanguinity is common. Harrimanand Miller (1955) demonstrated that the in-clusion bodies, which contain mucopolysac-charide, are also present in the liver and heart.An identical clinical picture of progressive myo-1 Address for reprints and correspondence: c/o Division of Neurology,University Hospitals of Cleveland, 2065 Adelbert Rd., Cleveland,Ohio, 44106, U. S. A.(Accepted 14 April 1975.)
849
clonic epilepsy without Lafora bodies has beenreported (Matthews et al., 1969).
In a second group, some patients with myo-clonic epilepsy have had cerebellar ataxia orextrapyramidal signs suggesting involvement ofthe olivodentate system by primary degenerativediseases. Dyssynergia cerebellaris myoclonica(Hunt, 1921) is included in this category as wellas patients with Friedreich's ataxia who developmyoclonus and epilepsy. The onset occurs fromthe second decade onwards and runs a morebenign course with less involvement of highercerebral functions.The third group of patients have an under-
lying lipidosis which is almost invariably juvenileamaurotic familial idiocy. The non-infantiletypes of amaurotic familial idiocy have becomeknown by the term neuronal ceroid lipofuscino-sis (Zeman, 1974) since the identification of thestored neuronal pigments. Sjogren (1931) clearlydistinguished between infantile amaurotic familialidiocy (Tay-Sachs disease) and the juvenile form.In the latter he recognized the characteristicsyndrome of epilepsy beginning between 6 and12 years of age, with progressive extrapyramidalrigidity. Although most patients with juvenileamaurotic familial idiocy have fits, in a fewinstances the degree of associated myoclonus hassuggested progressive myoclonic epilepsy. Mar-inesco (1925) reported a case of progressivemyoclonic epilepsy in a boy aged 6 years withamaurotic familial idiocy in whom the brainshowed lipid deposits in many ganglion cells

J. 0. King
with the additional feature of small roundedwell-defined bodies, similar to the nucleus, in thecytoplasm. Similar cases have been described byLiebers (1927), Haddenbrock (1950), Marchandet al. (1956), de Vries and Amir (1964), andKlinken-Rasmussen and Dyggve (1965). Diezel(1957), reinvestigating Haddenbrock's case andreporting another, demonstrated that the smallround bodies consisted predominantly of pro-tein with small amounts of glycolipid.
Seitelberger et al. (1967) defined this 'myo-clonic variant of amaurotic familial idiocy'when he reported eight patients, aged between2 and 10 years who presented with grand mal fitsand cerebellar ataxia followed by psychomotordeterioration, myoclonus, blindness with opticatrophy and retinitis pigmentosa, and whofinally died of dementia and cachexia. Theyshowed generalized neuronal lipid storage, withprotein type inclusion bodies in the cells of thethalamus, subthalamic nucleus, substantia nigra,dentate nucleus, inferior olive, and locus caeru-leus. It should be noted that these bodies arequite different from Lafora bodies, which con-sist of mucopolysaccharide in the form of poly-glucosans (Yokoi et al., 1968).Two patients with progressive myoclonic epi-
lepsy due to an underlying lipidosis do not fallinto the type described by Seitelberger et al.(1967). One, with features of amaurotic familialidiocy-namely, cherry red spots in the fundi,optic atrophy, and a family history of blindnessand death in infancy-also had cystic changes inradiographs of long bones, pathological frac-tures, and storage cells in the sternal bone mar-row which morphologically resembled Gauchercells. This patient developed generalized myo-clonus from the age of 10 years, grand malseizures at 23 years, and finally died at 31 yearsof age with minimal evidence of dementia(Glasgow, 1957; Halliday, 1967). The patientreported by Pallis et al. (1967) presented in thesixth decade with progressive cerebellar ataxia,intellectual deterioration, myoclonus and grandmal seizures and was clinically diagnosed asdyssynergia cerebellaris myoclonica. Neuronesthroughout the nervous system were heavilypigmented with lipofuscin and the authors sug-gested that diffuse lipofuscinosis should be con-sidered as another form of lipidosis.The following case report is of a 39 year old
man with a 22 year history of progressive myo-clonic epilepsy who was found to have histo-logical and biochemical evidence of Gaucher'sdisease.
CASE REPORT
M.S. (NHQS A406)2 This 39 year old single clerkwas admitted to the National Hospital in August1973 for investigation of intractable grand malseizures and myoclonus.He was born in South Africa of Jewish parents
who originated from Lithuania and who were firstcousins. There are two other unaffected siblings andno known family history of epilepsy or of anaemia.The patient himself was well until 17 years of agewhen he had a sudden episode of dizziness followedby brief loss of consciousness and generalized clonicmovements of his limbs. Thereafter, he continued tohave seizures at monthly intervals and in additiondeveloped shock-like jerking of his right arm, par-ticularly before seizures and in the early morning.At the time when the illness started he was study-
ing part-time for a degree in commerce which hepassed in 1956; however, in 1960 he failed to passhis final chartered accountancy examinations. In1961 he came to England as a senior assistant in afirm of accountants. In that year he was first seen atthe National Hospital and no abnormalities werenoted on examination and routine blood examina-tion; serology and skull radiographs were normal.He had had a normal pneumoencephalogram andcarotid angiogram in 1957 in South Africa. Hiselectroencephalogram was grossly abnormal withvery frequent paroxysms of generalized irregularmultiple spikes and waves. A diagnosis of idiopathicepilepsy was made and he was discharged on anti-convulsants.
His epilepsy remained reasonably well controlleduntil 1966 when, after an influenza-like illness, boththe seizures and myoclonic jerking increased in fre-quency. When next seen in 1968 he had been reducedto working as a ledger checker. Examination revealedslow deliberate speech broken up by jerks, typicalbrief irregular shock-like movements of his face andupper limbs with mild incoordination. His perform-ance IQ was 77 and verbal IQ 105 (WAIS) which wasfelt to indicate definite evidence of intellectual im-pairment, although subsequent psychometry hasshown no further change. Cerebral evoked responsesto electrical stimulation of either hand producedgrossly enlarged potentials with early surface posi-tive components of between 16 and 19 [±V from the2 This patient was presented at the meeting of the Royal Society ofMedicine held at the National Hospital on 5 December 1974.
850

Progressive myoclonic epilepsy due to Gaucher's disease in an adult
Left Fingers Right Fingers
I.........I.... I.... ........1.
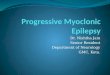
M.Si.30.6.69
FIG. 1 Cerebral evoked responses showing the grosslyenlargedpotentials recorded after contralateral stimu-lation of the hands.
right hemisphere and 11 to 13 ,uV from the lefthemisphere (Fig. 1). It was felt at this stage that thepatient had progressive myoclonic epilepsy.
In the next four years he had further admissionsfor adjustments to his anticonvulsant therapy but,despite trials of numerous drugs, his seizures con-
tinued to occur about once weekly.In 1973 his fits were entirely nocturnal and were
accompanied by urinary incontinence. Those ob-served in hospital were of sudden onset with rigidityof all four limbs and body followed by a clonic phaselasting several minutes. His major disability was hismyoclonic jerks which prevented him from writingand caused him to take an hour over dressing. Histreatment consisted of primidone, phenytoin sodium,sulthiame, nitrazepam, diazepam, and methylpheni-date.He had slow slurred speech with a mild nominal
dysphasia. His gait was normal, but for very markedmyoclonic jerking which involved his face, arms,and legs. The myoclonus was increased by voluntarymovement such as drinking from a cup or attemptingto adjust his spectacles, by sudden noises, lights,
tactile stimuli, and when his eyes were closed. Hisvisual acuity, fields, and fundi were normal but sac-cadic eye movements were slow in all directions (thiswill be reported separately). Muscle tone, power,reflexes, and sensation were normal but he hadfinger-nose and heel-shin ataxia which was thoughtto be mainly due to his myoclonus. His cardiovas-cular system, lungs, and abdomen were normal and,in particular, no spleen was palpable.
His electroencephalogram and cerebral evokedresponses were unchanged. Other investigationswere: haemoglobin 9.4 g/dl, sedimentation rate 7mm/h, white cell count 2400 mm-3, (neutrophils1 440mm- 3, lymphocytes 672 mm-3, monocytes 240mm- 3, eosinophils 24mm- 3), platelets 80 000mm - 3,serum iron 19.9 i±mol/l, iron binding capacity35.6 lumol/l (321 [±g/dl), faecal occult blood negative,serum vitamin B12 600 ng/l, serum folic acid6.0 t±g/l, and serum acid phosphatase 20 I.U./l(0-5). Radiological examination of long bones, skull,chest, and pelvis was normal. The sternal marrowwas hypocellular with normal erythropoiesis andgranulopoiesis but, in addition, large storage cellsresembling Gaucher cells were present (Fig. 2).Histochemical examination of the marrow con-firmed the numerous foamy cells which morpholo-gically resembled those seen in late onset GMIgangliosidosis or Gaucher's disease. The beta-galactosidase activity of peripheral blood leucocyteswas 205 nmol/mg protein/h (100-400) and beta-glucosidase activity of fibroblasts was 35 nmol/mgprotein/h (100-500), consistent with Gaucher'sdisease.
Since discharge the patient has been unable to keephis employment and it has been necessary to admithim to an institution with special facilities for epilep-tics. The recent introduction of clonazepam hasimproved the control of his myoclonic jerks and ithas been possible to reduce his other anticonvulsants.
Since Brady et al. (1965) demonstrated the de-ficiency of beta-glucosidase, the enzyme whichcleaves glucose from glucosyl ceramide (glucocere-broside), the diagnosis of Gaucher's disease hasrelied upon evidence of reduced enzyme activityrather than the finding of the typical Gaucher cell.The presence of the latter provides only a tentativediagnosis, as similar cells are found in GMI ganglio-sidosis where there is a deficiency of beta-galactosi-dase (Okada and O'Brien, 1968), and in chronicmyeloid leukaemia (Kattlove et al., 1969).
In the patient reported here, the storage cells in thebone marrow, the elevated serum acid phosphatase,normal beta-galactosidase, and deficient beta-glucosidase activity point to an unequivocal diag-nosis of Gaucher's disease. The absence of a palp-able spleen delayed diagnosis and is unusual,
851
,--,I
L,..L_..L&...L.~~~~~~,-...-I.

J. 0. King
FIG. 2 Sternal bone marrowwith a typical Gaucher cell.x 400.
although well recognized (Morgans, 1947; Maloneyand Cumings, 1960). The diagnosis of progressivemyoclonic epilepsy is justified on the grounds of theextensive myoclonus, and grand mal seizures and thegiant cerebral evoked potentials. The degree of in-tellectual deterioration is difficult to assess becauseof the effect of the anticonvulsant drugs and also theabsence of a formal assessment before the onset ofthe illness. If present it has been of only a milddegree in 20 years.
If one disregards the neurological features of thepresent case, the age of onset, prolonged survival,pancytopenia, and Ashkenazi Jewish origin suggestthat the patient is suffering from the chronic adultform ofGaucher's disease. However absenceofneuro-logical involvement is the sine qua non for classifica-tion in the adult or non-neuronopathic type ofGaucher's disease as opposed to the infantile formwhere neurological signs are the rule and deathoccurs under 2 years of age. There is a further smallgroup known as juvenile or subacute neuronopathicGaucher's disease where survival into the seconddecade is known. Frederickson and Sloan (1972) havereviewed 25 cases, 12 of whom were reported fromSweden by Hillborg (1959). The neurological featuresof this group were mental retardation, psychotic be-haviour disturbances, generalized rigidity, jerkymovements, epilepsy, and abnormal electroen-cephalograms. The jerky movements involved theeyes, mouth, and limbs, but were not described asmyoclonic in nature (Herrlin and Hillborg, 1962).The age of onset was in the first six months of lifewith survival up to 20 years, although six died in the
first three years. Of six studied in detail, five patientshad a pancytopenia and all had normal radiologicalexaminations before splenectomy.
Despite the absence of neurological signs, bydefinition, in adult Gaucher's disease, there havebeen several case reports of neurological involve-ment after the first decade (van Bogaert and Froh-lich, 1939; Davison, 1942). Miller et al. (1973)recently reported two siblings, aged 41 and 50 years,with histories of seizures for 12 and 15 years,respectively. Both patients had evidence of intellec-tual impairment and one had myoclonic jerks beforehis seizures. Both had supranuclear gaze pareses.The diagnosis of Gaucher's disease was establishedin both instances by the presence of Gaucher cells inthe spleen and bone marrow and evidence of deficientleucocyte beta-glucosidase activity. Although notingthat the neurological features of their patients re-sembled those seen in juvenile Gaucher's disease,they concluded that both had adult type Gaucher'sdisease. The subject of the present case reportappears to have a similar form of Gaucher's diseaseand all three cases suggest that, although rare, neuro-logical involvement in adult Gaucher's disease doesoccur. Neuropathological evidence of such isnecessarily limited. Davison's case, a 26 year oldPolish Jew with adult Gaucher's disease and facialimmobility, had swelling and loss of cells in the puta-men and caudate nuclei, slight swelling of Purkinjecells, and large foam cells in the spinal cord whenexamined histologically. Diezel (1955) has describedboth perivascular Gaucher cells and ganglion cellchanges in the cortex and cerebellum of a 61 year old
852

Progressive myoclonic epilepsy due to Gaucher's disease in an adult
man who apparently had adult Gaucher's disease.Gaucher cells have been reported in the pituitaryand hypothalamus (Teilum, 1944; Morrison andLane, 1955), spinal cord (Davison, 1942), andmeninges (Chang-lo et al., 1967).Even considering the pattern of involvement of
the nervous system in the infantile (Norman et al.,1956) and juvenile forms of Gaucher's disease (Bird,1948), there is no evidence of a specific pattern toaccount for the occurrence of progressive myoclonicepilepsy. The same can be said for the other lipidosesand Lafora body disease where the changes are sodiffuse. This contrasts with the frequent finding ofdentate and olivary atrophy in cases of the systemdegeneration type (Meyer, 1963).
Although the long term prognosis for the subjectof this case report must be poor, he has already sur-vived more than 20 years since his seizures began.His degree of intellectual impairment is mild and,provided that a drug is found which will control hisepilepsy and myoclonus without excessive side-effects, it is conceivable that he could return to someform of useful employment. The advent of clona-zepam has provided some hope in this direction andearly reports of its use in progressive myoclonicepilepsy are favourable (Laitinen and Toivakka,1973).
In the clinical context of a patient with persistentmyoclonus and epilepsy, Gaucher's disease must beconsidered among the lipidoses which cause this dis-order. Parental consanguinity, Ashkenazi Jewishorigins, and splenomegaly will suggest the diagnosisand an elevated serum acid phosphatase and Gauchercells in the sternal bone marrow are virtually diag-nostic. The demonstration of beta-glucosidase de-ficiency in fibroblasts is confirmatory.
I am grateful to Dr William Gooddy for permission toreport this case and to Dr A. M. Halliday for his interestand advice. He also measured the cerebral evoked re-sponses and supplied Fig. 1. Dr Patricia Norman suppliedFig. 2. Dr B. D. Lake kindly performed the histochemicalexamination of the bone marrow and Dr A. D. Patrickperformed the enzyme assays. The help of Dr Joseph M.Foley is also acknowledged.
REFERENCES
Bird, A. (1948). Lipidoses and central nervous system. Brain,71, 434-450.
van Bogaert, L., and Frohlich, A. (1939). Un cas de maladiede Gaucher de l'adulte avec syndrome de Raynaud, pig-mentation, et rigidite du type extrapyramidal aux membresinferieurs. Annales de MWdecine, 45, 57-70.
Brady, R. O., Kanfer, J. N., and Schapiro, D. (1965). Meta-bolism of glucocerebrosides. II. Evidence of an enzymaticdeficiency in Gaucher's disease. Biochemical and Bio-physical Research Communications, 18, 221-225.
Chang-lo, M., Yam, L. T., and Rubenstone, A. I. (1967).Gaucher's disease. Review of literature and report of 12
new cases. American Journal of Medical Science, 254, 303-315.
Davison, C. (1942). Disturbances in lipid metabolism and thecentral nervous system. Journal ofMount Sinai Hospital, 9,389-406.
Diezel, P. B. (1955). Histochemische Untersuchungen an denGloboidzellen der familiaren infantilen diffusen Sklerosevom Typus Krabbe. Virchowss Archiv, 327, 206-228.
Diezel, P. B. (1957). Die Stoffwechselstorungen der Sphingo-lipoide. In Monografien aus dem Gesamtgebiet der Neuro-logie und Psychiatrie, pp. 61-64.
Frederickson, D. S., and Sloan, H. R. (1972). Glucosylceramide lipidoses. In The Metabolic Basis of InheritedDisease. Edited by J. B. Stanbury, J. B. Wyngaarden, andD. S. Frederickson. McGraw-Hill: New York.
Glasgow, D. G. (1957). A case of amaurotic family idiocywith lipid storage disease of bone. Australasian Annals ofMedicine, 6, 295-299.
Haddenbrock, S. (1950). Zur Pathogenese systematischerBahndegeneration bei amaurotische Idiotie und zur Frageder Beziehung dieses Leidens zur Myoklonusepilepsie.Archivfur Psychiatrie und Nervenkrankheiten, 185, 129-164.
Halliday, A. M. (1966). The clinical incidence of myoclonus.In Modern Trends in Neurology, vol. 4. Edited by D.Williams. Butterworths: London.
Halliday, A. M. (1967). Cerebral evoked potentials in familialprogressive myoclonic epilepsy. Journal of the Royal Collegeof Physicians ofLondon, 1, 123-134.
Harriman, D. G. F., and Millar, J. H. D. (1955). Progressivemyoclonic epilepsy in 3 families: its clinical features andpathological basis. Brain, 78, 325-349.
Herrlin, K. M., and Hillborg, P. 0. (1962). Neurologicalsigns in a juvenile form of Gaucher's disease. Acta Paediat-rica Scandinavica, 51, 137-154.
Hillborg, P. 0. (1959). Morbus Gaucher i Norrbotten. Nor-disk Medicin, 61, 303-306.
Hodskins, M. B., and Yakovlev, P. 1. (1930). Anatomico-clinical observations on myoclonus in epileptics and onrelated symptom complexes. AmericanJournal ofPsychiatry,9, 827-848.
Hunt, J. R. (1921). Dyssynergia cerebellaris myoclonica,primary atrophy of the dentate system. Brain, 44, 490-538.
Kattlove, H. E., Williams, J. C., Gaynor, E., Spivack, M.,Bradley, R. M., and Brady, R. 0. (1969). Gaucher cells inchronic myeloid leukaemia: an acquired abnormality.Blood, 33, 379-390.
Klinken-Rasmussen, L., and Dyggve, H. V. (1965). A case oflate infantile amaurotic idiocy of the myoclonus type. ActaNeurologica Scandinavica, 41, 172-186.
Lafora, G. R., and Glueck, B. (1911). Beitrag zur Histo-pathologie der myoklonischen Epilepsie. Zeitschrift fur diegesamte Neurologie und Psychiatrie, 6, 1-14.
Laitinen, L., and Toivakka, E. (1973). Clonazepam (Ro 5-4023) in the treatment of myoclonus epilepsy. Acta Neuro-logica Scandinavica, 49, Suppl. 53, 72-76.
Liebers, M. (1927). Zur Histopathologie der amaurotischenIdiotie und Myoklonusepilepsie. Zeitschrift fur die gesamteNeurologie und Psychiatrie, III, 465-484.
Lundborg, H. (1903). Die progressive Myoklonus-Epilepsy(Unverricht's Myoklonie). Almqvist und Wiskell: Uppsala.
Lundborg, H. (1913). Medizinisch-Biologische Familienfor-schung innerhalb eines 2232-kdpfigen Bauerngeschlechtes inSchweden. Jena: Fischer.
Maloney, A. F. J., and Cumings, J. N. (1960). A case ofjuvenile Gaucher's disease with intraneuronal lipid storage.Journal of Neurology, Neurosuirgery, and Psychiatry, 23,207-2 13.
Marchand, L., Borel, J., Laroche, J., and Ganry, C. (1956).Idiotie infantile familiale de Tay-Sachs forme myoclono-epileptique chez deux freres. Encephale, 45, 1-40.
853

854 J. 0. King
Marinesco, G. (1925). Contribution a 1'etude anatomo-clinique et a la pathogenie de la forme tardive de l'idiotieamaurotique infantile. Bulletin de la Section Scientifique del'Academie Roumaine, 9, 1-27.
Matthews, W. B., Howell, D. A., and Stevens, D. L. (1969).Progressive myoclonus epilepsy without Lafora bodies.Journal of Neurology, Neurosurgery, and Psychiatry, 32,116-122.
Meyer, A. (1963). Epilepsy. In Greenfield's Neuropathology.Edited by W. Blackwood, W. H. McMenemy, A. Meyer,R. M. Norman, and D. S. Russell. Arnold: London.
Miller, J. D., McCluer, R., and Kanfer, J. N. (1973). Gau-cher's disease: Neurologic disorder in adult siblings. Annalsof Internal Medicine, 78, 883-887.
Morgans, M. F. (1947). Gaucher's disease without spleno-megaly. Lancet, 2, 576-577.
Morrison, A. N., and Lane, M. (1955). Gaucher's diseasewith ascites: a case report with autopsy findings. Annals ofInternal Medicine, 42, 1321-1329.
Norman, R. M., Urich, J., and Lloyd, 0. C. (1956). Theneuropathology of infantile Gaucher's disease. Journal ofPathology and Bacteriology, 72, 121-131.
Okada, S., and O'Brien, J. S. (1968). Generalised ganglio-sidosis, beta-galactosidase deficiency. Science, 160, 1002-1004.
Pallis, C. A., Duckett, S., and Pearse, A. G. E. (1967). Diffuselipofuscinosis of the central nervous system. Neurology(Minneap.), 17, 381-394.
Seitelberger, F., Jacob, H., and Schnabel, R. (1967). Themyoclonic variant of cerebral lipidoses. In Inborn Errors ofSphingolipid Metabolism. Edited by S. M. Aronson andB. W. Volk. Pergamon Press: Oxford.
Sjogren, T. (1931). Die juvenile amaurotische Idiotie.Hereditas, 14, 197-425.
Teilum, G. (1944). Die Gauchersche Krankheit. Acta MedicaScandinavica, 116, 170-190.
Unverricht, H. (1891). Die myoclonie, Leipzig und Wien:Denticke.
Unverricht, H. (1895). Ober familiare Myoclonie. DeutscheZeitschrift fur Nervenheilkunde, 7, 32-67.
de Vries, E., and Amir, A. P. (1964). An atrophic type ofamaurotic idiocy. Report of two cases. Psychiatria, Neuro-logia, Neurochirurgia, 67, 231-242.
Yokoi, S., Austen, J., Witmer, F., and Sakai, M. (1968).Studies in myoclonus epilepsy (Lafora body form). Archivesof Neurology (Chic.), 19, 15-33.
Zeman, W. (1974). Studies in the neuronal ceroid lipo-fuscinoses. Journal of Neuropathology and ExperimentalNeurology, 33, 1-12.