Embed Size (px)
DESCRIPTION
Poster presentation at the society of general internal medicine (SGIM) meeting.
Citation preview

1. Understanding the differences between progressive supranuclear paly (PSP) and parkinson disease (PD).
2- Recognizing the movement disorder patterns in PSP.
A 71 y/o woman with downward gaze palsy, dementia, and recurrent falls Kam Newman, Hesam Tabrizi, Parham Naghedechi, Kia Javaheri, Saeed Kahkeshani
San Jacinto Methodist Hospital, Baytown, TX
Learning Objectives Case History
The patient is a 71 year old Caucasian female with past history of walking problem and dementia who was admitted hospital for altered mental status. Her problems started with recurrent falls and the ability to walk gradually declined to the point that she stopped walking completely about 5 to 6 month ago and she had to use wheel chair. She has been declining in her mental function since a couple of years ago, and was treating for Alzheimer disease for about a year. According to her family, she has also been using diapers for several months. Also they have noticed that during the past several month, her arms became stiff and fingers flexed so that she could not open her fist. On physical exam, patient stares at the examiner all the time and is not communicative. She recognizes some family members around her, but completely disoriented to the place and time, and follows just some simple commands like squeezing fingers. Her speech is slow and somewhat slurred. She has a very poor eye movement in all directions. In motor exam, she is rigid in a generalized fashion, and her rigidity was seen in all extremities and trunk. She holds her right hand in a completely flexed position. Deep tendon reflexes are exaggerated in all four extremities. CBC, CMP, cardiac profile, LFT, SPEP, RPR, CEA, and spinal tap all were unremarkable. MRI of the brain revealed atrophy of the midbrain.
Discussion
Acknowledgements
The authors wish to thank Dr. Hamid Iranmanesh, and Dr. Kaveh Bahmanpour, Department of Family Medicine for their support.
Summary
Olszewski, Steele, and Richardson reviewed autopsied of patients who had a syndrome of pseudobulbar palsy, supranuclear ocular palsy, extrapyramidal rigidity, gait ataxia, and dementia.They found a consistent pattern of neuronal degeneration and neurofiblliray tangles, chiefly affecting the pons and midbrain. It is clear that PSP continues to be an under-recognized disorder with multilevel involvement of the neuraxis that helps differentiate it from other akinetic-rigid syndromes such as PD. After PD, PSP is the most common form of Parkinsonism with a prevalence of 10% of that of PD. It is an increasingly recognized akinetic-rigid syndrome with features that may initially mimic those of idiopathic PD. The clinical hallmarks of PSP are vertical gaze palsy, psudobulbar palsy, axial rigidity, and cognitive impairment.
Oculocephalic maneuver demonstrates intact reflex downgaze in a patient unable to look down voluntarily.
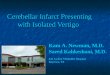
New radiologic sign for the diagnosis of PSP. Midsagittal MR image of a patient with PD (A) does not show any apparent abnormality, while that’s of apatient with PSP (B) shows marked atrophy of midbrain tegmentum, and a patient with multiple-system atrophy of the Parkinson type (MSA-P) shows marked atrophy of pons (C). The midbrain to pons ratio is always small in the patients with PSP. In pts with PSP, the shapes of midbrain tegmentum (bird’s head) and pons (bird’s body) on midsagittal MR images look like a lateral view of a standing penguin (especially the king penguin) with a small head and big body. Recognition of this penguin silhouette sign should strongly raise suspicion for the diagnosis of PSP.
Patients with PSP have an akinetic rigid Parkinson-like syndrome, rest tremor is uncommon. Thesymptoms consist of bradykinasia, decreased finemotor skills, and hypophonia. Gait difficulties progress faster than in PD. Unlike typical PD, falls begin within the first year. Presentation can range from unexpected falls, to visual (blurry or double vision), cognitive (apathy, dementia), or Parkinsonian symptoms with little or no tremor. Compared with PD, PSP patients have more axial than appendicular rigidity, more dystonia and a more symmetric exam. Weak voice with psudobulbar features can develop early; swallowing problem develop later. Downgaze isaffected before upgaze, whereas lateral movementsof eye are usually preserved. Motor examinationreveals axial hypertonia that is out of proportion to limb tone, which may be normal in contrast to PD Patients. Eyelid opening and closing aparaxias are far more common in PSP than in any other extrapyramidal disorder. “Applause sign” helps to discriminate PSP from FTD and PD. Pseudobulbarpalsy is an important symptom of PSP associateed with high morbidity and decreased survival.The pathology of PSP is characterized by widespread neurodegeneration associated with tau protein deposition in subcortical regions that include the SN, globus pallidus, subthalamic nucleus, midbrain, pontine reticular formation, dentate nucleus of the cerebellum and the superior cerebellar peduncle.Compared with PD, PSP pts drive a limited benefit from dopaminomimetics; nonethless in individual patients this benefit can be clinically important. Beyond dopamine, GABA receptors seem to be decreased in the frontal cortex of PSP patients.
Reference:1. Clinical aspects of progressive supranuclear palsy. Handb of Clin Neurol. 2008; 89:461-73.
Images