Embed Size (px)
Citation preview

Skeletal Radiol (1994) 23:411-419
Skeletal Radiology
Articles
Progressive pseudorheumatoid chondrodysplasia: a report of nine cases in three families Hossien Rezai-Delui, M.D. 1, Gholamali Mamoori, M.D. 2, Eqbal Sadri-Mahvelati, M.D. 3, Nor Mohammad Noori, M.D. 2
1 Department of Radiology, Mashad University, Ghaen Hospital, Mashad, Iran 2 Department of Pediatrics, Mashad University, Ghaen Hospital, Mashad, Iran 3 Department of Orthopedics, Mashad University, Ghaen Hospital, Mashad, Iran
Abstract. Nine cases of p rogress ive p seudorheuma to id chondrodysp l a s i a in subjects aged 7 - 6 0 years are repor t - ed. Six o f them were member s o f one large fami ly with several consangu ineous marr iages . Evalua t ion of six genera t ions of this f ami ly sugges ted an au tosomal reces- sive m o d e o f inher i tance. The presen ta t ion o f the d isease was be tween the ages o f 3 and 8 years wi th wadd l ing gai t and fus i fo rm swel l ing o f the in te rpha langea l jo in ts o f the hands, c l in ica l ly r e sembl ing juven i l e rheumato id arthritis. M o s t o f the other jo in t s b e c o m e progress ive ly involved, wi th c r ipp l ing disabi l i ty . One o f the pat ients had typica l features of Blount d i sease at presenta t ion .
Key words: Progress ive p seudo rheuma to id chondrodys - p las ia - A u t o s o m a l recess ive - Juveni le rheumato id arthrit is
A progress ive chondrodysp l a s i a r e sembl ing rheumato id arthrit is was first desc r ibed in three unre la ted pat ients by Spranger et al. in 1980 [1]. Since then several addi t iona l cases have been repor ted [2-10] , thus def in ing the cl ini- cal features, roen tgenograph ic character is t ics , and genet- ic pat tern, and d i s t inguish ing the d i sorder f rom other o s t eochondrodysp la s i a s or connect ive t issue diseases.
In this repor t we present nine pat ients wi th this dis- ease, aged f rom 7 to 60 years . Six were m e m b e r s o f one large fami ly with several consangu ineous marr iages , sugges t ing that the mode o f inher i tance was th rough an au tosomal recess ive gene.
Case histories
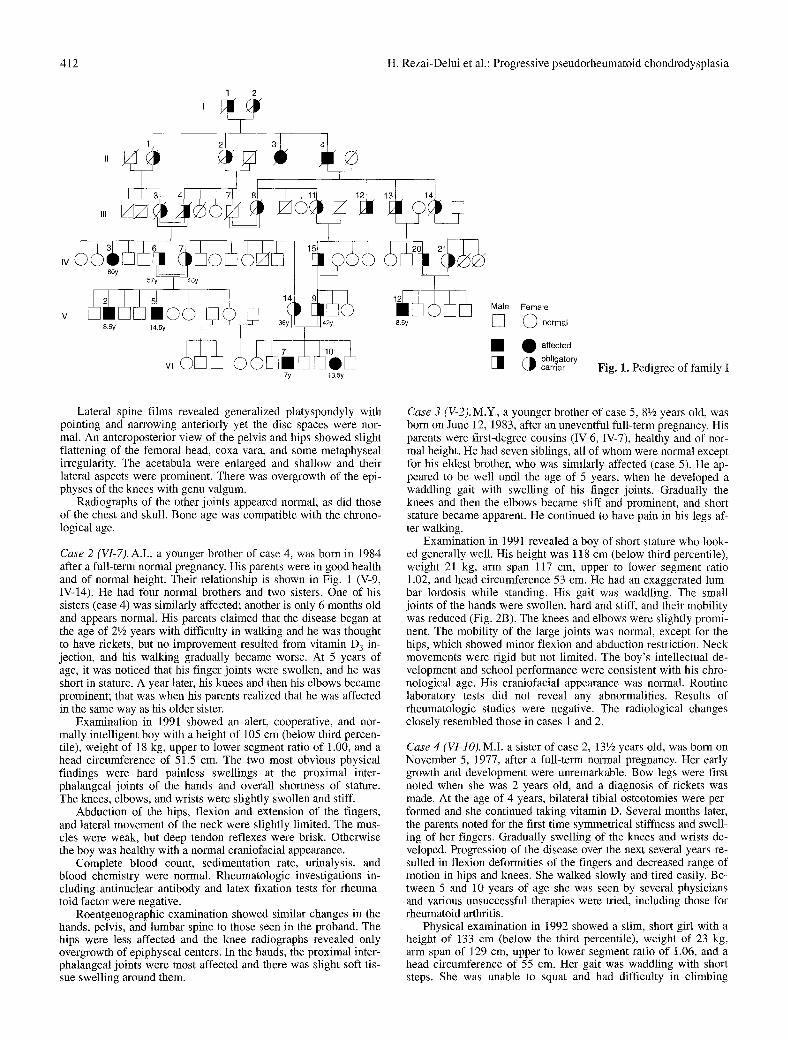
Family I (Fig. 1)
All affected members of this family (except those who were de- ceased), and many other apparently unaffected members, especial- ly younger children, were examined and pertinent radiographs
Correspondence to: Hossien Rezai-Delui M.D., Salman Farsi Street 135, Mehad, Iran
were obtained; previous radiographs and hospital files were studied. Six living family members were diagnosed as having this disease. Questioning of older members revealed that the patriarch (1I-4) of the most affected descendants had been a short man with multiple deformities of the joints; in addition he had one crippled sister [II-3) similar to case 6. They were apparently the first homozy- gotes of this family.
Case 1 (proband). A.D. an 81/2 year-old boy, was born on May 20, 1982, by cesarean section, because his mother had had prior sec- tions. His parents were first-degree cousins, both well and of nor- mal height. The patient had four siblings aged 6 months to 10 years; all are clinically normal at the present time. He appeared normal until aged 3 years, when he developed genu varum and bowing of the legs. On the basis of clinical and radiological fea- tures, a diagnosis of Blount disease was made, and correction by tibial osteotomy was carried out. At 5 years of age he was re-as- sessed because he had a waddling gait, swollen fingers, and was shorter than boys of the same age. A presumptive diagnosis of ju- venile rheumatoid arthritis was made, but no drug treatment was administered. The disease had an unremitting course, and in recent years he has had more difficulty in walking, fatigues easily, and has pain in his hips and legs.
Physical examination in 1991 showed a pleasant, cooperative, intelligent boy with a height of 113 cm (below third percentile), weight of 22.5 kg, upper to lower segment ratio of 1.10, and a head circumference of 53 cm. All his finger joints (Fig. 2A) were swollen and hard, but not tender or warm. The knees, wrists, el- bows, and ankles were stiff and slightly prominent, but had a nor- mal range of motion. The mobility of the hips and the fingers was moderately reduced. Lateral movement of the neck apeared to be within normal limits, but the boy could not flex his spine fully. The scars of the earlier operations were seen on the legs. There was genu valgum which had developed after his operation. The re- mainder of the findings from the physical and neurological exam- ination were consistently unremarkable.
Laboratory studies included complete blood count, urinalysis, serum alkaline phosphatase, phosphorus, calcium, and determina- tion of serum proteins; all were normal. Repeated serological tests for rheumatoid arthritis were negative.
Initial radiographs made for tibia vara at 3 years of age showed the typical features of Blount disease. Serial radiographs of the hands taken at various ages demonstrated firstly periarticular soft tissue swelling around the proximal interphalangeal joints; subsequently, there was overgrowth of the articular ends of the bones of all interphalangeal joints, most marked in proximal ones. Other findings were enlargement of the metacarpal heads, and peri articular osteoporosis.
�9 1994 International Skeletal Society
412 H. Rezai-Delui et al.: Progressive pseudorheumatoid chondrodysplasia
1 2
7y 13.5y
8.5y
Male Female
0 norrna'
�9 0 affected [ ] ob,,ga,o
carrier Fig. 1. Pedigree of family I
Lateral spine films revealed generalized platyspondyly with pointing and narrowing anteriorly yet the disc spaces were nor- mal. An anteroposterior view of the pelvis and hips showed slight flattening of the femoral head, coxa vara, and some metaphyseal irregularity. The acetabula were enlarged and shallow and their lateral aspects were prominent. There was overgrowth of the epi- physes of the knees with genu valgum.
Radiographs of the other joints appeared normal, as did those of the chest and skull. Bone age was compatible with the chrono- logical age.
Case 2 (VI-7). A.I., a younger brother of case 4, was born in 1984 after a full-term normal pregnancy. His parents were in good health and of normal height. Their relationship is shown in Fig. 1 (V-9, IV-14). He had four normal brothers and two sisters. One of his sisters (case 4) was similarly affected; another is only 6 months old and appears normal. His parents claimed that the disease began at the age of 21/2 years with difficulty in walking and he was thought to have rickets, but no improvement resulted from vitamin D 3 in- jection, and his walking gradually became worse. At 5 years of age, it was noticed that his finger joints were swollen, and he was short in stature. A year later, his knees and then his elbows became prominent; that was when his parents realized that he was affected in the same way as his older sister.
Examination in 1991 showed an alert, cooperative, and nor- mally intelligent boy with a height of 105 cm (below third percen- tile), weight of 18 kg, upper to lower segment ratio of 1.00, and a head circumference of 51.5 cm. The two most obvious physical findings were hard painless swellings at the proximal inter- phalangeal joints of the hands and overall shortness of stature. The knees, elbows, and wrists were slightly swollen and stiff.
Abduction of the hips, flexion and extension of the fingers, and lateral movement of the neck were slightly limited. The mus- cles were weak, but deep tendon reflexes were brisk. Otherwise the boy was healthy with a normal craniofacial appearance.
Complete blood count, sedimentation rate, urinalysis, and blood chemistry were normal. Rheumatologic investigations in- cluding antinuclear antibody and latex fixation tests for rheuma- toid factor were negative.
Roentgenographic examination showed similar changes in the hands, pelvis, and lumbar spine to those seen in the proband. The hips were less affected and the knee radiographs revealed only overgrowth of epiphyseal centers. In the hands, the proximal inter- phalangeal joints were most affected and there was slight soft tis- sue swelling around them.
Case 3 (V-2).M.Y., a younger brother of case 5, 81/2 years old, was born on June 12, 1983, after an uneventful full-term pregnancy. His parents were first-degree cousins (IV-6, IV-7), healthy and of nor- mal height. He had seven siblings, all of whom were normal except for his eldest brother, who was similarly affected (case 5). He ap- peared to be well until the age of 5 years, when he developed a waddling gait with swelling of his finger joints. Gradually the knees and then the elbows became stiff and prominent, and short stature became apparent. He continued to have pain in his legs af- ter walking.
Examination in 1991 revealed a boy of short stature who look- ed generally well. His height was 118 cm (below third percentile), weight 21 kg, arm span 117 cm, upper to lower segment ratio 1.02, and head circumference 53 cm. He had an exaggerated lum- bar lordosis while standing. His gait was waddling. The small joints of the hands were swollen, hard and stiff, and their mobility was reduced (Fig. 2B). The knees and elbows were slightly promi- nent. The mobility of the large joints was normal, except for the hips, which showed minor flexion and abduction restriction. Neck movements were rigid but not limited. The boy's intellectual de- velopment and school performance were consistent with his chro- nological age. His craniofacial appearance was normal. Routine laboratory tests did not reveal any abnormalities. Results of rheumatologic studies were negative. The radiological changes closely resembled those in cases 1 and 2.
Case 4 (VI-IO).M.I. a sister of case 2, 131/2 years old, was born on November 5, 1977, after a full-term normal pregnancy. Her early growth and development were unremarkable. Bow legs were first noted when she was 2 years old, and a diagnosis of rickets was made. At the age of 4 years, bilateral tibial osteotomies were per- formed and she continued taking vitamin D. Several months later, the parents noted for the first time symmetrical stiffness and swell- ing of her fingers. Gradually swelling of the knees and wrists de- veloped. Progression of the disease over the next several years re- sulted in flexion deformities of the fingers and decreased range of motion in hips and knees. She walked slowly and tired easily. Be- tween 5 and 10 years of age she was seen by several physicians and various unsuccessful therapies were tried, including those for rheumatoid arthritis,
Physical examination in 1992 showed a slim, short girl with a height of 133 cm (below the third percentile), weight of 23 kg, arm span of 129 cm, upper to lower segment ratio of 1.06, and a head circumference of 55 cm. Her gait was waddling with short steps. She was unable to squat and had difficulty in climbing

H. Rezai-Delui et al.: Progressive pseudorheumatoid chondrodysplasia 413
stairs. The knees, elbows, wrists, ankles, and all small joints of the hands were prominent and showed various degrees of limited mo- tion. There was stiffness in the small joints of the hands, resulting in inability to form a fist (Fig. 2C). The mobility of the hips was markedly restricted. Lateral movement of the neck as well as flex- ion and extension were limited. Her general health remained good, and in spite of her disabilities she was enrolled in school and was performing satisfactorily. She was not yet menstruating, although a moderate amount of pubic hair and breast development had appeared.
Routine laboratory studies showed no abnormalities, and re- peated screening tests for rheumatoid arthritis were negative.
On radiographic examination, the skull was essentially unaf- fected. Lateral spine films revealed generalized platyspondyly, more marked in the lumbar region, associated with central beaks and disc space narrowing (Fig. 5A).
Pelvic and hip radiographs showed dysplastic acetabula, wid- ened femoral heads and necks, osteoporosis, joint space narrow- ing, and secondary degenerative changes. The lateral aspect of each acetabulum was prominent, and the iliac wings appeared flat and small (Fig. 6B). Hand films disclosed overgrowth of the artic- ular ends of the bones of metacarpophalangeal joints and all inter- phalangeal joints. In addition the carpal bones were enlarged and became irregular (Fig. 7B). Osteoporosis was present, most prom- inently around joints. An anteroposterior view of the knees dem- onstrated generalized demineralization, loss of joint space, and ir- regularity of the articular surfaces. There was overgrowth of epi- physes and widening of the intercondylar notch (Fig. 9B). In the elbows and ankles, the articular ends of the bones were also en- larged, joint spaces became narrow, and there was periarticular osteoporosis. The small joints of the foot and shoulder appeared to be uninvolved.
Case 5 (V-5). A.Y. was born on July 27, 1976. Pregnancy and de- livery were normal. He is the elder brother of Case 3. He was well until 5 years of age, when parents first noticed his limp and swol- len fingers. Throughout his childhood his condition gradually be- came worse. At 7 years of age he walked slowly and could not climb stairs without using the banister. He was shorter than boys of the same age and had pain in his legs. In late childhood, most of his major joints were prominent, and generalized symmetrical muscle atrophy was present. He was assessed on several occasions; on one of these a diagnosis of atypical juvenile rheumatoid arthritis was made and he was given aspirin and cortisone, but both drugs were discontinued after approximately t year because no benefit was apparent. In recent years he has complained of vague pain in the left flank and radiographic examination has shown left renal calculi.
On examination he was a curious, slim, short boy 129 cm in height (below the third percentile), with an arm span of 128 cm, weight 28 kg, upper to lower segment ratio 1.01, and head circum- ference 54.5 cm. He had an exaggerated lumbar lordosis while standing and a short step on walking. The ribs showed a "rosary" at the costochondral junctions. The joints of the hands were swol- len and stiff and held in flexion deformity. He was not able to make a full fist. Most major joints were prominent, but motion was limited only in hips, elbows, and wrists. The right foot was out-turned. The neck appeared short and its lateral movement was reduced by 20~176 flexion and extension of the spine were also restricted.
Results of blood studies were normal, including complete blood count, sedimentation rate, glucose, blood urea nitrogen, creatinine, total protein, cholesterol, alkaline phosphatase, calcium, phosphorus, and serum parathyroid hormone concentration. Urinal- ysis revealed mildly increased 24-h calcium excretion. Findings from repeated blood tests for rheumatoid arthritis were negative.
Radiographic changes of the joints, spine, and pelvis resem- bled those of case 4. There was marked overgrowth of the epiphy- ses and metaphyses at the knees, elbows (Fig. 10) and small joints of the hands. The hips were more involved and showed cystic
changes in acetabular and femoral sites. A plain film of the abdo- men (Fig. 4), an intravenous pyelogram, and ultrasonographic studies disclosed a staghorn calculus, with mild hydronephrosis of the left kidney.
Case 6 (IV-3).M.Y., the paternal aunt of cases 3 and 5, was born in 1931. Her parents were first-degree maternal consins (III-3, III-4) who had been of normal height. Her younger five living siblings were apparently healthy. She could only remember developing a waddling gait and swollen joints when she was in her early teens. The mobility of her joints became steadily reduced and she devel- oped flexion contractures of the knees, hips, elbows, and ankles, as well as of the small joints of the hands and feet. The degree of the deformities at 30 years of age was such that she was unable to stand or walk. Over the following years she was confined to a wheelchair (Fig. 3).
On examination she was a pleasant, slightly obese woman with multiple contractures. Her measured height was 136 cm, upper to lower segment ratio 0.81, and weight 65 kg. Her most disabling deformity was contracture of the lower extremities. She moved around on the floor with her hips and knees flexed, supporting herself with her hands. Most of her joints were swollen and stiff and associated with various degrees of flexion deformities. The hips were mobile, but she had a fixed flexion deformity of 40 ~ which could be extended passively to 90 ~ . The knees were swol- len, and showed flexion contractures of about 60 ~ The shoulders could be abducted to 90 ~ and had a considerable limitation of ro- tation. The metacarpophalangeal joints and all interdigital joints were prominent and showed flexion contractures. Mobility of the wrists, ankles, and elbows was markedly reduced. Motion of the spine was limited in all planes and there was moderate lumbar scoliosis. She denied having pain in most affected joints.
Results of complete blood count, urinalysis, and blood chemis- try studies were normal. Blood tests for rheumatoid arthritis were negative. A skeletal survey displayed involvement of most joints, only the pubis, sacroiliac, temporomandibular costovertebral, and acromioclavicular joints were apparently unaffected. The main ra- diographic features were enlarged epiphyses and metaphyses, joint space narrowing, and osteoporosis. There were secondary osteoarthritic changes with flexion contractures; hips and knees were the most affected. The femoral head and neck formed a sin- gle mass and appeared not to fit the shallow acetabulum. The iliac bones were flat and broad at their base. Because of the severe flexion deformity of the knees, an anteroposterior view of them could not be obtained; lateral films showed marked joint space narrowing in all compartments, as well as osteoporosis and over- growth of the epiphyses. Radiographs of the shoulders showed flattening of the humeral head with a decreased glenohumeral joint space (Fig. 12). Other major joints were also affected (Fig. 11). As in the other previously described cases, the appearance of radiographs of the hands was characteristic (Fig. 7D). Both feet were involved in a similar manner to the hands; metatarsal heads were enlarged and articular ends of the interphalangeal joints were expanded (Fig. 8).
There was marked platyspondyly with extensive irregularity of upper and lower borders of the vertebrae. Moderate scoliosis had developed in the thoracolumbar region. In spite of severe joint space narrowing and flexion contractures, no apparent bony an- kylosis had developed.
Family H
M.Ch., the patient, and her normal brother were the products of an uncle-niece marriage. Because this family was from a rural area, we were not able to examine all its members, including some who were said to have similar joint features. The son of the patient's paternal uncle had two crippled children. Examination of these showed that the disease was osteogenesis imperfecta tarda.

414 H. Rezai-Delui et al.: Progressive pseudorheumatoid chondrodysplasia
Case 7. M.Ch., 18 years old, was born on November 3, 1973, at term. Her parents were first-degree cousins and of normal height. She had only one sibling, an elder brother who was healthy. The patient was well until she reached 3 years of age, when she devel- oped bow legs with a waddling gait. The diagnosis at that time was rickets. After 2 or 3 years, her finger joints and knees became swollen, and she walked with difficulty. On further evaluation, a misdiagnosis of juvenile rheumatoid arthritis was made and she was given salicylates. However, her condition became worse: pro- gressive flexion deformity of her hips and knees developed throughout her adolescence to the point that she was no longer ca- pable of standing or walking without the aid of a stick. Despite the disability she graduated from high school last year.
On examination she was cooperative but slightly depressed; height was 134 cm, weight 35 kg, arm span 127 cm, and upper to lower segment ratio 0.93. She was not able to stand without sup- port, and walked slowly with the aid of crutches. All her major joints were prominent, as well as the small joints of the hands and feet. There was marked flexion deformity in the hips, knees, and fingers, with limited motion. The range of movement of the el- bows, ankles, shoulders, and small joints of the feet was also re- duced. The neck was stiff. Mobility of the spine was limited in all planes. She had a thoracolumbar kyphosis with moderate scolio- sis. Her muscles appeared to be atrophic, but the limb reflexes were brisk. She complained of pain and easy fatigability after walking a short distance with the aid of crutches. Examination of the other systems showed no abnormalities. Routine blood tests and urinalysis were normal. Screening blood tests for rheumatoid arthritis were negative.
Radiographs showed similar changes to cases 5 and 6 (Fig. 7C). In the spine, kyphoscoliosis and marked platyspondyly were present. There was more irregularity in the lower and upper bor- ders of thoracic vertebrae (Fig. 5B). Osteoporosis and joint space narrowing were noticeable in most affected joints. The pelvis was dysplastic as in the other cases. The femoral heads were large and flattened.
Family III
In this family there were two affected siblings. The parents, a 27- year-old mother and 32-year-old father, were healthy and of nor- mal height, but were first cousins. They had five children, one boy and four girls. The unaffected children were all younger and ap- peared to be normal at the time of examination. Family members interviewed had no knowledge of other consanguineous marriag- es, nor of other affected cases.
Case 8. H.A., 12 years old, was born on July 27, 1980, after a nor- mal first pregnancy and delivery. His mother stated that he had a prolonged illness with fever and rash at 3 years of age and recov- ered completely. After that he was well, although he appeared to be shorter than his peers. At 8 years of age it was noticed that he had an abnormal gait and his fingers were swollen. Soon thereafter his knees and elbows became prominent. During the initial medical evaluation, a diagnosis of juvenile rheumatoid arthritis was made, but treatment with various anti-inflammatory agents did not pro- vide significant benefit.
Physical examination in 1992 showed a boy of short stature with a normal appearance; height was 133 cm (below the third percentile), weight 36 kg, arm span 130 cm, upper to lower seg- ment ratio 0.80, and head circumference 54 cm. His gait was wad- dling, and there was a lumbar lordosis when he stood. The knees, wrists, and elbows were slightly prominent. There was a de- creased range of motion of the hips, but mobility of the other ma- jor joints was within normal limits. Fusiform swelling was seen in all finger joints, most marked in the proximal ones. Flexion and extension of these small joints were slightly limited. The affected joints were hard on palpation, but there was no heat or erythema. Physical examination revealed no significant restriction of motion
of the spine. The remainder of the findings from the physical and neurological examinations were consistently unremarkable.
Results of the following routine tests were normal: complete blood count, calcium, phosphorus, serum alkaline phosphatase, creatinine, sedimentation rate, antinuclear antibody, latex fixation for rheumatoid factor, and serum IgG, IgM, and IgA.
The radiographic changes were identical to those in cases 2 and 3. The skull was normal. There was platyspondyly with rounded upper and lower margins of the vertebral bodies and ante- rior tonguing. The epiphyses of the knees (Fig. 9A) and hips were slightly enlarged and the acetabular roof was irregular. The pelvis was mildly dysplastic. Bone age was within normal limits.
Case 9. S.A., 8 years old, the younger sister of case 8, was born on August 15, 1984, after a term pregnancy. She had a healthy infan- cy. In early childhood, she was an active girl, but her short stature was of continuing concern to the parents. More recently, she was noted to have waddling gait, and her finger joints were swollen.
Examination in 1992 disclosed a pleasant, short girl who look- ed generally well. Her height was 109 cm, weight 18.5 kg, arm span 110 cm, upper to lower segment ratio 0.87, and head circum- ference 52 cm. The only significant physical finding was fusiform swelling of the proximal interphalangeal joints of the hands. The affected joints were hard, but not tender or warm. Her gait was waddling. There was increased lumbar lordosis when she was standing.
The range of motion of all major joints was within normal lim- its, including hips, knees, elbows, wrists, and ankles. The neck movement appeared stiff, but the range of motion was not restrict- ed. She was an intelligent girl with a normal craniofacial appear- ance. The other findings of the physical examination were unre- markable.
Routine laboratory examination yielded normal results and screening blood tests for antinuclear antibodies and lupus erythe- matosus (LE) cells. Radiographic changes resembled those of case 2 (Fig. 6A). In the hands, there was soft tissue swelling around the proximal interphalangeal joints, but overgrowth of the articular ends of the bones was less striking (Fig. 7A).
Features of progressive pseudorheumatoid ehondrodysplasia
Clinical features
Seven of the patients were under 15 years of age and two were adults. All were normal at birth and during infancy. In three patients the disease first manifes ted at the age of 2 or 3 years with bow leg deformity that required surgi- cal correction. Of part icular interest in one of them (case 1), were typical features of Blount disease. Al though Vi- tamin D deficiency rickets is a pediatric problem in Iran, the parents denied such deformity in their other children. Two or 3 years later, these patients all showed swell ing of the small joints of the hands, as in the other cases.
In the other patients (six cases) the disease began be- tween the ages of 5 and 8 years with waddl ing gait and painless symmetr ical swell ing of proximal inter- phalangeal joints , and then the knees, elbows, wrists, and distal joints of the fingers became prominent (Fig. 2). The affected joints were hard, but no signs of fluid, redness, or warmth were seen.
Most chi ldren had mildly exaggerated lumbar lordo- sis on standing and restricted mot ion of the hips and spine with decreased muscle mass, but the nervous sys- tem was intact. The most disabl ing features were f lexion
H. Rezai-Delui et al.: Progressive pseudorheumatoid chondrodysplasia 415
deformities and limitation of motion, especially in the lower extermities, which ultimately led to crippling. In our oldest patient (case 6, 60 years; Fig. 3), nearly all movable joints were affected. All of the patients have been investigated for juvenile rheumatoid arthritis, and six have been treated with anti-inflammatory drugs with neither improvement nor prevention or slowing of pro- gression.
Short stature was a constant sign. All children were below the third percentile for size but appeared to be proportionate. The final height in one of the adult pa- tients (case 7) was 134 cm; some of the reduction in height was due to flexion deformity and kyphoscoliosis.
Life span seems not to be affected. Our oldest patient was 60 years old, and apart from joint disorders was healthy. Other patients had no extraskeletal disease, ex- cept the patient in case 5 who had renal calculi (Fig. 4). In all patients routine laboratory studies yielded normal findings, in particular serum calcium, phosphorus, and alkaline phosphatase. Repeated screening for rheumatoid arthritis, including rheumatoid factor, antinuclear anti- bodies, and sedimentation rate, was consistantly nega- tive. All patients tested negative for HLA B27, and there was no excessive excretion of mucopolysaccharides in those who were examined.
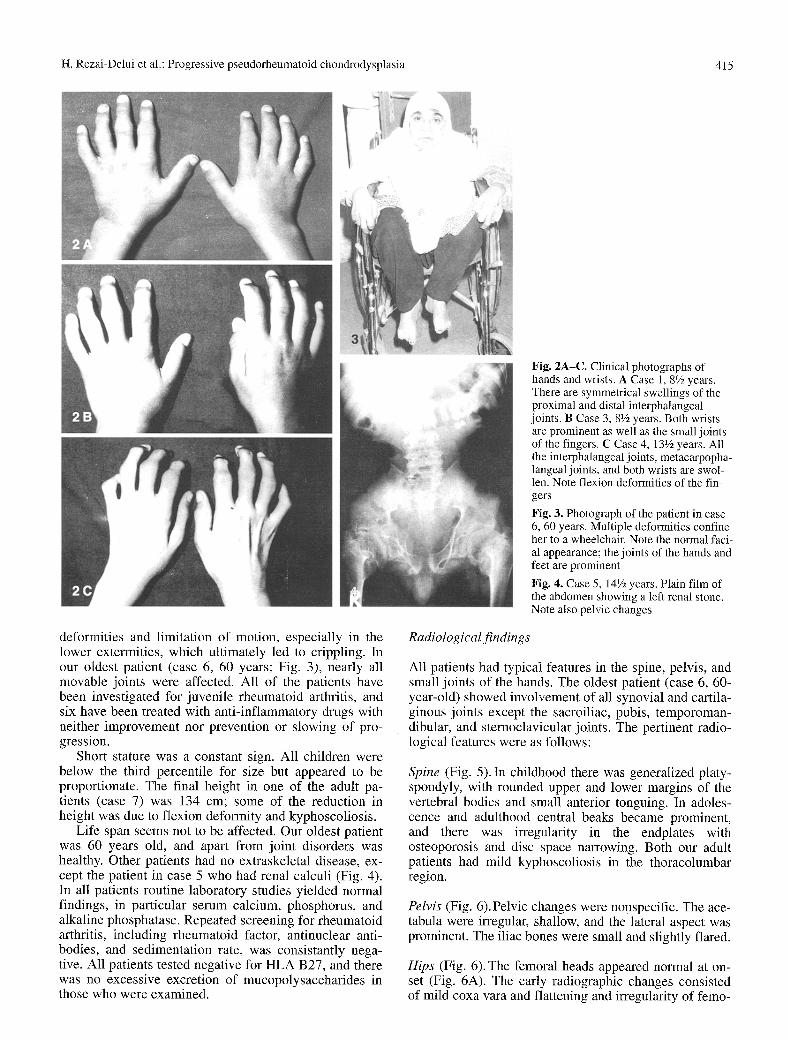
Fig. 2A-C. Clinical photographs of hands and wrists. A Case 1, 81/2 years. There are symmetrical swellings of the proximal and distal interphalangeal joints. B Case 3, 8V2 years. Both wrists are prominent as well as the small joints of the fingers. C Case 4, 131/2 years. All the interphalangeal joints, metacarpopha- langeal joints, and both wrists are swol- len. Note flexion deformities of the fin- gers
Fig. 3. Photograph of the patient in case 6, 60 years. Multiple deformities confine her to a wheelchair. Note the normal faci- al appearance; the joints of the hands and feet are prominent
Fig. 4. Case 5, 14Vz years. Plain film of the abdomen showing a left renal stone. Note also pelvic changes
Radiological findings
All patients had typical features in the spine, pelvis, and small joints of the hands. The oldest patient (case 6, 60- year-old) showed involvement of all synovial and cartila- ginous joints except the sacroiliac, pubis, temporoman- dibular, and sternoclavicular joints. The pertinent radio- logical features were as follows:
Spine (Fig. 5). In childhood there was generalized platy- spondyly, with rounded upper and lower margins of the vertebral bodies and small anterior tonguing. In adoles- cence and adulthood central beaks became prominent, and there was irregularity in the endplates with osteoporosis and disc space narrowing. Both our adult patients had mild kyphoscoliosis in the thoracolumbar region.
Pelvis (Fig. 6).Pelvic changes were no,nspecific. The ace- tabula were irregular, shallow, and the lateral aspect was prominent. The iliac bones were small and slightly flared.
Hips (Fig. 6). The femoral heads appeared normal at on- set (Fig. 6A). The early radiographic changes consisted of mild coxa vara and flattening and irregularity of femo-
416 H. Rezai-Delui et al.: Progressive pseudorheumatoid chondrodysplasia
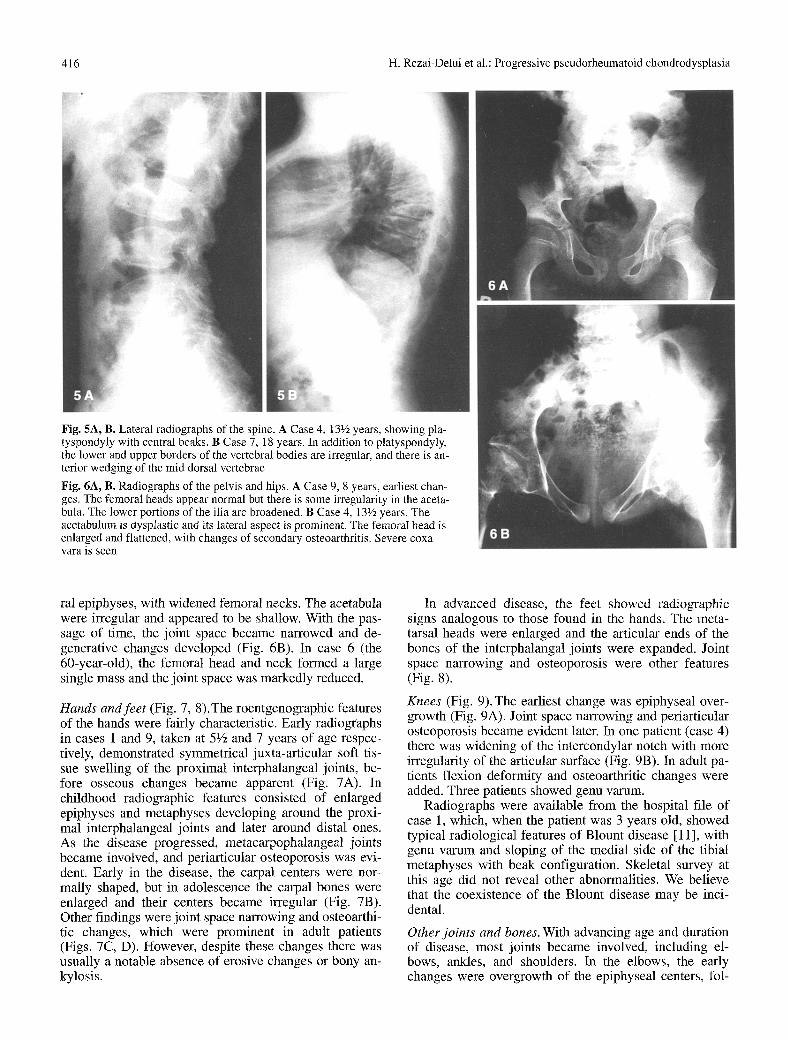
Fig. 5A, B. Lateral radiographs of the spine. A Case 4, 13�89 years, showing pla- tyspondyly with central beaks. B Case 7, 18 years. In addition to platyspondyly, the lower and upper borders of the vertebral bodies are irregular, and there is an- terior wedging of the mid dorsal vertebrae
Fig. 6A, B. Radiographs of the pelvis and hips. A Case 9, 8 years, earliest chan- ges. The femoral heads appear normal but there is some irregularity in the aceta- bula. The lower portions of the ilia are broadened. B Case 4, 13�89 years. The acetabulum is dysplastic and its lateral aspect is prominent. The femoral head is enlarged and flattened, with changes of secondary osteoarthritis. Severe coxa vara is seen
ral epiphyses, with widened femoral necks. The acetabula were irregular and appeared to be shallow. With the pas- sage of time, the joint space became narrowed and de- generative changes developed (Fig. 6B). In case 6 (the 60-year-old), the femoral head and neck formed a large single mass and the joint space was markedly reduced.
Hands and feet (Fig. 7, 8).The roentgenographic features of the hands were fairly characteristic. Early radiographs in cases 1 and 9, taken at 5�89 and 7 years of age respec- tively, demonstrated symmetrical juxta-articular soft tis- sue swelling of the proximal interphalangeal joints, be- fore osseous changes became apparent (Fig. 7A). In childhood radiographic features consisted of enlarged epiphyses and metaphyses developing around the proxi- mal interphalangeal joints and later around distal ones. As the disease progressed, metacarpophalangeal joints became involved, and periarticular osteoporosis was evi- dent. Early in the disease, the carpal centers were nor- mally shaped, but in adolescence the carpal bones were enlarged and their centers became irregular (Fig. 7B). Other findings were joint space narrowing and osteoarthi- tic changes, which were prominent in adult patients (Figs. 7C, D). However, despite these changes there was usually a notable absence of erosive changes or bony an- kylosis.
In advanced disease, the feet showed radiographic signs analogous to those found in the hands. The meta- tarsal heads were enlarged and the articular ends of the bones of the interphalangal joints were expanded. Joint space narrowing and osteoporosis were other features (Fig. 8).
Knees (Fig. 9). The earliest change was epiphyseal over- growth (Fig. 9A). Joint space narrowing and periarticular osteoporosis became evident later. In one patient (case 4) there was widening of the intercondylar notch with more irregularity of the articular surface (Fig. 9B). In adult pa- tients flexion deformity and osteoarthritic changes were added. Three patients showed genu varum.
Radiographs were available from the hospital file of case 1, which, when the patient was 3 years old, showed typical radiological features of Blount disease [11], with genu varum and sloping of the medial side of the tibial metaphyses with beak configuration. Skeletal survey at this age did not reveal other abnormalities. We believe that the coexistence of the Blount disease may be inci- dental.
Other joints and bones. With advancing age and duration of disease, most joints became involved, including el- bows, ankles, and shoulders. In the elbows, the early changes were overgrowth of the epiphyseal centers, fol-
H. Rezai-Delui et al.: Progressive pseudorheumatoid chondrodysplasia 417
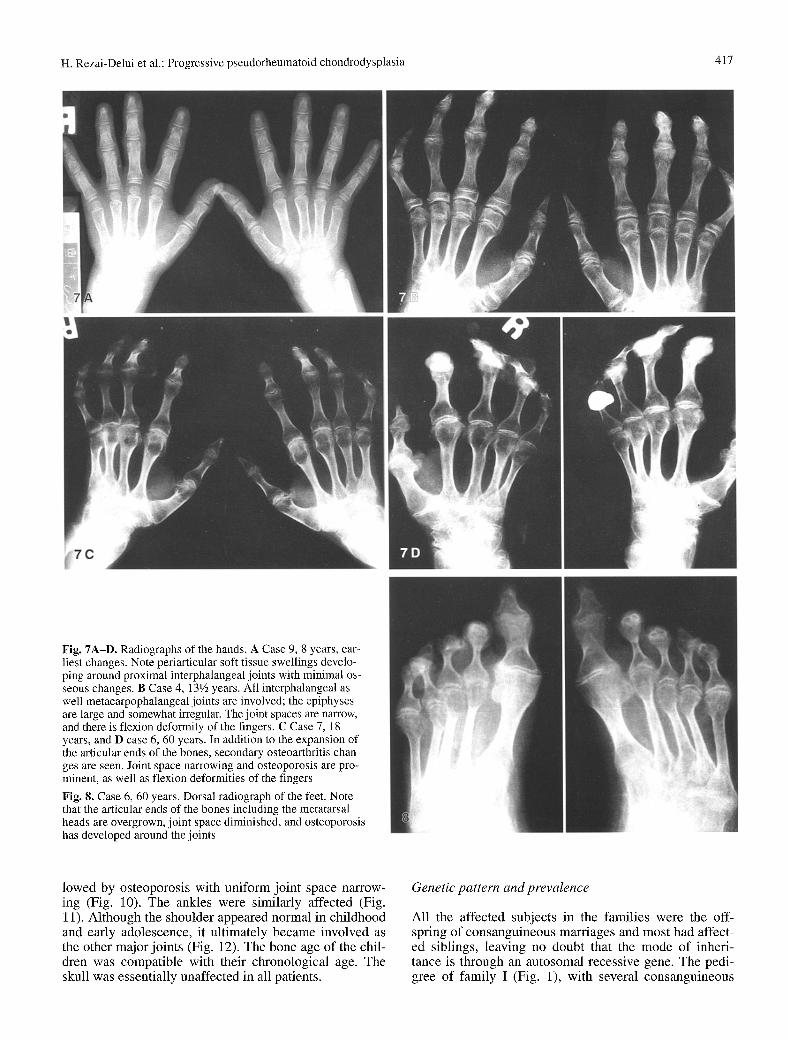
Fig. 7A-D. Radiographs of the hands. A Case 9, 8 years, ear- liest changes. Note periarticular soft tissue swellings develo- ping around proximal interphalangeal joints with minimal os- seous changes. B Case 4, 13�89 years. All interphalangeal as well metacarpophalangeal joints are involved; the epiphyses are large and somewhat irregular. The joint spaces are narrow, and there is flexion deformity of the fingers. C Case 7, 18 years, and D case 6, 60 years. In addition to the expansion of the articular ends of the bones, secondary osteoarthritis chan- ges are seen. Joint space narrowing and osteoporosis are pro- minent, as well as flexion deformities of the fingers
Fig. 8. Case 6, 60 years. Dorsal radiograph of the feet. Note that the articular ends of the bones including the metatarsal heads are overgrown, joint space diminished, and osteoporosis has developed around the joints
lowed by osteoporosis with uniform joint space narrow- ing (Fig. 10). The ankles were similarly affected (Fig. 11). Al though the shoulder appeared normal in chi ldhood and early adolescence, it ultimately became involved as the other major joints (Fig. 12). The bone age o f the chil- dren was compatible with their chronological age. The skull was essentially unaffected in all patients.
Genetic pattern and prevalence
All the affected subjects in the families were the off- spring of consanguineous marriages and most had affect- ed siblings, leaving no doubt that the mode of inheri- tance is through an autosomal recessive gene. The pedi- gree o f family I (Fig. 1), with several consanguineous
418 H. Rezai-Delui et al.: Progressive pseudorheumatoid chondrodysplasia
marriages, was developed during multiple interviews with the members of the family.
The incidence of this disorder is unknown. Wynne- Davies suggested one per million for England [12], but it might be more prevalent in Iran, as well as in other Asian and African countries, where consanguineous marriages constitute 20%-50% of all unions [13].
Discussion
The clinical features, radiological signs, and genetic pat- tern of our patients were similar to those in the other re- ported cases [2-10]. The onset of manifestation of dis- ease was between 3 and 8 years of age. In three patients the disease had an unusual onset with bow leg deformity that required surgical correction. One of them (case 1) showed typical features of Blount disease. To our knowl- edge the association of these two rare conditions in the same individual has not been reported and it may have occurred purely by chance. We believed the other two of
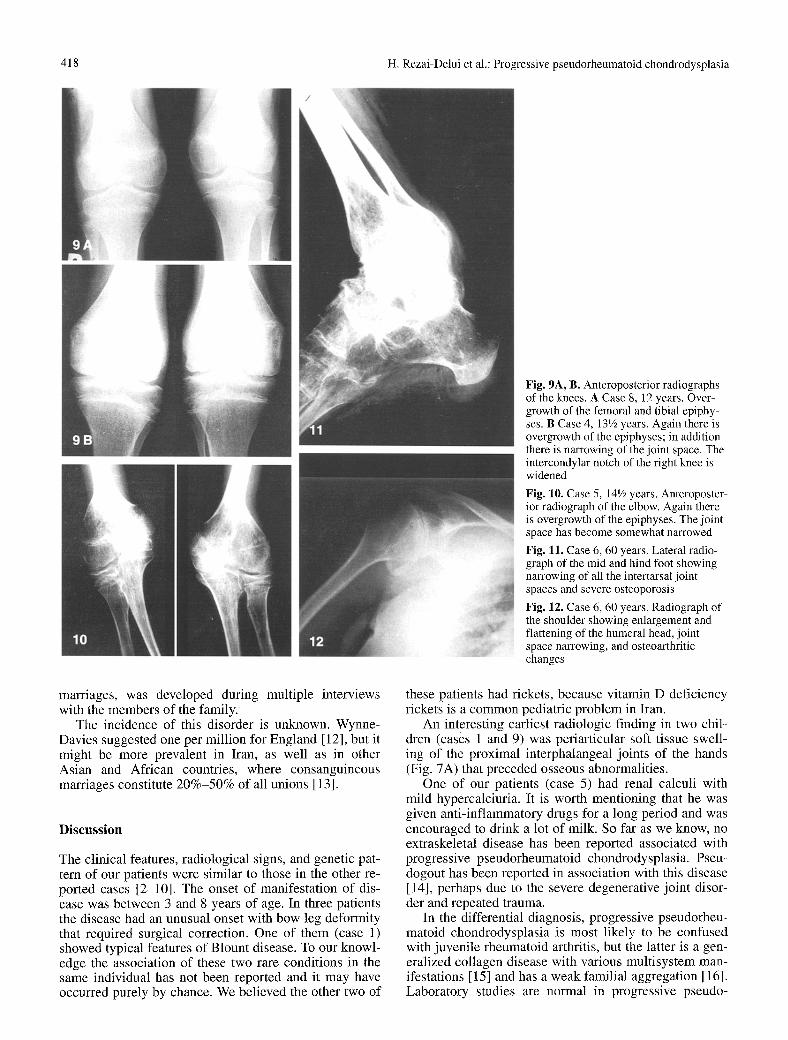
Fig. 9A, B. Anteroposterior radiographs of the knees. A Case 8, 12 years. Over- growth of the femoral and tibial epiphy- ses. B Case 4, 13V2 years. Again there is overgrowth of the epiphyses; in addition there is narrowing of the joint space. The intercondylar notch of the right knee is widened
Fig. 10. Case 5, 14~/2 years. Anteroposter- ior radiograph of the elbow. Again there is overgrowth of the epiphyses. The joint space has become somewhat narrowed
Fig. 11. Case 6, 60 years. Lateral radio- graph of the mid and hind foot showing narrowing of all the intertarsal joint spaces and severe osteoporosis
Fig. 12. Case 6, 60 years. Radiograph of the shoulder showing enlargement and flattening of the humeral head, joint space narrowing, and osteoarthritic changes
these patients had rickets, because vitamin D deficiency rickets is a common pediatric problem in Iran.
An interesting earliest radiologic finding in two chil- dren (cases 1 and 9) was periarticular soft tissue swell- ing of the proximal interphalangeal joints of the hands (Fig. 7A) that preceded osseous abnormalities.
One of our patients (case 5) had renal calculi with mild hypercalciuria. It is worth mentioning that he was given anti-inflammatory drugs for a long period and was encouraged to drink a lot of milk. So far as we know, no extraskeletal disease has been reported associated with progressive pseudorheumatoid chondrodysplasia. Pseu- dogout has been reported in association with this disease [14], perhaps due to the severe degenerative joint disor- der and repeated trauma.
In the differential diagnosis, progressive pseudorheu- matoid chondrodysplasia is most likely to be confused with juvenile rheumatoid arthritis, but the latter is a gen- eralized collagen disease with various multisystem man- ifestations [15] and has a weak familial aggregation [16]. Laboratory studies are normal in progressive pseudo-

H. Rezai-Delui et al.: Progressive pseudorheumatoid chondrodysplasia 419
rheumatoid chondrodysplasia , whereas in juvenile rheu- matoid arthritis the erythrocyte sedimentation rate is usually elevated and the serum may be positive for C-re- active protein, rheumatoid factor, and antinuclear anti- bodies [17]. Furthermore, radiographic signs of juvenile rheumatoid arthritis such as bone erosion, periostitis, ad- vanced skeletal maturation, and bony ankylosis are not found in the disorder described here.
Differentiation f rom other rheumatic diseases is rare- ly a problem, as correlation o f physical findings, roent- genographic studies, and selected laboratory studies will decide the issue. The X-l inked type o f spondyloepiphy- seal dysplasia tarda begins in late chi ldhood or early ad- olescence; premature osteoarthritis is c o m m o n compli- cation and usually involves the hips. The peripheral skel- eton is relatively unaffected and the disease has a benign course [18-21]. Further types o f spondyloepiphyseal dysplasia [22, 23] and other disorders characterized by platyspondyly, such as Morquio disease, spondylometaphyseal dysplasia, and rare forms of spondyloepimetaphyeal dysplasia, should not cause con- fusion.
References
1. Spranger J, Albert C, Schilling E A progressive connective tissue disease with features of juvenile rheumatoid arthritis and osteochondrodysplasia. Eur J Pediatr 1980; 133: 186.
2. A1-Awadi SA, Farag TI, Naguib K, E1-Kalifa G, et al. Spondyloepiphyseal dysplasia tarda with progressive arthropa- thy. J Med Genet 1984; 21: 193-196.
3. Archik SG, Kamat RD. Progressive pseudorheumatoid chondrodysplasia, simulating juvenile rheumatoid arthritis. In- dian J Pediatr 1990; 57: 785-788.
4. Kaibara N, Takagishi K, Katsuki I, Eguchi et al. Spondyloepiphyseal dyplasia tarda with progressive arthropa- thy. Skeletal Radiol 1983; 10: 13-16.
5. Kozlowski K, Kennedy J, Lewis I C. Radiographic features of progressive pseudorheumatoid arthritis. Australas Radiol 1986; 30: 244-250.
6. Robinson D, Tieder M, Halperin N, Copeliovitch L. Spondyloepiphyseal dysplasia associated with progressive ar- thropathy: an unusual disorder mimicking juvenile rheumatoid arthritis. Arch Orthop Trauma Surg 1989; 108: 397-400.
7. Stanescu V, Stanescu R, Maroteaux R Articular degeneration as a sequela of osteochondrodysplasia. Clin Rheum Dis 1985; 11: 239-270.
8. Spranger J, Albert C, Schilling F, Bartsocas C, St6ss H. Pro- gressive pseudorheumatoid arthritis of childhood (PPAC). Eur J Pediatr 1983; 140: 34-40.
9. Spranger J, Albert C, Schilling F, Bartsocas C. Pseudorheuma- toid arthropathy of childhood (PPAC): a hereditary disorder simulating juvenile rheumatoid arthtits. Am J Med Genet 1983; 14: 399-401.
10. Wynne-Davies R, Hall C, Ansell BM. Spondyloepiphyseal dysplasia tarda with progressive arthropathy: a "new" disorder of autosomal recessive inheritance. J Bone Joint Surg [Br] 1982; 64: 442-445.
11. Bathfield CA, Beighton PH. Blount disease. A review of etio- logical factors in 110 patients. Clin Orthop 1978; 135: 29-33.
12. Wynne-Davies R, Gormely J. The prevalence of skeletal dys- plasias. J Bone Joint Surg [Br] 1985; 67: 133-137.
13. Bittles AH, Mason WM, Greene J, Rao NA. Reproductive be- havior and health in consanguineous marriages. Science 1991; 252: 789-793.
14. Bradley J D. Case report: pseudoseptic pseudogout in progres- sive pseudorheumatoid arthritis of childhood. Ann Rheum Dis 1987; 46: 709-712.
15. Martel W, Holt JF, Cassidy JT. Roentgenologic manifestations of juvenile rheumatoid arthritis. AJR 1962; 88: 400-423.
16. Deighton CM, Walker DJ. The familiar nature of rheumatoid arthritis. Ann Rheum Dis 1991; 50: 62-65.
17. Kunnamo I, Kallio P, Pelkonen E Havi T. Clinical signs and laboratory test in the differential diagnosis of arthritis in chil- dren. Am J Dis Child 1987; 141: 34-40.
18. Diamond LS. A family study of spondyloepiphyseal dyspla- sia. J Bone Joint Surg [Am] 1970; 52: 1587-1594.
19. Harper PS, Jenkis P, Laurence KM. Spondyloepiphyseal dys- plasia tarda: a report of four cases in two families. Br J Radiol 1973; 46: 676-684.
20. Iceton JA, Home G. Spondyloepiphyseal dysplasia tarda: the X-linked variety in three brothers. J Bone Joint Surg [Br] 1986; 68: 616-619.
21. Poker N, Finby N, Archibald RM. Spondyloepiphyseal dys- plasia tarda: four cases in childhood and adolescence and some considerations regarding platyspondyly. Radiology 1965; 85: 474-480.
22. Felman A H. Multiple epiphyseal dysplasia: three cases with unusual vertebral abnormalities. Radiology 1969; 93: 119-125.
23. Pfeiffer RA, Suess J, Haagen M. An autosomal recessive vari- ant of spondylopiphyseal dysplasia in three sibs. Pediatr Ra- diol 1992; 22: 83-86.





























