Embed Size (px)
Citation preview

Progressive Addition Lensand Dispensing
Faculty Aravind School of Optometry
History
Benjamin Franklin invented bifocal in 1784.Owen Ave developed first patent PAL in 1907.ESSILOR launched commercially first in 1959.150 designs introduced till now.70 designs are currently available.
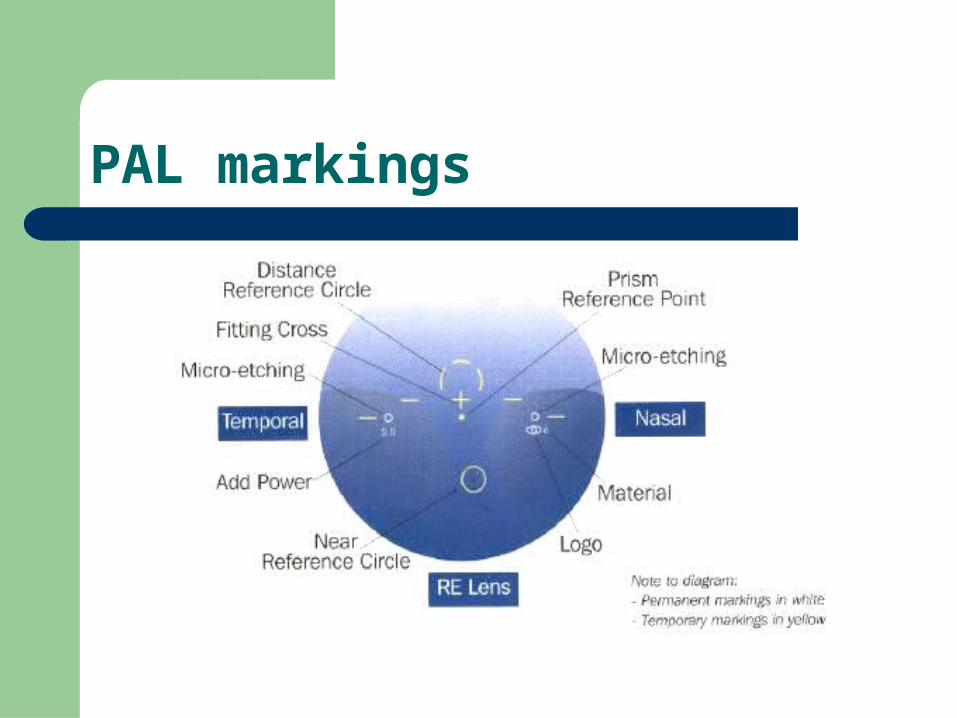
PAL markings
Optical Design
Aspheric front surface provides power progression. Progression determines
- the length of the intermediate zone,
- the position of near addition and - the gradient of peripheral lens aberrations. Peripheral surface to provide the comfortable down-
gaze vision. Advance designs are in transitions from ‘harder’ to
‘soft’.
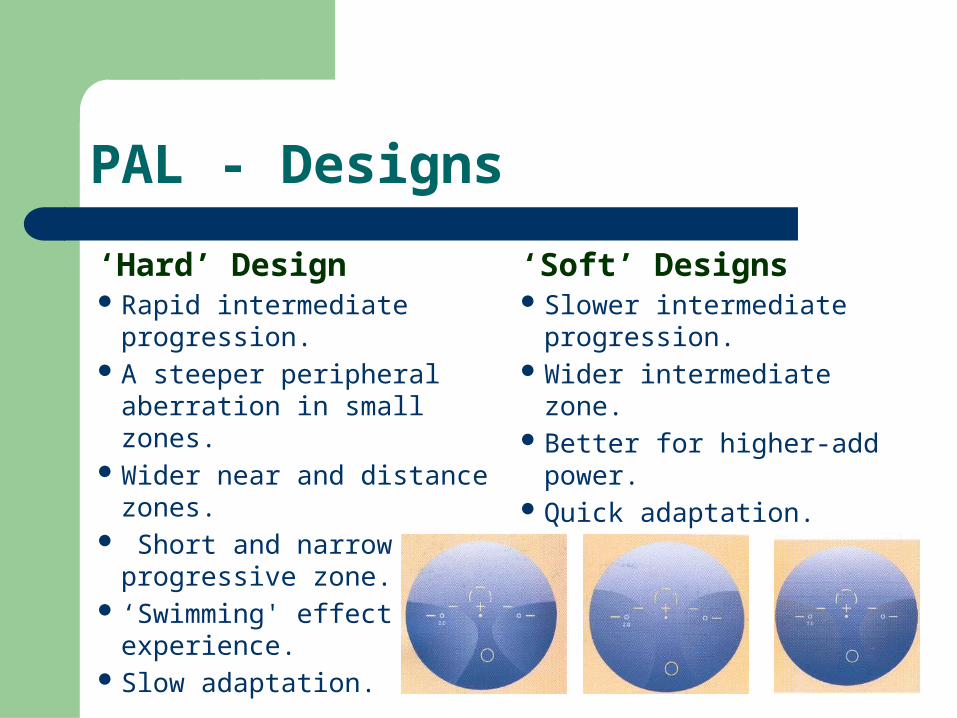
PAL - Designs
‘Hard’ Design Rapid intermediate progression. A steeper peripheral aberration in
small zones. Wider near and distance zones. Short and narrow progressive zone. ‘Swimming' effect visual
experience. Slow adaptation.
‘Soft’ Designs Slower intermediate progression. Wider intermediate zone. Better for higher-add power. Quick adaptation.
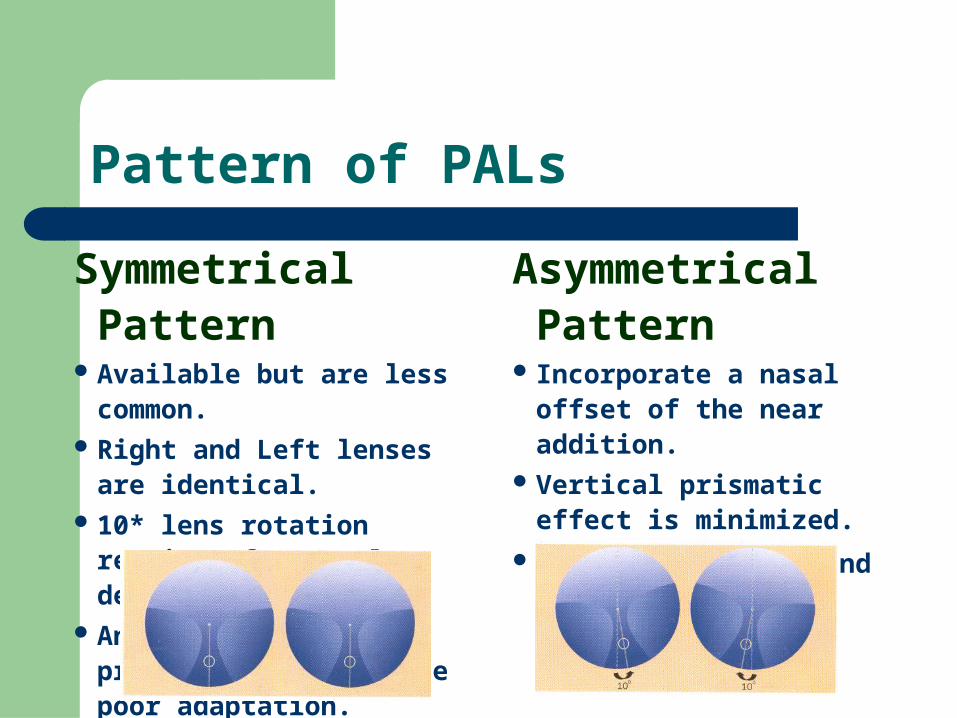
Pattern of PALs
Symmetrical Pattern Available but are less common. Right and Left lenses are identical. 10* lens rotation requires for
nasal decentration. An induced vertical prismatic
effect cause poor adaptation.
Asymmetrical Pattern Incorporate a nasal offset of the
near addition. Vertical prismatic effect is
minimized.
Better adaptation and visual
comfort.
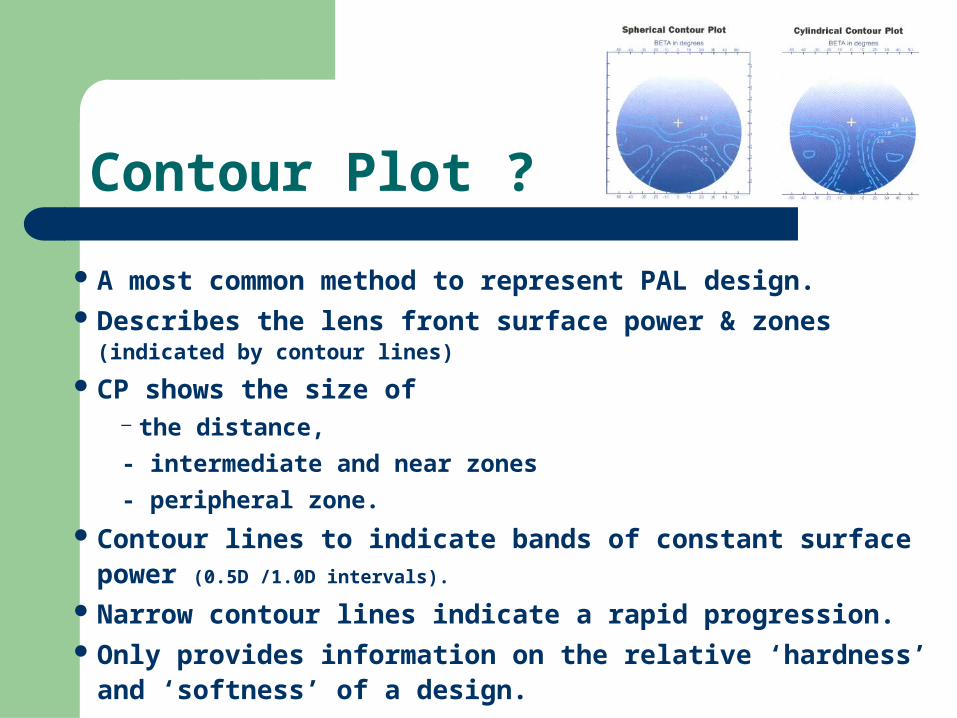
Contour Plot ?
A most common method to represent PAL design. Describes the lens front surface power & zones (indicated by contour lines)
CP shows the size of – the distance,
- intermediate and near zones
- peripheral zone.
Contour lines to indicate bands of constant surface power (0.5D /1.0D
intervals).
Narrow contour lines indicate a rapid progression. Only provides information on the relative ‘hardness’ and ‘softness’ of a
design.
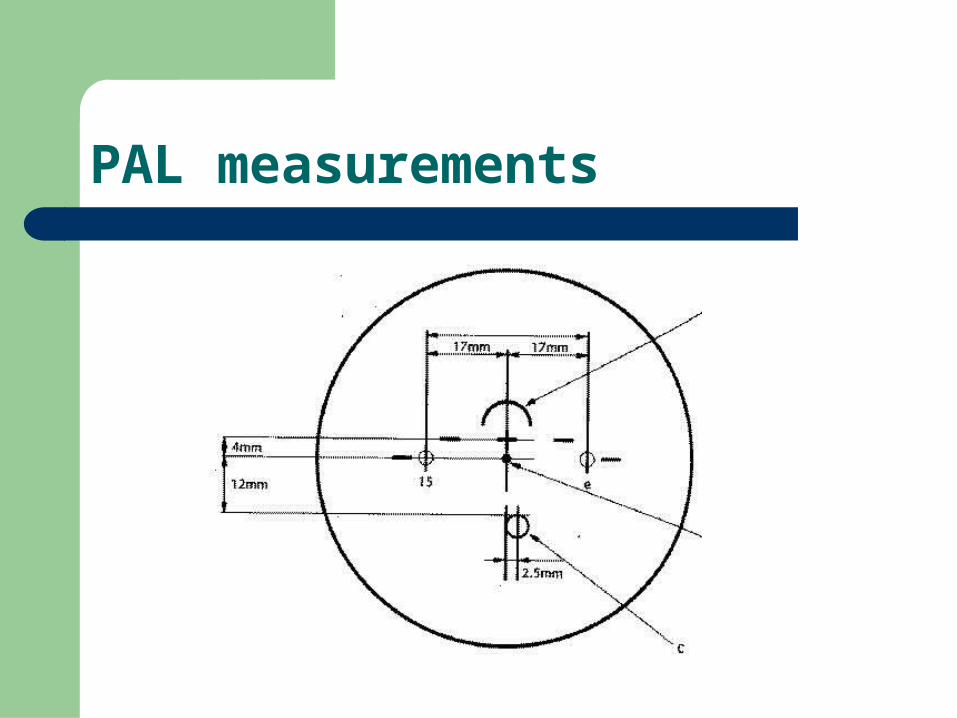
PAL measurements
Recommending the PAL
PAL provides the various range of focus to presbyopes.
Many Presbyopes are suited to use PAL. Consider the patient’s visual needs and refractive
status.
Who is suitable for PAL?
Early presbyopes. Constant bifocal wearers. Specific needs of intermediate vision. Near vision requirements on up-gaze. Person who needs cosmetic protection .
PAL can be avoided to…
Anisometrope
- greater than 2.5D in spherical power
- greater than 1.75D in cylindrical power Near addition above in 4.00D Person having an inadequate vision with best correction. Person who having pathological changes. Patients with shaky/unsteady heads. Vertical facial symmetry and vertical heterophorias.
Refraction and PAL
An accurate Rx is success with PAL.
An inaccurate Rx makes difficult to see clearly with
normal head posture.
To confirm the final Rx,use the supplementary tests.
(JCC,Duochrome,Astigmatic dial,etc.,)
Commonly used working distance(40cm)is to be
considered for clearest near vision.
Dispensing PALs – Frame selection
Metal frame with adjustable pads is a good option.
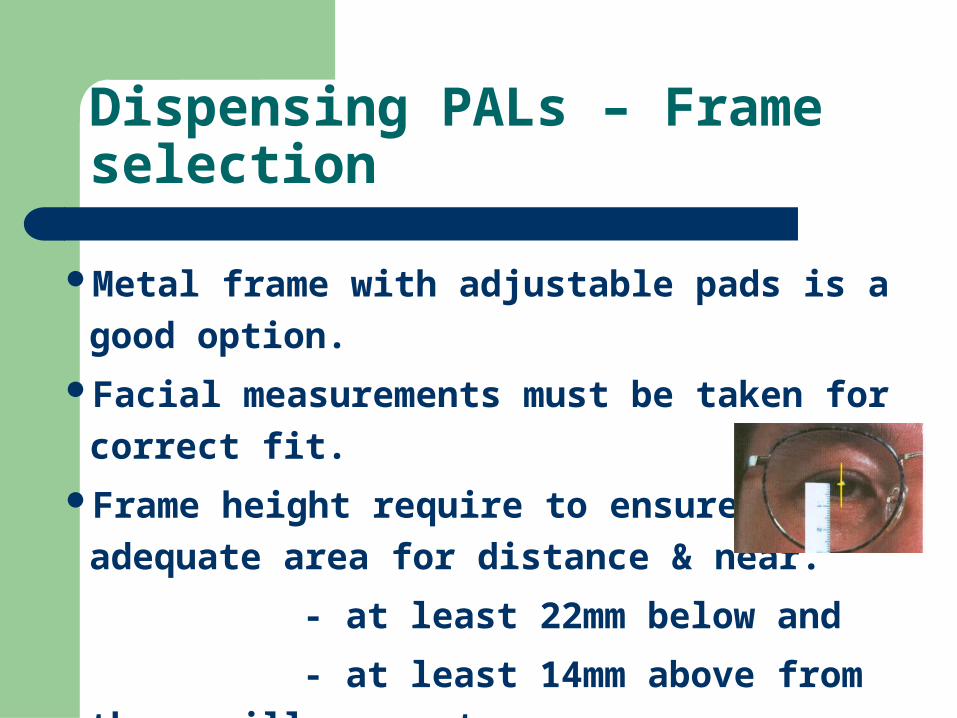
Facial measurements must be taken for correct fit.
Frame height require to ensure adequate area for
distance & near.
- at least 22mm below and
- at least 14mm above from the pupillary center.
Frame shape also to be considered for near vision.
Dispensing PAL -Frame adjustments
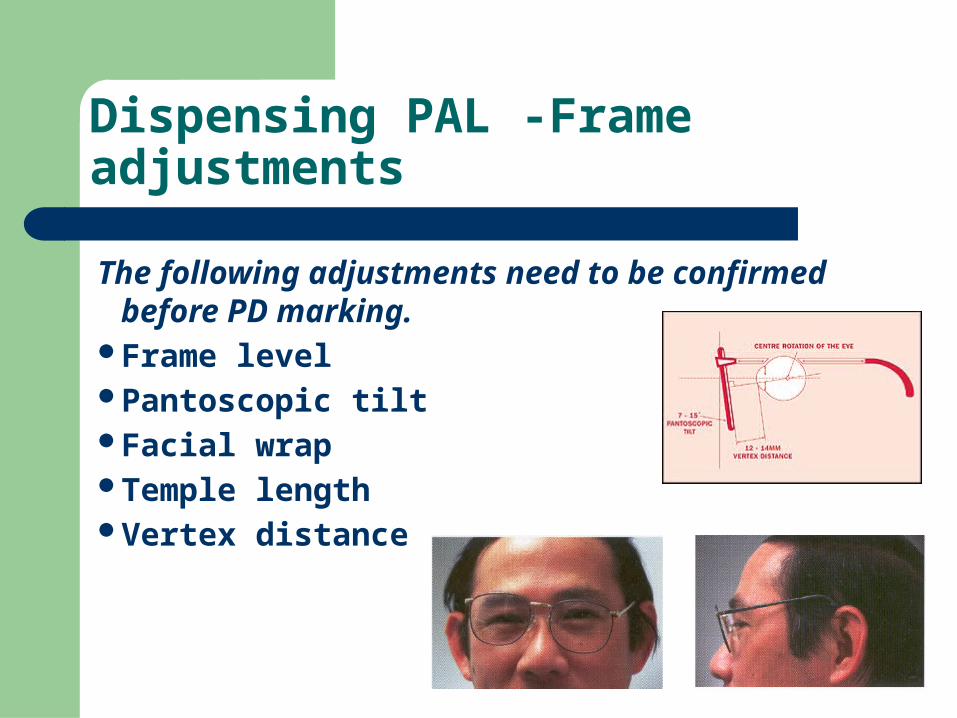
The following adjustments need to be confirmed before PD marking.
Frame level Pantoscopic tiltFacial wrapTemple lengthVertex distance
Dispensing PALs – PD measurements
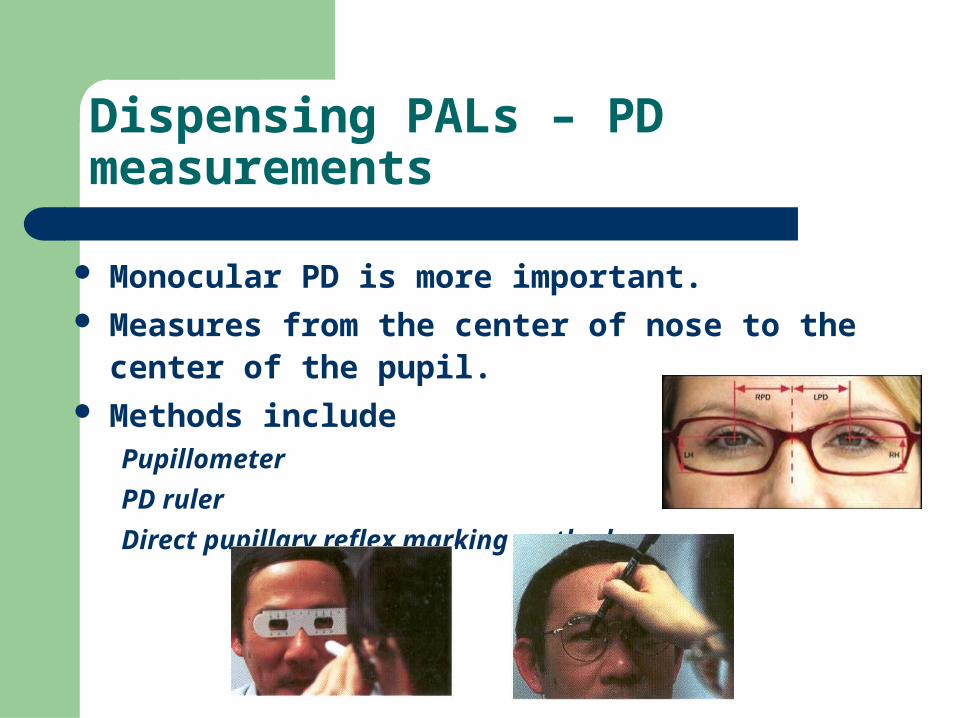
Monocular PD is more important. Measures from the center of nose to the center of the pupil. Methods include
Pupillometer
PD ruler
Direct pupillary reflex marking method.
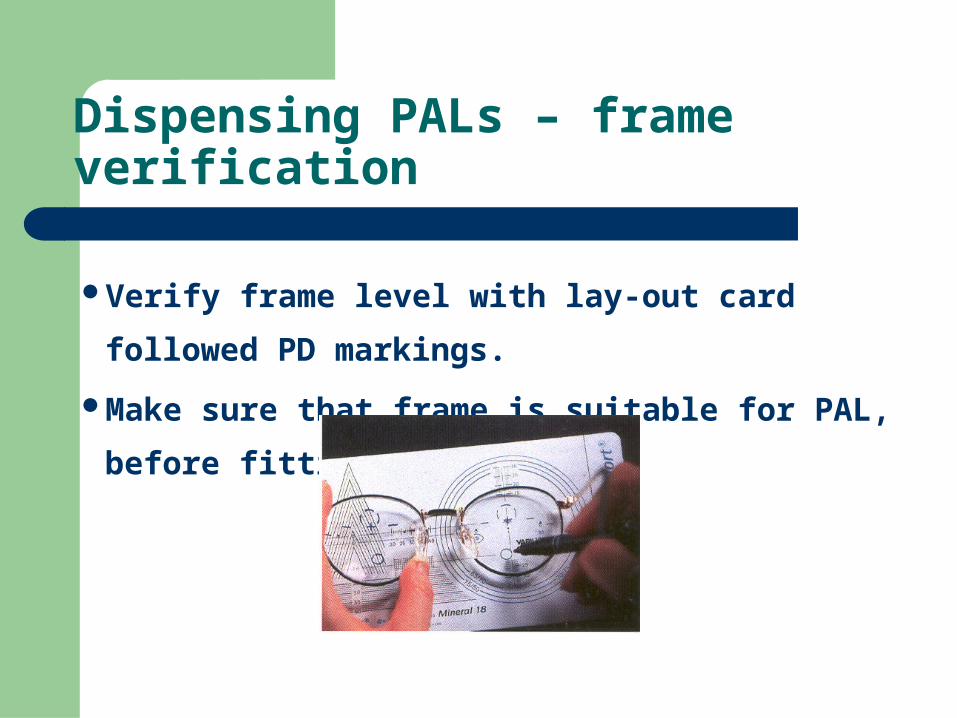
Dispensing PALs – frame verification
Verify frame level with lay-out card followed PD markings.
Make sure that frame is suitable for PAL, before fitting.
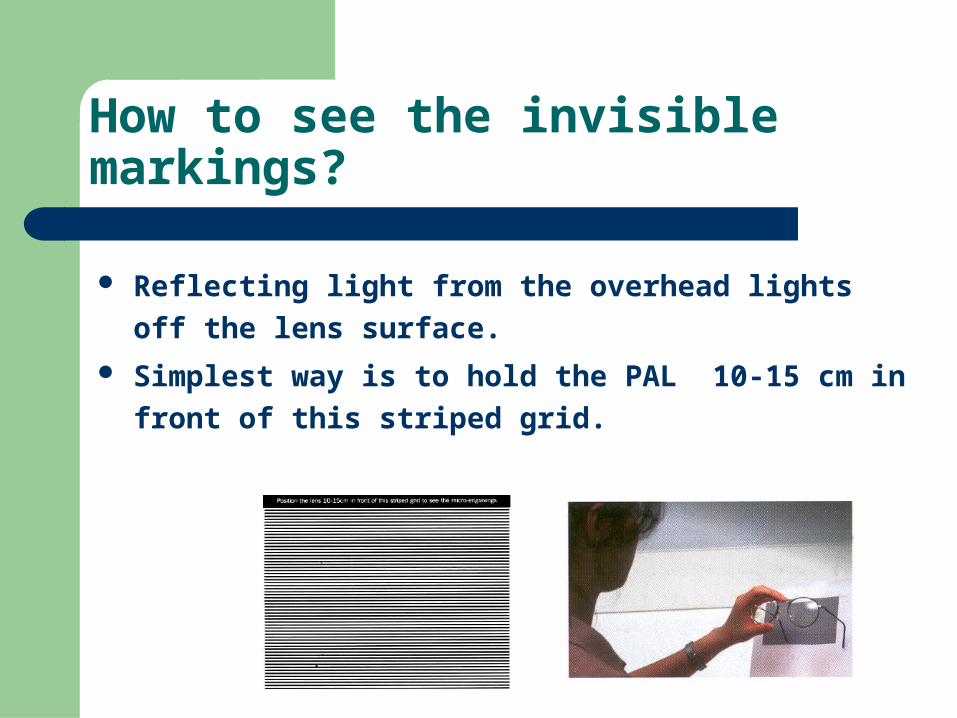
How to see the invisible markings?
Reflecting light from the overhead lights off the lens surface.
Simplest way is to hold the PAL 10-15 cm in front of this
striped grid.
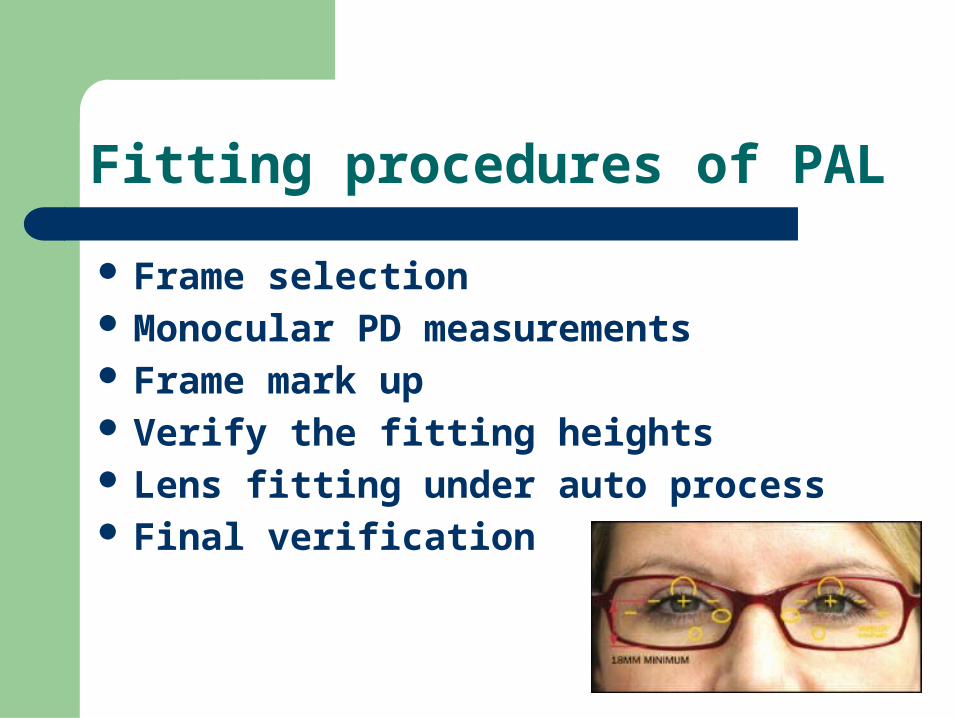
Fitting procedures of PAL
Frame selection Monocular PD measurements Frame mark up Verify the fitting heights Lens fitting under auto process Final verification
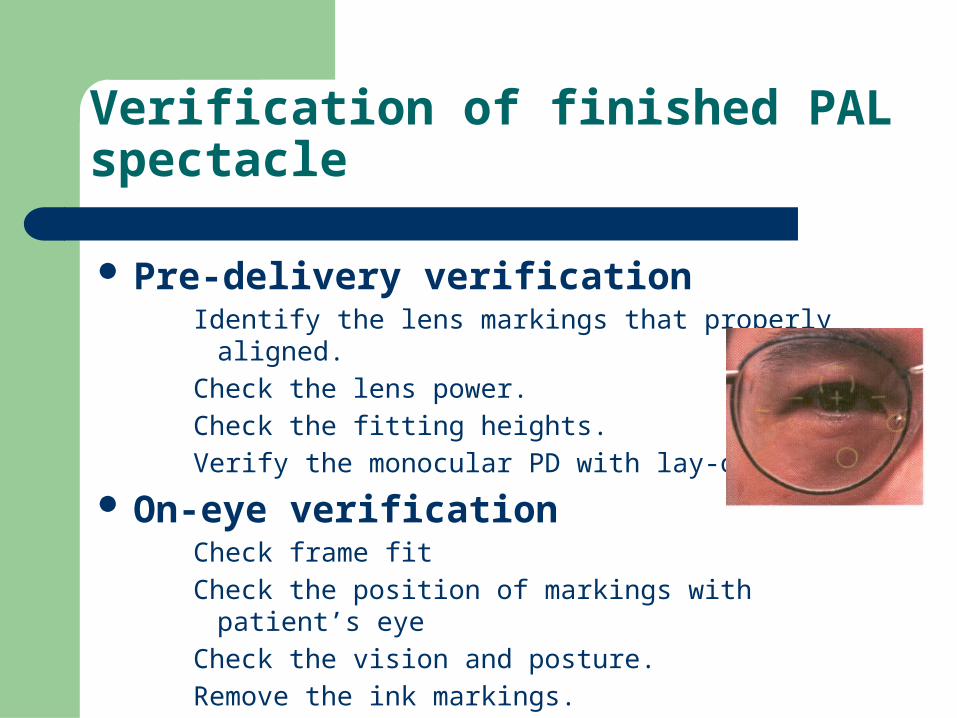
Verification of finished PAL spectacle
Pre-delivery verificationIdentify the lens markings that properly aligned.
Check the lens power.
Check the fitting heights.
Verify the monocular PD with lay-out card.
On-eye verificationCheck frame fit
Check the position of markings with patient’s eye
Check the vision and posture.
Remove the ink markings.
Possible errors with PAL
Incorrect PD measurements.Incorrect fitting heights.Inaccurate refraction.Inappropriate frame selection and fit.Base curve changes.
Problems and their possible causes
Distance blur visionFitting height too high.
Over ‘+’ correction / under ‘-’ correction.
Astigmatism
Near blur visionFitting height too low.
Increased vertex distance.
Incorrect prescription of near add and distance Rx.
Insufficient pantoscopic tilt.
Base curve of the lens.
Problems and their possible causes
Head tilt back at distance– over ‘-’ correction / under’+’correction.
– Incorrect Rx.
Head tilt back at near or intermediate– Incorrect Rx.
–Fitting height too low.
Problems and their possible causes
Head tilt forward at distance
Fitting height too high.
Head tilt forward at near or intermediate
Incorrect Rx.
Over ’+’correction.
Key points to success with PALs
An accurate refraction.
Correct size frame and adjustments
An accurate monocular PD measurements.
Perfect fitting.
Proper instruction on use.
Motivate the patient to adapt the new type of vision.
Thank You