Embed Size (px)
Citation preview

PROGRESS IN GENE THERAPY FOR HEMOPHILIA A AND B
Glenn Pierce MD PhDVice President, MedicalWorld Federation of HemophiliaLa Jolla, California, USA
대한혈액학회 KOREAN SOCIETY OF HEMATOLOGY
COI DISCLOSUREGLENN PIERCE
I currently have, or I have had in the past two years, an affiliation or financial interest with business corporation(s):
(1) Consulting fees: BioMarin, Genentech/ Roche, Shire, Pfizer, St Jude
(2) Research fundings: None
(3) Boards, Employment: Voyager Therapeutics, Third Rock Ventures, Ambys Medicines
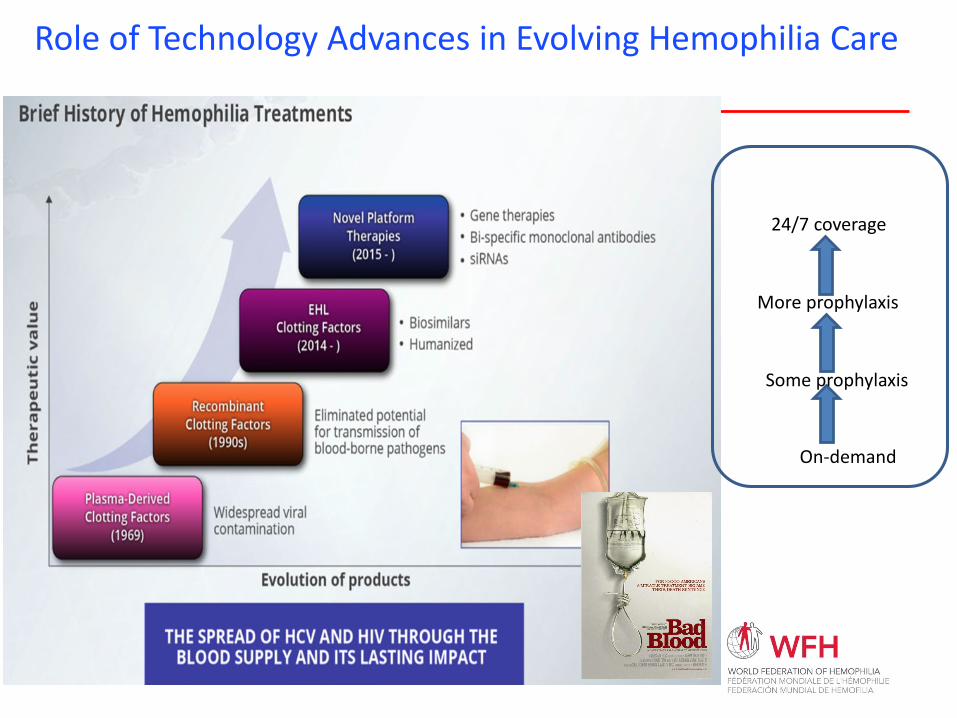
On-demand
Some prophylaxis
More prophylaxis
24/7 coverage
Role of Technology Advances in Evolving Hemophilia Care
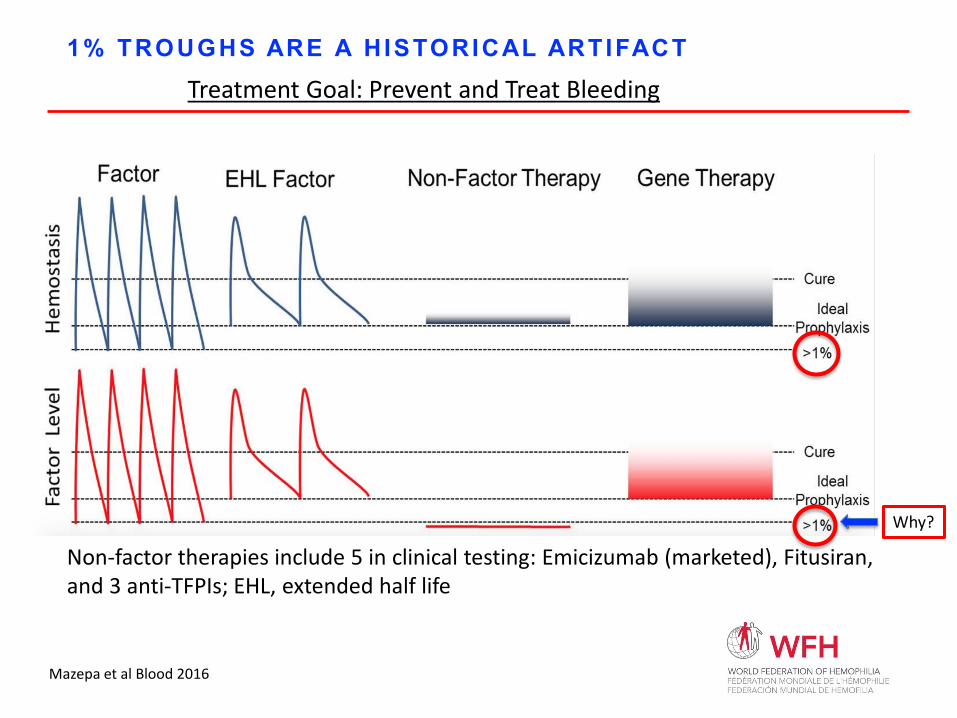
1% TROUGHS ARE A HISTORICAL ARTIFACT
Non-factor therapies include 5 in clinical testing: Emicizumab (marketed), Fitusiran, and 3 anti-TFPIs; EHL, extended half life
Why?
Treatment Goal: Prevent and Treat Bleeding
Mazepa et al Blood 2016
WHY GENE THERAPY FOR HEMOPHILIA?
Scientists
•“Perfect” disease to study with this novel biotechnologysingle gene defect with directly correlated phenotype
•Wide target range5-150% factor activity levelsno tight regulation needed
•Model for progress
Patients•High burden of replacement therapy
•Continued risk of Morbidity and
Mortality despite prophylaxis due to
• Target 1% factor troughs
• Variable compliance with regimen
•70% of world - no access to clotting
factor, no hope in foreseeable future
Pipe SW. Gene therapy for hemophilia. Pediatric Blood Cancer. 2017 Oct 27. doi: 10.1002/pbc.26865. Perales MA, Kebriaei P, Kean LS, Sadelain M. Building a Safer and Faster CAR: Seatbelts, Airbags and Crispr. Biol Blood Marrow Transplant. 2017 Oct 12. pii: S1083-8791(17)30776-0. doi: 10.1016/j.bbmt.2017.10.017.
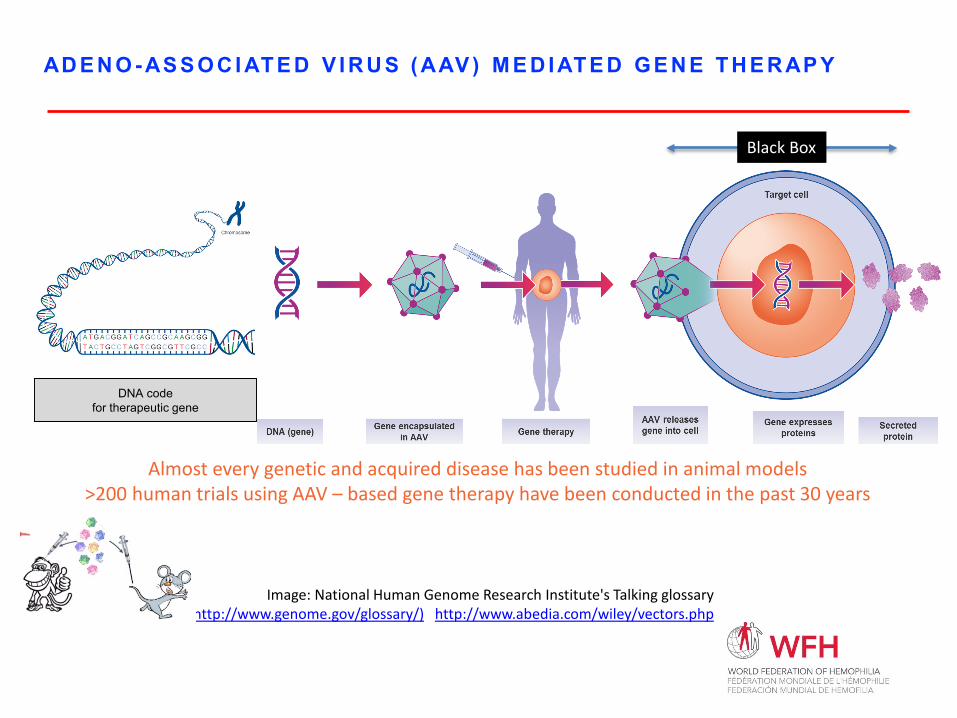
AD E N O- AS S O C I AT E D V I R U S ( AAV ) M E D I AT E D G E N E T H E R AP Y
Black Box
DNA codefor therapeutic gene
Almost every genetic and acquired disease has been studied in animal models>200 human trials using AAV – based gene therapy have been conducted in the past 30 years
Image: National Human Genome Research Institute's Talking glossary (http://www.genome.gov/glossary/) http://www.abedia.com/wiley/vectors.php
ADENO-ASSOCIATED VIRUS: ADVANTAGES AND DISADVANTAGES
Advantages
•Wild type not pathogenic•Many serotypes evolved with different species and tissue specificities•Minor, transient toxicity as vector administration •Only a minor amount of integration•It works
Disadvantages
•Difficult to manufacture
•Small payload capacity
•Variably high levels of immunity to many serotypes
•Antibody response precludes 2nd administration
•Variable toxicity upon administration
•Minor amount of integration
•Duration of effect unclear
•Variable responses
•Many steps from manufacture to protein expression in vivo not understood
D I S R U P T I V E T E C HN O L O G I E S : B AL AN C I N G B E N E F I T S AN D R I S K S
BENEFITS of Gene Therapy•Elimination of factor troughs
•Phenotypic ”cures”
•Benefit/risk differs in developing world
RISKS of Gene Therapy• May not be immediately obvious
• Known knowns
• Known Unknowns
• Unknown unknowns*
*Rumsfeld, Donald (2011). Known and Unknown: A Memoir. New York: Penguin Group. p. xiv. ISBN 9781101502495.Pierce, GF, Iorio, A Past, Present and Future of Haemophilia Gene Therapy: From Vectors and Transgenes to Known and Unknown Outcomes. Haemophilia, 2018;24 Suppl 6:60-67
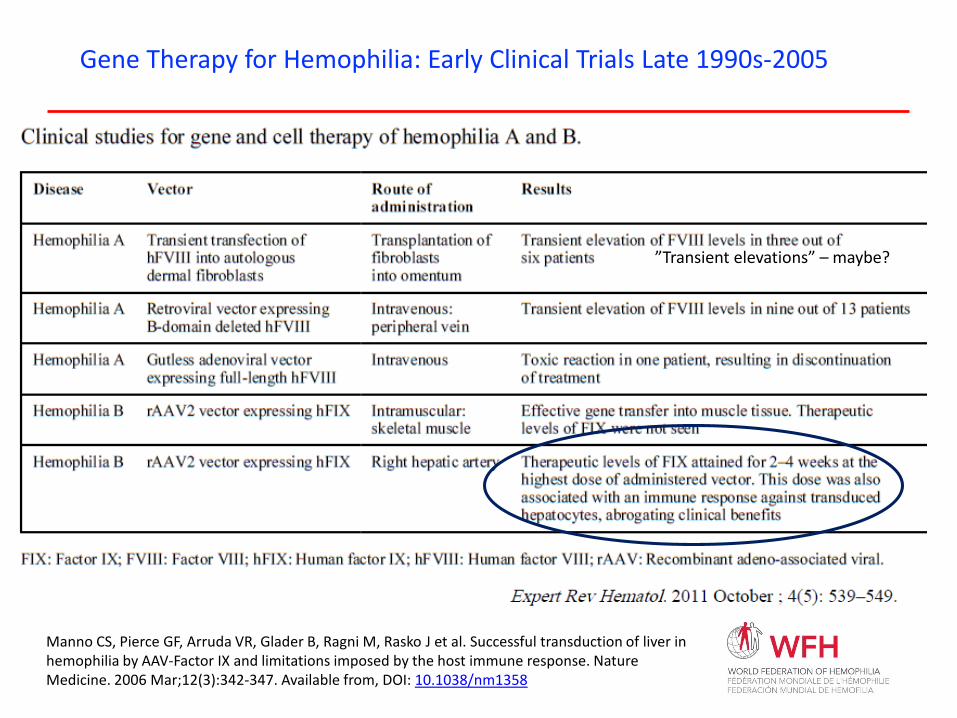
”Transient elevations” – maybe?
Gene Therapy for Hemophilia: Early Clinical Trials Late 1990s-2005
Manno CS, Pierce GF, Arruda VR, Glader B, Ragni M, Rasko J et al. Successful transduction of liver in hemophilia by AAV-Factor IX and limitations imposed by the host immune response. Nature Medicine. 2006 Mar;12(3):342-347. Available from, DOI: 10.1038/nm1358
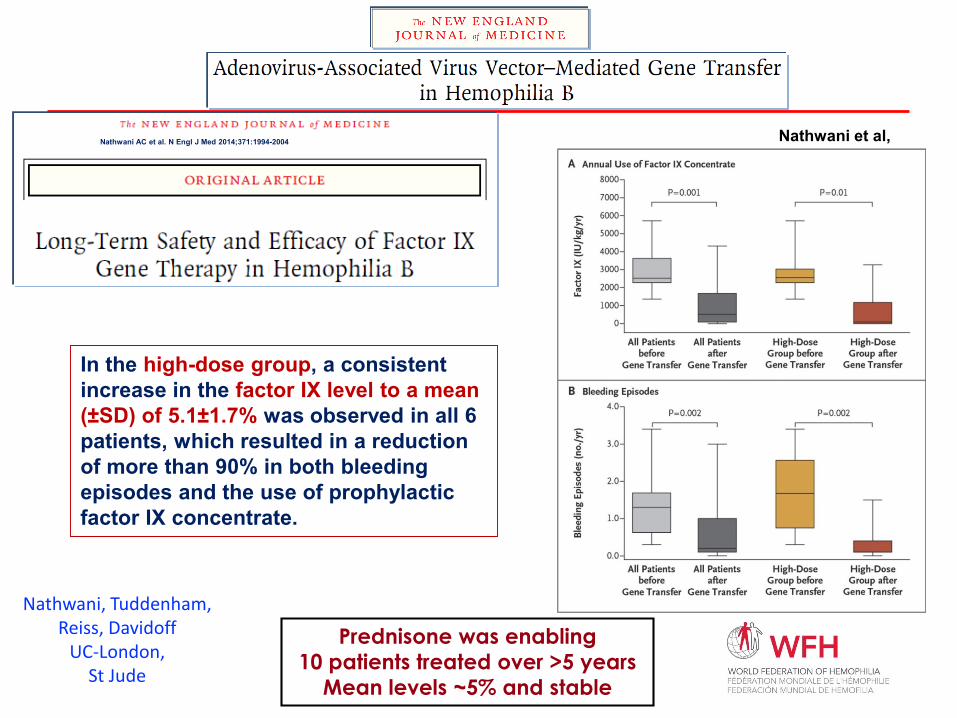
Nathwani et al, Dec 2011
Nathwani AC et al. N Engl J Med 2014;371:1994-2004
In the high-dose group, a consistent increase in the factor IX level to a mean (±SD) of 5.1±1.7% was observed in all 6 patients, which resulted in a reduction of more than 90% in both bleeding episodes and the use of prophylactic factor IX concentrate.
Prednisone was enabling10 patients treated over >5 years
Mean levels ~5% and stable
Nathwani, Tuddenham,Reiss, Davidoff
UC-London, St Jude
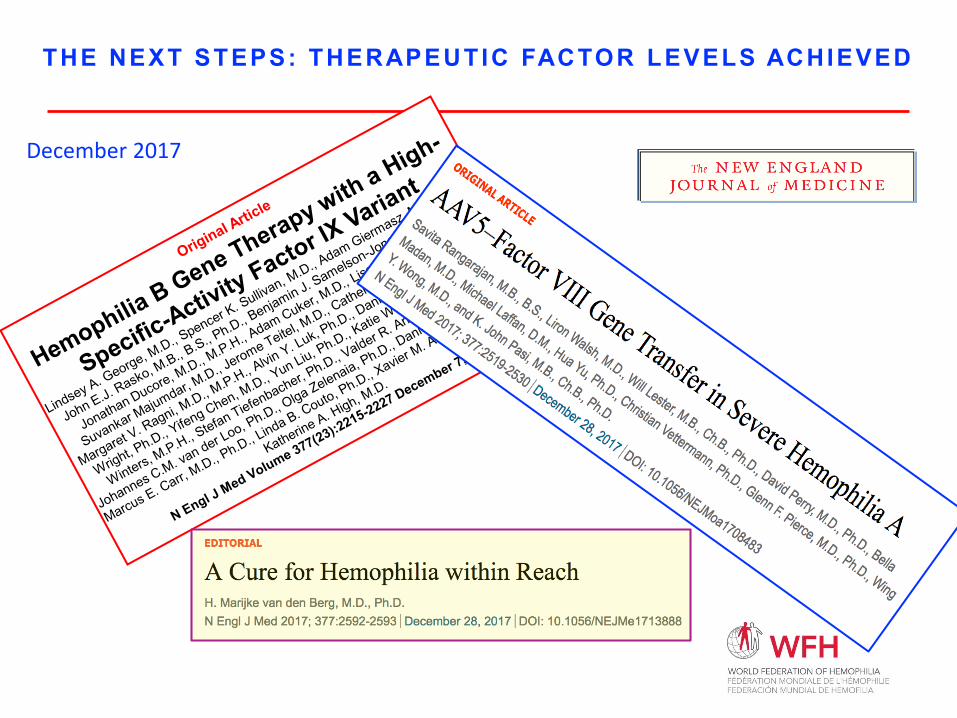
THE NEXT STEPS: THERAPEUTIC FACTOR LEVELS ACHIEVED
December 2017
AAV-Factor IX Studies
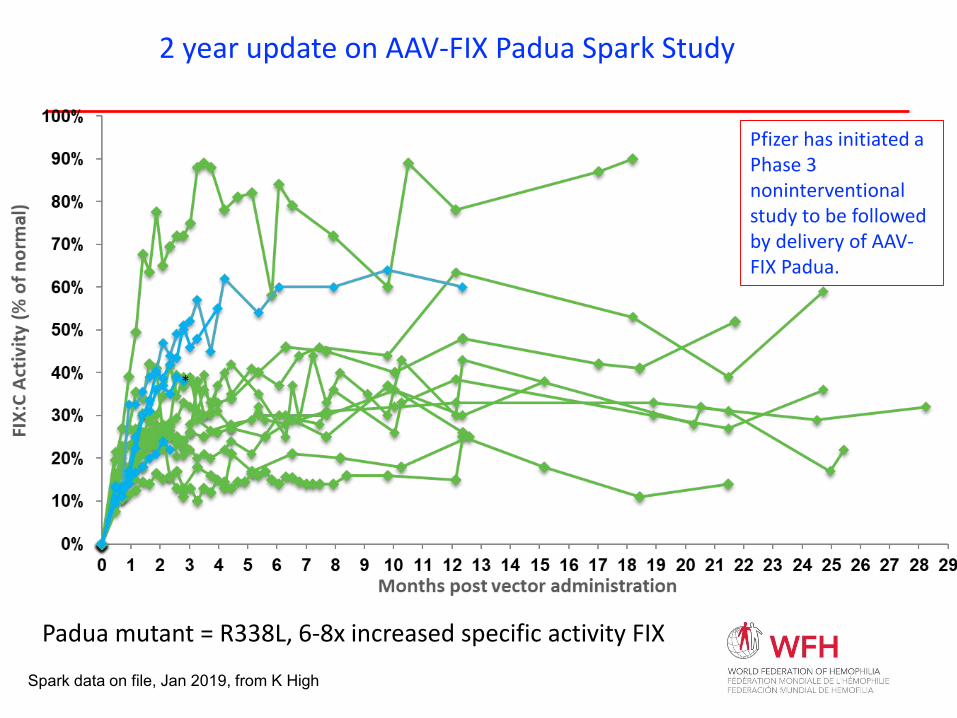
Spark data on file, Jan 2019, from K High
2 year update on AAV-FIX Padua Spark Study
Padua mutant = R338L, 6-8x increased specific activity FIX
Pfizer has initiated a Phase 3 noninterventional study to be followed by delivery of AAV-FIX Padua.
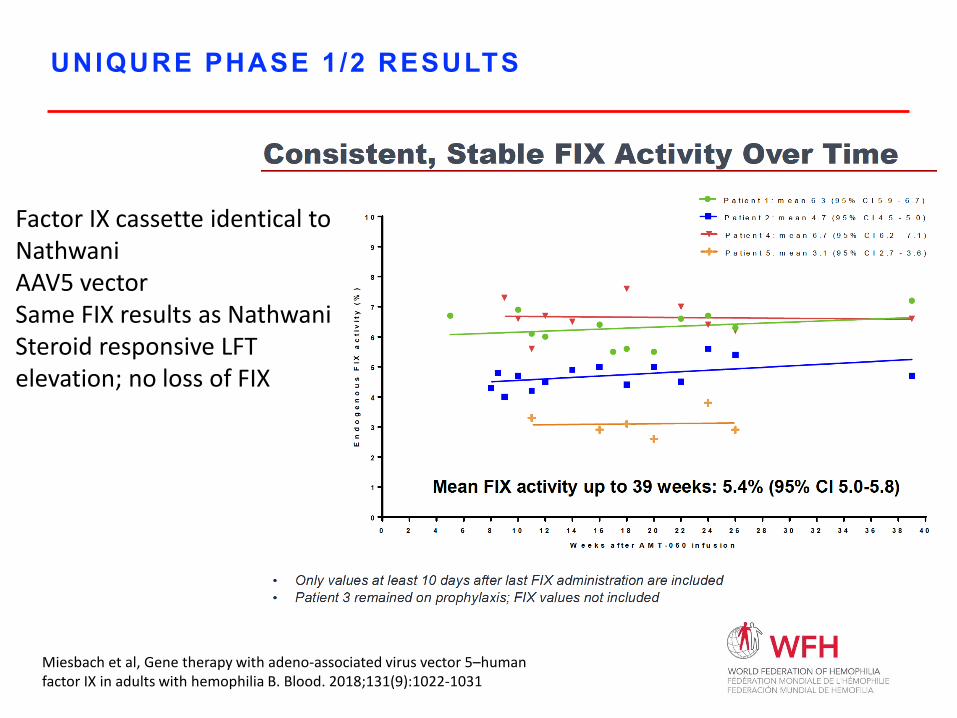
UNIQURE PHASE 1/2 RESULTS
Factor IX cassette identical to NathwaniAAV5 vectorSame FIX results as NathwaniSteroid responsive LFT elevation; no loss of FIX
Miesbach et al, Gene therapy with adeno-associated virus vector 5–humanfactor IX in adults with hemophilia B. Blood. 2018;131(9):1022-1031
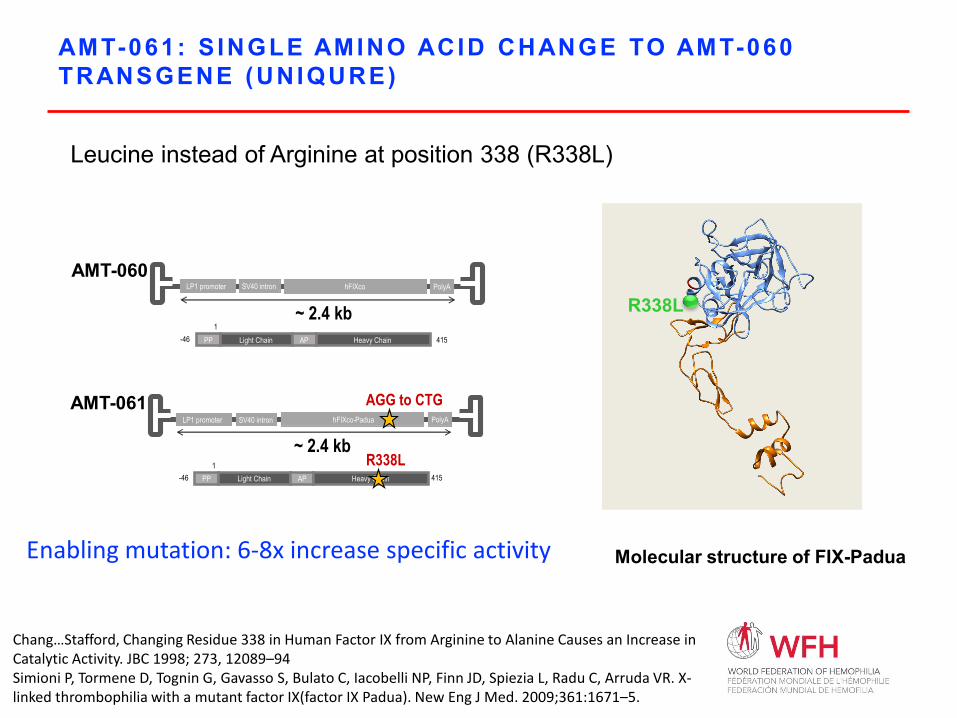
AMT-061: S INGLE AMINO ACID CHANGE TO AMT-060 TRANSGENE (UNIQURE)
Leucine instead of Arginine at position 338 (R338L)
R338LPP Light Chain AP Heavy Chain-46 415
~ 2.4 kbhFIXco PolyALP1 promoter SV40 intron
AMT-060
1
PP Light Chain AP Heavy Chain-46
R338L
hFIXco-Padua
AGG to CTG
~ 2.4 kbLP1 promoter SV40 intron PolyA
AMT-061
4151
Molecular structure of FIX-Padua
Chang…Stafford, Changing Residue 338 in Human Factor IX from Arginine to Alanine Causes an Increase in Catalytic Activity. JBC 1998; 273, 12089–94Simioni P, Tormene D, Tognin G, Gavasso S, Bulato C, Iacobelli NP, Finn JD, Spiezia L, Radu C, Arruda VR. X-linked thrombophilia with a mutant factor IX(factor IX Padua). New Eng J Med. 2009;361:1671–5.
Enabling mutation: 6-8x increase specific activity
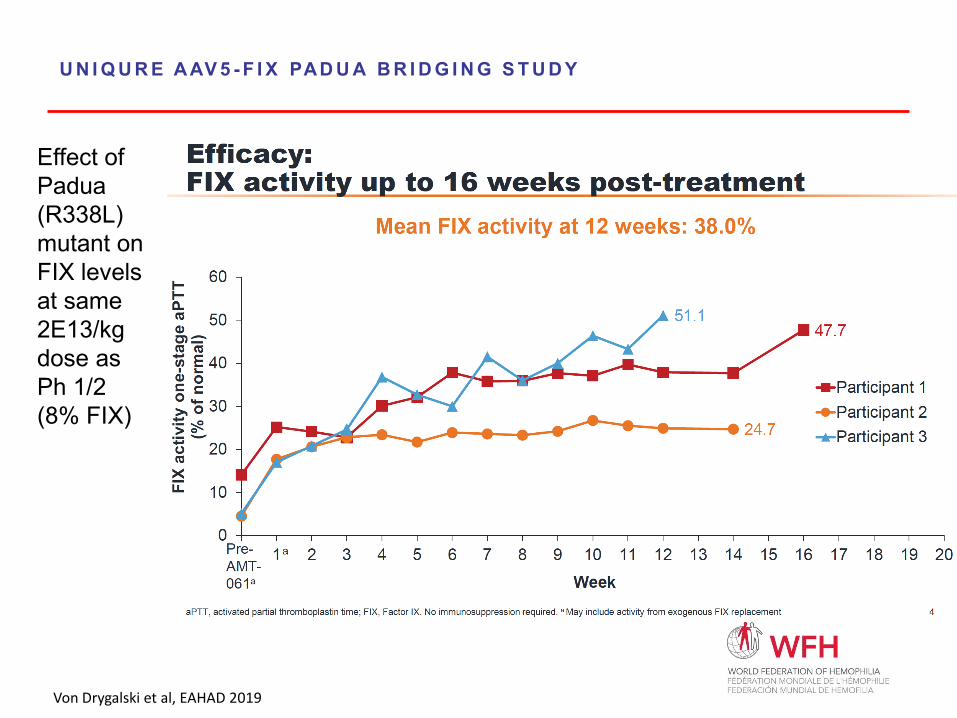
U N I Q U R E A AV 5 - F I X PAD U A B R I D G I N G S T U D Y
Effect of Padua (R338L) mutant on FIX levels at same 2E13/kg dose as Ph 1/2 (8% FIX)
Von Drygalski et al, EAHAD 2019
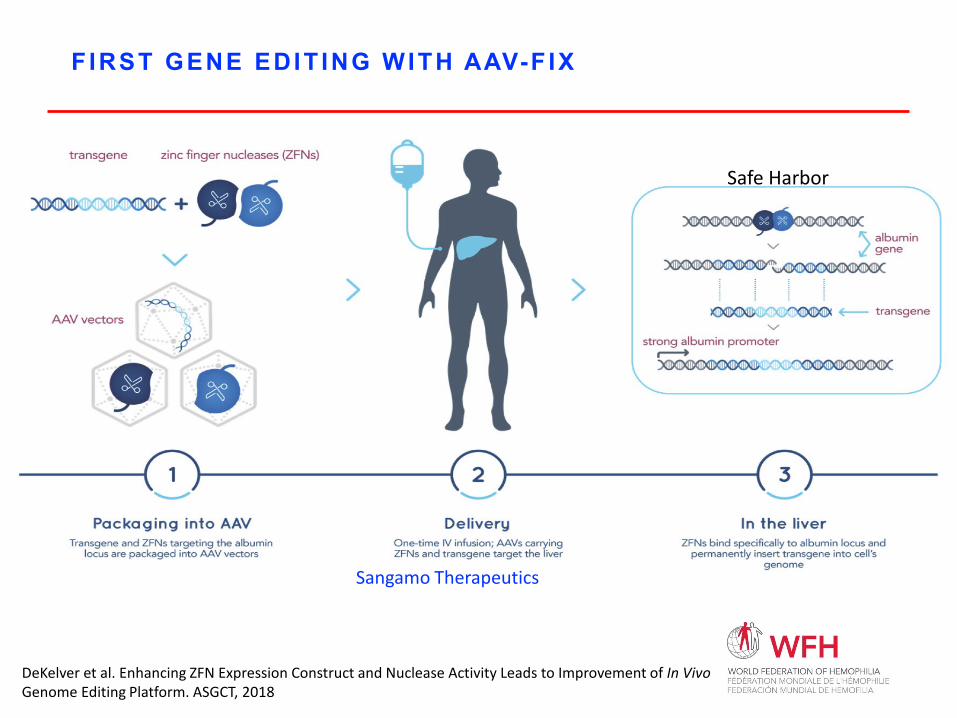
FIRST GENE EDIT ING WITH AAV-F IX
DeKelver et al. Enhancing ZFN Expression Construct and Nuclease Activity Leads to Improvement of In Vivo Genome Editing Platform. ASGCT, 2018
Safe Harbor
Sangamo Therapeutics
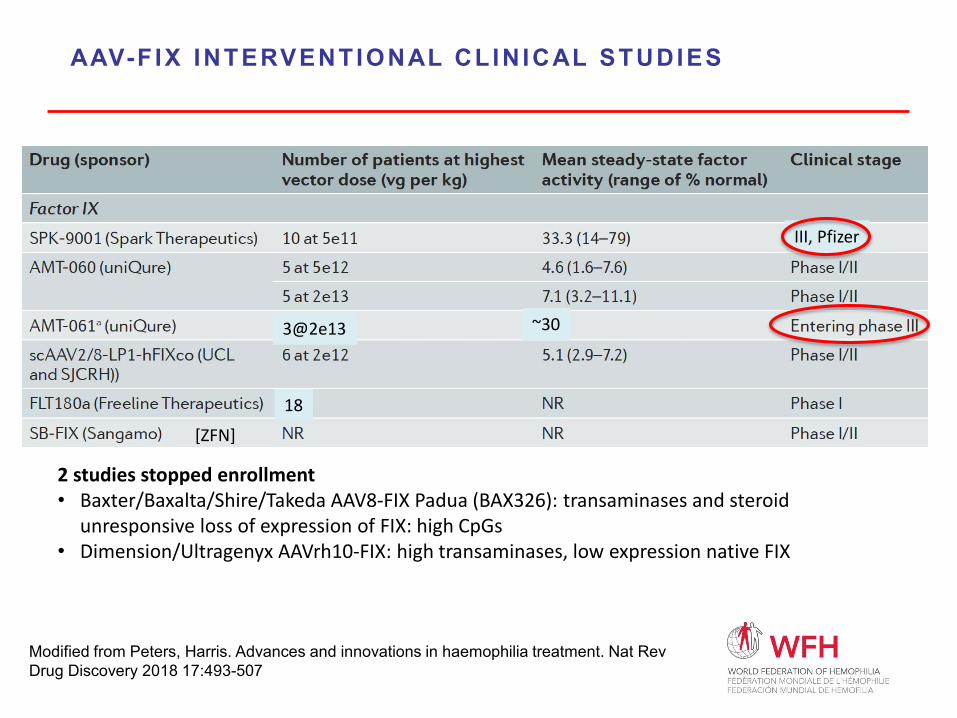
AAV-F IX INTERVENTIONAL CLINICAL STUDIES
Modified from Peters, Harris. Advances and innovations in haemophilia treatment. Nat Rev Drug Discovery 2018 17:493-507
2 studies stopped enrollment• Baxter/Baxalta/Shire/Takeda AAV8-FIX Padua (BAX326): transaminases and steroid
unresponsive loss of expression of FIX: high CpGs• Dimension/Ultragenyx AAVrh10-FIX: high transaminases, low expression native FIX
[ZFN]
18
III, Pfizer
~303@2e13
AAV-Factor VIII Studies
Pierce/WFH 28
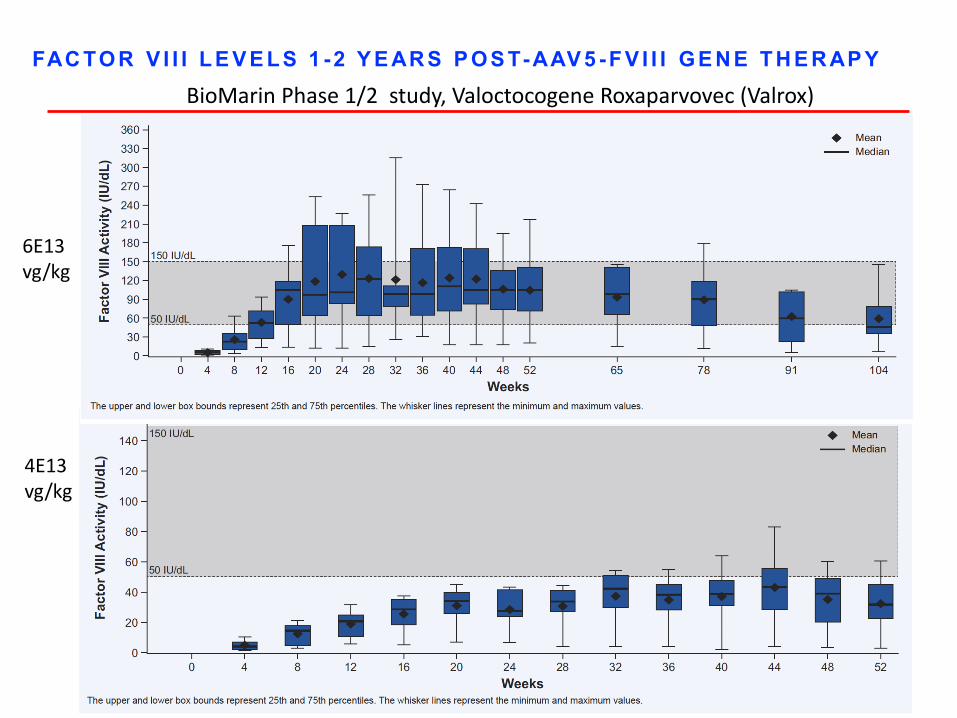
FAC TO R V I I I L E V E L S 1 - 2 Y E AR S P O S T- AAV 5 - F V I I I G E N E T H E R AP YBioMarin Phase 1/2 study, Valoctocogene Roxaparvovec (Valrox)
6E13 vg/kg
4E13 vg/kg
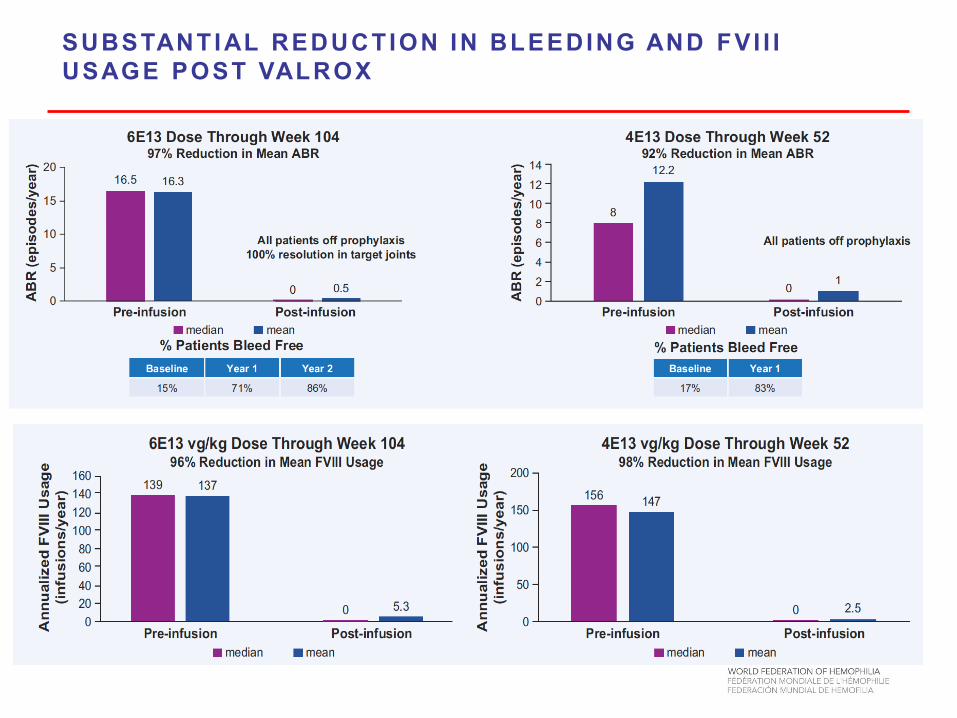
SUBSTANTIAL REDUCTION IN BLEEDING AND FVI I I USAGE POST VALROX
Pierce/WFH 34
SUMMARY OF SAFETY FOR VALROX PHASE 1 /2
• BMN 270 was well tolerated across all doses
• No subject developed inhibitors to FVIII
• No subject withdrew
• Most common AEs across all dose cohorts: ALT elevation (10 subjects, 67%), arthralgia (7 subjects, 47%) and back pain, fatigue, headache (5 subjects each, 33%)
• 2 Subjects reported SAE’s during the study:• Grade 2 pyrexia with myalgia and headache at time of infusion;
observed in hospital overnight and resolved without sequelae • Planned total knee replacement for chronic arthropathy
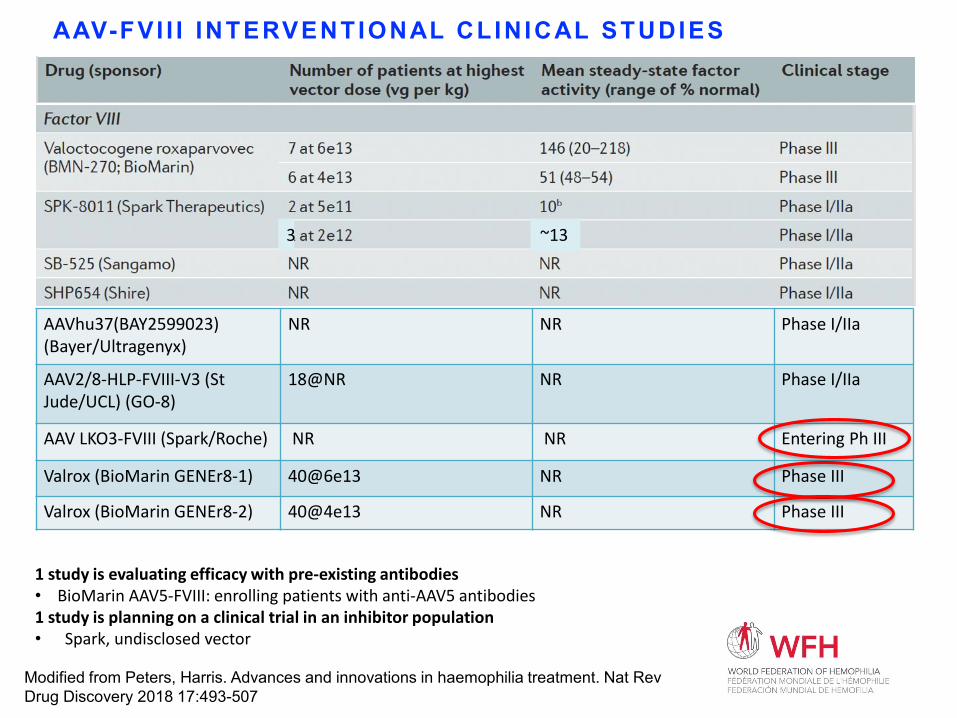
AAV-FVI I I INTERVENTIONAL CLINICAL STUDIES
AAVhu37(BAY2599023)(Bayer/Ultragenyx)
NR NR Phase I/IIa
AAV2/8-HLP-FVIII-V3 (St Jude/UCL) (GO-8)
18@NR NR Phase I/IIa
AAV LKO3-FVIII (Spark/Roche) NR NR Entering Ph III
Valrox (BioMarin GENEr8-1) 40@6e13 NR Phase III
Valrox (BioMarin GENEr8-2) 40@4e13 NR Phase III
Modified from Peters, Harris. Advances and innovations in haemophilia treatment. Nat Rev Drug Discovery 2018 17:493-507
1 study is evaluating efficacy with pre-existing antibodies• BioMarin AAV5-FVIII: enrolling patients with anti-AAV5 antibodies1 study is planning on a clinical trial in an inhibitor population• Spark, undisclosed vector
~133
AAV Vector Biology and Conundrums
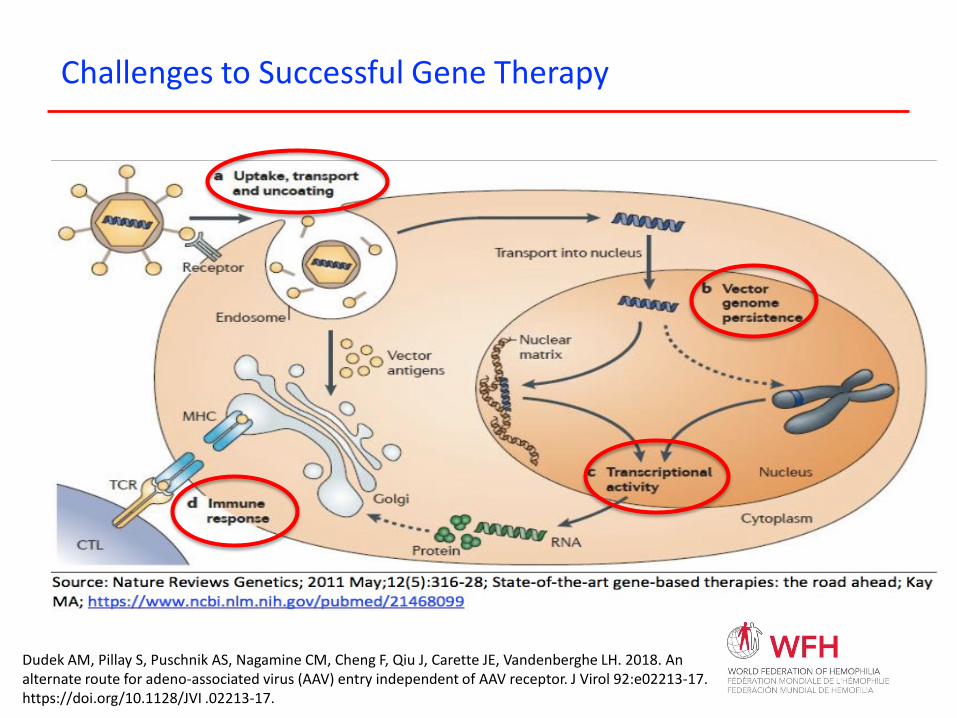
Challenges to Successful Gene Therapy
Dudek AM, Pillay S, Puschnik AS, Nagamine CM, Cheng F, Qiu J, Carette JE, Vandenberghe LH. 2018. An alternate route for adeno-associated virus (AAV) entry independent of AAV receptor. J Virol 92:e02213-17. https://doi.org/10.1128/JVI .02213-17.
WHAT ARE CAUSES OF L IVER TRANSAMINASE ELEVATIONS?
Variable but small elevations in liver transaminases in multiple AAV clinical studies in hemophilia and other diseases• First noted in Manno et al, w loss transgene expression
• Cytotoxic T-cell response to AAV capsid peptides displayed in w HLA class 1• Nathwani et al administered steroids when LFTs rose, saved some
FIX expression• Rangarajan et al: inc LFTs w/o loss of FVIII, unclear steroid benefit;
no evidence of cytotoxic T cell response• George et al: LFTs up w loss of FIX, FVIII, steroid responsive• UniQure study, LFTs up, steroid responsive w no loss of FIX
2 independent causes: Immune and intracellular toxicities?• FVIII induces ER stress and an unfolded protein response• Long term implications?
Manno Nat Med 2006; Nathwani NEJM 2011, 2014; Rangarajan NEJM 2017; George NEJM 2017; Miesbach Blood 2018; Wang and Kaufman Protein misfolding in the endoplasmic reticulum as a conduit to human disease. Nature 2016; 529:326-335
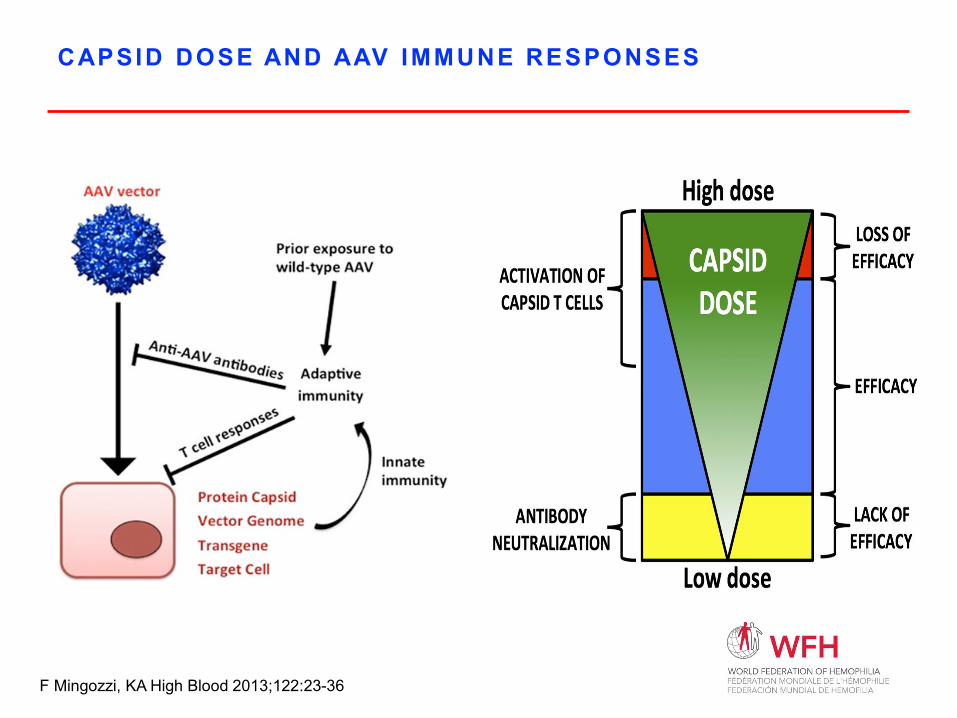
CAPSID DOSE AND AAV IMMUNE RESPONSES
F Mingozzi, KA High Blood 2013;122:23-36
AAV MEDIATED GENE THERAPY FOR HEMOPHIL IA: CONCLUSIONS AND OUTSTANDING ISSUES
KNOWN KNOWNS•SAFETYIntegrationPre-existing immunityVariable acute subclinical liver toxicity
•DOSING“High” doses needed
•MOAHeterogeneous transductionVariability in cellular protein production
•MANUFACTURINGCommercial scaling; purification and QC assays not well standardized
KNOWN UNKNOWNS• SAFETY
• Pre-existing immunity• Integration• Mild acute liver toxicity
• EFFICACY• Pediatrics?• Inhibitors?
• DURABILITY• MOA
• Opportunities to enhance transduction efficiency
AND the UNKNOWN UNKNOWNS?
Conclusions• Multiple ongoing Phase 3 clinical trials for both FVIII and FIX• Benefit/risk appears ok, huge benefit in developing world• Improvements needed from vector construction to capsid selection to in vivo delivery• Paradigm shift in treatment is coming