Embed Size (px)
Citation preview
Progress and delivery of health care in Bhutan, the Land of the
Thunder Dragon and Gross National Happiness
Tashi Tobgay1, Tandin Dorji1, Dorji Pelzom1 and Robert V. Gibbons2
1 Bhutan Ministry of Health, Thimphu, Bhutan2 United States Army Medical Command, Armed Forces Research Institute of Medical Sciences (AFRIMS), Bangkok, Thailand
Summary The Himalayan Kingdom of Bhutan is rapidly changing, but it remains relatively isolated, and it
tenaciously embraces its rich cultural heritage. Despite very limited resources, Bhutan is making a
concerted effort to update its health care and deliver it to all of its citizens. Healthcare services are
delivered through 31 hospitals, 178 basic health unit clinics and 654 outreach clinics that provide
maternal and child health services in remote communities in the mountains. Physical access to primary
health care is now well sustained for more than 90% of the population. Bhutan has made progress in key
health indicators. In the past 50 years, life expectancy increased by 18 years and infant mortality
dropped from 102.8 to 49.3 per 1000 live births between 1984 and 2008. Bhutan has a rich medical
history. One of the ancient names for Bhutan was ‘Land of Medicinal Herbs’ because of the diverse
medicinal plants it exported to neighbouring countries. In 1967, traditional medicine was included in the
National Health System, and in 1971, formal training for Drungtshos (traditional doctors) and sMenpas
(traditional compounders) began. In 1982, Bhutan established the Pharmaceutical and Research Unit,
which manufactures, develops and researches traditional herbal medicines. Despite commendable
achievements, considerable challenges lie ahead, but the advances of the past few decades bode well for
the future.
keywords Bhutan, national health programmes, delivery of health care, public health
Introduction
The Himalayan Kingdom of Bhutan is rapidly changing,
but it remains relatively isolated, and it tenaciously
embraces its rich cultural heritage. There are only one to
two flights a day at the lone airport in Paro, 60 km from
the capital city of Thimphu. There are no trains and only
three major roads that enter from India. Bhutan joined the
United Nations in 1971, tourism opened in 1974, and
television and internet arrived in 1999. After a century of
hereditary monarchy, it embarked on democracy in 2008.
Despite the changes, Bhutan is bound by its culture and
environmental ethic, visibly evident by the people wearing
traditional dress at work and in school, by small farms and
by the pristine wilderness. Like other aspects of life,
Bhutan’s health care is modernizing and at the same
maintaining strong ties to tradition.
Bhutan, also known as Druk-Yul or Land of the Thunder
Dragon, is extremely rugged and mountainous; it covers
approximately 38 394 km2 (about the size of Switzerland).
The altitude ranges from 75 m on the south-eastern border
with India to more than 7000 m in the Himalayas bordering
Tibet (Pommaret 2007). The country is divided into 20
districts. In 2005, the census counted 634 982 with popu-
lation density of approximately 16 people ⁄ km2. Although
the mountains leave only 8% of the land arable, 70% of the
people living in rural areas farm and raise livestock. In such
difficult terrain, travel and communication is a daunting
challenge. Roads and telephone networks were started in
the 1960s. As of 2009, more than 40 000 registered vehicles
ply 5363 km of roads. All districts have access to national
digital networks, and there are 149 439 mobile phone
subscribers (Bhutan National Statistics Bureau, 2009).
Bhutan’s per capita gross domestic product (GDP) was
1900 USD in 2009. Nearly half of the GDP is obtained
through selling hydroelectric power to India. Thirty per-
centage of the population live below the poverty line.
Bhutan is classified as a medium-developed country whose
human development index is 132 of 182 countries (United
Nations Development Program 2009; World Bank 2009).
Despite what is considered relative poverty, Bhutan
ranked 17th on the 2009 Happy Planet Index, ahead of
most of the developed world (White 2007; New Economics
Foundations 2009). Indeed, Bhutan may be most famous
Tropical Medicine and International Health doi:10.1111/j.1365-3156.2011.02760.x
volume 16 no 6 pp 731–736 june 2011
ª 2011 Blackwell Publishing Ltd 731

for the concept of Gross National Happiness and its four
pillars of good governance, sustainable development,
environmental conservation and preservation of culture
that guide government decisions.
In 1970, the fourth King of Bhutan, His Majesty Jigme
Singye Wangchuck, concerned about the consequences of
growth-oriented market economics and espoused the
concept, and since then, Bhutan has embraced Gross
National Happiness as its main developmental philosophy
(Ura 2009). The Centre for Bhutan Studies, mandated by
the Royal Government of Bhutan, developed the GNH
index under 9 domains: (i) psychological well-being, (ii)
time use, (iii) community vitality, (iv) culture, (v) health,
(vi) education, (vii) environmental diversity, (viii) living
standard and (ix) governance (Centre of Bhutan Studies
2008). The variables under each domain serve as a
yardstick of the developmental progress.
Bhutan is now a constitutional monarchy. In 2008, the
King introduced democracy and turned the monarchy over
to his son, the 5th King, His Majesty Jigme Khesar
Namgyel Wangchuck. The Country has been culturally
linked to Tibet since the 7th century, but when China took
control of Tibet in 1959, and after the Indo-China War in
1962, the Tibetan border was closed. Bhutan is the only
country whose official state religion is the Tantric form of
Mahayana Buddhism. Dzongkha is the official language,
but both Dzongkha and English are taught from elemen-
tary school, so English is widely spoken and used in
government. In addition, many dialects are spoken in the
different regions of the country.
Healthcare delivery
Despite very limited resources, Bhutan is making a
concerted effort to update its health care and deliver it to
all of its citizens. In 1961, Bhutan had only two hospitals,
11 dispensaries, three doctors (two Bhutanese and one
Scottish Presbyterian missionary), two nurses and 12
medicinal compounders (C.E. Taylor, unpublished obser-
vation). Bhutan became a signatory to the Alma-Ata
Declaration on Primary Health Care in 1978 (Bhutan
Ministry of Health 2009a) which affirmed health as a
fundamental human right and the attainment of the highest
possible level of health an important social goal. Since
then, Bhutan’s healthcare system has developed steadily.
Healthcare services, including referrals outside the country,
are provided at the nation’s expense. Health care is about
5.7% of the total planned budget (Gross National Happi-
ness Commission 2008), and the right to the free access to
the essential health services is anchored in the constitution.
Even visitors and tourists are provided free health care
within the kingdom should they need it.
Today, healthcare services are delivered through 31
hospitals, 178 basic health unit (BHU) clinics and 654
outreach clinics in all 20 districts and 201 subdistricts
(Table 1 and Figure 1) (Bhutan National Statistical Bureau
2005). Referral hospitals, district hospitals and BHUs refer
patients both to a higher level and back to the community
for monitoring and rehabilitative measures (Bhutan Min-
istry of Health 2009b). The national referral centre is a
350-bed hospital in Thimphu; another two regional refer-
ral hospitals are in Mongar in eastern Bhutan and in
Gelephu in the south. The national referral hospital has
most of the specialties of medicine and surgery, including
neurosurgery, and has MRI and CT scan facilities. The
regional referral hospitals have basic specialty facilities,
such as internal medicine, gynaecology and obstetrics,
paediatrics and orthopaedics. The South Asian Association
for Regional Cooperation (SAARC) Telemedicine and
Rural Telemedicine Projects was launched in April 200,
enabling consultation by the referral hospitals with tertiary
centres in India. District hospitals are built on the
backbone of one doctor, 4–5 nurses, one laboratory
technician and health assistants. These facilities have basic
diagnostic facilities comprising x-ray, complete blood
count, blood glucose levels and microscopic services for
diagnosing tuberculosis and malaria.
To make care more accessible, 178 BHUs are scattered
throughout the country. They are usually staffed with a
three health assistants who have completed 2 years of
training at the Royal Institute of Health Sciences (RIHS).
These frontline healthcare workers have been the backbone
of the primary care system in Bhutan since the inception of
modern health care (Berkeley 1979; Morris-Jones 1985).
The BHU caters to the communities for minor ailments,
assists at normal deliveries and takes care of prevention
and sanitation activities within the community. There are
no laboratory or radiological services in BHUs. Work has
begun to provide them with computers and internet
facilities and to train health workers on information
technology. To improve immunization and reduce mater-
nal and infant mortality, they organize outreach health
clinics once a month, where teams travel to remote
Table 1 Numbers of Bhutan’s healthcare facilities, doctors and
nurses
1977 1995 2000 2005 2008
Hospitals 10 26 29 29 31
BHUs 31 84 160 176 178
Doctors 52 112 109 145 171Nurses – – 443 534 567
BHU, basic health unit.
Tropical Medicine and International Health volume 16 no 6 pp 731–736 june 2011
T. Tobgay et al. Health care in Bhutan
732 ª 2011 Blackwell Publishing Ltd

communities to provide maternal and child health services.
Thus, care is delivered even to people who may find care
essentially inaccessible. Most trips to set up outreach
clinics require a few hours, but others may take a full day
or more. Each BHU has a catchment area, and there may
be two or more outreach clinics depending on the area.
Information and research
The Bhutan Health Management and Information System
(BHMIS) was established within the Ministry of Health to
keep computerized health data. Information is relayed
from the health facilities (BHUs, hospitals and referral
hospitals) through the district health office to the Ministry
of Health and entered into BHMIS. Depending upon the
information, the health facilities submit on a monthly,
quarterly, biannual or annual basis via the email or
through facsimile to the district health office, where reports
are compiled and forwarded to the MOH for entry into
BHMIS. There are many challenges in providing reliable,
credible and robust information. So far, the reliability of
the reported data has not been evaluated. Both the ministry
and the districts make little use of the data, and the
capacity of health staff to use data at the level it is
generated is poor, and many health staff are computer
illiterate. Neither the slow transfer of data does allow for
the timely reporting of outbreaks. New epidemics are
reported to the Department of Public Health by telephone
or urgent official mails by the district health office.
Research in Bhutan is still at an early stage, but there is
an interest in good research, and the first review board was
established in 2009 to review proposals for the scientific
and ethical issues. The board was quickly recognized by the
Forum for Ethical Review Committees in the Asian and
Western Pacific Region (FERCAP) and received a Federa-
tion-Wide Assurance number for the Protection of Human
Subjects for International Institutions from the United
States.
Medical education and training
The RIHS, established in 1974, is the country’s health
education institute and provides training for health assis-
tants, nurses and paramedics. In the absence of any other
health-related schools, the RIHS has been central to the
development of human resources for the Ministry of
Health for past 36 years. There are plans to upgrade the
nursing college and establish a medical college along with
other courses in public health to address the acute shortage
of human resources in Bhutan (Gross National Happiness
Commission 2008; Bhutan Ministry of Health 2009a).
Currently, there are 171 medical doctors in Bhutan who
have been mostly educated and trained in India, Bangla-
desh, Sri Lanka, Thailand, Myanmar and Nepal. As of
2008, along with these medical doctors, 567 nurses, 14
pharmacists, 10 laboratory technologists, and various
other technicians and basic health workers constituted a
total of 3414 healthcare personnel (Bhutan Ministry of
Health 2009b). To address the shortfall of healthcare
workers while they are training in foreign locations,
medical staff (mostly physicians) are recruited from
Myanmar, India and other countries. Volunteer healthcare
workers including Health Volunteers Overseas from USA
and other developed countries provide training and med-
ical services in Bhutan. Bhutan friendship associations
established in various countries also provide human
resources as well as infrastructure development and bud-
getary support.
Progress
In 2007, international consultants reviewed Bhutan’s
health sector development to assist with strategic planning
for the future (Enemark et al. 2007). They found that good
progress had been made on basic indicators, such as >90%
coverage of infant immunization, fewer low birthweight
newborns, more antenatal clinic attendance and less
dependence on external funding. The Ministry of Health
led national efforts to strengthen the training of primary
care providers and improve health information systems.
The ‘Child Health Card’, a tool to record birth date,
immunizations, medical records and growth chart, is issued
to all newborns and is especially important and effective
because the Ministry of Education requires it for school
admission (Bhutan Ministry of Health 2009b).
With the assistance from key partners such as the
Government of India, Danish International Development
Assistance, the United Nations and other government and
international agencies, Bhutan has made progress in health
indicators (Table 2). In the past 50 years, life expectancy
has risen by 18 years, and the infant mortality rate has
fallen from 102.8 to 49.3 per 1000 live births from 1984 to
2008 (World Health Organization 2009). Physical access
to primary health care is now well sustained over 90%
(Gross National Happiness Commission 2008). Through
strengthened prevention activities, Bhutan eliminated
iodine deficiency in 2003 and leprosy in 1997 (World
Health Organization 2003). The incidence of malaria and
tuberculosis has fallen: in 2008 there were only 329 cases
of malaria; in 1999 there were 12 591, and the number of
TB cases dropped from 1093 in 2004 to 921 in 2008.
Bhutan stands ahead of many countries in the WHO-
SEARO region in its efforts to reach the Millennium
Development Goals (MDG). The maternal mortality ratio
Tropical Medicine and International Health volume 16 no 6 pp 731–736 june 2011
T. Tobgay et al. Health care in Bhutan
ª 2011 Blackwell Publishing Ltd 733
per 100 000 live births is 440 for Bhutan, 830 for Nepal,
570 for Bangladesh and 450 for India. The under five-
mortality rate for Bhutan is 81 per thousand live births,
one of the lowest in the region. Bhutan also is doing better
in MDG target 6 for malaria, TB and HIV (World Health
Organization 2010).
Universal child immunization against diptheria,
pertussis, tetanus (DPT), bacillus Calmette-Guerin (BCG),
measles, rubella, polio (OPV), and hepatitis B was
achieved in 1991 (Zangpo 2009). In 2009, Bhutan also
began providing human papilloma virus vaccine to all
high-risk girls. Bhutan was a recipient of the GAVI award
for 2009, for excellence of immunization coverage and
sustaining the immunization coverage rate over 90% for
the past 5 years (Gross National Happiness Commission
2008; Pelden 2009). The Essential Drugs Program under
the Ministry of Health has been able to deliver essential
drugs, vaccines and medical equipment to all health
facilities with availability of over 90% essential drugs
throughout the year (Dorji 2007). This is achieved through
careful selection of essential drugs needed to address the
major health needs by the National Drug Committee. All
drugs are centrally procured annually and distributed
throughout the country before the rainy season. There is
functional internal mobilization of supplies within districts
and then regions to reduce under and over supplies of
medicines. Health workers and the pharmacy staff are
trained on rational use of medicines. Currently, all essential
medicines and medical equipment are procured through the
government’s budget with minimal external assistance to
reduce the donor dependency. For sustainability, a Health
Trust Fund was created in 1997; returns from its invest-
ments are used to procure essential drugs and vaccines. As
of June 2009, it has accumulated a total amount of
23.7 million USD (Bhutan Ministry of Health 2009c).
Traditional medicine
Bhutan has a rich medical history. One of the ancient
names for Bhutan was ‘Land of Medicinal Herbs’ because
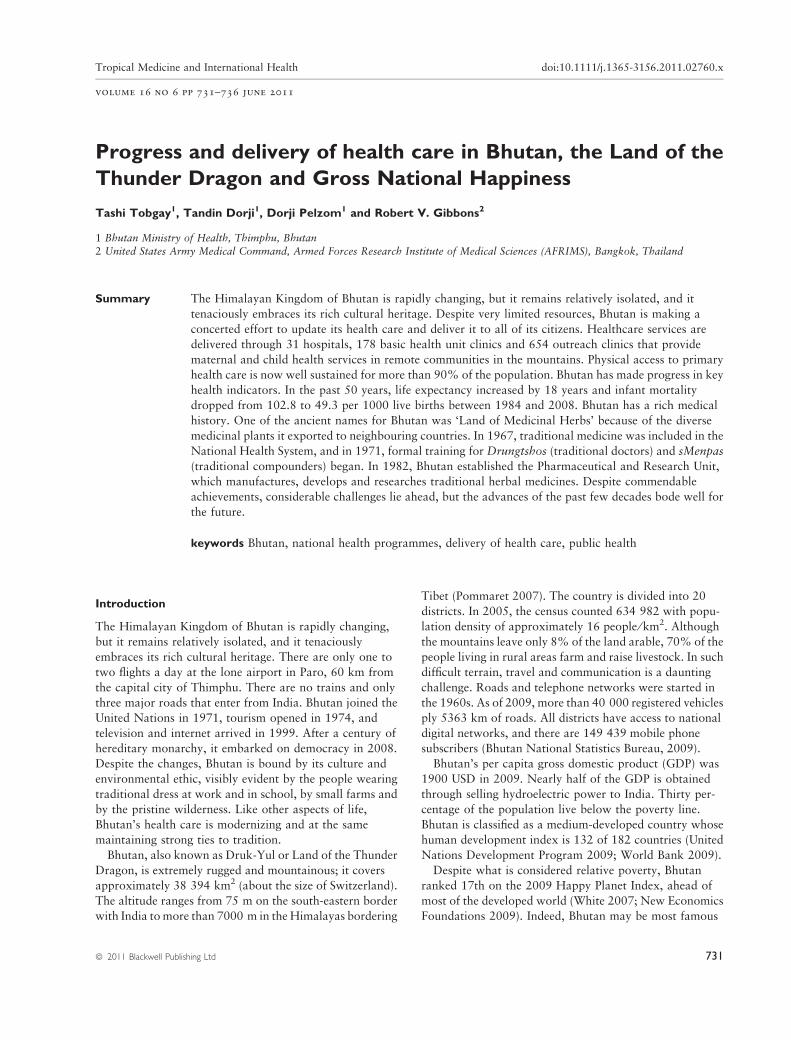
Table 2 Core demographic and health
indicators of Bhutan (Source National
Health surveys, 1984, 1994, 2000 andpopulation and housing census of Bhutan)
1984 1994 2000 2005 2008
Total fertility rate – 5.6 4.7 3.0 2.4
Population growth rate 2.6 3.1 2.5 1.3 1.3Infant mortality rate ⁄ 1000 live births 102.8 70.7 60.5 56.0 49.3
Maternal mortality ratio (per 100 000 live births) 770 380 260 440 –
Crude death rate ⁄ 1000 population 13.4 9.5 8.6 7.0 –Life expectancy – 49 66 65 66
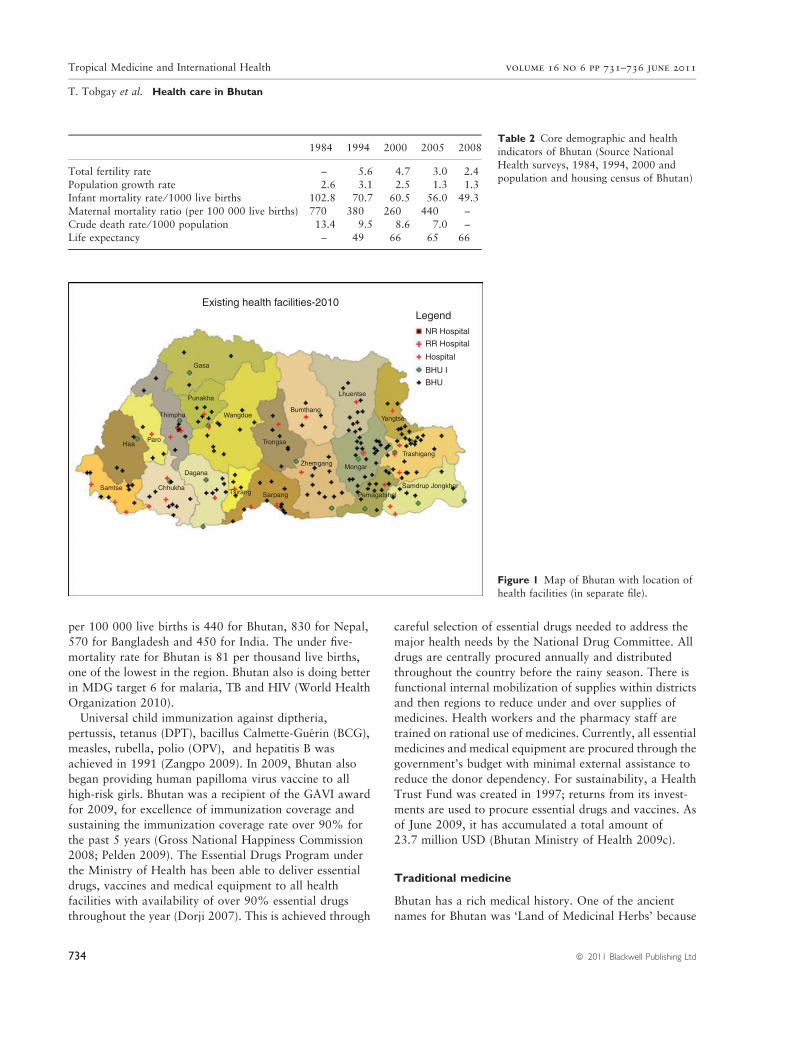
Existing health facilities-2010Legend
NR Hospital
Gasa
Punakha
Thimphu Wangdue
ParoHaa
Samtse Chhukha
Dagana
Tsirang Sarpang
Zhemgang
Trongsa
Bumthang
Mongar
PemagatshelSamdrup Jongkhar
Trashigang
Yangtse
Lhuentse
RR Hospital
Hospital
BHU I
BHU
Figure 1 Map of Bhutan with location of
health facilities (in separate file).
Tropical Medicine and International Health volume 16 no 6 pp 731–736 june 2011
T. Tobgay et al. Health care in Bhutan
734 ª 2011 Blackwell Publishing Ltd

of the diverse medicinal plants it exported to neighbouring
countries. Traditional medicine was influenced by the
Indian Ayurvedic and Chinese practices that came via Tibet
at least as far back as the 7th century. The practice includes
the theory of the three humours (bile, phlegm and wind),
the reading of pulses, herbal medicine and spiritual aspects
of healing. Uncertain composition and consistency of
herbal medicines (or supplements) and lack of functional
reporting of adverse events are of great concern (Goldman
2001; Marcus & Grollman 2002; Straus 2002). In 1982,
Bhutan established the Pharmaceutical and Research Unit
that manufactures, develops and researches traditional
herbal medicines. From more than 1000 formulations, 98
were selected for the unit to standardize and implement
quality control. The traditional medical services are well
integrated into the main healthcare system, and every
hospital has the traditional medical and modern medical
units under the same roof to enable patients to choose the
services they desire; often patients are referred between the
two services. In 1967, traditional medicine was included in
the National Health System, and in 1971, formal training
for Drungtshos (traditional doctors) and sMenpas (tradi-
tional compounders) began (Wangchuk et al. 2007). As of
2008, there are 36 Drungtshos and 54 sMenpas who are
trained at the Institute of Traditional Medicine Services in
Thimphu. In Bhutan, traditional medicine is a temporal
extension of ancient practice, but at the same time, modern
medicine is eagerly sought. This attitude allows the
venerated traditional system to collaborate with the
western medical system.
Challenges
Despite commendable achievements in primary care,
considerable challenges lie ahead. Bhutan is at the cross-
road of disease burdens from both communicable and
non-communicable diseases. Although the communicable
diseases are decreasing, cardiovascular, diabetes and men-
tal health diseases are on the rise. Development activities
such as urbanization and population migration could
create environments conducive to infectious diseases. The
widening socioeconomic gap is a growing concern, and
measures have been instituted to address land ownership,
rural income generation, education and scholarships for
rural citizens, and access to internet facilities. Such
development projects are in concordance with the princi-
ples of Bhutan’s overarching development philosophy of
Gross National Happiness which focuses on overall social,
cultural, environmental and economic developments rather
than a mere economic progress (Commission on Social
Determinants of Health (CSDH) 2008). Bhutan is extre-
mely concerned about the impact of tobacco on the health
of its citizens. The influence of Buddhism discouraged
tobacco farming and use, and tobacco control laws were in
force as early as 1729 (Ugen 2003). To our knowledge,
Bhutan is the first nation to make the sale of tobacco illegal.
The use of tobacco in public places is banned. Religious
institutions remain tobacco-free, and the majority of the
older generations abstain from using tobacco products.
Bhutan has a revered culture and medical history that
developed in relative isolation. Over the past few decades,
change has been rapid, and the government and people
strive to hold to their traditions while integrating beneficial
aspects of modern life. This is exemplified in a system that
stresses preventive measures, offers traditional and modern
health care side by side and endeavours to apply quality
standards to herbal medicine. Because of the rugged
country and sparse population, it is a challenge for Bhutan
to provide physical access to care, but great efforts are
made and priorities are set at a national level. Although
there is much progress to make, the advances of the past
few decades bode well for the future.
Acknowledgement and disclaimer
We express our gratitude to the Royal Government of
Bhutan, the Commission on Higher Education and
Ministry of Education of Thailand for their institutional
support. The opinions or assertions contained herein are
the private views of the authors and are not to be
construed as official, or as reflecting the views of the
Department of the Army, the Department of Defense or the
National Institute of Health.
References
Berkeley JS (1979) Primary medical care in Bhutan. The Journal of
the Royal College of General Practitioners 29, 530–533.
Bhutan Ministry of Health (2009a) General Synopsis and History.
Bhutan Ministry of Health, Thimphu. http://www.health.gov.bt/
healthOverview.php (accessed 17 September 2009).
Bhutan Ministry of Health (2009b) Annual Health Bulletin.
Ministry of Health, Bhutan.
Bhutan Ministry of Health (2009c) Bhutan Health Trust Fund.
http://www.health.gov.bt/bhtf/index.htm (accessed 10 October
2009).
Bhutan National Statistical Bureau (2005) Population and
Housing Census. National Statistical Bureau, Thimphu.
Bhutan National Statistics Bureau (2009) Statistical Year Book of
Bhutan 2009. National Statistics Bureau, Royal Government of
Bhutan, Thimphu.
Centre of Bhutan Studies (2008) Gross National Happiness.
Centre of Bhutan Studies, Thimphu, Bhutan.
Commission on Social Determinants of Health (CSDH) (2008)
Closing the Gap in a Generation: Health Equity Through Action
Tropical Medicine and International Health volume 16 no 6 pp 731–736 june 2011
T. Tobgay et al. Health care in Bhutan
ª 2011 Blackwell Publishing Ltd 735

on The Social Determinants of Health. Final Report of the
Commission on Social Determinants of Health. World Health
Organization, Geneva.
Dorji T (2007) Effect of TRIPS on pricing, affordability and access
to essential medicines in Bhutan. Journal of Bhutan Studies 16,
128–141.
Enemark U, Melgaard B & Sonderstrup E (2007) Health Sector
Review: Bhutan. Ministry of Health, Thimphu.
Goldman P (2001) Herbal medicines today and the roots of modern
pharmacology. Annals of Internal Medicine 135, 594–600.
Gross National Happiness Commission (2008) Tenth Five year
Plan (2008–2013). Vol I–II Main Document. Gross National
Happiness Commission, Thimphu.
Marcus DM & Grollman AP (2002) Botanical medicines – the
need for new regulations. New England Journal of Medicine
347, 2073–2076.
Morris-Jones SD (1985) Tales of the unexpected: the basic health
unit in Bhutan. British Medical Journal (Clinical Research ed.)
291, 877–878.
New Economics Foundations (2009) Happy Planet Index. http://
www.happyplanetindex.org/info/about-nef.html (accessed 10
October 2009).
Pelden S (2009) Bhutan Wins Best Immunization Award.
Kuenselonline. November 24, 2009. http://kuenselonline.com/
modules.php?name=News&file=article&sid=14050 (accessed
14 November 2010).
Pommaret F (2007) Bhutan – Himalayan Mountain Kingdom.
W.W. Norton & Company, New York.
Straus SE (2002) Herbal medicines – what’s in the bottle? New
England Journal of Medicine 347, 1997–1998.
Ugen S (2003) Bhutan: the world’s most advanced tobacco control
nation? Tobacco Control 12, 431–433.
United Nations Development Program (2009) Human Develop-
ment Reports 2009. http://hdr.undp.org/en/statistics/ (accessed
4 June 2010).
Ura K (2009) Explanation of GNH Index. http://www.
grossnationalhappiness.com/gnhIndex/intruductionGNH.aspx
(accessed 10 October 2009).
Wangchuk P, Wangchuk D & Aagaard-Hansen J (2007)
Traditional Bhutanese medicine (gSo-BA Rig-PA): an
integrated part of the formal health care services. Southeast
Asian Journal of Tropical Medicine and Public Health 38,
161–167.
White A (2007) A global projection of subjective well-being: a
challenge to positive psychology? Psychtalk 56, 17–20.
World Bank (2009) Data and Statistics. http://web.worldbank.org/
WBSITE/EXTERNAL/DATASTATISTICS/0,,contentMDK:
20421402~pagePK:64133150~piPK:64133175~theSitePK:
239419,00.html#South_Asia (accessed 10 October 2009).
World Health Organization (2003) Bhutan’s Story of
Controlling Iodine Deficiency. The Newsletter of the
South-East Asia Regional Office, World Health Organization,
Bangkok.
World Health Organization (2009) Country Profile:
Bhutan. http://www.who.int/countries/btn/en/ (accessed 4 July
2009).
World Health Organization (2010) World Health Statistics 2010.
World Health Organization, Geneva, Switzerland.
Zangpo K (2009) 30 years of Primary Health Care in Bhutan:
A Perspective. Ministry of Health, Thimphu.
Corresponding Author Robert V. Gibbons, USAMC-AFRIMS, APO AP, 96546, USA. Tel.: +66 2 644 5644; Fax: +66 2 644 4760;
E-mail: [email protected]
Tropical Medicine and International Health volume 16 no 6 pp 731–736 june 2011
T. Tobgay et al. Health care in Bhutan
736 ª 2011 Blackwell Publishing Ltd