Embed Size (px)
Citation preview

WELCOMEWELCOME


Programme1. Air Evacuation of Casualties Sqn Ldr AVK
Raju
2.Training Video: Casualty Evacuation & Life Support
IAF Presentation
3. Familiarisation: Level I Hospital, IAC II
4. Tea HQ Lawns
3

“When they take care of you like that, you don’t mind fighting”
- Wounded Army soldier on his evacuation by air
4

Air Evacuation of CasualtiesAir Evacuation of Casualties

PlanHistory and evolution of air evacuation
Aim
Aeromedical issues
System specific clinical conditions
Practical problems
Handy tips
Prioritisation
Pre flight – In flight – Post flight considerations6

History of air evacuation…1870: Aeromedical evacuation idea conceived
1910: Siege of Paris: 160 soldiers evacuated in hot air
balloon
1928: Nicaragua, first US military airlift
1929: Established air evacuation officially
1937: International Aeromedical Association- 62 nations
1936-39: Germans air evacuated soldiers
1941: USAF in WW II
1946: Helicopters used for medical air-evacuation 7

Death rate of woundedWorld War I – 8.5%
World War II – 4%
Korean War – 2%
Vietnam War – 1%
[ Aeromedical evacuation/Antibiotics/Advances in Medical Science]
8

Air EvacuationRevolutionised mode of evacuation
HelicoptersQuick access to trauma sitesLand where there are no air strips
Fixed wing aircraftsSpaciousComfortablePressurised
9

AimOvercome adverse terrain
Enable early institution of definitive treatment
Avoidance of infection
Save skilled man power
Keep morale of personnel high
Keeps communication lines free
Economy
Safety
Comfort
10

Circumstances of Casualty Evacuation
Life saving measures
Forward areas to hospitals
In between hospitals
Errands of mercy
11

Disadvantage of Aero-medical evacuation…
12
…lack of controlled environment

Aeromedical Issues in Cas evac1. Hypoxia2. Expansion of gases3. Acceleration4. Vibration5. Noise6. Humidity7. Physical requirements – space, toilets etc
13

HypoxiaDalton’s Law of Partial Pressures
“Hypoxia at altitude”
All patients must be on supplemental Oxygen regardless of their clinical condition
CVS cases/Ischaemic cases – special precautions
14

Expansion of gasesBoyle’s Law
Expansion of gases trapped within the body
Special precautions – Pneumothorax, Penetrating head or eye injury, Bowel obstruction, Ruptured Tympanic Membrane
15

Cardiovascular DiseasesSupplemental Oxygen – “Must”
Lack of Oxygen – Cardiac catastrophe/Arrythmia
AMI – ideally no air evacuation for 06 weeks (?)
CPR board
17

Respiratory SystemSupplemental OxygenObstructive Pulmonary Disease – thorough evaluationUntreated Pneumothorax – air evacuation
contraindicated in presence of respiratory embarrassment
Pulmonary Surgery – air evacuation after proper convalescence
Pneumonia – Supplemental Oxygen !
18

Blood DisordersHaemoglobin - < 7 gm%
Heamoglobin - < 8.5 gm% ‘or’ Sickle Cell Anaemia
19

Neurological ConditionsIncreased intracranial pressure –
supplemental Oxygen
Head Injury – Position of Head at towards the rear
20Acceleration

Neurological ConditionsCSF Leak through nose/ear – air evacuation
contraindicated[Suction of air/bacteria during descent of
aircraft]
Seizures – Hypoxia can trigger seizures
21

Orthopaedic casesSufficient time should have elapsed before air
evacuation
Pressure changes – soft tissue oedema - ? Vascular compromise
Air splint – avoided !
Traction equipment – possible missiles !
22

BurnsPulmonary burns to be ascertained before air
transportation
Air evacuation of patient with pulmonary burns – fatal
Pre flight Chest X-ray – mandatory
Stabilisation of patient – patency of airway, adequate ventilation, Oxygenation and fluid resuscitation
23

Gastro Intestinal CasesRecent Adbominal Surgery cases – extra care
Gas in abdomen – expansion - ? Pain/Bowel circulation compromise/ ? rupture of sutures
24

Neuro Psychiatry CasesAdequate observation prior to air
transportation
Kept adequately sedated
Availability of restraint system
25

PregnancyActive labour – only contraindication
High risk obstetric cases – safe
Placental insufficiency – supplemental Oxygen
Altitude restriction – 5000’ (abdominal gas distension)
26


Prior to any air evacuation….Ponder over the following questions:1.Is the risk to the patient being transferred
less than the risk of not being moved?2.Is the patient adequately stabilised?3.Do the benefits of the move justify the clinical
and fiscal costs?4.Is the move medically necessary or driven by
emotion or family based concern?5.Is the move based on necessity or
convenience?28

Practical problems !1. BP monitoring/checking of pulse difficult2. Auscultation is difficult3. Difficult to establish IV line4. Difficult to pass Naso Gastric tube, catheterise5. Nearly impossible to Intubate6. CPR is difficult7. Motion Sickness – vertigo/vomiting - ? Airway
compromise8. Electro Medical equipment – may interfere
with the flight instruments29
Handy tips...1. Electronic BP and HR monitor2. 2 x wide bore IV canulas in place, syringes
filled with drugs3. If needed, Intubate with ET tube before the
sortie4. NG tube, catheterisation pre flight procedure5. All catheters to be filled with Normal Saline6. For Air Sickness: Tab of Cinnarizine – 30 min
before air evacuation sortie & low flow Oxygen
7. Tab Pseudoephidrine/Vasoconstrictor Nasal Drops – prevents Otitic Barotrauma
8. CPR board9. Humidified Oxygen
30
Relative contraindicationsInfectious diseases
Moribund patient
Offensive patient
Decompression sickness
31

Priorities of evacuationPriority 1. Patient whose transfer by quickest
means is necessary as a life saving measure or to avoid serious permanent disability
Priority 2. Patient whose condition is likely to be adversely affected unless they are speedily evacuated or who need early specialized treatment
Priority 3. Patients whose immediate treatment are with in the powers of local medical units, but whose progress would benefit from movement by air rather than by surface transport
Priority 4. Patients for whom movement by air is a matter of convenience rather than a medical requirement
32

Preflight Procedures‘Understand the case well’
Briefing of pilot & crew1. Height limitations required 2. Intermediate stops3. Precaution in transfer of special cases4.The aircraft for use for Evacuation should
be fitted with proper equipment.5. Communication facilities with departure
intermediate & destination air field6. Captain of aircraft in charge of over all
discipline 33
InflightFluid management
Oxygen/ IV line management
Medicines intake
Brief cabin/ aircrew for any changes from planned
Prevent exacerbation deterioration in clinical condition
Manage emergencies
34

Post flightMake a note of problems encountered
Brief the Hospital who are receiving the patient
Brief the Hospital who have demanded air evacuation
Share your experiences and suggestions on ‘Lotus’
35

Mi - 17

Stretcher Spinal BoardOrtho Scoop stretcher + splints
Resuscitation equipment including
Oxygen Apparatus
Suction Apparatus
Physiological Monitor & Defibrillator
IV Fluids
Doctor’s Bag
Oxygen Mask
Urine/Vomitus/Stool Receptacles can be kept under the seats
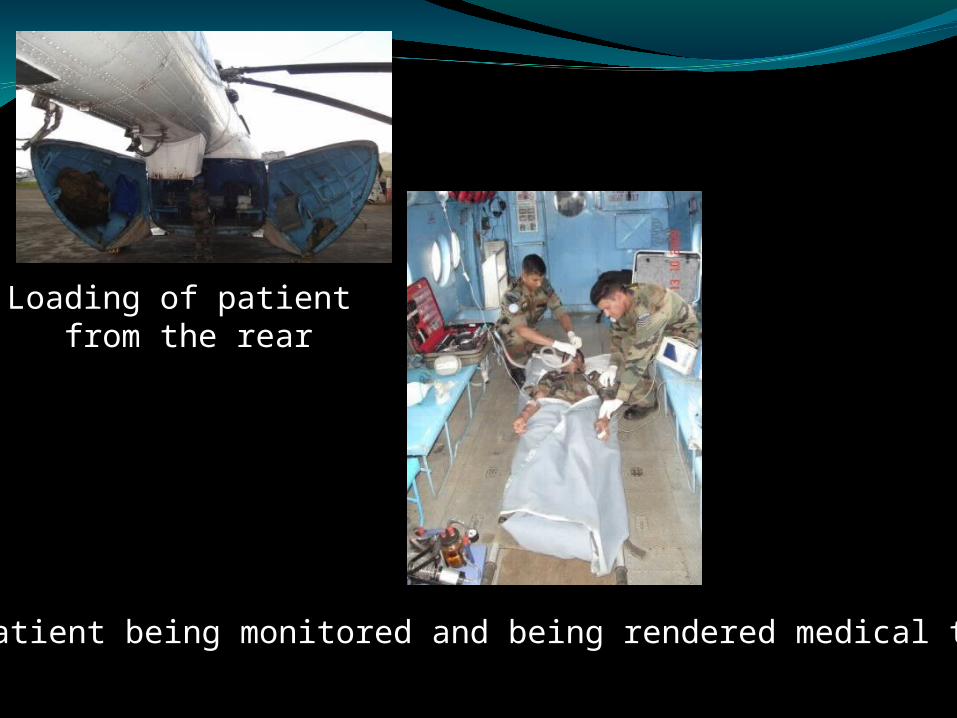
Patient being monitored and being rendered medical treatment
Loading of patient from the rear

Mass Casualties: Modification 12 Lying Patients

To summarise…. Special precautions
I. Condition susceptible to pressure change1. CNS
Air in CNS due to surgery or trauma, CSF Rhinorrhoea
2. Eye- Perforating Injury
3. EarASOM/ Mastoiditis/ Eustachian tube stenosis, Sinusitis
4. Respiratory SystemPneumothorax/ Mediastinal Emphysema/ Sucking Wounds/ Open case of TB 40

5. GITHernias/ Gangrenous Appendicitis/ Penetrating Perforating Wounds/ Post Operative Cases/ Colostomies/ Liver Abscess
6. SkinGas Gangrene/ Subcutaneous Emphysema
7. Maxillofacial injuriesTill wires are removed
8. Decompression sickness
41

Cases requiring special attentionII.Condition susceptible to hypoxia1. CNS
Head injury & epilepsy
2. EyeOcular injuries/ Post Surgical Cases/ Glaucomatous Eye
3. RS Reduced vital capacity/ Pulmonary HT/Pul surgery
4. CVSAngina/ MI/ HT/ CCF/ Cardiac arrhythmiaRequire supplemental oxygen
5. BloodAnemia less than 7 gm% 42
Remember......Murphy’s Law: “If anything has to
go wrong, it will go wrong”
“If you are prepared for the worst..the worst seldom happens;
If not prepared….the worst is guaranteed to happen”
43































