Embed Size (px)
Citation preview
P R O G R A M S Y L L A B U S
A CME-certified Oncology Exchange Activity

Challenges in Treating Renal Cell Carcinoma in the Community A Grand Rounds Series
Program #9989 A CME-certified Oncology Exchange Activity Page 2
TABLE OF CONTENTS Program Content and Format ..................................................... Page 3
Target Audience/Learning Objectives ......................................... Page 4
CME Statements ........................................................................ Page 4-5
Disclosures ................................................................................. Page 5
Steering Committee ................................................................... Pages 6-7
Program Slides ......................................................................... Page 8

Challenges in Treating Renal Cell Carcinoma in the Community A Grand Rounds Series
Program #9989 A CME-certified Oncology Exchange Activity Page 3
PROGRAM CONTENT AND FORMAT Community oncologists who treat patients with renal cell carcinoma (RCC) are constantly challenged to stay up to date with recently approved agents, emerging data from ongoing studies of novel investigational regimens, and evolving standards of care for RCC. Challenged by the lack of consensus surrounding treatment selection for patients with RCC, community oncologists need access to new information, tools, and insights, which they can integrate into their practices to improve patient outcomes. This engaging program will educate community oncologists on emerging data from ongoing studies in RCC and provide guidance on optimal treatment selection and management of treatment-related adverse effects in patients with RCC. Visit www.OncExchange.com for more information.

Challenges in Treating Renal Cell Carcinoma in the Community A Grand Rounds Series
Program #9989 A CME-certified Oncology Exchange Activity Page 4
TARGET AUDIENCE This activity is intended for community oncologists and other clinicians who are actively involved in the care of patients with renal cell carcinoma.
EDUCATIONAL OBJECTIVES
At the conclusion of this activity, participants should be able to demonstrate the ability to: • Compare the various treatment options available and choose the optimal treatment
based on patient characteristics and emerging data from clinical studies of patients with advanced RCC
• Discuss strategies for the management of side effects associated with the therapies for advanced RCC
• Review sequential and combination treatment strategies for patients with advanced RCC • Identify key investigational regimens for advanced RCC from ongoing clinical studies
ACCREDITATION
This activity has been planned and implemented in accordance with the Essential Areas and policies of the Accreditation Council for Continuing Medical Education through the joint sponsorship of Potomac Center for Medical Education and Rockpointe Oncology. The Potomac Center for Medical Education is accredited by the ACCME to provide continuing medical education for physicians.
CME CREDIT
The Potomac Center for Medical Education designates this live activity for a maximum of 1.0 AMA PRA Category I credit(s)TM. Physicians should claim only the credit commensurate with the extent of their participation in the activity.
For information about the accreditation of this program, please email [email protected].
SPECIAL SERVICES
Event staff will be glad to assist you with any special needs (e.g. physical, dietary, etc.).
FEE AND RECEIVING CME CREDIT
There is no fee for this educational activity. To receive CME credit the participant must: • Participate in this one-hour-long program in its entirety; • Sign in / sign out on the sheet provided by the host coordinator; • Complete and sign the registration and evaluation form; and • Return the registration and completed evaluation form to the host coordinator.

Challenges in Treating Renal Cell Carcinoma in the Community A Grand Rounds Series
Program #9989 A CME-certified Oncology Exchange Activity Page 5
DISCLOSURE STATEMENT Potomac Center for Medical Education (PCME) adheres to the policies and guidelines, including the Standards for Commercial Support, set forth to providers by the Accreditation Council for Continuing Medical Education (ACCME) and all other professional organizations, as applicable, stating those activities where continuing education credits are awarded must be balanced, independent, objective, and scientifically rigorous. All persons in a position to control the content of a continuing medical education program sponsored by the Potomac Center for Medical Education are required to disclose any relevant financial relationships with any commercial interest to PCME as well as to learners. All conflicts are identified and resolved by PCME in accordance with the Standards for Commercial Support in advance of delivery of the activity to learners. The content of this activity was vetted by an external medical reviewer to assure objectivity and that the activity is free of commercial bias.
PROGRAM DISCLOSURES The faculty/steering committee reported the following relevant financial relationships that they or their spouse/partner have with commercial interests:
Steering Committee:
Robert A. Figlin, MD, FACP: Research Funding: Argos, Bristol-Myers Squibb, Immatics, Novartis; Scientific Advisory Board: Onyx, Pfizer Brian I. Rini, MD, FACP: Advisor: Aveo, Bristol-Myers Squibb, GlaxoSmithKline, Pfizer; Primary Investigator: GlaxoSmithKline, Pfizer
Non-faculty Content Contributors:
Non-faculty content contributors and/or reviewers reported the following relevant financial relationships that they or their spouse/partner have with commercial interests: Latha Shivakumar, PhD; Blair St. Amand; Jay Katz, CCMEP; CME Peer Review: Nothing to disclose
FDA DISCLOSURE
The contents of some CME/CE activities may contain discussions of non-approved or off-label uses of some agents mentioned. Please consult the prescribing information for full disclosure of approved uses.

Challenges in Treating Renal Cell Carcinoma in the Community A Grand Rounds Series
Program #9989 A CME-certified Oncology Exchange Activity Page 6
STEERING COMMITTEE
Robert A. Figlin, MD, FACP Steven Spielberg Family Chair in Hematology/Oncology Professor of Medicine and Biomedical Sciences Director, Division of Hematology/Oncology Deputy Director, Samuel Oschin Comprehensive Cancer Institute Cedars-Sinai Medical Center Los Angeles, CA
Robert A. Figlin, MD, FACP is the Steven Spielberg Family Chair in Hematology/Oncology, a Professor of Medicine and Biomedical Sciences, the Director of the Division of Hematology/Oncology, and the Deputy Director of the Samuel Oschin Comprehensive Cancer Institute, all at Cedars-Sinai Medical Center in Los Angeles, CA. Dr. Figlin received his medical degree from the Medical College of Pennsylvania, then completed his residency and chief residency in internal medicine at Cedars-Sinai Medical Center and a fellowship in hematology/oncology at the David Geffen School of Medicine at UCLA. He is an Emeritus Professor of Medicine and Urology at the David Geffen School of Medicine at UCLA. Prior to joining Cedars-Sinai, Dr. Figlin was the Arthur and Rosalie Kaplan Endowed Chair of the Department of Medical Oncology and Therapeutics Research, and the Associate Director for Clinical Research at the City of Hope Comprehensive Cancer Center. Prior to that, Dr. Figlin served as the Henry Alvin and Carrie L. Meinhardt Endowed Chair in Urologic Oncology and Professor of Medicine and Urology in the Divisions of Hematology/Oncology and Urologic Oncology at the David Geffen School of Medicine at UCLA. Dr Figlin joined the UCLA faculty as Assistant Professor of Medicine in the Division of Hematology/Oncology and was appointed Co-director of the Jonsson Comprehensive Cancer Center’s Oncology Program. He also held the post of Medical Director of the Thoracic and Genitourinary Oncology Program in the Departments of Medicine, Surgery, and Urology, and served as Program Director of Solid Tumor Developmental Therapeutics within the Cancer Center. Dr. Figlin serves as Editor for Kidney Cancer Journal, and his studies have appeared in Clinical Cancer Research, Journal of Clinical Oncology, New England Journal of Medicine, Lancet, JNCI, Lancet Oncology, and Journal of Urology, among others. He has authored more than 300 peer-reviewed articles, more than 60 book chapters, and has published multiple books in kidney cancer. He is the Editor of the recently released book, Renal Cell Carcinoma: Translational Biology, Personalized Medicine, and Novel Therapeutic Targets. A nationally recognized leader in genitourinary and thoracic oncology, Dr. Figlin’s research focuses on renal cell carcinoma and thoracic malignancies. He established and directs the Kidney Cancer Program at Cedars-Sinai Medical Center, which aims to understand the biology of kidney cancer and translate that knowledge into novel treatment approaches.

Challenges in Treating Renal Cell Carcinoma in the Community A Grand Rounds Series
Program #9989 A CME-certified Oncology Exchange Activity Page 7
STEERING COMMITTEE
Brian I. Rini, MD, FACP Professor of Medicine, Lerner College of Medicine Department of Solid Tumor Oncology Cleveland Clinic Taussig Cancer Institute Glickman Urological Institute Cleveland, OH
Brian I. Rini, MD, FACP is a Professor of Medicine at the Cleveland Clinic Lerner College of Medicine of Case Western Reserve University in Cleveland, OH. A staff member of the Department of Solid Tumor Oncology and Co-leader of the Genitourinary Program of the CASE Comprehensive Cancer Center, Dr. Rini’s work focuses on genitourinary malignancies. Dr. Rini earned his medical degree at the Ohio State University College of Medicine. Dr. Rini completed a residency program in internal medicine and a fellowship in hematology/oncology at University of Chicago Hospitals. Dr. Rini was an Assistant Professor at the University of California San Francisco before moving to the Cleveland Clinic. Dr. Rini’s primary research has been in renal cell carcinoma (RCC) and prostate cancer, with special focus on antiangiogenic therapy and immunotherapy. Dr. Rini has been involved in the initial and ongoing development of targeted agents for metastatic RCC, and was an integral investigator in the clinical development of several agents which are now FDA approved. Dr. Rini was the Principal Investigator of an international phase III cooperative group trial of bevacizumab plus interferon and the PI of the phase III axitinib trial in metastatic RCC that lead to FDA approval, and is currently the PI of several global phase III trials in RCC. Dr. Rini’s research has been published in numerous peer-reviewed journals, such as Journal of the National Cancer Institute, Journal of Clinical Oncology, Cancer, Lancet, and JAMA. He is a member of the editorial board of Journal of Clinical Oncology and Co-chair of the NCI RCC Task Force.

CHALLENGESINTREATINGRENALCELLCARCINOMAINTHECOMMUNITY
©2013PCME Page8
A CME-certified Oncology Exchange ActivityA CME-certified Oncology Exchange Activity
This activity is supported by educational grants fromAstellas Scientific and Medical Affairs, AVEO Oncology, and Novartis Oncology.
Jointly sponsored byPotomac Center for Medical Education and Rockpointe Oncology.
DisclosuresAll relevant financial relationships with commercial interests reported by faculty speakers, steering committee members, non-faculty content contributors and/or reviewers, or their spouses/partners have been listed on page 5 of your program syllabus.
Off-label Discussion DisclosureThis educational activity may contain discussion of published and/or investigational uses of agents that are not indicated by the Food and Drug Administration. PCME does not recommend the use of any agent outside of the labeled indications. Please refer to the official prescribing information for each product for discussion of approved indications, contraindications and warnings. The opinions expressed are those of the presenters and are not to be construed as those of the publisher or grantors.
Educational Objectives
At the conclusion of this activity, participants should be able to demonstrate the ability to:
• Compare the various treatment options available and choose the optimal treatment based on patient characteristics and emerging data from clinical studies of patients with advanced RCC data from clinical studies of patients with advanced RCC
• Discuss strategies for the management of side effects associated with the therapies for advanced RCC
• Review sequential and combination treatment strategies for patients with advanced RCC
• Identify key investigational regimens for advanced RCC from ongoing clinical studies
Renal Cell Carcinoma
FH = fumarate hydratase; LOH = loss of heterozygosity; VHL = von Hippel-Lindau
DeVita VT et al, eds. Cancer: Principles and Practice of Oncology. 7th ed. Philadelphia, PA: Lippincott Williams & Wilkins; 2005:1142.
Signaling Pathways and Selective Inhibitors in RCC
VEGFR
VEGF
VEGFBevacizumab
EC
Growth factor receptor
Growth factor(e.g. PDGF, TGF-α, EGF)
Tumor cell
EC=endothelial cell; EGF=epidermal growth factor; MAPK=mitogen-activated protein kinase; mTOR=mammalian target of rapamycin; TGF=transforming growth factor; VEGFR=VEGF receptor.
Garcia. CA Cancer J Clin. 2007;57:112; Patel. Br J Cancer. 2006;94:614; Motzer. J Clin Oncol. 2006;24:5601; Sonpavde. Curr Oncol Rep. 2007;9:115; Hu-Lowe. Clin Cancer Res. 2008;14:7272; Kay. ASCO GU. 2009 (abstr 278); US National Institutes of Health website. http://clinicaltrials.gov/ct2/show/NCT00836927. Accessed 10/13/09.
↑ HIF1-α expression
Sorafenib Sunitinib
PazopanibAxitinib
TivozanibCediranibDovitinibVascular
permeability EC migration
TemsirolimusEverolimus
Ridaforolimus (Deforolimus)
Akt
PI3K
MAPK
Raf
MEK
Erk
P
P P
P
EC survival
EC proliferation
Sorafenib Akt
PI3K Raf
MEK
Erk
P
P P
P
mTOR
Tumor cell proliferation
CediranibDovitinibErlotinib
Patients with mRCC are Heterogeneous
Need no Predict risk of recurrence?
Previously untreated metastatic disease
Long-term responders
25%
Need no therapy
15% Primary refractory
15%Partial
responders20-40%
Toxicities15%
Choose appropriate therapy?
Predict risk of recurrence?
Avoid toxicity?
Modified from: Srinivas S. Presented at: ASCO 2011 Education session.

CHALLENGESINTREATINGRENALCELLCARCINOMAINTHECOMMUNITY
©2013PCME Page9
Management of mRCC: Strategies for today
• How can we optimise outcomes with current therapies in the treatment of mRCC?
I d ti t
Strategies for today
M lti l t t d Eff ti th Improved patient outcomes
Multiple targetedagents
Effective therapy management
Adverse event management
Maximize treatment duration
Dose optimization
Management of mRCC Strategies for Today and Tomorrow
How can we achieve our goal of long-term survival in mRCC?
Goal
Strategies for tomorrow
Challenge Potential solutions
Sequencing and combination of agents
Appropriate treatment selection
Individualization of treatment
Resistance to current agents
Novel agents
Long-term survival
Biomarkers
Adverse-event Management
• Patient education about potential adverse events
• Assess and stabilize baseline comorbidities
Prior to treatment
During treatment
• Monitor patients frequently
• Prompt adverse event management- Standard medical intervention
- Consider dose reductions/ interruptions
Schmidinger M et al. Cancer Invest. 2010;28:856-864.
Current State of RCC Therapy in 2013
• Explosion of choices in the last 7 years• 8 FDA-approved agents• 3 classes of drugs• Slowing of disease• Prolongation of life
• Immunotherapy– IL-2– IFN-α
• mTor Inhibitors– Temsirolimus– Everolimus
* Not FDA approved
NCCN Guidelines: Kidney Cancer v1.2013. www.nccn.org.
VEGF Inhibitors- Sunitinib- Sorafenib- Pazopanib- Axitinib - Bevacizumab + IFN-α- Tivozanib*
Potential Prognostic/Predictive Markers in RCC
• Hypertension (sunitinib, bevacizumab, and axitinib therapy)
• VEGF expression (TARGET trial; sorafenib therapy)
• HIF2 (sunitinib therapy)
VHL t t (VEGF t t d th )• VHL status (VEGF-targeted therapy)
• HFS (sunitinib therapy)
• Asthenia and fatigue (sunitinib therapy)
Rini. J Natl Cancer Inst. 2011;103:763. Rixe. ASCO. 2009 (abstr 5045). Escudier. J Clin Oncol. 2009;20:3312. Patel. ASCO. 2008 (abstr 5008).Choueiri. J Urol. 2008;3:860. Hutson. ASCO. 2008 (abstr 5046).Michaelson. ASCO GU. 2011 (abstr 320). Davis. ESMO. 2011 (abstr 1139).
Biomarker in RCC
Hypoxia-inducible factors/
angiogenesis
Regulators of apoptosis/
growth
Regulators of cell cycle
Regulator of T/dendritic cell
activity
Adhesion molecules
HIF-1 alpha P53 P27 B7H1 EpCAM
CA IX Bcl-2 pTEN B7H4 EphA2
VHL alteration Survivin PD1 Vascular-Cell VHL alteration (mutation/
methylation)
Survivin PD1 Vascular-Cell Adhesion
Molecule-1
VEGF and VEGF-receptors, CAIX
Smac/DIABLO B7H3
IMP3
Choueiri TK. Prognostic factors in metastatic renal cell carcinoma. In: Rini and Campbell, 2009.
Tumor/Host Single genes/Signatures DNA/RNA/miRNA/proteins

CHALLENGESINTREATINGRENALCELLCARCINOMAINTHECOMMUNITY
©2013PCME Page10
Risk Factor Criteria for Advanced RCC
Parameters
Karnofsky PS <80%
Time from diagnosis to treatment <12 mos
Hemoglobin <LLN
Risk Level Number of Factors
Favorable 0
Intermediate 1-2
Heng. J Clin Oncol. 2009;27:5794.
Calcium >ULN
Neutrophil count >ULN
Platelet count >ULN
LLN = lower limit of normal; ULN = upper limit of normal
Intermediate 1 2
Poor ≥3
Therapy ManagementAdverse Event Management
Key adverse events associated with targeted agents
VEGFR-targeted therapy mTOR inhibitors
Fatigue/astheniaSkin toxicities
Gastrointestinal symptomsStomatitis
Hypertension
Metabolic abnormalities (e.g. hyperglycaemia)
Fatigue/astheniaRash
AnemiaPneumonitis (rarely)
Motzer RJ et al. N Engl J Med. 2007;356:115-124. Escudier B et al. N Engl J Med. 2007;356:125-134. Escudier B et al. Lancet. 2007;370:2103-2111. Rini B et al. J Clin Oncol. 2008;26:3743-3748. Hudes G et al. N Engl J Med. 2007;356:2271-2281. Sternberg C et al. J Clin Oncol. 2010;28:1061-1068.Motzer RJ et al. Lancet. 2008;372:449-456. Schmidinger M, Bellmunt J. Cancer Treat Rev. 2010;36:416-424.
Common Adverse Events
Adverse Event Bevacizumab Sunitinib Sorafenib Pazopanib Temsirolimus Everolimus
Fatigue ++ +++ ++ + + ++
Rash - + ++ - +++ ++
Hand-foot syndrome - + ++ - - -
Hypertension + + + + -
Diarrhea + ++ ++ ++ + +
Stomatitis - ++ + - ++ ++
Myelosuppression - ++ - + + +
Metabolic syndrome - - - ++ ++ ++
Epistaxis/bleeding + - - -
Proteinuria ++ + + + - -
Prescribing information: Avastin (2013), Sutent, Nexavar, Votrient, Torisel, Afinitor (2012).
Case Discussion
• 52-year-old male, PS 0, Weight 102 kg, Height 180 cm, BP 130/78, pulse 82, resp rate 16
• Presenting symptoms: Left rib pain – 3 weeks duration, onset after playing touch football, minimal pain relief with ibuprofen
• PMH: hypertension, hyperlipidemia
• Meds: HCTZ 25 mg qd, atorvastatin 20 mg qd
• ROS: non-contributory
• CXR was obtained to rule out rib fracture and revealed lytic lesion, left fourth rib and numerous bilateral pulmonary nodules
• F/U CT scan recommended
• CT chest, abdomen, and pelvis performed– 8 cm mass, upper pole left kidney– Multiple bilateral pulmonary nodules suspicious for metastatic disease– Largest = 2.4 cm x 1.8 cm
Case Discussion
• Referred to urologist • Underwent laparoscopic nephrectomy• Pathology
– Revealed tumor extension into renal vein with invasion of left adrenal gland (T3a)of left adrenal gland (T3a)
– Lymph nodes negative (N0)– Tumor stage: T3aN0M1– Histology: clear cell– Fuhrman Grade 3
• Referred to medical oncologist for discussion of treatment options
What is the Optimal Treatment Choice for this Newly Diagnosed Patient with Metastatic Renal Cell Carcinoma? (choose all that apply)
1. Initiate radiation therapy for minimally symptomatic disease
2. Assessment of prognostic variables and comorbidities and initiate VEGF targeted therapy
3. Referral to an IRB-approved clinical trial
4. Initiate combination targeted therapy outside of a clinical trial
5. Screen for the presence of a VHL mutation

CHALLENGESINTREATINGRENALCELLCARCINOMAINTHECOMMUNITY
©2013PCME Page11
What Treatment Options are Reasonable in the Frontline Setting in Patients with Metastatic Disease and Intermediate Risk?
1. Bevacizumab plus interferon
2. Pazopanib
3. Temsirolimus
4. Everolimus
5. Sunitinib
6. Interleukin 2, high dose
NCCN Guidelines First-line Therapy for Clear Cell RCC
a Category 1. b Category 1 for poor-prognosis pts; category 2B for selected pts of other risk groups. c Category 2A for pts with excellent PS and normal organ function.
+Best Supportive Care
NCCN Guidelines: Kidney Cancer v1.2013. www.nccn.org.
NCCN GuidelinesSystemic Therapy for Non-clear Cell Histology
a Preferred. b Category 1 for poor-prognosis pts; category 2A for other risk groups. c Category 3.
+Best Supportive Care
Axitinibc
NCCN Guidelines: Kidney Cancer v1.2013. www.nccn.org.
Firstline Therapy
PFS: 11 vs 5 mo. PFS: 9.2 vs 4.2 mo.PFS: 10.2 vs 5.4 mo.
Pazopanib vs BSCBevacizumab + IFN-αSunitinib vs IFN-α
Temsirolimus vs IFN Ti o anib s Sorafenib
Motzer RJ et al. J Clin Oncol. 2007;25:3958-3964. Escudier B et al. Lancet. 2007;370:2103-2111.Sternberg C et al. J Clin Oncol. 2010;28:1061-1068. Rini BI at el. Lancet. 2009;373:1119-1132. Motzer RJ et al. J Clin Oncol. 2012;30:1371-1377.
Temsirolimus vs IFN Tivozanib vs Sorafenib
Temsirolimus1-3 Sunitinib4 Bev + IFN-α1.5,6 Pazopanib7,8 Tivozanib
Patient Population Poor risk Tx naive Tx naive Tx naive Tx naive
Comparator IFNα IFNα IFNα placebo Sorafenib
ORR, % 8.6 47 31/25.5* 32 33
Summary Firstline Therapy in mRCC
,(vs comparator) (vs 4.8) (vs 12) (vs 12/13.1) (vs 3) (vs 23)
PFS, mos
(vs comparator)
5.5(vs 3.1)
11 (vs 5)
10.2/8.4*(vs 5.4/5.2)
11.1(vs 2.8)
12.7(vs 9.1)
OS, mos(vs comparator)
10.9(vs 7.3)
26.4(vs 21.8)
23.3/18.3*(vs 21.3/17.4)
22.9(vs 23.5) NR
1. Escudier et al. J Clin Oncol. 2009;27:3312-3318.2. Nexavar® (sorafenib) Prescribing information, 2012.3. Hudes et al. N Engl J Med. 2007;356:2271-2281. 4. Motzer et al. J Clin Oncol. 2009;27:3584-3590.5. Escudier et al. J Clin Oncol. 2010;28::2144-2150. 6. Rini et al. J Clin Oncol. 2010; 28:2137-2143.
Effective Therapy Management
Dosing
Treatment Duration
Optimum Efficacy
Adverse Event Management
Ravaud A. Ann Oncol. 2009;20:i7-i12.
CHALLENGESINTREATINGRENALCELLCARCINOMAINTHECOMMUNITY
©2013PCME Page12
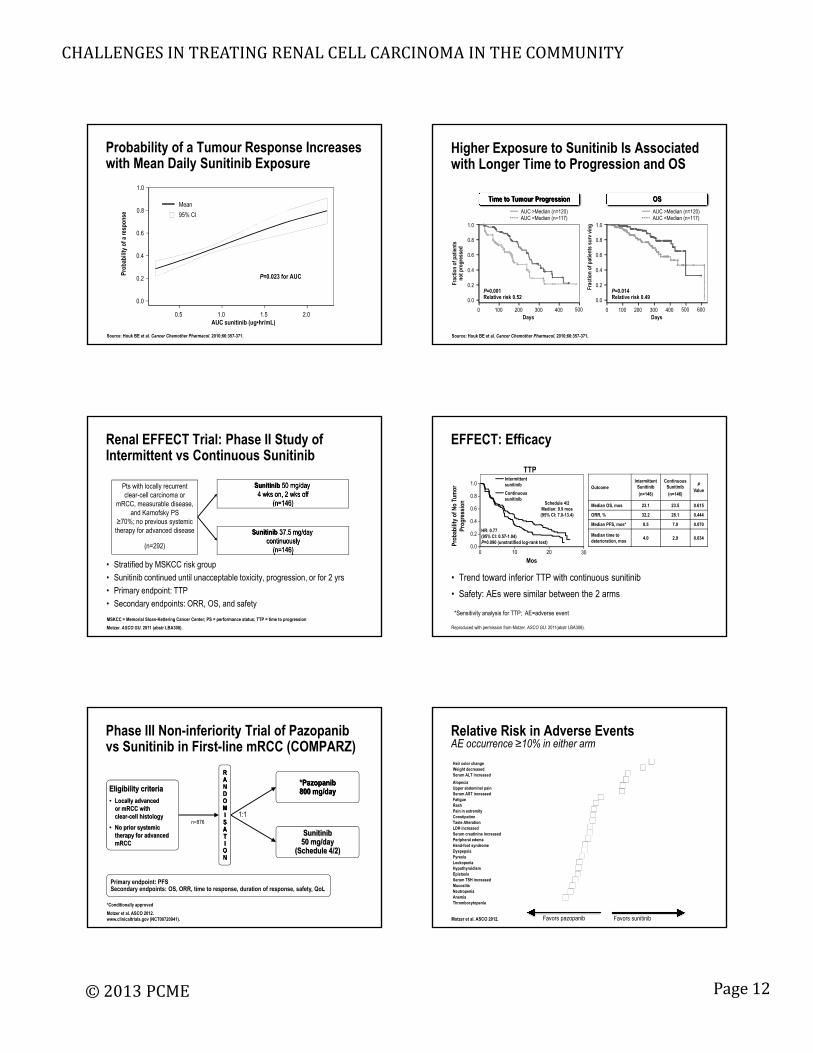
Probability of a Tumour Response Increases with Mean Daily Sunitinib Exposure
resp
onse
0 6
0.8
1.0
Mean
95% CI
P=0.023 for AUC
AUC sunitinib (ug•hr/mL)
Prob
abili
ty o
f a r
0.5 1.0 1.5 2.0
0.0
0.2
0.4
0.6
Source: Houk BE et al. Cancer Chemother Pharmacol. 2010;66:357-371.
Higher Exposure to Sunitinib Is Associated with Longer Time to Progression and OS
1.0
ivin
g 1.0
AUC >Median (n=120)AUC <Median (n=117)
AUC >Median (n=120)AUC <Median (n=117)
Time to Tumour Progression OS
Source: Houk BE et al. Cancer Chemother Pharmacol. 2010;66:357-371.
P=0.014Relative risk 0.49
P=0.001Relative risk 0.52
Days
Frac
tion
of p
atie
nts
not p
rogr
esse
d
0 100 200 300 400 500
0.0
0.2
0.4
0.6
0.8
Days
Frac
tion
of p
atie
nts
surv
0 100 200 300 400 500
0.0
0.2
0.4
0.6
0.8
600
Renal EFFECT Trial: Phase II Study of Intermittent vs Continuous Sunitinib
Pts with locally recurrent clear-cell carcinoma or
mRCC, measurable disease, and Karnofsky PS
≥70%; no previous systemic
Sunitinib 50 mg/day 4 wks on, 2 wks off
(n=146)
• Stratified by MSKCC risk group
• Sunitinib continued until unacceptable toxicity, progression, or for 2 yrs
• Primary endpoint: TTP
• Secondary endpoints: ORR, OS, and safety
therapy for advanced disease
(n=292)
Sunitinib 37.5 mg/day continuously
(n=146)
Motzer. ASCO GU. 2011 (abstr LBA308).
MSKCC = Memorial Sloan-Kettering Cancer Center; PS = performance status; TTP = time to progression
EFFECT: Efficacy
OutcomeIntermittent
Sunitinib
(n=146)
Continuous Sunitinib
(n=146)
PValue
Median OS, mos 23.1 23.5 0.615
ORR, % 32.2 28.1 0.444
Median PFS, mos* 8.5 7.0 0.070
TTP
lity
of N
o Tu
mor
ro
gres
sion
1.0
0.8
0.6
0.4
Schedule 4/2 Median: 9.9 mos(95% CI: 7.0-13.4)
Intermittent sunitinib
Continuous sunitinib
• Trend toward inferior TTP with continuous sunitinib
• Safety: AEs were similar between the 2 arms
Reproduced with permission from Motzer. ASCO GU. 2011(abstr LBA308).
,
Median time to deterioration, mos
4.0 2.9 0.034
*Sensitivity analysis for TTP; AE=adverse event
Prob
abi
Pr
0.2
0.00 10 20
Mos
HR: 0.77(95% CI: 0.57-1.04)P=0.090 (unstratified log-rank test)
30
Phase III Non-inferiority Trial of Pazopanibvs Sunitinib in First-line mRCC (COMPARZ)
*Pazopanib 800 mg/dayEligibility criteria
• Locally advanced or mRCC with clear-cell histology
RANDOMI 1:1
Motzer et al. ASCO 2012.www.clinicaltrials.gov (NCT00720941).
Sunitinib50 mg/day
(Schedule 4/2)
Primary endpoint: PFS Secondary endpoints: OS, ORR, time to response, duration of response, safety, QoL
n=876clear cell histology
• No prior systemic therapy for advanced mRCC
SATION
*Conditionally approved
Hair color changeWeight decreasedSerum ALT increased
AlopeciaUpper abdominal painSerum AST increasedFatigueRashPain in extremityConstipation
Relative Risk in Adverse EventsAE occurrence ≥10% in either arm
ConstipationTaste AlterationLDH increasedSerum creatinine increasedPeripheral edemaHand-foot syndromeDyspepsiaPyrexiaLeukopeniaHypothyroidismEpistaxisSerum TSH increasedMucositisNeutropeniaAnemiaThrombocytopenia
Favors pazopanib Favors sunitinibMotzer et al. ASCO 2012.

CHALLENGESINTREATINGRENALCELLCARCINOMAINTHECOMMUNITY
©2013PCME Page13
Summary of the COMPARZ trial
• This phase III trial demonstrates non-inferiority of pazopanib relative to sunitinib for progression-free survival
• Pazopanib efficacy is further supported by similar overall survival and higher response rates
• The differentiated safety profile of pazopanib includes:
– Lower incidence of hand-foot syndrome, fatigue, and mucositis
– Higher incidence of liver function test abnormalities
• Improved tolerability supported by better QoL scores for patients receiving pazopanib
Phase III Patient Preference Study of Sunitinib vs Pazopanib (PISCES)
*Pazopanib 800 mg/day
Eligibility criteria:• Locally advanced
or mRCC of any histology
• Non-measurable disease permitted if metastatic disease
Patient preference?
Sunitinib50 mg/day
(Schedule 4/2)
RANDMIZ
• Primary endpoints: Patient preference (questionnaire)
• Secondary endpoints: Reason for patient preference; fatigue; dose modifications and time to dose modification; safety/tolerability
*Conditionally approved
www.clinicaltrials.gov (NCT01064310).Escudier et al. ASCO 2012.
Sunitinib50 mg/day
(Schedule 4/2)
n=161metastatic disease confirmed
• No prior systemic therapy for advanced or mRCC
• ECOG PS 0 or 1 10-week treatment period
10-week treatment period
2-weekwashoutperiod
p
Pazopanib 800 mg/day
ZATION
Primary Endpoint: Patient Preference Primary Analysis Population
60
70
80
90
tient
s
70%
Difference (pazopanib vs sunitinib) 49.3%
90% CI for difference (37.0%, 61.5%)
P value <0.001
CI = confidence interval
Escudier et al. ASCO 2012.
0
10
20
30
40
Pazopanib Preferred Sunitinib Preferred No Preference
Perc
ent o
f Pat
22%
8%
50
Immunotherapy
• Interferon-α (IFN-α): “the control”– Median PFS: 4.7 mo – Median OS: 13 mo
• High dose Interleukin (IL-2)– Response rate: 15-20% – 5-7% durable CRs– NCI 1986-2006
Median Overall SurvivalCR: Not reachedPR: 39.1 moNo response: 15.1 mo
McDermott DF et al. J Clin Oncol. 2005;23:133-141.Klapper JA et al. Cancer. 2008;113:293-301.
High dose IL-2 NCI Experience 1986-2006
IMA901 Renal Cell Cancer Phase III Trial Study Design
n=330-350• 1st line metastatic and/or locally advanced RCC• HLA-A*02-positive• Documented tumor lesions• Favorable or intermediate risk (Heng et al. 2009)
Chief Investigator US: Brian Rini, ClevelandChief Investigator EU: Tim Eisen, London
Primary: OSSecondary: OS in biomarker subgroup, PFS
safety, immune responses, novel biomarkers
Stratification based upon number ofbaseline Heng risk factors (1, 2, 3, or 4)
Pivotal Phase III ADAPT Trial Initiating 2H’12
Diagnosis, Nephrectomy,Screening
↓Registration;
Leukapheresis (A A l )
Arm A: AGS-003 (8 doses) plusStandard treatment* for 48 weeks (n = 300)
Arm B: Standard treatment*
AGS-003 quarterly + Standard treatment*
until PD
Standard treatment*
≥ SD
Pre-treatment Induction Booster
• Open-label design, no placebo-control, single leukapheresis (Arm A only)
• Primary endpoint: Overall Survival (80% power; HR: 0.708)
• Initiating under Special Protocol Assessment (SPA) with FDA
• Global Study PIs: Robert Figlin, MD (Cedars-Sinai); Christopher Wood, MD (MDACC)
• Collaboration with SUO-CTC in North America to support multidisciplinary efforts
• Status: US sites are activating; Qualifying sites in EU, Canada and other select countries with enrollment commencing late 2012
(Arm A only) ≥ SDfor 48 weeks(n = 150)
Standard treatment* until PD
* Standard treatment initiates with 6-week sunitinib cycles (50mg daily, 4 weeks on, 2 weeks rest.)Other compatible agents may be substituted for intolerance and/or early PD prior to week 48.

CHALLENGESINTREATINGRENALCELLCARCINOMAINTHECOMMUNITY
©2013PCME Page14
Case 2
• Patient: Male, 64-year-old man
• Past History: hypertension and hypercholesterolemia
• Current Medications: amlodipine 5mg QD and atorvastatin 20mg QD
• Social History: married; father of 2 children; works as a consultant
• Family History: coronary artery disease and lung cancer
Case 2: History of Present Illness
• Presenting Symptoms: Hematuria
• Initial Treatment: Right radical nephrectomy (2008)
• Tumor Histology: Clear cell RCC, grade 3
• Tumor Stage: T2, NX
B i / h M N• Brain/other Metastases: None
• ECOG Performance Status: 0
• Recurrence: Multiple lung nodules and medistinal lymph nodes; biopsy-proven recurrent clear cell RCC (2010)
• Initial Systemic Treatment: Sunitinib 50 mg 4/2
• Response: Confirmed partial response after 4 cycles, continued (eventually dose-reduced to 37.5 mg 4/2 due to fatigue) for a total of 18 months before RECIST-defined PD
Best response on sunitinib PD on sunitinib
Sunitinib The next step is . . .
• Continue sunitinib, as patient is tolerating well with “clinical benefit” with no symptoms from progressive disease
• Change to axitinib at a starting dose of 5mg BID
• Change to everolimus 10mg QD• Change to everolimus 10mg QD
Resistance Appears Mediated by “Angiogenic Escape” – ASL MRI: Rodent Model
ASL MRI
Day 22Day 9Day 3Baseline
H & E
CD34
Schor-Bardach R et al. Radiology. 2009;251:731-742.
Eligibility criteria:• Histologically confirmed mRCC
with clear-cell component
• Failure of one prior first-line regimen containing ≥1 of: - Sunitinib
Phase III Study of Axitinib vs Sorafenib as Second-line Therapy for mRCC (AXIS)
Axitinib 5 mg BID
RANDOMI
Sorafenib 400 mg BID
Sunitinib- Bevacizumab + IFN-α- Temsirolimus- Cytokine(s)
Stratification• Prior regimen• ECOG PS 0 vs 1
n=723
Primary endpoint: PFS
Secondary endpoints: OS, ORR, duration of response, safety, QoL
IZATION
www.clinicaltrials.gov (NCT00920816).

CHALLENGESINTREATINGRENALCELLCARCINOMAINTHECOMMUNITY
©2013PCME Page15
Progression-free Survival (IRC Assessment)
1.0
0.9
0.8
0.7
0.6
0.5
P<0.0001 (log-rank)Stratified HR 0.665
AxitinibSorafenib
mPFS, mo 95% CI
6.74.7
6.3–8.64.6–5.6
n-fr
ee S
urvi
val
babi
lity)
IRC = Independent Review Committee
361 256 202 145 96 64 38 20 10 1 0362 224 157 100 51 28 12 6 3 1 0
Subjects at risk, nAxitinibSorafenib
0.4
0.3
0.2
0.1
0.00 2 4 6 8 10
Time (months)
12 14 16 18 20
(95% CI 0.544–0.812)
Prog
ress
ion
(pro
b
PFS by Prior Regimen
Prior Treatment RegimenAxitinib(n=361)
Sorafenib (n=362) HR P value*
Cytokines (n=251)IRCInvestigator
12.112.0
6.58.3
0.464 0.636
<0.00010.005
Sunitinib (n=389)4 8 3 4 0 741 0 011
( )IRCInvestigator
4.8 6.5
3.44.5
0.7410.636
0.0110.0002
Temsirolimus (n=24)IRCInvestigator
10.12.6
5.35.7
0.5111.210
0.1420.634
Bevacizumab (n=59)IRCInvestigator
4.26.5
4.74.5
1.1470.753
0.6370.213
*One-sided log-rank test stratified by ECOG PS
Best Response by RECIST(IRC Assessment)
Best Overall Response, % Axitinib Sorafenib
Partial response*
Stable disease
19.4
49 9
9.4
54 4Stable disease
Progressive disease
Indeterminate
49.9
21.6
6.1
54.4
21.0
11.6
Risk ratio (95% CI) 2.1 (1.4–3.0)
*Axitinib vs Sorafenib: P = 0.0001
Everolimus Phase III Study (RECORD-1)Design and Prior Therapy
Everolimus + BSC
Prior Treatment
Everolimus (n = 277)
%
Placebo (n = 139)
%
VEGFR-TKI therapy
RAND
Placebo + BSC(n = 139)
(n = 277)Patients progressed on/within 6 mo of sunitinib and/or sorafenib
Prior cytokines and/or bevacizumab also permitted
Sunitinib 45 43
Sorafenib 29 31
Both 26 26
Other systemic therapy
Immunotx 65 67
Chemotx 13 1679% of patients received 2 or more prior therapies
Motzer RJ et al. Cancer. 2010;116:4256-4265.
DOMIZATION
2:1
Everolimus Phase III StudyPFS
100
bilit
y, %
80
60 Log rank P value <0.001
Everolimus (n=277)
Hazard ratio = 0.3395% Confidence Interval (CI) [0.25, 0.43]
Median PFSEverolimus: 4.90 moPlacebo: 1.87 mo
100
bilit
y, %
80
60Log rank P value <0.001
Everolimus (n=277)
Hazard ratio = 0.3295% CI [0.25, 0.41]
Median PFSEverolimus: 5.49 moPlacebo: 1.87 mo
Central Radiology Review Investigator Assessment
Months
0 142 4 6 8 10 12
0
Prob
ab
40
20
139 47 15 6 2 0 0 0277 192 115 51 26 10 1 0
Everolimus (n=277)
Placebo (n=139)
Months
0 142 4 6 8 10 12
0
Prob
ab
40
20
Number of patients at risk
EverolimusPlacebo 139 62 25 8 5 0 0 0
277 210 149 76 33 11 2 0
( )
Placebo (n=139)
1Escudier et al. Ann Oncol. 2008;19:viii45. Abstract 72O. 2Motzer et al. ASCO-GU 2009. Abstract 278.
Clinical outcome to 2nd-line VEGF-targeted therapy based on 1st-line VEGF-targeted therapy response
OR to 1st-line VEGF-targeted therapy
OR to 2nd-line VEGF-targeted therapy
CR/PR SD PD
CR/PR (n=72) 14% 36% 50%
SD (n=175) 10% 50% 40%
PD (n=76) 11% 34% 55%
Al-Marrawi MY et al. Target Oncol. 2013 Jan 9. [Epub ahead of print].
CHALLENGESINTREATINGRENALCELLCARCINOMAINTHECOMMUNITY
©2013PCME Page16
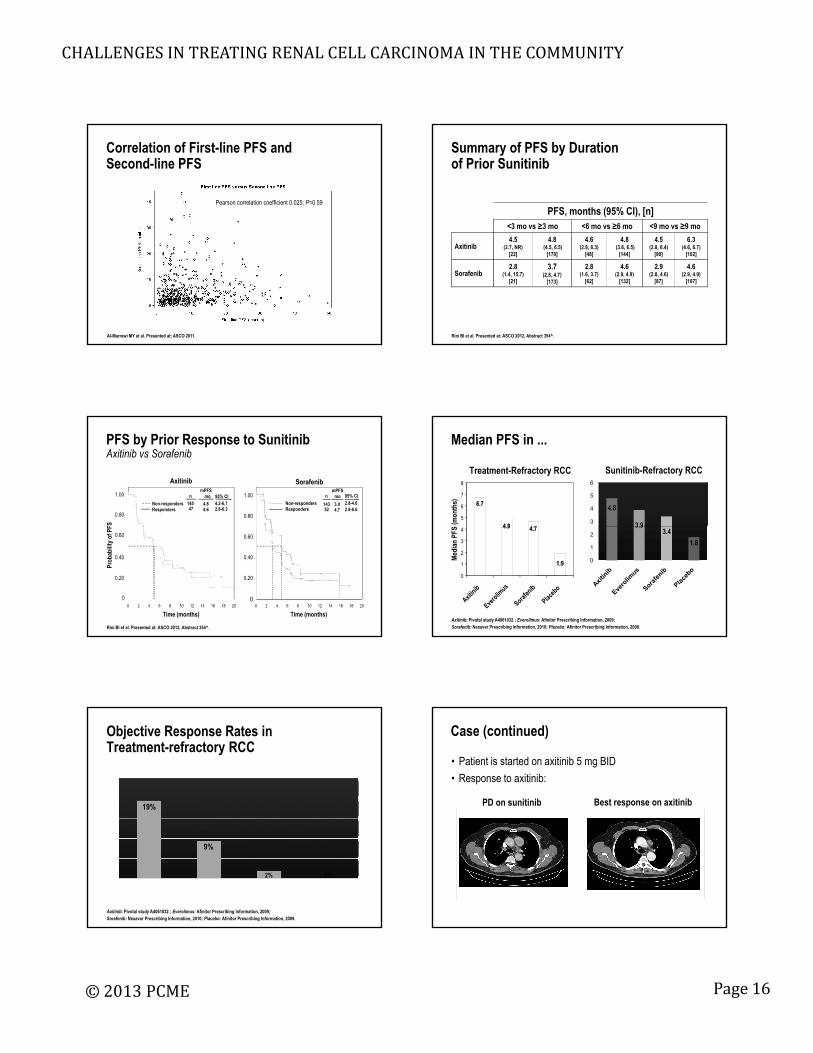
Correlation of First-line PFS and Second-line PFS
Pearson correlation coefficient 0.025; P=0.59
Al-Marrawi MY et al. Presented at: ASCO 2011.
Summary of PFS by Duration of Prior Sunitinib
PFS, months (95% CI), [n]<3 mo vs ≥3 mo <6 mo vs ≥6 mo <9 mo vs ≥9 mo
Axitinib4.5
(2.7, NR)[22]
4.8(4.5, 6.5)
[170]
4.6 (2.8, 8.3)
[48]
4.8(3.6, 6.5)
[144]
4.5(2.8, 6.4)
[90]
6.3(4.6, 6.7)
[102]
Sorafenib2.8
(1.4, 15.7)[21]
3.7(2.8, 4.7)
[173]
2.8 (1.6, 3.7)
[62]
4.6(2.9, 4.9)
[132]
2.9(2.8, 4.6)
[87]
4.6(2.9, 4.9)
[107]
Rini BI et al. Presented at: ASCO 2012, Abstract 354^.
PFS by Prior Response to SunitinibAxitinib vs Sorafenib
FS
Axitinib Sorafenib
1.00
0.80
1.00
0.80
Non-respondersResponders
n 95% CI
4.84.6
4.2-6.72.8-6.3
mPFSmo
14547
Non-respondersResponders
n 95% CI
3.04.7
2.8-4.62.9-6.6
mPFSmo
14352
Time (months)
Prob
abili
ty o
f PF
Time (months)
0.60
0.40
0.20
0
0.60
0.40
0.20
0 2 4 6 8 10 12 14 16 18 20 0 2 4 6 8 10 12 14 16 18 20
0
Rini BI et al. Presented at: ASCO 2012, Abstract 354^.
5
6
7
8
(mon
ths)
Sunitinib-Refractory RCC
Median PFS in ...
Treatment-Refractory RCC
4.8
3 93
4
5
6
6.7
4 9 4
0
1
2
3
4
Med
ian
PFS
Axitinib: Pivotal study A4061032 ; Everolimus: Afinitor Prescribing Information, 2009; Sorafenib: Nexavar Prescribing Information, 2010; Placebo: Afinitor Prescribing Information, 2009.
3.93.4
1.8
0
1
2
4.9 4.7
1.9
Objective Response Rates in Treatment-refractory RCC
19%
9%
2% 0%
Axitinib: Pivotal study A4061032 ; Everolimus: Afinitor Prescribing Information, 2009; Sorafenib: Nexavar Prescribing Information, 2010; Placebo: Afinitor Prescribing Information, 2009.
Case (continued)
• Patient is started on axitinib 5 mg BID
• Response to axitinib:
Best response on axitinibPD on sunitinib

CHALLENGESINTREATINGRENALCELLCARCINOMAINTHECOMMUNITY
©2013PCME Page17
Patients with mRCC and PD on 1st-line sunitinib(n=512)
Stratification factors:•Duration of sunitinib
Primary end point: PFS (per IRC)
INTORSECT* Study Design
RANDOMIZA
Temsirolimus25 mg IV weekly†
(n=259)
therapy (≤ or >6 mo)•MSKCC risk group•Histology (clear cell or non-clear cell)•Nephrectomy status
(per IRC)
BID = twice daily; IRC = independent review committee; IV = intravenous; mRCC = metastatic renal cell carcinoma; MSKCC = Memorial Sloan-Kettering Cancer Center; PD = progressive disease; PFS = progression-free survival
*ClinicalTrials.gov Identifier: NCT00474786.†Dose reductions were allowed: temsirolimus (to 20 mg then 15 mg), sorafenib (to 400 mg/day then every other day).
Treat until PD, unacceptable toxicity, or discontinuation for any other reason
ATION
1:1
Sorafenib400 mg oral BID†
(n=253)
1.0
0.9
0.8
0.7
0.6
0.5
Progression-free Survival Overall Survival
P=0.1933 (log-rank)Stratified HR: 0.87
(95% CI: 0.71, 1.07)
Median PFS,months 95% CI
4.283.91
4.01, 5.432.80, 4.21
roba
bilit
y)
1.0
0.9
0.8
0.7
0.6
0.5 val (
prob
abili
ty)
P=0.014 (log-rank)Stratified HR: 1.31
(95% CI: 1.05, 1.63)
12.2716.64
10.13, 14.8013.55, 18.72
Median OS,months 95% CI
0.4
0.3
0.2
0.1
0.0
CI = confidence interval; HR = hazard ratio; IRC = Independent Review Committee; PFS = progression-free survival
TemsirolimusSorafenib
252 72 22 11 6 0259 96 28 9 5 0
SorafenibTemsirolimus
Patients at risk, n
PFS
(pr
Time (months)0 5 10 15 20 25
0.4
0.3
0.2
0.1
0.0
Ove
rall
Surv
iv
0 10 20 30 40 50
TemsirolimusSorafenib
Time (months)
253 158 74 34 13 0259 132 54 22 8 0
Time to Treatment Failure From Second-line Drug Initiation (n=216)
Vickers MM et al. Urology. 2010;76:430-434.
The Benefit of Everolimus Does Not Differ Based on Number of Previous VEGFr-TKIs or MSKCC Risk
Everolimus + BSC n = 277
Placebo + BSC n = 139
Treatment Effect
n (%)Median PFS, mo
n (%)Median PFS, mo
HR (95% CI)
P
Number of previous VEGFr-TKIs
1 205 (74) 5.4 103 (74) 1.90.32
(0.24-0.43)<0.001
( )
2 72 (26) 4.0 36 (26) 1.80.32
(0.19-0.54)<0.001
MSKCC risk category
Favorable 81 (29) 5.8 39 (28) 1.90.31
(0.19-0.50)< 0.001
Intermediate 156 (56) 4.5 79 (57) 1.80.32
(0.22-0.44)< 0.001
Poor 40 (14) 3.6 21 (15) 1.80.44
(0.22-0.85)0.007
Calvo E et al. Eur J Cancer. 2012;48:333-339.
BSC = best supportive care; CI = confidence interval; HR = hazard ratio; PFS = progression-free survival; MSKCC = Memorial Sloan-Kettering Cancer Center; VEGFr-TKI = vascular endothelial growth factor receptor-tyrosine kinase inhibitor
RANDOMIZ
SWITCH: Phase III Sequential Study of Sorafenib and Sunitinib
Sunitinib 50 mg/day (Schedule 4/2)
Eligibility• mRCC with all
histologies
Stratification• ECOG PS 0 or 1 n=346
Sorafenib400 mg BID
ZATION
• Primary endpoints: overall PFS
• Secondary endpoints: total time to progression, OS, disease control rate and cardiotoxicity
Sorafenib400 mg BID
Discontinuation (due to progressive disease/toxicity)
ECOG PS 0 or 1• No prior systemic
therapy for advanced or mRCC
PI: Goebell P. www.clinicaltrials.gov. (NCT00732914).
n=346Sunitinib50 mg/day (Schedule 4/2)
RANDOMIZ
SWITCH: Phase III Sequential Study of Sorafenib and Everolimus
Sunitinib50 mg/day (Schedule 4/2)
Eligibility• Patients with
advanced RCC
Stratification• Karnofsky
performance status n=390
Everolimus10 mg/day
ZATION
• Primary endpoints: first PFS
• Secondary endpoints: second PFS, ORR, duration of response, patient-reported outcomes, OS
Everolimus
10 mg/day
Discontinuation (due to progressive disease/toxicity)
performance status ≥70%
• No prior systemic therapy for advanced or mRCC
www.clinicaltrials.gov. (NCT00903175).
n=390Sunitinib50 mg/day (Schedule 4/2)

CHALLENGESINTREATINGRENALCELLCARCINOMAINTHECOMMUNITY
©2013PCME Page18
Conclusions
• Deciding when to stop one therapy and change to another can be difficult in patients who have experienced significant clinical benefit to their first agent and are tolerating well.
• Axitinib has level one evidence of clinical benefit in the second line settingsecond-line setting.
• Everolimus has level one evidence of clinical benefit in the refractory setting.
• There is no reliable way to predict second-line therapy benefit based on patient, tumor, or response characteristics.
























![[Metatemas 041] Lewin, Roger - Complejidad [9989] (r1.2 koothrapali).pdf](https://img.pdfslide.us/doc/110x75/577cc3ed1a28aba71197963c/metatemas-041-lewin-roger-complejidad-9989-r12-koothrapalipdf.jpg)

