Embed Size (px)
Citation preview

Running Head: ARTHRITIS IN THE ELDERLY
Arthritis in the ElderlyA Community Health Promotion Program
Written Assignment #7Lindsay Ann Abrigo
December 15, 2013
MPH 585 – Programming and Evaluation in Public HealthDr. Madeline Angela Meyer
1

ARTHRITIS IN THE ELDERLY 2
Table of Contents
Introduction………………………………………………………………………………4
Needs Assessment…………………………………………………………………4
Osteoarthritis..........................................................................................................5
Rheumatoid Arthritis……………………………………………………………..6
Program Strategic Plan………………………………………………………………….7
Mission, Vision, and Values………………………………………………………7
SWOT Analysis…………………………………………………………………...8
Program Objectives and Priorities………………………………………………...8
Program Implementation Plan………………………………………………………….9
Logic Model……………………………………………………………………….8
Tasks, Timelines, Responsible Leads/Partners…………………………………..12
Tiffany Butac – Program Director, Hawaii Arthritis Foundation……………..13
Linda Adamson – Director of Lifestyles, Kahala Nui…………………………..13
Eric K.S. Yee, M.D., DMC – Medical Director, Kahala Nui…………………..14
Nutritionist/Dietician……………………………………………………………14
Personal Fitness Trainer/Wellness Coach………………………………………14
Financial Advisor……………………………………………………………….15
SMART Objectives………………………………………………………………15
Public Health Promotion: Tasks, People, and Timelines………………………...17
Gantt Chart……………………………………………………………………...19
Program Pro Forma……………………………………………………………………21
Budgetary Needs…………………………………………………………………21

ARTHRITIS IN THE ELDERLY 3
Program Evaluation Plan………………………………………………………………23
Outcome Measurements and Standards………………………….………………25
Evaluation Chart……………………………………………………….………...25
Program Strategies Summary…………………………………………………………29
Summative Evaluation Table………………………………….…………………30
References……………………………………………………………………………….34

ARTHRITIS IN THE ELDERLY 4
“Arthritis in the Elderly”A Community Health Promotion Program
Introduction
When people are healthy, they may take their bodies for granted. It is usually only when
it begins to break down, whether due to an accident, illness, disease, or everyday wear and tear,
that they recognize the importance of good health and the body’s extraordinary capabilities to
heal and repair itself. For optimum health, you should have a basic understanding of how your
body works and feels when you are well, so you can identify changes that can occur when you
are injured or in poor health.
“Arthritis in the Elderly” is a health promotion program focused on the elderly
population, aged 62 years and older, with the primary purpose of educating these individuals
about the importance of proper nutrition and physical activity in relation to arthritis. “Arthritis in
the Elderly” incorporates elements of successful arthritis management, nutrition, and exercise
programs, but will emphasize creating and tailoring the program to meet each individual
participant’s specific needs and successfully achieve the goals each participant has set.
Needs Assessment
Arthritis is one of the most common medical problems in the world, according to Dr.
Gene G. Hunder (2002). Arthritis is known to affect as many as one billion people of every age,
race, and culture (Lam & Horstman, 2002). According to research performed at the Johns
Hopkins Arthritis Center, approximately one out of three Americans – or 70 million – suffers
from some form of arthritis, making arthritis one of the most pervasive diseases and leading
cause of disability in the United States (2013). This disease causes a major financial burden on
the costs of health care (Lam & Horstman, 2002) and lost productivity amounts to an estimated

ARTHRITIS IN THE ELDERLY 5
$65 billion annually (Hunder, 2002). However, the human cost of coping with the pain, stiffness,
and disability of arthritis can be far greater.
Arthritis is not a single disease, but consists of more than 100 different disorders
involving the joints and is characterized by chronic pain, limited mobility and decreased range of
motion (The Johns Hopkins Arthritis Center, 2013). The term “arthritis” comes from to Greek
words: arthros, meaning, “joint” and the –itis, which means “inflammation” (1999). It is used to
describe a wide range of diseases of the joints and related tissues that cause pain, stiffness, joint
deformities, and loss of function (Lam & Horstman, 2002). The two most prevalent forms of
arthritis are osteoarthritis and rheumatoid arthritis (Hunder, 2002).
Osteoarthritis. Osteoarthritis (OA) is the most common form of arthritis affecting close
to 30 million nationwide and often accompanies age as it is characterized by the wear and tear of
joints over time (Johns Hopkins Arthritis Center, 2013). As our population ages, the prevalence
of this condition continues to increase (John Hopkins Arthritis Center, 2012), affecting nearly 80
percent of the population aged 65 and older (Iannucci & Horowitz, 1999).
The symptoms of osteoarthritis vary from person to person. One individual may have
some general stiffness each morning that never progresses into much more. Another person may
have severe, crippling pain all day long. Symptoms of OA include pain ranging from mild
discomfort to throbbing pain in the joints, stiffness, inflammation, and limited range of motion.
When considering stiffness, “it’s a catch-22: If you rest, the pain may subside; if you rest, the
joints may stiffen up” (Iannucci & Horowitz, 1999). It is likely that stiffness will occur after
sitting for a while, or after waking up in the morning, but should start to subside after a few
minutes of moving around. Inflammation is a common symptom in rheumatoid arthritis, but is
not as common in osteoarthritis. When a joint is overused, it can become warm, red, and

ARTHRITIS IN THE ELDERLY 6
inflamed. Joint damage prevents the joint from flexing and bending normally, making it difficult
to perform daily tasks, such as grasping door handles, turning a page, or walking up the stairs. In
sever cases of OA, all of the cushioning cartilage may be destroyed, leaving bones in direct
contact with no “padding,” causing more pain and limiting movement in that joint (Lam &
Horstman, 2002).
Rheumatoid Arthritis. Rheumatoid arthritis (RA) is an autoimmune disease that can
lead to joint destruction, deformity, and loss of function. Without proper treatment, the Johns
Hopkins Arthritis Center states, that chronic pain, disability, and excess mortality are outcomes
of this disease as “RA causes joint damage in 80% to 85% of patients, with the brunt of the
damage occurring during the first 2 years of the disease” (2012).
Rheumatoid arthritis is not the most common form of arthritis, but when it strikes, it does
not discriminate. It is, however, the most serious and disabling types of arthritis, often more
disabling than osteoarthritis (Dunkin & Klippel, 2001). Like osteoarthritis, the symptoms of RA
vary from person to person. One person may experience pain that remains stable, while another
person might have such a severe case, that a joint or joints may be virtually destroyed (Bernstein
& Klippel, 2003). Without proper treatment, The Johns Hopkins Arthritis Center states, chronic
pain, disability, and excess mortality are unfortunate outcomes of this disease, causing joint pain
in 80% to 85% of patients as a result (2013).
At present, arthritis is an almost inevitable part of aging as joints will naturally
degenerate over time and most over the age of 50 shows some signs of arthritis (Johns Hopkins
Arthritis Center, 2013). There is no known cure for arthritis (Johns Hopkins Arthritis Center,
2013), but with proper treatment, a strategy of joint protection, and changes in lifestyle, people
can still live long, productive lives after developing arthritis (Hunder, 2002). When dealing with

ARTHRITIS IN THE ELDERLY 7
arthritis, both profession care and self-care are essential. Starting early in the disease on a
carefully planned, individualized treatment program offers the best chance of reducing the
impact of the disease on your lifestyle.
Program Strategic Plan
Mission, Vision, Values
The mission of the “Arthritis in the Elderly” Program is to provide the best arthritis self-
management care to elderly individuals residing in the Kahala Nui retirement community. The
program will raise awareness of the importance and severity of arthritis and the effect it has on
the overall quality of life of those who live with and suffer from its symptoms. This program will
also emphasizes the importance of tailoring a program to address the unique needs of each
participant and to provide them with the tools and knowledge necessary to achieve personal
goals and manage arthritis symptoms successfully. The “Arthritis in the Elderly” Program will
incorporate the “aloha spirit” in each and every interaction and at each phase of the program. The
“aloha spirit” is “the attitude of friendly acceptance for which [Hawaii] is so famous. However, it
also refers to a powerful way to resolve any problem, accomplish any goal, and to achieve any
state of mind or body that you desire” (King, 2003).

ARTHRITIS IN THE ELDERLY 8
SWOT Analysis
Strengths, Weaknesses, Opportunities and Threats (SWOT Analysis)What are the strengths will contribute to planning and program success?
What weaknesses exist for your planning and program success?
- Need for arthritis self-management program in Hawaii- Interest among elderly population- Support from Hawaii Arthritis Foundation- Support from community organizations, such as retirement
communities- Arthritis often accompanies old age- Program staff invested in program for the long-run; desire to
achieve program goals and objectives
- Not many local/Hawaii arthritis-related data sources- Insufficient man power to conduct assessments and
evaluations necessary to determine program success
What are the opportunities your planning and program will create?
What are the threats to your planning and program success?
- Opportunity for the elderly living with arthritis to participant in self-management program customized according to their specific needs/capabilities, goals, and arthritis symptoms
- Encourage Hawaii State Department of Health to adopt Arthritis in the Elderly program
- Advocate and raise awareness for arthritis- Additional funding for arthritis research, treatment, and other
arthritis-related programs
- Lack of continuous funding- Participant failure to follow program guidelines to achieve goals and objectives
- Participant drop out- Existence of established and successful arthritis programs- Potential loss of interest by stakeholders
Program Objectives and Priorities
The goal of the “Arthritis in the Elderly” Program is to improve and increase self-
management attitudes and exercise behaviors among individuals aged 62 and older, living in a
retirement home in Hawaii, and who have arthritis.
Objective #1: IDENTIFY the symptoms, risk factors, and causes of arthritis
Objective #2: INCREASE the time spent engaging in physical activity
Objective #3: INCREASE the knowledge and ability to plan, prepare, and consume anti-
inflammatory foods to improve the symptoms of arthritis
Objective #4: PERFORM at least three physical activities taught during the program
Objective #5: DECREASE the level of pain caused by arthritis

ARTHRITIS IN THE ELDERLY 9Program Implementation Plan
Arthritis in the Elderly Logic ModelProgram Implementation Planning
Inputs OutputsActivities
Outcomes -- ImpactShort Medium Long
1) Staffing- Program manager- Program assistant- Nutritionist/ Dietician- Personal trainer/ Wellness coach- Contacts at Hawaii Arthritis Foundation- Contacts at Hawaii State Dept. of Health- Rheumatologist, Gerontologist, and other arthritis-related health care providers- Medical Director
2) Funding/Support- Funds to support development of program- Stakeholder support- Funds to compensate program staff- Policy/legislative support
3) Surveillance- Monitor/secure funding- Existing and emerging arthritis-related data sources (local/national)
- Assess nutrition status of all participants via medical record review, face-to-face interviews and diet histories- Provide nutrition education to participants- Educate participants on which foods cause and reduce inflammation- Aid in developing customized diet/ nutrition plan for each program participant- Monitor nutritional plan and progress- Assess needs and capabilities of all participants through fitness assessments- Advise participants on correct use of exercise machines/devices and proper form in a variety of fitness activities- Aid in developing individualized exercise programs based on needs and fitness level
- Develop realistic, attainable goals, and modify training objectives as necessary- Utilize wellness coaching to reduce or eliminate high-risk behaviors- Monitor exercise/ physical activity plan and progress of program participants- Funding to implement arthritis in the elderly population
- Increased knowledge about the symptoms, risk factors, and causes of arthritis- Increased time engaging in physical activity- Increased confidence to engage in regular physical activity- Participants able to perform at least three physical activities learned during program- Increased knowledge and ability to plan, prepare, and consume anti-inflammatory foods- Increased knowledge of foods that cause or reduce inflammation- Decreased level of pain- Improved quality of life- Improve and increase self-management attitudes and nutritional and physical activity behaviors
- Maintenance of arthritis management behaviors- Maintenance of regular physical activity- Maintenance of proper nutrition/dietary choices- Surveillance of trends and evolving information of arthritis in the elderly- Regular follow-ups with physician to monitor arthritis symptoms- Increased behavior among elderly population towards arthritis care- Available funding to continue Arthritis in the Elderly program- Implementation of more self-management programs related to arthritis that can be tailored to the individual needs of participants
- Documentation of improvement in arthritis symptoms as a result of participation in the program among target population- Decrease in level of pain caused by arthritis- Decreased prevalence of limited mobility caused by arthritis- Decreased morbidity and mortality of arthritis and arthritis-related conditions
Assumptions External FactorsIf participants properly follow program components, then they will be able to: 1) identify the symptoms, risk factors, and causes of arthritis, 2) increase the time spent engaging in physical activity, 3) increase the knowledge and ability to plan, prepare, and consume anti-inflammatory foods to improve the symptoms of arthritis, 4) perform at least three physical activities taught to participants during the program, and 5) decrease the level of pain caused by arthritis. Customizable self-management programs are necessary.
Additional funding from existing organizations can allow for continued implementation of the program and to modify/improve current program components. Development of or revisions to state/federal laws, unexpected changes in data sharing procedures, and other already established arthritis-related programs can all affect the program.

ARTHRITIS IN THE ELDERLY 10
A “one-size-fits-all” approach does not work for people with arthritis. The only expert on
you is you. It is important for individuals to learn to pay attention to his or her body. Experience
is the best teacher in determining what level of activity is appropriate for an individual. It is key
to remember how one feels at the start of an activity and to note again how they feel after
completing the activity. An activity level that is appropriate for you should make you feel the
same or better afterward. Feeling worse, especially after several hours or the next day, may
indicate that there is something wrong with what an individual is doing. “If you feel worse,
especially after several hours or the next day, there’s something wrong with what you’re doing.
You may be overdoing it,” says Dr. Gene G. Hunder (2002). “Or, you may be performing an
activity in a way that aggravates your condition. When your body talks – listen” (Hunder, 2002).
A program that is well designed specifically for an individual should include activities he or she
enjoys doing. One person’s goals can and will be very different from those of someone else with
arthritis. As an individual listens to his or her body, their goals should change from day to day as
their condition also changes.
Probably the strongest evidence is for the effectiveness of conditioning exercise,
including endurance and strengthening, in individuals with osteoarthritis and rheumatoid arthritis
(Vad, 2006). Walking, cycling, water aerobics, strength training, and low-impact exercise
programs report decreased pain and improved range of motion, cardiovascular fitness, strength,
endurance, function, and gait in individuals with arthritis (Vad, 2006). Well-controlled studies of
aerobic exercise consistently report that individuals with arthritis can safely exercise regularly
and vigorously enough to improve fitness and health without exacerbation of disease or
increased joint symptoms. The training regimens in most aerobic exercise studies progressively
increase the intensity and duration of the exercise sessions to achieve the guidelines for

ARTHRITIS IN THE ELDERLY 11
cardiovascular fitness set by the American College of Sports Medicine, which is 30 to 45
minutes of moderate-intensity, whole-body exercise, such as walking, cycling, or swimming, 3 to
5 days a week (Ripp, McCarthy, & Wait, 2001).
Controlled trials of exercise interventions designed specifically for individuals with knee
osteoarthritis include strengthening, aerobics, and functional exercises. These studies use a short
period of initial instruction followed by several months of self-directed home exercise and report
improved strength, proprioception, and function, and decreased pain (Gach, 2001). Low-intensity
active range-of-motion exercise, the traditional home exercise program for individuals with
arthritis, can provide benefits in addition to flexibility and joint motion. Gentle exercise
performed in the evening can significantly reduce morning stiffness in individuals with
rheumatoid arthritis (Gach, 2001). An exercise program of active exercise and relaxation (the
range of motion dance) has shown significant improvements in self-reported function and pain.
In addition to the aforementioned benefits, exercise seems to improve depression.
Although the exact mechanisms are not understood, it may be that depression and other negative
mood states are mediated by self-efficacy, or the belief that one can affect disease symptoms.
Several publications have documented that the combination of exercise and weight loss in
individuals with osteoarthritis leads to improvement in pain, function, mobility-related
performance, and other health-related quality-of-life measures. Today, the European League
Against Rheumatism and the American College of Rheumatology endorse weight loss and
exercise in overweight individuals with knee osteoarthritis (Ripp, McCarthy, & Wait, 2001).

ARTHRITIS IN THE ELDERLY 12
Tasks, Timelines, Responsible Leads/Partners
Action or Step to be CompletedMethod for Completion Timeline Milestones Person(s)
ResponsibleStatus/Completion
DateDetermine funding available to implement program and compensate program staff
3 meetings1 month
Received grant and additional funding from local sponsors
Program director/ Financial advisor
CompletedJanuary 2014
Determine if target population (elderly living in retirement/senior citizen homes in Hawaii) and subject matter are appropriate
1-2 meetings1 week
N/A Program director/ Program assistant
CompletedJanuary 2014
Establish communication with contact at Hawaii Arthritis Foundation
Daily attempts2 weeks
Communicated with Program Director of Hawaii Arthritis Foundation
Program director/ Program assistant
CompletedFebruary 2014
Solicit potential locations at which program will be presented/implemented and establish communication with retirement/senior citizen home(s)
Daily attempts1 week
3 potential locations suggested; Established all communication on the same day
Program director/ Program assistant/Director of Hawaii Arthritis Foundation
CompletedFebruary 2014
Determine if retirement home would be interested in participating in program and if there would be enough participants
1-2 meetings1 week
All locations showed interest in program
Program director/ Program assistant/Director of retirement home
CompletedFebruary 2014
Confirmation of program participation from Director at retirement home
1 meeting1 week
Director of Kahala Nui retirement home confirms participation and secures three months for implementation of all program components and assessment of nutrition and physical capabilities and needs of each program participant
Program director/ Program assistant/ Director of retirement home
CompletedFebruary 2014
Secure a series of dates and times for program implementation at retirement home
1-2 meetings1 week
Program director/ Program assistant/ Director of retirement home
CompletedFebruary 2014
Assess nutrition status of all participants via medical record review, face-to-face interviews, and diet histories
1 meeting with each participant1 month
Medical Director/ Nutritionist/ Dietician/Arthritis-related healthcare providers
CompletedMarch 2014
Assess needs and capabilities of all participants through fitness assessments and physical examination
1 meeting with each participant1 month
Medical Director/ Personal trainer/ Wellness coach/Arthritis-related healthcare providers
CompletedMarch 2014
Assess and document quality of life and level of pain via questionnaire or face-to-face interview
1 meeting with each participant2 weeks
N/A Medical Director/Arthritis-related healthcare providers
CompletedMarch 2014
Educate participants on which foods cause and reduce inflammation caused by arthritis
5 group sessions1 week
Funding received from local produce company and farmers market
Medical Director/ Nutritionist/ Dietician/Arthritis-related healthcare providers
CompletedApril 2014
Advise participants on correct use of exercise machines/devices and proper form in a variety of fitness activities
5 group sessions1 week
Local YMCA learns about program and offers discounted membership rates and exercise/fitness classes to program participants
Medical Director/ Personal trainer/ Wellness coach
CompletedApril 2014
Aid in developing customized diet/nutrition plan for each program participant
1-2 meetings with each participant2 weeks
Participants utilize daily food journals and exercise/ physical activity logs; Used as a means of monitoring nutrition and exercise/
Medical Director/ Nutritionist/ Dietician/Arthritis-related healthcare providers
CompletedApril 2014
Aid in developing individualized exercise programs based on needs and fitness levels
1-2 meetings with each participant
Medical Director/ Personal trainer/
CompletedApril 2014

ARTHRITIS IN THE ELDERLY 13
2 weeks physical activity plan and progress made
Wellness coachMonitor exercise/physical activity and nutrition plan and progress of participants
2-3 meetings with each participant3 months
Medical Director/ Nutritionist/ Dietician/Arthritis-related healthcare providers
Completed/OngoingMay 2014 - PresentParticipants encouraged to follow up with nutritionist/ dietician and/or personal trainer/ wellness coach about questions/ progress made and to also follow up with healthcare provider regarding arthritis symptoms improvements or symptom worsening that should occur.
Reassess nutritional needs and physical capabilities of participants by reevaluating medical records, reviewing diet histories, performing physical examinations and repeat face-to-face interviews to determine current health status
1 meeting with each participant1 month
Increase in participant knowledge and confidence to plan, prepare, and consume anti-inflammatory foods; increase in time spent engaging in physical activity; decreased levels of pain among all participants; improvement and increase in self-management attitudes and behaviors
Medical Director/ Nutritionist/ Dietician/Arthritis-related healthcare providers
Reassess quality of life and level of pain via questionnaire or face-to-face interview
1 meeting with each participant2 weeks
Medical Director/Arthritis-related healthcare providers
Tiffany Butac – Program Director, Hawaii Arthritis Foundation – Pacific Region.
Tiffany was contacted to solicit possible presentation opportunities with which the program
would be presented and implemented upon interest. Tiffany did not have an upcoming events or
presentation dates that could serve as the jumping off point for the program. As such she
suggested that we contact some of the retirement or senior citizen homes around the island to see
if any of the sites would be interested. Upon having narrowed down a lengthy list of care homes
to just three, the program director and program assistant were able to contact them directly to
inquire with these sites about the proposed program.
Linda Adamson – Director of Lifestyles, Kahala Nui. Ms. Adamson was contacted to
determine whether Kahala Nui and their residents would be interested in participating in this
three-session program and whether there was enough interest to implement this particular type of
program. Upon receiving confirmation from Linda and their on-site medical director that this
would be of interest to the residents at Kahala Nui, Linda worked very closely with the program
director and program assistant to secure a series of dates and times for program implementation.

ARTHRITIS IN THE ELDERLY 14
Eric K.S. Yee, M.D., DMC – Medical Director, Hi’olani Care Center at Kahala Nui. Dr.
Yee provides input into the clinical policies governing the Kahala Nui, supervises the medical
staff, and directly oversees clinical safety and risk management. Dr. Yee is involved at all levels
of individualized patient care and supervision and for all persons served at Kahala Nui and he is
the clinician who oversees and guides the care that is provided and leads to help define a vision
of quality improvement. Dr. Yee will be active in assessing and educating participants on proper
nutrition and adequate exercise/physical activity, and well as monitor all participants’ arthritis
symptoms throughout the duration of the program.
Nutritionist/dietician. The Nutritionist/Dietician will provide nutrition care and education
to the program participants who are residents at Kahala Nui. They will assess the nutrition status
of individual patients via medical record review, face-to-face interviews, and diet histories;
monitor the nutritional plan and progress of each resident; construct, implement, evaluate, and
document nutrition care plans; and provide nutrition education to the residents and follow-up as
appropriate. In addition, the nutritionist/dietician will actively consult the Medical Director of
Kahala Nui and other healthcare team members to coordinate the proper nutritional care.
Personal fitness trainer/wellness coach. A personal fitness trainer has many
responsibilities when working with individuals. These responsibilities include, but are not
limited to: assessing the needs and capabilities of individuals through fitness assessment
procedures; developing individualized exercise programs tailored to each individual based on
each participant’s unique needs and fitness levels; providing instruction in a variety of fitness
activities; assure all exercises are done with proper form and technique; help clients develop
realistic, attainable goals, and continually modify training objectives with consultation from

ARTHRITIS IN THE ELDERLY 15
Medical Director and other healthcare team members who have assessed the physical health and
ability of each resident.
The wellness coach will work along side the personal trainer to provide appropriate
wellness coaching and coordinate care with other healthcare team members. The wellness coach
will also be responsible for encouraging the adoption of habits that are conducive to improved
quality of life and arthritis symptoms and decrease in pain; conducting onsite arthritis-related
seminars and training courses for residents of Kahala Nui and their families; and developing a
customized care plan for program participants including individualized goals and plans of action.
Financial advisor. A financial advisor will be consulted to determine how to best spend
the funding set aside for the program and how much funding is available for program
implementation/assessments. The financial advisor communicates with all personnel involved
with the program, but reports directly to the program director in reaching final decisions that deal
with the budget. The financial advisor is also responsible for properly paying all those involved
with the program, specifically those aforementioned, in a timely manner.
SMART Objectives
The goal of the Arthritis in the Elderly Program is to “Improve and increase self-
management attitudes and exercise behaviors among individuals aged 62 and older, living in a
retirement home in Hawaii, and who have arthritis.”
Not-so-SMART Objective 1: Test participants’ knowledge of ALL arthritis symptoms, risk factors, and causes learned/retained form program.
Key Component Objective
Specific - What is the specific task? Determine whether participants’ knowledge of the symptoms, risk factors, and causes of arthritis have increased as a result of participation in the program.
Measurable - What are the standards or parameters?
Number of participants who can identify the symptoms of arthritis; Number of participants who can identify the risk factors for arthritis; Number of participants who can identify the causes of arthritis

ARTHRITIS IN THE ELDERLY 16
Achievable - Is the task feasible? No, we cannot test the participants’ knowledge of ALL arthritis symptoms, risk factors, and causes learned/retained from program because there are more that 100+ types of arthritis/arthritis-related conditions.
Realistic - Are sufficient resources available? Yes, each participant will be required to complete the two questionnaires/examinations midway and at completion of the program.
Time-Bound - What are the start and end dates? Three months (duration of program implementation) – March 2014–May 2014
SMART Objective 1: Increase each participant’s knowledge about the symptoms, risk factors, and causes of their SPECIFIC FORM of arthritis.
Not-so-SMART Objective 2: Assess each participants’ daily and weekly time spent engaging in physical activity.
Key Component Objective
Specific - What is the specific task? Assess each participants’ time spent engaging in physical activity on a daily and weekly basis to determine if there has been an increase in time spent engaging in physical activity as a result of participating in the program.
Measurable - What are the standards or parameters?
Amount of time spent each day engaging in physical activity as reported by participants; Amount of time spent each week engaging in physical activity as reported by participants; Amount of time spent engaging in physical activity in total at end of program compared to start of program as reported by participants.
Achievable - Is the task feasible? Yes, participants can record time spend engaging in physical activity and these records can be used to determine if there has been an increase in physical activity levels.
Realistic - Are sufficient resources available? No, there aren’t enough program personnel to assess EACH participants’ daily/weekly physical activities in a timely manner; No time to commit to this activity on a daily basis due to other program activities
Time-Bound - What are the start and end dates? Three months (duration of program implementation) – March 2014–May 2014
SMART Objective 2: Assess participants’ TOTAL time spent engaging in physical activity at COMPLETION of the program compared to the time spend engaging in physical activity at the start of the program.
Not-so-SMART Objective 3: Participants cannot be evaluated and assessed equally due to differences in physical capabilities and arthritis symptom severity.
Key Component Objective
Specific - What is the specific task? Assess whether program participants are able to perform at least three physical activities learned during the program.
Measurable - What are the standards or Number of physical activities each participant is able to perform; Number of

ARTHRITIS IN THE ELDERLY 17
parameters? participants who can perform each physical activity
Achievable - Is the task feasible? Yes, each participant is evaluated and assessed according to what physical activities they can perform; There are a variety of physical activities taught to participants during program.
Realistic - Are sufficient resources available? Participants cannot all be evaluated and assessed equally because participants do not have the same physical capabilities and arthritis symptoms; some participants may be significantly limited in the activities they can engage in depending on their arthritis symptom severity.
Time-Bound - What are the start and end dates? Three months (duration of program implementation) – March 2014–May 2014
SMART Objective 3: Assess participants’ ability to perform physical activities learned during the program based on their individual physical capabilities and arthritis symptom severity.
Not-so-SMART Objective 4: Assess participants’ ability to plan, prepare, and consume anti-inflammatory foods.
Key Component Objective
Specific - What is the specific task? Determine whether participants’ knowledge of foods that cause or reduce arthritis inflammation and the ability to plan, prepare, and consume anti-inflammatory foods has increased as a result of participation in the program.
Measurable - What are the standards or parameters?
Ability to list foods that cause/reduce arthritis inflammation; Ability to plan and prepare anti-inflammatory foods
Achievable - Is the task feasible? Yes, when assessing whether participants are able to identify foods that cause or reduce inflammation caused by arthritis.
Realistic - Are sufficient resources available? No, we cannot assess participants’ ability to plan, prepare, and consume anti-inflammatory foods because some participants may have dietary restrictions or food sensitivities that may prevent them from consuming some of the foods recommended for their anti-inflammation properties.
Time-Bound - What are the start and end dates? Three months (duration of program implementation) – March 2014–May 2014
SMART Objective 4: Assess whether participants are able to IDENTIFY foods that cause or reduce inflammation.
Not-so-SMART Objective 5: Assessing participants’ level of pain accurately.
Key Component Objective
Specific - What is the specific task? Determine if there has been a decrease in participants’ reported level of pain as a result of participation in the program.

ARTHRITIS IN THE ELDERLY 18
Measurable - What are the standards or parameters?
Level of pain as recorded on pain scale (at the start of program, midway through, and at program completion)
Achievable - Is the task feasible? Yes, when evaluating each participants’ level of pain based on pain scale
Realistic - Are sufficient resources available? We cannot perform an accurate assessment of participants’ level of pain because it can be affected by factors such as symptom severity and may be controlled by use of medications, affecting actual levels of pain recorded.
Time-Bound - What are the start and end dates? Three months (duration of program implementation) – March 2014–May 2014
SMART Objective 5: Assess participants’ level of pain accurately through consideration of arthritis symptom severity and use of medications at the start of program, midway through, and at program completion (assuming all factors remained consistent).
Public Health Promotion: Tasks, People, and Timelines
Social marketing, as defined by Kotler, Lee, and Rothschild, is “a process that applies
marketing principles and techniques to create, communicate, and deliver value in order to
influence target audience behaviors that benefit society as well as the target audience” (2006). It
has been widely used in solving public health problems, has become part of the health domain,
and will play an even larger role in public health (Ling, Franklin, Lindsteadt, & Gearson, 1992).
The term social marketing is often used synonymously with advertising or mass media
campaigns seeking to shape attitudes, increase awareness, and encourage either the use of certain
services or changes in personal or collective behavior. Social marketing has its roots in social
advertising and a focus on messages but has since developed in several directions. It may be
viewed as an American invention in the 20th century because the concept was initially formulated
in the United States (Cheng, Kotler, & Lee, 2009), although the practice of social marketing as
well as successful social marketing campaigns can be found worldwide.
Social marketers utilize the 4Ps (product, price, place, and promotion) to create,
communicate, and deliver values for their targeted behaviors. Product involves benefits from
performing behaviors and any objects or services offered to assist adoption; Price includes any

ARTHRITIS IN THE ELDERLY 19
costs that will be associated with adopting the behavior; Place involves making access
convenient; and Promotion involves persuasive communications highlighting product benefits
and features, fair price, and ease of access (Cheng et al., 2009). Today, social marketing has been
applied to a broader array of public health activities/programs and has offered public health
professionals an effective approach for developing programs to promote health behaviors and has
also provided public health with a new institutional mindset in which solutions to programs are
solicited from consumers by means of conducting research to determine the target audience’s
needs and wants (Cheng et al., 2009). “An organization that has adopted the social marketing
mindset continually evaluated and remakes itself so as to increase the likelihood that it is
meeting the needs of its ever-changing constituency” (Coreil, Bryant, & Henderson, 2001).
Design program brochure
Contact facilities to distribute brochure
Revise/finalize brochure design
Send brochures to printing company
Disseminate program brochures
Create TV/radio PSA
Contact local TV and radio stations
Revise/finalize PSA
Air PSA on local TV/radio stations
Create newspaper ad
Contact local newspapers
Revise/finalize newspaper ad
Submit ad to newspapers for printing
Run newspaper ad
5-Jan 12-Jan 19-Jan 26-Jan 2-Feb 9-Feb 16-Feb 23-Feb
Arthritis in the Elderly Program - Gantt ChartJanuary - February 2014

ARTHRITIS IN THE ELDERLY 20
Gantt Chart. The Gantt chart above is a graphical representation of the tasks involved in
promotion, one of the 4Ps of social marketing. McKenzie, Neiger, and Thackeray describe a
Gantt chart as a tool used to provide “an indication of the progress made toward completing the
task by using different size lines to distinguish between the projected time frame for a task and
the progress toward completing the task” (2013, p. 349). The Gantt chart is very useful and
serves the same purpose for tracking the progress of the tasks identified in the Arthritis in the
Elderly program. There are three main tasks that are to be completed between January and
February 2014: 1) Design program brochure, 2) Create TV/radio PSA, and 3) Create newspaper
ad. Each task consists of 3-4 additional tasks, which will be referred to as subtasks. These
subtasks are essential because they also ensure that each task is completed within the projected
time frame to effectively promote the program. As such, the Arthritis in the Elderly program will
utilize two types of media, TV and radio PSAs, and will also use brochures and newspapers as
the materials for distributing information about the program and the services it offers.
The program brochures will serve a dual purpose both to promote the program and as a
program material distributed to program participants because the brochures contain valuable
information that is both beneficial and useful to the elderly population to as a reference for
general arthritis facts and statistics and as a tool to manage their arthritis symptoms. The
brochures will be distributed to individuals, local businesses, organizations, and institutions in
addition to local primary care providers, specialists, clinics, and retirement communities/elderly
homes that are involved in providing arthritis-related care and treatment to the elderly. The PSAs
will be broadcasted on local TV and radio stations because the elderly population is believed to
have access to a TV and/or a radio at the retirement/elderly care homes, their own homes, or the
homes of family and friends. This will be an effective method of promoting the program on a

ARTHRITIS IN THE ELDERLY 21
regular basis and at multiple times throughout the day and night to ensure that there are many
opportunities for the PSA to be heard. Finally, the newspaper ad will serve as a way to further
promote the program and the services it provides by reaching the elderly living with some form
of arthritis or those who have elderly family members or friends and provide care to them. By
distributing the brochures to relevant individuals, organizations, and institutions within the
community and utilizing the local TV and radio stations, local newspapers as a means of
promoting the Arthritis in the Elderly program, we are able to appeal to the target population,
and increase the amount of people we are able to reach. In addition, this presents an opportunity
to disseminate valuable information about our program and services that we otherwise would not
be able to do without using the selected media and materials.
Program Pro Forma
Budgetary Needs
“Arthritis in the Elderly” Program Pro FormaJanuary 2014 - May 2014
Revenue and Support AmountContribution from Sponsors $180,000.00Gifts $1,113.00Grants $11,000.00Participant Fee $0.00Sale of Curriculum Material $0.00
Total Income $192,113.00Expenditures AmountDirect CostsPersonnelSalary & Wages $167,032.11Program Director $23,243.94Program Assistant $20,452.45Medical Director $58,940.10Nutritionist/Dietician $17,415.00Personal Fitness Trainer/Wellness Coach $11,442.30Financial Advisor $2,733.32Arthritis-related Healthcare Providers (3) $32,805.00Fringe Benefits $900.00

ARTHRITIS IN THE ELDERLY 22
Consultants $142.02Program Director, Hawaii Arthritis Foundation $47.34Director of Lifestyles Kahala Nui $94.68SuppliesInstructional Materials $9,049.00Meeting Costs $300.00Equipment $4,599.00Travel $350.00Postage $250.00Advertising $3,550.00Incentives $0.00
Total of Direct Costs $177,123.13Indirect CostsRent $1,550.00Insurance $250.00Telephone & Fax $525.65Other Utilities $875.00
Total of Indirect Costs $3,200.65Total Expenditures $180,323.78
Balance $11,789.220
Salary and wages for the program personnel were determined by accessing the United
States Bureau of Labor Statistics site under the Occupation Employment Statistics page for the
May 2012 National Occupational Employment and Wage Estimates (U.S. Bureau of Labor
Statistics, 2013). To calculate the appropriate salary for each personnel participating in the
planning, implementation and evaluation of the program and its participants, I used the estimated
Mean Hourly Wage provided in the table according to occupation. Some of the program
personnel occupations were not listed on the Occupation employment Statistics page (Program
Director, Program Assistant, Program Director – Hawaii Arthritis Foundation, and Director of
Lifestyles Kahala Nui) and as a result, it was necessary to make a rough estimation as to what the
hourly rate would be, according to estimates of similar occupations. Upon identifying the
estimated Mean Hourly Wage for each of the nine personnel and two consultants, it was
necessary to approximate the number of hours that each individual contributed during the
program, approximately five months in length. From this point we were able to calculate the total

ARTHRITIS IN THE ELDERLY 23
salary for the program personnel. The table below shows calculations for the determining
program personnel salaries.
Program Occupation # Of People Hourly Wage Hours Total EarnedPersonnelProgram Director 1 $47.34 491 $23,243.94Program Assistant 1 $42.17 485 $20,452.45Medical Director 1 $91.38 645 $58,940.10Nutritionist/Dietician 1 $27.00 645 $17,415.00Personal Fitness/Wellness Coach 1 $17.74 645 $11,442.30Financial Advisor 1 $59.42 46 $2,733.32Arthritis-related Healthcare Providers 3 $27.00 405 $32,805.00ConsultantsProgram Director, Hawaii Arthritis Foundation 1 $47.34 1 $47.34Director of Lifestyles, Kahala Nui 1 $47.34 2 $94.68

ARTHRITIS IN THE ELDERLY 24
Program Evaluation Plan
An evaluation is “a systematic approach to gathering and analyzing performance,
programs, or services” (NWCPHP, 2013) which allows for informed decision making for the
future. Program planning and evaluation go hand-in-hand. Program evaluation documents a
program’s impact on the intended recipients and answers the question: Did the program produce
the desired results? It is necessary to perform adequate and appropriate program evaluations, by
utilizing the six steps of the CDC’s framework as the starting points to tailor the evaluations,
regardless of the size, type, or duration of the program. The two most critical and basic purposes
of program evaluation, according to McKenzie, Neiger, and Thackeray, include: 1) assessing and
improving quality, and 2) determining effectiveness (2013, p. 373). The Centers for Disease
Control and Prevention’s Framework for public health program evaluation is comprised of six
steps (CDC, 2011; McKenzie, Neiger, & Thackeray, 2013):
Step 1 – Engaging Stakeholders: Stakeholders include those who are involved in the program operations, those served or affected by the program, and the primary users of the evaluation results. It is important to involve stakeholders early in your program because stakeholders can provide different perspectives on the program and establish common expectations (NWCPHP, 2013).
Step 2 – Describing the program: The program should be described with enough detail that its mission, goals, and objectives are clearly understood. The capacity to effect change, stage of development, and how it fits into the larger picture should also be described.
Step 3 – Focusing the evaluation design: This step involves utilizing time and resources efficiently while ensuring that the interests of the stakeholders are addressed. Both the program processes and outcomes can be evaluated (NWCPHP, 2013).
Step 4 – Gathering credible evidence: Evaluators will decide on measures, sources of evidence, quality/quantity of evidence, and methods to collect the evidence. This step also involves data organization. Qualitative data provides descriptive information that illustrates experiences, behaviors, opinions, values, feelings, knowledge, and anything observable, whereas quantitative data is anything that can be measured (NWCPHP, 2013).

ARTHRITIS IN THE ELDERLY 25
Step 5 – Justifying conclusions: Evaluators will justify conclusions using five elements: standards, analysis/synthesis, interpretation, judgment, and recommendations. The NWCPHP (2013) states that this step is where program evaluators can answer the question: “Are we getting better, getting worse, or staying the same?”
Step 6 – Ensuring use and sharing lessons learned: This step requires that the needs of the stakeholders be addressed and it also focuses on the use and dissemination of the evaluation results. Stakeholders can use the program evaluation data to determine whether a program is effective and should continue or is ineffective and be stopped.
Evaluation encourages program personnel to closely examine the operations their
program and can show how well the program has followed implementation protocols. As such,
evaluation helps to determine if program activities are being implemented as originally planned
and to identify the strength, weaknesses, and areas for improvement within the program (CDC,
2006). It is also a tool that can demonstrate accountability of the program to the stakeholders.
Depending on the needs of stakeholders, program evaluation may demonstrate that the program
contributes to reducing morbidity or mortality or relevant risk factors; that the funding is being
spent in an appropriate and effective manner; or that more funding, support, and policy change
may be needed to produce improved health outcomes (CDC, 2006). When programs are held
accountable, program evaluation can help to ensure that the most effective approaches are being
maintained and that the limited resources are used efficiently.
Program evaluation can, and should, be done at various phases of the program. The
American Psychological Association asserts that evaluations should not just be done as a one-
time event to prove that the progress was either a success or a failure (2013). It is important to
remember “program success is contingent on continuous feedback” (APA, 2013). Rather than
proving that a program was good or bad, program evaluation verifies that the program is running
as originally planned, identifies the strengths and weaknesses, and allows for continuing

ARTHRITIS IN THE ELDERLY 26
feedback in order to adjust the program accordingly (APA, 2013). Evaluation is essentially an
applied research activity seeking to discover whether a program has beneficial effects for the
public’s health. The program may be a specific activity within a public health clinic or a
comprehensive communitywide activity. Evaluations may involve determining if an activity or
series of activity have worked (past) or if they are currently working (present) to ensure that the
program is accountable and that there is improvement in the outcomes. Finally, evaluations can
help program planners, stakeholders, and decision makers become more aware of what
components of the program work best for the target population, whether the target population is
receiving the best possible values of the services offered by the program, and how to
increase/improve the impact of existing programs (Stoto & Cosler, 2008).
Outcome Measurements and Standards
Arthritis in the Elderly Evaluation ChartFormative Elements Definition How is this element addressed in the program?Justification Degree to which a program,
service, or activity is mandated or approved by relevant stakeholders and justified by needs assessment data and analysis
This program is supported and approved by the Director of the Hawaii Arthritis Foundation, Director of the Kahala Nui retirement community (setting for the program and where majority of the participants were recruited), Medical Director of Kahala Nui, Nutritionist/dietician, personal trainer/wellness coach, and other arthritis-related healthcare providers. The needs assessment justifies the need for this program because arthritis is the most common medical condition in the world, is one of the leading causes of disability in the U.S., but has no known cure (Johns Hopkins Arthritis Center, 2013). In addition, osteoarthritis, one of the most common forms of arthritis, affects nearly 80 percent of people 65 and older. Tailoring the program for each individual participant to include a combination of behavior changes regarding nutrition and physical activity can benefit participants and reduce the impact and severity of their arthritis symptoms. Both professional care and self-care are essential to treating/living with arthritis, in addition to a carefully planned, individualized treatment program that offers the best chance of reducing the impact of arthritis on participants' lives.
Evidence Degree to which the program, service, or activity is evidence based (i.e., documented evaluation results in the literature suggest the program is
The literature suggests that activities such as walking, cycling, water aerobics, strength training, and low-impact exercises can aid in decreasing pain and improving range of motion in people with arthritis (Vad, 2006). Studies show that short periods of initial instruction followed by self-directed exercise result in improved strength, function, and

ARTHRITIS IN THE ELDERLY 27
effective or at least promising)
decreased pain (Gach, 2001). Low-intensity range-of-motion exercises can provide addition benefits such as flexibility and joint motion. Director and Medical Director of Kahala Nui confirmed an interest in and identified the relevance of the program/activities for the residents.
Capacity Extent to which professionals have adequate knowledge, skills, and abilities to design and implement a program, service, or activity or the degree to which they can access or contract with other organizations and professionals to provide the same program, service, or activity
Medical Director, Kahala Nui: provides input into clinical policies governing Kahala Nui; supervises medical staff; oversees clinical safety, risk management, and participant care; involved at all levels of individualized care and supervision; assesses and educates participants on proper nutrition and adequate exercise/physical activity; monitors participants' arthritis symptoms. Program Director, Hawaii Arthritis Foundation: provides contacts specifically within the target population (i.e., retirement/senior citizen homes in the community) to contact as potential locations for program implementation; establishes contacts with local organizations/businesses such as farmers markets and fitness centers in the community. Nutritionist/Dietician: provides nutritional care and education to participants; assess nutrition status of participants; monitor nutritional plan and progress; construct, implement, evaluate, and document care plans; coordinates nutritional care with Medical Director and other healthcare providers. Personal Fitness Trainer/Wellness Coach: assess needs and capabilities of participants; advises participants on proper form/technique for exercises; develops individualized exercise program based on participant's needs/fitness level; counsels participants to developing realistic, attainable goals; consult with Medical Director and other healthcare provider to modify exercise plan as necessary.
Resources Adequacy of resources (e.g., budget, community resources or assistance, assets, time, etc.)
The funding for this program includes contributions from sponsors, gifts, and grants. No participant fee included and no charge for participants as they are residents at Kahala Nui retirement community. The program will utilize community resources such as the local YMCAs and fitness/recreation facilities and the local farmers markets that will offer program participants discounted rates for using exercise equipment/facilities and to allow participants to purchase fresh produce.
Consumer-Operations Degree to which the program, activity, or service is tailored to the priority population (i.e., culturally appropriate and based on consumer preferences)
This program was designed specifically for elderly individuals who have some form of arthritis and can be tailored to address each individual's unique arthritis symptoms, physical capabilities, and nutritional needs/restrictions. The idea of customizing the program appeals to the participants and that allows them address their unique needs and achieve their personal goals. The program also focuses on the diverse culture of Hawaii and its people while also incorporating the aloha spirit with every interaction and at each phase of the program to resolve any problem and accomplish any goal.
Multiplicity Degree to which multiple components (i.e., intervention strategies) are built into the program, service or activity (e.g.,
Educating participants on: their specific form of arthritis and associated symptoms; foods that cause inflammation or are anti-inflammatory; how to shop for/prepare anti-inflammatory foods based on nutritional needs/restrictions; engaging in regular physical activity; specific activities and

ARTHRITIS IN THE ELDERLY 28
education, communication, policy, environmental change, etc.)
exercises they can perform based on their physical capabilities and symptoms. Communicating with all participants during weekly face-to-face meetings with the Medical Director, dietician/nutritionist, personal trainer/wellness coach, and other arthritis-related healthcare providers to assess the progress, symptoms (improvement/worsening), and behavioral change to engage in regular physical activity and consume anti-inflammatory foods, and address any questions and/or concerns.
Support Degree to which a support component is built into a program, service, or activity (e.g., a hot line/quit line for a tobacco media campaign, development of walking paths for a community physical activity campaign)
The Medical Director, Nutritionist/Dietician, personal trainer/wellness coach and other arthritis-related healthcare providers meet face-to-face with participants 1-2 times each week throughout the duration of the program (3 months).These face-to-face meetings offer participants with the support and counseling necessary to ensure that they are confident in their ability to maintain the positive health behaviors (consuming nutritious anti-inflammatory foods and engaging in regular physical activity) that were learned and adopted as a result of participation in the program.
Inclusion Extent to which an adequate range and number of appropriate partners or organizations are involved with the program, service, or activity
The program is affiliated with the Hawaii Arthritis Foundation, local YMCAs and other fitness/recreation facilities, local farmers markets, arthritis-related healthcare providers, nutritionists/dieticians, and personal fitness trainers/wellness coaches that each plays a vital role in the success of the program and its participants.
Accountability Extent to which internal staff and external partners are fulfilling their responsibilities as planned and are communicating needs appropriately
All program staff including the Medical Director, nutritionist/dietician, personal trainer/wellness coach, and other arthritis-related healthcare providers successfully perform and fulfill their responsibilities by meeting with participants on a regular basis to assess/reassess each individual's nutritional and physical needs/progress made, modify each participant's diet/nutritional and/or exercise plan as need, and to examine the quality of life and level of pain of each participant.
Adjustment Degree to which programs, services, or activities are modified based on feedback received from participants, partners, or other stakeholders
The program was specifically designed to be entirely customizable for each individual's specific type of arthritis and the associated symptoms as well as each participant’s unique nutritional and physical needs. Participants are able to meet with program personnel on a regular basis during scheduled meetings and also have the option to meet more frequently and at any time as they feel is necessary. This allows participants to have the ability to continuously modify and adjust their nutritional and physical activity plan should their symptoms improve or worsen, or if their needs and goals should change at any time throughout the program. The Medical Director, nutritionist/dietician, personal fitness trainers/wellness coaches, and other arthritis-related healthcare providers are encouraged to provide feedback to the Arthritis in the Elderly program director regarding the activities and services offered to participants to determine if they are effective or if they do not benefit the participants in ways that they were projected to do.
Recruitment* Degree to which members of the priority population are adequately recruited through
Participants were recruited from Kahala Nui, as retirement community, where a significant number of the target population resides. The Director and Medical Director of

ARTHRITIS IN THE ELDERLY 29
appropriate channels and places consistent with cultural and other unique characteristics
Kahala Nui expressed that many of the residents had some form of arthritis. The belief was that many of them would be interested in the services/activities being offered and the potential benefits of participating in a program that is entirely customizable depending on the unique symptoms and nutritional needs and physical capabilities/restrictions.
Reach* Proportion of the priority population given the opportunity to participate in the program, activity, or service
As mentioned in the Recruitment element, this program was implemented at a single retirement community, Kahala Nui. The priority population of the Arthritis in the Elderly Program includes individuals 62 years of age and older, who has some form of arthritis. Those residents who had not heard about the program initially, but were identified as having arthritis by either another resident or the Medical Director, were invited and encourage to participate.
Response* Proportion of the priority population actually participating in the program, activity, or service
All residents of Kahala Nui retirement community who had some form of arthritis willingly participated in the program and worked in collaboration with program personnel to design a nutritional and physical activity plan tailored specifically to address their unique arthritis symptoms, the severity of those symptoms, nutritional needs/restrictions, physical capabilities/limitations, and goals to be achieved.
Interaction Quality of interactions (e.g., customer service; interpersonal, counseling, and presentation skills; clarity of instructions) between professionals (those providing programs, services, and activities) and participants
The Medical Director, Nutritionist/Dietician, personal trainer/wellness coach and other arthritis-related healthcare providers maintained effective communication with all program participants during one-on-one, face-to-face counseling sessions and regularly scheduled meetings. The professionals ensured that each participant understood the information they were given and further explained/clarified what they did not with regard to nutrition and/or physical activity. The program personnel discussed progress made or identified any areas where the participant is struggling/regressing and tailored their plan accordingly.
Satisfaction Degree to which the needs of participants are being met, how satisfied they are with the program, service, or activity, and their belief that a positive impact is being made in their lives
It is important to reiterate that the Arthritis in the Elderly Program is entirely customizable and can be tailored at any point during the program to address each participant's needs and help them to achieve their personal goals. This customizability appeals to all participants because they are receiving the necessary professional care for their arthritis symptoms and they are also presented with the opportunity to adopt valuable arthritis self-management skills, knowledge, and behaviors. Utilizing the skills, knowledge, and behaviors gained will be beneficial for them to successfully care for themselves and manage their arthritis symptoms, increasing their confidence to maintain these self-management behaviors while reducing their symptoms/pain and improving their overall quality of life.
Process Elements Definition How is this element addressed in the program?Fidelity Extent to which the program,
activity, or service was delivered as planned or as per protocol including the use of Gantt charts (i.e., time lines) and logic models
Each task was completed in a timely manner by utilizing the timelines established by program personnel. The tasks identified were essential in delivering the program and the planned activities to all participants in a timely, organized manner to ensure that the participants reaped the benefits of the skills and knowledge learned, thus allowing them to successfully adopt arthritis self-management behaviors.
Dose Number of program units The most common method of disseminating information

ARTHRITIS IN THE ELDERLY 30
delivered (e.g., presentations, products, services, messages)
throughout the duration of the program included face-to-face meetings and consultations with all participants. Each participant met with the Medical Director, nutritionist/dietician, personal trainer/wellness coach, and other arthritis-related healthcare providers on a regular basis (1-2 times per week with each participant for 3 months) to assess nutritional needs/restrictions and physical capabilities/limitations, assess quality of life and level of pain, advise and assist each individual in the development of a personalized nutritional and exercise plan, and address any questions/concerns. In addition, group sessions (5 group sessions per week for 2 weeks, total of 10 group sessions) were held to educate participants on the foods that cause and reduce inflammation caused by arthritis and to advise and instruct participants on the proper form of a variety of fitness activities.
Context External factors that may influence program results (e.g., competing programs, conflicting messages, other confounders)
While there are arthritis programs that have already been established and implemented, the Arthritis in the Elderly Program is unique in that it targets a specific population and can be tailored to each individual according to their personal needs and goals they hope to achieve as a result of participating in the program. Although the Arthritis in the Elderly Program is relatively new and still in its infancy compared to other well-known arthritis programs, it does incorporate many of the components from the most successful programs. It is designed in such a way that recognizes the diversity of Hawaii and its people, a component that many other programs do not have, which ultimately shows that this program is centered around the participants and has their best interests in mind from start to completion.
Program Strategies Summary
Program planners, stakeholders, and decision makers perform a program evaluation as a
means of tracking the progress of the program to achieve its objectives. It is important to select
data indicators based on program objectives because they measure the activities designed
specifically to produce desired outcomes as well as the program focus and specific circumstances
in the community of interest. These indicators (also referred to as measurements) can be either
qualitative or quantitative. Measurement is the process of applying numerical or narrative data
from an instrument or other data-yielding tools to objects, events, or people (McKenzie, Neiger,
& Thackeray, 2013). Quantitative measures are “numerical data collected to understand

ARTHRITIS IN THE ELDERLY 31
individuals’ knowledge, understanding, perceptions, and behavior” whereas qualitative measures
are “data collected with the use of narrative and observational approaches to understand
individuals’ knowledge, perceptions, attitudes, and behaviors” (McKenzie et al., 2013). The five
objectives of the Arthritis in the Elderly Program as aforementioned and listed in the table below
include: Identifying the symptoms, risk factors, and causes of arthritis; Increasing the time spent
engaging in physical activity; Increasing the knowledge and ability to plan, prepare, and
consume anti-inflammatory foods to improve the symptoms of arthritis; Performing at least three
physical activities taught during the program; and Decreasing the level of pain caused by
arthritis.
Arthritis in the Elderly Summative Evaluation Table
Program Objectives Data Indicators/ Measures Data Collection Tool(s) Data Analysis Measurement
TimelinesIdentify the symptoms, risk factors, and causes of arthritis
Qualitative Group meeting/information session; Individual, in-depth face-to-face interview/meeting
Multivariate 3 months
Increase the time spent engaging in physical activity
Qualitative; Quantitative
Individual, in-depth face-to-face interview/meeting; Questionnaire
Univariate 3 months
Increase the knowledge and ability to plan, prepare, and consume anti-inflammatory foods to improve the symptoms of arthritis
Qualitative Group meeting/information session; Individual, in-depth face-to-face interview/meeting
Multivariate 3 months
Perform at least three physical activities taught during the program
Qualitative Group meeting/information session; Individual, in-depth face-to-face interview/meeting; Questionnaire
Univariate 3 months
Decrease the level of pain caused by arthritis
Qualitative; Quantitative
Individual, in-depth face-to-face interviews/meeting; Questionnaire
Univariate 3 months
In order to determine if the program was successful in achieving the five objectives, a
combination of methods including individual, in-depth face-to-face interviews/meetings, group
meetings/information sessions, and distribution of a simple questionnaire were used. Individual,
in-depth face-to-face interviews/meetings were conducted on a regular basis, approximately 1-2
times a month, with each participant. Group meetings and information sessions were conducted

ARTHRITIS IN THE ELDERLY 32
for two weeks, which involved five group meetings per week, to educated participants on which
foods caused and reduced inflammation caused by arthritis and to advise participants on the
proper form for a variety of fitness activities taught during the program. The data were collected
over a three-month period, the duration of the program.
The individual, in-depth face-to-face interviews/meetings were conducted to assess the
nutritional status of all participants by reviewing medical records and diet histories; assess the
needs and capabilities of all participants through fitness assessments and physical examinations;
assess and document the quality of life and level of pain by distributing a questionnaire to
participants and interviewing each individual; develop a customized diet/nutrition and
exercise/physical activity plan. In addition, the meetings and interviews with each participant
served the purpose of monitoring the customized diet/nutritional and exercise/physical activity
plans designed for each participant and allowed program personnel to reassess the nutritional
needs and physical capabilities and the quality of life and level of pain of each participant to
determine if any progress has been made and if individuals adopted positive health behaviors as
a result of program participation. Finally, the questionnaires were distributed to all participants at
the beginning of the program and upon completion of the program to determine the time spent
engaging in physical activity and quality of life and level of pain caused by arthritis. A
comparison of the two questionnaires were used along with the qualitative data obtained during
the individual, in-depth face-to-face interviews/meetings to identify whether there was an
increase the time spent engaging in physical activity and if participants’ level of pain caused by
arthritis decreased as result of participating in the program.
McKenzie, Neiger, and Thackeray defined three types of statistical analyses to measure
the association and relationships between and among variables: univariate data analysis,

ARTHRITIS IN THE ELDERLY 33
analyzing one variable; bivariate data analysis, analysis of two variables; and multivariate data
analysis, analysis of more than two variables (2013). The two objectives that use multivariate
data analysis include an individual’s ability to identify the symptoms, risk factors, and causes of
arthritis, specifically the type of arthritis unique to them and whether an individual exhibits an
increase in their knowledge and ability to plan, prepare, and consume anti-inflammatory foods.
The evaluation question that can be answered using multivariate analysis is: “Is the participant
able to identify the symptoms, risk factors, and causes of arthritis associated with their form of
arthritis?” and “Does the participant exhibit an increase in his/her knowledge and ability to plan,
prepare, and consume anti-inflammatory foods to improve their arthritis symptoms?” The
remaining three objectives are analyzed using univariate data analysis and focus on determining
whether an individual spends more time engaging in physical activity; performing at least three
physical activities taught during the program; and if there was a decrease in their arthritis-related
pain. Univariate data analysis can answer the evaluation questions: “Is there an increase in the
time spent engaging in physical activity at program completion compared to the beginning of the
program?” “Is the participant able to perform at least three physical activities as a result of
participating in the program?” and “Does the participant report a decrease in their level of pain
caused by arthritis at completion of the program?”
Qualitative data was the primary data indicator/measure used throughout the program and
provides program evaluators with detailed explanations from each participant, which shows that
the program was successful in successfully achieving the program objectives. It is evident that
the data collected at program completion will be useful in improving and continuing the Arthritis
in the Elderly Program to serve others in the target population.

ARTHRITIS IN THE ELDERLY 34
References
American Psychological Association, Behavioral & Social Science Volunteer Program. (2013). The role and importance of program monitoring and evaluation. Retrieved from website: http://www.apa.org/pi/aids/programs/bssv/program-monitoring-evaluation.pdf
Bernstein, S., & Klippel, J. (2003). The arthritis foundation’s guide to pain management. Atlanta, GA: Arthritis Foundation.
Centers for Disease Control and Prevention, Office of the Associate Director for Program. (2011). Program evaluation steps. Retrieved from website: http://www.cdc.gov/eval/steps/index.htm
Centers for Disease Control and Prevention, Office of the Director, Office of Strategy and Innovation. (2006). Introduction to program evaluation for public health programs. Retrieved from website: http://www.cdc.gov/eval/steps/index.htm
Dunkin, M., & Klippel, J. (2001). The arthritis foundation’s guide to managing your arthritis. Atlanta, GA: Arthritis Foundation.
Gach, M. R. (2001). Arthritis relief at your fingertips: The complete self-care guide to easing aches and pains without drugs. New York, NY: Warner Books.
Hunder, G. (2002). Mayo clinic on arthritis: Conquering the pain and leading an active life. (2nd ed.). Rochester, Minnesota: Mayo Foundation for Medical Education & Research.
Iannucci, L., & Horowitz, M. (1999). The unofficial guide to overcoming arthritis. (1st ed.). New York, NY: Macmillan.
Johns Hopkins Arthritis Center. Johns Hopkins Division of Rheumatology, (2013). Arthritis research. Retrieved from website: http://www.hopkinsarthritis.org/arthritis-research/
Johns Hopkins Arthritis Center. Johns Hopkins Division of Rheumatology, (2012). Osteoarthritis information. Retrieved from website: http://www.hopkinsarthritis.org/arthritis-info/osteoarthritis/
Johns Hopkins Arthritis Center. Johns Hopkins Division of Rheumatology, (2012). Rheumatoid arthritis. Retrieved from website: http://www.hopkinsarthritis.org/arthritis-info/rheumatoid-arthritis/
King, S. K. (2003). The aloha spirit. Retrieved from http://www.alohainternational.org/html/aspirit1.html
Lam, P., & Horstman, J. (2002). Overcoming arthritis: How to relieve pain and restore mobility through a unique tai chi program. (1st ed.). New York, NY: DK Publishing.

ARTHRITIS IN THE ELDERLY 35
McKenzie, J. F., Neiger, B. L., & Thackeray, R. (2013). Planning, implementing, & evaluating health promotion programs: A primer. (6 ed.). Pearson Education, Inc.
Northwest Center for Public Health Practice. University of Washington, School of Public Health. (2013). Six steps of program evaluation. Retrieved from website: http://www.nwcphp.org/evaluation/learn-evaluation/program-evaluation-tips
Ripp, J. M., McCarthy, S., & Waite, M. (2001). The joint health prescription: 8 weeks to stronger, healthier, younger joints. New York, NY: St. Martin's Press.
Stoto, M. A., & Cosler, L. E. (2008). Evaluation of public health interventions. In L. Novick, C. Morrow & G. Mays (Eds.), Public Health Administration: Principles for Population-Based Management (2nd ed., pp. 495-539). Retrieved from http://www.jblearning.com/samples/0763738425/38425_00fm_i_xxiv.pdf
U.S. Department of Labor Statistics, Division of Occupational Employment Statistics. (2013). Occupational employment statistics: May 2012 national occupational employment and wage estimates United States. Retrieved from website: http://www.bls.gov/oes/current/oes_nat.htm
Vad, V. (2006). Arthritis Rx: A cutting-edge program for a pain-free life. New York, NY: Gotham Books.











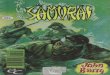







![585 Actuator Manual Active]](https://img.pdfslide.us/doc/110x75/55019c594a795971028b4795/585-actuator-manual-active.jpg)







