Embed Size (px)
DESCRIPTION
Prognostic Value of Lemur Tyrosine Kinase-3 (LMTK3) Polymorphism in Japanese Patients with Localized Gastric Adenocarcinoma Afsaneh Brazi 1 , Takeru Wakatsuki 1 , Wu Zhang 1 , Dongyun Yang 2 , Fotios Loupakis 1 , Nin Yang 1 , Rita El-Khoueiry 1 , Melissa J LaBonte 1 , Mizutomo Azuma 1 , - PowerPoint PPT Presentation
Citation preview

Prognostic Value of Lemur Tyrosine Kinase-3 (LMTK3) Polymorphism in Japanese Patients with Localized Gastric Adenocarcinoma
Afsaneh Brazi1, Takeru Wakatsuki1, Wu Zhang1, Dongyun Yang2, Fotios Loupakis1, Nin Yang1, Rita El-Khoueiry1, Melissa J LaBonte1, Mizutomo Azuma1, Pierre Bohanes1, Leonor Benhaim1, Armin Gerger1, Georgios Giamas3, Justin Stebbing3, and Heinz-Josef Lenz1,2
1. Department of Medical Oncology, University of Southern California/Norris Comprehensive Cancer Center, Los Angeles, CA 2. Department of Preventive Medicine, University of Southern California/Norris Comprehensive Cancer Center
3. Department of Surgery and Cancer, Division of Cancer, Imperial College London, London,UK
We obtained either blood or FFPE tissue specimens from 169 localized (stage Ib-IV) GAC patients (60 females &109 males). Genomic DNA was extracted using the QIAmp kit. All samples were analyzed by means of PCR-based direct DNA- sequencing.All patients were treated with D2 surgery with or without adjuvant fluoropyrimidine based Chemotherapy at Fukushima Red Cross and Kitasato University East Hospitals. The median follow-up were 4 years. The primary and secondary endpoints of the study were disease-free survival (DFS) and overall survival (OS). To evaluate prognostic value of this polymorphism, endpoints were estimated using Kaplan-Meier method and compared by log-rank test. The level of significance was set to p < 0.05, and all statistical tests were two-sided. Multivariate analysis was performed to test the interaction between polymorphism and gender adjusting for other variables. All statistical cells performed using the SAS statistical package version 9.2 (SAS Institute, Cary, NC).
LMTK3 is a modulator of estrogen receptor (ER)α. Its level of expression and its germline polymorphism is prognostic and predictive of estrogen resistance in breast cancer.(1,2) Epidemiologic studies support that estrogen exposure is protective against intestinal type gastric cancer. Furthermore expression of ERα and lack of expression of ERβ are poor prognostic markers in gastric adenocarcinoma (GAC).(3)We have previously demonstrated that rs9989661(r9) AA allele is associated with shorter time to recurrence in non-metastatic GAC only in females in a US cohort of patients.(4) GAC has diverse pathologic pathways and risk factors in different racial backgrounds and geographic areas. Additionally, the allelic frequency of LMTK3 in Japanese population is different. We intended to verify the prognostic value of LMTK3 and its polymorphism in a cohort of Japanese patients with GAC.
These results confirm our previous findings that LMTK3 is an independent prognostic factor for localized GAC. Interestingly the relationship between gender and prognostic significance is the opposite in Japanese cohort. The gender disparity can be due to the differences in the etiology (histological subtypes), management strategies, allele frequency, and
degree of estrogen exposure in the two populations. Additional studies are warranted to identify the underlying biological mechanism.
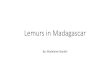
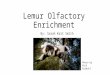
Characteristics of the patients in this cohort are reported in table 1. The median age of the cohort was 67(31-88). Prognosis was worse in men with rs9989661 AA than AG/GG. At 3-years probability of DFS was 39%(95%CI 17-60%) vs. 56% (95%CI 45-66%) and OS was 44% (95%CI 21-67%) vs. 66% (95%CI 56-77%) in patient harboring AA vs AG/GG group (P= 0.03 & 0.039 respectively).
Median survival was not reached in the AG/GG group; in the AA group median DFS was 1 yr and OS 2ys. In the multivariate analysis adjusting for stage, age, and ACT, males carrying rs9989661 AA had increased risk of disease recurrence (HR 4.37 95%CI 2.08-9.18, p < 0.001) and dying (HR 3.69 95%CI 1.65-8.24 p = 0.002) compared to those with AG/GG (HR=1, reference). There was no statisticaly significant finding in females.
Abstract ID:
Results
Conclusions
Introduction
Methods
4088
References
1. Giamas, G., et al. Nat Med. 2011 ; 17(6):715-9.2. Stebbing, J., et al. Breast Cancer Res Treat. 2012 132(2): 537-44.3. Xu, C.Y., et al. Annals of surgical oncology, 2010. 17(9): 2503-9.
4. Wakatsuki, T et al. Gastrointestinal Cancer Symposium. 2012, abstract 63.
0 5 10 15 200.0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
1.0LMTK3rs9989661 in males
G/G, G/A (n=90)
A/A (n=18)
Years Since Surgery
Est
ima
ted
P
rob
ab
ility
o
f D
ise
ase
-Fre
e S
urv
iva
l
Log-rank p value = 0.030
0 5 10 15 200.0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
1.0LMTK3rs9989661 in males
G/G, G/A (n=90)A/A (n=18)
Years Since Surgery
Est
ima
ted
P
rob
ab
ility
o
f O
vera
ll S
urv
iva
l Log-rank p value = 0.039
Characteristics N(%) Median DFS, yrs HR (95%) P-value Median OS, yrs HR (95%) P-valueAge 0.001 <.001 <65 65 (38%) 20.1+ (4.8, 20.1+) 1 (Reference) 20.1+ (5.7, 20.1+) 1 (Reference) 65-74 60 (36%) 9.0+ (1.7, 9.0+) 1.59 (0.92, 2.75) 4.3 (2.8, 9.0+) 1.97 (1.08, 3.60) 75+ 44 (26%) 1.7 (1.2, 2.5) 2.67 (1.53, 4.65) 2.1 (1.5, 2.8) 4.04 (2.18, 7.49) Sex 0.980 0.50 Male 109 (64%) 4.8 (2.0, 20.1+) 1 (Reference) 5.7 (3.4, 20.1+) 1 (Reference) Female 60 (36%) 16.1+ (1.9, 16.1+) 1.01 (0.64, 1.59) 3.9 (2.7, 16.1+) 1.18 (0.73, 1.91) Stage <.001 <.001 IB 28 (16%) 20.1+ 1 (Reference) 20.1+ 1 (Reference) II 53 (31%) 16.1+ (2.4, 16.1+) 4.56 (1.38, 15.11) 16.1+ (3.4, 16.1+) 3.96 (1.20, 13.12) III 60 (36%) 2.5 (2.0, 6.3+) 6.45 (2.00, 20.80) 4.3 (2.7, 6.3+) 5.27 (1.63, 17.03) IV 28 (16%) 0.7 (0.4, 1.6) 17.30 (5.22, 57.29) 1.2 (0.8, 2.7) 15.71 (4.72, 52.27) Tumor Site 0.230 0.19 Lower 55 (32%) 2.3 (1.6, 16.1+) 1 (Reference) 16.1+ (2.1, 16.1+) 1 (Reference) Middle 59 (35%) 20.1+ (2.0, 20.1+) 0.87 (0.51, 1.46) 4.1 (3.0, 20.1+) 0.89 (0.51, 1.54) Upper 49 (29%) 15.2+ (3.0, 15.2+) 0.69 (0.38, 1.23) 5.7 (3.9, 15.2+) 0.66 (0.35, 1.22) GEJ 3 (2%) 2.2 (1.1, 2.3) 1.99 (0.60, 6.58) 2.8 (1.4, 2.9+) 2.28 (0.68, 7.61) UML 3 (2%) 0.9 (0.9-2.0) 2.22 (0.52, 9.44) 4.0+ - Differentiation 0.670 0.63 Well – Mod 68 (40%) 20.1+ (1.9, 20.1+) 1 (Reference) 20.1+ (3.4, 20.1+) 1 (Reference) Poor 101 (60%) 3.0 (2.2, 7.2+) 1.10 (0.70, 1.74) 4.3 (3.0, 7.2+) 1.12 (0.69, 1.82) PS <.001 <.001 ECOG 0 157 (93%) 20.1+ (2.9, 20.1+) 1 (Reference) 20.1+ (3.9, 20.1+) 1 (Reference) ECOG 1 12 (7%) 1.2 (0.3, 1.9) 3.41 (1.79, 6.47) 1.2 (0.2, 2.3) 4.75 (2.45, 9.22) Chemotherapy 0.008 0.07 No 60 (36%) 20.1+ 1 (Reference) 20. 1+ 1 (Reference) Yes 109 (64%) 2.3 (1.9, 4.8) 1.97 (1.18, 3.30) 3.4 (2.8, 16.1+) 1.62 (0.96, 2.75)









![ARTICLE IN PRESS ACCEPTED FOR PUBLICATION IN ......prognostic factors for poor survival in PDAC [8,9]. Masitinib is a potent oral tyrosine kinase inhibitor (TKI) that targets a limited](https://img.pdfslide.us/doc/110x75/61328b26dfd10f4dd73a84d0/article-in-press-accepted-for-publication-in-prognostic-factors-for-poor.jpg)






![The red ruffed lemur[1]](https://img.pdfslide.us/doc/110x75/5451a068af7959b9648b5e19/the-red-ruffed-lemur1.jpg)








