Embed Size (px)
Citation preview

Prognostic significance of venous tumourthrombus consistency in patients with renalcell carcinoma (RCC)Valerie L. Weiss, Martin Braun*†, Sven Perner*†, Andreas Harz‡, Roland Vorreuther‡,Glen Kristiansen*, Stefan C. Müller and Jörg EllingerKlinik und Poliklinik für Urologie und Kinderurologie, Universitätsklinikum Bonn, *Institut für Pathologie, †Institut fürProstatakarzinom-Forschung, and ‡Urologische Abteilung, Evangelische Kliniken Bonn, Bonn, Germany
V.L.W. and M.B. contributed equally to the work.
Objectives• To identify the prognostic impact of venous tumour
thrombus (VTT) in locally advanced renal cell carcinomas(RCCs).
• To further differentiate the clinical course of patients withVTT who have similar clinicopathological characteristics.
Patients and Methods• We determined the VTT consistency (solid vs friable)
in a retrospective cohort of 200 patients with RCCwho had undergone nephrectomy between 1994 and 2011.
• We examined the correlation of VTT consistency in thesepatients with clinical and pathological variables.
Results• A total of 65% of the patients had solid VTT and 35% had
friable VTT, which has a significantly lower amount ofcell-cell adhesion molecules and connective tissue than solidVTT.
• We found that friable VTT was associated with advanced pTstage, higher VTT level, papillary RCC subtype and a lowerage.
• Patients with friable VTT had a significantly shorter medianoverall survival than those with solid VTT (29 vs 89months), but VTT consistency was not found to bean independent predictor of patients’ survival in themultivariate Cox analysis.
• We found that VTT consistency was an independentsignificant predictor of overall survival in patients withoutevidence of distant and nodal metastases(N = 119).
Conclusions• The VTT consistency is caused by the tumour and not by
different surgical handling.• Friable VTT is an important adverse prognostic predictor of
overall survival in patients with non-metastatic RCC.
Keywordsrenal cell carcinoma, RCC, tumour thrombus, metastasis,survival, prognosis
IntroductionRenal cell carcinoma is one of the most commonmalignancies [1]. Improved diagnostics have led to a stagemigration in RCC, but a third of patients are diagnosedat an advanced stage, which is still highly lethal [2]. Venoustumour thrombus (VTT) is observed in 12–19% of patientswith RCC [3–5], and is associated with a poor prognosis[6,7]. The clinical variables tumour size, Fuhrman grade,nodal/distant metastases and VTT level are predictiveof a patient’s outcome [8], but the clinical course ofpatients with similar characteristics is still heterogeneous,
and additional variables to guide patient counselling arewarranted.
Recently, Bertini et al. [3] reported that VTT consistency hadan impact on patients’ survival and, specifically, that thepresence of friable VTT was an independent predictor of poorsurvival; however, to date, the findings of their retrospectivestudy have not been confirmed in an independent cohort. Theaim of the present study, therefore, was to assess a cohort ofpatients with RCC and VTT, to classify the VTT histologically(friable vs solid) and to assess the impact of this histology onpatients’ survival.
© 2013 The AuthorsBJU International © 2013 BJU International | doi:10.1111/bju.12322 BJU Int 2014; 113: 209–217Published by John Wiley & Sons Ltd. www.bjui.org wileyonlinelibrary.com

Material and MethodsPatients
After approval from our local ethics committee (vote number331/11), we reviewed the archived files of the Department ofPathology at the University Hospital Bonn and identifiedpatients who had undergone surgery for RCC at theUniversitätsklinikum Bonn and the Evangelische KlinikenBonn, Germany, between 1994 and 2011. We identified 200from 1657 patients with RCC and VTT (12.07%) who hadundergone radical nephrectomy and thrombectomy. Table 1
shows the detailed clinicopathological characteristics of thesepatients. The patients’ records were then reviewed to assessthe following information: age; gender; body weight;histological RCC subtype; Fuhrman grade; TNM stage; andVTT level (level 1: VTT involving the renal vein; level 2: VTTextending into the vena cava but below the intrahepatic venacava; level 3: VTT extending into the intrahepatic vena cavabut below the diaphragm; level 4: VTT extending above thediaphragm into the right atrium). Patients with clinicallyunsuspicious lymph nodes did not always undergolymphadenectomy; therefore, patients with pN0 (N = 118) and
Table 1 Patient characteristics and descriptive statistics.
All patients Friable VTT Solid VTT P
Total no. of patients 200 20 130pTstage, n (%) 0.024*
pT3a 137 (68.5) 41 (58.6) 96 (73.8)pT3b 51 (25.5) 23 (32.9) 28 (21.5)pT3c 3 (1.5) 3 (4.3) 0 (0)pT4 9 (4.5) 3 (4.3) 6 (4.6)
Fuhrman grade, n (%) 0.227*1 10 (5) 2 (2.9) 8 (6.2)2 132 (66) 43 (61.4) 89 (68.5)3 50 (25) 23 (32.9) 27 (20.8)4 8 (4) 2 (2.9) 6 (4.6)
VTT level, n (%) 0.013*1 145 (72.5) 43 (61.4) 102 (78.5)2 35 (17.5) 15 (21.4) 20 (15.4)3 17 (8.5) 9 (12.9) 8 (6.2)4 3 (1.5) 3 (4.3) 0 (0)
Histological subtype, n (%) 0.004*Clear-cell RCC 180 (90.0) 58 (82.9) 122 (93.8)Papillary RCC 12 (6.0) 10 (14.3 2 (1.5)Chromophobe RCC 3 (1.5) 1 (1.4) 2 (1.5)Sarcomatoid RCC 5 (2.5) 1 (1.4) 4 (3.1)
Sarcomatoid differentiation, n (%) 0.476*No 195 (97.5) 69 (98.6) 126 (96.9)Yes 5 (2.5) 1 (1.4) 4 (3.1)
Nodal status, n (%) 0.168*pN0/cN0 167 (83.5) 55 (78.6) 112 (86.2)pN+ 33 (16.5) 15 (21.4) 18 (13.8)
Distant metastases, n (%) 0.265*cM0 133 (66.5) 43 (61.4) 90 (69.2)cM+ 67 (33.5) 27 (38.6) 40 (30.8)
Surgical margins, n (%) 0.402*R0 174 (87) 59 (84.3) 115 (88.5)R1 26 (13) 11 (15.7) 15 (11.5)
Tumour necrosis, n (%) 0.064*No 112 (56) 33 (47.1) 79 (60.8)Yes 88 (44) 37 (52.9) 51 (39.2)
Perinephric fat invasion, n (%) 0.280*No 64 (32) 19 (27.1) 45 (34.6)Yes 136 (68) 51 (72.9) 85 (65.4)
Gender, n (%) 0.505*Female 71 (35.5) 27 (38.6) 44 (33.8)Male 129 (64.5) 43 (61.4) 86 (66.2)
Age 0.041†
Mean (median) 65.84 (67) 64.16 (64.5) 66.76 (67.0)Range 37–86 37–83 38–86
Body mass index 0.947†
Mean (median) 26.44 (25.93) 26.41 (25.1) 26.46 (26.3)Range 16.6–54.93 18.99–54.93 16.6–38.3
*Chi-squared test; †Student’s t-test.
Weiss et al.
© 2013 The Authors210 BJU International © 2013 BJU International

pNx (N = 49) were combined to form a pN0/pNx group forstatistical analysis. The study included 12 patients withpapillary RCC; of these, five patients had subtype 1 and sevenhad subtype 2. The TNM staging was re-classified according tothe 2009 Union Internationale Contre le Cancer/AmericanJoint Committee on Cancer TNM staging system based on thehistopathological report. Where TNM stage was not clear, thehistological slides were reassessed. None of the patientsunderwent neoadjuvant therapy before surgery.
The follow-up after surgery was performed at the discretion ofthe urologists and general practitioners. The treatment ofrecurrence differed among the patients (metastasectomy,medical therapy [immunotherapy or targeted therapy]palliative care), and was not considered in the analyses. Theoutcome (time to death and cause of death) was obtained by atelephone interview of the treating physicians or the patients’relatives. The survival time was calculated from the date ofsurgery to the last follow-up.
Assessment of VTT Consistency
The microscopy slides were reviewed retrospectively by twoinvestigators (V.W. and M.B.), and divergent results werere-evaluated; there was discorcordance in 10.5% of cases. Themorphological aspect of the VTT was classified as friable orsolid as described by Bertini et al. [3]: VTT was classified assolid if >90% of the VTT showed solid features (compact andcohesive, rounded linear profile, endothelial lining simulatinga pseudocapsule), and friable if it was incoherent, irregularand loose with fibrin film, had numerous necrosis zones and afragmented aspect (Fig. 1).
Immunohistochemistry
Sections mounted on superfrost slides were deparaffinized.Immunohistochemistry was conducted using an Autostainer480S automated staining system (Thermo Scientific, Waltham,MA, USA) with Medac reagents (Medac GmbH, Wedel,Germany). For E-cadherin immunohistochemistry,anti-E-cadherin mouse monoclonal antibody (1:100 dilution,clone SC-8426, Santa Cruz Biotechnology, CA, USA) wasused. Dilution was performed using a Medac diluent. Afterheat-induced epitope retrieval, the primary antibody wasincubated for 30 min at room temperature (20°C). Asecondary antibody was applied (Poly-HRP-anti-mouse,Medac) for 15 min at room temperature. Secondary antibodydetection was performed using DAB (8 min). Slides werecounterstained with haematoxylin and eosin for 3 min thenwith a bluing reagent (Medac). The samples were analysedunder a 10x dry objective, using a standard bright fieldmicroscope. The evaluation of the tests was carried out by anexperienced observer (M.B.). Membranous immunoreactivitywas scored as follows: 0, negative/very weak; 1, weak; 2,
moderate; and 3, strong. Renal tubules with high expression ofE-cadherin protein were used as an intrinsic positive controlfor the staining procedure.
Elastica-van-Gieson Staining
Sections mounted on superfrost slides were deparaffinized.Elastica-van-Gieson staining was performed using a TissueStainer automated staining system (Medite, Winter Garden,FL, USA) using Chroma reagents (Chroma Waldeck, Münster,Germany). After dehydration, slides were incubated withresorcin-fuchsin for 30 min, followed by washing steps andincubation with haematoxylin for 2 min and van-Giesonmixture for 2 min (all Chroma). Finally, slides weredehydrated rapidly, cleaned and mounted. Evaluation of thetests was carried out by an experienced observer (M.B.). AfterElastica-van-Gieson staining, nuclei stain brownish-black,fibrous connective tissue red and muscle, cytoplasm and fibrinyellow. The amount of fibrous connective tissue was scored asfollows: 0, negative/very low; 1, low; 2, medium; and 3, high.
Statistical Analysis
The impact of VTT consistency on the study variables wasanalysed using a chi-squared test And VTT consistencywas compared based on Elastica-van-Gieson stainingand E-cadherin immunohistochemistry using theMann–Whitney U-test. Survival curves were estimated usingthe Kaplan–Meier method and differences among survivalcurves were tested using the log-rank test. Univariate andmultivariate Cox regression analyses were used to correlateclinicopathological variables with overall survival. A P value<0.05 was considered to indicate statistical significance. Allstatistical analyses were performed using IBM SPSS Statisticsv20 (IBM, Chicago, IL, USA).
ResultsVTT Consistency and Clinicopathological Variables
The study cohort comprised 200 patients with RCC and VTT,of whom 130 (65%) had solid and 70 (35%) friable VTT.Patients with friable VTT had a significantly more advancedpT-stage (P = 0.024), a significantly higher VTT level (P =0.013), more often a papillary RCC subtype (P = 0.004) and alower age (P = 0.041). VTT consistency was not associatedwith Fuhrman grade, lymph node metastases, distantmetastases, tumour necrosis, perinephric fat invasion,surgical margins, tumour size, age, gender or BMI (all P >0.05; Table 1).
Consistency of VTT and Survival
Follow-up information was available for 184 patients with amedian follow-up of 49 months. Of these patients, 78 (42.4%)were still alive and 106 (57.6%) had died; 69 patients died
Tumour thrombus consistency in patients with RCC
© 2013 The AuthorsBJU International © 2013 BJU International 211

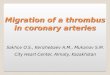
Fig. 1 Representative microscopic images of a solid (A–D) and a friable (E–H) example of VTT selected from 200 patients. Solid VTT is characterized by
a cohesive and compact profile, as well as an endothelial lining simulation a pseudocapsule. By contrast, friable VTT shows an irregular, fragmented
shape and has several necrotic areas. E-cadherin immunohistochemistry of the solid VTT shows strong membranous staining of tumour cells, implying a
high amount of cell-cell adhesions (C) in contrast to a low amount of cell-cell adhesions in the friable thrombus tumor cells (G). Elastica-van-Gieson
staining of the solid VTT gives a deep red impression, indicating plenty of connective tissue and intermingling bundles of collagen fibers (D). By
contrast, the friable VTT only yields a very low amount of connective tissue (H).
A E
B F
C G
D H
1000 µm 1000 µm
500 µm 500 µm
100 µm 100 µm
100 µm 100 µm
Weiss et al.
© 2013 The Authors212 BJU International © 2013 BJU International

from RCC, 30 died from other causes and in seven patientsthe cause of death was undetermined. The median overallsurvival in patients with friable VTT was significantly shorterthan in those with solid VTT (29 vs 89 months, log-rankP = 0.03; Fig. 2).
As expected, pT-stage, Fuhrman grading, histological subtype,lymph node metastases, distant metastases, tumour necrosis,perinephric fat invasion and surgical margins were predictiveof patient outcomes as determined using Kaplan–Meieranalyses (all P < 0.05; Table 2). We next applied uni- and
multivariate Cox regression analyses to assess the role of eachvariable on patients’ survival. pT-stage (P = 0.046), lymphnode metastases (P = 0.002), distant metastases (P < 0.001),tumour necrosis (P = 0.014) and age (P < 0.001) weresignificant predictors of overall survival; VTT consistency lostits predictive value in the multivariate analysis (P = 0.277;Table 3).
We next investigated the subgroup of patients without distantand nodal metastases (N = 119). The Kaplan–Meier analysisshowed that overall survival was shorter in patients withfriable VTT (40 vs 135 months; P = 0.016; Fig. 2).The Cox regression analysis showed that friable VTTconsistency was a significant predictor of poorer survival inthe univariate (P = 0.019) and multivariate (P = 0.009) model;tumour necrosis was also a significant predictor (P = 0.012;Table 4).
Consistency of VTT, Connective Tissue Content andCell Adhesion
The amount of connective tissue was determined usingElastica-van-Gieson staining and cell-adhesion molecules wereassessed using E-cadherin immunohistochemistry in each ofthe 10 friable and solid VTT cases. We observed a significantlygreater amount of connective tissue (mean score: 2.2. vs 0.6;P < 0.001) and E-cadherin (mean score: 1.6 vs 0.7; P = 0.043)in solid compared with friable VTT (Figs 1,3).
DiscussionRenal cell carcinoma with VTT remains a challenge inuro-oncology, with a 5-year cancer-specific survival of ∼50%[4,9–13]. Patients with metastases have an estimated 5-yearsurvival rate of <10% [4,12]. Complete surgical removal of theaffected kidney and the VTT is still regarded as the mosteffective and standard therapeutic approach in general [7,14].Nevertheless, despite the fact that a small portion of RCC withVTT can actually be cured with surgery, the majority ofpatients develop recurrence a short time after primary surgicaltherapy.
In today’s clinical routine, several factors (local extension,nodal involvement and metastases) are used to predict theprognosis of patients with RCC [5,9,12,15,16]. Several studieshave shown poor outcomes in patients with RCC and VTT[3,5,8,12,17,18]. Bertini et al. [3] recently reported that VTTconsistency might be an independent predictor of anunfavourable clinical course and, specifically, that patients withVTT showing friable features, such as an irregular shape, afragmented aspect, necrosis and fibrin exsudate, have worseoutcomes.
Drawing on these studies, we reviewed VTT consistency in aclinically well-defined cohort of 200 patients with locallyadvanced RCC and the presence of VTT. Furthermore, as
Fig. 2 Kaplan–Meier estimates for the effect of VTT consistency on overall
survival in the study cohort of 184 patients (A) and in 119 patients
without evidence of distant and nodal metastases (B). A friable VTT
consistency is a significant predictor of poor overall survival in patients
with RCC.
A
Ove
rall
Surv
ival
, %
100
90
80
70
60
50
40
30
20
10
00 1 2 3 4 5 6 7 8 9 10
Years11 12 13 14 15 16 17 18
0
B
Ove
rall
Surv
ival
, %
100
90
80
70
60
50
40
30
20
10
0 1 2 3 4 5 6 7 8 9 10Years
solid friable
11 12 13 14 15 16 17 18
Tumour thrombus consistency in patients with RCC
© 2013 The AuthorsBJU International © 2013 BJU International 213

recent reports have suggested the therapeutic benefit ofstratifying patients according to their individual risk fordisease progression and recurrence, we further subclassifiedour cohort into patients with and without distant and nodalmetastases. In concordance with Bertini et al. [3], we foundthat VTT consistency was an independently predictor ofoverall survival in patients without metastases. Furthermore,we showed that friable VTT was significantly associated with ahigher pathological stage and higher VTT level, suggesting abiological aggressiveness of tumours developing friable VTT.Interestingly, a friable VTT was most commonly associatedwith a papillary histological subtype.
In our analysis, we could further confirm the influence ofpreviously reported clinico-pathological variables on thepatients’ prognoses, such as pathological stage [19],perinephric fat invasion [3,8,15,18], tumour size [8,9,18],Fuhrman grade [6,8,12], tumour necrosis [5] and sarcomatoidfeatures [3,5,15]. Somewhat surprising was the finding thateven patients with low grade (grade 1) RCC developed VTT; itshould be noted, however, that Fuhrman classification of lowgrade tumours may be difficult, a fact that is supported by lowinterobserver agreement in the classification of grade 1 and2 tumours [20]. Interestingly, VTT level was not associatedwith patients’ outcome in our study. Notably, in our study
Table 2 Clinicopathological variables and overall survival.
n (%) 5-year OS % Median OS, months (IQR) P
VTT 0.03Friable 125 (67.9) 22.4 29 (8–59)Solid 59 (32.1) 32.2 89 (9.5–80.5)
pT-stage <0.001pT3a 127 (69) 30.9 57 (10–78)pT3b 46 (25) 28.8 49 (13–70.75)pT3c 3 (1.6) 50 n.r. (0.0–n.r.)pT4 8 (4.3) 0 4 (2.3–14.8)
Fuhrman grade 0.0311 10 (5.4) 66.6 98 (45.3–103.5)2 124 (67.4) 30.8 57 (16–73.8)3 43 (23.4) 21.42 36 (3–45)4 7 (3.8) 0 7 (2–14)
VTT level 0.7541 134 (72.8) 29.3 48 (9–71.5)2 32 (17.4) 32.2 73 (14–74.5)3 15 (8.2) 21.4 34 (10–34))4 3 (1.6) 50 11 (0.0–n.r.)
Histological subtype 0.003Clear-cell RCC 166 (90.2) 29.7 53 (10-71.3)Papillary RCC 10 (5.4) 33.3 40 (16.3–109.2)Chromophob RCC 3 (1.6) 50 73 (7–n.r.)Sarcomatoid RCC 5 (2.7) 0 4 (1–6.5)
Sarcomatoid differentiation <0.001No 179 (97.3) 29.7 53 (11–73)Yes 5 (2.7) 0 4 (1–6.5)
Nodal status <0.001pN0/cN0 153 (83.2) 34.2 85 (14–82.5)pN+ 31 (16.8) 3.3 15 (3–18)
Distant metastases <0.001cM0 125 (67.9) 37.9 111 (19.5-93.5)cM1 59 (32.1) 10.3 15 (3–29)
Surgical margins <0.001R0 159 (86.4) 32.2 59 (13–78)R1 25 (13.6) 8.3 8 (2–31)
Tumour necrosis <0.001No 107 (58.2) 35.8 99 (17–92)Yes 77 (41.8) 19.7 25 (4.5–47)
Perinephric fat invasion 0.002No 59 (32.1) 32.7 99 (25–89)Yes 125 (67.9) 27.4 34 (7.5–65)
Age 0.139Age < 60 years 43 (23.4) 30.9 101 (8–76)Age ≥ 60 years 141 (76.6) 28.5 42 (9.8–66.2)
Body mass index 0.193<25 kg/m2 72 (40.7) 22.5 29 (8–57.5)>25 kg/m2 72 (40.7) 29.5 59 (10.5–79.5)>30 kg/m2 32 (18.6) 34.3 78 (8–77)
OS, overall survival; IQR, interquartile range (25th–75th percentiles); n.r., not reached.
Weiss et al.
© 2013 The Authors214 BJU International © 2013 BJU International

population, the presence of nodal involvement and metastaticdisease had the most significant effect on overall survival[5,9,12,15,16]. Furthermore, Bertini et al. [21] showed thatthere was a higher risk of cancer-specific mortality for RCCpatients with VTT and perinephric fat invasion.
Kim et al. [22] reported that the presence of VTT wasassociated with a higher risk of recurrence after nephrectomy.In the present study, VTT consistency was not associatedwith metastatic disease and nodal involvement, although allvariables were independent predictors of patients’ overallsurvival. It was notable that the effect of friable VTT onoverall survival was most significant in patients withnon-metastatic RCC. This supports the hypothesis thatpatients with non-metastatic disease and friable VTT havehigher-risk disease than patients with non-metastatic diseaseand solid VTT. As with VTT consistency, our data show thatpatients with non-metastatic RCC and VTT can be dividedinto other distinct risk subgroups, e.g. those with tumournecrosis. We suggest that patients with RCC, VTT and
simultaneous risk factors (such as friable VTT or tumournecrosis), but without preoperative evidence of distant andnodal metastatic disease, will most likely follow anunfavourable clinical course.
There is a lack of evidence for adjuvant therapy for patientsat risk of disease recurrence after nephrectomy fornon-metastatic RCC. By contrast, for patients with metastaticRCC, targeted-therapies with vascular endothelial growthfactor pathway and mammalian target of rapamycin inhibitorshave substantially improved survival rates [23]. Tobert et al.[24] point out that there is universal support in theuro-oncological community for investigation of these agentsin patients with high- and intermediate-risk localized RCCafter nephrectomy. We suggest that patients with high-riskdisease may benefit from adjuvant therapy with targetedagents. Zhao et al. [25] have shown that such an approach maybe promising; they observed a longer disease-free survivalin high-risk patients with locally advanced RCC treatedadjuvantly with sorafenib or sunitinib. Nevertheless, level 1
Table 3 Univariate and multivariate Cox regression analyses predicting overall survival in the wholestudy cohort (N = 200).
Univariate analysis Multivariate analysis
P HR(95% CI)
P HR(95% CI)
VTTSolid vs friable 0.032 1.543 (1.037–2.296) 0.227 1.300 (0.850–1.988)
pT stage 0.002 1.525 (1.166–1.993) 0.046 1.317 (1.005–1.727)pT3b vs pT3a 0.436 1.191 (0.767–1.850)pT3c vs pT3a 0.774 0.865 (0.322–2.324)pT4 vs pT3a <0.001 1.822 (1.383–2.400)
Fuhrman grade 0.008 1.562 (1.123–2.172) 0.295 1.199 (0.854–1.683)3/4 vs 1/2 0.023 1.658 (1.072–2.564)3 vs 2 0.098 1.481 (0.930–2.358)4 vs 2 0.026 1.806 (1.074–3.036)
VTT level 0.389 1.127 (0.859–1.480)2 vs 1 0.977 1.007 (0.608–1.668)3 vs 1 0.522 1.120 (0.791–1.585)
Histological subtype 0.078 1.401 (0.962–2.039)Papillary vs clear-cell 0.519 0.758 (0.327–1.759)
Nodal statuspN+ vs pN0/cN0 <0.001 3.816 (2.350-6.195) 0.002 2.361 (1.381–4.036)
Distant metastasescM+ vs cM0/cMx <0.001 4.013 (2.676–6.019) <0.001 3.640 (2.330–5.688)
Surgical marginsR1 vs R0/Rx <0.001 2.627 (1.549–4.454) 0.956 0.982 (0.520–1.857)
Tumour necrosisTN vs no TN <0.001 2.183 (1.485–3.209) 0.014 1.662 (1.110–2.488)
Perinephretic fat invasionPFI vs no PNF 0.002 2.018 (1.293–3.151) 0.299 1.288 (0.799–2.077)
Sarcomatoid differentiationSD vs no SD 0.002 6.617 (1.991–21.998) 0.020 5.018 (1.294–19.456)
AgeContinous variable 0.011 1.029 (1.006–1.051) <0.001 1.050 (1.026–1.075)
Body mass indexContinous variable 0.165 0.967 (0.923–1.014)
Tumour sizeContinous variable <0.001 1.120 (1.056–1.188) 0.303 1.038 (0.967–1.114)
HR, hazard ratio; TN, tumour necrosis; PFI, perinephritic fat invasion; SD, sarcomatoid differentiation.
Tumour thrombus consistency in patients with RCC
© 2013 The AuthorsBJU International © 2013 BJU International 215

evidence for adjuvant therapy remains to be established, andthe results from several phase III trials testing tyrosine kinaseinhibitors in an adjuvant setting (i.e. the SORCE, sorafinib;ASSURE, sorafinib/sunitinib; S-TRAC, sunitinib; andPROTECT, pazopanib trials) will be available in a few years.
Other studies even suggest the integration of neoadjuvanttherapy as a viable option for some patients with RCC[12,26,27].
In terms of diagnosis, we found that VTT consistency canbe comfortably assessed using standard haematoxylin andeosin stained specimens. A consensus was reached by twoinvestigators in the small number of uncertain cases. Becauseof its informative impact on prognosis and ease ofevaluation, the introduction of VTT consistency assessmentinto routine diagnostic procedure would be both helpful andfeasible.
Similarly to the previous study by Bertini et al. [3], weanalysed the content of connective tissue (Elastica-van-Gieson) and cell-cell adhesions (E-cadherin) in patients withsolid and friable VTT. We showed that solid VTT has agreater amount of connective tissue and cell-cell adhesioncompared with friable VTT. These molecular differenceshighlight the fact that biological factors are responsible forthe VTT consistency, which may facilitate metastases andaccount for the poor prognosis of patients with friable VTT.Furthermore, these findings prove that consistency is not aconsequence of different specimen handling (e.g. ischaemia,pressure and processing).
The present study has some limitations. The retrospectiveapproach and the relatively short-term follow-up restricted,to some extent, the significance of our results. Also, ourconclusions could have been influenced by the involvement of
Table 4 Univariate and multivariate Cox analyses predicting overall survival in patients with N0/x M0disease (N = 119).
Univariate analysis Multivariate analysis
P HR(95.0% CI)
P HR(95.0% CI)
VTTSolid vs friable 0.019 2.027 (1.125–3.653) 0.009 2.227 (1.224–4.054)
pT stage 0.163 1.454 (0.859–2.461)pT3b vs pT3a 0.143 1.577 (0.857–2.902)pT3c vs pT3a 0.738 1.187 (0.436–3.229)pT4 vs pT3a n.r. n.r. (n.r.)
Fuhrman grade 0.389 1.275 (0.733–2.2193/4 vs 1/2 0.606 1.211 (0.585–2.506)3 vs 2 0.653 1.183 (0.569–2.458)4 vs 2 0.742 0.221 (0.000–1797?)
VTT level 0.107 1355 (0.936–1.960)2 vs 1 0.322 1.420 (0.710–2.839)3 vs 1 0.233 1.337 (0.830–2.153)
Histological subtypePapillary vs clear-cell 0.315 0.477 (0.113–2.013)
Surgical marginsR1 vs R0 0.973 0.976 (0.235–4.045)
Tumour necrosisTN vs no TN 0.024 1.946 (1.091–3.472) 0.012 2.136 (1.185–3.850
Perinephric fat invasionPFI vs no PFI 0.083 1.723 (0.931–3.189)
HR, hazard ratio; TN, tumour necrosis; PFI, perinephritic fat invasion; n.r., not reached.
Fig. 3 Comparison of VTT consistency and connective tissue
(Elastica-van-Gieson staining (EVG) and cell-cell adhesions (E-cadherin
[ECAD]) content in solid and friable VTT. Solid VTT is characterized by a
significant increase of cell-cell-adhesion molecules and connective
tissue. We analysed the VTT consistency (friable/solid) in each of 10
patients with RCC and VTT.
EVG ECAD VTTEVG ECAD
0 1 2 3
VTT
solid
fria
ble
Weiss et al.
© 2013 The Authors216 BJU International © 2013 BJU International

multiple surgeons and by the different therapies after diseaserecurrence. Important events (e.g. targeted therapy) of thetreatment of patients with RCC occurred during the studyperiod, and this may also have led to a bias when analysingsurvival data. Unlike Bertini et al. [3], we did notuse cancer-specific survival but overall survival as ourendpoint; cause of death was not definitively available in allpatients, and thus overall survival was a more robust measurethan cancer-specific survival. It should be noted that overallsurvival is the most preferred, precise and reliable cancerendpoint according to the US Food and Drug Administration,and should be used in preference to cancer-specific survival.
In conclusion, VTT consistency is an important prognosticpredictor of overall survival for patients with localized RCC.The inclusion of VTT consistency in current staging systemscould be useful for better prognostication.
Conflict of InterestNone declared.
References1 Siegel R, Naishadham D, Jemal A. Cancer statistics, 2012. CA Cancer J
Clin 2012; 62: 10–292 Kane CJ, Mallin K, Ritchey J, Cooperberg MR, Carroll PR. Renal cell
cancer stage migration: analysis of the National Cancer Data Base. Cancer2008; 113: 78–83
3 Bertini R, Roscigno M, Freschi M et al. Impact of venous tumourthrombus consistency (solid vs friable) on cancer-specific survival inpatients with renal cell carcinoma. Eur Urol 2011; 60: 358–65
4 Blute ML, Leibovich BC, Lohse CM, Cheville JC, Zincke H. The MayoClinic experience with surgical management, complications and outcomefor patients with renal cell carcinoma and venous tumour thrombus. BJUInt 2004; 94: 33–41
5 Coons BJ, Stec AA, Stratton KL et al. Prognostic factors in T3b renal cellcarcinoma. World J Urol 2009; 27: 75–9
6 Garcia-Fadrique G, Budia-Alba A, Ruiz-Cerda JL, Morales-Solchaga G,Pontones JL, Jimenez-Cruz JF. [Prognostic value of venous tumorthrombus in renal cell carcinoma]. Actas Urol Esp 2012; 36: 29–34
7 Kirkali Z, Van Poppel H. A critical analysis of surgery for kidney cancerwith vena cava invasion. Eur Urol 2007; 52: 658–62
8 Martinez-Salamanca JI, Huang WC, Millan I et al. Prognostic impact ofthe 2009 UICC/AJCC TNM staging system for renal cell carcinoma withvenous extension. Eur Urol 2011; 59: 120–7
9 Miyake H, Terakawa T, Furukawa J, Muramaki M, Fujisawa M.Prognostic significance of tumor extension into venous system inpatients undergoing surgical treatment for renal cell carcinoma withvenous tumor thrombus. Eur J Surg Oncol 2012; 38: 630–6
10 Al Otaibi M, Abou Youssif T, Alkhaldi A et al. Renal cell carcinoma withinferior vena caval extention: impact of tumour extent on surgicaloutcome. BJU Int 2009; 104: 1467–70
11 Zisman A, Wieder JA, Pantuck AJ et al. Renal cell carcinoma with tumorthrombus extension: biology, role of nephrectomy and response toimmunotherapy.J Urol 2003; 169: 909–16
12 Vergho DC, Loeser A, Kocot A, Spahn M, Riedmiller H. Tumorthrombus of inferior vena cava in patients with renal cell
carcinoma – clinical and oncological outcome of 50 patients after surgery.BMC Res Notes 2012; 5: 264
13 Libertino JA, Zinman L, Watkins E Jr. Long-term results of resection ofrenal cell cancer with extension into inferior vena cava. J Urol 1987; 137:21–4
14 Haferkamp A, Bastian PJ, Jakobi H et al. Renal cell carcinoma withtumor thrombus extension into the vena cava: prospective long-termfollowup. J Urol 2007; 177: 1703–8
15 Klatte T, Pantuck AJ, Riggs SB et al. Prognostic factors for renal cellcarcinoma with tumor thrombus extension. J Urol 2007; 178: 1189–95;discussion 95
16 Spiess PE, Kurian T, Lin HY et al. Preoperative metastatic status, level ofthrombus and body mass index predict overall survival in patientsundergoing nephrectomy and inferior vena cava thrombectomy. BJU Int2012; 110: E470–4
17 Parekh DJ, Cookson MS, Chapman W et al. Renal cell carcinoma withrenal vein and inferior vena caval involvement: clinicopathologicalfeatures, surgical techniques and outcomes. J Urol 2005; 173:1897–902
18 Wagner B, Patard JJ, Mejean A et al. Prognostic value of renal vein andinferior vena cava involvement in renal cell carcinoma. Eur Urol 2009; 55:452–9
19 Budia Alba A, Gomez Perez L, Bango V et al. [Prognostic factors fordisease progression in patients with renal cell carcinoma]. Actas Urol Esp2007; 31: 831–44
20 Lang H, Lindner V, de Fromont M et al. Multicenter determination ofoptimal interobserver agreement using the Fuhrman grading system forrenal cell carcinoma: assessment of 241 patients with >15-year follow-up.Cancer 2005; 103: 625–9
21 Bertini R, Roscigno M, Freschi M et al. The extent of tumour fatinvasion affects survival in patients with renal cell carcinoma and venoustumour thrombosis. BJU Int 2011; 108: 820–4
22 Kim HL, Zisman A, Han KR, Figlin RA, Belldegrun AS. Prognosticsignificance of venous thrombus in renal cell carcinoma. Are renal veinand inferior vena cava involvement different? J Urol 2004; 171: 588–91
23 Lee JL, Park I, Park K et al. Efficacy and safety of vascular endothelialgrowth factor receptor tyrosine kinase inhibitors in patients withmetastatic renal cell carcinoma and poor risk features. J Cancer Res ClinOncol 2012; 138: 687–93
24 Tobert CM, Uzzo RG, Wood CG, Lane BR. Adjuvant and neoadjuvanttherapy for renal cell carcinoma: a survey of the Society of UrologicOncology. Urol Oncol 2012; 31: 1316–20
25 Zhao J, Zhu Y, Zhang C et al. Sorafenib or sunitinib as postoperativeadjuvant therapy for Chinese patients with locally advanced clear cellrenal cell carcinoma at high risk for disease recurrence. Urol Oncol 2013;doi: 10.1016/j.urolonc.2012.04.019. [Epub ahead of print]
26 Margulis V, Master VA, Cost NG et al. International consultation onurologic diseases and the European Association of Urology internationalconsultation on locally advanced renal cell carcinoma. Eur Urol 2011; 60:673–83
27 Thomas AA, Rini BI, Stephenson AJ et al. Surgical resection of renal cellcarcinoma after targeted therapy. J Urol 2009; 182: 881–6
Correspondence: Jörg Ellinger; Klinik und Poliklinik fürUrologie und Kinderurologie, Universitätsklinikum Bonn,Sigmund-Freud-Strasse 25, 53105 Bonn, Germany.
e-mail: [email protected]
Abbreviations: VTT, venous tumor thrombus; RCC, renal cellcarcinoma.
Tumour thrombus consistency in patients with RCC
© 2013 The AuthorsBJU International © 2013 BJU International 217