Embed Size (px)
Citation preview
333
Prognostic Significance of Exercise BloodPressure and Heart Rate in Middle-aged Men
Jan Filipovsk^, Pierre Ducimetiere, and Michel E. Safar
Systolic blood pressure and heart rate measured at rest and during a standardized exercise test wereanalyzed in the cohort of middle-aged male employees followed-up an average of 17 years in the ParisProspective Study L The population sample selected for the analysis included 4,907 men who completedat least 5 minutes of bicycle ergometry, who had no heart disease at entry, and whose resting bloodpressure was s 180/105 nun Hg. Exercise-induced increase in systolic blood pressure was positivelycorrelated with resting systolic blood pressure (r=0.104, p<0.0001), whereas the correlation of exercise-induced heart rate increase with resting heart rate was negative (r=—0.169, p<0.0001). Using Coxregression analysis with the inclusion of resting systolic blood pressure and heart rate; exercise-inducedelevations of systolic blood pressure and heart rate; and controlling for age, smoking, total cholesterol,body mass index, electrical left ventricular hypertrophy, and sports activities, cardiovascular mortalitywas found to be associated with the systolic blood pressure increase (p<0.05), whereas no association withresting systolic blood pressure was found. Total mortality was predicted by resting systolic blood pressureand its elevation (p<0.01 for both) and by resting heart rate (p<0.0001). The heart rate increase did notcontribute to death prediction. In conclusion, the magnitude of the exercise-induced increase of systolicblood pressure, but not of heart rate, may represent a risk factor for death from cardiovascular as well asnoncardiovascular causes, independently of resting blood pressure and heart rate. (Hypertension1992^0-333-339)
KEY WORDS • blood pressure • heart rate • exercise test • prospective studies • mortality
A rterial blood pressure (BP) is a strong determi-/ \ nant of life prognosis, and cardiovascular
A. A . (CV) as well as total mortality are definitelyhigher in subjects who are classified as hypertensiveaccording to BP measurement at rest. Although rela-tively less attention has been drawn to heart rate (HR)level, it was also found to be associated with mortali-ty.1 There is a logical tendency to measure these twoparameters in basal conditions at rest to achievemaximal standardization; however, it does not implythat this way of assessing BP and pulse rate is the mostpredictive of individual risk. Exercise testing yieldsimportant 'information about circulatory status andperhaps about life prognosis since it may reflect, withother factors, physical fitness and presence or absenceof coronary atherosclerosis.
Exercise tests are widely used in patients in whomcoronary heart disease is suspected, and the strongpredictive value of pathological electrocardiographicchanges, mainly of the ST segment, has been confirmed
From INSERM U258 (P.D.) and U337 (M.E.S.), Paris, andthe Second Department of Medicine (J.F.), University Hospital,Pilzen, Czechoslovakia. J.F. is presently with INSERM U258.
Parts of this work were presented at the 11th Congress of theFrench Society of Arterial Hypertension, December 1991, Paris.
Supported by a research grant from the French Society ofArterial Hypertension.
Address for correspondence: Pierre Ducimetiere, PhD, IN-SERM U258, Epiddmiologie Cardiovasculaire, Hdpital Broussais,% rue Didot, 75674 Paris Cede* 14, France.
Received December 27, 1991; accepted in revised form May 5,1992.
several times.2-4 Several authors have studied BP andHR changes on physical load in various populations4-3;however, the prognostic value of these parameters in anintact population remains unestablished. Recently,Fagard et al6 published interesting results on the prog-nostic outcome of direct BP measurement at rest and atseveral workload levels in 143 hypertensive men. Theyfound no additive prognostic information of exercise BPcompared with resting BP in this relatively small groupof hypertensive subjects.
The present report represents, to our knowledge, thefirst study based on a long-term follow-up of a largecohort that evaluates the prognostic significance ofnoninvasive systolic BP (SBP) and HR measured duringbicycle ergometry. Since the majority of drugs thatdecrease resting BP seem less efficient in lowering BPlevels during exercise, the knowledge of mortality riskpredicted by exercise BP and HR might be valuable forfuture views on antihypertensive therapy. The mainquestion raised in the present study is whether theexercise-induced elevations of SBP and HR are riskfactors for CV and non-CV mortality in middle-agednormotensive and mild-to-moderate hypertensive menwho are free of coronary heart disease at entry. Since allconditions that are related to the development of ath-erosclerosis are likely to influence circulatory responseto exercise, we also studied the association of SBP andHR parameters with smoking, total cholesterol level,obesity expressed by the body mass index (BMI), historyof sports activities, and the presence of electrical leftventricular hypertrophy (LVH).
by guest on April 22, 2018
http://hyper.ahajournals.org/D
ownloaded from

334 Hypertension Vol 20, No 3 September 1992
MethodsStudy Population
The details about the Paris Prospective Study Iprotocol are published elsewhere.7 In brief, 7,746 na-tive-born Frenchmen aged 42-53 years and employedby the Paris Civil Service, were examined for the firsttime between 1967 and 1972 after giving their informedconsent to participate in this study. The screeningoccurred in the morning, and it consisted mainly of aclinical examination by a cardiologist, a questionnaireconcerning health history and smoking habits filled in bya technician, two BP measurements with a standard cufftechnique while the subject was in a sitting positionafter a 5-minute rest, and a fasting blood sampleobtained from the subject. Bicycle ergometry was per-formed in 6,565 subjects. Weight and height weremeasured with the subjects in their underclothes.
The population sample selected for this study in-cluded those subjects who completed at least 5 minutesof the standardized bicycle ergometry test and whoseresting BP (mean of two measurements) was ^180/105mm Hg; more severe hypertensive subjects were a prioriexcluded from the exercise test. We further excludedtreated hypertensive subjects (n = 114) and another 162subjects whose electrocardiographic (ECG) changesduring exercise were assessed as positive (horizontal ordescending ST segment depression s i mm). Alto-gether, 4,907 subjects were included in the presentanalysis.
Exercise ProtocolThe standardized protocol of bicycle ergometry has
been described previously.7 Subjects with any of thefollowing conditions were excluded from the test:cardiac insufficiency of any etiology, resting 12-leadstandard ECG signs of ischemic heart disease (Min-nesota Code was used8: definite Q waves, atrioventric-ular blocks and conduction defects, ST segment ab-normalities, atrial fibrillation or flutter, ventricularectopic beats with polymorphism), resting SBP >180mm Hg, angina pectoris determined as definite accord-ing to the World Health Organization questionnaire,valvular heart disease, evidence of heart enlargementon x-ray film, and any history of cerebrovascularinsufficiency. The test consisted of three successivework loads: 2 minutes at 82 W, 164 W from the thirdto the eighth minute, and finally 191 W up to amaximal 10-minute test duration. The criteria forinterruption of the exercise were any chest pain, ECGpathological changes (ST segment abnormalities, i.e.,horizontal or descending depression ^ 1 mm, atrioven-tricular blocks and conduction defects, ventricularpremature beats), HR >180 beats per minute, SBP^250 mm Hg. SBP was measured immediately beforethe test while the subject was sitting on the ergometer,at the fifth minute of exercise (SBP-5), and immedi-ately at the end of the exercise test while the subjectwas still sitting on the ergometer. HR was assessedfrom the electrocardiogram, which was recorded at2-minute intervals from leads V5 through V5R.
Follow-upDuring the follow-up period, the administrative de-
partment in charge of the population provided annually
a list of the deceased subjects. All available data rele-vant to the causes of death were collected from specificinquiries, i.e., medical records from hospital depart-ments or general practitioners indicated by the relativesof the deceased. The data were then reviewed by anindependent medical committee. The eighth revision ofthe International Classification of Diseases9 was usedfor coding. CV deaths include codes No. 390-438, 782,and 795. The deadline of the follow-up period wasDecember 31, 1987. The basic information of whetherthe subject had died or was still alive was obtained forall the members of the cohort. Five hundred andseventy-eight deaths occurred in the population sampleof the present study of which 146 were of CV and 337 ofnon-CV origin; in 95 deaths the cause could not bedetermined mainly because the family could not bereached at the time of the death report.
Definition of Parameters and Statistical AnalysisIn this report, the mean of the two SBP values
measured during the screening examination indepen-dently of the exercise test is called baseline SBP.Baseline HR is the mean of two measurements, oneassessed clinically after one BP measurement and theother from the standard electrocardiogram. InitialSBP and HR are those measured immediately beforethe test while the subject was sitting on the ergometer.SBP during exercise is that measured at the fifthminute of the test (SBP-5), and HR during exercise isthe pulse frequency at the fourth minute of the test(HR-4). The ASBP (AHR) differences are those be-tween SBP-5 (HR-4) and the initial parameters. Dia-stolic BP during exercise was not evaluated since itsrecording is known to be less reliable. BMI is definedaccording to the usual formula weight (kg)/height(m)2. Smoking is defined as the average daily cigaretteconsumption during the 5 years preceding the screen-ing. Electrical LVH was assessed according to stan-dard techniques10 involving the indexes of Sokolowand Lewis. To assess habitual physical activity, onlydata about sports activities were available. Men whoreported participating in sports regularly for 50 hoursor more per year at the time of screening wereconsidered active.
Statistical analysis was performed using StatisticalAnalysis System procedures.11 Age-adjusted partial cor-relation coefficients were calculated among SBP andHR measurements. To assess relations with covariates,multiple linear regressions were performed (GLM pro-cedure). The Cox proportional hazards model was usedto analyze mortality (PHREG procedure). In all mod-els, age was systematically introduced as an indepen-dent continuous variable. Age-adjusted relative risksamong various groups are reported.
ResultsBasic characteristics of the population sample, in-
cluding age, BP and HR parameters, total cholesterollevel, smoking, and BMI, are presented in Table 1.
Cross Correlations of Systolic BloodPressure and Heart Rate
In Table 2, the age-adjusted partial linear correlationcoefficients between all the considered SBP and HRvalues are indicated. There is a high correlation be-
by guest on April 22, 2018
http://hyper.ahajournals.org/D
ownloaded from
Filipovsky et al Exercise Blood Pressure and Heart Rate 335
TABLE 1. Characteristics of 4,907 Men, Foilowed-np in theParis Prospective Study L, Who Completed at Least 5 Minutesof a Standardized Exercise Test
Parameter
Age (years)SBP (mm Hg)
Baseline SBPBaseline DBPInitial SBPSBP-5 minutesASBP
HR (min"1)Baseline HRInitial HRHR-4 minutesAHR
Total cholesterol (mg/dl)Smoking (No. per day)BMI (kg/m2)
47.5 ±1.9
133.8±14.577.5 ±10.3
135.1 ±16.4195.9±31.760.8±25.5
66.6 ±8.675.6±13.0
1493±15.173.7±16.0
221.4±41.210.0±10.126.0±3.0
SBP, systolic blood pressure; Baseline SBP, DBP, and HR,means of two casual measurements; Initial SBP and HR, measure-ments taken immediately before the test while the subject wassitting on the ergometer; SBP-5 minutes and HR-4 minutes,measurements taken during the test; ASBP and AHR, differencebetween measurements taken during the test and the initialmeasurements; DBP, diastolic blood pressure; HR, heart rate;smoking, average daily cigarette consumption in the 5 yearspreceding the screening; BMI, body mass index. Values aremean±SD.
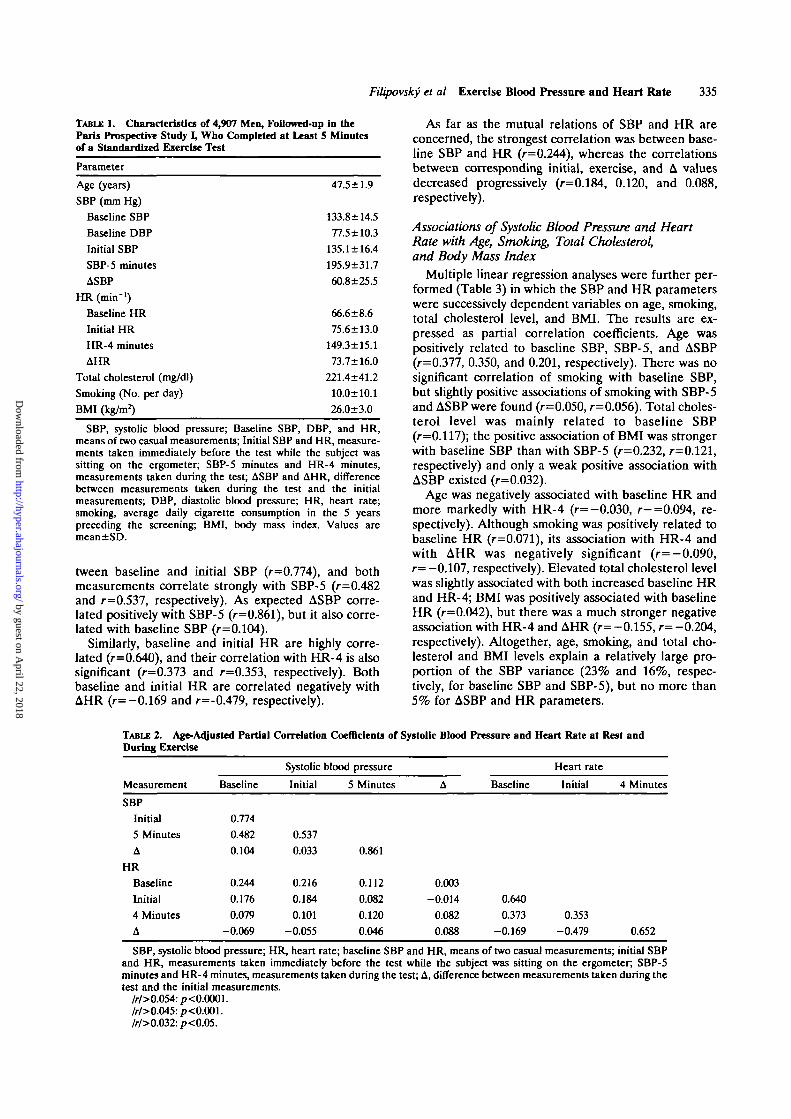
tween baseline and initial SBP (r=0.774), and bothmeasurements correlate strongly with SBP-5 (r=0.482and r=0.537, respectively). As expected ASBP corre-lated positively with SBP-5 (r=0.861), but it also corre-lated with baseline SBP (r=0.104).
Similarly, baseline and initial HR are highly corre-lated (r=0.640), and their correlation with HR-4 is alsosignificant (r=0.373 and r=0.353, respectively). Bothbaseline and initial HR are correlated negatively withAHR (r= -0.169 and r=-0.479, respectively).
As far as the mutual relations of SBP and HR areconcerned, the strongest correlation was between base-line SBP and HR (/-=0.244), whereas the correlationsbetween corresponding initial, exercise, and A valuesdecreased progressively (r=0.184, 0.120, and 0.088,respectively).
Associations of Systolic Blood Pressure and HeartRate with Age, Smoking, Total Cholesterol,and Body Mass Index
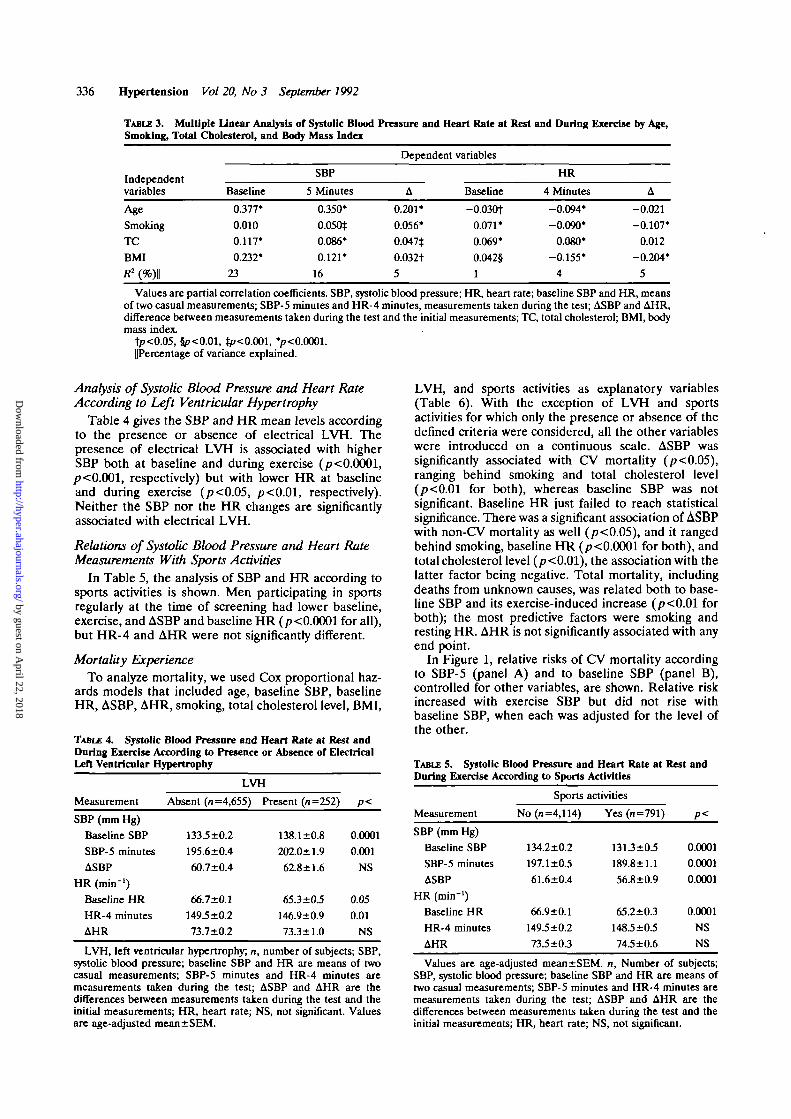
Multiple linear regression analyses were further per-formed (Table 3) in which the SBP and HR parameterswere successively dependent variables on age, smoking,total cholesterol level, and BMI. The results are ex-pressed as partial correlation coefficients. Age waspositively related to baseline SBP, SBP-5, and ASBP(r=0.377, 0.350, and 0.201, respectively). There was nosignificant correlation of smoking with baseline SBP,but slightly positive associations of smoking with SBP-5and ASBP were found (r=0.050, r=0.056). Total choles-terol level was mainly related to baseline SBP(r=0.117); the positive association of BMI was strongerwith baseline SBP than with SBP-5 (r=0.232, r=0.121,respectively) and only a weak positive association withASBP existed (r=0.032).
Age was negatively associated with baseline HR andmore markedly with HR-4 (r=-0.030, r-=0.094, re-spectively). Although smoking was positively related tobaseline HR (r=0.071), its association with HR-4 andwith AHR was negatively significant (r=—0.090,r= —0.107, respectively). Elevated total cholesterol levelwas slightly associated with both increased baseline HRand HR-4; BMI was positively associated with baselineHR (r=0.042), but there was a much stronger negativeassociation with HR-4 and AHR (r= -0.155, r= -0.204,respectively). Altogether, age, smoking, and total cho-lesterol and BMI levels explain a relatively large pro-portion of the SBP variance (23% and 16%, respec-tively, for baseline SBP and SBP-5), but no more than5% for ASBP and HR parameters.
TABLE 2. Age-Adjusted Partial Correlation Coefficients of Systolic Blood Pressure and Heart Rate at Rest andDuring Exercise
Measurement
SBP
Initial5 MinutesA
HR
BaselineInitial4 MinutesA
Baseline
0.7740.4820.104
0.2440.1760.079
-0.069
Systolic
Initial
0.5370.033
0.2160.1840.101
-0.055
blood pressure
5 Minutes
0.861
0.1120.0820.1200.046
A
0.003-0.014
0.0820.088
Baseline
0.6400.373
-0.169
Heart rate
Initial 4 Minutes
0.353-0.479 0.652
SBP, systolic blood pressure; HR, heart rate; baseline SBP and HR, means of two casual measurements; initial SBPand HR, measurements taken immediately before the test while the subject was sitting on the ergometer; SBP-5minutes and HR-4 minutes, measurements taken during the test; A, difference between measurements taken during thetest and the initial measurements.
/r/>0.054:p<0.0001./r/>0.045:p<0.001./r/>0.032:p<0.05.
by guest on April 22, 2018
http://hyper.ahajournals.org/D
ownloaded from
336 Hypertension Vol 20, No 3 September 1992
TABLE 3. Multiple Linear Analysis of Systolic Blood Pressure and Heart Rate at Rest and Daring Exercise by Age,Smoking, Total Cholesterol, and Body Mass Index
Independentvariables
Age
Smoking
TC
BMI
R1 (%)||
Baseline
0.377'
0.010
0.117*
0.232*
23
SBP
5 Minutes
0.350*
0.050*
0.086*
0.121*
16
Dependent
A
0.201*
0.056*
0.047$
0.032t5
variables
Baseline
-0.030t0.071*
0.069*
0.042§
1
HR
4 Minutes
-0.094*
-0.090*
0.080*
-0.155*
4
A
-0.021
-0.107*
0.012
-0.204*
5
Values are partial correlation coefficients. SBP, systolic blood pressure; HR, heart rate; baseline SBP and HR, meansof two casual measurements; SBP-5 minutes and HR-4 minutes, measurements taken during the test; ASBP and AHR,difference between measurements taken during the test and the initial measurements; TC, total cholesterol; BMI, bodymass index.
tp<o.O5,5p<o.oi, ip<o.ooi, v<o.oooi.UPercentage of variance explained.
Analysis of Systolic Blood Pressure and Heart RateAccording to Left Ventricular Hypertrophy
Table 4 gives the SBP and HR mean levels accordingto the presence or absence of electrical LVH. Thepresence of electrical LVH is associated with higherSBP both at baseline and during exercise (/><0.0001,p<0.001, respectively) but with lower HR at baselineand during exercise (/?<0.05, /><0.01, respectively).Neither the SBP nor the HR changes are significantfyassociated with electrical LVH.
Relations of Systolic Blood Pressure and Heart RateMeasurements With Sports Activities
In Table 5, the analysis of SBP and HR according tosports activities is shown. Men participating in sportsregularly at the time of screening had lower baseline,exercise, and ASBP and baseline HR (/XO.0001 for all),but HR-4 and AHR were not significantly different.
Mortality ExperienceTo analyze mortality, we used Cox proportional haz-
ards models that included age, baseline SBP, baselineHR, ASBP, AHR, smoking, total cholesterol level, BMI,
TABLE 4. Systolic Blood Pressure and Heart Rate at Rest andDuring Exercise According to Presence or Absence of ElectricalLeft Ventricular Hypertrophy
LVH, and sports activities as explanatory variables(Table 6). With the exception of LVH and sportsactivities for which only the presence or absence of thedefined criteria were considered, all the other variableswere introduced on a continuous scale. ASBP wassignificantly associated with CV mortality (/?<0.05),ranging behind smoking and total cholesterol level(/7<0.01 for both), whereas baseline SBP was notsignificant. Baseline HR just failed to reach statisticalsignificance. There was a significant association of ASBPwith non-CV mortality as well (p<0.05), and it rangedbehind smoking, baseline HR (p< 0.0001 for both), andtotal cholesterol level (p<0.01), the association with thelatter factor being negative. Total mortality, includingdeaths from unknown causes, was related both to base-line SBP and its exercise-induced increase (p<0.01 forboth); the most predictive factors were smoking andresting HR. AHR is not significantly associated with anyend point.
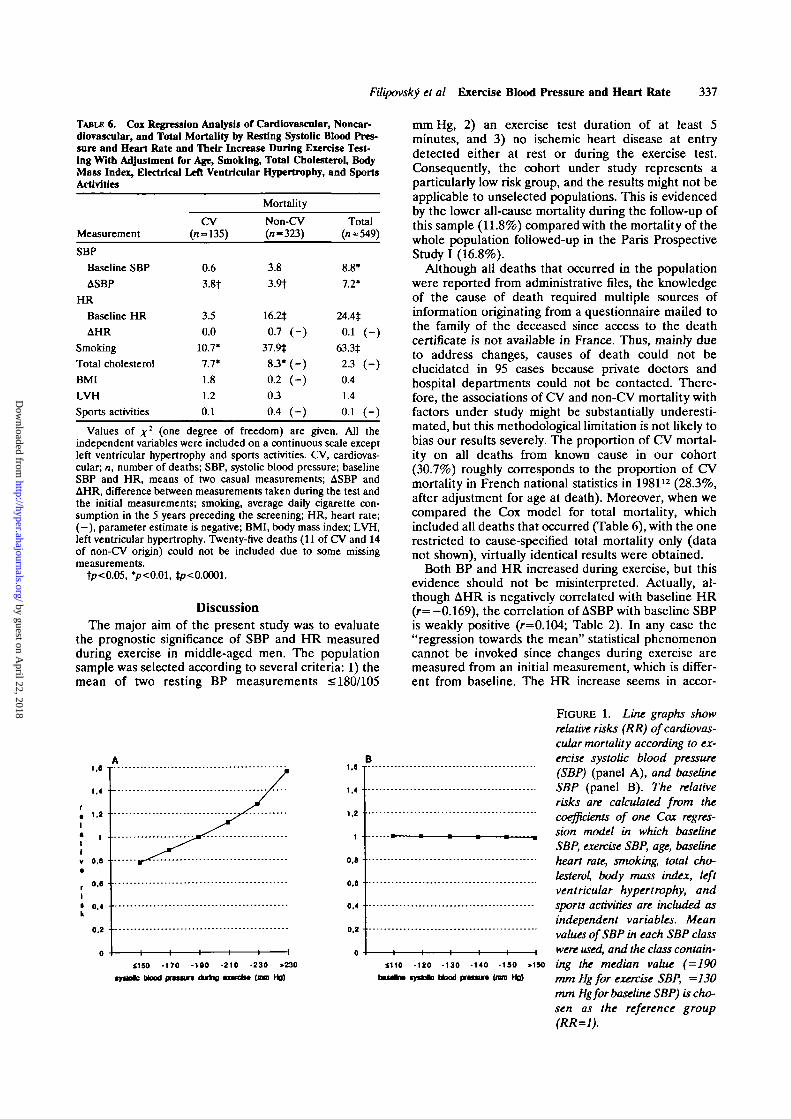
In Figure 1, relative risks of CV mortality accordingto SBP-5 (panel A) and to baseline SBP (panel B),controlled for other variables, are shown. Relative riskincreased with exercise SBP but did not rise withbaseline SBP, when each was adjusted for the level ofthe other.
Measurement
SBP (mm Hg)
Baseline SBP
SBP-5 minutes
ASBP
HR (min"1)
Baseline HR
HR-4 minutes
AHR
LVH
Absent (n=4,655)
133.5 ±0.2
195.6±0.4
60.7±0.4
66.7±0.1
149 5 ±0.2
73.7±0.2
LVH. left ventricular hypertrophy; n
Present (n=252)
138.1 ±0.8
202.0±1.9
6X8 ±1.6
65.3±03
146.9±0.9
73.3 ±1.0
!. number of subiec
P<
0.0001
0.001
NS
0.05
0.01
NS
ts; SBP.
During Exercise According to Sports
Measurement
SBP (mm Hg)
Baseline SBP
SBP-5 minutes
ASBP
HR (min"1)
Baseline HR
HR-4 minutes
AHR
Sports
No (n=4,114)
134.2±0.2
197.1 ±0.5
61.6±0.4
66.9±0.1
149.5 ±0.2
73-5±03
Activities
activities
Yes (n=791)
1313±0.5
189.8±1.1
56.8±0.9
65.2±0.3
148.5 ±0.5
74.5 ±0.6
P<
0.0001
0.0001
0.0001
0.0001
NS
NS
systolic blood pressure; baseline SBP and HR are means of twocasual measurements; SBP-5 minutes and HR-4 minutes aremeasurements taken during the test; ASBP and AHR are thedifferences between measurements taken during the test and theinitial measurements; HR, heart rate; NS, not significant. Valuesare age-adjusted mean±SEM.
Values are age-adjusted mean±SEM. n, Number of subjects;SBP, systolic blood pressure; baseline SBP and HR are means oftwo casual measurements; SBP-5 minutes and HR-4 minutes aremeasurements taken during the test; ASBP and AHR are thedifferences between measurements taken during the test and theinitial measurements; HR, heart rate; NS, not significant.
by guest on April 22, 2018
http://hyper.ahajournals.org/D
ownloaded from
Filipovsky et al Exercise Blood Pressure and Heart Rate 337
TABLE 6. Cox Regression Analysis of Cardiovascular, Noncar-diovascnlar, and Total Mortality by Resting Systolic Blood Pres-sure and Heart Rate and Their Increase During Exercise Test-ing With Adjustment for Age, Smoking, Total Cholesterol, BodyMass Index, Electrical Left Ventricular Hypertrophy, and SportsActivities
Measurement
SBP
Baseline SBP
ASBP
HR
Baseline HR
AHR
Smoking
Total cholesterol
BMI
LVH
Sports activities
CV(II = 135)
0.6
3.8t
3.5
0.0
10.7*
7.7*
1.8
1.2
0.1
Mortality
Non-CV(n-323)
3.8
3.9t
16.2*0.7 ( - )
37.9*S3'(-)0.2 ( - )0 3
0.4 (-)
Total(n»549)
8.8'7.2*
24.4*
0.1 (-)633*23 (-)0.4
1.4
0.1 (-)
Values of x2 ( o n e degree of freedom) are given. All theindependent variables were included on a continuous scale exceptleft ventricular hypertrophy and sports activities. CV, cardiovas-cular, n, number of deaths; SBP, systolic blood pressure; baselineSBP and HR, means of two casual measurements; ASBP andAHR, difference between measurements taken during the test andthe initial measurements; smoking, average daily cigarette con-sumption in the 5 years preceding the screening; HR, heart rate;( - ) , parameter estimate is negative; BMI, body mass index; LVH,left ventricular hypertrophy. Twenty-five deaths (11 of CV and 14of non-CV origin) could not be included due to some missingmeasurements.
tp<0.05, */?<0.01, *p<0.0001.
DiscussionThe major aim of the present study was to evaluate
the prognostic significance of SBP and HR measuredduring exercise in middle-aged men. The populationsample was selected according to several criteria: 1) themean of two resting BP measurements s 180/105
mm Hg, 2) an exercise test duration of at least 5minutes, and 3) no ischemic heart disease at entrydetected either at rest or during the exercise test.Consequently, the cohort under study represents aparticularly low risk group, and the results might not beapplicable to unselected populations. This is evidencedby the lower all-cause mortality during the follow-up ofthis sample (11.8%) compared with the mortality of thewhole population followed-up in the Paris ProspectiveStudy I (16.8%).
Although all deaths that occurred in the populationwere reported from administrative files, the knowledgeof the cause of death required multiple sources ofinformation originating from a questionnaire mailed tothe family of the deceased since access to the deathcertificate is not available in France. Thus, mainly dueto address changes, causes of death could not beelucidated in 95 cases because private doctors andhospital departments could not be contacted. There-fore, the associations of CV and non-CV mortality withfactors under study might be substantially underesti-mated, but this methodological limitation is not likely tobias our results severely. The proportion of CV mortal-ity on all deaths from known cause in our cohort(30.7%) roughly corresponds to the proportion of CVmortality in French national statistics in 198112 (28.3%,after adjustment for age at death). Moreover, when wecompared the Cox model for total mortality, whichincluded all deaths that occurred (Table 6), with the onerestricted to cause-specified total mortality only (datanot shown), virtually identical results were obtained.
Both BP and HR increased during exercise, but thisevidence should not be misinterpreted. Actually, al-though AHR is negatively correlated with baseline HR(r=-0.169), the correlation of ASBP with baseline SBPis weakly positive (r=0.104; Table 2). In any case the"regression towards the mean" statistical phenomenoncannot be invoked since changes during exercise aremeasured from an initial measurement, which is differ-ent from baseline. The HR increase seems in accor-
1.8 1
1.4
1 . 2 •
tIv o.a
0,6
• 0.4k
0.2
1.4
1.2
1
0.8
o.a
0,4
0.2
0ilSO -170 -190 -210 -230 >230
Mood n « m n during t w c l M (ma Hg)
1110 -120 -130 -140 -ISO >1S0bauln* tyifctc blood p r o w (mm Hg)
FIGURE 1. Line graphs showrelative risks (RR) of cardiovas-cular mortality according to ex-ercise systolic blood pressure(SBP) (panel A), and baselineSBP (panel B). The relativerisks are calculated from thecoefficients of one Cox regres-sion model in which baselineSBP, exercise SBP, age, baselineheart rate, smoking, total cho-lesterol, body mass index, leftventricular hypertrophy, andsports activities are included asindependent variables. Meanvalues of SBP in each SBP classwere used, and the class contain-ing the median value (=190mm Hgfor exercise SBP, =130mm Hgfor baseline SBP) is cho-sen as the reference group(RR=1).
by guest on April 22, 2018
http://hyper.ahajournals.org/D
ownloaded from

338 Hypertension Vol 20, No 3 September 1992
dance with the "law of initial value,"13 which stipulatesthat the higher the initial level of the parameter understudy, the smaller the reaction on stimulus. This doesnot apply to BP change since subjects with elevatedresting SBP have on the average higher ASBP. In somehemodynamic studies,14"16 it has been demonstratedthat subjects with elevated baseline vascular resistancepresent a further exaggerated increase on various sym-pathetic stimuli. This fact is usually related to structuralchanges of the vascular bed of subjects with chronic BPelevation, i.e., hypertrophy of the vessel wall, and inthese subjects, physical exercise would trigger an exces-sive rise in peripheral vascular resistance. Thus, wehypothesize that the different prognostic significance ofASBP and AHR observed in our study is related to thedifferent characters of BP and HR elevation thatroughly reflect mechanical and neurohumoral responsesto exercise.
The positive independent partial correlations of SBPwith age, BMI, and total cholesterol (Table 3) areconsistent with other studies,17 but there is no relationof resting SBP with smoking; however, a slightly nega-tive correlation is usually found within populations.1819
This might be partly due to the adjustment with theother factors, especially BMI, in the present study, butalso to the particular smoking rating used here thatintegrates tobacco consumption during the preceding 5years. The SBP rise during exercise is, as expected,significantly higher in smokers, and a lesser complianceof large arteries in smokers20 might account for thesteeper BP elevation during exercise.
Total, CV, and non-CV mortality experiences in thecohort were shown to be related to the SBP increaseduring exercise independently of the baseline SBP level.CV deaths, however, seem to be more strongly relatedto ASBP than to baseline SBP, which was no longerstatistically significant in this analysis. This result is atvariance with the conclusion of Fagard et al,6 whoevaluated the prognostic significance of exercise BP inhypertensive men. Brachial artery BP levels measuredat 50 W, peak work load, and 50% peak work werepredictive of both total mortality and CV event rates(fatal and nonfatal) but did not add any prognosticprecision to resting BP when age was taken into ac-count. Obviously no definite explanation may be givenfor such a discrepancy that concerns completely differ-ent populations and methods; different exercise proto-cols, in particular, might be important. In the work ofFagard et al,6 the initial work load of 20 W wasaugmented successively by 30 W every 4 minutes. Thisrelatively slow rise is usual in the majority of clinicalstudies and is likely to simulate changes of the physicalcharge in every day life. Conversely, in the protocolused in the Paris Prospective Study, the work loadimposed on the subjects increased very sharply: after 2minutes at 80 W, the work load was increased to 164 Wwithout interruption. The heart load is thus far greater,and it is possible that SBP increase in these conditionsreflects not only structural changes of peripheral vesselsbut the status of the whole CV system in subjects withelevated resting BP. Therefore, this type of exercisemight improve the prognostic power of exercise-inducedBP in comparison with more physiological protocols.
An exaggerated SBP increase during such a demand-ing exercise test might also be partly the consequence of
poor physical fitness, which has been shown to be anindependent risk factor of mortality when measured bythe duration of a maximal treadmill test.21-23 In ourcurrent study, a positive history of sports activities at thetime of screening was associated with lower baselineSBP and HR, SBP-5, and ASBP. These relations mightexplain the beneficial effects of physical fitness on lifeprognosis. However, for a more precise evaluation ofhabitual physical activity, more detailed data would beneeded.
Men with electrical LVH had a higher resting BP butnot a higher ASBP at exercise, and they were not athigher risk of death after adjusting for the other factors.The last finding differs from the well-known observa-tions of the Framingham study.24 The particular popu-lation selection for our analysis, namely, excluding thesevere hypertensive subjects and subjects with overtcoronary heart disease or heart enlargement as shownon x-ray film, is very likely to account for this lack ofassociation.
As found in some other cohort studies in both menand women,1'25-26 resting HR is a potent independentrisk factor for mortality, especially of non-CV origin.Explanations for these associations have not been es-tablished yet. Elevated resting HR might merely indi-cate a low level of physical activity and fitness,25 thatmay predispose an individual to CV and possibly toother chronic diseases. In two of three Chicago cohortstudies, resting heart rate was significantly associatedwith sudden death1 and with non-CV mortality. Con-cerning CV risk, several specific mechanisms have beenproposed: according to animal studies,27 high HR en-hances myocardial oxygen consumption and thereforemight be implied in the development of coronary ath-erosclerosis. Increased HR may be the result of en-hanced neural activity that predisposes an individual toa lowered threshold for ventricular fibrillation.28 On theother hand, subjects with elevated HR seem to be proneto death from cancer.26 The similarity of the HR riskfactor patterns for both CV and non-CV mortality inthe present study might indicate that more generalmechanisms are involved.
In conclusion, the present cohort study showed thatan exaggerated systolic pressure but not HR response toexercise contributes independently to the mortality risk.Further studies are needed to validate these data and toestablish to what extent the predictive power of exerciseBP is dependent on the type of exercise protocol.
AcknowledgmentsThe Paris Prospective Study I was organized by the "Groupe
d'Etude sur l'Epiddmiologie de l'Atheroscleiose," which asso-ciates INSERM and the "Direction de l'Action Sociale, del'Enfance et de la Sante," Paris.
References1. Dyer AR, Pcrsky V, StamJer J, Paul O, Shekelle RB, Berkson DM,
Lepper M, Schoenberger JA, lindbcrg HA: Heart rate as a prog-nostic factor for coronary heart disease and mortality: Findings inthree Chicago epidcmiologic studies. Am J Epidemiol 1980;112:736-749
2. Gordon DJ, Ekelund LG, Karon JM, Probstfield JL, Rubenstein C,Sheffield T, Weissfeld L: Predictive value of the exercise tolerancetest for mortality in North American men: The Lipid ResearchClinics Mortality Follow-up Study. Circulation 1986;74:252-261
3. Elgrishi I, Durimetiere P, Richard JL, Bonnaud G: Valeur prono-sique des modifications isch£miques de l'eiectrocardiogranune
by guest on April 22, 2018
http://hyper.ahajournals.org/D
ownloaded from

Filipovsky et al Exercise Blood Pressure and Heart Rate 339
pendant et apres l'effort dans une population masculine active.Arch Mai Coeur 1976;69:1241-1247
4. Astrand I: Blood pressure during physical work in a group of 221women and men 48-63 years old. Ada Med Scand 1965;178:41-45
5. Mallion JM, Debru JL, Doyon B, Morin B, Perdrix A, Cau G:Devenir dans le temps du profil tensionnel d'effort des sujcts quipresenters une hypertension art6rielle labile. Arch Mai Coair 1979;139-45
6. Fagard R, Staessen J, Thijs L, Amery A; Prognostic significance ofexercise versus resting blood pressure in hypertensive men. Hyper-tension 1991;17:574-578
7. Ducimetiere P, Richard JL, Claude JR, Wamet JM: Les Cardio-pathia Ischimiquei: Incidence et Facteurs de Risque. L 'Etude Pro-spective Parisienne. Paris, Editions 1NSERM, 1981, vol 1, pp 9-20
8. Rose GA, Blackburn H: Cardiovascular Survey Methods. Geneva,Switzerland, World Health Organization, 1968, p 140
9. International Classification of Diseases: 1965 Revision. Geneva,Switzerland, World Health Organization, 1968, vol 1, pp 3-41
10. Blackburn H, Keys A, Simonson E, Rautaharju P, Punsar S: Theelectrocardiogram in population studies: A classification system.Circulation 1960;21:1160-1175
11. SAS Procedures Guide, Version 6,ed4. Cary, NC, SAS Institute Inc,1990, vol 2, pp 891-996
12. Causes midicales de dices - annie 1981: Resultats dtfinitifs - France.Le Vesinet, France, Editions INSERM, 1981, pp 3-6
13. Wilder J: Stimulus and Response: The Law of Initial Value. Bristol,England, John Wright & Sons, 1967, pp 10-84
14. Folkow B: Importance of adaptive changes in vascular design forestablishment of primary hypertension: Studies in man and inspontaneously hypertensive rats. Cue Res 1973J2(suppl I):I-2—1-5
15. London GM, Weiss YA, Pannier BP, Laurent SL, Safar ME: Tilttest in essential hypertension: Differential responses in heart rateand vascular resistance. Hypertension 1987;10:29-34
16. Myers HA, Honig CL; Influence of initial resistance on magnitudeof response to vasomotor stimuli.yOn/ifyjio/1969;216:1429-1436
17. Gordon DJ, Leon AS, Ekelund LG, Sopko G, Probstfield JL,Rubenstein C, Sheffield LT: Smoking, physical activity, and otherpredictors of endurance and heart rate response to exercise in
asymptomatic hypercholesterolemic men. Am J Epidemiol 1987;125:587-600
18. Goldbourt U, Medalie JH: Characteristics of smokers, non-smokers and ex-smokers among 10000 adult males in Israel: II.Physiologic, biochemical and genetic characteristics. Am J Epide-miol 1977;105:75-86
19. Erikssen J, Enger SC: The effect of smoking on selected coronaryheart disease risk factors in middle-aged men. Acta Med Scand1978;203:27-30
20. Girerd X, Brunei P, Laurent S, Pannier B, Isnard R, Safar M:Effets des bfita-bloqueurs sur liiSmodynamique de Pavant-brasapres stimulation tabagjque. Arch Mai Coeur 1988;81(suppl HTA):133-136
21. Ekelund LG, Haskell W, Johnson JL, Whaley FS, Criqui MH,Sheps DS: Physical fitness as a predictor of cardiovascular mortal-ity in asymptomatic North American men. NEnglJMed 1988319:1379-1384
22. Blair SN, Kohl HW, Paffenbarger RS, Clark DG, Cooper KH,Gibbons LW: Physical fitness and all-cause mortality: A prospec-tive study of healthy men and women. JAMA 1989;262:2395-2401
23. Wilhelmsen L, Bjure J, Ekstrom-Jddal B, Aurell M, Grimby G,Svardsudd K, Tibblin G, Wedel H: Nine years' foUow-up of amaximal exercise test in a random population sample of middle-aged men. Cardiology 1981;68(suppl 2):l-8
24. Kannel W, Gordon T, Offutt D: Left ventricular hypertrophy byECG: Prevalence, incidence and mortality in the FraminghamStudy. Ann Intern Med 1969;71:89-104
25. Gillum RF, Makuc DM, Feldman JJ: Pulse rate, coronary heartdisease, and death: The NHANES I Epidemiologic Folkrw-UpStudy. Am Heart J 1991;121:171-177
26. Persky V, Dyer AR, Leonas J, Stamler J, Berkson DM, LindbergHA, Paul O, Shekelle RB, Lepper MH, Schoenberger JA: Heartrate: A risk factor for cancer? Am J Epidemiol 1981;114:477-487
27. Kaplan JR, Manuck SB, Clarfcson TB: The influence of heart rateon coronary artery atherosclerosis. J Cardiovasc Pharmacol 1987;10(suppl 2):100-102
28. Lown B, Verrier RL, Rabinowitz SH: Neural and psychologicmechanisms and the problem of sudden cardiac death. Am J Car-diol 197739:890-902
by guest on April 22, 2018
http://hyper.ahajournals.org/D
ownloaded from
J Filipovský, P Ducimetière and M E SafarPrognostic significance of exercise blood pressure and heart rate in middle-aged men.
Print ISSN: 0194-911X. Online ISSN: 1524-4563 Copyright © 1992 American Heart Association, Inc. All rights reserved.
is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231Hypertension doi: 10.1161/01.HYP.20.3.333
1992;20:333-339Hypertension.
http://hyper.ahajournals.org/content/20/3/333World Wide Web at:
The online version of this article, along with updated information and services, is located on the
http://hyper.ahajournals.org//subscriptions/
is online at: Hypertension Information about subscribing to Subscriptions:
http://www.lww.com/reprints Information about reprints can be found online at: Reprints:
document. Permissions and Rights Question and Answer process is available in the
Request Permissions in the middle column of the Web page under Services. Further information about thisOffice. Once the online version of the published article for which permission is being requested is located, click
can be obtained via RightsLink, a service of the Copyright Clearance Center, not the EditorialHypertension Requests for permissions to reproduce figures, tables, or portions of articles originally published inPermissions:
by guest on April 22, 2018
http://hyper.ahajournals.org/D
ownloaded from











![Original Article Prognostic significance of MST1R ... · Original Article Prognostic significance of MST1R dysregulation ... [21]. Some of these variants are con - ... was performed](https://img.pdfslide.us/doc/110x75/5af36b967f8b9a190c8b9b83/original-article-prognostic-significance-of-mst1r-article-prognostic-significance.jpg)

















