Embed Size (px)
Citation preview

1
Prognostic impact of natural killer cell count in follicular lymphoma and
diffuse large B-cell lymphoma patients treated with immunochemotherapy
Magdalena Klanova,1–3* Mikkel Z Oestergaard,3* Marek Trněný,1 Wolfgang Hiddemann,4
Robert Marcus,5 Laurie H Sehn,6 Umberto Vitolo,7 Alexandra Bazeos,8 Valentin Goede,9
Harald Zeuner,3 Andrea Knapp,3 Deniz Sahin,3 Nathalie Danesi,3 Christopher R Bolen,10
Andres Cardona,3 Christian Klein,11 Jeffrey M Venstrom,10 Tina Nielsen,3 and Günter
Fingerle-Rowson3
*equal contribution
Affiliations
1Charles University General Hospital, Prague, Czech Republic; 2Institute of Pathological
Physiology, Charles University, Prague, Czech Republic; 3F. Hoffmann-La Roche Ltd, Basel,
Switzerland; 4University of Munich, Munich, Germany; 5Kings College Hospital, London,
United Kingdom; 6Centre for Lymphoid Cancer, British Columbia Cancer Agency and the
University of British Columbia, Vancouver, Canada; 7A.O.U. Citta' Della Salute e della
Scienza, S.C. Ematologia, Turin, Italy; 8Imperial College London, London, United Kingdom;
9Center of Integrated Oncology Cologne-Bonn, University Hospital Cologne, Cologne,
Germany; 10Genentech Inc., South San Francisco, USA; 11Roche Innovation Center Zurich,
Schlieren, Switzerland
Corresponding Author:
Dr Magdalena Klanova, 1st Department of Medicine, Charles University General Hospital, U
Nemocnice 2, Prague 2, 12808, Czech Republic
Email: [email protected]; Tel: +420 774 097 744
Dr Mikkel Z Oestergaard, Oncology Biomarker Development, F. Hoffman-La Roche,
Grenzacherstrasse 124, 4070 Basel, Switzerland
Email: [email protected]; Tel: +41 61 688 32 15
Cancer Research. on November 10, 2020. © 2019 American Association forclincancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on May 3, 2019; DOI: 10.1158/1078-0432.CCR-18-3270

2
Running title: Prognostic impact of NK cell count in FL and DLBCL
Word count manuscript: 3365
Tables/Figures: 3 Tables/3 Figures
Keywords: natural killer cells, natural killer cell count, follicular lymphoma, diffuse large B-
cell lymphoma, progression-free survival
Conflict-of-interest disclosures
MK, MZO, HZ, AC, AK, ND, and JV, report employment for F. Hoffmann-La Roche Ltd. JV
and CB report employment for Genentech. CB, TN, DZ, CK, and GFR report employment
and equity ownership for F. Hoffmann-La Roche Ltd. LHS reports consultancy and honoraria
for F. Hoffmann-La Roche Ltd, Genentech, Janssen, Amgen, Celgene, AbbVie, and Seattle
Genetics. WH reports research funding, honoraria, and advisory board membership for F.
Hoffmann-La Roche AG, Janssen, and Celgene. RM reports consultancy, honoraria, and
speakers bureau for F. Hoffmann-La Roche Ltd; and support for attending meetings for
Celgene. UV reports honoraria for F. Hoffmann-La Roche Ltd, Celgene, Janssen, Takeda,
and Gilead; advisory board membership for F. Hoffmann-La Roche Ltd, Celgene, and
Janssen; and research funding for F. Hoffmann-La Roche Ltd. VG reports advisory board
membership for F. Hoffmann-La Roche Ltd, Janssen, and Gilead; and honoraria and travel
grants for F. Hoffmann-La Roche Ltd and Janssen. AB reports a year-long academic
collaboration contract with F. Hoffmann-La Roche Ltd. MT reports consultancy and honoraria
for F. Hoffmann-La Roche Ltd, Celgene, Janssen, AbbVie, BMS, Takeda, and Gilead; and
research funding for F. Hoffmann-La Roche Ltd and Celgene.
Cancer Research. on November 10, 2020. © 2019 American Association forclincancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on May 3, 2019; DOI: 10.1158/1078-0432.CCR-18-3270

3
Translational relevance: NK cells are key effector cells for anti-CD20 monoclonal
antibodies, such as obinutuzumab and rituximab. However, it is unclear whether
pretreatment NK cell count (NKCC) affects outcome in patients receiving these therapies.
Here, we report that low peripheral blood NKCC at baseline is independently associated with
shorter PFS in both FL and DLBCL, and shorter OS in FL. We also show that low tumor NK
cell gene expression is associated with shorter PFS in obinutuzumab-treated, but not
rituximab-treated, DLBCL patients, which may reflect the stronger ability of obinutuzumab, a
Fc-glycoengineered antibody, to trigger ADCC compared with rituximab. These findings are
of translational relevance as they indicate the number of NK cells in peripheral blood at
baseline could impact the clinical outcome of FL and DLBCL patients treated with anti-CD20
antibodies. Peripheral blood NKCC might therefore represent a valuable and easily
accessible biomarker in clinical practice.
Cancer Research. on November 10, 2020. © 2019 American Association forclincancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on May 3, 2019; DOI: 10.1158/1078-0432.CCR-18-3270

4
Abstract
Purpose: Natural killer (NK) cells are key effector cells for anti-CD20 monoclonal antibodies,
such as obinutuzumab (G) and rituximab (R). We assessed whether low pretreatment NK
cell count (NKCC) in peripheral blood or tumor tissue was associated with worse outcome in
patients receiving antibody-based therapy.
Methods: Baseline peripheral blood NKCC was assessed by flow cytometry (CD3-CD56+
and/or CD16+ cells) in 1064/1202 follicular lymphoma (FL) patients treated with G or R plus
chemotherapy in the phase III GALLIUM trial (NCT01332968) and 1287/1418 diffuse large
B-cell lymphoma (DLBCL) patients treated with G or R plus cyclophosphamide, doxorubicin,
vincristine, and prednisone (CHOP) in the phase III GOYA trial (NCT01287741). The
prognostic value of tumor NK cell gene expression, as assessed by whole transcriptome
gene expression using Truseq RNA sequencing, was also analyzed. The association of
baseline variables, such as treatment arm, was evaluated using multivariate Cox regression
models using a stepwise approach.
Results: In this exploratory analysis, low baseline peripheral blood NKCC was associated
with shorter PFS in both FL (hazard ratio [HR] 1.48, 95% confidence interval [CI], 1.02-2.14,
P = 0.04) and DLBCL (HR, 1.36, 95% CI, 1.01-1.83, P = 0.04), and OS in FL (HR, 2.20, 95%
CI, 1.26-3.86, P = 0.0058). Low tumor NK cell gene expression was associated with shorter
PFS in G-CHOP-treated DLBCL patients (HR, 1.95, 95% CI, 1.22-3.15, P < 0.01).
Conclusion: These findings indicate that the number of NK cells in peripheral blood may
affect the outcome of B-cell non-Hodgkin lymphoma patients receiving anti-CD20-based
immunochemotherapy.
Cancer Research. on November 10, 2020. © 2019 American Association forclincancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on May 3, 2019; DOI: 10.1158/1078-0432.CCR-18-3270

5
Introduction
Natural killer (NK) cells are a key element of the innate immune system, with an
important role in maintaining immune surveillance of virus-infected or transformed cells. NK
cells are part of the hematopoietic system and are derived from CD34+ hematopoietic
progenitor cells (1). In general, NK cells are characterized by their absence of the T-cell
receptor complex (CD3) along with the presence of CD56, a 140 kDa isoform of neural cell
adhesion molecule. The surface expression of CD56 defines two main subsets of NK cells,
CD56bright and CD56dim (2, 3). CD56bright NK cells make up approximately 10% of circulating
blood NK cells, and are characterized by a high surface expression of CD56 and low or
negative levels of Fcγ receptor IIIA (FcγRIIIa or CD16) (3, 4). In contrast, CD56dim NK cells
represent at least 90% of the NK cell population in peripheral blood, and are characterized
by a low surface expression of CD56 and high levels of FcγRIIIa (3, 4).
FcγRIIIa is a low affinity activating receptor that can bind to the constant (Fc) region
of IgG antibodies when immobilized on the cell surface (5). Ligation of FcγRIIIa on NK cells
with the Fc region of antibody-coated tumor cells results in degranulation of NK cells, with
subsequent lysis of tumor cells by perforins and granzymes and secretion of
proinflammatory cytokines; this consequently leads to the activation of other immune cells,
including monocytes/macrophages, dendritic cells, and granulocytes. This process is known
as antibody-dependent cellular cytotoxicity (ADCC), and represents an important mechanism
of action of monoclonal antibodies, such as the anti-CD20 monoclonal antibody, rituximab
(R). Other mechanisms responsible for the antitumor efficacy of R have been described,
including direct cell death and complement-mediated cellular cytotoxicity (6-9).
ADCC enhancement through Fc domain modification has also shown promise in the
development of next generation antibodies (10). Obinutuzumab (GA101; G) is a type II anti-
CD20 monoclonal antibody with enhanced direct cell death activity and a glycoengineered
Fc region that enhances its binding affinity to FcγRIIIa on NK and other effector cells,
Cancer Research. on November 10, 2020. © 2019 American Association forclincancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on May 3, 2019; DOI: 10.1158/1078-0432.CCR-18-3270

6
thereby resulting in stronger ADCC compared with R (11-14). Such high affinity ligation of
FcγRIIIa has been shown to prime NK cells for interferon-gamma (IFN-γ) production (15).
As NK cells are the key mediators of ADCC, we postulated that low pretreatment NK
cell count (NKCC) may be associated with worse outcomes in patients with B-cell non-
Hodgkin lymphoma (B-NHL) treated with anti-CD20-based immunochemotherapy. Here, we
evaluate the prognostic impact of baseline NKCC in follicular lymphoma (FL) patients treated
with G or R plus chemotherapy in the phase III GALLIUM trial and diffuse large B-cell
lymphoma (DLBCL) patients treated with G or R plus cyclophosphamide, doxorubicin,
vincristine, and prednisone (CHOP) in the phase III GOYA trial (16, 17). The prognostic
value of tumor NK cell gene expression was also analyzed in DLBCL patients.
Methods
Patients, treatments, and assessments
The GALLIUM and GOYA study designs are described in full elsewhere (16, 17). In
brief, in the GALLIUM study, eligible patients had previously untreated, histologically
documented, CD20-positive FL (histological grades 1–3a), Eastern Cooperative Oncology
Group (ECOG) performance status 0–2, stage III/IV disease (or stage II with bulky disease,
i.e., largest tumor diameter ≥7 cm), and required treatment according to the Groupe d’Étude
des Lymphomes Folliculaires (GELF) criteria. Patients were treated with G or R plus
chemotherapy (bendamustine; cyclophosphamide, vincristine, and prednisone [CVP]; or
CHOP) for six or eight cycles depending on the chemotherapy. Choice of chemotherapy was
stipulated by site, with all patients at a given site receiving the same chemotherapy
backbone. Patients who achieved complete or partial remission at the end of induction
received maintenance therapy with G or R every two months for two years, or until disease
progression or study withdrawal if earlier. In the GOYA study, eligible patients had previously
untreated, histologically documented, CD20-positive DLBCL, an ECOG performance status
0–2, and an International Prognostic Index (IPI) score ≥2 (or IPI score 1 if aged ≤60 years,
Cancer Research. on November 10, 2020. © 2019 American Association forclincancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on May 3, 2019; DOI: 10.1158/1078-0432.CCR-18-3270

7
with or without bulky disease; or IPI score 0 with bulky disease, i.e., one lesion ≥7.5 cm).
Patients were treated with eight 21-day cycles of G or R plus six-to-eight cycles of CHOP
chemotherapy. In both studies, tumor response was assessed using a modified response
criteria for NHL (18). GALLIUM was conducted in accordance with the Declaration of
Helsinki and the International Conference on Harmonization guidelines for Good Clinical
Practice. GOYA was conducted in accordance to the Declaration of Helsinki. The protocols
for the GALLIUM and GOYA trials were approved by the ethics committees of participating
centers and the trials were registered at ClinicalTrials.gov (NCT01332968 and
NCT01287741, respectively). All patients provided written informed consent.
Flow cytometry analysis
Baseline NKCCs were centrally assessed from EDTA-anticoagulated peripheral
blood by flow cytometry (Quintiles laboratories Ltd, Marietta, Georgia). Briefly, peripheral
blood was collected in Cytochex BCT tubes and shipped to central laboratories located in
the US, Europe, and Asia. Whole blood (50 μL) was stained with the BD Multitest 6-color
TBNK assay in TruCount tubes (BD Biosciences, San Jose, California). BD lyse solution was
used for red blood cell lysis. The number of NK cells, which were defined as CD3-CD56+
and/or CD16+ cells, was measured by flow cytometry (FACSCanto II; BD Biosciences, San
Jose, California; normal range [determined by central laboratory]: 95–640 cells/µL).
Cell-of-origin analysis
Cell-of-origin (COO) classification was based on gene expression profiling using the
NanoString Lymphoma Subtyping Research-Use-Only assay (NanoString Technologies,
Inc., Seattle, US) on RNA extracted from formalin-fixed paraffin-embedded (FFPE) tumor
tissue.
Whole transcriptome RNA sequencing
RNA was extracted from FFPE tissues using the RNeasy FFPE kit (Qiagen, Hilden,
Germany). Whole transcriptome gene expression was analyzed using TruSeq RNA
Cancer Research. on November 10, 2020. © 2019 American Association forclincancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on May 3, 2019; DOI: 10.1158/1078-0432.CCR-18-3270

8
sequencing. A 57-gene signature designed to reflect NK cell tumor infiltration was
subsequently applied to RNA sequencing data, as previously described (19), and a signature
score was calculated as the first principal component of expression in those 57 genes.
Median score was used to define low/high subgroups for tumor NK cell gene expression.
Statistical analysis
This exploratory post-hoc analysis was carried out in FL (GALLIUM) and DLBCL
(GOYA) patients with an evaluable peripheral blood NKCC at baseline. The optimal cut-off
for defining low and normal/high NKCC subpopulations was analyzed in FL and DLBCL
patients using a SAS macro that implements the maximal Chi-square statistic (20, 21); this
cut-off, which led to the greatest difference in PFS between low and normal/high NKCC
subgroups, was 99 cells/μL for FL and 102 cells/μL for DLBCL. Low NKCC was thus defined
as <100 cells/µL and normal/high NKCC was defined as ≥100 cells/μL, as previously
described by He et al (22).
The association of baseline variables (sex, geographic region, treatment arm,
chemotherapy backbone/number of planned chemotherapy cycles, Follicular Lymphoma
International Prognostic Index [FLIPI]/IPI, extranodal/bone marrow involvement, sum of
products of diameter [SPD], and Ann Arbor stage) with peripheral blood NKCC was
evaluated using multivariate Cox regression models using a stepwise approach. These
statistical tests were two-sided with no adjustment for multiplicity. For the tumor NK cell gene
expression signature, hazard ratios (HRs) and 95% confidence intervals (CIs) were
estimated using a multivariate Cox proportional hazard, with treatment arm, number of
planned chemotherapy cycles, IPI, geographic region (GOYA) or treatment arm, FLIPI, and
chemotherapy backbone (GALLIUM) included as covariates. A Cox multivariate model was
used to evaluate the potential predictive value of NKCC as a biomarker factor for
progression-free survival (PFS) and overall survival (OS), and of tumor NK cell gene
expression signature as a biomarker factor for PFS, in patients treated with R-chemo and G-
chemo (treatment-by-NKCC interaction).
Cancer Research. on November 10, 2020. © 2019 American Association forclincancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on May 3, 2019; DOI: 10.1158/1078-0432.CCR-18-3270

9
Qualified researchers may request access to individual patient level data through the
clinical study data request platform (www.clinicalstudydatarequest.com). Further details on
Roche's criteria for eligible studies are available here
(https://clinicalstudydatarequest.com/Study-Sponsors/Study-Sponsors-Roche.aspx). For
further details on Roche's Global Policy on the Sharing of Clinical Information and how to
request access to related clinical study documents, see here
(https://www.roche.com/research_and_development/who_we_are_how_we_work/clinical_tri
als/our_commitment_to_data_sharing.htm).
Results
Patients and baseline peripheral blood NKCCs
The analysis population consisted of patients with an evaluable NKCC at baseline
(1064/1202 FL patients [88.5% of the GALLIUM ITT population] and 1287/1418 DLBCL
patients [90.8% of the GOYA ITT population]. Baseline patient and disease characteristics
were comparable between the analysis population and the respective ITT populations
(Supplemental Table 1). Median (range) baseline peripheral blood NKCCs were 222 cells/μL
(13–3327) in FL and 196 cells/μL (5–1930) in DLBCL patients. Overall, 108/1064 (10.2%) FL
patients and 255/1287 (19.8%) DLBCL patients had a low baseline peripheral blood NKCC
(<100 cells/μL) (Supplementary Fig. 1A).
COO and baseline NKCC were available in 857/1418 (60.4%) DLBCL patients. By
COO subtype, median (range) baseline peripheral blood NKCCs were 186 cells/μL (6–
1659), 167 cells/μL (7–1715), and 200 cells/μL (8–1930) in germinal center B-cell-like
(GCB), unclassified, and activated B-cell-like (ABC) DLBCL, respectively. Low baseline
peripheral blood NKCC was detected in 83/485 (17.1%) GCB, 37/140 (26.4%) unclassified,
and 54/232 (23.3%) ABC DLBCL patients (P = 0.022 representing a significant imbalance
between COO subtypes) (Supplementary Fig. 1B).
Cancer Research. on November 10, 2020. © 2019 American Association forclincancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on May 3, 2019; DOI: 10.1158/1078-0432.CCR-18-3270

10
Baseline patient and disease characteristics of FL and DLBCL patients with low vs.
normal/high baseline peripheral blood NKCCs are shown in Table 1. FL patients with low
baseline peripheral blood NKCC more frequently had extranodal involvement, elevated
lactate dehydrogenase (LDH) levels, and high FLIPI score compared with patients with
normal/high NKCC. Similarly, DLBCL patients with low baseline peripheral blood NKCC
more frequently had higher Ann Arbor stage, ECOG performance status, and IPI score,
extranodal involvement, and elevated LDH levels compared with patients with normal/high
NKCC. SPD was higher in patients with low baseline peripheral blood NKCC compared with
patients with normal/high NKCC in FL and DLBCL. No difference in the frequency of bone
marrow involvement between patients with low vs. normal/high baseline peripheral blood
NKCC was observed in either FL or DLBCL.
Impact of low baseline peripheral blood NKCC on clinical outcome
Multivariate analyses with baseline patient and disease characteristics, treatment
arm, and chemotherapy backbone (in the case of GALLIUM) as covariates showed that low
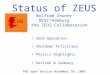
baseline peripheral blood NKCC was independently associated with shorter PFS in FL (HR,
1.48, 95% CI, 1.02-2.14, P = 0.04; 3-year PFS rate, 71.6% vs. 80.1% in patients with
normal/high baseline peripheral blood NKCC) and DLBCL (HR, 1.36, 95% CI, 1.01-1.83, P =
0.04; 3-year PFS rate, 62.8% vs. 70.0%) (Table 2; Fig. 1A), and OS in FL (HR, 2.20, 95%
CI, 1.26-3.86, P = 0.0058; 3-year OS rate, 87.6% vs. 94.3%); (Table 3; Fig. 1B). The DLBCL
PFS result appeared to be driven by COO subtype, with the highest estimated HR in the
GCB subtype (HR 1.58, 95% CI, 1.00-2.50, P = 0.05; 3-year PFS rate, 70.0% vs. 77.4% in
patients with normal/high baseline peripheral blood NKCC); no effect was observed in the
unclassified and ABC subtypes (Fig. 2A). No significant impact of low baseline peripheral
blood NKCC on OS was observed in the GCB, unclassified, or ABC subtypes (Fig. 2B).
Low baseline peripheral blood NKCC was associated with shorter PFS irrespective of the
type of anti-CD20 antibody used ([univariate analysis] FL: R-chemo, HR, 1.19, 95% CI, 0.71-
Cancer Research. on November 10, 2020. © 2019 American Association forclincancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on May 3, 2019; DOI: 10.1158/1078-0432.CCR-18-3270

11
1.99; G-chemo, HR, 2.06, 95% CI, 1.24-3.41; DLBCL: R-CHOP, HR, 1.47, 95% CI, 1.06-
2.06; G-CHOP, HR, 1.26, 95% CI, 0.90-1.77).
Multivariate analysis with treatment-by-NKCC interaction showed the treatment effect
of G-chemo/CHOP and R-chemo/CHOP on PFS and OS persisted regardless of the NKCC
of patients.
Impact of low tumor NK cell gene expression signature on clinical outcome
Gene expression by whole transcriptome RNA sequencing was assessed in tumor
tissue of 236/1202 (19.6%) FL patients in GALLIUM and 552/1418 (38.9%) DLBCL patients
in GOYA. Low CD56 mRNA expression alone (as a continuous variable) correlated with
shorter PFS (P = 0.043) in DLBCL, but not in FL (P = 0.447). Baseline peripheral blood
NKCC and tumor NK cell gene expression were evaluable in 201/1202 (16.7%) and
508/1418 (35.8%) FL and DLBCL patients, respectively. There was no correlation between
baseline peripheral blood NKCC and tumor NK cell gene expression among biomarker-
evaluable FL (r = 0.053, P = 0.46) and DLBCL (r = 0.05, P = 0.25) patients (Supplemental
Fig. 2A/B). Multivariate analysis showed no significant difference in PFS between low vs.
high tumor NK cell gene expression in patients with FL (HR, 0.84, 95% CI, 0.50-1.4; P = 0.5)
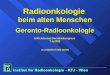
or DLBCL (HR, 1.31, 95% CI, 0.95-1.81; P = 0.11) (Fig. 3A and 3D). In a subgroup
(multivariate) analysis of tumor NK cell gene expression and outcome, no effect of low tumor
NK cell gene expression on PFS was observed in FL patients treated with R-chemo (HR,
0.56, 95% CI, 0.29-1.10; P = 0.09) or G-chemo (HR, 1.68, 95% CI, 0.72-3.94; P = 0.23) (Fig.
3B and 3C), or in DLBCL patients treated with R-CHOP (HR, 0.92, 95% CI, 0.57-1.48, P =
0.72) (Fig. 3E); by contrast, low tumor NK cell gene expression was associated with shorter
PFS in DLBCL patients treated with G-CHOP (HR, 1.95, 95% CI, 1.22-3.15, P < 0.01) (Fig.
3F). Results of an interaction test showed that the prognostic value of the NK cell signature
was significantly stronger among G-CHOP-treated patients compared with R-CHOP-treated
patients (P = 0.016).
Cancer Research. on November 10, 2020. © 2019 American Association forclincancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on May 3, 2019; DOI: 10.1158/1078-0432.CCR-18-3270

12
Baseline NKCC and risk or severity of infusion-related reactions and infections
The frequency of grade 3–5 and serious infusion-related reactions (IRRs) were
comparable in patients with low and normal/high baseline peripheral blood NKCC in both FL
and DLBCL (Supplemental Table 2). No grade 5 IRRs were observed in either GOYA or
GALLIUM. The frequency of grade 3–5 and serious infections were comparable in DLBCL
patients with low and normal/high baseline peripheral blood NKCC. In contrast, there
appeared to be more grade 3–5 and serious infections among FL patients with low NKCC,
driven by more infections in the G-chemo arm (Supplemental Table 3).
Discussion
In the current study, we evaluated the prognostic impact of baseline peripheral blood
NKCC in patients with FL and DLBCL who were treated with the anti-CD20 monoclonal
antibodies, G or R, in combination with chemotherapy in the first-line, phase III GALLIUM
(FL) and GOYA (DLBCL) trials. In this exploratory, post-hoc analysis carried out on the
largest prospective collection of NKCCs to date, we found that a subset of patients with FL
and DLBCL had a low NKCC at baseline, which was independently associated with shorter
PFS in both FL and DLBCL, and shorter OS in FL (but not DLBCL). The prognostic impact of
baseline peripheral blood NKCC in these lymphoma subtypes is consistent with the results
of previous smaller retrospective studies (22-26) and is in accordance with findings from in
vitro studies of ADCC, which unequivocally demonstrate that the of level tumor-cell killing is
decreased with lower effector-to-target ratios (27, 28).
We showed evidence for a prognostic role of NK cells in germinal center-derived
lymphomas, such as FL and GCB DLBCL, while no significant effect was observed in the
unclassified or ABC DLBCL subtypes. The reason for this observation remains unclear,
although it could be explained by differences in their microenvironment and underlying tumor
genetics given that particular COO subtypes exhibit distinct mutational profiles and are
driven by different oncogenic pathways (29-31). For example, the GCB DLBCL subtype,
Cancer Research. on November 10, 2020. © 2019 American Association forclincancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on May 3, 2019; DOI: 10.1158/1078-0432.CCR-18-3270

13
which has a more favorable prognosis than other DLBCL subtypes, is molecularly similar to
FL, with frequent alterations in epigenetic modifiers, such as EZH2, or translocation of the
BCL2 gene resulting in deregulation of apoptosis (31-33). In contrast, the hallmarks of ABC
DLBCL include constitutive activation of the NFkB pathway and cell cycle deregulation due
to loss of CDKN2A (30, 34). It may be the case that low NKCC loses its importance in the
presence of the latter genetic abnormalities and an unfavorable microenvironment, both of
which are associated with the poor prognosis of ABC DLBCL. The number of patients with
unclassified (n = 140) and ABC (n = 232) DLBCL was fewer than those with GCB DLBCL (n
= 485), and thus limited information was available on NKCC in patients with these DLBCL
subtypes.
A subset of patients with FL and DLBCL had reduced peripheral blood NKCC at
baseline; of note, low NKCC was almost twice as prevalent in DLBCL patients compared
with FL patients (19.8% vs. 10.2%). The precise mechanism explaining the observed
incidence of reduced NKCC is unknown. NK cells develop from bone marrow hematopoietic
stem cells and mature in secondary lymphoid tissue; thus, bone marrow infiltration by
lymphoma cells could suppress normal hematopoiesis, thereby reducing the absolute
number of circulating NK cells. However, consistent with findings from other studies, bone
marrow involvement at baseline was similar here for low versus normal/high baseline
peripheral blood NKCC in FL and DLBCL, suggesting that other mechanisms are involved.
It has been shown that lymphoma cells may block maturation of NK cells in the bone
marrow by interrupting pathways necessary for their development or via mechanisms
leading to direct inhibition or killing of immune cells, including NK cells (35, 36). These
mechanisms operate differently in FL and DLBCL, as well as in particular COO subtypes
(36), and thus may contribute to different levels of host immune suppression in B-NHL
subtypes. In line with this, we observed that FL and DLBCL patients with low baseline
peripheral blood NKCCs had adverse clinical characteristics compared with patients with
normal/high NKCCs. The association of low NKCC or impaired NK cell function with high-risk
Cancer Research. on November 10, 2020. © 2019 American Association forclincancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on May 3, 2019; DOI: 10.1158/1078-0432.CCR-18-3270

14
or advanced-stage disease has also been shown in solid tumors and in hematologic
malignancies (37). These data suggest that low levels of NK cells or defective NK cells may
contribute to inadequate immunity against tumor cells, leading to more aggressive disease
manifestation and vice versa.
A low number of circulating NK cells was associated with worse outcome in
lymphoma patients treated with R or G in combination with chemotherapy. It is not well
known how representative the peripheral blood is for the overall number of NK cells in the
body. The tumor compartment may better reflect the functional interaction between
lymphoma and NK cells. However, the technical difficulties associated with the acquisition of
tumor tissue and the limited amount of tissue available may limit the value of a tissue-based
approach. Interestingly, we found no correlation between peripheral blood NKCC and tumor
NK cell gene expression signature (representative of the number of NK cells in tumor tissue).
The extent of NK cell recruitment to tumor tissue depends not only on their availability (i.e.
on their release from bone marrow to peripheral blood), but also on the intensity of local
chemokine signaling, which attracts NK cells into the tumor tissue and enables penetration
and local activation (38). Lack of such chemoattractant signaling would likely result in
insufficient NK cell infiltration even in the presence of a normal/high peripheral blood NKCC.
We observed that G-treated DLBCL patients with low expression of a tumor NK cell gene
expression signature had significantly shorter PFS compared with those with high
expression of the tumor NK cell signature. This effect was not observed in R-treated
patients, which may reflect the stronger ability of the Fc-glycoengineered G antibody to
trigger ADCC compared with R (12). Although this hypothesis was not confirmed in FL, it
should be noted that the number of FL patients with an evaluable NK cell gene expression
signature was much lower than that for DLBCL patients. Future studies are needed to
provide further insight.
Our results provide a rationale for investigating anti-CD20 antibodies in combination
with agents that enhance NK cell function. New therapeutic IL-2-based molecules have been
Cancer Research. on November 10, 2020. © 2019 American Association forclincancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on May 3, 2019; DOI: 10.1158/1078-0432.CCR-18-3270

15
developed and are currently under clinical evaluation in various types of malignancies. In
addition to stimulating cytokines, such as IL-2 and IL-15, other agents have shown the ability
to activate NK cells. Immunomodulatory agents, such as thalidomide or lenalidomide, can
increase the number of circulating NK cells and augment their direct cytotoxic activity against
tumor cells (39). These data also encourage the investigation of combining anti-CD20
antibodies with adoptive T cell therapy using cytokine-induced killer cells (40). Further
studies are certainly needed to explore if such treatments would be more effective than
standard immunochemotherapy.
In conclusion, the results from the current exploratory analysis of the GALLIUM and
GOYA trials indicate that the number of NK cells in peripheral blood may impact the clinical
outcome of patients with B-NHL treated with anti-CD20 antibodies. Specifically, we found
that low peripheral blood NKCC impacted PFS in both FL and DLBCL, and OS in FL. Our
findings suggest that peripheral blood NKCC could represent a valuable biomarker in clinical
practice, and could pave the way to the development of novel combination treatment
approaches that aim to enhance the activity of anti-CD20 antibodies by providing them with
a sufficient number of functional effector cells in B-NHL.
Cancer Research. on November 10, 2020. © 2019 American Association forclincancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on May 3, 2019; DOI: 10.1158/1078-0432.CCR-18-3270

16
Author’s Contributions
Conception and design: MK, MZO, TN, GFR, HZ, DS, ND, CK, and AK; CB and JV
conceived and designed the sequencing data analysis
Acquisition of data (provided animals, acquired and managed patients, provided
facilities, etc): MT, WH, RM, LHS, UV, AB, and VG provided study materials or patients
Writing of the manuscript: MK
Analysis and interpretation of the data (e.g., statistical analysis, biostatics,
computational analysis): all authors
Critical review and approval of manuscript: all authors
Acknowledgments
The authors wish to thank the study investigators, coordinators, nurses, and patients of the
GOYA and GALLIUM trials, and Susan Robson for her invaluable contribution to the data
analysis and interpretation. GOYA and GALLIUM were supported by F. Hoffmann-La Roche
Ltd. Editorial support was provided by Janis Noonan, PhD (Gardiner-Caldwell
Communications Ltd, Macclesfield, UK), and funded by F. Hoffmann-La Roche Ltd.
Cancer Research. on November 10, 2020. © 2019 American Association forclincancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on May 3, 2019; DOI: 10.1158/1078-0432.CCR-18-3270

17
References
1. Galy A, Travis M, Cen D, Chen B. Human T, B, natural killer, and dendritic cells arise
from a common bone marrow progenitor cell subset. Immunity. 1995;3(4):459-73.
2. Lanier LL, Testi R, Bindl J, Phillips JH. Identity of Leu-19 (CD56) leukocyte
differentiation antigen and neural cell adhesion molecule. J Exp Med. 1989;169(6):2233-8.
3. Caligiuri MA. Human natural killer cells. Blood. 2008;112(3):461-9.
4. Cooper MA, Fehniger TA, Caligiuri MA. The biology of human natural killer-cell
subsets. Trends in immunology. 2001;22(11):633-40.
5. Nimmerjahn F, Ravetch JV. Fcgamma receptors as regulators of immune responses.
Nat Rev Immunol. 2008;8(1):34-47.
6. Abulayha A, Bredan A, El Enshasy H, Daniels I. Rituximab: modes of action,
remaining dispute and future perspective. Future oncology (London, England).
2014;10(15):2481-92.
7. Maloney DG, Smith B, Rose A. Rituximab: Mechanism of action and resistance.
Seminars in oncology. 2002;29(1s2):2-9.
8. Weiner GJ. Rituximab: mechanism of action. Seminars in hematology.
2010;47(2):115-23.
9. Boross P, Leusen JH. Mechanisms of action of CD20 antibodies. American journal of
cancer research. 2012;2(6):676-90.
10. Kellner C, Zhukovsky EA, Potzke A, Bruggemann M, Schrauder A, Schrappe M, et
al. The Fc-engineered CD19 antibody MOR208 (XmAb5574) induces natural killer cell-
mediated lysis of acute lymphoblastic leukemia cells from pediatric and adult patients.
Leukemia. 2013;27(7):1595-8.
11. Niederfellner G, Lammens A, Mundigl O, Georges GJ, Schaefer W, Schwaiger M, et
al. Epitope characterization and crystal structure of GA101 provide insights into the
molecular basis for type I/II distinction of CD20 antibodies. Blood. 2011;118(2):358-67.
12. Mossner E, Brunker P, Moser S, Puntener U, Schmidt C, Herter S, et al. Increasing
the efficacy of CD20 antibody therapy through the engineering of a new type II anti-CD20
antibody with enhanced direct and immune effector cell-mediated B-cell cytotoxicity. Blood.
2010;115(22):4393-402.
13. Bologna L, Gotti E, Manganini M, Rambaldi A, Intermesoli T, Introna M, et al.
Mechanism of action of type II, glycoengineered, anti-CD20 monoclonal antibody GA101 in
B-chronic lymphocytic leukemia whole blood assays in comparison with rituximab and
alemtuzumab. J Immunol. 2011;186(6):3762-9.
Cancer Research. on November 10, 2020. © 2019 American Association forclincancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on May 3, 2019; DOI: 10.1158/1078-0432.CCR-18-3270

18
14. Klein C, Lammens A, Schafer W, Georges G, Schwaiger M, Mossner E, et al.
Epitope interactions of monoclonal antibodies targeting CD20 and their relationship to
functional properties. MAbs. 2013;5(1):22-33.
15. Capuano C, Pighi C, Molfetta R, Paolini R, Battella S, Palmieri G, et al.
Obinutuzumab-mediated high-affinity ligation of FcgammaRIIIA/CD16 primes NK cells for
IFNgamma production. Oncoimmunology. 2017;6(3):e1290037.
16. Marcus R, Davies A, Ando K, Klapper W, Opat S, Owen C, et al. Obinutuzumab for
the First-Line Treatment of Follicular Lymphoma. N Engl J Med. 2017;377(14):1331-44.
17. Vitolo U, Trneny M, Belada D, Burke JM, Carella AM, Chua N, et al. Obinutuzumab
or Rituximab Plus Cyclophosphamide, Doxorubicin, Vincristine, and Prednisone in
Previously Untreated Diffuse Large B-Cell Lymphoma. J Clin Oncol. 2017:JCO2017733402.
18. Cheson BD, Pfistner B, Juweid ME, Gascoyne RD, Specht L, Horning SJ, et al.
Revised response criteria for malignant lymphoma. J Clin Oncol. 2007;25(5):579-86.
19. Newman AM, Liu CL, Green MR, Gentles AJ, Feng W, Xu Y, et al. Robust
enumeration of cell subsets from tissue expression profiles. Nat Methods. 2015;12(5):453-7.
20. D MRaS. Maximally selected chi square statistics. Biometrics. 1982;38(4).
21. B ZQaD. A SAS® Macro for biomarker analysis using maximally selected Chi square
statistics with application in oncology. PharmaSUG. 2012:8.
22. He L, Zhu HY, Qin SC, Li Y, Miao Y, Liang JH, et al. Low natural killer (NK) cell
counts in peripheral blood adversely affect clinical outcome of patients with follicular
lymphoma. Blood Cancer J. 2016;6(8):e457.
23. Plonquet A, Haioun C, Jais JP, Debard AL, Salles G, Bene MC, et al. Peripheral
blood natural killer cell count is associated with clinical outcome in patients with aaIPI 2-3
diffuse large B-cell lymphoma. Ann Oncol. 2007;18(7):1209-15.
24. Shafer D, Smith MR, Borghaei H, Millenson MM, Li T, Litwin S, et al. Low NK cell
counts in peripheral blood are associated with inferior overall survival in patients with
follicular lymphoma. Leukemia research. 2013;37(10):1213-5.
25. Du J, Lopez-Verges S, Pitcher BN, Johnson J, Jung SH, Zhou L, et al. CALGB
150905 (Alliance): rituximab broadens the antilymphoma response by activating unlicensed
NK cells. Cancer immunology research. 2014;2(9):878-89.
26. Jurczak W, Zinzani PL, Gaidano G, Goy A, Provencio M, Nagy Z, et al. Phase IIa
study of the CD19 antibody MOR208 in patients with relapsed or refractory B-cell non-
Hodgkin's lymphoma. Ann Oncol. 2018;29(5):1266-72.
27. Palazzo A Herter S Grosmaire L JR, Frey CR, Limani F, et al. The PI3Kδ-selective
inhibitor idelalisib minimally interferes with immune effector function mediated by rituximab or
obinutuzumab and significantly augments B cell depletion in vivo. J Immunol. 2018;200
(7):2304-12.
Cancer Research. on November 10, 2020. © 2019 American Association forclincancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on May 3, 2019; DOI: 10.1158/1078-0432.CCR-18-3270

19
28. Wang SY Racila E TR, Weiner GJ. NK-cell activation and antibody-dependent
cellular cytotoxicity induced by rituximab-coated target cells is inhibited by the C3b
component of complement. Blood. 2008;111(3):1456-63.
29. Alizadeh AA, Eisen MB, Davis RE, Ma C, Lossos IS, Rosenwald A, et al. Distinct
types of diffuse large B-cell lymphoma identified by gene expression profiling. Nature.
2000;403(6769):503-11.
30. Lenz G, Wright GW, Emre NC, Kohlhammer H, Dave SS, Davis RE, et al. Molecular
subtypes of diffuse large B-cell lymphoma arise by distinct genetic pathways. Proc Natl Acad
Sci U S A. 2008;105(36):13520-5.
31. Oestergaard M, Bolen C, Mattiello F, et al. Superiority of obinutuzumab over
rituximab in a new molecular follicular lymphoma-like subgroup of DLBCL: results from an
exploratory analysis of the phase 3 Goya trial. Blood. 2017;130(1543).
32. Morin RD, Mendez-Lago M, Mungall AJ, Goya R, Mungall KL, Corbett RD, et al.
Frequent mutation of histone-modifying genes in non-Hodgkin lymphoma. Nature.
2011;476(7360):298-303.
33. Pasqualucci L, Trifonov V, Fabbri G, Ma J, Rossi D, Chiarenza A, et al. Analysis of
the coding genome of diffuse large B-cell lymphoma. Nat Genet. 2011;43(9):830-7.
34. Davis RE, Ngo VN, Lenz G, Tolar P, Young RM, Romesser PB, et al. Chronic active
B-cell-receptor signalling in diffuse large B-cell lymphoma. Nature. 2010;463(7277):88-92.
35. Richards JO, Chang X, Blaser BW, Caligiuri MA, Zheng P, Liu Y. Tumor growth
impedes natural-killer-cell maturation in the bone marrow. Blood. 2006;108(1):246-52.
36. de Charette M, Houot R. Hide or defend, the two strategies of lymphoma immune
evasion: potential implications for immunotherapy. Haematologica. 2018;103(8):1256-68.
37. Hejazi M, Manser AR, Frobel J, Kundgen A, Zhao X, Schonberg K, et al. Impaired
cytotoxicity associated with defective natural killer cell differentiation in myelodysplastic
syndromes. Haematologica. 2015;100(5):643-52.
38. Przewoznik M, Homberg N, Naujoks M, Potzl J, Munchmeier N, Brenner CD, et al.
Recruitment of natural killer cells in advanced stages of endogenously arising B-cell
lymphoma: implications for therapeutic cell transfer. J Immunother. 2012;35(3):217-22.
39. Davies FE, Raje N, Hideshima T, Lentzsch S, Young G, Tai YT, et al. Thalidomide
and immunomodulatory derivatives augment natural killer cell cytotoxicity in multiple
myeloma. Blood. 2001;98(1):210-6.
40. Pievani A, Belussi C, Klein C, Rambaldi A, Golay J, Introna M. Enhanced killing of
human B-cell lymphoma targets by combined use of cytokine-induced killer cell (CIK)
cultures and anti-CD20 antibodies. Blood. 2011;117(2):510-8.
Cancer Research. on November 10, 2020. © 2019 American Association forclincancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on May 3, 2019; DOI: 10.1158/1078-0432.CCR-18-3270

20
Table 1. Baseline patient demographics and disease characteristics.
FL (GALLIUM)
n = 1064 DLBCL (GOYA)
n = 1287
NKCC <100
cells/μL n = 108
NKCC ≥100
cells/μL n = 956
NKCC <100
cells/μL n = 255
NKCC ≥100
cells/μL n = 1032
Age, years ≥65 31 (28.7) 303 (31.7) 86 (33.7) 423 (41.0)
ECOG PS ≥2 5 (4.6) 30 (3.1)a 45 (17.6) 125 (12.1)f
Ann Arbor stage
III–IV 98 (90.7) 872 (91.9)b 220 (86.3) 758 (73.4)
Extranodal involvement
Yes 77 (71.3) 625 (65.4) 185 (72.5) 683 (66.2)
Bone marrow involvement
Yes 55 (51.4)c 491 (51.8)d 32 (12.7)g 103 (10.1)d
Bulky disease Yes 48 (44.4) 425 (44.5)e 110 (43.1) 356 (34.6)g
FLIPI High 54 (50.0) 393 (41.1) – –
IPI High – – 50 (19.6) 153 (14.8)
SPD, mm2 Mean (SD) 7762
(8961) 7053
(6520) 8624
(14302) 6631
(16850)
LDH Elevated 42 (38.9) 276 (29.0) 175 (68.6) 568 (55.2)
Treatment group
R-chemo/CHOP 56 (51.9) 456 (47.7) 116 (45.5) 532 (51.6)
G-chemo/CHOP 52 (48.1) 500 (52.3) 139 (54.5) 500 (48.4)
Data are n (%) unless otherwise specified. aData missing in 3 patients; bdata missing in 7 patients; cdata missing in 1 patient; ddata missing in 9 patients; edata missing in 2 patients; fdata missing in 1 patient; gdata missing in 3 patients.
Chemo, chemotherapy; CHOP, cyclophosphamide, doxorubicin, vincristine, and prednisone; DLBCL, diffuse large B-cell lymphoma; ECOG PS, Eastern Cooperative Oncology Group performance status; FL, follicular lymphoma; FLIPI, Follicular Lymphoma International Prognostic Index; G, obinutuzumab; IPI, International Prognostic Index; LDH, lactate dehydrogenase; NKCC, natural killer cell count; R, rituximab; SD, standard deviation, SPD, sum of products of diameter of up to 6 target lesions.
Cancer Research. on November 10, 2020. © 2019 American Association forclincancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on May 3, 2019; DOI: 10.1158/1078-0432.CCR-18-3270

21
Table 2. Multivariate analysis of the association between baseline variables and PFS in FL
(A) and DLBCL (B).a
A
FL, n = 1057 HR 95% CIc P value
NKCC <100 cells/μL, n = 108 1.48 1.02-2.14 0.0377
Treatment arm R-chemo, n = 508 1.31 1.02-1.70 0.0369
Chemotherapy backbone
CHOP, n = 349 1.09 0.82-1.45 0.5590
CVP, n = 108 1.73 1.18-2.54 0.0047
FLIPI Low, n = 219 0.67 0.46-0.98 0.0389
Intermediate, n = 393 0.79 0.59-1.06 0.1167
Sex Male, n = 497 1.60 1.24-2.08 0.0004
Extranodal involvement
Yes, n = 698 1.46 1.09-1.96 0.0102
SPD, mm2b 1.00 1.00-1.00 0.0010
B
DLBCL, n = 850 HR 95% CIc P value
NKCC <100 cells/μL, n = 173 1.36 1.01-1.83 0.0416
Geographic region
Western Europe, n = 314 0.64 0.47-0.88 0.0060
Eastern Europe, n = 145 0.79 0.54-1.14 0.2051
North America, n = 143 0.63 0.42-0.96 0.0301
Other, n = 30 0.53 0.23-1.25 0.1455
IPI
Low, n = 165 0.37 0.24-0.56 <0.0001
Low-intermediate, n = 294 0.47 0.33-0.66 <0.0001
High-intermediate n = 255 0.62 0.44-0.86 0.0046
COO subtype GCB, n = 479 0.63 0.47-0.84 0.0017
Unclassified, n = 140 0.91 0.64-1.30 0.6113
SPD, mm2b 1.00 1.00-1.00 0.0057
Cancer Research. on November 10, 2020. © 2019 American Association forclincancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on May 3, 2019; DOI: 10.1158/1078-0432.CCR-18-3270

22
aThe reference variables used included: (GALLIUM) NKCC, ≥100 cells/μL; treatment arm, G-chemo; chemotherapy backbone, bendamustine; FLIPI, high; sex, female; extranodal involvement, no; (GOYA) NKCC, ≥100 cells/μL; geographic region, Asia; IPI, high; COO subtype, ABC; banalyzed as
continuous variable; cWald confidence interval.
ABC, activated B-cell like; Chemo, chemotherapy; CHOP, cyclophosphamide, doxorubicin, vincristine, and prednisone; CI, confidence interval; COO, cell-of-origin; CVP, cyclophosphamide, vincristine, and prednisone; DLBCL, diffuse large B-cell lymphoma; FL, follicular lymphoma; FLIPI, Follicular Lymphoma International Prognostic Index; G, obinutuzumab; GCB, germinal center B-cell like; HR, hazard ratio; IPI, International Prognostic Index; NKCC, natural killer cell count; PFS, progression-free survival; R, rituximab; SPD, sum of products of diameter of up to six target lesions.
Cancer Research. on November 10, 2020. © 2019 American Association forclincancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on May 3, 2019; DOI: 10.1158/1078-0432.CCR-18-3270

23
Table 3. Multivariate analysis of the association between baseline variables and OS in FL
(A) and DLBCL (B).a
A
FL, n = 1057 HR 95% CIc P value
NKCC <100 cells/μL, n = 108 2.20 1.26-3.86 0.0058
Chemotherapy backbone
CHOP, n = 349 0.41 0.23-0.73 0.0024
CVP, n = 108 0.68 0.29-1.58 0.3725
FLIPI Low, n = 219 0.31 0.14-0.69 0.0043
Intermediate, n = 393 0.56 0.33-0.93 0.0260
Sex Male, n = 497 2.13 1.34-3.40 0.0014
Extranodal involvement
Yes, n = 698 1.69 0.98-2.91 0.0587
SPD, mm2b 1.00 1.00-1.00 <0.0001
B
DLBCL, n = 850 HR 95% CIc P value
IPI
Low, n = 165 0.25 0.14-0.45 <0.0001
Low-intermediate, n = 294 0.41 0.27-0.62 <0.0001
High-intermediate n = 255 0.54 0.36-0.80 0.0024
Number of planned CHOP cycles
Eight, n = 235 1.81 1.32-2.49 0.0003
COO subtype GCB, n = 479 0.64 0.45-0.90 0.0115
Unclassified, n = 140 0.91 0.58-1.43 0.6904
SPD, mm2c 1.00 1.00-1.00 0.0031
aThe reference variables used included: (GALLIUM) NKCC, ≥100 cells/μL; chemotherapy backbone, bendamustine; FLIPI, high; sex, female; extranodal involvement, no; (GOYA) IPI, high; number of planned CHOP cycles, six; COO subtype, ABC; banalyzed as continuous variable; cWald confidence interval. ABC, activated B-cell like; CHOP, cyclophosphamide, doxorubicin, vincristine, and prednisone; CI, confidence interval; COO, cell-of-origin; CVP, cyclophosphamide, vincristine, and prednisone; DLBCL, diffuse large B-cell lymphoma; FL, follicular lymphoma; FLIPI, Follicular Lymphoma International Prognostic Index; GCB, germinal center B-cell like; HR, hazard ratio; IPI, International Prognostic Index; NKCC, natural killer cell count; OS, overall survival; SPD, sum of
products of diameter of up to six target lesions.
Cancer Research. on November 10, 2020. © 2019 American Association forclincancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on May 3, 2019; DOI: 10.1158/1078-0432.CCR-18-3270

24
Figure 1. Association of baseline peripheral blood NKCC with PFS (A) and OS (B) in FL and
DLBCL.
aMultivariate analysis adjusted for treatment arm, chemotherapy backbone, FLIPI-1, geographic region, sex, Ann Arbor stage, extranodal involvement, and SPD; bmultivariate analysis adjusted for treatment arm, number of planned CHOP cycles, IPI, geographic region, sex, bone marrow involvement, SPD, and COO. CHOP, cyclophosphamide, doxorubicin, vincristine, and prednisone; CI, confidence interval; COO, cell-of-origin; DLBCL, diffuse large B-cell lymphoma; FL, follicular lymphoma; FLIPI, Follicular Lymphoma International Prognostic Index; HR, hazard ratio; IPI, International Prognostic Index; NKCC, natural killer cell count; OS, overall survival; PFS, progression-free survival; SPD, sum of products of diameter of up to six target lesions.
Figure 2. Association of baseline peripheral blood NKCC with PFS (A) and OS (B) by COO.
aMultivariate analysis adjusted for treatment arm, number of planned CHOP cycles, IPI, geographic region, sex, bone marrow involvement, COO, and SPD. ABC, activated B-cell-like; CHOP, cyclophosphamide, doxorubicin, vincristine, and prednisone; CI, confidence interval; COO, cell-of-origin; GCB, germinal center B-cell-like; HR, hazard ratio; IPI, International Prognostic Index; NKCC, natural killer cell count; OS, overall survival; PFS, progression-free survival; SPD, sum of products of diameter of up to six target lesions.
Figure 3. Association of tumor NK cell gene expression and PFS in FL patients treated with
R-chemo and G-chemo (pooled data) (A), R-chemo (B), and G-chemo (C) and DLBCL
patients treated with R-CHOP and G-CHOP (pooled data) (D), R-CHOP (E), and G-CHOP
(F).
Median score was used to define high/low subgroups; amultivariate analysis adjusted for number of planned chemotherapy cycles, IPI, and geographic region. CI, confidence interval; chemo, chemotherapy; CHOP, cyclophosphamide, doxorubicin, vincristine, and prednisone; DLBCL, diffuse large B-cell lymphoma; FL, follicular lymphoma; HR, hazard ratio; NK, natural killer; PFS, progression-free survival.
Cancer Research. on November 10, 2020. © 2019 American Association forclincancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on May 3, 2019; DOI: 10.1158/1078-0432.CCR-18-3270

Cancer Research. on November 10, 2020. © 2019 American Association forclincancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on May 3, 2019; DOI: 10.1158/1078-0432.CCR-18-3270

Cancer Research. on November 10, 2020. © 2019 American Association forclincancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on May 3, 2019; DOI: 10.1158/1078-0432.CCR-18-3270

Cancer Research. on November 10, 2020. © 2019 American Association forclincancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on May 3, 2019; DOI: 10.1158/1078-0432.CCR-18-3270

Published OnlineFirst May 3, 2019.Clin Cancer Res Magdalena Klanova, Mikkel Z Oestergaard, Marek Trnený, et al. with immunochemotherapylymphoma and diffuse large B-cell lymphoma patients treated Prognostic impact of natural killer cell count in follicular
Updated version
10.1158/1078-0432.CCR-18-3270doi:
Access the most recent version of this article at:
Material
Supplementary
http://clincancerres.aacrjournals.org/content/suppl/2019/07/04/1078-0432.CCR-18-3270.DC1
Access the most recent supplemental material at:
Manuscript
Authorbeen edited. Author manuscripts have been peer reviewed and accepted for publication but have not yet
E-mail alerts related to this article or journal.Sign up to receive free email-alerts
Subscriptions
Reprints and
To order reprints of this article or to subscribe to the journal, contact the AACR Publications
Permissions
Rightslink site. Click on "Request Permissions" which will take you to the Copyright Clearance Center's (CCC)
.http://clincancerres.aacrjournals.org/content/early/2019/05/31/1078-0432.CCR-18-3270To request permission to re-use all or part of this article, use this link
Cancer Research. on November 10, 2020. © 2019 American Association forclincancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on May 3, 2019; DOI: 10.1158/1078-0432.CCR-18-3270