Embed Size (px)
Citation preview

PrognosisDoes Exercise Training Reduce
Adverse Events in Heart Failure?Jonathan Myers, PhDa,*, Clinton A. Brawner, PhDb,Mark J.F. Haykowsky, PhDc, Rod S. Taylor, PhDd,e
KEYWORDS
� Prognosis � Oxygen uptake � Aerobic capacity � Cardiac rehabilitation � Cardiac output
KEY POINTS
� Exercise training in patients with heart failure (HF) is associated with numerous physiologic benefits.
� The HF-ACTION (Heart Failure: A Controlled Trial Investigating Outcomes of Exercise Training) trialalong with systematic reviews and meta-analyses using the Cochrane database have greatlyenhanced our understanding of the outcome benefits associated with endurance exercise trainingin patients with HF.
� Recent studies demonstrate that the benefits of training are similar between men and womenwith HF.
INTRODUCTION
Exercise intolerance, frequently exhibited by fa-tigue or shortness of breath with a minimal degreeof exertion, is a hallmark of chronic heart failure(HF). Quantifying exercise intolerance has pro-found implications for the determination of dis-ability, quality of life (QOL), prognosis, and thecapacity to perform daily activities in patientswith HF. One of the principal goals of treatmentin HF is therefore to improve exercise capacity;therapies designed to improve exercise capacityin patients with HF are thus critical to improvingoutcomes. The pathophysiologic features of HFthat underlie reduced exercise tolerance havebeen the focus of numerous investigations forseveral decades.1,2 These features involve bothcentral (cardiac) and peripheral (skeletal muscleand vascular) abnormalities, including impaired
a Cardiology Division, Palo Alto VA Health Care System,Avenue, Palo Alto, CA 94304, USA; b Division of CardiovAvenue, Detroit, MI 48202, USA; c Alberta CardiovascularAlberta Heart Institute, University of Alberta, 3-16 CorbeSchool of Education, University of Exeter Medical SchoolUK; e National Institute of Public Health, University of SoDenmark* Corresponding author.E-mail address: [email protected]
Heart Failure Clin 11 (2015) 59–72http://dx.doi.org/10.1016/j.hfc.2014.08.0121551-7136/15/$ – see front matter Published by Elsevier In
cardiac output responses to exercise, abnormalredistribution of blood flow, reduced mitochondrialvolume and density, abnormal oxidative enzymeactivity, impaired vasodilatory capacity, height-ened systemic vascular resistance, and autonomicnervous system changes.1–4 Until the late 1980s,patients with HF were commonly excluded fromexercise programs because of concerns oversafety, whether training caused further harm toan already damaged myocardium, and questionsas to whether these patients could benefit fromexercise. These concerns have been allayed bynumerous studies performed over the last 25 yearsdocumenting that exercise training in stablepatients with HF is safe; that training causes nofurther damage to the myocardium; and thattraining is associated with numerous physiologic,musculoskeletal, and psychosocial benefits.1,4,5
Many studies preformed over the last 2 decades
Stanford University, Cardiology 111C, 3801 Mirandaascular Medicine, Henry Ford Hospital, 6525 Secondand Stroke Research Centre (ABACUS), Mazankowskitt Hall, Edmonton, AB T6G 2G4, Canada; d Graduate, Veysey Building, Salmon Pool Lane, Exeter EX2 4SG,uthern Denmark, Campusvej 55, DK-5230, Odense M,
c. heartfailure.th
eclinics.com
Myers et al60
have also demonstrated improved clinical out-comes following exercise training in HF, includingreductions in morbidity, mortality, and hospitaliza-tion, along with enhanced QOL.1,4,6,7 This articleprovides an overview of the benefits of exercisetraining in HF and the implications of these bene-fits for improving outcomes. The application ofrecent meta-analyses, novel observations on exer-cise training and outcomes among women, andrecent findings from the landmark HF-ACTION(Heart Failure: A Controlled Trial Investigating Out-comes of Exercise Training) trial are discussed.
MECHANISMS OF BENEFIT WITH EXERCISETRAINING AND IMPLICATIONS FORIMPROVING OUTCOMES
Potential mechanisms by which exercise trainingmay improve exercise capacity and reduce car-diac events in HF are outlined in Table 1; impor-tantly, the extent to which one or a combinationof these mechanisms may affect an individualpatient’s exercise tolerance varies considerably.Peak oxygen consumption (VO2) is strongly relatedto prognosis in patients with HF, and exercisetraining generally improves peak VO2 in the rangeof 10% to 25%1,4; however, even small changesin peak VO2 are associated with significantlyimproved outcomes.8 Numerous central and pe-ripheral factors influence peak VO2, but increasesin peak VO2 and related benefits from training arefundamentally related to the combination of animprovement in peak cardiac output, improvedvascular reactivity, better utilization of oxygen
Table 1Potential mechanisms by which exercise training imp
System Response to Training
Cardiac function � Increased cardiac output� Increase or no change in contr� Increased peak VO2
� Improved ventilatory efficienc
Regional bloodflow
� Increased vasodilatory capacity� Improved endothelial function� Improved redistribution of flo
Skeletal muscle � Increased aerobic enzymes� Increased mitochondrial volum� Increased capillary density� Decreased muscle receptor sen
Autonomicnervous system
� Decrease in plasma norepinep� Increased heart rate variability� Reduced chemoreceptor and esensitivity
� Reduced ventilatory response
Abbreviation: VO2, peak oxygen consumption.
through metabolic changes in the skeletal muscle,and more efficient ventilation. These mechanismsare outlined in the following section.
Central Adaptations
A general consensus exists that the benefits ofexercise training in patients with HF are causedlargely by adaptations in the peripheral vascula-ture and skeletal muscle rather than the heartitself.4,9 Although the focus of these studies hasbeen on patients with HF and reduced ejectionfraction (HFrEF), this also seems to be the caseamong patients with HF and preserved EF(HFpEF).10 This consensus evolved in part be-cause of the recognition that EF is poorly cor-related with exercise capacity.1,3,4 However,although the preponderance of studies havereported that EF and other measures of contrac-tility show minimal change following training,several studies have reported significant improve-ments in these indices.11–14 Most of these studieshave focused on resting EF, and less is knownregarding indices of contractility during exercise.Because of the difficulty measuring cardiac outputdirectly, it has not been widely reported; butstudies using thermodilution techniques havereported increases in maximal cardiac outputfollowing training in the range of 5% to 20%.15 Ameta-analysis of 104 patients reported a meanincrease in maximal cardiac output of 2.5 L/min,corresponding to a 21% increase.9 Whether thisincrease in cardiac output is a result of increasesin maximal heart rate or stroke volume is unclear;
roves outcomes
Effect on Outcomes
actility
y
� Increased exercise capacity� Improved QOL� Reduced mortality� Reduced hospitalizations
w
� Increased exercise capacity
e and density
sitivity
� Increased exercise capacity� Improved physical function� Reduced ventilatory response� Reduced mortality
hrine
rgoreceptor
� Reduced cardiac rhythmdisturbances
� Reduced or no change inmortality
Exercise Training and Adverse Events in Heart Failure 61
studies have reported small improvements in bothindices as well as no change.15 When changesin maximal cardiac output do occur, they havebeen attributed to some combination of smallchanges in peak heart rate, stroke volume, andafterload reduction (caused by enhancedendothelial-dependent vasodilation).1,13,15,16
Vascular Adaptations
Numerous recent studies have characterizedabnormal endothelial function in HF, and favor-able adaptations in endothelial function havebeen consistently reported after rehabilitationprograms.1,2,13,17,18 Exercise training decreasescirculating catecholamine levels in patients withHF, has antiinflammatory and antioxidative effects,reduces natriuretic peptide concentrations, andincreases shear stress and nitric oxide bioavail-ability,18–22 all leading to reduced peripheral vaso-constriction, improved endothelial function, andenhanced endothelial repair.16,17,23,24 These ad-aptations result in better skeletal muscle perfusionduring exercise. There have been dozens of suchstudies over the last 2 decades, and the volumeof work by Hambrecht and colleagues24 is partic-ularly notable. They reported that a regimen usinghandgrip exercise training 6 times per day signifi-cantly improved endothelial-dependent vasodila-tion after 4 weeks in patients with HF; the effectsof training were similar to those of the potentvasodilator L-arginine. Circulating progenitor cells,which have the ability to differentiate and ex-hibit endothelial properties and enhance endo-thelial function, increase following training inHF.16,19,24,25 Numerous studies have reportedthat changes in endothelium-dependent periph-eral blood flow after training are paralleled byimprovements in peak VO2.
25–27
Skeletal Muscle Adaptations
Metabolic changes in the skeletal muscle withaerobic training include increases in aerobic en-zymes, increases in mitochondrial size and den-sity, and increases in capillary density.1,2,4,17–21
Muscle biopsy studies have demonstrated shiftsfrom type II to type I muscle fibers after training.28
Cytochrome c oxidase–positive mitochondria, animportant rate-limiting enzyme in oxidative phos-phorylation, was demonstrated to increase 41%after 6 months of training.29 31P MRI spectroscopyhas been used to document abnormalities in skel-etal muscle metabolism in HF, including earlyintracellular acidification, accumulation of inor-ganic phosphate (Pi), accelerated utilization ofphosphocreatine (PCr), and delayed PCr duringrecovery from exercise.30–34 Exercise training has
been demonstrated to partially reverse theseabnormalities in oxidative metabolism measuredby MRI and near-infrared spectroscopy tech-niques, including a slower increase in Pi, a declinein phosphocreatine, a decrease in Pi/creatinephosphate (CP) versus power output, and fasterrecovery of O2 stores after exercise.35,36 Regularexercise also reduces muscle wasting and helpsrestore the anabolic/catabolic imbalance that iscommon in HF.37,38
Ventilatory Adaptations
Ventilatory inefficiency has been demonstrated tobe strongly associatedwithmorbidity andmortalityin HF; in fact, studies performed over the last15 years have shown that markers of ventilatoryinefficiency, such as the minute ventilation/carbondioxide production (VE/VCO2) slope and oxygen up-take efficiency slope (OUES), are more powerfulpredictors of risk for adverse outcomes thanmany clinical and cardiopulmonary exercise testresponses in HF.39 Application of these indicesfor the identification of high-risk patients has beenrecommended in recent guidelines on the evalua-tion and management of HF40; the influence oftraining on these indices is, therefore, importantto document. Excessive ventilation in patientswithHFhasbeen associatedwith ventilation/perfu-sion mismatching caused by impaired cardiacoutput responses to exercise, early lactate accu-mulation (which stimulates ventilation through thebuffering of lactate), and chemoreceptor and mus-cle receptor hyperactivity.39–41 Improvements inabnormal ventilation after training involves somecombination of hemodynamic changes (reducedpulmonary pressures or improved ventilation-perfusion mismatching), metabolic changes re-flected by a delay in lactate accumulation, achange in ventilatory control, and a change in theventilatory pattern that makes breathing more effi-cient. Recent studies have reported that theseindices respond favorably to training.42,43 In addi-tion, a growing number of studies have demon-strated that specific training of the respiratorymuscles results in improved ventilatory dynamicsand exercise performance.44,45 Improvement inthe ventilatory response to exercise is a criticallyimportant mechanism underlying the enhancedfunctional capabilities and outcomes followingtraining in patients with HF.
Studies have also identified a pathophysiologicmechanism unique to HF that underlies abnormalventilation and that responds favorably to training.This mechanism involves specific ventilatory sig-nals arising from the exercising muscle, whichare abnormally enhanced in HF (termed an

Myers et al62
ergoreflex contribution to ventilation).46,47 Thesesignals have been demonstrated to contribute tothe abnormal hemodynamic, autonomic, and ven-tilatory responses to exercise that characterizeHF. Afferent fibers present in skeletal muscle (er-goreceptors) are sensitive to metabolic changesthat occur during muscular work. These receptorsseem to mediate circulatory adaptations occurringin the early stages of exercise, are stimulated bymetabolic acidosis, and are partially responsiblefor sympathetic vasoconstriction.46–48 It has alsobeen demonstrated that hypoxic chemosensitivityis increased in HF and that this heightened chemo-sensitivity is correlated with the VE/VCO2 slope.The results of these enhanced ergoreflex andchemoreceptor responses are hyperventilationand heightened sympathetic outflow, which causean increase in peripheral resistance and, thus, adecrease in muscle perfusion. These musclereceptors are less sensitive to stimulation aftertraining; it has been demonstrated that after a6-week forearm training protocol, the ergoreflexcontribution to exercise ventilation was reducedby 58%.48 These salutary effects on ventilatorycontrol are an additional mechanism by which out-comes are improved with regular exercise in HF.
EXERCISE TRAINING AND OUTCOMES INHEART FAILURE
By 2004, there had been more than 80 publishedtrials (30 randomized controlled trials [RCTs]) ofexercise training in patients with HFrEF.49 Basedon a meta-analysis of these studies, exercisetraining in patients with HFrEF seemed to be safeand effective.49 In spite of this, adoption of exer-cise training for these patients in clinical practicewas slow because of the limited sample size ofthese trials, the lack of data from a large multi-center trial, and limited data on safety. As a result,in the United States, although cardiac rehabilita-tion (CR) was a covered benefit for beneficiariesof Medicare and many private health insurancesfor several heart disease–related diagnoses (eg,acute myocardial infarction, valve disease, cardiactransplant), HFrEFwas not a CR-eligible diagnosis.
Implications from Heart Failure: A ControlledTrial Investigating Outcomes of ExerciseTraining (HF-ACTION)
To address this gap, HF-ACTION was designedand funded by the US National Heart, Lung, andBlood Institute (NHLBI). Investigators randomizedpatients with HFrEF (EF <35%, New York HeartAssociation [NYHA] class II–IV) to endurance exer-cise training or usual care.50 Patients randomizedto exercise participated in 3 months of supervised
exercise training (3 days per week), with exerciseintensity prescribed at 60% to 70% of themeasured heart rate reserve. Patients were transi-tioned from supervised exercise to 5 days perweek of home-based exercise training. Thesepatients were provided a heart rate monitor toguide exercise intensity and a leg ergometer ortreadmill for their home. Patients in the usual-care group were provided secondary preventioneducation, including information on the impor-tance of regular physical activity. Both groupswere contacted every 2 to 4 weeks. The primaryoutcome was a composite end point of incidentall-cause mortality or all-cause hospitalization.The study was designed to detect an 11% reduc-tion in this end point at 2 years based on enroll-ment of 3000 subjects.50
Although the study was designed to enroll3000 subjects, a planned interim analysis revealedthat, because of a higher-than-expected eventrate, 2300 subjects would be sufficient to evaluatethe primary outcome.50 In the end, between2003 and 2007, HF-ACTION investigators ran-domized 2331 patients (median age 5 59 years,27%–30% women) with HFrEF from 82 sites inthe United States, Canada, and France. In anintent-to-treat analysis, exercise training wasassociated with an 11% lower adjusted risk(hazard ratio [HR] 0.89; 95% confidence interval[CI] 0.81, 0.99) for incident all-cause mortality/hospitalization and a 15% lower adjusted risk(HR 0.85; 95% CI 0.74, 0.99) for incidentcardiovascular-related mortality or HF hospitaliza-tion. This effect was seen in spite of significantcrossover between groups. Only 30% of the pa-tients in the exercise group achieved the goal of120 minutes per week of exercise, and 22% to28% of the patients in the usual-care groupself-reported regular exercise participation.50
In a planned secondary analysis, Keteyian andcolleagues51 examined the dose-response rela-tionship between the volumeof exerciseperformedand clinical outcomes among patients randomizedto the exercise group inHF-ACTION. They reporteda reverse J-shaped relationship between the vol-ume of exercise performed (ie, product of exercisetime and workload expressed in metabolic equiva-lents [METs]) and adjusted risk for all-causemortal-ity/hospitalization aswell as cardiovascular-relatedmortality or HF hospitalization. The lowest risk forboth outcomes was observed among patientswho performed 3 to 5 MET-hours per week and 5to 7 MET-hours per week of exercise comparedwith patients who did not exercise (ie, 0 to 1 MET-hours per week of exercise).51
In spite of the lower risk for clinical eventsobserved among patients in the exercise group

Exercise Training and Adverse Events in Heart Failure 63
compared with the control group of HF-ACTION,patients in the exercise group showed only amild improvement in exercise capacity. On av-erage, peak VO2 increased just 0.6 mL/kg/min at3 months after randomization (P<.001, comparedwith change in control group).50 Swank and col-leagues8 evaluated whether the change in peakVO2 at 3 months was associated with a lower riskfor mortality/hospitalization, regardless of groupassignment. Among patients who were eventfree through 3 months after randomization, every6% (eg, w1 mL/kg/min) increase in peak VO2 at3 months was associated with a 5% loweradjusted risk (HR 5 0.95; 95% CI 0.93, 0.98) forall-cause mortality/hospitalization, a 4% loweradjusted risk (HR 5 0.96; 95% CI 0.94, 0.99)for cardiovascular-related mortality/hospitaliza-tion, and a 7% lower adjusted risk (HR 5 0.93;95% CI 0.90, 0.97) for all-cause mortality.8
In another analysis of data from the HF-ACTIONtrial, Reed and colleagues52 evaluated the cost-effectiveness of the exercise training interventionas it was applied in the trial. Consistent with othereconomic evaluations of health care interventions,the investigators considered all patient-level directcosts, including the patients’ time to travel to andfrom the exercise facility and to perform the exer-cise (center or home based), and staff time toperform follow-up phone calls intended to pro-mote adherence. Importantly, this was a cost anal-ysis of the intervention delivered in the HF-ACTIONtrial, which was more comprehensive than atypical CR program. Reed and colleagues52 useda patient-to-staff ratio of 1.7 in the analysis. Thisratio contrasts with the recommended ratio of upto 5 patients per staff member in CR programs.53
According to the investigators,52 with the excep-tion of the patients’ time, the cost of the exerciseintervention was considered relatively low for thehealth care system. The total health care costduring follow-up was not significantly different be-tween the exercise and control groups, and therewas no consistent difference in medical resourceutilization. The investigators concluded that costmay be improved if these patients are incor-porated into a standard CR program wherebypatient-to-staff ratios are more efficient. The inves-tigators concluded that intervention costs may bereduced if patients were incorporated into a morestandard CR program whereby patient-to-staffratios are more efficient than in the trial.
With a final enrollment of 2331 patients54 and atotal cost exceeding $37.5 million,55 HF-ACTIONwas the largest and most expensive trial of exer-cise training to be funded by the US National Insti-tutes of Health. Results from the HF-ACTIONtrial confirmed the safety and clinical benefit of
moderate-intensity cardiorespiratory exercisetraining for patients with HFrEF. These data werehelpful in persuading the US Centers for Medicareand Medicaid to approve coverage of phase 2 CRfor Medicare beneficiaries with HFrEF beginning in2014. In addition, as stated by Michael Lauer, MD(director of the Division of Cardiovascular Sci-ences at the NHLBI), HF-ACTION investigatorsdemonstrated that large, multisite, end-pointdriven behavioral trials (such as exercise training)can be successfully conducted (comments fol-lowing the initial presentation of the primary resultsduring the HF-ACTION investigators meeting inconjunction with the 2008 American Heart Associ-ation Scientific Sessions).
EXERCISE TRAINING AND OUTCOMES INWOMEN WITH HEART FAILUREImpaired Exercise Tolerance in Women withHeart Failure
Women with HF have reduced exercise tolerance,measured objectively as decreased peak VO2 anddistance walked in 6 minutes (6MWD).56 Data fromthe HF-ACTION trial revealed that the baselinepeak VO2 and 6MWD were 10% and 7% lower,respectively, in clinically stable women (n 5 661)compared with men (n 5 1670) with HFrEF.56,57
Scott and associates58 extended these findingsto patients with HFpEF and reported that peakVO2 was 16% lower in women compared withmen.58 Given that peak VO2 is inversely associatedwith all-cause death in men and women,59,60 aconsequence of the impaired exercise toleranceis that women with HF may have reduced survivalcompared with men with similar health status andventricular function. Moreover, peak VO2 in womenwith HF is less than the minimal threshold levelrequired for full and independent living.61 Accord-ingly, therapies that improve exercise tolerancemay be especially relevant to maintaining func-tional independence and improving survival inwomen with HF.
Exercise Training and Improvement in ExerciseTolerance and Quality of Life in Women withHeart Failure
Women with HF have been underrepresented inexercise intervention trials.57,61 Indeed, to date,only 4 RCTs have examined the efficacy of exer-cise training on health-related outcomes in womenwith HF (total sample size, n 5 84).62–65
Tyni-Lenne and colleagues64 performed the firstrandomized cross-over trial comparing 8 weeks ofknee extensor exercise training (3 days per weekat 65%–75% peak power output � 15 minutes)versus an 8-week control (no training) period on

Myers et al64
peak VO2, 6MWD, skeletal muscle metaboliccapacity, and QOL in 16 women with clinicallystable HFrEF (mean age 5 62 years). Comparedwith control subjects, 8 weeks of exercise trainingsignificantly increased peak VO2, 6MWD, quadri-ceps muscle citrate synthase, lactate dehydroge-nase, along with physical and psychosocial QOL.Pu and colleagues63 compared 10 weeks of
high-intensity upper and lower extremity strengthtraining (3 sets � 8 repetitions at 82% maximalstrength) versus low-intensity stretching on peak6MWD, peak VO2, muscle strength and endurance,skeletal muscle mass and morphology, and car-diac function in 16 older women (mean age 577 years) with HFrEF. No adverse events werefound with the strength-training program; thismode of training was associated with a significantincrease in 6MWD, lower extremity maximalstrength, and endurance compared with controls.No significant difference was found for peak VO2,skeletal muscle fiber distribution or oxidativecapacity, or global systolic or diastolic function.In addition, it seemed that the improved aerobicendurance was mediated by favorable skeletalmuscle adaptations because the increase invastus lateralis type I (oxidative) fiber area and cit-rate synthase activity were positively related to theincrease in 6WMD.Haykowsky and colleagues62 examined the
effects of 6 months (3 months supervised followedby 3 months unsupervised) aerobic and strengthtraining (n 5 10) versus aerobic training alone(n 5 10) on peak VO2, muscle strength, and QOLin older women with HFrEF (mean age5 72 years).Supervised (cycle) training was performed 2 daysper week at 60% to 70% of the heart rate reserve,whereas unsupervised (walking) training was per-formed 2 days per week at a rate of perceivedexertion between 12 and 14. The combined groupalso performed 1 to 2 sets of supervised upper andlower extremity strength training at 50% to 70% ofmaximal strength and unsupervised upper andlower extremity strength training using handheldand leg weights.62 The main finding of this studywas that 3 months of supervised aerobic or com-bined aerobic and strength training increasedpeak VO2 and leg press maximal strength thatwas not maintained with unsupervised training.62
No significant change was found in QOL afterexercise training.Gary and colleagues65 performed the first
exercise RCT in women with HFpEF (meanage 5 68 years; mean EF 5 55%). Subjects wererandomly assigned to 12 weeks of unsupervisedexercise (walking 3 days per week at 40%–60%peak heart rate) plus an education program (HFdisease management and women’s health) versus
an education program alone. The primary out-comes were 6MWD and QOL. The investigatorsreported that the intervention group had a signifi-cantly greater improvement in 6MWD and QOLcompared with the control group after 12 weeks.Although there has been a relative paucity of
studies in women, taken together, these findingssuggest that supervised aerobic training is an ef-fective therapy to improve peak VO2, 6MWD, andQOL, whereas supervised strength training per-formedaloneor incombinationwithaerobic trainingimproves muscle strength in women with HF.
Exercise Training, All-Cause Mortality, andHospitalization in Women with Heart Failure
Pina and colleagues57 recently reported findingsfrom an exploratory analysis on the effects ofexercise training on peak VO2 and a combinedend point of all-cause mortality and hospital stayin women (exercise group, n 5 290; usual caregroup, n 5 229) and men (exercise group, n 5682; usual care group, n 5 668) from the HF-ACTION trial. Despite adherence to endurancetraining being higher among men (45% of menmaintained a goal of 90 minutes of exercise perweek vs 37% of women), the mean difference be-tween exercise and usual-care participants wassimilar in men (0.5 mL/kg/min, 95% CI 0.22–0.79)and women (0.73 mL/kg/min, 95% CI 0.27–1.19)after 3 months of training. Endurance trainingwas also associated with a 26% reduction in thecombined end point in women, whereas therewas no decrease in men (estimated effect inwomen: 0.74 95% CI 0.59–0.92; estimated effectin men: 0.99 95%CI 0.86–1.13; P value for interac-tion 5 .027). Accordingly, the findings from thissubanalysis provide proof of concept that theendurance training–mediated increase in peakVO2 may be associated with favorable improve-ments in all-cause mortality and hospitalization inwomen with HF. Despite this potential benefit, alimitation of the HF-ACTION trial is that the medianage of participants was lower than the age at firstdiagnosis of HF in population-based studies(59 years vs �70 years, respectively).66–68
Summary and Future Directions
Women with either HFpEF or HFrEF have severelyreduced peak VO2. The mechanisms responsiblefor the reduced peak VO2 in women with HF havenot been studied extensively; however, it is likelycaused by impaired cardiac, vascular, and skeletalmuscle function that result in reduced convectiveor diffusive O2 transport and/or by abnormalitiesin oxygen utilization by the active muscles. Regularaerobic training improves peak VO2 and 6MWD in
Table 2Selected characteristics of the 33 trials in theCochrane meta-analysis
CharacteristicNumber (%) orMedian (Range)
Exercise-only CR 10 (30)
Setting
Center based 14 (43)
Home based 5 (15)
Both 13 (39)
Unspecified 1 (3)
Sample size 52 (19–2331)
Publication date
1990–99 5 (15)
Exercise Training and Adverse Events in Heart Failure 65
women with HF. Moreover, strength training aloneor in combination with aerobic training improvesmaximal muscular strength in women with HFrEF.The mechanisms responsible for the improvementin exercise tolerance have not been well studied,but the limited data to date suggest that theymay be related to favorable changes in skeletalmuscle oxidative capacity.63,64 Finally, theincreased peak VO2 in women with HFrEF withshort-term training may be associated with agreater reduction in all-cause mortality and hospi-tal stay than men with similar health status andventricular function. Future prospective trials arerequired to determine whether the increase inpeak VO2 is associated with favorable improve-ments in survival and hospitalization in olderwomen with HF.
2000–09 22 (66)
2010 or later 6 (18)
Single center 30 (91)
Study location
Europe 20 (60)
North Americaa 11 (33)
Other 2 (6)
Sex
Men only 12 (36)
Women only 0 (0)
Both 20 (61)
Unspecified 1 (3)
Age (years) 60.5 (51–81)
Diagnosis
HFrEF only 29 (88)
HFpEF only 0 (0)
Both 4 (12)
Left ventricular EF (%) 29 (21–41)
Included NYHA IV 6 (18)
NYHA class unspecified 4 (12)
a HF-ACTION trial also included 6 French centers (out of82 centers).
Data from Taylor RS, Sagar VA, Davies EJ, et al. Exercise-based rehabilitation for heart failure. Cochrane DatabaseSyst Rev 2014;4:CD003331. http://dx.doi.org/10.1002/14651858.CD003331.pub4.
META-ANALYSES OF EXERCISE TRAININGAND OUTCOMES IN HEART FAILURE: THE2014 COCHRANE REVIEW
The latest update of the Cochrane systematicreview and meta-analysis of RCTs of exercise-based CR for HF was published in April2014.69,70 In brief, the methods of this reviewwere as follows: MEDLINE, EMBASE, and theCochrane Library were searched up to January2013 for RCTs that included adults (�18 years)with HFpEF or HFrEF and reported follow-upfor 6 months or more after randomization; furthertrials were retrieved through a manual search ofreferences including studies and recent reviews;there was no language restriction; trials werepooled when possible using either fixed or randomeffects meta-analysis.
This review included 33 RCTs in a total of 4740patients predominantly with HFrEF and NYHAclass II to III (Table 2). Most trials were small(<100 participants) and single center (30 trials),with the HF-ACTION trial2,3 contributing approxi-mately 50% (2331 participants) of all included pa-tients. The mean age of patients across the trialsranged from 51 to 81 years. Although there wasevidence of more women recruited in recent trials,most patients were predominantly men (median87%). Eleven trials reported follow-up in excessof 12 months. All trials evaluated a cardiorespira-tory exercise training intervention, and 11 alsoincluded resistance training. Exercise trainingwas most commonly delivered in either an exclu-sively center-based setting or a center-based set-ting in combination with some home exercisesessions. A small number of studies (N 5 5) wereconducted in an exclusively home-based setting.The dose of exercise training ranged widely ac-ross studies, with session durations of 15 to
120 minutes, 1 to 7 sessions per week, intensityof 40% to 80% of maximal heart rate (or equivalentof 50%–85% of peak VO2 or Borg rating of 12–18),delivered over 15 to 120 weeks. The main out-comes of the Cochrane review are summarizedin the following section.
Mortality
There was no significant difference in pooledmortality up to 12 months follow-up between
Myers et al66
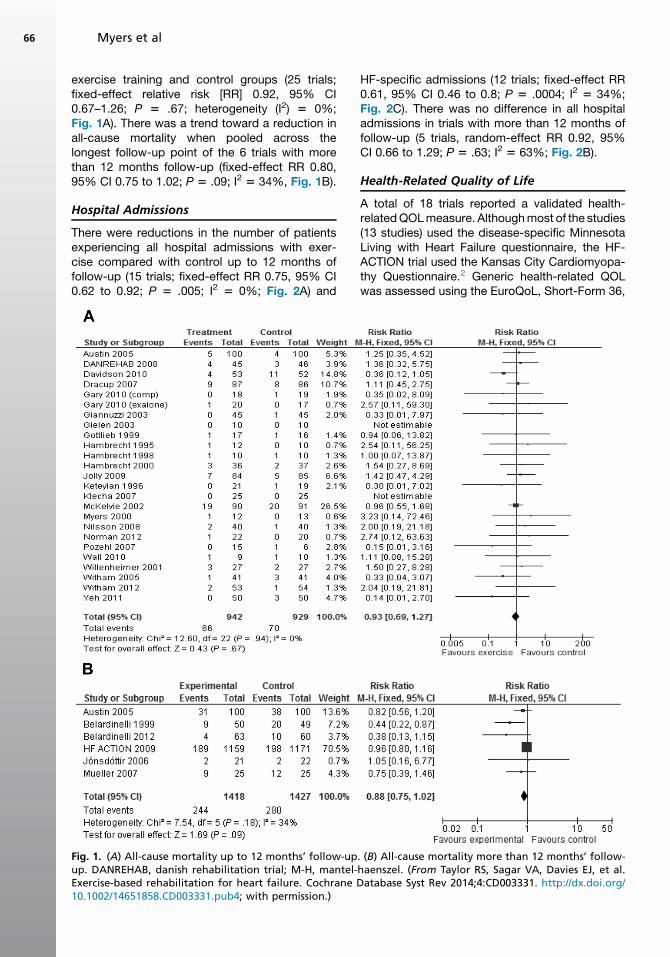
exercise training and control groups (25 trials;fixed-effect relative risk [RR] 0.92, 95% CI0.67–1.26; P 5 .67; heterogeneity (I2) 5 0%;Fig. 1A). There was a trend toward a reduction inall-cause mortality when pooled across thelongest follow-up point of the 6 trials with morethan 12 months follow-up (fixed-effect RR 0.80,95% CI 0.75 to 1.02; P 5 .09; I2 5 34%, Fig. 1B).
Hospital Admissions
There were reductions in the number of patientsexperiencing all hospital admissions with exer-cise compared with control up to 12 months offollow-up (15 trials; fixed-effect RR 0.75, 95% CI0.62 to 0.92; P 5 .005; I2 5 0%; Fig. 2A) and
Fig. 1. (A) All-cause mortality up to 12 months’ follow-upup. DANREHAB, danish rehabilitation trial; M-H, mantel-Exercise-based rehabilitation for heart failure. Cochrane D10.1002/14651858.CD003331.pub4; with permission.)
HF-specific admissions (12 trials; fixed-effect RR0.61, 95% CI 0.46 to 0.8; P 5 .0004; I2 5 34%;Fig. 2C). There was no difference in all hospitaladmissions in trials with more than 12 months offollow-up (5 trials, random-effect RR 0.92, 95%CI 0.66 to 1.29; P 5 .63; I2 5 63%; Fig. 2B).
Health-Related Quality of Life
A total of 18 trials reported a validated health-relatedQOLmeasure. Althoughmost of the studies(13 studies) used the disease-specific MinnesotaLiving with Heart Failure questionnaire, the HF-ACTION trial used the Kansas City Cardiomyopa-thy Questionnaire.2 Generic health-related QOLwas assessed using the EuroQoL, Short-Form 36,
. (B) All-cause mortality more than 12 months’ follow-haenszel. (From Taylor RS, Sagar VA, Davies EJ, et al.atabase Syst Rev 2014;4:CD003331. http://dx.doi.org/
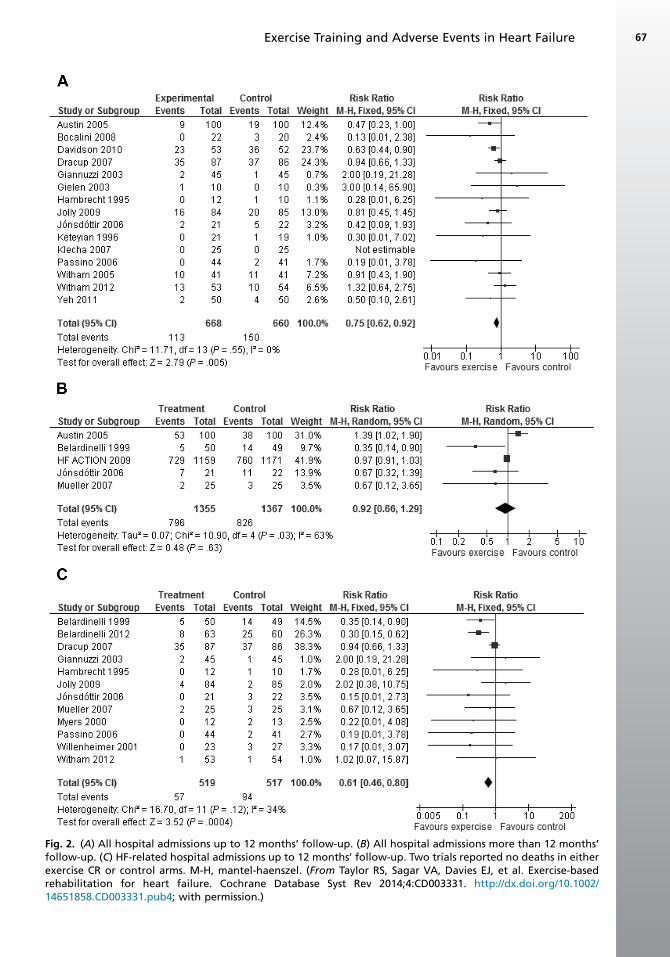
Fig. 2. (A) All hospital admissions up to 12 months’ follow-up. (B) All hospital admissions more than 12 months’follow-up. (C) HF-related hospital admissions up to 12 months’ follow-up. Two trials reported no deaths in eitherexercise CR or control arms. M-H, mantel-haenszel. (From Taylor RS, Sagar VA, Davies EJ, et al. Exercise-basedrehabilitation for heart failure. Cochrane Database Syst Rev 2014;4:CD003331. http://dx.doi.org/10.1002/14651858.CD003331.pub4; with permission.)
Exercise Training and Adverse Events in Heart Failure 67
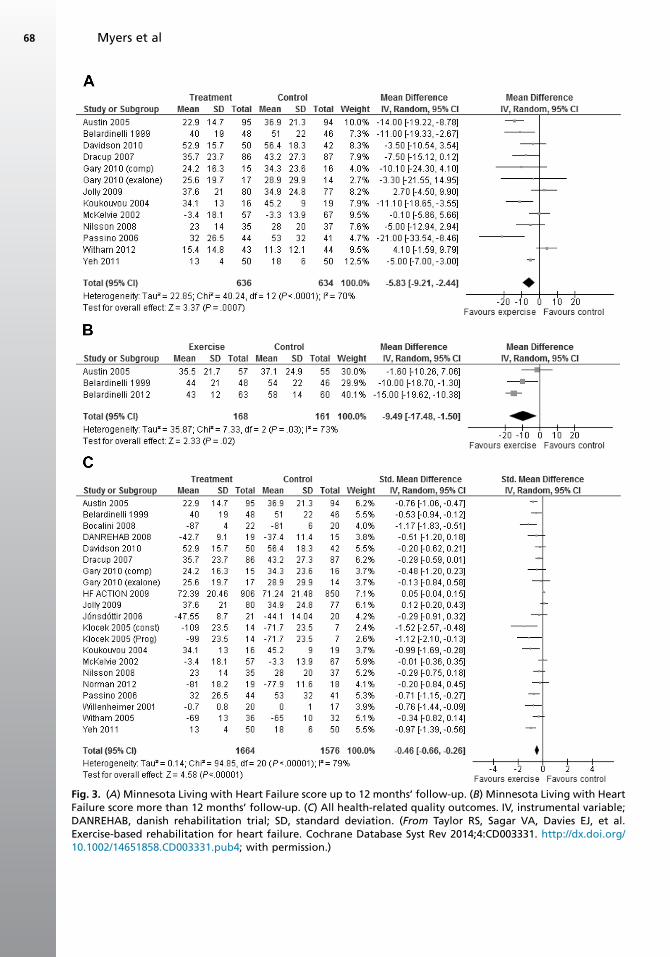
Fig. 3. (A) Minnesota Living with Heart Failure score up to 12 months’ follow-up. (B) Minnesota Living with HeartFailure score more than 12 months’ follow-up. (C) All health-related quality outcomes. IV, instrumental variable;DANREHAB, danish rehabilitation trial; SD, standard deviation. (From Taylor RS, Sagar VA, Davies EJ, et al.Exercise-based rehabilitation for heart failure. Cochrane Database Syst Rev 2014;4:CD003331. http://dx.doi.org/10.1002/14651858.CD003331.pub4; with permission.)
Myers et al68
Exercise Training and Adverse Events in Heart Failure 69
Psychological General Wellbeing index, Patient’sGlobal Assessment of QOL, and Spritzer’s QOLIndex. Across the studies reporting the total Min-nesota Living with Heart Failure questionnairescore up to 12 months of follow-up, there was evi-dence of a clinically important improvement withexercise (random-effects weighted mean differ-ence (WMD) �5.8, 95% CI �9.2 to �2.4; P 5.0007; I2 5 70%; Fig. 3A). This benefit was alsoseen in the 3 trials that reported follow-up of morethan 12 months (random-effect WMD �9.5, 95%CI �17.5 to �1.5; P 5 .022; I2 5 73%; Fig. 3B).Pooling across all studies, regardless of theoutcome measure used, showed a significantimprovement inQOLwith exercise (random-effectsstandardized mean difference [SMD] �0.46, 95%CI �0.66 to �0.26; P<.0001; I2 5 79%; Fig. 3C).
SUMMARY
Regular exercise training reduces adverse eventsin patients with either HFrEF or HFpEF. Studiesperformed over the last 3 decades have providedextensive insights into both the health outcomebenefits of exercise training and the physiologicmechanisms underlying these benefits. Physio-logic adaptations that occur following exercisetraining involve both central and peripheral mech-anisms that include increases in peak cardiacoutput, improved vascular reactivity, better utiliza-tion of oxygen through metabolic changes in theskeletal muscle, changes in autonomic function,and more efficient ventilation.
Although women have been underrepresented inprevious studies, the available data indicate thatwomen generally achieve physiologic benefits fromexercise training to an extent that is similar to men.Using the combined end point of mortality andhospitalization, some evidence exists that womenmay even derive outcome benefits from CR thatare greater than those of men.57 The landmarkHF-ACTION trial has had a major impact on ourunderstanding of the effects of endurance exercisetraining on health outcomes in patients with HF.This knowledge has provided insight not only intothe benefits of CR in HF but has also provided aclearer understanding of the dose-response rela-tionship between the volume of exercise performedand clinical outcomes, the cost-effectiveness oftraining in HF, and the difficulties associated withconducting such a large and ambitious multicentertrial. The results of HF-ACTION have had an impor-tant impact on the recent approval of coverage forCR for patients with HFrEF by US Centers for Medi-care and Medicaid.
Systematic reviews and meta-analyses usingthe Cochrane database have provided level 1
evidence (evidence obtained from properly de-signed RCTs) that exercise-based rehabilitationis associated with important reductions in hospi-talization and improvements in health-relatedQOL of participants with HF. Moreover, these ben-efits seem to be consistent across patients regard-less of age, sex, disease severity, and CR programcharacteristics (exercise only vs comprehensiveCR). Exercise interventions seem to be safe for pa-tients with HF with no increased mortality in theshort-term, and there is some evidence supportingreductions in mortality in the longer-term (>12months of follow-up). Although more recent trialshave recruited patients with HFpEF and NHYAclass IV and include a greater proportion of womenand older patients, these groups remain underrep-resented and need to be the focus of future clinicaltrials. Future trials also need to evaluate interven-tions to enhance the long-term maintenance ofexercise-based CR for HF and the outcomes,costs, and cost-effectiveness of programs deliv-ered exclusively in a home-based setting.
REFERENCES
1. Downing J, Balady GJ. The role of exercise
training in heart failure. J Am Coll Cardiol 2011;
58:561–9.
2. Piepoli MF, Guazzi M, Boriani G, et al. Exercise intol-
erance in chronic heart failure: mechanisms and
therapies. Part 1. Eur J Cardiovasc Prev Rehabil
2010;17:637–42.
3. Myers J, Froelicher VF. Hemodynamic determi-
nants of exercise capacity in chronic heart failure.
Ann Intern Med 1991;115:377–86.
4. Pina IL, Apstein CS, Balady GJ, et al. Exercise and
heart failure: a statement from the American Heart
Association Committee on exercise, rehabilitation,
and prevention. Circulation 2003;107:1210–25.
5. Haykowsky M, Scott J, Esch B, et al. A meta-anal-
ysis of the efforts of exercise training on left ventric-
ular remodeling following myocardial infarction:
start early and go longer for greatest exercise
benefits on remodeling. Trials 2011;12:92.
6. Davies EJ, Moxham T, Rees K, et al. Exercise
training for systolic heart failure: Cochrane system-
atic review and meta-analysis. Eur J Heart Fail
2010;12:706–15.
7. Davies EJ, Moxham T, Rees K, et al. Exercise
based rehabilitation for heart failure. Cochrane
Database Syst Rev 2010;(4):CD003331.
8. Swank AM, Horton J, Fleg JL, et al. Modest in-
crease in peak VO2 is related to better clinical
outcomes in chronic heart failure patients: results
from heart failure and a controlled trial to investi-
gate outcomes of exercise training (HF-ACTION).
Circulation 2012;5:579–85.
Myers et al70
9. Van Tol BA, Huijsmans RJ, Droon DW, et al. Effects
of exercise training on cardiac performance, exer-
cise capacity and quality of life in patients with
heart failure: a meta-analysis. Eur J Heart Fail
2006;8:841–50.
10. Haykowsky MJ, Brubaker PH, Stewart KP, et al.
Effect of endurance training on the determinants
of peak exercise oxygen consumption in elderly
patients with stable compensated heart failure
and preserved ejection fraction. J Am Coll Cardiol
2012;60:120–8.
11. Wisloff U, Stoylen A, Leonnenchen JP, et al. Supe-
rior cardiovascular effect of aerobic interval training
versus moderate continuous training in heart failure
patients: a randomized study. Circulation 2007;
115:3086–94.
12. Giannuzzi P, Temporelli PL, Corra U, et al, ELVD-
CHF Study Group. Antiremodeling effect of long-
term exercise training in patients with stable
chronic heart failure: results of the Exercise in
Left Ventricular Dysfunction and Chronic Heart
Failure (ELVD-CHF) trial. Circulation 2003;108:
557–9.
13. Hambrecht R, Gielen S, Linke A, et al. Effects of
exercise training on left ventricular function and
peripheral resistance in patients with chronic
heart failure: a randomized trial. JAMA 2000;
283:3095–101.
14. Erbs S, Linke A, Gielen S, et al. Exercise training in
patients with severe chronic heart failure: impact
on left ventricular performance and cardiac size.
A retrospective analysis of the Leipzig Heart Failure
Training Trial. Eur J Cardiovasc Prev Rehabil 2003;
10:336–44.
15. Mezzani A, Corra U, Gianuzzi P. Central adapta-
tions to exercise training in patients with chronic
heart failure. Heart Fail Rev 2008;13:13–20.
16. Erbs S, Hollriegel R, Linke A, et al. Exercise training
in patients with advanced chronic heart failure
(NYHA IIIb) promotes restoration of peripheral
vasomotor function, induction of endogenous
regeneration, and improvement of left ventricular
function. Circ Heart Fail 2010;3:486–94.
17. Duscha BD, Schulze PC, Robbins JL, et al.
Implications of chronic heart failure on peripheral
vasculature and skeletal muscle before and after
exercise training. Heart Fail Rev 2008;13:21–37.
18. Peipoli MF. Exercise training in chronic heart failure:
mechanisms and therapies. Neth Heart J 2013;21:
85–90.
19. Gielen S, Schuler G, Adams V. Cardiovascular
effects of exercise training: molecular mecha-
nisms. Circulation 2010;122:1221–38.
20. Gielen S, Adams V, Mobius-Winkler S, et al. Anti-in-
flammatory effects of exercise training in the skel-
etal muscle of patients with chronic heart failure.
J Am Coll Cardiol 2003;42:861–8.
21. Tabet J, Meurin P, Driss AB, et al. Benefits of exer-
cise training in chronic heart failure. Arch Cardio-
vasc Dis 2009;102:721–30.
22. Mendes-Ribeiro AC, Mann GE, Meirelles LR, et al.
The role of exercise on L-arginine nitric oxide
pathway in chronic heart failure. Open Biochem J
2009;3:55–65.
23. Van Craenebroeck EM, Hoymans VY, Beckers PJ,
et al. Exercise training improves function of circu-
lating angiogenic cells in patients with chronic
heart failure. Basic Res Cardiol 2010;105:665–76.
24. Hambrecht MD, Hillbrich L, Erbs S, et al. Correc-
tion of endothelial dysfunction in chronic heart
failure: additional effects of exercise training and
oral L-arginine supplementation. J Am Coll Cardiol
2000;35:706–13.
25. Hambrecht R, Fiehn E, Weigl C, et al. Regular
physical exercise corrects endothelial dysfunction
and improves exercise capacity in patients with
chronic heart failure. Circulation 1998;98:2709–15.
26. Linke A, Schoene N, Gielen S, et al. Endothelial
dysfunction in patients with chronic heart failure:
systemic effects of lower-limb exercise training.
J Am Coll Cardiol 2001;37:392–7.
27. Hornig B, Maier V, Drexler H. Physical training im-
proves endothelial function in patients with chronic
heart failure. Circulation 1996;93:210–4.
28. Hambrecht R, Fiehn E, Yu J, et al. Effects of endur-
ance training on mitochondrial ultrastructure and
fiber type distribution in skeletal muscle of patients
with stable chronic heart failure. J Am Coll Cardiol
1997;29:1067–73.
29. Hambrecht R, Niebauer J, Fiehn E, et al. Physical
training in patients with stable chronic heart failure:
effects on cardiorespiratory fitness and ultrastruc-
tural abnormalities of leg muscles. J Am Coll
Cardiol 1995;25:1239–49.
30. Kao W, Helpern JA, Goldstein S, et al. Abnormal-
ities of skeletal muscle metabolism during nerve
stimulation determined by 31P nuclear magnetic
resonance spectroscopy in severe congestive
heart failure. Am J Cardiol 1995;76:606–9.
31. Van Der Ent M, Jeneson JA, Remme WJ, et al.
A non-invasive selective assessment of type I fibre
mitochondrial function using 31P NMR spectros-
copy. Evidence for impaired oxidative phosphory-
lation rate in skeletal muscle in patients with
chronic heart failure. Eur Heart J 1998;19:124–31.
32. Stassijns G, Lysens R, Decramer M. Peripheral and
respiratory muscles in chronic heart failure. Eur
Respir J 1996;9:2161–7.
33. Cohen-Solal A, Laperche T, Morvan D, et al. Pro-
longed kinetics of recovery of oxygen consumption
after maximal graded exercise in patients with
chronic heart failure. Analysis with gas exchange
measurements and NMR spectroscopy. Circulation
1995;91:2924–32.
Exercise Training and Adverse Events in Heart Failure 71
34. Belardinelli R, Barstow TJ, Nguyen P, et al. Skeletal
muscle oxygenation and oxygen uptake kinetics
following constant work rate exercise in chronic
congestive heart failure. Am J Cardiol 1997;80:
1319–24.
35. Vasileiadis I, Kravari M, Terrovitis J, et al. Interval
exercise training improves tissue oxygenation in
patients with chronic heart failure. World J Cardio-
vasc Dis 2013;3:301–7.
36. Adamopoulos S, Coats AJ, Brunotte F, et al. Phys-
ical training improves skeletal muscle metabolism
in patients with chronic heart failure. J Am Coll
Cardiol 1993;21:1101–6.
37. Gielen S, Sandri M, Kozarez I, et al. Exercise
training attenuates MuRF-1 expression in the skel-
etal muscle of patients with chronic heart failure
independent of age: the randomized Leipzig Exer-
cise Intervention in Chronic Heart Failure and
Aging catabolism study. Circulation 2012;125:
2716–27.
38. Adams V, Doring C, Schuler G. Impact of physical
exercise on alterations in the skeletal muscle in
patients with chronic heart failure. Front Biosci
2008;13:302–11.
39. Arena R, Myers J, Guazzi M. The clinical and
research applications of aerobic capacity and
ventilator efficiency in heart failure: an evidence-
based review. Heart Fail Rev 2008;13:245–69.
40. Balady GJ, Arena R, Sietsema K, et al, American
Heart Association Exercise, Cardiac Rehabilitation,
and Prevention Committee of the Council on Clin-
ical Cardiology, Council on Epidemiology and Pre-
vention, Council on Peripheral Vascular Disease,
Interdisciplinary Council on Quality of Care and
Outcomes Research. Clinicians guide to cardiopul-
monary exercise testing in adults: a scientific state-
ment from the American Heart Association.
Circulation 2010;122:191–225.
41. Ingle L. Theoretical rationale and practical recom-
mendations for cardiopulmonary exercise testing
in patients with chronic heart failure. Heart Fail
Rev 2007;12:12–22.
42. Myers J, Gademan M, Brunner K, et al. Effects of
high-intensity training on indices of ventilatory effi-
ciency in chronic heart failure. J Cardiopulm Reha-
bil Prev 2012;32:9–16.
43. Gademan MG, Swenne CA, Verwey HF, et al. Exer-
cise training increases oxygen uptake efficiency
slope in chronic heart failure. Eur J Cardiovasc
Prev Rehabil 2008;15:140–4.
44. Cahalin LP, Semigran MJ, Dec GW. Inspiratory
muscle training in patients with chronic heart failure
awaiting cardiac transplantation: results of a pilot
clinical trial. Phys Ther 1997;77:830–8.
45. Lin S, McElfresh J, Hall B, et al. Inspiratory muscle
training in patients with heart failure: a systematic
review. Cardiopulm Phys Ther J 2012;23:29–36.
46. Clark AL, Piepoli M, Coats AJ. Skeletal muscle and
the control of ventilation on exercise: evidence for
metabolic receptors. Eur J Clin Invest 1995;25:
299–305.
47. Ponikowski PP, Chua TP, FrancisDP, et al. Muscle er-
goreceptor overactivity reflects deterioration in clin-
ical status and cardiorespiratory reflex control in
chronic heart failure. Circulation 2001;104:2324–30.
48. Piepoli M, Clark AL, Volterrani M, et al. Contribution
of muscle afferents to the hemodynamic, auto-
nomic, and ventilator responses to exercise in pa-
tients with chronic heart failure: effects of physical
training. Circulation 1996;93:940–52.
49. Smart N, Marwick TH. Exercise training for patients
with heart failure: a systematic review of factors
that improve mortality and morbidity. Am J Med
2004;116(10):693–706. http://dx.doi.org/10.1016/j.
amjmed.2003.11.033.
50. O’Connor CM, Whellan DJ, Lee KL, et al. Efficacy
and safety of exercise training in patients with
chronic heart failure: HF-ACTION randomized
controlled trial. JAMA 2009;301(14):1439–50.
http://dx.doi.org/10.1001/jama.2009.454.
51. Keteyian SJ, Leifer ES, Houston-Miller N, et al.
Relation between volume of exercise and clinical
outcomes in patients with heart failure. J Am Coll
Cardiol 2012;60(19):1899–905. http://dx.doi.org/
10.1016/j.jacc.2012.08.958.
52. Reed SD, Whellan DJ, Li Y, et al. Economic evalua-
tion of the HF-ACTION (Heart Failure: A Controlled
Trial Investigating Outcomes of Exercise Training)
randomized controlled trial: an exercise training
study of patients with chronic heart failure. Circ Car-
diovasc Qual Outcomes 2010;3(4):374–81. http://
dx.doi.org/10.1161/CIRCOUTCOMES.109.907287.
53. Lawson GJ. Cardiac rehabilitation staffing. In:
Kraus WE, Keteyian SJ, editors. Contemporary
cardiology: cardiac rehabilitation. Totowa (NJ):
Humana Press; 2007. p. 277–87.
54. Whellan DJ, O’Connor CM, Lee KL, et al. Heart fail-
ure and a controlled trial investigating outcomes of
exercise training (HF-ACTION): design and ratio-
nale. Am Heart J 2007;153(2):201–11. http://dx.
doi.org/10.1016/j.ahj.2006.11.007.
55. National Heart Lung and Blood Institute. NHLBI
fact book, fiscal year 2008. [108]. Bethesda, MD:
National Institutes of Health. Available at: http://
www.nhlbi.nih.gov/files/docs/factbook/FactBook
2008.pdf.
56. Pina IL, Kokkinos P, Kao A, et al. Baseline differ-
ences in the HF-ACTION by sex. Am Heart J
2009;158:S16–23.
57. Pina IL, Bittner V, Clare RM, et al. Effects of exer-
cise training on outcomes in women with heart
failure: analysis of HF-ACTION (Heart Failure-A
Controlled Trial Investigating Outcomes of Exercise
Training) by sex. JACC Heart Fail 2014;2:180–6.
Myers et al72
58. Scott JM, Haykowsky MJ, Eggebeen J, et al. Reli-
ability of peak exercise testing in patients with
heart failure with preserved ejection fraction. Am
J Cardiol 2012;110:1809–13.
59. Gulati M, Pandey DK, Arnsdorf MF, et al. Exercise
capacity and the risk of death in women: the St
James women take heart project. Circulation
2003;108:1554–9.
60. Myers J, Prakash M, Froelicher V, et al. Exer-
cise capacity and mortality among men referred
for exercise testing. N Engl J Med 2002;346:
793–801.
61. Haykowsky MJ, Ezekowitz JA, Armstrong PW. Ther-
apeutic exercise for individuals with heart failure:
special attention to older women with heart failure.
J Card Fail 2004;10:165–73.
62. Haykowsky M, Vonder Muhll I, Ezekowitz J, et al.
Supervised exercise training improves aerobic
capacity and muscle strength in older women
with heart failure. Can J Cardiol 2005;21:1277–80.
63. Pu CT, Johnson MT, Forman DE, et al. Randomized
trial of progressive resistance training to counteract
the myopathy of chronic heart failure. J Appl Phys-
iol (1985) 2001;90:2341–50.
64. Tyni-Lenne R, Gordon A, Jansson E, et al. Skeletal
muscle endurance training improves peripheral
oxidative capacity, exercise tolerance, and health-
related quality of life in women with chronic
congestive heart failure secondary to either
ischemic cardiomyopathy or idiopathic dilated car-
diomyopathy. Am J Cardiol 1997;80:1025–9.
65. Gary RA, Sueta CA, Dougherty M, et al. Home-
based exercise improves functional performance
and quality of life in women with diastolic heart
failure. Heart Lung 2004;33:210–8.
66. Niederseer D, Thaler CW, Niederseer M, et al.
Mismatch between heart failure patients in clinical
trials and the real world. Int J Cardiol 2013;168:
1859–65.
67. Cleland JG, Swedberg K, Follath F, et al. The Euro-
heart failure survey programme– a survey on the
quality of care among patients with heart failure in
Europe. Part 1: patient characteristics and diag-
nosis. Eur Heart J 2003;24:442–63.
68. Lee DS, Gona P, Vasan RS, et al. Relation of disease
pathogenesis and risk factors to heart failure with
preserved or reduced ejection fraction: insights
from the Framingham Heart Study of the National
Heart, Lung, and Blood Institute. Circulation 2009;
119:3070–7.
69. Taylor RS, Sagar VA, Davies EJ, et al. Exercise-
based rehabilitation for heart failure. Cochrane
Database Syst Rev 2014;(4):CD003331. http://dx.
doi.org/10.1002/14651858.CD003331.pub4.
70. Flynn KE, Pina IL, Whellan DJ, et al. Effects of exer-
cise training on health status in patients with
chronic heart failure: HF-ACTION randomized
controlled trial. JAMA 2009;153:1451–9.