-
Prognosis and Palliative Care in COVID-19
IHA Grand Rounds 2 Apr 2020
Dr Kevin Wade, Palliative Care, KGH/CCSI Vicki Kennedy, CNS,
Interior Health Palliative & End of Life Care
-
Overview
1. Prognosis in Covid-19 2. Discussing Goals of Care 3. Health
Care Rationing 4. Non-ICU Supportive Management Orders
4/7/2020 2
-
Prognosis in COVID-19
4/7/2020
-
Prognosis in COVID-19 - Caveats
• Still early – detailed natural history and prognostic data at
each phase of illness are lacking
• Most reports so far represent raw case-fatality rates
4/7/2020 5
PresenterPresentation NotesCase fatality rates are subject to
biasUnderestimate by survivor delayOverestimate by not testing
asymptomatic or minimally symptomatic
This data is mostly useful as we lead into the discussion of
goals of care – the benefits of critical care and intubation may be
very small in elderly patients with multiple comorbidities
-
Prognosis in COVID-19 • Varies widely by country • 6,320 cases
including 66
deaths have been reported in Canada (PHAC, as of 1100hrs
30Mar2020)
• 935,957 cases including 47,245 deaths have been reported
worldwide (www.worldometers.info/coronavirus)
4/7/2020 6
1.0% Case-fatality rate
Canada
5.0% Case-fatality rate
Worldwide
PresenterPresentation NotesWHO Formal Case-Fatality Rate 3.4%,
from early March, based mainly on Chinese data
-
Prognosis in COVID-19 – By Age AGE ITALY
case-fatality rate (%)
CHINA case-fatality rate
(%) 80+ years old 20.2 14.8 70-79 years old 12.8 8.0 60-69 years
old 3.5 3.6 50-59 years old 1.0 1.3 40-49 years old 0.4 0.4 30-39
years old 0.3 0.2 20-29 years old 0 0.2 10-19 years old 0 0.2 0-9
years old 0 0.0 Overall 7.2 2.3
4/7/2020 7
Case-fatality rates by Age-group in Italy and China (Onder et
al., JAMA, 23Mar2020)
• Includes all confirmed cases
• Includes inpatients and outpatients
PresenterPresentation NotesItalian data as of 17Mar2020Chinese
data as of 11Feb2020Note that Italian data includes all deaths (of
any cause) in patients with Covid-19 confirmed on PCRItalian
testing strategy may have played a part – testing shifted to only
hospitalized patients
-
Prognosis in COVID-19 – By Age
Age distribution of patients with confirmed COVID-19 (Ruan et
al. Intensive Care Med, 2020)
4/7/2020 8
• Data from 150 inpatients in Wuhan, China
-
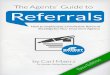
Prognosis in COVID-19 – ICU Survival
Interval from onset of symptoms to death (Ruan et al. Intensive
Care Med, 2020)
• Data from 68/150 inpatients who died in Wuhan, China
4/7/2020 9
Median 16 days from symptoms to death
2 peaks: 14 days and 22 days
PresenterPresentation NotesMedian time from ICU admission to
death is 7 days (Yang et al. Lancet Respir Med, 2020)
-
Prognosis in COVID-19 – Cause of Death
53% 32%
8% 7%
CAUSE OF DEATH
RespiratoryFailure
RespiratoryFailure andMyocardial InjuryMyocardial Injury
Unkown
• Data from 68/150 inpatients who died in Wuhan, China
Cause of death (Ruan et al. Intensive Care Med, 2020)
4/7/2020 10
-
Prognosis in the ICU
4/7/2020 11
• Data from 52 critically ill patients in Wuhan, China
Baseline Characteristics of Survivors and Non-Survivors (Yang et
al., Lancet Respir Med, 2020)
PresenterPresentation NotesWe still have not answered the
question of whether a given patient would benefit from intensive
care and intubationNeed to rearrange data from the Yang study, look
across rows rather than down columns
-
Prognosis in the ICU – By Age
4/7/2020 12
• 75% Mortality in ICU patients 60+ yo
• 90% Mortality in ICU patients 70+ yo
-
Prognosis in the ICU - Comorbidities
4/7/2020 13
• 100% mortality (0/7) in ICU patients with cerebrovascular
disease
• 78% Mortality (2/9) in ICU patients with diabetes
-
Prognosis in the ICU – Outcomes
Outcome of ICU Admission (Arentz et al. JAMA, 2020)
52%
10%
38%
Outcomes
Death
Transfer outof ICURemainCritically Ill
• Data from 21 critically Ill patients in Seattle
4/7/2020 14
PresenterPresentation NotesMean time to follow up of 7.5
days
-
Prognosis in COVID-19 - Summary • Case fatality rates are a
moving target, likely
somewhere between 1-5% • Prognosis for hospitalised patients
worse with
age • Prognosis for elderly and those with
comorbidities is very poor, even with aggressive
interventions
4/7/2020 15
PresenterPresentation NotesStatistics here support the value of
exploring patients goals and fears, especially with respect to
intubation and ventilation.Patients and families are influenced by
the media, and may be overly optimistic about the benefits of
critical care.
-
Discussing Goals of Care
4/7/2020
-
MOST Indicators – Our Current State C2 C1 C0 M3 M2 M1 No
MOST Population %
MOST/Pop.
All Ages
46,350 2,322 7,714 11,011 3,773 1,613 695,698 768,481 9.5
65+ 25,069 2,106 7,183 10,517 3,633 1,526 139,251 189,285
26.4
85+ 2,423 514 2,482 5,446 2,197 862 10,229 24,153 57.7
Reference: Interior Health insight, MOST Indicators report,
retrieved March 25 2020.
4/7/2020 17
PresenterPresentation NotesWe know from a BC 2016 public opinion
poll that only about 10% of people have talked to their doctor
about their health care wishes.
Of Interior Health’s 65+ population nearly 68% of people with a
MOST indicator have a C designation.
And 40% of people aged 85 and older with a MOST indicator have a
C designation.
In the midst of a COVID-19 pandemic this highlights the need to
address this and have conversations around goals of care, so we can
provide appropriate enhanced goal-concordant care to the population
who have been identified as most vulnerable to COVID-19. Benefits
of these conversations also include; better patient and family
coping, eased burden of decision-making for families, higher
patient satisfaction and improved quality of life.
Following that, we also need to consider triaging appropriately
– so those people who are not offered life-sustaining measures are
cared for appropriately and provided appropriate symptom
management.
A publication from Arya et al., hot off the press from last
month stated: “In a triage situation our obligation to provide
palliative care for those denied life-sustaining measures is
increased”.
-
Discussing Goals of Care in Serious Illness
• Current Time • Necessary • Earlier the better • Palliative
Care is a ‘Team Sport’ • Purpose is not to establish a new MOST
status,
but if the discussion naturally flows in this direction, explore
this in your recommendations.
4/7/2020 18
PresenterPresentation NotesGoals of Care conversations are about
the hear and now.In a perfect world everyone would be comfortable
thinking and talking about their mortality, that death is a part of
living and the circle of life. Everyone would have an Advance Care
Plan, have had meaningful and real discussions with their families
in advance, not only if they had a serious illness, but also
thinking about ‘What If?’….kind of like insurance. And to top it
off everyone would have formal and perhaps legal documentation
completed.
This would be certainly helpful for the population and health
care professionals in these extraordinary times where the COVID-19
pandemic is resulting in significant fear, anxiety, and unknowns.
It would help to inform and provide understanding and context in
Goals of Care discussions, considering the current circumstances,
so that we are providing goal-concordant care.
The reality may be that we are not quite there yet…… which means
now in a pandemic, Goals of Care discussions are necessary, they
may be initial discussions, so the earlier Goals of Care
conversations are held when a person is suspected of having COVID,
and particularly when they are older and have a serious illness –
the better.
Knowing that Palliative Care is a “Team Sport”, this is an
important time for collaboration, communication and documentation
amongst inter-professional team members. The key components of
these conversations can be shared amongst the team and must be
communicated amongst the team.
The purpose of discussing Goals of Care is not to establish a
new MOST status BUT if the discussion naturally goes in that
direction, then explore that in your recommendations.
-
Principles of Goals of Care discussions
• Person-centered and purpose-oriented • You will not harm your
patient by talking about
their illness and the importance of planning • Anxiety is normal
for both patients and
clinicians - acknowledge and validate the emotion(s)
• People want and need the truth about their prognosis to make
informed decisions
4/7/2020 19
PresenterPresentation NotesPerson-centered and purpose-oriented:
A publication from Kaldjian stated that “By making the patient’s
most important goals of care the conversational focal point,
decision making is patient-centered, purpose-oriented, and premised
on the patient’s beliefs, values, priorities, preferences, and
circumstances.”
You will not Harm your patient by talking about their
illness:Ariadne (Dr. Gawande – founding ED) have found that “People
who think through what is important to them and what their wishes
are often feel less anxious, more at peace, and more in
control”.
Anxiety is normal for both patients and clinicians – it is
important to be compassionate, acknowledge and validate emotions
that arise before and to enable you to move forward.
People want and need the truth: “The hallmarks of a successful
goals of care discussion is that it allows everyone to take a step
back from the intense focus, by considering the broader purpose and
context of the intervention.” So specifically on whether the
patient knows and understands all the possible outcomes (including
lack of benefit and prolonged rehabilitation), and would want
intubation and ventilation in the case of a COVID infection.
“Goal-oriented discussions take a larger, longer view. Framed by
goals of care, conversation about decision making moves the
question from “Would you like us to do this, ornot?” to “Will this
help us achieve your goals of care, or not?” (Kaldjian, 2019)
“The central practical concern is to identify and discuss goals
that should be pursued and the means most likely to accomplish
them. These discussions should allow us to understand patients well
enough to know what matters most to them”
-
Identifying those at high risk • Surprise Question • Clinical
Frailty Scale • SPICT • Others….
4/7/2020 20
PresenterPresentation NotesNow you know the populations at risk,
there are many tools available to help identify these people who
would particularly benefit from discussing Goals of Care.
The Position Statement from Dr. Kow from the UBC Division of
Geriatric Medicine Position on Frailty and ICU candidacy released
last month indicated that people with a CFS score of 5 (mildly
frail) or more have a typically poor prognosis if hospitalized for
COVID-19.
https://www.google.ca/url?sa=i&url=https://twitter.com/ktcanada&psig=AOvVaw1s_E49pfpPkyUREzik6YZT&ust=1585872133075000&source=images&cd=vfe&ved=0CAIQjRxqFwoTCKCWqKO4yOgCFQAAAAAdAAAAABAD
-
Elements of a Serious Illness Conversation
• Set up the conversation – asking permission • Assess
understanding & information preferences • Share prognosis –
“Wish/Worry”, “Hope/Worry” • Explore key topics – goals, fears,
sources of strength,
family • Close the conversation – Recommendation “I’ve
heard you say...” • Communicate and Document with key health
care
team members
4/7/2020 21
PresenterPresentation NotesThe literature has demonstrated that
Conversations often fail to address key elements of quality
discussions.Fortunately, adaptations of Ariadne Labs SICG, specific
to COVID have been created and made available to clinicians through
UBC and the BC Center for Palliative Care. These tools identify the
key elements and provide patient tested language which they
understand, will resonate and evokes a response. The Key elements
are: Setting up the conversation. This builds trust and gives the
patient control by gaining the person’s permission to proceed with
the discussion
Assessing understanding of their illness (where they are right
now and what further changes lie ahead for them) and preferences
for information on what is likely ahead allows the clinician to
provide the desired information and gives the clinician confidence
to proceed with a difficult discussion
Sharing prognosis to the degree desired by the person and within
limits known to the clinician, is a responsibility of clinicians,
and enable patients to factor this information into their goals of
care decisions. Framing this as a ‘Wish/Worry’, ‘Hope/Worry’
statement enables the clinician to align with the patients hopes,
acknowledge their concerns, and be truthful while being
sensitive.
Exploring Key Topics such as; Goals, Fears, Sources of Strength
and what their Family knows about what is important to them helps
to articulate their goals of care. All patients have goals besides
living longer. Understanding patient goals aids the clinician in
tailoring recommendations to address the person’s priorities.
Closing the conversation with Recommendations summarizing what
you heard them say and provides recommendations in regards to their
Wellbeing, their Illness and their Support System and reassures you
will help them.
Finally, Communicating and Documenting the conversation ensures
the health care team know about the discussion that took place.
Extra info just in case needed: What would you like to know
about your illness, COVID-19, and what may happen if you were sick?
What information do you need to help you make decisions about your
future? How do you like to make decisions? Who would you like to
help you? What are you afraid of about your illness and
COVID-19?
Are there some kinds of medical care you may not want? What
makes you feel that way? How do you feel about sharing these
thoughts and feelings with the people who support you? If you have
not already asked someone to be your substitute decision maker, who
could fill that role?
-
Adapting to different clinical situations • If the patient is an
ICU candidate
– Function – Trade-offs
• Patient/Family insists on ICU despite it not being an option –
Consult – Re-iterate focus – Wish/Worry, Hope/Worry framework –
Offer ongoing support
4/7/2020 22
PresenterPresentation NotesThese SIC tools provide adaptations
for different clinical situations. If a person is an ICU candidate,
it would important to explore the topic of Function and
Trade-Offs.
Patients view impairment in function differently & make
choices based on these perspectives. “What abilities are so
critical to your life that you can’t imagine living without them”
OR “What does meaningful quality of life look like to you?”
And allowing to reflect on trade-offs that might be necessary to
achieve different outcomes promotes informed decision-making.“If
you become sicker, how much are you willing to go through for the
possibility of gaining more time?” (i.e. in the case of COVID
infection, are they willing to go through intubation, ventilation
and a potentially prolonged ICU stay for the possibility of
survival?)
When a patient/family insists on ICU despite it not being an
option:
• Consider requesting a consult from ICU, so they can share
their perspective with the family.• Re-iterate/Focus on the active
medical treatments that you will continue to provide to the
patient, and Frame ICU in terms of the prolongation of suffering as
opposed to provision of cure.• Use wish/worry/wonder: "I wish this
weren't the case, but I worry that if we bring you to the ICU, you
will suffer more. I wonder if we can take this opportunity to
ensure you have a peaceful death."• Offer ongoing support: “We will
be here for you/your loved one no matter what happens”
-
Ethical Framework
23
PresenterPresentation NotesThis is an excellent framework that
can guide health care professionals, and demonstrates that the
perspectives and input of the patient, family and health care team
are integral and equally important components to formulate goals of
care.
-
Goals of Care - Billing • Multiple codes now allowed by
Telehealth • 14063 (Palliative Care Planning Fee)
• For patients in community or assisted living • Must qualify
for palliative care benefits program • Not for patients in
residential/long term care • 30min minimum • $100
24 4/7/2020
PresenterPresentation NotesPractical applications – advance care
planning is important both to your patients and for the health care
system as a whole
-
Goals of Care - Billing • Multiple codes now allowed by
Telehealth • 14033 (Complex Care Management Fee)
• Payable once per year for patients with 2 or more
comorbidities in community or assisted living
• Must develop complex care plan incorporating patients values
and goals
• $315
25 4/7/2020
-
Goals of Care - Billing • Multiple codes now allowed by
Telehealth • 14077 (Facility Patient Conference Fee)
• To discuss goals of care with specialists or the
interprofessional care team
• $40/15min increment
26 4/7/2020
-
Goals of Care - Billing • Multiple codes now allowed by
Telehealth • 00114 (Long Term Care Facility Visit)
– Typically payable once every 2 weeks – $35.86
• 00127 (Terminal Care Facility Visit) – Payable in last 6mo of
life – May use for virtual visit with patient, or with RN/LPN
if patient unable to use phone – $53.20
27 4/7/2020
-
Health Care Rationing
4/7/2020
-
Health Care Rationing
• Rationing and allocation of resources are very different from
discussing and providing goal-concordant palliative care
• Dangerous to conflate these two processes
4/7/2020 29
PresenterPresentation NotesMedia and public focus has been very
intent on rationing and the idea that patients will not have a
ventilator availableWe need to be conscious of this when discussing
goals of care – this is about what people want and will benefit
from, not about what they can getFailure in this may lead to a loss
of trust in caregivers and especially in decisions re goals of
care
-
Health Care Rationing - Principles • Many existing
frameworks
– Pittsburgh (White et al. Ann Intern Med 2010) – Maryland
(Daugherty Biddison et al. Chest 2019) – New York Ventilator
Allocation Guidelines (Zucker
et al., 2015) • “Soft utilitarianism” • Emphasize prioritization
of short term survival
(eg SOFA score) over long term prognosis
4/7/2020 30
PresenterPresentation NotesNew York developed Ventilator
Allocation Guidelines in 2015Eg by using SOFA score for short term
survivalGoal is to avoid excluding certain groups (eg the elderly
or disabled) arbitrarily
-
Health Care Rationing - Application • Rationing decisions are
not made by the
treating clinician due to the stress and moral injury it
imparts
• Separate “Triage Committees” decide on allocations by applying
a framework or score
4/7/2020 31
PresenterPresentation NotesTriage committees usually consist of
intensivists, ethicists, palliative care physicians - often similar
to ethics committees
-
Symptom Management outside the ICU
4/7/2020
-
Hospital Transfer
4/7/2020 33
-
Symptom Management - Principles 1. Ensure all patients receive
care 2. Avoid harm 3. Reduce suffering by providing appropriate
symptom control (esp of dyspnea) 4. Protect health care staff 5.
Support families 6. Conserve resources (eg PPE, medications)
4/7/2020 34
PresenterPresentation NotesFor symptom management outside the
ICUNot necessarily restricted to expected EOL patients
-
Dyspnea • Oxygen up to 6Lpm without generating
aerosols (Hendin et al., CJEM, 2020) • Avoid use of fans • Avoid
nebulizers, CPAP, BiPAP • No evidence for bronchodilators/ICS
unless
patient has underlying asthma/COPD
4/7/2020 35
PresenterPresentation NotesSome sources alternately say 15Lpm
(VCH guidelines) – err on the side of caution given the lack of
evidence for symptomatic benefitMed shortages of MDIs –
salbutamol/atrovent both very short, don’t use for placebo
effectTolerate some hypoxia – won’t increase their dyspnea
-
Dyspnea Opioids – Opioid Naive
• Morphine 2.5-5mg PO Q1H PRN • Morphine 1-2mg IV/SC Q30min PRN
Or • HydroMORPHONE 0.5-1mg PO Q1H PRN • HydroMORPHONE 0.25-0.5mg
IV/SC Q30min
PRN • Review often, start Q4H scheduled if using frequent
PRNs
36 4/7/2020
PresenterPresentation NotesAllow nursing staff to determine
appropriate route based on patient assessment and riskSporadic
reports of medication shortages esp parenteral hydromorphone in
IHA, so use morphine in appropriate patients (younger w/ no renal
impairment and no allergy)
Not necessarily only for expected EOL patients (ie M1/M2) – may
also use in M3No evidence of increased mortality with low dose
opioids in end stage COPD or pulmonary fibrosis, but evidence of
increased mortality in acute decompensated CHFChoose wisely,
discuss goals of care with patient
-
Dyspnea Opioids – Opioid Tolerant
• Calculate total daily dose
• Give breakthrough dose as 10% of the total daily dose, IV/SC
Q30min PRN
4/7/2020 37
PresenterPresentation NotesUse of long-acting opioids is
unclear, most patients seem to progress quickly to EOLFentanyl
patch 12mcg/hrHydromorph-Contin 3mg PO BIDKadian 10-30mg PO
Daily
-
Dyspnea • Consider transition to opioid continuous
IV/SC infusion if still taking frequent PRNs on top of regular
dosing
• Minimizes risk to nursing staff from frequent dosing
• Talk to local nursing leads – easier than you think • Consult
palliative care for help
– Provincial hotline 1-877-711-5757
38 4/7/2020
PresenterPresentation NotesAll parenteral opioids can be given
as infusions – via CADD pump or IV pump – incl fentanyl, morphine,
hydromorphone
-
Dyspnea • Consider palliative sedation if refractory
dyspnea with patient distress • Midazolam 1-4mg/hr CSCI •
Methotrimeprazine 5-25mg Q8H and Q3H
PRN • Protocol and order set pending approval
39 4/7/2020
PresenterPresentation NotesCJEM article mentions dissociative
dose ketamine as a temporizing measure until opioids take
effect
-
Respiratory Congestion • For copious airway secretions •
Glycopyrrolate 0.4mg IV/SC Q4H PRN • Atropine 0.6mg SC Q6H PRN •
Atropine 1% (ophthalmic drops) 1-2 drops
SL Q4H PRN
40 4/7/2020
PresenterPresentation NotesSome notes mention scopolamine subcut
or patch, less used in BC (much more widely used in Ontario), can
be associated with delirium
-
Other Symptoms Pain
• Morphine 2.5-5mg IV/SC Q1H PRN • HydroMORPHONE 0.5-1mg IV/SC
Q1H PRN
Fever • Acetaminophen 650mg PO/PR Q4H PRN
Agitation • Haloperidol 0.5-1mg IV/SC Q3H PRN •
Methotrimeprazine 12.5-25mg SC Q4H PRN • Midazolam 0.5-1mg IV/SC
Q30min PRN
41 4/7/2020
PresenterPresentation NotesGenerally pain dose is double the
dyspnea dose of the equivalent medication and route
-
Symptom Management - Summary
4/7/2020 42
“All patients must be cared for”
https://palliativecare.med.ubc.ca/coronavirus/
4/7/2020
https://palliativecare.med.ubc.ca/coronavirus/https://palliativecare.med.ubc.ca/coronavirus/
-
Conclusion • Establish goals of care early – ideally before
any infection or decline, at their current place of care
• Many patients will not benefit from critical care measures
• Care for every patient, every time
4/7/2020 43
-
Questions?
• Kevin Wade • [email protected] • 604-379-1655
• Vicki Kennedy • [email protected] •
250-212-7807
4/7/2020 44
mailto:[email protected]:[email protected]
Prognosis and Palliative Care in COVID-19OverviewSlide Number
3Prognosis in COVID-19Prognosis in COVID-19 - CaveatsPrognosis in
COVID-19Prognosis in COVID-19 – By AgePrognosis in COVID-19 – By
AgePrognosis in COVID-19 – ICU SurvivalPrognosis in COVID-19 –
Cause of DeathPrognosis in the ICUPrognosis in the ICU – By
AgePrognosis in the ICU - ComorbiditiesPrognosis in the ICU –
OutcomesPrognosis in COVID-19 - SummaryDiscussing Goals of CareMOST
Indicators – Our Current StateDiscussing Goals of Care in Serious
IllnessPrinciples of Goals of Care discussionsIdentifying those at
high riskElements of a Serious Illness ConversationAdapting to
different clinical situationsEthical FrameworkGoals of Care -
BillingGoals of Care - BillingGoals of Care - BillingGoals of Care
- BillingHealth Care RationingHealth Care RationingHealth Care
Rationing - PrinciplesHealth Care Rationing - ApplicationSymptom
Management outside the ICUHospital TransferSymptom Management -
PrinciplesDyspneaDyspneaDyspneaDyspneaDyspneaRespiratory
CongestionOther SymptomsSymptom Management -
SummaryConclusionQuestions?